



ESPEN Congress Leipzig 2013
A life inside: probiotics in practice
Probiotics in acute diarrhoea: friends or foe?
S. Kolacek (HR)
Sanja Kolaček
FRIENDS or FOE ??
IN ACUTE DIARRHOEA
PROBIOTICS
Children’s Hospital Zagreb

aims To discuss
Role in treatment of acute diarrhoea
GUT flora & Probiotics Basic facts
Role in prevention of acute diarrhoea: - Nosocomial / health related
- Antibiotic associated / Clostridium difficile - Traveller’s diarrhoea
Probiotics Safety issues
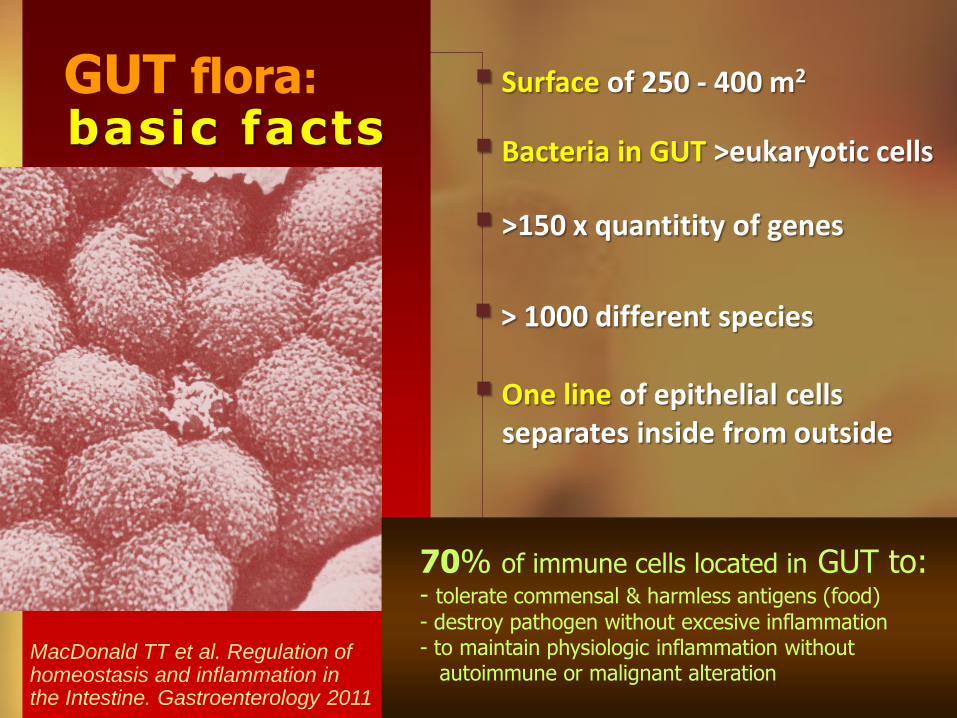
GUT flora: basic facts
Surface of 250 - 400 m2
One line of epithelial cells separates inside from outside
> 1000 different species
MacDonald TT et al. Regulation of homeostasis and inflammation in the Intestine. Gastroenterology 2011
Bacteria in GUT >eukaryotic cells
70% of immune cells located in GUT to: - tolerate commensal & harmless antigens (food)
- destroy pathogen without excesive inflammation - to maintain physiologic inflammation without autoimmune or malignant alteration
>150 x quantitity of genes
Firmicutes Bacteroides
Kelly et al. Immunological Review, 2012
Immunomodulatory
role of GUT flora
Anti-infectious
Trophic and metabolic
Vael C, et al. Importance of development of intestinal microflora. Curr Opin Pediatr 2009; Thomas FW, et al. Probiotics and prebiotics in pediatrics. Pediatrics 2010;126
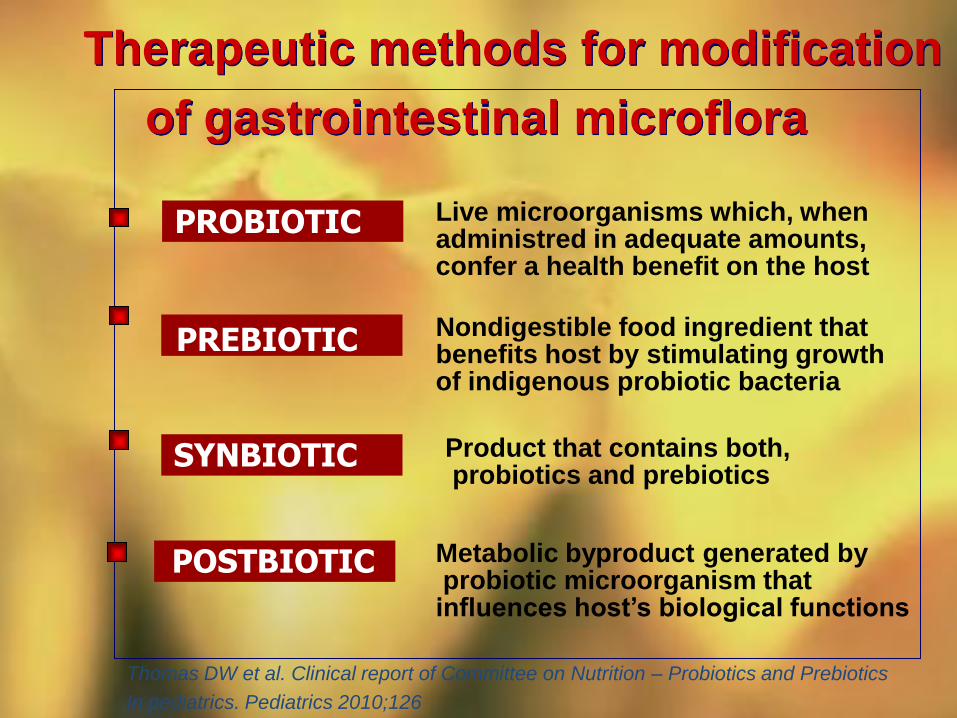
of gastrointestinal microflora
Live microorganisms which, when administred in adequate amounts, confer a health benefit on the host
SYNBIOTIC
Therapeutic methods for modification
PROBIOTIC
Thomas DW et al. Clinical report of Committee on Nutrition – Probiotics and Prebiotics
In pediatrics. Pediatrics 2010;126
POSTBIOTIC
PREBIOTIC Nondigestible food ingredient that benefits host by stimulating growth of indigenous probiotic bacteria
Product that contains both, probiotics and prebiotics
Metabolic byproduct generated by probiotic microorganism that influences host’s biological functions
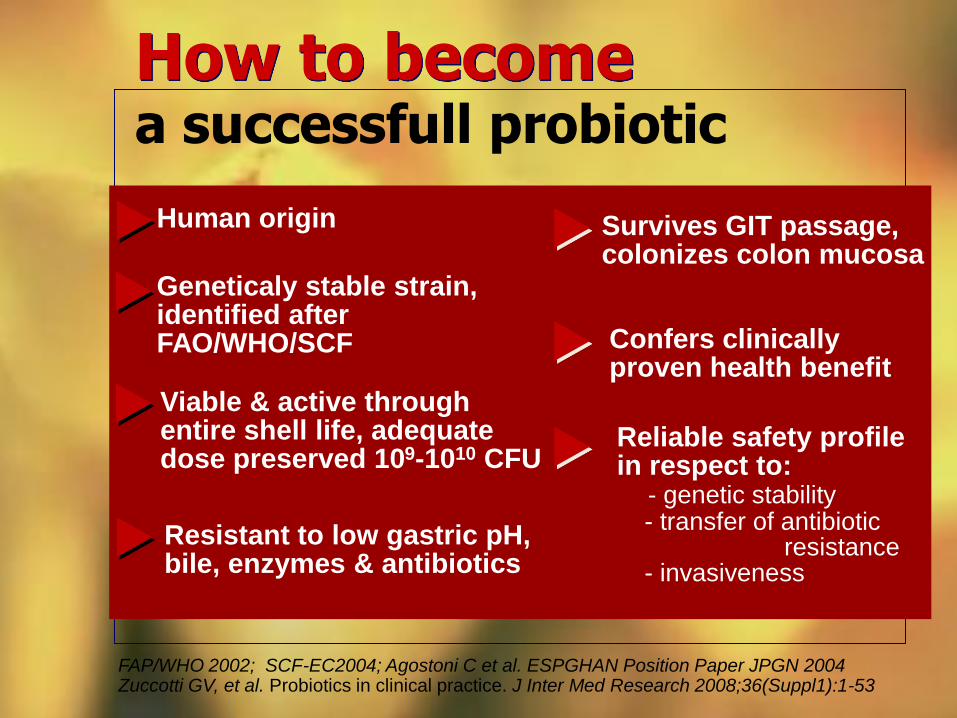
a successfull probiotic How to become
Human origin
Confers clinically proven health benefit
Viable & active through entire shell life, adequate dose preserved 109-1010 CFU
Geneticaly stable strain, identified after FAO/WHO/SCF
FAP/WHO 2002; SCF-EC2004; Agostoni C et al. ESPGHAN Position Paper JPGN 2004 Zuccotti GV, et al. Probiotics in clinical practice. J Inter Med Research 2008;36(Suppl1):1-53
Resistant to low gastric pH, bile, enzymes & antibiotics
Survives GIT passage, colonizes colon mucosa
Reliable safety profile in respect to: - genetic stability - transfer of antibiotic resistance - invasiveness
ROLE OF PROBIOTICS IN THE TREATMENT OF ACUTE
DIARRHOEA
Developing countries
- highest incidence (> 6x/y in a child)
- accounts for 1.78 million deaths (3.7% of total deaths)
most in children ≤ 5y
Is diarrhoea still a burden ?
