UPPER RESPIRATORY TRACT INFECTION

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

UPPERRESPIRATORYTRACTINFECTION

OVERVIEW
• TolearntheepidemiologyandvariousclinicalpresentationofURT
• Toidentifythecommonetiologicalagentscausingthesesyndromes
• Tostudythelaboratorydiagnosisofthesesyndromes
• Todeterminetheantibioticofchoicefortreatment

WHYISTHISIMPORTANT?
• Therespiratorysystemisthemostcommonlyinfectedsystem.
• Healthcareproviderswillseemorerespiratoryinfectionsthananyothertype.
• Doctorswillprescribemoreantibioticsfortheseinfectionsthanforanyothertype.


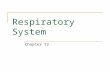
THERESPIRATORYSYSTEM
• Amajorportalofentryforinfectiousorganisms
• Itisdividedintotwotracts– upperandlower.– Thedivisionisbasedonstructuresandfunctionsineachpart.
• Thetwopartshavedifferenttypesofinfection.

THERESPIRATORYSYSTEM
• Theupperrespiratorytract:– Nasalcavity,sinuses,pharynx,andlarynx– Infectionsarefairlycommon.– Usuallynothingmorethananirritation
• Thelowerrespiratorytract:– Lungsandbronchi– Infectionsaremoredangerous.– Canbeverydifficulttotreat

DEFENSESOFTHERESPIRATORYSYSTEM
• Thebodyhasavarietyofhostdefensemechanisms.– Innateimmuneresponse- thecellsandmechanismsthatdefendthehostfrominfectionbyotherorganisms,inanon-specificmanner
– Adaptiveimmunity- thebody'simmunesystempreparesitselfforfuturechallenges
• Therespiratorysystemhassignificantdefenses.– Theupperrespiratorytracthas:
• Mucociliaryescalator.• Coughing.
– Thelowerrespiratorytracthas:• Alveolarmacrophages.

PATHOGENSOFTHERESPIRATORYSYSTEM
§ Respiratorypathogensareeasilytransmittedfromhumantohuman.ú Theycirculatewithinacommunity.ú Infectionsspreadeasily.
§ Somerespiratorypathogensexistaspartofthenormalflora.
§ Othersareacquiredfromanimalsource,water,air,etc.§ Fungiarealsoasourceofrespiratoryinfection.
ú Usuallyinimmunocompromisedpatientsú MostdangerousareAspergillusand Pneumocystis.
PATHOGENSOFTHERESPIRATORYSYSTEM
• Somepathogensarerestrictedtocertainsites.
– Legionellaonlyinfectsthelung.
• Otherpathogenscauseinfectioninmultiplesites.
– Streptococcuscancause:
• Middleearinfections.
• Sinusitis.
• Pneumonia.

INFECTIONSOFTHEUPPERRESPIRATORYTRACT
• Laryngitis&Epiglottitis
• Otitismedia,mastoiditis,andsinusitis
• Pharyngitis
• Scarletfever
• Diphtheria
• Pertussis

