Aspectos patogAspectos patogéénicos y nicos y terapterapééuticos de los linfocitos B. uticos de los linfocitos B.
Presente y futuro Presente y futuro
Division of Clinical Immunology & Rheumatology.
Autoimmunity Center of Excellence
Iñaki Sanz Paz

What do these diseases have in What do these diseases have in common?common?
Rheumatoid ArthritisRheumatoid ArthritisSystemic Lupus ErythematosusSystemic Lupus Erythematosus
ANCA-associated vasculitisANCA-associated vasculitis
Type 1 DiabetesType 1 Diabetes
Multiple SclerosisMultiple Sclerosis
Thrombotic Thrombocytopenic PurpuraThrombotic Thrombocytopenic PurpuraBullous Pemphigoid Bullous Pemphigoid
Sjogren’s syndromeSjogren’s syndrome
DermatomyositisDermatomyositis
Opsoclonus-myoclonus syndromeOpsoclonus-myoclonus syndrome
Primary Billiary CirrhosisPrimary Billiary CirrhosisInflammatory Bowel DiseaseInflammatory Bowel Disease
Pemphigus vulgaris Pemphigus vulgaris

What do these What do these diseases have in diseases have in
common?common?
Autoimmune etiology
Autoantibodies (most)
Good therapeutic response to B cell depletion therapy (BCDT)

What do these diseases have in What do these diseases have in common?common?
Rheumatoid ArthritisRheumatoid ArthritisSystemic Lupus Erythematosus
ANCA+ vasculitisANCA+ vasculitis
Type 1 DiabetesType 1 Diabetes
Multiple SclerosisMultiple Sclerosis
Autoimmune blistering diseases
Sjogren’s syndrome
Dermatomyositis
Primary Billiary Cirrhosis
B cell-mediated T cell-mediated

OverviewOverview
• Review the status of B cell depletion therapy (Rituximab)
• How extensive is its use now and in the future?
• Why and how are B cells important in disease
• Concerns about chronic B cell depletion
• B cells are important in maintaining health
• Can we afford to deplete them chronically?
• What remains to be learned?

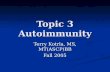
Response of SLE to BCDTResponse of SLE to BCDT African-American female (24-year old) with chronic
history of autoimmune hemolytic anemia refractory to conventional therapy with high-dose glucocorticoids and cyclophosphamide.
After 3 years of follow-up she developed arthritis, rash, elevated anti-ds DNA antibodies and depressed serum complement levels.
The patient was treated with IV Rituximab (4 doses of 375 mg/m2 one week apart) as part of a phase I/II clinical trial

Course of SLE in Subject #14
Anti-dsDNAC3%SLAM
0
100
200
300
400
500
600
700
0 20 40 60 80Months0
20
40
60
80
100
120
140Rituximab
Looney, Anolik, Sanz. Arthritis and Rheum 50:2580, 2004
Response of SLE to Response of SLE to BCDTBCDT

• 45 year-old male with SLE for 10 years recently diagnosed 45 year-old male with SLE for 10 years recently diagnosed with class IV nephritis together with membranous features. with class IV nephritis together with membranous features.
• Clinically stable on Prednisone (15 mg/d) and Azathioprine Clinically stable on Prednisone (15 mg/d) and Azathioprine (2 mg/kg/d). (2 mg/kg/d).
• Treated with low-dose Rituximab (single dose of 100 mg/mTreated with low-dose Rituximab (single dose of 100 mg/m22) ) with good peripheral B-cell depletion (< 5/with good peripheral B-cell depletion (< 5/l). l).
• SLAM index decreased from 11 at baseline to 4 and 2 at 3 SLAM index decreased from 11 at baseline to 4 and 2 at 3 and 12 months respectively. and 12 months respectively.
• Anti-ds DNA antibodies decreased by 84% over 12 months. Anti-ds DNA antibodies decreased by 84% over 12 months.
• One year after Rx. a repeat kidney biopsy showed almost One year after Rx. a repeat kidney biopsy showed almost complete resolution of proliferative changes. complete resolution of proliferative changes.
• The patient remains on complete clinical remission 7 years The patient remains on complete clinical remission 7 years after treatment with Rituximab on no drugs except for after treatment with Rituximab on no drugs except for Plaquenil.Plaquenil.
Case presentationCase presentation

Post-Rituximab (1y)Pre-Rituximab
Response of SLE to Response of SLE to BCDTBCDT
Activity index: 12Proteinuria (24 h): 1.2 g
Activity index: 1Proteinuria (24 h): 0.13 g
• Clinical course: complete remission sustained 7 years after Clinical course: complete remission sustained 7 years after treatment in the absence of additional therapy treatment in the absence of additional therapy• ANA ANA

3/12/2005 3/26/2005 4/9/2005 2/23/2007
B cell depletion in refractory B cell depletion in refractory Thrombotic Thrombocytopenic PurpuraThrombotic Thrombocytopenic Purpura

Anti-CD20 and/or Rituximab articles in the English literatureAnti-CD20 and/or Rituximab articles in the English literature
Blinded, Blinded, placebo placebo
controlled controlled (<10)(<10)
0
100
200
300
400
500
600
700
800
900
1994 1997
1998 2001
2002 2004 200620052003 2007
5 203 2971

B cell depletion with anti-CD20 B cell depletion with anti-CD20 monoclonal antibodies (Rituximab)monoclonal antibodies (Rituximab)
FDA approved for the treatment of non-Hodgkin follicular lymphoma (1997)
FDA approved for the treatment of Rheumatoid Arthritis refractory to anti-TNF agents (2006)
Impressive initial results in multiple autoimmune diseases:
• SLE, ITP, acquired factor VIII inhibitors, IgM-associated polyneuropathy, Sjogren’s….
• ANCA-associated vasculitis (Wegener’s)
• Multiple sclerosis

Rituximab targets CD20 specifically Rituximab targets CD20 specifically expressed on the surface of B-cellsexpressed on the surface of B-cells
Mouse
HumanHumanIgG1IgG1

Markers of B-Cell MaturationMarkers of B-Cell Maturation
Stem Pro-B Pre-B Immature Transitional Activated Memory Plasma Cell
Reprinted from Silverman G. Arthritis Rheum. 2006. 54:2356-2367.
MHC II
CD19
CD20
CD22
CD27
CD38
CD39
CD138

Rituximab targets. Plasma cells are Rituximab targets. Plasma cells are sparedspared
Pro-B Pre-B
Immature
Transitional
Naïve
Memory
Plasma Cell (long-lived)
Plasmablast (short-lived)
CD20CD20
RituximabRituximab
Protective vs pathogenic antibodies
Anti-microbial
Anti-ds DNA
Anti-RBP antibodies (Ro, La, Sm/RNP)

