PARKINSON DISEASE BY: MARLENE RHODES AMNA ALRAMADHANI MADONA GUIRGIS 03/27/2014

Parkinson Disease
Jan 01, 2016
Parkinson Disease. 03/27/2014. By: Marlene Rhodes Amna Alramadhani Madona Guirgis. Spontaneous motor impulses is an essential facet of control linked to frontal-basal ganglia circuitry. Basal ganglia dysfunction caused by Parkinson’s disease disrupts proficiency. Sings and Symptoms:. - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PARKINSON DISEASE
BY: MARLENE RHODES
AMNA ALRAMADHANI
MADONA GUIRGIS
03/27/2014

Spontaneous motor impulses is an essential facet of control linked to frontal-basal ganglia circuitry. Basal ganglia dysfunction caused by Parkinson’s disease disrupts proficiency.
SINGS AND SYMPTOMS:
•Tremor•Rigidity•Akinesia and Bradykinesia•Postural Instability
Myth/Misconception• Parkinson’s Disease only affects movement,
movement-related (motor) symptoms such as tremor, stiffness and slowness.
Reality• Many symptoms are unrelated to movement.
Nonmotor.

COGNITIVE CHANGES
• One cause is a drop in the level of dopamine, the neurotransmitter that is involved in regulating the body’s movements.

Myth/Misconception• Parkinson’s Disease has spontaneous “exacerbations”
and can “flare up” unexpectedly.
Reality• Although symptoms may fluctuate throughout the
day, the progression of Parkinson’s Disease is very slow.
Instability and falls
Falls occur in 40–70% of patient.
Step training and strength training improve gait characteristic.

