TUBERCULOSIS Presentators : Fildzah Yamami Rizal ; Regina Marhadisony Day, Date : Supervisor : dr. Hj. Tiangsa Sembiring, Sp.A(K) Introduction Tuberculosis remains one of the most important causes of death from an infectious disease, and it poses formidable challenges to global health at the public health, scientific, and political level. 1 The urgency of the problem of TB in children, whose full scope is still not fully known, cannot be underestimated. 2 It is estimated that one third of the world’s population is infected with Mycobacterium tuberculosis (the bacterium that causes tuberculosis (TB)), and that each year, about 9 million people develop TB, of whom about 2 million die. Of the 9 million annual TB cases, about 1 million (11%) occur in children (under 15 years of age). Of these childhood cases, 75% occur annually in 22 high-burden countries that together account for 80% of the world’s estimated incident cases. In countries worldwide, the reported 3

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

TUBERCULOSIS
Presentators : Fildzah Yamami Rizal ; Regina Marhadisony
Day, Date :
Supervisor : dr. Hj. Tiangsa Sembiring, Sp.A(K)
Introduction
Tuberculosis remains one of the most important causes of death from an
infectious disease, and it poses formidable challenges to global health at the
public health, scientific, and political level.1 The urgency of the problem of TB in
children, whose full scope is still not fully known, cannot be underestimated.2 It is
estimated that one third of the world’s population is infected with Mycobacterium
tuberculosis (the bacterium that causes tuberculosis (TB)), and that each year,
about 9 million people develop TB, of whom about 2 million die. Of the 9 million
annual TB cases, about 1 million (11%) occur in children (under 15 years of age).
Of these childhood cases, 75% occur annually in 22 high-burden countries that
together account for 80% of the world’s estimated incident cases. In countries
worldwide, the reported percentage of all TB cases occurring in children varies
from 3% to more than 25%.3
Tuberculosis is a direct contagious disease caused by Mycobacterium
tuberculosis. The disease primarily involves the lungs, and at times distant blood-
borne spread results in the development of extrapulmonary TB.1,4 Pediatric
tuberculosis (TB) is different than that in adults in several ways. Children with TB
differ from adults in their immunological and pathophysiological response in
ways that may have important implications for the prevention, diagnosis and
treatment of TB in children.3 The diagnosis of TB is more difficult in children due
to non-specific or complete absence of symptoms and difficulty in confirming the
diagnosis microbiologically. So for making the diagnose for children, need other
criteria with using the scoring system.4,5 Coordination Work Division Unit of
3

Respirology PP IDAI has made National Guideline of Pediatric Tuberculosis with
using scoring system, which giving score for each signs or symptoms found.4
Table 1. TB Scoring System for Child based on Clinical and Supportive
Work-Up4
Parameter 0 1 2 3 Total
TB Contact Not
clear
Family
report, AFB
negative or
not sure,
Acid Fast
Bacilli not
clear
Acid Fast Bacilli
positive
Tuberculin Test negative Positive (≥ 10
mm, or ≥ 5
mm in immune
compromised state
Body
Weight/Nutritional
State
Under red
line on KMS
or BW for
age
< 80%
Poor
nutrition
state
(BW for age
< 60%)
Febrile without
cause
> 2 weeks
Cough ≥3 weeks
Enlargement of
Coli/Axilla/Inguina
l Lymph Node
>1 cm, >1,
No
tenderness
Swollen of hip
/knee/phalang joint
positive
Thorax X-Ray Normal TB
4

or not
clear
suggestive
Total
After taking careful history, physical examination and another work up
such us tuberculin test and chest x-ray, the scoring system can be done. If the
patient got score 6 or more, should be treat as TB patient and get ATT (Anti-
Tuberculosis Therapy). If the score is below 6 but the clinically support for TB,
another work up should be done in indication such us, gastric lavage, pathological
anatomy, lumbal punction, pleural punction, bone and joint x-ray, funduscopy,
CT-Scan and etc.4
In most cases of childhood tuberculosis, 6 months treatment is adequately
enough. After 6 months therapy, evaluation should be performed clinically and
based on laboratory or another supportive examination results. The clinical
evaluation is the best parameter for check the successfulness of the therapy given.4
. The aim of this paper is to report the case of 12
years 4 months old girl with tuberculosis with poor
nutrition and suspect of intra abdominal mass.
Case Report
5

VM, female, 12 years 4 months, came to RSHAM on 1st November 2013
with cough as the main complaint. This happened since 2 months ago and worsen
in the last 5 days. Sputum (+) but can’t be expelled, bloody cough (-). Contact
history with chronic coughing person directly were doubted. Dyspnea was not
found.
History of recurrent fever (+), felt by the patient for the past 5 months. The
fever come especially at night and relieved by anti pyretic drugs. History of
seizure (-), shivering (-)
Enlargement of the abdomen (+) was felt since 5 months ago and getting
bigger since then. At first, there was two mass at the umbilical regio about an egg
size for each. Then, the family brought her to the alternative treatment and get
some poison covered the abdomen. But there’s no improvement, the abdomen
getting bigger and the mass blended with the stomach. This complain
accompanied with intermitten pain, that resolved with analgetics.
Patient also complain for loss of appetite since 3 months ago. The patient
loss some weight since then. But from the start she always malnourished, the
maximum weight that she ever achieved was 30kg, but now she’s only weigh
20kg.
Another complain was swelling at both of the leg and foot. The patient
realized this since 2 weeks ago. At first, it just a fine swelling but get worsen in
these 2 days.
History of birth : normal, assisted by ‘dukun beranak’, cried as soon as
baby was born. Body weight and length was not recorded. History of feeding was
not remembered by patient’s mother. The patient did not receive any
immunization.
Physical Examination
BW : 20kg, BH: 130cm, Arm Circumference : 10cm
BW/Age : 47,6%
BH/Age : 86%
BW/BH : 74%
6

Presens status
Sens : Compos Mentis , Body temperature: 36,8oC, Pulse: 78 bpm, Respiratory
Rate: 24 bpm.
Localized status
1. Head : Flag sign (+) Eye : Light reflexes (+/+), isochoric pupil,
conjunctiva palpebra inferior normal, icteric was not found, ear :
normal appereance, mouth : no sianosis, nose: normal appereance
2. Neck : Lymph node enlargement (+), 1 piece about 5mm
3. Thorax : Symmetrical fusiformis. epigastrial retraction (+). easily seen ribs
HR: 94 bpm, reguler, no murmur. RR: 40 bpm, regular, no
crackles.
4. Abdomen : Symmetrical enlargement. Rigid. liver/spleen/renal : not
palpable. Peristaltic was normal. Tenderness (+) at left hypochondrial regio
5. Extremities : Pulse 94 bpm, regular, adequate pressure and volume, warm
acral, CRT<3”, hypotropy muscle (+) subcutan fat decreasing
(+) pretibial edema (+), pitting edema (+)
Differential Diagnosis
TB + Malnutrition + Susp. Intraabdominal Tumor
Bronchopneumonia + Malnutrition + Susp. Intraabdominal Tumor
Working Diagnosis
TB + Malnutrition + Susp. Intraabdominal Tumor
Treatment
- IVFD D5% NaCl 0,45% 50gtt/i
- Diet F75 80cc/3hours
- Ceftriaxone 200 mg/6 hours/IV
- Gentamycin 50 mg/24 hours/IV
7