Anti-CD20: Mechanism of ActionAnti-CD20: Mechanism of Action
Antibody-Dependent Antibody-Dependent Cell-Mediated Cell-Mediated Cytotoxicity (ADCC)Cytotoxicity (ADCC)
Complement-dependentComplement-dependentCytotoxicityCytotoxicityComplement-dependentComplement-dependentCytotoxicityCytotoxicity
FcFcRIIIRIIIAA
CD20CD20
CD2CD200 MACMAC
ApoptosisApoptosisApoptosisApoptosis
B B cellcell
Anti-CD20 Anti-CD20 antibodyantibody
Macrophage, monocyte, NK cell

Rituximab in non-Hodgkin’s Rituximab in non-Hodgkin’s LymphomaLymphoma
• FDA-approved in 1997 (refractory, low-grade FL)
• Close to 1.0 million patients treated
• Monotherapy: 50% response
10% complete remission
• RTX + chemotherapy: 81-97% response 35-74%
complete remission
• Almost complete peripheral B-cell depletion ≥ 6 months
• Stable levels of total serum immunoglobulins
• Good safety profile without significant increase in infectious complications

Infusion-related reactions in multicenter trial (N=166)Infusion-related reactions in multicenter trial (N=166)1,21,2
1 McLaughlin P, et al. J Clin Oncol.
Num
ber
of
pati
en
ts
1st
infusion2d
infusion3rd
infusion4th
infusion
Grade 1Grade 2Grade 3/4 12% (3)
3% (4)
2 NCI Common Terminology Criteria for Adverse Events v3.0

Pre-Dose#2
Pre-Dose#4
3 MOPost-Rx
6 MOPost-Rx
9 MOPost-Rx
12 MOPost-Rx
Media
n a
bso
lute
CD
19
count
in p
eri
phera
l blo
od (
cells
/l)
Peripheral B-cell depletion Peripheral B-cell depletion in lymphoma patients (pivotal trial)in lymphoma patients (pivotal trial)
McLaughlin P, et al. J Clin Oncol. 1998;16:2825-2833.

Fleischmann R et al. Arthritis Rheum. 2006;54(9 suppl):S238 [abstract 483].
Rituximab 2 x 500 mg + MTX
Phase IIOpen -label extension study of rituximab treatment
Course of rituximab Course of rituximab
Phase IIa
Placebo
Rituximab 2 x 1000 mg
Phase IIb DANCER
Placebo
Rituximab 2 x 1000 mg + MTX
Long-term follow-up
-
Rituximab 2 x 1000 mg + MTX
Rituximab 2 x 1000 mg
+ MTX
Rituximab 2 x 1000 mg
+ MTX
Rituximab 2 x 1000 mg +
cyclophosphamide
Phase III REFLEX
Placebo
Rituximab 2 x 1000 mg + MTX
Rituximab 2 x 500 mg + MTX
Phase 2/3Open-label extension study of rituximab treatment
Phase 2a
Placebo
Rituximab 2 x 1000 mg
Phase 2b DANCER
Placebo
Rituximab 2 x 1000 mg + MTX
Long-termFollow-up
–
Rituximab 2 x 1000 mg + MTX
Rituximab 2 x 1000 mg + MTX
Rituximab 2 x 1000 mg
+ MTX
Rituximab 2 x 1000 mg +
cyclophosphamide
Phase 3 REFLEX
Placebo
Rituximab 2 x 1000 mg + MTX
All patients in the OL extension studyreceived MTX 10–25 mg/wk plus methylprednisolone 100 mg IV X 2 and570 mg oral between infusions
Timing of the 2nd course depended on MD discretion
Studies of Rituximab in RAStudies of Rituximab in RA


REFLEX Trial: Change inRadiographic End Points at Week 56
2.31
0.99
1.32
1
0.410.59
0.0
0.5
1.0
1.5
2.0
2.5
Total Genant-Modified Sharp
Score
Joint SpaceNarrowing
Erosion Score
Placebo + MTX (n = 184) RTX + MTX (n = 273)
Mean
Ch
an
ge
Primary analysis: radiographs within time window, linear extrapolation from Week 24 for missing values.
Keystone EC et al. Ann Rheum Dis. 2006;65(suppl 2):58 [abstract OP0016].
P = 0.0043
P = 0.0007
P = 0.0106

Mean serum IgG (up to wk 56)
Lower normal limit
0
2
4
6
8
10
12
14
16
-5 5 15 25 35 45 55
Time (Weeks)
Me
an
Ig
G (
ng
/mL
)
MTX R R+CTX R+MTX

Mean IgM (up to week 56)
0
0.5
1
1.5
2
2.5
-5 5 15 25 35 45 55
Time (Weeks)
Me
an
Ig
M (
ng
/mL
)
MTX R R+CTX R+MTX
Lower normal limit

Changes in total RF (median)
-160
-140
-120
-100
-80
-60
-40
-20
0
20
0 10 20 30 40 50
Time (Weeks)
Med
ian
Ch
an
ge (
IU/L
)
MTX R R+CTX R+MTX

Rituximab targets. Plasma cells are Rituximab targets. Plasma cells are sparedspared
Pro-B Pre-B
Immature
Transitional
Naïve
Memory
Plasma Cell (long-lived)
Plasmablast (short-lived)
CD20CD20
RituximabRituximab
Protective vs pathogenic antibodies
Anti-microbial
Anti-ds DNA
Anti-RBP antibodies (Ro, La, Sm/RNP)RF/anti-CCP
antibodies

Adverse effects of Rituximab in RA patientsAdverse effects of Rituximab in RA patients
MTX(n=40)
Rituximab(n=40)
Rituximab/CTX(n=41)
Rituximab/MTX(n=40)
All Events 145 (85%) 169 (88%) 161 (85%) 138 (85%)
RA exacerbation 55% 40% 37% 18%
Hypotension 18% 30% 29% 18%
Hypertension 15% 18% 7% 25%
Nasopharyngitis 15% 10% 7% 15%
Arthralgia 8% 8% 5% 13%
Back pain 8% 13% 7% 3%
Hyperglycaemia 10% 5% 7% 8%
Cough- 15% 5% 8%
Flushing 8% 13% 5% 3%
Headache 5% 5% 7% 8%

Infections: Most Frequently Reported(up to week 48)
MTX
(n=40)
Rituximab
(n=40)
Rituximab + CTX(n=41)
Rituximab + MTX (n=40)
Infections 24 (33%) 14 (30%) 16 (29%) 24 (33%)
-
Herpes simplex 5% 3% 5% 3% Herpes zoster 5% - 2% 5% URTI viral 3% - 2% 5% UTI 5% 3% 2% -
Bronchitis (bacterial) 5% - 2% - Pharyngitis (viral) 3% 3% - 3%
-UTI (bacterial) 5% 3%

