Personality Disorders: Theory, Research, and Treatment Maternal Borderline Personality Disorder Symptoms and Convergence Between Observed and Reported Infant Negative Emotional Expressions Diana J. Whalen, Elizabeth J. Kiel, Matthew T. Tull, Robert D. Latzman, and Kim L. Gratz Online First Publication, March 23, 2015. http://dx.doi.org/10.1037/per0000116 CITATION Whalen, D. J., Kiel, E. J., Tull, M. T., Latzman, R. D., & Gratz, K. L. (2015, March 23). Maternal Borderline Personality Disorder Symptoms and Convergence Between Observed and Reported Infant Negative Emotional Expressions. Personality Disorders: Theory, Research, and Treatment. Advance online publication. http://dx.doi.org/10.1037/per0000116

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Personality Disorders: Theory, Research, andTreatment
Maternal Borderline Personality Disorder Symptoms andConvergence Between Observed and Reported InfantNegative Emotional ExpressionsDiana J. Whalen, Elizabeth J. Kiel, Matthew T. Tull, Robert D. Latzman, and Kim L. GratzOnline First Publication, March 23, 2015. http://dx.doi.org/10.1037/per0000116
CITATIONWhalen, D. J., Kiel, E. J., Tull, M. T., Latzman, R. D., & Gratz, K. L. (2015, March 23). MaternalBorderline Personality Disorder Symptoms and Convergence Between Observed andReported Infant Negative Emotional Expressions. Personality Disorders: Theory, Research,and Treatment. Advance online publication. http://dx.doi.org/10.1037/per0000116

Maternal Borderline Personality Disorder Symptoms and ConvergenceBetween Observed and Reported Infant Negative Emotional Expressions
Diana J. WhalenUniversity of Mississippi Medical Center
Elizabeth J. KielMiami University
Matthew T. TullUniversity of Mississippi Medical Center
Robert D. LatzmanGeorgia State University
Kim L. GratzUniversity of Mississippi Medical Center
To date, the influence of maternal borderline personality disorder (BPD) on perceptions of infants’emotional expressions has not been examined. This study investigated the relation of maternal BPDsymptoms to discrepancies between mother-reported and observed infant expressions of fear and anger.Emotional expressions in response to fear- and anger-eliciting stimuli were observed among 101 12- to23-month-old infants of mothers with a range of BPD symptoms. Mothers also reported on their infants’past-month fear and anger expressions. Findings from polynomial regression analyses revealed thatmaternal BPD symptoms (particularly BPD interpersonal symptoms) are associated with greater con-vergence of mother-reported and observed infant anger expressions. Furthermore, although maternalBPD symptoms were not related to discrepancies between mother-reported and observed infant fear,findings did reveal a relation between maternal BPD symptoms and observed infant fear expressions,such that maternal BPD symptoms related to both low and high (vs. moderate) levels of fear expressionsin the laboratory. Moreover, BPD behavioral symptoms in particular were associated with greaterconvergence of mother-reported and observed infant fear expressions. Overall, findings contribute to theliterature on the impact of maternal BPD on parenting and infant outcomes, and highlight the relevanceof maternal BPD symptoms to discrepancies between perceived and observed infant negative emotionalexpressions.
Keywords: behavioral observations, borderline personality disorder, infant emotional expressions,mothers, parent ratings
Borderline personality disorder (BPD) is a serious and costlymental health problem (Skodol et al., 2002; van Asselt, Dirksen,Arntz, & Severens, 2007) associated with severe functional im-pairment, elevated risk for suicide, and high rates of co-occurring
psychiatric disorders (Skodol et al., 2002). Surprisingly little re-search has examined the influence of maternal BPD on parenting,offspring outcomes, and the mother–child relationship, despite thefact that disturbances in interpersonal relationships and emotionregulation represent key features of this disorder (Gunderson &Lyons-Ruth, 2008; Hill et al., 2008; Linehan, 1993; Rosenthal etal., 2008). For example, in stark contrast to the vast literature onthe impact of maternal depression on perceptions of offspringsymptoms and behaviors (De Los Reyes & Kazdin, 2005), theimpact of maternal BPD symptoms on perceptions of offspringemotional and behavioral functioning remains largely unknown.The influence of maternal BPD symptoms on perceptions of in-fants’ emotional expressions may be particularly important toexamine, given their relevance to infant emotion regulation. Spe-cifically, maternal perceptions of infant emotions likely influencematernal responses to those emotions (Dix, 1991; Johnson, Emde,Pannabecker, Stenberg, & Davis, 1982) and maternal responses toinfant emotions play a central role in the development of adaptiveemotion regulation (Eisenberg, Cumberland, & Spinrad, 1998).Thus, maternal perceptions of infant emotional expressions mayhave consequences for later emotional development and adjust-ment (Calkins, 1994).
Diana J. Whalen, Department of Psychiatry and Human Behavior, Uni-versity of Mississippi Medical Center; Elizabeth J. Kiel, Department ofPsychology, Miami University; Matthew T. Tull, Department of Psychiatryand Human Behavior, University of Mississippi Medical Center; Robert D.Latzman, Department of Psychology, Georgia State University; Kim L.Gratz, Department of Psychiatry and Human Behavior, University ofMississippi Medical Center.
Dr. Whalen is now at the Department of Psychiatry, Washington Uni-versity.
Dr. Whalen’s work on this paper was supported by Grant T32MH100019, awarded to Drs. Deanna Barch and Joan Luby from theNational Institutes of Health.
Correspondence concerning this article should be addressed to Kim L.Gratz, Department of Psychiatry and Human Behavior, University ofMississippi Medical Center, 2500 North State Street, Jackson, MS 39216.E-mail: [email protected]
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
Personality Disorders: Theory, Research, and Treatment © 2015 American Psychological Association2015, Vol. 6, No. 2, 000 1949-2715/15/$12.00 http://dx.doi.org/10.1037/per0000116
1

With regard to the impact of maternal BPD symptoms onperceptions of infant emotional expressions, literature on emo-tional functioning in BPD highlights the importance of examiningperceptions of infant anger and fear expressions in particular.Specifically, theoretical and clinical literature on BPD emphasizethe relevance of anger and anxiety to this disorder (APA, 2000;Gunderson & Singer, 1975; Kernberg, 1967), noting the promi-nence of these emotions among individuals with BPD. Moreover,research suggests that some of the emotional dysfunction observedin BPD may be specific to anger and anxiety (e.g., Koenigsberg etal., 2002). Although often examined as an intrapersonal process,this emotional dysfunction likely has implications for perceptionsof and responses to others’ emotions as well. For example, adultswith BPD have been found to demonstrate heightened sensitivityto facial expressions of both anger and fear (Domes et al., 2008;Lynch et al., 2006; Wagner & Linehan, 1999), as well as atendency to interpret neutral facial expressions as negative, fearful,or threatening (Donegan et al., 2003; Dyck et al., 2009; Wagner &Linehan, 1999). It is likely that this heightened sensitivity to angryand fearful expressions extends to the mother-child relationshipand influences mothers’ perceptions of their children’s anger andfear expressions, resulting in heightened reports of children’snegative emotional expressions.
Indeed, although not specific to maternal BPD, a number ofstudies have shown only modest associations between maternalreports and laboratory assessments of child behavior and temper-ament (Hayden, Durbin, Klein, & Olino, 2010; Kochanska, Coy,Tjebkes, & Husarek, 1998; Rothbart, Derryberry, & Hershey,2000; Sameroff, Seifer, & Elias, 1982). De Los Reyes and col-leagues have also published extensively on discrepancies betweenmother and youth reports of behavior and psychopathology (DeLos Reyes, Goodman, Kliewer, & Reid-Quinones, 2008; De LosReyes, Lerner, Thomas, Daruwala, & Goepel, 2013; De Los Reyes& Kazdin, 2006), providing strong evidence that maternal psycho-pathology (particularly depression) is associated with a negativebias in reporting (see also Boyle & Pickles, 1997; Fergusson,Lynskey, & Horwood, 1993).