Planning
- Complete Blood Count
- Blood glucose
- Electrolyte
- Chest X-Ray
- Mantoux Test
- CT-Scann Upper Lower Abdomen with IV Contrast
8

Follow up
1st November 2013 (First day)
S: Coughing, Shortness of breath
O: Sens: Compos Mentis , Temp: 37oC, Body weight: 20 kg
Head Eye : light reflexes (+/+), isochoric pupil, conjunctiva palpebra inferior
normal, icteric was not found , ear : normal appearance, mouth : no
sianosis, nose: normal appereance.
Thorax Symmetrical fusiform. easily seen ribs. Epigastrial retraction (+) HR: 110
bpm, reguler, no murmur. RR: 45 bpm, regular, no crackles.
Abdomen Enlargement (+) Rigid. peristaltic (+) normal. liver/spleen/renal: not
palpable. Pain on pressure at the left hypochondrium (+).
Extremitie
s
Pulse 100 bpm, regular, adequate pressure and volume, warm acral, CRT
< 3”, Pitting edema (+)
A: DD TB + Malnutrition + Suspect Intra abdominal Tumor
Bronchopneumonia + Malnutrition + Suspect Intra abdominal tumor
P: Management
- IVFD D5 NaCl 0.45% IV, 50 drops/minute micro
- Diet F 75 1500 kkal + 40 g protein
- Ampicilin 1000 mg/12hours/IV
- Gentamycin 1000 mg/24 hours/IV
Plan :
- Complete Blood Count, LFT, AFP, LDH, CRP, SI/TIBC/Ferritin, Blood Cultures,
Urinalysis, Urine Culture Mantoux Test, Sputum BTA test
- Abdominal USG
- Consult to Respirology division
- Consult to Nutrition and metabolic diseases division
- Consult to Hematooncology division
- Consult to Gastro-enterohepatology division
9

Laboratory Result:
November , 1st 2013
Complete Blood Count
Hemoglobin (HGB) g% 6.7 11.3 – 14.1
Eritrosit (RBC) 106/ mm3 2.61 4.40 – 4.48
Leukosit (WBC) 103/ mm3 15.56 4.5- 13.5
Hematokrit % 22.70 37 – 41
Trombosit (PLT) 103/ mm3 442 217 – 497
MCV fL 87.0 81 – 95
MCH Pg 25.7 25 – 29
MCHC g% 29.5 29 – 31
RDW % 19.9 11.6 – 14.8
MPV fL 9.8 7.2 - 10.0
PCT % 0.43
PDW fL 10.4
Diftel
Neutrofil % 91.3 37 – 80
Limfosit % 5.2 20 – 40
Monosit % 3.3 2 – 8
Eosinofil % 0.1 1 – 6
Basofil % 0.1 0 – 1
Neutrofil Absolut 103/µL 14.19 2.4 - 7.3
Limfosit Absolut 103/µL 0.81 1.7 - 5.1
Monosit Absolut 103/µL 0.52 0.2 - 0.6
Eosinofil Absolut 103/µL 0.02 0.10 - 0.30
Basofil Absolut 103/µL 0.02 0 - 0.1
Laboratory Result:
November, 1st 2013
Hemorrhagic Screening Test
10

PT + INR
Prothrombin Time
Control 13.00
Patient 16.6
INR
APTT
Control 33.0
Patient 38.0
Thrombin Time
Control 16.0
Patient 22.2
Clinical Chemistry
Blood Gas Analysis
pH 7.49 7.35-7.45
pCO2 mmHg 23.0 38-42
pO2 mmHg 160.4 85-100
Bikarbonat (HCO3) mmol/L 17.2 22-26
Total CO2 mmol/L 17.9 19-25
Base Excess mmol/L -3.9 (-2) – (+2)
O2 Saturation % 96.8 95-100
Liver Function
Albumin g/dL 1.9 3.8-5.4
Carbohydrate Metabolism
Blood Glucose mg/dL 111.10 <200
Kidney Function
Ureum mg/dL 21.0 <50
Creatinin mg/dL 0.99 0.53-0.79
11

Electrolyte
Natrium (Na) mEq/L 128 135-155
Kalium (K) mEq/L 3.3 3.6-5.5
Klorida (Cl) mEq/L 102 96-106
2nd November (Second Day)
S : Coughing (+), Shortness of breath (+)
O : Sens: Compos Mentis , Temp: 37,2oC, Body weight: 20 kg
Head Eye : light reflexes (+/+), isochoric pupil, conjunctiva palpebra inferior
normal, icteric was not found , ear : normal appearance, mouth : no
sianosis, nose: normal appereance.
Thorax Symmetrical fusiform. easily seen ribs. Epigastrial retraction (+) HR: 100
bpm, reguler, no murmur. RR: 40 bpm, regular, no crackles.
Abdomen Enlargement (+) Rigid. peristaltic (+) normal. liver/spleen/renal: not
palpable. Pain on pressure at the left hypochondrium (+).
Extremitie
s
Pulse 100 bpm, regular, adequate pressure and volume, warm acral, CRT
< 3”, Pitting edema (+)
A: DD TB + Malnutrition + Suspect Intra abdominal Tumor
Bronchopneumonia + Malnutrition + Suspect Intra abdominal tumor
P: Management
- IVFD D5 NaCl 0.45% IV, 50 drops/minute micro
- Diet F 75 1500 kkal + 40 g protein
- Ampicilin 1000 mg/12hours/IV
- Gentamycin 1000 mg/24 hours/IV
Plan :
- Hypoalbumin Correction
Laboratory Result, 2nd November 2013
Anemia Profile
Ferritin ng/mL 299.6 Adult : 15-300
Child : 15-240
12