LARYNGITIS• Laryngitis isswellingandirritation(inflammation)ofthevoicebox(larynx)thatisusuallyassociatedwithhoarsenessorlossofvoice– Rhinoviruses– Parainfluenzaviruses– Respiratorysyncytialvirus– Adenoviruses– Influenzaviruses– Measlesvirus– Mumpsvirus– Bordetellapertussis– Varicella-zostervirus.
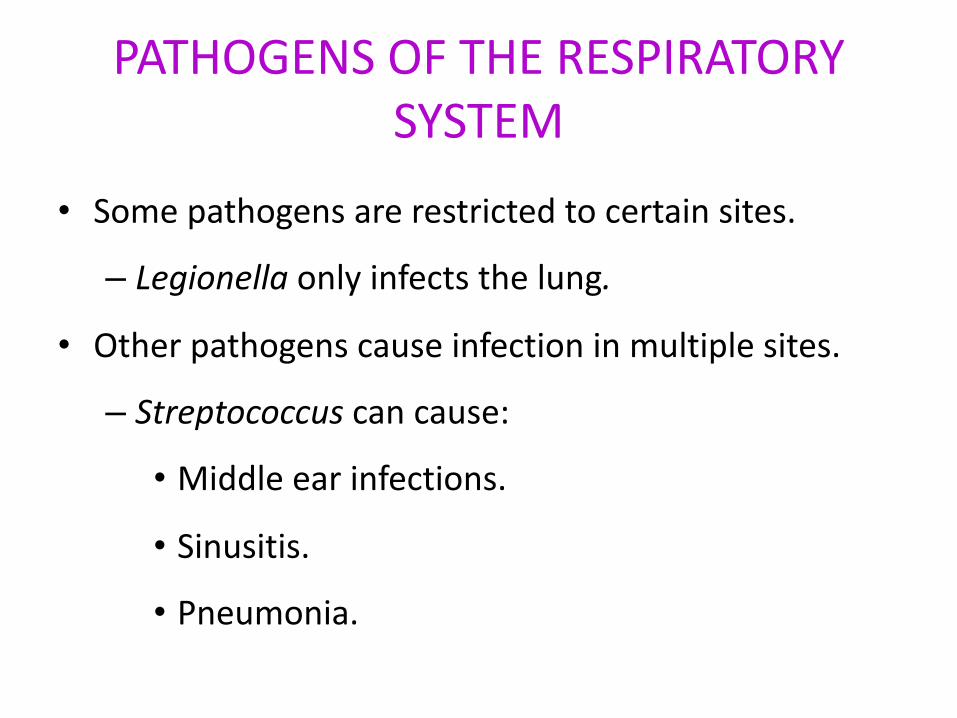
EPIGLOTTITIS• Usuallyyoungunimmunizedchildrenpresentedwithdysphagia,andrespiratorydistress
• H.influenzae (++)• H.parainfluenzae• S.pneumoniae• StreptococcusgroupA• Viral
AntibioticTreatment:-Ceftriaxone/Cefotaxime- Amoxi/clav
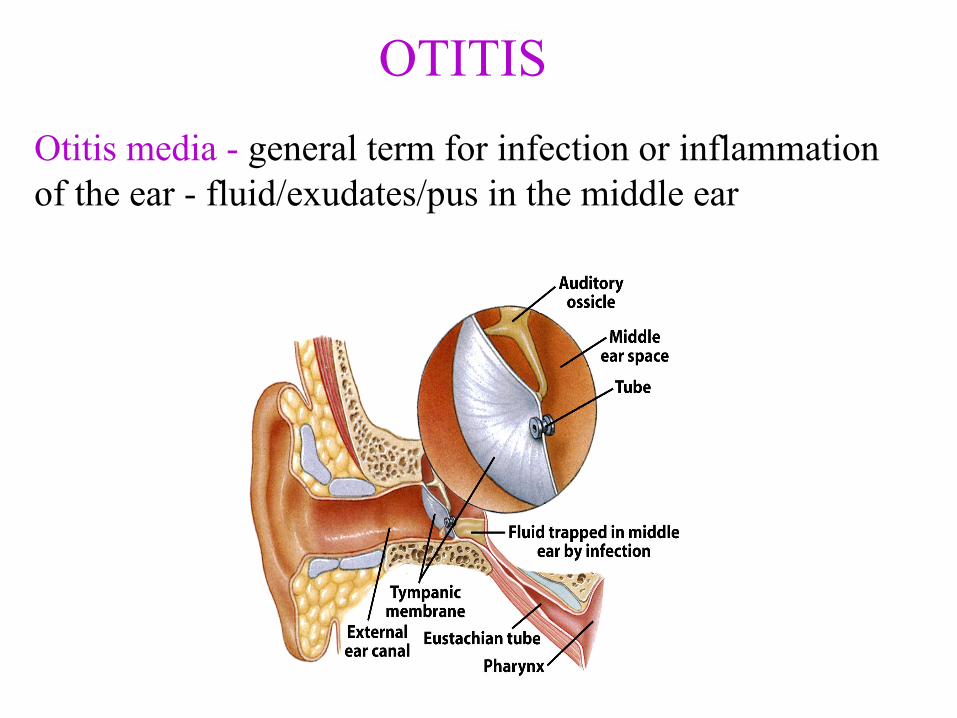
OTITISOtitis media - general term for infection or inflammation of the ear - fluid/exudates/pus in the middle ear
