VOL 22, NO. 1, 1996 Mental Disorder and Criminality: Male Schizophrenia 69 by Jlrl Modestln and Roland Ammann Abstract This study investigated lifetime prevalence of criminal behavior in a population of male schizo- phrenia patients. A total of 282 schizophrenia patients was di- vided into three subgroups (rep- resenting schizophreniform dis- order, acute schizophrenia, and chronic schizophrenia). The same number of control subjects was drawn from the general popula- tion and matched with the pa- tients for sex, age, marital status, occupational level, and commu- nity size. The full account of conviction records in the crimi- nal register was used as a meas- ure of criminal behavior. Patients were 5 times more likely to have been convicted of violent crimes, 2V4 times more likely to have been convicted of crimes against property, and almost 3 times more likely to have violated drug laws. Criminality rates in schizophrenia depended, how- ever, not only on the type of offense but also on the type or stage of the illness, which con- tributes to criminal behavior to some extent independently of sociodemographic factors. Schizophrenia Bulletin, 22(1): 69-82, 1996. Crime and mental disorder are dif- ficult to relate to each other. Both are difficult to define, heteroge- neous, and partially determined by culture (Gunn 1977). Most studies of mental disorder and criminality have been based on unselected groups of discharged male psy- chiatric patients, differing propor- tions of whom have suffered from schizophrenia. In these studies, ar- rest rate was taken as a measure of criminal behavior, and compar- isons were made at best with the general population. Some of these studies showed a higher arrest rate in mental patients than in the general population overall (Cocozza et al. 1978; Sosowsky 1978, 1980; Steadman et al. 1978; McFarland et al. 1989), some, more arrests for particular offenses (Rap- peport and Lassen 1965; Giovan- noni and Gurel 1967; Zitrin et al. 1976), and others, more arrests for patients with prior police records (Melick et al. 1979). In contrast, some older studies reported either no differences in arrest rate, or fewer arrests in patients than in the general population (Pollock 1938; Cohen and Freeman 1945). The same trend has been observed in rural settings (Durbin et al. 1977), in cases where adequate fol- lowup was provided (Lafave et al. 1993), and in patients not pre- viously convicted (Cook 1983; Shore et al. 1990). There seems to be a positive correlation between criminality and the acuity of pa- tients' illness (Bovier et al. 1987; Link et al. 1992; Taylor 1993; Mulvey 1994). Correlations have also been made with lack of active treatment (Green 1981; Taylor 1987; Grubin 1991), delusions (Hafner and Boker 1982; De Pauw and Szulecka 1988), noncompliance with medication (McFarland et al. 1989), substance abuse (Bovier et al. 1987; McFarland et al. 1989; Swanson et al. 1990), homelessness (Martell 1991), and prior arrests (Melick et al. 1979; Shore et al. 1989; Cirincione et al. 1992). Reprint requests should be sent to Dr. J. Modesrin, Psychiatric University Hospital Zurich, Lenggstrasse 31, CH-8029 Zurich 8, Switzerland. Downloaded from https://academic.oup.com/schizophreniabulletin/article/22/1/69/1919225 by guest on 21 August 2022

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
VOL 22, NO. 1, 1996 Mental Disorder andCriminality: MaleSchizophrenia
69
by Jlrl Modestln andRoland Ammann
Abstract
This study investigated lifetimeprevalence of criminal behaviorin a population of male schizo-phrenia patients. A total of 282schizophrenia patients was di-vided into three subgroups (rep-resenting schizophreniform dis-order, acute schizophrenia, andchronic schizophrenia). The samenumber of control subjects wasdrawn from the general popula-tion and matched with the pa-tients for sex, age, marital status,occupational level, and commu-nity size. The full account ofconviction records in the crimi-nal register was used as a meas-ure of criminal behavior. Patientswere 5 times more likely to havebeen convicted of violent crimes,2V4 times more likely to havebeen convicted of crimes againstproperty, and almost 3 timesmore likely to have violateddrug laws. Criminality rates inschizophrenia depended, how-ever, not only on the type ofoffense but also on the type orstage of the illness, which con-tributes to criminal behavior tosome extent independently ofsociodemographic factors.
Schizophrenia Bulletin, 22(1):69-82, 1996.
Crime and mental disorder are dif-ficult to relate to each other. Bothare difficult to define, heteroge-neous, and partially determined byculture (Gunn 1977). Most studiesof mental disorder and criminalityhave been based on unselectedgroups of discharged male psy-chiatric patients, differing propor-tions of whom have suffered fromschizophrenia. In these studies, ar-rest rate was taken as a measure
of criminal behavior, and compar-isons were made at best with thegeneral population. Some of thesestudies showed a higher arrestrate in mental patients than inthe general population overall(Cocozza et al. 1978; Sosowsky1978, 1980; Steadman et al. 1978;McFarland et al. 1989), some, morearrests for particular offenses (Rap-peport and Lassen 1965; Giovan-noni and Gurel 1967; Zitrin et al.1976), and others, more arrests forpatients with prior police records(Melick et al. 1979). In contrast,some older studies reported eitherno differences in arrest rate, orfewer arrests in patients than inthe general population (Pollock1938; Cohen and Freeman 1945).The same trend has been observedin rural settings (Durbin et al.1977), in cases where adequate fol-lowup was provided (Lafave et al.1993), and in patients not pre-viously convicted (Cook 1983;Shore et al. 1990). There seems tobe a positive correlation betweencriminality and the acuity of pa-tients' illness (Bovier et al. 1987;Link et al. 1992; Taylor 1993;Mulvey 1994). Correlations havealso been made with lack of activetreatment (Green 1981; Taylor 1987;Grubin 1991), delusions (Hafnerand Boker 1982; De Pauw andSzulecka 1988), noncompliancewith medication (McFarland et al.1989), substance abuse (Bovier etal. 1987; McFarland et al. 1989;Swanson et al. 1990), homelessness(Martell 1991), and prior arrests(Melick et al. 1979; Shore et al.1989; Cirincione et al. 1992).
Reprint requests should be sent toDr. J. Modesrin, Psychiatric UniversityHospital Zurich, Lenggstrasse 31,CH-8029 Zurich 8, Switzerland.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/1/69/1919225 by guest on 21 August 2022

70 SCHIZOPHRENIA BULLETIN
Samples of (mostly) randomlyselected male prisoners or peniten-tiary inmates have also been stud-ied to determine the prevalence ofmental disorders. In these subjectsthe lifetime prevalence of schizo-phrenia was found either to becomparable to that in the commu-nity (Guze 1976; Bland et al. 1990;Gunn et al. 1991) or to exceed it—especially with concurrent sub-stance abuse (Taylor and Gunn1984; C6t<§ and Hodgins 1990;Abram and Teplin 1991). The spe-cial group of persons found notguilty by reason of insanity orjudged incompetent to stand trialor unfit to plead consists mainlyof chronic mental patients (Bloomet al. 1992), the majority of whomsuffer from schizophrenia (Pfeifferet al. 1967; Pasewark et al. 1979;Hodgins and He"bert 1984; Reichand Wells 1985; Lamb et al. 1988;Grubin 1991). Schizophrenia pa-tients seem also to be overrepre-sented among mentally disordered,seriously violent offenders (Hafnerand Boker 1982), murderers (Lind-qvist 1986; Gottlieb et al. 1987),and murderers diagnosed as men-tally ill (Lanzkron 1963; Millaud1989; Fido et al. 1992). Matricideseems to be highly specific toschizophrenia patients (Gillies 1965;Green 1981).
In a general population birthcohort study, men with a majormental disorder, including schizo-phrenia, were found to be 2.6times more likely to have beenconvicted of a criminal offensethan healthy men and were regis-tered for more crimes of everytype (Hodgins 1992). In two well-controlled field studies, self-reported violence correlated withmental illness, including schizo-phrenia (Swanson et al. 1990; Linket al. 1992).
Studies of criminality and mentalillness devoted specifically toschizophrenia are rare. A highproportion (49%) of twins withschizophrenia had criminal records(Coid et al. 1993). Schizophreniapatients have been found to fre-quently be threatening and violentbefore admission (Tardiff andSweillam 1980; Humphreys et al.1992) and to have frequent contactwith the police after discharge,though charges are usuallydropped (Johnstone et al. 1991). Ina sample of ICD-8 (World HealthOrganization 1967) males withschizophrenia, the proportion ofcriminally registered persons wasthe same as in the general popula-tion, though they had committedalmost four times as many violentoffenses (Lindqvist and Allebeck1990). Substance abuse representeda risk factor for criminal behaviorin this population (Lindqvist andAllebeck 1989; Soyka et al. 1993).No differences in self-reportedcriminality were found betweenschizophrenia patients and normalpatients (Chuang et al. 1987) andbetween offenders with schizophre-nia and matched nonoffenderswith schizophrenia (Schanda et al.1992). Also, a lower postdischargecriminality recidivism rate wasfound in offenders with schizo-phrenia than in matched offenderswithout schizophrenia who werereferred for pretrial psychiatric as-sessments (Rice and Harris 1992).
