Dr. J.N.Banavaliker, MD,DTCD,MBA

Diagnosis & Management of MDR-TB & XDR-TB AIMS
Aug 05, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dr. J.N.Banavaliker, MD,DTCD,MBA

Definitions
MDR-TB: resistance to isoniazid and rifampicin, independent of any other resistance
XDR TB is defined as… TB which is resistant to isoniazid and
rifampin, plus resistant to any fluoroquinolone and at least one of three injectable second-line drugs (i.e., amikacin, kanamycin, or capreomycin).

The global TB situationThe global TB situation
Estimated number of cases, 2010
Estimated number of deaths, 2010
1.1 million*(0.9–1.2 million)
8.8 million(8.5–9.2 million)
~ 650,000 out of 12 million (11-14 million)
prevalent TB cases
All forms of TB
Multidrug-resistant TB
HIV-associated TB 1.1 million (1.0–1.2 million)
350,000(320,000–390,000)
Source: WHO Global Tuberculosis Control Report 2011 (www.who.int/tb/publications/global_report/2011/gtbr11_full.pdf)* Excluding deaths attributed to HIV/TB

Proportion of MDR among new TB cases Latest available data, 1994-2010
0-<3
3-<6
6-<12
12-<18
>18
No data available
Subnational data only
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border
lines for which there may not yet be full agreement. WHO 2011. All rights reserved

0-<6
6-<12
12-<30
30-<50
>50
No data available
Subnational data only
Proportion of MDR among previously treated TB cases Latest available data, 1994-2010
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border
lines for which there may not yet be full agreement. WHO 2011. All rights reserved

Causes of inadequate treatment
Providers/Programmes: Inadequate regimens
Drugs: Inadequate supply/quality
Patients: Inadequate drug intake
-Absence of guidelines or inappropriate guidelines -Non-compliance with guidelines -Inadequate training of health staff -No monitoring of treatment -Poorly organized or funded TB control programmes
-Non-availability of certain drugs (stock-outs or delivery disruptions) -Poor quality -Poor storage conditions -Wrong dosages or combination
Poor adherence (or poor DOT) -Lack of information -Non-availability of free drugs -Adverse drug reactions -Social and economic barriers -Malabsorption -Substance abuse disorders

DIAGNOSIS OF M(X)DR TB
Least reliable
Drug Resistant TB
Clinical
Less reliable
Radiological
Gold Standard
Bacteriological C/S or DSTMolecular
Rapid MDR Screen
BACTEC MGIT 960HAINS TEST
GeneXpert

How Is Tuberculosis Diagnosed?
Pulmonary TB: SPUTUM
EP TB: Other Body Fluids
Patients of TB are diagnosed with the help of microscopic examination of Sputum, body fluids or tissue samples for mycobacteria.
A specimen of body fluids or tissue samples is spread on a slide (smear) and stained by Ziehl-Nielsen method
AFB smear
AFB (shown in red) are tubercle bacilli

AFB SMEAR Inexpensive
Rapid (1 day)
Specific (99%)
Less Sensitive (50-60%) LOW SENSITIVITY

Mycobacterial Cultures
Culture media Solid media (Lowenstein-Jensen media) 6-8 Weeks Liquid media (BACTEC CULTURE) MGIT 960
Colonies of M. tuberculosis growing on media
GOLD STANDARDLJ: Takes Long Time

RAPID TB Culture- MGIT 960
•Use to confirm diagnosis of TB
•Results in 10 to 14 days when liquid medium systems used (BACTEC CULTURE: MGIT 960)

Sensitivity of Diagnostic tests
Microscopy: 1,00,000 bacilli per ml
LJ culture: 100-1000 bacilli per ml
BACTEC CULTURE MGIT 960: 10-100 bacilli per ml
TB PCR: <10 bacilli per ml

TIME TO DIAGNOSIS IN MDR TB

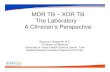
Diagnosis of MDR / XDR TB
Limitations of Culture technique
Difficult to implement in the field
Dedicated and trained staff required
Use of different media by different labs
Prolonged period for getting results

Molecular Diagnostic Tests For Tuberculosis Nucleic Acid Based Tests- NAAT: Nucleic Acid Amplification Tests
TB PCR (POLYMERASE CHAIN REACTION)
The key advantages are speed, sensitivity & specificity
It is a rapid method; (within 24 hours).
It is a very sensitive method (less than 10 bacilli per ml of the specimen).

