Eur J Appl Physiol (2008) 104:193–199 DOI 10.1007/s00421-008-0727-5 123 ORIGINAL ARTICLE The trainability and contralateral response of cold-induced vasodilatation in the Wngers following repeated cold exposure Igor B. Mekjavic · Uron Dobnikar · Stylianos N. Kounalakis · Bojan Musizza · Stephen S. Cheung Accepted: 13 March 2008 / Published online: 12 April 2008 © Springer-Verlag 2008 Abstract Cold-induced vasodilatation (CIVD) is pro- posed to be a protective response to prevent cold injuries in the extremities during cold exposure, but the laboratory- based trainability of CIVD responses in the hand remains equivocal. Therefore, we investigated the thermal response across the Wngers with repeated local cold exposure of the whole hand, along with the transferability of acclimation to the Wngers of the contralateral hand. Nine healthy subjects immersed their right hand up to the styloid process in 8°C water for 30 min daily for 13 days. The left hand was immersed on days 1 and 13. Skin temperature was recorded on the pads of the Wve Wngertips and the dorsal surface of the hand. The presence of CIVD, deWned as an increase in Wnger skin temperature of 0.5°C at any time during cooling, occurred in 98.5% of the 585 (9 subjects £ 5 sites £ 13 trials) measurements. Seven distinct patterns of thermal responses were evident, including plateaus in Wnger temper- ature and superimposed waves. The number (N) of CIVD waves decreased in all digits of the right hand over the accli- mation period (P = 0.02), from average (SD) values ranging from 2.7 (1.7) to 3 (1.4) in diVerent digits on day 1, to 1.9 (0.9) and 2.2 (0.7) on day 13. Average (SD) Wnger skin tem- perature (T avg ) ranged from 11.8 (1.4)°C in Wnger 5 to 12.7 (2.8)°C in Wnger 3 on day 1, and then decreased signiWcantly (P < 0.001) over the course of the training immersions, attaining values ranging from 10.8 (0.9)°C in Wnger 4 to 10.9 (0.9)°C in Wnger 2 on day 13. In the contralateral hand, N was reduced from 2.5 to 1.5 (P < 0.01) and T avg by »2°C (P < 0.01). No changes were observed in thermal sensation or comfort of the hand over the acclimation. We conclude that, under conditions of whole-hand immersion in cold water, CIVD is not trainable and may lead to systemic atten- uation of thermal responses to local cooling. Keywords CIVD · Cold water immersion · Adaptation Introduction Shortly upon exposure to cold environments, skin tempera- ture of the extremities can rapidly increase and decrease in a cyclic fashion. This cold-induced vasodilatation (CIVD) phenomenon was Wrst reported by Lewis (1930) in the Wngers and has since been observed in various sites of the human body (Fox and Wyatt 1962). CIVD has generally been presumed to perform a cryoprotective function to maintain tissue integrity and minimize the risk of cold inju- ries. Therefore, the question arises whether the CIVD response can be trained so as to enhance the protection against cold injury. It is generally agreed that cold-adapted or acclimatized subjects have improved CIVD parameters I. B. Mekjavic (&) · S. N. Kounalakis Department of Automation, Biocybernetics and Robotics, Jozef Stefan Institute, Jamova 39, 1000 Ljubljana, Slovenia e-mail: [email protected] U. Dobnikar Department of Traumatology, University Clinical Centre, Ljubljanska 5, 2000 Maribor, Slovenia B. Musizza Department of Systems and Control, Jozef Stefan Institute, Jamova 39, 1000 Ljubljana, Slovenia S. N. Kounalakis National and Kapodistrian University of Athens, Ethnikis Antistasis 41, 17532 Dafne, Athens, Greece S. S. Cheung Department of Physical Education and Kinesiology, Brock University, 500 Glenridge Ave., L2S-3A1 St. Catharines, ON, Canada

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Eur J Appl Physiol (2008) 104:193–199
DOI 10.1007/s00421-008-0727-5ORIGINAL ARTICLE
The trainability and contralateral response of cold-induced vasodilatation in the Wngers following repeated cold exposure
Igor B. Mekjavic · Uron Dobnikar · Stylianos N. Kounalakis · Bojan Musizza · Stephen S. Cheung
Accepted: 13 March 2008 / Published online: 12 April 2008© Springer-Verlag 2008
Abstract Cold-induced vasodilatation (CIVD) is pro-posed to be a protective response to prevent cold injuries inthe extremities during cold exposure, but the laboratory-based trainability of CIVD responses in the hand remainsequivocal. Therefore, we investigated the thermal responseacross the Wngers with repeated local cold exposure of thewhole hand, along with the transferability of acclimation tothe Wngers of the contralateral hand. Nine healthy subjectsimmersed their right hand up to the styloid process in 8°Cwater for 30 min daily for 13 days. The left hand wasimmersed on days 1 and 13. Skin temperature was recordedon the pads of the Wve Wngertips and the dorsal surface of thehand. The presence of CIVD, deWned as an increase inWnger skin temperature of 0.5°C at any time during cooling,occurred in 98.5% of the 585 (9 subjects £ 5 sites £13 trials) measurements. Seven distinct patterns of thermal
responses were evident, including plateaus in Wnger temper-ature and superimposed waves. The number (N) of CIVDwaves decreased in all digits of the right hand over the accli-mation period (P = 0.02), from average (SD) values rangingfrom 2.7 (1.7) to 3 (1.4) in diVerent digits on day 1, to 1.9(0.9) and 2.2 (0.7) on day 13. Average (SD) Wnger skin tem-perature (Tavg) ranged from 11.8 (1.4)°C in Wnger 5 to 12.7(2.8)°C in Wnger 3 on day 1, and then decreased signiWcantly(P < 0.001) over the course of the training immersions,attaining values ranging from 10.8 (0.9)°C in Wnger 4 to10.9 (0.9)°C in Wnger 2 on day 13. In the contralateral hand,N was reduced from 2.5 to 1.5 (P < 0.01) and Tavg by »2°C(P < 0.01). No changes were observed in thermal sensationor comfort of the hand over the acclimation. We concludethat, under conditions of whole-hand immersion in coldwater, CIVD is not trainable and may lead to systemic atten-uation of thermal responses to local cooling.