In sum, the studies performedafter 1965 demonstrate that mentalpatients' total arrest or convictionrates equal or exceed the corre-sponding general population rates.The latter finding has repeatedlybeen explained with the deinstitu-tionalization or criminalization hy-pothesis: Mentally ill offendersare more frequently arrested and
shifted into the penal system nowbecause of unavailability of mentalhealth disposition resulting frommore stringent commitment crite-ria, more rapid discharges frompsychiatric hospitals, refusal ofthese hospitals to admit especiallydangerous patients, lack of psychi-atric beds, inadequate communitymental health resources, and so on(Rabkin 1979; Borzecki and Wor-mith 1985; Abram and Teplin 1991;Davis 1992). Accordingly, some re-searchers have found an increasingproportion of State mental hospitalpatients with prior arrests (Co-cozza et al. 1978; Melick et al.1979) and of young, mentally illincoming prisoners (Jemelka et al.1989). Among homeless persons,those who had previous psychiat-ric hospitalizations were most fre-quently involved in criminal be-havior (Gelberg et al. 1988). Otherresearchers, however, have foundlittle evidence that seriously men-tally disturbed persons are prefer-entially placed in jails (Monahan etal. 1979) and have stressed biasesin practically all studies (Wesselyand Taylor 1991).
The present investigation wascarried out to deepen our knowl-edge of criminal behavior in schiz-ophrenia patients. We restrictedour study to males, who are re-sponsible for 85 to 90 percent ofcriminal offenses. Particular sub-groups of mental patients shouldbe studied (Cirincione et al. 1992),since criminality rates among themdiffer (Coid et al. 1993). The pres-ent study has six outstanding fea-tures. (1) Schizophrenia patientsexclusively were studied (diagnosiswas based on modern opera-tionalized diagnostic criteria). (2)The patients were compared witha carefully matched control groupdrawn from the general popula-
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/1/69/1919225 by guest on 21 August 2022
VOL. 22, NO. 1, 1996 71
tion. (3) Both patients and controlsubjects were recruited from thesame catchment area. (4) The datawere tested and found to be reli-able. (5) A full account of courtconvictions was used as an objec-tive measure of criminal behavior.(6) Lifetime prevalence of criminalbehavior was investigated.
Methods
Subjects. Our subjects weremales with schizophrenia hospi-talized at least once at the Psychi-atric University Hospital of Bemefrom 1985 to 1987. (The hospitalprovides complete care for all res-idents of the catchment area whoneed inpatient psychiatric treat-ment.) Eligible patients fulfilled thefollowing criteria: They were be-tween 18 and 78 years old at thetime of data collection (1987); toour knowledge, they were stillalive by the end of 1989; they metthe Research Diagnostic Criteria(RDC; Spitzer et al. 1978) forschizophrenia; and basic demo-graphic data were available, mak-ing identification of matched con-trol subjects possible. A total of1,590 men were treated in the hos-pital in the 3-year study period.Of these, 78 were excluded be-cause they did not fulfill the agecriteria. The 1,331 patients whohad received the clinical diagnosisof schizophrenia or a related disor-der (ICD-9 [World Health Organi-zation 1978] Nos. 295 [except295.7], 297-298 [except 298.0]; n -369), alcohol abuse/dependency(ICD-9 Nos. 291, 303, 304.7/8/9,305.0/9; n - 624), or affective dis-order (ICD-9 Nos. 295.7, 2%,298.0, 300.4, 301.1, 308.0/4,309.0/1/4, 311, 312.3, 313.1/8; n -338) were rediagnosed with thehelp of the RDC.
Using the method of retrospec-tive evaluation of clinical charts,RDC schizophrenia was diagnosedin 292 patients, 246 (84%) ofwhom had been clinically diag-nosed with schizophrenia. For fourof these patients, matching wasnot possible; for two no controlperson could be found. One pa-tient was known to have died,and three dropped out for otherreasons. Thus, 282 patients werequalified for the study. DSM-IH-R(American Psychiatric Association1987) criteria for schizophreniawere also applied and found to befulfilled in 224 (79%) of these pa-tients. In contrast to RDC, DSM-III-R requires deterioration in psy-chosocial functioning and a sub-stantially longer symptom duration(6 months vs. 2 weeks).
The control group was selectedfrom the catchment area's generalpopulation. The registration of thepopulation in Switzerland takesplace at the level of highly inde-pendent local communities. To ob-tain a matched control group, wecontacted the local authorities in55 out of 101 communities in thecatchment area; 42 were willing tocollaborate. With the exception ofthe city of Beme, each local au-thority was provided with the se-lected patients' demographic data,along with the initials of the po-tential controls (the next in the al-phabet following the initials of thepatients' names) to indicate thestarring point for the search in thecommunity file. These files registerall inhabitants whose permanentplace of residence is in the par-ticular communities. Temporary ab-sences, including long hospital orprison stays, do not lead to exclu-sion from the file. We instructedour collaborators from the respec-tive local authorities by phone un-
til we were sure they understoodthe procedure well. Phone callswere followed up by writteninstructions.
We were careful to recruit bothpatients and controls from commu-nities of comparable size in thesame catchment area. The collab-orators searched the files for per-sons of the same sex, age (± 2years), marital status, and occupa-tional level, the latter to allow thesocial class designation accordingto Moore and tQeining (1960) andmodified by Dilling and Weyerer(1978). For the city of Beme itself,we received the coded list of allinhabitants containing the appro-priate data, and we looked forcontrols ourselves.
Hospital clinical records of all282 patients were scrutinized andrelevant data extracted by an in-vestigator (R.A.) blind to the pa-tients' criminal status. These demo-graphic and psychosocial variableswere evaluated: age, marital status,foreign-born status, place of res-idence, educational level, highestsocial class ever reached by thepatient and his family, intergenera-tional social mobility, living andvocational situation at the time ofindex admission, and guardianshipmeasures. The psychiatric variablesexamined included RDC andDSM-III-R diagnosis of schizo-phrenia, age at first psychiatrictherapy, age at first psychiatrichospitalization, duration of psychi-atric illness, number and durationof psychiatric hospitalizations, totaltime spent in psychiatric hospitals;psychiatric disorders leading tohospitalization and alcoholism infirst-degree relatives; broken home,childhood abuse, aggressive be-havior, previous suicide attempts,and alcohol and drug abuse (as-sessed with the help of RDC). All
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/1/69/1919225 by guest on 21 August 2022
72 SCHIZOPHRENIA BULLETIN
references in the hospital charts tocriminal activity and to psychiatrichospitalizations resulting from de-compensation during arrests werealso noted. All variables wereeither clearly determinable (e.g.,age) or were defined and opera-tionalized as exactly as possible(e.g., patients were judged as com-ing from broken homes if at leastone parent or parent surrogatewas lacking for at least 2 yearsbefore age 18; the first contactwith psychiatric services was de-cided to represent the beginning ofthe illness). In the absence of clearpositive chart information (e.g., nomention of suicide attempts), nega-tive ratings were encoded.
Clinical charts give informationof sufficient validity and reliabilityprovided they are filled out prop-erly (Csernansky et al. 1983). Ourclinical charts were generally ofacceptable quality, and the ratingswere reliable. A total of 66 clinicalcharts (15 of 282, every 20th of1,331, all studied in the same way)were evaluated independently bytwo other investigators. The threescorings were compared with eachother; four variables of low re-liability were excluded from theanalysis. The average correlationcoefficients for all continuous vari-ables included in the analysis werebetween 0.90 and 1.00. The aver-age weighted kappas (Spitzer et al.1967) for all the variables listedabove (12 variables including twocategories, 8 variables includingthree to six categories) were be-tween 0.70 and 1.00. In manycases the charts included psychia-trists' expert opinions and clinicalrecords from other psychiatric in-stitutions. Therefore, hardly anydata were missing. Social class ofthe family of origin could not beidentified in 32 patients, educa-
tional level in 4 patients, work sit-uation before index admission in 3patients, and living situation at in-dex admission in 1 patient.
In this study, full account ofconviction records in the criminalregister served as a measure ofcriminal behavior. Individuals'criminal activity in Switzerland isregistered most completely in theSwiss Central Criminal Record De-partment. All court convictions arerecorded, except for some smallfines and trivial offenses. No com-pulsory registration is required forthose under age 18, and no regis-tration at all is required for thoseover age 80. The Division of PenalControl of the Canton of Berneregisters convictions of citizens ofBerne; here, even some minor lawinfractions not registered by theSwiss Central Criminal Record De-partment are recorded. Registrationof some minor offenses can be de-leted by the Swiss Central Crimi-nal Record Department after 15years and by the Division of PenalControl of the Canton of Berne af-ter 3 years.