Iron (Fe) Mg/dL 10 61-157
TIBC µg/dL 95 112-346
Liver Function
Alkali Posphatase
(AFP)
U/L 949 <300
AST/SGOT U/L 74 <32
ALT/SGPT U/L 44 <31
Total Protein g/dL 5.8 6.0-8.0
Albumin g/dL 1.5 3.8-5.4
Globulin g/dL 4.3 2.6-3.6
LDH U/L 636 240-480
Immunoserolgy
Qualitative CRP Positive
Procalcitonin ng/mL 1.97 <0.05
IT Ratio 0.21 <0.2
13

3rd November (Third day)
S: No fever, cough (+), shortness of breath (+)
O: Sens: Compos Mentis , Temp: 37.1oC
Head Eye : light reflexes (+/+), isochoric pupil, conjunctiva palpebra inferior
normal, icteric was not found , ear : normal appearance, mouth : no
sianosis, nose: normal appereance.
Thorax Symmetrical fusiform. easily seen ribs. Epigastrial retraction (+) HR: 92
bpm, reguler, no murmur. RR: 44 bpm, regular, no crackles.
Abdomen Enlargement (+) Rigid. peristaltic (+) normal. liver/spleen/renal: not
palpable. Pain on pressure at the left hypochondrium (+).
Extremitie
s
Pulse 100 bpm, regular, adequate pressure and volume, warm acral, CRT
< 3”, Pitting edema (+)
A: DD TB + Malnutrition + Suspect Intra abdominal Tumor
Bronchopneumonia + Malnutrition + Suspect Intra abdominal tumor
P: Management:
- IVFD D5 NaCl 0.45% IV, 50 drops/minute micro
- Diet F 75 1500 kkal + 40 g protein
- Ampicilin 1000 mg/12hours/IV
- Gentamycin 1000 mg/24 hours/IV
- Albumin correction
Plan :
- Chest X-Ray PA/Lateral
- Blood Culture
- Mantoux Test
- Sputum Test for AFB
14

4th November (fourth day)
S : Fever was not found, Coughing (+)
O : Sens: Compos Mentis, temp: 36.8oC
Head Eye : light reflexes (+/+), isochoric pupil, conjunctiva palpebra inferior
normal, icteric was not found , ear : normal appearance, mouth : no
sianosis, nose: normal appereance.
Thorax Symmetrical fusiform. easily seen ribs. HR: 90 bpm, reguler, no murmur.
RR: 28 bpm, regular, no crackles.
Abdomen Enlargement (+) Rigid. peristaltic (+) normal. liver/spleen/renal: not
palpable. Pain on pressure at the left hypochondrium (+).
Extremitie
s
Pulse 90 bpm, regular, adequate pressure and volume, warm acral, CRT
< 3”, Pitting edema (+)
A: DD TB + Malnutrition + Suspect Intra abdominal Tumor
Bronchopneumonia + Malnutrition + Suspect Intra abdominal tumor
P: Management:
- IVFD D5 NaCl 0.45% IV, 50 drops/minute micro
- Diet F 75 1500 kkal + 40 g protein
- Ampicilin 1000 mg/12hours/IV
- Gentamycin 1000 mg/24 hours/IV
Plan :
- Work Up for Abdominal Mass
- Urin Routine, Feces routine
- Tumor Marker
- Abdominal CT Scan with contrast IV
15

Laboratory Result, 4th November 2013
Tumor Marker
AFP ng/mL 0.61 0-15
Blood β-HCG U/mL 0 0-1
5th November (fifth day)
S : Coughing (+), Fever was not found
O: Sens: Compos Mentis, temp: 36.8oC
Head Eye : light reflexes (+/+), isochoric pupil, conjunctiva palpebra inferior
normal, icteric was not found , ear : normal appearance, mouth : erosion (+)
at the lip mucose, nose: normal appereance.
Thorax Symmetrical fusiform. easily seen ribs. HR: 96 bpm, reguler, no murmur.
RR: 30 bpm, regular, no crackles.
Abdomen Enlargement (+) Rigid. peristaltic (+) normal. liver/spleen/renal: not
palpable. Pain on pressure at the left hypochondrium (+).
Extremitie
s
Pulse 90 bpm, regular, adequate pressure and volume, warm acral, CRT
< 3”, Pitting edema (+)
A: DD TB + Malnutrition + Suspect Intra abdominal Tumor
Bronchopneumonia + Malnutrition + Suspect Intra abdominal tumor
P: Management:
- IVFD D5 NaCl 0.45% IV, 50 drops/minute micro
- Diet F 75 210cc/3hours + mineral mix 4.2cc
- Ampicilin 1000 mg/12hours/IV
- Gentamycin 1000 mg/24 hours/IV
Plan :
- Respirology consult
- Gastric Lavage
- Urine culture
- Wait for the abdominal CT scan to be scheduled
- Wait for the answer from the nutrition division
16

6th November (sixth day)
S : Coughing (+), Shortness of breath (+)
O : Sens : Compos Mentis, Temp : 37.3 oC
Head Eye : light reflexes (+/+), isochoric pupil, conjunctiva palpebra inferior
normal, icteric was not found , ear : normal appearance, mouth : erosion (+)
at the lip mucose, nose: normal appereance.
Thorax Symmetrical fusiform. easily seen ribs. HR: 96 bpm, reguler, no murmur.
RR: 30 bpm, regular, no crackles.
Abdomen Enlargement (+) Rigid. peristaltic (+) normal. liver/spleen/renal: not
palpable. Pain on pressure at the left hypochondrium (+).
Extremitie
s
Pulse 96 bpm, regular, adequate pressure and volume, warm acral, CRT
< 3”, Pitting edema (+)
A : DD TB + Malnutrition + Suspect Intra abdominal Tumor
Bronchopneumonia + Malnutrition + Suspect Intra abdominal tumor
P : Management:
- IVFD D5 NaCl 0.45% IV, 50 drops/minute micro
- Diet F 100 210cc/3hours + mineral mix 4.2cc
- Ampicilin 1000 mg/12hours/IV
- Gentamycin 1000 mg/24 hours/IV
Plan :
- Liver USG
Chest X Ray Result, 6th November 2013 :
Both of costophrenicus sinus are sharp, both of the diaphragm smooth. Infiltration
was seen in both lungs, some of it were consolidated. The heart was normal with
CTR less than 55%. Tarchea was in the middle. Bone and soft tissue were normal.
Radiologic Summary :
Suspect Active Lung TB + Suspect Bronchopneumonia
17

