www.metcardio.org STRESS ECG AND STRESS ECHOCARDIOGRAPHY Giuseppe Biondi Zoccai Giuseppe Biondi Zoccai Division of Cardiology, University of Turin, Turin, Italy Division of Cardiology, University of Turin, Turin, Italy Meta-analysis and Evidence-based medicine Training in Meta-analysis and Evidence-based medicine Training in Cardiology (METCARDIO), Ospedaletti, Italy Cardiology (METCARDIO), Ospedaletti, Italy

Www.metcardio.org STRESS ECG AND STRESS ECHOCARDIOGRAPHY Giuseppe Biondi Zoccai Division of Cardiology, University of Turin, Turin, Italy Meta-analysis.
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

www.metcardio.org
STRESS ECG AND STRESS ECHOCARDIOGRAPHY
Giuseppe Biondi ZoccaiGiuseppe Biondi Zoccai
Division of Cardiology, University of Turin, Turin, ItalyDivision of Cardiology, University of Turin, Turin, Italy
Meta-analysis and Evidence-based medicine Training in Meta-analysis and Evidence-based medicine Training in Cardiology (METCARDIO), Ospedaletti, ItalyCardiology (METCARDIO), Ospedaletti, Italy

www.metcardio.org
LEARNING GOALS
• Scope of the problem• Stress ECG• Stress echocardiography• Reconciling the evidence

www.metcardio.org
LEARNING GOALS
• Scope of the problem• Stress ECG• Stress echocardiography• Reconciling the evidence

www.metcardio.org
FINDING AN APPROPRIATE DIAGNOSTIC LEVEL
www.metcardio.org
FINDING AN APPROPRIATE PROGNOSTIC LEVEL

www.metcardio.org
DIAGNOSTIC AND PROGNOSTIC WORK-UP OF SUSPECTED
CORONARY HEART DISEASE• Clinical history• Physical examination• Resting ECG• Resting echocardiography• Stress ECG• Stress echocardiography• Stress nuclear scan• Coronary CT• Coronary angiography• ….

www.metcardio.org
EFFECTIVE RADIATION DOSES
Picano, Am J Med 2003

www.metcardio.org
CORONARY STEAL PHENOMENON
Picano, Circ 1998

www.metcardio.org
CORONARY STEAL PHENOMENON
Picano, Circ 1998

www.metcardio.org
THREE STATES OF THE SODIUM CHANNEL AND THE NORMAL SODIUM CURRENT (INa)
Ca++
out
in
out
in
Na+/Ca++
Exchanger
Ca++
Ca++
Ca++
Ca++
Na+
Na+
Na+
Na+Na+
Na+
Na+
RestingClosedRestingClosed
Na+
ActivatedActivated InactivatedInactivated
Na+
Na+
Na+ Ca++
Ca++
0
Late
Peak
SodiumCurrent
[Na]140 mM ~ 10mM
www.metcardio.org
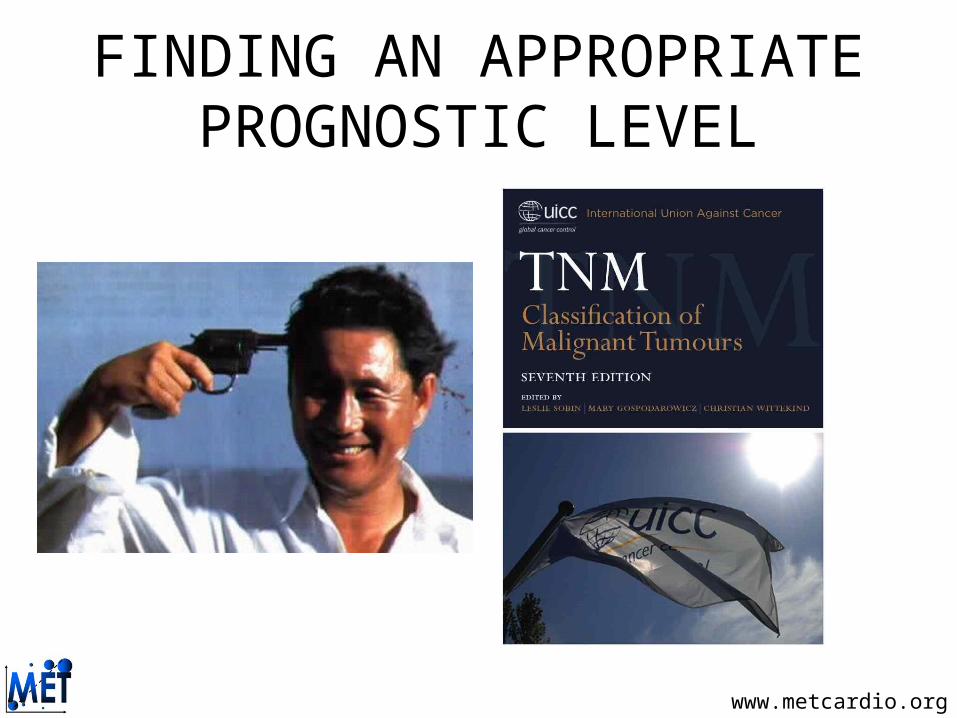
ISCHEMIA INDUCED EFFECTS ON LATE INa AND INTRACELLULAR CALCIUM
Ca++
Na+/Ca++
Exchanger
Ca++Ca++
Na+
Na+Na+
Na+
Na+Na+
Na+Na+Na+
Na+
Na+
Ca++Ca++Ca++
Ca++
Ca++Ca++ Ca++
Ca++
Ca++
Ca++ Ca++
Excess Calcium:• Electrical instabilityElectrical instability• Contractile Contractile
dysfunctiondysfunction• ECG changesECG changes
Excess Calcium:• Electrical instabilityElectrical instability• Contractile Contractile
dysfunctiondysfunction• ECG changesECG changes
0
Late
Peak
out
in
out
in
Na+
Na+
Na+
Na+ Ca++
Ca++
ImpairedInactivation
ImpairedInactivation
Ca++Ca++
SodiumCurrent

