




C
1282 Meta-analysis
Comparison between angioten
sin-converting enzymeinhibitors and angiotensin receptor blockers on the riskof myocardial infarction, stroke and death: a meta-analysisGianpaolo Reboldia, Fabio Angelib, Claudio Cavallinib, Giorgio Gentilea,Giuseppe Manciac and Paolo VerdecchiabObjectives To compare the effects of angiotensin II
receptor blockers and angiotensin-converting enzyme
inhibitors on the risk of myocardial infarction, stroke,
cardiovascular mortality and total mortality.
Methods We conducted a meta-analysis of randomized
comparative trials between angiotensin II receptor blockers
and angiotensin-converting enzyme inhibitors. Inclusion
criteria were publication in peer-reviewed journals indexed
in Medline, randomized comparison of angiotensin II
receptor blockers vs. angiotensin-converting enzyme
inhibitors, or angiotensin II receptor
blockers R angiotensin-converting enzyme inhibitors vs.
angiotensin-converting enzyme inhibitors, report of major
complications including myocardial infarction, stroke,
cardiovascular mortality or all-cause mortality; average
follow-up of at least 1 year in at least 200 patients.
Results Six trials fulfilled the inclusion criteria, for a total of
49 924 patients. In the pooled estimate, there were no
significant differences between angiotensin II receptor
blockers and angiotensin-converting enzyme inhibitors on
the risk of myocardial infarction (odds ratio 1.01; 95%
confidence interval 0.95–1.07; P U 0.75), cardiovascular
mortality (odds ratio 1.03; 95% confidence interval 0.98–
1.08; P U 0.23) and total mortality (odds ratio 1.03; 95%
confidence interval 0.97–1.10; P U 0.20). This was the case
also when the analysis involved only the comparison
between angiotensin-converting enzyme inhibitors and
angiotensin II receptor blockers. Overall, the risk of stroke
was slightly lower with angiotensin II receptor blockers than
angiotensin-converting enzyme inhibitors (odds ratio 0.92;
95% confidence interval 0.85–0.99; P U 0.037), the direct
opyright © Lippincott Williams & Wilkins. Unautho
0263-6352 � 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins
angiotensin-converting enzyme inhibitors and angiotensin II
receptor blockers comparison showing a nonsignificant
trend in a similar direction. Statistical heterogeneity among
trials was not significant, with a low to null inconsistency
statistic, for stroke (P U 0.67), myocardial infarction
(P U 0.86), cardiovascular mortality (P U 0.14) and total
mortality (P U 0.12).
Conclusion This overview suggests that angiotensin II
receptor blockers are as effective as angiotensin-converting
enzyme inhibitors on the risk of myocardial infarction,
cardiovascular mortality and total mortality. Angiotensin II
receptor blockers may be slightly more protective than
angiotensin-converting enzyme inhibitors on the risk of
stroke. J Hypertens 26:1282–1289 Q 2008 Wolters Kluwer
Health | Lippincott Williams & Wilkins.
Journal of Hypertension 2008, 26:1282–1289
Keywords: hypertension, meta-analysis, mortality, myocardial infarction,prevention, prognosis, stroke, therapy
Abbreviations: ACEIs, Angiotensin converting enzyme inhibitors; ARBs,Angiotensin receptor blockers; AT1, Angiotensyn type I; AT2, Angiotensintype II; BP, Blood Pressure; CHF, Congestive heart failure; CI, Confidenceinterval; MI, Myocardial infarction; RCTs, Randomised clinical trials
aDepartment of Internal Medicine, University of Perugia, bDepartment ofCardiology, Hospital ‘Santa Maria della Misericordia’, Perugia and cDepartment ofMedicine, University of Milano-Bicocca, Milan, Italy
Correspondence to Paolo Verdecchia, MD, FACC, FAHA, Clinical Research Unit‘Preventive Cardiology’, Department of Cardiology, Hospital ‘Santa Maria dellaMisericordia’, 06156 Perugia, ItalyE-mail: [email protected]
Received 16 April 2008 Revised 28 April 2008Accepted 30 April 2008
IntroductionAngiotensin-converting enzyme inhibitors (ACEIs) and
angiotensin II receptor blockers (ARBs) are widely used
in patients with hypertension, heart failure and diabetes
as well as in a wide spectrum of other clinical conditions
sharing an increased cardiovascular risk [1]. Individual
trials and meta-analyses showed that both ACEIs and
ARBs are effective in reducing the risk of total cardio-
vascular events and specific events [2,3] such as stroke,
myocardial infarction (MI) and heart failure. Further-
more, two systematic overviews [4,5] suggested that part
of the protective effects of ACEIs on coronary artery
disease may be independent of the degree of blood
pressure (BP) reduction, which appeared to explain,
however, the greater proportion of the benefit exerted
by these drugs.
Randomized comparative trials between ACEIs and ARBs
have been relatively rare and largely limited to specific
clinical conditions such as heart failure and a post-MI state
accompanied by left ventricular dysfunction [6–10]. This
has hindered information on a clinically important issue
because ACEIs and ARBs act on the renin–angiotensin
system at different levels, and experimental data suggest
rized reproduction of this article is prohibited.

