ANGIOTENSIN CONVERTING ENZYME INHIBITORS (ACE-Is) IN THE MANAGEMENT OF MYOCARDIAL INFARCTION Emmanuel D Benjamín

ANGIOTENSIN CONVERTING ENZYME NHIBITORS IN THE MANAGEMENT OF MYOCARDIAL INFARCTION
Aug 21, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ANGIOTENSIN CONVERTING ENZYME INHIBITORS (ACE-Is) IN THE
MANAGEMENT OF MYOCARDIAL INFARCTION
Emmanuel D Benjamín
OUTLINE
• Intro; MI- Management• ACEIs- class definition• Examples• MOA• Rationale for the use of ACEIs in MI• RAAS• SAR of ACEIs• Pharmacology of a prototypical ACEI; CAPTOPRIL• Pharmacology of Lisinopril• Drug interractions• Counselling points• Side effects• Discussion• Conclusion 2

INTRO
• Myocardial infarction is myocardial necrosis caused by acute occlusion of a coronary artery due to plaque rupture or erosion with superimposed thrombosis.
• Approximately 1 million Americans will have a new or recurrent myocardial infarction this year (National registry of myocardial infarction). Nigeria?
• Coronary heart disease is the single largest cause of death in the United States.
• The estimated direct and indirect costs of coronary heart disease to GDP= $95.6 billion/year (National Registry of Myocardial infarction)
• Management involves non-drug measures and drug therapy, including, thrombolytics, β- blockers, statins, ARBs, Antiplatelet therapy, aldosterone receptor antagonism, ACE inhibitors. 3

DEFINITION OF CLASS
• ACEIs are drugs that competitively inhibit angiotensin converting enzyme (ACE).
• Thus inhibiting the production of angiotensin II.
• ↓ TPR, hence BP• ↓ aldosterone• ↓ Na retetion• ↓ H2O retention
4

EXAMPLES
• Captopril
• Enalapril
• Lisinopril
• Fosinopril
• Quinapril
• Trandolapril
• Benazepril
CLASSIFICATION OF ACEIs
(Based on Zn+2 binding moeity)• Sulfhydryl-containing agents: Captopril (Active drug),
the first ACE inhibitor, Zofenopril,Alacepril and Moveltipril.
• Dicarboxylate-containing agents: This is the largest group, including: Enalapril, Ramipril,Quinapril, Perindopril, Lisinopril (Active drug), Benazepril, Cilazapril, Delapril andSpirapril
• Phosphonate-containing agents: Fosinopril and SQ 29852
• Naturally occuring ACEIs; Casokinins and lactokinins, breakdown products of casein and whey, occur naturally after ingestion of milk products, especially cultured milk. Their role in blood pressure control is uncertain (Fitzgerald et al, 2004). 5

MOA
• Binding to ACE
• Inhibition of angiotensin II synthesis leading to decreased blood pressure + cardiovascular protection from hemodynamically mediated effects of angiotensis II on cardiac cells.
• cardiopretective action from angiotensinII effects on the heart.
6

RATIONALE FOR THE USE OF ACEIs IN MI – THE RAAS
7

RAAS
• The renin-angiotensin-aldosterone system (RAAS) is a signaling pathway responsible for regulating the body's blood pressure.
• Stimulated by low blood pressure or certain nerve impulses (e.g. in stressful situations), the kidneys release an enzyme called renin. This triggers a signal transduction pathway: renin splits the protein angiotensinogen, producing angiotensin I. This is converted by another enzyme, the angiotensin-converting enzyme (ACE), into angiotensin II.
• Angiotensin II not only causes blood vessels to narrow (vasoconstriction), it also simultaneously stimulates the secretion of the water-retaining hormone vasopressin (also called AVP) in the pituitary gland (hypophysis) as well as the release of adrenaline, noradrenaline and aldosterone in the adrenal gland.
8

RATIONALE FOR THE USE OF ACEIs IN MI
• This underlines the role of the Renin-Angiotensin-Aldosterone System (RAAS) in the pathological changes that occur post MI.
• RAAS contributes to the eccentric cardiac hypertrophy and fibrosis seen in MI by stimulating the migration (Bell and Madri, 1990; Dubey et al., 1995), proliferation (Daemen et al., 1991), hypertrophy and increased ECF production by cardiac fibroblasts (Villarreal et al., 1993; Crawford et al., 1994; Ostrom et al., 2003).
• RAAS also contributes to the hypertophy (Itoh et al., 1993), and increased production of ECF by vascular smooth muscle cells (Scott-Burden et al., 1990). 9