Keywords CIVD · Cold water immersion · Adaptation
Introduction
Shortly upon exposure to cold environments, skin tempera-ture of the extremities can rapidly increase and decrease ina cyclic fashion. This cold-induced vasodilatation (CIVD)phenomenon was Wrst reported by Lewis (1930) in theWngers and has since been observed in various sites of thehuman body (Fox and Wyatt 1962). CIVD has generallybeen presumed to perform a cryoprotective function tomaintain tissue integrity and minimize the risk of cold inju-ries. Therefore, the question arises whether the CIVDresponse can be trained so as to enhance the protectionagainst cold injury. It is generally agreed that cold-adaptedor acclimatized subjects have improved CIVD parameters
I. B. Mekjavic (&) · S. N. KounalakisDepartment of Automation, Biocybernetics and Robotics, Jozef Stefan Institute, Jamova 39, 1000 Ljubljana, Sloveniae-mail: [email protected]
U. DobnikarDepartment of Traumatology, University Clinical Centre, Ljubljanska 5, 2000 Maribor, Slovenia
B. MusizzaDepartment of Systems and Control, Jozef Stefan Institute, Jamova 39, 1000 Ljubljana, Slovenia
S. N. KounalakisNational and Kapodistrian University of Athens, Ethnikis Antistasis 41, 17532 Dafne, Athens, Greece
S. S. CheungDepartment of Physical Education and Kinesiology, Brock University, 500 Glenridge Ave., L2S-3A1 St. Catharines, ON, Canada
123
194 Eur J Appl Physiol (2008) 104:193–199
(shorter onset time, higher minimal and mean Wnger skintemperatures) unless the adaptation is a hypothermic one, inwhich case a lower central body temperature attenuates theCIVD response (Daanen 2003).
Most studies investigating the eVect of adaptation on theCIVD response have compared diVerent ethnic groups liv-ing in diVerent climates. For example, Meehan (1955)found that the Wnger skin temperatures of Alaskan nativeswere higher compared with the respective temperatures ofCaucasians and blacks during immersion in ice water.Brown and Page (1952), Miller and Irving (1962) andLeBlanc et al. (1975) showed that Inuits have higher Wngerskin temperatures and hand blood Xows with strongerCIVD responses during local hand cooling than Cauca-sians. On the contrary, Paik et al. (1972) found that coldadapted divers had weaker CIVD responses with reducedWnger blood Xows than a non-diver group. They suggestedthat the insulative cold adaptation of the divers was respon-sible for the observed diVerences between groups. In someof the few longitudinal training studies, Purkayastha et al.(1992, 1993) showed that the CIVD of tropical residentsbecame more pronounced 7 weeks after they moved to anarctic region but did not reach the levels of Arctic natives.Rintamaki et al. (1993) observed increased Wnger tempera-tures with partial general cold adaptation during immersionof the hand in 10°C water of indoor workers who spent53 days working outdoors in Antarctica.
Controlled laboratory studies present equivocal evidenceof Wnger adaptation to repeated cold exposures. Adams andSmith (1962) immersed subject’s terminal two phalanges ofthe index Wnger in ice water 4–6 times per day for 1 month,and found that the CIVD of the exposed Wngers wasenhanced with earlier onset, more rapid increase and with ahigher plateau. Geurts et al. (2005) immersed the wholehand in 8°C water for 30 min for 15 sessions and measuredtemperature at the nail bed of the index Wnger. They foundthat all CIVD parameters of the index Wngers decreasedafter 3 weeks of acclimation, speculating that repeatedimmersions in cold water might actually blunt CIVDresponse and increase the risk of cold injury of the hands.In contrast, a subsequent study by the same research groupfound no change in CIVD parameters after 2 weeks ofrepetitive immersions, using a similar experimental proto-col (Geurts et al. 2006). O’Brien (2005) demonstrated ahigh degree of CIVD reproducibility over Wve daily immer-sions of the middle Wnger in ice water, implying minimaladaptation in CIVD response. One possible reason for thediscrepancy across lab studies is diVerences in the intensity,duration, and degree of extremity exposure to cold.
With the continued lack of consensus on the short-termtrainability of the CIVD response in the hand, the primaryobjective of this study was to evaluate, in a controlled labo-ratory trial, the eVect of 13 daily repetitive immersions of
the whole hand in 8°C water on local Wnger thermoregula-tory and blood Xow responses. In addition, we investigatedthe transferability of adaptations by testing responses in thenon-trained contralateral hand.
Methods
Subjects
Nine male subjects with an average (SD) age of 25 (5) years,height 1.81 (0.05) and mass 80.4 (5.9) kg participated in thepresent study. The National Medical Ethics Committee ofthe Republic of Slovenia approved the experimental proce-dure. Written informed consent was obtained from all sub-jects before the start of the experiments. A health-screeningtest was used before recruiting the participants. The aim wasto exclude subjects with a history of cold injury, cold handsyndrome, Raynauds disease, smokers and/or subjects whouse any anti-hypertensive medication. Data were collectedduring September to October to avoid acclimatization toeither sustained heat or cold exposure.
