1 N e opl as i a & cancer Dr.Nafea Sami Al Esawi General pathology 2014 2 n d stage students

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 1/174
1
Neoplasia & cancer
Dr.Nafea Sami Al Esawi
General pathology 2014
2
nd
stage students
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 2/174
2
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 3/174
3
What is neoplasia ? Neoplasia is new, uncontrolled growth of cells that is not
under physiologic control . Pathogenesis :
1-Process of new growth of cells ( not single step).
2-Induced by certain stimuli .
3-Leading to new features TRANSFORMED CELL
- Persistent & useless growth.
- Uncontrolled (autonomy growth)
- Immortality .- Transplantability .
Any cell can be transformed growth Tumor
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 4/174
Carcinogenic factor, causes a cell to be transformed to a
neoplastic cell that is not controlled by normal body
processes.Probably most transformed cells die because they are
too abnormal to function or are abnormal enough for the
body's immune system to destroy them.
However, if the factors promoting transformation persist, a transformed cell may give rise to a clone that
does continue to grow resulting in neoplasia.
4
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 5/174
Tumor:
An abnormal mass of tissue the growth of which is
1-Virtually autonomous ( independent of
physiological growth stimuli ).
2-Exceeds that of normal tissue.
3-Uncoordinated with that of normal tissues (unlike
non neoplastic proliferations like (hyperplasia ,
regeneration, repair).
4-Persists in the same excessive manner after the
cessation of the stimuli which evoked the change
( the genetic alterations are passed down to the
progeny of tumor cells ). 5
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 6/174
Characteristics of Transformed Cells : ?
Clonality :All tumor cells are clonal : Monoclonal .
All tumor cells (the entire population of neoplastic cells) within the individual tumor arise from a single cell
that has incurred genetic changes and hence the tumor
are said to be clonal . All tumors ( benign & malignant ) composed of :
1-Clonal neoplastic cells ( parenchyma ):which determine
the tumor behavior and consequence.2-Reactive stroma (connective tissue ,BVS , inflammatory
cells ) : provide framework for neoplastic cells growth
and nutrients for tumor growth & evolution .6
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 7/174
7
- Autonomous growth :The growth of neoplastic cells isindependent of growth factors ,regarding mechanismoperating inside normal cells.
Excessive growth :The excess may be evident in thesize of the outgrowth & duration of the proliferation .
Disorganized growth ( cytoarchitectural level ) :Thestructures formed by tumor cells differ from the normaltissue & don't fit into general organization scheme ofthe normal body .
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 8/174
8
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 9/174
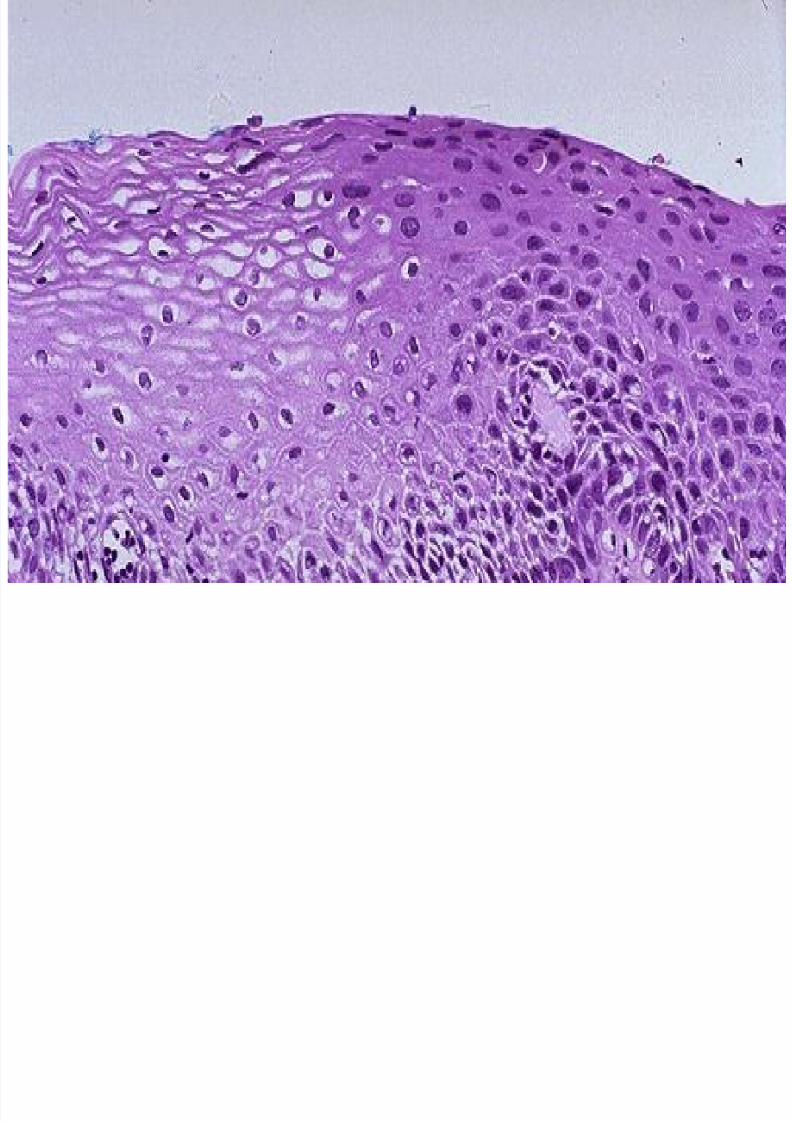
Dysplasia: A disordered growth and maturation of an epithelium,
which is still reversible if the factors driving it areeliminated .
1st is hypercellularity .
A - Nuclear changes :
1-Nuclear enlargement ( increase N/C ratio ).
2-Pleomorphism ( variation in size & shape of nuclei).
3-Hyperchromatism &chromatin irregularity .
4-Multinucleation ( unequal size multiple nuclei ).
5-Irregularity of nuclear membrane .
6-Prominent & giant & multiple nucleoli ( differ in size &
shape) . 9
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 10/174
B – Cytoplasmic changes :
1-Scanty cytoplasm .
2-Variation in size & shape .
3-Cytoplasmic staining :
Deep orange in keratinized squamous cell carcinoma.
Basophilic in poorely differentiated carcinoma.
4-Cytoplasmic inclusion :melanin in malignant melanoma
.
10
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 11/174
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 12/174
In capillaries and postcapillary venules, T. media
whichpericytesmay be replaced by cells called
have contractile function and can proliferate and
differentiate after injury to new blood vessels .
Tun ica advent i t ia
oriented collagenous andlongitudinallyConsists ofelastic fibers that become continuous with the
surrounded C.T.
•:Innervation of Blood vesselsBl. Vessels supplied by autonomic nervous system
that regulate their relaxation and contraction by
special neurotransmitters.
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 13/174
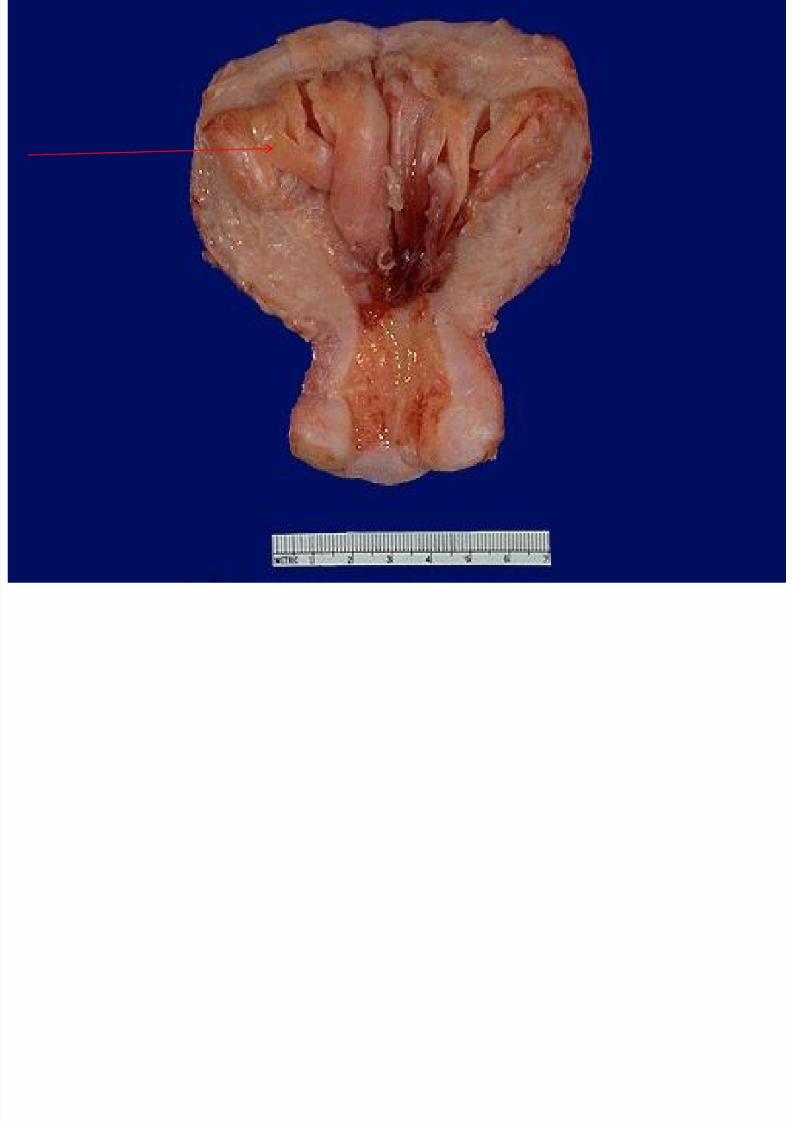
Hyperplasia: Is an increase in the size of a tissue or organ due to
increase number of constituent cells or increase in
the number of cells resulting in growth lesion.
Postpartum breast lobules undergo hyperplasia for
lactation is normal physiological process.
Endometrial hyperplasia in a postmenopausal
woman is abnormal .
13
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 14/174
14
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 15/174
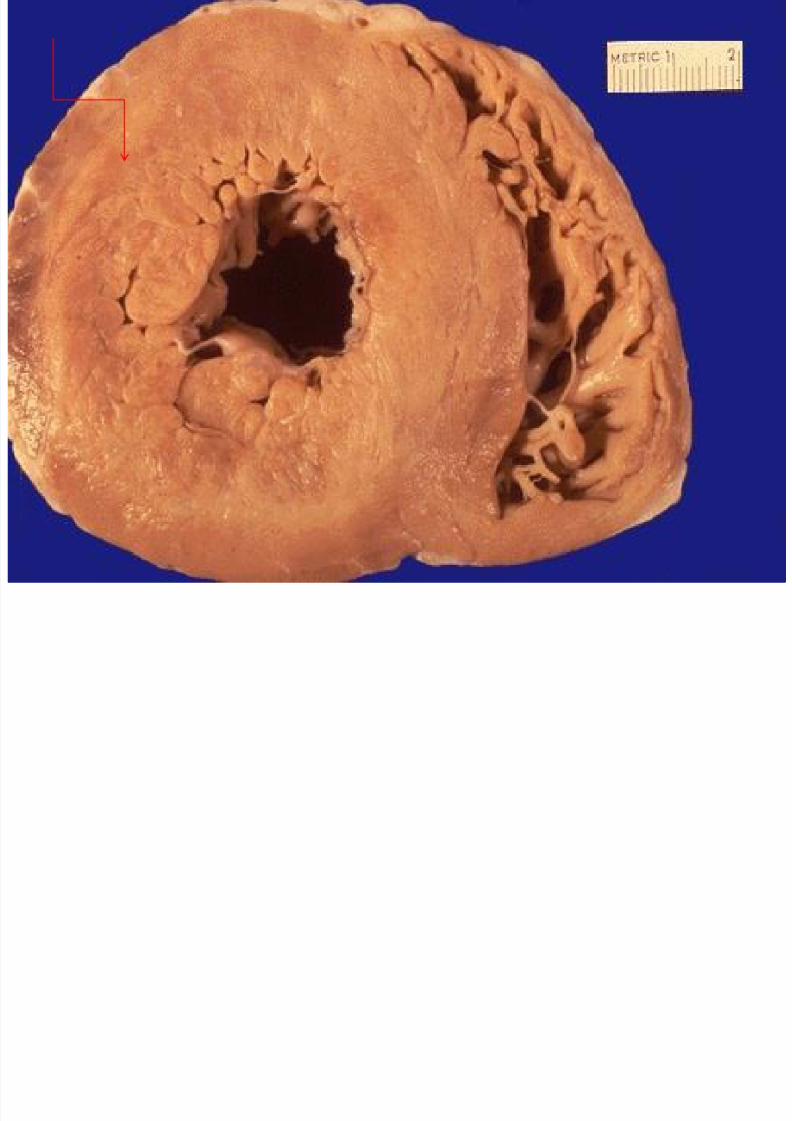
Hypertrophy:.
An increase in organ size due to increase in cell size
without increase number of constituent cells .
Increase in skeletal muscle fiber size is a physiologic
response to exercise . The cardiac hypertrophy is a pathologic response to
abnormally elevated blood pressure.:
15
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 16/174
.
16
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 17/174
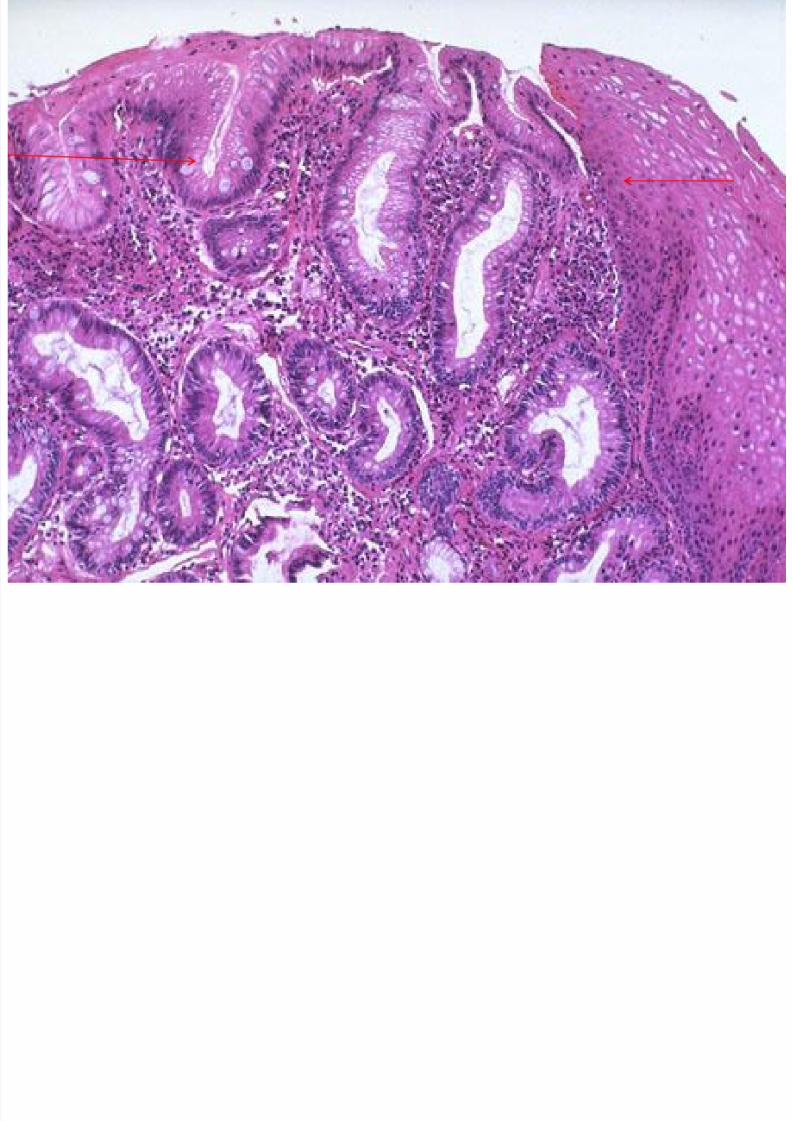
Metaplasia Is the replacement of one matur adult cell type by
another one mature adult cell type .
It is a reversible process .
Metaplasia: an initial change from normal cells to a
different cell type (such as chronic irritation of cigarette
smoke causing ciliated pseudostratified columinar
epithelium to be replaced by squamous epithelium more
able to withstand the insult). Consider a first step toward neoplasia in many sites in
the body ( bronchus , cervix , esophagues ) .
17
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 18/174
18

8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 19/174
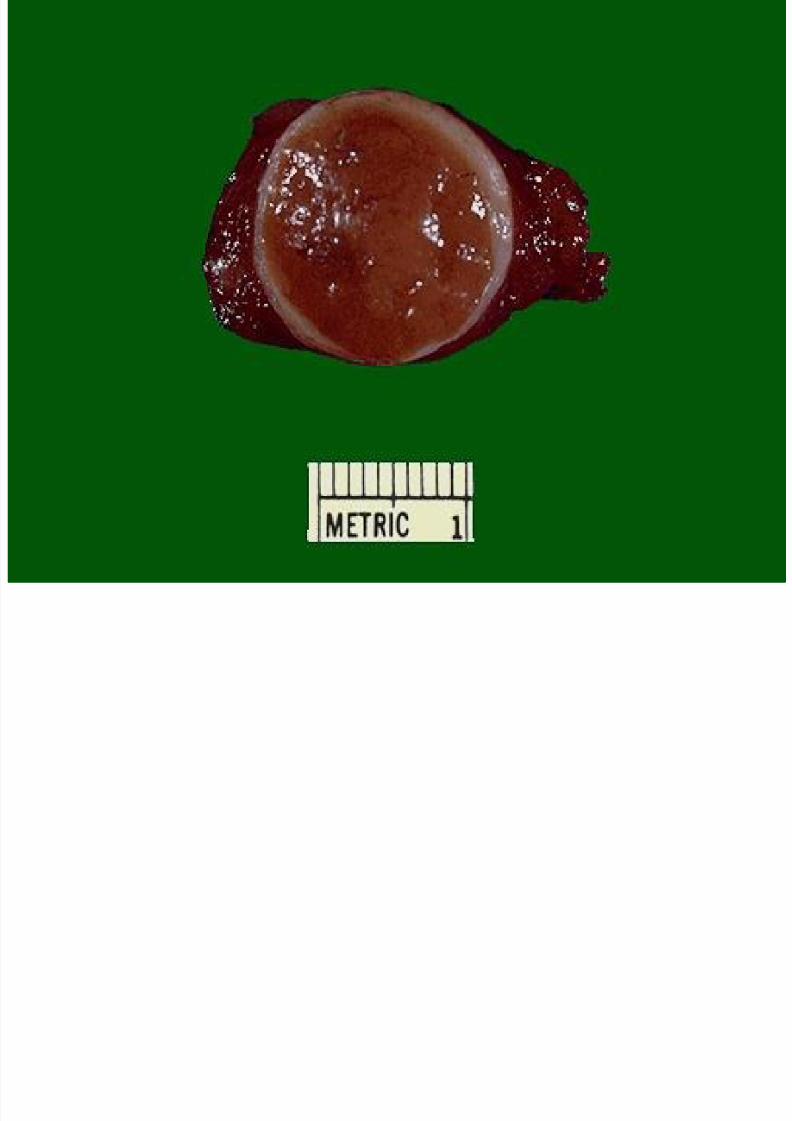
Benign tumor: A benign neoplasm looks microscopically a lot like the
tissue of normal cells from which it originated, and itsgeneral characteristics include:
Slow growth ( innocent ).
Resemblance to tissue of origin (well differentiated) . Circumscription ( localize ).
Capsulation .
Lack of invasion . Absence of metastases .
Prognosis : Good .
19
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 20/174
20
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 21/174
:A malignant neoplasm is composed of
1- Cells that look less like the normal cell of origin (
less differentiation ).
2- It has a higher rate of proliferation ( mitosis ).
3-It can potentially invade and destroyed the adjacent
structure .
4- It can metastasize .
Prognosis : poor :potentially lethal .
21
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 22/174
22
Tumors are classified by:
1 -Histological :Cell of origin (epithelial or stromal ).
2- Clinical behavior of tumor :
Benign :good prognosis .
Malignant :potentially lethal .
Borderline : low grade malignant tumor
(intermediate).
3- Gross Appearance of the tumor :localize or
infiltrative.
4- Grade :Degree of differentiation & anaplasia .
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 23/174
23
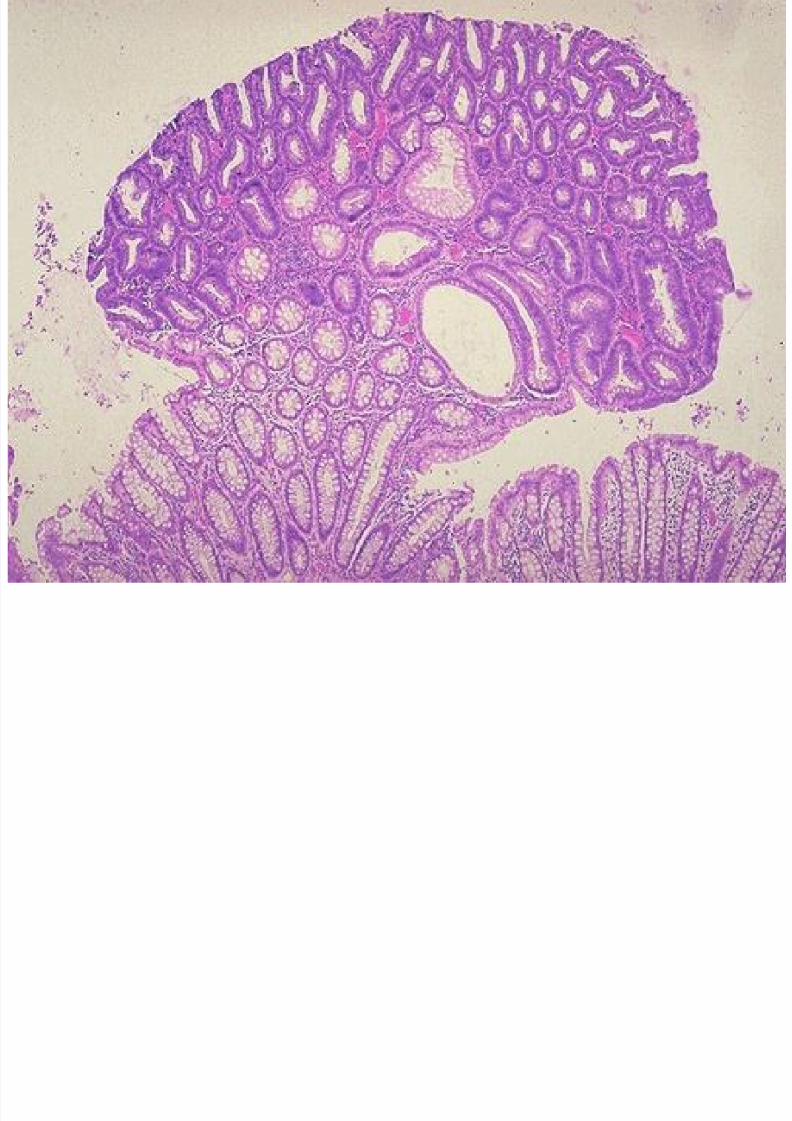
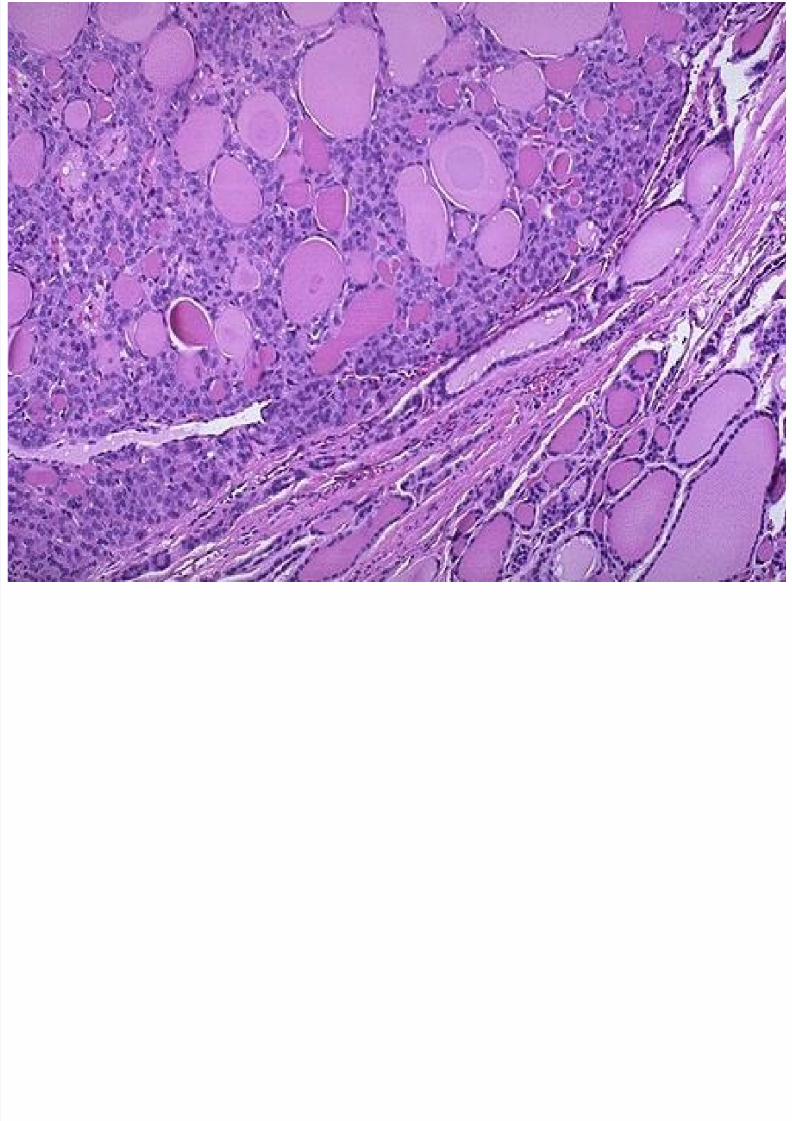
naming : Classif ication by origin EPITHELIAL CELL : Benign tumors of epithel ial cel ls:
Adenoma : is term applied to a benign epithelial
neoplasm derived from glands, although they may ormay not form glandular structures.
