The Body as One Upper Extremity Movement Mechanics By: Fabio Comana, MA., MS. NASM CPT, CES, PES; NSCA CSCS; ACS< HFS: ACE CPT, HC; CISSN NASM Faculty Instructor April 24, 2014 Scapulothroacic Region = Stable Thoracic Spine = Mobile

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
The Body as OneUpper Extremity Movement Mechanics
By: Fabio Comana, MA., MS. NASM CPT, CES, PES; NSCA CSCS; ACS< HFS: ACE CPT, HC; CISSNNASM Faculty Instructor
April 24, 2014
Scapulothroacic Region = Stable
Thoracic Spine = Mobile
What Do You Want to Learn?
Learning Outcomes: • Describe the overall function of the human body in
movement.
• Explain primary components of human movement science.
• Administer and interpret an upper extremity movement screen.
• Implement a simple UE corrective exercise program.
• Instruct proper mechanics for UE movements.
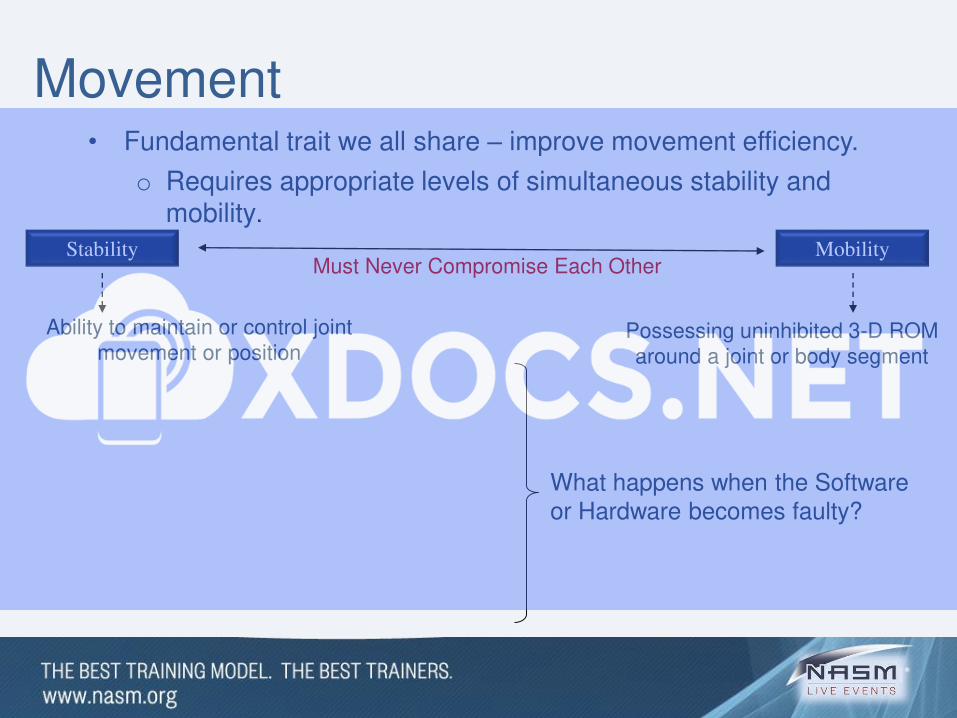
Movement• Fundamental trait we all share – improve movement efficiency.
o Requires appropriate levels of simultaneous stability and mobility.
What happens when the Software or Hardware becomes faulty?