Experimental design
The overall goal of the adaptation protocol was balancedbetween the demonstrated need for prolonged multipleexposures (Adams and Smith 1962) to ensure adaptation andthe practical limits of what individuals may reasonably per-form prior to cold exposure in the Weld. All subjects partici-pated in 15 experimental sessions that were conducted in13 days and included 13 training immersions for the righthand and 2 immersions for the contralateral (left) hand. Thesubjects completed one session per day except on the Wrstand the last day, during which two immersions (Wrst theirright and later the left hand) were conducted. All the immer-sions were conducted at the same time of the day for eachsubject to avoid diurnal variations in the CIVD response.The subjects were asked not to drink coVee or caVeinatedbeverages and to abstain from any sport, recreational activityor heavy physical exertion at least 2 h before the tests.
Experimental protocol
In each experiment, subjects arrived in the lab at least20 min before the start of the measurements to adapt to thecontrolled thermoneutral (»27°C, 35% relative humidity)environment in the laboratory. Subjects were lightlydressed in a T-shirt and long trousers, and remained restingon a semi reclining chair for the duration of the experiment.Upon arrival, subjects were instrumented for the measure-ment of heart rate (HR), blood pressure and skin tempera-ture. The right hand was then covered with a thin plastic
123

Eur J Appl Physiol (2008) 104:193–199 195
bag that was sealed with air-permeable tape to the skin,approximately 10 cm above the wrist. Care was taken toremove all the air from the bag and to free the thermocou-ple sites from any plastic bag folds.
All parameters (HR, blood pressure, skin temperatures,tympanic temperature) were recorded in the pre-immersionphase, and during the warm and cold-water immersionphases. During the cold-water immersion, measurementswere made at minutes 1, 3 and 5 and every 5 min thereafter.At the same time periods, subjects were asked to provide arating of their temperature perception and thermal comfort.All participants were familiarized with the temperature per-ception and thermal comfort scales to avoid any misinter-pretations during the immersion.
After the start of the measurements, subjects remained inthe semi reclining chair for 3 min with their hands at thelevel of the hips, and resting values were recorded. After 3-min rest, the right hand was immersed up to the ulnar andradial styloids in warm (35°C) water for 5 min. After 5 minin warm water, subjects immersed their right hand in coldwater (8°C). The hand was immersed up to the radial andulnar styloids. An air pillow was positioned between theedge of the immersion bath and the forearm, so that the armrested on the pillow and the wrist was 45° Xexed in thewater. The duration of the cold-water immersion was30 min. After 30 min, the hand was removed from thewater, and dried with a towel, if wet.
On days 1 and 13, following the right hand immersiontrial, subjects had a 20 min break in the same environmentand then all the procedures were repeated for the left hand.
Analytical procedure and equipment
Finger pad skin temperature measurements were used in allexperiments to determine the vascular changes duringimmersion of Wngers in cold water. The Wnger pads proved tobe a reliable temperature measuring site for evaluation ofthese changes (Daanen 2003; O’Brien 2005). The Wnger padhas a rich blood supply and is a site where AV anastomosesare present, and these are responsible for the CIVD response.
Copper-constantan (T-type) thermocouples (PhysitempInstruments Inc., Clifton, NJ, USA) were used in all experi-ments. Six skin probes were used. The probes were posi-tioned in the middle of the palmar side of the distal phalanxof all Wve Wngers of the hand. An additional probe wasattached to the dorsal side of a hand between the 3rd and4th metacarpal bones. The probes were attached directly tothe skin by thin air-permeable tape (Tegaderm, 3 M,Healthcare, St. Paul, MN, USA).
Skin temperature of the Wngers and hands were continu-ously measured and logged every 8 s by an Almemo dataacquisition system (Almemo 5290-9 V5, Ahlborn, Holzkir-chen, Germany). The data were Wrst stored in the data log-
ger and then downloaded to a personal computer for furtheranalysis after each experiment.
Beat-by-beat heart rate was measured continuously witha Polar system (Polar Electro Inc., Lake Success, NY,USA), and stored in the Polar wristwatch. Data were down-loaded to the same computer after each experiment.
Systolic (SAP, mmHg) and diastolic (DAP, mmHg)blood pressures were measured continuously with a nonin-vasive blood pressure monitor (Finapress, Ohmeda 2300,ON, Canada). The cuV of the blood pressure monitor wasplaced on the middle phalanx of the middle Wnger of thenon-immersed hand, which was positioned on the left thighduring experiments and subjects were asked not to movetheir hand and Wngers during the monitoring.
Tympanic temperature was measured using a commer-cially available infrared thermometer (ThermoScan IRT3020, Braun, Kronberg, Germany). Three consecutive mea-surements were performed each time and the highest valuewas considered representative of core temperature.
Subjective ratings of thermal perception and thermalcomfort were recorded before, during and after the cold-water immersion. The thermal sensation scale ranged from0 (unbearably cold) to 9 (very hot). The thermal comfortscale ranged from 1 (comfortable) to 4 (very uncomfort-able).
An insulated metal immersion tank (80 £ 30 £ 25 cm)with active cooling system (Haake, Germany) was used forthe cold-water immersions in all the experiments. A propel-ler continuously stirred the water inside the tank. A smallerplastic bucket was used for warm-water immersion (35°C)set with the aid of a mercury thermometer control.
