7/21/09 1 ASPERGILLOSIS Gina Milick Jennifer Hornick Andraele Reed Tiffany Shugart HISTORY OF ASPERGILLOSIS 1729 – Fungus Aspergillus first identified and catalogued by Italian biologist/priest Micheli Noticed under microscope the fungi looked like an aspergillum which is used to sprinkle holy water and named the genus after it. 1815 – Aspergillus first observed in birds by Mayer 1842 – British physician John Hughes Bennett discovered first case of pulmonary aspergillosis in humans. Called aspergilloma which means “fungus ball” in the lungs HISTORY OF ASPERGILLOSIS Many early cases of aspergillosis were found in patients with tuberculosis or high risk occupations such as pigeon-crammers and wig combers Some were invasive but most were aspergillomas 1953 – Rankin described the ability of Aspergillus to cause opportunistic infection in immunocompromised patients 1970 – Histopathology and clinical features of disease described in 98 patients TAXONOMY Kingdom: Fungi Phylum: Ascomycota Order: Eurotiales Family: Trichocomaceae Genus: Aspergillus ETIOLOGY Genus Aspergillus includes over 185 species ~20 species reported to cause infections 7 are facultatively pathogenic Aspergillus fumigatus most commonly isolated species Found in 90% of infections Widespread in nature Commonly found in soil and compost heaps Can also be found indoors Thermophilic species (Growth at 40° C and above) Angioinvasive ASPERGILLUS FUMIGATUS http://www.mycology.adelaide.edu.au/gallery/photos/ aspergillus11.gif Conidios pores are short ,s mooth- walled with conical shaped terminal vesicles

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

7/21/09
1
ASPERGILLOSIS
Gina Milick Jennifer Hornick Andraele Reed Tiffany Shugart
HISTORY OF ASPERGILLOSIS
1729 – Fungus Aspergillus first identified and catalogued by Italian biologist/priest Micheli
Noticed under microscope the fungi looked like an aspergillum which is used to sprinkle holy water and named the genus after it.
1815 – Aspergillus first observed in birds by Mayer
1842 – British physician John Hughes Bennett discovered first case of pulmonary aspergillosis in humans.
Called aspergilloma which means “fungus ball” in the lungs
HISTORY OF ASPERGILLOSIS