Developed countries - still cause of hospitalization
- costs of health care
- work absentism of diseased adults / parents
- increased incidence & severity of CDAD
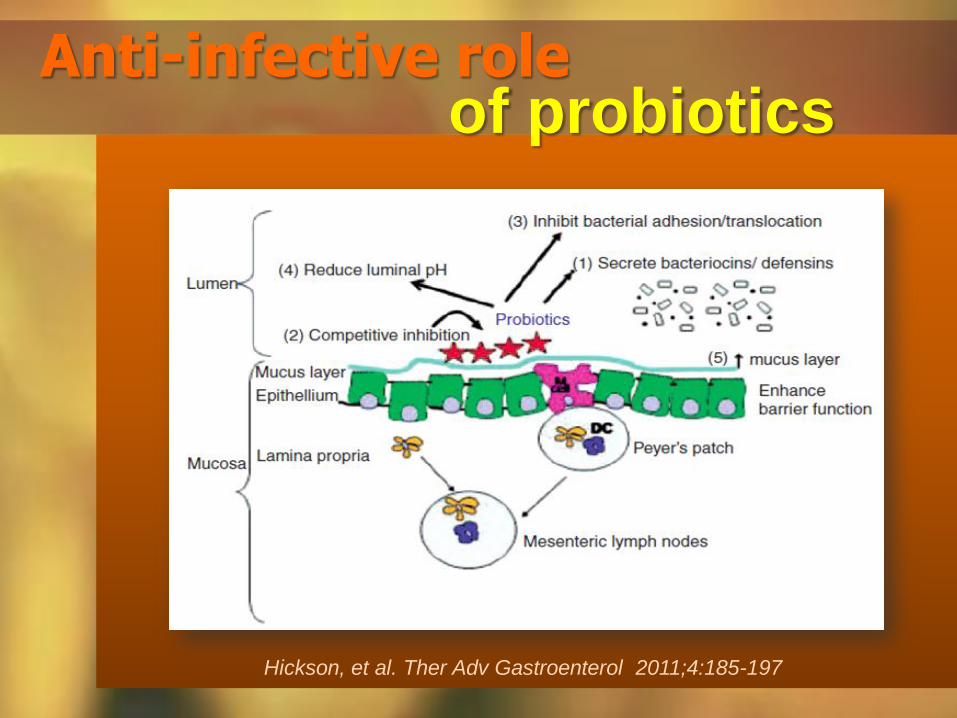
Anti-infective role of probiotics
Hickson, et al. Ther Adv Gastroenterol 2011;4:185-197
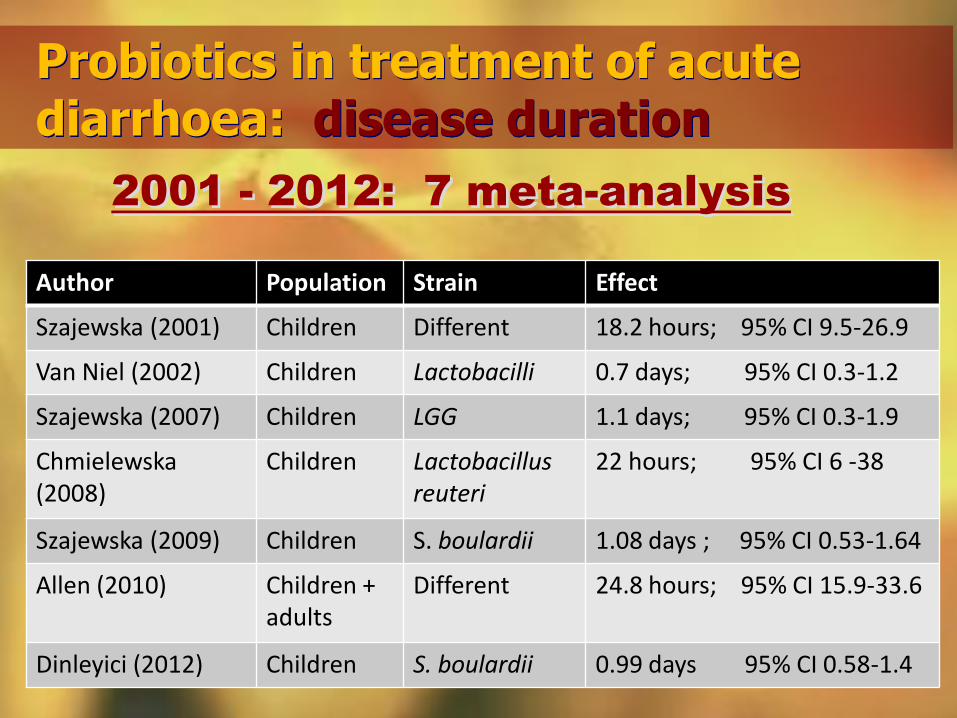
Author Population Strain Effect
Szajewska (2001) Children Different 18.2 hours; 95% CI 9.5-26.9
Van Niel (2002) Children Lactobacilli 0.7 days; 95% CI 0.3-1.2
Szajewska (2007) Children LGG 1.1 days; 95% CI 0.3-1.9
Chmielewska (2008)
Children Lactobacillus reuteri
22 hours; 95% CI 6 -38
Szajewska (2009) Children S. boulardii 1.08 days ; 95% CI 0.53-1.64
Allen (2010) Children + adults
Different 24.8 hours; 95% CI 15.9-33.6
Dinleyici (2012) Children S. boulardii 0.99 days 95% CI 0.58-1.4
Probiotics in treatment of acute diarrhoea: disease duration
2001 - 2012: 7 meta-analysis
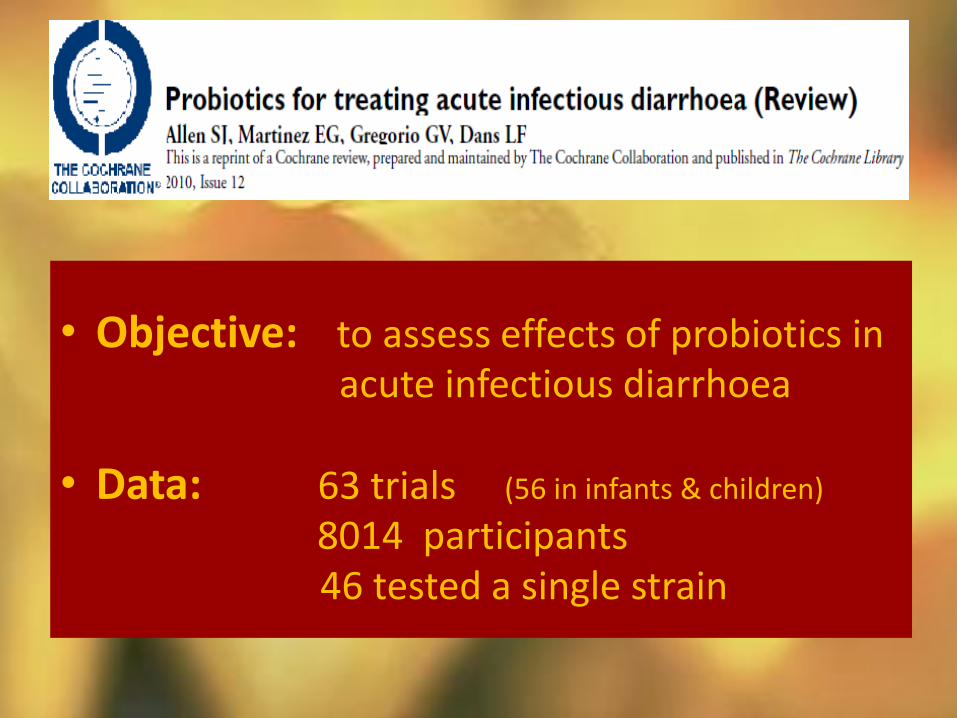
• Objective: to assess effects of probiotics in acute infectious diarrhoea • Data: 63 trials (56 in infants & children)
8014 participants 46 tested a single strain
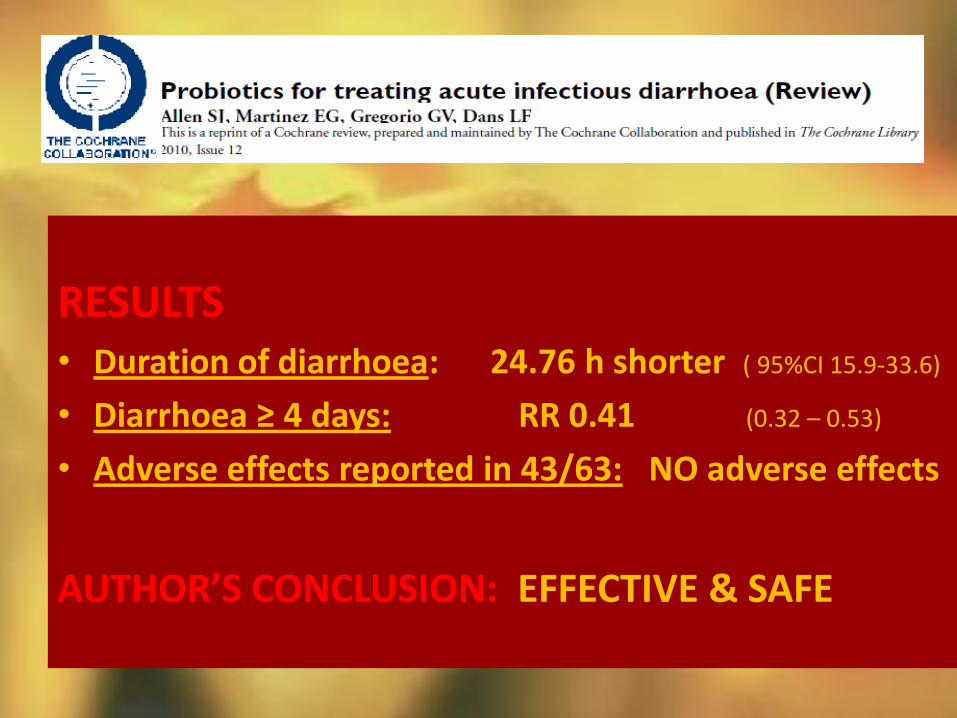
RESULTS • Duration of diarrhoea: 24.76 h shorter ( 95%CI 15.9-33.6)