Importantly, however, little work has extended the investigationof discrepancies between observed and mother-reported symptomsand behaviors into infancy (Gartstein & Marmion, 2008; Kiel &Buss, 2010; Leerkes & Crockenberg, 2003). Nonetheless, prelim-inary evidence suggests that maternal emotional dysfunction maybe associated with heightened perceptions of infant negative emo-tional expressions (relative to observed levels of these emotions).For example, in a recent study examining the influence of maternalpersonality traits (i.e., negative and positive emotionality) on dis-crepancies between laboratory and mother-report measures of in-fant temperament, Gartstein and Marmion (2008) found that ma-ternal negative emotionality was associated with higher reports ofinfant fear relative to laboratory ratings of infant fear expressions.Maternal depression has also been linked to divergence betweenmother-reported and observed measures of infant distress, withdepressed mothers reporting greater infant distress than what wasobserved in the laboratory (Leerkes & Crockenberg, 2003).
Despite literature suggesting the relevance of maternal BPDsymptoms to perceptions of infant anger and fear expressions andtheir convergence with laboratory-based assessments of infantemotional expressions, no studies to date have examined thisquestion. Thus, the goal of this study was to examine the relation
of maternal BPD symptoms to discrepancies between mother-reported and observed infant anger and fear expressions. Based onfindings of heightened sensitivity to anger and fear expressions inBPD, we hypothesized that maternal BPD symptoms would relateto greater divergence between mother-reported infant anger andfear expressions and infant anger and fear expressions observed inthe laboratory (in the form of higher reported emotional expres-sions than observed).
Method
Participants
Mother–infant dyads were recruited through advertisements(some of which specifically requested mothers with mood, rela-tionship, and impulse control difficulties) for a “mother–childresearch study” posted online and in nursery schools, daycarefacilities, hospitals, churches, coffee shops, and stores in thegreater Jackson, Mississippi area. Mother–infant dyads were eli-gible for participation if the infant was 12 to 23 months of age andtypically developing, and the mother was fluent in English; noother exclusion criteria were used. Data were collected from 101mothers and their infants.
Mothers were ethnically diverse (53% African American; 44%White) and ranged in age from 18 to 42 years (M � 28.55 � 5.28).Infants (55 female) ranged in age from 12 to 23 months (M �16.46 � 3.62). The mean annual income of the sample wasbetween $36,000 and $50,000, with 36% reporting less than$25,000 per year. With regard to the educational background of themothers, 16% had completed high school or received a GED, 35%had attended some college or technical school, and 47% hadgraduated college. The majority of the infants’ fathers (70%) wereliving in the home.
Procedure
All procedures were approved by the institution’s institutionalreview board. Study advertisements instructed mothers to call thelaboratory for further details about the study. Upon calling, moth-ers were informed that the purpose of the study was to examine themother–infant relationship and the factors that influence this rela-tionship, including personality traits. Eligible participants whoexpressed an interest in participating met with a research assistantto obtain informed consent and schedule the laboratory visit. Afterproviding written informed consent, mothers were provided with aquestionnaire packet (see Measures) and informed that they couldcomplete the questionnaires before the laboratory session or at theend of the laboratory session.
During the laboratory session, a lead experimenter (E1) guidedmothers and their infants through several procedures, includingfour episodes from the Locomotor version of the LaboratoryTemperament Assessment Battery (Lab-TAB; Goldsmith & Roth-bart, 1999). Two of these episodes elicited fear (UnpredictableDog [UD]; Spider [S]) and two elicited anger (Gentle Arm Re-straint [GAR]; Toy Behind Barrier [TBB]). Episodes always oc-curred in the order in which they are described. Except wherenoted, mothers were instructed to refrain from interaction unlessinfants became extremely distressed. In the UD episode, the infantsat in a highchair at the end of a table, and the mother sat in a chair
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
2 WHALEN, KIEL, TULL, LATZMAN, AND GRATZ

to the side. In front of the infant was a black cardboard barrier witha curtain-covered opening. A mechanical dog that moved ran-domly and made noises was moved from the opening to the childand back on a rolling platform controlled by E1 behind the barrier.The dog was left in front of the child for 10 s and then wheeledback to the front of the barrier for 5 s. This was repeated twice fora total of three trials. In the GAR episode, the infant sat in ahighchair at the end of a table, and the mother sat in a chair to theinfant’s left. E1, seated on the infant’s right, put a perpetual motiontoy on the table and showed the infant how to play with it. Themother was then cued to stand behind the infant and hold theinfant’s arms by her or his side for a maximum of 30 s or untilthe infant expressed extreme distress. After the infant played forat least 30 s and returned to a baseline state, the mother wascued to repeat the procedure.
In the S episode, the mother sat on a chair in the corner of theroom with her infant on her lap. In the opposite corner was a largeplush spider on top of a remote-controlled truck, which was hiddenby a black shoe box. A secondary experimenter, hidden from view,controlled the spider remotely, moving it halfway toward the infantand mother (where it paused for 10 s), then back to the corner(where it paused for 10 s), then all the way to the feet of the motherand infant (where it paused for 10 s), then back to the corner. In theTBB episode, the infant sat in a highchair at the end of a table andthe mother sat to the infant’s side. E1 brought out an attractive toy(a ball that lit up and played music), demonstrated how it worked,and placed it within the infant’s reach. After the infant played forat least 30 s, E1 took the toy and placed it behind a transparentPlexiglas barrier for 30 s. E1 then returned the ball to within theinfant’s reach. This procedure was repeated two more times for atotal of three trials.
At the end of the laboratory session, mothers were compensated$30 and infants received a small gift. Visits were videotaped forlater scoring.
Measures
Maternal BPD symptoms. Mothers completed the Border-line Evaluation of Severity over Time (BEST; Pfohl et al., 2009),a 15-item, self-report measure of BPD symptom severity, or thedegree of impairment from each of the 9 DSM BPD criteria overthe past month. Research indicates that the BEST has adequatetest–retest reliability, as well as good convergent and discriminantvalidity (Pfohl et al., 2009). Notably, and consistent with pastresearch examining levels of BPD pathology (both BPD symptomson the BEST and BPD features on the PAI-BOR) among adults innonclinical settings (e.g., Chapman, Leung, & Lynch, 2008; Gratz,Breetz, & Tull, 2010; Trull, 1995), 23% (n � 23) of mothersendorsed clinically relevant levels of BPD symptoms (consistentwith the mean BPD symptom severity reported in BPD outpatientsamples; see Gratz & Gunderson, 2006). Primary analyses used thetotal BPD symptom severity score (� � 0.86 in this sample). Toexplore the relations of specific BPD symptom domains to dis-crepancies between mother-reported and observed infant anger andfear expressions, BEST variables reflecting BPD affective (4items, � � .85), interpersonal (3 items; � � .82), cognitive (2items; r � .49), and behavioral (3 items; � � .85) symptomdomains were also calculated. Across all variables, BPD symp-toms were examined dimensionally, as consistent evidence indi-
cates that dimensional scores are more reliable, stable, and predic-tive of psychosocial morbidity and impairment (Durbin & Klein,2006; Zimmerman, Chelminski, Young, Dalrymple, & Martinez,2013).
Maternal depression symptoms. Mothers completed the 21-item Depression Anxiety Stress Scales (DASS; Lovibond & Lovi-bond, 1995) to assess mood symptoms. The DASS has been foundto have good test–retest reliability, as well as adequate constructand discriminant validity (Lovibond & Lovibond, 1995). Givenevidence of a strong relation between depression and both BPD(Grant et al., 2008) and mother reports of child emotions andtemperament (see Boyle & Pickles, 1997), as well as findings thatmaternal depression is associated with divergence betweenmother-reported and observed measures of infant distress (seeLeerkes & Crockenberg, 2003), the depression scale (7 items; � �.87) was examined as a potential covariate to control for theinfluence of maternal depressive symptom severity on the relationsof interest. This provides a more conservative test of study hy-potheses and ensures that any observed relations between maternalBPD symptoms and discrepancies between mother-reported andobserved infant emotional expressions are not solely attributable totheir shared associations with maternal depression symptoms.
