D R A F T CVJ / VOL 55 / MARCH 2014 1 Case Report Rapport de cas Uncommon acute neurologic presentation of canine distemper in 4 adult dogs Alba Galán, Araceli Gamito, Beatrice E. Carletti, Alicia Guisado, Juana Martín de las Mulas, José Pérez, Eva M. Martín Abstract — Four uncommon cases of canine distemper (CD) were diagnosed in vaccinated adult dogs. All dogs had acute onset of neurologic signs, including seizures, abnormal mentation, ataxia, and proprioceptive deficits. Polymerase chain reaction for CD virus was positive on cerebrospinal fluid in 2 cases. Due to rapid deterioration the dogs were euthanized and CD was confirmed by postmortem examination. Résumé — Rare présentation neurologique aiguë de la maladie de Carré chez 4 chiens adultes. Quatre cas peu communs de maladie de Carré chez des chiens adultes vaccinés. Tous les cas ont présenté un début aigu ou suraigu des signes neurologiques, comportant principalement des crises épileptiques, altération de l’état mental, ataxie, et déficits proprioceptifs. Dans deux cas, la PCR a été positive à la maladie de Carré dans le liquide céphalo- rachidien. En raison de la progression rapide des signes, les chiens ont été euthanasiés et la maladie de Carré confirmée par la nécropsie. (Traduit par Ana Roman) Can Vet J 2014;55:0000–0000 A lthough canine distemper (CD) is not a common disease, in large part due to effective vaccines against canine distemper virus (CDV) (1), it remains a severe systemic viral disease of dogs worldwide. The typical course is characterized by a variety of clinical signs, including fever, respiratory, and enteric signs (2) that could progress to neurological signs (3). Infection with CDV can also result in ocular disease, cutaneous lesions, dental defects, and abortions (4). The degree of clini- cal illness and the tissues involved vary depending on the age of the animal, the strain of the virus, and the immune status of the host (2). Dogs of any age are susceptible, although the disease is most common in puppies between the ages of 3 and 6 mo (2,5), correlating with the decline in maternally derived immunity. Polysystemic and acute disease occurs in dogs with poor immune responses, while dogs with good cell-mediated responses and virus-neutralizing antibody titers may not be clini- cally affected (5). When dogs develop a weak immune response, the virus is able to reach the epithelial tissues and the central nervous system (CNS) (2). Once in the CNS, CDV can invade astrocytes, microglia, oligodendrocytes, neurons, ependymal cells, and choroid plexus cells. Infected oligodendrocytes are directly affected by the virus, leading to the characteristic lesions of demyelination; however, astrocytes are the main cell popula- tion that is typically infected (4). Most infected dogs have CNS involvement but clinical signs of CNS disease occur only in dogs with low or no antibody response (5). Localization in the CNS results in acute or chronic demyelination (2,5), and perivascular cuffing with lymphocytes, plasma cells, and monocytes is the main change in the demyelinated areas (2,6). Typically, neurologic signs associated with CDV include progressive partial or complete tetraparesis, vestibular signs, seizures, and dementia (2,3,5,6). Mioclonus of the temporal and forelimb muscles, and chewing-gum movements of the mouth are typical of CDV infection (2,3,5). The aim of this article is to highlight an uncommon acute neurologic CD presentation in 4 adult vaccinated dogs without previous systemic signs. Case descriptions Four adult dogs with acute or peracute onset of neurological signs (12 to 24 h before our first examination) were presented to the Veterinary Teaching Hospital of the University of Córdoba. These patients included a French bulldog and 3 mixed breeds, between 6 and 9 years old. None of the dogs had a history of respiratory, digestive, or neurologic disease. Three dogs had been vaccinated yearly and 1 of them had not been vaccinated in the past 4 y. In all cases vaccines included modified live strains of CDV (Onderstepoort and DICT-50 strains, Novivac DHPPi; Department of Animal Medicine and Surgery (Galán, Carletti, Guisado, Martin), Teaching Veterinary Hospital (Galán, Gamito, Guisado, Martin), Department of Anatomy and Comparative Pathology (de las Mulas, Pérez), University of Córdoba, Spain. Address all correspondence to Dr. Alba Galán; e-mail: [email protected] Use of this article is limited to a single copy for personal study. Anyone interested in obtaining reprints should contact the CVMA office ([email protected]) for additional copies or permission to use this material elsewhere.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
DR
AF
TD
RA
FT
CVJ / VOL 55 / MARCH 2014 1
Case Report Rapport de cas
Uncommon acute neurologic presentation of canine distemper in 4 adult dogs
Alba Galán, Araceli Gamito, Beatrice E. Carletti, Alicia Guisado, Juana Martín de las Mulas, José Pérez, Eva M. Martín
Abstract — Four uncommon cases of canine distemper (CD) were diagnosed in vaccinated adult dogs. All dogs had acute onset of neurologic signs, including seizures, abnormal mentation, ataxia, and proprioceptive deficits. Polymerase chain reaction for CD virus was positive on cerebrospinal fluid in 2 cases. Due to rapid deterioration the dogs were euthanized and CD was confirmed by postmortem examination.