Many early cases of aspergillosis were found in patients with tuberculosis or high risk occupations such as pigeon-crammers and wig combers Some were invasive but most were
aspergillomas 1953 – Rankin described the ability of
Aspergillus to cause opportunistic infection in immunocompromised patients
1970 – Histopathology and clinical features of disease described in 98 patients
TAXONOMY
Kingdom: Fungi Phylum: Ascomycota Order: Eurotiales Family: Trichocomaceae Genus: Aspergillus
ETIOLOGY
Genus Aspergillus includes over 185 species ~20 species reported to cause infections 7 are facultatively pathogenic
Aspergillus fumigatus most commonly isolated species Found in 90% of infections Widespread in nature Commonly found in soil and compost heaps Can also be found indoors Thermophilic species (Growth at 40° C and above) Angioinvasive
ASPERGILLUS FUMIGATUS
http://www.mycology.adelaide.edu.au/gallery/photos/aspergillus11.gif
Conidiospores are short ,smooth-walled with conical shaped terminal vesicles
7/21/09
2
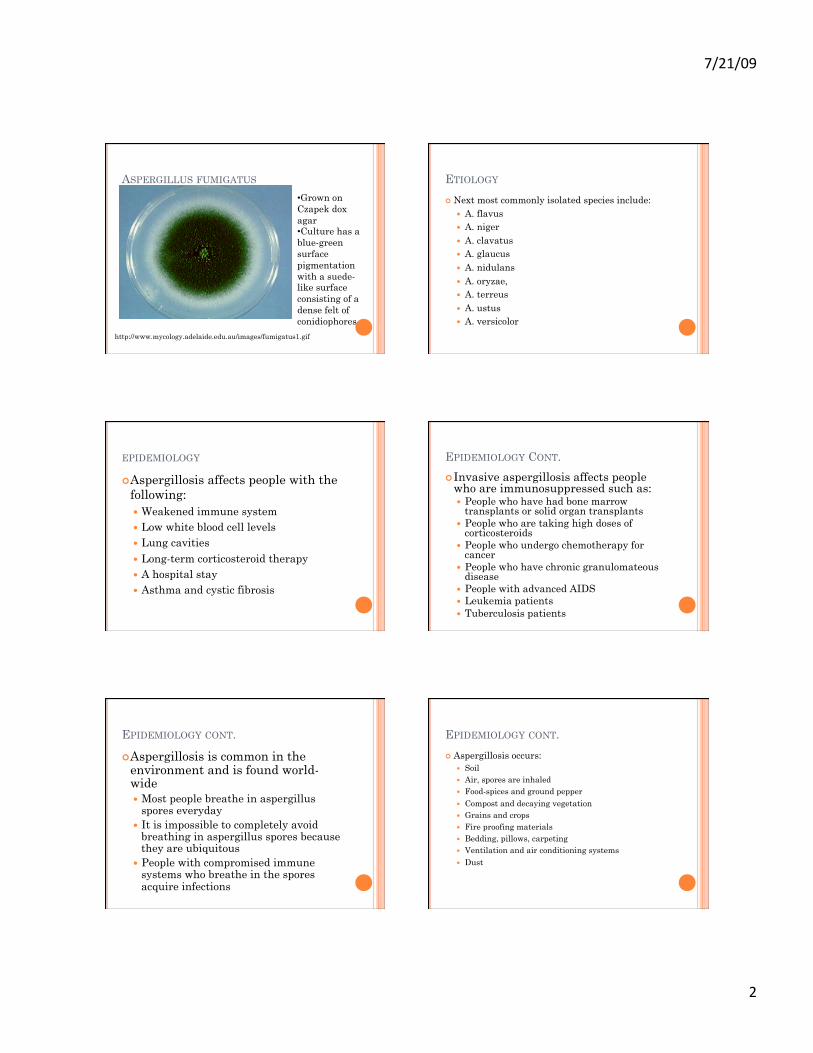
ASPERGILLUS FUMIGATUS
http://www.mycology.adelaide.edu.au/images/fumigatus1.gif
• Grown on Czapek dox agar • Culture has a blue-green surface pigmentation with a suede-like surface consisting of a dense felt of conidiophores
ETIOLOGY
Next most commonly isolated species include: A. flavus A. niger A. clavatus A. glaucus A. nidulans A. oryzae, A. terreus A. ustus A. versicolor
EPIDEMIOLOGY
Aspergillosis affects people with the following: Weakened immune system Low white blood cell levels Lung cavities Long-term corticosteroid therapy A hospital stay Asthma and cystic fibrosis
EPIDEMIOLOGY CONT.
Invasive aspergillosis affects people who are immunosuppressed such as: People who have had bone marrow
transplants or solid organ transplants People who are taking high doses of
corticosteroids People who undergo chemotherapy for
cancer People who have chronic granulomateous
disease People with advanced AIDS Leukemia patients Tuberculosis patients
EPIDEMIOLOGY CONT.
Aspergillosis is common in the environment and is found world-wide Most people breathe in aspergillus
spores everyday It is impossible to completely avoid
breathing in aspergillus spores because they are ubiquitous
People with compromised immune systems who breathe in the spores acquire infections
EPIDEMIOLOGY CONT.
