UNIVERSITAT DE BARCELONA Facultat de Medicina Departament de Cirurgía i Especialitats Mèdico-Quirúrgiques TESIS DOCTORAL ASOCIACIÓN DE BRONQUIECTASIAS PULMONARES Y PATOLOGÍA NASOSINUSAL. ESTUDIO DE LOS ASPECTOS EPIDEMIOLÓGICOS, ETIOLÓGICOS, DE DIAGNÓSTICO Y TRATAMIENTO. José Mª Guilemany Toste

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

UNIVERSITAT DE BARCELONA Facultat de Medicina
Departament de Cirurgía i Especialitats Mèdico-Quirúrgiques
TESIS DOCTORAL
ASOCIACIÓN DE BRONQUIECTASIAS PULMONARES Y PATOLOGÍA
NASOSINUSAL. ESTUDIO DE LOS ASPECTOS EPIDEMIOLÓGICOS,
ETIOLÓGICOS, DE DIAGNÓSTICO Y TRATAMIENTO.
José Mª Guilemany Toste

UNIVERSITAT DE BARCELONA Facultat de Medicina
Departament de Cirurgía i Especialitats Mèdico-Quirúrgiques
Tesis presentada por el Licenciado José Mª Guilemany Toste a fin de optar al título de Doctor por la Universidad de Barcelona, realizado en la Unitat de Rinologia i Clínica de l’Olfacte, Servei d’Oto-rino-laringologia, Hospital Clínic i Universitari de Barcelona. Directores de tesis Tutor de tesis Joaquim Mullol i Miret Manuel Bernal-Sprekelsen Cèsar Picado i Vallés

5
ÍNDICE
Publicaciones ............................................................................................... 9
Agradecimientos ....................................................................................... 11
Abreviaturas ............................................................................................. 13
I. Parte teórica
Capítulo 1. El aparato respiratorio ............................................................. 19
1. Función nasal ................................................................................ 22
2. Función pulmonar ......................................................................... 23
Capítulo 2. Diferencias y similitudes: mucosa nasal y bronquial.............. 25
1. Epitelio .......................................................................................... 27
2. Submucosa .................................................................................... 28
3. Transporte mucociliar ................................................................... 29
4. Inflamación ................................................................................... 30
5. Respuesta al ejercicio.................................................................... 33
Capítulo 3. Interacción nariz-bronquio ...................................................... 35
1. Hipótesis de la interacción ............................................................ 37
2. Patologías con interacción nariz-bronquio.................................... 39
2.1 Rinitis y asma.................................................................... 39
2.2 Poliposis nasal y asma ...................................................... 43
2.3 Rinosinusitis crónica y EPOC........................................... 54
Capítulo 4. Rinosinusitis crónica sin pólipos............................................. 55
1. Definición de rinosinusitis crónica ............................................... 57
2. Rinosinusitis crónica sin pólipos .................................................. 58
2.1 Epidemiología y comorbilidades ...................................... 58
2.2 Histopatología ................................................................... 62
2.3 Tratamiento ....................................................................... 68

6
Capítulo 5. Rinosinusitis crónica con pólipos............................................ 71
1. Epidemiología y comorbilidades .................................................. 73
2. Histopatología de los pólipos nasales ........................................... 75
2.1 Células inflamatorias ........................................................ 76
2.2 Mediadores inflamatorios ................................................. 78
3. Tratamiento de la rinosinusitis crónica con pólipos ..................... 79
3.1 Tratamiento médico .......................................................... 79
3.2 Tratamiento quirúrgico ..................................................... 82
Capítulo 6. Bronquiectasias ....................................................................... 83
1. Definición...................................................................................... 85
2. Epidemiología ............................................................................... 86
3. Etiología ........................................................................................ 86
3.1 Fibrosis quística ................................................................ 88
3.2 Discinesia ciliar primaria .................................................. 89
3.3 Síndrome de Young .......................................................... 90
3.4 Déficit de alfa 1-antitripsina ............................................. 91
4. Histopatología ............................................................................... 92
5. Aspectos clínicos y diagnóstico .................................................... 93
6. Microbiología................................................................................ 94
7. Tratamiento de las bronquiectasias............................................... 94
7.1 Tratamiento médico .......................................................... 94
7.2 Tratamiento quirúrgico ..................................................... 96
7.3 Otros tratamientos............................................................. 96
II. Hipótesis y objetivos
Hipótesis de trabajo........................................................................... 99
Objetivo general ................................................................................ 99
Objetivos específicos ........................................................................ 99
Interés y aplicabilidad asistencial ................................................... 101
7
III. Trabajo experimental
Artículo original 1 ........................................................................... 105
Artículo original 2 ........................................................................... 109
Artículo original 3 ........................................................................... 113
Artículo de revisión......................................................................... 141
Carta al editor.................................................................................. 149
IV. Discusión ............................................................................................ 153
V. Investigación futura ........................................................................... 167
VI. Conclusiones ..................................................................................... 171
VII. Bibliografía ...................................................................................... 177


