Ayman Emam et al. 737 Post-Traumatic Epilepsy: Clinical, Neurophysiological and Neuroimaging Study Ayman Emam 1 , Nagia Fahmy 2 , Nagla El-Khayat 2 Departments of Neuroscience, SGHJ, Jeddah, SA 1 ; Neurology, Ain Shams University 2 ABSTRACT Post-traumatic epilepsy (PTE) is a recurrent seizure disorder due to traumatic injury of the brain. There is controversy regarding the precise mechanism by which epilepsy may results from traumatic brain injury. Mesial temporal lobe sclerosis (MTS) is reported as a major risk factor for intractability of posttraumatic epilepsy. We aimed from this work to revise patients with post-traumatic epilepsy, to define risk factors, and assess the clinical, neurophysiological and neuroradiological characteristics. The frequency of mesial temporal epilepsy in contrast to neocortical epilepsy was also assessed in these patients. Twenty- three patients with post-traumatic epilepsy were included in this study. Clinical assessment, video EEG monitoring and MRI brain results were reviewed. We found that 14 patients (60.9%) with neocortical epilepsy (NCE), 8 patients (34.8%) of them had their trauma below or equal to 10 years and 6 patients (26.1%) had their trauma above 10 years old. We found also 8 patients (34.8%) with mesial temporal epilepsy (MTE), 5 patients (21.8%) had their trauma below or equal to 10 years and 3 patients (13%) had their trauma above 10 years. There was one patient (4.3%) with mixed neocorical and mesial temporal epilepsy. Of these patients, 6 had temporal lobectomy with successful post-operative results and the diagnosis of mesial temporal sclerosis was pathologically definite in 5 patients. We concluded that MTS could occur in patients with PTE in young or old ages. Detection of MTS is mandatory for all patients with PTE as resective surgeries of these patients gave a good outcome for the control of their intractable epilepsy. (Egypt J. Neurol. Psychiat. Neurosurg., 2007, 44(2): 737-749) INTRODUCTION Post-traumatic epilepsy (PTE) is defined as recurrent seizure disorder due to injury to the brain following trauma 1 . It is an established consequence of head injury and its incidence is highest among young adults as they are more prone to head injury 2,3 . PTE accounts for 20% of symptomatic epilepsy in the general population and 5% of all epilepsy patients referred to specialized epilepsy centers 3,4 . In military series, the incidence of PTE is much higher (up to 50%), as these studies also include many patients with penetrating head injuries 5 . PTE is classified as immediate seizures (less than 24 hours after injury), early seizures (less than 1 week after injury) and late seizures (more than a week after injury) 6 . The incidence of immediate seizure is 1-4%, early seizures 4-25% and late seizures 9-42% in civilian head injuries 5,7 . Definitions for severity of head injury vary, but one of the most established paradigms is that proposed by Annegers et al., in which head injury is classified as mild, moderate, or severe. Mild injuries are defined by lack of skull fracture and a period of posttraumatic amnesia or loss of consciousness that is 30 minutes or less. Moderate injuries may or may not be associated with skull fractures, but there is a period of 30 minutes to 24 hours of posttraumatic amnesia or loss of consciousness. Severe injuries are characterized by brain contusion, intracranial hematoma, or 24 hours or more of either unconsciousness or posttraumatic amnesia 8 .

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Ayman Emam et al.
737
Post-Traumatic Epilepsy: Clinical, Neurophysiological
and Neuroimaging Study
Ayman Emam1, Nagia Fahmy
2, Nagla El-Khayat
2
Departments of Neuroscience, SGHJ, Jeddah, SA1; Neurology, Ain Shams University
2
ABSTRACT
Post-traumatic epilepsy (PTE) is a recurrent seizure disorder due to traumatic injury of the brain. There is
controversy regarding the precise mechanism by which epilepsy may results from traumatic brain injury. Mesial
temporal lobe sclerosis (MTS) is reported as a major risk factor for intractability of posttraumatic epilepsy. We
aimed from this work to revise patients with post-traumatic epilepsy, to define risk factors, and assess the clinical,
neurophysiological and neuroradiological characteristics. The frequency of mesial temporal epilepsy in contrast
to neocortical epilepsy was also assessed in these patients. Twenty- three patients with post-traumatic epilepsy
were included in this study. Clinical assessment, video EEG monitoring and MRI brain results were reviewed. We
found that 14 patients (60.9%) with neocortical epilepsy (NCE), 8 patients (34.8%) of them had their trauma
below or equal to 10 years and 6 patients (26.1%) had their trauma above 10 years old. We found also 8 patients
(34.8%) with mesial temporal epilepsy (MTE), 5 patients (21.8%) had their trauma below or equal to 10 years and
3 patients (13%) had their trauma above 10 years. There was one patient (4.3%) with mixed neocorical and
mesial temporal epilepsy. Of these patients, 6 had temporal lobectomy with successful post-operative results and
the diagnosis of mesial temporal sclerosis was pathologically definite in 5 patients. We concluded that MTS could
occur in patients with PTE in young or old ages. Detection of MTS is mandatory for all patients with PTE as
resective surgeries of these patients gave a good outcome for the control of their intractable epilepsy. (Egypt J.