C
Comparison between ACEIs and angiotensin receptor blockers Reboldi et al. 1283
that such a difference might translate into a different
clinical outcome. For example, the increased levels of
bradykinin associated with the administration of ACEIs
but not, at least to a significant degree, with that of ARBs
might exert specific cardioprotective effects [11]. Further-
more, overstimulation of type 2 (AT2) receptors by the
increased levels of angiotensin II associated with long-
term selective blockade of type 1 (AT1) receptors might
trigger apoptosis, inhibit angiogenesis and reduce the
synthesis of fibrotic tissue [12–14]; these effects could
potentially lead to a depressed growth of collateral vessels
in the setting of ischemia as well as to a reduced collagen
content, a thinner cap and a greater vulnerability of ather-
omas to rupture [15]. Finally, unopposed overstimulation
of AT2 receptors could have protective cerebrovascular
effects by increasing recruitment of collateral vessels and
enhancing resistance of neurons to anoxia [16,17]. Indeed,
that differences in clinical outcome between ACEIs and
ARBs may exist is in line with the results of some clinical
trials in which ACEIs or ARBs were compared with other
antihypertensive treatments. One, on the basis of an
examination of selected trials, the hypothesis has been
advanced that ARBs reduce the risk of MI to a lesser
degree than that of obtained with other antihypertensive
drugs [18]. Two, some trials [19,20] have shown ARBs to
exert a greater protective effect against stroke than beta-
blockers and calcium antagonists for a similar reduction in
BP. The data provided by trials, and their systematic
overviews, are not entirely consistent, however [21–26].
The recent publication [26] of the results of a large trial
on patients at high cardiovascular risk with or without
hypertension who were randomized to an ARB or an
ACEI has substantially increased the availability of data
comparing these two treatments, and expanded it beyond
specific conditions such as heart failure and MI with left
ventricular dysfunction. We have included this trial in a
meta-analysis of randomized clinical trials comparing
ACEIs and ARBs for their ability to affect the incidence
of total and specific cardiovascular events, and this study
reports the results.
MethodsWe searched for randomized controlled outcome trials
which met all of the following prespecified criteria;
comparison between ARBs and ACEIs regardless of
the background therapy in either group, publication in
peer-reviewed journals indexed in Medline, MI, stroke,
cardiovascular mortality and total mortality as prespeci-
fied events, although not necessarily a primary endpoint,
follow-up of at least 1 year, total sample size of 200
patients or more. Some of the trials did not report
completely the total number of patients who developed
cardiovascular or coronary events, as well as the number
of those with congestive heart failure (CHF). Further-
more, CHF was absent at entry in some trials [10,26],
but not in others [6–9]. Therefore, these important
opyright © Lippincott Williams & Wilkins. Unauth
clinical outcomes were not included in our overview
(see Discussion).
We searched for eligible studies through Medline, using
research Methodology Filters [27].
The search identified six trials [6–11], which fulfilled all
inclusion criteria. Data were extracted on the basis of an
intention-to-treat approach. Discrepancies were resolved
in conference.
We accepted the definition of MI, stroke, cardiovascular
mortality and total mortality as reported in the eligible
trials. The number of patients with MI and stroke (fatal
and nonfatal events) in the valsartan-treated patients
recruited for acute myocardial infarction (VALIANT)
trial was not reported in the original article [9], but
published later [28].
We calculated odds ratios (ORs) and 95% confidence
intervals (CIs) for stroke, MI, cardiovascular mortality
and total mortality for each trial according to fixed and
random-effect models, and we undertook a series of
‘head-to-head’ meta-analyses [29]. For multiarm trials,
we analyzed only preplanned comparisons defined in the
original study design [29]. Thus, each meta-analysis
included two subgroups formed by the comparison of
ARBs vs. ACEIs [6–10,26] or ARBsþACEIs vs. ACEIs
[9,26]. The statistical significance of subgroup inter-
actions and heterogeneity between groups was assessed
[29]. Comparisons not included in the original study
protocol were not performed. We tested the null hypo-
thesis of homogeneity by the chi-squared test. Pooled
estimates were assessed for heterogeneity by computing
the I2 statistic. Typically, values above 50% are deemed
to suggest large between-study heterogeneity, values of
25–50% are deemed to show modest heterogeneity, and
values below 25% denote low heterogeneity [30].
We assessed the influence of individual studies on pooled
estimates by excluding one study at the time according to
Tobias’ method [31]. If the point estimate of the pooled
effect with one study omitted lies outside the CI of the
overall estimate with all available trials contributing, then
the study in question has an excessive influence.
The Jadad’s score was used to assess the methodological
quality of the randomized controlled trials included in our
systematic review [32]. This validated score lies in the
range of 0–5. Studies are scored according to the presence
of three key methodological features of randomization,
blinding and accountability of all patients, including
withdrawals [32].
Analyses were done using Stata, version 10 (StataCorp
LP, College Station, Texas, USA) and R version 2.6.2
(R Foundation for Statistical Computing, Vienna, Austria).
orized reproduction of this article is prohibited.
C
1284 Journal of Hypertension 2008, Vol 26 No 7
Table 1 Randomized comparative trials between ARBs and ACEIs
Study ARB ACEIPublication
yearFollow-up
yearsPatients in the
ARB armPatients in the
ACEI armJadad’sScore
ELITE [6] Losartan Captopril 1997 1 352 370 4ELITE-II [7] Losartan Captopril 2000 1.5 1578 1574 5OPTIMAAL [8] Losartan Captopril 2002 2.7 2744 2733 5VALIANT/Val [9,28] Valsartan Captopril 2003, 2006 2.1 4909 4909 5VALIANT/ValþCap [9,28] Valsartan Captopril 2003, 2006 2.1 4885 4909DETAIL [10] Telmisartan Enalapril 2004 5 120 130 4ONTARGET/Tel [26] Telmisartan Ramipril 2008 4.7 8542 8576 5ONTARGET/Tel + Ram [26] Telmisartan Ramipril 2008 4.7 8502 8576
ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; DETAIL, diabetics exposed to telmisartan and enalapril; ELITE, evaluation of losartan inthe elderly study; ELITE-II, losartan heart failure survival study; ONTARGET, the ongoing telmisartan alone and in combination with ramipril global endpoint trial; OPTIMAAL,optimal trial in myocardial infarction with the angiotensin II antagonist losartan; Tel, telmisartan vs. ramipril; Tel+Ram, telmisartanþ ramipril vs. ramipril; Val, valsartan vs.caproptil; ValþCap, valsartanþ captopril vs. captopril; VALIANT, valsartan in acute myocardial infarction study.