7th November (seventh day)
S: Fever was not found, Coughing (+), Abdominal pain (+)
O: Sens: Compos Mentis, temp: 37oC
Head Eye : light reflexes (+/+), isochoric pupil, conjunctiva palpebra inferior
normal, icteric was not found , ear : normal appearance, mouth : erosion (+)
at the lip mucose, nose: normal appereance.
Thorax Symmetrical fusiform. easily seen ribs. HR: 98 bpm, reguler, no murmur.
RR: 32 bpm, regular, no crackles.
Abdomen Enlargement (+) Rigid. peristaltic (+) normal. Venectation (+)
liver/spleen/renal: not palpable. Pain on pressure at the left hypochondrium
(+).
Extremitie
s
Pulse 98 bpm, regular, adequate pressure and volume, warm acral, CRT
< 3”, Pitting edema (+)
A: DD TB + Malnutrition + Suspect Intra abdominal Tumor
Bronchopneumonia + Malnutrition + Suspect Intra abdominal tumor
P: Management:
- IVFD D5 NaCl 0.45% IV, 50 drops/minute micro
- Diet F 100 210cc/3hours + mineral mix 4.2 cc
- Multivitamin without Fe 1xcth 1
- Ampicilin 1000 mg/12hours/IV
- Gentamycin 1000 mg/24 hours/IV
Plan :
- Repeat Renal Function Test examination
- Urinalysis
- Abdominal CT scan or USG
18

8th November (eighth day)
S: Fever was not found, Abdominal pain (-), pain on pressure (+), Coughing (+)
O: Sens: Compos Mentis, temp: 37.1oC
Head Eye : light reflexes (+/+), isochoric pupil, conjunctiva palpebra inferior
normal, icteric was not found , ear : normal appearance, mouth : erosion (+)
at the lip mucose, nose: normal appereance.
Thorax Symmetrical fusiform. easily seen ribs. HR: 90 bpm, reguler, no murmur.
RR: 26 bpm, regular, no crackles.
Abdomen Enlargement (+) Rigid. peristaltic (+) normal. Venectation (+)
liver/spleen/renal: not palpable. Pain on pressure at the left hypochondrium
(+).
Extremitie
s
Pulse 90 bpm, regular, adequate pressure and volume, warm acral, CRT
< 3”, Pitting edema (+)
A: DD TB + Malnutrition + Suspect Intra abdominal Tumor
Bronchopneumonia + Malnutrition + Suspect Intra abdominal tumor
P: Management:
- IVFD D5 NaCl 0.45% IV, 50 drops/minute micro
- Diet F 100 210cc/3hours + mineral mix 4.2 cc
- Multivitamin without Fe 1xcth 1
- Ampicilin 1000 mg/12hours/IV
- Gentamycin 1000 mg/24 hours/IV
Plan :
- Gastric Lavage
- AP lateral Foto thorax
- Abdominal USG
Mantoux Test Result : Negative
19

9th November (Ninth day)
S: Abdominal pain (+) Heartburn is felt after patient is fed. Vomitting (-).
Coughing (+)
O: Sens: Compos Mentis, temp: 36.8oC
Head Eye : light reflexes (+/+), isochoric pupil, conjunctiva palpebra inferior
normal, icteric was not found , ear : normal appearance, mouth : erosion (+)
at the lip mucose, nose: normal appereance.
Thorax Symmetrical fusiform. easily seen ribs. HR: 90 bpm, reguler, no murmur.
RR: 28 bpm, regular, no crackles.
Abdomen Enlargement (+) Rigid. peristaltic (+) lessen. Venectation (+)
liver/spleen/renal: not palpable. Pain on pressure at the left hypochondrium
(+).
Extremitie
s
Pulse 90 bpm, regular, adequate pressure and volume, warm acral, CRT
< 3”, Pitting edema (+)
A: DD TB + Malnutrition + Suspect Intra abdominal Tumor
Bronchopneumonia + Malnutrition + Suspect Intra abdominal tumor
P: Management:
- IVFD D5 NaCl 0.45% IV, 50 drops/minute micro
- Diet F 100 210cc/3hours + mineral mix 4.2 cc
- Univit 1x1 Cth
- Ampicilin 1000 mg/12hours/IV
- Gentamycin 1000 mg/24 hours/IV
Plan :
- Gastric Lavage
- Lateral foto thorax
Laboratory Result, 9th November 2013 :
Complete Blood Count
Hemoglobin (HGB) g% 6.7 11.3 – 14.1
Eritrosit (RBC) 106/ mm3 2.56 4.40 – 4.48
20

Leukosit (WBC) 103/ mm3 16.61 4.5- 13.5
Hematokrit % 22.6 37 – 41
Trombosit (PLT) 103/ mm3 357 217 – 497
MCV fL 89.1 81 – 95
MCH Pg 26.2 25 – 29
MCHC g% 29.4 29 – 31
RDW % 20.5 11.6 – 14.8
MPV fL 9.7 7.2 - 10.0
PCT % 0.35
PDW fL 10.4
Diftel
Neutrofil % 95.1 37 – 80
Limfosit % 3.2 20 – 40
Monosit % 1.5 2 – 8
Eosinofil % 0.1 1 – 6
Basofil % 0.1 0 – 1
Neutrofil Absolut 103/µL 15.99 2.4 - 7.3
Limfosit Absolut 103/µL 0.54 1.7 - 5.1
Monosit Absolut 103/µL 0.25 0.2 - 0.6
Eosinofil Absolut 103/µL 0.01 0.10 - 0.30
Basofil Absolut 103/µL 0.02 0 - 0.1
Clinical Chemistry
Liver Function
AST/SGOT U/L 58 <32
ALT/SGOT U/L 25 <31
Albumin g/dL 1.6 3.8-5.4
Carbohydrate Metabolism
Blood Glucose mg/dL 86 <200
Renal Function
21

Ureum mg/dL 24.9 <50
Creatinin mg/dL 0.54 0.53-0.79
Uric Acid mg/dL 2.9 <5.7
USG Liver Result, 9th November 2013 :
Size and shape of the liver seems a little bigger, internal echostructural heterogen
elevated. Vena porta wall differentiation slightly dark. Intraabdominal free fluid
collection were seen with floating bowel pattern.
Radiologic Summary :
Mild hepatomegaly with ascites
Suggestion : Abdominal CT Scan with IV Contrast
10th November (Tenth day)
22