After the names of the studysubjects had been forwarded by us(in the case of the patients) andby the local authorities (in thecase of the controls) to the SwissCentral Criminal Records Depart-ment and to the Division of PenalControl of the Canton of Berne,we were provided with data in-dicating the type and number oflaw infractions and the type andnumber of sentences. The proce-dure corresponded to the Instruc-tions of the Swiss Government fortreating personal data for scientificpurposes (issued March 16, 1981)and was approved by the repre-sentative of the Canton of Berneresponsible for questions of dataprotection. Full confidentiality was
strictly maintained throughout thestudy. Altogether, we were able tostudy life prevalence (starting atthe age of 18) of all infractionsleading to prison sentences ofmore than 3 months duration, allinfractions committed in the prior15 years and leading to fines of atleast 500 Swiss francs (sFr) orprison sentences, and all infrac-tions committed in the prior 3years and leading to fines of atleast 200 sFr (or 80 sFr in the caseof traffic law violations).
Statistics. Statistical analysis usedthe chi-square test (with continuitycorrection when appropriate) andFisher exact test for categoricalvariables. The f-test and the non-parametric Kruskal-Wallis test wereused for continuous variables. Tocompare the likelihood of commit-ting offenses in patients and con-trols, odds ratios were calculated.As a multivariate procedure, astepwise discriminant analysis wasused to select the set of variablesbest discriminating between pa-tients with and without criminalrecords. The significance level forthe variables to enter and stay inthe model was 0.05. In the entirestudy, only results yielding ap-value of 0.05 or less were con-sidered statistically significant.
Results
First, our 282 schizophrenia pa-tients were compared with thegeneral male population of thecatchment area aged 18 to 78.Highly significant differences inthe matching criteria were found:The patients were younger (meanage - 39 vs. 43), mostly single(85% vs. 33%), of low social class(64% vs. 32%) and resided more
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/1/69/1919225 by guest on 21 August 2022

VOL 22, NO. 1, 1996 73
frequently in the city of Berne(40% vs. 33%).
All 282 patients fulfilled theRDC criteria for schizophrenia.Nevertheless, the group was het-erogeneous. Therefore, it was di-vided into three subgroups: (1) 58patients fulfilling RDC criteria forschizophrenia but not DSM-III-Rcriteria for schizophrenia (schizo-phreniform disorder subgroup); (2)160 patients fulfilling both RDCand DSM-UI-R criteria for schizo-phrenia and hospitalized less than1 year (acute schizophrenia sub-group); and (3) 64 patients ful-filling both RDC and DSM-III-Rcriteria for schizophrenia and hos-pitalized more than 1 year duringthe index hospitalization (chronicschizophrenia subgroup).
The sample's heterogeneity wasconfirmed by significant differencesbetween the three subgroups inmatching criteria and in personal,social, and illness-related variables.Patients with schizophreniformdisorder more frequently wereforeign-born and came from bro-ken homes. Most had regular jobsbefore index admission, and theirhospitalizations were shorter. Incontrast, the chronic schizophreniasubgroup consisted of older pa-tients who were more severely ill,had been ill longer, and weremore socially handicapped. Thepatients of all three subgroups fellill at a similar mean age of 25years. The increasing mean illnessduration (7, 11, and 30 years) andmean total duration of psychiatrichospitalizations (0.5, 2.5, and 23years) reflect the increasing illnessseverity across the three sub-groups. These figures also yield anestimate of the mean risk periodfor the patients of the three sub-groups: 65, 8.5, and 7 years.
Table 1 compares criminal be-
havior in the patient and controlsamples. The criminal registrationrate was similar for patients andcontrols in the total sample aswell as in the three subgroups; thepatients were not criminally regis-tered more frequently than theircorresponding controls. In agree-ment with this finding, no dif-ferences in kind of sentence werefound between patients and con-trols, except for the expectedhigher rate of psychiatric measures(i.e., sentences to psychiatric treat-ment) in the case of the patients(12% vs. 3%). Altogether, 34 per-cent of patients and 36 percent ofcontrols had criminal records. Thehigh percentage of controls withcriminal records underscores theneed for matching; only 15 percentof the general male population ofthe Canton of Berne had a crimi-nal record.
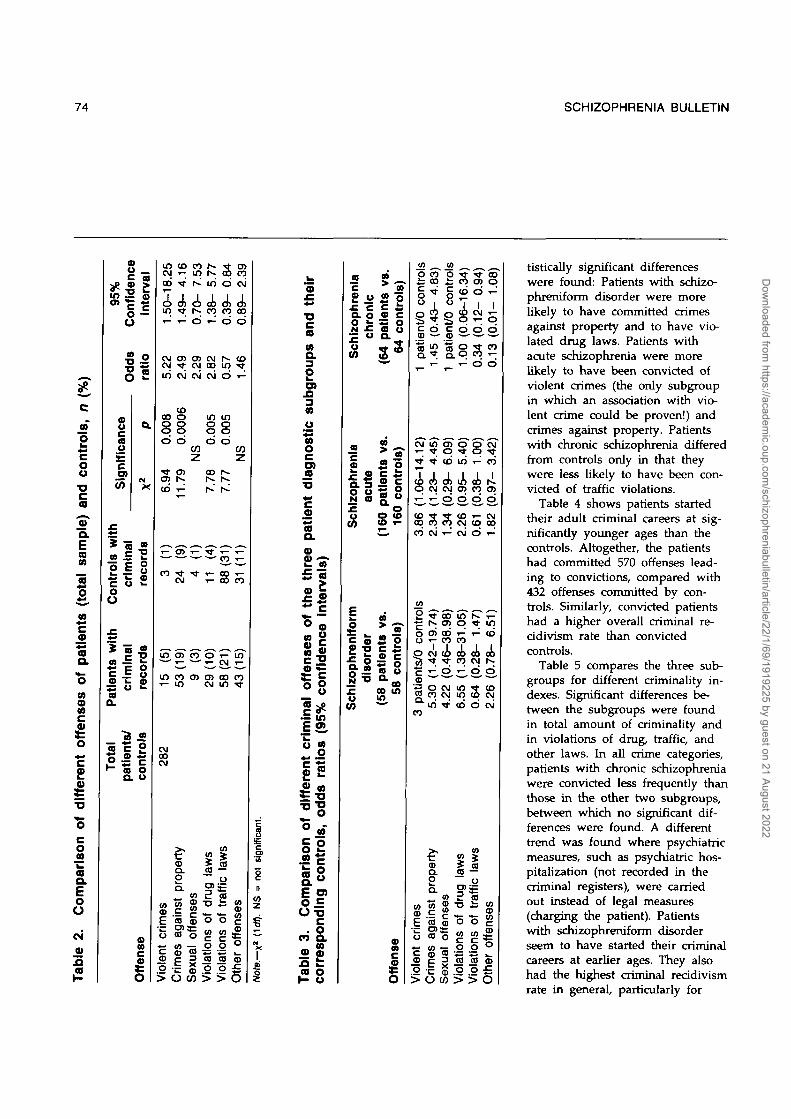
Significant differences betweenpatients and controls appearedwhen individual crime categorieswere considered (table 2). Patientswere five times more likely tohave been convicted of violentcrimes, 2Vi times more likely tohave been convicted of crimesagainst property, and almost 3times more likely to have violateddrug laws. In contrast, they wereless likely to have violated trafficlaws. Nevertheless, traffic viola-tions and property crimes werethe most frequent offenses. Mostviolent crimes were assaults result-ing in bodily harm. One murderwas identified (a 46-year-old mandiagnosed with schizophreniformdisorder at index hospitalizationhad committed murder 9 yearsbefore).
Table 3 compares the three di-agnostic subgroups with the cor-responding controls in type ofcriminal offense. The following sta-
c
iCO
trol
su
l
ou•g
tch
COE
• o
CO
0)ea.E
**0)
COao
•28£"5c
imi
u
tal
0
0
UO
8ed
ui<
oO
(0
m
*(0
|
ou
Ith*c—aa.
To
tal
nee
fid
e
cp
Od
ds
Inal
e
:rln
Inal
Ul|.
op
atie
nt
CD
terv
c
rati
ord
s
o
2
irds
8C
CO
con
tro
CO
5c5d
0.92
36)
|
34)
r>-c»
282
ECOCO
so
in00
5d
98
0
co-co^ • • ^
CVJ
33)
O)
s
8
|
reni
x:Q.ON!cuCO
CO00
d
1.17
CO
CVJCO
43)
00CO
160
0
3
a, a
cre
ni
.cQ.ON
SIo
CO
s
d
0.44
c?• ^
16)
o
sm
ic
£u
reni
Q.oNx:cv5
con
and
nts
tie
S
B
fI
n c
rimin
al
%iCDV
eren
•a
"c
c"32c
f*~**Mxao
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/1/69/1919225 by guest on 21 August 2022
74 SCHIZOPHRENIA BULLETIN
a*.c
itro
ls,
oo•oca
'3TQ.
tal
sam
o
CO
aQ.
oCO
nse
CD
o
20)
•o
"o
riso
n
COQ .