Mother-reported infant emotional expressions. Motherscompleted the Toddler Behavior Assessment Questionnaire(TBAQ; Goldsmith, 1996), a widely used and well-validated mea-sure of infant temperament that assesses the frequency of specificchild behaviors during the past month on a 1 (never) to 7 (always)scale. Evidence for the construct and discriminant validity of thismeasure for infants aged 12 to 36 months has been provided(Goldsmith, 1996; Watamura, Donzella, Kertes, & Gunnar, 2004).The current study used the Anger (10 items; � � .63) and Fear(comprising Social Fear and Object Fear items; 20 items; � � .73)scales to assess mother-reported infant anger and fear expressions.
Observed infant emotional expressions. Infant emotionalexpressions were also assessed observationally as the intensity ofemotional responses to the four Lab-TAB episodes (an observa-tional measure of infant temperament based on the same concep-tualization of infant temperament as the TBAQ; see Goldsmith &Rothbart, 1991). Evidence for the convergent validity of Lab-TABand TBAQ assessments of infant temperament has been provided(see Carnicero, Pérez-López, Salinas, & Martínez-Fuentes, 2000;Goldsmith & Rothbart, 1991).
In each of the Lab-TAB episodes, facial and bodily expressionsof emotion and distress vocalizations were scored in 5- to 10-sepochs across each of the various trials of stimulus exposure.Facial expressions were scored on a 0 (none) to 3 (strong expres-sion in at least 2 regions of the face) scale according to the AFFEXcoding system (Izard, Dougherty, & Humbree, 1983); bodily ex-pressions (i.e., bodily fear, escape, struggle) were scored on a 0(none) to 3 (extreme) scale; and distress vocalizations were scoredon a 0 (none) to 5 (full intensity cry/scream) scale. Codersachieved and maintained reliability (ICCs � .79 to .98) with amaster coder (the second author) throughout coding. Analyses ofdiscrete behaviors suggested that the sample spanned the range ofpossible values for most codes. Data reduction followed the guide-lines set forth in the Lab-TAB Locomotor Version 3.1 manual(Goldsmith & Rothbart, 1999), relying on correlations amongbehaviors and principle components analyses (PCA) to determinefinal composites.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
3MATERNAL BPD SYMPTOMS AND INFANT EMOTION

The overall Fear composite comprised a fear expression com-posite and distress vocalization composite from each of the fear-eliciting episodes (UD and S). The UD fear expression compositeincluded standardized scores of average and maximum values offacial fear, bodily fear, and escape, as well as the speed (reversedlatency) to the first fear expression. Fear expression in the Sepisode did not include the bodily fear variables due to lowinterrelations with the other variables. Standardized scores of theaverage, maximum, and speed of distress vocalizations were av-eraged to create distress vocalization composites for each episode.The fear expression and distress vocalization composites wereinterrelated across the two fear episodes (range � .25 to .59,average r � .42) and loaded on one principle component in thePCA (loadings � .68 to .82; % variance � 57.02); thus, they wereaveraged to create the final Fear composite.
A similar process of coding and data reduction occurred for theanger-eliciting episodes (GAR and TBB). For both episodes, theanger expression composite included the average and maximumvalues of facial anger and struggle. The speed to first angerexpressions was not as strongly related to the other variables, so itwas not included in the composites. The anger expression anddistress vocalization composites were interrelated across the twoepisodes (range � .28 to .70, average r � .45) and loaded on oneprinciple component in the PCA (loadings � .71 to .81, % vari-ance � 58.99). Thus, their average formed the overall Angercomposite.
Results
Analysis Plan
The relation of maternal BPD symptoms to discrepancies be-tween mother-reported and observed infant expressions of fear andanger was examined in two steps. First, preliminary analysesexamined the relation of maternal BPD symptoms to differencesbetween mother-reported and observed infant emotional expres-sions (calculated by standardizing infant emotional expressionvariables and subtracting the observed score from the mother-reported score). To understand the direction of these differences,we used these difference scores to categorize mothers as underre-porting, converging, or overreporting, and examined differences inmean levels of maternal BPD symptoms across these three cate-gories. Although recent research on informant discrepancies hasrevealed several limitations with regard to the statistical propertiesand interpretability of difference scores (as well as how they relateto other variables; De Los Reyes et al., 2011; Laird & De LosReyes, 2013), the examination of difference scores in preliminaryanalyses allows comparisons to past research in this area that hasrelied on this approach (e.g., Gartstein & Marmion, 2008) andcontributes to the growing body of research comparing this ap-proach with more recent innovations in the assessment of infor-mant discrepancies (as used in our primary analyses). Specifically,and consistent with the most current examinations of informantdiscrepancies (e.g., Laird & De Los Reyes, 2013), primary anal-yses examined the interaction between mother-reported and ob-served infant emotional expression variables using multiple regres-sion analyses with powered polynomials. As explained by Lairdand De Los Reyes (2013), the interaction between multiple sourcesof information on a trait or characteristic allows for the examina-
tion of how convergence or divergence relates to a third variable.According to their methodology, each source of information isincluded as a predictor and the third variable of interest serves asthe dependent variable. The inclusion of the polynomial termsprevents variance associated with a quadratic effect from beingattributed to the interaction, thereby more accurately isolating themoderation effect (Ganzach, 1997; Laird & De Los Reyes, 2013).Thus, these analyses were expected to provide the clearest infor-mation on the relation between maternal BPD symptoms andpatterns of convergence and divergence between mother-reportedand observed infant anger and fear expressions.
Of note, informant discrepancies within the clinical literature areusually examined between two individuals using the same measure(e.g., parent and teacher, mother and father) and reporting on olderchildren or adolescents. Research with young children such asinfants, primarily in the developmental literature, is much morelikely to use observational methods in addition to parent report;thus, understanding convergence and divergence between thesetwo methods has been a salient and long-standing concern (e.g.,Rothbart & Bates, 2006). Treating parent-report and observation as“informants” and considering that discrepancies may relate mean-ingfully to other constructs (rather than reflecting nuisance errorvariance) therefore bridges and extends the more clinically basedinformant discrepancies and developmental literatures.
Missing Data
Two mothers were missing relevant questionnaire measures and,thus, were excluded from analyses. In addition, one child wasmissing Lab-TAB data and was excluded from analyses. The finalsample consisted of 98 mother–infant dyads with complete data.
Preliminary Analyses
Descriptive data on the BPD symptoms of the mothers arepresented in Table 1, and descriptive statistics and bivariate cor-relations among all primary variables are presented in Table 2. Allvariables approximated normal distributions. Notably, maternaldepression symptoms related positively to maternal BPD symp-
Table 1Descriptive Data on Maternal Borderline Personality Disorder(BPD) Symptoms
BPD symptom M SD% moderateimpairment
1. Fear of abandonment 1.99 1.30 27.7%2. Unstable relationships 2.34 1.28 39.8%3. Identity disturbance 1.79 1.27 22.7%4. Emotional instability 1.59 1.02 16.9%5. Paranoid thoughts 1.37 0.78 9.9%6. Intense anger 2.16 1.26 29.7%7. Emptiness 1.74 1.21 21.7%8. Self-injurious behavior 1.25 0.87 7.0%9. Impulsivity 1.51 1.04 15.9%
Note. The Borderline Evaluation of Severity over Time (BEST) was usedas the measure of BPD symptoms. The range of each item was 1 �none/slight to 5 � extreme. Moderate impairment is indicated by a score of3 or higher on each item.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
4 WHALEN, KIEL, TULL, LATZMAN, AND GRATZ

toms and, thus, were included as a covariate in all subsequentanalyses.
As noted above, difference scores were created by standardizingthe infant emotional expression variables and subtracting the ob-served score from the mother-reported score. Thus, positive valuesindicate that mothers reported more intense emotional expressionsthan observed, negative scores indicate that mothers reported lessintense emotional expressions than observed, and scores of zeroindicate that mother-report and observation yielded similar levelsof infant emotional expressions.