Culture: MGIT 960 Bactec culture.
Molecular techniques: Detection of MTB:- GeneXpert
MTB/RIF. HAINS Test

Alternative method of grouping anti-TB agents
Grouping Drugs
Group 1: First-line oral anti-TB agents Isoniazid (H); Rifampicin (R); Ethambutol (E); Pyrazinamide (Z)
Group 2: Injectable anti-TB agents Streptomycin (S); Kanamycin (Km); Amikacin (Am); Capreomycin (Cm); Viomycin (Vm).
Group 3: Fluoroquinolones Ciprofloxacin (Cfx); Ofloxacin (Ofx); Levofloxacin (Lvx); Moxifloxacin (Mfx); Gatifloxacin (Gfx)
Group 4: Oral second-line anti-TB agents
Ethionamide (Eto); Prothionamide (Pto); Cycloserine (Cs); Terizadone (Trd); para-aminosalicylic acid (PAS)
Group 5: Agents with unclear efficacy (not recommended by WHO for routine use in MDR-TB patients)
Clofazimine (Cfz); Linezolid (Lzd); Amoxicillin/Clavulanate (Amx/Clv); thioacetazone (Thz); imipenem/cilastatin (Ipm/Cln); high-dose isoniazid (high-dose H); Clarithromycin (Clr)

MDR-TB MANAGEMENT1. Standardized
RNTCP CATEGORY IV REGIMEN: 6 (9) Km Ofx (Lvx)
Eto Cs Z E / 18 Ofx (Lvx)Eto Cs ET
2. Individualized

Dosage and weight band recommendations
S.No Drugs 16-25 Kgs 26-45 Kgs >45 Kgs
1. Kanamycin 500 mg 500 mg 750 mg
2. Ofloxacin (Levofloxacin)
400 mg(200 mg)
600 mg(500 mg)
800 mg(750 mg)
3. Ethionamide 375 mg 500 mg 750 mg
4. Ethambutol 400 mg 800 mg 1000 mg
5. Pyrazinamide 500 mg 1250 mg 1500 mg
6. Cycloserine 250 mg 500 mg 750 mg
7. PAS (80% Bioavailability)
5 gm 10 gm 12 gm

Adverse effects of drugs
1. Gastro-intestinal symptoms (nausea and vomiting)
2. Giddiness3. Ocular toxicity4. Renal toxicity5. Arthralgia6. Cutaneous reactions7. Hepatitis8. Neurological symptoms9. Psychiatric disturbances10. Vestibulo-auditory disturbances11. Hypothyroidism

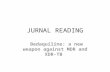
Outcomes of MDR-TB treatmentFor MDR-TB patients started on treatment in
2008*
0%
20%
40%
60%
80%
100%
Kazakhstan (2268)
Turkey (263) Uzbekistan (294)
Ecuador (210) Georgia (417) Democratic Republic of the
Congo (202)
Philippines (520)
Namibia (221) Russian Federation
(1537)
Brazil (444) Kyrgyzstan (262)
Republic of Moldova (522)
South Africa (4383)
Romania (816)
Success Died Failed Defaulted Not evaluated
* In countries reporting outcomes for >200 MDR-TB cases with <20% unevaluated (cohort size shown below country names)

MDR-TB with HIV co-infectionCD 4 Cell count ART Recommendation Timing of ART in
relation to treatment for MDR TB
≤ 350 cells/mm3 Recommend ART After 2 weeks, as soon as the treatment for MDR TB is tolerated
> 350 cells/mm3 Defer ART Re-evaluate patient monthly for consideration of ART. CD4 testing is recommended every 3 months during treatment for MDR TB
Not available Recommend ART After 2 weeks, as soon as the treatment for MDR TB is tolerated

XDR-TBMay – 2006
Partners Meeting, Atlanta, Georgia, USA XDR-TB with HIV in Tugela Ferry, KwaZulu- Natal Province, South
Africa
August – 2006
Neel Gandhi of Albert Einstein College of Medicine of Yeshiva University at
XVI International AIDS Conference in Toronto,1539 Patients - 221 had MDR TB
- 53 of these had XDR-TB- 52 of 53 patients died within 25 days- 44 were HIV Positive
Ref: Gandhi NR et al; Extensively Drug Resistant Tuberculosis as a cause of death in patients co-infected with tuberculosis & HIV in rural area of South Africa; Lancet 2006,368;1575-80