• Diarrhoea ≥ 4 days: RR 0.41 (0.32 – 0.53)
• Adverse effects reported in 43/63: NO adverse effects
AUTHOR’S CONCLUSION: EFFECTIVE & SAFE
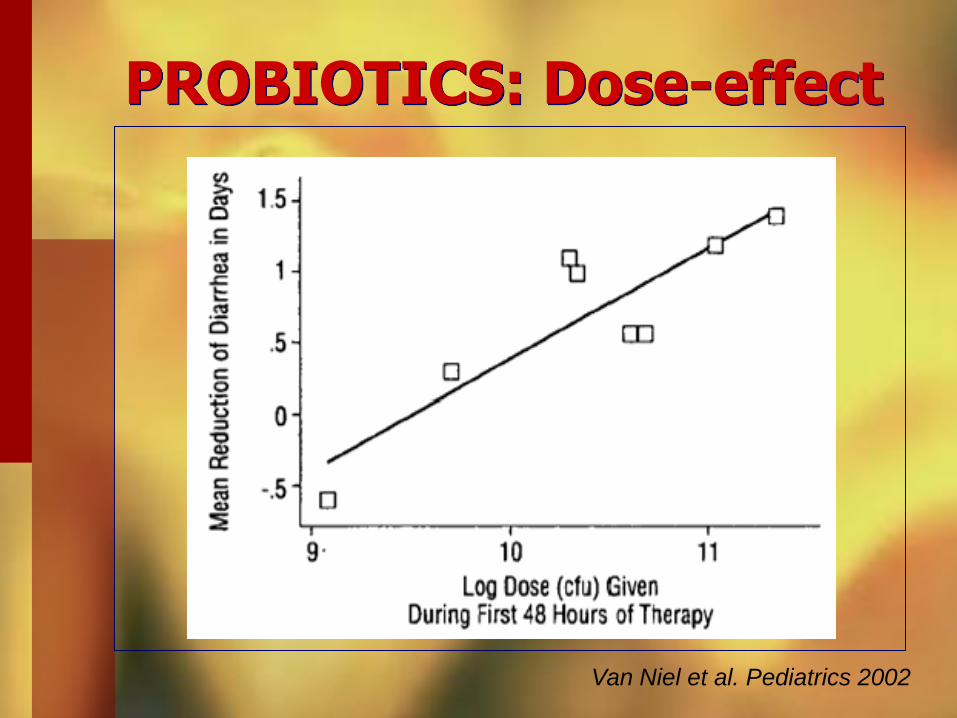
PROBIOTICS: Dose-effect
Van Niel et al. Pediatrics 2002
Role of probiotics in treatment of acute diarrhoea: CONCLUSIONS
Dose related: better if >1010 CFU
Effective: shorten diarrhoea
diarrhoea less severe
Work better in watery (viral)
diarrhoea & if initiated early
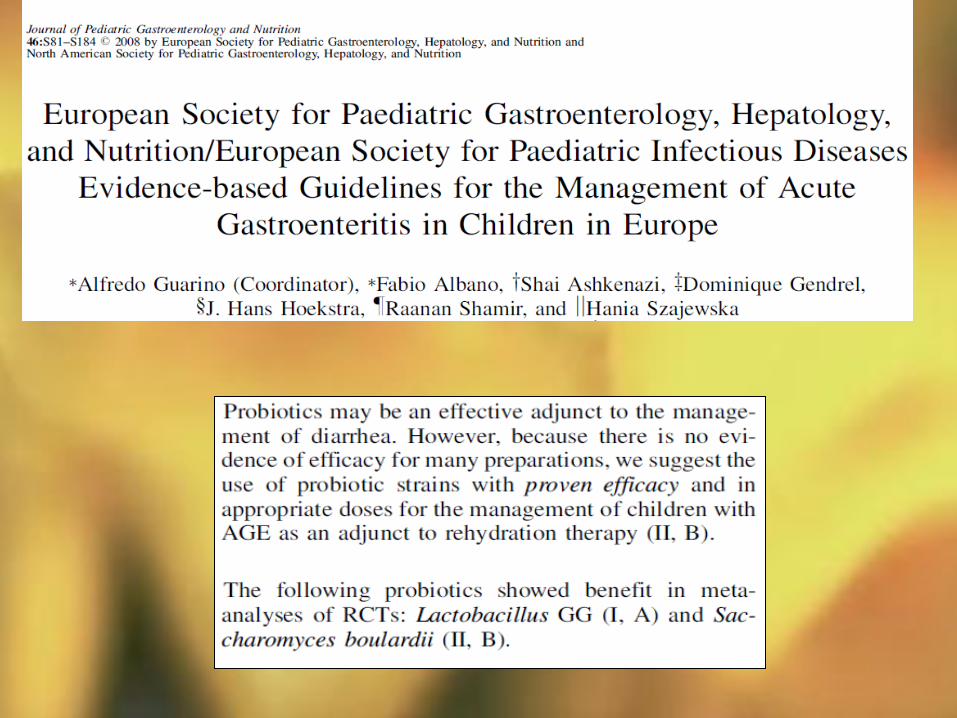
Strain related: S. boulardii, LGG
however!!
Guarino et al. J Pediatr Gastroenterol Nutr. 2008;46:619-21.
Probiotics in PREVENTION of acute diarrhoea
Nosocomial diarrhoea
Traveller’s diarrhoea
Antibiotic associated
Clostridium difficile prevention & treat.
Nosocomial infection – incidence
Acute care hospitals – 5 to 10% of hospitalized patients
– 90,000 deaths/year (5th leading cause of mort.)
– 25% in ICU
– add extra $5 billion/year to cost of patient care
– risk of acquiring infection 2–20x higher in developing countries
Chen et al. Infect Control Hosp Epidemiol. 2009;30:39–46.
Sydnor et al. Clin Microbiol Rev. 2011 Jan;24(1):141-73.
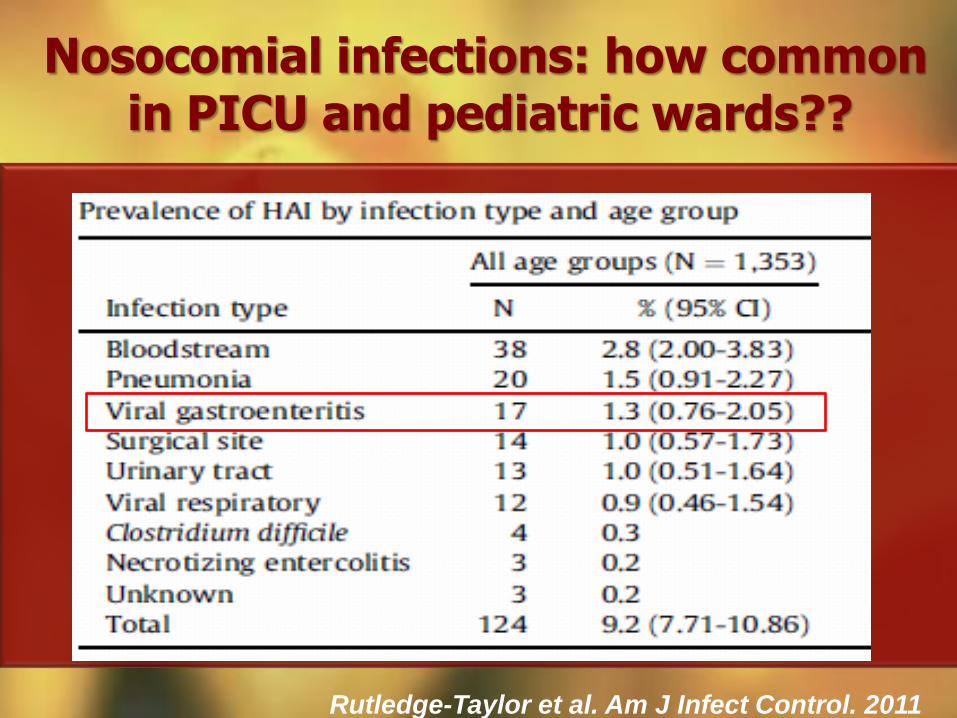
Nosocomial infections: how common in PICU and pediatric wards??