Two multiple linear regression analyses (one for infant angerexpressions and one for infant fear expressions) were conducted,with maternal depression symptoms included as a covariate ineach. In the infant anger model, R2 � .17, F(2, 95) � 9.93, p �.001, the difference score related positively to maternal BPDsymptoms (� � 0.30, t � 3.18, p � .002) above and beyond theeffect of maternal depression symptoms (� � 0.23, t � 2.40, p �.018), indicating that mothers with higher levels of BPD symptomsreported more anger relative to what was observed. In the infantfear expressions model, R2 � .10, F(2, 95) � 5.25, p � .007, thedifference score did not relate to maternal BPD symptoms (� �0.12, t � 1.25, p � .215) above and beyond maternal depressionsymptoms (� � 0.27, t � 2.79, p � .006).
To further understand the relation between maternal BPD symp-toms and the difference scores, we categorized difference scores asindicating underreporting if the score was lower than 1 SD belowthe mean, overreporting if the score was higher than 1 SD abovethe mean, or converging if within � 1 SD of the mean. We thenexamined differences in mean levels of maternal BPD symptomsacross these three categories. For the anger difference scores, F(2,95) � 5.99, p � .004, mean BPD symptoms increased across theunderreporting (n � 18, M � 18.33, SD � 6.14), converging (n �61, M � 24.34, SD � 9.90), and overreporting (n � 19, M �29.47, SD � 12.03) groups, with a significant difference existingbetween the underreporting and overreporting groups (p � .002,Cohen’s d � 1.16). This suggests that mothers with high levels ofBPD symptoms tend to overreport their infants’ anger and motherswith low levels of BPD symptoms tend to underreport infant anger.For the fear difference scores, the omnibus test did not reachsignificance, F(2, 95) � 1.25, p � .293, nor did any pairwisecomparisons (ps � .25) among the underreporting (n � 12, M �20.75, SD � 8.69), converging (n � 68, M � 24.18, SD � 9.63),and overreporting (n � 18, M � 26.78, SD � 13.21) groups.
Polynomial Regression Analyses
Infant anger and fear expressions were examined in separateregression models predicting maternal BPD symptoms. Eachmodel contained linear and quadratic terms of the maternal reportvariable of infant anger/fear, linear and quadratic terms of ob-served infant anger/fear, and the interaction (cross-product) be-tween the linear terms of mother-reported and observed anger/fear.Maternal report and observed variables were centered prior toanalyses. A significant interaction was probed by recentering ob-served infant anger/fear at standard values (mean and � 1 SD) andexamining simple slopes of the maternal report variable in relationto maternal BPD symptoms. Maternal depression symptoms wereincluded as a covariate in both models. Summaries of regressionmodels are presented in Table 3.
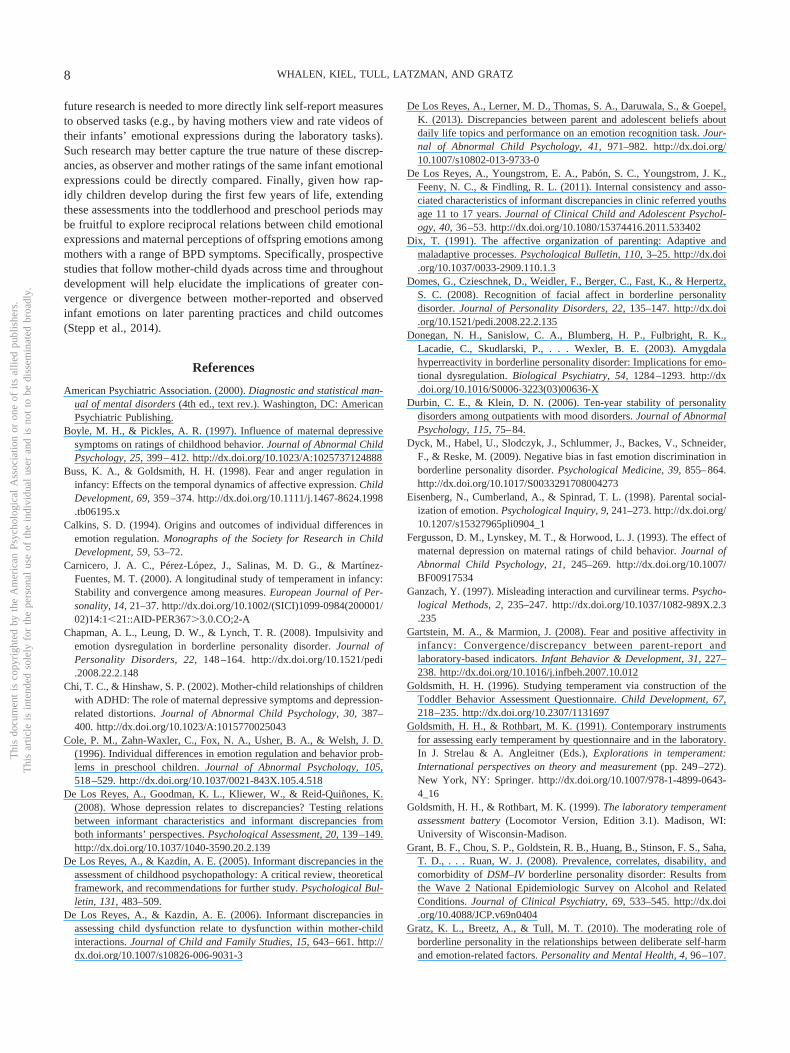
Anger. The overall regression model predicting maternal BPDsymptoms from the infant anger variables was significant, with theinteraction between mother-reported and observed infant angerexpressions emerging as significant. Probing of this interaction(see Figure 1) revealed that mother-reported anger did not relate tomaternal BPD symptoms at low (�1 SD) values of observed infantanger (� � 0.07, t � 0.50, p � .621), but related positively tomaternal BPD symptoms at mean (� � 0.34, t � 3.56, p � .001)and high (1 SD; � � 0.61, t � 3.82, p � .001) values of observedinfant anger. Thus, for infants low in observed anger expressivity,maternal reports of infant anger did not relate to BPD symptoms;however, as observed infant anger increased, maternal report ofinfant anger related more strongly to BPD symptoms. In otherwords, convergence between observed and mother-reported infantanger expressions related to higher maternal BPD symptoms.Notably, post hoc analyses exploring the relevance of particularBPD symptom domains to the observed interaction suggest that itis the interpersonal symptoms of BPD that are driving this inter-action. Specifically, whereas the interaction term was not signifi-cant for BPD affective, cognitive, or behavioral symptoms (�s �0.17, ts � 1.61, ps � .10), it was significant for BPD interpersonalsymptoms (� � 0.21, t � 2.19, p � .031), with mother-reportedanger relating positively to BPD interpersonal symptoms at mean(� � 0.32, t � 3.28, p � .001) and high (� � 0.57, t � 3.50, p �.001) values of observed infant anger, but not at low values ofobserved infant anger (� � 0.07, t � 0.49, p � .626).