Rationale contd
• Angiotensin II acts directly on cells to induce the expression of specific proto-oncogenes
• Angiotensin II rapidly (within minutes) increases steady-state levels of mRNAs which alters the expression of several genes that stimulate cell growth (hypertrophy and hyperplasia), including basic fibroblast growth factor, platelet-derived growth factor, and transforming growth factor ᵝ
• changes in cardiac preload (volume expansion owing to Na+ retention) and afterload (increased arterial blood pressure) probably contribute to cardiac hypertrophy and remodeling
(goodman and gilman, 2006). 10
Rationale contd
• Arterial hypertension also contributes to hypertrophy and remodeling of blood vessels.
11

SAR OF ACEIs (Rajeev et al, 2010)
12

SAR Contd
• The N-ring must contain a carboxylic acid to mimic the C-terminal carboxylate of ACE substrates.
• Large hydrophobic heterocyclic rings (i.e., the N-ring) increase potency and alter pharmacokinetic parameters.
• The zinc binding groups can be either sulfhydryl (A), a carboxylic acid (B), or a phosphinic acid (C).
• The sulfhydryl group shows superior binding to zinc (the side chain mimicking Phe in carboxylate and phosphinic acid compounds compensates for the lack of a sulfhydryl group)
13

SAR Contd
• Sulfhydryl-containing compounds produce high incidence of skin rash and taste disturbances.
• Sulfhydryl-containing compounds can form dimers and disulfides which may shorten duration of action.
• Compounds which bind to zinc through either a carboxylate or phosphinate mimic the peptide hydrolysis transition state.
• Esterification of the carboxylate or phosphinate produces an orally bioavailable prodrug.
14

SAR Contd
• X is usually methyl to mimic the side chain of alanine. Within the dicarboxylate series, when X equals n-butylamine (lysine side chain) this produces a compound which does not require prodrug for oral activity.
• Optimum activity occurs when stereochemistry of inhibitor is consistent with L-amino acid stereochemistry present in normal substrates
15

Structure of angiotensin I
16

Date of download: 10/23/2014
Copyright © The American College of Cardiology. All rights reserved.
From: Are all angiotensin-converting enzyme inhibitors interchangeable?
J Am Coll Cardiol. 2001;37(5):1456-1460. doi:10.1016/S0735-1097(01)01161-5
The chemical structures of the 10 ACE inhibitors currently available in the U.S. The term “proven” refers to ACE inhibitors shown to improve survival or reduce morbidity. ACEI = angiotensin-converting enzyme inhibitor.
Figure Legend:

CAPTOPRIL (CAPOTEN)
• Captopril was the first inhibitor for clinical trial. • Reported to have a more favorable effect on QOL (Testa et al, 1993)• According to the mechanism proposed by Ondetti and colleagues,
captopril interacts with the enzyme through several bonds, i.e. electrostatic, hydrogenic and lipophilic connections.
• Among these, a co-ordinance bond formed between the free thiol group of captopril and zinc ion in the active site of ACE.
18

Captopril contd
• INTERRACTION OF CAPTOPRIL WITH ACE BINDING SITES(Vane, 1999 )
19

Captopril contd
• Captopril, the first ACE inhibitor to be marketed, is a potent ACE inhibitor.
• It is the only ACE inhibitor approved for use in the United States that contains a sulfhydryl moiety.
• Given orally, captopril is absorbed rapidly and has a bioavailability of about 75%.
• Peak concentrations in plasma occur within an hour, and the drug is cleared rapidly with a half-life of approximately 2 hours
20

Captopril contd
• Most of the drug is eliminated in urine, 40% to 50% as captopril and the rest as captopril disulfide dimers and captopril-cysteine disulfide.
• The oral dose of captopril ranges from 6.25 to 150 mg two to three times daily, with 6.25 mg three times daily or 25 mg twice daily being appropriate for the initiation of therapy.
• Most patients should not receive daily doses in excess of 150 mg. Since food reduces the oral bioavailability of captopril by 25% to 30%, the drug should be given 1 hour before meals
21