Résumé — Rare présentation neurologique aiguë de la maladie de Carré chez 4 chiens adultes. Quatre cas peu communs de maladie de Carré chez des chiens adultes vaccinés. Tous les cas ont présenté un début aigu ou suraigu des signes neurologiques, comportant principalement des crises épileptiques, altération de l’état mental, ataxie, et déficits proprioceptifs. Dans deux cas, la PCR a été positive à la maladie de Carré dans le liquide céphalo-rachidien. En raison de la progression rapide des signes, les chiens ont été euthanasiés et la maladie de Carré confirmée par la nécropsie.
(Traduit par Ana Roman)
Can Vet J 2014;55:0000–0000
A lthough canine distemper (CD) is not a common disease, in large part due to effective vaccines against canine
distemper virus (CDV) (1), it remains a severe systemic viral disease of dogs worldwide. The typical course is characterized by a variety of clinical signs, including fever, respiratory, and enteric signs (2) that could progress to neurological signs (3). Infection with CDV can also result in ocular disease, cutaneous lesions, dental defects, and abortions (4). The degree of clini-cal illness and the tissues involved vary depending on the age of the animal, the strain of the virus, and the immune status of the host (2). Dogs of any age are susceptible, although the disease is most common in puppies between the ages of 3 and 6 mo (2,5), correlating with the decline in maternally derived immunity. Polysystemic and acute disease occurs in dogs with poor immune responses, while dogs with good cell-mediated responses and virus-neutralizing antibody titers may not be clini-cally affected (5). When dogs develop a weak immune response,
the virus is able to reach the epithelial tissues and the central nervous system (CNS) (2). Once in the CNS, CDV can invade astrocytes, microglia, oligodendrocytes, neurons, ependymal cells, and choroid plexus cells. Infected oligodendrocytes are directly affected by the virus, leading to the characteristic lesions of demyelination; however, astrocytes are the main cell popula-tion that is typically infected (4). Most infected dogs have CNS involvement but clinical signs of CNS disease occur only in dogs with low or no antibody response (5). Localization in the CNS results in acute or chronic demyelination (2,5), and perivascular cuffing with lymphocytes, plasma cells, and monocytes is the main change in the demyelinated areas (2,6).
Typically, neurologic signs associated with CDV include progressive partial or complete tetraparesis, vestibular signs, seizures, and dementia (2,3,5,6). Mioclonus of the temporal and forelimb muscles, and chewing-gum movements of the mouth are typical of CDV infection (2,3,5). The aim of this article is to highlight an uncommon acute neurologic CD presentation in 4 adult vaccinated dogs without previous systemic signs.
Case descriptionsFour adult dogs with acute or peracute onset of neurological signs (12 to 24 h before our first examination) were presented to the Veterinary Teaching Hospital of the University of Córdoba. These patients included a French bulldog and 3 mixed breeds, between 6 and 9 years old. None of the dogs had a history of respiratory, digestive, or neurologic disease. Three dogs had been vaccinated yearly and 1 of them had not been vaccinated in the past 4 y. In all cases vaccines included modified live strains of CDV (Onderstepoort and DICT-50 strains, Novivac DHPPi;
Department of Animal Medicine and Surgery (Galán, Carletti, Guisado, Martin), Teaching Veterinary Hospital (Galán, Gamito, Guisado, Martin), Department of Anatomy and Comparative Pathology (de las Mulas, Pérez), University of Córdoba, Spain.Address all correspondence to Dr. Alba Galán; e-mail: [email protected] of this article is limited to a single copy for personal study. Anyone interested in obtaining reprints should contact the CVMA office ([email protected]) for additional copies or permission to use this material elsewhere.
DR
AF
TD
RA
FT
2 CVJ / VOL 55 / MARCH 2014
RA
PP
OR
T D
E C
AS
Intervet/Schering-Plough Animal Health, Madrid, Spain and Duramune DAP 1 L; Pfizer, Madrid, Spain) and were adminis-tered 6 mo before clinical signs appeared. Physical examination, complete hematology, serum biochemistry, thoracic radiographs, and abdominal ultrasound were unremarkable in all dogs. The dogs were hospitalized so that we could make a diagnosis and provide supportive treatment.