Stability
Ability to maintain or control joint movement or position
Mobility
Possessing uninhibited 3-D ROM around a joint or body segment
Must Never Compromise Each Other
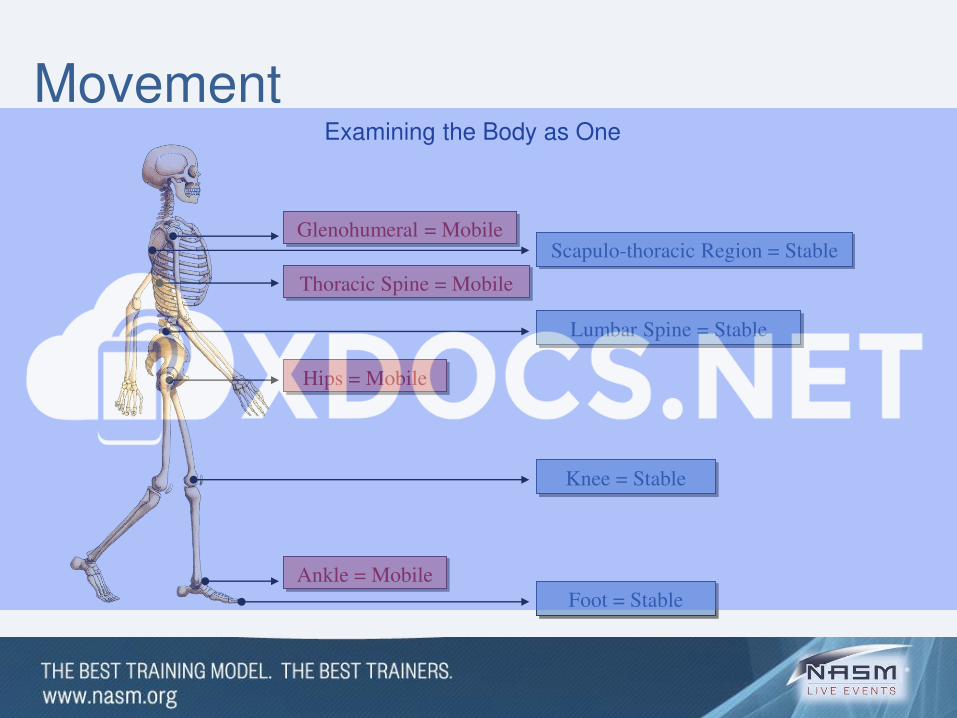
Foot = Stable
Knee = Stable
Lumbar Spine = Stable
Scapulo-thoracic Region = Stable
Ankle = Mobile
Hips = Mobile
Thoracic Spine = Mobile
Glenohumeral = Mobile
Examining the Body as One
Movement
Movement
What Happens if the Body Loses / Lacks this Relationship?
• Step One: Law of Facilitation = ‘Dyskinesis’o Compensation: Compromised stability to facilitate mobility.
o Compensation: Movement into other planes.
Example: Bird-dog
Why?
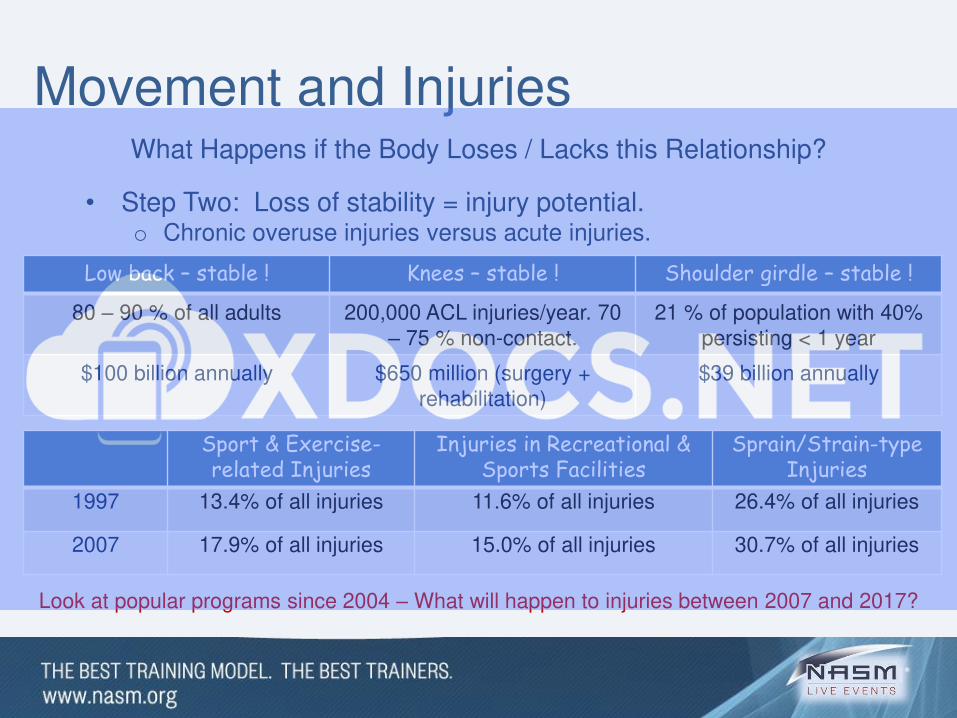
Movement and InjuriesWhat Happens if the Body Loses / Lacks this Relationship?
• Step Two: Loss of stability = injury potential.o Chronic overuse injuries versus acute injuries.
Low back – stable ! Knees – stable ! Shoulder girdle – stable !
80 – 90 % of all adults 200,000 ACL injuries/year. 70 – 75 % non-contact.
21 % of population with 40% persisting < 1 year
$100 billion annually $650 million (surgery + rehabilitation)
$39 billion annually
Sport & Exercise-related Injuries
Injuries in Recreational & Sports Facilities
Sprain/Strain-type Injuries
1997 13.4% of all injuries 11.6% of all injuries 26.4% of all injuries
2007 17.9% of all injuries 15.0% of all injuries 30.7% of all injuries
Look at popular programs since 2004 – What will happen to injuries between 2007 and 2017?