Rutledge-Taylor et al. Am J Infect Control. 2011
Probiotics in prevention of nosocomial diarrhoea
- 4 in acute care centres - 2 in hospitals for prolonged care
- 3 used LGG - 3 used other probiotics
6 RANDOMIZED CONTROLLED TRIALS -RCT
TYPE OF FACILITY
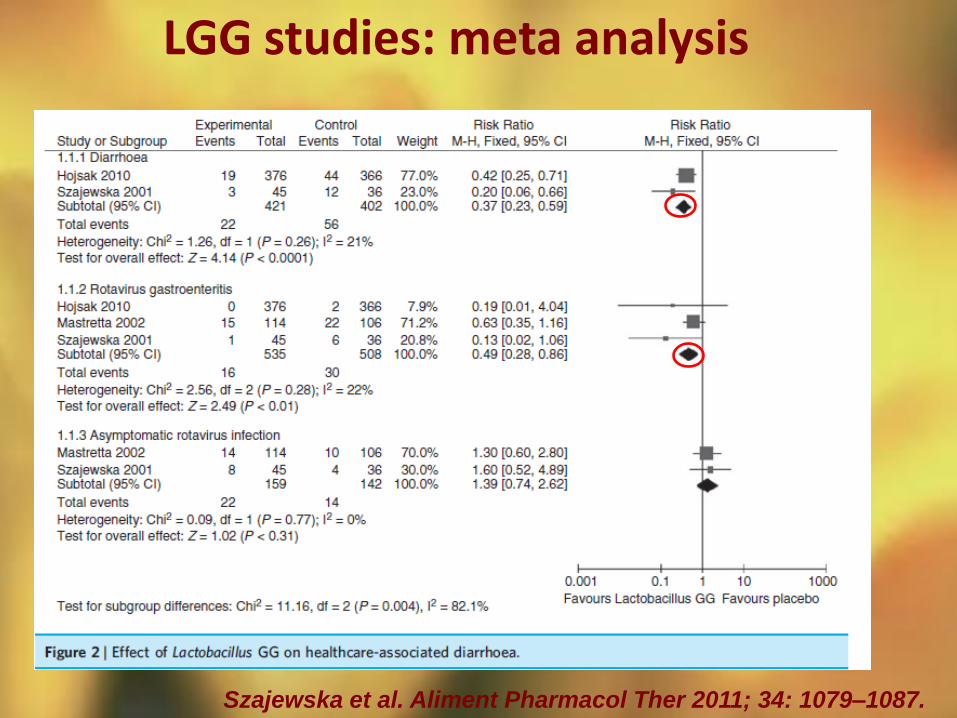
LGG studies: meta analysis
Szajewska et al. Aliment Pharmacol Ther 2011; 34: 1079–1087.
Role of probiotics in prevention of nosocomial diarrhoea: CONCLUSIONS
PROMISING in prevention of
nosocomial diarrhoea (LGG)
Work best in ACUTE hospital
setting but with PROLONGED
in-hospital stay
ROLE OF PROBIOTICS IN PREVENTION OF
ANTIBIOTIC ASSOCIATED DIARRHOEA (ADD) & CDAD

• Oral broad spectrum antibiotics:
- clindamycin - beta-lactams - amoxicillin - cephalosporines • Very young / very old
• ProIonged antibiotic use
• Hospitalization
• Previous AAD
Risk factors for AAD Clinical data & epidemiology • Incidence: 5% - 40% of
patients
• Mostly mild course
• In hospitalized old& young immunocomp. patients:
- toxic megacolon
- bowel preforation
- death
Antibiotic associated diarrhoea - AAD
Butler et al. BMJ. 2012;344:e682.
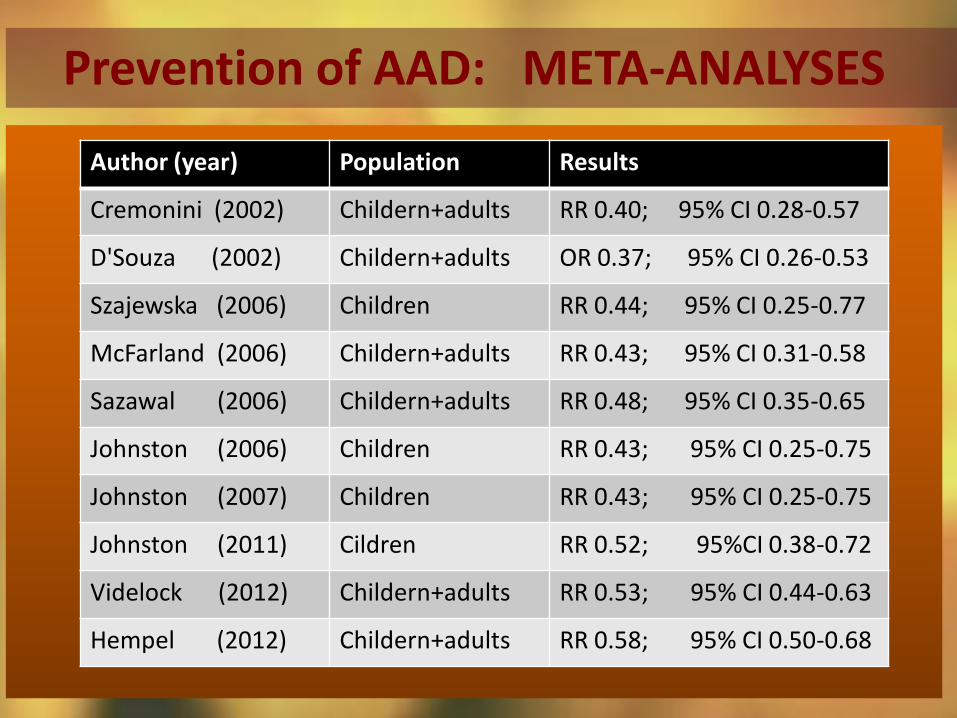
Prevention of AAD: META-ANALYSES
Author (year) Population Results
Cremonini (2002) Childern+adults RR 0.40; 95% CI 0.28-0.57
D'Souza (2002) Childern+adults OR 0.37; 95% CI 0.26-0.53
Szajewska (2006) Children RR 0.44; 95% CI 0.25-0.77
McFarland (2006) Childern+adults RR 0.43; 95% CI 0.31-0.58
Sazawal (2006) Childern+adults RR 0.48; 95% CI 0.35-0.65
Johnston (2006) Children RR 0.43; 95% CI 0.25-0.75
Johnston (2007) Children RR 0.43; 95% CI 0.25-0.75
Johnston (2011) Cildren RR 0.52; 95%CI 0.38-0.72
Videlock (2012) Childern+adults RR 0.53; 95% CI 0.44-0.63
Hempel (2012) Childern+adults RR 0.58; 95% CI 0.50-0.68
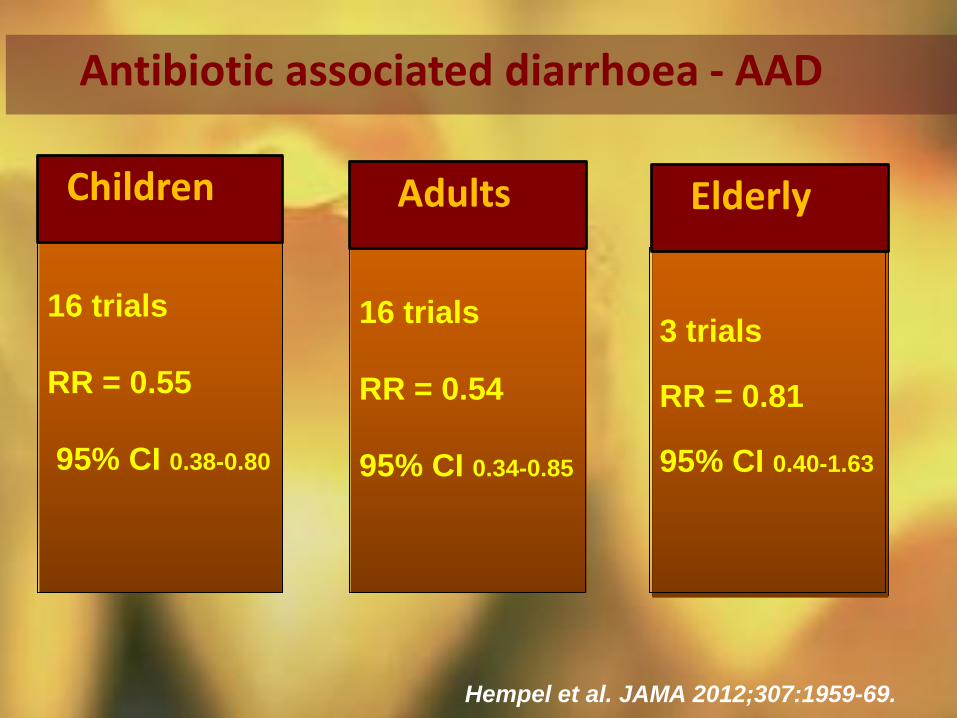
16 trials
RR = 0.55
95% CI 0.38-0.80
Children
16 trials
RR = 0.54
95% CI 0.34-0.85
Antibiotic associated diarrhoea - AAD
3 trials
RR = 0.81
95% CI 0.40-1.63
Adults Elderly
Hempel et al. JAMA 2012;307:1959-69.
