




1
Legal Limits onLegal Limits onHME MarketingHME Marketing
Carrie Bryant, Esq., CHCCarrie Bryant, Esq., CHCCompliance OfficerCompliance Officer
American HomePatientAmerican HomePatient
William T. Mathias, Esq.William T. Mathias, Esq.PrincipalPrincipal
Ober|KalerOber|Kaler
2
Outline of PresentationOutline of Presentation
BackgroundBackground Legal Limits on MarketingLegal Limits on Marketing
Anti-kickback StatuteAnti-kickback Statute Stark Self-referral LawStark Self-referral Law False Claims ActFalse Claims Act Prohibition Against Beneficiary InducementsProhibition Against Beneficiary Inducements State LawState Law HIPAA/HITECHHIPAA/HITECH Medicare Anti-solicitation LawMedicare Anti-solicitation Law
Recent GuidanceRecent Guidance Changing Compliance EnvironmentChanging Compliance Environment
3
Some Things Don’t ChangeSome Things Don’t Change
Medicare and Medicaid regulations Medicare and Medicaid regulations remain incredibly complexremain incredibly complex
4
““There can be no doubt but that the statutes There can be no doubt but that the statutes and provisions in question, involving the and provisions in question, involving the financing of Medicare and Medicaid, are financing of Medicare and Medicaid, are among the most completely impenetrable among the most completely impenetrable texts within human experience. Indeed, texts within human experience. Indeed, one approaches them at the level of one approaches them at the level of specificity herein demanded with dread, for specificity herein demanded with dread, for not only are they dense reading of the most not only are they dense reading of the most tortuous kind, but Congress also revisits the tortuous kind, but Congress also revisits the area frequently, generously cutting and area frequently, generously cutting and pruning in the process and making any solid pruning in the process and making any solid grasp of matters addressed merely a grasp of matters addressed merely a passing phase.”passing phase.”
— Chief Judge ErvinUnited States Court of Appeals for the Fourth Circuit in Rehabilitation Association of Virginia v. Kozlowski, 42 F. 3d 1444, 1450 (4th Circuit 1994)
5
More Things That Don’t ChangeMore Things That Don’t Change
Government continues to view Fraud, Government continues to view Fraud, Waste, and Abuse as a significant Waste, and Abuse as a significant source of revenuesource of revenue
Enforcement remains aggressiveEnforcement remains aggressive

6
Have You Seen the OIG’s Have You Seen the OIG’s Website Lately?Website Lately?
7
Aggressive EnforcementAggressive Enforcement
From new joint DOJ/OIG website From new joint DOJ/OIG website www.stopmedicarefraud.govwww.stopmedicarefraud.gov ““A joint effort by HHS and the A joint effort by HHS and the
Department of Justice recovered a Department of Justice recovered a record $4 billion from fraudsters in record $4 billion from fraudsters in FY2010.”FY2010.”

8
Fighting Fraud is a Good Fighting Fraud is a Good InvestmentInvestment
The return-on-investment (ROI) for The return-on-investment (ROI) for Health Care Fraud and Abuse Control Health Care Fraud and Abuse Control (HCFAC) program(HCFAC) program Since 1997, $4.9 returned for every $1.0 Since 1997, $4.9 returned for every $1.0
expended.expended. 3-year average (2008-2010), $6.8 3-year average (2008-2010), $6.8
returned for every $1.0 expendedreturned for every $1.0 expended

9
Government [Mis]perception of Government [Mis]perception of DME IndustryDME Industry
Government is skeptical of DME Government is skeptical of DME industryindustry
Lack of trustLack of trust Few bad apples have poisoned the Few bad apples have poisoned the
well with governmentwell with government Lead to questions about the overall Lead to questions about the overall
medical necessity of some DMEmedical necessity of some DME Central to government’s regulation Central to government’s regulation
and investigation of DME industryand investigation of DME industry

10
DME Industry Feeling DME Industry Feeling UndervaluedUndervalued
11
Government Balancing IssuesGovernment Balancing Issues
Additional CostAdditional Cost Over, Under, and Mis-UtilizationOver, Under, and Mis-Utilization Quality of CareQuality of Care Access to CareAccess to Care Patients’ Freedom of ChoicePatients’ Freedom of Choice CompetitionCompetition Exercise of Professional JudgmentExercise of Professional Judgment