On this basis, a benign epithelial neoplasm that arises
from renal tubular cells growing in the form ofnumerous tightly clustered small glands would betermed an adenoma, as would a heterogeneous mass
of adrenal cortical cells growing as a solid sheet.
-Tubular adenoma of colon .
-Follicular adenoma of thyroid .
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 24/174
24
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 25/174
25
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 26/174
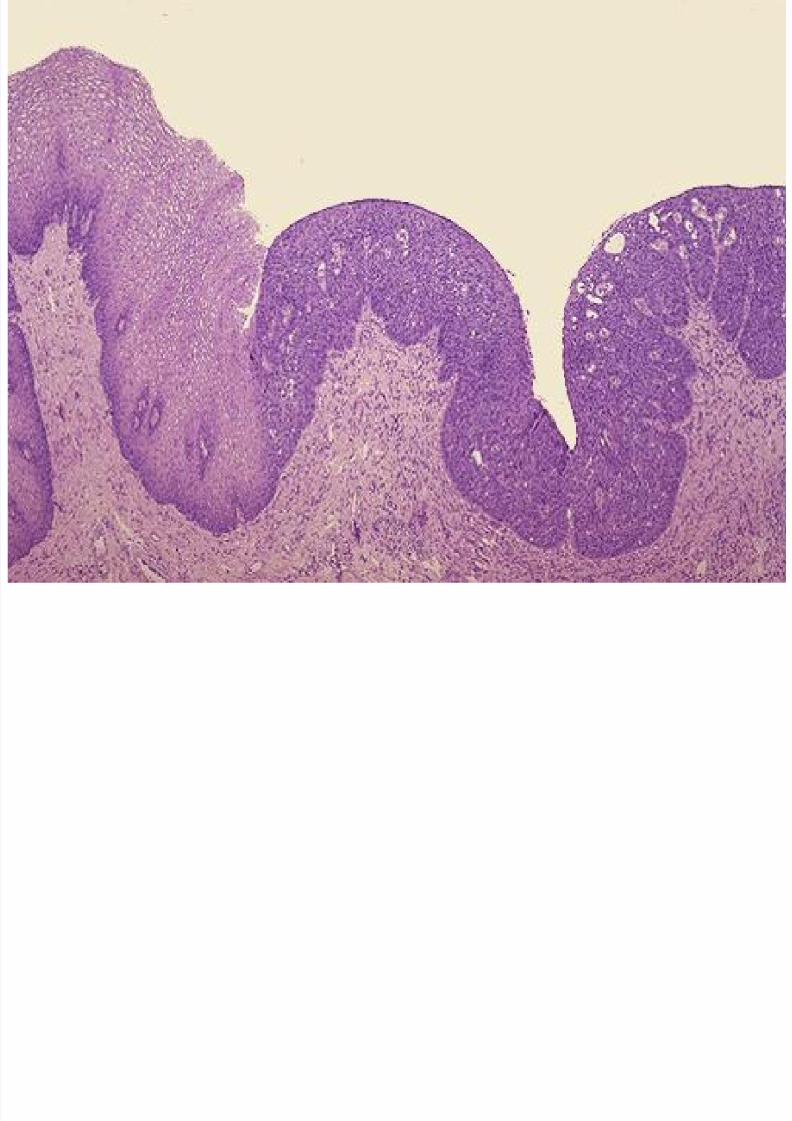
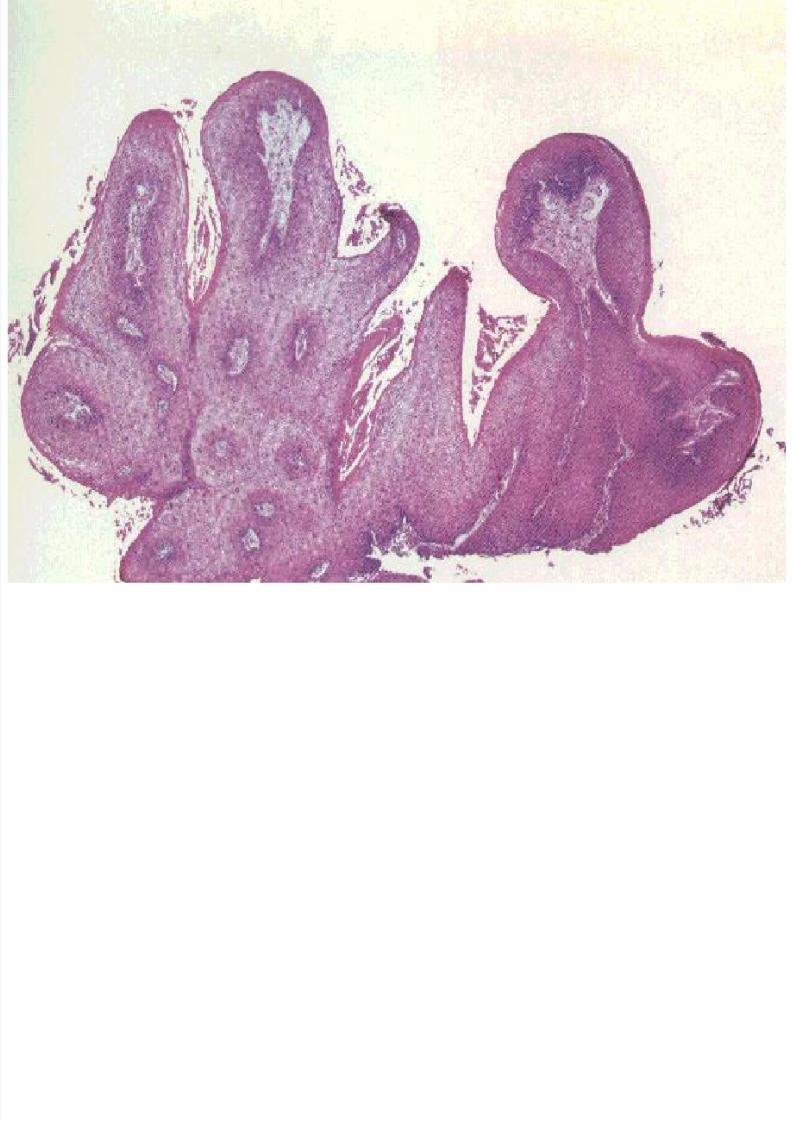
:PapillomaTerm applied for benign tumor arising from surface
epithelium e.g skin or mucosal surface:Grossly appear as finger like protrusion on surface or
warty projection on mucosa of hallow organ .
Microscopically :It is composed of finger-likeepithelial cell growing overlying fibrovascular core(connective tissue with blood vessels) .
e.g Squamous papilloma of skin .
Squamous papilloma of larynx .
Transitional Papilloma of bladder.
26
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 27/174
27
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 28/174
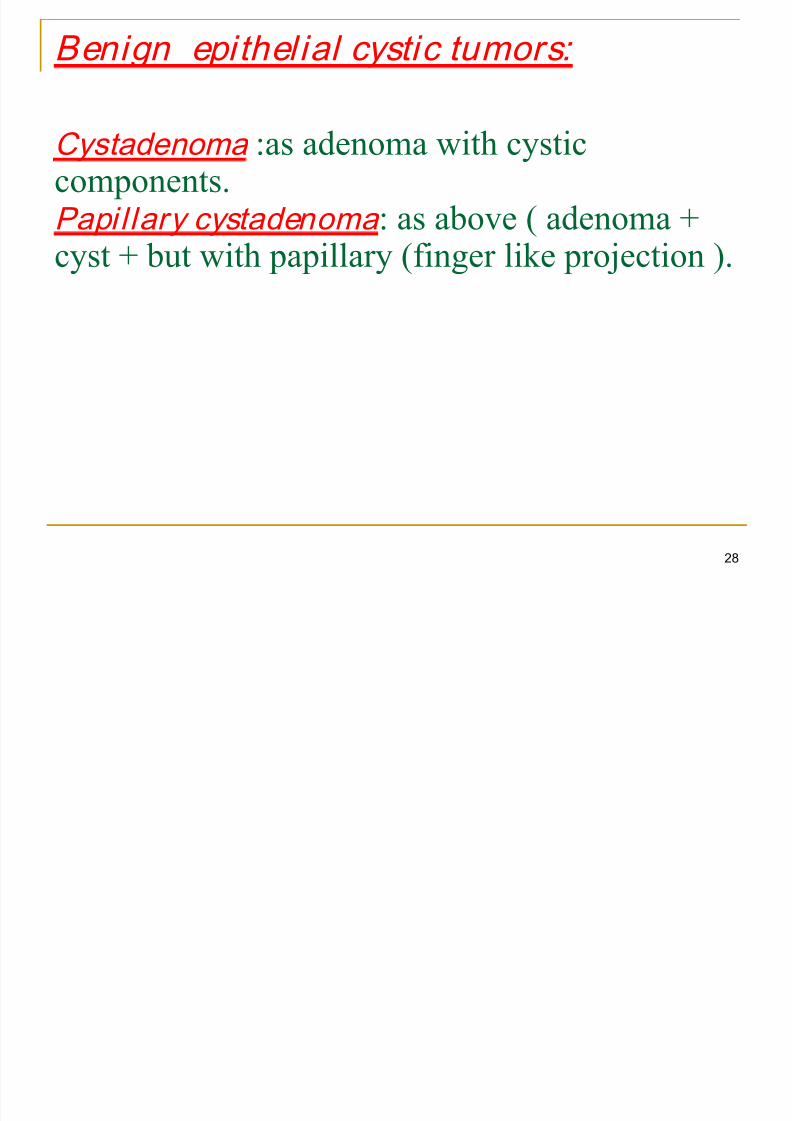
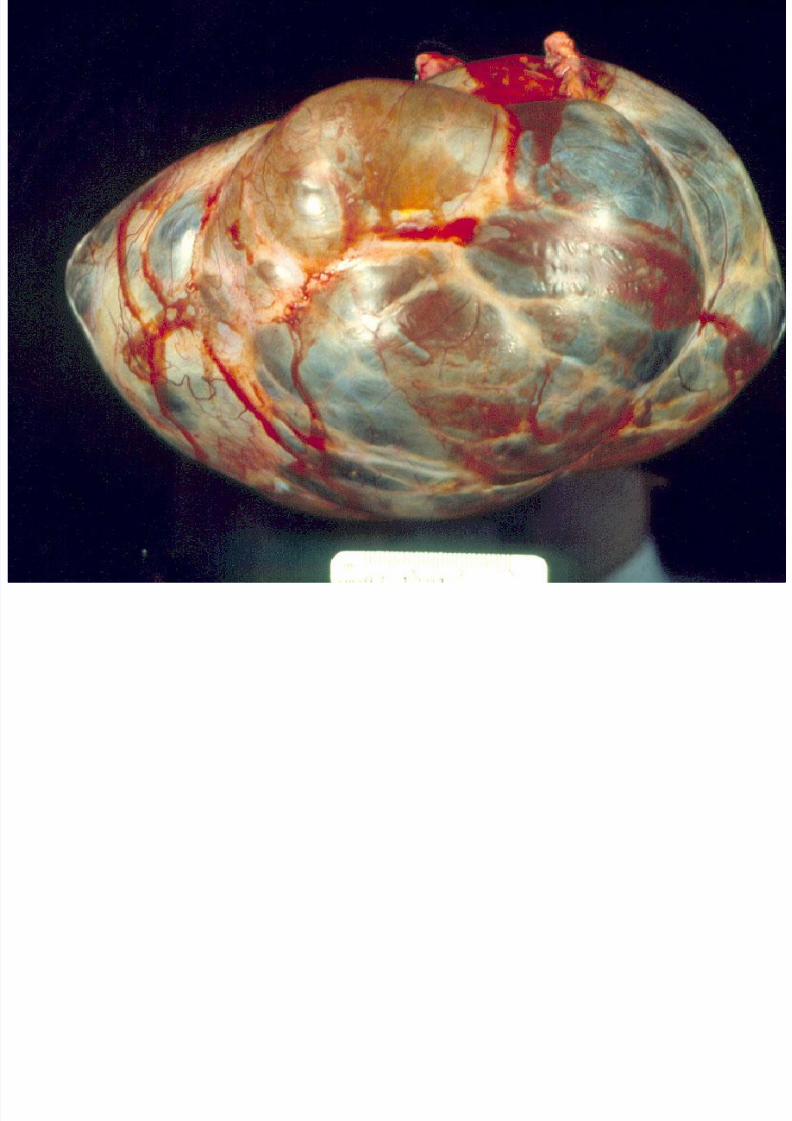
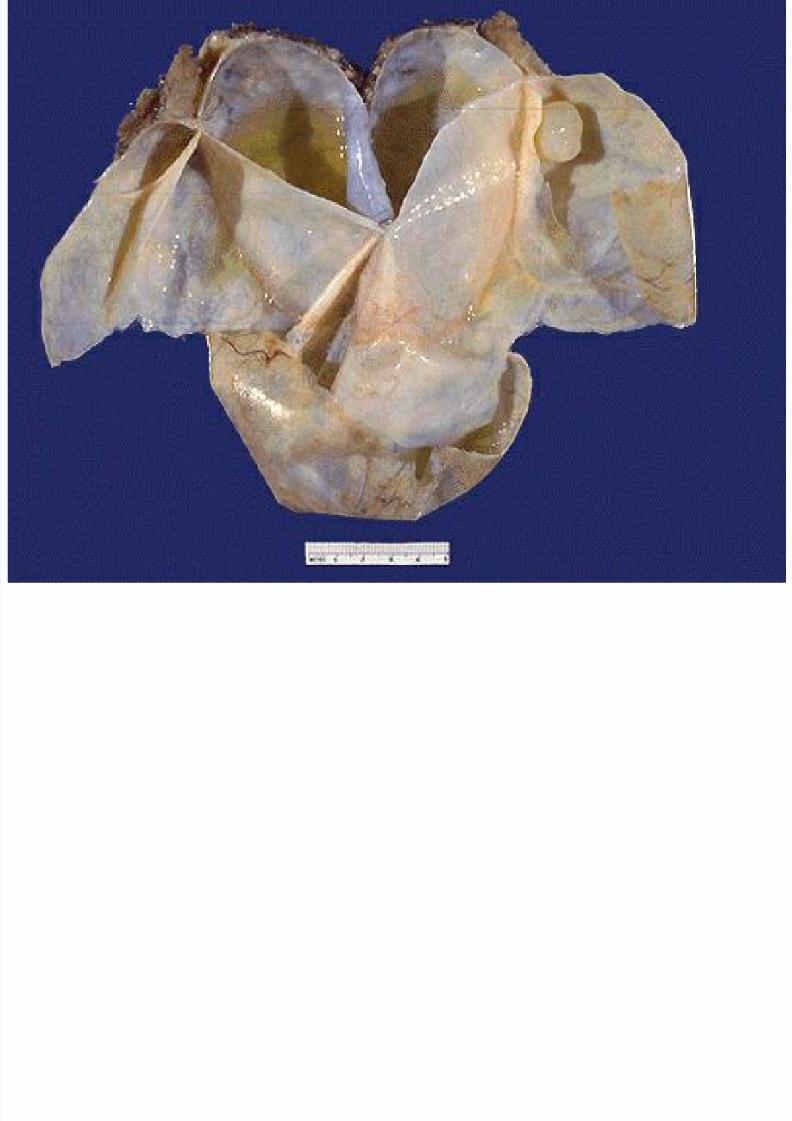
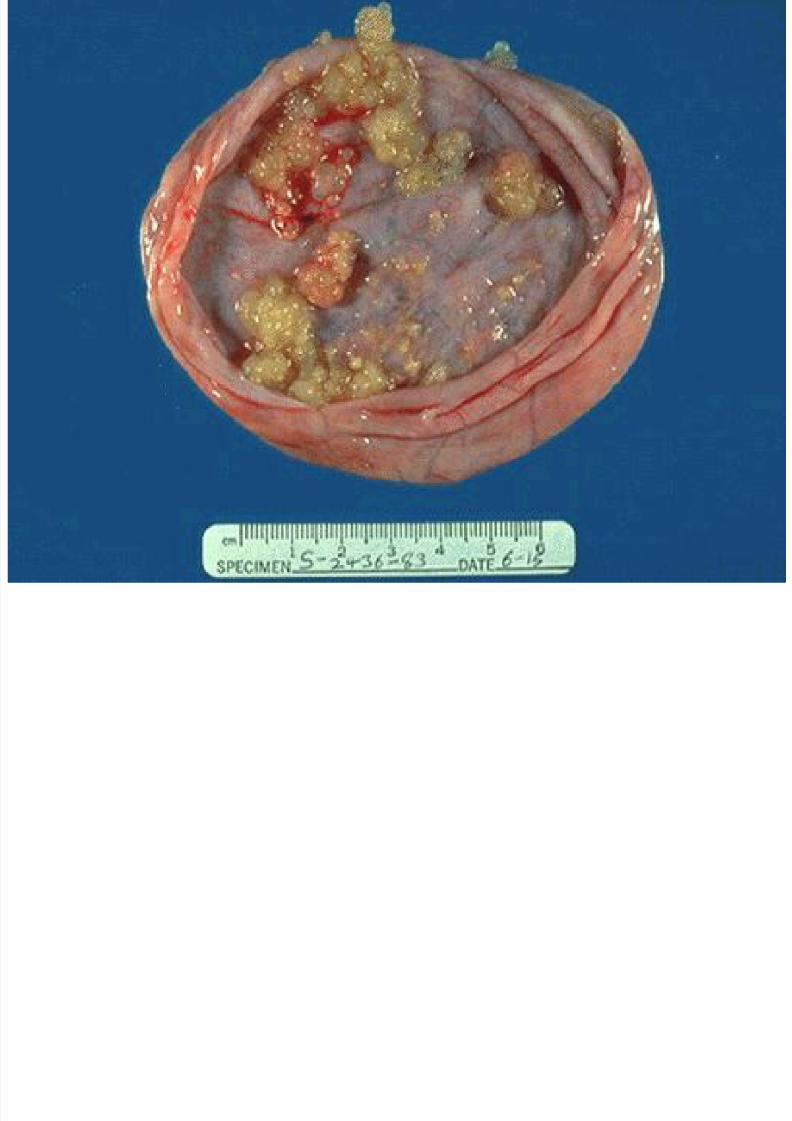
Benign epithel ial cystic tumors:
Cystadenoma :as adenoma with cysticcomponents.Papil lary cystadenoma : as above ( adenoma +cyst + but with papillary (finger like projection ).
28
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 29/174
29
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 30/174
30
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 31/174
31
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 32/174
32
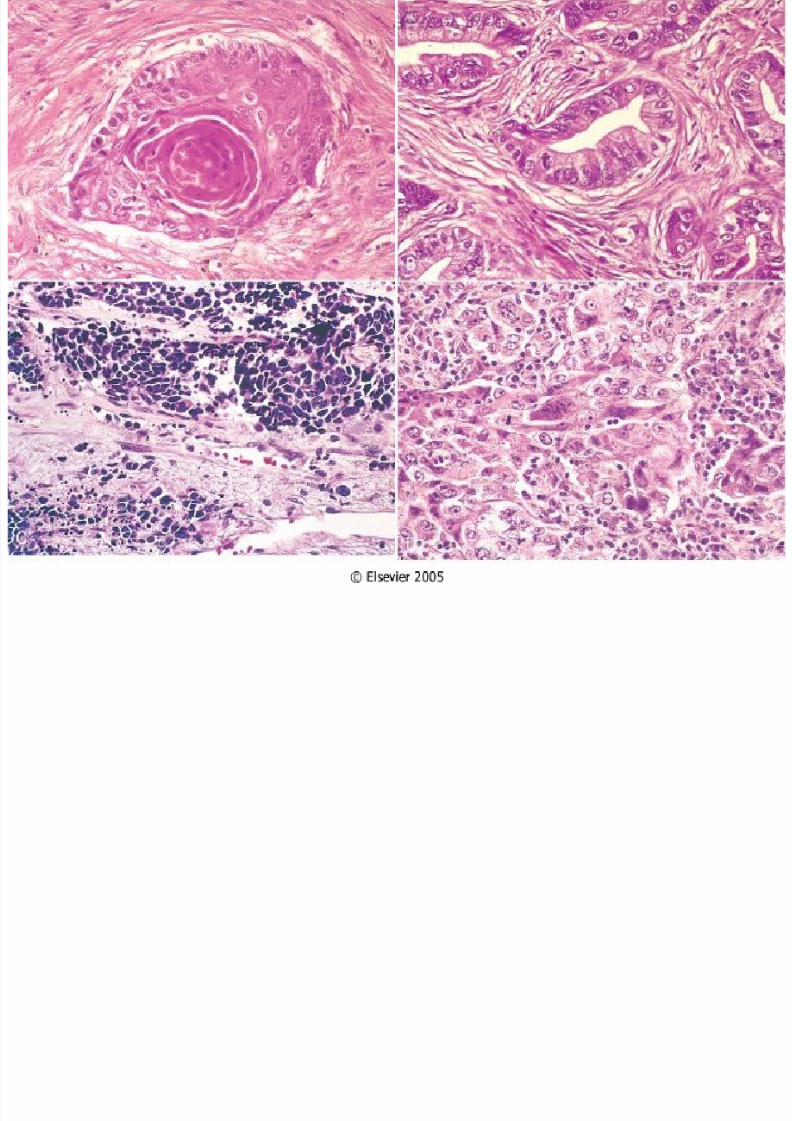
Malignant tumor of epithelial or igin: Carcinoma
Squamous cell carcinoma : would denote a cancer in
which the tumor cells resemble stratified squamousepithelium, arise in organs with squamous epithelial lining
:e.g. skin , mouth ,cervix, bronchus….etc
Adenocarcinoma :denotes a lesion in which the neoplastic
epithelial cells grow in glandular patterns , arise from
glandular origin, e.g.G.I.T. ,endometrium,breast, kidney,
thyroid…..etc .
Transitional cell carcinoma :arise from epithelial lining ofurinary bladder.
Small cell carcinoma :arise from neuroendocrine
cells.(mainly in lung ,although can arise in other tissue &
organs ) , so it considered as systemic disease .