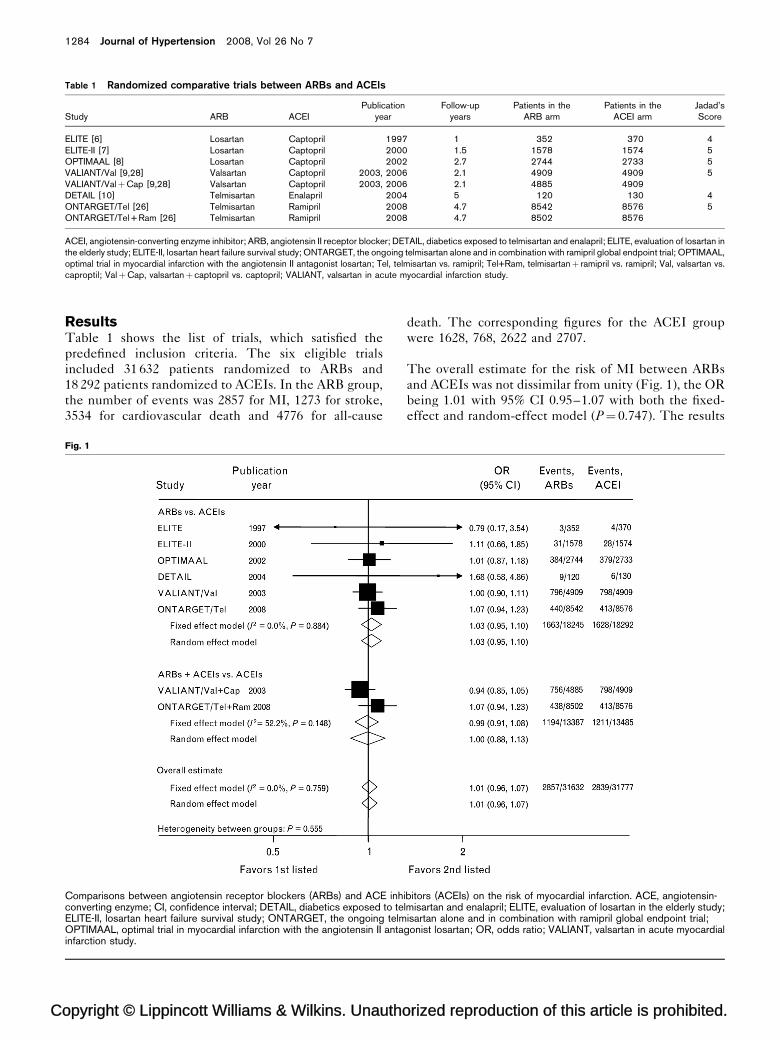
ResultsTable 1 shows the list of trials, which satisfied the
predefined inclusion criteria. The six eligible trials
included 31 632 patients randomized to ARBs and
18 292 patients randomized to ACEIs. In the ARB group,
the number of events was 2857 for MI, 1273 for stroke,
3534 for cardiovascular death and 4776 for all-cause
opyright © Lippincott Williams & Wilkins. Unautho
Fig. 1
Comparisons between angiotensin receptor blockers (ARBs) and ACE inhconverting enzyme; CI, confidence interval; DETAIL, diabetics exposed to teELITE-II, losartan heart failure survival study; ONTARGET, the ongoing telmOPTIMAAL, optimal trial in myocardial infarction with the angiotensin II antainfarction study.
death. The corresponding figures for the ACEI group
were 1628, 768, 2622 and 2707.
The overall estimate for the risk of MI between ARBs
and ACEIs was not dissimilar from unity (Fig. 1), the OR
being 1.01 with 95% CI 0.95–1.07 with both the fixed-
effect and random-effect model (P¼ 0.747). The results
rized reproduction of this article is prohibited.
ibitors (ACEIs) on the risk of myocardial infarction. ACE, angiotensin-lmisartan and enalapril; ELITE, evaluation of losartan in the elderly study;isartan alone and in combination with ramipril global endpoint trial;
gonist losartan; OR, odds ratio; VALIANT, valsartan in acute myocardial
C
Comparison between ACEIs and angiotensin receptor blockers Reboldi et al. 1285
Fig. 2
Comparisons between angiotensin receptor blockers (ARBs) and ACE inhibitors (ACEIs) on the risk of cardiovascular mortality. ACE, angiotensin-converting enzyme; CI, confidence interval; DETAIL, diabetics exposed to telmisartan and enalapril; ELITE, evaluation of losartan in the elderly study;ELITE-II, losartan heart failure survival study; ONTARGET, the ongoing telmisartan alone and in combination with ramipril global endpoint trial;OPTIMAAL, optimal trial in myocardial infarction with the angiotensin II antagonist losartan; OR, odds ratio; VALIANT, valsartan in acute myocardialinfarction study.
were similar also for the separate subgroup analyses of
ARBs vs. ACEIs and ARBsþACEIs vs. ACEIs, with a
low to null heterogeneity across the trials (P¼ 0.769,
I2¼ 0%) and no evidence of heterogeneity or interaction
between subgroups.