Statistical analysis
A computer program written in Matlab language (Math-Works Inc., USA) was developed to determine all theCIVD parameters from the raw data (for deWnition of theparameters see Table 2). The results of the computer analy-sis were always manually checked to ensure that noextremes of the temperature versus time curves were misin-terpreted. A CIVD event was deWned as an increase in digit/site skin temperature >0.5°C to provide the most liberalinterpretation of CIVD.
A two-way analysis of variance (Statistica 5.0, USA)with repeated measures was used for statistical analysiswith independent variables, the Wngers (5 Wngers) and time(13 immersion days). A one-way analysis of variance(ANOVA) was used to deWne the diVerences in average HRor BP over the 30 min immersion period. A Tukey post hocanalysis was performed, if main eVects were found for aparticular independent variable. DiVerences in temperatureperception (TSS) and thermal comfort (TCS) betweenexperiments at speciWc times of immersion were evaluated
123
196 Eur J Appl Physiol (2008) 104:193–199
with a Wilcoxon matched pairs non-parametric test. Para-metric data are presented as means (SD) and non-param-teric as median (range). The signiWcance level was set at0.05.
Results
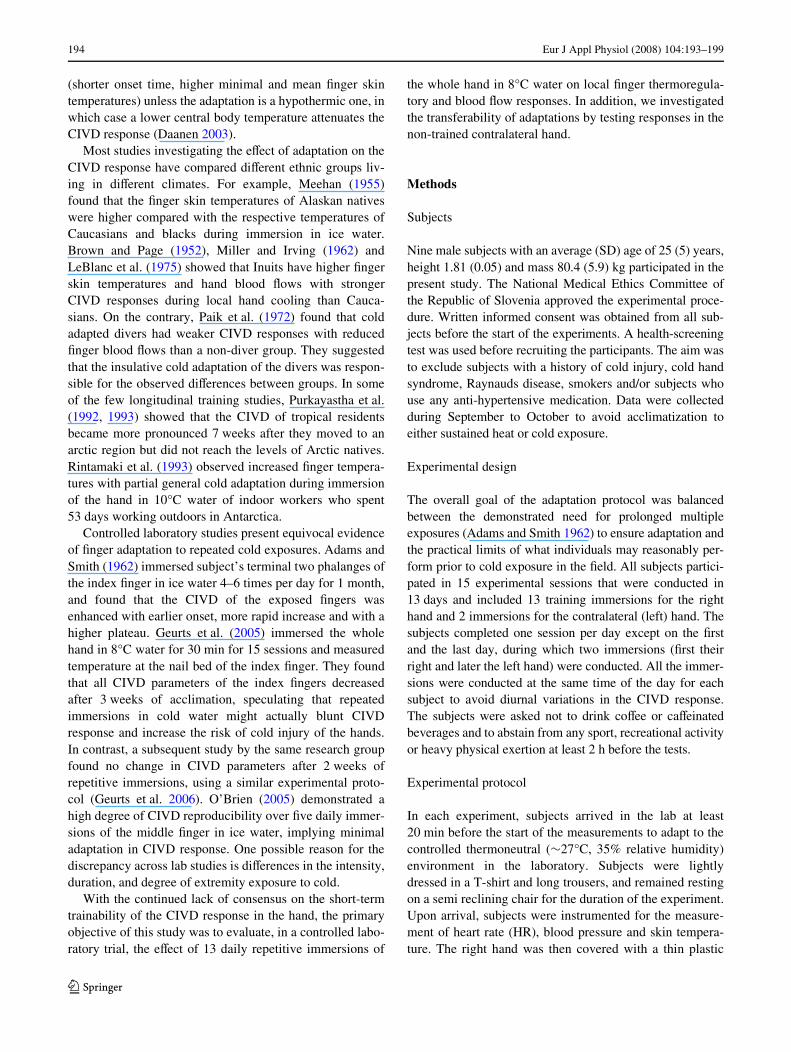
The prevalence of CIVD during the 13-day immersiontraining is shown in Table 1. There were no signiWcant
diVerences between Wngers, but the number of waves (N)was reduced during the 13-day training period. On day 1 ofthe training immersions, the average (SD) value for Nranged from 2.7 (1.7) in Wnger 2 to 3 (1.4) in Wnger 5, anddecreased signiWcantly (P < 0.05) over the 13-day trainingperiod. N ranged between 1.9 (0.9) in Wnger 2 and 2.2 (0.7)in Wnger 3 on day 13. The average Wnger skin temperature(Tavg) was also reduced after the 13-day immersion train-ing. On day 1 of the training immersions, Tavg ranged from11.8 (1.4)°C in Wnger 5 to 12.7 (2.8)°C in Wnger 3, and thendecreased signiWcantly (P < 0.001) over the course of thetraining immersions, attaining values ranging from 10.8(0.9)°C in Wnger 4 to 10.9 (0.9)°C in Wnger 2 on day 13.The remainder of the CIVD parameters remainedunchanged during immersion training period (Table 2).There was a tendency, albeit not signiWcant, for diVerencesbetween Wngers in the number of waves and maximum tem-perature (Table 2).