Neurol. Psychiat. Neurosurg., 2007, 44(2): 737-749)
INTRODUCTION
Post-traumatic epilepsy (PTE) is defined as
recurrent seizure disorder due to injury to the
brain following trauma1. It is an established
consequence of head injury and its incidence is
highest among young adults as they are more
prone to head injury2,3
. PTE accounts for 20% of
symptomatic epilepsy in the general population
and 5% of all epilepsy patients referred to
specialized epilepsy centers3,4
. In military series,
the incidence of PTE is much higher (up to 50%),
as these studies also include many patients with
penetrating head injuries5.
PTE is classified as immediate seizures (less
than 24 hours after injury), early seizures (less
than 1 week after injury) and late seizures (more
than a week after injury)6. The incidence of
immediate seizure is 1-4%, early seizures 4-25%
and late seizures 9-42% in civilian head injuries5,7
.
Definitions for severity of head injury vary,
but one of the most established paradigms is that
proposed by Annegers et al., in which head injury
is classified as mild, moderate, or severe. Mild
injuries are defined by lack of skull fracture and a
period of posttraumatic amnesia or loss of
consciousness that is 30 minutes or less. Moderate
injuries may or may not be associated with skull
fractures, but there is a period of 30 minutes to 24
hours of posttraumatic amnesia or loss of
consciousness. Severe injuries are characterized
by brain contusion, intracranial hematoma, or 24
hours or more of either unconsciousness or
posttraumatic amnesia8.

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 44 (2) – July 2007
738
It was found in some studies that mesial
temporal lobe epilepsy may result from traumatic
brain injury (TBI) and occurs mainly in young
children, while neocortical epilepsy occurs later in
life. This may be because of the vulnerability of the
developing brain to trauma9,10
. In up to two-thirds
of patients, late post-traumatic seizures are
generalized or focal with secondary generalization,
and often both seizure types may coexist11,12
.
The incidence of subclinical seizure activity
is much higher than that of overt seizures and is
even higher in penetrating brain injuries than in
non-penetrating injuries. In one series, the
reported incidence of combined non-convulsive
seizures and overt seizures was 22%, of these the
incidence of non-convulsive seizures was about
52%.13,14
Much less is known about the characteristics
of TBI, which is associated with increased risk of
seizures. However, certain risk factors have been
consistently identified, placing TBI patients at
significant risk of developing post-traumatic
epilepsy. These risk factors include duration of
loss of consciousness, missile injuries,
intracerebral hemorrhage, diffuse cerebral
contusions, prolonged (3 days) pos-traumatic
amnesia, acute subdural hematoma with surgical
evacuation, early post-traumatic seizures and
depressed skull fracture15,16,17,12
. Brain contusions
and subdural hematomas are the strongest risk
factors for late seizures and this increased risk
persists for up to 20 years2. Individuals with
bilateral or multiple cerebral contusions have
increased risk of developing seizures due to large
amount of tissue destruction12
. Patients with
multiple post-traumatic intracranial surgeries have
also high rates of late PTE12
.
We aimed from this work to revise patients
with post-traumatic epilepsy, to define risk
factors, assess the clinical, neurophysiological and
neuroradiological characteristics. The frequency
of mesial temporal epilepsy in contrast to
neocortical epilepsy was also assessed in these
patients.
PATIENTS AND METHODS
Patients:
They were selected from patients attending
the Epilepsy Unit, Neuroscience Department,
Saudi German hospital Jeddah (SGHJ). Patients
were included if they had moderate or severe head
injury that preceded the onset of epilepsy and was
of sufficient magnitude to result in prolonged loss
of consciousness (30 minutes). Amnesia,
hospitalization or neuroradiologic evidence of
traumatic brain injury12
.
Patients must not have in their past history
other risk factors for epilepsy or family history of
epilepsy.
Clinical assessment:
All patients were subjected for detailed
history and neurological examination. Detailed
history of the head trauma, with revising previous
hospital records of trauma, hospitalization, ICU
admission, surgeries done and onset of seizures.
Semiology of seizures was revised with
family members, attending hospital staff and
prolonged video recordings.