I. PARTE TEÓRICA

Capítulo 1. El aparato respiratorio


Tesis Doctoral I. Parte Teórica
21
Capítulo 1. El aparato respiratorio
En la fisiología respiratoria la nariz es un órgano de gran importancia
que supone el 50% de las resistencias al flujo aéreo y cuya patología reúne
en muchas ocasiones a profesionales de especialidades diferentes como
alergólogos, médicos de atención primaria, inmunólogos, neumólogos,
otorrinolaringólogos o pediatras. En los últimos años se ha demostrado que
patologías asumidas como exclusivamente pulmonares o bronquiales
suelen asociarse a patología nasal y paranasal. El concepto de
rinobronquitis1 ha suscitado la idea de que la vía respiratoria superior e
inferior constituyen una única vía, con una enfermedad común que afecta a
todo el aparato respiratorio. Esto ha sido demostrado y confirmado en
múltiples estudios epidemiológicos, apareciendo el concepto de “una única
vía respiratoria, una única patología”. El ejemplo más claro de dicha
asociación es la rinitis y el asma,2,3 habiéndose demostrado que la rinitis se
presenta en la mayoría de los asmáticos y que el tratamiento de la rinitis
puede tener efectos beneficios sobre el curso del asma.4 Datos más
recientes también vislumbran una relación entre EPOC y rinosinusitis
crónica.5
Hasta hace poco la práctica clínica consideraba la patología
rinosinusal y la pulmonar de manera independiente posiblemente debido a
su manejo por especialidades diferentes. En los últimos años esta situación
ha ido cambiando de tal manera que se hace difícil concebir una Unidad de
Rinología moderna sin la colaboración multidisciplinaria de alergólogos,
neumólogos y otorrinolaringólogos.

I. Parte Teórica Tesis Doctoral
22
1. Función nasal
La nariz cumple una serie de funciones bien conocidas como son el
acondicionamiento del aire que respiramos,6 la fonación (resonancia y
modulación de la voz) y la olfación7 (Tabla 1). El flujo nasal, al ser más
lento, proporciona un mayor tiempo de intercambio gaseoso
alveolopulmonar y un mayor número de alveolos dilatados. La nariz es la
responsable de crear los factores de resistencia y conductancia necesarias
para que la barrera hematogaseosa funcione correctamente. Para que la
nariz pueda realizar correctamente el acondicionamiento aéreo
(calentamiento, humidificación y filtrado del mismo), es indispensable la
producción de secreciones nasales por parte de las células caliciformes y
glándulas seromucosas, una efectiva vascularización nasal, una fase de
congestión-descongestión alternante de los cornetes y zonas eréctiles del
tabique (ciclo nasal) y una actividad coordinada del transporte mucociliar.
Aparte de ser una barrera física, la nariz también es una barrera
inmunitaria, siendo el primer órgano de choque para los microorganismos
que penetren en la vía aérea.8
El olfato es otra función importante de la nariz. Su actividad
sensorial la ejercen las ramificaciones del nervio olfatorio (primer par
craneal), las cuales penetran en el techo de la cavidad nasal a través de la
lámina cribosa del hueso etmoides.

Tesis Doctoral I. Parte Teórica
23
Tabla 1. Funciones del epitelio nasosinusal.
Funciones Mecanismos Resultado final
1. Protección física · Complejos de adhesión intercelular (desmosomas)
· Secreción de mucinas
· Absorción selectiva
· Humidificación y calentamiento del aire inhalado
· Limpieza de agentes nocivos
2. Transporte · Transporte ciliar · Transporte de moco desde la nariz y el pulmón a la garganta
3. Secreción · Celular · Mucinas, citocinas, moleculas de adhesion, factores de crecimiento y otros
4. Diana de agentes pro y antiinflamatorios
· Receptores específicos · Respuesta a citocinas, antihistamínicos, cromonas, corticoides y otros.
2. Función pulmonar
Los pulmones9,10 tienen una función respiratoria y otras no
respiratorias:
A) Respiratoria: la función de los pulmones es realizar el intercambio
gaseoso con la sangre,11 por ello los alvéolos están en estrecho contacto con
capilares. En los alvéolos se produce el paso de O2 desde el aire a la sangre
y el paso de CO2 desde la sangre al aire. Este paso se produce por la
diferencia de presiones parciales de O2 y CO2 (difusión simple) entre la
sangre y los alvéolos.
B) No respiratorias:12