Com
CN
9)
t
ir<r
(
1
ntr
ols
'
oo
ithat
ien
ts w
O.
ota
l
t—
COu _C M
iterv
i
o —u
•S °•o rO 2
nee
a0E
75
E•co
crim
inal
aa
a
(0
o
reco
rds
ce
ntr
o
8
S
Off
ei
inCM
oo
in
CMCMin
oo8d
CO
CO
12-in
282
coCD
nt
crim
Vio
le
CO
•<*•
T -
O )
CM
COO
8d
1.79
CM
53
(19
]er
tyro
pi n
st
p
CO
in2o
o>OJ
CM
(0
z
CO.
nses
es
aga
al o
ffei
cCJ
CD
in
ooCOT-
CMCO
CM
in
.00
o
7.78
29 (
10)
CO
-
T3
tions
oV
iola
so
CO
o
f -i no
m8d
7.77
88 (
31;
58
(21
)
CO
as
o
iBCO
o
BIO
IA
O)COCM
0 0
o
CO
ifi
z
31 (
11]
43
( 15
)
COCDm
r of
fem
i
ICD
not
D
w
fX1I
thei
i•o
(0
s.sCO
tic
aOcO)
dia
len
tth
ree
vals
)
"5"09 jZ
1 o
ffen
seco
nfld
er
•§ ^
is•t •§
O "
| |
28
Com
|d
ing
e 3.
Bsp
onT
abI
corn
m
iren
ii
ao
Z
UIJO
c
shiz
ophr
e
CO
o
o•g
cute
CO
CD•D
OJ»
s
c
1
§ce
itien
aa(O
V8.
•
58 p
atle
n!
rols
)on
ti
"3
"3"•3
ontr
S
ce0
58
con
tr
CDCO
Off
er
coO
cont
rt/
0
ca
c
CM
06-
1 —
CO0 0
CO
CO
2
8
1CD
CO
CO
1c•5>
CO
cc
i0
.45
T ~
10
23-
CO
CM
;i .4
2-
0CO
in
fP
nst
pi
a>
co
m
Crim
<
ols
cont
rt/0
CD
pati
a>0CO
29-
0
CO
r-
O)
CO*
0
CM
ises
al o
ffer
Sex
u
-16.
3
*
d
.00
0
i n95
-
0
COCM
CM
O
COiinmCO
co
«
f dr
ug
[O
SU
OI)
>
CJ)
d
0
0
8*-
38-
0
CO
0
28-
0
s0
I
\ tra
Hi
tions
ol
BIO
IA
0 0
- 1.
0.0
1-
0
1.13
0
CO
97-
0
OJ0 0^ *
inCO
78-
0
COCM
OJ
CO
O
5
tistically significant differenceswere found: Patients with schizo-phreniform disorder were morelikely to have committed crimesagainst property and to have vio-lated drug laws. Patients withacute schizophrenia were morelikely to have been convicted ofviolent crimes (the only subgroupin which an association with vio-lent crime could be proven!) andcrimes against property. Patientswith chronic schizophrenia differedfrom controls only in that theywere less likely to have been con-victed of traffic violations.
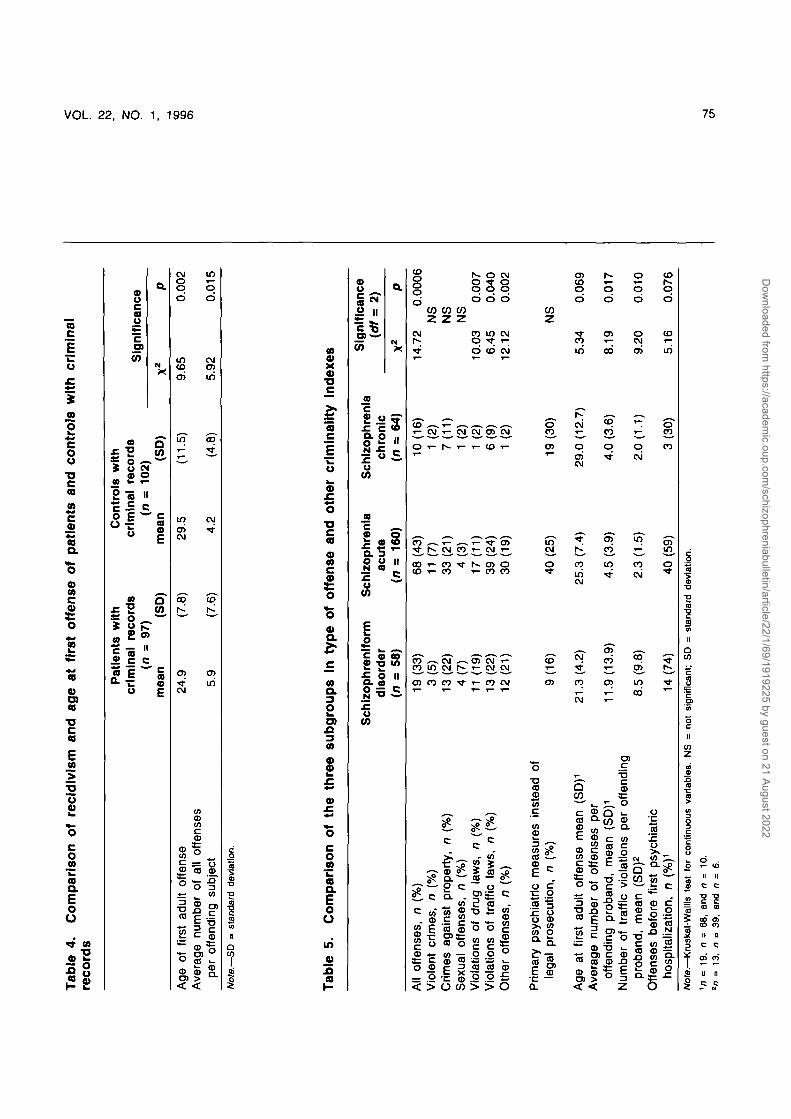
Table 4 shows patients startedtheir adult criminal careers at sig-nificantly younger ages than thecontrols. Altogether, the patientshad committed 570 offenses lead-ing to convictions, compared with432 offenses committed by con-trols. Similarly, convicted patientshad a higher overall criminal re-cidivism rate than convictedcontrols.
Table 5 compares the three sub-groups for different criminality in-dexes. Significant differences be-tween the subgroups were foundin total amount of criminality andin violations of drug, traffic, andother laws. In all crime categories,patients with chronic schizophreniawere convicted less frequently thanthose in the other two subgroups,between which no significant dif-ferences were found. A differenttrend was found where psychiatricmeasures, such as psychiatric hos-pitalization (not recorded in thecriminal registers), were carriedout instead of legal measures(charging the patient). Patientswith schizophreniform disorderseem to have started their criminalcareers at earlier ages. They alsohad the highest criminal recidivismrate in general, particularly for
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/1/69/1919225 by guest on 21 August 2022
Ta
ble
4
. C
om
pa
ris
on
o
f re
cid
ivis
m
an
d a
ge
a
t fi
rst
off
en
se
o
f p
ati
en
ts
an
d c
on
tro
ls w
ith
c
rim
ina
lre
co
rds
O
Age
of
first
ad
ult
offe
nse
Ave
rage
nu
mbe
r of
all
offe
nses
per
offe
ndin
g su
bjec
t
Pat
ien
ts w
ith
crim
inal
re
cord
s(n
= 9
7)
mea
n
(SD
)
Co
ntr
ols
wit
hcr
imin
al
reco
rds
(n =
102)
mea
n
(SD
)
24.9 5.9
(7.8
)
(7.6
)
29.5 4.2
(11.
5)
(4.8
)
Sig
nif
ican
ce
9.65
5.92
0.00
2
0.01
5
O CO
CO o
Not
e.—
SD
••
sta
ndar
d de
viat
ion.
Ta
ble
5.