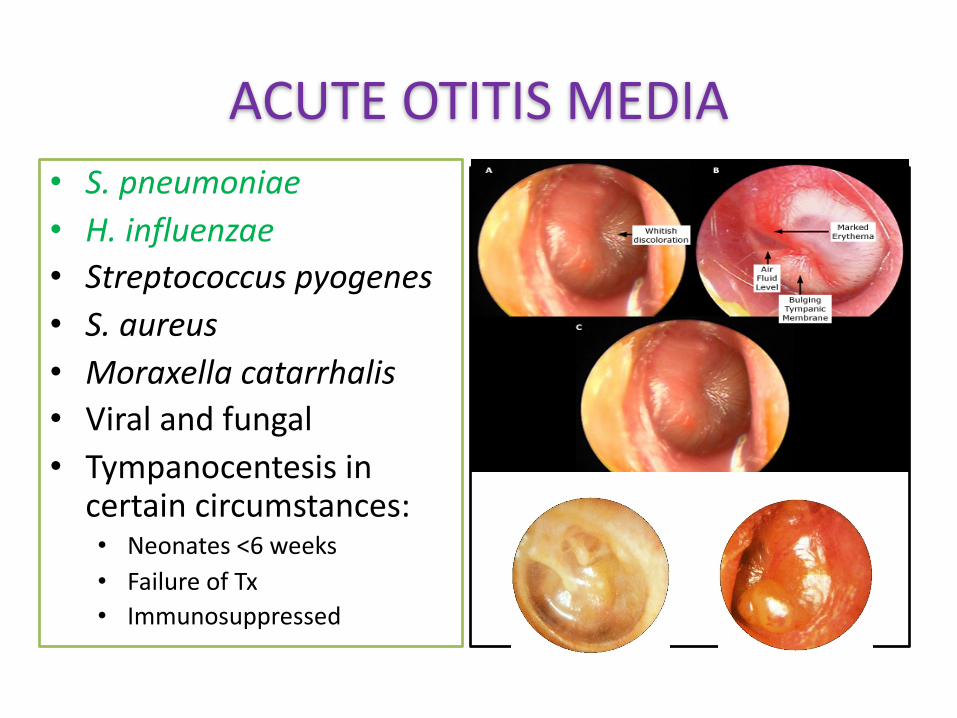
ACUTEOTITISMEDIA• S.pneumoniae• H.influenzae• Streptococcuspyogenes• S.aureus• Moraxellacatarrhalis• Viralandfungal• Tympanocentesis incertaincircumstances:• Neonates<6weeks• FailureofTx• Immunosuppressed
ACUTEOTITISMEDIAAntibiotictreatment
• Antibioticisnotalwaysnecessary(symptomatictreatment).
• Amoxicillin isthefirstchoiceofantibiotictherapy;ifamoxicilliniscontraindicated,azithromycin istheappropriatefirst-linetherapy.
• ForAOMthatisunresponsivetoamoxicillinafter72hoursoftherapy,administeramoxicillin-clavulanateorazithromycin.
• Patientswithsignificant,persistentsymptomsonhigh-doseamoxicillin-clavulanateorazithromycinmayrespondtointramuscularceftriaxone.