Lisinopril (PRINIVIL, ZESTRIL).
• Lisinopril, the third ACE inhibitor approved for use in the United States, is the lysine analogue of enalaprilat; unlike enalapril, lisinopril itself is active (Goodman ad Gilman, 2004).
• In vitro, lisinopril is a slightly more potent ACE inhibitor than is enalaprilat. Lisinopril is absorbed slowly, variably, and incompletely (about 30%) after oral administration (not reduced by food); peak concentrations in plasma are achieved in about 7 hours.
• It is cleared as the intact compound by the kidney, and its half-life in plasma is about 12 hours.
Lisinopril contd
• Lisinopril does not accumulate in tissues.
• The oral dosage of lisinopril ranges from 5 to 40 mg daily (single or divided dosage), with 5 and 10 mg daily being appropriate for the initiation of therapy.
• A daily dose of 2.5 mg is recommended for patients with heart failure who are hyponatremic or have renal impairment
23
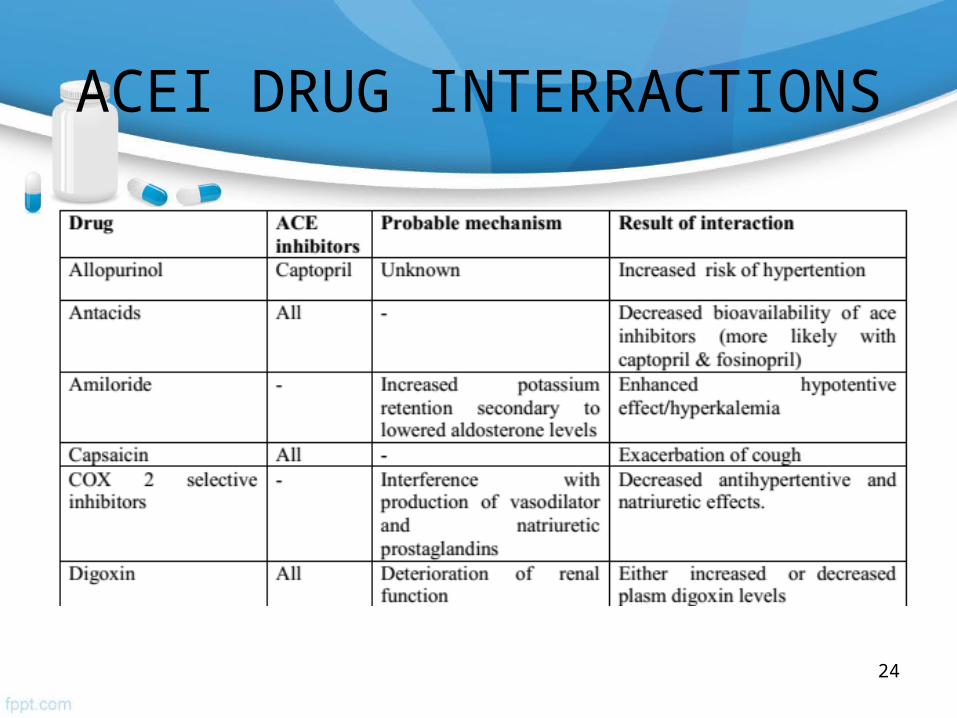
ACEI DRUG INTERRACTIONS
24

Interractions contd
25

Counselling points for ACEIs
• Might feel dizzy when you start taking this medicine. Get up gradually from sitting or lying position to minimize this effect. Sit or lie down if patient becomes light headed or dizzy.
• Do not take potassium supplements or consume too much banana while taking this medication unless your doctor instructs otherwise.
• When starting ACEIs, stop potassium-sparing diuretics, for 24 hours.
• Always start with low doses.• Check renal function and electrolytes before starting ACEIs and
review after 1-2 weeks.• Report promptly when untoward effects occur.
26

Common side effects of ACEIs
• Angioedema• Fetotoxicity• Skin rashes (esp. Captopril due to sulfhydryl group)• Acute renal failure• Dry cough• Headache• Nausea • Dizziness• Fatigue
27

DISCUSSION
• ACEIs increase survival when administered early after an acute myocardial infarction (MI) (Khalil et al).
• The early benefit of ACE inhibitor therapy suggests that starting ACE inhibitors within 24 h has aneffect on the infarcted myocardium either by limiting infarctsize or by reducing infarct expansion (GISSI Trial, 1994)
28

Effect of ACE-inhibitor therapy on cumulative mortality during days 0 to 30 in all trials combined.
ACE Inhibitor Myocardial Infarction Collaborative Group Circulation. 1998;97:2202-2212
Copyright © American Heart Association, Inc. All rights reserved.