12
Anti-Kickback StatuteAnti-Kickback Statute

13
Anti-Kickback StatuteAnti-Kickback Statute
Federal anti-kickback law generally Federal anti-kickback law generally prohibits the provision of any prohibits the provision of any economic benefit in exchange for the economic benefit in exchange for the referral of patients or business that referral of patients or business that will be reimbursed under any Federal will be reimbursed under any Federal health care program.health care program. 42 U.S.C. § 1320a-7b(b).42 U.S.C. § 1320a-7b(b).
14
Anti-Kickback StatuteAnti-Kickback Statute
Prohibited ConductProhibited Conduct Knowing & willfulKnowing & willful Solicitation or receipt orSolicitation or receipt or Offer or payment ofOffer or payment of RemunerationRemuneration In return for referring a federal health care In return for referring a federal health care
program patient, orprogram patient, or To induce the purchasing, leasing, or arranging To induce the purchasing, leasing, or arranging
for or recommending purchasing or leasing for or recommending purchasing or leasing items or services paid by a federal health care items or services paid by a federal health care programprogram

15
Anti-Kickback StatuteAnti-Kickback Statute
““Two-way Street”Two-way Street” Meaning that it is just as illegal to solicit Meaning that it is just as illegal to solicit
or accept payments for referrals, as it is or accept payments for referrals, as it is to offer or make such payments. to offer or make such payments.

16
Anti-Kickback StatuteAnti-Kickback Statute
PenaltiesPenalties Criminal fines & imprisonmentCriminal fines & imprisonment Civil money penalty of $50,000 plus 3X Civil money penalty of $50,000 plus 3X
the amount of the remuneration the amount of the remuneration ExclusionExclusion False Claims Act liabilityFalse Claims Act liability
Section 6402 (f)(1) of PPACA makes Anti-Section 6402 (f)(1) of PPACA makes Anti-Kickback violations actionable under FCAKickback violations actionable under FCA
17
Relevant AKS Safe HarborsRelevant AKS Safe Harbors [42 C.F.R. § 1001.952] [42 C.F.R. § 1001.952]
Personal Services & Management Personal Services & Management Contracts Safe HarborContracts Safe Harbor
Employment Exception and Safe Employment Exception and Safe HarborHarbor
Space Lease Safe HarborSpace Lease Safe Harbor Equipment Lease Safe HarborEquipment Lease Safe Harbor
18
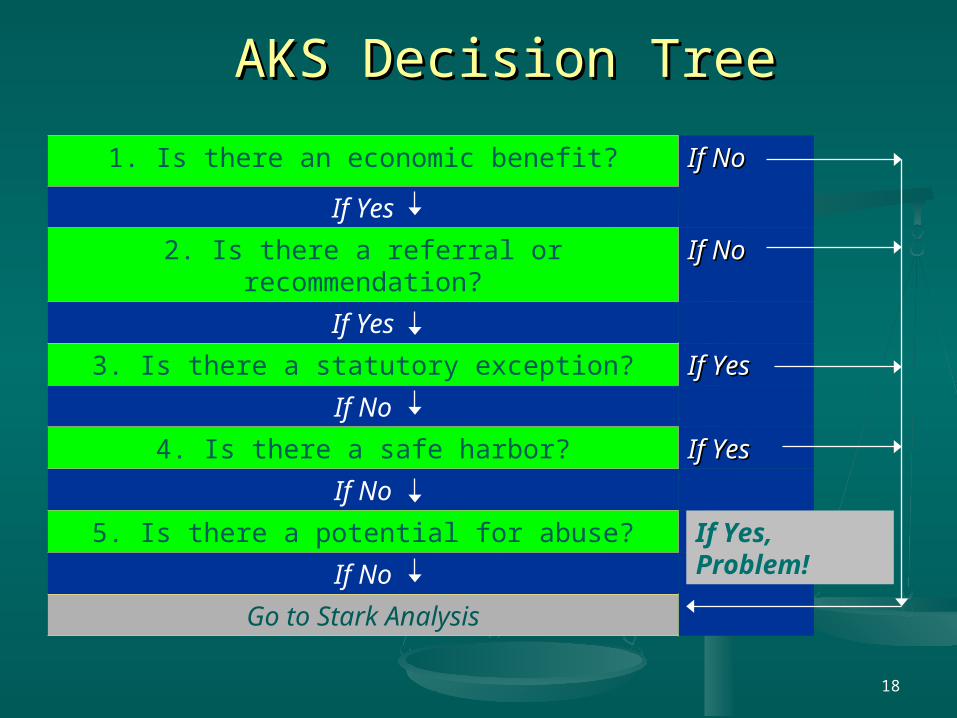
AKS Decision TreeAKS Decision Tree
1. Is there an economic benefit? If NoIf No
If Yes
2. Is there a referral or recommendation? If NoIf No
If Yes
3. Is there a statutory exception? If YesIf Yes
If No
4. Is there a safe harbor? If YesIf Yes
If No
5. Is there a potential for abuse?
If No
Go to Stark Analysis
If Yes, Problem!
19
Stark Physician Stark Physician Self-Referral LawSelf-Referral Law