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 33/174
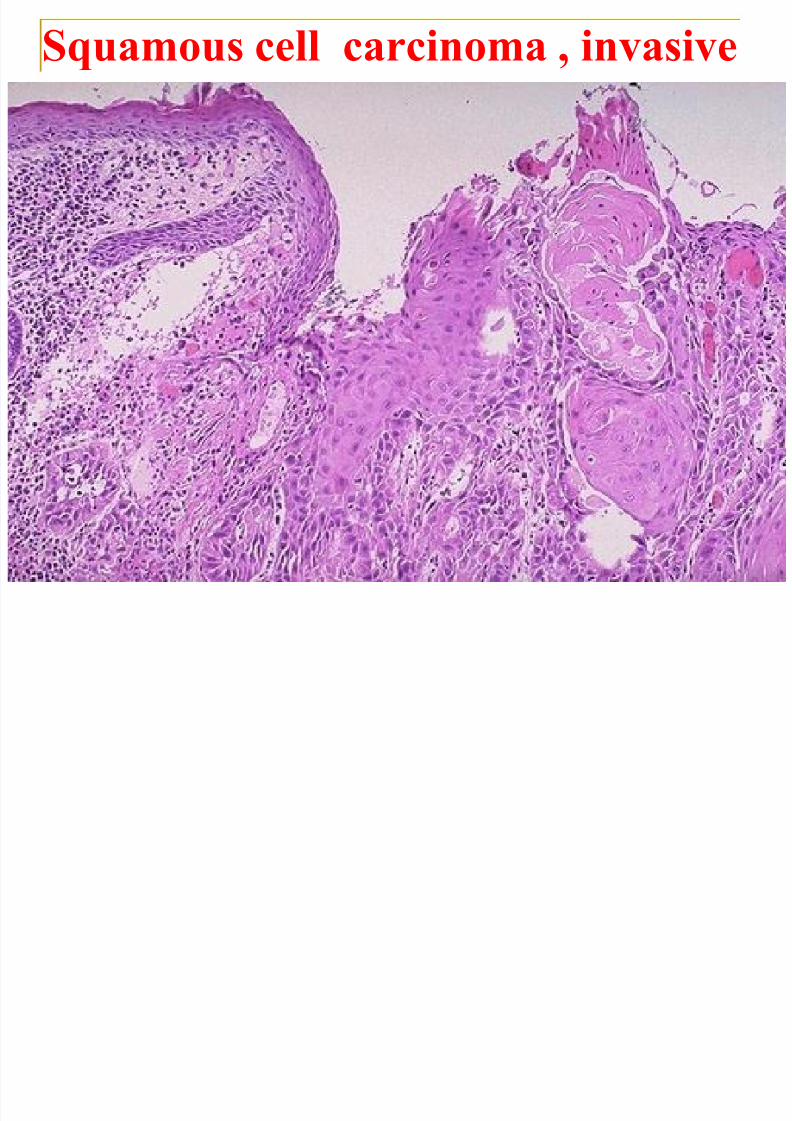
33
Squamous cell carcinoma , invasive
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 34/174
34
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 35/174
35
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 36/174
36
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 37/174
37
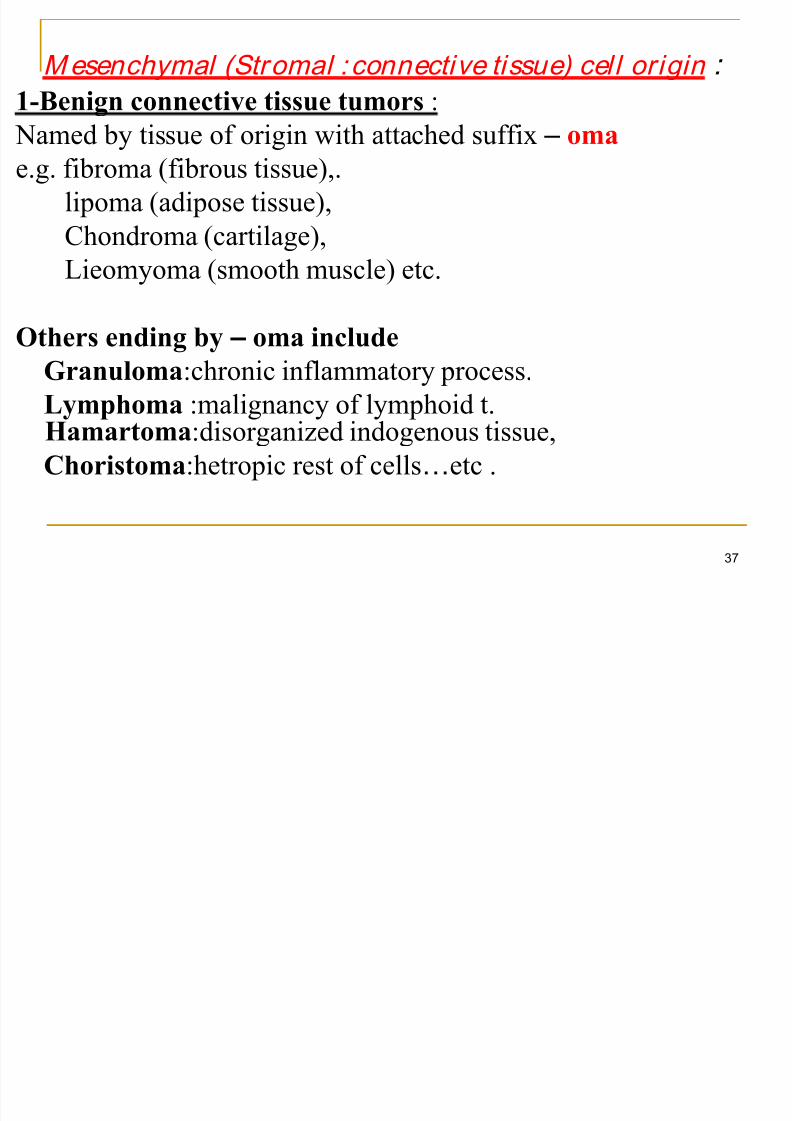
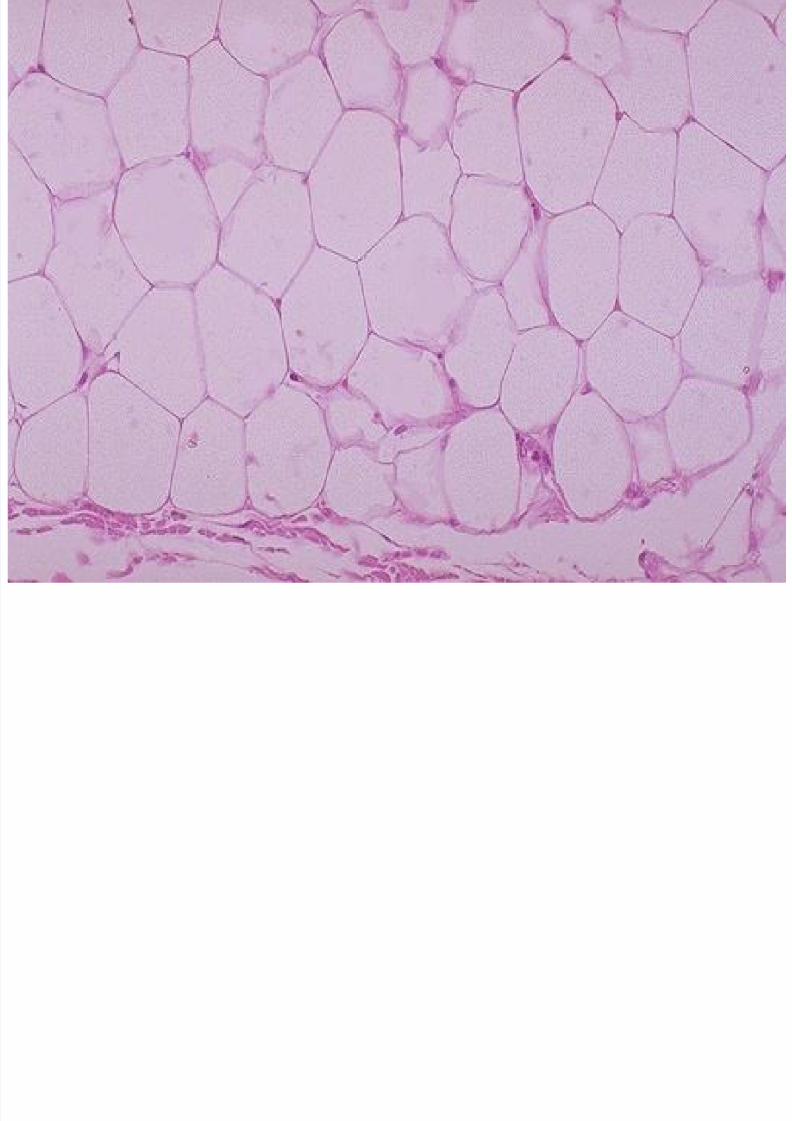
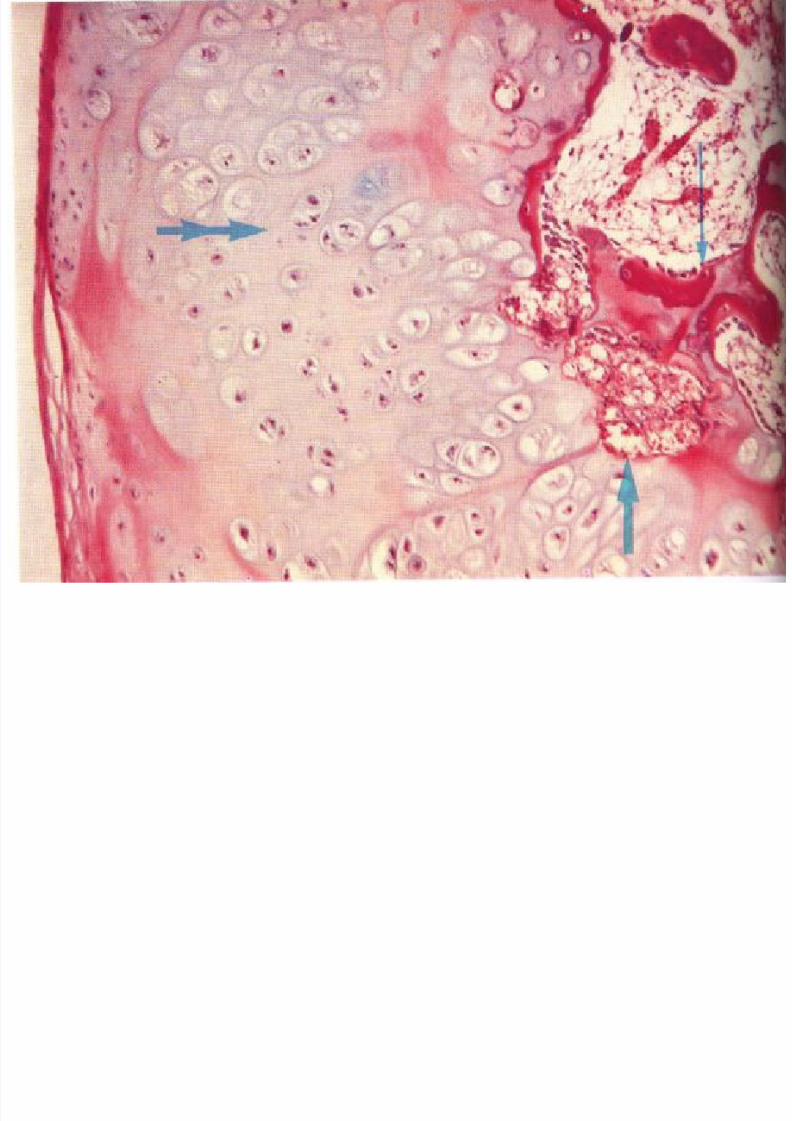
Mesenchymal (Stromal :connective tissue) cell origin :
1-Benign connective tissue tumors :
Named by tissue of origin with attached suffix – omae.g. fibroma (fibrous tissue),.
lipoma (adipose tissue),
Chondroma (cartilage),
Lieomyoma (smooth muscle) etc.
Others ending by – oma include
Granuloma:chronic inflammatory process.
Lymphoma :malignancy of lymphoid t.Hamartoma:disorganized indogenous tissue,
Choristoma:hetropic rest of cells…etc .
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 38/174
38
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 39/174
39
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 40/174
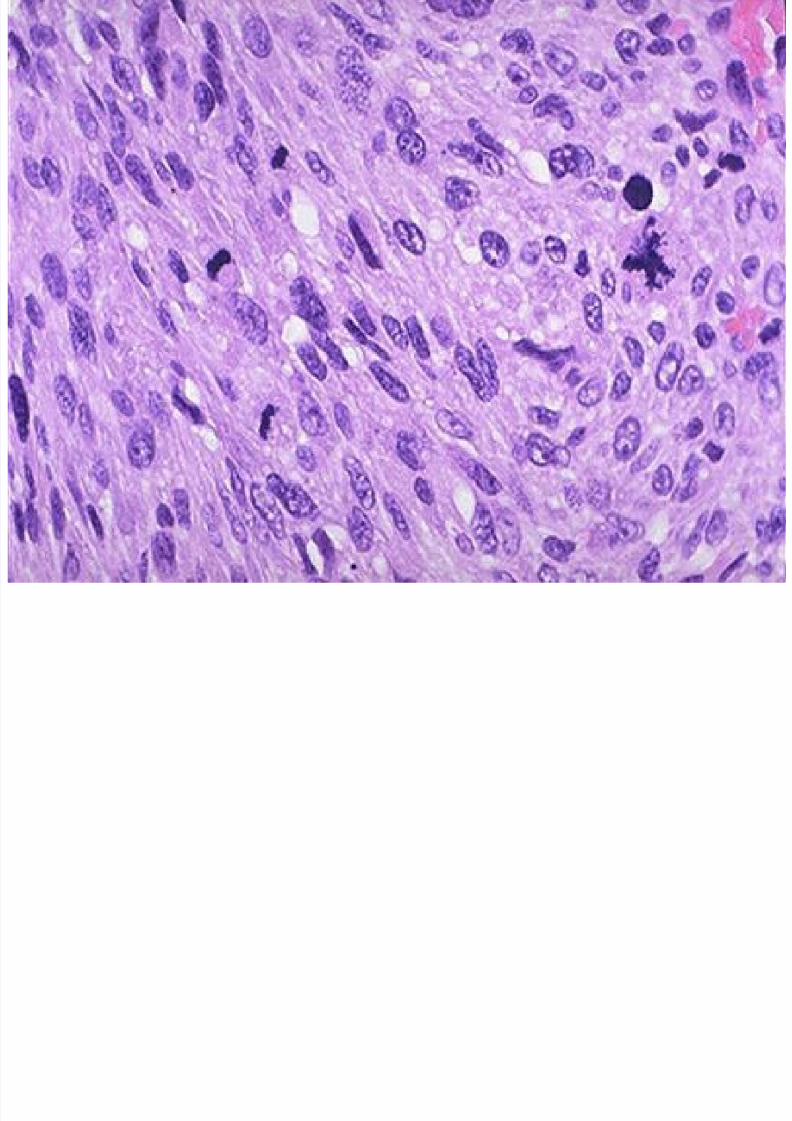
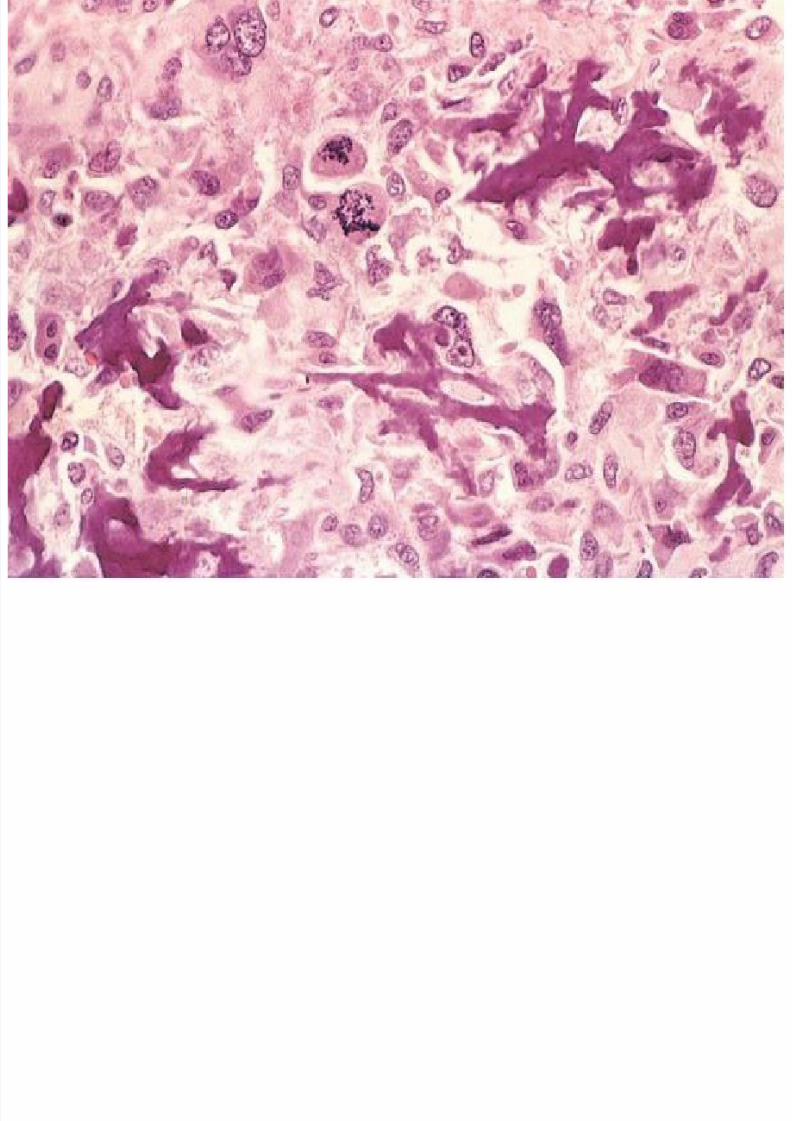
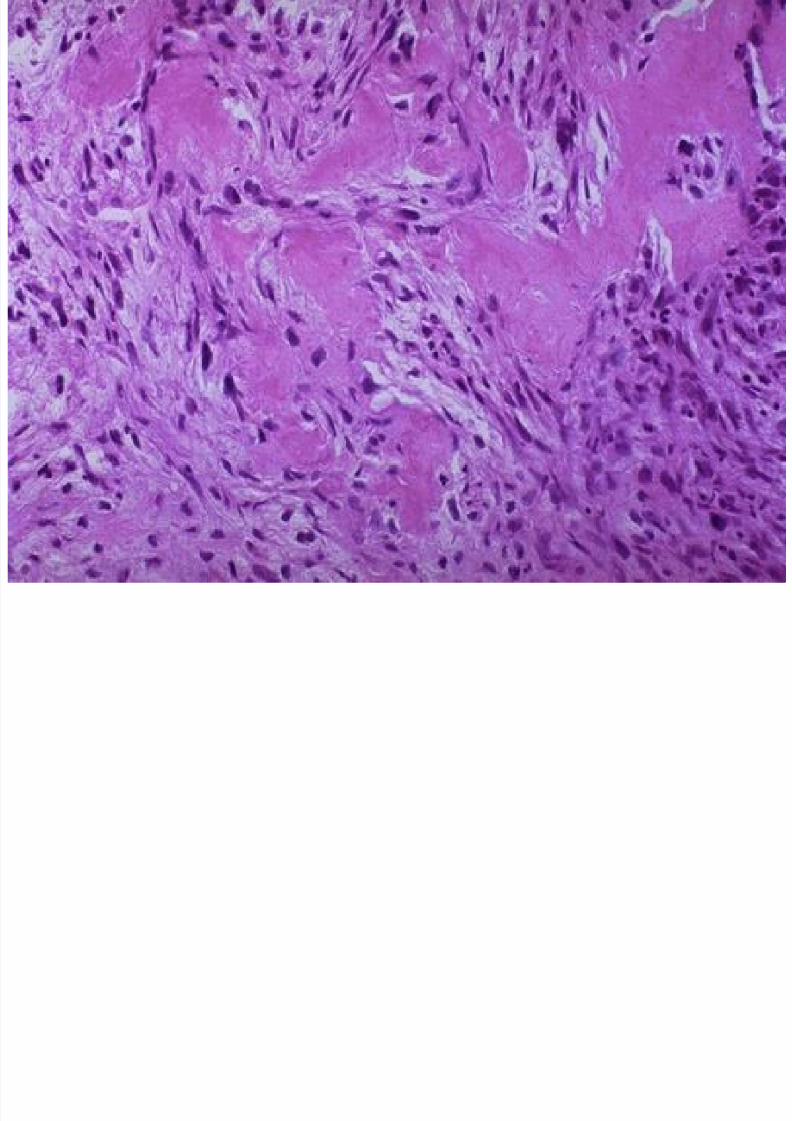
.2-Malignant connective tissue tumors: ( Sarcoma ) :
Prefix (origin)+ suffix (sarcoma) .e.g. Bone :Osteosarcoma ,
Adipose tissue : Liposarcoma,
Blood vessels : Angiosarcoma,Smooth muscle :Leiomyosarcoma,
Skeletal muscle :Rhabdomyosarcoma .
Cartilage : Chondrosarcoma .
40
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 41/174
41
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 42/174
42
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 43/174
43
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 44/174
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 45/174
45
*Some tumors have more than one paranchymal cell
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 46/174
46
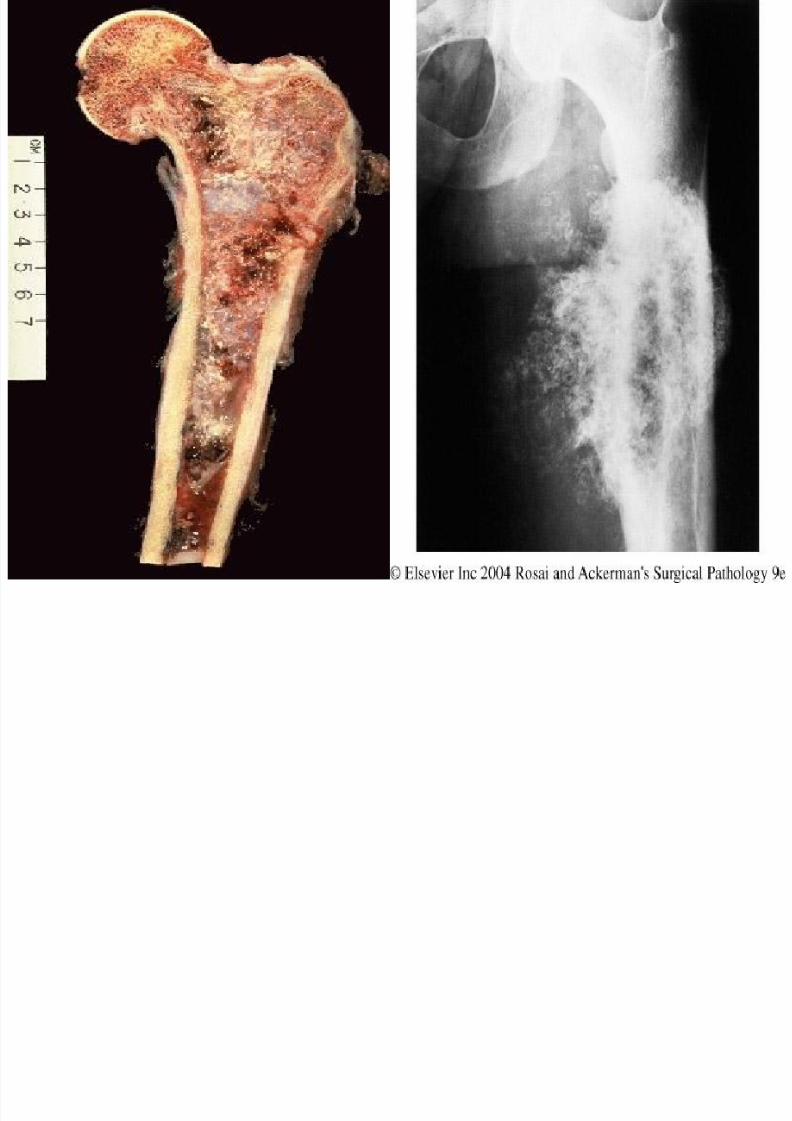
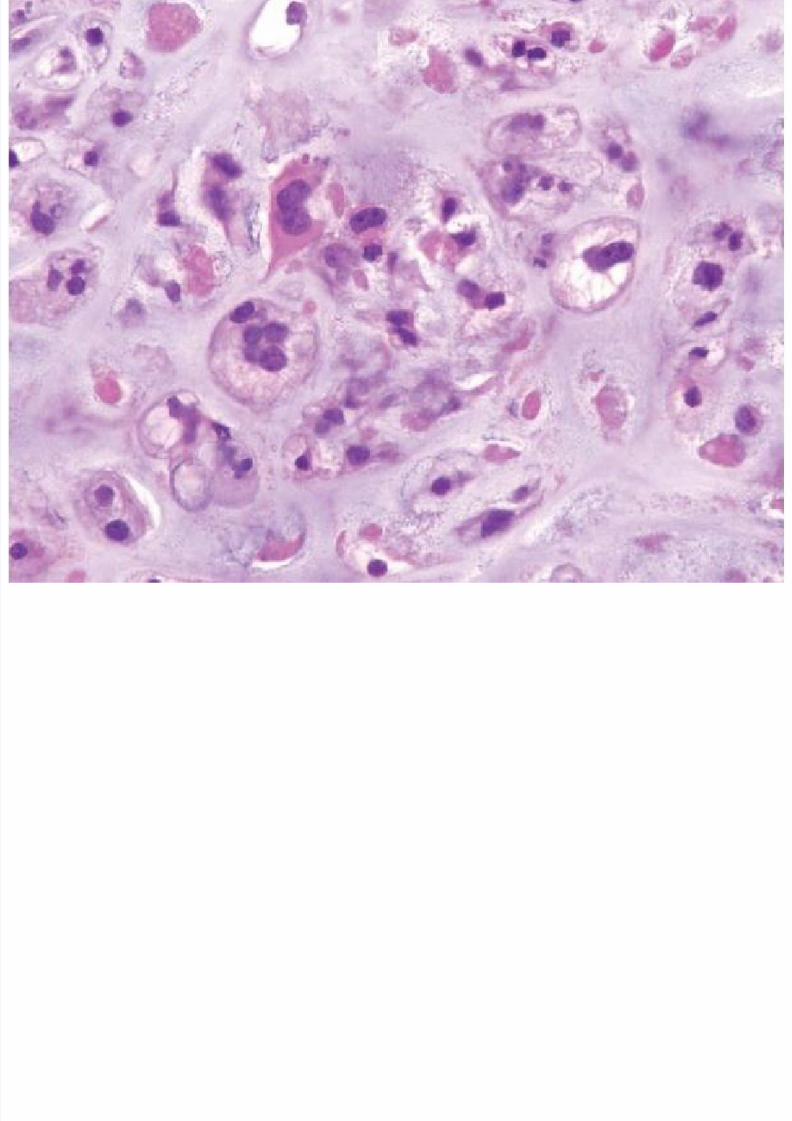
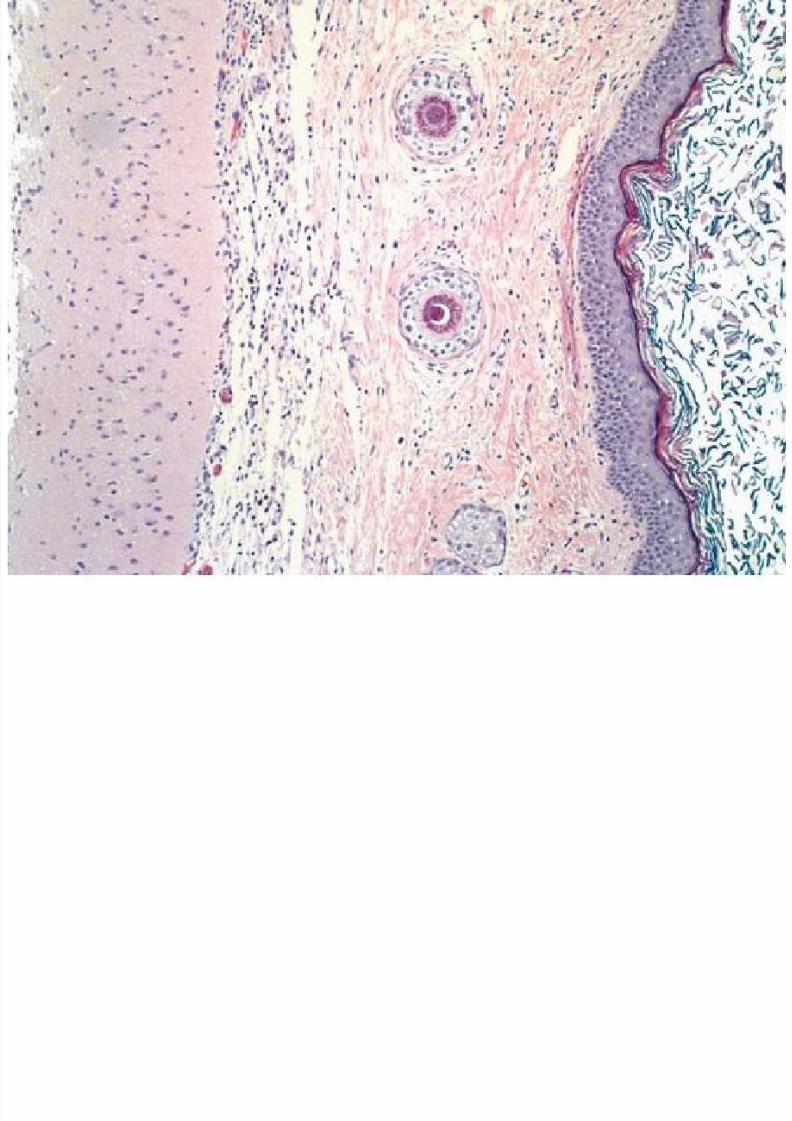
Some tumors have more than one paranchymal cell
type,these include tumors of Germ cell origin : able to
differentiate into 3germ layers (ectoderm , mesoderm &
endoderm).1-TERATOMA : Term applied for tumor with recognized
mature or immature cells or tissue representive of more
than one germ cell layer & some time all three (ectoderm ,
mesoderm & endoderm).