Fear. The overall regression predicting maternal BPD symp-toms from the infant fear expression variables was significant. Inthis model, the interaction between mother-reported and observedinfant fear was not significant. When it was dropped from the
Table 2Descriptive Statistics and Bivariate Correlations
Variable Mean (SD) Range 2 3 4 5 6
1. Maternal BPD symptoms 24.15 (10.27) 12.00 to 56.00 .29�� �.12 .33�� �.03 .162. Maternal depression symptoms 5.07 (7.15) 0.00 to 34.00 — �.07 .20� �.14 .063. Observed infant anger �0.01 (0.64) �1.47 to 1.64 — .03 �.03 �.114. Mother-reported infant anger 4.75 (1.05) 1.90 to 7.00 — �.08 .29��
5. Observed infant fear �0.01 (0.61) �0.91 to 1.77 — .116. Mother-reported infant fear 3.62 (0.96) 1.75 to 6.25 —
Note. BPD � borderline personality disorder. Observed infant anger and fear were computed as the mean of z scores of individual behaviors.� p � .05. �� p � .01.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
5MATERNAL BPD SYMPTOMS AND INFANT EMOTION
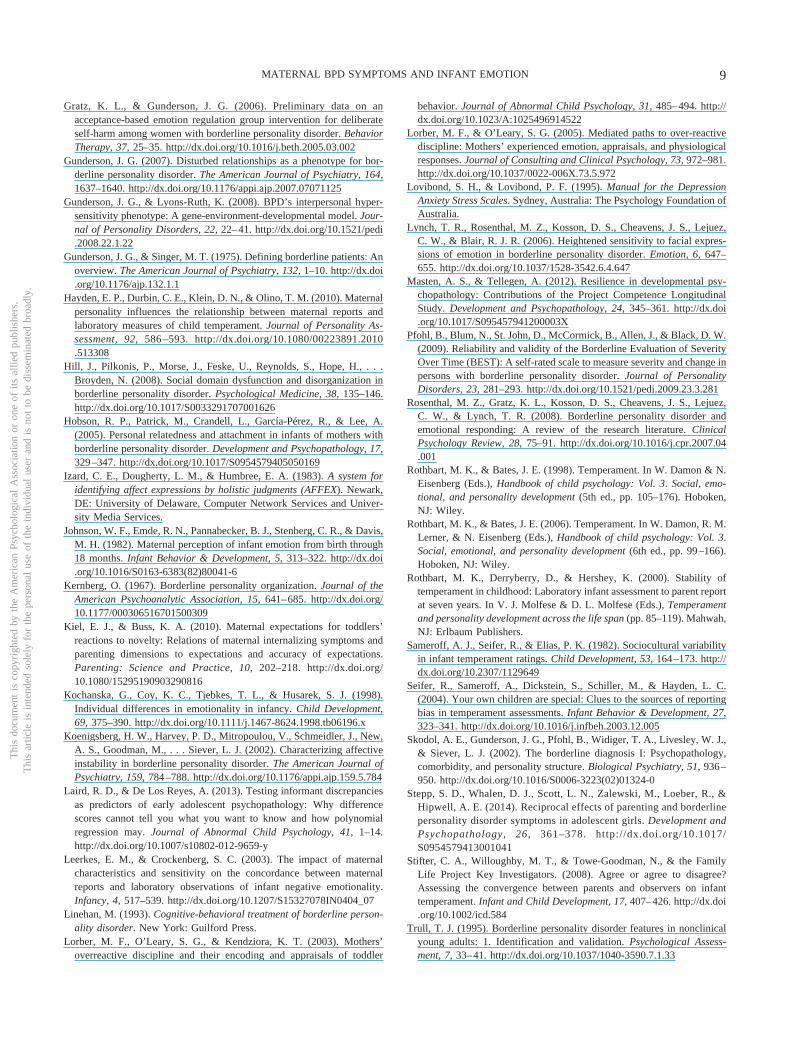
model, negative linear (� � �0.25, t � �2.24, p � .028) andpositive quadratic (� � 0.43, t � 3.84, p � .001) effects emergedfor observed infant fear, suggesting that moderate observed infantfear related to lower maternal BPD symptoms, whereas moreextreme values in either the positive or negative direction relatedto higher maternal BPD symptoms (see Figure 2). Post hoc anal-yses examining specific BPD symptom domains revealed a similarpattern for BPD affective, cognitive, and interpersonal symptoms,including both nonsignificant interaction terms (�s � 0.05, ts �0.55, ps � .58) and, when the interaction term was dropped fromthe model, significant positive quadratic effects (�s � 0.32, ts �2.85, ps � .05). Interestingly, however, a different pattern ofresults emerged for BPD behavioral symptoms, for which theinteraction term was significant (� � 0.26, t � 2.84, p � .006).Probing of this interaction revealed that mother-reported fear didnot relate to BPD behavioral symptoms at low (� � �0.15,t � �1.18, p � .241) or mean (� � 0.11, t � 1.17, p � .245)values of observed infant fear, but it did relate at high values ofobserved infant fear (� � 0.37, t � 2.70, p � .008). This suggeststhat BPD behavioral symptoms relate to convergence betweenmother-reported and observed infant fear expressions.
Discussion
This study examined the relation of maternal BPD symptoms todiscrepancies between maternal reports of infant anger and fearexpressions and observed infant emotional expressions duringstandardized laboratory tasks. The results of this study extendextant literature on the impact of maternal BPD on the mother–child relationship, highlighting the importance of examining ma-ternal perceptions of infants’ emotions and other characteristics.Specifically, using a difference score method, findings suggested aheightened sensitivity to infant anger among mothers with higherBPD symptoms, revealing a positive association between maternalBPD symptoms and greater reports of infant anger (relative to thelevel of infant anger observed during the laboratory tasks). How-ever, findings of polynomial regressions examining the interactionbetween mother-reported and observed infant anger in relation tomaternal BPD symptoms (Laird & De Los Reyes, 2013) revealeda more nuanced relationship, suggesting that this heightened sen-sitivity to infant anger among mothers with higher BPD symptomsmay take the form of maternal reports that converge with infantanger expressions in the laboratory (rather than simply an overre-porting of infant anger vs. observed levels).
Indeed, although different from our predictions, findings thatmaternal BPD symptoms were associated with greater conver-gence between mother-reported and observed infant anger expres-
Table 3Regression Models Predicting Maternal Borderline Personality Disorder Symptoms
Variable
Anger model Fear model
R2 � .25, F(6, 91) � 4.96��� R2 � .24, F(6, 91) � 4.69���
b (SE) � t value b (SE) � t value
Intercept 24.18 (1.42) 17.00��� 19.55 (1.50) 13.00���
Maternal depression symptoms 0.35 (0.14) 0.25 2.57� 0.31 (0.14) 0.21 2.26�
Reported affect 3.27 (0.92) 0.34 3.56�� 1.80 (1.04) 0.17 1.73†
Observed affect �1.48 (1.48) �0.09 �1.00 �4.28 (1.90) �0.26 �2.26�
Reported2 0.57 (0.63) 0.09 0.90 0.01 (0.78) 0.00 0.01Observed2 �1.66 (1.74) �0.09 �0.96 7.99 (2.08) 0.43 3.84���
Observed Reported 4.09 (1.70) 0.23 2.42� 1.54 (1.64) 0.09 0.94
Note. Observed and reported anger and fear were centered at their means before calculation of higher-order terms. Reported affect and Observed affectrepresent linear terms; Reported2 and Observed2 represent quadratic terms. Probing of the significant interaction for the anger model and results afterdropping the nonsignificant interaction in the fear model are reported in text.† p � .10. � p � .05. �� p � .01. ��� p � .001.
Figure 1. Interaction between observed and mother-reported infant angerin relation to maternal BPD symptoms. The linear effect of mother-reported anger was not significant at low observed infant anger, but it wassignificant and became increasingly strong across mean and high levels ofobserved anger. The quadratic effect of mother-reported anger was notsignificant. �� p � .01, ��� p � .001.
Figure 2. Relation between observed infant fear and maternal BPDsymptoms. Plot reflects significant negative linear and positive quadratictrends.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
6 WHALEN, KIEL, TULL, LATZMAN, AND GRATZ

sions are not inconsistent with past literature on heightened angersensitivity in BPD (Domes et al., 2008; Lynch et al., 2006).Specifically, these findings stand in contrast to past research indi-cating a positivity bias in maternal reports of young children’sanger and negative affect (Seifer, Sameroff, Dickstein, Schiller, &Hayden, 2004; Stifter, Willoughby, & Towe-Goodman, 2008),particularly among mothers with low levels of negative emotion-ality (Hayden et al., 2010). This research indicates a tendency formothers to report lower levels of infant negative affect than trainedobservers. Thus, the absence of such a positivity bias amongmothers with higher BPD symptoms may reflect a heightenedsensitivity to and/or reporting of infant anger. Notably, given thata positivity bias in mothers is considered a protective factorassociated with more sensitive parenting (Weis & Lovejoy, 2002),the absence of this maternal bias may have a negative impact onboth maternal parenting and child outcomes, influencing mothers’emotional communication, sensitivity, and responsiveness (e.g.,Chi & Hinshaw, 2002; Lorber, O’Leary, & Kendziora, 2003;Lorber & O’Leary, 2005).