Clinical presentation, neurologic examination, and develop-ments over 24 to 48 h are described in each case. In all cases, severe generalized seizures were unresponsive to anticonvul-sivant therapy and euthanasia was elected by the owners. Cerebrospinal fluid (CSF) was collected from all dogs at the cisterna magna. Details of the cases are presented in Table 1. All 4 dogs received supportive therapy consisting of trimethoprim/sulfadiazine (Borgal; Virbac, Barcelona, Spain), 30 mg/kg body weight (BW), q12h, IV, and intravenous fluid (Ringer-Lactate; B. Braun, Barcelona, Spain), 40 mL/kg BW per day. All 4 dogs also received diazepam (Valium; Roche Farma, Madrid, Spain) and phenobarbital (Luminal; Kern Pharma, Barcelona, Spain) as shown in Table 1.
Case 1This was a 9-year-old mixed breed neutered male that had been vaccinated yearly. The owner reported that 1 day before presen-tation the dog had shown abnormal mental status but no other signs. At the time of first examination, neurological signs were abnormal mentation (delirium), moderate ataxia, proprioceptive deficits, and absence of menace response. Cerebrospinal fluid (CSF) was collected and recovery from anesthesia was unevent-ful. During hospitalization the patient suffered generalized seizures unresponsive to diazepam; phenobarbital, 2 mg/kg BW, IV, bolus was necessary to control the first episode (Table 1). Due to the return of seizures, phenobarbital, 2 mg/kg BW per hour continuous rate infusion (CRI) was maintained for 6 h. Seizures recurred when the infusion rate was tapered and after 10 h of hospitalization humane euthanasia was performed.
Case 2This case involved a 7-year-old mixed breed neutered male that had been vaccinated yearly. The patient had been taken to a local veterinarian 2 d before presentation due to acute gener-alized seizures and anticonvulsivant therapy with diazepam, 1 mg/kg BW per rectum, was started (Table 1). At the time of first examination, neurological signs were ataxia, circling, and proprioceptive deficits. A sample of CSF was collected and recovery from anesthesia was slower than normal but uneventful. Ten hours after CSF collection the patient suffered generalized seizures unresponsive to diazepam, 2 mg/kg BW, IV, phenobar-bital, 3 mg/kg BW, IV bolus, and phenobarbital, 2 mg/kg BW/h CRI maintained for 5 h. Propofol (Propofol Lipuro; B. Braun) 6 mg/kg BW/h CRI was maintained for 6 h but seizures returned when the propofol CRI was tapered. After 35 h of treatment humane euthanasia was performed.
Case 3This case involved a 6-year-old entire female French bulldog that had been vaccinated yearly. The patient was seen by a local
veterinarian 1 day before presentation due to acute generalized seizures and diazepam, 2 mg/kg BW per rectum, was started. At the time of examination, the dog had abnormal mentation (depressed), compulsive walking, circling, ataxia, moderate hemiparesis, and proprioceptive deficits. Collection of CSF was uneventful; however, after anesthesia the patient remained in a depressed mental status. Three hours after CSF collection the patient suffered generalized seizures unresponsive to diazepam: 2 mg/kg BW, per rectum and 2 mg/kg BW, IV bolus, and to phenobarbital, 2 mg/kg BW, IV, bolus and 2 mg/kg BW per hour CRI maintained for 3 h (Table 1). Propofol (Propofol Lipuro; B. Braun), 6 mg/kg BW/h CRI, was maintained for 4 h but it was ineffective. Ketamine (Imalgene 1000; Mérial, Barcelona), 5 mg/kg BW, IV bolus and 5 mg/kg BW/h CRI were also ineffective. After 20 h of hospitalization the dog was humanely euthanized.
Case 4This dog was an 8-year-old mixed breed neutered male, which had not been vaccinated in the past 4 y. Mild pyrexia (from 38.8°C to 39.3°C) and bilateral mucous ocular discharge had been noted for the past 2 d. At the time of examination, the dog had generalized seizures (cluster), maintaining focal sensory seizure (aggression) between generalized seizure episodes, moder-ate tetraparesis, ataxia and proprioceptive deficits. Immediate anticonvulsivant therapy with diazepam, 2 mg/kg BW, IV bolus, was used to control the seizure. Recovery from anesthesia follow-ing collection of CSF was uneventful. Fifteen hours after CSF collection the patient suffered generalized seizures unresponsive to diazepam, 2 mg/kg BW, IV, but initially responsive to phe-nobarbital, 2 mg/kg BW, IV bolus and phenobarbital, 2 mg/kg BW per hour CRI was maintained for 3 h. Seizures returned after 4 h without CRI of phenobarbital but under phenobarbital maintenance dose of 2 mg/kg BW, q8h. During hospitalization, myoclonus of the temporal muscles and chewing activity were observed. Due to unresponsiveness to anticonvulsivant therapy and initial signs of aggression, the dog was humanely euthanized 40 h after the first examination.