May be benign or malignant.
Contain skin ,sebaceous& mucus glands ,hair ,cartilage,
bone, respiratory epithelium, glial tissue…..etc. Usual location is ovary or testes (contain totipotential
cells=primitive cells) .
Stroma ovarii: ovarian teratoma with predominant thyroid
tissue (may undergo pathological change , .

8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 47/174
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 48/174
.
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 49/174
49
Teratoma pleomorphic adenoma
.
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 50/174
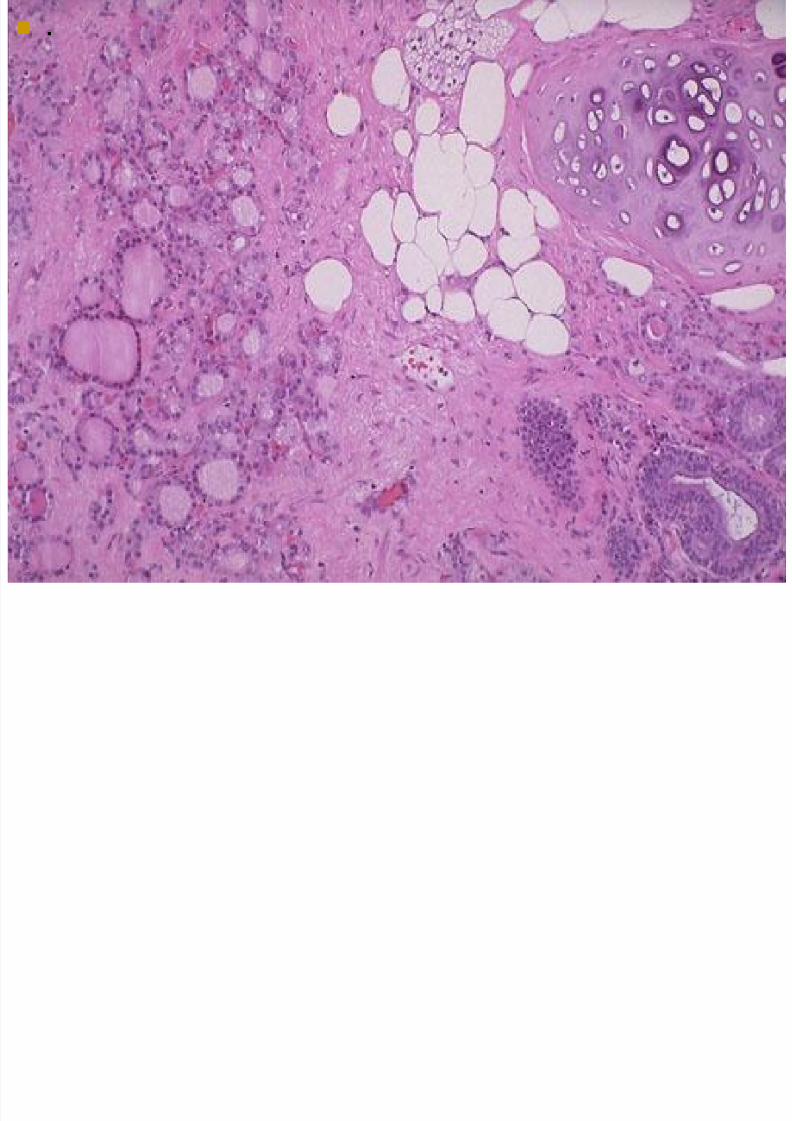
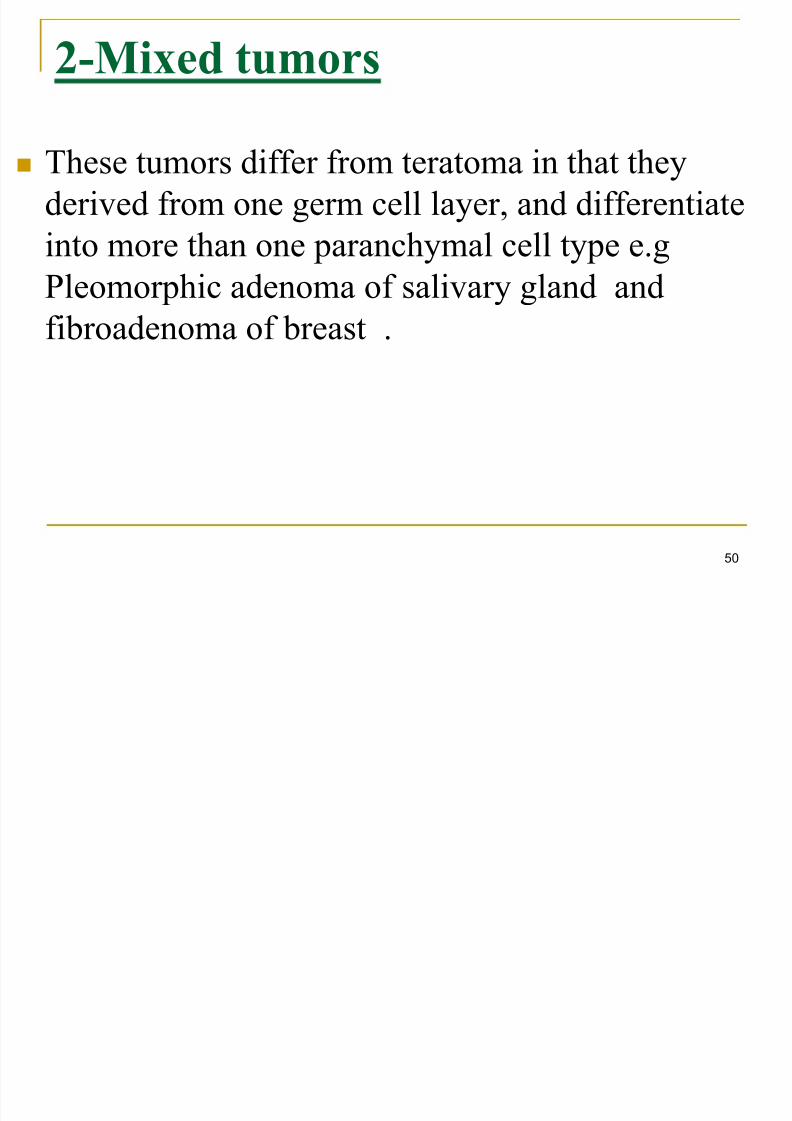
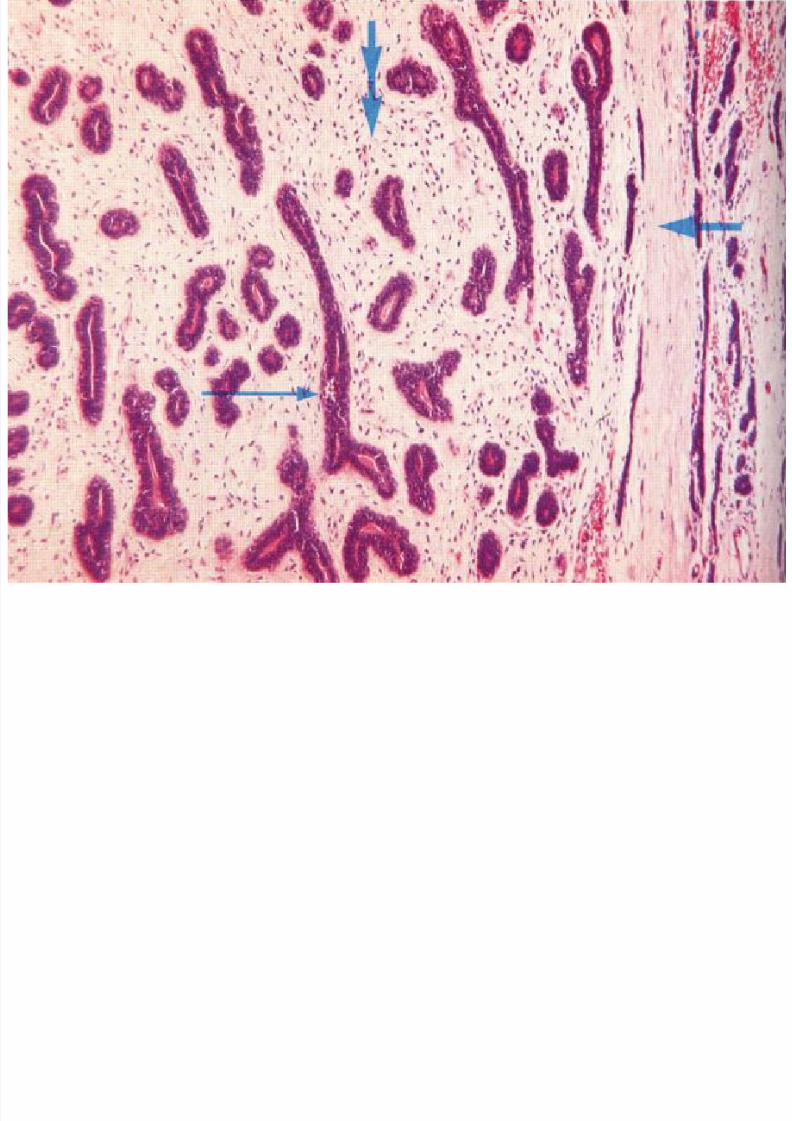
Mixed tumors-2
These tumors differ from teratoma in that they
derived from one germ cell layer, and differentiate
into more than one paranchymal cell type e.g
Pleomorphic adenoma of salivary gland andfibroadenoma of breast .
50
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 51/174
51
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 52/174
52
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 53/174
53
.Tumors of blood cells & lymphocytes :All tumors in this group
are malignant ( leukemia ,lymphoma , polycythemia rubra vera ).
Neural,gl ial cell& neural supporting structures tumor: Like glioma , neuroblastoma &meningioma.
Germ cell tumors : This include seminoma , teratoma &
choriocarcinoma .
Tumors of pr imitive fetal or igin :
Blastoma :(small primitive cells). e.g. Retinoblastoma
Nephroblastoma, Neuroblastoma, Medulloblastoma
HepatoblastomaNote : The great majority of these tumors are malignant.
Majority occur in infants & children
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 54/174
54
Non neoplastic masses :
1-Hamartoma : Tumor like malformation (mass or
nodule) in which there is abnormal mixing ofnormal native tissue components of the organ ,eitherin the form of change in quantity or arrangement oftissue elements: e.g. Lung Hamartoma ,most
haemangioma, melanocytic nevi.: usually developduring fetal development .
2-Choristoma : Mass composed of normal cells ortissue found in a wrong location ( Ectopia ) :
Different types of tissue, ectopic to the region. e.g.Meckle’s Diverticulum,(ectopic pancreatic &gastrictissue) , Salivary tissue in lymph nodes .
Both are present at birth & do not have malignant
potential
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 55/174
55
E i b i d lE i
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 56/174
Exception to above mentioned rules:Exceptions
include tumors that are always malignant such as :
Lymphoma: malignant tumor of lymphoid tissue .
Melanoma :malignant tumor of melanocytes .
Seminoma &dysgerminoma :tumor of primitivegerm cells.
56
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 57/174
57
-
How do benign tumor dif fer f rom malignant tumor
1-Differentiation & anaplasia: Extent to which the
transformed cells resemble their normal forebearsmorphologically &functionally.
2-Rate of growth : Correlates in general with their level of
differentiation ( slowly=well diff *rapidly =poorly diff)
3-Local invasion : benign tumor remain localize.
Malignant tumor :grow by progressive infiltration, invasion,
destruction & penteration of surrounding normal tissue.
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 58/174
.
4-Distant metastases: development of secondary
implants in site that anatomically discontinous with
primary malignant tumor, possibly in remote tissue
(absolute feature of malignant tumor).
5-Gross features :
Benign : smooth , capsulated , uniform color.
Malignant: irregular , no capsule ,variegated color.
58
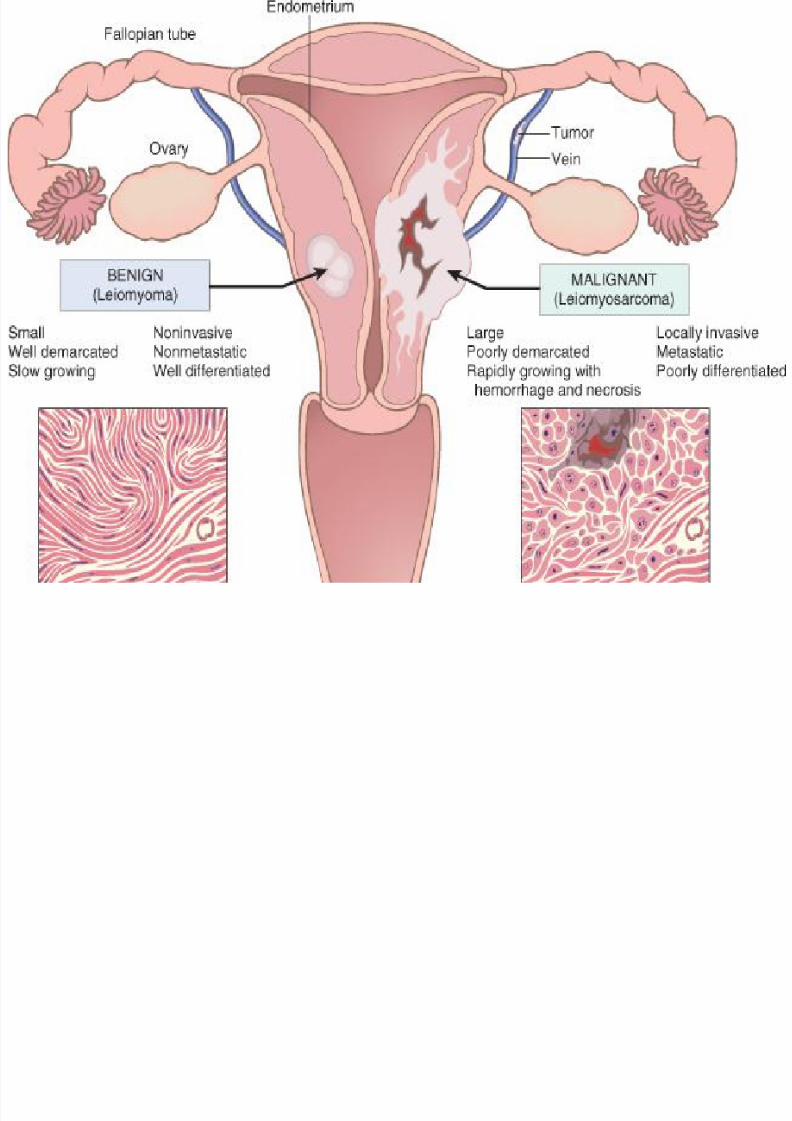
Benign versus malignant tumors
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 59/174
59
Benign versus malignant tumors
:Differentiation-1
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 60/174
60
:Differentiation - 1
- This indicates the degree of resemblance of the tumor
cell to its cell of origin,functionally &morphologically.- In most benign tumors constituent cell closely
corresponding to normal cells :e.g - Cells of a lipoma
may look exactly like normal fat cells.
- Malignant tumors display a range of differentiation,
which form the basis of tumor grading (well , moderate
, poorly) :
-Malignant tumor can be extremely well differentiated -e.g. a well differentiated liposarcoma or anaplastic in
which tumor cells lack of differentiation .
Ab l h (di i i f iD l i
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 61/174
61
: Abnormal growth (disorganization of tissueDysplasia structural &cytological) which may precede malignancy.
Disorder growth & maturation of cells that are not normal , but are
not obviously malignant .
Considered as precursor of invasive malignancy .
Process of gradual loss of differentiation .
Complete loss of differentiation ANAPLASIA
Differentiation features include functional &morphological:
- Formation of glands( morphology).
- Formation of squamous nest ( morphology).
- Production of keratin ( Functional ).- Formation of mucin secretion (functional).
- Formation of osteoid ( functional).
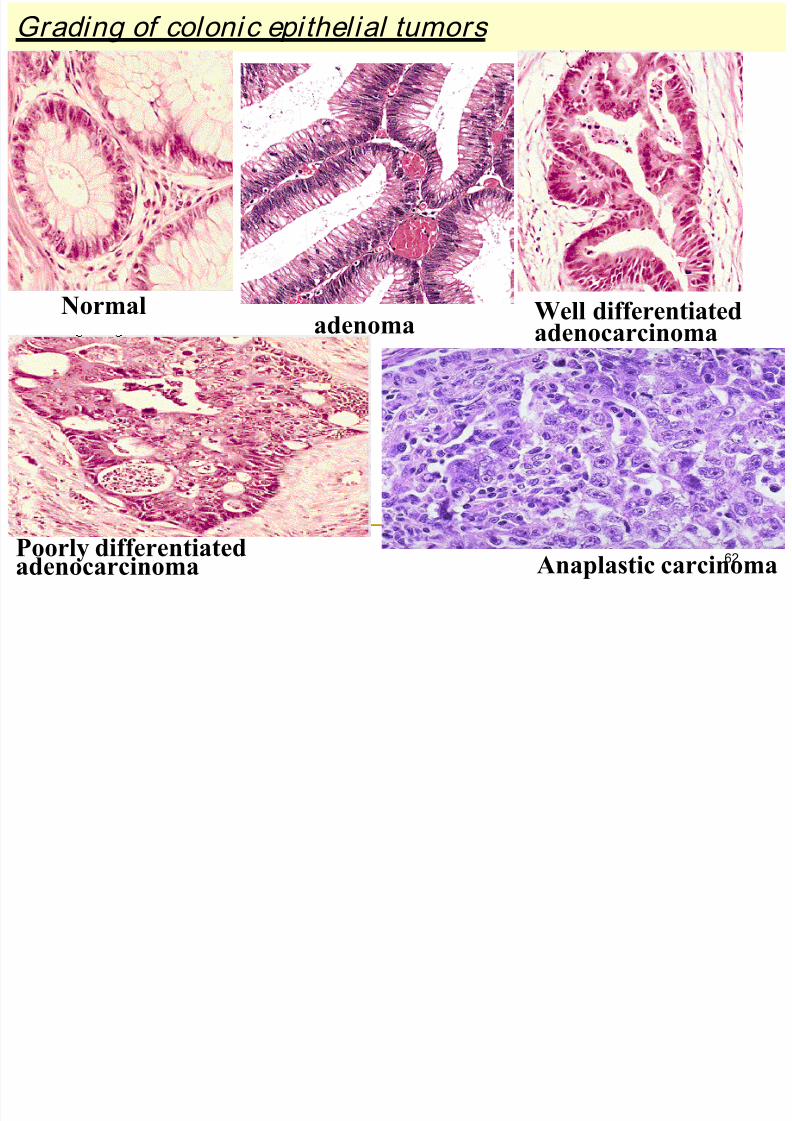
Grading of colonic epithelial tumors
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 62/174
62
Normaladenoma
Well differentiatedadenocarcinoma
Poorly differentiatedadenocarcinoma Anaplastic carcinoma
Cytological Features of Dysplasia
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 63/174
63
Cytological Features of Dysplasia 1-I ncreased nuclear size: N/C ratio(nuclear/cytoplasmic)
2- Pleomorphism :Variation in nuclear & cell size .
3-Loss of cell differentiating features (Giant cells & bizarre
cells with multiple nuclei ).
4- Hyperchromatism :Increased nuclear DNA content .
5-Mitosis : often numerous : increase proliferative activity &
distinctly atypical (tripolar ).
6-Celluarity :increase degree of cellularity ..
7-Loss of polar ity in an epithelial surface (loss of orientation
&dissary of tissue architecture).
8-Prominent nucleoli .
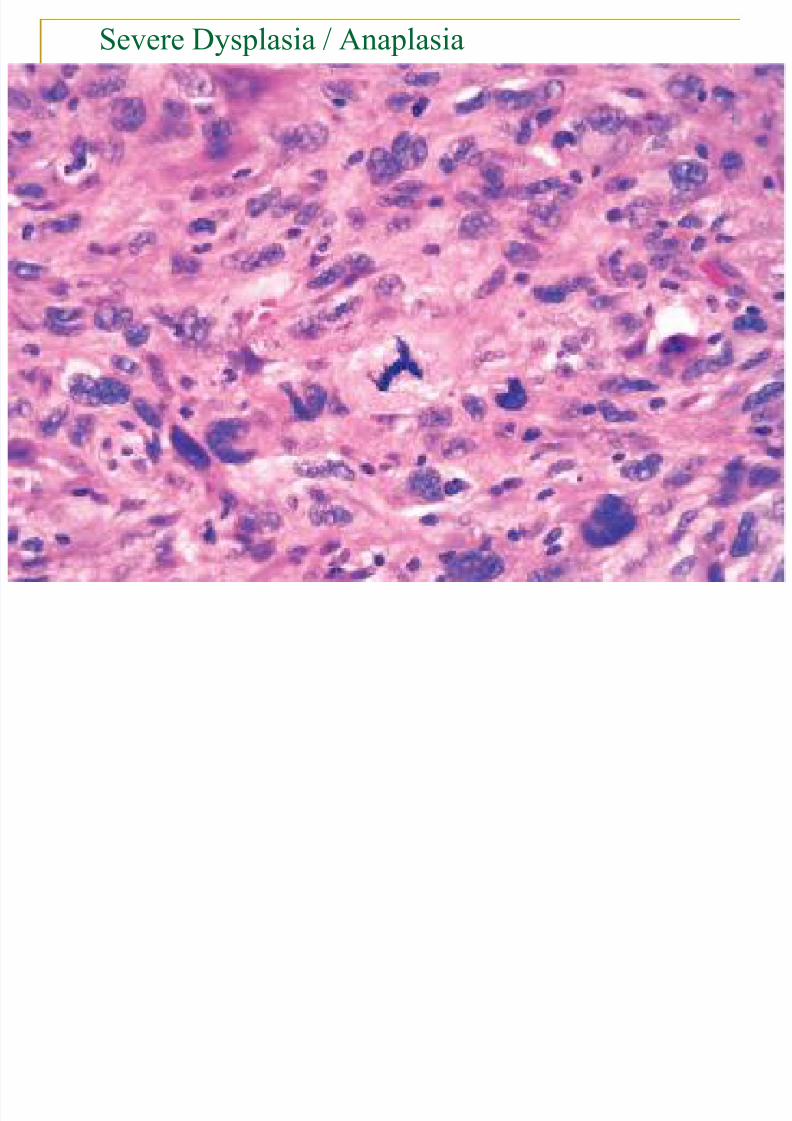
Severe Dysplasia / Anaplasia
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 64/174
64
Severe Dysplasia / Anaplasia
:I ntraepithel ial Neoplasia
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 65/174
65
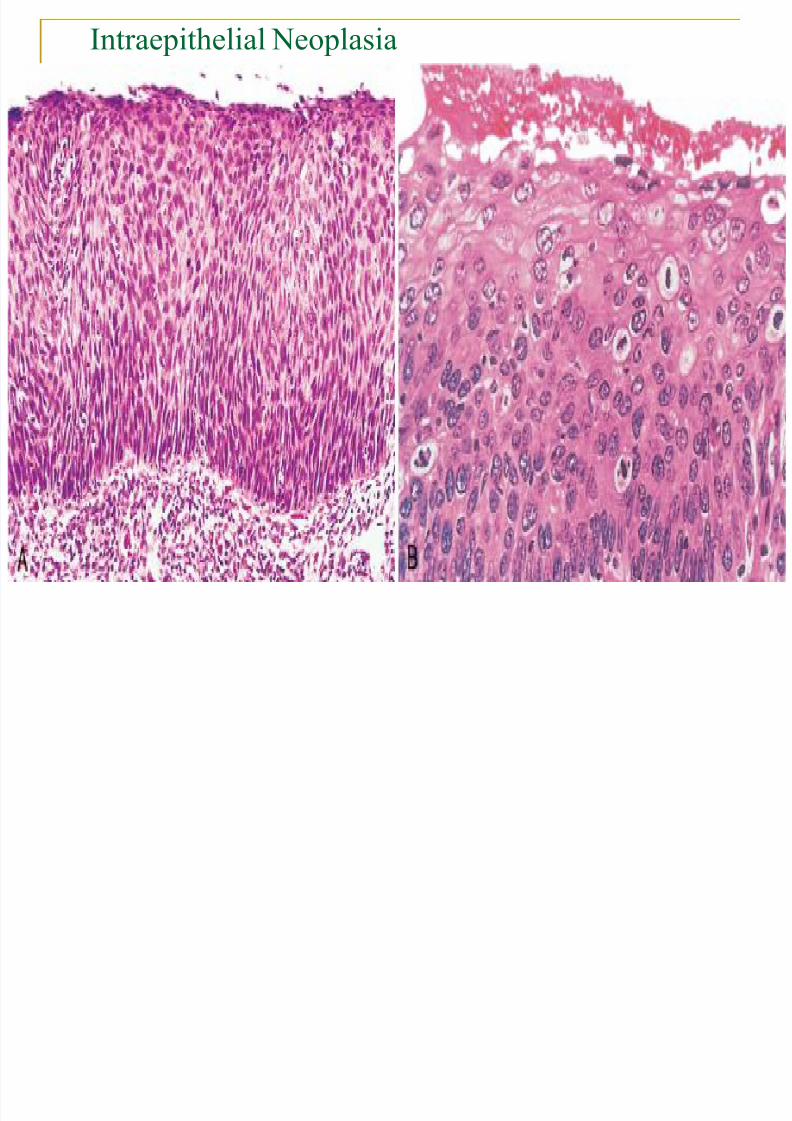
:I ntraepithel ial Neoplasia Dysplasia involving an epithelial surface
Low grade & High grade.