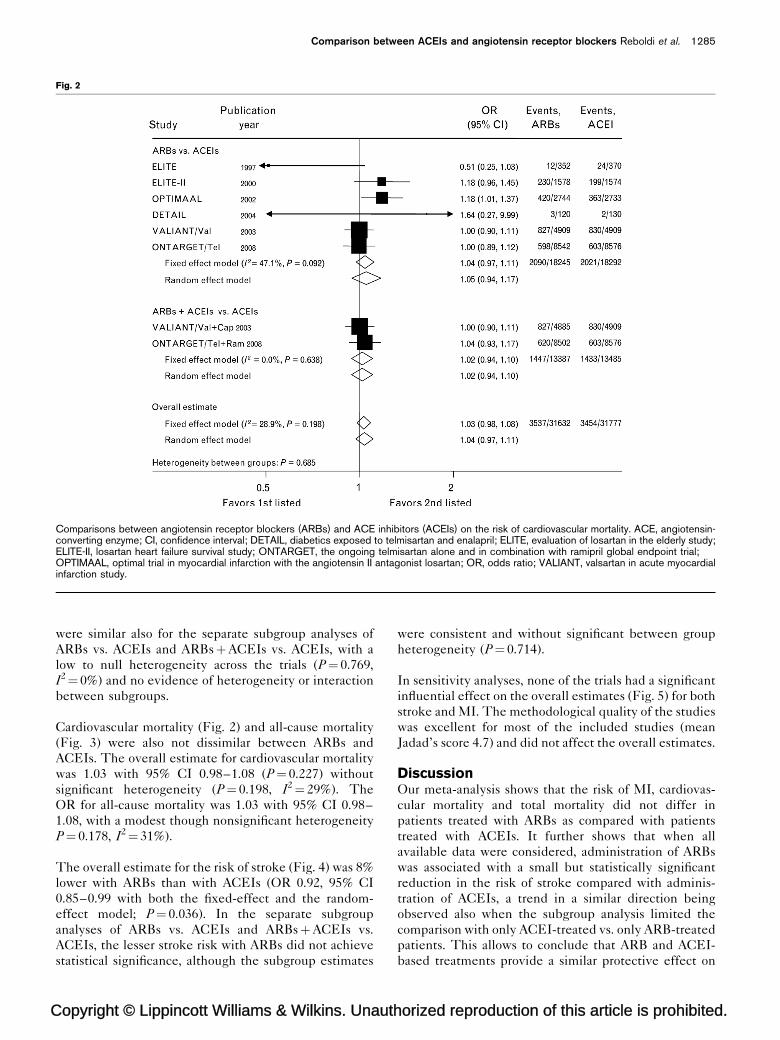
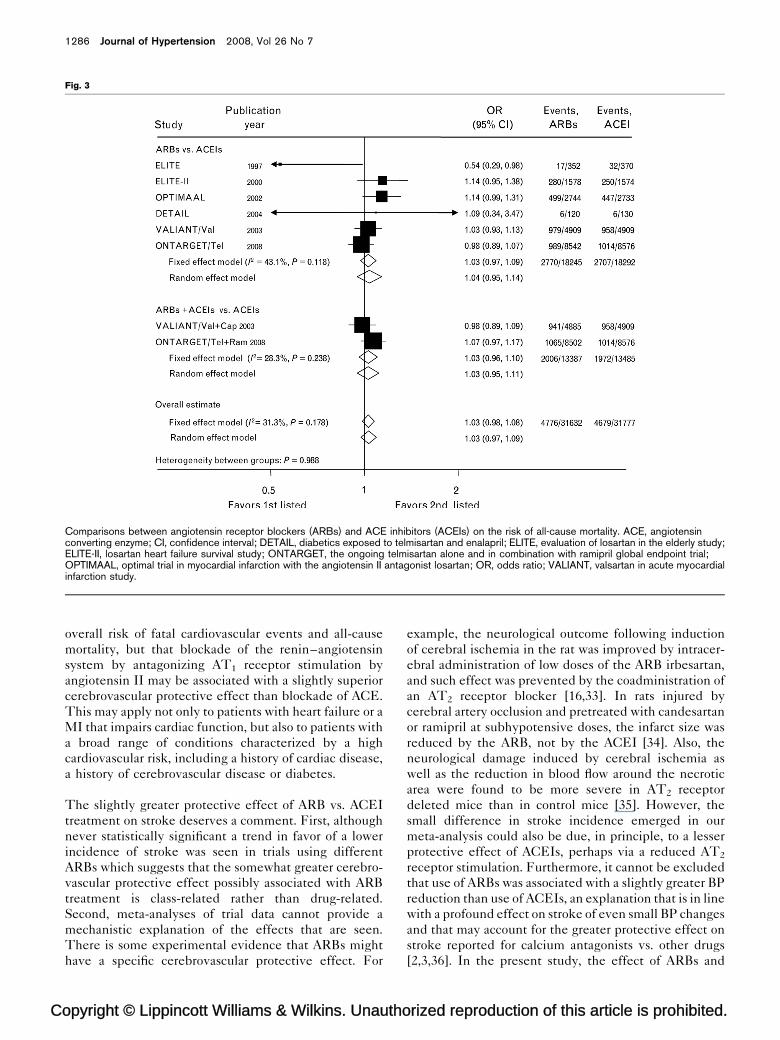
Cardiovascular mortality (Fig. 2) and all-cause mortality
(Fig. 3) were also not dissimilar between ARBs and
ACEIs. The overall estimate for cardiovascular mortality
was 1.03 with 95% CI 0.98–1.08 (P¼ 0.227) without
significant heterogeneity (P¼ 0.198, I2¼ 29%). The
OR for all-cause mortality was 1.03 with 95% CI 0.98–
1.08, with a modest though nonsignificant heterogeneity
P¼ 0.178, I2¼ 31%).