XDR-TB
Place of Study Year of Study No. of MDR TB strains tested
No. of XDR resistant strains (%)
References
Italy 1993-2004 83 8 (14.3) Migliori GB, et al.
Germany 1993-2004 43 3 (10.3) Migliori GB, et al.
France 2006 - 4% Bouvet E., et al.
Iran 2006 113 12 (10.9) Masjedi MR, et al.
Hong Kong 2004 75 9 (12.01) Kam K.M., et al.
Industrialsed nations 2000-04 821 53 (6.5) Shah SN, et al.
Eastern Europe and Russia
2000-04 406 56 (13.6) Shah SN, et al.
Republic of Korea 2000-04 1298 200 (15.4) Shah SN, et al.
India 2006 68 5 (7.3) Mondal R, et al.
India 2008 12 4 (33.3) Singh S, et al.
India 2007 326 36 (11) Jain S, et al.
India 2007 66 1 (1.5) Thomas A, et al.
India 2009 211 5 (2.4) Sharma SK, et al.
India 2009 216 7 (3.1) Ramachandran R, et al.
Delhi, India 2011 223 45 (20.17) Myneedu V.P., et al.
Source: Indian Journal of Tuberculosis, TAI, Apr.2011

XDR-TB Predominant Reasons for resistance
Primarily due to poorly managed TB programme
Incorrect drug prescribing practices Poor quality of drugs Erratic supply of drugs Non adherence to treatment by patients

XDR-TB - Diagnosis Culture & Sensitivity of M.TB - Gold
standard
Resistance to First Line Drugs
+ Resistance to Second Line Drugs
Good History of Chemotherapy of Anti-TB Drugs
Serial X-rays of Chest

Countries that had reported at least oneXDR-TB case by Oct 2011
Argentina Burkina Faso Estonia Japan Namibia Republic of Korea The Former Yugoslav Republic of MacedoniaArmenia Bhutan France Kazakhstan Nepal Republic of Moldova TogoAustralia Cambodia Georgia Kenya Netherlands Romania TunisiaAustria Canada Germany Kyrgyzstan Niger Russian Federation TurkeyAzerbaijan Chile Greece Latvia Norway Slovenia UkraineBangladesh China India Lesotho Pakistan South Africa United Arab EmiratesBelarus Colombia Indonesia Lithuania Peru Spain United KingdomBelgium Czech Republic Iran (Islamic Rep. of) Mexico Philippines Swaziland United Republic of TanzaniaBenin Dominican Republic Ireland Mongolia Poland Sweden United States of AmericaBotswana Ecuador Israel Mozambique Portugal Tajikistan UzbekistanBrazil Egypt Italy Myanmar Qatar Thailand Viet Nam

TIME TO DIAGNOSIS IN XDR TB

XDR-TB REGIMENS Intensive Phase (6-12 months7 drugs –
Capreomycin (Cm), PAS, Moxifloxacin (Mfx), High dose-INH, Clofazimine, Linezolid, and Amoxyclav
The Continuation Phase (18 months) 6 drugs – PAS, Moxifloxacin (Mfx), High dose-INH, Clofazimine, Linezolid, and Amoxyclav
RNTCP Regimen for XDR TB: 6-12 Cm, PAS, Mfx, High dose-H, Cfz, Lzd, Amx/Clv /18 PAS, Mfx, High dose-H, Cfz, Lzd, Amx/Clv [Reserve/Substitute drugs: Clarithromycin, Thiacetazone]

Regimen for XDR TB dosage and weight band recommendations
DRUGS DOSAGE / DAY
<45Kg >45Kg
Inj. Capreomycin (Cm) 750 mg 1000 mg
PAS 10 gm 12 gm
Moxifloxacin (Mfx) 400 mg 400 mg
High dose INH (High dose-H) 600 mg 900 mg
Clofazimine (Cfz) 200 mg 200 mg
Linezolid (Lzd) 600 mg 600 mg
Amoxyclav(Amx/Clv) 875/125 mg BD 875/125 mg BD
Pyridoxine 100 mg 100 mg
Reserve/Substitute drugs
Clarithromycin (Clr) 500 mg BD 500 mg BD
Thiacetazone (Thz) # 150 mg 150 mg
# Depending on availability, not to be given to HIV positive cases

XDR-TBKorean Study 155 patients
18 (12%) had MDR TB 81 (52%) had previously received treatment with first-line
drugs 56 (36%) had received treatment with second-line drugs. 27 (17%) had extensively drug-resistant (XDR) TB at the
start of treatment.
102 patients (66%) were cured or completed therapy
Surgical resection was performed more frequently for patients with XDR-TB than for those with non-XDR MDR TB (48% vs. 17%)
Ref: Kwon Y.S., Kim Y.H.,Suh G.Y. et al; Treatment Outcomes for HIV-Uninfected Patients with Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis, Clin.Infect.Dis 2008; 47:496-5021