SINUSITIS

SINUSITIS• Acutesinusitis
– Viral(+++)– S.pneumoniae– H.influenzae– M.catarrhalis– S.aureus(sphenoid)
• Chronicsinusitis– S.pneumoniae– H.influenzae– M.catarrhalis– Oralanaerobes– Fungus

Acutebacterialsinusitis.AxialCTscan(A)showsanair-fluidlevelintherightantrum.Theattenuationofthisfluidislessthanthatofmuscleandtypicallyiswaterysinussecretions.Thiscouldrepresentanacutelyobstructedsinus,asinuswithpoordrainageinachronicallysupine(unconscious)patient,orapatientwhohadarecentantralwashingforsinusitis.CoronalCTscan(B)showsatypicalair-fluidlevelintheleftantrumwithminimalmucosalthickeningandobstructionoftheostiomeatal unit.Somemucosaldiseaseisalsopresentintheleftethmoidandrightmaxillarysinuses.Clinically,thispatienthadacutesinusitis.(FromSomPM,CurtinHD:Headandneckimaging,ed5,Philadelphia,2011,Elsevier,2011,p174,Fig.3-10.)
Non-NeoplasticLesionsoftheSinonasalTractWenig,BruceM.,MD,AtlasofHeadandNeckPathology,Chapter2,9-80.e9Copyright©2016Copyright©2016byElsevier,Inc.Allrightsreserved.

Acutebacterialsinusitis.Axialcontrast-enhancedCTscansofthreedifferentpatients.A,Enhancementoftheinflamedmucosawithintheleftmaxillarysinus.Thereisazoneofwaterattenuationseparatingthismucosafromthebonywallofthesinus.Thiszoneissubmucosaledema.Therearealsowaterattenuationsecretionswithinthesinuscavitythatrepresentincreasedsurfacesecretionsfromtheinflamedmucosa.Thisisthetypicalpictureofsinusinflammation.(FromSomPM,CurtinHD:Headandneckimaging,ed5,Philadelphia,2011,Elsevier,2011,p168,Fig.3-2.)
Non-NeoplasticLesionsoftheSinonasalTractWenig,BruceM.,MD,AtlasofHeadandNeckPathology,Chapter2,9-80.e9Copyright©2016Copyright©2016byElsevier,Inc.Allrightsreserved.

SINUSITIS
• Acutesinusitis(durationrange,1–33days)usuallyiscausedbyaviralinfectionassociatedwiththecommoncold;symptomsincludenasalcongestion,purulentnasaldischarge,maxillarytoothpain,facialpain,fever,andearpain.
• Acutebacterialsinusitiscandevelopsecondarytoaviralupperrespiratoryinfection(URI);however,fewerthan2%ofviralURIsarecomplicatedbybacterialrhinosinusitis.