Neurological examination was done and
compared with hospital files at time of trauma.
Anti-epileptic medications, types, doses and
response of patients were revised. Intracranial
surgeries done whether as a management of
traumatic brain injury or as an epilepsy surgery,
were all revised.
Neurophysiological study:
All patients underwent prolonged surface
interictal EEG recording using the international
10-20 system of electrode placement (Machine).
Patients were subjected for continuous video EEG
monitoring for ictal and interictal changes.
Detailed descriptions of seizure semiology and
focus detection were done.
Neuroradiological study:
All patients underwent magnetic resonance
imaging (MRI) of the brain. T1-weighted sagittal

Ayman Emam et al.
739
and gradient echo axial images were obtained. T1-
and T2-weighted and Fluid attenuated inversion
recovery (FLAIR) coronal images were obtained
at a 3mm-slice thickness through the region of
hippocampus. Mesial temporal sclerosis (MTS)
was defined by the finding of hippocampal
atrophy, T2- weighted hyperintensity, or bright
FLAIR signal of hippocampus18
.
Pathological study:
Pathological examination was done for en
bloc resections of either temporal or frontal
lobectomy. Criteria for mesial temporal sclerosis
were identified19
. These criteria consisted of
neuron loss in CA1 and CA4 and the presence of
associated reactive gliosis.
RESULTS
Twenty-three patients were included in the
study. There were twenty males (87%) and three
females (13%) (Graph 1). The mean age was 30.5
years, the youngest was 9 years old and the eldest
was 46 years old. The mean age of trauma was
12.7 years. The youngest age of trauma was 3
months while the eldest age of trauma was 30
years (Table 1).
Patients with their trauma below or equal to
10 years were 13 patients (56.5%), while patients
with their trauma above age of 10 years were 10
patients (43.5%) (Table 1).
The exact time of starting seizures could not
be known of some of the patients as patients had
management of head trauma at different hospitals
with lacking of some information. But we could
differentiate between 2 groups of patients.
Patients had onset of seizures within the first week
(early seizures,16 patients, 69.6%) and patients
with onset of seizures after the first week (late
seizures,7 patients, 30.4%). In the latter group,
time of onset of seizures ranged between 6 months
(patient no. 3) and 13 years (patient no. 23)
(Graph 2).
Patients had five types of head trauma. Road
traffic accident (RTA) in 14 patients (60.9%),
falling from height in 3 patients (13%), falling to
ground in 3 patients (13%), direct blunted head
trauma in 2 patients (8.7%) and firearm injury in
one patient (4.4%) (Graph 3).
The seizure semiology, EEG findings and
MRI results of all patients were summarized in
Table (2).
Mesial temporal epilepsy (MTE) was
diagnosed according to: (1) seizure semiology (2)
Ictal EEG change showing onset in temporal lobes
(3) Radiological evidence of atrophy of
hippocampus and T2 signal shortening on high
resolution MRI or both20,21
. These criteria of MTE
is widely accepted and is correlated
pathologically.20
We found 14 patients (60.9%) with
neocortical Epilepsy (NCE), 8 patients (34.8%) of
them had their trauma below or equal to 10 years
and 6 patients (26.1%) had their trauma above 10
years old. We found also 8 patients (34.8%) with
mesial temporal epilepsy (MTE), 5 patients
(21.8%) had their trauma below or equal to 10
years and 3 patients (13%) had their trauma above
10 years. There was one patient (4.3%) with
mixed neocorical and mesial temporal epilepsy
and he had his trauma above 10 years of age
(patient number 9), (Table 3 and Graph 4).
Six patients had temporal lobectomy and one
patient had frontal lobectomy and another patient
had aspiration of frontal cyst. Surgical outcome
according to Engel‟s classification22
showed
successful results as 3 patients had class 1 (Sizure
free, or few residual auras after withdrawal of
antiepileptic drugs) and 5 patients had class 2
(Rare seizure, fewer than three complex partial
seizures per year) (Table 4).
Pathological results confirmed mesial
temporal sclerosis in five of six patients with
temporal lobectomy (neuron loss in CA1 and CA4
and the presence of associated reactive gliosis).

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 44 (2) – July 2007
740
Table 1. Patient Characteristics, Type of Trauma and Brain Lesion.