20
Stark Self-Referral LawStark Self-Referral Law
The federal Stark physician self-The federal Stark physician self-referral law generally prohibits a referral law generally prohibits a physician from making referrals to an physician from making referrals to an entity for any of eleven (11) entity for any of eleven (11) designated health services if the designated health services if the physician (or an immediate family physician (or an immediate family member) has a “financial member) has a “financial relationship” with the entity. relationship” with the entity. 42 U.S.C. § 1395nn42 U.S.C. § 1395nn

21
Stark Self-Referral LawStark Self-Referral Law
Physician may not refer:Physician may not refer: Medicare [or Medicaid] patientsMedicare [or Medicaid] patients For “designated health services”For “designated health services” to an entity with which the physician orto an entity with which the physician or an immediate family member has an immediate family member has a “financial relationship”a “financial relationship”
Ownership interest – through equity or debtOwnership interest – through equity or debt Compensation arrangementCompensation arrangement
Unless the relationship fits in an exceptionUnless the relationship fits in an exception
22
Stark Self-Referral LawStark Self-Referral Law ““Designated health services”Designated health services”
Clinical laboratoryClinical laboratory DMEDME Orthotics & ProstheticsOrthotics & Prosthetics PEN PEN Home HealthHome Health Radiology Radiology Radiation TherapyRadiation Therapy PT/OTPT/OT Inpatient Hospital Services Inpatient Hospital Services Outpatient Hospital servicesOutpatient Hospital services Outpatient drugsOutpatient drugs

23
Stark Self-Referral LawStark Self-Referral Law
PenaltiesPenalties Denial of PaymentDenial of Payment $15,000 per service$15,000 per service 2X damages2X damages ExclusionExclusion False Claims Act liabilityFalse Claims Act liability
24
Relevant Stark ExceptionsRelevant Stark Exceptions
Personal services Personal services Employment Employment Space rentalsSpace rentals Equipment rentalsEquipment rentals Fair market value compensationFair market value compensation Non-monetary compensation Non-monetary compensation
(<$359 in 2011)(<$359 in 2011)
25
Relevant Stark Exceptions (cont.)Relevant Stark Exceptions (cont.)
In-office Ancillary Services Exception In-office Ancillary Services Exception Limited exception for DMEPOS itemsLimited exception for DMEPOS items
Canes, crutches, walkers, and folding Canes, crutches, walkers, and folding wheelchairswheelchairs
Blood glucose monitorsBlood glucose monitors Infusion pumps that are DME (not Infusion pumps that are DME (not
infusion pumps used for parenteral infusion pumps used for parenteral and enteral nutrition)and enteral nutrition)
No other DME covered by this exceptionNo other DME covered by this exception

26
Stark Decision Tree
If No
If Yes
Okay!
If Yes
If Yes
If Yes
If Yes
6. Is there a regulatory exception?
If Yes5. Is there a statutory exception?
If No4. Is there a designated health service?
If No3. Is there a referral?
If No2. Is there a direct or indirect financial relationship?
If No1. Is there a physician or immediate family member?
If No, Problem!