A similar relation between maternal BPD symptoms and con-vergence of mother-reported and observed infant fear expressionswas found for only the behavioral symptoms of BPD; maternalBPD symptoms in general were not related to discrepancies be-tween mother-reported and observed infant fear. However, find-ings did reveal a relation between maternal BPD symptoms andlevels of infant fear expressions in the laboratory, such that ma-ternal BPD symptoms related to both low and high (vs. moderate)levels of fear expressions in the laboratory. Given evidence thatboth high and low levels of emotional expressivity (vs. modulatedexpressivity) in young children may be indicative of emotionregulation difficulties (Buss & Goldsmith, 1998; Cole, Zahn-Waxler, Fox, Usher, & Welsh, 1996), findings that maternal BPDsymptoms are related to both high and low levels of infant fearexpressions in the laboratory may suggest a relation betweenmaternal BPD symptoms and infant emotion regulation difficul-ties. Future work should continue to explore emotion-specificpatterns of convergence or divergence between mother-reportedand observed infant negative emotional expressions among moth-ers with BPD symptoms.
At the level of specific BPD symptom domains, results revealedgreater convergence between mother-reported and observed levelsof infant anger and fear among mothers with higher BPD inter-personal and behavioral symptoms, respectively. These resultsdiffer from previous findings of divergence between mother-reported and observed infant fear and general distress amongmothers with depression and high negative emotionality (Gartstein& Marmion, 2008; Leerkes & Crockenberg, 2003). Althoughdifferences in the methods used to determine discrepancies be-tween mother-reported and observed infant emotions may accountfor this different pattern of findings (with extant research generallyrelying on the difference score method to calculate discrepancies,rather than the polynomial regressions used here), these findingsmay also reflect something unique about the impact of maternalBPD interpersonal and behavioral symptoms in particular (vs.negative emotionality or psychopathology in general) on percep-tions of infant anger and fear. For example, it is possible thatinterpersonal sensitivity and related fears of rejection increasesensitivity to emotional expressions that may signal the possibilityof rejection (i.e., anger expressions; see Domes et al., 2008;
Donegan et al., 2003; Gunderson, 2007; Gunderson & Lyons-Ruth, 2008). Indeed, literature suggests a relation between theinterpersonal sensitivity in BPD and both heightened sensitivity toanger cues and a bias toward the perception of anger in others(Domes et al., 2008).
As for the relation between BPD behavioral symptoms andperceptions of infant fear, it is likely that these particular BPDsymptoms are frightening to infants (similar to the maternal fright-ening behaviors that have been linked to infant fearful expressionsand related fear responses in disorganized attachment; Hobson,Patrick, Crandell, García-Pérez, & Lee, 2005). Consequently, it ispossible that these particular BPD symptoms may be associatedwith increased sensitivity to infant fear expressions attributable torepeated exposure to and related increased familiarity with suchexpressions. Future research examining the mechanisms underly-ing specific BPD symptoms and heightened sensitivity to infantemotional expressions (across discrete negative and positive emo-tions) is needed.
Several limitations of the current study should be noted. First,this study examined BPD symptoms among women in the com-munity. Replication of these findings in larger samples of motherswith a BPD diagnosis is necessary to ensure the validity andgeneralizability of these findings. Likewise, future studies includ-ing clinical control groups of mothers with depression, anxiety,and/or other personality disorders are needed to examine thespecificity of these findings to mothers with BPD symptoms, aswell as the specific influences of different forms of maternalpsychopathology on discrepancies between reported and observedinfant emotional expressions. Moreover, this study focused onexploring convergence of maternal reports and observations ofinfant anger and fear in particular, given evidence for the particularrelevance of these emotions to the emotional dysfunction of BPD(Domes et al., 2008; Koenigsberg et al., 2002). Future work shouldextend these findings by investigating convergence betweenmother-reported and observed positive emotional expressions ininfants (Stifter et al., 2008). Indeed, given evidence of a relationbetween positive emotionality and both positive outcomes andresilience (Masten & Tellegen, 2012), an infant’s ability to expressand maintain positive emotions may serve as an important indica-tor of resilience in this high-risk group.
An additional limitation that is often discussed in research oninfant emotional expressions (Rothbart & Bates, 1998) has to dowith the generalizability and scope of laboratory assessments ofinfant negative emotionality, relative to maternal reports of infantemotions. Specifically, whereas mothers are likely drawing onnumerous data points when reporting on infant behaviors, thelaboratory assessments capture infant behavior at a single point intime (which may be influenced by numerous factors, including theinfant’s fatigue, hunger, or level of distress before the assessment).These limitations of the laboratory tasks may artificially restrictconvergence with maternal reports of infant emotionality. Futureresearch should aim to address these limitations by repeatedlyexamining infant emotional expressions in a variety of contexts,both in and outside of the laboratory. Likewise, the specific do-mains assessed in the laboratory tasks were not a direct match tothe temperament questionnaire domains (consistent with past re-search examining this question with infants; Gartstein & Marmion,2008). Although the incorporation of both observed and mother-reported infant emotional expressions is a strength of this study,
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
7MATERNAL BPD SYMPTOMS AND INFANT EMOTION
future research is needed to more directly link self-report measuresto observed tasks (e.g., by having mothers view and rate videos oftheir infants’ emotional expressions during the laboratory tasks).Such research may better capture the true nature of these discrep-ancies, as observer and mother ratings of the same infant emotionalexpressions could be directly compared. Finally, given how rap-idly children develop during the first few years of life, extendingthese assessments into the toddlerhood and preschool periods maybe fruitful to explore reciprocal relations between child emotionalexpressions and maternal perceptions of offspring emotions amongmothers with a range of BPD symptoms. Specifically, prospectivestudies that follow mother-child dyads across time and throughoutdevelopment will help elucidate the implications of greater con-vergence or divergence between mother-reported and observedinfant emotions on later parenting practices and child outcomes(Stepp et al., 2014).
References
American Psychiatric Association. (2000). Diagnostic and statistical man-ual of mental disorders (4th ed., text rev.). Washington, DC: AmericanPsychiatric Publishing.
Boyle, M. H., & Pickles, A. R. (1997). Influence of maternal depressivesymptoms on ratings of childhood behavior. Journal of Abnormal ChildPsychology, 25, 399–412. http://dx.doi.org/10.1023/A:1025737124888
Buss, K. A., & Goldsmith, H. H. (1998). Fear and anger regulation ininfancy: Effects on the temporal dynamics of affective expression. ChildDevelopment, 69, 359–374. http://dx.doi.org/10.1111/j.1467-8624.1998.tb06195.x
Calkins, S. D. (1994). Origins and outcomes of individual differences inemotion regulation. Monographs of the Society for Research in ChildDevelopment, 59, 53–72.
Carnicero, J. A. C., Pérez-López, J., Salinas, M. D. G., & Martínez-Fuentes, M. T. (2000). A longitudinal study of temperament in infancy:Stability and convergence among measures. European Journal of Per-sonality, 14, 21–37. http://dx.doi.org/10.1002/(SICI)1099-0984(200001/02)14:1�21::AID-PER367�3.0.CO;2-A
Chapman, A. L., Leung, D. W., & Lynch, T. R. (2008). Impulsivity andemotion dysregulation in borderline personality disorder. Journal ofPersonality Disorders, 22, 148–164. http://dx.doi.org/10.1521/pedi.2008.22.2.148
Chi, T. C., & Hinshaw, S. P. (2002). Mother-child relationships of childrenwith ADHD: The role of maternal depressive symptoms and depression-related distortions. Journal of Abnormal Child Psychology, 30, 387–400. http://dx.doi.org/10.1023/A:1015770025043
Cole, P. M., Zahn-Waxler, C., Fox, N. A., Usher, B. A., & Welsh, J. D.(1996). Individual differences in emotion regulation and behavior prob-lems in preschool children. Journal of Abnormal Psychology, 105,518–529. http://dx.doi.org/10.1037/0021-843X.105.4.518
De Los Reyes, A., Goodman, K. L., Kliewer, W., & Reid-Quiñones, K.(2008). Whose depression relates to discrepancies? Testing relationsbetween informant characteristics and informant discrepancies fromboth informants’ perspectives. Psychological Assessment, 20, 139–149.http://dx.doi.org/10.1037/1040-3590.20.2.139
De Los Reyes, A., & Kazdin, A. E. (2005). Informant discrepancies in theassessment of childhood psychopathology: A critical review, theoreticalframework, and recommendations for further study. Psychological Bul-letin, 131, 483–509.