Patient
No./Sex/
Age (yrs)
Age of
trauma
(Years)
Type of trauma Type of brain injury
Age of
seizures
(Years)
1/M/20 2 RTA Rt. temporal contusion 2
2/M/34 14 RTA Lt frontal &temporal contusion 14
3/M/25 10 RTA Lt frontal &temporal contusion 10
4/F/19 3 Falling to ground Multiple cerebral contusions 13
5/M/36 7 Falling from height Multiple cerebral contusions 7
6/M/23 5 RTA Bilateral frontal & temporal contusions 5
7/M/35 3 months Falling to ground Bilateral frontal contusions 6
8/M/39 6 RTA Lt. frontal contusion 6
9/M/34 23 RTA Multiple cerebral contusions 23
10/M/24 19 RTA Multiple cerebral contusions 19
11/F/20 8 RTA Multiple cerebral contusions 8
12/M/20 6 RTA Rt. Extradural hematoma, evacuated 6
13/F/9 2.5 Falling from height Multiple cerebral contusions 2.5
14/M/46 21 Direct blunted head trauma Brain concussion, brain edema 21
15/M/39 19 RTA Rt. Intracerebral hemorrhage, operated 19
16/M/35 22 Direct head trauma Rt. Intracerebral hemorrhage 22
17/M/46 6 Falling from height Rt. Parietal contusion 6
18/M/37 17 RTA Fracture skull and spine 18
19/M/37 30 Falling to ground Fracture skull, biparietal contusions 30
20/M/31 8 RTA Bifrontal contusions 8.5
21/M/13 7.5 RTA Bifrontal contusions 8.5
22/M/35 25 Fire arm injury Rt. Occipital injury 28
23/M/45 30 RTA Multiple cerebral contusions 44
( M: Male, F: Female, RTA: Road traffic accident, Rt.: Right, Lt: Left)
females,
3, 13%
Males,
20, 87%
Graph (1): Number of male and female patients.

Ayman Emam et al.
741
Late
seizures; 7;
30%
Early
seizures, 16;
70%
Graph (2): Patients with early and late seizures.
0
10
20
30
40
50
60
70
RTA FFH FTG DT FAI
(RTA: Road traffic accident, FFH: Falling from height, FTG:
Falling to ground, DT: Direct head trauma, FAI: Fire arm injury).
Graph (3): Type of head trauma.
0
1
2
3
4
5
6
7
8
Bel/Equal 10Ys Above 10 ys
MTE
NCE
Mixed
Graph (4): Number of patients with MTE and NCE below and above 10 years of age.

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 44 (2) – July 2007
742
Table 2: Clinical data, EEG findings and MRI results.
Pat.
No. Seizure Semiology EEG Findings MRI Results
Conclusion (Type of
epilepsy)
1 Epigastric aura, Lt. UL
automatism, Rt dystonia
Rt. Temporal slowing Rt. Inferior temporal sclerosis
(Cortical sclerosis)
Rt. Temporal
neocortical
2 Amnesia, Speech arrest,
GTC
Lt. Temporal slowing Lt. Hippocampal sclerosis● Lt. MTE
3 Epigastric aura, Lt. motor
& Lt. adversive, GTC
Rt. Fronto-temporal
epileptic activity
Rt, Fronto-temporal
encephalomalacia
Rt. Fronto-temoral
neocortical
4 Vertigo, Lt. adversive,
GTC
Bilateral temporal
epileptic activity, more Rt.