An enzyme-linked immunosorbent assay (ELISA) for CDV was conducted on serum from the unvaccinated dog and high CD virus-antibody titers were detected. Basal CSF study included cell count (methylene blue technique), protein level [pyrogallol red colorimetric reaction (Biosystem A15; Atom, Barcelona, Spain)], glucose oxidase/peroxidase spectophotometry (Biosystem A15), and cytology (Diff-quick stain). Mild lymphocytic pleocytosis (9 to 21 cells/mL) and mild increased protein levels (mean 0.36 g/L; range: 0.32 to 0.40 g/L) were shown in all cases. All dogs were anesthetized using standard hospital protocols, medeto-midine (Domtor; Pfizer), 3 mg/kg BW, butorphanol (Butomidor; Virbac), 0.3 mg/kg BW, and propofol (Propofol-Lipuro 1%; B. Braun) at 4 mg/kg BW. Anesthesia was maintained with isoflurane (Isovet; B. Braun) in 100% oxygen at a flow rate of 50 mL/kg BW per minute using a circle rebreathing system (Excel 210SE; Ohmeda, Madrid). Heart rate, blood pressure, and blood oxygen-ation levels were monitored during anesthesia.
Polymerase chain reaction (PCR) for CDV, Ehrlichia canis, Neospora canis, and Toxoplasma gondii were performed on CSF in
DR
AF
TD
RA
FT
CVJ / VOL 55 / MARCH 2014 3
CA
SE
RE
PO
RT
all cases. Canine distemper virus was detected in cases 1 and 3. Microscopically, all tissue samples analyzed had severe vascular congestion, edema, and occasionally, focal hemorrhages. The lungs had severe vascular congestion and multifocal alveolar edema, as well as desquamation of bronchiolar epithelium with isolated acidophilic intracytoplasmic inclusion bodies (Cases 3 and 4). Severe mucosal desquamation and numerous mono-nuclear cells in the lamina propria and severe vascular congestion and edema in the submucosa were observed in the stomach and small intestine (Case 4). The transitional epithelium of the gall
bladder had isolated acidophilic intracytoplasmic inclusion bod-ies and the Bowman’s space contained abundant homogeneous, acidophilic material (Cases 2 and 3). Lymph nodes, spleen, and mucosa-associated lymphoid tissues had severe lymphoid depletion (Case 3).
Sections of CNS were examined for CDV-induced lesions. Microscopically, cerebral cortex, cerebellum, brain stem, and spinal cord showed marked hyperemia and focal hemorrhages in Virchow-Robbin spaces. Leptomeninges showed a severe inflammatory infiltrate composed of lymphocytes and plasma
Table 1. Clinical signs, evolution, treatment, and results of ELISA, RT-PCR and histopathology of the cases reported
Neurological signsClinical evolution and duration of clinical signs Treatment
RT-PCR with CSF Histopathologic changes
Case 1Mb, M, 9 yo, V
Abnormal mentation (depression, and delirium), moderate ataxia, propioceptive deficits, absence of menace response.
GS initially responsive to Pheno. GS returned in 2 h as status epilepticus unresponsive to anticonvulsivant therapy.10 h (1 d before owner reported abnormal mental status).
S/T and fluids, Dz 2 mg/kg BW, IV bolus (3 3). Pheno 2 mg/kg BW IV bolus (3 2) and 2 mg/kg BW/h as a CRI.
Positive Severe, non-purulent inflammation in the leptomeninges, gray matter and white matter of CNS and multifocal demyelination associated with multifocal hemorrhages.
Case 2Mb, M, 7yo, V
Generalized seizures responsive to diazepam, ataxia, circling, propioceptive deficits.
GS initially responsive to Dz (2 d)GS unresponsive to any anticonvulsivant therapy 10 h after CSF collection35 h (2 d before GS treated by a local veterinarian).
S/T and fluids, Dz 1 mg/kg BW per rectum (3 3) and 2 mg/kg BW, IV bolus (3 2).Pheno 3 mg/kg BW IV bolus (3 2) and 2 mg/kg BW/h as a CRI.Propofol 6 mg/kg BW/h as CRI.
Negative Acidophilic intracytoplasmic inclusion bodies in the transitional epithelium of the gall bladder.Severe, non-purulent inflammation in the leptomeninges, gray matter and white matter of CNS and multifocal demyelination associated with multifocal hemorrhages.
Case 3French bulldog, F, 6 yo, V
Seizures initially responsive to diazepam, abnormal mentation (obtunded), compulsive walking, circling, ataxia, moderate hemiparesis, propioceptive deficits.
GS initially responsive Dz (1 d)GS unresponsive to any anticonvulsivant therapy 3 h after CSF collection20 h (1 d before GS treated by a local veterinarian).
S/T and fluidsDz 2 mg/kg BW per rectum (3 2) and 2 mg/kg BW, IV bolus (3 2).Pheno 2 mg/kg BW, IV bolus (3 2) and 2 mg/kg BW/h as a CRI.Propofol 6 mg/kg BW/h as CRI. Ketamine 5 mg/kg BW, IV bolus and 5 mg/kg BW/h as a CRI.