I. Parte Teórica Tesis Doctoral
24
- Acción de filtro externo. Los pulmones se defienden de la intensa
contaminación aérea a la que están expuestas por acción del sistema
mucociliar y fagocitario de los macrófagos alveolares.
- La producción de moco, donde impactan las partículas de cierto tamaño,
se realiza por células serosas y mucosas de las glándulas submucosas
bronquiales y por las células calciformes del epitelio bronquial.
- Sistema anti-proteasa (principalmente α1-antitripsina) que ocurre en los
alveolos ante elementos inflamatorios del sistema inmune alveolar. Las
proteasas principales liberadas en el pulmón son la elastasa, colagenasa,
hialuronidasa y tripsina.
- Acciones metabólicas: participación hormonal del sistema renina-
angiotensina-aldosterona, eliminación de fármacos, equilibrio ácido-base,
metabolismo lipídico por acción del surfactante pulmonar.
- Producción de prostaglandinas las cuales causan broncodilatación
(prostaglandina E) o broncoconstricción (prostaglandina A, B, D, F y I).

Capítulo 2. Diferencias y similitudes entre
la mucosa respiratoria nasal y bronquial


Tesis Doctoral I. Parte Teórica
27
Capítulo 2. Diferencias y similitudes entre la mucosa respiratoria nasal
y bronquial.
La mucosa respiratoria está constituida por un epitelio
pseudoestratificado ciliado con abundantes células, muchas de ellas
productoras de moco (células caliciformes). Por debajo hay una submucosa
que contiene las glándulas submucosas, los nervios y los vasos sanguíneos.
La secreción de moco es la característica de la mucosa respiratoria,
cubriendo toda su superficie y presentándose en dos estados: gel y sol.13,14
En el tracto respiratorio superior e inferior existen más similitudes
que diferencias que se puedan objetivar desde las ciencias básicas, como
son la anatomía, la histología y la fisiología. La mucosa nasal y la
bronquial tienen una estructura similar de su epitelio y de su lámina propia.
Una de las funciones más importantes de la nariz es actuar como barrera
para evitar la inhalación de sustancias nocivas. La nariz actúa, además,
como acondicionador del aire inspirado calentándolo y humidificándolo. La
función que más diferencia la nariz de las vías aéreas inferiores es, sin
duda, la función olfatoria propia de la nariz y que tiene su base en la
pituitaria situada en el techo de la fosa nasal.15
1. Epitelio. La mucosa respiratoria presenta un epitelio respiratorio
columnar ciliado pseudoestratificado. Dicho epitelio columnar está
formado por células ciliadas, no ciliadas, basales, caliciformes o goblet,
diferenciándose del epitelio respiratorio de las vias respiratorias bajas por
la no existencia de células serosas, células de Clara y células en cepillo16
(Figura 1). En condiciones fisiológicas, hay un predominio de células
serosas (60%) sobre las mucosas (40%). En los senos paranasales la
superficie del epitelio es más delgada, menos especializada, con menos
cilios y células caliciformes.17

I. Parte Teórica Tesis Doctoral
28
Figura 1. Histología básica del epitelio respiratorio.
Estas circunstancias explican en parte, la menor resistencia a las
infecciones de los senos paranasales respecto a la mucosa nasal.
La membrana basal está compuesta por colágeno tipo IV,
proteinglicanos, laminina y fibronectina. Debajo de ésta existe la
denominada lámina reticularis que se encuentra engrosada de manera
difusa en los pacientes asmáticos.18 Engrosamientos focales de dicha
membrana los encontramos en los pacientes afectos de bronquiectasias,
tuberculosis y rinosinusitis crónica.19 En los pacientes con rinitis no se han
detectado cambios a este nivel.20
2. Submucosa. Se encuentran glándulas, vasos sanguíneos, nervios, células
extravasculares y matriz extracelular. Una de las grandes diferencias la
encontramos a este nivel ya que el músculo liso se encuentra en la capa
submucosa del bronquio pero no en la submucosa de la nariz16 (Figura 2).
En la nariz predominan las glándulas y los vasos. A parte de los
vasos arteriales la vascularización nasal está formada por lechos capilares,
cortocircuitos arteriovenosos, sinusoides y vasos venosos. Las venas que
drenan a los sinusoides contienen músculo liso. Cuando dichas venas se
contraen se produce una expansión de los sinusoides, por lo que se
Células ciliadas / no ciliadas Células caliciformes Células basales