27
False Claims ActFalse Claims Act
28
Federal False Claims ActFederal False Claims Act Prohibits Prohibits
filing, or causing to be filedfiling, or causing to be filed ““false or fraudulent” claimsfalse or fraudulent” claims Using false statement to “conceal, avoid Using false statement to “conceal, avoid
or decrease” a government obligationor decrease” a government obligation IntentIntent
““Intent to defraud” not requiredIntent to defraud” not required Filing claims with “reckless disregard” of Filing claims with “reckless disregard” of
their truth or falsity is sufficienttheir truth or falsity is sufficient LiabilityLiability
3X Damages3X Damages $5,500 to $11,000 per claim$5,500 to $11,000 per claim

29
Prohibition Against Beneficiary Prohibition Against Beneficiary InducementsInducements
30
Prohibition Against Beneficiary Prohibition Against Beneficiary InducementsInducements
Prohibits offering or paying remuneration Prohibits offering or paying remuneration to any Medicare or Medicaid beneficiary to any Medicare or Medicaid beneficiary that the offeror knows, or should know, is that the offeror knows, or should know, is likely to influence the recipient to order an likely to influence the recipient to order an item from a particular supplier.item from a particular supplier. 42 U.S.C. § 1320a-7a(a)42 U.S.C. § 1320a-7a(a)
Exception for items of nominal value – $10 Exception for items of nominal value – $10 per item and $50 per beneficiary per yearper item and $50 per beneficiary per year
31
State LawsState Laws
32
State LawsState Laws
Don’t forget about state lawsDon’t forget about state laws State fraud and abuse lawsState fraud and abuse laws State mini-Stark lawsState mini-Stark laws Fee splitting prohibitionsFee splitting prohibitions Patient brokering lawsPatient brokering laws State licensing lawsState licensing laws Corporate practice of medicineCorporate practice of medicine State False Claims ActsState False Claims Acts

33
Health Insurance Portability and Health Insurance Portability and Accountability Act (HIPAA)Accountability Act (HIPAA)

34
HIPAA/PrivacyHIPAA/Privacy
HIPAA requires “covered entities” to HIPAA requires “covered entities” to adhere to certain basic requirements adhere to certain basic requirements aimed at protecting the privacy of aimed at protecting the privacy of “protected health information” (PHI)“protected health information” (PHI)

35
HIPAA/PHIHIPAA/PHI
Protected Health InformationProtected Health Information Information related to past, present, or Information related to past, present, or
future physical or mental health condition future physical or mental health condition or provision of health care services –and–or provision of health care services –and–
Information related to payment for health Information related to payment for health care services.care services.
Information can be linked to a particular Information can be linked to a particular individual.individual.
Information regardless of form or medium Information regardless of form or medium (electronic, written, or verbal).(electronic, written, or verbal).

36
HIPAA/Uses & DisclosuresHIPAA/Uses & Disclosures
PHI may not be used or disclosed unless PHI may not be used or disclosed unless use or disclosure is specifically permitted use or disclosure is specifically permitted by HIPAA or authorized by patient.by HIPAA or authorized by patient.
Permitted Uses and Disclosures include: Permitted Uses and Disclosures include: TreatmentTreatment PaymentPayment Health Care OperationsHealth Care Operations Other uses and disclosures as specified in Other uses and disclosures as specified in
Notice of Privacy PracticesNotice of Privacy Practices
37
HIPAA/Original DefinitionHIPAA/Original Definitionof Marketingof Marketing
Marketing means:Marketing means: ““To make a communication about a To make a communication about a
product or service that encourages product or service that encourages recipients of the communication to recipients of the communication to purchase or use the product or purchase or use the product or service....”service....”