www.metcardio.org
THE ISCHEMIC CASCADE

www.metcardio.org
LEARNING GOALS
• Scope of the problem• Stress ECG• Stress echocardiography• Reconciling the evidence

www.metcardio.org
TREADMILL STRESS TEST

www.metcardio.org
KEY ACCESSORY

www.metcardio.org
EQUIPMENT FOR STRESS TESTING• Treadmill or bicycle or steps• ECG machine• Blood pressure cuff• Computer is a ‘nice to have’• ACLS certification• Defibrillation/intubation cart• Exit strategy• Good help* (it takes two to
test)

www.metcardio.org
PROTOCOLS

www.metcardio.org
TYPICAL BRUCE OR RAMP STRESS
WORK WORK
TIME TIME TIME TIME
WORK WORK
www.metcardio.org
WHY USE A BIKE ERGOMETER?
1. Accurate measurement of POWER. 2. Ramping protocols allow for assessment of physiologic function across all
work levels. 3. Independent of patient’s weight. 4. Less danger of fall and injury to patient. 5. Easier to take accurate B/P at high work rates. 6. Patient can stop at anytime. 7. Holding handle bars does not effect test (Holding treadmill handrails can
significantly effect results). 8. Fits into smaller space and is portable.9. Patients with knee or hip problems tend to perform better and report being
more comfortable on the bike.
www.metcardio.org
WHY USE A BIKE ERGOMETER?
10. Bike ramp protocols are designed to last 6-10 minutes, resulting in less fatigue (yet peak work is maximized).
11. HR, Work, and VO2 (Cardiac Output) are linearly related. Bike ramp protocols produce linear increases in Work, thereby mimicking the expected physiologic response in health and disease.
12. Determination of the Anaerobic Threshold (AT) by the most popular methods (V-slope and VE/VO2 nadir) were developed and proven through the use of bike ramp protocols. To use another method means to lose AT detection accuracy.
13. Bike ramp protocols are used by many of the leading clinical and research cardiopulmonary exercise testing labs (UCLA, Duke, Mayo, Stanford, Bowman-Gray, Johns Hopkins, UAB, Temple to name a few). Recently, treadmills capable of performing ramp protocols have been developed.

www.metcardio.org
MY VIEW: TREADMILL IS BEST
www.metcardio.org
INDICATIONS TO STRESS TEST
• Diagnosis of coronary artery disease• Risk-stratification of coronary artery disease• Risk-stratification in cardiac valve disease• Appraisal of rate response• Appraisal of pressure response to stress• Appraisal of functional capacity

www.metcardio.org
INFORMATION OBTAINED FROM EXERCISE STRESS BUT NOT AVAILABLE WITH PHARMACOLOGICAL TEST
• Exercise duration/tolerance• Reproducibility of symptoms with activity• Heart rate response to exercise• Blood Pressure response • Detection of stress induced arrhythmias• Assess control of angina with medical therapy• Prognosis

www.metcardio.org
KEY ASPECTS• Exercise duration and work-load (minutes, METs, Watts)• Maximum blood pressure• Maximum heart rate (given that predicted for age)
• Rate-pressure product• Baseline ECG
• ST-segment changes• T-wave changes• Q waves• Duke treadmill score• Heart rate recovery

www.metcardio.org
ABNORMAL RESPONSE TO STRESS TESTING
1) Heart rate fails to rise above 120 or unable to attain target heart rate of 85% of max
2) Blood pressure shows a drop in systolic3) Patient physically unable to complete test4) Marked hypertension, >260/1155) Chest Pain and/or unusual shortness of
breath