Tesis Doctoral I. Parte Teórica
29
incrementa el tamaño de los cornetes (tejido eréctil) y se refleja en los
flujos nasales. Esto no sucede en los bronquios donde los cambios de
resistencia al flujo son debidos a la contracción de la musculatura lisa.
Figura 2. Diferencias de la submucosa nasal y bronquial. E: epitelio, G: glándula submucosa, V:
vaso sanguíneo; ML: musculatura lisa.
3. Transporte mucociliar. El aparato mucociliar está formado por los
numerosos cilios que emergen de la superficie de las células epiteliales
columnares pseudoestratificadas. Cada célula ciliada, contiene alrededor de
200 a 300 cilios que realizan unas 500 batidas por minuto. En condiciones
fisiológicas, el epitelio respiratorio ciliar esta recubierto de moco desde la
nariz a los bronquiolos mayores. El moco es un medio de protección y
eliminación de las partículas inhaladas, células descamadas, detritus y otros
productos celulares La frecuencia de batida disminuye distalmente,21
siendo en la vía inferior dónde es de menor frecuencia. Su alteración puede
conducir al estancamiento de secreciones y predisposición a padecer
infecciones locales, posiblemente contribuyendo al desarrollo de
bronquiectasias en esa parte de las vías respiratorias.20 El defecto en la
ultraestructura de los cilios, que altera y evita su normal motilidad,
ML E
Bronquio Nariz

I. Parte Teórica Tesis Doctoral
30
predispone a las infecciones crónicas y recurrentes (rinosinusitis crónica,
infecciones pulmonares que provocan la aparición de bronquiectasias).
Todas estas observaciones son las que avalan la hipótesis de la
unidad entre el tracto respiratorio superior e inferior, así como un
mecanismo patogénico común, que se observa en patologías como el asma
y la rinitis/RSC.22,23 La existencia de una única mucosa respiratoria explica
la igualdad del tipo de inflamación frente a las diferentes noxas. Si se
produce una inflamación nasal, exclusivamente en la nariz, por un
alérgeno, esto tiene una repercusión en las vías respiratorias bajas hasta el
punto que se observan cambios en la función pulmonar, en la musculatura
bronquial y cambios inflamatorios en la mucosa bronquial.24-26 Si
estimulamos la nariz somos capaces de provocar lesiones y alteraciones en
la vía respiratoria inferior. En pacientes con rinitis sin asma, en los que se
estudia la inflamación a nivel pulmonar mediante óxido nítrico exhalado
(ONe) durante la estación polínica y la no polínica, se observa que su
inflamación bronquial aumenta en la estación polínica sin tener síntomas.27
Lo mismo ocurre con los esputos inducidos y en las biopsias bronquiales de
pacientes con exacerbaciones de su rinitis con más lesiones a nivel
bronquial, más síntomas y peor función pulmonar.28,29 Se está estudiando
por qué mecanismo existe esta interrelación y si esta respuesta es un
reflejo, pudiendo ser que estos alérgenos lleguen a la vía aérea, al aspirarse.
La hipótesis que actualmente mejor explica esta interrelación es la
sistémica basada en que a nivel nasal se secretarían mediadores que a
través de la sangre serían capaces de influir en la vía aérea inferior y
viceversa.30
4. Inflamación. En las personas sanas la estructura de la mucosa nasal y
bronquial es similar. Ambas se caracterizan por la presencia de un epitelio
pseudoestratificado columnar y ciliado. En la submucosa hay presencia de
Tesis Doctoral I. Parte Teórica
31
glándulas submucosas, vasos sanguíneos, células estructurales, nervios, y
algunas células inflamatorias.2 En presencia de patologías como la rinitis o
el asma, el infiltrado inflamatorio también es parecido, encontrándose los
mismos mediadores, citoquinas derivadas del linfocito Th2, quemoquinas y
moléculas de adhesión.31
También existen diferencias entre la nariz y los bronquios: en la
nariz, existe una gran red de capilares subepiteliales, un sistema arterial y
sinusoides venosos. El alto grado de vascularización es una característica
primordial de la mucosa nasal debido a que los cambios que se generen en
esta amplia red pueden ocasionar una obstrucción nasal grave. En los
bronquios, a diferencia de la nariz, hay presencia de músculo liso, lo cual
explica la presencia de broncoconstricción en el asma.16
La magnitud de la inflamación también puede ser diferente. En los
pacientes con asma moderada a grave la infiltración eosinofílica es más
pronunciada en el bronquio que en la nariz,32 mientras que en aquellos con
asma leve, el grado de inflamación es similar en ambas mucosas. Tal como
se mencionó previamente, la inflamación eosinofílica de la nariz está
presente en los pacientes asmáticos con o sin síntomas nasales.33 El
remodelado de las vías aéreas parece ser menos extenso en la mucosa nasal
que en la bronquial.20,34 Mientras que en los pacientes con asma existe un
aumento en el grosor de la membrana basal e hipertrofia del músculo liso,
en aquellos con rinitis sólo se han demostrado daños menores del epitelio
nasal.20
Inflamación nasal y respuesta bronquial. Diversos estudios clínicos y
experimentales han estudiado la conexión existente entre la rinitis y la
respuesta inflamatoria y funcional en la vía aérea inferior. Tras provocación
nasal con alérgenos en pacientes con rinitis alérgica se ha demostrado un
incremento en la hiperreactividad bronquial y cambios en la función
pulmonar.24-26,35 En otros estudios se ha descrito la presencia de