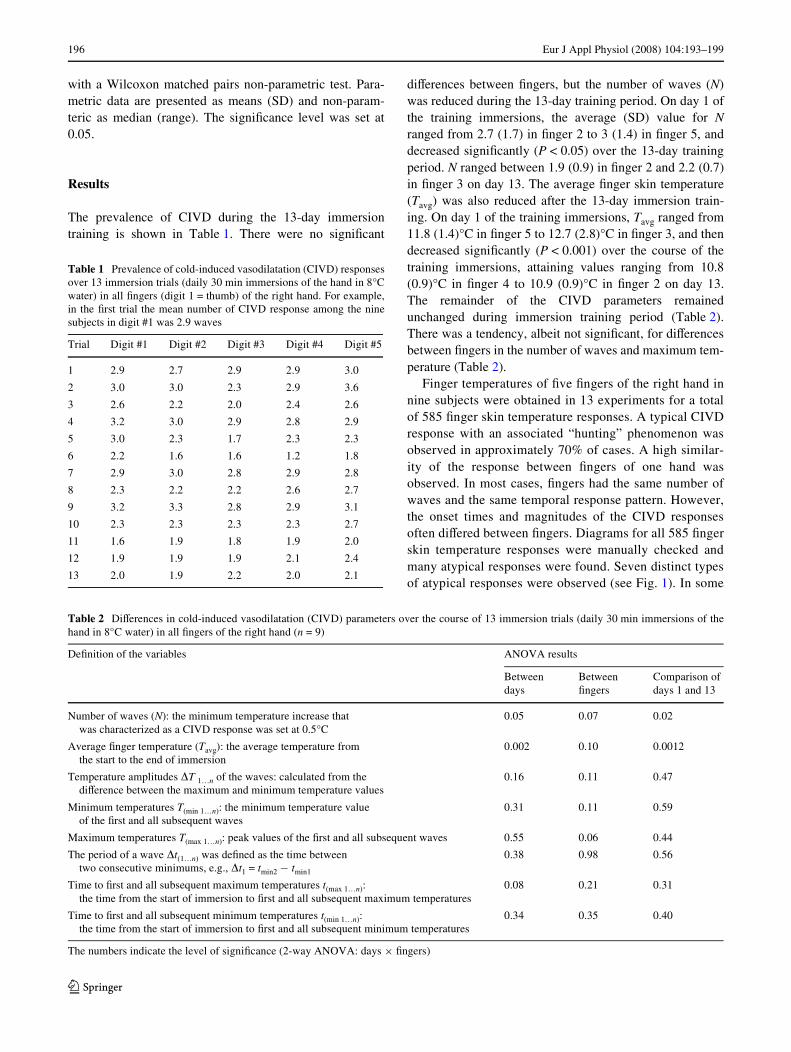
Finger temperatures of Wve Wngers of the right hand innine subjects were obtained in 13 experiments for a totalof 585 Wnger skin temperature responses. A typical CIVDresponse with an associated “hunting” phenomenon wasobserved in approximately 70% of cases. A high similar-ity of the response between Wngers of one hand wasobserved. In most cases, Wngers had the same number ofwaves and the same temporal response pattern. However,the onset times and magnitudes of the CIVD responsesoften diVered between Wngers. Diagrams for all 585 Wngerskin temperature responses were manually checked andmany atypical responses were found. Seven distinct typesof atypical responses were observed (see Fig. 1). In some
Table 1 Prevalence of cold-induced vasodilatation (CIVD) responsesover 13 immersion trials (daily 30 min immersions of the hand in 8°Cwater) in all Wngers (digit 1 = thumb) of the right hand. For example,in the Wrst trial the mean number of CIVD response among the ninesubjects in digit #1 was 2.9 waves
Trial Digit #1 Digit #2 Digit #3 Digit #4 Digit #5
1 2.9 2.7 2.9 2.9 3.0
2 3.0 3.0 2.3 2.9 3.6
3 2.6 2.2 2.0 2.4 2.6
4 3.2 3.0 2.9 2.8 2.9
5 3.0 2.3 1.7 2.3 2.3
6 2.2 1.6 1.6 1.2 1.8
7 2.9 3.0 2.8 2.9 2.8
8 2.3 2.2 2.2 2.6 2.7
9 3.2 3.3 2.8 2.9 3.1
10 2.3 2.3 2.3 2.3 2.7
11 1.6 1.9 1.8 1.9 2.0
12 1.9 1.9 1.9 2.1 2.4
13 2.0 1.9 2.2 2.0 2.1
Table 2 DiVerences in cold-induced vasodilatation (CIVD) parameters over the course of 13 immersion trials (daily 30 min immersions of thehand in 8°C water) in all Wngers of the right hand (n = 9)
The numbers indicate the level of signiWcance (2-way ANOVA: days £ Wngers)
DeWnition of the variables ANOVA results
Between days
Between Wngers
Comparison of days 1 and 13
Number of waves (N): the minimum temperature increase that was characterized as a CIVD response was set at 0.5°C
0.05 0.07 0.02
Average Wnger temperature (Tavg): the average temperature from the start to the end of immersion
0.002 0.10 0.0012
Temperature amplitudes �T 1…n of the waves: calculated from the diVerence between the maximum and minimum temperature values
0.16 0.11 0.47
Minimum temperatures T(min 1…n): the minimum temperature value of the Wrst and all subsequent waves
0.31 0.11 0.59
Maximum temperatures T(max 1…n): peak values of the Wrst and all subsequent waves 0.55 0.06 0.44
The period of a wave �t(1…n) was deWned as the time between two consecutive minimums, e.g., �t1 = tmin2 ¡ tmin1
0.38 0.98 0.56
Time to Wrst and all subsequent maximum temperatures t(max 1…n): the time from the start of immersion to Wrst and all subsequent maximum temperatures
0.08 0.21 0.31
Time to Wrst and all subsequent minimum temperatures t(min 1…n): the time from the start of immersion to Wrst and all subsequent minimum temperatures
0.34 0.35 0.40
123
Eur J Appl Physiol (2008) 104:193–199 197
instances, two or more of these atypical responses wereobserved in diVerent digits during the course of singleimmersion.