Summary for RASummary for RA A single course of rituximab added to existing MTX
produced significant and sustained improvement in patients
with severe, seropositive, active rheumatoid arthritis.
Significant improvement in clinical outcomes was
achieved at week 24 and was maintained out to at least 48
weeks without further treatment.
Treatment with rituximab was well tolerated, with a
favorable safety profile being observed over 48 weeks
follow-up.
Decrease in disease-associated autoantibodies but not on
total Ig levels or protective anti-microbial antibodies

Recommendations for RARecommendations for RA
Indicated for active RA with resistance or toxicity to anti-TNF
drugs
Combination with MTX
Administered as two IV infusions of 1,000 mg two weeks
apart
Pre-medication with glucocorticoids and anti-histamines
recommended
Re-treatment possible (safe and effective) after 6 months

Indications and recommendationsIndications and recommendations
•FDA approved for the treatment of follicular non-Hodgkin lymphoma
•FDA approved for the treatment of Rheumatoid Arthritis refractory or
unable to use anti-TNF
•Other autoimmune diseases when conventional therapy fails or has
unacceptable toxicity:
• Kidney transplant:
• treatment of humoral rejection
• tolerance induction in HLA-sensitized recipients
• Future indications or applications:
•Pulmonary diseases: Asthma, COPD?
•Adjuvant therapy in some malignancies?

Rituximab: adverse effects and other safety consideraionsRituximab: adverse effects and other safety consideraions
1. Infusion reactions:1. Frequent in lymphoma and SLE2. Rare in other diseases including RA3. Usually mild (NCI grade 1-2), mostly with first infusion4. May be due to lymphocyte (tumor) lysis or serum sickness-like
disease due to HACA2. Infections
1. Not increased2. Usually common and mild infections3. However, fulminant hepatitis B reactivation and PML have been
reported3. Hypo-gammaglobulinemia: rare may require IVIG replacement4. Late-onset neutropenia: uncommon (10%), transient, responds to GM-
CSF, may preclude further treatment

Why – how are B cells involved Why – how are B cells involved
in in
many different conditions?many different conditions?

Ectopic GCs in RA synovium
CD8+IFN+
CD8+IFN-
Kang YM, Zhang X, Wagner UG, Yang H, Beckenbaugh RD, Kurtin PJ, Goronzy JJ, Weyand CM.
J Exp Med. 2002 May

Human Lupus NephritisHuman Lupus NephritisWith Infiltrating PlasmaWith Infiltrating PlasmaCells Cells
CD138 Human Lupus Human Lupus NephritisNephritisWith Germinal With Germinal CentersCenters
B-Cell Subsets and MicrostructuresB-Cell Subsets and Microstructuresin Lupus Nephritis in Lupus Nephritis
CD21
CD20
Courtesy of Dr. M. Clark, University of ChicagoCourtesy of Dr. M. Clark, University of Chicago

A B
Cortesia del Dr. J. Perez, Servicio de Nefrologia, Hospital General de Albacete
Renal B cell infiltrates in Churg-Strauss Syndrome

T Cell Activation in Rheumatoid Synovium is B Cell Dependent
S. Takemura, et al J.Immunol. 167: 4710-8, 2001
Interferon-
0
200
400
600
800
1000
1200
0 mcg 300 mcg 600 mcg
anti-CD20 mAb/day

Ectopic neolymphogenesis. Role of B Ectopic neolymphogenesis. Role of B cellscells
T
FDC
DC
LTßR
BLC (CXCL13)
LTαß B
ELCSLCBLC
BLC
LTßR
LTαß
ELCSLC
ChemokinesChemokines
ChemokinesChemokines
BLCStroma

B-cell functions
Formation and organization of peripheral lymphoid tissue
B cell follicles, germinal centers, T cell zone, marginal zoneB cell follicles, germinal centers, T cell zone, marginal zone
AntibodyAntibodyindependentindependent
Antigen presentation
Cytokine production
Chemokineproduction
B-cell (Auto)-antibody production(Auto)-antibody productionPlasma
cellAntibodyAntibodydependentdependent
LTα-dependent
LTα-independent
• T-cell activation (CD4 and CD8)T-cell activation (CD4 and CD8)• Th cell polarization (Th cell polarization ( Th Th22?)?)
• FFTHTH cell recruitment? (CXCL13-CXCR5) cell recruitment? (CXCL13-CXCR5)• Treg cell regulation: priming vs. suppressionTreg cell regulation: priming vs. suppression• Recruitment and regulation of DCs Recruitment and regulation of DCs • Anti-inflammatory actions (IL-10, TGFAnti-inflammatory actions (IL-10, TGF) ) • Pro-inflammatory actions (IL-6 + TGFPro-inflammatory actions (IL-6 + TGFββ): ): TH17?TH17?
Secondary tissue: protective or pathogenic responsesTertiary tissue: protective (BALT-influenza), pathogenic (BALT-RA/COPD)…….

Cytokine dependent effector Cytokine dependent effector functions of B cellsfunctions of B cells
Antibody
Regulation of T cell responses (APC function)
Lymphoid architecture(ectopic lymphoid tissue)
Cytokines/Chemokines
B cell
Courtesy of F. Lund (Trudeau Institute)

Multiple Roles for B Cells in RAMultiple Roles for B Cells in RA
Autoantibody productionAutoantibody production Cytokine secretionCytokine secretionAntigen presentationAntigen presentationT cell co-stimulationT cell co-stimulation

Antibody
APC function
Regulation of Th1/Th2 balance
Lymphoid architecture
B cellB cell
Generation of T cell memory
Cytokines/Chemokines
B cell effector functions
“New” “effector” and “regulatory” functions described for B cells, some of which are independent of antibody production
Courtesy of F. Lund (Trudeau Institute)

What do these diseases have in What do these diseases have in common?common?
Rheumatoid ArthritisRheumatoid ArthritisSystemic Lupus Erythematosus
ANCA+ vasculitisANCA+ vasculitis
Type 1 DiabetesType 1 Diabetes
Multiple SclerosisMultiple Sclerosis
Autoimmune blistering diseases
Sjogren’s syndrome
Dermatomyositis
Primary Billiary Cirrhosis
B cell-mediated T cell-mediated

Functional Implications of Functional Implications of
TargetedTargeted
B cell DepletionB cell Depletion
What happens when you deplete B cells?
Will it be safe to chronically deplete B cells?