Rt. Hippocampal atrophy &
sclerosis●
Rt. MTE
5 Expressive dysphasia, Rt.
Motor & adversive, GTC
Left anterior temporal
epileptic activity
Lt. Mesial temoral sclerosis● Lt. MTE
6 Oral automatism, Rt.
Hand dystonia, GTC
Lt. Temoral epileptic
activity
Lt. temporal & bifrontal
encephalomalacia
Lt. Temporal and
Bifrontal neocortical
7 Fear, oral automatism,
GTC
Lt. ant temporal & frontal
epileptic activity
Lt. frontal cyst Lt. Fronto-temoral
neocortical
8 Lt. motor Lt. frontal slowing Lt. frontal cyst Lt. frontal
neocortical
9 Epigastric, Rt. UL
dystonia, GTC
Lt. temporal epileptic
activity
Rt. Frontal encephalomalacia,
Lt. mesial temporal sclerosis●
Rt. Frontal
neocortical & Lt
MTE
10 GTC Rt. Frontal epileptic
activity
Rt. Frontal encephalomalacia Rt. Frontal
neocortical
11 Vertigo, oral automatism,
Rt. Adversive, GTC
Normal Rt. Hippocampal sclerosis● &
cystic lesion
Rt. MTE
12 Lt. Motor & sensory,
GTC
Rt. Anterior temporal
epileptic activity
Rt. Extradural hematoma
(evacuated), Rt. Temporal
sclerosis●
Rt. MTE
13 Attacks of lost
consciousness
Rt. Temporal epileptic
activity
Rt. Mesial temporal sclerosis● Rt. MTE
14 GTC Generalized dysrhythmia Rt. Mesial temporal sclerosis● Rt. MTE
15 Left motor, GTC Rt. Parietal epileptic
activity
Rt. Prietal hematoma
(evacuated)
Rt. Parietal
neocortical
16 Left motor, Rt. dystonia Rt. Fronto-temporal
epileptic activity
Rt. Frontal hematoma
(resolved)
Rt. Frontal
neocortical
17 Lt. adversive, GTC Rt. Post parietal &
occipital epileptic activity
Rt. Parietal encephalomalacia Rt. Parietal
neocortical
18 Chest compression, GTC Rt. Fronto-temporal
epileptic activity
Rt. Frontal gliosis Rt. Frontal
neocortical
19 GTC Lt. Parietal slowing Lt. Parietal encephalomalacia Lt. Parietal
neocortical
20 Rt. Motor, GTC Lt. frontal epileptic
activity
Lt. frontal encephalomalacia Lt. Frontal
neocortical
21 Lt. motor, GTC Rt. Frontal epileptic
activity
Bifrontal encephalomalacia Bifrontal neocortical
22 Vertigo, flashes of light,
GTC
Rt. Occipital epileptic
activity
Rt. Occipito-parietal
encephalomalacia
Rt. Occipito-parietal
neocortical
23 Rt. adversive, post-ictal
confusion, GTC
Lt. temporal epileptic
activity
Lt. Temporal sclerosis● Lt. MTE
(GTC: Generalized tonic-clonic convulsions, Rt: right, Lt: Left, MTE: Mesial temporal epilepsy)

Ayman Emam et al.
743
Table 3. Number of patients with Mesial temporal epilepsy (MTE) & Neocortical epilepsy (NCE).
NCE MTE Mixed NCE &MTE
No. % No. % No. %
Below, equal 10 ys 8 34.8% 5 21.8% --- ---
Above 10 ys 6 26.1% 3 13% 1 4.3%
Total 14 60.9% 8 34.8% 1 4.3%
Table 4. Drug treatment and surgical intervention of all patients.
Patient
No. Drug treatment
Surgical Intervention Outcome after
surgery
(Engel’s class.) Surg. TBI Epilepsy Surg.
1 CBZ, PHT, LTG - Rt. Temporal lobectomy Class 2
2 PHT, CBZ - Lt. Temporal lobectomy Class 1
3 CBZ, VPA, LTG - Rt. Ant. Temporal lobectomy Class 2
4 LTG, CBZ - Rt. Temporal lobectomy Class 1
5 VGT. CBZ, LTG, VPA - Lt. Temporal lobectomy Class 1
6 CBZ, VPA, TPA - Lt. Temporal lobectomy Class 2
7 PHT, VPA, LTG - Drainage of cyst Class 2
8 VPA, CBZ, LTG - Rt. Frontal lobectomy Class 2
9 PHT, TPA, VPA, CBZ - - -
10 CBZ, TPA - - -
11 CBZ, VPA - - -
12 LTG, CBZ, CZM Evacuated Extradural H. - -
13 PHT - - -
14 PHT - - -
15 CBZ, VPA Operated cerebral H. - -
16 VPA, TPA Operated cerebral H. - -
17 CBZ, LMG - - -
18 CBZ, TPA Fixation of fracture spine - -
19 CBZ, PHT - - -
20 LTG - - -
21 CBZ - - -
22 CBZ - - -
23 PHT - - -
(PHT: Phynytoin, CBZ: Carbamazepine, VPA: Valproate, TPA: Topiramate, LTG: Lamotrigine, CZM: Clonazepam,
TBI: Traumatic brain injury, H: Hematoma)

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 44 (2) – July 2007
744
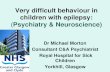
Fig. (1): Patient with Rt. Temporal sclerosis and lobectomy.
Fig. (2): Patient with Lt temporal sclerosis and lobectomy.
Fig. (3): DEEG showed left temporal focus.

Ayman Emam et al.
745
Fig. (4): Patient with Right frontal encephalomalacia
Fig. (5): Patient with right frontal and left temporal encephalomalacia.
Fig. (6): Patient with extensive right parietal encephalomalacia.

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 44 (2) – July 2007
746
Fig. (7): Patient with bilateral frontal encephalomalacia.
DISCUSSION
In this study, we reviewed twenty-three
patients with post-traumatic epilepsy who had
their head trauma at any age.
We found large percentage of male patients
(87%) as compared to female patients (13%) (Graph
1). This could be explained by the large number of
males who are more prone to RTA than females2.