38
HIPAA/Exceptions to Definition HIPAA/Exceptions to Definition of Marketingof Marketing
Definition of marketing does not Definition of marketing does not include:include: communications to describe a health-communications to describe a health-
related product or service (or payment for related product or service (or payment for such product or service) that is provided by, such product or service) that is provided by, or included in a plan of benefits of, the or included in a plan of benefits of, the covered entity making the communicationcovered entity making the communication
communications for treatment of the communications for treatment of the individualindividual
communications for case management or communications for case management or care coordination for the individual, or to care coordination for the individual, or to direct or recommend alternative direct or recommend alternative treatments, therapies, health care treatments, therapies, health care providers, or settings of care to the providers, or settings of care to the individualindividual
39
HIPAA/HITECH ChangesHIPAA/HITECH Changesto Marketingto Marketing
HITECH Act made changes to the definition HITECH Act made changes to the definition of “Marketing”of “Marketing” Where covered entity receives “direct or Where covered entity receives “direct or
indirect payment” marketing communication indirect payment” marketing communication not considered “health care operation” (so not considered “health care operation” (so patient authorization required)patient authorization required)
Limited exceptions :Limited exceptions : Communication regarding a currently Communication regarding a currently
prescribed drug or biological (for which prescribed drug or biological (for which payment must be “reasonable”)payment must be “reasonable”)
Communication made by business associate Communication made by business associate according to the terms of business associate according to the terms of business associate agreement.agreement.
““Direct or indirect payment” does not Direct or indirect payment” does not include payment for treatment.include payment for treatment.
40
HIPAA/HITECH Changes to HIPAA/HITECH Changes to Marketing – Proposed RuleMarketing – Proposed Rule
PROPOSED Rule – not finalPROPOSED Rule – not final Differentiates between “treatment” Differentiates between “treatment”
and “marketing” communicationsand “marketing” communications Under PROPOSED RuleUnder PROPOSED Rule
Notice of potentially subsidized Notice of potentially subsidized treatment communications must be treatment communications must be included in notice of privacy practices included in notice of privacy practices with opt-out procedurewith opt-out procedure
Communication must identify what is Communication must identify what is subsidized.subsidized.

41
HIPAA/HITECH Changes to HIPAA/HITECH Changes to Marketing – Proposed RuleMarketing – Proposed Rule
Examples:Examples: Manufacturer pays practice to send out Manufacturer pays practice to send out
flier to all patients advertising new device flier to all patients advertising new device – Marketing– Marketing
Manufacturer pays practice to send out Manufacturer pays practice to send out notice of new device to all patients whose notice of new device to all patients whose treatment might be benefited by new treatment might be benefited by new device – Uncleardevice – Unclear
Manufacturer pays practice to send out Manufacturer pays practice to send out notice of new device to those patients notice of new device to those patients that the practice (not the manufacturer) that the practice (not the manufacturer) identifies as patients who could benefit identifies as patients who could benefit from new device – Treatmentfrom new device – Treatment

42
HIPAA/Marketing & AuthorizationsHIPAA/Marketing & Authorizations
If covered entity’s activities are If covered entity’s activities are “marketing,” the covered entity must “marketing,” the covered entity must obtain an individual’s authorization obtain an individual’s authorization to use or disclose his/her informationto use or disclose his/her information
An authorization is not required:An authorization is not required: if the marketing is a “face-to-face” if the marketing is a “face-to-face”
communication made by a covered communication made by a covered entity to an individual; orentity to an individual; or
the marketing is the provision of a the marketing is the provision of a promotional gift of nominal value promotional gift of nominal value provided by the covered entity.provided by the covered entity.
45 C.F.R. §§ 164.508(a)(3)(i)(A)&(B).45 C.F.R. §§ 164.508(a)(3)(i)(A)&(B).

43
Medicare Anti-solicitation LawMedicare Anti-solicitation Law

44
Medicare Anti-solicitation LawMedicare Anti-solicitation Law[42 U.S.C. § 1395m(a)(17)][42 U.S.C. § 1395m(a)(17)]
Prohibits suppliers from contacting Prohibits suppliers from contacting Medicare beneficiaries by telephone Medicare beneficiaries by telephone regarding covered items unless:regarding covered items unless: Beneficiary has given supplier written Beneficiary has given supplier written
permissionpermission Supplier has previously provided the Supplier has previously provided the
covered item to the beneficiary and covered item to the beneficiary and contact relates to such covered itemcontact relates to such covered item
Supplier has furnished a covered item to Supplier has furnished a covered item to beneficiary in last 15 months, then beneficiary in last 15 months, then contact may relate to any covered itemcontact may relate to any covered item