Janus quality of B cells
Treg primingTreg primingTreg inhibition
T cell activationT cell activation T cell anergy
Cancer surveillanceCancer surveillanceCancer progression
DC recruitment DC inhibition (IL-10)DC inhibition (IL-10)
Th1 cytokines (Be1) Th2 cytokines (Be2)Th2 cytokines (Be2)
Protective AbPathogenic AutoabPathogenic Autoab
Pro-inflammatory TNF, IFN, IL-12p40
Anti-inflammatory Anti-inflammatory IL-10, TGFIL-10, TGFββ
Vaccine protectionAutoimmunity

Ab
solu
te B
cell
#
0.1
1.0
10.0
100.0
1000.0
0 2 12 36
Months
Group A (30%)•Overshoot of PBL B-cells•Eventual disappearance of autoantibodies •Complete, sustained clinical remission (up to 5 years)•Negative anti-RBP antibodies (Sm, Ro, La, U1RNP) at baseline
Group B (70%)Group B (70%)•Normal B-cells levels post BCDTNormal B-cells levels post BCDT•Autoantibodies persistAutoantibodies persist•Clinical relapse 3 months (mean) Clinical relapse 3 months (mean) after B-cell repopulationafter B-cell repopulation•Positive anti-RBP antibodies at Positive anti-RBP antibodies at baselinebaseline
Two types of response in SLE after BCDT

Group A is characterized by expansion of transitional B Group A is characterized by expansion of transitional B cells and greatly delayed memory B cell repopulationcells and greatly delayed memory B cell repopulation
CD38
SLE-group A
TT
NNMM
Neonate
NNMM
TT
Healthy adult
TT
NNMM
CD
24
SLE-group B Short-term
responder
MM
SLE post-Rituximab (32 mo)
N
T1
T2
M
T2
N
M
Normal control
T1
Rhodamine 123 Rhodamine 123
T3

Rituximab: adverse effects and other safety consideraionsRituximab: adverse effects and other safety consideraions
- Vaccination and immunization status
- Poor responses to neo-antigens:
- Vaccination should preceed treatment
- Diminished responses to recall antigens:
- Will re-vaccination be necessary upon B cell replenishmnent?
- Will B cell memory responses come back upon repopulation?
- Will pre-existing T cell memory survive and maintain appropriate
quality (Th1 versus Th2)?

Clinical considerations for Chronic B cell depletionClinical considerations for Chronic B cell depletion
•When to re-treat?•How to monitor response?•Who to re-treat
•Safety recommendations:•Hepatitis B vaccination status – revaccinate before treatment•Pneumococcal vaccination•Surveillance for EBV/CMV reactivation?•Surveillance for Progressive Multifocal Leukoencephalopathy
•Clinical•Immunological: JC virus titers, JC-specific T cell responses
•Needed epidemiological and clinical studies•Mycobacterial and other opportunistic/chronic infections? •Cancer incidence•Progression of atherosclerosis•Development of second autoimmune disease?
•

A lot remains to be learnedA lot remains to be learned
• Final outcome will depend on the balance of B cell reconstitution
between different B cell populations
• Immature versus memory
• Autoimmune memory versus protective memory
• Pro-inflammatory versus anti-inflammatory cytokine
• Careful analysis of emerging populations may indicate:
• Prognosis’
• How and when to retreat
• Risk of infections
• Risk of disease relapse

"Some cause happiness "Some cause happiness wherever they go; others, wherever they go; others,
whenever they go." whenever they go."
Oscar Wilde

CD20CD3

T:B Aggregates in HumanLupus Nephritis
CD3 CD20

Summary• B cell depletion therapy has demonstrated efficacy and safety in NHL and RA• Efficacy has been suggested in open label/uncontrolled studies in multiple other autoimmune disease.• Preliminary efficay and safety has also been found in controlled, randomized studies • Safety profile has been favorable

Fleischmann R et al. Arthritis Rheum. 2006;54(9 suppl):S238 [abstract 483].
Rituximab 2 x 500 mg + MTX
Phase IIOpen -label extension study of rituximab treatment
Course of rituximab Course of rituximab
Phase IIa
Placebo
Rituximab 2 x 1000 mg
Phase IIb DANCER
Placebo
Rituximab 2 x 1000 mg + MTX
Long-term follow-up
-
Rituximab 2 x 1000 mg + MTX
Rituximab 2 x 1000 mg
+ MTX
Rituximab 2 x 1000 mg
+ MTX
Rituximab 2 x 1000 mg +
cyclophosphamide
Phase III REFLEX
Placebo
Rituximab 2 x 1000 mg + MTX
Rituximab 2 x 500 mg + MTX
Phase 2/3Open-label extension study of rituximab treatment
Phase 2a
Placebo
Rituximab 2 x 1000 mg
Phase 2b DANCER
Placebo
Rituximab 2 x 1000 mg + MTX
Long-termFollow-up
–
Rituximab 2 x 1000 mg + MTX
Rituximab 2 x 1000 mg + MTX
Rituximab 2 x 1000 mg
+ MTX
Rituximab 2 x 1000 mg +
cyclophosphamide
Phase 3 REFLEX
Placebo
Rituximab 2 x 1000 mg + MTX
All patients in the OL extension studyreceived MTX 10–25 mg/wk plus methylprednisolone 100 mg IV X 2 and570 mg oral between infusions
Timing of the 2nd course depended on MD discretion
Study Schema of All Rituximab Retreatment Presentations

Rituximab Clinical Questions
2. Can a patient treated with rituximab be safely/effectively vaccinated?

Oren C et al. Arthritis Rheum. 2006;54(9 suppl):S515 [abstract 1234].
Response to Vaccination of RA Patients Treated with Rituximab
29 RA treated with DMARDs
• 8 RA treated with rituximab
• 21 healthy controls
Vaccinated with split virion inactivated vaccine (B/Shanghai, A/New Caledonian, A/California
Criterion for active response:
• > 4-fold rise in antibody titer or seroconversion
All patients increased in titers to New Caledonian
DMARD RA and healthy responded to A/California strain, rituximab-treated patients with RA did not respond to A/California strain
Rituximab may impair immune responses to vaccination

Immunization of Systemic Lupus Erythematosus Patients Treated With
Rituximab 12 patients in a Phase 1 trial were immunized 7 months after
rituximab treatment
Patients were assessed for a doubling of antipneumococcus and anti-TT antibody levels at Weeks 0 and 4
B-cell depletion was heterogeneous with those totally depleting (6) failing to respond to either vaccine and those with partial/short-lived depletion with variable responses (2 normal)
Conclusions:
B-cell depletion can impair responsiveness to bacterial vaccine challenge
Clinicians should be vigilant about recommended immunizations and consider vaccination before starting B-cell depletion therapy
Albert DA et al. Arthritis Rheum. 2006;54(9 suppl):S550 [abstract 1323].

Rituximab Clinical Questions
3. Which patients are appropriate for treatmentwith rituximab?
Can we predict who will respond to Rituximab?

