Needs Analysis Concerning Interpreting in the Turkish Public Health Sector İbrahim Dereboy & Jonathan Ross Boğaziçi University, Istanbul WHO-HPH Task Force on Migrant-Friendly and Culturally Competent Health Care COST Action HOME (Health and Social Care for Migrants and Ethnic Minorities in Europe) Reggio Emilia Meeting

Needs Analysis Concerning Interpreting in the Turkish Public Health Sector İbrahim Dereboy & Jonathan Ross Boğaziçi University, Istanbul WHO-HPH Task Force.
Dec 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Needs Analysis ConcerningInterpreting in the
Turkish Public Health Sector
İbrahim Dereboy&
Jonathan Ross
Boğaziçi University, Istanbul
WHO-HPH Task Force on Migrant-Friendly and Culturally Competent Health Care
COST Action HOME (Health and Social Care for Migrants and Ethnic Minorities in Europe)
Reggio Emilia Meeting
• The place of the Turkish partner within the TRICC project.– Cultural Mirroring
• Description / Analysis of– Turkish Health Service– Problems / Challenges of THS– Common Beliefs / Expectations / Practices of
» Turkish Health Workers» Turkish Citizens
– Culture-specific (?) aspects of doctor-patient interaction
– Research on challenges in medical communication in the Turkish public health sector

Research Aims• To establish the extent, common aspects and
challenges of interpreter-mediated encounters in public sector hospitals in Eastern / South Eastern Anatolia.– This region chosen based on the assumption that
problems in medical communication are especially prevalent in those areas with a predominantly Kurdish-speaking (Kurmandji , Zazaki and Gorani) population. • + Feudal social structure• + Patriarchal cultures• + Religious conservatism

Ethnic Groups in Turkey
Source: www.konda.com.tr (2006)

Regions of Turkey
Source: http://www.mezatforum.com/forum/showthread.php?t=5047
Previous findings…
• Turkish Medical Association Report, Health Service Provision and Problems of Health Workers in the South East (1994)– More than half of the doctors interviewed needed a
third person to interpret between them and patients.• Dr. Selçuk Mızraklı (head of Diyarbakır Chamber of
Medicine) in Güney Doğu Ekspres newspaper, 10th August 2009– 2/3 of doctors serving in Eastern / South Eastern
Anatolia don’t know Kurdish – 1/3 of patients don’t know Turkish
Two questionnaires
• For patients and companions / interpreters at two state hospitals (Van / Diyarbakır)– n=100• 54 patients• 46 companions
– Face-to-face questionnaire• For doctors – n= max. 3000– Online survey
Findings of the first questionnaire• 46 out of 54 patients interviewed came to see
the doctor with a companion• ‘In contrast to the findings of research mostly carried out in
the USA and Europe, my data indicate that the third party in this study -and if we are to make generalizations, in Turkey- is present in the room to (1) deal with the chores of the hospital and bureaucracy, (2) to hear the medical information provided by the doctor at first hand, and (3) to provide physical and/or psychological support to the patient. However, contrary to what one might expect, or at least what I expected, the third party is not silent during the talk. Therefore, the last motivation behind the third party’s presence is (4) to take medical decisions instead of, or together with, the patient.’
– Özge Çaglar Aksoy, Ph.D. Student at Lancaster University, UK: Discourse Analysis of Research on Trialogues in an Ankara Oncology Ward
Q4. Did the patient communicate with the doctor using a language other than Turkish? Yes 46 (Directly? Via an interpreter?)No 8
Q6. If an interpreter was used: was the communication with the doctor successful?Very successful 2Successful 10Not very successful 26Unsuccessful 8