www.metcardio.org
NORMAL RESPONSE OF ECG TO STRESS TESTING
ECG Changes1) QRS complex decreases in size2) J point depresses, resulting in up sloping of ST
segment3) ST segment returns to baseline by 80
milliseconds4) PR segment may down slope – thus baseline is
defined as PQ junction5) R amplitude may decrease at rates that go
above 1306) T wave decreases
www.metcardio.org
ABNORMAL RESPONSE OF ECG TO STRESS TESTING
ECG Changes– Horizontal or down sloping ST segments – ST segment depressed or elevated – ST segment does not return to baseline by 80
milliseconds– U or T wave inversion – Dysrhythmias – rate dependent blocks above
first degree, WPW appears, Atrial fib/flutter, multiform and/or increasing PVC’s, V-tach occurs

www.metcardio.org
ECG CHANGES

www.metcardio.org
ECG CHANGES
www.metcardio.org
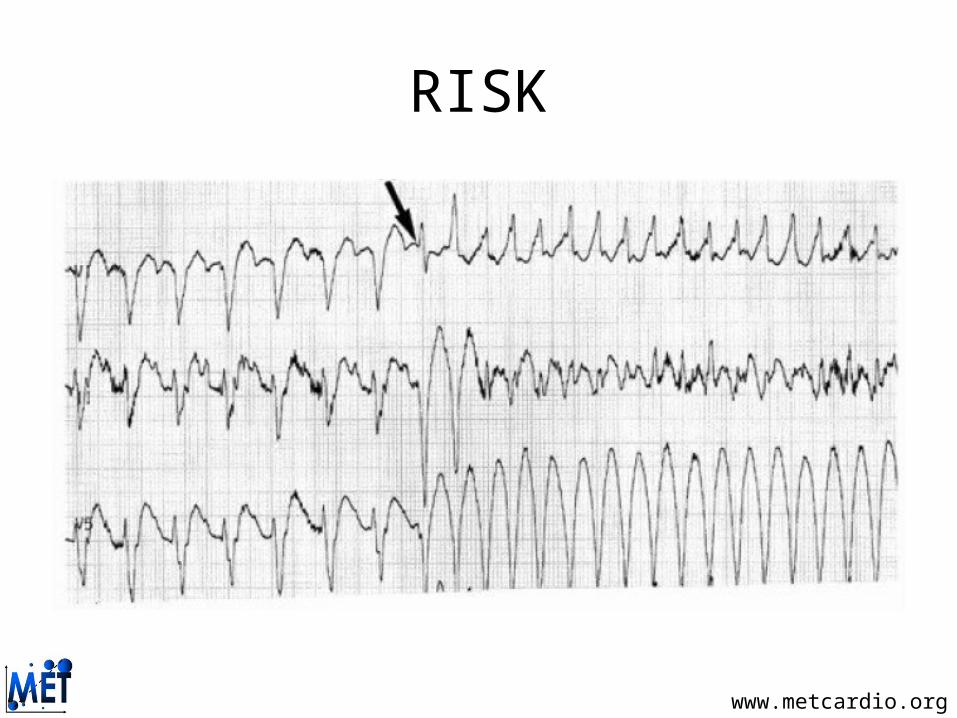
RISK