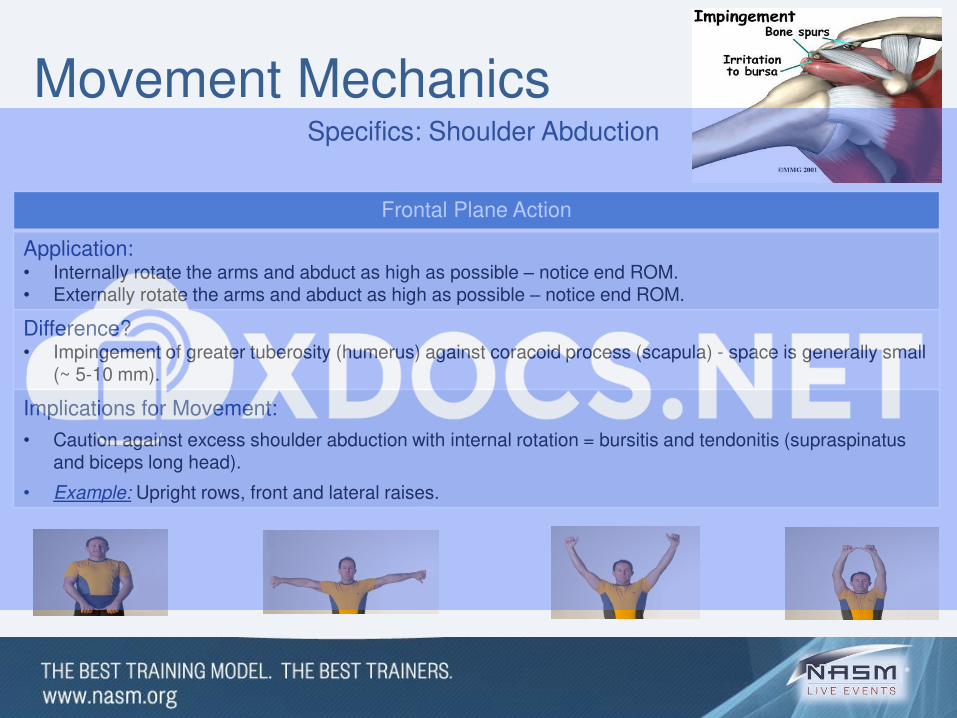
Movement MechanicsSpecifics: Shoulder Abduction
Frontal Plane Action
Application: • Internally rotate the arms and abduct as high as possible – notice end ROM.• Externally rotate the arms and abduct as high as possible – notice end ROM.
Difference?• Impingement of greater tuberosity (humerus) against coracoid process (scapula) - space is generally small
(~ 5-10 mm).
Implications for Movement:
• Caution against excess shoulder abduction with internal rotation = bursitis and tendonitis (supraspinatus and biceps long head).
• Example: Upright rows, front and lateral raises.
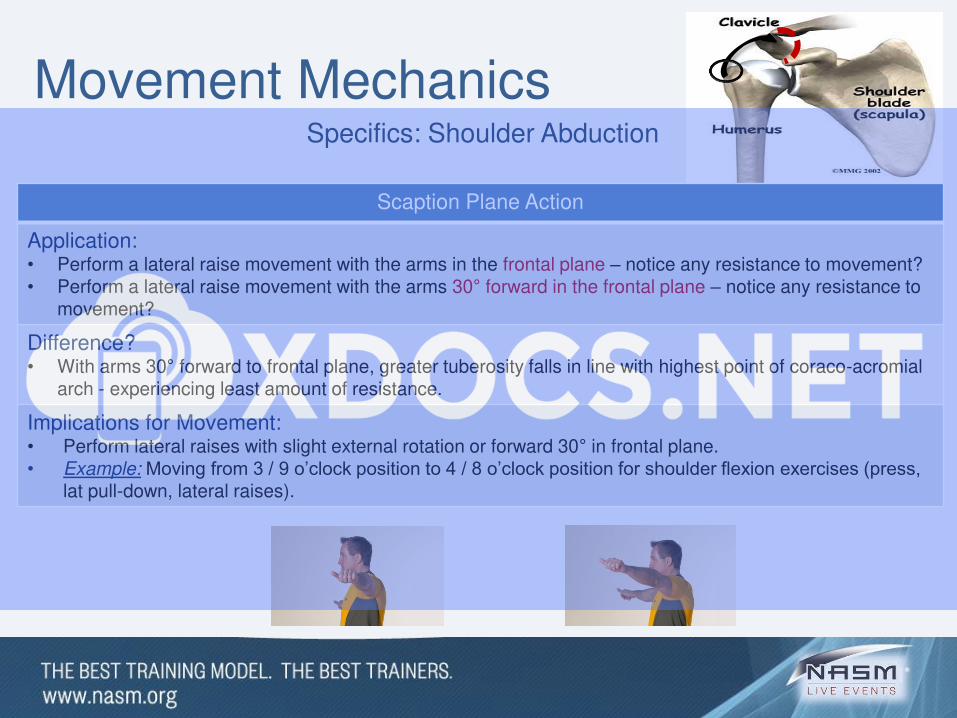
Movement MechanicsSpecifics: Shoulder Abduction
Scaption Plane Action
Application: • Perform a lateral raise movement with the arms in the frontal plane – notice any resistance to movement?• Perform a lateral raise movement with the arms 30° forward in the frontal plane – notice any resistance to
movement?