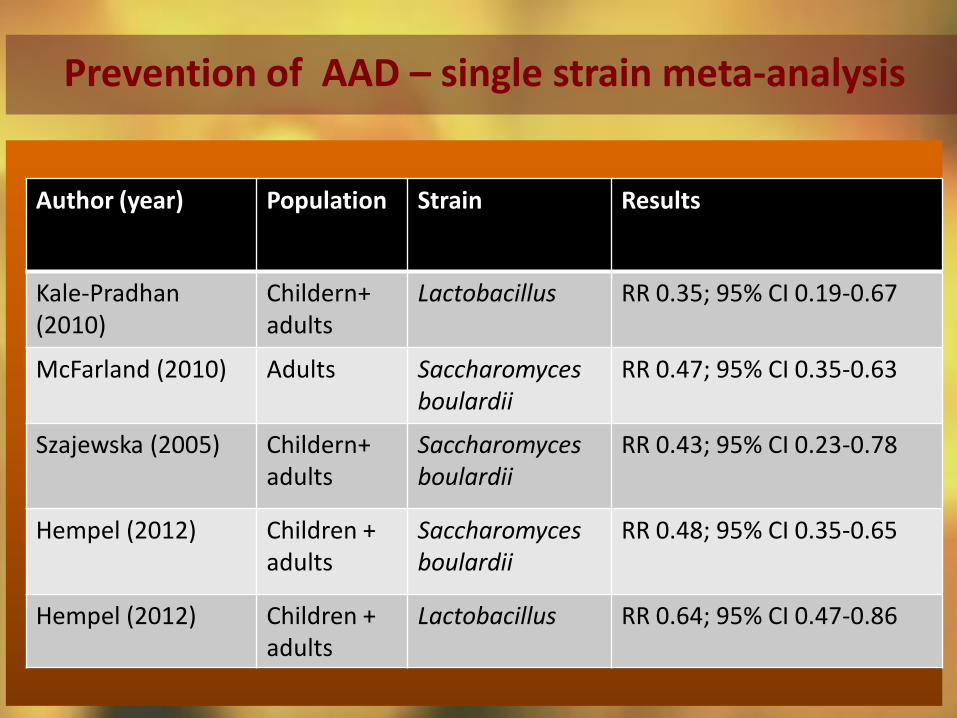
Prevention of AAD – single strain meta-analysis
Author (year) Population Strain Results
Kale-Pradhan (2010)
Childern+ adults
Lactobacillus RR 0.35; 95% CI 0.19-0.67
McFarland (2010) Adults Saccharomyces boulardii
RR 0.47; 95% CI 0.35-0.63
Szajewska (2005) Childern+ adults
Saccharomyces boulardii
RR 0.43; 95% CI 0.23-0.78
Hempel (2012) Children + adults
Saccharomyces boulardii
RR 0.48; 95% CI 0.35-0.65
Hempel (2012) Children + adults
Lactobacillus
RR 0.64; 95% CI 0.47-0.86
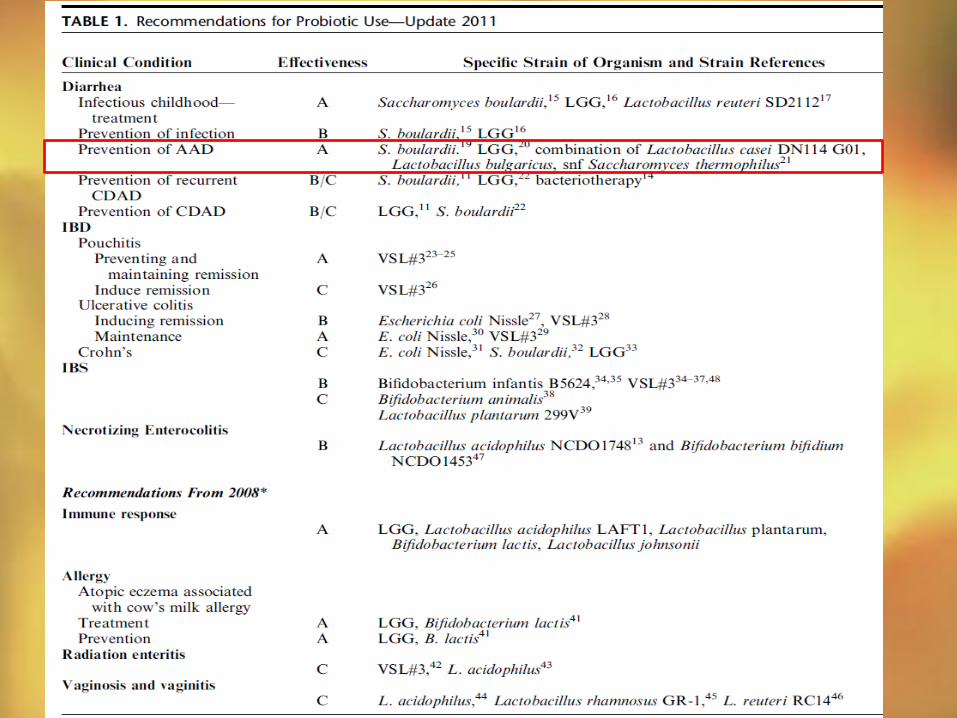
J Clin Gastroenterol 2011;45:S168–S171
AAD is mostly mild, self-limited
condition!! WHEN TO PREVENT??
Risk factors for severe disease: - very young / elderly
- hospitalized & chronically ill
- caused by Clostridium difficile
Probiotic in prevention of AAD
Serious problem: more virulent strains
resistant, 10% mortality
recurrence 10%-30%
Increased costs: 3.6 d longer in hospital
3.669 USD / day
Clostridium diff associated diarrhoea - CDAD
Common: 10%-30% of AAD
> 300 000 hospitalized/y in USA
Risk factors: old, hospitalized,
on antibiotics, immunocompromised
Cartman ST. Intern Med Microb 2010; Friedman G. Gastroenterol Clin N Am 2012
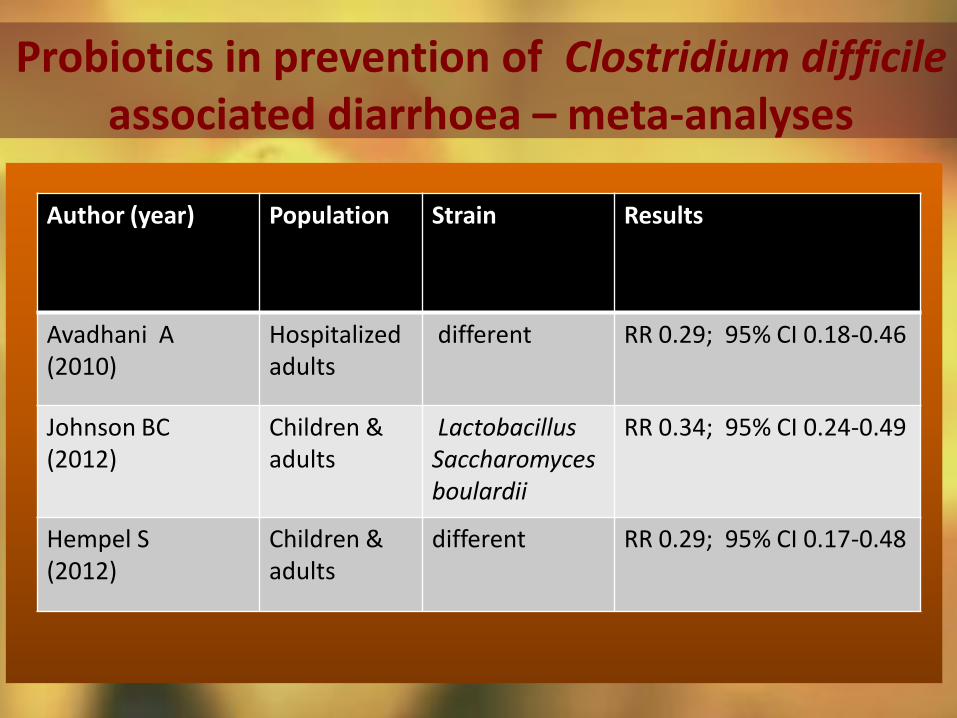
Probiotics in prevention of Clostridium difficile associated diarrhoea – meta-analyses
Author (year) Population Strain Results
Avadhani A (2010)
Hospitalized adults
different RR 0.29; 95% CI 0.18-0.46
Johnson BC (2012)
Children & adults
Lactobacillus Saccharomyces boulardii
RR 0.34; 95% CI 0.24-0.49
Hempel S (2012)
Children & adults
different RR 0.29; 95% CI 0.17-0.48
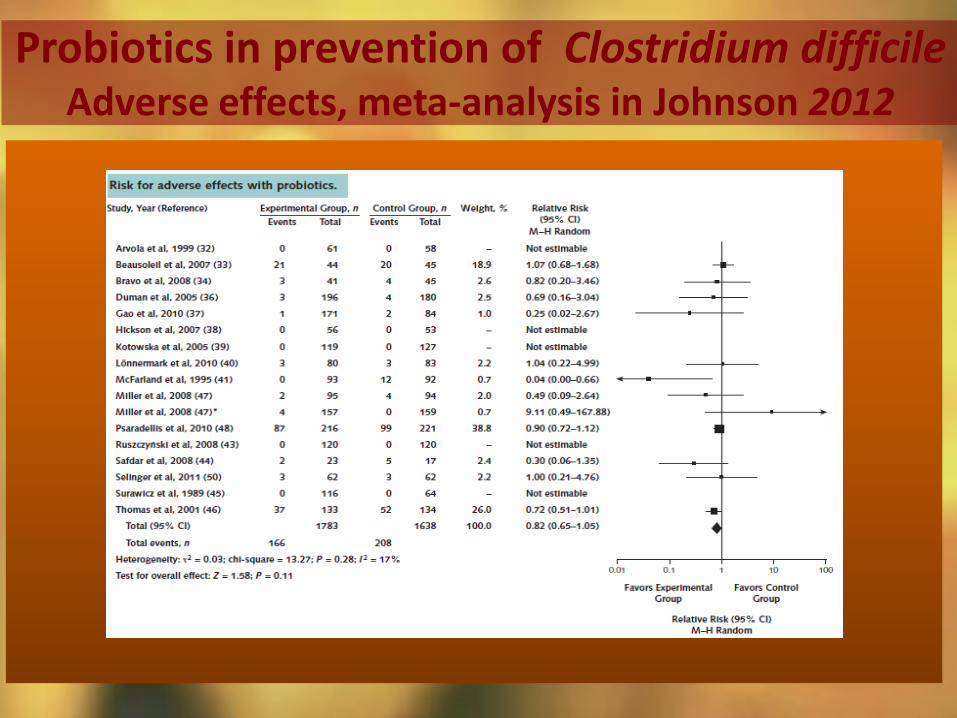
Probiotics in prevention of Clostridium difficile Adverse effects, meta-analysis in Johnson 2012
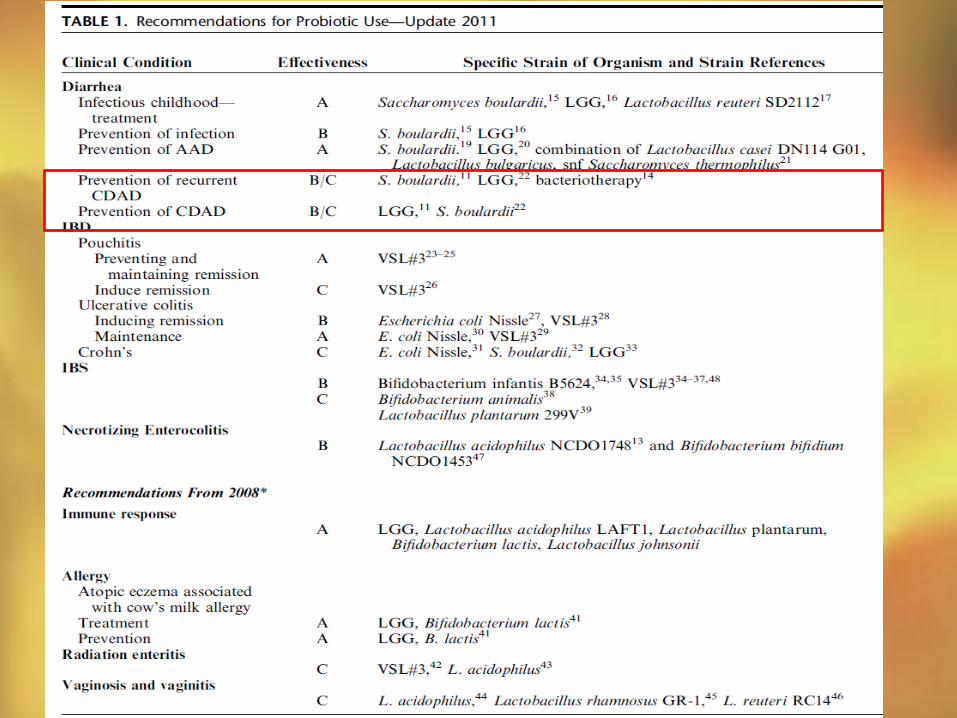
Probiotics in prevention of AAD & CDAD CONCLUSIONS
Effective !!!