45
OIG Special Fraud Alert on OIG Special Fraud Alert on DME TelemarketingDME Telemarketing
46
OIG Special Fraud Alert on OIG Special Fraud Alert on DME TelemarketingDME Telemarketing
First issued in 2003 First issued in 2003 68 Fed. Reg. 10254 (Mar. 4, 2003)68 Fed. Reg. 10254 (Mar. 4, 2003)
Updated in 2010Updated in 2010 75 Fed. Reg. 2105 (Jan. 14, 2010)75 Fed. Reg. 2105 (Jan. 14, 2010)
Reflects OIG concerns about DME Reflects OIG concerns about DME telemarketingtelemarketing
47
Original Fraud Alert onOriginal Fraud Alert onDME TelemarketingDME Telemarketing
OIG reiterated the statutory OIG reiterated the statutory telemarketing prohibitionstelemarketing prohibitions
OIG emphasized that “suppliers OIG emphasized that “suppliers cannot do indirectly that which they cannot do indirectly that which they are prohibited from doing directly.”are prohibited from doing directly.” DMEPOS supplier cannot hire an unrelated DMEPOS supplier cannot hire an unrelated
marketing entity to make unsolicited marketing entity to make unsolicited telephone calls to Medicare beneficiaries telephone calls to Medicare beneficiaries to market their products or services. to market their products or services.

48
Updated Fraud Alert on DME Updated Fraud Alert on DME TelemarketingTelemarketing
Largely repeated prior AlertLargely repeated prior Alert Added a concern about DME Added a concern about DME
suppliers contacting beneficiaries suppliers contacting beneficiaries based solely on treating physicians’ based solely on treating physicians’ preliminary verbal or written orderpreliminary verbal or written order
Added reference to criminal and civil Added reference to criminal and civil penalties for using interstate penalties for using interstate telephone calls as part of fraud telephone calls as part of fraud schemescheme
49
Additional Guidance onAdditional Guidance onDME TelemarketingDME Telemarketing
On February 17, 2010, OIG posted On February 17, 2010, OIG posted letter with CMS FAQsletter with CMS FAQs
FAQs provide some helpful guidance FAQs provide some helpful guidance but do not fully resolve issuebut do not fully resolve issue
50
Additional Guidance onAdditional Guidance onDME TelemarketingDME Telemarketing
Not “unsolicited” to return beneficiary’s Not “unsolicited” to return beneficiary’s phone callphone call
Not “unsolicited” if physician contacts Not “unsolicited” if physician contacts supplier on behalf of beneficiary with supplier on behalf of beneficiary with beneficiary’s knowledgebeneficiary’s knowledge
Does supplier need to collect Does supplier need to collect documentation from physician reflecting documentation from physician reflecting beneficiary’s knowledge that physician beneficiary’s knowledge that physician would contact supplier?would contact supplier? No, but it is business decision by supplier to No, but it is business decision by supplier to
collect such documentation.collect such documentation. Supplier cannot ask beneficiary about Supplier cannot ask beneficiary about
other items during initial call, but may on other items during initial call, but may on subsequent call if beneficiary becomes a subsequent call if beneficiary becomes a customercustomer

51
Practical GuidancePractical Guidance

52
Practical GuidancePractical Guidance
Various laws impose restrictions on Various laws impose restrictions on HME marketing activities.HME marketing activities.
Compliance with 1 law does not Compliance with 1 law does not necessarily result in compliance with necessarily result in compliance with other laws.other laws.

53
Practical GuidancePractical GuidanceHIPAA Marketing HIPAA Marketing RestrictionsRestrictions
Medicare Telemarketing Medicare Telemarketing ProhibitionProhibition
Face-to-Face Face-to-Face CommunicationsCommunications
OKOK OKOK
Written communication Written communication without using protected without using protected health information (PHI) health information (PHI)
OKOK OKOK
Written communication Written communication using PHI using PHI
Depends on content:Depends on content:Describing health related Describing health related products – OKproducts – OKTreatment – OKTreatment – OKCare coordination or Care coordination or recommending alternative recommending alternative treatments or settings – treatments or settings – OKOKSelling item unrelated to Selling item unrelated to treatment – NO (need treatment – NO (need authorization)authorization)
OKOK