Rituximab and Belimumab: Is RF or anti-CCP important?
Rituximab:
Patients who are seronegative for RF and/or anti-CCP respond less well to rituximab¹
0
10
20
30
40
50
60
70
PBO RTX PBO RTX
ACR20 ACR50 ACR70
RF + anti-CCP + RF – anti-CCP –
1Tak PP et al. Arthritis Rheum. 2006;54(9 suppl):S368 [abstract 833]. ²Huizinga TW et al. Arthritis Rheum. 2006;54(9 suppl):S368 [abstract 832].
(n = 107) (n = 157) (n = 16) (n = 29)

Anti-RNA binding protein autoantibodies are associated Anti-RNA binding protein autoantibodies are associated with poorer response to Rituximab in SLE (May Be with poorer response to Rituximab in SLE (May Be
Upstream Pathogenetic Factors for Type I Interferon)Upstream Pathogenetic Factors for Type I Interferon)
IgG-IgG-ENA ENA immunimmune e complecomplexx
PlasmacytoidPlasmacytoiddendritic celldendritic cell
(involves Fc(involves FcR)R)
IFN-IFN-MyeloidMyeloid
dendritic celldendritic cell
APRILAPRILBAFFBAFF
B cell survival factorsB cell survival factors
Banchereau J et al.Banchereau J et al. Immunity. Immunity. 2004;20:539-550. 2004;20:539-550.Litinskiy MB et al. Litinskiy MB et al. Nat Immunol.Nat Immunol. 2002;3:822-829. 2002;3:822-829.Jego G et al. Jego G et al. ImmunityImmunity. 2003;19:225-234.. 2003;19:225-234.
Plasma cellPlasma celldifferentiationdifferentiation
(with other factors e.g. IL-6)(with other factors e.g. IL-6)
Courtesy of Gregg Silverman. All rights reserved.Courtesy of Gregg Silverman. All rights reserved.
IL-6IL-6
B cell

Rituximab Clinical Questions
4. Are there new radiographic data?

REFLEX Trial: Change inRadiographic End Points at Week 56
2.31
0.99
1.32
1
0.410.59
0.0
0.5
1.0
1.5
2.0
2.5
Total Genant-Modified Sharp
Score
Joint SpaceNarrowing
Erosion Score
Placebo + MTX (n = 184) RTX + MTX (n = 273)
Me
an
Ch
an
ge
Primary analysis: radiographs within time window, linear extrapolation from Week 24 for missing values.
Keystone EC et al. Ann Rheum Dis. 2006;65(suppl 2):58 [abstract OP0016].
P = 0.0043
P = 0.0007
P = 0.0106

REFLEX Trial: Change inRadiographic End Points at Week 56 Is Not Dependent on Clinical Response at
Week 24
2.39
0.93
1.46
0.93
0.44 0.49
0.0
0.5
1.0
1.5
2.0
2.5
Total Genant Score Joint SpaceNarrowing
Erosion Score
Placebo + MTX (n = 151) RTX + MTX (n = 125)
Subgroup analysis of patients who were ACR20 nonresponders at Week 24 was also conducted using imputation for all withdrawals/rescue patients prior to Week 24.
Keystone EC et al. Ann Rheum Dis. 2006;65(suppl 2):58 [abstract OP0016].
P = 0.0271
P = 0.0396
P = 0.0126
Mea
n C
han
ge
ACR20 nonresponders at Week 24

Janus properties of B cells
Treg primingTreg primingTreg inhibition
T cell activationT cell activation T cell anergy
Cancer surveillanceCancer surveillanceCancer progression
DC recruitment DC inhibition (IL-10)DC inhibition (IL-10)
Th1 cytokines (Be1) Th2 cytokines (Be2)Th2 cytokines (Be2)
Protective AbPathogenic AutoabPathogenic Autoab
Pro-inflammatory TNF, IFN, IL-12p40
Anti-inflammatory Anti-inflammatory IL-10, TGFIL-10, TGFββ
Vaccine protectionAutoimmunity

•Outline•Introduction. Clinical Vignettes•Scope of BCDT•Anti-CD20, mechanisms•RA:
•Initial trial. Efficacy, safety•Re-treatment•Effect on bone erosions
•SLE•Trial•AE: HACA data•Clinical example•Immunology•Tolerance?
•Mechanisms of B cell depletion•Effects on T cells, lymphoid tissue
•Challenges:•Safety: PML•Vaccination•Th1 deviation•Janus effects
•Conclusions

Effector B cell subsets have distinct cytokine and transcriptional profiles
Con
trol
Be1 cells days 1-4
Be2 cells days 1-4
Courtesy of F. Lund (Trudeau Institute)
Harris et al. Nat Immunol 2001

Rituximab Therapy in Adults With Chronic Rituximab Therapy in Adults With Chronic ITPITP
• Twenty-five patients with chronic ITP• Treatment refractory (failed 2-5 Rxs)• Four weekly doses of rituximab 375 mg/m2
• Response criteria– Complete response (CR): platelets rise to normal counts
(ie, >100 109/L)– Partial response (PR): platelets rise to counts between 50
and 100 109/L– Minor response (MR): platelets rise to counts <50 109/L
with no need for continued treatment– No response or refractory disease: no rise in platelet
count or a rise 50 109/L, with a need for continued treatment
Stasi R et al. Blood. 2001;98:952–957.

Clinical Course of a Patient With Chronic Clinical Course of a Patient With Chronic ITP Responding to RituximabITP Responding to Rituximab
Stasi R et al Blood. 2001;98:952–957.
700
600
500
400
300
200
100
0
PDN
lv lg
VCR
Splemectomy
Cy
Rituximab
Pts
. X
10
9/L
05/95 06/95 08/9510/95 11/95 01/96 02/9604/96 05/96 10/98 12/98 03/99 04/99 05/9906/99 07/99 10/00

• Acetaminophen: 1 gram PO • Diphenhydramine: 50 mg PO • Methyl-prednisolone: 100 mg IV over 10 minutes• Rituximab: 1000 mg IV at 50mg/hr, 30 min after Solumedrol
• Rituxan infusion may be increased 12.5ml/hr (50mg/hr) every half hour to a max of 100ml/hr (400mg/hr) as long as patient is stable.
Guidelines for the administration of Rituximab
Two infusions of 1000 mg IV two weeks apart

HACAs (Human Anti-Chimeric Antibodies) HACAs (Human Anti-Chimeric Antibodies)
• Negative/low in most patients (11/17)
• High titer (>100 ng/mL) in 6/17 including 2 in high dose group
• Average peak for high titer = 4767 ng/mL
• Long term persistence
110
1001000
10000
0 4 8 12
Month
HA
CA
(ng/
ml)
Non-depleters
Depleters

High HACAs are associated with High HACAs are associated with poor B-cell depletion and active lupuspoor B-cell depletion and active lupus
0.1
1
10
0 3 6 9 12Month
% C
D19
+ l
ymp
ho
cyte
s
High HACA
No or Low HACA