High grade dysplasia ,limited by intact epithelial
basement membrane CARCINOMA IN SITU.
Not all dysplasias progress to higher grade or
carcinoma in situ.
Not all carcinoma in situ progress to invasive CA.
Mild to moderate degrees of “dysplasia”can be seen
in reactive & inflammatory lesions.
Dysplasia can regress.
Intraepithelial Neoplasia
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 66/174
66
Intraepithelial Neoplasia
: Based on le el of differentionGrade of tumor
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 67/174
67
:: Based on level of differentionGrade of tumor
Grading :Is the attempt to assign a rough numerical value
( Score of differentiation ) to the extent of histologicaldeviation from the normal. This indicates the degree of
resemblance of tumor cells to cell of origin and is
always based on microscopic criteria.
Grade I : Well differentiated tumor.
Grade II :Moderately differentiated tumor.
Grade III : Poorly differentiated tumor.
Grade IV : Anaplastic tumor.
:hRate of growt-2
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 68/174
68
: h Rate of growt 2
Most cancers grow faster than benign tumors .
Rate of growth usually correlates with level of
differentiation.
May be rapid in some benign tumors .
Some tumors may shrink in size (lieomyoma & pituitary
adenoma). Some malignant tumors may outgrow their blood
supply ( choriocarcinoma).i.e rapidly growing tumors
may develop areas of ischemic necrosis because outgrow
their blood supply .
Some cancers are hormone sensitive , their rate of
growth may be affected by variation in hormone level
associated with pregnancy , menapause like breast cancer
:Local invasion-3

8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 69/174
69
:Local invasion 3
Second most important feature distinguishing
malignant tumors after metastases. Benign tumors frequently have a capsule.
Not all benign tumor are encapsulated
(lieomyoma)
Malignant tumors progressively invade
(infiltrative ) & destroy surrounding normal
tissue: e.g. Breast cancer infiltrating
skin,muscle.
Basal cell carcinoma of skin infiltrating nerve
:Metastasis-4
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 70/174
70
: Metastasis 4
Metastasis is the absolute criteria of malignancy .
Spread of malignant tumors to distant sites not
contigious with the main primary tumor ( secondarydeposit or metastatic foci ).
All tumors can potentially metastasize except
BASAL CELL CA ., GLIAL TUMORS Metastasis is often proportionate to the size and grade
of the primary tumor
Routes of metastases:
1-Lymphatics. 2-Blood vessels.
3-Seeding within body cavities.
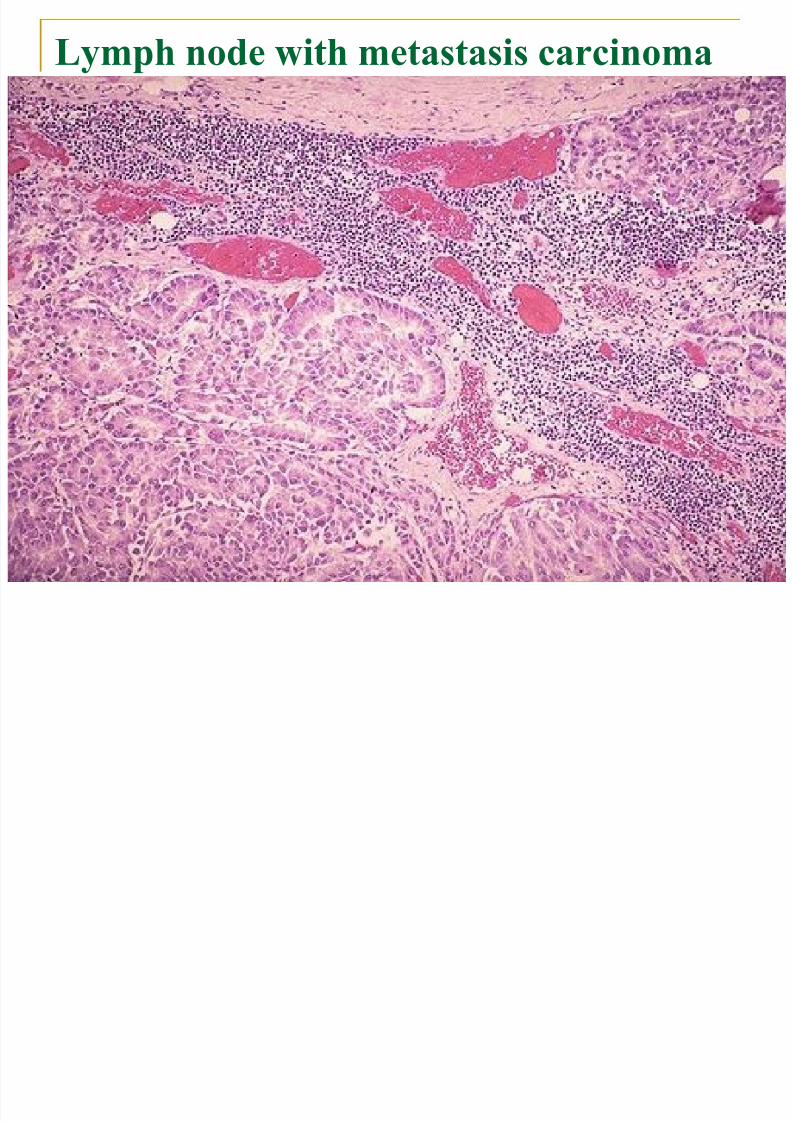
Lymph node with metastasis carcinoma
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 71/174
71
Lymph node with metastasis carcinoma
:Lymphatic Spread1
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 72/174
72
:Lymphatic Spread - 1
Invasion of lymphatic vessels followed by spread oftumor to regional lymph nodes , ultimately to othersites in the body.
More characteristic in Carcinoma than sarcoma.
Not all enlarged lymph nodes located at the sites of
drainage of a malignancy signifies a metastasis(immune response in form of lymphoid hyperplasisa
Spread follows the anatomical route of drainage e.g. : - Breast cancer in upper outer quadrant
axillary L.N.- Lung Carcinoma - Peribronchial hilar Paratracheal lymph nodes.
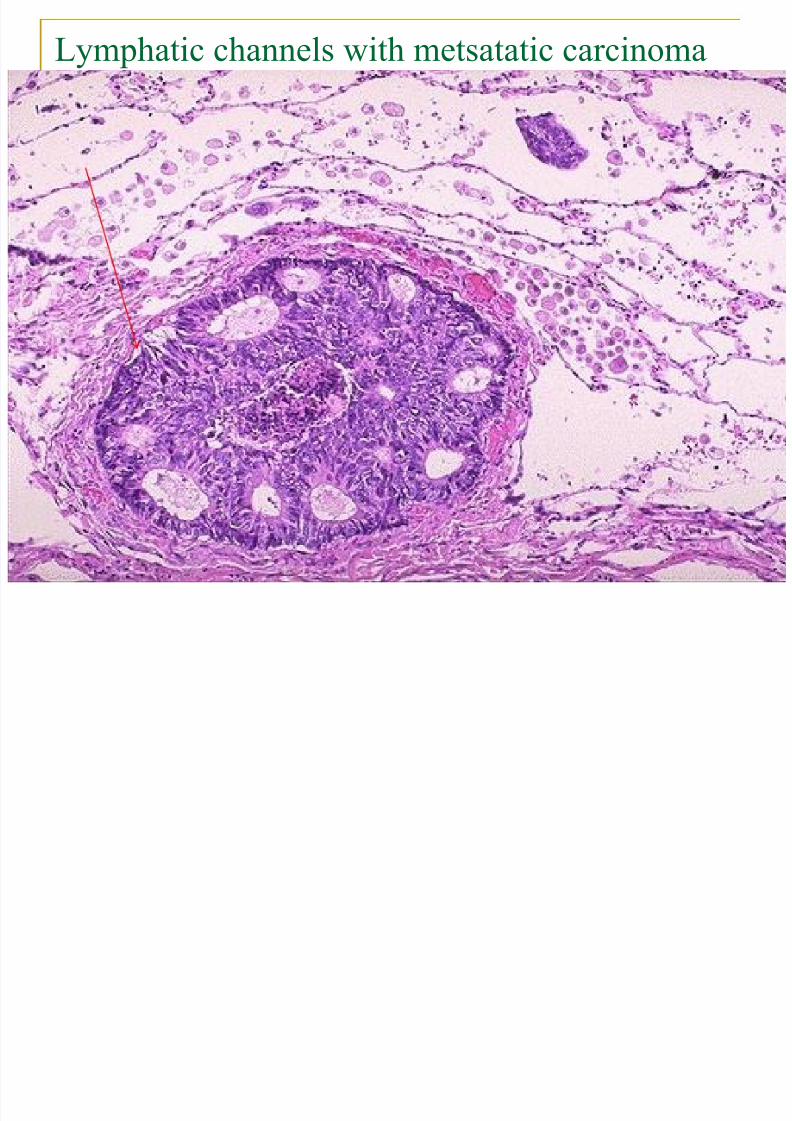
Lymphatic channels with metsatatic carcinoma
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 73/174
73
Lymphatic channels with metsatatic carcinoma
Hematogenous spread :2
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 74/174
74
Hematogenous spread : - 2 Usually venous (veins are more readily ).
More characteristic of Sarcoma , although in later
stages of carcinoma they also use Blood Vessels. Lung & liver are the commenest site of haematogenous
spread , because they receive dual circulation ( thesystemic &portal venous blood )respectively .
Other major sites are the bones & brain (wellvascularized organs with abundant blood supply).
Certain carcinomas invade veins early e.g.
RENAL Carcinoma renal vein IVA
Hepatocellular Carcinoma Portal &Hepatic v.
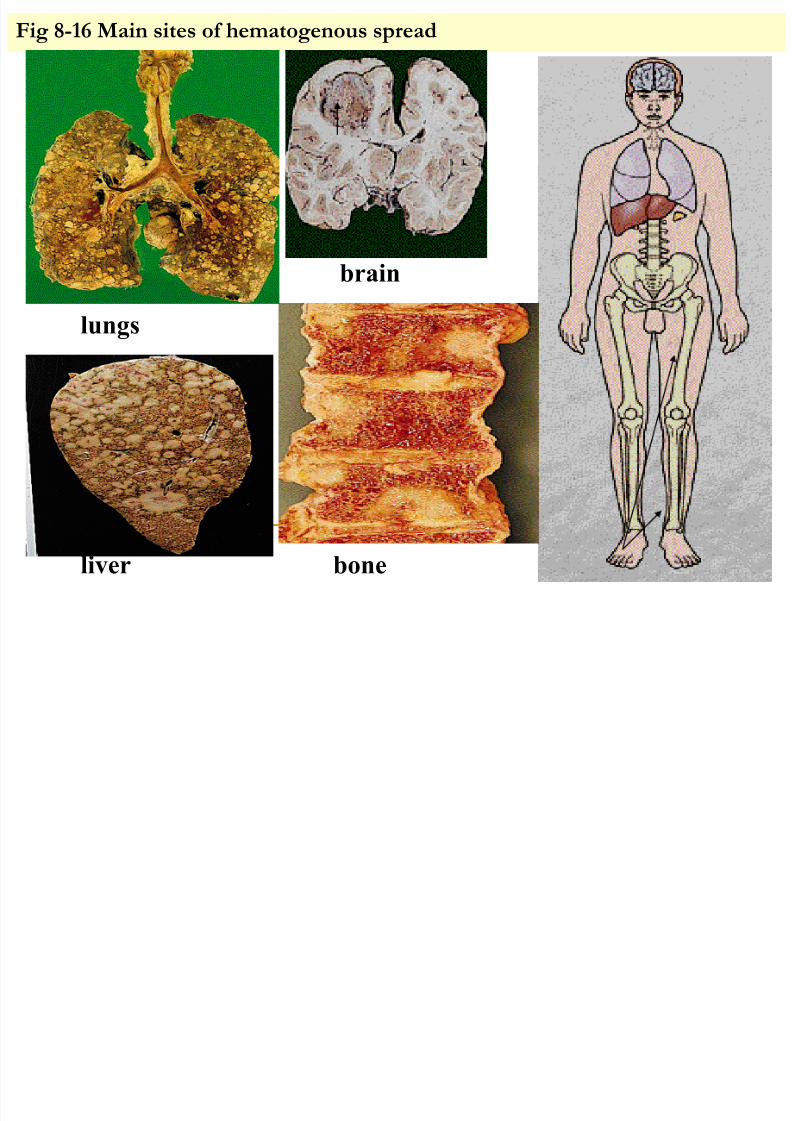
Fig 8-16 Main sites of hematogenous spread
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 75/174
75
brain
lungs
boneliver
3- Transcelomic spread :
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 76/174
76
3- Transcelomic spread : By seeding of surface of cavity :Tumor cells enter
the cavities & floate in the serous fluid to attached
on the surface of peritoneal cavity .
Within peritoneal or pleural cavity
e.g.: - CA of upper lobe of lung to lower lobe.
- CA of stomach to ovary (krukenburge tumor).
- CA of ovary spread widely through peritoneal
surface (mucinous adenocarcinoma spread to
peritoneal cavity to give pseudomyxoma peritoni )- CA of colon across peritoneum to S.I.& colon
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 77/174
77
:Staging of Tumor
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 78/174
78
: Staging of Tumor
This indicates the extent of spread of the tumor.
It based on correlating Clinical data ,investigative procedures (radiological ) and pathological findingappearance of tumor have to be used to assess it.
It depends on :
* Size of tumor (local infiltrations).* Regional lymph node involvement.
* Metastases to distant organs .
Prove to be of greater cl inical value , when compared
with grading ( more valuable for prognosis ).
Both staging & grading of tumors are valuable for the
1- Determination of prognosis.
2- Planning of therapy .
TNM Staging System :
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 79/174
79
Stag g Syste
T : Size and extent of primary tumor(1-4).
N : Presence and extent of lymph node
involvement ( 0-3).
M : Presence or absence of distant
metastasis
e.g.T1,N1, M0 ( Small tumor that hasmetastasized to lymph nodes &distant site ).
-----------------------------------
Others: AJC(American Joint Committee) staging system (0-IV)
Duke’s staging for colonic CA
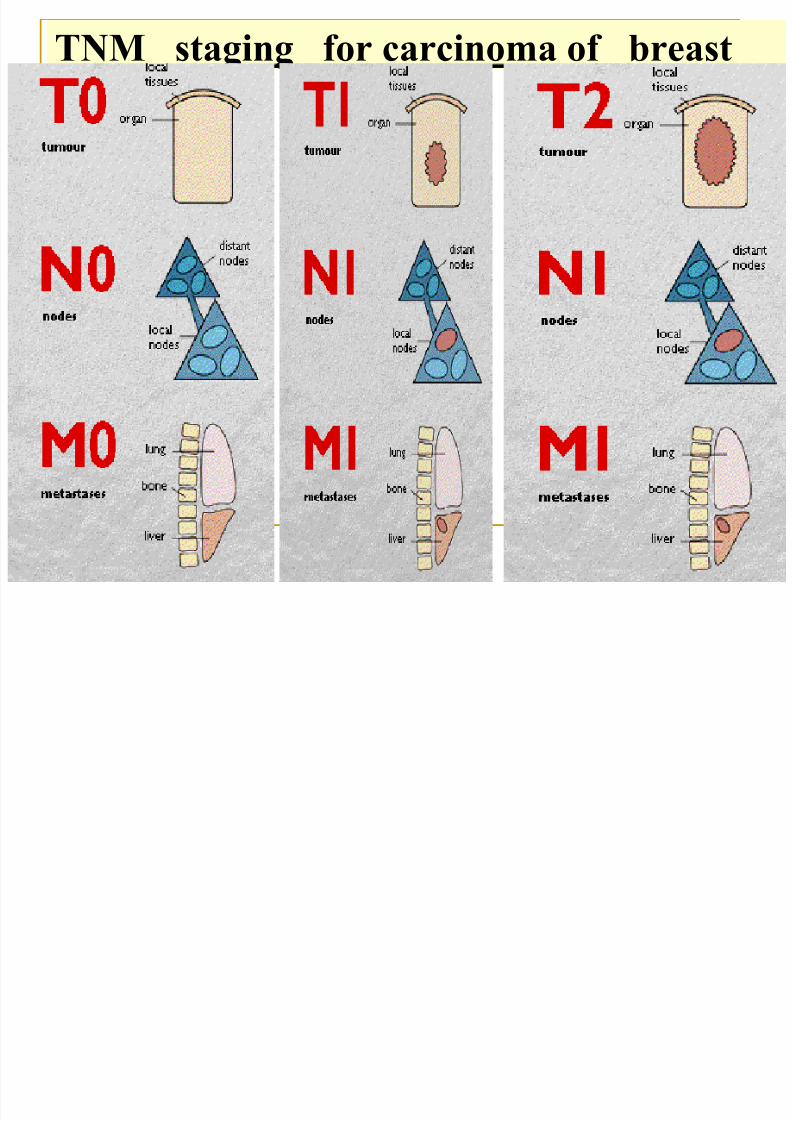
TNM staging for carcinoma of breast
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 80/174
80
TNM staging for carcinoma of breast
:Tumor Therapy
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 81/174
81
: Tumor Therapy
Staging, and to a less extent, grading, affect therapy :
1- Surgical excision .
2- Radiotherapy .
3- Chemotherapy .
4- Immunotherapy .
5- MULTIMODALITY of treatment .Prognosis :
This indicates the final outcome of the disease in terms of5year or 10 year survival.
This is influenced by :Tumor Type e.g. Lung CA versus Lip CA
Tumor Grade & Stage.
Host reactions
:EPIDEM IOLOGY OF CANCER
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 82/174
82
Cancer epidemiology deals with the occurrence of tumors inhuman populations , by study the incidence , prevalence &
mortality .Epidemiologist are trying to identifyenvironmental , genetic causes of cancer , thus contribute to
better diagnosis ,treatment and prevention .Epidemiologydata may point to a cause & effect relationship between a
cancer and potential carcinogen .In Iraq males the comments cancers are those of lung ,
bladder , larynx , non Hodgkin lymphoma & leukemias .
In Iraq females , breast cancer , non Hodgkin lymphoma ,
leukemias , CNS tumors , lung cancers.
Incidence :is the number of new cases of a specific registered

8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 83/174
83
. over a specified period in a defined population .Incidence may
be related to ethnic &geographic differences in community .
Prevalence :Is the number of all cases of cancer – both new &old registered within a defined population at a given point in
time.
Mortality : Is the number of deaths from a given form of cancer
during a specified period of time in defined population .I ncrease incidence : lung carcinoma in female ( smoking)
:Prostate carcinoma (PSA test) : early DX.
:kaposi sarcoma : homosexual AIDS person.
Decrease incidence : gastric carcinoma ( food refrigeration).
:cervical carcinoma (pap smear – preinvasive)
INFECTIONS & CANCER
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 84/174
84
INFECTIONS & CANCER
1-Epstein-Barr infection (EBV)-Burkitt
lymphoma &nasopharyngeal carcinoma.
2-Viral hepatitis B&C :Hepatocellular carcinoma
3-Humen papilloma virus : Uterine cervix
carcinoma .
4-AIDS (HIV) : Lymphoma &kaposi sarcoma.
:Geographic location - 1
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 85/174
85
g p
Esophageal CA -- High in Iran &north of iraq.
Gastric CA -- High in Japan Skin CA------ High in New Zealand
Hepatocellular CA --- High in China &south east Asia.
Breast CA , Prostatic CA ,Colorectal CA ---- High in USA
Significantly affect the occurrence:Environment factors - 2
of specific forms of cancers in different parts of the world.
* Diet: e.g :gastric cancers in Japan & USA.
* Occupation :e.g : anyline dye with bladder cancer.
* Sunlight e.g : melanoma in Australia .
* Personal habits e.g : cigarette with lung cancer.
:Age-3

8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 86/174
86
:Age 3
In general , cancer incidence ≈ AGE : Cancers is most
common in those over 55 years of age( fact pointing that
cancer evolution requires multiple independent events,
apparently taking place over along period of time e.g.
prostatic carcinoma & lung carcinoma .
Certain cancers occur more in chi ldren less than 5yearsAcute Leukemia ,Lymphoma , CNS Tumors
(retinoblastoma ,neuroblastoma),soft tissue Sarcomas
(rabdomyosarcoma).
Adolescence age tumors :Osteosarcoma , Ewing sarcoma
, Medulloblastoma .
Biphasic age incidence : Hodgkin lymphoma ( 20 & 60 ).
4- Hereditery :
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 87/174
87
Hereditary play a role in the development of cancers even in the
presence of clearly defined environmental factor Usually well
defined inheritance & phenotype : 1-Inherited cancer syndromes:
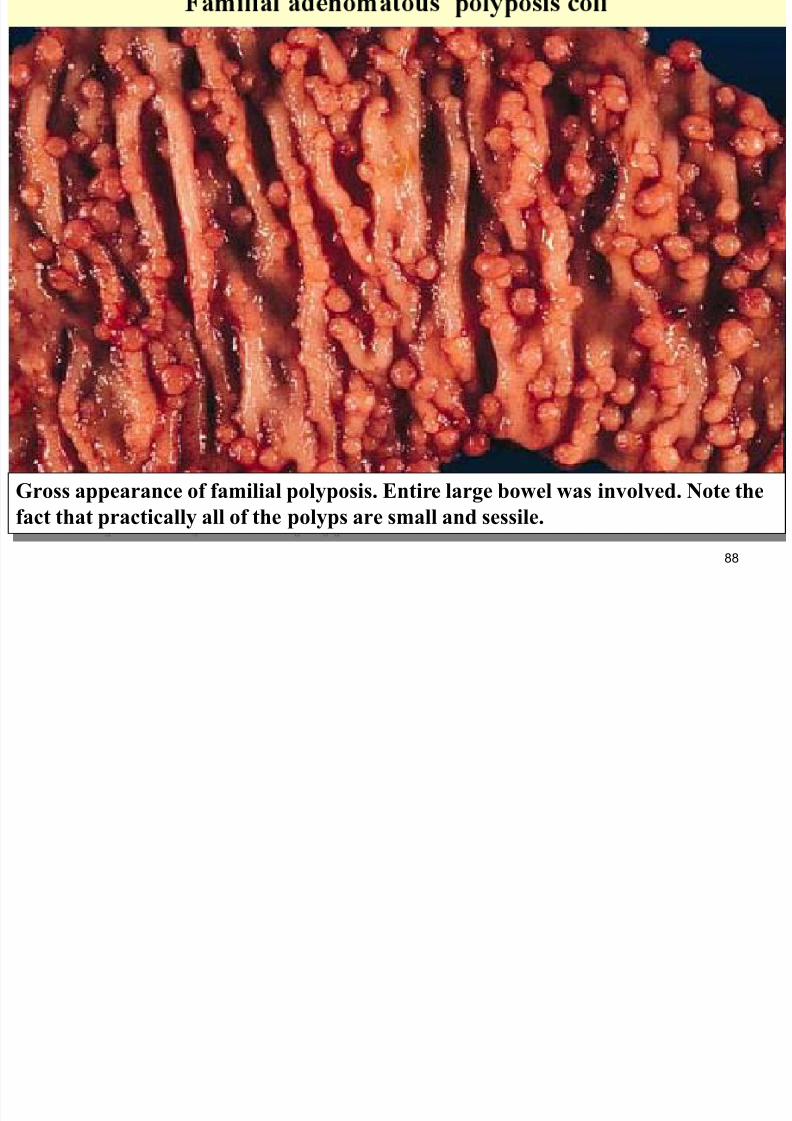
- Familial Adenomatous Polyposis Coli & - MEN Syndrome
2- Autosomal recessive syndrome of defective DNA repair: - -
Xeroderma Pigmentos &- X linked immune deficiency:due togenetic defect of nucleated excision enzyme lead to increase
susceptibility to UV irradiation .