I. Parte Teórica Tesis Doctoral
32
inflamación alérgica sistémica tras la provocación nasal tanto en modelos
animales como en humanos. McCusker et al.36 realizaron provocaciones
nasales con ovoalbúmina en un modelo murino demostrando cambios
inflamatorios tanto en vías aéreas nasales como bronquiales, encontrando
niveles elevados de IL-5 y eosinófilos en el lavado broncoalveolar.
Braunstahl et al.37 estudiaron la expresión de las moléculas de adhesión en
biopsias nasales y bronquiales obtenidas de forma previa y a las 24 horas
tras la provocación nasal con alérgeno en pacientes con rinitis estacional.
Encontraron un aumento significativo de los eosinófilos en el epitelio y la
lámina propia nasal y en el epitelio bronquial a las 24 horas de la
provocación, lo cual se correlacionó con la expresión de las moléculas de
adhesión. Igualmente detectaron un aumento significativo del número de
eosinófilos y del nivel de IL-5 en las muestras de sangre obtenidas a las 24
horas del estímulo. Beeh et al.38 estudiaron marcadores de la inflamación
en esputo inducido y en plasma antes y 24 horas después de realizar una
provocación nasal con extractos de pólenes en pacientes alérgicos fuera de
la época estacional. Encontraron un aumento de los marcadores de la
inflamación como la proteína catiónica de los eosinófilos (PCE) y la
molécula de adhesión intercelular (ICAM-1) en esputo que se correlacionó
con un aumento de la IL-5 en plasma.
Otros trabajos han demostrado una respuesta inflamatoria bronquial
en pacientes con rinitis alérgica sin asma tras la exposición natural a
pólenes, y tras provocaciones bronquiales repetidas a bajas dosis.39-42
Inflamación bronquial y respuesta nasal. Braunstahl et al.28,29
estudiaron desde el punto de vista opuesto, la respuesta inflamatoria nasal
tras la provocación bronquial segmentaria con alergeno en pacientes con
rinitis polínica pero sin asma. Encontraron que a través de este
procedimiento se inducían síntomas nasales y bronquiales, así como un

Tesis Doctoral I. Parte Teórica
33
aumento de los eosinófilos en sangre periférica, e infiltración de eosinófilos
y basófilos en la mucosa nasal y bronquial.
5. Respuesta al ejercicio. La nariz y los bronquios responden de forma
diferente al ejercicio. Entre un 40 y un 90% de los pacientes con asma
presentan una reducción en el valor del volumen espirado máximo en el
primer segundo (VEMS) cuando son sometidos a una prueba de esfuerzo.
Algunos autores sugieren que esta broncoconstricción parece estar mediada
por la degranulación de los mastocitos como consecuencia de un aumento en
la osmolaridad del líquido que recubre las vías aéreas,43 si bien no ha sido
demostrado claramente.
A diferencia de los bronquios, la nariz siempre se dilata tras el
esfuerzo. En diferentes estudios realizados, tanto en sujetos sanos como en
pacientes con diversas patologías respiratorias (desviación septal, rinitis,
asma, fibrosis quística),44-49 se ha podido demostrar que el ejercicio produce
una disminución de las resistencias y un aumento de los volúmenes nasales.
El cambio en las resistencias nasales ocurre de manera inmediata tras
realizar el esfuerzo y la recuperación de los valores normales suele tardar de
30 a 40 minutos.44-47 Se ha considerado que estos cambios son debidos en su
mayor parte a un fenómeno de vasoconstricción nasal que disminuye el
volumen de los sinusoides venosos. Esta vasoconstricción se cree que está
causada por un aumento en la actividad simpática, ya que se ha podido
comprobar que el bloqueo del ganglio estrellado y la aplicación local de
fentolamina impiden la respuesta vasoconstrictora nasal durante el
ejercicio.44
A diferencia de la broncoconstricción que ocurre tras el esfuerzo,
mucho mayor al respirar por la boca a consecuencia de la falta de
acondicionamiento del aire inspirado, la dilatación nasal ocurre
independientemente de respirar por la boca o la nariz.50
Capítulo 3. Interacciones nariz-bronquio