S: Abdominal pain (+), Coughing (+)
O: Sens: Compos Mentis, temp: 36.8oC
Head Eye : light reflexes (+/+), isochoric pupil, conjunctiva palpebra inferior
normal, icteric was not found , ear : normal appearance, mouth : erosion (+)
at the lip mucose, nose: normal appereance.
Thorax Symmetrical fusiform. easily seen ribs. HR: 92 bpm, reguler, no murmur.
RR: 32 bpm, regular, no crackles.
Abdomen Enlargement (+) Rigid. peristaltic (+) lessen. Venectation (+)
liver/spleen/renal: not palpable. Pain on pressure at the left hypochondrium
(+).
Extremitie
s
Pulse 92 bpm, regular, adequate pressure and volume, warm acral, CRT
< 3”, Pitting edema (+)
A: DD TB + Malnutrition + Suspect Intra abdominal Tumor + Mild
Hepatomegaly + Ascites
Bronchopneumonia + Malnutrition + Suspect Intra abdominal tumor +
Mild Hepatomegaly + Ascites
P: Management:
- IVFD D5 NaCl 0.45% IV, 50 drops/minute micro
- Diet F 100 210cc/3hours + mineral mix 4.2 cc
- Univit 1x1 Cth
- Ampicilin 1000 mg/12hours/IV
- Gentamycin 1000 mg/24 hours/IV
- Ranitidine 20mg/8hours/IV
- Albumin Correction (2.5-1.6) x 20 x 0.8 = 16 ; Plasbumin 25% = 64cc
11th November (Eleventh day)
S: Cough (+), Shortness of breath (+), Abdominal Pain (+) less than before
O: Sens: Compos Mentis, temp: 36.8oC
23

Head Eye : light reflexes (+/+), isochoric pupil, conjunctiva palpebra inferior
normal, icteric was not found , ear : normal appearance, mouth : erosion (+)
at the lip mucose, nose: normal appereance.
Thorax Symmetrical fusiform. easily seen ribs. HR: 92 bpm, reguler, no murmur.
RR: 32 bpm, regular, no crackles.
Abdomen Enlargement (+) Rigid. peristaltic (+) lessen. Venectation (+)
liver/spleen/renal: not palpable. Pain on pressure at the left hypochondrium
(+).
Extremitie
s
Pulse 92 bpm, regular, adequate pressure and volume, warm acral, CRT
< 3”, Pitting edema (+)
A: DD TB + Malnutrition + Suspect Intra abdominal Tumor + Mild
Hepatomegaly + Ascites
Bronchopneumonia + Malnutrition + Suspect Intra abdominal tumor +
Mild Hepatomegaly + Ascites
P: Management:
- IVFD D5 NaCl 0.45% IV, 50 drops/minute micro
- Diet F 100 210cc/3hours + mineral mix 4.5 cc
- Univit 1x1 Cth
- Ampicilin 1000 mg/12hours/IV
- Gentamycin 1000 mg/24 hours/IV
Plan :
- Waiting for Abdominal CT Scan
Gastric Lavage Result : Negative-Positive-Negative
Urinalysis Result, 11th November 2013 :
Complete Urine Examination
Colour Clear Yellow Yellow
Glucose Negative Negative
Bilirubin Negative Negative
24
Aff, change with Ceftriaxone 1gr/12 hours/IV

Keton Negative Negative
Berat Jenis 1.015 1.005-1.030
pH 6.0 5-8
Protein Negative Negative
Urobilinogen Negative
Nitrit Negative Negative
Blood Negative Negative
Urine Sedimentation
Erythrocyte LPB 0-1 <3
Leucocyte LPB 1-2 <5
Epithel LPB 0-1
Casts LPB Negative Negative
Crystal LPB Negative
12th November (Twelfth day)
S: Cough (+), Shortness of breath (+)
O: Sens: Compos Mentis, temp: 37oC
25

Head Eye : light reflexes (+/+), isochoric pupil, conjunctiva palpebra inferior
normal, icteric was not found , ear : normal appearance, mouth : erosion (+)
at the lip mucose, nose: normal appereance.
Thorax Symmetrical fusiform. easily seen ribs. HR: 96 bpm, reguler, no murmur.
RR: 36 bpm, regular, no crackles.
Abdomen Enlargement (+) Rigid. peristaltic (+) lessen. Venectation (+)
liver/spleen/renal: not palpable. Pain on pressure at the left hypochondrium
(+).
Extremitie
s
Pulse 96 bpm, regular, adequate pressure and volume, warm acral, CRT
< 3”, Pitting edema (+)
A: DD TB + Malnutrition + Suspect Intra abdominal Tumor + Mild
Hepatomegaly + Ascites
Bronchopneumonia + Malnutrition + Suspect Intra abdominal tumor +
Mild Hepatomegaly + Ascites
P: Management:
- IVFD D5 NaCl 0.45% IV, 50 drops/minute micro
- Diet F 100 210cc/3hours + mineral mix 4.5 cc
- Univit 1x1 Cth
- Ceftriaxone 1gr/12hours/IV
Plan :
- Repeat Electrolyte Test
13th November (Thirteenth day)
S: Cough (+), Shortness of breath (+)
O: Sens: Compos Mentis, temp: 37.1oC
26

Head Eye : light reflexes (+/+), isochoric pupil, conjunctiva palpebra inferior
normal, icteric was not found , ear : normal appearance, mouth : erosion (+)
at the lip mucose, nose: normal appereance.
Thorax Symmetrical fusiform. easily seen ribs. HR: 104 bpm, reguler, no murmur.
RR: 40 bpm, regular, no crackles.
Abdomen Enlargement (+) Rigid. peristaltic (+) lessen. Venectation (+)
liver/spleen/renal: not palpable. Pain on pressure at the left hypochondrium
(+).
Extremitie
s
Pulse 96 bpm, regular, adequate pressure and volume, warm acral, CRT
< 3”, Pitting edema (+)
A: DD TB + Malnutrition + Suspect Intra abdominal Tumor + Mild
Hepatomegaly + Ascites
Bronchopneumonia + Malnutrition + Suspect Intra abdominal tumor +
Mild Hepatomegaly + Ascites
P: Management:
- IVFD D5 NaCl 0.45% IV, 50 drops/minute micro
- Diet F 100 210cc/3hours + mineral mix 4.2 cc
- Univit 1x1 Cth
- Ceftriaxone 1gr/12hours/IV
- Rifampisin 1x300mg
- INH 1x200mg
- Pyrazinamide 1x400mg
- Ethambutol 1x400mg
Gastric Lavage Culture Results, 13th November 2013 : Negative
14th November (Fourteenth day)
S: Cough (+), Shortness of breath (+) lessen
O: Sens: Compos Mentis, temp: 36.9oC
27