Saccharomyces, Lactobacillus
most commonly studied
To be used in patients when severe course is anticipated: - Hospitalized , sick, very young/very old, recurrent ADD
- In Clostridium difficile associated diarrhoea
- However, patients often immunocompromised
→ SAFETY ISSUES
ROLE OF PROBIOTICS IN PREVENTION OF
TRAVELER’S DIARRHOEA
> 100 million travelers / year
10%-15% travel into high risk areas tropical/subtropical Latin America
the Caribbean, South Asia, Africa
TRAVELER’S DIARRHOEA - A PROBLEM ??
Up to 40 million cases / year
de la Cabada Bauche et al. Gastroenterol Hepatol (N Y) 2011;7:88-95
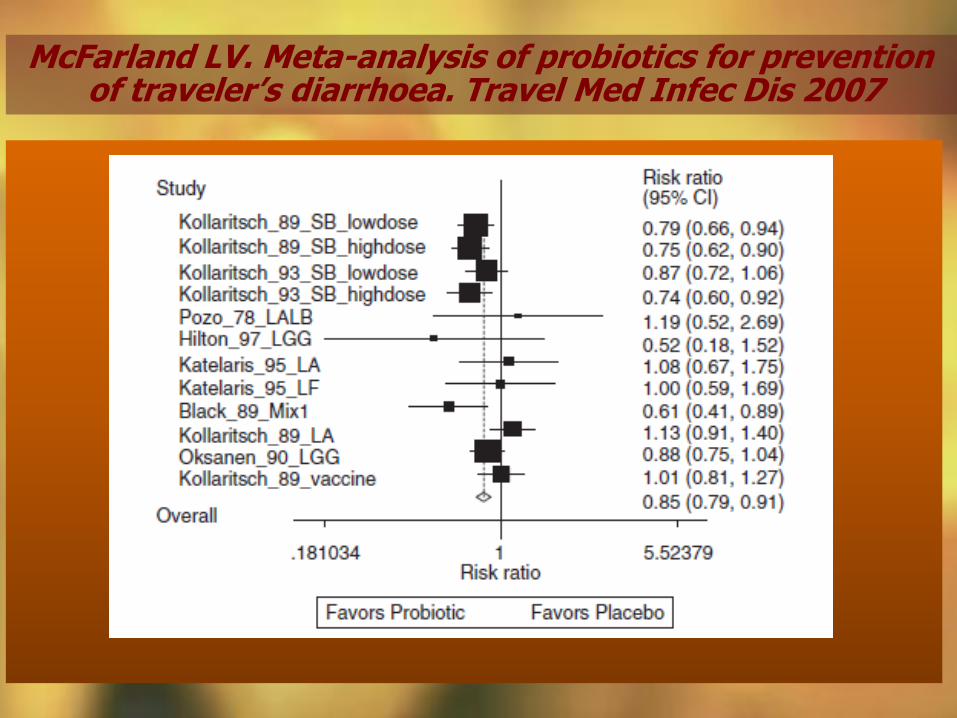
McFarland LV. Meta-analysis of probiotics for prevention of traveler’s diarrhoea. Travel Med Infec Dis 2007
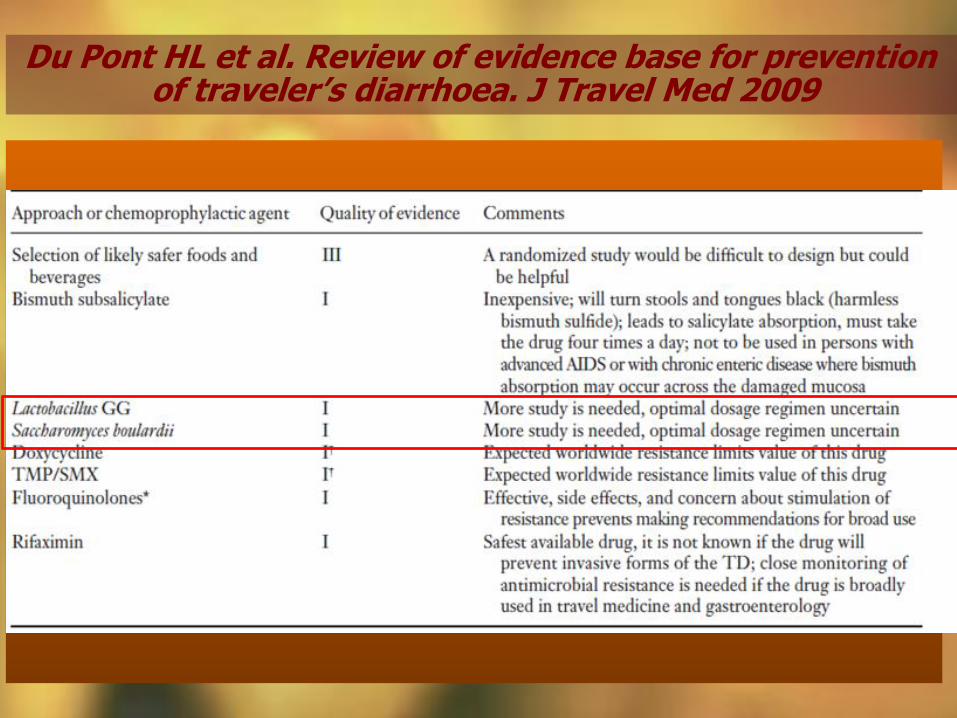
Du Pont HL et al. Review of evidence base for prevention of traveler’s diarrhoea. J Travel Med 2009
PROBIOTICS
SAFETY ISSUES
Probiotics as a foe??
Potential mechanisms ??