The left hand exhibited changes in a number of CIVDparameters pre- and post-acclimation of the right hand.SpeciWcally, the average immersed Wnger temperature wasreduced by »2°C [from 12.6 (1.2) to 10.8 (0.8)°C;P < 0.01] and the minimum temperature by »0.9°C [from9.9 (1.1) to 9.0 (0.5)°C; P < 0.01]. N also decreased signiW-cantly in the left hand from 2.5 to 1.5 (P < 0.01). No signiW-cant diVerences were observed between Wngers of thecontralateral hand during immersion.
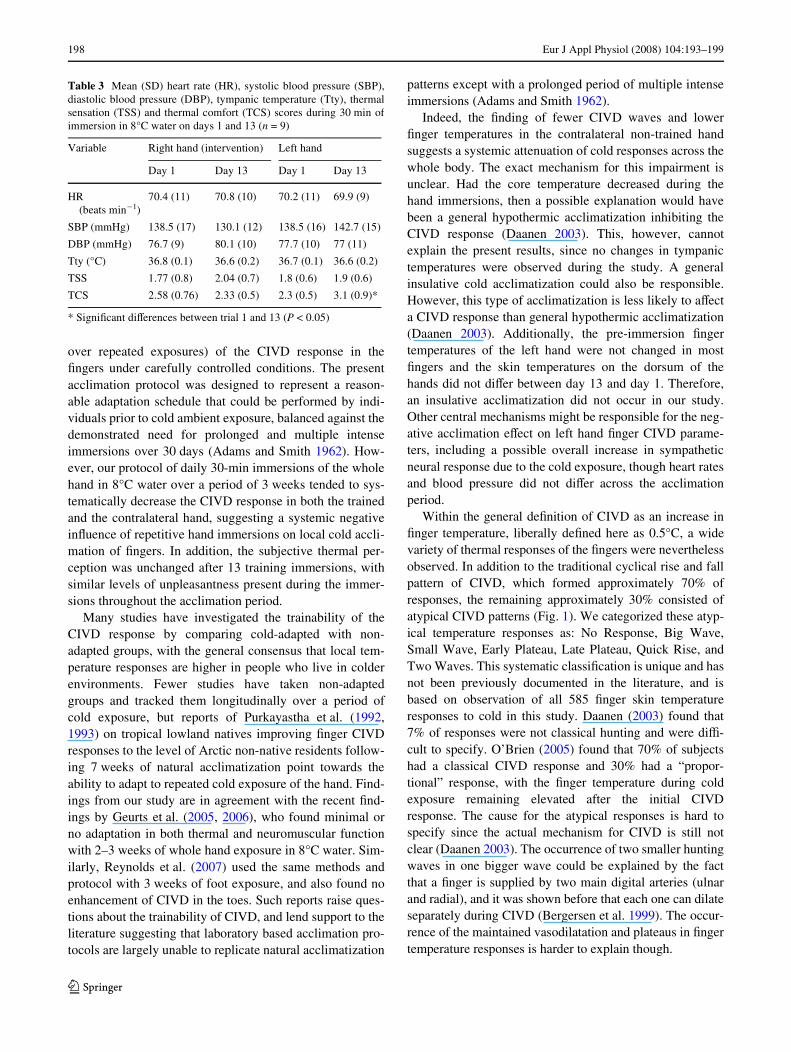
There were no signiWcant diVerences in heart rate, bloodpressure, tympanic temperature and thermal sensationscores between the immersions conducted on days 1 and 13for the right hand, as well as between left and right hands(Table 3). Thermal comfort scores were higher for the lefthand at the end of immersion period.
Discussion
The aim of this study was to investigate the trainability(systematic changes in frequency, onset time, and magnitude
Fig. 1 Typical (a) and atypical (b–h) Wnger skin temperature re-sponses and frequency of occur-rence during cold-water (8°C) immersion derived from 9 sub-jects and 5 Wngers over 13 immersions of the right hand. a Typical: two or more increases >0.5°C during 30 min with an associated “hunting” phenome-non, totaling 70% of all CIVD observations; b No CIVD; c Small wave: a single wave <2°C in amplitude; d Big wave: a sin-gle wave >2°C in amplitude; e Early plateau: a prolonged pla-teau in skin temperature in the Wrst 15 min of immersion; f Late plateau: a prolonged plateau in skin temperature in the latter 15 min of immersion; g Quick Wrst wave: a CIVD wave occur-ring during the initial drop in Wn-ger temperature, typically at Wnger temperature >15°C; h Double wave: a pattern of a second wave initiating before the completion of the Wrst wave. More than one of the atypical patterns may occur within the immersion of a single Wnger, such that the percentages listed in the Wgure exceeds the 30% of total CIVD classiWed as atypical
Tsk (°C) (a) (b)
(c)
(e) (f)
(h)(g)
(d)
Tsk (°C)
5
25
0 30
Typical wave (70% of all cases)
5
25
0 30
No CIVD (1.5% of all cases)
5
25
0 30
Small wave (4% of all cases)
5
25
0 30
Big wave (13.7% of all cases)
5
25
0 30
Early plateau (15.5% of all cases)
5
25
0 30
Late plateau (15.5% of all cases)
5
25
0 30
Quick first wave (8% of all cases)
5
25
0 30
Double wave (15.2% of all cases)
Time (min)
123
198 Eur J Appl Physiol (2008) 104:193–199
over repeated exposures) of the CIVD response in theWngers under carefully controlled conditions. The presentacclimation protocol was designed to represent a reason-able adaptation schedule that could be performed by indi-viduals prior to cold ambient exposure, balanced against thedemonstrated need for prolonged and multiple intenseimmersions over 30 days (Adams and Smith 1962). How-ever, our protocol of daily 30-min immersions of the wholehand in 8°C water over a period of 3 weeks tended to sys-tematically decrease the CIVD response in both the trainedand the contralateral hand, suggesting a systemic negativeinXuence of repetitive hand immersions on local cold accli-mation of Wngers. In addition, the subjective thermal per-ception was unchanged after 13 training immersions, withsimilar levels of unpleasantness present during the immer-sions throughout the acclimation period.