www.metcardio.org
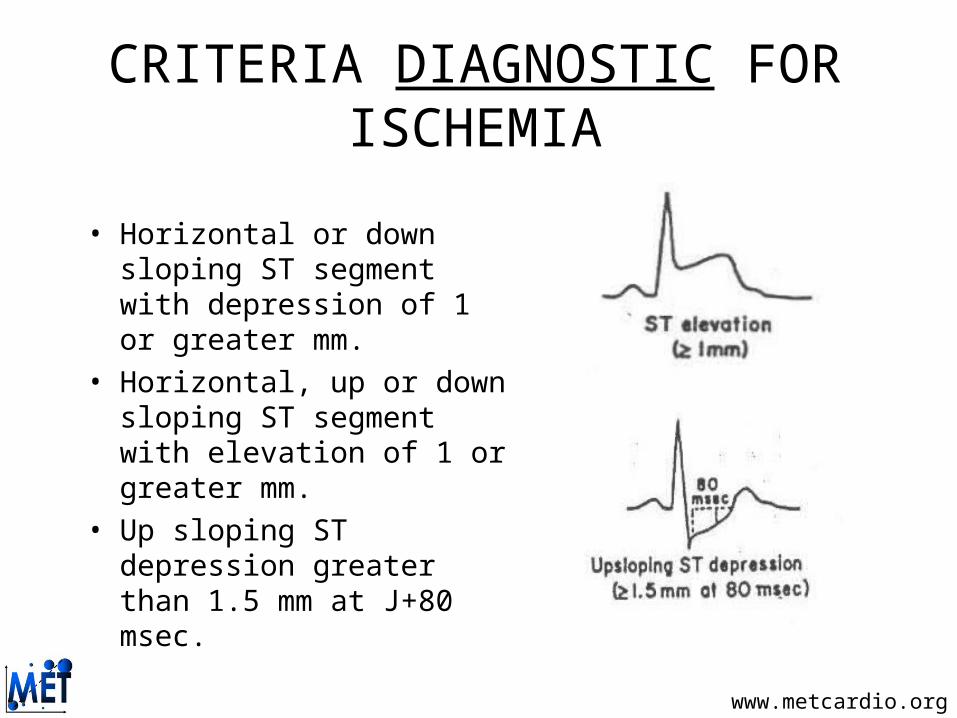
CRITERIA DIAGNOSTIC FOR ISCHEMIA
• Horizontal or down sloping ST segment with depression of 1 or greater mm.
• Horizontal, up or down sloping ST segment with elevation of 1 or greater mm.
• Up sloping ST depression greater than 1.5 mm at J+80 msec.
www.metcardio.org
CRITERIA DIAGNOSTIC FOR ISCHEMIA
• Horizontal or down sloping ST segment with depression of 1 or greater mm.
• Horizontal, up or down sloping ST segment with elevation of 1 or greater mm.
• Up sloping ST depression greater than 1.5 mm at J+80 msec.
www.metcardio.org
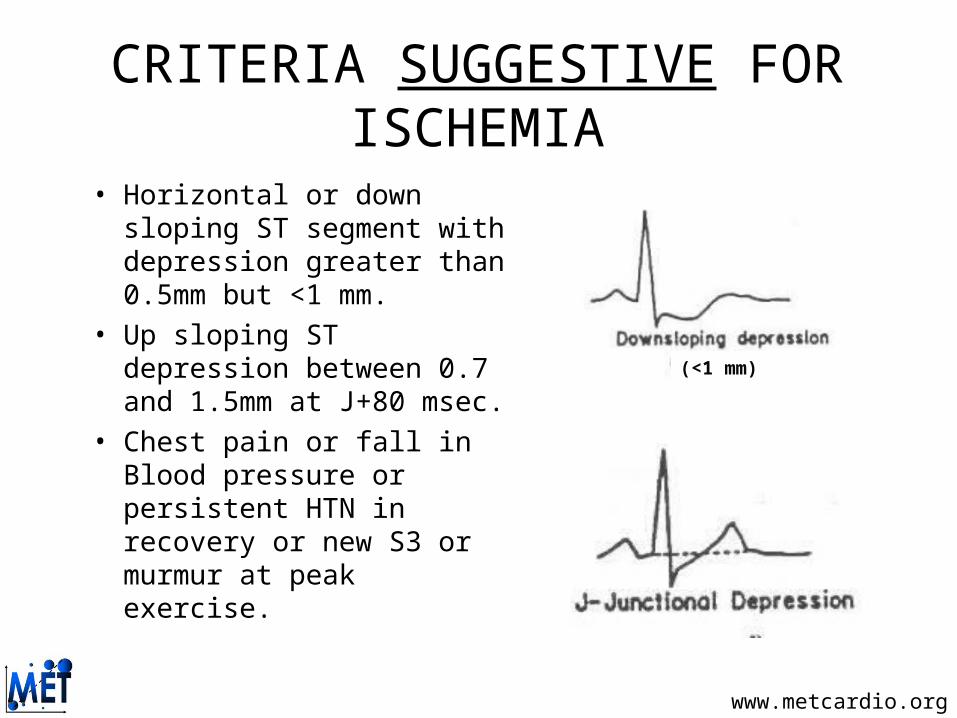
CRITERIA SUGGESTIVE FOR ISCHEMIA
• Horizontal or down sloping ST segment with depression greater than 0.5mm but <1 mm.
• Up sloping ST depression between 0.7 and 1.5mm at J+80 msec.
• Chest pain or fall in Blood pressure or persistent HTN in recovery or new S3 or murmur at peak exercise.
(<1 mm)