Positive Acidophilic intracytoplasmic inclusion bodies in bronchiolar epithelium and in the transitional epithelium of the gall bladder.Lymph nodes, spleen and mucosa-associated lymphoid tissues had severe lymphoid depletion.No inflammatory or demyelination changes in the cervical spinal cord but severe edema of the leptomeninges at that level.
Case 4Mb, M, 8 yo, uV
Cluster 24 h, maintaining focal sensory seizure (aggression), moderate tetraparesis, ataxia and propioceptive deficits.Mild pyrexia (38.8°C–39.3°C), bilateral mucous ocular discharge.
GS initially responsive Dz (at first examination)GS responsive to anticonvulsivant therapy 15 h after CSF collectionGS returned 4 h after Pheno CRI was stoppedMyoclonus of the temporal muscles and chewing activity.
S/T and fluids,Dz 2 mg/kg BW, IV bolus — responsive.Dz 2 mg/kg BW, IV bolus (3 2).Pheno 2 mg/kg BW, IV bolus (3 2) and 2 mg/kg BW per hour as a CRI.
Negative Acidophilic intracytoplasmic inclusion bodies in bronchiolar epithelium. Severe mucosal desquamation, mononuclear cells infiltration and vascular congestion in the stomach and small intestine. Severe, non-purulent inflammation in the leptomeninges, gray matter and white matter of CNS and multifocal demyelination associated with multifocal hemorrhages.
BW — body weight, Mb — mixed breed, M — male, F — female, yo — years old, V — vaccinated yearly, uV — unvaccinated in the last 4 years, GS — generalized seizures, S/T — sufonamide/trimethoprim, Dz — diazepam, Pheno — phenobarbital, CNS — central nervous system, CSF — cerebrospinal fluid, CRI — continuous rate infusion, RT-PCR — reverse transcription-polymerase chain reaction. An ELISA was done for Case 4 and was positive.
DR
AF
TD
RA
FT
4 CVJ / VOL 55 / MARCH 2014
RA
PP
OR
T D
E C
AS
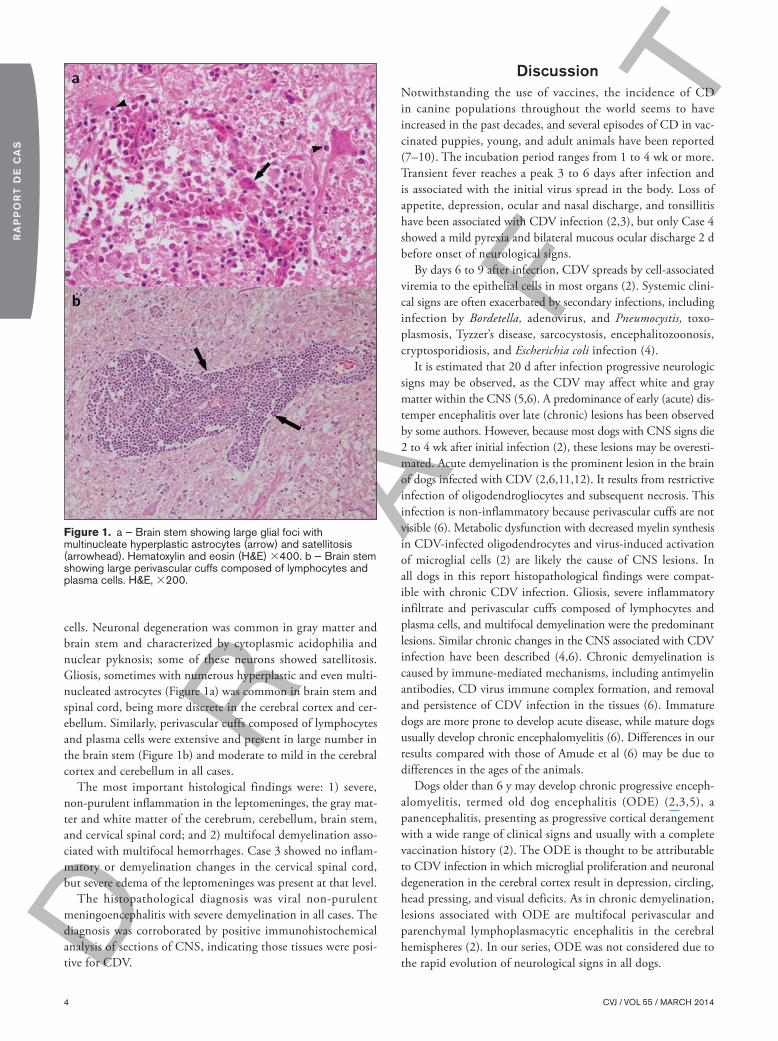
cells. Neuronal degeneration was common in gray matter and brain stem and characterized by cytoplasmic acidophilia and nuclear pyknosis; some of these neurons showed satellitosis. Gliosis, sometimes with numerous hyperplastic and even multi-nucleated astrocytes (Figure 1a) was common in brain stem and spinal cord, being more discrete in the cerebral cortex and cer-ebellum. Similarly, perivascular cuffs composed of lymphocytes and plasma cells were extensive and present in large number in the brain stem (Figure 1b) and moderate to mild in the cerebral cortex and cerebellum in all cases.