Q8. What kind of difficulties did the interpreter face while interpreting?
• Translation skills insufficient– Lack of terminology– Difficulty in finding ‘equivalents’– Inclination to add his / her version of the story
• Patient not comfortable in relating all problems with interpreter present– Issue of intimacy / Mahremiyet
• Doctor’s language too complex
HASTA HAKLARI YÖNETMELİĞİHASTA HAKLARI YÖNETMELİĞİ (1998) (1998)[REGULATION ON PATIENTS’ RIGHTS][REGULATION ON PATIENTS’ RIGHTS]
Article 18 (Principle of Provision of Information)‘Information should be supplied to the patient in a comprehensible manner, using an interpreter if necessary…’
–Who is the interpreter?–Who arranges & pays the interpreter?• Currently no other legislation in Turkey regulating
medical interpretation (unlike legal interpreting).
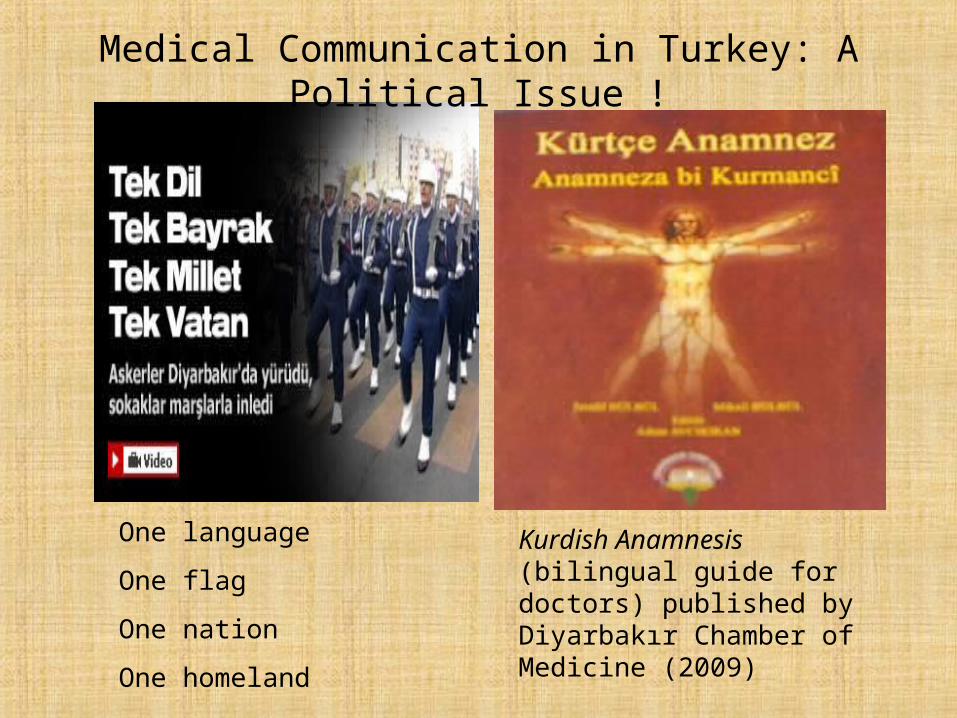
One language
One flag
One nation
One homeland
Kurdish Anamnesis (bilingual guide for doctors) published by Diyarbakır Chamber of Medicine (2009)
Medical Communication in Turkey: A Political Issue !

“Mother Tongue and Health” symposium organised by Turkish Medical Association and the health workers’ union
“Mesopotamia Health Days” trilingual (Turkish, English, Kurmandji) congress, Diyarbakır, 2009 & 2010
Ground- / Taboo-breaking Meetings

“Kurdish-speaking doctors hard at work” (Medimagazin, 20/08/2010)
•Adıyaman State Hospital reports an increase in the number of patients consulting Kurdish-speaking doctors.•One lung specialist has particularly attracted attention from local villagers and serves as an interpreter for other colleagues.• Chief doctor explains this new approach with reference to Atatürk‘s phrase “The peasant is the true master of the nation.”

Relevance to ‘cultural competence’?• In the case of patients from Turkey, for instance,
health workers need to be aware of …– Ethnic, cultural and linguistic diversity within the
country– The heavily political character of all issues
concerning language, including language & health care
– The realities on the ground: change, and the coexistence of conventional and innovative beliefs and practices
Related Documents