Infective dissemination
Transfer of antibiotic resistance
Transfer of genetic material
Long term saftey issues
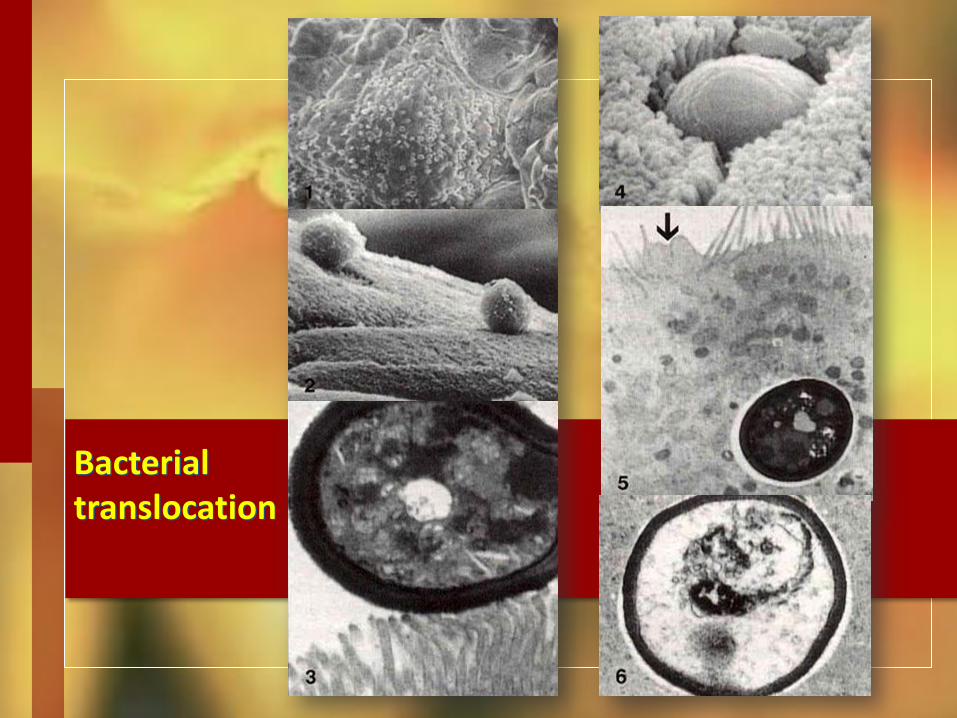
Bacterial translocation
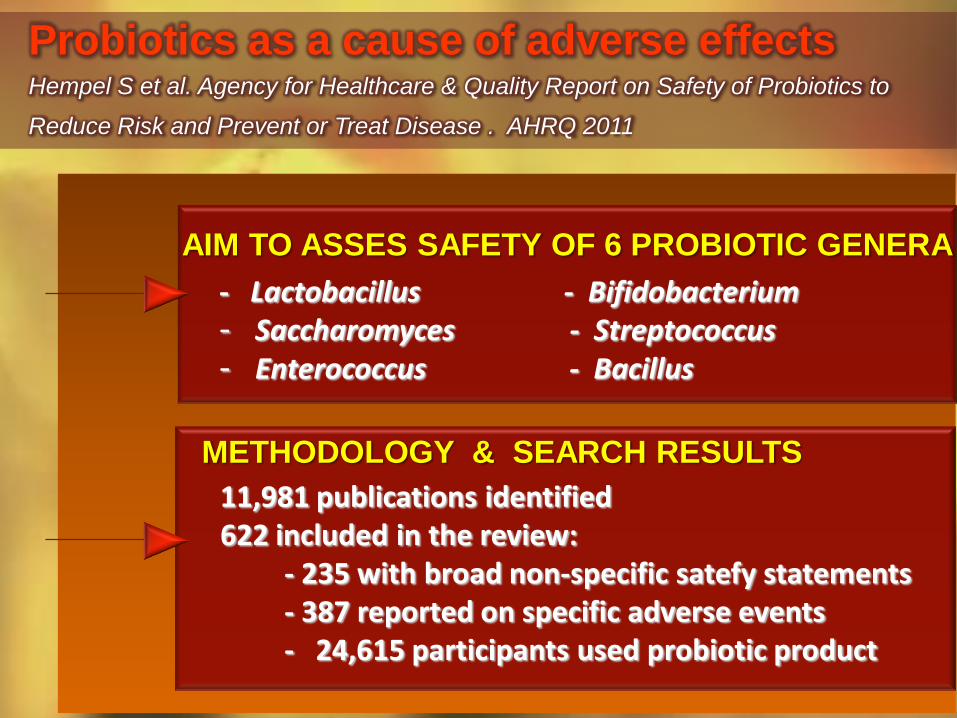
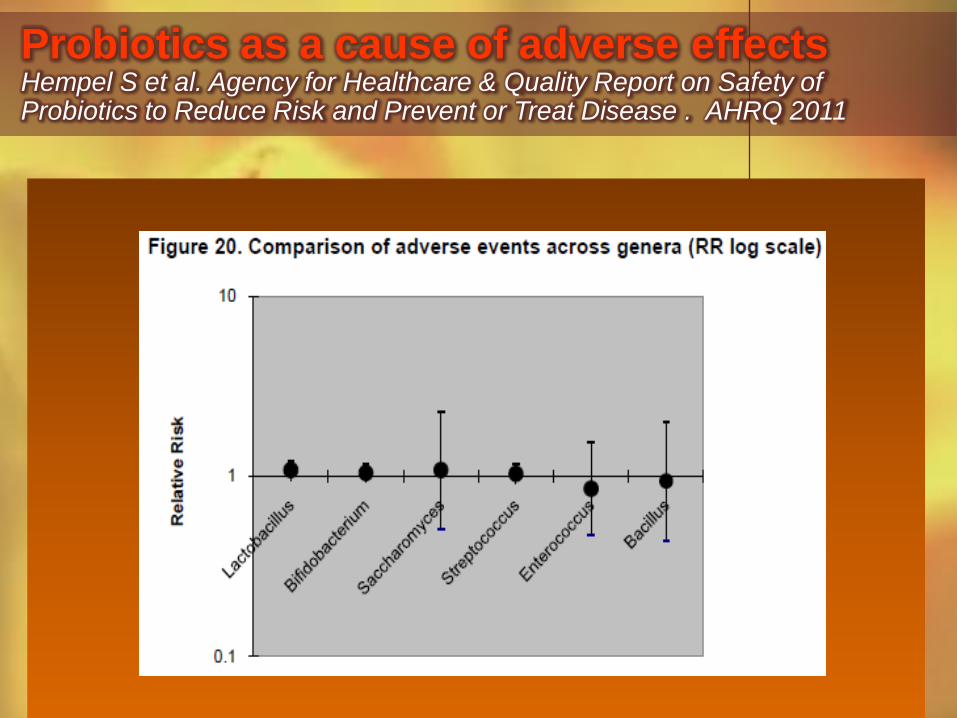
Probiotics as a cause of adverse effects Hempel S et al. Agency for Healthcare & Quality Report on Safety of Probiotics to
Reduce Risk and Prevent or Treat Disease . AHRQ 2011
11,981 publications identified 622 included in the review: - 235 with broad non-specific satefy statements - 387 reported on specific adverse events - 24,615 participants used probiotic product
- Lactobacillus - Bifidobacterium - Saccharomyces - Streptococcus - Enterococcus - Bacillus
AIM TO ASSES SAFETY OF 6 PROBIOTIC GENERA
METHODOLOGY & SEARCH RESULTS
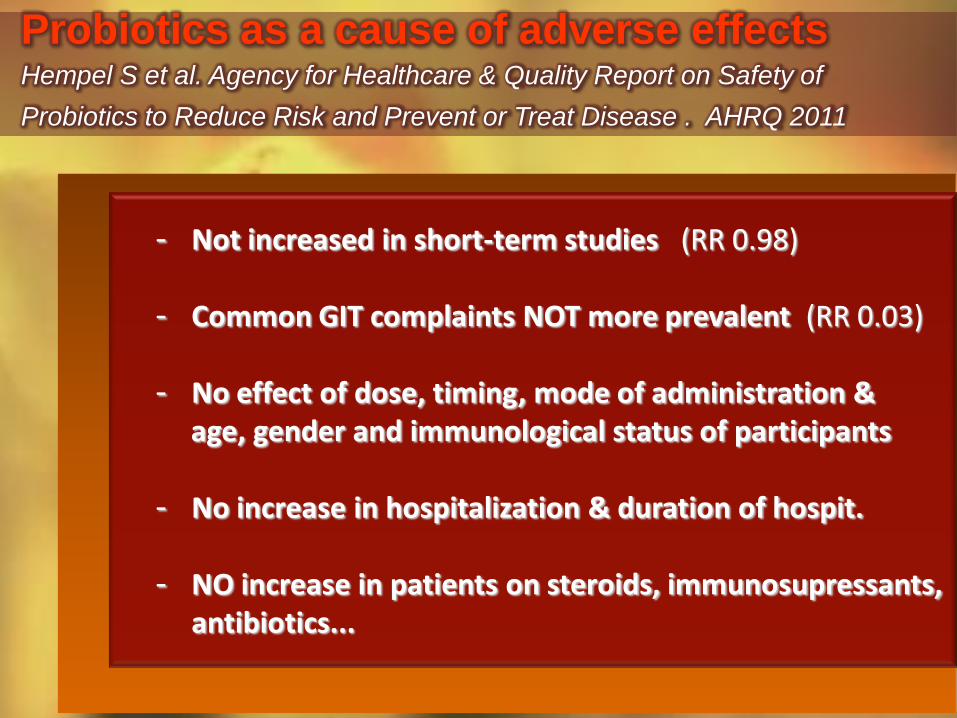
Probiotics as a cause of adverse effects Hempel S et al. Agency for Healthcare & Quality Report on Safety of
Probiotics to Reduce Risk and Prevent or Treat Disease . AHRQ 2011
- Not increased in short-term studies (RR 0.98) - Common GIT complaints NOT more prevalent (RR 0.03) - No effect of dose, timing, mode of administration & age, gender and immunological status of participants - No increase in hospitalization & duration of hospit. - NO increase in patients on steroids, immunosupressants,
antibiotics...