Tesis Doctoral I. Parte Teórica
37
Capítulo 3. Interacción nariz-bronquio
1. Hipótesis de interacción
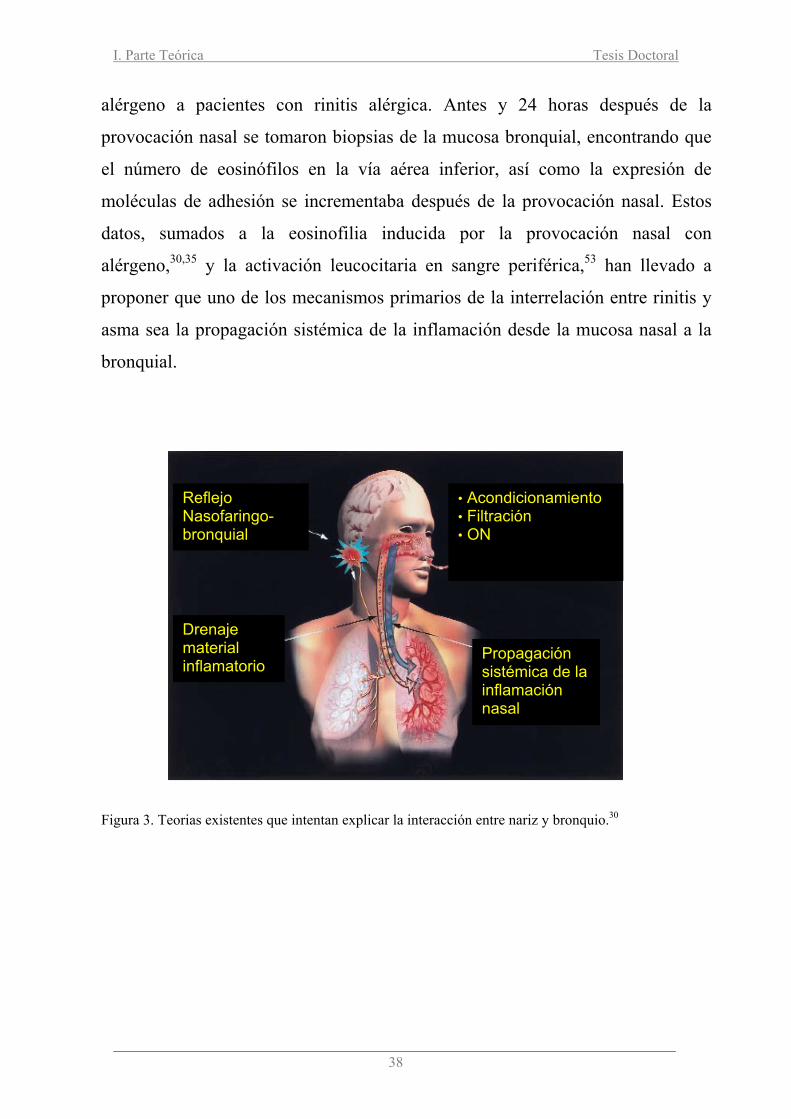
Se han propuesto varios mecanismos para explicar la interelacción entre
la nariz y los bronquios y se describen a continuación (Figura 3):
1. Reflejo nasobronquial. No existe una evidencia firme de que exista un
aumento en la expresión de este reflejo en los pacientes con rinitis. Un área que
requiere investigación en el futuro es la posibilidad de que las interacciones
neurales entre la nariz y los bronquios sean las responsables de la tos crónica
relatada por muchos pacientes con síndrome respiratorio alérgico.30
2. Drenaje de mediadores inflamatorios. Esta hipótesis plantea una
aspiración de mediadores presentes en las secreciones o en el aire inspirado que
alcanzan la vía aérea inferior, especialmente durante la noche, llevando a un
deterioro de la función pulmonar, aumento de la hiperreactividad bronquial y
presencia de síntomas al despertarse30. Sin embargo, el único estudio realizado en
humanos que ha tratado de aclarar este aspecto no ha mostrado los resultados
esperados. En dicho trabajo, Bardin et al.51, inyectaron Tc99 en los senos
maxilares de pacientes con sinusitis crónica y asma moderada a grave, evaluando
la presencia de reactividad en bronquios durante 24 horas. No encontraron
indicios de material radioactivo en ningún punto de los campos pulmonares,
aunque sí lo hallaron en el tracto gastrointestinal. No obstante, se sabe que varias
sustancias inflamatorias producidas durante las reacciones alérgicas pueden
entrar en fase gaseosa o generar aerosoles que se pueden distribuir en el árbol
bronquial,52 por lo que esta hipótesis no puede ser descartada de forma
categórica.
3. Diseminación sistémica de mediadores. Probablemente la información
más relevante y más reciente con respecto a los mecanismos de interacción entre
la vía aérea superior e inferior se ha derivado de uno de los trabajos realizados
por Braunstahl et al.37. Estos investigadores realizaron provocaciones nasales con
I. Parte Teórica Tesis Doctoral
38
alérgeno a pacientes con rinitis alérgica. Antes y 24 horas después de la
provocación nasal se tomaron biopsias de la mucosa bronquial, encontrando que
el número de eosinófilos en la vía aérea inferior, así como la expresión de
moléculas de adhesión se incrementaba después de la provocación nasal. Estos
datos, sumados a la eosinofilia inducida por la provocación nasal con
alérgeno,30,35 y la activación leucocitaria en sangre periférica,53 han llevado a
proponer que uno de los mecanismos primarios de la interrelación entre rinitis y
asma sea la propagación sistémica de la inflamación desde la mucosa nasal a la
bronquial.
Figura 3. Teorias existentes que intentan explicar la interacción entre nariz y bronquio.30
Reflejo Nasofaringo-bronquial
Drenaje material inflamatorio
Propagación sistémica de la inflamación nasal
• Acondicionamiento • Filtración • ON