XDR-TB “XDR-TB is not a Death Sentence”
Carole Mitnick, Harvard Medical School,2008
Peru 1999-2002 810 patients on individualized drug treatment
Additional services- Surgery Adverse event Management Nutritional support Psychological support
Received treatment at home at community based settings 48 patients XDR-TB but HIV Negative 603 patients were MDR TB
Outcome of Treatment 60.4% of XDR-TB cured 66.3% of MDR TB cured
Ref: Minick C.D.,Shin S.S.,Seung K.J. et al; Comprehensive Treatment of Extensively Drug Resistant Tuberculosis; New Eng. J. Med.; 2008,359;563-74

XDR-TB - Diagnosis Why XDR-TB is of Prime Importance
Due to increasing no. of HIV cases
High mortality
High infectivity
Poor outcome of treatment
Exorbitant cost of drugs
High in resource crunch places
High in poor developing countries

XDR-TBChallenges Health System Related
Absence of Data on drug resistance against second line drugs Daily DOTS for 2 year
Private Practitioner Related Large and unorganized private sector Lack of faith in Public sector Health Programmes Low priority for carrying out Public Health Programmes
Patient Related Holding patients to defined geographical area for 2 year Lack of trust in the quality of care provided by Public Sector Issues of stigma and confidentiality

XDR-TBOperational Problems
Setting up Proper linkages with peripheral DOTS Centres
Managing severe adverse drug reactions in field conditions
Lack of ready access to specialized lab facilities
Arranging proper training to Medical, Laboratory and Non Medical workers for DOTS Plus programme

XDR-TB - DiagnosisXDR-TB grave public health threat
Preventive Measures
Strengthen basic TB care to prevent the emergence of drug-resistance
Ensure prompt diagnosis and treatment of drug resistant cases to cure existing cases and prevent further transmission
Increase collaboration between HIV and TB control programmes to provide necessary prevention and care to co-infected patients
Increase investment in laboratory infrastructures to enable better detection and management of resistant cases.

XDR-TBPoints to Ponder
Large diseased population Multiplicity of Health Units Over the counter availability of anti TB drugs Amplification of Resistance Quality Labs in India Specialized centre for treatment HIV Infection

Diagnosis of tuberculosis
Latent Infection Active tuberculosis
AFB Smear examination
Solid and liquid culture
Identification
Susceptibility testing methods
TST orMantoux
IFN-/IGRA techniquesTB feron TestT-SPOT TB Test
Molecular methods-Detection of MTB
-Detection of resistance
GeneXpert MTB/RIF HAINS MDR / XDR TB

TB & M(X)DR TB as per WHO endorsement
Year TechnologyTurnaround
timeSensitivity
gain
Before 2007ZN microscopy
Solid Culture2-3 days
30-60 daysBaseline
2007Liquid Culture
Rapid speciation15-30 days
+10% compared to
LJ
2010Line Probe Assay
(1st line, Rif & INH)
2-4 daysAt this time for S+ only
Relevance for HIV/TB or Pulmonary sputum Positive TB or Failure cases:
Importance of
a) early diagnosis & care;
b) smear-positive TB,
c) rapid MDR/XDR detection
39
2011 GeneXpert MTB/RIF 1-2 Days Sputum Negative

Even if most TB patients in the world are not drug-resistant, they present a formidable challenge to global TB control.
Treatment of MDR-TB is longer, more complicated and less effective than for drug-susceptible TB. Most programmes in the world recruit small numbers of patients and successful outcome is achieved in <75% of individuals overall, the threshold envisaged for 2015 by the Global Plan.
Conclusions..

Coverage of DST for TB patients remains low and resultantly a minority of drug-resistant TB patients are detected and notified. Information remains incomplete.
To reach the Global Plan targets, substantial resource mobilization will be needed, both from domestic and from external sources. The price of treating a patient needs to be reduced.
Conclusions

Global coverage of drug resistance surveillance data
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. WHO 2011. All rights reserved

Looking to the Future
Overall goal of DOTS Plus strategy to reduce morbidity, mortality from MDR TB and cut the chain of transmission
New and Emerging best medical practices to supplement DOTS Plus
Evolving better, safer and effective services delivery
WHO Target- To eliminate Tuberculosis by 2050

THANK YOU
Related Documents