www.metcardio.org
SYMPTOM-SIGN LIMITED TESTING ENDPOINTS – WHEN TO STOP!
Dyspnea, fatigue, chest pain
Systolic blood pressure drop
ECG--ST changes, arrhythmias
Physician Assessment
Borg Scale (17 or greater)
www.metcardio.org
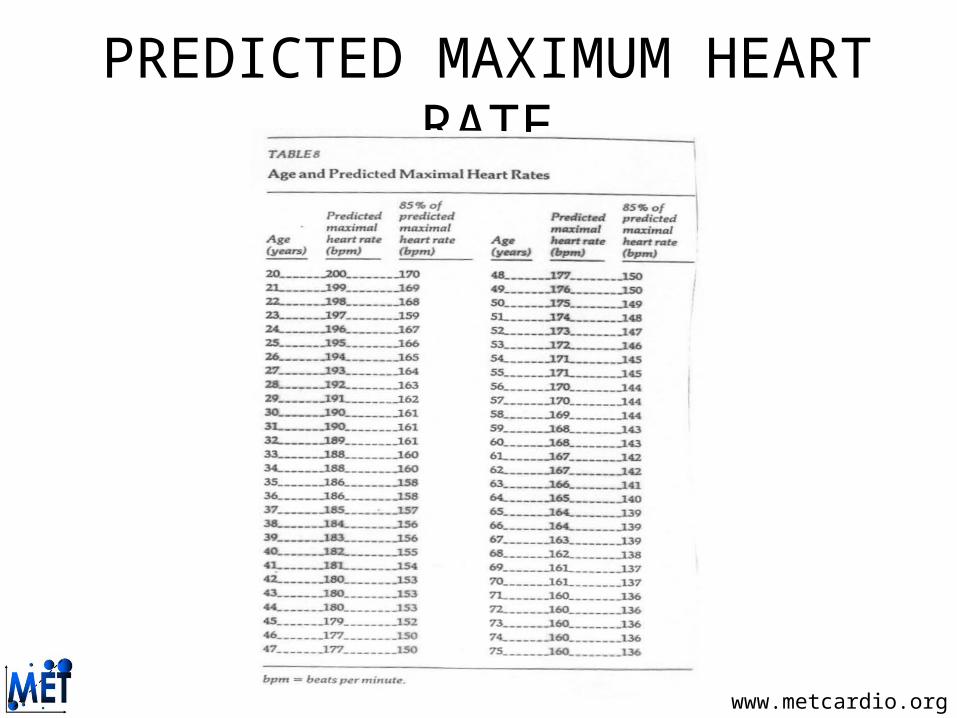
PREDICTED MAXIMUM HEART RATE

www.metcardio.org
WHAT IS A MET?
Metabolic Equivalent Term
1 MET = "Basal" aerobic oxygen consumption to stay alive = 3.5 ml O2 /Kg/min
Actually differs with thyroid status, post exercise, obesity, disease states
But by convention just divide ml O2/Kg/min by 3.5
www.metcardio.org
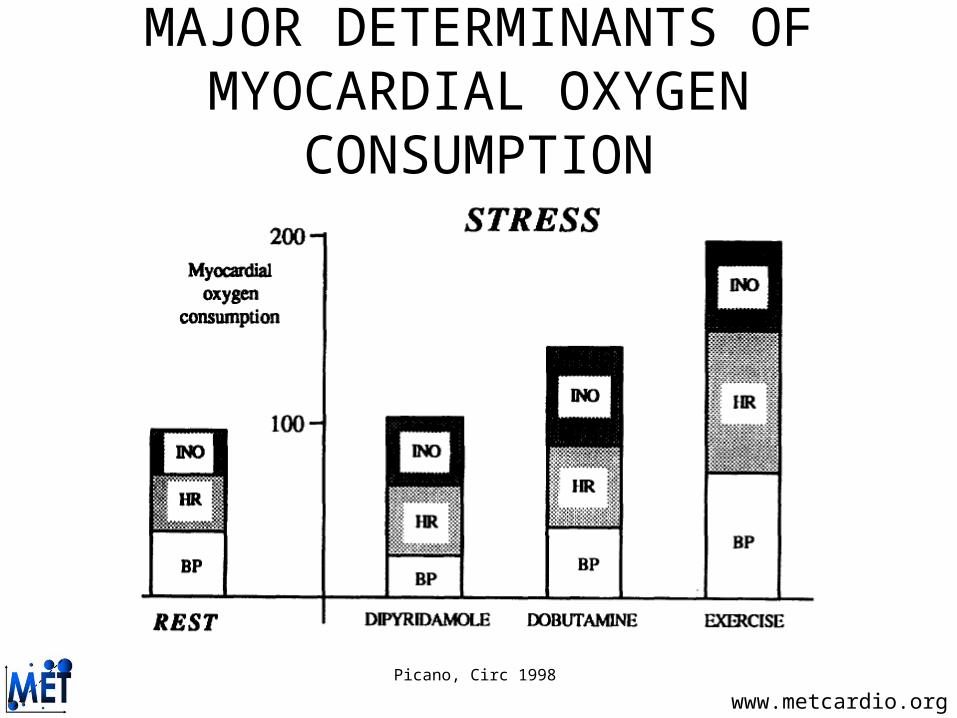
MAJOR DETERMINANTS OF MYOCARDIAL OXYGEN CONSUMPTION
Picano, Circ 1998