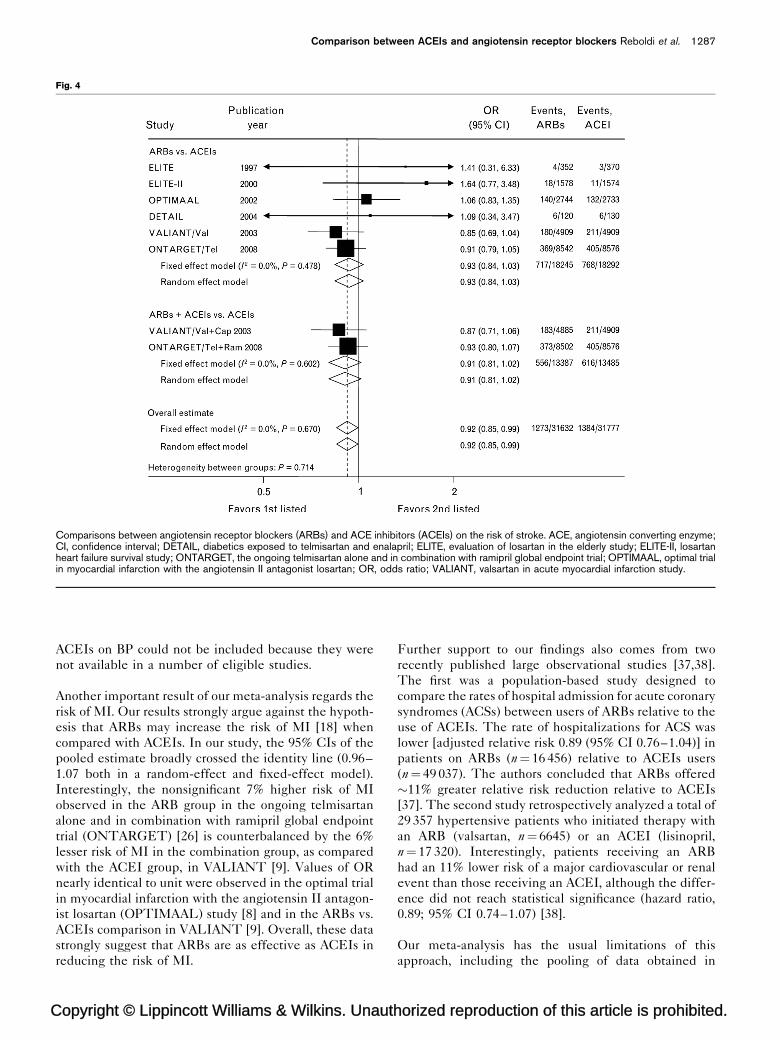
The overall estimate for the risk of stroke (Fig. 4) was 8%
lower with ARBs than with ACEIs (OR 0.92, 95% CI
0.85–0.99 with both the fixed-effect and the random-
effect model; P¼ 0.036). In the separate subgroup
analyses of ARBs vs. ACEIs and ARBsþACEIs vs.
ACEIs, the lesser stroke risk with ARBs did not achieve
statistical significance, although the subgroup estimates
opyright © Lippincott Williams & Wilkins. Unauth
were consistent and without significant between group
heterogeneity (P¼ 0.714).
In sensitivity analyses, none of the trials had a significant
influential effect on the overall estimates (Fig. 5) for both
stroke and MI. The methodological quality of the studies
was excellent for most of the included studies (mean
Jadad’s score 4.7) and did not affect the overall estimates.
DiscussionOur meta-analysis shows that the risk of MI, cardiovas-
cular mortality and total mortality did not differ in
patients treated with ARBs as compared with patients
treated with ACEIs. It further shows that when all
available data were considered, administration of ARBs
was associated with a small but statistically significant
reduction in the risk of stroke compared with adminis-
tration of ACEIs, a trend in a similar direction being
observed also when the subgroup analysis limited the
comparison with only ACEI-treated vs. only ARB-treated
patients. This allows to conclude that ARB and ACEI-
based treatments provide a similar protective effect on
orized reproduction of this article is prohibited.
C
1286 Journal of Hypertension 2008, Vol 26 No 7
Fig. 3
Comparisons between angiotensin receptor blockers (ARBs) and ACE inhibitors (ACEIs) on the risk of all-cause mortality. ACE, angiotensinconverting enzyme; CI, confidence interval; DETAIL, diabetics exposed to telmisartan and enalapril; ELITE, evaluation of losartan in the elderly study;ELITE-II, losartan heart failure survival study; ONTARGET, the ongoing telmisartan alone and in combination with ramipril global endpoint trial;OPTIMAAL, optimal trial in myocardial infarction with the angiotensin II antagonist losartan; OR, odds ratio; VALIANT, valsartan in acute myocardialinfarction study.
overall risk of fatal cardiovascular events and all-cause
mortality, but that blockade of the renin–angiotensin
system by antagonizing AT1 receptor stimulation by
angiotensin II may be associated with a slightly superior
cerebrovascular protective effect than blockade of ACE.
This may apply not only to patients with heart failure or a
MI that impairs cardiac function, but also to patients with
a broad range of conditions characterized by a high
cardiovascular risk, including a history of cardiac disease,
a history of cerebrovascular disease or diabetes.
The slightly greater protective effect of ARB vs. ACEI
treatment on stroke deserves a comment. First, although
never statistically significant a trend in favor of a lower
incidence of stroke was seen in trials using different
ARBs which suggests that the somewhat greater cerebro-
vascular protective effect possibly associated with ARB
treatment is class-related rather than drug-related.
Second, meta-analyses of trial data cannot provide a
mechanistic explanation of the effects that are seen.
There is some experimental evidence that ARBs might
have a specific cerebrovascular protective effect. For
opyright © Lippincott Williams & Wilkins. Unautho
example, the neurological outcome following induction
of cerebral ischemia in the rat was improved by intracer-
ebral administration of low doses of the ARB irbesartan,
and such effect was prevented by the coadministration of
an AT2 receptor blocker [16,33]. In rats injured by
cerebral artery occlusion and pretreated with candesartan
or ramipril at subhypotensive doses, the infarct size was
reduced by the ARB, not by the ACEI [34]. Also, the
neurological damage induced by cerebral ischemia as
well as the reduction in blood flow around the necrotic
area were found to be more severe in AT2 receptor
deleted mice than in control mice [35]. However, the
small difference in stroke incidence emerged in our
meta-analysis could also be due, in principle, to a lesser
protective effect of ACEIs, perhaps via a reduced AT2
receptor stimulation. Furthermore, it cannot be excluded
that use of ARBs was associated with a slightly greater BP
reduction than use of ACEIs, an explanation that is in line
with a profound effect on stroke of even small BP changes
and that may account for the greater protective effect on
stroke reported for calcium antagonists vs. other drugs
[2,3,36]. In the present study, the effect of ARBs and
rized reproduction of this article is prohibited.