The most common type of head trauma in
our study was RTA (60.9%), followed by falling
from height and falling to ground, each 13% then
direct head trauma 8.7% and fire arm injury, 4.4%
(Graph 3). This showed the magnitude of road
traffic accidents in civilians as a major risk for
post-traumatic epilepsy.
Early seizure were high in our study as we
found 16 patients (70%) with their seizures in the
first week, while only 7 patients (30%) had their
seizures late, even up to 13 years of trauma (Pt.
No. 23) (Graph 3). In some studies the incidence
of immediate seizure was 1-4%, early seizures 4-
25% and late seizures 9-42% in civilian head
injuries5,7
.Other studies showed higher percentage
as our study as they found approximately 80% of
individuals with TBI had their first seizure within
the first 12 months post injury and more than 90%
by the end of the second year23
.Some patients
were followed up to 15 years and found increased
risk especially in penetrating head injuries to
reach 50%2.
Several studies searched for the percentage
of mesial temporal lobe epilepsy and sclerosis in
patients with post-traumatic epilepsy. Many
studies found higher percentage in patients with
head trauma at young age (Below 5 years) and
others found that MTE could occur also in
patients with head trauma occurred at older ages.
In our study, we found 14 patients (60.9%)
with neocortical Epilepsy (NCE), 8 patients
(34.8%) of them had their trauma below or equal
to 10 years and 6 patients (26.1%) had their
trauma above 10 years old. We found also 8
patients (34.8%) with mesial temporal epilepsy
(MTE), 5 patients (21.8%) had their trauma below
or equal to 10 years and 3 patients (13%) had
their trauma above 10 years. There was one
patient (4.3%) with mixed neocorical and mesial
temporal epilepsy and he had his trauma above 10
years of age (patient number 9). So, by addition of
this patient, we had 9 patients with mesial
temporal epilepsy and sclerosis (39.1%)(Table 3,
Graph 4).
Of these patients, 6 had temporal lobectomy
with successful post-operative results and the
diagnosis of mesial temporal sclerosis was
definite in 5 patients (Table 4). Several groups have studied patients who
underwent anterior temporal lobectomy (ATL) as a therapy for refractory epilepsy. Mathern et al.
9,
studied 259 patients who underwent ATL from 1961 to 1992. They found that 26 (10%) of these patients had TBI as a major risk factor and 50%

Ayman Emam et al.
747
of these patients had hippocampal sclerosis. They emphasized also that the mean±SD of these patients was 6.3±1.6 years.
Marks et al.24
described 25 patients with PTE who were examined in Yale University from 1982 to 1992, 21 of whom treated surgically. They found seventeen patients with mesial temporal lobe epilepsy (MTE) and eight with neocortical epilepsy (NCE). Fourteen of the patients with MTE were treated surgically with ATL. Of these, 6 (35%) had hippocampal sclerosis confirmed pathologically and they had excellent postoperative outcomes. Again, these researchers emphasized that all patients with hippocampal sclerosis had their head trauma younger than 5 years (mean age 3.4 years). Patients with NCE were significantly older at time of head trauma (mean age 18.25 years).
Another surgical series describe 102 patients who underwent ATL at the university of Michigan from 1990 to 1996. Twenty-nine (28.4%) had head trauma as a cause, of which, 20 (69%) had hippocampal sclerosis identified pathologically. But this study didn‟t find correlation between MTS and age of head trauma
25.
These earlier reports focused on highly selected patients who were prepared for resective epilepsy surgery.
Our results were compatible with these previous results and one recent retrospective case series, which studied presence of temporal lobe sclerosis in adult patients with intractable epilepsy following TBI. They found that 35% had foci in the mesial temporal lobe while 48% had neocortical foci
10 .So, this supports the findings
that TBI can lead to hippocampal sclerosis in adults as well as in children.
The pathogenesis of temporal lobe sclerosis was studied by many workers. In humans, direct injury to hippocampus from TBI is uncommon. Courville
26, examined the brains of 108 patients
who had fatal TBI and found contusions in the hippocampus in only 11 (10.2%). Other studies have found neuronal loss primarily in CA1 subfield of the hippocampus, which was frequently bilateral. They presumed that hippocampal sclerosis and MTS resulted from diffuse secondary effects of TBI
27,28.
Because of the retrospective nature of these
studies and our study, we can‟t exclude the
possibility that these patients had pre-existing,
clinically silent hippocampal sclerosis, and that
epilepsy was expressed only after injury. This
explanation is unlikely as hippocampal sclerosis is
rare in non-elderly patients who do not have
temporal lobe epilepsy28,29
.It is possible however,
that patients who develop head injury have genetic
predisposition to hippocampal injury.
Epidemiologic support for this possibility is the
studies showed increased family history for
epilepsy in patients with PTE30,31
.