3-Familial cancer :Familial clusters of specific forms of cancers,
but the transmission pattern is not clear (breast , colon ,brain &
ovary ). Younger age groups, multiple or bilateral, two or more
family members are affected. Some linked to inheritance of
mutant genes e.g. BRCA-1
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 88/174
88
Gross appearance of familial polyposis. Entire large bowel was involved. Note the
fact that practically all of the polyps are small and sessile.
A i d P l ti diti
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 89/174
89
Acquired Preneoplastic conditions :
These are certain clinical conditions that are associated with increased
risk for CA and most are related to rapid or abnormal cell proliferation1- Endometrial Hyperplasia & endometrial adenocarcinoma
2- Cervical Dysplasia & Cervical CA &Bronchial dysplasia & lung CA
3- Liver Cirrhosis & Hepatocellular carcinoma .
4- Chronic healing process (skin squamous carcinoma & skin burn). 5- Ulcerative Colitis & Colorectal CA.
6- Villous Adenoma of colon & Colorectal CA.
7- Oral Leukoplakia & Squamous cell CA.
8-Atrophic gastritis & gastric CA.9-Paget disease of bone & Osteosarcoma .
:the subsequent development of malignancy in benign tumors isNotequite uncommon (i.e most malignant tumors arise denovo).
However :there are few exceptions e.g .villous adenoma of colon often
Neoplasia & cancer
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 90/174
90
Neoplasia & cancer
MOLECULAR BASIS OF CANCER
Dr.Nafea Sami Al Esawi
General pathology 2010
Al
–
anbar medical college
3
rd
stage medical students
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 91/174
91
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 92/174
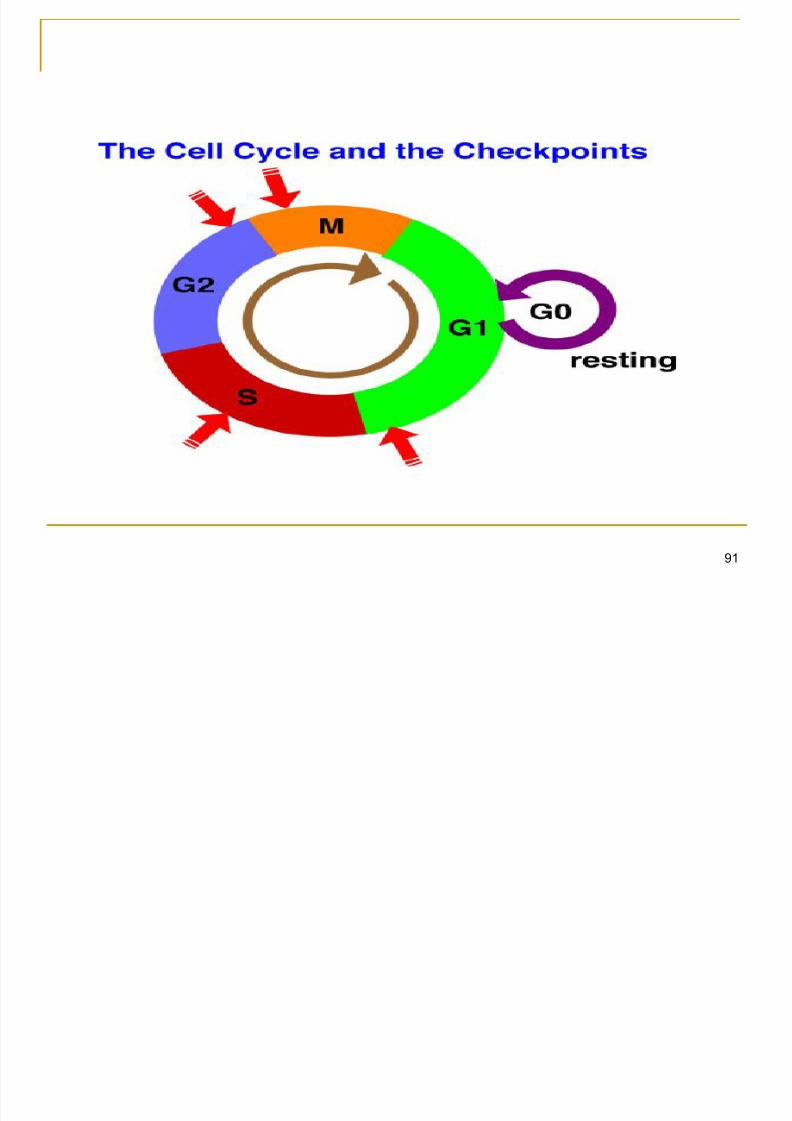
Cell cycle stages, also called phases, are thecomponents that make up a cell's life cycle.
There are four stages in a cell cycle, gap
phase 1 (G1), synthesis (S), gap phase 2(G2), and mitosis (M). Mitosis is further
divided into four stages, prophase,
metaphase, anaphase, and telophase. Some
descriptions of cell cycle stages include athird gap phase, known as G0.
92
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 93/174
The G1, S, and G2 stages are collectivelyknown as interphase. A cell in the G1 phase
is actively growing and undergoing the
metabolic changes that are required for cellsto divide. The G1 phase ends at the
restriction point, when the cell "decides" to
undergo division and moves on to the S
phase
93
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 94/174
All of the cell's DNA is replicated during the synthesisphase of cell cycle stages. During DNA synthesis, or
replication, special cell components separate the
double-stranded DNA helix into two single strands.
An enzyme called DNA polymerase then goes alongeach template strand of DNA and builds on a second
strand to exactly copy the cell's original DNA. Other
enzymes in the cell check to make sure the DNA
was copied correctly. The end result of synthesis is
two exact double-stranded copies of the cell's
original DNA, called chromosomes
94
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 95/174
Cells prepare for mitosis during the secondgap stage. Special materials are required in
the cytoplasm of the cell in order for mitosis
to occur. The cell undergoes metabolicchanges during G2 in order to form these
cytoplasmic materials
95
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 96/174
After G2, mitosis begins with the prophasestage. A structure known as the mitotic spindle
is formed during this phase. Another structure
called the centrosome duplicates itself, and theduplicates move to opposite ends of the cell.
The chromosomes move toward a region of
the mitotic spindle called the metaphase plate,
and the centromeres attach to the spindleusing structures known as kinetochores. This
last step of prophase is sometimes further
divided into a stage called prometaphase 96
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 97/174
During metaphase, the chromosomes alignwith the metaphase plate to help the
chromosomes separate properly during
anaphase. Once the chromosomes arealigned, anaphase occurs as the
chromosomes separate and move to
opposite ends of the cell. The separated
chromosomes are called daughterchromosomes
97
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 98/174
Telophase is the final phase of mitosis and ofthe cell cycle stages. The daughter
chromosomes each acquire their own nuclear
membranes, and the spindle fibers detachand disappear. Cell division is not complete,
however, until cytokinesis occurs and the cell
splits completely into two new cells. At this
point the cell cycle begins again with G1
98
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 99/174
Some researchers include a fifth phase of cellcycle stages. The G0 phase is inserted
between mitosis and G1. If cells enter the G0
phase, they are no longer growing. Theymay, however, become reactivated and enter
the G1 phase again
99
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 100/174
During development from stem to fullydifferentiated, cells in the body alternately divide
(mitosis) and "appear" to be resting (interphase).
This sequence of activities exhibited by cells iscalled the cell cycle.
Interphase, which appears to the eye to be a
resting stage between cell divisions, is actually a
period of diverse activities. Those interphase
activities are indispensible in making the next
mitosis possible.
100
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 101/174
Interphase: Interphase generally lasts at least 12 to 24 hours inmammalian tissue. During this period, the cell is constantly
synthesizing RNA, producing protein and growing in size. By
studying molecular events in cells, scientists have determined
that interphase can be divided into 4 steps: Gap 0 (G0), Gap 1 (G1), S (synthesis) phase, Gap 2 (G2). Gap
0 (G0): There are times when a cell will leave the cycle and quit
dividing. This may be a temporary resting period or more
permanent. An example of the latter is a cell that has reached
an end stage of development and will no longer divide (e.g.
neuron).
101
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 102/174
Gap 1 (G1): Cells increase in size in Gap 1,produce RNA and synthesize protein. An important
cell cycle control mechanism activated during this
period (G1 Checkpoint) ensures that everything isready for DNA synthesis. (Click on the
Checkpoints animation, above.)
S Phase: To produce two similar daughter cells,
the complete DNA instructions in the cell must be
duplicated. DNA replication occurs during this S
(synthesis) phase.
102
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 103/174
Gap 2 (G2): During the gap between DNA synthesis andmitosis, the cell will continue to grow and produce new
proteins. At the end of this gap is another control checkpoint
(G2 Checkpoint) to determine if the cell can now proceed to
enter M (mitosis) and divide. Mitosis or M Phase: Cell growth and protein production stop
at this stage in the cell cycle. All of the cell's energy is
focused on the complex and orderly division into two similar
daughter cells. Mitosis is much shorter than interphase,
lasting perhaps only one to two hours. As in both G1 and
G2, there is a Checkpoint in the middle of mitosis
(Metaphase Checkpoint) that ensures the cell is ready to
complete cell division. Actual stages of mitosis can be
viewed at Animal Cell Mitosis. 103
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 104/174
Cancer cells reproduce relatively quickly inculture. In the Cancer Cell CAM compare the
length of time these cells spend in interphase to
that for mitosis to occur.
104
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 105/174
Cycle, Checkpoint Control and DNA Damage
Control of eukaryotic cell growth and division
involves molecular circuits known as
“checkpoints” that ensure proper timing ofcellular events. Passage through a checkpoint
from one cell cycle phase to the next requires a
coordinated set of proteins that monitor cell
growth and DNA integrity. Uncontrolled cell
division or propagation of damaged DNA can
contribute to genomic instability and
tumorigenesis. 105
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 106/174
The G1/S checkpoint controls progression of cells throughthe restriction point (R) into the DNA synthesis S-phase.
During G1, the tumor suppressor Rb binds and inhibits
transcription factor E2F. Phosphorylation of Rb by cyclin-
bound cyclin dependent kinases (CDK) in late G1 inducesdissociation of Rb and permits E2F-mediated transcription
of S-phase-promoting genes. Responding to upstream
signals, INK4 and Kip/Cip family inhibitors control CDK
activity and prevent entry into S-phase. DNA damage
activates response pathways through ATM/ ATR andChk1/2 kinases to block CDK activity, leading to cell cycle
arrest and DNA repair or cell death.
106
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 107/174
The G2/M checkpoint prevents cells containing damaged DNAfrom entering mitosis (M). Activated CDK1 (cdc2) bound to
cyclin B promotes entry into M-phase. Wee1 and Myt1 kinases
and cdc25 phosphatase competitively regulate CDK1 activity;
Wee1 and Myt1 inhibit CDK1 and prevent entry into M-phase,while cdc25 removes inhibitory phosphates. DNA damage
activates multiple kinases that phosphorylate kinases Chk1/2
and tumor suppressor protein p53. Chk1/2 kinases stimulate
Wee1 activity and inhibit cdc25C, preventing entry into M-
phase. Phosphorylation of p53 promotes dissociation betweenp53 and MDM2 and allows binding of the transcription factor to
DNA
107
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 108/174
The spindle checkpoint ensures properchromatid attachment prior to progression
from metaphase to anaphase. The SCF and
APC/C protein complexes play prominentroles, with APC-cdc20 initiating the entry into
anaphase by promoting ubiquitin-mediated
degradation of multiple substrates, including
cyclin B and the regulatory protein securin.
108
MOLECULAR BASIS OF CANCER
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 109/174
109
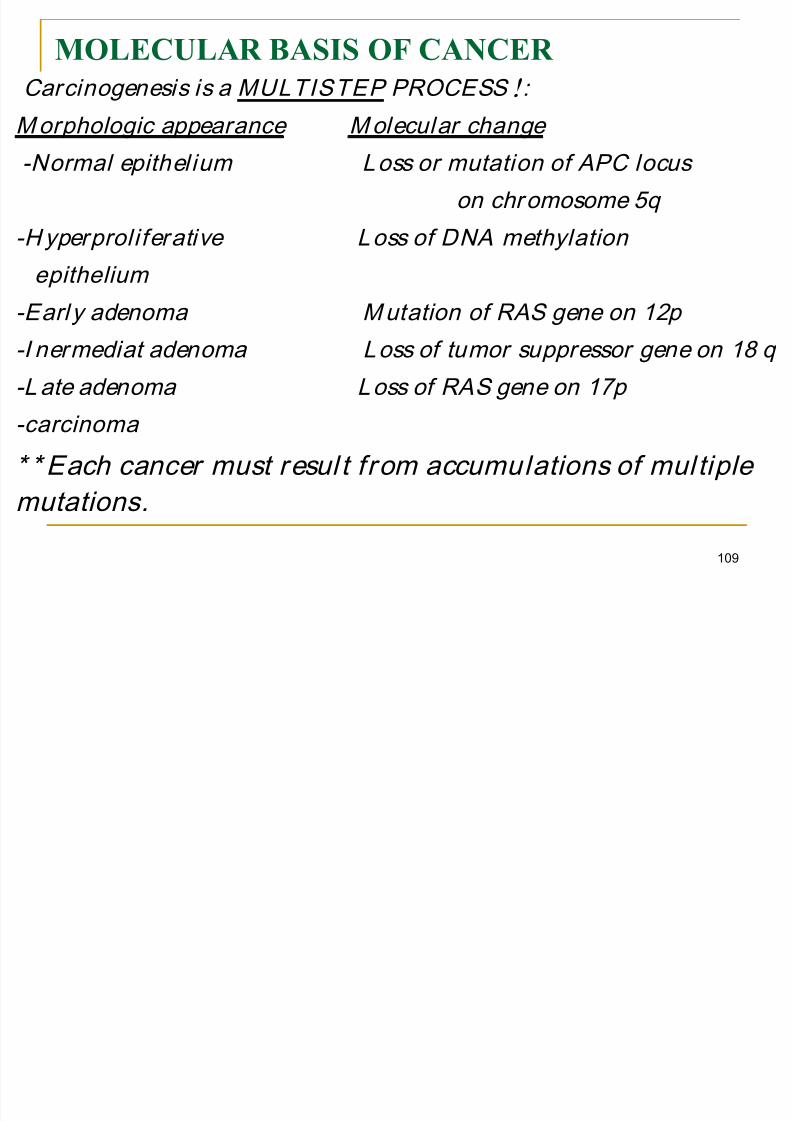
PROCESS ! : MULTISTEP Carcinogenesis is a
Molecular change Morphologic appearance
-Normal epithel ium Loss or mutation of APC locus
on chromosome 5q
-Hyperproli ferative Loss of DNA methylation
epithelium
-Earl y adenoma Mutation of RAS gene on 12p
-I nermediat adenoma Loss of tumor suppressor gene on 18 q
-Late adenoma Loss of RAS gene on 17p
-carcinoma
* * Each cancer must resul t from accumulations of mul tiple
mutations.
MOLECULAR BASIS OF CANCER
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 110/174
110
1-Non lethal genetic damage (mutation: irreversible
alteration of DNA ): TRANSFORMATION inherited in
germ line or acquired (radiation, chemicals, virus ,etc).
2-Involvement of normal regulatory genes that involved in
cell replication & death .
3-The tumor mass is the result of clonal expansion of single precursor (progenitor ) cell . (Cell Proliferation ) initially
Polyclonal Monoclonal :most of malignant tumors are
monoclonal i.e. result from transformation of a single cells.
4-Progression of tumor cells inducing new features : i.e
become heterogeneous cells with different capability for
INVASION & METASTASES .
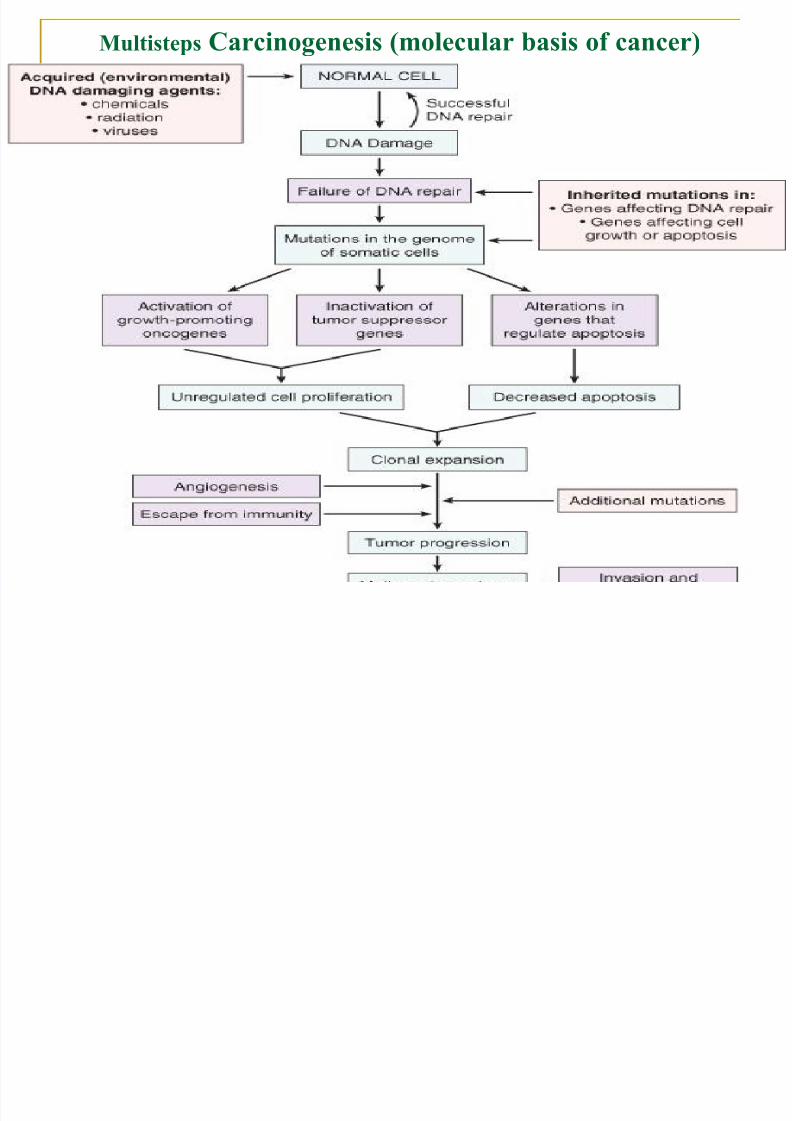
Multisteps Carcinogenesis (molecular basis of cancer)
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 111/174
111
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 112/174
Oncogenes :are cancer inducing genes derived from
cellular genes called protooncogenes

8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 113/174
113
cellular genes called protooncogenes.
OncogenProtooncogenFunction
SISPDGFGrowth factor
ERB-B2EGF-ReceptorGrowth factor receptor
ABLTyrosine kinaseSignal transduction
MYCTranscription activatorDNA binding protein
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 114/174
: Methods of gene activation
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 115/174
115
1- Point mutation .
2- Chromosomal translocation. 3- Gene amplification.
4- Gene deletion .
Result : Change in structure or quantity of gene product ( functional proteins).
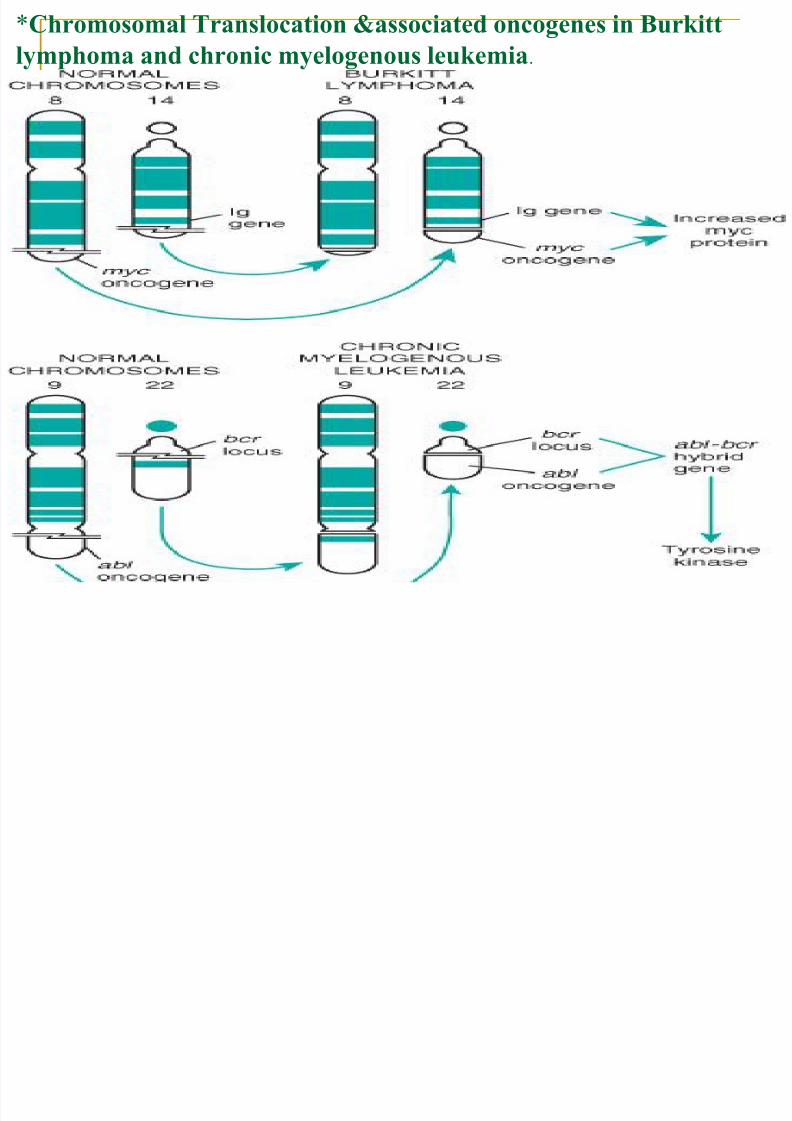
*Chromosomal Translocation &associated oncogenes in Burkittlymphoma and chronic myelogenous leukemia.
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 116/174
116
Gene Amplification of N-MYC gene in Neuroblastoma:
N MYC present normally on 2p become amplified & seen either as

8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 117/174
117
N-MYC present normally on 2p , become amplified & seen either as
extra chromosomal double minutes or as a chromosomally
integrated homogenous staining region (HSR)
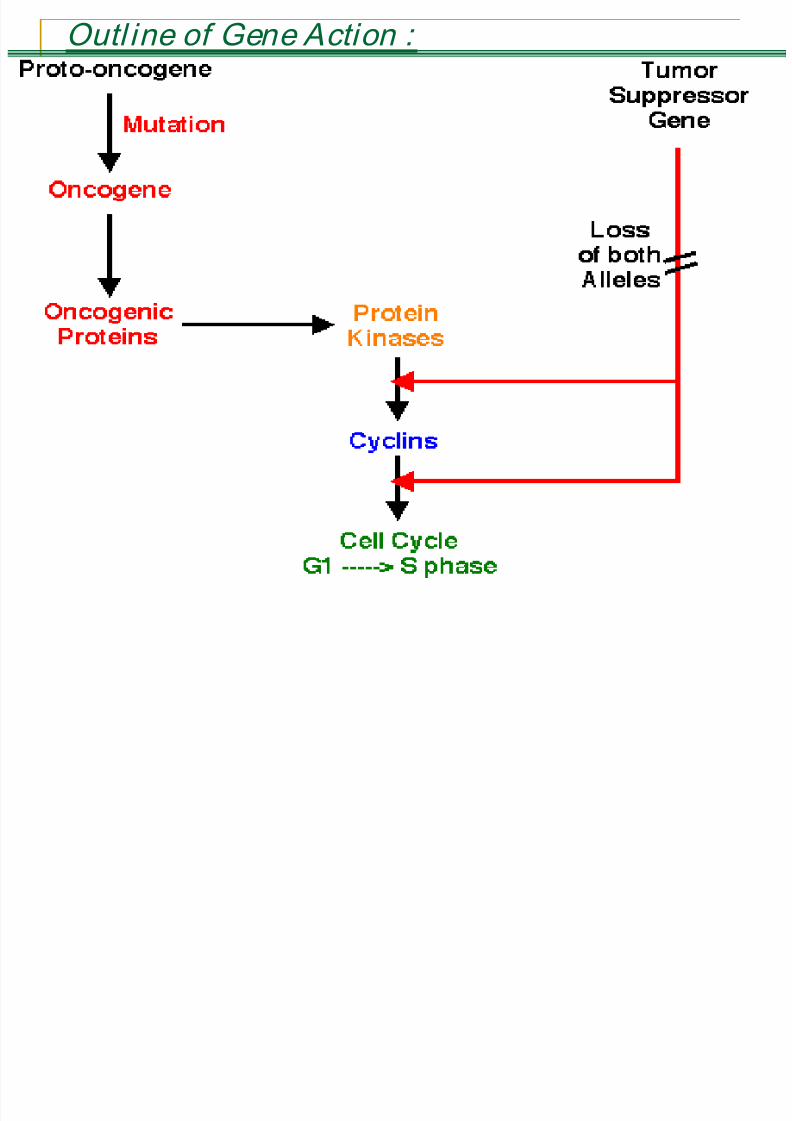
Changes necessary for malignant phenotype : 1 S lf ffi i i th i l ( O )
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 118/174
118
1- Self sufficiency in growth signals ( Oncogenes ).