De Los Reyes, A., & Kazdin, A. E. (2006). Informant discrepancies inassessing child dysfunction relate to dysfunction within mother-childinteractions. Journal of Child and Family Studies, 15, 643–661. http://dx.doi.org/10.1007/s10826-006-9031-3
De Los Reyes, A., Lerner, M. D., Thomas, S. A., Daruwala, S., & Goepel,K. (2013). Discrepancies between parent and adolescent beliefs aboutdaily life topics and performance on an emotion recognition task. Jour-nal of Abnormal Child Psychology, 41, 971–982. http://dx.doi.org/10.1007/s10802-013-9733-0
De Los Reyes, A., Youngstrom, E. A., Pabón, S. C., Youngstrom, J. K.,Feeny, N. C., & Findling, R. L. (2011). Internal consistency and asso-ciated characteristics of informant discrepancies in clinic referred youthsage 11 to 17 years. Journal of Clinical Child and Adolescent Psychol-ogy, 40, 36–53. http://dx.doi.org/10.1080/15374416.2011.533402
Dix, T. (1991). The affective organization of parenting: Adaptive andmaladaptive processes. Psychological Bulletin, 110, 3–25. http://dx.doi.org/10.1037/0033-2909.110.1.3
Domes, G., Czieschnek, D., Weidler, F., Berger, C., Fast, K., & Herpertz,S. C. (2008). Recognition of facial affect in borderline personalitydisorder. Journal of Personality Disorders, 22, 135–147. http://dx.doi.org/10.1521/pedi.2008.22.2.135
Donegan, N. H., Sanislow, C. A., Blumberg, H. P., Fulbright, R. K.,Lacadie, C., Skudlarski, P., . . . Wexler, B. E. (2003). Amygdalahyperreactivity in borderline personality disorder: Implications for emo-tional dysregulation. Biological Psychiatry, 54, 1284–1293. http://dx.doi.org/10.1016/S0006-3223(03)00636-X
Durbin, C. E., & Klein, D. N. (2006). Ten-year stability of personalitydisorders among outpatients with mood disorders. Journal of AbnormalPsychology, 115, 75–84.
Dyck, M., Habel, U., Slodczyk, J., Schlummer, J., Backes, V., Schneider,F., & Reske, M. (2009). Negative bias in fast emotion discrimination inborderline personality disorder. Psychological Medicine, 39, 855–864.http://dx.doi.org/10.1017/S0033291708004273
Eisenberg, N., Cumberland, A., & Spinrad, T. L. (1998). Parental social-ization of emotion. Psychological Inquiry, 9, 241–273. http://dx.doi.org/10.1207/s15327965pli0904_1
Fergusson, D. M., Lynskey, M. T., & Horwood, L. J. (1993). The effect ofmaternal depression on maternal ratings of child behavior. Journal ofAbnormal Child Psychology, 21, 245–269. http://dx.doi.org/10.1007/BF00917534
Ganzach, Y. (1997). Misleading interaction and curvilinear terms. Psycho-logical Methods, 2, 235–247. http://dx.doi.org/10.1037/1082-989X.2.3.235
Gartstein, M. A., & Marmion, J. (2008). Fear and positive affectivity ininfancy: Convergence/discrepancy between parent-report andlaboratory-based indicators. Infant Behavior & Development, 31, 227–238. http://dx.doi.org/10.1016/j.infbeh.2007.10.012
Goldsmith, H. H. (1996). Studying temperament via construction of theToddler Behavior Assessment Questionnaire. Child Development, 67,218–235. http://dx.doi.org/10.2307/1131697
Goldsmith, H. H., & Rothbart, M. K. (1991). Contemporary instrumentsfor assessing early temperament by questionnaire and in the laboratory.In J. Strelau & A. Angleitner (Eds.), Explorations in temperament:International perspectives on theory and measurement (pp. 249–272).New York, NY: Springer. http://dx.doi.org/10.1007/978-1-4899-0643-4_16
Goldsmith, H. H., & Rothbart, M. K. (1999). The laboratory temperamentassessment battery (Locomotor Version, Edition 3.1). Madison, WI:University of Wisconsin-Madison.
Grant, B. F., Chou, S. P., Goldstein, R. B., Huang, B., Stinson, F. S., Saha,T. D., . . . Ruan, W. J. (2008). Prevalence, correlates, disability, andcomorbidity of DSM–IV borderline personality disorder: Results fromthe Wave 2 National Epidemiologic Survey on Alcohol and RelatedConditions. Journal of Clinical Psychiatry, 69, 533–545. http://dx.doi.org/10.4088/JCP.v69n0404
Gratz, K. L., Breetz, A., & Tull, M. T. (2010). The moderating role ofborderline personality in the relationships between deliberate self-harmand emotion-related factors. Personality and Mental Health, 4, 96–107.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
8 WHALEN, KIEL, TULL, LATZMAN, AND GRATZ
Gratz, K. L., & Gunderson, J. G. (2006). Preliminary data on anacceptance-based emotion regulation group intervention for deliberateself-harm among women with borderline personality disorder. BehaviorTherapy, 37, 25–35. http://dx.doi.org/10.1016/j.beth.2005.03.002
Gunderson, J. G. (2007). Disturbed relationships as a phenotype for bor-derline personality disorder. The American Journal of Psychiatry, 164,1637–1640. http://dx.doi.org/10.1176/appi.ajp.2007.07071125
Gunderson, J. G., & Lyons-Ruth, K. (2008). BPD’s interpersonal hyper-sensitivity phenotype: A gene-environment-developmental model. Jour-nal of Personality Disorders, 22, 22–41. http://dx.doi.org/10.1521/pedi.2008.22.1.22
Gunderson, J. G., & Singer, M. T. (1975). Defining borderline patients: Anoverview. The American Journal of Psychiatry, 132, 1–10. http://dx.doi.org/10.1176/ajp.132.1.1
Hayden, E. P., Durbin, C. E., Klein, D. N., & Olino, T. M. (2010). Maternalpersonality influences the relationship between maternal reports andlaboratory measures of child temperament. Journal of Personality As-sessment, 92, 586 –593. http://dx.doi.org/10.1080/00223891.2010.513308
Hill, J., Pilkonis, P., Morse, J., Feske, U., Reynolds, S., Hope, H., . . .Broyden, N. (2008). Social domain dysfunction and disorganization inborderline personality disorder. Psychological Medicine, 38, 135–146.http://dx.doi.org/10.1017/S0033291707001626
Hobson, R. P., Patrick, M., Crandell, L., García-Pérez, R., & Lee, A.(2005). Personal relatedness and attachment in infants of mothers withborderline personality disorder. Development and Psychopathology, 17,329–347. http://dx.doi.org/10.1017/S0954579405050169
Izard, C. E., Dougherty, L. M., & Humbree, E. A. (1983). A system foridentifying affect expressions by holistic judgments (AFFEX). Newark,DE: University of Delaware, Computer Network Services and Univer-sity Media Services.