The most important histological findings were: 1) severe, non-purulent inflammation in the leptomeninges, the gray mat-ter and white matter of the cerebrum, cerebellum, brain stem, and cervical spinal cord; and 2) multifocal demyelination asso-ciated with multifocal hemorrhages. Case 3 showed no inflam-matory or demyelination changes in the cervical spinal cord, but severe edema of the leptomeninges was present at that level.
The histopathological diagnosis was viral non-purulent meningoencephalitis with severe demyelination in all cases. The diagnosis was corroborated by positive immunohistochemical analysis of sections of CNS, indicating those tissues were posi-tive for CDV.
DiscussionNotwithstanding the use of vaccines, the incidence of CD in canine populations throughout the world seems to have increased in the past decades, and several episodes of CD in vac-cinated puppies, young, and adult animals have been reported (7–10). The incubation period ranges from 1 to 4 wk or more. Transient fever reaches a peak 3 to 6 days after infection and is associated with the initial virus spread in the body. Loss of appetite, depression, ocular and nasal discharge, and tonsillitis have been associated with CDV infection (2,3), but only Case 4 showed a mild pyrexia and bilateral mucous ocular discharge 2 d before onset of neurological signs.
By days 6 to 9 after infection, CDV spreads by cell-associated viremia to the epithelial cells in most organs (2). Systemic clini-cal signs are often exacerbated by secondary infections, including infection by Bordetella, adenovirus, and Pneumocystis, toxo-plasmosis, Tyzzer’s disease, sarcocystosis, encephalitozoonosis, cryptosporidiosis, and Escherichia coli infection (4).
It is estimated that 20 d after infection progressive neurologic signs may be observed, as the CDV may affect white and gray matter within the CNS (5,6). A predominance of early (acute) dis-temper encephalitis over late (chronic) lesions has been observed by some authors. However, because most dogs with CNS signs die 2 to 4 wk after initial infection (2), these lesions may be overesti-mated. Acute demyelination is the prominent lesion in the brain of dogs infected with CDV (2,6,11,12). It results from restrictive infection of oligodendrogliocytes and subsequent necrosis. This infection is non-inflammatory because perivascular cuffs are not visible (6). Metabolic dysfunction with decreased myelin synthesis in CDV-infected oligodendrocytes and virus-induced activation of microglial cells (2) are likely the cause of CNS lesions. In all dogs in this report histopathological findings were compat-ible with chronic CDV infection. Gliosis, severe inflammatory infiltrate and perivascular cuffs composed of lymphocytes and plasma cells, and multifocal demyelination were the predominant lesions. Similar chronic changes in the CNS associated with CDV infection have been described (4,6). Chronic demyelination is caused by immune-mediated mechanisms, including antimyelin antibodies, CD virus immune complex formation, and removal and persistence of CDV infection in the tissues (6). Immature dogs are more prone to develop acute disease, while mature dogs usually develop chronic encephalomyelitis (6). Differences in our results compared with those of Amude et al (6) may be due to differences in the ages of the animals.
Dogs older than 6 y may develop chronic progressive enceph-alomyelitis, termed old dog encephalitis (ODE) (2,3,5), a panencephalitis, presenting as progressive cortical derangement with a wide range of clinical signs and usually with a complete vaccination history (2). The ODE is thought to be attributable to CDV infection in which microglial proliferation and neuronal degeneration in the cerebral cortex result in depression, circling, head pressing, and visual deficits. As in chronic demyelination, lesions associated with ODE are multifocal perivascular and parenchymal lymphoplasmacytic encephalitis in the cerebral hemispheres (2). In our series, ODE was not considered due to the rapid evolution of neurological signs in all dogs.
Figure 1. a — Brain stem showing large glial foci with multinucleate hyperplastic astrocytes (arrow) and satellitosis (arrowhead). Hematoxylin and eosin (H&E) 3400. b — Brain stem showing large perivascular cuffs composed of lymphocytes and plasma cells. H&E, 3200.

