Adrenal Haemorrhage
By Andrew McGovern
Image: Underwood (2006)
The use of different imaging methods in:

Introduction
PART 1. Adrenal haemorrhage:• An overview• Pathophysiology
PART 2. Imaging in adrenal haemorrhage:
• Different imaging possibilities• Positive and negative aspects of each
type• Image examples

What is adrenal haemorrhage?• Uncommon, usually presents as bilateral
haemorrhage. (Light, 2006)
• Can occur at any age. (Light, 2006)
• Extensive necrosis of all three cortical layers and medulla. (Tritos, 2007)
• Can cause volume lossand shock in infantsand acute adrenalinsufficiency unlessrecognised andtreated properly.(Light, 2006)
Adrenal haemorrhage at autopsy Image: Underwood
(2004)

PathophysiologyCauses of adrenal haemorrhage:• Coagulopathies: causing thrombosis in
renal and adrenal veins.
• Waterhouse-Friderichsen syndrome: in children and young adults (occurring in 20% of meningitis cases).
• Trauma: found in 28% of severe trauma cases autopsy. (Sevitt, 1955)
• Asphyxia: in neonates – at birth the adrenal gland is very large and vascular.
• Also associated with adrenal tumours. (Light, 2006)

Imaging: Computed tomographyCT scanning is the preferred method for
identifying adrenal haemorrhage in all patients over 6 months old.
CT is rapid, widely available and accurate in diagnosis.
• Useful for the identification of an underlying neoplasm, tumour or large thrombosis.
• Allows examination of the adrenal glands in trauma patients with other imaging indications.
Adrenal haemorrhage is detected as a round or oval mass obliterating the normal chevron shape of the adrenal gland. (Light, 2006)

Imaging: Computed tomographyCT of normal adrenals several
months before the onset of haemorrhage.
CT two weeks after the onset of an acute haemorrhage.
Images excerpted from: Rao et al. (1989)

Imaging: Computed tomography
CT of acute bilateral haemorrhage. Image: Hentel (2008)

Imaging: Magnetic ResonanceIn general MRI identifies adrenal
abnormalities at a rate which is comparable to CT.
• Not as widely available as CT.• May be preferable in younger people due to CT
radiation risk:– 1 fatal cancer per 2000 scans. (FDA, 2007)
– 20% increased lifetime cancer mortality risk. (FDA, 2007)
– 5 fatal cancers per 6000 scans in under 15s.– May account for up to 2% of cancers in the US.
(Brenner, 2007)
• Evidence for these studies is 25,000 survivors of Hiroshima bombing. Not directly comparable?
(BRER, 2006)

Imaging: Magnetic Resonance
T1 weighted MRI displaying right adrenal infarction without haemorrhage, in a 42-year-old man with anti phospholipid syndrome. Image: Riddell and Khalili (2004)

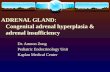
Imaging: UltrasoundUS is the standard in neonates for
imaging adrenal masses.
• It is sensitive for enlargements of the adrenal glands.
• Can differentiate between causes of adrenal mass.
• Echogenicity is variable with the age of the haemotoma – can estimate age.
• Widely available.
• No ionising radiation.
• But US is operator dependant. (Light, 2006)

Imaging: Ultrasound
An adrenal haemorrhage as seen on ultrasound.Image: Hentel
(2008)

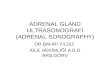
Imaging: Ultrasound
An adrenal haemorrhage as seen with Doppler ultrasound. This enables the avascular nature of the mass to be identified. Image: Hentel (2008)

Imaging: UltrasoundAdrenal
haemorrhage in a foetus at 34 weeks gestation caused by a neuroblastoma.
Image: Trop and Levine (2001)

Imaging: Other modalitiesPlain radiographs: Acute adrenal
haemorrhage is rarely detectable. It may cause mass effect in the upper abdomen. (Light, 2006)
Image: Kawashima et al. (1999)

Imaging: Other modalitiesNuclear medicine studies: Of very
little use as the main contrast agents used are not taken up by haematoma or normal adrenal tissue. (Light, 2006)
Image: Kawashima et al. (1999)

Summary
• Adrenal haemorrhage is an uncommon but serious condition which causes adrenal insufficiency.
• CT is the diagnostic method of choice.
• MRI should be considered as an alternative in children.
• Ultrasound should be used in neonates.

ReferencesBRENNER, D. J. (2007) Computed Tomography — An Increasing Source of Radiation Exposure. the New England
Journal of Medicine, 357 pp. 2277-2284.
BRER (2006) Health risks from exposure to low levels of ionizing radiation — BEIR VII, 1st ed. Washington, DC: The National Academies Press.
FDA (2007) What are the Radiation Risks from CT? [online]. Available from: http://www.fda.gov/cdrh/ct/risks.html [accessed: 28 Feb 2008].
HENTEL, B. (2008) Adrenal hemorrhage [online]. Available from: http://www.radswiki.net/main/index.php?title=Adrenal_hemorrhage [accessed: 23 Feb 08].
KAWASHIMA, A., SANDLER, C. M., ERNST, R. D., TAKAHASHI, N., ROUBIDOUX, M. A., GOLDMAN, S. M. et al. (1999) Imaging of Nontraumatic Hemorrhage of the Adrenal Gland. RadioGraphics, 19 pp. 949-963.
LIGHT, D. (2006) Adrenal Hemorrhage [online]. Available from: http://www.emedicine.com/radio/topic15.htm [accessed: 23 Feb 2008].
RAO, R. H., VAGNUCCI, A. H. and AMICO, J. A. (1989) Bilateral massive adrenal hemorrhage: early recognition and treatment. Annals of Internal Medicine, 110 (3), pp. 227-235.
RIDDELL, A. M. and KHALILI, K. (2004) Sequential Adrenal Infarction Without MRI-Detectable Hemorrhage in Primary Antiphospholipid-Antibody Syndrome. American Journal of Roentgenology, 183 pp. 220-222.
SEWITT, S. (1995) Post-traumatic adrenal apoplexy. Journal of Clinical Pathology, 8 (3), pp. 184-194.
TRITOS, N. A. (2007) Adrenal Hemorrhage [online]. Available from: http://www.emedicine.com/MED/topic3009.htm [accessed: 28 Feb 2008].
TROP, I. and LEVINE, D. (2001) Hemorrhage During Pregnancy Sonography and MR Imaging. American Journal of Roentgenology, 176 pp. 607-615.
UNDERWOOD, J. C. E. (Ed.) (2004) General and Systemic Pathology, 4th ed. London: Churchill Livingstone.