Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript


MDR / XDR
Tuberculosis
Dr. Wagdy AminTraining Coordinator
NTP Egypt


Global TB Situation
Tuberculosis (TB) remains one of the world’s
deadliest communicable diseases.
In 2013, an estimated :
9.0 million people developed TB
1.5 million died from the disease,
360 000 of whom were HIV-positive.

Of the estimated 9 million people who developed TB,
more than half (56%) were in the South-East Asia and
Western Pacific Regions.
A further one quarter were in the African Region, which also
had the highest rates of cases and deaths relative to
population.
India and China alone accounted for 24% and 11% of total
cases, respectively.

An estimated 1.1 million (13%) of the 9 million
people who developed TB in 2013 were HIV-
positive.
The African Region accounts for about four out of
every five HIV-positive TB cases and TB deaths
among people who were HIV positive.

TB detection and treatment outcomes 2013,
6.1 million TB cases were reported to WHO.
Of these, 5.7 million were people newly diagnosed
and another 0.4 million were already on treatment.
the treatment success rate continued to be high at
86% among all new TB cases.

MDR-TB detection and treatment outcomes
Globally, 3.5% of new and 20.5% of previously
treated TB cases were estimated to have had MDR-
TB
This translates into an estimated 480 000 people
having developed MDR-TB.
On average, an estimated 9% of patients with
MDRTB had extensively drug resistant TB (XDR-TB).

If all notified TB patients (6.1 million, new and
previously treated) had been tested for drug
resistance, an estimated 300 000 cases of MDR-TB
would have been detected, more than half of these
in three countries alone: India, China and the
Russian Federation
The proportion of MDR-TB cases with XDR-TB was
highest in Georgia (20.0%), Kazakhstan (22.7%),
Latvia (21.7%), Lithuania (24.8%) and Tajikistan.
By the end of 2013, 100 countries had notified at
least one case of XDR-TB.

136 000 of the estimated 300 000 MDR-TB patients who
could have been detected were diagnosed and notified.
A total of 97 000 patients were started on MDR-TB
treatment in 2013, a three-fold increase compared with
2009.

9 Million
7 Billion
6.1million
notified 64%
Deaths
1.5 million
1.1 million
TB/HIV
Estimated MDR 480 000 / 9 M
300 000 /6.1M
97 000 enrolled

Estimates of burden Number (thousands)Rate
(per 100 000 pop)
Mortality (excludes HIV+TB) 0.55 (0.49–0.62) 0.67 (0.6–0.75)
Prevalence (includes HIV+TB) 22 (12–36)
27 (14–44)
Incidence (includes HIV+TB) 13 (12–15) 16 (15 - 18)
Case detection, TB all forms 59% (53% – 65%)

Millennium Development Goals (MDGs)
Egypt had achieved Millennium Development Goals (MDGs)
However, the case detection rate is still at 59%.
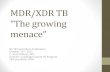
Prevalence has declined from 85 cases/ 100 000 population in
1990 to 27 cases / 100 000 population in 2013
Incidence of TB has declined from 34 cases / 100 000 population
to 16 cases / 100 000 population in 2013
Mortality cases has declined from 4 cases / 100 000 population
to 0.6 cases / 100 000 population

85
60
42
3430 29 29
27
34 32
2621
18 17 17 16
0
10
20
30
40
50
60
70
80
90
1990 1995 2000 2005 2010 2011 2012 2013
Prevelance rate /100000 incidence rate /100000

Trend of mortality Rate

Burden of MDR in Egypt
3.4% (1.9%-4.9%) in new
32.1% (24.3%-39.9%) in retreated cases
(Drug resistance survey 2011).

MDR-TB management in Egypt
Egypt applied to the green light committee, GLC, in 2003.
We received a review mission in January 2004.
The program was approved and the first team was trained in
Latvia.
The first MDR-TB center was established in Abbassia chest
hospital and patient enrolled in June 2006.
Later on, another two centers were established, one in Maamoura
chest hospital in 2008 and a third one in Mansoura chest hospital
in 2012
A fourth center is being prepared now in Asuit chest hospital.

Second line drugs used in management of theses cases are
funded from global fund grant.
The average treatment course costs around 4000 US$ and lasts up
to two years compared to 6 months for susceptible tuberculosis
and less than a 1000 EP.
From 2006 to 2013 ( 461 patients enrolled in the treatment) with
success treatment 68%
MDR-TB management in Egypt, cont.