SINUSITIS
• Giventhesimilarradiographicappearanceofviralsinusitisandbacterialsinusitis,imagingisnothelpful.
• Antibioticsshouldbereservedforpatientswhosesymptomspersistfor>10days,aresevere(i.e.,fever>39°C,purulentnasaldischarge,facialpainfor>3consecutivedays),ordeteriorateafterinitialimprovement.
• Amoxicillin-clavulanateisthepreferredagentifantibioticsarenecessary
PHARYNGITIS
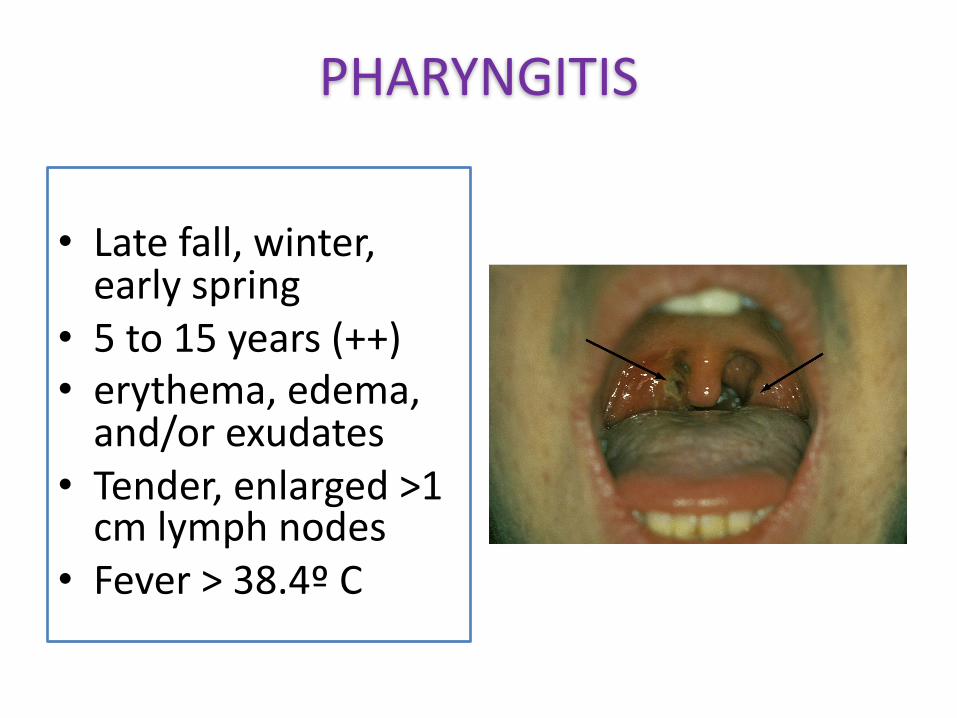
• Latefall,winter,earlyspring
• 5to15years(++)• erythema,edema,and/orexudates
• Tender,enlarged>1cmlymphnodes
• Fever>38.4ºC

PHARYNGITIS• Etiology• Viral isthemostcommon
• Enterovirus,HSV,EBV,HIV,Respiratoryviruses
• Bacterial• GroupAStreptococcus• Neisseriagonorrhoeae• Anaerobicbacteria(e.g.
Lemierre's syndrome)• Corynebacterium
diphtheriae

PHARYNGITIS• Pharyngitismostoftenisviral;aviraletiologyismorelikelyin
patientswithassociatedcough,nasalcongestion,conjunctivitis,ororalulcersorvesicles.
• PatientswithfewerthanthreeCentorcriteria(i.e.,feverbyhistory,tonsillarexudates,tenderanteriorcervicaladenopathy,absenceofcough)havealowprobabilityofgroupAstreptococcalinfectionanddonotrequirefurthertesting.
• Antibiotics(e.g.,penicillin,amoxicillin)shouldbeprescribedonlyifgroupAstreptococcalpharyngitisisconfirmed.