Aspergillosis occurs: Soil Air, spores are inhaled Food-spices and ground pepper Compost and decaying vegetation Grains and crops Fire proofing materials Bedding, pillows, carpeting Ventilation and air conditioning systems Dust

7/21/09
3
MANIFESTATIONS
Respiratory Cranial Pathologic Clinical Thoracic Initial CT
DISEASE SPECTRUM
Forms of the disease involve: Sinuses Lungs Pre-existing lung cavity Pulmonary aspergillosis CNS aspergillosis Sinonasal aspergillosis Osteomyelitis Endophthalmitis Endocarditis Renal Abscesses Cutaneous (Burns, post surgical wounds, IV insertion sites) Otomycosis Exogenous endophthalmitis Allergic fungal sinusitis Urinary tract fungus balls
HISTOPATHOLOGY
Tissue reaction in aspergillosis is acute suppurative inflammation with areas of ischemic necrosis
The fungus proliferates as septate hyphae 2.5-4.5 µm in diameter
Hyphae can be characterized as branching dichotomously (Approx 45° angle)
Blood vessel invasion, thrombosis, infarction, and dissemination are common
The mortality rate for invasive aspergillosis is 50-100% and diagnosis by culutre may take as long as 4 weeks.
HISTOPATHOLOGY
Grocott’s methenamine silver (GMS) stained tissue sections showing Aspergillus fumigatus in lung tissue, Note : conidial heads forming in an alveolus.
Taken from: http://www.mycology.adelaide.edu.au/gallery/photos/aspergillus08.gif
PATHOGENESIS
Virulence factors: A. fumigatus has about 4 virulence factors alone:
Gliotoxin-inhibits mucociliary system Fumagillin Fumagatin Helvolic acid
Since Aspergillus can be found almost everywhere world-wide, it is primary acquired through the respiratory tract. However, there have been cases of disseminated
disease after skin or gastrointestinal infections.
PATHOGENESIS
Host response in normal host (non-immunosuppressed) Normal immune system response:
Mucosal barriers – Traps Macrophages – Phagocytosis Neutrophils
Kills conidiae and inhibits germination of hyphae
7/21/09
4
PATHOGENESIS
Normal host response can be impaired by a number of factors: Granulocytopenia Impaired macrophages/neutropenia Underlying disease impairing immune system Lung destruction Large numbers/prolonged exposure to organism Hypersensitivity/allergic response
In the immunocompromised: Conidia spores colonize lesions or cavities Hyphae begins to form and grow throughout
body
PATHOGENESIS
There are three major ways Aspergillus involves the lungs: Mycetoma (non-invasive) IPA
Invasive Pumonary Aspergillosis Allergic
DIAGNOSIS