54
Practical GuidancePractical Guidance
HIPAA Marketing HIPAA Marketing RestrictionsRestrictions
Medicare Telemarketing Medicare Telemarketing ProhibitionProhibition
Telephone call to Telephone call to currentcurrent patientpatient
Depends on content:Depends on content:Describing health related Describing health related products – OKproducts – OKTreatment – OKTreatment – OKCare coordination or Care coordination or recommending alternative recommending alternative treatments or settings – treatments or settings – OKOKSelling item unrelated to Selling item unrelated to treatment – NO (need treatment – NO (need authorization)authorization)
OKOK

55
Practical GuidancePractical Guidance
HIPAA Marketing HIPAA Marketing RestrictionsRestrictions
Medicare Telemarketing Medicare Telemarketing ProhibitionProhibition
Telephone call to Telephone call to formerformer patientpatient
Depends on content:Depends on content:Describing health related Describing health related products – OKproducts – OKTreatment – OKTreatment – OKCare coordination or Care coordination or recommending alternative recommending alternative treatments or settings – treatments or settings – OKOKSelling item unrelated to Selling item unrelated to treatment – NO (need treatment – NO (need authorization)authorization)
Depends on circumstances:Depends on circumstances:Patient has given written Patient has given written permission – OKpermission – OKContacting patient only Contacting patient only regarding covered item regarding covered item previously furnished by previously furnished by Company – OK.Company – OK.Contacting regarding Contacting regarding furnishing a different furnishing a different covered item – OK covered item – OK if within if within 15 months of when 15 months of when Company furnished service Company furnished service to patient.to patient.
56
Recent GuidanceRecent Guidance
57
Advisory Opinions 10-23 & 10-24Advisory Opinions 10-23 & 10-24 OIG analyzed 2 different, but related OIG analyzed 2 different, but related
arrangements between sleep testing arrangements between sleep testing provider and hospitalprovider and hospital
OIG rejected proposed arrangement with OIG rejected proposed arrangement with part-time marketing and per-click paymentspart-time marketing and per-click payments
OIG approved proposed arrangement with OIG approved proposed arrangement with full-time marketing and fixed, annual feesfull-time marketing and fixed, annual fees
Not all such arrangements are illegalNot all such arrangements are illegal High standard for favorable advisory High standard for favorable advisory
opinionopinion Helpful discussion of risks associated with Helpful discussion of risks associated with
“under arrangements” transactions“under arrangements” transactions

58
Advisory Opinion 11-06Advisory Opinion 11-06 OIG analyzed payments for electronically receiving OIG analyzed payments for electronically receiving
and responding to referral requests from hospitals and responding to referral requests from hospitals through online post-acute care referral service. through online post-acute care referral service.
OIG found that the payments did not meet referral OIG found that the payments did not meet referral services safe harbor because they were not services safe harbor because they were not assessed uniformly and were not based solely on assessed uniformly and were not based solely on cost of operating referral service.cost of operating referral service.
OIG issued unfavorable opinion out of concern that OIG issued unfavorable opinion out of concern that payments created an uneven playing field and that payments created an uneven playing field and that payments could be an unlawful pay-to-play fee. payments could be an unlawful pay-to-play fee.
Many hospitals participate in online post-acute care Many hospitals participate in online post-acute care referral services and need to re-assess those referral services and need to re-assess those relationships in light of this Opinion. relationships in light of this Opinion.

59
Advisory Opinion 11-08Advisory Opinion 11-08
OIG analyzed existing and proposed CPAP OIG analyzed existing and proposed CPAP set up arrangements between DME supplier set up arrangements between DME supplier and IDTF.and IDTF.
OIG issued unfavorable opinion.OIG issued unfavorable opinion. With regard to existing arrangement, the With regard to existing arrangement, the
OIG found that “carve out” of Federal OIG found that “carve out” of Federal business was not sufficient protection for business was not sufficient protection for favorable advisory opinion.favorable advisory opinion.
With regard to proposed arrangement, the With regard to proposed arrangement, the OIG reiterated longstanding concerns about OIG reiterated longstanding concerns about arrangements between DME suppliers and arrangements between DME suppliers and IDTFs as potential referral sources.IDTFs as potential referral sources.
60
Advisory Opinion 11-08Advisory Opinion 11-08
Opinion represents warning about Opinion represents warning about CPAP set-up services arrangementsCPAP set-up services arrangements
... but does not rule out possibility that ... but does not rule out possibility that such arrangements could be such arrangements could be appropriately structured.appropriately structured.
Keys will be existence of a legitimate Keys will be existence of a legitimate business purpose of arrangement and business purpose of arrangement and FMV of payments.FMV of payments.