Many studies have investigated the trainability of theCIVD response by comparing cold-adapted with non-adapted groups, with the general consensus that local tem-perature responses are higher in people who live in colderenvironments. Fewer studies have taken non-adaptedgroups and tracked them longitudinally over a period ofcold exposure, but reports of Purkayastha et al. (1992,1993) on tropical lowland natives improving Wnger CIVDresponses to the level of Arctic non-native residents follow-ing 7 weeks of natural acclimatization point towards theability to adapt to repeated cold exposure of the hand. Find-ings from our study are in agreement with the recent Wnd-ings by Geurts et al. (2005, 2006), who found minimal orno adaptation in both thermal and neuromuscular functionwith 2–3 weeks of whole hand exposure in 8°C water. Sim-ilarly, Reynolds et al. (2007) used the same methods andprotocol with 3 weeks of foot exposure, and also found noenhancement of CIVD in the toes. Such reports raise ques-tions about the trainability of CIVD, and lend support to theliterature suggesting that laboratory based acclimation pro-tocols are largely unable to replicate natural acclimatization
patterns except with a prolonged period of multiple intenseimmersions (Adams and Smith 1962).
Indeed, the Wnding of fewer CIVD waves and lowerWnger temperatures in the contralateral non-trained handsuggests a systemic attenuation of cold responses across thewhole body. The exact mechanism for this impairment isunclear. Had the core temperature decreased during thehand immersions, then a possible explanation would havebeen a general hypothermic acclimatization inhibiting theCIVD response (Daanen 2003). This, however, cannotexplain the present results, since no changes in tympanictemperatures were observed during the study. A generalinsulative cold acclimatization could also be responsible.However, this type of acclimatization is less likely to aVecta CIVD response than general hypothermic acclimatization(Daanen 2003). Additionally, the pre-immersion Wngertemperatures of the left hand were not changed in mostWngers and the skin temperatures on the dorsum of thehands did not diVer between day 13 and day 1. Therefore,an insulative acclimatization did not occur in our study.Other central mechanisms might be responsible for the neg-ative acclimation eVect on left hand Wnger CIVD parame-ters, including a possible overall increase in sympatheticneural response due to the cold exposure, though heart ratesand blood pressure did not diVer across the acclimationperiod.
Within the general deWnition of CIVD as an increase inWnger temperature, liberally deWned here as 0.5°C, a widevariety of thermal responses of the Wngers were neverthelessobserved. In addition to the traditional cyclical rise and fallpattern of CIVD, which formed approximately 70% ofresponses, the remaining approximately 30% consisted ofatypical CIVD patterns (Fig. 1). We categorized these atyp-ical temperature responses as: No Response, Big Wave,Small Wave, Early Plateau, Late Plateau, Quick Rise, andTwo Waves. This systematic classiWcation is unique and hasnot been previously documented in the literature, and isbased on observation of all 585 Wnger skin temperatureresponses to cold in this study. Daanen (2003) found that7% of responses were not classical hunting and were diY-cult to specify. O’Brien (2005) found that 70% of subjectshad a classical CIVD response and 30% had a “propor-tional” response, with the Wnger temperature during coldexposure remaining elevated after the initial CIVDresponse. The cause for the atypical responses is hard tospecify since the actual mechanism for CIVD is still notclear (Daanen 2003). The occurrence of two smaller huntingwaves in one bigger wave could be explained by the factthat a Wnger is supplied by two main digital arteries (ulnarand radial), and it was shown before that each one can dilateseparately during CIVD (Bergersen et al. 1999). The occur-rence of the maintained vasodilatation and plateaus in Wngertemperature responses is harder to explain though.
Table 3 Mean (SD) heart rate (HR), systolic blood pressure (SBP),diastolic blood pressure (DBP), tympanic temperature (Tty), thermalsensation (TSS) and thermal comfort (TCS) scores during 30 min ofimmersion in 8°C water on days 1 and 13 (n = 9)
* SigniWcant diVerences between trial 1 and 13 (P < 0.05)
Variable Right hand (intervention) Left hand
Day 1 Day 13 Day 1 Day 13
HR (beats min¡1)
70.4 (11) 70.8 (10) 70.2 (11) 69.9 (9)
SBP (mmHg) 138.5 (17) 130.1 (12) 138.5 (16) 142.7 (15)
DBP (mmHg) 76.7 (9) 80.1 (10) 77.7 (10) 77 (11)
Tty (°C) 36.8 (0.1) 36.6 (0.2) 36.7 (0.1) 36.6 (0.2)
TSS 1.77 (0.8) 2.04 (0.7) 1.8 (0.6) 1.9 (0.6)
TCS 2.58 (0.76) 2.33 (0.5) 2.3 (0.5) 3.1 (0.9)*
123

Eur J Appl Physiol (2008) 104:193–199 199
The synchronicity and spatial homogeneity of the CIVDresponse across the Wngers has recently been questioned(Cheung and Mekjavic 2007). With our immersion proto-col, all Wve Wngers usually showed the same number ofCIVD waves. However, these waves often appeared withslightly variable onset times. In addition, the magnitude ofthe waves in each Wnger also varied randomly since noWnger showed consistently higher or lower values. Overall,these Wndings support the proposed need to obtain multiplethermal measurements in order to model overall thermalresponses of the extremities to cold exposure (Chen et al.1996).