www.metcardio.org
PROGNOSTIC ROLE OF METs
Myers et al, New Engl J Med 2002

www.metcardio.org
PREDICTING CARDIAC DEATH
Marcus et al, Chest 1995

www.metcardio.org
DUKE TREADMILL SCORE
www.metcardio.org
BAYES THEOREM
If P(B) ≠ ), then
P(A/B) = “ P(B/A)P(A) “P(B/A)P(A) + P(B/not A)P (not A)

www.metcardio.org
CONTINUOUS OF RISK

www.metcardio.org
TYPICAL REPORTTreadmill stress test stopped at the end of the 3rd standard Bruce stage for fatigue (max BP 200/100 mm Hg, max HR 140 bpm, RPP 28,000).No symptoms. No arrhythmias. No abnormalities in the baseline ECG. In the 2nd stage development of ST depression, which becomes diagnostic in the 3rd stage (max 1.5 mm in V5 at the peak), with quick recovery after the stress.Duke treadmill score: 1 (<-11 high risk; >4 low risk).Heart rate recovery: 10 (valore di riferimento >12).Positive stress test for myocardial ischemia at mid-to-high work-load.

www.metcardio.org
GUIDELINES
Gibbons et al, Circ 2002

www.metcardio.org
GUIDELINES: RECOMMENDATIONS
Gibbons et al, Circ 2002

www.metcardio.org
GUIDELINES: RECOMMENDATIONS
Gibbons et al, Circ 2002

www.metcardio.org
STRESS EKG IS NOT A SLAM DUNK
• 5/10,000 result in serious cardiovascular event
• 1/10,000 result in death• Results are based on Bayes Theorem• Requires proper selection, preparation, and
execution• Not the GOLD standard