Head Eye : light reflexes (+/+), isochoric pupil, conjunctiva palpebra inferior
normal, icteric was not found , ear : normal appearance, mouth : erosion (+)
at the lip mucose, nose: normal appereance.
Thorax Symmetrical fusiform. easily seen ribs. HR: 108 bpm, reguler, no murmur.
RR: 30 bpm, regular, no crackles.
Abdomen Enlargement (+) Rigid. peristaltic (+) lessen. Venectation (+)
liver/spleen/renal: not palpable. Pain on pressure at the left hypochondrium
(+).
Extremitie
s
Pulse 108 bpm, regular, adequate pressure and volume, warm acral, CRT
< 3”, Pitting edema (+)
A: DD TB + Malnutrition + Suspect Intra abdominal Tumor + Mild
Hepatomegaly + Ascites
Bronchopneumonia + Malnutrition + Suspect Intra abdominal tumor +
Mild Hepatomegaly + Ascites
P: Management:
- IVFD D5 NaCl 0.45% IV, 50 drops/minute micro
- Diet F 100 210cc/3hours + mineral mix 4.2 cc
- Univit 1x1 Cth
- Ceftriaxone 1gr/12hours/IV
- Rifampisin 1x300mg
- INH 1x200mg
- Pyrazinamide 1x400mg
- Ethambutol 1x400mg
- Vit B6 1x1
Plan :
- Check for Liver Function Test include Albumin
28

Laboratory Result, 14th November 2013 :
Liver Function
AST/SGOT U/L 80 <32
ALT/SGPT U/L 31 <31
Albumin g/dL 1.7 3.8-5.4
Immunodeficiency Profile
Anti HIV (3 methode)
Anti HIV Non Reactive Non Reactive
Anti HIV (Rapid I) Non Reactive Non Reactive
Anti HIV (Rapid II) Non Reactive Non Reactive
CT Scan Whole Abdomen with IV Contrast , 14th November 2013 :
Shape and size of the liver seems enlarge. Regular side, parenchym homogen.
Billiary system and intrahepatic are not wider. Vascular structural are intact.
Ascites were found and there were infiltration on both of the lungs. Shape and
size of the spleen were seems bigger with hipodense multiple lesions.
Pancreas : shape and size are good. Parenchym homogeny.
Kidney : shape and size are good. Regular side. Cortico-meduler differentiation
are clear, no stone were seen. No dilatation of PCS and ureter.
No para-aortal, parailliaca, and bilateral inguinal lymph node enlargement.
Gall Bladder : size and shape are good. Wall is regular.
Vesica Urinaria : size and shape are good. Wall is regular.
The bowel seems distended with thickening of the wall, but the air of the bowell
still seen minimally, pelvic minor projection.
Bone and soft tissue around the wall look good.
Summary :
- Mild splenomegaly with hypodense multiple lesions and hepatomegaly.
- Ascites
- Pneumonia
- Partial Ileus Obstructive
29

- Any other intraabdominal organ are in good conditions
Suggestion : MRI Abdomen
15th November (Fifteenth day)
S: Cough (+), Shortness of breath (+) lessen
O: Sens: Compos Mentis, temp: 37oC
Head Eye : light reflexes (+/+), isochoric pupil, conjunctiva palpebra inferior
normal, icteric was not found , ear : normal appearance, mouth : erosion (+)
at the lip mucose, nose: normal appereance.
Thorax Symmetrical fusiform. easily seen ribs. HR: 110 bpm, reguler, no murmur.
RR: 36 bpm, regular, no crackles.
Abdomen Enlargement (+) Rigid. peristaltic (+) lessen. Venectation (+)
liver/spleen/renal: not palpable. Pain on pressure at the left hypochondrium
(+).
Extremitie
s
Pulse 110 bpm, regular, adequate pressure and volume, warm acral, CRT
< 3”, Pitting edema (+)
A: DD TB + Malnutrition + Suspect Intra abdominal Tumor + Mild
Hepatomegaly + Ascites
Bronchopneumonia + Malnutrition + Suspect Intra abdominal tumor +
Mild Hepatomegaly + Ascites
P: Management:
- IVFD D5 NaCl 0.45% IV, 50 drops/minute micro
- Diet F 100 210cc/3hours + mineral mix 4.2 cc
- Univit 1x1 Cth
- Ceftriaxone 1gr/12hours/IV
- Rifampisin 1x300mg
- INH 1x200mg
- Pyrazinamide 1x400mg
- Ethambutol 1x400mg
- Vit B6 1x1
- Albumin correction : Plasbumin 25% = 100cc
30

16th November (Sixteenth day)
S: Cough (+), Shortness of breath (+) lessen
O: Sens: Compos Mentis, temp: 37.1oC
Head Eye : light reflexes (+/+), isochoric pupil, conjunctiva palpebra inferior
normal, icteric was not found , ear : normal appearance, mouth : erosion (+)
at the lip mucose, nose: normal appereance.
Thorax Symmetrical fusiform. easily seen ribs. HR: 114 bpm, reguler, no murmur.
RR: 36 bpm, regular, no crackles.
Abdomen Enlargement (+) Rigid. peristaltic (+) lessen. Venectation (+)
liver/spleen/renal: not palpable. Pain on pressure at the left hypochondrium
(+).
Extremitie
s
Pulse 114 bpm, regular, adequate pressure and volume, warm acral, CRT
< 3”, Pitting edema (+)
A: DD TB + Malnutrition + Suspect Intra abdominal Tumor + Mild
Hepatomegaly + Ascites
Bronchopneumonia + Malnutrition + Suspect Intra abdominal tumor +
Mild Hepatomegaly + Ascites
P: Management:
- IVFD D5 NaCl 0.45% IV, 50 drops/minute micro
- Diet F 100 210cc/3hours + mineral mix 4.2 cc
- Univit 1x1 Cth
- Ceftriaxone 1gr/12hours/IV
- Rifampisin 1x300mg
- INH 1x200mg
- Pyrazinamide 1x400mg
- Ethambutol 1x400mg
- Vit B6 1x1
- Prednison 2-1-1
Patient PAPS on 16th November 2013 afternoon
31

Discussion
Tuberculosis is a direct contagious disease caused by Mycobacterium
tuberculosis. The disease primarily involves the lungs, most children with TB
have pulmonary TB, and at times distant blood-borne spread results in the
development of extrapulmonary TB.1,3,4 Pediatric tuberculosis (TB) is different
than that in adults in several ways. (1) The diagnosis of TB is more difficult in
children due to non-specific or complete absence of symptoms and difficulty in
confirming the diagnosis microbiologically. (2) Young children suffer more
extrapulmonary and disseminated TB than adults. (3) Treatment of TB in children
is challenging due to the lack of pediatric drug formulations and challenges in
monitoring for toxicity. Fortunately, children generally do very well with
treatment and tolerate the medications well. Treatment regimens are very similar
to those used in adults. Four drug treatment should be initiated for treatment of
presumed active TB if there are any risks of drug resistance in the child or adult
source case (including residence or travel to an area where there is > 4%
resistance to INH). (4) Children should be TB skin tested only if they have risks
for TB infection, are likely to progress to active TB, or are suspected of having
active TB. Unlike adults, all children should be treated for latent TB infection if
identified because the therapy is very safe in young people, they were likely to
have been infected relatively recently, and they have a long time to reactivate their
latent infection. (5) Young children are not contagious with active TB and
acquired their disease from shared airspace with adolescents or adults with
pulmonary TB or ingestion of unpasturized milk products (M. bovis).5
Making the TB diagnosis in children is hard, since it’s always
misdiagnosis for being overdiagnosis or underdiagnosis. In children, cough is not
the main complaint. Sputum collecting also really hard to obtain, so for making
the diagnosis we need a scoring system. Coordination Work Division of
Respirology Unit PP IDAI has made ‘Pedoman Nasional Tuberkulosis Anak’
using scoring system which giving score for each signs and symptoms found. This
guideline were officially use by national program for treating TB for making
diagnosis in children.4 For the criteria of the scoring, look Table 1.
32