Oral Care

ORAL MANIFESTATIONS:• Dysphagia• Salivary dysfunction• Burning mouth• Change in taste and smell• Dry mouth• Difficulty speaking• Angular chelitis
CARIES AND PERIODONTAL DISEASE:• Study investigates the oral health of patients
with PD compared to healthy patients. • Result: patient with Parkinson’s disease has
poorer oral hygiene. • Gingival recession• Mobility• Xerostomia
RECOMMENDATIONS FOR DENTAL APPOINTMENT
• Schedule patient for short appointment between 60-90 minutes.• Calm the patient down.• Semi supine position.• The patient arrive with her/his caregiver for interpretation • Good nutrients that contains vitamin B and iron to treat burning
mouth syndrome.• Place a blanket over patient with comorbid shy-drager disease.
HOW TO MANAGE DENTAL APPOINTMENT:• The use of powered scaling device and air
polishing are NOT recommended.• Use of Bite block and suctioning more often. • No need for antibiotic, consult with physician.• Recall for every 3 -4 months• Apply fluoride varnish every visit.
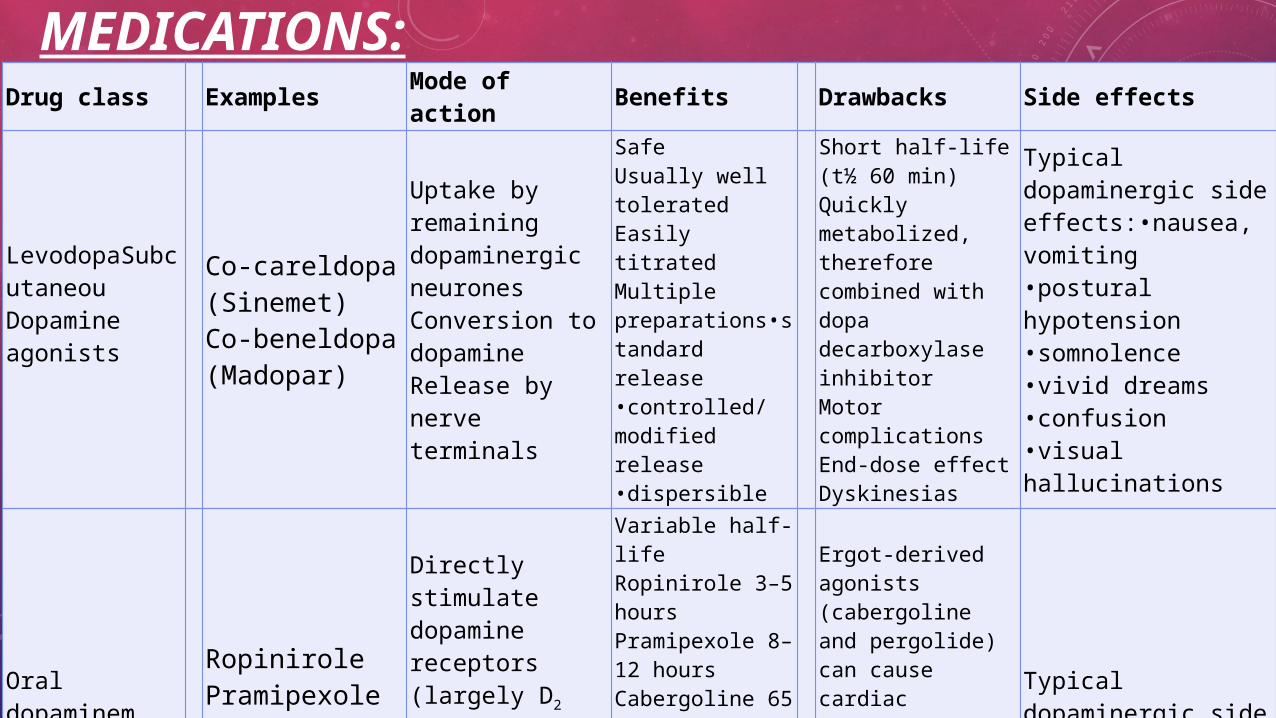
MEDICATIONS:Drug class Examples Mode of action Benefits Drawbacks Side effects
LevodopaSubcutaneou Dopamine agonists
Co-careldopa (Sinemet)Co-beneldopa (Madopar)
Uptake by remaining dopaminergic neuronesConversion to dopamineRelease by nerve terminals
SafeUsually well toleratedEasily titratedMultiple preparations•standard release•controlled/modified release•dispersible
Short half-life (t½ 60 min)Quickly metabolized, therefore combined with dopa decarboxylase inhibitorMotor complicationsEnd-dose effectDyskinesias
Typical dopaminergic side effects:•nausea, vomiting•postural hypotension•somnolence•vivid dreams•confusion•visual hallucinations
Oral dopaminem agonists
RopinirolePramipexoleCabergolinePergolide
Directly stimulate dopamine receptors (largely D2 receptors)Variable affinities for receptor subtypes
Variable half-lifeRopinirole 3–5 hoursPramipexole 8–12 hoursCabergoline 65 hoursLevodopa-sparing therefore fewer motor complications later
Ergot-derived agonists (cabergoline and pergolide) can cause cardiac valvulopathyTroublesome adverse effectsLess well tolerated in the elderly
Typical dopaminergic side effectsa
Transdermal dopamine agonists
Rotigotine Directly stimulate dopamine receptors No tablets needed Less familiar to
patients and doctors
Typical dopaminergic side effectsSkin site reactions
Subcutaneous dopamine agonists
Apomorphine Stimulates D1 and D2 receptors
Useful in patients with distressing dyskinesias and off periodsNo tablets requiredRapid onset
Specialist administration requiredCostlyVery short half-life, therefore prolonged infusion required
Typical dopaminergic side effectsPotently emetogenicSevere skin site reactions

HOW TO OVERCOME XEROSTOMIA:• Sipping water frequently.• Consuming sugar-free hard candies.• Chew on sugar-free xylitol containing gum. • salivary substitutes or pharmaceutical drug
such as pilocarpine and cevimeline HCl.