PHARYNGITIS
ú Treatment Firstline
PenicillinGBenzathine 1.2millionunitsIMx1(adults)
Amoxicillin
Alternatives Firstgenerationoralcephalosporin Macrolide(?)
10daysoftreatment(?)
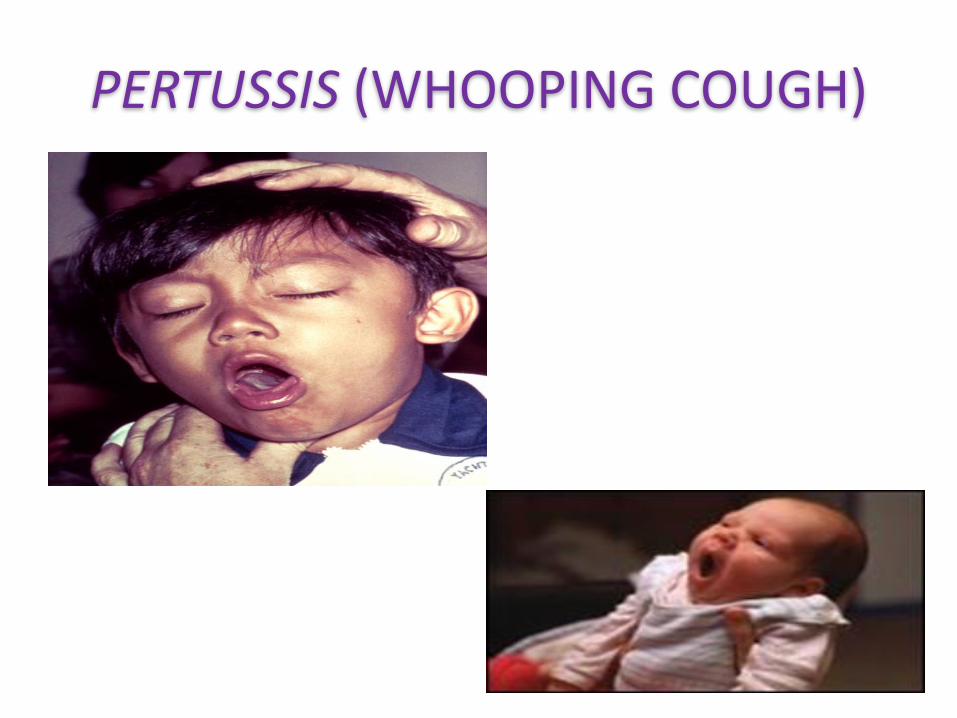
PERTUSSIS(WHOOPINGCOUGH)

PERTUSSIS
• CausedbyBordetellapertussis– Gram-negativecoccobacillus– Doesnotsurviveintheenvironment– Reservoirishumans.
• Symptomscanbesimilartothoseofacold.– Infectedadultsoftenspreadtheinfectiontoschoolsandnurseries.

PERTUSSIS
• Spreadbyairbornedropletsfrompatientsintheearlystages.
• Highlycontagious– Infects80-100%ofexposedsusceptibleindividuals.
– Spreadsrapidlyinschools,hospitals,offices,andhomes– justaboutanywhere.

PERTUSSIS• Mortalityishighestininfantsandchildrenunder
1yearold.• Immunizationagainstpertussisstartedinthe
1940s,andinthe60sinPortugal– ContinuestodayaspartofDTaP vaccination
• Pertussisappearstobemakingacomeback.– Epidemicsareoccurringevery3-5years.– Greatestnumbersofinfectionsareamong10-20
year-olds.– Peoplewhowerenotimmunized– Showsarelationshipbetweenlackofvaccination
andinfection

PERTUSSIS: Pathogenesis
• Bordetellapertussishasanaffinityforciliatedbronchialepithelium.
• Afterattaching,itproducesatrachealtoxin.– Immobilizesandprogressivelydestroystheciliated
cells.– Causespersistentcoughing
• Causedbytheinabilitytomovethemucusthatbuildsup
• Pertussisdoesnotinvadecellsoftherespiratorytractordeepertissues.
• Incubationperiodis7to10days.

PERTUSSIS:Pathogenesis
• Infectionhasthreestages:– CatarrhalStage1-2weeks
• Persistentperfuseandmucoidrhinorrhea(runnynose)
• Mayhavesneezing,malaise,andanorexia
• Mostcommunicableduringthisstage
– ParoxysmalStage1-6weeks
– ConvalescentStage3-6weeks
• Complicationofpertussiscanleadtosuperinfectionwith
Streptococcuspneumonia.

PERTUSSIS:Diagnosis
• Aconfirmedcaseisdefinedasoneofthefollowing:– AnycoughillnessinwhichB.pertussis isisolatedandcultured
– Acaseconsistentwiththeclinicalcasedefinitionconfirmedbypolymerasechainreaction(PCR)assayfindings
– Serologic antibodytitertestingisavailable,butoftenneedstobecomparedwithresults1-2weekslaterandthusisnotcommonlyhelpful

PERTUSSIS:Treatment
• Antibioticscanbeusedintheearlystages.
– Limitsthespreadofinfection
– Azithromycin isthechoiceforallages
• Oncetheparoxysmalstageisreached,therapy
isonlysupportive.
• Vaccinationisthebestoption.