Johnson, W. F., Emde, R. N., Pannabecker, B. J., Stenberg, C. R., & Davis,M. H. (1982). Maternal perception of infant emotion from birth through18 months. Infant Behavior & Development, 5, 313–322. http://dx.doi.org/10.1016/S0163-6383(82)80041-6
Kernberg, O. (1967). Borderline personality organization. Journal of theAmerican Psychoanalytic Association, 15, 641–685. http://dx.doi.org/10.1177/000306516701500309
Kiel, E. J., & Buss, K. A. (2010). Maternal expectations for toddlers’reactions to novelty: Relations of maternal internalizing symptoms andparenting dimensions to expectations and accuracy of expectations.Parenting: Science and Practice, 10, 202–218. http://dx.doi.org/10.1080/15295190903290816
Kochanska, G., Coy, K. C., Tjebkes, T. L., & Husarek, S. J. (1998).Individual differences in emotionality in infancy. Child Development,69, 375–390. http://dx.doi.org/10.1111/j.1467-8624.1998.tb06196.x
Koenigsberg, H. W., Harvey, P. D., Mitropoulou, V., Schmeidler, J., New,A. S., Goodman, M., . . . Siever, L. J. (2002). Characterizing affectiveinstability in borderline personality disorder. The American Journal ofPsychiatry, 159, 784–788. http://dx.doi.org/10.1176/appi.ajp.159.5.784
Laird, R. D., & De Los Reyes, A. (2013). Testing informant discrepanciesas predictors of early adolescent psychopathology: Why differencescores cannot tell you what you want to know and how polynomialregression may. Journal of Abnormal Child Psychology, 41, 1–14.http://dx.doi.org/10.1007/s10802-012-9659-y
Leerkes, E. M., & Crockenberg, S. C. (2003). The impact of maternalcharacteristics and sensitivity on the concordance between maternalreports and laboratory observations of infant negative emotionality.Infancy, 4, 517–539. http://dx.doi.org/10.1207/S15327078IN0404_07
Linehan, M. (1993). Cognitive-behavioral treatment of borderline person-ality disorder. New York: Guilford Press.
Lorber, M. F., O’Leary, S. G., & Kendziora, K. T. (2003). Mothers’overreactive discipline and their encoding and appraisals of toddler
behavior. Journal of Abnormal Child Psychology, 31, 485–494. http://dx.doi.org/10.1023/A:1025496914522
Lorber, M. F., & O’Leary, S. G. (2005). Mediated paths to over-reactivediscipline: Mothers’ experienced emotion, appraisals, and physiologicalresponses. Journal of Consulting and Clinical Psychology, 73, 972–981.http://dx.doi.org/10.1037/0022-006X.73.5.972
Lovibond, S. H., & Lovibond, P. F. (1995). Manual for the DepressionAnxiety Stress Scales. Sydney, Australia: The Psychology Foundation ofAustralia.
Lynch, T. R., Rosenthal, M. Z., Kosson, D. S., Cheavens, J. S., Lejuez,C. W., & Blair, R. J. R. (2006). Heightened sensitivity to facial expres-sions of emotion in borderline personality disorder. Emotion, 6, 647–655. http://dx.doi.org/10.1037/1528-3542.6.4.647
Masten, A. S., & Tellegen, A. (2012). Resilience in developmental psy-chopathology: Contributions of the Project Competence LongitudinalStudy. Development and Psychopathology, 24, 345–361. http://dx.doi.org/10.1017/S095457941200003X
Pfohl, B., Blum, N., St. John, D., McCormick, B., Allen, J., & Black, D. W.(2009). Reliability and validity of the Borderline Evaluation of SeverityOver Time (BEST): A self-rated scale to measure severity and change inpersons with borderline personality disorder. Journal of PersonalityDisorders, 23, 281–293. http://dx.doi.org/10.1521/pedi.2009.23.3.281
Rosenthal, M. Z., Gratz, K. L., Kosson, D. S., Cheavens, J. S., Lejuez,C. W., & Lynch, T. R. (2008). Borderline personality disorder andemotional responding: A review of the research literature. ClinicalPsychology Review, 28, 75–91. http://dx.doi.org/10.1016/j.cpr.2007.04.001
Rothbart, M. K., & Bates, J. E. (1998). Temperament. In W. Damon & N.Eisenberg (Eds.), Handbook of child psychology: Vol. 3. Social, emo-tional, and personality development (5th ed., pp. 105–176). Hoboken,NJ: Wiley.
Rothbart, M. K., & Bates, J. E. (2006). Temperament. In W. Damon, R. M.Lerner, & N. Eisenberg (Eds.), Handbook of child psychology: Vol. 3.Social, emotional, and personality development (6th ed., pp. 99–166).Hoboken, NJ: Wiley.
Rothbart, M. K., Derryberry, D., & Hershey, K. (2000). Stability oftemperament in childhood: Laboratory infant assessment to parent reportat seven years. In V. J. Molfese & D. L. Molfese (Eds.), Temperamentand personality development across the life span (pp. 85–119). Mahwah,NJ: Erlbaum Publishers.
Sameroff, A. J., Seifer, R., & Elias, P. K. (1982). Sociocultural variabilityin infant temperament ratings. Child Development, 53, 164–173. http://dx.doi.org/10.2307/1129649
Seifer, R., Sameroff, A., Dickstein, S., Schiller, M., & Hayden, L. C.(2004). Your own children are special: Clues to the sources of reportingbias in temperament assessments. Infant Behavior & Development, 27,323–341. http://dx.doi.org/10.1016/j.infbeh.2003.12.005
Skodol, A. E., Gunderson, J. G., Pfohl, B., Widiger, T. A., Livesley, W. J.,& Siever, L. J. (2002). The borderline diagnosis I: Psychopathology,comorbidity, and personality structure. Biological Psychiatry, 51, 936–950. http://dx.doi.org/10.1016/S0006-3223(02)01324-0
Stepp, S. D., Whalen, D. J., Scott, L. N., Zalewski, M., Loeber, R., &Hipwell, A. E. (2014). Reciprocal effects of parenting and borderlinepersonality disorder symptoms in adolescent girls. Development andPsychopathology, 26, 361–378. http://dx.doi.org/10.1017/S0954579413001041
Stifter, C. A., Willoughby, M. T., & Towe-Goodman, N., & the FamilyLife Project Key Investigators. (2008). Agree or agree to disagree?Assessing the convergence between parents and observers on infanttemperament. Infant and Child Development, 17, 407–426. http://dx.doi.org/10.1002/icd.584
Trull, T. J. (1995). Borderline personality disorder features in nonclinicalyoung adults: 1. Identification and validation. Psychological Assess-ment, 7, 33–41. http://dx.doi.org/10.1037/1040-3590.7.1.33
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
9MATERNAL BPD SYMPTOMS AND INFANT EMOTION

van Asselt, A. D. I., Dirksen, C. D., Arntz, A., & Severens, J. L. (2007).The cost of borderline personality disorder: Societal cost of illness inBPD-patients. European Psychiatry, 22, 354–361. http://dx.doi.org/10.1016/j.eurpsy.2007.04.001
Wagner, A. W., & Linehan, M. M. (1999). Facial expression recognitionability among women with borderline personality disorder: Implicationsfor emotion regulation? Journal of Personality Disorders, 13, 329–344.http://dx.doi.org/10.1521/pedi.1999.13.4.329
Watamura, S. E., Donzella, B., Kertes, D. A., & Gunnar, M. R. (2004).Developmental changes in baseline cortisol activity in early childhood:
Relations with napping and effortful control. Developmental Psycho-biology, 45, 125–133. http://dx.doi.org/10.1002/dev.20026
Weis, R., & Lovejoy, M. C. (2002). Information processing in everydaylife: Emotion-congruent bias in mothers’ reports of parent-child inter-actions. Journal of Personality and Social Psychology, 83, 216–230.
Zimmerman, M., Chelminski, I., Young, D., Dalrymple, K., & Marti-nez, J. (2013). Is dimensional scoring of borderline personalitydisorder important only for subthreshold levels of severity? Journalof Personality Disorders, 27, 244 –251. http://dx.doi.org/10.1521/pedi_2012_26_022
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
10 WHALEN, KIEL, TULL, LATZMAN, AND GRATZ
Related Documents