Co
mp
ari
so
n
of
the
th
ree
s
ub
gro
up
s
In t
yp
e
of
off
en
se
a
nd
oth
er
cri
min
ali
ty
ind
ex
es
All
offe
nses
, n
(%
)V
iole
nt c
rim
es,
n (
%)
Crim
es a
gain
st
prop
erty
, n
(%
)S
exua
l of
fens
es,
n (
%)
Vio
latio
ns o
f dr
ug l
aws,
n (
%)
Vio
latio
ns of
traf
fic
law
s, n
(%
)O
ther
off
ense
s, n
(%
)
Prim
ary
psyc
hiat
ric
mea
sure
s in
stea
d of
lega
l pr
osec
utio
n, n
(%
)
Age
at
first
ad
ult
offe
nse
mea
n (S
D)1
Ave
rage
num
ber
of
offe
nses
per
offe
ndin
g pr
oban
d, m
ean
(SD
)1
Num
ber
of
traf
fic
viol
atio
ns per
offe
ndin
gpr
oban
d, m
ean
(SD
)2
Offe
nses
be
fore
firs
t ps
ychi
atric
hosp
italiz
atio
n, n
(%
)1
Sch
izo
ph
ren
lfo
rmd
iso
rder
(n =
58
)
19(3
3)
3(5
)1
3(2
2)
4(7
)11
(19
)13(2
2)
12
(21
)
9(1
6)
21.3
(4.
2)
11.9
(13.9
)
8.5
(9.
8)
14 (7
4)
Sch
izo
ph
ren
iaac
ute
(n =
16
0)
68
(43
)11
(7)
33 (
21)
4(3
)1
7(1
1)
39 (
24)
30
(19
)
40 (25
)
25.3
(7.4
)
4.5
(3.9
)
2.3
(1.5
)
40 (59)
Sch
izo
ph
ren
iach
ron
ic(n
= 6
4)
10(1
6)
1 (
2)7
(11
)1
(2)
1 (
2)6
(9)
1 (
2)
19 (3
0)
29.0
(12
.7)
4.0
(3.
6)
2.0
(1.1
)
3(3
0)
Sig
nif
ican
ce
\QT
—
£
.)
X2
P
14.7
2 0.
0006
NS
NS
NS
10.0
3 0.
007
6.45
0.
040
12.1
2 0.
002
NS
5.34
0.
069
8.19
0
.01
7
9.20
0
.01
0
5.16
0.
076
Not
e.—
Kru
skal
-Wal
lls t
est
(or
cont
inuo
us v
aria
bles
. N
S =
not
sig
nific
ant;
SD
= s
tand
ard
devi
atio
n.1n
=1
9,(
1 =
68,
and
n =
10.
2n
= 1
3, n
o 3
9, a
nd n
= 6
.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/1/69/1919225 by guest on 21 August 2022
76 SCHIZOPHRENIA BULLETIN
traffic violations. Most had en-gaged in criminal activity beforetheir first psychiatric hospitai-ization.
Altogether, 57 patients (59%)with a criminal record had beenregistered for the first time beforetheir first psychiatric hospitaii-zation, and 40 (41%) afterward.Thus, the beginning of the crimi-nal behavior was quite equally dis-tributed around the time of thefirst inparient treatment. This find-ing could be confirmed for all of-fenses except violent crime: of the15 patients with criminal recordsfor violent crimes, 3 (20%) hadbeen convicted before, and 12(80%) were convicted after their
first hospitaiization. The patientswith criminal records before theirfirst hospitaiization were morelikely than patients without suchcriminal records to be criminallyactive later (47% vs. 18%).
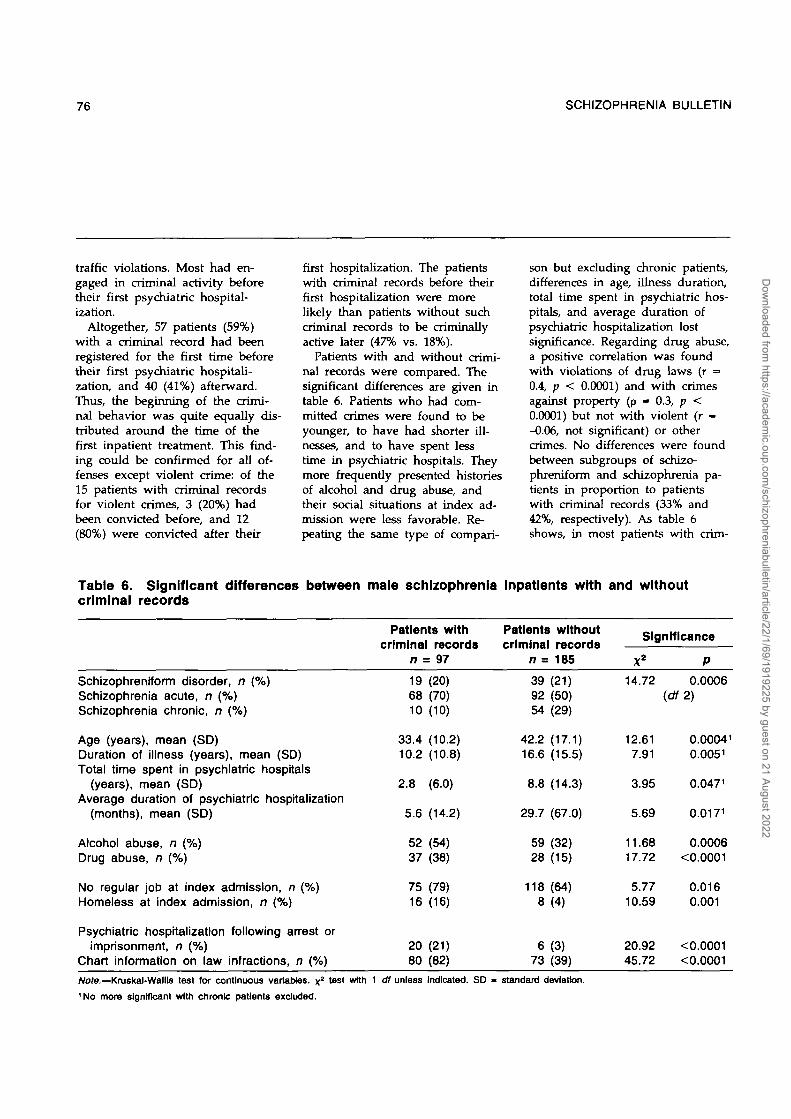
Patients with and without crimi-nal records were compared. Thesignificant differences are given intable 6. Patients who had com-mitted crimes were found to beyounger, to have had shorter ill-nesses, and to have spent lesstime in psychiatric hospitals. Theymore frequently presented historiesof alcohol and drug abuse, andtheir social situations at index ad-mission were less favorable. Re-peating the same type of compari-
son but excluding chronic patients,differences in age, illness duration,total time spent in psychiatric hos-pitals, and average duration ofpsychiatric hospitaiization lostsignificance. Regarding drug abuse,a positive correlation was foundwith violations of drug laws (r =0.4, p < 0.0001) and with crimesagainst property (p » 0.3, p <0.0001) but not with violent (r --0.06, not significant) or othercrimes. No differences were foundbetween subgroups of schizo-phreniform and schizophrenia pa-tients in proportion to patientswith criminal records (33% and42%, respectively). As table 6shows, in most patients with crim-
Table 6. Significant differences between male schizophrenia inpatlents with and withoutcriminal records
Patients withcriminal records
n = 97
Patients withoutcriminal records
n = 185
Significance
Schizophreniform disorder, n (%)Schizophrenia acute, n (%)Schizophrenia chronic, n (%)
Age (years), mean (SD)Duration of illness (years), mean (SD)Total time spent in psychiatric hospitals
(years), mean (SD)Average duration of psychiatric hospitaiization
(months), mean (SD)
Alcohol abuse, n (%)Drug abuse, n (%)
No regular job at index admission, n (%)Homeless at index admission, n (%)
Psychiatric hospitaiization following arrest orimprisonment, n (%)
Chart information on law infractions, n (%)
196810
33.410.2
2.8
5.6
5237
7516
2080
(20)(70)(10)
(10.2)(10.8)
(6.0)
(14.2)
(54)(38)
(79)(16)
(21)(82)
39 (21)92 (50)54 (29)
42.2 (17.1)
16.6 (15.5)
8.8 (14.3)
29.7 (67.0)
59 (32)28 (15)
118 (64)8 (4)
6 (3)73 (39)
14.72 0.0006(df2)
12.617.91
3.95
5.69
11.6817.72
5.7710.59
20.9245.72
0.000410.0051
0.0471
0.0171
0.0006<0.0001
0.0160.001
<0.0001<0.0001
Note—Kruskal-Wallis test for continuous variables, x1No more significant with chronic patients excluded.
test with 1 dl unless Indicated. SD - standard deviation.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/1/69/1919225 by guest on 21 August 2022

VOL 22, NO. 1, 1996 77
inal records, the law infractionswere noted in our clinical charts.Interestingly, law infractions werealso noted in almost 40 percent ofthe patients without criminalrecords.