DR
AF
TD
RA
FT
CVJ / VOL 55 / MARCH 2014 5
CA
SE
RE
PO
RT
Usually, CNS-infected dogs show neurological signs such as circling, hyperesthesia, seizures, cerebellar or vestibular disease (head tilt, nystagmus), paresis or paralysis and myoclonus in addition to systemic signs (3,5,6). A few uncommon CD cases with neurologic signs but without characteristic signs of the disease in adult dogs have been reported (4,6,10). An atypical case was diagnosed in a vaccinated healthy adult dog showing circling, seizures, optic neuritis, and blindness (10). Lisiak et al (13) and Amude et al (6) described CDV infected dogs (7 mo and 13 y old) with distemper encephalomyelitis presenting atypical neurological signs such as seizures, cerebellar and/or vestibular signs and tetraparesis/plegia in the absence of systemic signs. As in our cases, clinical presentation of these cases dif-fers from typical extraneural signs and myoclonus observed in adult dogs. In the Amude et al (6) study (which included 8 dogs with CD) an acute onset of neurological signs was observed in 2 cases and a gradual progressive course in the remaining 6 cases; however, the nervous signs were progressive and multifocal in all 8 dogs. In our series, despite chronic histopathological CNS lesions, all dogs had an acute onset of signs with rapid clinical deterioration. Refractory seizures were the critical factor that may have determined the poor outcome.
The only dog that had systemic (mild pyrexia and bilateral mucous ocular discharge) and neurologic (myoclonus of the temporal muscles and chewing activity) signs in addition to acute neurological signs was the unvaccinated dog (Case 4). Although this dog was vaccinated yearly earlier, he should be considered as unvaccinated; since protective immunity induced by live modified vaccines persist for no more than 3 y.
Vaccination occasionally fails (14), and approximately 30% of CDV encephalitis cases have been reported in immunized dogs (15). Vaccine failures are mostly attributable to incorrect vaccine protocols or vaccine alteration after improper storage (2), but host factors (immunodeficiency, maternal antibody interference, vaccination during incubation period) or possible mutation of the wild CDV have been considered (15). Also, new CD virus genetic variants may be associated with pathogenesis changes or immune evasion in dogs vaccinated with current vaccines (16). In our series 3 dogs were vaccinated yearly with attenu-ated strains of CDV in common combined vaccines (CDV plus adenovirus, hepatitis, parainfluenza, and parvovirus) employed in Spain. Vaccination should therefore never be considered completely effective (15,17).
Canine distemper virus diagnosis is established by a combina-tion of fluorescent antibody staining, reverse transcription PCR, electron microscopy, and histopathology (1). Various assays have been suggested for the definitive antemortem diagnosis of distemper. However, due to the variable course of the disease, organ manifestation and a lack of or delayed humoral and cellu-lar immune responses, the final diagnosis for most cases remains uncertain (17). Immunofluorescence (IF) on conjunctival, nasal, and vaginal smears is not sensitive. It can detect CDV antigens only within 3 wk after infection, when the virus is still present in the epithelial cells (2). Virus-specific immunoglobulin M (IgM) persists for at least 3 mo after infection and may be spe-cifically recognized by ELISA and used as a marker of recent CDV infection (18). However, high antibody titers to CDV
may also be detected for several months after vaccination (2). The determination of CDV serum neutralizing antibodies in CSF may be helpful in cases of CNS chronic infection, but the results are variable and depend on the stage of the disease (17). Reverse transcription-polymerase chain reaction (RT-PCR) with serum or whole blood is a highly specific, sensitive, and rapid method for ante-mortem diagnosis of distemper in dogs, regard-less of the form of distemper, humoral immune response, and viral antigen distribution (17). However, a negative PCR assay does not rule out the presence of the infectious agent (19). Shin et al (20) used RT-PCR for detection of CDV ribonucleic acid (RNA) in peripheral blood mononuclear cells from dogs with suspected distemper. However, only 53% of the animals were positive by RT-PCR, and the diagnosis of distemper was not confirmed by or correlated with the results of other methods, including immunohistochemistry, histopathology, and in-vitro virus isolation. Although serum, whole blood, and CSF appeared to be equally suitable as substrate for the RT-PCR, Frisk et al (17) showed that use of RT-PCR with all 3 of these body fluids increased sensitivity. Studies by Frisk et al (17) indicate that previous vaccination does not cause false positives. In our series only RT-PCR in CSF was performed. Since the last vaccination was administered 6 mo before CSF collection false positives were unlikely.
The various neurological signs associated with CDV encepha-litis and the limited value of methods available for ante-mortem diagnosis may complicate the clinical diagnosis (3,17,21). Immunohistochemistry represents a highly sensitive and specific method for detection of CDV in tissues obtained postmortem (17), thus postmortem histological examination of CNS is essential for the specific diagnosis (17,19). In our series, the positive RT-PCR and immunohistochemistry results associated with histopathological findings supported the diagnosis.
Acute neurological signs in spite of chronic histological lesions have been unusually reported in the literature associ-ated with CDV infection in adult dogs. However, CD should be considered in differential diagnoses in adult dogs with acute and severe neurological signs even if they are vaccinated and PCR for CDV in CSF is negative.