www.metcardio.org
LEARNING GOALS
• Scope of the problem• Stress ECG• Stress echocardiography• Reconciling the evidence
www.metcardio.org
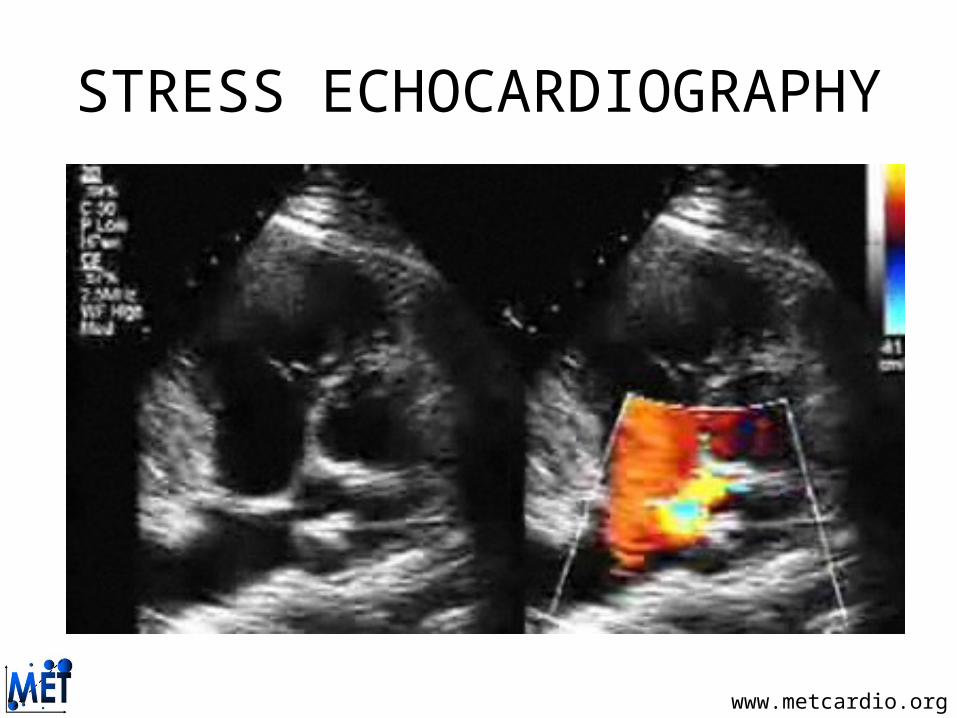
STRESS ECHOCARDIOGRAPHY
www.metcardio.org
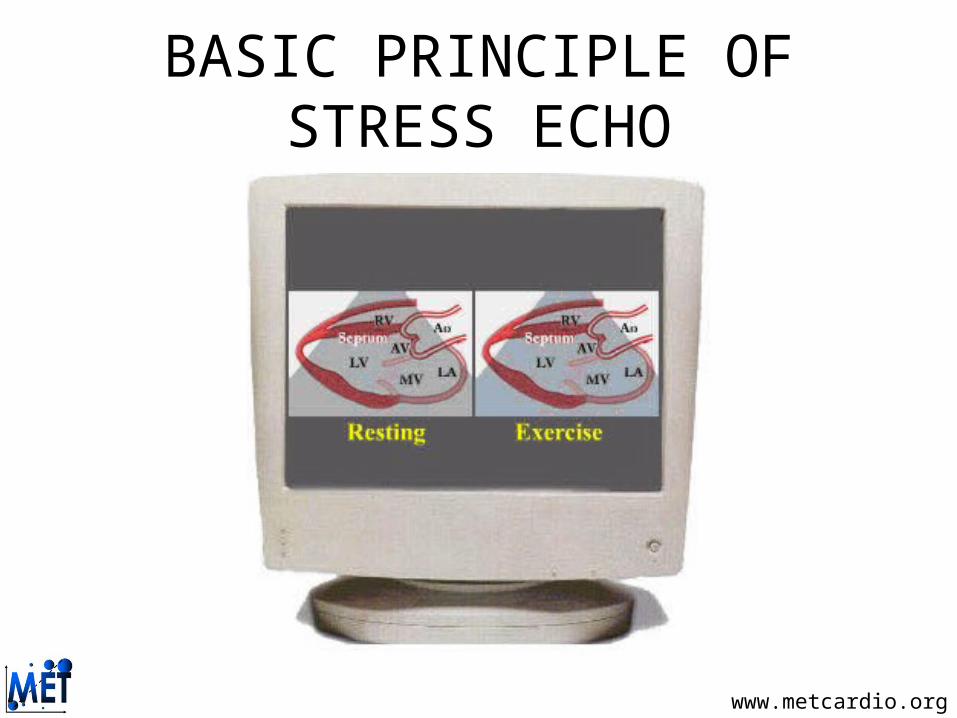
BASIC PRINCIPLE OF STRESS ECHO
www.metcardio.org
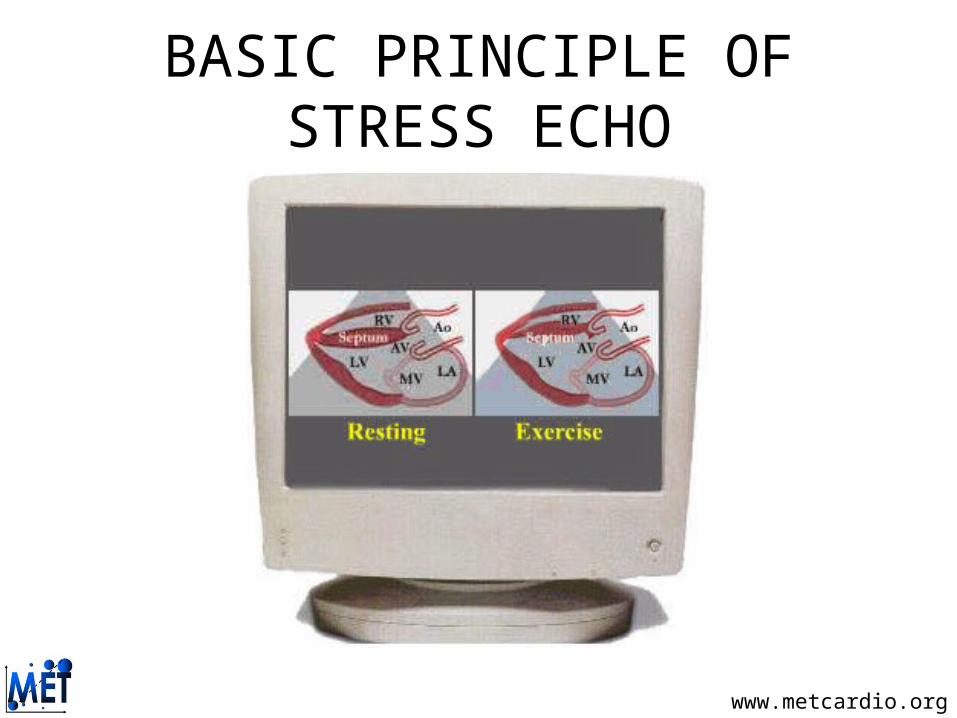
BASIC PRINCIPLE OF STRESS ECHO

www.metcardio.org
WALL MOTION RESPONSES
Sicari et al, Eur Heart J 2009

www.metcardio.org
CARDIAC SEGMENTS

www.metcardio.org
WALL SEGMENTS AND CORONARY DISTRIBUTION

www.metcardio.org
CURRENT STRESS PROTOCOLS
ECG ECHONUCLEAR
Exercise: Tread Post-Tread TreadBicycle Bicycle
Pharmacologic: Catecholamines: Dobutamine Dobutamine Vasodilators: Dipyridamole Dipyridamole
DipyridamoleAdenosine Adenosine
Vasospastic: Ergonovine Ergonovine Adjuncts: Atropine
Handgrip