C
Comparison between ACEIs and angiotensin receptor blockers Reboldi et al. 1287
Fig. 4
Comparisons between angiotensin receptor blockers (ARBs) and ACE inhibitors (ACEIs) on the risk of stroke. ACE, angiotensin converting enzyme;CI, confidence interval; DETAIL, diabetics exposed to telmisartan and enalapril; ELITE, evaluation of losartan in the elderly study; ELITE-II, losartanheart failure survival study; ONTARGET, the ongoing telmisartan alone and in combination with ramipril global endpoint trial; OPTIMAAL, optimal trialin myocardial infarction with the angiotensin II antagonist losartan; OR, odds ratio; VALIANT, valsartan in acute myocardial infarction study.
ACEIs on BP could not be included because they were
not available in a number of eligible studies.
Another important result of our meta-analysis regards the
risk of MI. Our results strongly argue against the hypoth-
esis that ARBs may increase the risk of MI [18] when
compared with ACEIs. In our study, the 95% CIs of the
pooled estimate broadly crossed the identity line (0.96–
1.07 both in a random-effect and fixed-effect model).
Interestingly, the nonsignificant 7% higher risk of MI
observed in the ARB group in the ongoing telmisartan
alone and in combination with ramipril global endpoint
trial (ONTARGET) [26] is counterbalanced by the 6%
lesser risk of MI in the combination group, as compared
with the ACEI group, in VALIANT [9]. Values of OR
nearly identical to unit were observed in the optimal trial
in myocardial infarction with the angiotensin II antagon-
ist losartan (OPTIMAAL) study [8] and in the ARBs vs.
ACEIs comparison in VALIANT [9]. Overall, these data
strongly suggest that ARBs are as effective as ACEIs in
reducing the risk of MI.
opyright © Lippincott Williams & Wilkins. Unauth
Further support to our findings also comes from two
recently published large observational studies [37,38].
The first was a population-based study designed to
compare the rates of hospital admission for acute coronary
syndromes (ACSs) between users of ARBs relative to the
use of ACEIs. The rate of hospitalizations for ACS was
lower [adjusted relative risk 0.89 (95% CI 0.76–1.04)] in
patients on ARBs (n¼ 16 456) relative to ACEIs users
(n¼ 49 037). The authors concluded that ARBs offered
�11% greater relative risk reduction relative to ACEIs
[37]. The second study retrospectively analyzed a total of
29 357 hypertensive patients who initiated therapy with
an ARB (valsartan, n¼ 6645) or an ACEI (lisinopril,
n¼ 17 320). Interestingly, patients receiving an ARB
had an 11% lower risk of a major cardiovascular or renal
event than those receiving an ACEI, although the differ-
ence did not reach statistical significance (hazard ratio,
0.89; 95% CI 0.74–1.07) [38].
Our meta-analysis has the usual limitations of this
approach, including the pooling of data obtained in
orized reproduction of this article is prohibited.
C
1288 Journal of Hypertension 2008, Vol 26 No 7
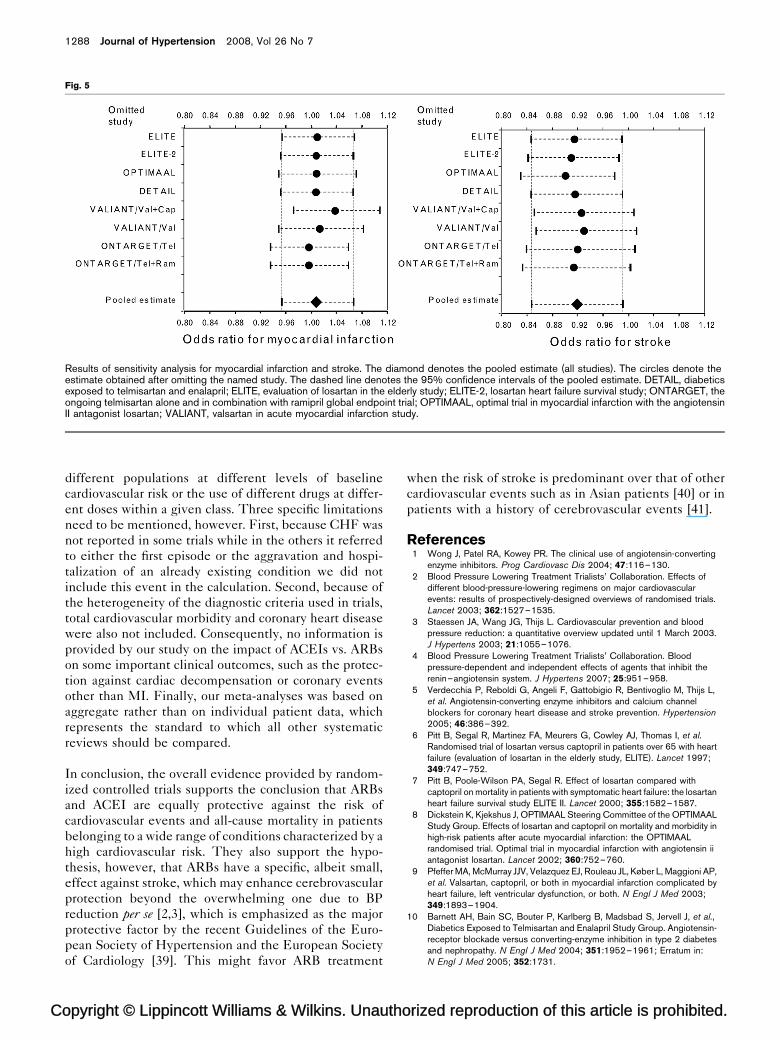
Fig. 5
Results of sensitivity analysis for myocardial infarction and stroke. The diamond denotes the pooled estimate (all studies). The circles denote theestimate obtained after omitting the named study. The dashed line denotes the 95% confidence intervals of the pooled estimate. DETAIL, diabeticsexposed to telmisartan and enalapril; ELITE, evaluation of losartan in the elderly study; ELITE-2, losartan heart failure survival study; ONTARGET, theongoing telmisartan alone and in combination with ramipril global endpoint trial; OPTIMAAL, optimal trial in myocardial infarction with the angiotensinII antagonist losartan; VALIANT, valsartan in acute myocardial infarction study.
