Pediatric TB Meningitis Alex Kay, MD California Department of Public Health Many Faces of TB April 20 th , 2016 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
![Page 1: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/1.jpg)
Pediatric TB Meningitis
Alex Kay, MDCalifornia Department of Public Health
Many Faces of TBApril 20th, 2016
1
![Page 2: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/2.jpg)
2
![Page 3: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/3.jpg)
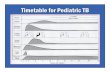
EpidemiologyEpidemiology
• Pediatric TB and TB meningitisPediatric TB and TB meningitis (TBM) are “sentinel events” as markers of recent TBmarkers of recent TB transmission
PPD Conversion
ction
I II III Disseminated (TBM)
Primary Pulmonary
Infec
0 1 2 3 4 5 6 7 8
Marais et al. The natural history of childhood tuberculosis. Int J Tuberc Lung Dis. 2004; 8; 392‐402 3
Months0 1 2 3 4 5 6 7 8
![Page 4: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/4.jpg)
Risk of TBMRisk of TBM
A I f i Ri k f DiAge at Infection Risk of Disease< 1 year Pulmonary disease 30‐40%
TBM or miliary disease 10‐20%
1‐2 years Pulmonary disease 10‐20%1 2 years Pulmonary disease 10 20%TBM or miliary disease 2‐5%
2 years‐adult Pulmonary disease 5%TBM or miliary disease 0.5%
4Marais et al. The natural history of childhood tuberculosis. Int J Tuberc Lung Dis. 2004; 8; 392‐402
![Page 5: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/5.jpg)
5
![Page 6: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/6.jpg)
The Epidemiology ClinicalThe Epidemiology, Clinical Characteristics and Outcomes of Pediatric Central Nervous System TB in California from 1993‐2011TB in California from 1993 2011
![Page 7: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/7.jpg)
Al D Sil MD• Alex Duque‐Silva, MDPediatric Infectious Diseases ClinicianContra Costa County Health Department
• Pennan Barry, MD, MPHChief Surveillance and Epidemiology Sectionp gyCalifornia Department of Public HealthTuberculosis Control BranchTuberculosis Control Branch
7
![Page 8: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/8.jpg)
ObjectivesObjectives1. Identify risk factors for pediatric CNS TB and
death from TB
2. Determine how clinical and demographic factors impact outcome following CNS TBfactors impact outcome following CNS TB
3. Examine the effect of time to treatment on clinical outcome and stage at presentation
8
![Page 9: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/9.jpg)
Pediatric CNS TBPediatric CNS TB• Rates of clinical morbidity (40‐50%) and
li (10 25%) i US di i imortality (10‐25%) in US pediatric series– Largest series are from resource limited settings b hi hl i blbut highly variable
• Poor outcomes associated with–Young age–Advanced clinical stage at presentationAdvanced clinical stage at presentation
Doerr C. et al. Clinical and public health aspects of TB meningitis in children. Jpeds; 1995.p p g p ;Yaramis A. et al. Central Nervous System Tuberculosis in Children: A review of 2016 cases. Pediatrics 1998.van Well G. et al. Twenty Years of Pediatric Tuberculous Meningitis: A retrospective cohort study in the Western Cape of South Africa. Pediatrics; 2009. 9
![Page 10: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/10.jpg)
Pediatric CNS TB in CaliforniaPediatric CNS TB in CaliforniaIncrease proportion of 9%
10%14S
TB
proportion of pediatric CNS disease in 7%
8%
9%
14
14
ic Non
‐CNS
California in 2011
Prompted this4%
5%
6%
19 15
19
12
14
1113
6
8TB
/Ped
iatri
Prompted this large U.S. population based 1%
2%
3%19
7
1215
86
8 7 56
2
iatric CNS T
study of pediatric CNS TB
0%
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
7
Pedi
10
![Page 11: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/11.jpg)
Risk Factors For CNS Tuberculosis1Risk Factors For CNS Tuberculosis1
6,193 pediatric TB 5,993 Cases of
Registry Data
6, 93 pediatric Tcases in California TB Registry 1993‐
2011
Non‐CNS TB TB registry data analysis
200 Cases of CNS 2011TB
1) Identify demographic and clinical factors associated1) Identify demographic and clinical factors associated with pediatric CNS TB
2) Identify features associated with death from TB1Duque‐Silva, A et al. Risk Factors For Central Nervous System Tuberculosis. Pediatrics; 2015. 11
![Page 12: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/12.jpg)
Demographics
Demographic Factors
CNS TBn (%)
Non‐CNS TBn (%)
MultivariateOR (95% CI)( ) ( ) ( )
Age 0‐4 y 144 (72) 2615 (44) 2.6 (1.6‐4.2)
Ethnicity Hispanic
150 (75) 3787 (63) 2.5 (1.0‐6.3)
^ 76% of US born children with CNS TB in 2010‐2011 had at
U.S. birth^ 164 (82) 3482 (58) 1.9 (1.3‐2.9)
76% of US born children with CNS TB in 2010 2011 had at least one foreign born parent
12Duque‐Silva, A et al. Risk Factors For Central Nervous System Tuberculosis. Pediatrics; 2015.