VIRALINFECTIONSOFTHEUPPERRESPIRATORYTRACT
• RHINOVIRUSINFECTION-Thereareseveralhundredserotypesofrhinovirus.– Fewerthanhalfhavebeencharacterized.– 50%thathaveareallpicornaviruses.– Extremelysmall,non-enveloped,single-strandedRNAviruses
• Optimumtemperatureforpicornavirusgrowthis33˚C.– Thetemperatureinthenasopharynx

VIRALINFECTIONSOFTHEUPPERRESPIRATORYTRACT
• PARAINFLUENZA:Therearefourtypesofparainfluenzavirus.– Allbelongtotheparamyxovirusgroup.– Single-strandedenvelopedRNAviruses– Containhemagglutininandneuraminidase
• Transmissionandpathologysimilartoinfluenzavirus,buttherearedifferences.– Parainfluenzavirusreplicatesinthecytoplasm.– Influenzavirusreplicatesinthenucleus.

VIRALINFECTIONSOFTHEUPPERRESPIRATORYTRACT
• Parainfluenzaisgeneticallymorestablethaninfluenza.– Verylittlemutation– Littleantigenicdrift– Noantigenicshift
• Parainfluenza isaseriousproblemininfantsandsmallchildren.– Onlyatransitoryimmunitytoreinfection– Infectionbecomesmilderasthechildages.

Epstein-BarrVirus
38
Infectious mononucleosis and Epstein-Barr virus
• EBVisagammaherpesvirus– TwodistincttypesofEBV:
• type1(typeA):moreprevalentworldwide• type2(typeB):morecommoninAfrica
• Indevelopingcountries,subclinicalinfectioninchildhoodisvirtuallyuniversal.
• Indevelopedcountries,primaryinfectionmaybedelayeduntilearlyadultlife.
• Thevirusisacquiredfromasymptomaticexcretersviasaliva,bydropletinfection,orbykissing.
• EBVisnothighlycontagious,isolationisunnecessary.

DISEASEASSOCIATION1.InfectiousMononucleosis2.Burkitt'slymphoma3.Nasopharyngealcarcinoma4.Lymphoproliferativediseaseandlymphomaintheimmunosuppressed.
5.X-linkedlymphoproliferativesyndrome6.Chronicinfectiousmononucleosis7.OralleukoplakiainAIDSpatients8.ChronicinterstitialpneumonitisinAIDSpatients.
40

INFECTIOUSMONONUCLEOSIS• PrimaryEBVinfectionisusuallysubclinicalinchildhood.
Howeverinadolescentsandadults,thereisa50%chancethatthesyndromeofinfectiousmononucleosis(IM)willdevelop.
• IMisusuallyaself-limiteddiseasewhichconsistsoffever,lymphadenopathyandsplenomegaly.Insomepatientsjaundicemaybeseenwhichisduetohepatitis.Atypicallymphocytesarepresentintheblood.
• Complicationsoccurrarelybutmaybeseriouse.g.splenicrupture,meningoencephalitis,andpharyngealobstruction.
• Insomepatients,chronicIMmayoccurwhereeventuallythepatientdiesoflymphoproliferativediseaseorlymphoma.
41

INFECTIOUSMONONUCLEOSIS
Exudative pharyngotonsillitis42

INFECTIOUS MONONUCLEOSIS
• Whereas~90%ofcasesofIMareduetoEBV,5–10%ofcasesareduetoCytomegalovirus(CMV).
• CMVisthemostcommoncauseofheterophile-negativemononucleosis.
• Lesscommoncauses:rubella,Toxoplasma,HIV,herpesvirus6,hepatitisvirusesanddrugreactions.