different populations at different levels of baseline
cardiovascular risk or the use of different drugs at differ-
ent doses within a given class. Three specific limitations
need to be mentioned, however. First, because CHF was
not reported in some trials while in the others it referred
to either the first episode or the aggravation and hospi-
talization of an already existing condition we did not
include this event in the calculation. Second, because of
the heterogeneity of the diagnostic criteria used in trials,
total cardiovascular morbidity and coronary heart disease
were also not included. Consequently, no information is
provided by our study on the impact of ACEIs vs. ARBs
on some important clinical outcomes, such as the protec-
tion against cardiac decompensation or coronary events
other than MI. Finally, our meta-analyses was based on
aggregate rather than on individual patient data, which
represents the standard to which all other systematic
reviews should be compared.
In conclusion, the overall evidence provided by random-
ized controlled trials supports the conclusion that ARBs
and ACEI are equally protective against the risk of
cardiovascular events and all-cause mortality in patients
belonging to a wide range of conditions characterized by a
high cardiovascular risk. They also support the hypo-
thesis, however, that ARBs have a specific, albeit small,
effect against stroke, which may enhance cerebrovascular
protection beyond the overwhelming one due to BP
reduction per se [2,3], which is emphasized as the major
protective factor by the recent Guidelines of the Euro-
pean Society of Hypertension and the European Society
of Cardiology [39]. This might favor ARB treatment
opyright © Lippincott Williams & Wilkins. Unautho
when the risk of stroke is predominant over that of other
cardiovascular events such as in Asian patients [40] or in
patients with a history of cerebrovascular events [41].
References1 Wong J, Patel RA, Kowey PR. The clinical use of angiotensin-converting
enzyme inhibitors. Prog Cardiovasc Dis 2004; 47:116–130.2 Blood Pressure Lowering Treatment Trialists’ Collaboration. Effects of
different blood-pressure-lowering regimens on major cardiovascularevents: results of prospectively-designed overviews of randomised trials.Lancet 2003; 362:1527–1535.
3 Staessen JA, Wang JG, Thijs L. Cardiovascular prevention and bloodpressure reduction: a quantitative overview updated until 1 March 2003.J Hypertens 2003; 21:1055–1076.
4 Blood Pressure Lowering Treatment Trialists’ Collaboration. Bloodpressure-dependent and independent effects of agents that inhibit therenin–angiotensin system. J Hypertens 2007; 25:951–958.
5 Verdecchia P, Reboldi G, Angeli F, Gattobigio R, Bentivoglio M, Thijs L,et al. Angiotensin-converting enzyme inhibitors and calcium channelblockers for coronary heart disease and stroke prevention. Hypertension2005; 46:386–392.
6 Pitt B, Segal R, Martinez FA, Meurers G, Cowley AJ, Thomas I, et al.Randomised trial of losartan versus captopril in patients over 65 with heartfailure (evaluation of losartan in the elderly study, ELITE). Lancet 1997;349:747–752.
7 Pitt B, Poole-Wilson PA, Segal R. Effect of losartan compared withcaptopril on mortality in patients with symptomatic heart failure: the losartanheart failure survival study ELITE II. Lancet 2000; 355:1582–1587.
8 Dickstein K, Kjekshus J, OPTIMAAL Steering Committee of the OPTIMAALStudy Group. Effects of losartan and captopril on mortality and morbidity inhigh-risk patients after acute myocardial infarction: the OPTIMAALrandomised trial. Optimal trial in myocardial infarction with angiotensin iiantagonist losartan. Lancet 2002; 360:752–760.
9 Pfeffer MA, McMurray JJV, Velazquez EJ, Rouleau JL, Køber L, Maggioni AP,et al. Valsartan, captopril, or both in myocardial infarction complicated byheart failure, left ventricular dysfunction, or both. N Engl J Med 2003;349:1893–1904.
10 Barnett AH, Bain SC, Bouter P, Karlberg B, Madsbad S, Jervell J, et al.,Diabetics Exposed to Telmisartan and Enalapril Study Group. Angiotensin-receptor blockade versus converting-enzyme inhibition in type 2 diabetesand nephropathy. N Engl J Med 2004; 351:1952–1961; Erratum in:N Engl J Med 2005; 352:1731.
rized reproduction of this article is prohibited.
C
Comparison between ACEIs and angiotensin receptor blockers Reboldi et al. 1289
11 Unger T, Stoppelhaar M. Rationale for double renin–angiotensin–aldosterone system blockade. Am J Cardiol 2007; 100 (3A):25J–31J.
12 Bennett MR, Macdonald K, Chan S, Boyle JJ, Weissberg PL. Cooperativeinteractions between RB and p53 regulate cell proliferation, cellsenescence, and apoptosis in human vascular smooth muscle cells fromatherosclerotic plaques. Circ Res 1998; 82:704–712.
13 Diep QN, Li JS, Schiffrin EL. In vivo study of AT1 and AT2 angiotensinreceptors in apoptosis in rat blood vessels. Hypertension 1999; 34:617–624.
14 Levy BI. Can angiotensin II type 2 receptors have deleterious effects incardiovascular disease? Implications for therapeutic blockade of therenin–angiotensin system. Circulation 2004; 109:8–13.
15 Vacanti L. Could angiotensin receptor blockers and activation of AT2induce plaque rupture, rather than repair? BMJ 2004; Rapid Response (23December 2004).