SummarySummary Targeting of B cells can provide an effective alternative
to TNF inhibitors or T-cell–directed therapies for the treatment of autoimmune rheumatic diseases
RA patients retreated with rituximab had a successful therapeutic response with no increase safety issues or infections
Rituximab may impair clinical response to vaccination
• Physicians should be vigilant regarding vaccination during therapy
A host of B-cell targeting agents are now in development for the treatment of autoimmune diseases and organ rejection
• RA, SLE, Vasculitis, WG, SS, ITP, Diabetes, TTP, blistering diseases, myositis,

Atacicept(TACI-Ig)
Rituximab is a chimeric antibody consisting of both human and mouse regions
Other agents are fully humanized so the entire construct has human components
TRU-015 is a SMIP (small modular immunopharmaceutical) with a shortened light chain attached to the heavy chains
Decoy receptor agents fuse the ligand binding domains to human IgG Fc portion
Human (green)
Mouse (red)
Human (green)
Human (green)
Human (green)
Mouse (red)
Human (green) BR3-FC
Rituximab
TRU-015
OcrelizumabOfatumumabBelimumab
Construction of B-Cell Targeting AgentsConstruction of B-Cell Targeting Agents

SummarySummary
B cell depletion appears to be a safe and highly promising modality for the treatment of multiple autoimmune diseases.
Safety and efficacy appears to also extend to chronic or repeated B cell depletion achieved by repeated infusions of Rituximab
Clinically relevant hypoglobulinemia appears to be rare although IVIG replacement may be required (mostly in young children)
Serious infusion reactions are rare and occur mostly with the first infusion. However, HACA formation may occur mostly in patients with SLE leading to infusion reactions, faster Rituximab clearance and decreased efficacy.

SummarySummary Serious infectious are rare. However,
fulminant hepatitis B has been reported. Similarly, two cases of Progressive Multifocal Leukoencephalopathy (PML) have been reported in two SLE patients.
Immune responses to neo-antigen and recall responses to previous immunizations may be compromised.
Longer surveillance may be required to understand the consequences of prolonged B cell depletion

Rituximab Clinical Questions
1. How effective/safe is retreatment?
2. When should patients be retreated?
3. Which patients are appropriate for rituximab treatment?Can we predict who will respond to rituximab?
4. Can a patient treated with rituximab be safely/effectively vaccinated?
5. How should we monitor patients (before and after Rx.)?

Rituximab Clinical Questions
1. What’s the impact of B cell therapies on mycobacterial infections?
2. What’s the impact of B cell depletion on pre-established B and T cell memory for chronic viral infections
1. EBV, CMV
2. Hepatitis B virus
3. JC/BK polyoma virus (PML, kidney graft loss)
3. How is autoimmunity impacted: secondary autoimmunity?
4. Is cancer surveillance altered?

Platelet Response to Platelet Response to RituximabRituximab
Stasi R et al. Blood. 2001;98:952–957.
Weeks
600
500
400
300
200
100
01 2 3 4 5 6 7 8 9 10 11 12
CR (n=5)
PR (n=5)
NR (n=15)
Pre
Pts
. X
10
9/L

Rituximab Therapy in Children With Rituximab Therapy in Children With Refractory Autoimmune Hemolytic Refractory Autoimmune Hemolytic AnemiaAnemia
• Fifteen children, median age at diagnosis 2 years (range 0.3 to 14 years)
• All refractory to 2 courses of immunosuppressive therapy
• Two to 4 weekly doses of rituximab 375 mg/m2
• All pre-medicated with diphenhydramine and methylprednisolone
• After completing treatment, all children received 400 mg/kg IVIG every 3 weeks for 6 months
Zecca et al. Blood. 2003;101:3857–3861.

Zecca et al. Blood. 2003;101:3857–61.
Hgb and Absolute Reticulocyte Hgb and Absolute Reticulocyte CountsCounts
The difference between pretreatment and posttreatment values is statistically significant (P<.001)
Pretreatment 2 Months
800
700
600
500
400
300
200
100
0R
etic
ulo
cyte
s (x
109 /
L)
16
Pretreatment
14
12
10
8
6
4
2
0
2 Months
Hem
og
lob
in (
g/d
L)

Treatment of IgM Antibody-Treatment of IgM Antibody-associated Polyneuropathy With associated Polyneuropathy With RituximabRituximab
• Patients
– Twenty-one patients treated with 375 mg/m2 rituximab x 4
– Thirteen untreated controls
• Re-treatment of 16 patients with 375 mg/m2 rituximab x 2 then x 1 every 10 week
Pestronk A et al. J Neuro Neurosurg Psych. 2003; 74:485–489.

Pestronk A et al. J Neuro Neurosurg Psych. 2003;74:485–489.
Treatment With Rituximab Resulted Treatment With Rituximab Resulted in Improved Strengthin Improved Strength
Error bars= SEMP<.001
Treated Untreated
Dis
tal st
rength
(%
norm
al)
Baseline 1 Year 2 Years

Antibody Titers and Immunoglobulin levels in Antibody Titers and Immunoglobulin levels in Rituximab-treated PatientsRituximab-treated Patients
Pestronk A et al. J Neuro Neurosurg Psych. 2003;74:485–489.
020
4060
80100
120140
Untreated
IgM Anti-GM1 MAG
IgM Anti-tet IgG
Mea
n %
bas
elin
e (S
EM
)
1 Year 2 Year
IgM Anti-GM1 MAG

Caveats of Rituximab Therapy• Controlled clinical trials are needed to determine efficacy
• Combination therapy may be needed in certain patients and/or diseases
• Effects of rituximab on host defenses needs additional study
• Rituximab has been used safely in children as young as 3 months old. However, IV Ig in young children may be necessary
• Total IgG and IgG anti-tetanus antibodies appear to be unaffected even after 2 years of therapy with rituximab alone; however, significant reductions in total IgM do occur
• Antibody response to immunization may be blunted or even completely eliminated
• High level HACAs can be induced, at least in SLE.

REFLEX Trial: REFLEX Trial: Median CD19+ B-Lymphocyte Median CD19+ B-Lymphocyte
CountsCounts
0
50
100
150
200
250
300
350
400
450
500
0 4 8 12 16 20 24
Weeks
Med
ian
CD
19+
cou
nt (
cells
/uL)
Placebo + MTX (n = 209)Rituximab + MTX (n = 308)
Error bars represent the interquartile range.Cohen S et al. Arthritis Rheum. 2006;54:2793-2806.