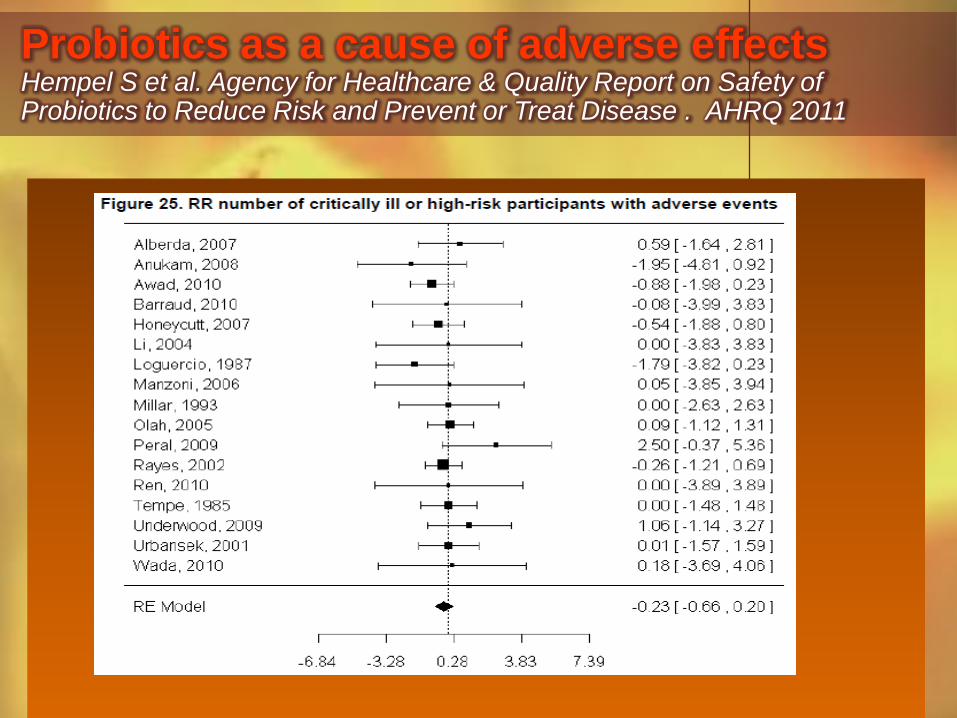
Probiotics as a cause of adverse effects Hempel S et al. Agency for Healthcare & Quality Report on Safety of Probiotics to Reduce Risk and Prevent or Treat Disease . AHRQ 2011
Probiotics as a cause of adverse effects Hempel S et al. Agency for Healthcare & Quality Report on Safety of Probiotics to Reduce Risk and Prevent or Treat Disease . AHRQ 2011
Probiotics as a cause of adverse effects Hempel S et al. Agency for Healthcare & Quality Report on Safety of Probiotics to Reduce Risk and Prevent or Treat Disease . AHRQ 2011
- Lack of assessment & systematic reporting - Very few studies with adverse effects as
primary outcome
- Current evidence not equipped to answer specific questions on safety
HOWEVER
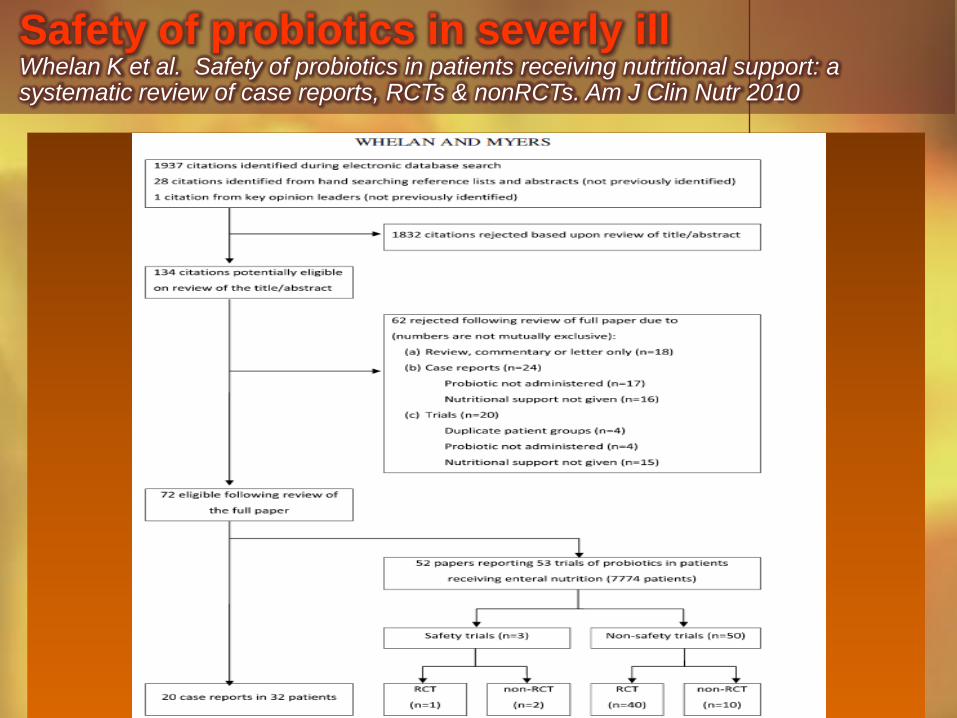
Safety of probiotics in severly ill Whelan K et al. Safety of probiotics in patients receiving nutritional support: a systematic review of case reports, RCTs & nonRCTs. Am J Clin Nutr 2010
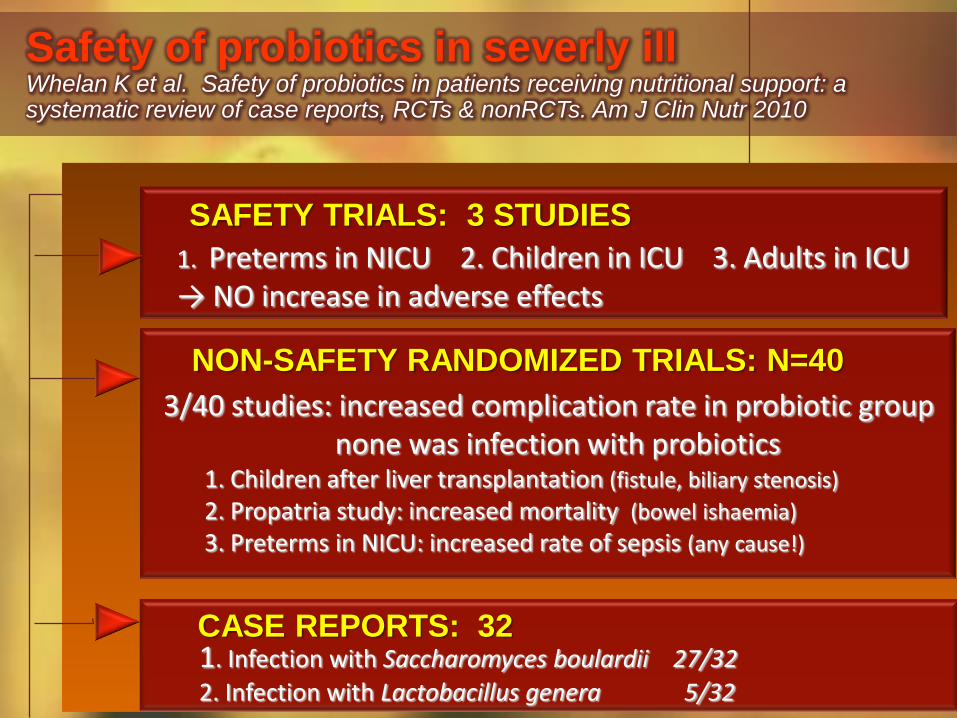
3/40 studies: increased complication rate in probiotic group none was infection with probiotics 1. Children after liver transplantation (fistule, biliary stenosis)
2. Propatria study: increased mortality (bowel ishaemia)
3. Preterms in NICU: increased rate of sepsis (any cause!)
1. Preterms in NICU 2. Children in ICU 3. Adults in ICU → NO increase in adverse effects
SAFETY TRIALS: 3 STUDIES
NON-SAFETY RANDOMIZED TRIALS: N=40
Safety of probiotics in severly ill Whelan K et al. Safety of probiotics in patients receiving nutritional support: a systematic review of case reports, RCTs & nonRCTs. Am J Clin Nutr 2010
CASE REPORTS: 32 1. Infection with Saccharomyces boulardii 27/32
2. Infection with Lactobacillus genera 5/32
SAFETY OF PROBIOTICS Hojsak I, Shamir R. In Guarino A... Probiotic bacteria... Basel, Karger 2013, Vol 107
- All together 45 episodes - S. Boulardii & cerevisiae 27 - Lactobacillus 13 (Lactobacillus GG, acidophilus, casei)
- Bacillus cereus 3 - Bifidobacterium 2
- All episodes were in severelly ill patients
PUBLISHED CASE REPORTS ON PROBIOTIC
STRAIN CAUSED SEPSIS
Probiotics as a foe??
Potential mechanisms ??
Infective dissemination: proven but
only in severly ill patients
Transfer of antibiotic resistance: possible, not documented in humans
Transfer of genetic material possible, particularly to designed „turbo”
probiotics, but never in vivo proven
Long term saftey issues important for use in infant formula - unknown
Current evidence does not indicate increased risk in not severly sick
PROBIOTICS AS A FOE: CONCLUSIONS
FDA grants GRAS status to Bidifobacteria & Lactobacillus
Probiotics could be very usefull in sick patients (prevention of CD infection) but special caution is required
When introducing probiotic strain: premarketing assessment & postmark. surveillance
RCT with adverse effects as primary outcome
THANK YOU
FOR YOUR
KIND
ATTENTION


























![Probiotics: A New Horizon for Treating Childhood Diarrhea in … · 2017-06-21 · [25]. Two systematic reviews of probiotics in acute diarrhea have been published where the effects](https://static.cupdf.com/doc/110x72/5f956936f32fc2056e41e4e1/probiotics-a-new-horizon-for-treating-childhood-diarrhea-in-2017-06-21-25.jpg)