16 Li J, Culman J, Hortnagl H, Zhao Y, Gerova N, Timm M, et al. AngiotensinAT2 receptor protects against cerebral ischemia-induced neuronal injury.FASEB J 2005; 19:617–619.
17 Fournier A, Achard JM, Boutitie F, Mazouz H, Mansour J, Oprisiu R, et al. Isthe angiotensin II type 2 receptor cerebroprotective? Curr Hypertens Rep2004; 6:182–189.
18 Verma S, Strauss M. Angiotensin receptor blocker and myocardialinfarction. BMJ 2004; 329:1248–1249.
19 Dahlof B, Devereux RB, Kjeldsen SE, Julius S, Beevers G, de Faire U, et al.Cardiovascular morbidity and mortality in the losartan intervention forendpoint reduction in hypertension study (LIFE): a randomised trial againstatenolol. Lancet 2002; 359:995–1003.
20 Schrader J, Luders S, Kulschewski A, Hammersen F, Plate K, Berger J, et al.Morbidity and mortality after stroke, eprosartan compared with nitrendipinefor secondary prevention: principal results of a prospective randomizedcontrolled study (MOSES). Stroke 2005; 36:1218–1226.
21 Verdecchia P, Angeli F, Gattobigio R, Reboldi GP. Do angiotensin IIreceptor blockers increase the risk of myocardial infarction? Eur Heart J2005; 26:2381–2386.
22 Volpe M, Mancia G, Trimarco B. Angiotensin II receptor blockers andmyocardial infarction: deeds and misdeeds. J Hypertens 2005; 23:2113–2118.
23 Strauss MH, Hall AS. Angiotensin receptor blockers may increase risk ofmyocardial infarction: unravelling the ARB-MI paradox. Circulation 2006;114:838–854.
24 Tsuyuki RT, McDonald MA. Angiotensin receptor blockers do not increaserisk of myocardial infarction. Circulation 2006; 114:855–860.
25 Boutitie F, Oprisiu R, Achard JM, Mazouz H, Wang J, Messerli FH, et al.Does a change in angiotensin II formation caused by antihypertensive drugsaffect the risk of stroke? A meta-analysis of trials according to treatmentwith potentially different effects on angiotensin II. J Hypertens 2007;25:1543–1553.
26 The ONTARGET Investigators. Telmisartan, ramipril, or both in patients athigh risk for vascular events. N Engl J Med 2008; 358:1547–1559.
27 Haynes RB, Wilczynski N, McKibbon KA, Walker CJ, Sinclair JC.Developing optimal search strategies for detecting clinically sound studiesin MEDLINE. J Am Med Inform Assoc 1994; 1:447–458.
28 McMurray J, Solomon S, Pieper K, Reed S, Rouleau J, Velazquez E, et al.The effect of valsartan, captopril, or both on atherosclerotic events afteracute myocardial infarction: an analysis of the Valsartan in Acute MyocardialInfarction Trial (VALIANT). J Am Coll Cardiol 2006; 47:726–733.
29 Whitehead A. Estimating the treatment difference in an individual trial. In:Meta-analysis of Controlled Clinical Trials. Chichester: John Wiley & SonsLtd. 2002. pp. 23–50.
30 Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistencyin meta-analyses. BMJ 2003; 327:557–560.
31 Tobias A. Assessing the influences of a single study in meta-analysis. StataTech Bull 1999; 47:15–17.
32 Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ,et al. Assessing the quality of reports of randomized clinical trials: is blindingnecessary? Control Clin Trials 1996; 17:1–12.
33 Iwai M, Liu HW, Chen R, Ide A, Okamoto S, Hata R, et al. Possible inhibitionof focal cerebral ischemia by angiotensin II type 2 receptor stimulation.Circulation 2004; 110:843–848.
34 Krikov M, Thone-Reineke C, Muller S, Villringer A, Unger T. Candesartanbut not ramipril pretreatment improves outcome after stroke and stimulatesneurotrophin BNDF/TrkB system in rats. J Hypertens 2008; 26:544–552.
35 Dai W, Funk A, Herdegen T, Unger T, Culman J. Blockade of centralangiotensin AT1 receptors improves neurological outcome and reducesexpression of AP-1 transcription factors after focal brain ischemia in rats.Stroke 1999; 30:2391–2399.
36 Zhang H, Thijs L, Staessen JA. Blood pressure lowering for primary andsecondary prevention of stroke. Hypertension 2006; 48:187–195.
opyright © Lippincott Williams & Wilkins. Unauth
37 Verma S, Mamdani M, Al-Omran M, Melo M, Rouleau JL. Angiotensinreceptor blockers vs. angiotensin converting enzyme inhibitors and acutecoronary syndrome outcomes in elderly patients: a population-basedcohort study (UMPIRE study results). J Am Soc Hypertens 2007; 1:286–294.
38 Delea TE, Taneja C, Moynahan A, Thomas SK, Frech-Tamas F, Oster G.Valsartan versus lisinopril or extended-release metoprolol in preventingcardiovascular and renal events in patients with hypertension. Am J HealthSyst Pharm 2007; 64:1187–1196.
39 Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G,et al. Guidelines for the Management of Arterial Hypertension: The TaskForce for the Management of Arterial Hypertension of the European Societyof Hypertension (ESH) and of the European Society of Cardiology (ESC).J Hypertens 2007; 25:1105–1187.
40 Zhou M, Offer A, Yang G, Smith M, Hui G, Whitlock G, et al. Body massindex, blood pressure, and mortality from stroke: a nationally representativeprospective study of 212 000 Chinese men. Stroke 2008; 39:753–759.
41 Vickrey BG, Rector TS, Wickstrom SL, Guzy PM, Sloss EM, Gorelick PB,et al. Occurrence of secondary ischemic events among persons withatherosclerotic vascular disease. Stroke 2002; 33:901–906.
orized reproduction of this article is prohibited.





