HOME CARE

THERAPEUTIC AGENTS
1)Toothbrushes2)Floss 3)Mouth rinses4)Fluoride
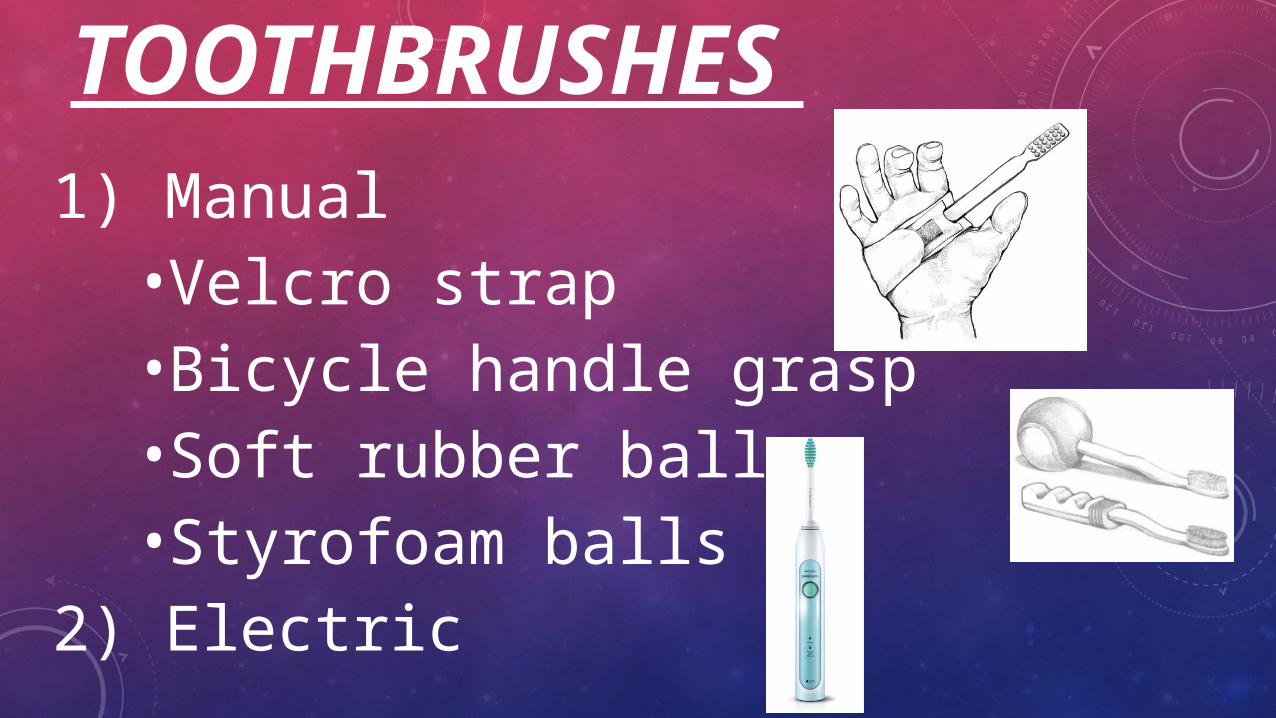
TOOTHBRUSHES 1) Manual
•Velcro strap•Bicycle handle grasp•Soft rubber ball •Styrofoam balls
2) Electric

SURROUND TOOTHBRUSH
https://www.google.com/search?q=surround+toothbrush&espv=210&es_sm=93&source=lnms&tbm=isch&sa=X&ei=cWgzU8jLN6GwygHsvICAAg&ved=0CAkQ_AUoAg&biw=1097&bih=560#imgdii=_

FLOSS
•Floss holders

MOUTH RINSE AND FLUORIDE
Antimicrobial Agents:• Liquid mouth rinse is NOT recommended • Chlorohexidine gel
Fluoride:• OTC Fluoride gel
CAREGIVERS• Their importance
• Help patients with home care (medications, food, shower, & brushing)
• Their feelings about their tasks• Stress, anxiety, and burden• Less stress when PD is managed with
subthalamic deep brain stimulation (STN-DBS)