The stepwise discriminant anal-ysis yielded the set of three vari-ables best discriminating betweenpatients with and without criminalrecords: drug abuse, homelessnessat index admission, and divorcedor widowed marital status. Dis-criminatory power of the model isvery modest (13% of explainedvariance), confirming the difficul-ties in differentiating between pa-tients with and without criminalrecords using the variables westudied. Likewise, the specificity ofthe model is 78 percent and itssensitivity only 55 percent.
Discussion
In contrast to many previous stud-ies of criminal behavior of mentalpatients, court convictions and notarrests were used here as a meas-ure of criminal behavior. Arrestrates are influenced by noncrimi-nological variables (Teplin 1985),do not indicate seriousness ofcrimes (Davis 1991), and do notdenote guilt, since criminal activityis necessarily determined only bya judge in court (Rabkin 1979).Only a small proportion of ar-rested patients are convicted(McFarland et al. 1989). Swiss lawdoes not recognize the categoriesof "incompetent to stand trial" or"not guilty by reason of insanity."All offenses—but serious offensesespecially (e.g., those involvingguns, easily available in Switzer-land)—are judged by the court,which may rule, however, for psy-chiatric instead of penal measures.These measures are also registered.
Conviction records are objectivebut may underestimate the crimi-nality of people with mental disor-ders. As reported, many patientsbreak the law or are violent beforehospital admission (Levine 1970;Tardiff and Sweillam 1980; Hum-phreys et al. 1992) without beingarrested (Lagos et al. 1977), andthe police avoid arresting those in-dividuals for minor crimes whoenter a mental hospital (Craft1984). Confronted with less seriousoffenses, Swiss police have consid-erable discretionary powers andcan present mentally disorderedsuspects to physicians (who maydecide on hospital referrals),charge them, or both. Accordingly,in almost 40 percent of our pa-tients without criminal records,some references to law infractionswere found in the clinical charts.Healthy people may be handledby Swiss police in less considerateways but may be better at con-cealing their offenses. Unfortu-nately, we do not know the fre-quency of undetected crime in thegeneral population, or whether un-recorded crimes favor the rela-tively healthy or the mentally dis-ordered (Taylor 1993).
All our patients were hospi-talized at least once for mentalproblems. There might be a selec-tion bias in comparing hospitalizedpatients with community controls,since the hospital entry procedurelikely selects patients at higher riskfor violence and therefore criminalconviction. Unfortunately, there isno community-based psychiatricregister in Switzerland. Most schiz-ophrenia patients, however, willhave been hospitalized at sometime during their patient career.For example, all 51 schizophreniapatients who contacted the psychi-atric outpatient service in Berne
during a 1-year period had beenhospitalized in the past (Hoffmann1994). Some of the mentally illcould have been included in ourcontrol group, which also mighthave contained some subjects withdrug abuse problems and person-ality disorders. Unfortunately, theschizophrenia and control groupscould not be matched for thesevariables. The effect that this lackof matching may have had on ourresults is not known. There aremethodological problems in study-ing crime in mental illness, and nosingle study will overcome themall (Wessely and Taylor 1991).
Significant differences werefound between our patient sampleand the general population inmatching criteria. These differences,along with the finding of a highpercentage of matched controlswith criminal records (36% vs.15% of the male general popula-tion) underline the importance ofmatching. Sex, age, marital status,place of residence, and social classare among the factors most signifi-cantly affecting crime rates (Guze1976; Braithwaite 1981; Rice andHarris 1992). Differences in thesevariables were found betweencriminal and noncriminal mentallyill patients (Beran and Hotz 1984),between imprisoned persons andthe general population (Bland etal. 1990), and among expatients,exoffenders, and the general popu-lation (Steadman and Felson 1984).Admittedly, controlling for factorsthat can themselves be influencedby mental disorder may be prob-lematic (Monahan 1993). For thisreason, the highest social classever achieved, rather than currentsocial class, was considered in ourstudy.
As our results indicate, thegroup of patients with RDC schiz-
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/1/69/1919225 by guest on 21 August 2022
78 SCHIZOPHRENIA BULLETIN
ophrenia is heterogeneous, andeven patients with the more nar-rowly defined DSM-IH-R schizo-phrenia do not represent a uni-form population. The subgroup oflong-stay/chronic inpatients espe-cially is different in being moreseverely ill and more handicapped.This heterogeneity is also reflectedin differences in criminal behavior.In both the total sample and thediagnostic subgroups, the samehigh proportions of criminally reg-istered individuals were found inthe patients as in the controls(34% vs. 36%). Significant dif-ferences appeared when differenttypes of offenses were considered,however, the diagnostic subgroupscontributed in various ways tothese differences. Altogether, asignificantly higher proportion ofpatients committed violent crimes,crimes against property, and drug-related crimes; a significantlylower proportion violated trafficlaws. Nevertheless, even in the pa-tients, traffic violations representedthe most common kind of offense.Patients with chronic schizophreniahad been convicted less frequentlythan patients in the other twogroups, in spite of their similarlylong mean risk period as patientsdischarged to the community. Be-cause they represent significantlyolder patients, the differences incriminality rates between them andother patients could result from acohort effect, particularly pro-nounced in violations of drug andtraffic laws. Compared with con-trols, patients with schizophreni-form disorder were 6Vi times morelikely to break drug laws, whilepatients with acute schizophreniawere 4 times more likely to havebeen convicted of violent crimes.In contrast to the latter finding,patients with schizophrenifonn dis-
order and chronic schizophreniawere found to be as likely as con-trols to commit violent crimes.These results explain the differentfindings of this and our previousstudy (Modestin and Ammann1995), in which no differences inthe frequency of violent crimeswere found between the groupconsisting of patients with ICD-9schizophrenia (74%) and schizo-phrenia-related disorders (26%)and the group of matched con-trols. That ICD-9 "schizophrenia"group will have contained only asmall proportion of DSM-II1-Racute schizophrenia patients ac-cording to our definition.
A higher recidivism rate wasfound in the patients than in thecontrols. The subgroup with schiz-ophreniform disorder especiallyhad a high recidivism rate, possi-bly because of traffic violations.Some of these patients may belongto a new generation of youngadult chronic outpatients present-ing with considerable social hand-icaps and stormy lifestyles yet notgetting the benefits of more ex-tended hospital treatment (Lamb1993).
Since we were not able to deter-mine the beginning of the illnessreliably, we cannot comment on itsrelationship to the beginning ofcriminal behavior. The finding of asignificant correlation (r - 0.66) be-tween age at first psychiatric con-tact and age at first conviction(Coid et al. 1993) could not bereplicated in this study (r - 0.17,p - 0.093). Generally, a patient canstart a criminal career at any age(Hodgins 1992). Our patientsstarted their adult criminal careersat significantly earlier ages thanthe controls, and a considerablenumber of patients, particularlythose with schizophrenifonn disor-
der and acute schizophrenia, hadalready been criminally active be-fore their first psychiatric hospital-ization. This was, however, not thecase for violent crimes: 12 of 15patients with histories of violentcrime had been hospitalized beforebecoming criminal. These data in-dicate that violent crime is moreclosely connected with the illnessthan other types of crime. Like-wise, violence was observed toprogress as the illness progressed(Taylor 1987). The finding thatpast criminality predicts futurecriminality (Melick et al. 1979;Shore et al. 1989; Cirincione et al.1992) could be fully confirmed.
Compared with noncriminalschizophrenia patients, our criminalpatients were younger and less ill.They were also more frequentlyinvolved in substance abuse andwere less well integrated socially(i.e., more frequently unemployedand homeless). The latter findingsremained significant even after thechronic schizophrenia subgroupwas excluded. It is possible thatsymptom acuity, which is knownto correlate with criminal behavior(Link et al. 1992; Taylor 1993), alsoinfluenced the social situations andsocial behavior of patients. How-ever, an independent—even ifmodest—contribution by these fac-tors to criminal behavior cannot beexcluded. May the deinstitutional-ization of patients have been im-portant in this context? Deinstitu-tionalization indeed took place inSwitzerland, but it was not com-plete, and patients were providedwith alternatives. However, be-cause they delay getting treat-ment—and often are noncompliantanyway—patients still are nottreated sufficiently despite theavailability of psychiatric services.