![Page 13: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/13.jpg)
Clinical CharacteristicsClinical Characteristics
CNS TB N (%)
Non‐CNS TB N (%)
MultivariateOR (95% CI)Characteristics ( ) ( ) ( )
TST Positive 105 (61) 5322 (93) 0.1 (0.1‐0.2)( ) ( ) ( )
Culture Positive 118 (59) 1978 (33)( ) ( )
78 % of cultures from CSF and 22% from non‐CSF
13Duque‐Silva, A et al. Risk Factors For Central Nervous System Tuberculosis. Pediatrics; 2015.
![Page 14: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/14.jpg)
Factors Associated with DeathFactors Associated with DeathDied (N = 32)N (%)
Survived (N = 6142) N(%)
MultivariateOR (95% CI)N (%) 6142) N(%) OR (95% CI)
CNS TB 9 (28) 191 (3) 3.8 (1.4‐9.9)CultureCulture Positive 25 (78) 2056 (34) 6.2 (2.2‐17.3)
Factors Associated with SurvivalFactors Associated with SurvivalTST Positive 8 (25) 5418 (88) 0.1 (0.04‐0.02)
Age, gender, ethnicity, country of origin, susceptibilities and receipt of DOT were not associated with death
14Duque‐Silva, A et al. Risk Factors For Central Nervous System Tuberculosis. Pediatrics; 2015.
![Page 15: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/15.jpg)
SummarySummary
• Pediatric CNS TB cases were more likely <5Pediatric CNS TB cases were more likely <5 years, U.S.‐ born and Hispanic
• AFB culture positive and TST negative results i d i h b h CNS TB d d hwere associated with both CNS TB and death
• CNS TB had a 4.5% vs. 0.4% mortality for non‐CNS TB
15
![Page 16: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/16.jpg)
Pediatric CNS TB Chart Review• TB registry data lack information about1. Clinical presentation 2. Outcome 3. Time
to treatment
200 Cases of
151 (76%) cases 92 (61%) with
complete79 (86%) cases with complete
Chart Review
200 Cases of CNS TB reviewed
& 18 LHJ visited
complete outcome
information
with complete date
information
Clinical Features
Time to Treatment A l i
Outcome Analysis
16
Analysis y
![Page 17: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/17.jpg)
CNS TB Cli i l F tCNS TB Clinical Features
0‐4 yrs0 4 yrs
5‐18 yrs
17
![Page 18: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/18.jpg)
Presenting symptoms by age0‐4 yrs 5 ‐ 18 yrs
Presenting symptoms by age
708090100
3040506070
%
0102030
18
![Page 19: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/19.jpg)
Severity at PresentationSeverity at Presentation
Total
MMRC N (%)MMRC III (31 vs. 3%)MMRC I (50 vs. 16%)
100
Stage I 30 (26)50%
Stage II 59 (51)50%
Stage III 26 (23) 0
I II III
19
*MMRC = Modified Medical Research Council
![Page 20: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/20.jpg)
CSF ParametersInitial LP N (%)
Normal 8 (6)Abnormal 125 (94)
CSF ParametersWBC ≥10 cells/µl 115 (92)
Lymphocytes>50% 67 (63) • Protein (70 )
Glucose <40 mg/dl 86 (66)vs. 50%)
Protein >100 mg/dl 85 (64)
Trend (p = 0.09) for normal CSF from an EVD vs LP
20
(p )Marais, S et al. Tuberculous Meningitis; a uniform case definition for use in clinical research. Lancet Infectious Disease, 2010.