Tesis Doctoral I. Parte Teórica
39
Además, se ha visto que no es un fenómeno unidireccional pues tal como
se comentó previamente, Braunstahl et al.28,29 también encontraron un aumento
de los marcadores inflamatorios en la mucosa nasal al realizar provocaciones
bronquiales segmentarias con alergeno.
Finalmente, Magnusson et al.54 practicaron biopsias de duodeno a 9
pacientes con alergia al polen de abedul al final de la época estacional y
repitieron el procedimiento 6 meses más tarde, encontrando que en la primera
muestra existía un aumento significativo de eosinófilos con presencia de proteína
básica mayor, y de células positivas para la inmunoglobulina E (IgE) con
respecto a la segunda muestra, aportando una evidencia importante de la
interrelación entre células inmunológicamente activas en la vía aérea y en el
intestino.
Todo lo anterior sugiere la existencia de una cascada inflamatoria
alérgica que tendría su origen sobre una superficie mucosa, pero que tendería a
propagarse sistémicamente.30
4. Otras teórias. Existen dos teorías más que tratan de explicar la
interacción nariz-bronquio. Una sería la del óxido nítrico (ON) que actuaría de
intermediador entre la vía aérea superior e inferior; la otra que habla de las
consecuencias de una respiración bucal crónica debido a la obstrucción nasal con
el correspondiente déficit de acondicionamiento nasal.
2. Patologías con interacción nariz-bronquio
2.1 Rinitis y asma. La rinitis y el asma son enfermedades muy comunes. Su alta
prevalencia se asocia a una elevada morbilidad y un alto coste económico. El
documento de consenso ARIA3 (Allergic Rhinitis and its Impact on Asthma)
publicado en el año 2001, y su actualización del 2008,55 ha sido el resultado de un
grupo de trabajo internacional sobre la rinitis alérgica y su impacto sobre el asma,

I. Parte Teórica Tesis Doctoral
40
en el que se realizó una amplia revisión sobre la clasificación, epidemiología,
genética, desencadenantes, mecanismos fisiopatológicos, comorbilidades de la
rinitis, diagnóstico y tratamiento. Además, incorporó unas recomendaciones
basadas en las pruebas científicas, resaltando también las necesidades de
investigación sobre la rinitis no alérgica.
2.1.1 Co-existencia epidemiológica de rinitis alérgica y asma. Los
estudios epidemiológicos han demostrado que la rinitis y el asma coexisten
frecuentemente.22,56 La mayoría de pacientes con asma tienen rinitis,
presentándose ésta más frecuentemente en los pacientes con asma alérgica que en
los pacientes con asma no alérgica. Sin embargo, en muchas ocasiones, el
paciente sólo refiere los síntomas que más le preocupan y/o le son molestos, que
en la mayoría de los casos son las manifestaciones bronquiales. En este sentido,
Gaba et al,33 constataron la presencia de inflamación nasal en un grupo de
pacientes asmáticos que negaba la presencia de síntomas de rinitis. Es decir,
aunque estos pacientes se consideren libres de síntomas, casi siempre se
demuestra la presencia de una afectación nasal (Figura 4).
Figura 4. Interrelación entre asma y rinitis. La gravedad del asma está
determinada por la presencia y la gravedad de la afectación nasal.
Grave
Leve
Grave
Leve
Gravedad general del síndrome
Interacción
ASMA
RINITIS