Clinical Presentations: Fever Cough Dyspnea
Difficulty breathing Hemoptysis
Coughing up blood Chest Pain
LABORATORY DIAGNOSIS
Radiographic picture Classical CT Scan Serological testing Sputum culture Transthoracic needle aspiration
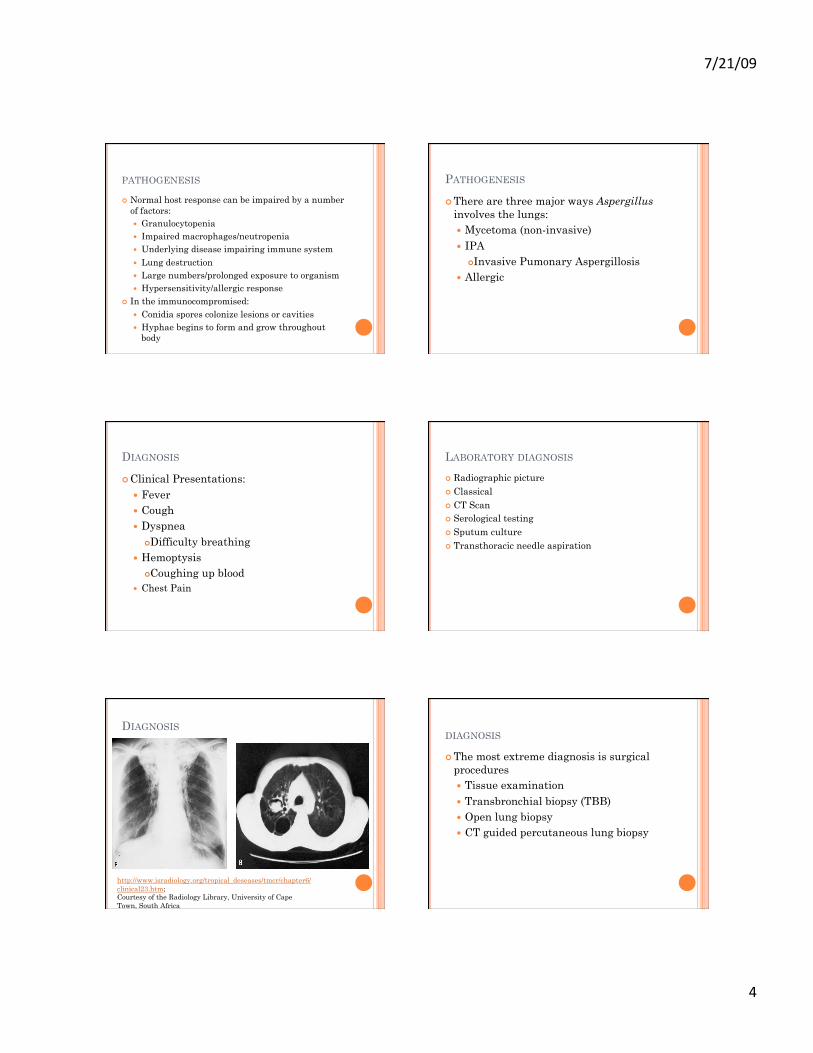
DIAGNOSIS
http://www.isradiology.org/tropical_deseases/tmcr/chapter6/clinical23.htm; Courtesy of the Radiology Library, University of Cape Town, South Africa
DIAGNOSIS
The most extreme diagnosis is surgical procedures Tissue examination Transbronchial biopsy (TBB) Open lung biopsy CT guided percutaneous lung biopsy

7/21/09
5
DISEASE MANAGEMENT
Allergic BronchopulmonaryAspergillosis (ABPA) Caused by an allergy to the spores of the
Aspergillus moulds. Commonly effects people with asthma and
cystic fibrosis patients. Steroids by aerosol or mouth
Prednisolone Itraconazole
An oral antifungal drug
DISEASE MANAGEMENT
Aspergilloma and Chronic Pulmonary Aspergillosis Fungus caused by the Aspergillous mould Grows in the lung cavity Treatment depends on the symptoms
present Itraconazole Voriconazole Surgery Amphotercin B
DISEASE MANAGEMENT
Aspergillus Sinusitis Disease occurs in the sinuses May be associated with long standing
symptoms of runny blocked nose May lead to nasal polyps Surgical drainage, removal of polyps Local steroids Oral Steroids Antifungals
DISEASE MANAGEMENT
Invasive Aspergillosis Effects people with poor immune systems Fungus can transfer from the lung through the
blood to the brain and other organs Antifungal Drugs
Voriconazole Caspefungin Itraconazole Amphotericin B
DISEASE PREVENTION
This disease commonly effects people with a weak immune system Avoid medications that may further weaken
the immune system. Avoid forests, grain stores, rotting vegetation,
and piles of dead leaves. Hospitals should have good ventilation
Dust control Adequate air flow rate
CASE STUDY – “SUDDEN DEATH DUE TO PULMONARY ASPERGILLOSIS”
35 yr old Moderately built and malnourished TB patient for a year Hemoptysis while traveling in a train. Was declared dead upon arrival to the
hospital. Same day autopsy was performed.

7/21/09
6
CASE STUDY - SYMPTOMS
External examination Internal examination
Blood stains were present over the oral and nasal orifices
Clubbing of fingers and toes
No external injuries
Trachea and bronchi contained blood clots.
Right sided pleural internal scarring was present.
Surface of lungs was grayish black with necrotic material.
Enlarged lymph nodes. Pale gastrointestinal
organs filled with blood.