2- Insensitivity to growth inhibitory signals ( Suppressors).
3- Evasion of apoptosis (programmed cell death :i.e.immortality of neoplastic cells)
4- Genetic instability ( Accumulation of mutation Enablerof malignancy).
5- Limitless replication potential (Telomeres :determinethe life of individual cell) i.e overcoming cellularsenescence .
6- Development of Sustained angiogenesis.7- Ability to invade & metastasize (new features acquired
during new mutations ).
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 119/174
119
Oncogenes:Genes that promote autonomaous cellgrowth in cancer cells. These are usually dominant
genes & include:
Growth factors.
Cell surface growth factor receptors.
Signal transduction proteins.
Nuclear transcription factors.
Cell cycle proteins (cycline &cyclin-dependent
kinases).
Inhibitors of apoptosis.
1-Oncogenes :Classified by site of action
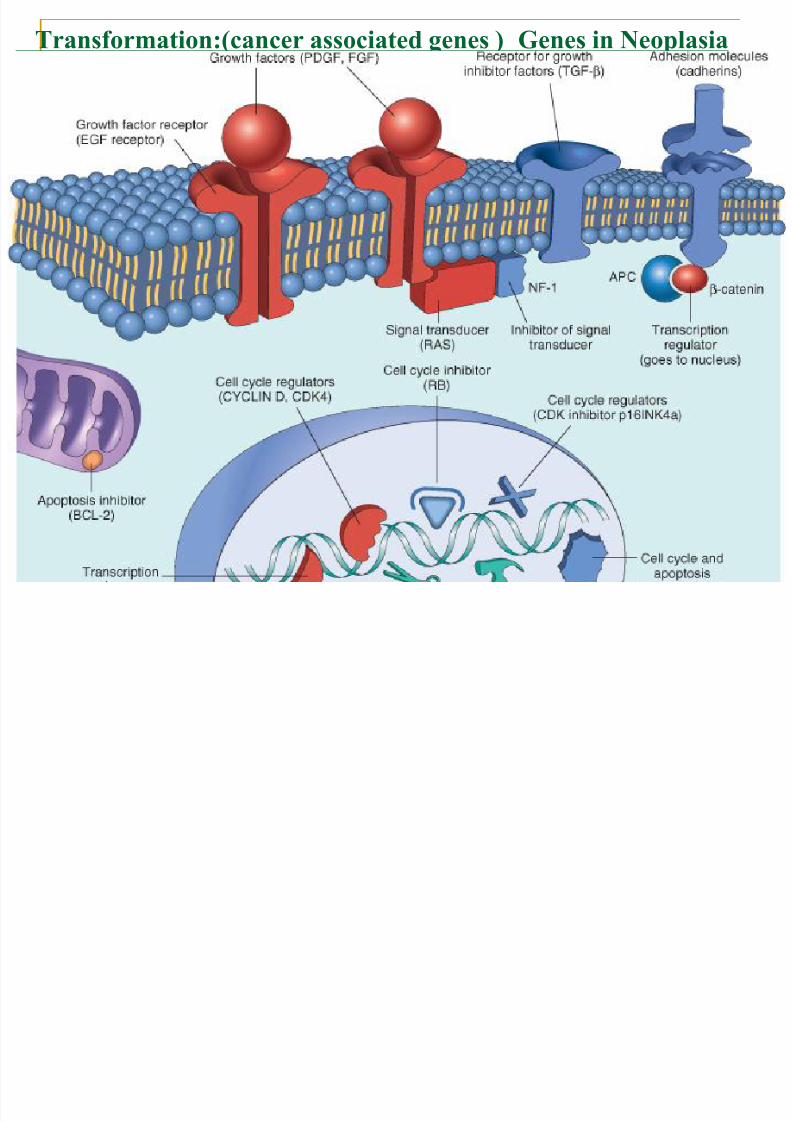
Genes in Neoplasia Transformation:(cancer associated genes )
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 120/174
120
Oncogenes coding for Growth Factors - 1
All normal cells require stimulation by growth factor
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 121/174
121
All normal cells require stimulation by growth factorto undergo proliferation .(Cell growth is stimulated
by Growth factors) Cancer cells acquire growth self-sufficiency by:
1-Ability to synthesize the same growth factors towhich they are responsive( persistent activation).
Platelet derived growth factor (PDGF) seen inglioblastomas .
Fibroblast growth factor(FGF)-stomach Carcinoma.
2-Overexpresion of growth factor genes. (TGF). Products of other oncogens (e.g.RAS) may cause
over expression of GF e.g. Transforming GrowthFactor (TGF-)in sarcomas
Oncogenes coding for GF Receptors: - 2 Growth Factors integrate with membrane receptors
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 122/174
122
Growth Factors integrate with membrane receptors tyrosine kinase activity nucleus .
Mutant receptor proteins continuous mitogenicsignals to cells even in the absence of GF inenvironment.
Or normal but overexpressed (amplifications ) hypersensitive to GF.
Epidermal GF receptor family:
ERBB1 in 80% of sq.CA lung
ERBB2 ( HER 2 ) in 25-30% of breast & ovariancarcinoma .
Increase expression = POOR PROGNOSIS
Oncogenes in Signal Transduction: - 3
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 123/174
123
g g
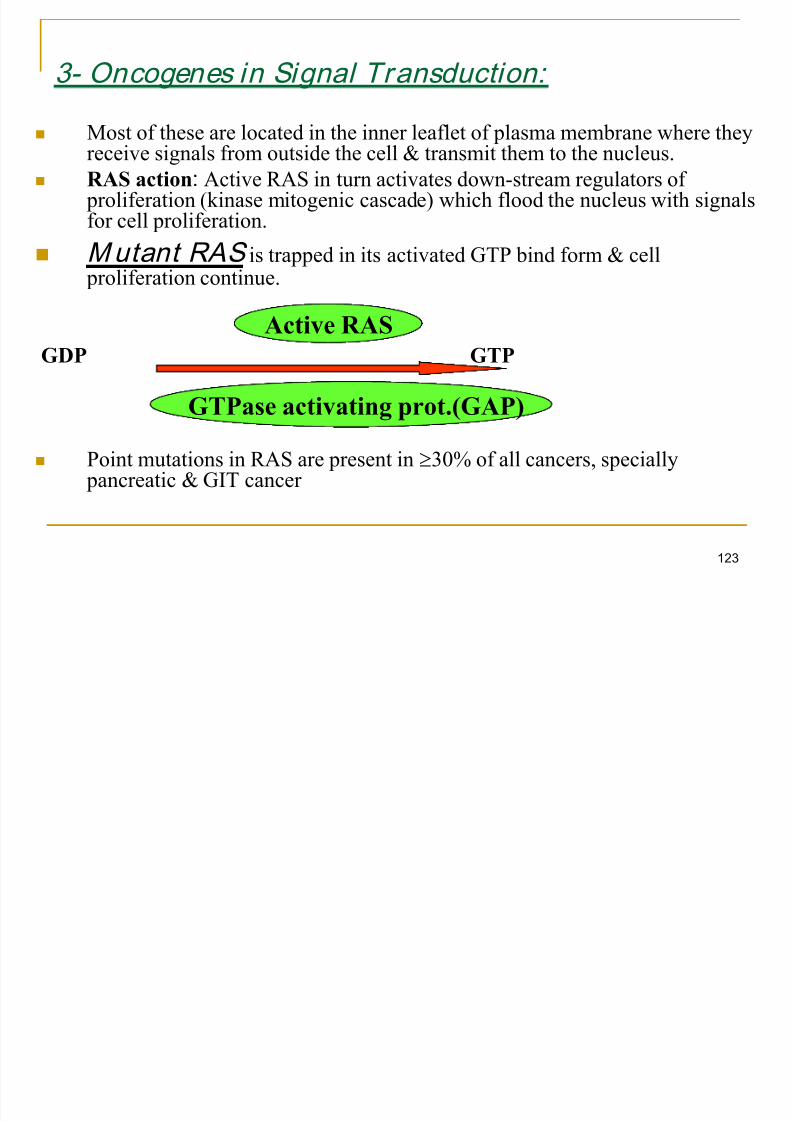
Most of these are located in the inner leaflet of plasma membrane where they
receive signals from outside the cell & transmit them to the nucleus. RAS action: Active RAS in turn activates down-stream regulators of
proliferation (kinase mitogenic cascade) which flood the nucleus with signalsfor cell proliferation.
Mutant RAS is trapped in its activated GTP bind form & cell proliferation continue.
GDP GTP
Point mutations in RAS are present in 30% of all cancers, specially pancreatic & GIT cancer
Active RAS
GTPase activating prot.(GAP)
: Non receptor associated tyrosineAction of ABL
kinase signal transmission
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 124/174
124
kinase signal transmission
Normal ABL (proto-oncogene has tyrosine kinase
activity )is located in nucleus where it promotesapoptosis of cells that suffer DNA damage .
Chronic myeloid leukemia : Mutation ( 9:22translocation ) BCR- ABL hybrid gene .
This new hybrid gene is retained in cytoplasm whereit has tyrosine kinase activity cell proliferation.
Action is Proliferation + Absent Apoptosis.
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 125/174
: Dependent Kinases - Cyclins & Cyclin - 5 Cancers may become autonomous if the genes that
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 126/174
126
Cancers may become autonomous if the genes thatderives the cell cycle become dysregulated by mutations
or amplification . Cyclins bind to CDKs, activating them.
Cyclin D family CDK4 & CDK6 at G1 S phasecheckpoint.
Activity of CDK/Cyclin regulated by CDK inhibitors
Cyclin D overexpressed in breast, liver, & esophagealcancers
Amplif ication of CDK4 gene present in melanoma,sarcomas, glioblastoma .
2- Cancer Suppressor Genes:-
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 127/174
127
Growth inhibitory pathway by:
* Regulate cell cycle : Rb gene
* Regulate cycle & apoptosis: PT 53
* Block GF signals: TGF-
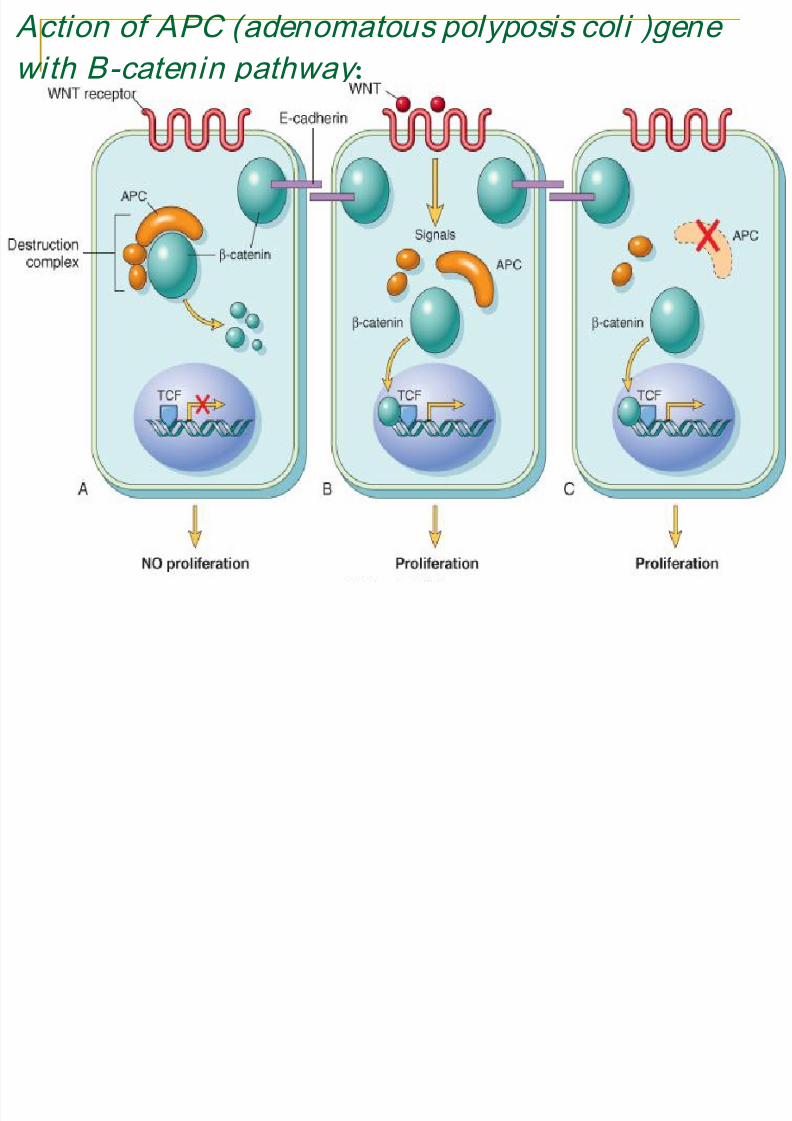
• APC regulates -catenin• APC gene loss in APC & mutated in colon carcinoma.
-Cancer suppressor genes are recessive genes which may be lost infamilial or sporadic cases or mutated .
APC gene exert antiproliferative effect –it is cytoplasmic protein that regulate intracellular level of -catenin .
-catenin :is transcription activation factor (TcF) of growth promoting genes ( Cyclin D1 , MYC).
Action of APC (adenomatous polyposis coli )genewith B-catenin pathway :
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 128/174
128
): RetinoblastomaRb gene ( - 1 Rb role is regulating the G1 S check point of cell
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 129/174
129
Rb role is regulating the G1 S check point of cellcycle.
Rb exists in active nonphosphorylated & inactive phosphorylated forms.
Normal Active pRb binds to transcription factors
NO TRANSCRIPTION( of genes whose products are
required for S phase of cell cycle). Mutated I nactive pRb releases transcription factors TRANSCRIPTION ( of genes whose products arerequired for S phase of cell cycle ) , so drive the cell to
proliferation.
This is a trigger the cell cycle at G1 phase pushing cellinto S phase
:Retinoblastoma Example :
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 130/174
130
Autosomal dominant hereditary disease.
May be sporadic. Patients carry one mutation in their genome .
No tumor develops unless two alleles in 13q14
become mutant (Knudson’s two hit theory).
Patients have high incidence of Retinoblastoma and
osteosarcoma.
I nher itance (pathogenesis )of Retinoblastoma
T t ti f RB l 13 14 l d t l ti
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 131/174
131
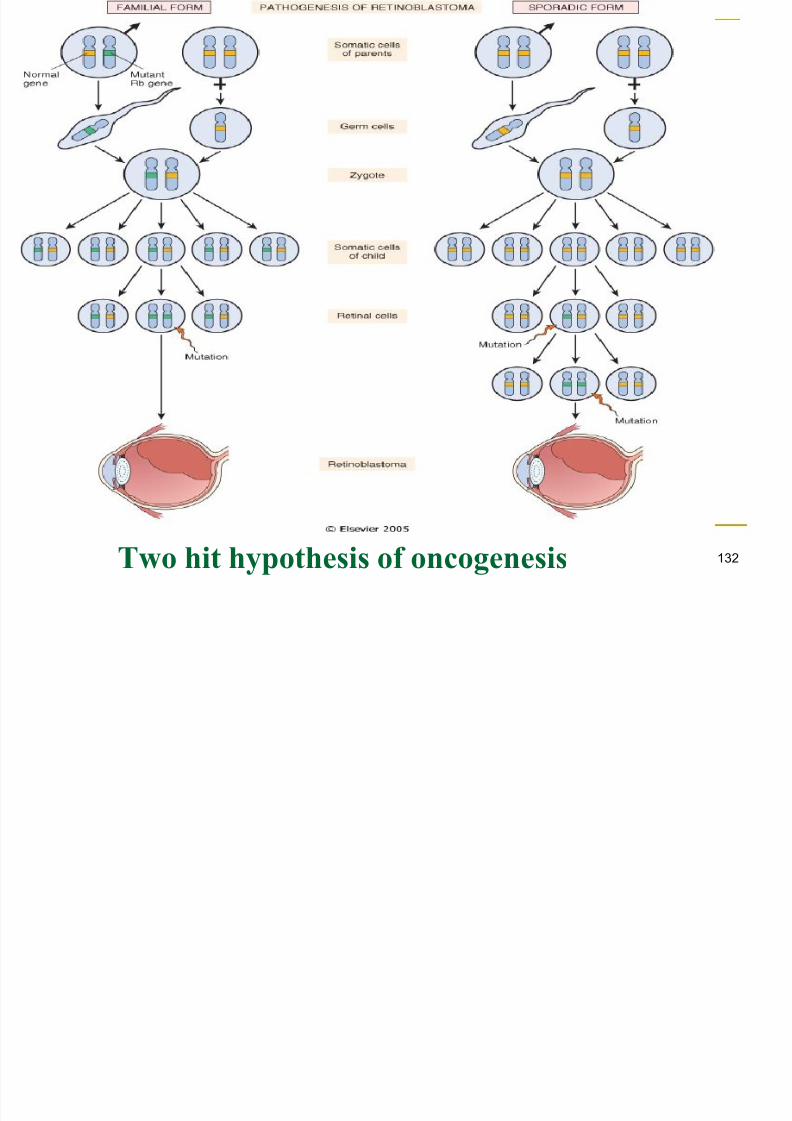
Two mutation of RB locus on 13q14 lead to neoplastic
proliferation of retinal cells (two hit theory).
In familial form all somatic cells inherit on mutant RB gene
from a carrier parent: i.e inherited 1st hit.
The second mutation affect RB locus in one of retinal cells
after birth: i.e acquired 2nd hit . In sporadic form , both mutation at RB locus are acquired
by retinal cells after birth.
Rb mutation renders the protein inactive , thus the celldivides non stop.
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 132/174
132
Two hit hypothesis of oncogenesis
Summary Cyclin/CDK/RB function
L f l ll l t l i t l t
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 133/174
133
Loss of normal cell cycle control is central to
malignant transformation& at least one of the
following is mutated in most human cancers :
- Cyclin D
- CDK 2, CDK 4, CDK 6
- RB
- CDK inhibitors
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 134/174
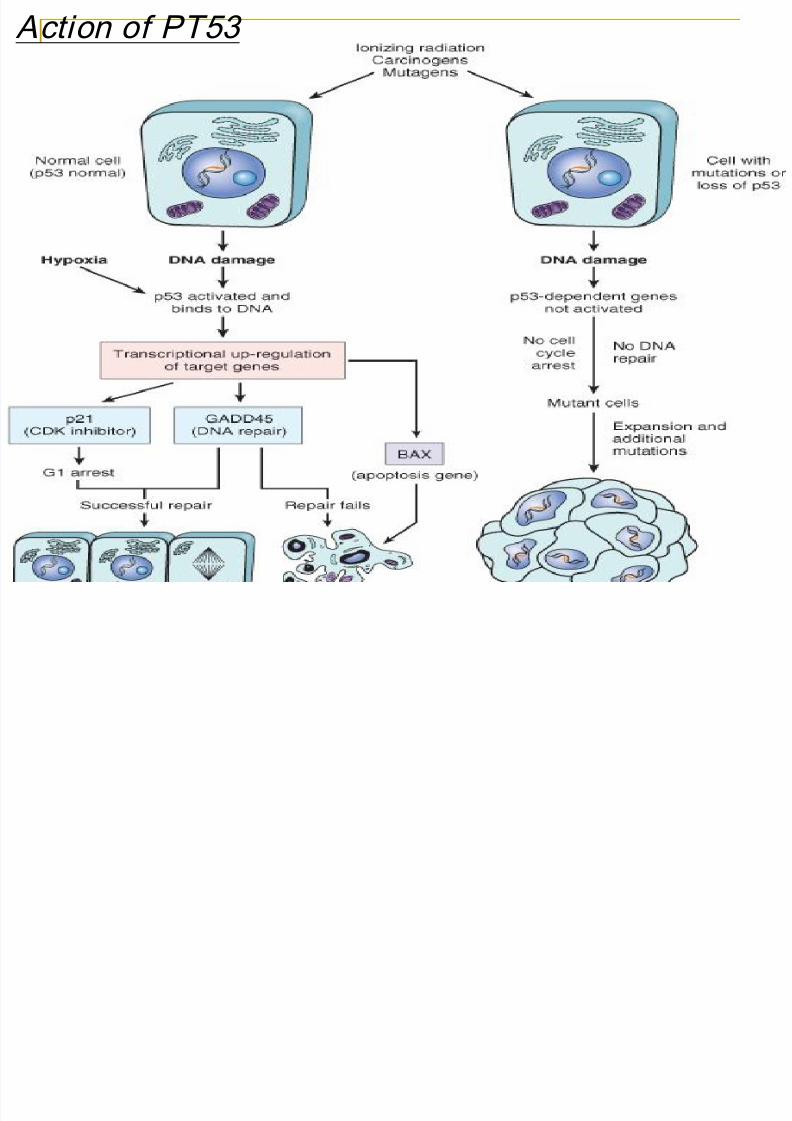
: 53Mode of Action of PT Normal PT53 binds to DNA (maintain the integrity of genome .
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 135/174
135
P 21 & GADD45 Transcription Delay
*More time for repair Normal
*Failed repair APOPTOSIS(by activation of BAX gene)
*Fixed mutation (mutant PT 53) NEOPLASIA Acquired mutation in many cancers :
e.g.colon, breast, lung , leukemia…etc
Inherited mutation in Li - Fraumeni S.
sarcoma, leukemia,breast&brain CA..etc
May be blocked by some DNA viruses .
Damaged DNA PT53 activated & bind to DNA cause transcription upregulation of targeted gene i.e. faulty PT53 molecules allow cell withdamaged DNA (mutant DNA)to survive & replicate :
P21-CDK inhibitor Arrest cell at G1.
GADD45-DNA repair requir DNA damage
53 Action of PT
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 136/174
136
These are genes involved in programmed cell death ,promoting
3- Apoptosis Genes :
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 137/174
137
or suppressing this process.
BAX, BCL-2 , BCL-x , BAD…..etc BCL-2 prevents apoptosis, i.e.prolonging cell life.
Activated by translocation (18:14 ): Low grade B cell
Lymphoma .
4 DNA Repair Genes :*Repair mutations in other genes, preventing themfrom continuing in further cell cycles.*Defective DNA repair= Genomic Instability &
Enabler of Malignancy .These include :1- Nucleotide excision repair genes :Damage by U V light . Defective in genes encode
for certain enzyme involve in DNA synthesis:
Xeroderma Pigmentosum
These repair errors in:DNA M ismatch repair genes - 2
-
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 138/174
138
pp g
pairing of nucleotides during cell division .
e.g. G+T instead of A+T .a.) (HNPCC).ColonicConpolyposis NereditaryH(
These genes are not oncogenic but allow mutation in
other genes in normal cell cycle .
BRCA -1 in familial breast cancer & ovarian CABRCA –2 in breast CA in both sex ,e.g: prostate, ovary,
pancreas, stomach CA.
Both above are important in repairing breaks in DNA but
are rarely inactivated in sporadic cases.
These are specialized structures (nucleotide repeats )at the
5- Telomeres (Cellular senescence)
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 139/174
139
These are specialized structures (nucleotide repeats )at theend of chromosomes which are shortened after each celldivision till eliminated when the cell stop dividing (thisreach to point whereby loss of telomere lead to an end-end fusion of chromosome during mitosis wheretelomerase enzyme lost gradually ) and may play a role in
determining the life of individual cells. This shortening is prevented by TELOMERASE (which
absent in most somatic cells ) .
Majority of cancers telomerase activity (tumor cellshave the ability to reactivate this enzyme ) so contributeto immortalization of cancer cells by prevention ofnaturally programmed shortening of the telomere.