![Page 21: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/21.jpg)
Imaging Features
Neuroimaging(MRI CT )
N (%)(MRI or CT scan)
Normal 18 (14)• Normal (24 vs 10%)
Basilar enhancement
75 (58) Normal (24 vs. 10%)
Hydrocephalus 85 (66)
I f t 50 (39) Infarct 50 (39)
Focal lesion 32 (25)
• Hydrocephalus (78 vs. 35%)
• Infarct (47 vs. 19%)
21
Infarct (47 vs. 19%)Marais, S et al. Tuberculous Meningitis; a uniform case definition for use in clinical research. Lancet Infectious Disease, 2010.
![Page 22: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/22.jpg)
Clinical Features
Site of disease N (%)
CNS TB only 90 (69)y ( )Disseminated 39 (30)
Other 1 (0.8)• CNS Only (86 vs 63%)
Culture for Mtb
Positive 88 (58)
• CNS Only (86 vs. 63%)
Negative 63 (41)Susceptibility results
ibl 69 ( 8)• Disseminated TB (37
Pansusceptible 69 (78)INH resistance 4 (4)
MDR 3 (3)
vs. 8%)• Culture + (64 vs. 44%)• Pan susceptible (86 vs.
22
MDR 3 (3)PZA mono‐resistance 10 (11)
p (53%)
![Page 23: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/23.jpg)
TreatmentN (%)
I iti l TB iInitial TB regimen3 drugs (not EMB) 79 (56)≥ 4 CNS drugs 62 (44)≥ 4 CNS drugs 62 (44)
Steroids Yes 106 (70)
• ≥4 drugs 50 vs. 30%• Surgery 57 vs. 21%
No 45 (30)Surgery
EVD/VP h t 70 (46)
g y
EVD/VP shunt 70 (46)Tuberculoma biopsy 7 (5)
23
![Page 24: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/24.jpg)
Predictors of good vs.Predictors of good vs. poor outcomepoor outcome
![Page 25: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/25.jpg)
Measuring post‐treatment outcomesMeasuring post treatment outcomes• Six deficit areas assessed
• Hearing Vision Language Ambulation Development• Hearing, Vision, Language, Ambulation, Development, Focal neurologic deficits
• Developed a standardized protocol for classifying deficits • Cases with information on ≥4 areas included for outcome analysis
• Determination of outcomes• Determination of outcomes• Good: Normal (no deficits) or mild (1 area abnl) clinical sequelae
• Poor: Moderate (2 areas abnl)/Severe clinical sequelae (3 areas abnl or complete deficit in 1) or death
25
![Page 26: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/26.jpg)
Pediatric CNS TB OutcomesPediatric CNS TB Outcomes
Good outcome = 40% Poor outcome = 60%Mild S
Normal20.7%
Mild clinical sequelae19.6%
Moderate clinical sequelae13%
Severe clinical sequelae33.7%
Death13%
N = 37 N = 55
0 20 40 60 80 100%
N = 92N = 92
26
![Page 27: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/27.jpg)
![Page 28: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/28.jpg)
Clinical Severity ScoreClinical Severity Score
Clinical Severity Good Poor Adjusted forClinical Severity Score*
Good Outcome
Poor Outcome
Adjusted for Age
PRR^ (95%CI)( )Stage I 13 (39) 2 (5) Ref
Stage II 17 (52) 23 (52) 1.2 (0.99‐1.5)Stage II 17 (52) 23 (52) 1.2 (0.99 1.5)
Stage III 3 (9) 19 (43) 1.4 (1.1‐1.9)
*MMRC = Modified Medical Research Council^PRR = Prevalence Rate Ratio
28
![Page 29: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/29.jpg)
Clinical Parameters CSF AnalysisI d P t i
NeuroimagingI f ti• Increased Protein
• *PRR 1.2 (1.03‐1.4)• Infarction• *PRR 1.2 (1.04‐1.3)
Cli i l S it AMultivariate
Clinical SeverityMMRC II or III
Age• PRR 1.4 (1.2 – 1.7)
• PRR 1.2 (1.03 – 1.5)
29*Age adjusted
![Page 30: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/30.jpg)
No difference detected in good vs. poor outcome for:poor outcome for:
– Clinical Symptomsy p– MTb culture positive– Susceptibilities– Clinical case definition: definite vs. probable vs. possible– Number of drugs in regimen– Steroid use– Duration of therapySurgical treatment– Surgical treatment
30
![Page 31: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/31.jpg)
Impact of time to treatment on outcome?