This was studied in animal models for post-
traumatic epilepsy. Several animal studies
documented clear anatomical changes in the
hippocampus and other brain structures together
with increased excitability of specific networks31-37
.
More recent study demonstrated an increase
in the excitability of CA1 pyramidal cells in
response to stimulation, 3 months after fluid
percussion injury in animal models38
.
Other animal models of direct cortical injury
showed epileptiform potentials arising from area
V of cortex39,40
.
More recent work on animal models showed
that following injury, spontaneous partial seizure
originate from the neocortex at site of injury.
Then seizures became chronic and progressive in
course (electrographically and behaviourally). By
follow-up, they found progression of the
phenotype from neocortical (at site of injury) to a
predominance of mesial temporal seizures at later
time points41
.
So, the Importance of our work is that MTS
could occur in patients with head trauma in young
or old ages. Detection of MTS, clinically,
neurophysiologically and radiologically is
mandatory for all patients with PTE as resective
surgeries of these patients gave a good outcome
for the control of their intractable epilepsy. So, we recommend detailed study of patients
with post-traumatic epilepsy, for proper seizure localization and for detection of mesial temporal sclerosis as the source of epileptic activity. Resective surgeries of temporal lobe sclerosis gave successful results for those patients with intractable epilepsy.

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 44 (2) – July 2007
748
REEFRENCES
1. Wrightson P, Gronwall D, 1999: Post-traumatic
epilepsy. In: Mild head injury. London: Oxford
University Press; p. 72-75
2. Annegers JF, Hauser WA, Coan SP, Rocca WA,
1998: A population based study of seizures after
traumatic brain injuries. N Engl J Med; 338:20-24.
3. Annegers JF, Coan SP, 2000: The risks of
epilepsy after traumatic brain injury. Seizure; 9:
453-7.
4. Semah F, Picot M, Adam C, et al, 1998: Is the
underlying cause of epilepsy a major prognostic
factor for recurrence? Neurology; 51: 1256-62.
5. Salazar A, Jabbari B, Vance S, et al, 1985:
Epilepsy after penetrating head injury. I. Clinical
correlates: a report of the Vietnam Head Injury
Study. Neurology; 35: 1406-14.
6. Iudice A, Murri L, 2000: Pharmacological
prophylaxis of posttraumatic epilepsy. Drugs; 59:
1091-9.
7. Asikainen I, Kaste M, Sarna S, 1999: Early and
late posttraumatic seizures in traumatic brain
injury rehabilitation patients: brain injury factors
causing late seizures and influence of seizures on
long-term outcome. Epilepsia; 40: 584-589.
8. Annegers JF, Grabow JD, Groover RV, et al,
1980: Seizures after head trauma: a population
study. Neurology 1980; 30: 683-689.
9. Mathern G, Babb T, Vickrey b, et al, 1994:
Traumatic compared to non-traumatic clinical-
pathologic associations in temporal lobe epilepsy.
Epilepsy Res; 19: 129-39.
10. Diaz-Arrastia R, Agostini MA, Frol AB, et al,
2000: Neurophysiologic and neuroradiologic
features of intractable epilepsy after traumatic brain
injury in adults. Arch Neurol; 57: 1611–1616.
11. Haltiner AM, Temkin NR,Dikmen SS, 1997: Risk
of seizure recurrence after the first late
posttraumatic seizure. Arch Phys Med Rehabil;
78: 835-840.
12. Englander J, Bushnik T,Duong TT, 2003:
Analyzing risk factors for late posttraumatic
seizures: a prospective, multicenter investigation.
Arch Phys Med Rehabil; 84:365–373.
13. Vespa PM, et al, 1999: In creased incidence and
impact of non-convulsive and convulsive seizures
after traumatic brain injury as detected by
continuous electroencephalographic monitoring. J
Neurosurg; 91: 750-60
14. Sarah O, 2004: Review of the role of anticonvulsant prophylaxis folloing brain injury, J Clin Neurosci; 11: 1-3
15. Jennett B, 1975: Epilepsy after non-missile head injuries. Chicago: William Heinmann Medical books.
16. Yablon SA, 1993: Posttraumatic seizures. Arch phys Med Rehabil; 74: 983-1001
17. The Brain Trauma Foundation, The American Association of Neurological Surgeons, The Joint section on Neurotrauma and Critical Care, 2000: Role of Antiseizure prophylaxis following head injury. J Neurotrauma; 17: 549-53.