DISCUSSION contd
• Since activation of the renin-angiotensinsystem has been shown to be an independent predictor ofischemic event (Alderman et al, 1991), ACEIs help prevent MI.
• Additionally, ACE inhibition has been shown to counteractseveral atherosclerotic processes including thrombosis, lowdensity lipoprotein oxidation, proliferation of vascularsmooth muscle cells and local accumulation of neutrophils contributing to MI (Mancini, 1996).
• Preliminary data have shown that ACEinhibition improves endogenous fibrinolytic function (Moriyama et al 1997).
30
CONCLUSION
• ACEIs have proven to be aces in the hole for virtually all cardiac patients as the RAAS appears to be a constant meddler in majority of cardiovascular events, which contribute a high percentage to morbidity and mortality worlwide.
• They have a proven efficacy in the management of MI especially when started early in the post-infarction period.
• A meta-analysis of all published, major trials investigating the use of an ACEI after an MI conclusively supports a role for ACEI therapy in the early phase and ongoing management of MI (Latini et al, 1995).
31
REFERENCES
• FitzGerald RJ, Murray BA, Walsh DJ; Murray, BA; Walsh, DJ (2004). "Hypotensive peptides from milk proteins". The Journal of nutrition 134 (4): 980S–8S. PMID 15051858
• Goodman & Gilman's The Pharmacological Basis Of Therapeutics - 11th Ed. (2006)
• Bell, L., and Madri, J.A. Influence of the angiotensin system on endothelial and smooth muscle cell migration. Am. J. Pathol., 1990, 137:7-12. PUBMED
• Daemen, M.J.M.P., Lombardi, D.M., Bosman, F.T., and Schwartz, S.M. Angiotensin II induces smooth muscle cell proliferation in the normal and injured rat arterial wall. Circ. Res., 1991, 68:450-456. PUBMED
32

REFERENCES
• Villarreal, F.J., Kim, N.N., Ungab, G.D., Printz, M.P., and Dillmann, W.H. Identification of functional angiotensin II receptors on rat cardiac fibroblasts. Circulation, 1993, 88:2849-286l. PUBMED
• Crawford, D.C., Chobanian, A.V., and Brecher, P. Angiotensin II induces fibronectin expression associated with cardiac fibrosis in the rat. Circ. Res., 1994, 74:727-739. PUBMED
• Ostrom, R.S., Naugle, J.E., Hase, M., et al. Angiotensin II enhances adenylyl cyclase signaling via Ca++/calmodulin: Gq-Gs cross-talk regulates collagen production in cardiac fibroblasts. J. Biol. Chem., 2003, 278:24461-24468. PUBMED
• Testa, M.A., Anderson, R.B., Nackley, J.F., Hollenberg, N.K., and the Quality-of-Life Hypertension Study Group. Quality of life and antihypertensive therapy in men: A comparison of captopril with enalapril. New Engl. J. Med., 1993, 328:907-913. PUBMED
33

REFERENCES
• Itoh, H., Mukoyama, M., Pratt, R.E., Gibbons, G.H., and Dzau, V.J. Multiple autocrine growth factors modulate vascular smooth muscle cell growth response to angiotensin II. J. Clin. Invest., 1993, 91:2268-2274. PUBMED
• Scott-Burden, T., Hahn, A.W.A., Resink, T.J., and Buhler, F.R. Modulation of extracellular matrix by angiotensin II: Stimulated glycoconjugate synthesis and growth in vascular smooth muscle cells. J. Cardiovasc. Pharmacol., 1990, 16(suppl. 4):S36-S41
• Rajeev Kumar, Ramji Sharma, Khamji Barwa, Ram kumar Roy, Aran Kumar, Atul Baruwa. Moder developmet in ACE Ihibitors. Der Pharmacia Lettre, 2010; 2(3):388-419
• Mohammed E. Khalil, Abul W. Basher, Edward J. Brown, JR, Imad A. Alhaddad. A Remarkable Medical Story: Benefits of Angiotensin-Converting Enzyme Inhibitors in Cardiac Patients. Journal of the American College of Cardiology. 2001. 37(7):
34
REFERENCES
• Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico. GISSI-3: effects of lisinopril and transdermal glyceryl trinitrate singly and together on six-week mortality and ventricular function after acute MI. Lancet 1994;343:1115–22
• Ng, K.K.F. & Vane, J.R. Conversion of angiotensin I to angiotensin II. Nature 216,762–766 (1967)
35

CREDITS:• Pharm. Khadijat S Adejumo• Pharm. Nicholas A• Pharm. Ibrahim James Oyibo• Mr Isa Buba and Mr Nasiru
THANK YOU ALL FOR LISTENING.
QUESTIONS?36
Related Documents