After taking careful history, physical examination and another work up
such us tuberculin test and chest x-ray, the scoring system can be done. If the
patient got score 6 or more, should be treat as TB patient and get ATT (Anti-
Tuberculosis Therapy). If the score is below 6 but the clinically support for TB,
another work up should be done in indication such us, gastric lavage, pathological
anatomy, lumbal punction, pleural punction, bone and joint x-ray, funduscopy,
CT-Scan and etc.4 Although bacteriological confirmation of TB is not always
feasible, it should be sought whenever possible, e.g. by sputum microscopy for
children with suspected pulmonary TB who are old enough to produce a sputum
sample. A trial of treatment with anti-TB medications is not recommended as a
method to diagnose TB in children. 3
This patient was admitted to the hospital with coughing as the chief
complaint. Cough may include in the scoring after excluding other cause of
chronic cough as asthma, sinusitis etc.4 From history taking, there were no clear
evidence of the patient being ever contact with TB patient. Mantoux test that have
been done has negative result. Assessment of the nutritional state by using CDC-
NCHS 2000 shown severe malnutrition. The patient also complain about
intermittent fever that felt for about 5 months. There was an enlargement of lymph
node on the coli about 5mm in size on physical examination. And last, the chest x-
ray were suspecting pulmonary TB because of the infiltration shown. Total TB
Score for VM is 6, details are shown on Table 2.
Table 2. TB Scoring System for VM
Parameter 0 1 2 3 Total
TB Contact Not
clear
Family
report, AFB
negative or
not sure,
Acid Fast
Bacilli not
clear
Acid Fast Bacilli
positive
0
Tuberculin Test negative Positive (≥ 10 0
33

mm, or ≥ 5
mm in immune
compromised state
Body
Weight/Nutritional
State
Under red
line on KMS
or BW for
age
< 80%
Poor
nutrition
state
(BW for age
< 60%)
2
Febrile without
cause
> 2 weeks 1
Cough ≥3 weeks 1
Enlargement of
Coli/Axilla/Inguina
l Lymph Node
>1 cm, >1,
No
tenderness
0
Swollen of hip
/knee/phalang joint
positive 0
Thorax X-Ray Normal
or not
clear
TB
suggestive
2
Total 6
With total score of 6, following the reference that said children with score
more than or equal to 6 were diagnosed as TB4, this patient are considered to be
diagnosed by Tuberculosis.
Other than scoring system that been used in Indonesia to diagnose TB in
children, WHO recommend some approach to diagnose TB in children. First,
careful history taking. Contact, just like one point in the Indonesian TB Scoring
System. Close contact is defined as living in the same household as or in frequent
contact with a source case with sputum smear-positive pulmonary TB. Source
cases that are sputum smear-negative but culture-positive are also infectious, but
34

to a much lesser degree.3 This patient has no clear evidence of being contact with
sputum smear-positive pulmonary TB or else.
Then, the symptoms. In most cases, children with symptomatic TB
develop chronic symptoms. The commonest are Chronic cough, an unremitting
cough that is not improving and has been present for more than 21 days. Fever,
body temperature of >38 °C for 14 days, after common causes such as malaria or
pneumonia have been excluded. Weight loss or failure to thrive, in addition to
asking about weight loss or failure to thrive, it is necessary to look at the child's
growth chart.3 This patient has chronic cough that been felt for the past 5 months,
followed by intermittent fever. Since the nutritional state indicate severe
malnutrition and no signs of gaining weight for the past 5 months, may suggest
the third symptoms. Documented weight loss or failure to gain weight, especially
after being treated in a nutritional rehabilitation programme, is a good indicator of
chronic disease in children, of which TB may be the cause.3
Mantoux test or Tuberculin Skin Test (TST) is another recommended
approach for diagnose TB in children. A positive TST occurs when a person is
infected with M. tuberculosis, but does not necessarily indicate disease. However,
the TST can also be used as an adjunct in diagnosing TB in children with signs
and symptoms of TB and when used in conjunction with other diagnostic tests. A
TST should be regarded as positive as follows; in high-risk children (includes
HIV-infected children and severely malnourished children, i.e. those with clinical
evidence of marasmus or kwashiorkor): >5 mm diameter of induration; in all
other children (whether they have received a bacille Calmette–Guérin (BCG)
vaccination or not): >10 mm diameter of induration.3
There can be false-positive as well as false-negative TSTs. Possible causes
for these results are in table 3. Sometimes it is useful to repeat the TST in children
once their nutritional status has improved or their severe illness (including TB)
has resolved, as they may be initially TST negative, but positive after 2–3 months
on treatment. A negative TST never rules out a diagnosis of TB in a child. 3 In this
patient, the TST test shown negative result, this maybe happen because of her
nutritional state that were severe malnourished.3
35

Table 3. Causes of False-Negative and False Positive TST3
Like on adult TB diagnosis, in children, the gold standard for diagnose TB
still bacteriological confirmation, whenever possible. Appropriate specimens from
the suspected sites of involvement should be obtained for microscopy and, where
facilities and resources are available, for culture (and also histopathological
examination). Appropriate clinical samples include sputum, gastric aspirates and
certain other material (e.g. lymph node biopsy or any other material that is
biopsied).3 Because there’s no expectoration from this patient, gastric lavage were
arrange to get some specimens for examinations, but still, there’s no evidence of
acid fast-bacilli.
Chest radiography is useful in the diagnosis of TB in children. In the
majority of cases, children with pulmonary TB have CXR changes suggestive of
TB. In areas with a high prevalence of HIV infection in the general population,
where TB and HIV infection are likely to coexist, HIV counselling and testing is
indicated for all TB patients as part of their routine management.3 This patient
chest X-ray shown suggestive TB as said from consultation from Radiology
Department. And for HIV Testing, this patient had been test for 3-methodes
ELISA and the result are negative.
After the diagnose were obtained, the next step is to treat. The main
objectives of anti-TB treatment are to:
1. cure the patient of TB (by rapidly eliminating most of the bacilli)
36