In sum, our results indicate that
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/1/69/1919225 by guest on 21 August 2022
VOL. 22, NO. 1, 1996 79
the question of criminality amongschizophrenia patients has to beconsidered less narrowly than ithas been. Altogether, schizophreniapatients were not found to havecriminal records more often thanmatched controls. However, theywere found to be more frequentlyregistered for particular types ofcrime further depending on thetype or, perhaps, the stage of ill-ness. These results were obtainedwith appropriate controls carefullymatched for sociodemogTaphic fac-tors. Contrary to a previous as-sumption (Monahan and Steadman1983), controlling for these factorsdid not cause a relationship be-tween crime and mental disorderto disappear. Our findings confirmthat mental illness helps explainsome kinds of criminal behaviorindependently of sociodemographicvariables (Link et al. 1992). How-ever, these findings must be putin perspective. We should not for-get that persons with mental disor-ders are responsible only for asmall fraction of the crime and vi-olence in society (Monahan 1993).Also, criminal acts performed bythe mentally ill are not necessarilyrelated to their mental disorders.Remitted psychotics can commitcrimes for the same reasons aspeople without psychiatric histor-ies—crimes for which they are justas responsible (Morissette 1986).Correspondingly, some of our pa-tients were sentenced for their of-fenses long after their first psychi-atric hospitalization.
References
Abram, K.M., and Teplin, L.A. Co-occurring disorders among men-tally ill jail detainees. AmericanPsychologist, 46:1036-1045, 1991.
American Psychiatric Association.DSM-III-R: Diagnostic and Statisti-cal Manual of Mental Disorders. 3rded., revised. Washington, DC: TheAssociation, 1987.
Beran, N.J., and Hotz, A.M. Thebehavior of mentally disorderedcriminals in civil mental hospitals.Hospital and Community Psychiatry,35:585-589, 1984.
Bland, R.C.; Newman, S.C; Dyck,R.J.; and Om, H. Prevalence ofpsychiatric disorders and suicideattempts in a prison population.Canadian Journal of Psychiatry,35:407-413, 1990.
Bloom, J.D.; Williams, M.H.; andBigelow, D.A. The involvement ofschizophrenic insanity acquitees inthe mental health and criminal jus-tice systems. Psychiatric Clinics ofNorth America, 15:591-604, 1992.
Borzecki, M., and Wormith, J.S.The criminalization of psychiat-rically ill people: A review with aCanadian perspective. PsychiatricJournal of the University of Ottawa,10:241-247, 1985.
Bovier, P.; Hilleret, H.; and Tissot,R. Meurtre et schizophrenic: L'av-ant et l'apr^s. L'Evolution Psychi-atrique, 52:729-753, 1987.
Braithwaite, J. The myth of socialclass and criminality reconsidered.American Sociological Review, 46:36-57, 1981.
Chuang, H.T.; Williams, R.; andDalby, J.T. Criminal behaviouramong schizophrenics. CanadianJournal of Psychiatry, 32:255-258,1987.
Cirincione, C; Steadman, H.J.;Robbins, P.C; and Monahan, J.Schizophrenia as a contingent riskfactor for criminal violence. Inter-national Journal of Law and Psychia-try, 15:347-358, 1992.
Cocozza, J.J.; Melick, M.E.; andSteadman, H.J. Trends in violentcrime among ex-mental patients.Criminology, 16317-334, 1978.
Cohen, L.H., and Freeman, H.How dangerous to the communityare State mental hospital patients?Connecticut State Medical Journal,9:697-700, 1945.
Coid, B.; Lewis, S.W.; and Reveley,A.M. A twin study of psychosisand criminality. British Journal ofPsychiatry, 162:87-92, 1993.
Cook, D.A.G. A study of criminalbehaviour in discharged male psy-chiatric patients. Medicine Scienceand the Law, 23:279-282, 1983.
Cote", G., and Hodgins, S. Co-occurring mental disorders amongcriminal offenders. Bulletin of theAmerican Academy of Psychiatry andthe Law, 18:271-281, 1990.
Craft, M. Who are mentally abnor-mal offenders? In: Craft, M., andCraft, A. eds. Mentally AbnormalOffenders. London, England:Bailliere Tindall, 1984. pp. 15-27.
Csernansky, J.G.; Yesavage, J.A.;Maloney, W.; and Kaplan, J. Thetreatment response scale: A retro-spective method of assessing re-sponse to neuroleptics. AmericanJournal of Psychiatry, 140:1210-1212,1983.
Davis, S. An overview: Are men-tally ill people really more dan-gerous? Social Work, 36:174-180,1991.
Davis, S. Assessing the "criminali-zation" of the mentally ill in Can-ada. Canadian Journal of Psychiatry,37:532-538, 1992.De Pauw, K.W., and Szulecka, K.Dangerous delusions: Violence andthe misidentification syndromes.British Journal of Psychiatry, 152:91-96, 1988.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/1/69/1919225 by guest on 21 August 2022
80 SCHIZOPHRENIA BULLETIN
Dilling, H., and Weyerer, S. Epi-demiologie psychischer Storungenund psychiatrischer Versorgung.Munich, Germany: Urban undSchwarzenberg, 1978.Durbin, J.R.; Pasewark, R.A.; andAlbers, D. Criminality and mentalillness: A study of arrest rates in arural state. American Journal ofPsychiatry, 134:80-83, 1977.
Fido, A.A.; Razik, MA.; Mizra, I.;and El-Islam, M.F. Psychiatric dis-orders in prisoners referred for as-sessment: A preliminary study. Ca-nadian Journal of Psychiatry, 37:100-103, 1992.
Gelberg, L.; Linn, L.S.; and Leake,B.D. Mental health, alcohol anddrug use, and criminal historyamong homeless adults. AmericanJournal of Psychiatry, 145:191-196,1988.Gillies, H. Murder in the west ofScotland. British Journal of Psychia-try, 111:1087-1094, 1965.
Giovannoni, J.M., and GureL L.Socially disruptive behavior of ex-mental patients. Archives of GeneralPsychiatry, 17:146-153, 1967.
Gottlieb, P.; Gabrielsen, G.; andKramp, P. Psychotic homicides inCopenhagen from 1959 to 1983.Acta Psychiatrica Scandinavica,76:285-292, 1987.
Green, CM. Matricide by sons.Medicine Science and the Law,21:207-214, 1981.
Grubin, D.H. Unfit to plead inEngland and Wales, 1976-88: Asurvey. British Journal of Psychiatry,158:540-548, 1991.
Gurtn, J. Criminal behaviour andmental illness. British Journal ofPsychiatry, 130:317-329, 1977.Gunn, J.; Maden, A.; and Swinton,M. Treatment needs of prisonerswith psychiatric disorders. BritishMedical Journal, 303:338-341, 1991.
Guze, S.B. Criminality and Psychiat-ric Disorders. New York, NY: Uni-versity Press, 1976.
Hafner, H., and Boker, W. Crimesof Violence by Mentally AbnormalOffenders. Cambridge, England:Cambridge University Press, 1982.
Hodgins, S. Mental disorder, intel-lectual deficiency, and crime: Evi-dence from a birth cohort. Archivesof General Psychiatry, 49:476-483,1992.
Hodgins, S., and He"bert, J. Unee"tude de relance aupres de ma-lades mentaux ayant commis desactes criminels. Revue Canadiennede Psychiatrie, 29:669-675, 1984.
Hoffmann, H. Age and other fac-tors relevant for rehospitalizationof schizophrenic outpatients. ActaPsychiatrica Scandinavica, 89:205-210, 1994.
Humphreys, M.S.; Johnstone, E.C.;MacMillan, J.F.; and Taylor, P.J.Dangerous behaviour precedingfirst admission for schizophrenia.British Journal of Psychiatry,161:501-505, 1992.
Jemelka, R.; Trupin, E.; and Chiles,J.A. The mentally ill in prisons: Areview. Hospital and CommunityPsychiatry, 40:481-491, 1989.
Johnstone, E.C.; Leary, J.; Frith,CD.; and Owens, D.G.C Dis-abilities and circumstances ofschizophrenic patients—A follow-up study: VII. Police contact. Brit-ish Journal of Psychiatry, 159(Suppl.):37-39, 1991.
Lafave, G.H.; Pinkney, A.A.; andGerber, GJ. Criminal activity bypsychiatric clients after hospitaldischarge. Hospital and CommunityPsychiatry, 44:180-181, 1993.
Lagos, J.M.; Perlmutter, K.; andSaexinger, H. Fear of the mentallyill: Empirical support for the com-mon man's response. American
Journal of Psychiatry, 134:1134-1137,1977.Lamb, H.R. Lessons learned fromdeinstitutionalisation in the U.S.British Journal of Psychiatry,162:587-592, 1993.Lamb, H.R.; Weinberger, L.E.; andGross, B.H. Court-mandated com-munity outpatient treatment forpersons found not guilty by rea-son of insanity: A five-year follow-up. American Journal of Psychiatry,145:45CM56, 1988.Lanzkron, J. Murder and insanity:A survey. American Journal of Psy-chiatry, 119:754-758, 1963.
Levine, D. Criminal behavior andmental institutionalization. Journalof Clinical Psychology, 26:279-284,1970.
Lindqvist, P. Criminal homicide inNorthern Sweden, 1970-1981: Alco-hol intoxication, alcohol abuse andmental disease. International Journalof Law and Psychiatry, 8:19-37,1986.