18. Kuzniecky B and Jackson G, 1995: Magnetic Resonance Imaging in Epilepsy. Raven Press, New York; 107-182.
19. Rushing E, Barnard J, Bigio E, et al, 1997: Frequency of unilateral and bilateral mesial temporal sclerosis in primary and secondary epilepsy. Am J Forensic Med Pathol; 18: 335-341
20. Ajmone-Marsan C, 1993: When are non-invasive tests enough? In: Engel J (ed): Surgical Treatment of the Epilepsies. Raven Press, New York, 2nd ed, 313-318
21. Risinger N, Engel J, van Ness P, et al, 1989: Ictal localoization of temporal lobe seizures with scalp/sphenoidal recordings. Neurology; 39: 1288- 1293.
22. Engel J, van Ness P, Rasmussen T, et al, 1993: Outcome with respect to epileptic seizures. In: engel J (ed): Surgical treatment of epilepsy. Raven press, New York, 2nd ed. 609-621
23. Da Silva A, Vas A, ribeiro I, et al, 1990: controversies in post-traumatic epilepsy. Acta Neurochir suppl; 50: 48-51
24. Marks DA, Kim J, Spencer DD, Spencer SS. Seizure localization and pathology following head injury in patients with uncontrolled epilepsy. Neurology 1995;45:2051–2057.
25. Schuh L, Henry T, Fromes G, et al, 1998: Influence of head trauma on outcome following anterior temporal lobectomy. Arch Neurol; 55: 1325-1328
26. Courville C, 1958: traumatic lesions of the temporal lobe as the causative cause of psychomotor epilepsy. In: Baldwin M, Bailey P (eds): Temporal Lobe Epilepsy. Springfield; 220-239.
27. Kotapka M, Graham D, adams J, et al, 1993: Hippocampal damage in fatal pediatric head injury. Neuropathol Appl Neurobiol; 19: 128-133.
28. Cook M, Fish D, Shorvon S, et al, 1992: Hippocampal volumetric and morphologic studies in frontal and temporal lobe epilepsy. Brain; 115: 1001-1015

Ayman Emam et al.
749
29. Cascino G, Jack C, Parisi E, et al, 1992: MRI in the presurgical evaluation of patients with frontal lobe epilepsy and children with temporal lobe epilepsy: Pathologic correlations and prognostic importance. Epilepsy Res; 11: 51-59
30. Evans JH, 1962: Post-traumatic epilepsy. Neurology; 12: 665-657
31. Caveness WF, 1963: Onset and cessation of fits following craniocerebral trauma. J Neurosurg; 10: 570-582
31. McIntosh TK,Vink R,Noble L, et al, 1989: Traumatic brain injury in the rat: Characterization of a lateral fluid-percussion model. Neuroscience; 28: 233–244.
32. Laurer H and McIntosh T, 1999: Experimental models of brain trauma. Curr Opin Neurol; 12: 715-721.
33. Lowenstein DH, Thomas MJ, Smith DH, et, 1992: Selective vulnerability of dentate hilar neurons following traumatic brain injury: a potential mechanistic link between head trauma and disorders of the hippocampus. J Neurosci; 12: 4846-4853.
34. Coulter DA, Rafiq A, Shumate M, 1996: Brain injury-induced enhanced limbic epileptogenesis: anatomical and physiological parallels to an animal model of temporal lobe epilepsy. Epilepsy Res; 26: 81-91.
35. Toth Z, Hollrigel GS, Gorcs T, et al, 1997: Instantaneous perturbation of interneuronal networks by a pressure wave-transient delivered to the neocortex. J Neurosci;17:8106–8117.
36. Santhakumar V, Bender R, Frotscher M, et al, 2000: Granule cell hyperexcitability in the early posttraumatic rat dentate gyrus: the „irritable mossy cell‟ hypothesis. J Physiol; 524: 117-134.
37. Sloviter RS, 1991: Permanently altered hippocampal structure, excitability, and inhibition after experimental status epilepticus in the rat: the “dormant basket cell” hypothesis and its possible relevance to temporal lobe epilepsy. Hippocampus; 1: 41-66.
38. Santhakumar V, Ratzliff ADH, Jeng J, et al, 2001: Longterm hyperexcitability in the hippocampus after experimental head trauma. Ann Neurol; 50: 708-717.
39. Prince D and Tseng G, 1993: Epileptogenesis in chronically injured cortex: in vitro studies. J Neurophysiol; 69: 1276-1291.
40. Hoffman S, Salin P, Prince D, 1994: Chronic neocortical epileptogenesis in vitro. J Neurophysiol; 71: 1762-1773.
41. D‟Ambrosio R, Fender JS, Fairbanks JP, et al, 2005: Progression from frontal-parietal to mesialtemporal epilepsy after fluid percussion injury in the rat. Brain; 128: 174-188.
ــص العربىخاملل
٫٫
٫
Related Documents