www.metcardio.org
INDICATIONS TO STRESS ECHOCARDIOGRAPHY
• Diagnosis of coronary artery disease• Risk-stratification of coronary artery disease• Risk-stratification in cardiac valve disease• Appraisal of myocardial viability• Patients unable to ambulate
www.metcardio.org
PREPARATION
• Avoid smoking• Avoid food/beverages• Take all medications unless
instructed otherwise• Wear comfortable clothes and shoes

www.metcardio.org
KEY PHARMACOLOGICAL TESTS
Picano, Circ 1998

www.metcardio.org
DOBUTAMINE PROTOCOL
Sicari et al, Eur Heart J 2009

www.metcardio.org
DIPYRIDAMOLE PROTOCOL
Sicari et al, Eur Heart J 2009

www.metcardio.org
FURTHER APPLICATIONS
Sicari et al, Eur Heart J 2009
www.metcardio.org
LEARNING GOALS
• Scope of the problem• Stress ECG• Stress echocardiography• Reconciling the evidence

www.metcardio.org
PATIENTS APPROPRIATE FOR ROUTINE ECG STRESS TEST WITHOUT IMAGING
• Patient can exercise for 6 or more minutes• Normal baseline ECG• No history of diabetes• No history of coronary revascularization• No history of myocardial infarction

www.metcardio.org
ABSOLUTE CONTRAINDICATIONS• Within 24 hours of troponin positive ACS• Within 7 days for high dose DSE after STEMI• Left ventricular failure with symptoms at rest (in tertiary centres
viability may be assessed using low dose dobutamine stress).• Recent history (within the last week) of life threatening arrhythmias.• Severe dynamic or fixed left ventricular outflow tract obstruction
although low dose DSE may be useful.• BP >220/120• Recent pulmonary embolism or infarction.• Thrombophlebitis or active deep vein thrombosis.• Known hypokalaemia (particularly for Dobutamine stress)• Active endocarditis, myocarditis, or pericarditis.

www.metcardio.org
POSSIBLE CONTRAINDICATIONS TO STRESS TESTING BASED ON RESTING ECG
• ST-segment changes 1 mm or greater, either depression or elevation
• Ventricular strain patterns or hypertrophy• T-wave inversions• Left bundle branch block• Right bundle branch block, if significant• Prolonged QT interval
www.metcardio.org
ABSOLUTE CONTRAINDICATIONS TO DOBUTAMINE STRESS ECHO
• Suspected or known severe bronchospasm• 2nd or 3rd degree AV block without pacemaker• Sick sinus syndrome without pacemaker• BP <90mmHg systolic• Xanthines taken in the last 12 hours, or dipyridamole use in
the last 24 hours

www.metcardio.org
FIRST THINGS FIRST: DIAGNOSTIC PERFORMACE OF DIFFERENT TESTS
Grouping # of Studies
Total # Patients
Sens Spec Predictive Accuracy
Standard ET 147 24,047 68% 77% 73% ET Scores 24 11,788 80% Score Strategy 2 >1000 85% 92% 88%
Thallium Scint 59 6,038 85% 85% 85% SPECT 16+14 5,272 88% 72% 80% Adenosine SPECT 10+4 2,137 89% 80% 85% Exercise ECHO 58 5,000 84% 75% 80% Dobutamine ECHO 5 <1000 88% 84% 86% Dobutamine Scint 20 1014 88% 74% 81% Electron Beam Tomography (EBCT)
16 3,683 60% 70% 65%

www.metcardio.org
CHOOSING YOUR TEST
Heijenbrok-Kal et al, Am Heart J 2007

www.metcardio.org
CHOOSING YOUR TEST
Froelicher et al, Chest 1999

www.metcardio.org
CARDIAC STRESS IMAGING
Picano, Am J Med 2003

www.metcardio.org
ADVANTAGES OF STRESS ECHOCARDIOGRAPHY COMPARED TO NUCLEAR STRESS TESTING
• Higher Specificity• Visualization of cardiac valves• Evaluate for presence of pericardial effusion• Ability to measure RV Systolic Pressure• More accurate assessment of LV ejection fraction• Doppler interrogation to determine Diastolic Function • Lower Cost• Lack of Radiation Exposure

www.metcardio.org
TAKE HOME MESSAGES• Stress testing, by either stress ECG, stress nuclear scan,
dipyrididamol/dobutamine nuclear scan, stress echocardiography, dipyrididamol/dobutamine echocardiography, is crucial in the diagnostic work-up of patients with suspected coronary heart disease
• These tests are also useful in the prognostic work-up of patients with established coronary heart disease
• Given financial and logistic constraints, stress ECG should be performed in most suitable subjects as 1st line test, followed/substituted by imaging tests in all the other cases

www.metcardio.org
Thank you for your attention
For any correspondence: [email protected]
For these and further slides on these topics feel free to visit the metcardio.org website:
http://www.metcardio.org/slides.html
Related Documents