Lindqvist, P., and Allebeck, P.Schizophrenia and assaultive be-haviour: The role of alcohol anddrug abuse. Acta Psychiatrica Scan-dinavica, 82:191-195, 1989.
Lindqvist, P., and Allebeck, P.Schizophrenia and crime: A longi-tudinal follow-up of 644 schizo-phrenics in Stockholm. British Jour-nal of Psychiatry, 157:345-350, 1990.
Link, B.G.; Andrews, H.; andCullen, F.T. The violent and illegalbehavior of mental patients recon-sidered. American Sociological Re-view, 57:275-292, 1992.
Martell, D.A. Homeless mentallydisordered offenders and violentcrimes. Preliminary research find-ings. Law and Human Behavior,15:333-347, 1991.
McFarland, B.H.; Faulkner, L.R.;Bloom, J.D.; Hallaux, R.; and Bray,
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/1/69/1919225 by guest on 21 August 2022
VOL. 22, NO. 1, 1996 81
J.D. Chronic mental illness and thecriminal justice system. Hospitaland Community Psychiatry, 40:718-723, 1989.
Melick, M.E.; Steadman, H.J.; andCocozza, J.J. The medicalization ofcriminal behavior among mentalpatients. Journal of Health and So-cial Behavior, 20:228-237, 1979.
Millaud, F. L'homicide chez le pa-tient psychotique: Une dtude de 24cas en vue d'une prediction acourt terme. Revue Canadienne dePsychiatric, 34:340-346, 1989.
Modestin, J., and Ammann, R.Mental disorders and criminal be-haviour. British Journal of Psychia-try, 166:667-675, 1995.
Monahan, J. Mental disorder andviolence: Another look. In:Hodgins, S., ed. Mental Disorderand Crime. London, England: SagePublications, 1993. pp. 287-302.
Monahan, J.; Caldeira, C; andFriedlander, H.D. Police and thementally ill: A comparison of com-mitted and arrested persons. Inter-national Journal of Law and Psychia-try, 2:509-518, 1979.
Monahan, J., and Steadman, H.J.Crime and mental disorder: Anepidemiological approach. In:Tonry, M., and Morris, N., eds.Crime and Justice: An Annual Re-view of Research. Chicago, IL: Uni-versity of Chicago Press, 1983.pp. 145-189.
Moore, H., and Kleining, G. Dassoziale Selbstbild der Gesellschafts-schichten in Deutschland. KolnerZeitschrift fur Soziologie undSozialpsychiatrie, 12:86-119, 1960.
Morissette, L. Criminality et vio-lence chez les malades mentauxtrait^s dans la communaute': Pre-vention possible? L'Union Midicaledu Canada, 115:690-694, 1986.
Mulvey, E.P. Assessing the evi-dence of a link between mental ill-ness and violence. Hospital andCommunity Psychiatry, 45:663-668,1994.
Pasewark, R.A.; Pantle, M.L.; andSteadman, H.J. Characteristics anddisposition of persons found notguilty by reason of insanity inNew York State, 1971-1976. Ameri-can Journal of Psychiatry, 136:655-660, 1979.
Pfeiffer, E.; Eisenstein, R.B.; andDabbs, E.G. Mental competencyevaluation for the federal courts:I. Methods and results. Journal ofNervous and Mental Disease,144:320-328, 1967.
Pollock, H.M. Is the paroled pa-tient a menace to the community?Psychiatric Quarterly, 12:236-244,1938.
Rabkin, J.G. Criminal behavior ofdischarged mental patients: A crit-ical appraisal of the research. Psy-chological Bulletin, 86:1-27, 1979.
Rappeport, J.R., and Lassen, G.Dangerousness-Arrest rate com-parisons of discharged patientsand the general population. Ameri-can Journal of Psychiatry, 121:776-783, 1965.
Reich, J., and Wells, J. Psychiatricdiagnosis and competency to standtrial. Comprehensive Psychiatry,26:421^132, 1985.
Rice, M.E., and Harris, G.T. Acomparison of criminal recidivismamong schizophrenic and non-schizophrenic offenders. Interna-tional Journal of Law and Psychia-try, 15:397-^08, 1992.
Schanda, H.; Foldes, P.; Topitz, A.;Fliedl, R.; and Knecht, G. Premor-bid adjustment of schizophreniccriminal offenders. Acta PsychiatricaScandinavica, 86:121-126, 1992.
Shore, D.; Filson, C.R.; Johnson,W.E.; Rae, D.S.; Muehrer, P.; Kel-ley, D.J.; Davis, T.S.; Waldman,I.N.; and Wyart, R.J. Murder andassault arrests of White Housecases: Clinical and demographiccorrelates of violence subsequentto civil commitment. AmericanJournal of Psychiatry, 146:645-651,1989.
Shore, D.; Filson, C.R.; and Rae,D.S. Violent crime arrest rates ofWhite House case subjects andmatched control subjects. AmericanJournal of Psychiatry, 147:746-750,1990.
Sosowsky, L. Crime and violenceamong mental patients recon-sidered in view of the new legalrelationship between the state andthe mentally ill. American Journalof Psychiatry, 135:33-12, 1978.
Sosowsky, L. Explaining the in-creased arrest rate among mentalpatients: A cautionary note. Ameri-can Journal of Psychiatry, 137:1602-1605, 1980.
Soyka, M.; Immler, B.; and Sand,P. Alkohol- und Drogenmissbrauchals Riskofaktoren fur Gewalrtatenund Delinquenz Schizophrener.Psychiatrische Praxis, 20:172-175,1993.
Spitzer, R.L.; Cohen, J.; Fleiss, J.L.;and Endicott, J. Quantification ofagreement in psychiatric diagnosis:A new approach. Archives of Gen-eral Psychiatry, 17:83-87, 1967.
Spitzer, R.L.; Endicott, J.; andRobins, E. Research Diagnostic Cri-teria (RDC) for a Selected Group ofFunctional Disorders. 3rd ed. NewYork, NY: Biometrics Research Di-vision, New York State PsychiatricInstitute, 1978.
Steadman, H.J.; Cocozza, J.J.; andMelick, M.E. Explaining the in-
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/1/69/1919225 by guest on 21 August 2022

82 SCHIZOPHRENIA BULLETIN
creased arrest rate among mentalpatients: The changing clientele ofstate hospitals. American Journal ofPsychiatry, 135:816-620, 1978.
Steadman, H.J., and Felson, R.B.Self-reports of violence: Ex-mentalpatients, ex-offenders, and the gen-eral population. Criminology,22:321-342, 1984.
Swanson, J.W.; Holzer, C.E.; Ganju,V.K.; and Jono, R.T. Violence andpsychiatric disorder in the com-munity: Evidence from the epide-miologic catchment area surveys.Hospital and Community Psychiatry,41:761-770, 1990.
Tardiff, K., and Sweillam, A. As-sault, suicide, and mental illness.Archives of General Psychiatry,37:164-169, 1980.
Taylor, PJ. Social implications ofpsychosis. British Medical Bulletin,43:718-740, 1987.
Taylor, PJ. Schizophrenia andcrime. In: Hodgins, S., ed. MentalDisorder and Crime. London, Eng-land: Sage Publications, 1993.pp. 63-85.
Taylor, P.J., and Gunn, J. Violenceand psychosis: I. Risk of violenceamong psychotic men. British Med-ical Journal, 288:1945-1949, 1984.
Teplin, L.A. The criminality of thementally ill: A dangerous miscon-ception. American Journal of Psychi-atry, 142:593-599, 1985.
Wessely, S., and Taylor, P.J. Mad-ness and crime: Criminologyversus psychiatry. Criminal Be-haviour and Mental Health, 1:193-228, 1991.
World Health Organization. Man-ual of the International Classificationof Diseases, Injuries, and Causes ofDeath. Vol. I., 8th ed. Geneva,Switzerland: The Organization,1967.
World Health Organization. MentalDisorders: Glossary and Guide toTheir Classification in AccordanceWith the Ninth Revision of the In-ternational Classification of Diseases.Geneva, Switzerland: The Organi-zation, 1978.
Zitrin, A.; Hardesty, A.S.; Burdock,E.I.; and Drossman, A.K. Crimeand violence among mental pa-tients. American Journal of Psychia-try, 133:142-149, 1976.
The Authors
Jiri Modestin, M.D., is Professor ofPsychiatry, Psychiatric UniversityHospital, Zurich, Switzerland. Ro-land Ammann, M.D., was SeniorResident in Psychiatry, PsychiatricUniversity Hospital, Beme, Switzer-land, at the time of the study andis now Senior Resident in generalmedicine, District General Hospital,Burgdorf, Switzerland.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/1/69/1919225 by guest on 21 August 2022
Related Documents