0
20
40
60
80
100
120
0 10 20 30 40
Months
PR CR
Transient B-cell Depletion With Rituximab Resulted in Lasting Complete Response
Cooper N et al. Blood. 2002;100:Abstract:187.
Per
cen
t M
ain
tain
ing
Res
po
nse

Long Term Efficacy of Retreatment With Long Term Efficacy of Retreatment With Rituximab in DMARD Failures/TNF IRRituximab in DMARD Failures/TNF IR
Placebo patients eligible to receive their first course of rituximab within the extension study
Need for retreatment was determined by the treating physician• Only criterion for retreatment
was residual disease activity (defined as ≥ 8 SJC and TJC)
Completer analysis• 145 patients received C2• 99 reached Week 24 C2
0
10
20
30
40
50
60
70
80
C1 Week 24 C2 Week 24
ACR 20 ACR 50 ACR 70
C1, course 1; C2, course 2; SJC, swollen joint count; TJC, tender joint count.Emery P et al. Arthritis Rheum. 2006;54(9 suppl):S228 [abstract 458].

Long-Term Efficacy of Retreatment Long-Term Efficacy of Retreatment with Rituximab in anti-TNF Failureswith Rituximab in anti-TNF Failures
279 patients prior Rx with anti-TNF: had 2 courses of rituximab
155 reached wk 24 of 2nd course
Repeated courses not associated with increase in infections/overall incidence of adverse event (AE)
1669 pt-years of follow-up, one or multiple courses of rituximab showed no new safety signals
Patients maintained their HAQ-DI response and improved their
SF-36 with retreatment.²
65
33
12
66
33
12
72
42
21
56
31
16
0
10
20
30
40
50
60
70
80
ACR20 ACR50 ACR70 ACR20 ACR50 ACR70
79
13
6
79
13
6
88
25
13
81
25
13
0
10
20
30
40
50
60
70
80
90
100
Moder
ate/
Good
Low Dis
ease
Remis
sion
Mod
erat
e/G
ood
Low Dis
ease
Remis
sion
% P
atie
nts
Course 1
Course 2
¹Keystone E et al. Arthritis Rheum. 2006;54(9 suppl):S328 [abstract 725]. ²Tak PP et al. Arthritis Rheum. 2006;54(9 suppl):S403 [abstract 926].
% P
atie
nts
Course 1
Course 2
12 weeks 24 weeks

Infusion Associated Events withRetreatment
0
5
10
15
20
25
30
C1 N 1039 C2 N 570 C3 N 191 C4 N 40
1st INF
2nd INF
0
1
2
3
4
5
C1 C2 C3 C4
% Infusion Events
% Serious Events
C1
N 1039
C2
N 570
C3
N 191
C4
N 40
1st Infusion
Any AE 269 81 20 6
Total AE 446 104 26 7
SAE 5 1 0 0
Severe 11 2 0 0
Life Threatening 1 0 0 0
Dose Modification 100 32 6 4
D/C 12 0 0 0
2nd Infusion
Any AE 95 30 4 1
Total AE 124 39 5 1
SAE 2 1 0 0
Severe 1 1 0 0
Life Threatening 0 0 0 0
Dose Modification 13 6 0 0
D/C 0 1 0 0
Fleischmann R et al. Arthritis Rheum. 2006;54(9 suppl):S238 [abstract 483].

0
0.5
1
1.5
2
2.5
0 4 8 12 16 20 24
Weeks
Mea
n I
gM
(m
g/m
L)
IgM
0
3
6
9
12
15
0 4 8 12 16 20 24
Weeks
Mea
n I
gG
(m
g/m
L)
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
0 4 8 12 16 20 24
Weeks
Mea
n I
gA
(m
g/m
L)
IgG IgA
Placebo + MTX (n = 201) Rituxan + MTX (n = 298)
REFLEX Trial: Mean (SD) Serum Immunoglobulin Levels
SD = standard deviation.Cohen S et al. Arthritis Rheum. 2006;54:2793-2806.
LLN

Subanalysis: Retreatment B-Cell and Immunoglobulin Levels Relation to
Infections
Near-complete CD19+ B-cell depletion
Prior to C2 and C3
• 72% of patients < LLN
• B-cell repletion did not begin until at least Week 24
SIE similar in patients with normal IgG and IgM vs those with levels < LLN
Genovese M et al. Arthritis Rheum. 2006;54(9 suppl):S779 [abstract 1983].
All
N = 1039
Normal
IgM/IgG
N = 804
IgM < LLN
N = 207
IgG < LLN
N = 50
Years exposure 1670 1225 1376 125
SIE [N,(%)] 68 (6.5) 45 (5.6) 18 (8.7) 6 (12)
AE 84 58 21 6
SIE/100 pt-yrs 5.0 4.7 5.6 4.8
C1 C2 C3
IgM < LLN 8%–10% 18%–19% 22%–23%
IgG < LLN 0.5%–1.5% 4% 5%–6%

SIE with Use of TNF Inhibitors After Rituximab Therapy
78 patients treated with an anti-TNF after RTX• All had peripheral B-cell counts below LLN
14 (18%) had 22 AE• 10 SAE (3 RA flare, 2 pleuritis, 1 DVT, 4 SIE)
SIE• 2 skin (erysipelas, cellulitis)
• 1 bacterial arthritis
• 1 aseptic meningitis Rate of SIE
• After anti-TNF = 7.62 events/100 pt-yrs
• Before anti-TNF = 5.23 events/100 pt-yrs
Genovese M et al. Arthritis Rheum. 2006;54(9 suppl):S329 [abstract 726].

1
10
100
1000
10000
0 4 8 12
Month
Rit
uxi
mab
(m
ean
in n
g/m
L)
High HACA
No or low HACA
HACAs = more rapid rituximab pharmacokinetics

Rheumatology 2001; 40: 205-211
Sustained improvement in rheumatoid arthritis following a protocol designed to deplete B lymphocytes
J. C. W. Edwards and G. Cambridge University College London Centre for Rheumatology, London, UK
Arthritis & Rheumatism, Oct 2002
An open study of B lymphocyte depletion in systemic lupus erythematosusMaria J. Leandro *, Jonathan C. Edwards, Geraldine Cambridge, Michael R. Ehrenstein,
David A. IsenbergMiddlesex Hospital, University College, London, UK
Arthritis & Rheumatism, Oct 2001
B lymphocyte depletion as a novel treatment for Systemic Lupus Erythematosus: Phase I/II trial of Rituximab (Rituxan) in SLEJennifer Anolik, Joe Rosenblatt, Fay Young, Iñaki Sanz, John LooneyUniversity of Rochester School of Medicine, Rochester, New York, USA

Arthritis & Rheumatism, 2004
B cell depletion as a novel treatment for systemic lupus erythematosus: A phase I/II dose-escalation trial of rituximab R. John Looney, Jennifer H. Anolik, Debbie Campbell, Raymond E. Felgar,
Faith Young, Lois J. Arend, James A. Sloand, Joseph Rosenblatt, Iñaki Sanz University of Rochester School of Medicine, Rochester, New York, USA
Efficacy of B-Cell–Targeted Therapy with Rituximab in Patients with Rheumatoid Arthritis
Jonathan C.W. Edwards, M.D., Leszek Szczepanski, M.D., Ph.D., Jacek Szechinski, M.D., Ph.D., Anna Filipowicz-Sosnowska, M.D., Ph.D., Paul Emery, M.D., David R. Close, Ph.D., Randall M. Stevens, M.D., and Tim Shaw, B.Sc.
New England Journal of Medicine, 2004