CASE STUDY
CLUBBING OF FINGERS AND TOES. Source: Courtesy of Journal of
Forensic and Legal Medicine
CASE STUDY - DIAGNOSIS
Microscopy Grocott’s methanamine silver stain
(GMS) Biopsy of the lungs Autopsy Findings of the lungs
Dilated bronchioles Alveolar septae showed congested
vessels. Edema and hemorrhage
CASE STUDY - CONCLUSION
It was diagnosed to be a case of old fibrocavitatory tuberculosis with Aspergillus colonization.
No active TB was present. Cause of death was as hemorrhage
secondary to pulmonary aspergillosis.
CASE STUDY
Fig. 1. Cut section of the lung showing grayish black areas and cavity containing yellowish black necrotic material.
Fig. 2. Microscopy of the lung with Grocott’s methanamine silver stain showing a cavity lined by fibrocollaginous tissue and colonized byAspergillus.
Source: Courtesy of Journal of Forensic and Legal Medicine
REFERENCES "The Aspergillus Website, Fungal Research Trust". July 18, 2009 <http://
www.aspergillus.org.uk/languages/english.php>.
Bhagavath, Prashantha, et al. "Sudden death due to pulmonary aspergillosis." Journal of Forensic and Legal Medicine 16.1 (2009), 27-30.
“Comparison of multiple typing methods for Aspergillus fumigatus.CrossRef DOI Query." Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases [No Volume/Issue] (2009) [No Pagination].
"Doctor Fungus". July 18, 2009 <http://www.doctorfungus.org/mycoses/human/aspergillus/aspergillosis.htm>.
Harmen, E (2008, March 7). eMedicine Specialties. Retrieved July 17, 2009, from Aspergillosis Web site: http://emedicine.medscape.com/article/296052-overview

7/21/09
7
REFERENCES 6K.Marr, T.Patterson, D.Denning. Aspergillosis Pathogenesis, clinic
al manifestations, and therapy Infectious Disease Clinics of North America, Volume 16, Issue 4, Pages 875-894
"Knowledge Storage". July 18, 2009 <http://knowledge-storage.com/medicine/37-medicine/84-aspergillosis>.
Mayo Clinic Staff, (2009, May 2). Mayo Clinic. Retrieved July 17, 2009, from Aspergillosis Web site: http://www.mayoclinic.com/health/aspergillosis/ds00950
REFERENCES Nguyen MH. (2007). Use of bronchoalveolar lavage to detect
galactomannan for diagnosis of pulmonary aspergillosis among nonimmunocompromised hosts. Journal Of Clinical Microbiology, 45(9), 2787.
Unknown, (2008, March 27). Centers for Disease Control and Prevention. Retrieved July 17, 2009, from Aspergillosis (Aspergillus) Web site: http://www.cdc.gov/nczved/dfbmd/disease_listing/aspergillosis_gi.html
Zmeili, O.S. and A.O. Soubani. "Pulmonary aspergillosis: a clinical update." Journal of the Association of Physicians 100.6 (2007), 317-334.
QUESTIONS
1. What species of Aspergillus most commonly causes infections?
A) A. fumigatus B) A. niger C) A. versicolor D) A. flavus
2. Aspergillus most commonly affects the: A) Heart B) Skin C) Lungs D) GI tract
QUESTIONS
3. In a normal host, which immune defense mechanism usually inhibits hyphae germination?
A) Mucosal barriers B) Thrombocytes C) Neutrophils D) All of the Above
4. What type of medications should people affected by Aspergillus avoid?
A) Amphotericin B B) Any that weaken the immune system C) Anti-depressants D) All above
QUESTIONS
5) What is a virulence factor for Aspergillus fumigatus?
A) Fumagillin B) Fumagatin C) Gliotoxin D) All of the above
Related Documents







![Aspergillosis - Youngstown State Universitypeople.ysu.edu/~crcooper01/Aspergillosis[1]- Katie Jacquie Qazi.pdf•People with Aspergillosis are in three distinct groups •Healthy immune](https://static.cupdf.com/doc/110x72/5e3883b0e2f2970b7b1c24ad/aspergillosis-youngstown-state-crcooper01aspergillosis1-katie-jacquie-qazipdf.jpg)