COMPLICATIONS OF EPSTEIN–BARR VIRUS INFECTION

INFECTIOUSMONONUCLEOSIS
HepatosplenomegalyCervical lymphadenopathy 45

INFECTIOUSMONONUCLEOSIS
IMwithrashaftertreatmentwithamoxicillinorampicillin
46

Epstein–BarrVirus(MononucleosisandLymphoproliferativeDisorders)Katz,BenZ.,PrinciplesandPracticeofPediatricInfectiousDiseases,208,1059-1065.e6Copyright©2012©2012,ElsevierInc.Allrightsreserved.
MOLECULARBIOLOGY :LATENCY
• LatentlyinfectedBcellsaretheprimaryreservoirofEBVinthebody.
• >100geneproductsmaybeexpressedduringactiveviralreplication,only11areexpressedduringvirallatency.
• Inthisway,theviruslimitscytotoxicT-cellrecognitionofEBV-infectedcells.
48

Inchildrenunder10yearstheillnessismildandshort-lived,butinadultsover30yearsofageitcanbesevereandprolonged.InvestigationsAtypicallymphocytes arecommoninEBVinfectionbutalsooccurinothercausesofIM.Themostcommonlyuseddiagnosticcriteriaisthepresenceof50%lymphocytes(atleast10%atypical).AcuteEBVinfectiondiagnosisisusuallymade
bytheheterophilantibodytestand/ordetectionofanti-EBVVCAIgM.
Atypical lymphocytes.
Enlarged lymphocytes thathave abundantcytoplasm, vacuoles,and indentations ofthe cell membrane .
DIAGNOSIS
INFECTIOUSMONONUCLEOSIS:LAB
• A'heterophile'antibodyispresentduringtheacuteillnessandconvalescence,agglutinateserythrocytesofotherspecies,e.g.sheepandhorse.
• DetectedbytheclassicalPaul-Bunnelltitrationoramoreconvenientslidetestsuchasthe'Monotest'.

INFECTIOUSMONONUCLEOSIS:LAB
• SpecificEBVserology(immunofluorescence)canbeusedtoconfirmthediagnosisifnecessary.– AcuteinfectionischaracterizedbyIgMantibodiesagainsttheviralcapsid,antibodiestoEBVearlyantigenandtheinitialabsenceofantibodiestoEBVnuclearantigen(anti-EBNA).
– Seroconversionofanti-EBNAatapproximately1monthaftertheinitialillnessmayconfirmthediagnosisinretrospect.
• CNSinfectionsmaybediagnosedbydetectionofviralDNAincerebrospinalfluid.

ANTIBODIESINEBVINFECTION
Infection VCA IgG
VCA IgM
EA EBNA
No previous infection
- - - -
Acute infectionRecent infection
+
+
+
+/-
+/-
+/-
-
+/-
Past infection
+ - +/- +

response to viral capsid antigen (VCA) is divided because ofthe significant differences noted according to age of the patient.
Specific EBV antibodies
I.M.- TREATMENT
• Largelysymptomatic• Ifathroatcultureyieldsaβ-haemolyticStreptococcus,acourseofpenicillinshouldNOT beprescribed(colonization,notinfection).– ampicillinoramoxicillininthisconditioncommonlycausesanitchymacularrash,andshouldalsobeavoided.
• Whenpharyngealedemaissevere,ashortcourseofcorticosteroids,e.g.prednisolone30mgdailyfor5days,mayhelp.– Someadviseusingalsometronidazole
• AntiviralsarenotsufficientlyactiveagainstEBV.
I.M.- EVOLUTION
• Returntoworkorschoolisgovernedbythepatient'sphysicalfitness.
• Contactsportsshouldbeavoideduntilsplenomegalyhascompletelyresolvedbecauseofthedangerofsplenicrupture.
• 10%ofpatientswithIMsufferachronicrelapsingsyndrome.
Related Documents