Many diVerent immersion protocols have been utilizedin CIVD studies, and an appropriate protocol to test thetrainability of CIVD must balance the need for suYcientstimulus with subject tolerance and practicality. Our13 days of 30-min immersion was similar in immersionduration (Adams and Smith 1962; Savourey et al. 1996;Yoshimura and Iida 1952) and acclimation length (Geurtset al. 2006) used in other acute or training studies, and itwas not deemed feasible to request that subjects performmultiple immersions each day. It is also recognized that thedegree of thermal stress may inXuence CIVD response.While our use of 8°C water may be less cold than other pro-tocols, average skin temperature throughout the immersionswere always lower than the 15–18°C skin temperaturedeemed necessary to elicit a CIVD response (Lewis 1930).Furthermore, out of 585 potential measurements, there wasno CIVD response only in 1.5% of cases, suggesting a suY-cient intensity of stimulus. Prior pilot work has also estab-lished that hand immersion in <8°C water with non-acclimatized subjects increases the risk of hypotension andfainting, while hand immersion at 8°C can produce consis-tent CIVD responses at the index Wnger in most subjectswith no dropout due to either pain intolerance or hypoten-sion (Geurts et al. 2005).
In conclusion, we suggest that the CIVD in Wngers can-not be trained by a laboratory based acclimation periodusing repetitive immersion of the hand in 8°C water. On thecontrary, a pattern of attenuated local thermal responseswere found in both the trained and the non-trained handafter the acclimation period, suggesting a systemic ratherthan local mechanism of impairment from the repeatedimmersions.
Acknowledgments The authors wish to express their gratitude tothe subjects for their participation. The study was supported, in part, bya Knowledge for Security and Peace grant from the Ministries ofDefence and of Science (Republic of Slovenia).
References
Adams T, Smith RE (1962) EVect of chronic local cold exposure onWnger temperature responses. J Appl Physiol 17:317–322
Bergersen TK, Hisdal J, Walloe L (1999) Perfusion of the human Wn-ger during cold-induced vasodilatation. Am J Physiol 276:R731–R737
Brown GM, Page J (1952) The eVect of chronic exposure to cold ontemperature and blood Xow of the hand. J Appl Physiol 5:221–227
Chen F, Liu ZY, Holmer I (1996) Hand and Wnger skin temperatures inconvective and contact cold exposure. Eur J Appl Physiol OccupPhysiol 72:372–379
Cheung SS, Mekjavic IB (2007) Cold-induced vasodilatation is nothomogenous or generalizable across the hand and feet. Eur J ApplPhysiol 99:701–705
Daanen HA (2003) Finger cold-induced vasodilation: a review. Eur JAppl Physiol 89:411–426
Fox RH, Wyatt HT (1962) Cold-induced vasodilatation in various ar-eas of the body surface of man. J Physiol 162:289–297
Geurts CL, Sleivert GG, Cheung SS (2005) Local cold acclimation ofthe hand impairs thermal responses of the Wnger without improvinghand neuromuscular function. Acta Physiol Scand 183:117–124
Geurts CL, Sleivert GG, Cheung SS (2006) Central and peripheral fac-tors in thermal, neuromuscular, and perceptual adaptation of thehand to repeated cold exposures. Appl Physiol Nutr Metab31:110–117
LeBlanc J, Dulac S, Cote J, Girard B (1975) Autonomic nervous sys-tem and adaptation to cold in man. J Appl Physiol 39:181–186
Lewis T (1930) Observations upon the reactions of the vessels of thehuman skin to cold. Heart 15:177–208
Meehan JP (1955) Individual and racial variations in a vascular re-sponse to a cold stimulus. Mil Med 116:330–334
Miller LK, Irving L (1962) Local reactions to air cooling in an Eskimopopulation. J Appl Physiol 17:449–455
O’Brien C (2005) Reproducibility of the cold-induced vasodilation re-sponse in the human Wnger. J Appl Physiol 98:1334–1340
Paik KS, Kang BS, Han DS, Rennie DW, Hong SK (1972) Vascularresponses of Korean ama to hand immersion in cold water. J ApplPhysiol 32:446–450
Purkayastha SS, Selvamurthy W, Ilavazhagan G (1992) Peripheralvascular response to local cold stress of tropical men during so-journ in the Arctic cold region. Jpn J Physiol 42:877–899
Purkayastha SS, Ilavazhagan G, Ray US, Selvamurthy W (1993) Re-sponses of Arctic and tropical men to a standard cold test andperipheral vascular responses to local cold stress in the Arctic.Aviat Space Environ Med 64:1113–1190
Reynolds LF, Mekjavic IB, Cheung SS (2007) Cold-induced vasodila-tation in the foot is not homogenous or trainable over repeatedcold exposure. Eur J Appl Physiol 102:73–78
Rintamaki H, Hassi J, Smolander J, Louhevaara V, Rissanen S, OksaJ, Laapio H (1993) Responses to whole body and Wnger coolingbefore and after an Antarctic expedition. Eur J Appl Physiol Oc-cup Physiol 67:380–384
Savourey G, Barnavol B, Caravel JP, Feuerstein C, Bittel JH (1996)Hypothermic general cold adaptation induced by local cold accli-mation. Eur J Appl Physiol Occup Physiol 73:237–244
Yoshimura H, Iida T (1952) Studies on the reactivity of skin vessels toextreme cold II. Factors governing the individual diVerence of thereactivity, or the resistance against frostbite. Jpn J Physiol 2:177–185
123
Related Documents