2. prevent death from active TB or its late effects;
3. prevent relapse of TB (by eliminating the dormant bacilli);
4. prevent the development of drug resistance (by using a combination of
drugs);
5. decrease TB transmission to others
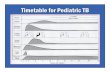
Picture 1. TB Treatment Plot for Children at Basic Health Facility4
The decision to treat a child should be carefully considered and once such
a decision is made, the child should be treated with a full course of therapy.3 Basic
principle of TB treatment is at least 3 kind of drugs and given in 6 months term.
ATT in children were given everyday, on intensive phase and on continuation
phase and the dose were based on the weight of each child.4
Anti-TB treatment is divided into two phases: an intensive phase and a
continuation phase. The purpose of the intensive phase is to rapidly eliminate the
majority of organisms and to prevent the emergence of drug resistance. This phase
uses a greater number of drugs than the continuation phase. The purpose of the
continuation phase is to eradicate the dormant organisms. Fewer drugs are
generally used in this phase because the risk of acquiring drug resistance is low,
37
Score ≥ 6
Give ATT for 2 months and evaluate
Response (+)Response (-)
Continue therapy Continue therapy while looking other cause

as most of the organisms have already been eliminated. In either phase, treatment
can be given daily or three times weekly.3
Table 4. Recommended doses of first-line anti TB drugs
This patient were treated with broad spectrum antibiotic as the working up
for diagnose TB were perform before she received any ATT. As it goes she
received F100 diet with mineral mix for correct her malnourished state. And then
she received RHZE for initial phase, each 300/200/400/400 in dose for initial
phase for 2 months.
In most cases of childhood tuberculosis, 6 months treatment is adequately
enough. After 6 months therapy, evaluation should be performed clinically and
based on laboratory or another supportive examination results. The clinical
evaluation is the best parameter for check the successfulness of the therapy given.
If there any clinical improvement even though radiologically not shown any
significant change, ATT still stopped.4
Prevention for TB was done in high prevalence country including
Indonesia, with BCG vaccination. BCG is a live attenuated vaccine derived from
M. bovis. The WHO Expanded Programme on Immunization recommends BCG
vaccination as soon as possible after birth in countries with a high TB prevalence.
Although BCG has been given to children since the 1920s, controversies about its
effectiveness in preventing TB disease among adults remain. Efficacy ranges from
0% to 80% in published studies from several areas of the world. The reasons for
this variability may be multiple, including different types of BCG used in
different areas, differences in the strains of M. tuberculosis in different regions,
38

different levels of exposure and immunity to environmental mycobacteria and
differences in immunization practices. However, it is generally accepted that after
effective BCG vaccination there is protection against the more severe types of TB
such as miliary TB and TB meningitis, which are most common in young
children.3 This patient never receive any kind of immunization since she were
born, including BCG vaccination.
In countries with a high TB prevalence, the benefits of BCG vaccination
outweigh the risks. In these countries, WHO recommends a policy of routine BCG
immunization for all neonates. A child who has not had routine neonatal BCG
immunization and has symptoms of HIV disease/acquired immunodeficiency
syndrome should not be given BCG because of the risk of disseminated BCG
disease. There is no evidence that revaccination with BCG affords any additional
protection and therefore revaccination is not recommended.3
39

Summary
VM, female, 12 years 4 months was admitted to RS Haji Adam Malik
with the main complaint of cough, fever and enlargement of the abdomen. On
physical examination the patient looks extreme wasting in appereance, easily seen
ribs (+), hypotropy muscle (+) subcutan fat decreasing (+), enlargement, rigidity
and tenderness of the abdomen (+), pitting edema of lower extremities (+).
Laboratory finding shows anemia, leucocytosis and hypoalbuminemia. Physical
examination shows tachipnea but no crackles in both lung, chest X-ray was
performed in the fourth day and the result was : suspect TB and pneumonia.
Mantoux test and gastric lavage were performed to provide diagnosis of
tuberculosis but the result was negative. The patient is treated as severly
malnourished patient with co-morbid of infection. As for the infection, the patient
were assess for TB diagnose using scoring system and the result are 6.
She was diagnosed with TB, malnutrition and susp. intra abdominal tumor
on first admission. While working up for diagnosing the Intraabdominal tumor,
the patient were treated as malnourished TB patient, managed with IVFD D5
NaCl 0.45% 50 drips per minute micro, diet F100 210cc/3hours with mineral mix
4.2cc, Univit 1x1 cth, Ceftriaxone 1gr/12hours/IV, Rifampisin 1x300mg, INH
1x200mg, Pyrazinamide 1x400mg, Ethambutol 1x400mg and Vit B6 1x1.
Unfortunately, the patient was back home as her family request and thought will
be missed her TB treatment and didn’t receive any other work up for her disease.
40

References
1. Diagnosis and Management of Miliary Tuberculosis : Current State and Future
Perspectives. Ray, Sayantan, et al. West Bengal, India : Dove Press Journal,
2013, Therapeutics and Clinical Risk Management.
2. World Health Organization. [Online] 2013. [Cited: November 5, 2013.]
http://www.who.int/tb/challenges/children/en/.
3. —. Guidance for National Tuberculosis Programmes on the Management of
tuberculosis in Children. [Online] 2006. [Cited: November 5, 2013.] WHO/HTM/
TB/2006.371.
4. PEDOMAN NASIONAL PENANGGULANGAN TUBERKULOSIS .
DEPARTEMEN KESEHATAN REPUBLIK INDONESIA. 2006.
5. Pediatric Tuberculosis. Loeffler, Ann M. s.l. : Elsevier, 2003.
41
Related Documents


![Pediatric TB radiographsnid]/05a...1 Pediatric TB radiographs Ann M. Loeffler, MD Curry International Tuberculosis Center Radiology Best quality frontal and lateral views of the chest](https://static.cupdf.com/doc/110x72/609633be3922801af21c02d2/pediatric-tb-radiographs-nid05a-1-pediatric-tb-radiographs-ann-m-loeffler.jpg)


![Treatment of Pediatric TB€¦ · 1/5/2011 6 TB DRUGS IN CHILDREN Aminoglycosides: Mostly CNS, drug-resistant TB Amikacin preferred for CNS [more resistance to streptomycin] OtoOto--](https://static.cupdf.com/doc/110x72/5e94e78ad0de0f234a03c22a/treatment-of-pediatric-tb-152011-6-tb-drugs-in-children-aminoglycosides-mostly.jpg)