Different resistance patterns

Mono-resistance
colonies are resistant to only one of the first-line anti-
TB drugs.
Poly-resistance
Colonies are resistant to more than one of thefirst line anti-TB drugs but do not combineresistance to both Isoniazid and Rifampicin.Examples of poly-resistance may includeStreptomycin, Isoniazid and Ethambutol orStreptomycin, Rifampicin and Ethambutol.

Multiple drug resistant
colonies combine resistance to at least Isoniazidand Rifampicin.
Extensively Drug Resistant TB (XDR-TB):
Colonies are resistant to: 1. 1st Line drugs , at least Rifampicin and Isoniazid, (MDR-TB) 2. A fluoroquinolone3. One or more of the following injectable drugs:
kanamycinAmikacinCapreomycin

Totally Drug–Resistant Tuberculosis (TDR-TB)
“for TB strains that showed in-vitro resistance
to all first and second line drugs tested
Rifampicin resistance
resistance to rifampicin detected using phenotypic or genotypic
methods, with or without resistance to other anti-TB drugs.
It includes any resistance to rifampicin, whether mono-
resistance, multidrug resistance, poly drug resistance or extensive drug
resistance.
Any Patient found to have an RR-TB strain at any point in time
should be started on an adequate second-line drug regimen.

Primary resistance and acquired resistance
“Primary resistance” means that the patient was
infected with already resistant bacilli.
“Acquired resistance” means that patient was initially
infected with sensitive bacilli but developed resistance
of any pattern during the course of treatment


Composition of second-line anti-tuberculosis regimens
Fluoroquinolones should be used to all patients.
Later-generation Fluoroquinolones rather than an earlier-
generation
Fluoroquinolones should be used (levofloxacin -
Moxifloxacin).
Ciprofloxacin is contraindicated as anti-TB drugs
because of rapid emerging of resistant strain.
Ofloxacin is not recommended because of weak efficacy

Ethionamide (or Protiomamide) should be used.
Four second-line anti-tuberculosis drugs likely to
be effective (including a parenteral agent), as well
as Pyrazinamide (regardless the
susceptibility), should be included in the intensive
phase.
Pyrazinamide may be used during the whole
treatment course if the patient can tolerate.

MDR-TB, regimens should include at least:
1) pyrazinamide,
2) a Fluoroquinolones,
3) a parenteral agent,
4) Ethionamide (or Protiomamide),
5) and either Cycloserine or PAS (p-amino-salicylic acid)
if Cycloserine cannot be used.

Intensive phase of at least 8 months’
duration
total treatment duration of at least 20
months is recommended in patients without
any previous MDR-TB treatment.

MDR-TB/HIV co-infection
Antiretroviral therapy is recommended for all patients with
HIV and drug-resistant TB requiring second-line anti-
tuberculosis drugs, irrespective of CD4 cell-count, as
early as possible (within the first 8 weeks) following
initiation of anti-tuberculosis treatment.


New treatment approach is highly needed in Egypt to overcome the
challenge of patients’ adherence to treatment.
Community based ambulatory care rather than facility based treatment is the needed one where:
DR-TB patients receive their treatment at their homes
This help addressing serious barriers to adherence and DOT
Can be more cost-effective than hospital care (need to be investigated)
Compatible with hospital care and does not exclude it
Increases community awareness about DR-TB.
This needs developing a mass of trained treatment supporters to implement to ensure
Quality clinical care
Socioeconomic support
Psycho-emotional support
In addition, this needs incentives for the network personnel responsible for community based treatment of MDR-TB.

New rapid diagnostics are urgently needed in Egypt to enhance
case detection and patients’ enrollment on treatment
The Gene-Xpert MTB/RIF system is a recently developedTB-specific application, designed for the Gene-Xpertplatform, to detect M. tuberculosis as well as rifampicinresistance directly from sputum.
Other rapid molecular testing technique detectingresistance against both Isoniazid and Rifampicin are morepreferable in Egypt because the relatively high prevalenceof Rifampicin mono-resistance among newly diagnosed TBcases which is around 9% while the MDR-TB prevalence isonly 3.4%.
Increasing number of labs doing DST (currently only 2)

New Medicine
Bedaquiline and delamanid are two new drugs for
use in the treatment of MDR-TB which have
emerged over 2013–14, and WHO has developed
interim guidance on their use.


Related Documents