REFERENCES1. S.A. Wylie, D.O. Claassen, H.M. Huizenga, K.D. Schewel, K.R. Ridderinkhof, T.R. Bashore, and W.P.M. van den Wildenberg. Dopamine Agonists and the Suppression of Impulsive Motor Actions in Parkinson’s Disease. J Cogn Neurosci. 2012 August; 24(8): 1709–1724. 2. Melissa J. Nirenberg, M.D., Ph.D. Understanding Parkinson’s, Secrets, Myths & Misconceptions [Internet]. www.pdf.org PDF News & Review, Winter 2010 [updated 2011; cited 2014 March 18]. Available from: http://www.pdf.org/pdf/fs_parkinson_secrets_myths_10[1].pdf 3. Alexander Tröster, Ph.D. Understanding Parkinson’s, Cognition and Parkinson’s [Internet]. www.pdf.org PDF News & Review; 2012 [updated 2012; cited 2014 March 18]. Available from: http://www.pdf.org/pdf/fs_cognitive_changes_12.pdf 4. Roy G. Elbers, MSc, Erwin E. H. van Wegen, PhD, John Verhoef, PhD andGert Kwakkel, PhD. Is gait speed a valid measure to predict community ambulation in patients with Parkinson’s disease? Journal of Rehabilitation Medicine 2013; 45: 370–375. 5. Xia Shen, MPT, Margaret K.Y. Mak, PhD. Repetitive Step Training with Preparatory Signals Improves Stability Limits in Patients with Parkinson’s Disease. J Rehabil Med 2012; 44: 944–949. 6. Grover S, Rhodus Nl. Dental implications of Parkinson’s disease. Journal of the Minnesota Dental Association. 7. Muller T, Palluch R, Jackowski J. Caries and periodontal disease in patients with parkinson’s disease. Special Care Denistry Association and Wiley Periodicals 2011; 31(5): 178-181. 8. Burgess J, Editor C, Meyers AD. Management of the dental patient with neurological Disease. Medscape 2013. 9. Yarnall A, Archibald N, Burn D. Parkinson’s disease. Medicine 2012.
10. DeBowes SL, Tolle SL, Bruhn AM. Parkinson’s disease: considerations for dental hygienist. International Journal of Dental Hygiene 2013; 15-12.
11. Yamanishi T, Tachibana H, Oguru M, Matsui K, Toda K, Okuda B, Oka N. Anxiety and depression in patients with parkinson’s disease. Internal Medicine 2013; 52: 539-545.
12. Al-Omari FA, Al Moaleem MM, Al-Qahtani SS, Al Garni AS, Sadatullah S, Luqman M. Oral rehabilitation of parkinson’s disease patient: A Review and Case Report. Case Reports in Dentistry 2014; (2014): 4.
13. Katyayan PA, Katyayan MK, Nugala B. Dental management of parkinson's disease. New York State Dental Journal 2013; 79(5):33-9.
14. Wilkins, EM. Clinical practice of the dental hygienist. 11th ed. Philadelphia: Lippincott Williams and Wilkins; 2013. 1147 p.
15. Tew EH, Naismith SL., Pereira M, Lewis SJ. Quality of life in parkinson's disease caregivers: the contribution of personality traits. BioMed Research International 2013; (2013): 6.
16. Dotchina CL, Paddicka SM, Longdona AR, Kisolia A, Graya WK, Dewhursta F, Chaotea P, Dewhursta M and Walker RW. A comparison of caregiver burden in older persons and persons with parkinson's disease or dementia in sub-Saharan Africa. International Psychogeriatric Association 2014; 26(04): 687-692.
17. Lewis CJ, Maiera F, Eggersa C, Pelzera EA, Maaroufb M, Moroc M, Zurowskid M, Kuhne J, Woopenf C, Timmermanna L. Parkinson's disease patients with subthalamic stimulation and carers judge quality of life differently. Elsevier B.V 2014; (2014): 1-6.
Thank you
Related Documents