Difference?• With arms 30° forward to frontal plane, greater tuberosity falls in line with highest point of coraco-acromial
arch - experiencing least amount of resistance.
Implications for Movement: • Perform lateral raises with slight external rotation or forward 30° in frontal plane. • Example: Moving from 3 / 9 o’clock position to 4 / 8 o’clock position for shoulder flexion exercises (press,
lat pull-down, lateral raises).
Movement MechanicsSpecifics: Overhead Press
Frontal Plane Action
Application: • Three heads offer anterior, middle and posterior containment of shoulder (lowered position).• Place index finger and thumb over origin and insertion points of anterior deltoid - perform overhead raise
movement.
Difference?• Observe external rotation of humerus - changes muscle’s orientation. • Arm lowering - no anterior stabilizer to prevent anterior humeral displacement (exacerbated with behind
the head presses).
Implications for Movement: • Overhead positions – External humeral rotation creates no anterior containment beyond passive structures
– need to engage lats as stabilizers.
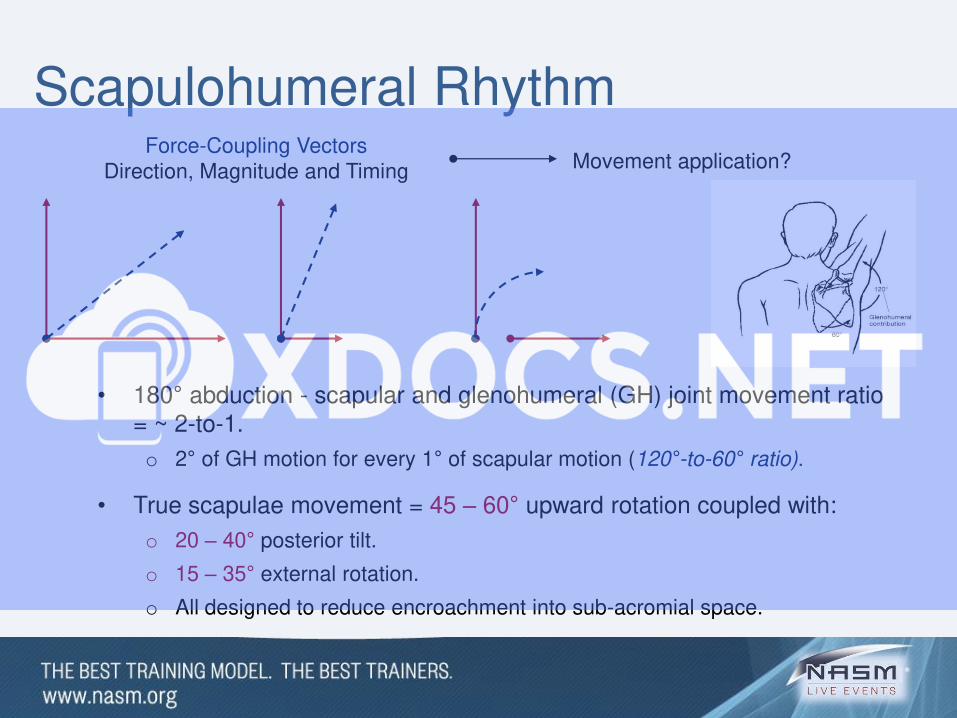
Force-Coupling VectorsDirection, Magnitude and Timing Movement application?
Scapulohumeral Rhythm
• 180° abduction - scapular and glenohumeral (GH) joint movement ratio = ~ 2-to-1.
o 2° of GH motion for every 1° of scapular motion (120°-to-60° ratio).
• True scapulae movement = 45 – 60° upward rotation coupled with:
o 20 – 40° posterior tilt.
o 15 – 35° external rotation.
o All designed to reduce encroachment into sub-acromial space.
Related Documents