61
Changing Compliance Changing Compliance EnvironmentEnvironment

62
60-Day Repayment 60-Day Repayment RequirementRequirement
§6402 of PPACA requires reporting and §6402 of PPACA requires reporting and repayment of overpayments within 60 repayment of overpayments within 60 days of identification (or due date of next days of identification (or due date of next cost report, if applicable)cost report, if applicable) What’s “identification”?What’s “identification”?
Violations actionable under FCAViolations actionable under FCA Regulatory guidance will be forthcoming... Regulatory guidance will be forthcoming...
(or so we’ve heard)(or so we’ve heard) Absent guidance, providers must struggle Absent guidance, providers must struggle
to come up with practical approaches to to come up with practical approaches to complying with the 60-day requirement.complying with the 60-day requirement.
63
Monthly Exclusion CheckingMonthly Exclusion Checking Seriously.... every monthSeriously.... every month
Growing number of State Medicaid Programs Growing number of State Medicaid Programs are requiring monthly screening of current are requiring monthly screening of current employees and contractors.employees and contractors. SeeSee TennCare Policy PI 11-002 (effective TennCare Policy PI 11-002 (effective
6/22/2011)6/22/2011) State Medicaid Director Letter instructed State Medicaid Director Letter instructed
states to “states to “require providers to search the require providers to search the HHS-OIG website monthly to capture HHS-OIG website monthly to capture exclusions and reinstatements that exclusions and reinstatements that have occurred since the last search.” have occurred since the last search.”
HHS-OIG CIAs still only require annual HHS-OIG CIAs still only require annual screening.screening.

64
Mandatory Compliance Mandatory Compliance ProgramsPrograms
It’s coming.... eventually.It’s coming.... eventually.
§§6401 of PPACA makes compliance 6401 of PPACA makes compliance programs mandatory.... programs mandatory....
....but only after implementing regulations ....but only after implementing regulations establish the core elements for mandatory establish the core elements for mandatory compliance programscompliance programs
Growing numbers of providers are Growing numbers of providers are establishing (or updating) compliance establishing (or updating) compliance programs in anticipation of them becoming programs in anticipation of them becoming mandatory.mandatory.
65
What’s Next?What’s Next?
OIG/DOJ increased emphasis on pursuing OIG/DOJ increased emphasis on pursuing individual liability for fraud and abuse individual liability for fraud and abuse perpetrated by health care entitiesperpetrated by health care entities Goal is “to alter the cost-benefit calculus of the Goal is “to alter the cost-benefit calculus of the
corporate executives who run these companies”corporate executives who run these companies” Increasingly aggressive federal/state Increasingly aggressive federal/state
enforcementenforcement Qui Tam Relators driving government Qui Tam Relators driving government
prioritiespriorities Increasing importance of comprehensive Increasing importance of comprehensive
and aggressive corporate compliance effortsand aggressive corporate compliance efforts
66
““Be careful out there”Be careful out there”
67
Carrie Bryant, Esq., CHCCarrie Bryant, Esq., CHCCompliance OfficerCompliance Officer
American HomePatientAmerican HomePatient
William T. Mathias, Esq.William T. Mathias, Esq.PrincipalPrincipal
Ober|KalerOber|Kaler
Questions?Questions?






















![PRECEDENTIALSimran Dhillon, Esq. Max C. Kaufman, Esq. [ARGUED] Nancy Winkelman, Esq. Lawrence S. Krasner. Esq. Carolyn Engel Temin, Esq. Philadelphia County Office of District Attorney](https://static.cupdf.com/doc/110x72/5f591458cf1cd86f902d709f/simran-dhillon-esq-max-c-kaufman-esq-argued-nancy-winkelman-esq-lawrence.jpg)

![Electronic Discovery Preparedness Checklist [Ober|Kaler]](https://static.cupdf.com/doc/110x72/61f4b9049fb7614dc939e2b9/electronic-discovery-preparedness-checklist-oberkaler.jpg)