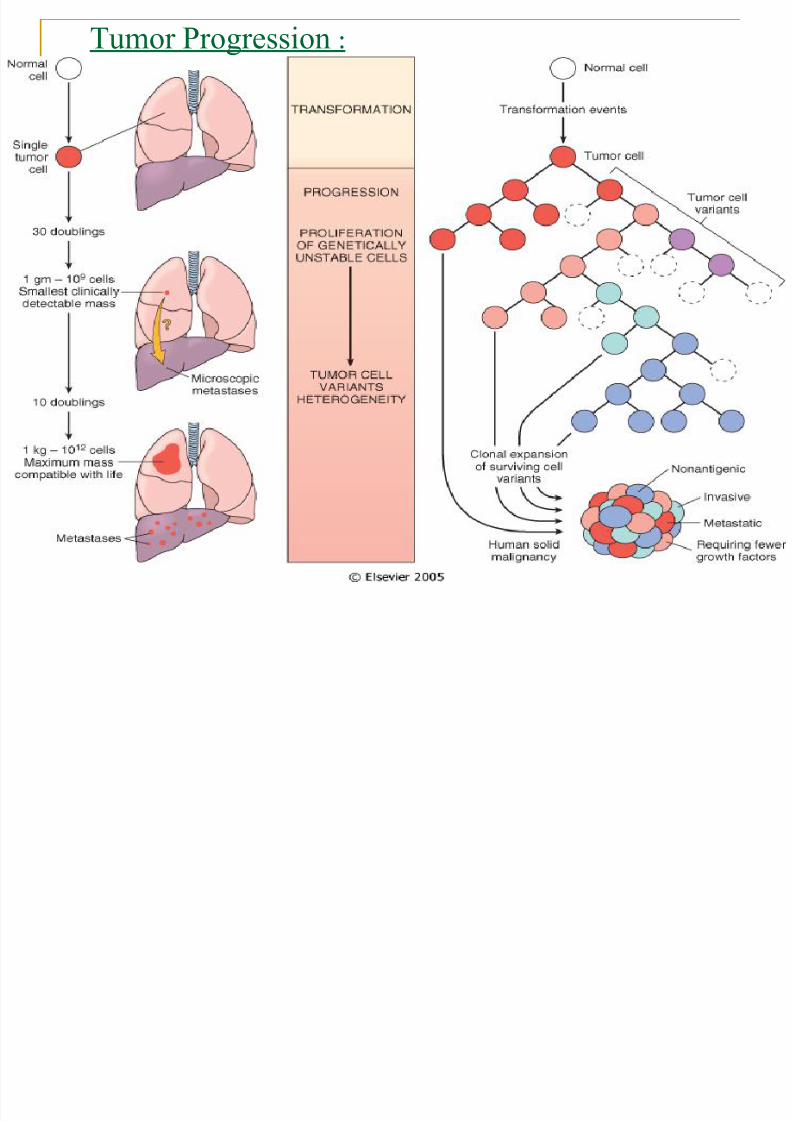
:TUMOR PROGRESSION
Despite the fact that most malignant cells are
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 140/174
140
Despite the fact that most malignant cells are
monoclonal in origin , by the time they become clinically
evident , their constituent cells are extremely
hetrogenous ( result frome multiple mutations ).
Tumors may generate clones with different phenotypic
features, leading to a more aggressive nature e.g. Non antigenic growth
Invasion
Metastases Rate of generation of these clones differs in individual
tumors e.g. Osteosarcoma versus Seminoma
:Tumor Progression
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 141/174
141
BIOLOGY OF METASTASES
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 142/174
142
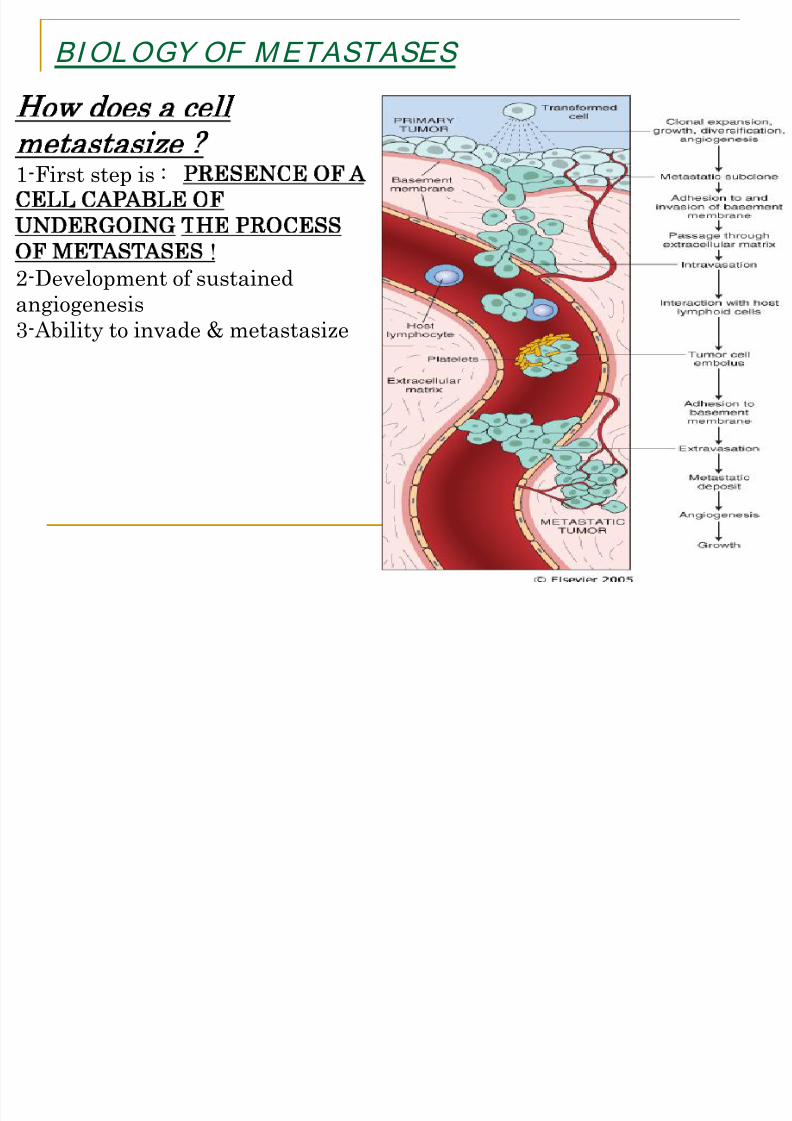
How does a cell
metastasize ? 1-First step is :
PRESENCE OF A
CELL CAPABLE OF
UNDERGOING THE PROCESS
OF METASTASES
!2-Development of sustained
angiogenesis3-Ability to invade & metastasize
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 143/174
I I ABIL I TY TO INVADE & METASTASISE
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 144/174
144
1- Invasion through the (ECM) :
E-cadher in is an intercel lular adhesion molecule
Inactivation detachment of tumor cells
Brought about by laminin & integrin receptors to basementmembrane & ECM
i-Detachment (loosening )of tumor cells
ii- Attachment of tumor cells to matrix components
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 145/174
2- Metastases( vascular dissemination &homing of tumor cells)
Invasion of the circulation (intravasation):Adhesion to
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 146/174
146
Invasion of the circulation (intravasation):Adhesion to
endothelium retraction of endothelium vessel
Attack by NK cells, some escape by formation of a thrombus
Escape from circulation :Adhesion to endothelium retraction of
endothelium escape to tissue (extravasation ).
HORMONE DEPENDENCE : : - Some tumor
cells are hormone dependant for growth. This is through presence
of receptors on surface e.g- Breast CA , Thyroid CA , Prostatic
CA
-Some genes may be important in metastases :
- nm 23in breast CA ,- KAI -1in prostatic CA , - KiSS in
Melanoma
Examples of Tropism ( Homing ) Prostatic Carcinoma Bone
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 147/174
147
Lung Carcinoma Adrenals & Brain
Neuroblastoma Liver & BoneLess common sites of metastases include skin,muscle
thyroid,breast….etc.
*Spleen & Cartilage are almost never involved by
metastatic tumours.WHAT INFLUENCES SI TE OF METASTASES ?
1-Anatomical Location
2-Complimentary adhesion molecule between
tumor cells & target organs. 3-Chemoatractants liberated by target organs.
4-Protease inhibitors present in certain tissues.
CARCINOGENIC AGENTS : Chemical Mutagenes are detected & graded by the AMES TEST
Factors influencing carcinogenesis include :
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 148/174
148
g g
- Genetic susceptibility
- Sex & hormonal status- Diet
Chemical carcinogens act by inducing ras mutation
Some strong chemicals act as Initiator & Promoter
1- CHEMICAL CARCINOGENS :
Direct Carcinogens -
Directly produce damage without prior metabolic conversion
Indirect Carcinogens- (Procarcinogen)
Metabolic conversion in liver bycytochrome P-450 dependent mono-
oxygenases ultimate carcinogen
: Action of chemical carcinogens
Initiator - Chemical inducing irreversible
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 149/174
149
g
DNA damage
Promoter -Augment effect of initiator by
promoting cell growth:
e.g. phorbol ester (PTA) activate signal transduction
or GF secretion , hormones, saccharine …..etc No tumor develops unless the promoter
is applied AFTER the initiator.
:Classes of Chemical Carcinogens
1- Alkylating Agents : Direct, used in chemotherapy of
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 150/174
150
1 Alkylating Agents : Direct, used in chemotherapy of
cancer may induce Leukemia.
2- Polycyclic Hydrocarbons : Indirect & very strong e.g.
cigarette smoke CA Lung.
3- Aromatic Amines & Azo dyes : Rubber & Food Industry
e.g. naphthylamine Bladder CA.
4- Nitrosamines : Endogenous or food preservatives e.g.
Gastric & Colon CA…etc.
5- Aflatoxin B1 : Naturally occurring carcinogen present infungus. Aspergillus flavus Hepatocellular CA.
2- PHYSICAL CARCINOGENS : 1- U-V light : - Effect depends on intensity of exposure
& quantity of melanin
Production of pyrimidine dimers in DNA MUTATION in ras p 53
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 151/174
151
- Production of pyrimidine dimers in DNA MUTATION in ras , p 53
- Failed repair Skin CA
- Skin cancer includes : Squamous Cell CA, Basal Cell CA, Melanoma .
2- I onizing Radiation :
- Present in environment
- Explosions Leukemia after 7 yrs.
Latent period Breast,colon, thyroid, lung CA.-Therapeutic exposure Thyroid CA, Leukemia- Mechanism:Free radical injury
Mutations in RAS, RB. PT53
3-Asbestos fiber inhalation : Mesothelioma & Lung CA
3- VIRAL CARCINOGENESIS :
A - DNA Vi ruses :Vi rus have DNA transforming genes (E6,E7)inactivate suppressor genes, activates cyclins, & inhibit
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 152/174
152
inactivate suppressor genes, activates cyclins, & inhibitapoptosis.
1- HPV : Human Papilloma Virus* Low risk groups (6, 11) Squamous Cell Papilloma
(wart ).
* High risk group ( 16, 18 ) Squamous Cell CA in cervix.
2- EBV : Ebstein Barr Vi rus
* BURKITT’S LYMPHOMA , * B CELL LYMPHOMA
* HODGKIN’S LYMPHOMA, * NASOPHARYNGEAL CA
Mode of action :
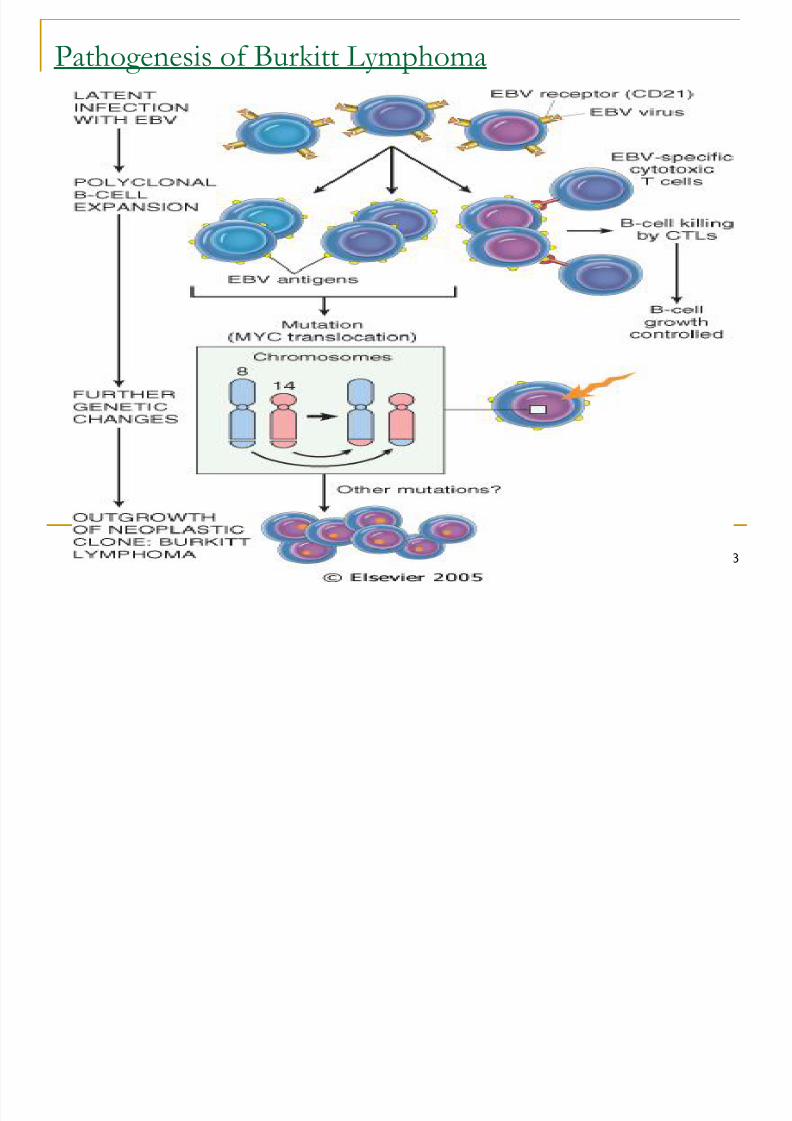
Receptors for virus on B cells Activated B cells Polyclonal
Proliferation, under T cell control ,- MONOCLONAL B proliferation due to deregulation of C-
MYC by translocation : BURKITT’S Lymphoma (t 8:14)
- In endemic cases Malaria & Malnutrition may play a role in immunity ( Lost T cell control ).
Pathogenesis of Burkitt Lymphoma
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 153/174
153
3- HBV ( Hepatitis B Virus )
Chronic liver disease Cirrhosis
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 154/174
154
HEPATOCELLULAR CA
Action :* Cell proliferation mutation* HBV encodes Hbxprot. growth
promoting genes
*Hbx binds to p 53 Inactivates suppressorfunction.
*Aflatoxin in endemic areas
(HBC is similar to above but no X-protein)
4 - HHV-8 ( KSHV ) Kaposi Sarcoma in AIDS
RNA virus tumors :

8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 155/174
155
HTLV-1 induces Leukemia /Lymphoma in humans
Transmitted sexually,blood or milk
- Mode of action :
Target cells are CD4+ T cells which have receptors for
the virus tax gene (transforming agent ) proliferationPOLYCLONAL MONOCLONAL LEUKEMIA
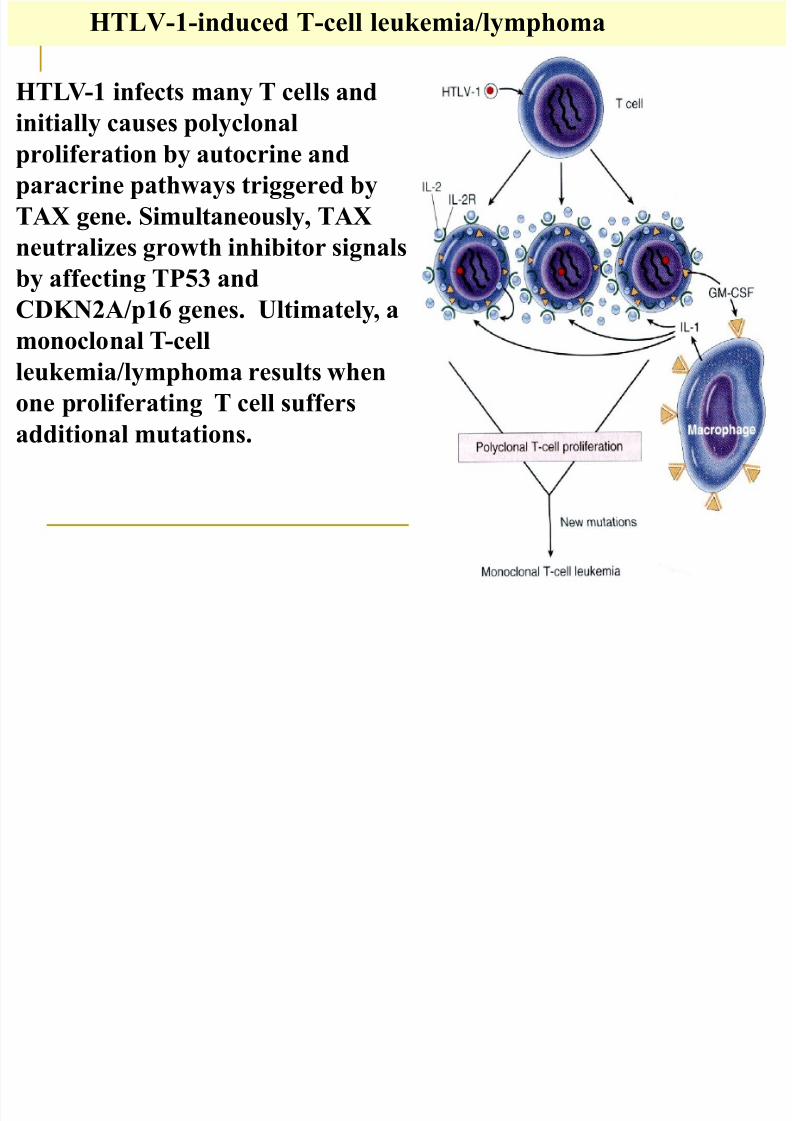
HTLV-1-induced T-cell leukemia/lymphoma
HTLV-1 infects many T cells and
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 156/174
156
initially causes polyclonal
proliferation by autocrine andparacrine pathways triggered by
TAX gene. Simultaneously, TAX
neutralizes growth inhibitor signals
by affecting TP53 and
CDKN2A/p16 genes. Ultimately, a
monoclonal T-cell
leukemia/lymphoma results when
one proliferating T cell suffers
additional mutations.
Helicobacter in carcinogenesis
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 157/174
157
First described as a cause for peptic ulcer
Plays a role in etiology of gastric CA & gastric
lymphoma
LYMPHOMA :
Chronic gastritis mucosal lymphoid follicles reactiv
polyclonal B cells monoclonal B cells LYMPHOM
CARCINOMA :
Chronic gastritis Gastric atrophy intestinalmetaplasia dysplasia Gastric Carcinoma
CANCERS --ASSOCIATED CARCINOGEN
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 158/174
158
CA LUNG Smoking.
CA CERVIX Sexual transmision of HPV.
CA BLADDER Rubber Industry.
CA LIVER Aflatoxin & HBV infection
CA THYROID Radiation.
ANGIOSARCOMA of LiverPlastic(PVC).
MESOTHELIOMA Asbestose.
TUMOR IMMUNOLOGY:
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 159/174
159
Tumor Antigens :Tissue specific Ag (peptide of mutant gene),tissue associatedAg (glycoprotein), viral, Oncofetal ( AFP , CEA)…..etc
Anti tumor Host Mechanisms :
1- Sensitized Cytotoxic T lymphocytes (directed against T-Cell defined tumor Ag).
2- Natural Killer cells may kill tumor cells without previous sensitization lyse a wide range of tumors .
3- Macrophages activated by IFN- to secrete TNF- whichis lytic to tumor cells.
4- Humoral mechanisms .
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 160/174
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 161/174
- Cancer Cachexia :
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 162/174
162
Wasting syndrome characterized by anorexia , loss of body fat ,with marked weakness,anemia & fever.
Possibly due to :
1- Release of cachectin ( TNF and IL-1) by
macrophages & some tumor cells.2- Loss of appetite.
3- Metabolic changes leading to reduced synthesis &storage of fats & increased mobilization of fatty acids from
adipocytes.
4 - Paraneoplastic Syndrome :
Symptoms that not directly related to the primary tumor or
i i l b i f h i di h
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 163/174
163
its metastasis or elaboration of hormones indigenous to the
tissue from which the tumor arose . Syndrome that can’t be explained by the effects of either
local or distant spread of tumor or by hormones indigenous
to cell of origin.
They may precede the tumor or mimic metastases.
They occur in about 10% of malignant tumors.
PARANEOPLASTIC SYNDROMES : 1- Ectopic hormone production (endocinopathy )
ACTH ADH Parathormonelike polypeptide
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 164/174
164
ACTH, ADH,Parathormonelike polypeptide,
Insulin like GF, erythropoietin .2- Coaggulative abnormalities & hematologic syndromes
Venous thrombosis, Erythrocytosis,
Eosinophilia, Thrombocytosis,
Autoimmune hemolytic anemia…etc3- Neurological abnormalities (encephalopathy ).
4- Skin changes ( acanthosis nigricans )& Myopathy .
5- Malabsorption in up to 50% of cases
6- Nephrotic syndrome .7-hypertrophic osteoarthropathy & finger clubbing .
Some Paraneoplastic Syndromes :
Small Cell CA lung ACTH ADH Bone
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 165/174
165
Small Cell CA lung ACTH , ADH, Bone
changes,nervous system disorders Squamous Cell CA lung Hypercalcemia
Pancreatic & lung CA Deep vein thrombosis.
Breast CA Hypercalcemia (lytic bone metastases).
Hepatic & Renal CA Polycythemia
Pancreatic, Gastric CA Carcinoid S.
Advanced Cancers Nonbacterial thrombotic
endocarditis.
Colonic Adenocarcinoma Acanthosis nigricans
TUMOR MARKERS & CANCER
These are tumor derived or associated antigens enzyme
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 166/174
166
These are tumor derived or associated antigens , enzyme ,cytoplasmic proteins and hormons that can be detected in
blood or other body fluid.-Tumor markers represent biochemical indicators of the
presence of a tumor.
Their uses are to :
I - Confirm diagnosis (not for primary diagnosis ).
II -Determine the response to treatment .
III - Detect early relapse.
Present in serum or urine.
Many are present in normal & tumor tissue, so they are notvery specific but their level is important.
Types of Tumor Markers
1- Hormones :
H Ch i i G d t hi H ( HCG)
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 167/174
167
Human Chorionic Gonadotrophic Hormone ( HCG)
Elevated levels are seen in- testicular tumors
- pregnancy
- Gestational Trophoblastic Disease :Hydatidiform Mole , Choriocarcinoma
Calcitonin useful in diagnosis of Medullary CAthyroid.
ACTH :ectopic production in small cell carcinoma.
2- Oncofetal Antigens :
Carcinoembryonic Antigen ( CEA ) : in fetal tissue &
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 168/174
168
some malignancies - Colorectal CA & Pancreatic CA .
CEA value in detected tumor burden in colorectal cancer
& in detecting recurrences after surgery
-Alpha Fetoprotein (AFP:produced by fetal yolk sac&liver
-Normal 15 g / L- Cirrhosis 200-300 g / L -
- Hepatoma 400g / L
-Non seminomatous testicular germ cell tumor.
Less consistent elevation may be seen in some non
neoplastic conditions (alcoholic hepatitis
,cirrhosis,ulcerative colitis ).
3- I soenzymes :
Prostatic Acid Phosphatase ( PAP )
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 169/174
169
levels seen in Metastatic prostatic CA
Useful in : * Staging prostatic CA
* Assessment of prognosis
* Response to therapy.
Neuron -specific enolase :Small Cell CA of lung & Neuroblastoma.
4- Specif ic Proteins :
Immunoglobulins secreted in Multiple Myeloma &
NHL . Prostate -specific antigen ( PSA ) :
Present in epithelium of prostatic ducts.* BPH & Prostatic CA .
* Level correlates with stage
LABORATORY DIAGNOSIS OF CANCER
1- Cytological methods : Cytological diagnosis dependth id tifi ti f f t f l i i ll
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 170/174
170
on the identification of features of anaplasia in cells
exfoliated , aspirated or brushed . Study exfoliated cells :
- FNA: for superfacial, palpable mass (breast mass ) ordeep mass under u/s control ( liver mass) .
Brush cytology : like bronchial tree brush .Fluid tapping : aspirated pleural effusion & ascetis.
PAP often used for early detection of cervicaldysplasia.
Natural exfolative cytology :for urine , sputum- False(+), False (-)
- A negative report does not exclude malignancy
- Advise biopsy !
: H istological methods - 2
Biopsy of tissue: Needle Biopsy , Endoscopic Biopsy,
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 171/174
171
Biopsy of tissue: Needle Biopsy , Endoscopic Biopsy,Open Biopsy.
Frozen Section (Rapid technique & rapid diagnosis duringoperation): Define the lesion & surgical margins ofexcision .
Paraffin Section ( 36-48 hrs. or longer ).
3 -Immunocytochemistry
:Staining by use of monoclonal AB directed against variouscomponents in cell
May help in diagnosis of undifferentiated cancers or helpin identifying source of a metastatic tumor.e.g.Cytokeratin Carcinoma
Common leukocyte antigenLymphoma
S 100 Melanoma
:Electron microscopy - 4 For recognition of desmosomes (epithelial tumors ) , or
neurosecretory granules ( neuroendocrine tumors)….etc.
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 172/174
172
5- F low cytometry :
For measuring DNA content , detecting diploid versusaneuploid tumors….etc.
Correlates with rate of growth
&prognosis(aneuploidy=poor). Useful in the diagnosis of Lymphoma (identification of cell
surface Ag).
DNA-probe analysis (molecular diagnosis):
diagnosis of malignant neoplasm by detection of polyclonal(benign) B&T-Cell proliferation from monoclonal(malignant).
:EARLY DI AGNOSIS of CANCER
This is very important as many cancers are curable if theydi d l

8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 173/174
173
are diagnosed early.
Specific symptoms should be followed upe.g. Abnormal bleeding ( GIT , uterine ).
Change of voice
Change in a nevusAbnormal lump in breast
An ulcer that does not heal……etc.
Specif ic procedures :
- Self examination of the breast .
- Mammography of breast .
8/10/2019 neoplasia 2015.ppt
http://slidepdf.com/reader/full/neoplasia-2015ppt 174/174
Mammography of breast .
- Serial PAP smears for the cervix.- Serial sputum cytology in smokers.
- Serial urine cytology in some cases, e.g. bilharziasis,workers in rubber.
Screening for genetic mutations in familial cancers.
Related Documents