21
Symptom onset
1st medical encounter
TB treatment
Post‐treatment onset encounter started outcomes
1. Date of TB treatment – Date of symptom onset2. Date of TB Treatment – Date of 1st medical
encounter 31
![Page 32: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/32.jpg)
Time to TreatmentGood
OutcomePoor
Outcome
Adjusted for Age PRR
1. Sx Onset–TB Rxmedian (days) 16 15 n/a
d ( ) ( )< 10 days 8 (22) 8 (17)≥ 10 days 28 (78) 39 (83) 1.04 (0.9‐1.2)
2. 1st Medical Encounter–TB Rx
median (days) 11 11 n/a7 d 11 (31) 12 (27)< 7 days 11 (31) 12 (27)
≥ 7 days 24 (69) 32 (73) 1.01 (0.9‐1.2)
No association between time from symptom onset to presentation
32
No association between time from symptom onset to presentation and the clinical stage at presentation
![Page 33: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/33.jpg)
1. Early diagnosis remains critical for a good outcome2. No clear linear relationship between time to treatment and
outcome in this analysis
Symptom OnsetGood Outcome
1st Medical EvaluationGood Outcome
I
tage Treatment
II
nical St
I
BM Clin
Poor Outcome
IIITB
33Time
![Page 34: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/34.jpg)
Source Case Identified
Contact
N = 58 (38%) Source CaseContact
Investigation40%
Source Case Investigation57%40% 57%
76% Poor Outcome61% Poor Outcome 76% Poor Outcome
Source Parent 52% Foreign
61% Poor Outcome
case found in home 95%
Relative 40%Other 8%
gBorn 78%
34
95%
![Page 35: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/35.jpg)
LimitationsLimitations
• No pre‐existing validated outcome scaleNo pre existing validated outcome scale• Limited access to pre‐hospitalization records
ff h h d l bl• Difference in group that had outcomes available • Small numbers limited:
– Power to detect differences between outcome groups
–Ability to adjust for confounding variables
35
![Page 36: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/36.jpg)
Summary• Almost 2/3 of pediatric CNS TB cases in California had poor clinical outcomes
• Age and severity of disease at presentation are g y passociated with poor outcome but are not easily amenable to intervention
• Outcomes are better in Stage 1 disease but recognition of early non‐specific CNS TB symptoms is challenging in young infants and with an increasingly rare disease
36
![Page 37: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/37.jpg)
Clinical Interventions For CNS TBClinical Interventions For CNS TB
• Think CNS TB for non‐specific symptoms suchThink CNS TB for non specific symptoms such as fever and vomiting in a young infant with TB exposure or who is high risk for exposureTB exposure or who is high risk for exposure
• Treat empirically based on imaging findings, CSF parameters and the absence of anotherCSF parameters and the absence of another etiologyR b id f CNS TB d• Remember steroids for CNS TB treatment and that TST is only positive in about 50% of CNS TBTB cases
37
![Page 38: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/38.jpg)
Public health focus on TB preventionPublic health focus on TB prevention• Prioritize rapid contact investigations involving children with appropriate treatmentchildren with appropriate treatment
• Emphasize LTBI risk assessment /testing/ treatment for adult caregivers (Cocooning)treatment for adult caregivers (Cocooning)
• Emphasize routine TB risk assessments in infants (2 weeks 6 mo 1 yr annually)infants (2 weeks, 6 mo, 1 yr, annually)
• Consider BCG in communities with high rates of recent TB transmission or for infants withrecent TB transmission or for infants with extended travel to high TB incidence countries
38
![Page 39: Pediatric TB Meningitisnid]/3._kay...Pediatric CNS TB • Rates of clinical morbidity (40‐50%) and mortality (10‐25%) in US pedi idiatric series – Largest series are from resource](https://reader030.cupdf.com/reader030/viewer/2022040511/5e5a59e5dab4cf44ac189b9d/html5/page/39.jpg)
AcknowledgementsAcknowledgements
Alex Duque‐Silva MD Thank You!Alex Duque Silva, MD CDPH Pennan Barry, MD, MPH
Thank You! Varsha Nimbal, MPH Jennifer Flood, MD, MPH Amit Chitnis, MD, MPH, , Neha Shah, MD, MPH Janice Wastenhouse, MPH Saul Kanowitz Saul Kanowitz Gisela Schecter MD, MPH
Infectious Diseases Department at CHRCO
39
Related Documents