REFLEX Trial: Change inRadiographic End Points at Week 56 Is Not Dependent on Clinical Response at
Week 24
2.39
0.93
1.46
0.93
0.44 0.49
0.0
0.5
1.0
1.5
2.0
2.5
Total Genant Score Joint SpaceNarrowing
Erosion Score
Placebo + MTX (n = 151) RTX + MTX (n = 125)
Subgroup analysis of patients who were ACR20 nonresponders at Week 24 was also conducted using imputation for all withdrawals/rescue patients prior to Week 24.
Keystone EC et al. Ann Rheum Dis. 2006;65(suppl 2):58 [abstract OP0016].
P = 0.0271
P = 0.0396
P = 0.0126
Mea
n C
han
ge
ACR20 nonresponders at Week 24


Blood, Jan 1994
Depletion of B cells in vivo by a chimeric mouse human monoclonal antibody to CD20
ME Reff, K Carner, KS Chambers, PC Chinn, JE Leonard, R Raab, RA Newman, N Hanna and DR Anderson
IDEC Pharmaceuticals Corporation, San Diego, CA 92121.
Blood, Sept 1997
IDEC-C2B8 (Rituximab) Anti-CD20 Monoclonal Antibody Therapy in Patients With Relapsed Low-Grade Non-Hodgkin's Lymphoma
David G. Maloney, Antonio J. Grillo-López, Christine A. White, David Bodkin, Russell J. Schilder, James A. Neidhart, Nalini Janakiraman, Kenneth A. Foon, Tina-Marie Liles,
Brian K. Dallaire, Ken Wey, Ivor Royston, Thomas Davis, and Ronald Levy Stanford University, Stanford, CA
Blood, Feb 1987
Monoclonal antibody 1F5 (anti-CD20) serotherapy of human B cell lymphomas OW Press, F Appelbaum, JA Ledbetter, PJ Martin, J Zarling, P Kidd and ED Thomas
University of Washington: the Fred Hutchinson Cancer Research Center andOncogen Inc. Seattle Washington.



Rituximab: adverse effects and other safety consideraionsRituximab: adverse effects and other safety consideraions
1. Infusion reactions:1. Frequent in lymphoma and SLE2. Rare in other diseases including RA3. Usually mild (NCI grade 1-2), mostly with first infusion4. May be due to lymphocyte (tumor) lysis or serum sickness-like
disease due to HACA2. Infections
1. Not increased2. Usually common and mild infections3. However, fulminant hepatitis B reactivation and PML have been
reported3. Hypo-gammaglobulinemia: rare may require IVIG replacement4. Late-onset neutropenia: uncommon (10%), transient, responds to GM-
CSF, may preclude further treatment

Chronic B cell depletion as maintenance therapy
•Which diseases: •Lymphoma, CLL•Rheumatoid Arthritis•SLE subset




Infusion Associated Events withRetreatment
0
5
10
15
20
25
30
C1 N 1039 C2 N 570 C3 N 191 C4 N 40
1st INF
2nd INF
0
1
2
3
4
5
C1 C2 C3 C4
% Infusion Events
% Serious Events
C1
N 1039
C2
N 570
C3
N 191
C4
N 40
1st Infusion
Any AE 269 81 20 6
Total AE 446 104 26 7
SAE 5 1 0 0
Severe 11 2 0 0
Life Threatening 1 0 0 0
Dose Modification 100 32 6 4
D/C 12 0 0 0
2nd Infusion
Any AE 95 30 4 1
Total AE 124 39 5 1
SAE 2 1 0 0
Severe 1 1 0 0
Life Threatening 0 0 0 0
Dose Modification 13 6 0 0
D/C 0 1 0 0
Fleischmann R et al. Arthritis Rheum. 2006;54(9 suppl):S238 [abstract 483].

Rituximab in Rheumatoid Rituximab in Rheumatoid ArthritisArthritis
Baseline 48 weeks
Rituximab (1g x 2)
Rituximab (1g x 2) Cytoxan (750 mg x 2)
MTX ( >10mg/wk)
Rituximab (1g x 2)
MTX ( > 10 mg/wk)
MTX inadequateresponders
RANDOMIZED
17 day corticosteroids
in all arms
Edwards et al. NEJM 2004

ACR Response at 24 weeks
0
20
40
60
80
100
MTX Rituximab Rituximab +CTX
Rituximab +MTX
% p
atie
nts ACR20
ACR50
ACR70
p = 0.025 P = 0.001 P = 0.003
P = 0.005 P = 0.005
P = 0.048
Rituximab in rheumatoid arthritis: efficacy and safety from a randomised controlled
trial. Stahl et al. Ann Rheum Dis 2003, 62 (Suppl): 0P004.
ACR Response at 48 weeks
0
20
40
60
80
100
MTX Rituximab Rituximab +CTX
Rituximab +MTX
% p
atie
nts
ACR20
ACR50
ACR70
P = 0.0001
P = 0.002
P = 0.03
P = 0.01
P = 0.01

Phase I/II Open-label Dose-escalating Phase I/II Open-label Dose-escalating Trial of Rituximab in Patients With Trial of Rituximab in Patients With
SLESLE
Dose escalation: 6 subjects per group
one dose of 100 mg/m2 rituximab
one dose of 375 mg/m2 rituximab
four weekly doses of 375 mg/m2 rituximab
Efficacy outcomes:
B cell depletion
SLAM
Serology

Clinical Response in Clinical Response in SLESLE
****
0 Months 1 Month 2 Months 3 Months
Non-depleters (n=6)
Depleters (n=10)
02468
1012141618
SLA
M (
mea
n an
d 95
% C
I)
Looney, Anolik et al. Arthritis and Rheum 50:2580, 2004

Anolik et al. Arthritis & Rheumatism, 2004, 50:3580.
Clinical response is independent Clinical response is independent of serological responseof serological response
1
10
100
0 1 2 3 6 9 12 360
20
40
60
80
100
120
140
160
180
200
Months post-Rx: #4 low dose
Months post-Rx: #15 high dose
1000
0.10
1
10
100
0 1 2 3 6 9 12 20 240
50
100
150
200
250
Per
cen
t o
f b
asel
ine
Ab
solu
te B
cel
l #
Months post-Rx: #1 low dose
1
10
100
0 1 2 3 6 9 12 360
20
40
60
80
100
120
140
160
B cell countB cell countSLAM index Anti-ds DNAAnti-ds DNA

Anti-dsDNA in depletersAnti-dsDNA in depleters
1
10
100
1000
10000
0 1 2 3
Month
An
ti-d
sD
NA