AcknowledgmentThe authors thank Ms. Ana Roman for providing the French translation of the abstract. CVJ
References1. Schumaker BA, Miller MM, Grosdidier P, et al. Canine distemper out-
break in pet store puppies linked to a high-volume dog breeder. J Vet Diagn Invest 2012;24:1094–1098.
2. Martella V, Elia G, Buonavoglia C. Canine distemper virus. Vet Clin Small Anim 2008;38:787–797.
3. Rance KS. Virosis Caninas. En Ettinger S, Feldman E, eds. Tratado de Medicina Interna Veterinaria. St. Louis, Missouri: Elsevier Saunders, 2007:649–650.
4. Roady PJ, Singh K, Basavarajappa MS. Pathology in practice. Distemper. J Am Vet Med Assoc 2012;15:1169–1171.
5. Taylor SM: Encephalitis, myelitis and meningitis. In: Couto CG, Nelson RW, eds. Small Animal Internal Medicine. 4th ed. St. Louis, Missouri: Mosby Elsevier, 2009:1059–1062.
6. Amude AM, Alfieri AA, Alfieri AF. Clinicopathological findings in dogs with distemper encephalomyelitis presented without characteristic signs of the disease. Res Vet Sci 2007;82:416–422.
DR
AF
TD
RA
FT
6 CVJ / VOL 55 / MARCH 2014
RA
PP
OR
T D
E C
AS
7. Appel MJ, Summers BA. Pathogenicity of morbilliviruses for terrestrial carnivores. Vet Microbiol 1995;44:187–191.
8. Blixenkrone-Møller M, Svansson V, Appel M, Krogsrud J, Have P, Orvell C. Antigenic relationship between field isolates of morbilliviruses from different carnivores. Arch Virol 1992;123:279–294.
9. Decaro N, Camero M, Greco G, et al. Canine distemper and related diseases: Report of a severe outbreak in a kennel. New Microbiol 2004; 27:177–181.
10. Richards TR, Whelan NC, Pinard CL, Alcala FC, Wolfe KC. Optic neuritis caused by canine distemper virus in a Jack Russell terrier. Can Vet J 2011;52:398–402.
11. Vandevelde M, Kristensen B, Braund KG, Greene CE, Swango LJ, Hoerlein BF. Chronic canine distemper virus encephalitis in mature dogs. Vet Pathol 1980;17:17–28.
12. Headley SA, Amude AM, Alfieri AF, Bracarense AP, Alfieri AA, Summers BA. Molecular detection of canine distemper virus and the immunohistochemical characterization of the neurologic lesions in naturally occurring old dog encephalitis. J Vet Diagn Invest 2009;2: 588–597.
13. Lisiak JA, Vandevelde M. Polioencephalomalacia associated with canine distemper virus infection. Vet Pathol 1979;16:650–660.
14. Blixenkrone-Møller M, Svansson V, Have P, et al. Studies on manifesta-tions of canine distemper virus infection in an urban dog population. Vet Microbiol 1993;37:163–173.
15. Koutinas AF, Puolizopuolou ZS, Baumgaertner W, Lekkas S, Kontos V. Relation to clinical signs to pathological changes in 19 cases of canine distemper encephalomyelitis. J Comp Pathol 2002;126:47–56.
16. Kapil S, Yeary T. Canine distemper spillover in domestic dogs from urban wildlife. Vet Clin Small Anim 2011;41:1069–1086.
17. Frisk AL, Koènin M, Moritz A, Baumgärtner W. Detection of canine distemper virus nucleoprotein RNA by reverse transcription-PCR using serum, whole blood and cerebrospinal fluid from dogs with distemper. J Clin Microbiol 1999;37:3634–3643.
18. Blixenkrone-Møller M, Pedersen IR, Appel MJ, Griot C. Detection of IgM antibodies against canine distemper virus in dog and mink sera employing enzyme-linked immunosorbent assay (ELISA). J Vet Diagn Invest 1991;3:3–9.
19. Di Terlizzi R, Platt SR. The function, composition and analysis of cerebrospinal fluid in companion animals: Part II — Analysis. Vet J 2009;180:15–32.
20. Shin YS, Mori T, Okita M, Gemma T, Kai C, Mikami T. Detection of canine distemper virus nucleocapsid protein gene in canine peripheral blood mononuclear cell by RT-PCR. J Vet Med Sci 1995;57:439–445.
21. Amude AM, Alfieri AF, Alfieri AA. Use of immunohistochemistry and molecular assay such as RT-PCR for precise post mortem diagnosis of distemper-related encephalitis. En Méndez-Vilas, ed. Communicating Current Research and Educational Topics and Trends in Applied Microbiology. Formatex 2007:1539–1545.
Related Documents