Tesis Doctoral I. Parte Teórica
41
Por otro lado, la prevalencia de asma en pacientes con rinitis varía entre un 15 y
un 40%, destacando el hecho de que en aquellos con rinitis intermitente
(estacional) el asma se presenta en el 10 a 15% de los casos, mientras que en
aquellos con rinitis persistente grave se presenta en un 25 a 40%.57-59
2.1.2 Rinitis alérgica como factor de riesgo para el desarrollo de asma. En
varios estudios se ha demostrado que la rinitis alérgica constituye un factor de
riesgo importante para el desarrollo de asma. En los niños, su presencia se ha
asociado, independientemente, con un riesgo doble de sufrir asma a la edad de 11
años60. En los adultos, los estudios han mostrado resultados similares en
pacientes seguidos a largo plazo,61,62 resaltando el hecho de que el asma se ha
encontrado asociada tanto a la rinitis alérgica como no alérgica.
La edad de inicio de la atopia puede ser un factor muy influyente en el
desarrollo de asma y/o rinitis. En un estudio australiano,63 el desarrollo de atopia
a temprana edad (antes de los 6 años de vida) fue un importante factor predictivo
para el desarrollo de asma en la infancia tardía, mientras que la atopia adquirida
durante la vida adulta sólo se asoció de forma importante con el desarrollo de
rinitis.
a) Efecto de los corticoides nasales sobre el asma. La interrelación que
existe entre rinitis y asma también ha sido descrita en estudios que han evaluado
el efecto de los corticoides tópicos nasales sobre la vía respiratoria inferior.
Sandrini et al.64 demostraron que la administración de triamcinolona intranasal
reduce los valores de óxido nítrico exhalado en pacientes con rinitis y asma,
aunque no encontraron cambios en ningún parámetro funcional. En otros estudios
se ha demostrado una mejoría moderada de la función pulmonar y la
hiperreactividad bronquial.65,66 Se ha descrito además que un correcto tratamiento
de la rinitis con estos fármacos reduce la frecuencia de visitas a urgencias y de
ingresos hospitalarios por exacerbaciones de asma.67,68,69
b) Efecto de los antihistamínicos en el asma. Los antihistamínicos
constituyen una de las principales opciones de tratamiento para la rinitis alérgica.

I. Parte Teórica Tesis Doctoral
42
Se han estudiado los efectos antiinflamatorios en algunos de estos fármacos, que
podrían representar una ventaja adicional, especialmente en el control de la
congestión nasal. Algunos estudios previos sugieren que la loratadina y la
cetirizina podrían mejorar de un modo variable los síntomas de asma en los
pacientes con rinitis.70
También se ha publicado que el tratamiento continuo con cetirizina
podría reducir la frecuencia y la gravedad de los síntomas bronquiales.71
Recientemente se publicó un estudio comparativo que observó que la loratadina y
el montelukast fueron igualmente efectivos en reducir los síntomas de asma y el
uso de broncodilatadores en pacientes con rinitis alérgica estacional y asma.72 Por
otro lado, se ha descrito una terapia combinada (desloratadina y montelukast) en
pacientes con asma y rinitis que parece más eficaz que su uso individual. De
acuerdo con lo expuesto en la presente revisión, y teniendo en cuenta que los
antihistamínicos no son medicamentos antiasmáticos, es probable que sus
posibles efectos benéficos sobre los síntomas bronquiales sean explicados por
una mejoría de la inflamación nasal.73
c) Efecto de la inmunoterapia sobre el desarrollo de asma. La
inmunoterapia es un tratamiento efectivo en la rinitis y en el asma causadas por
diferentes alergenos cuando se aplica en dosis óptimas, ya sea de forma
subcutánea o sublingual. Su administración debe apoyarse en la sensibilización
alergénica más que en el predominio de rinitis o de asma, ya que ambas
condiciones coexisten en la mayoría de los pacientes. Su efecto inmunológico es
la restauración del equilibrio normal entre los linfocitos Th1 y Th2, siendo la
única terapia disponible con capacidad de modificar la historia natural de la
enfermedad. En este sentido, Moller et al.74 realizaron un estudio aleatorizado, a
doble ciego y controlado con placebo, con el propósito de evaluar si la
administración de inmunoterapia específica podía prevenir el desarrollo de asma
y reducir la hiperreactividad bronquial en niños con rinoconjuntivitis alérgica
estacional. Encontraron que, después de tres años, los pacientes del grupo activo

Tesis Doctoral I. Parte Teórica
43
mejoraron significativamente su hiperreactividad bronquial y tuvieron una
incidencia de asma significativamente menor. Las anteriores observaciones
sugieren que el manejo del paciente alérgico debe hacerse de forma integral, y de
acuerdo con la gravedad general del síndrome.75
d) Efecto de los anitileucotrienos en la rinitis y el asma. Los
antileucotrienos también son un tratamiento efectivo en la asociación de rinitis y
asma. En un estudio en el que se evaluó montelukast como tratamiento para la
rinitis alérgica en pacientes sintomáticos con asma activo durante la estación
polinica, se concluyó que Montelukast es efectivo, ya que mejoró
significativamente los síntomas de la rinitis alérgica estacional y del asma.76 A su
vez, en otro estudio se objetivó que montelukast tiene efecto protector, tanto en la
via aérea superior como en la inferior, ante una provocación con alergeno.77
2.2 Poliposis nasal y asma. Algunos estudios sugieren que el asma es más
prevalente y grave en aquellos con afectación nasosinusal extensa.78 Bresciani et
al.79 evaluaron la presencia de rinosinusitis en pacientes con asma leve a
moderada comparada con asmáticos graves dependientes de corticoides. La
proporción de pacientes con síntomatología nasal fue similar en ambos grupos,
mientras que las anormalidades tomográficas nasosinusales estuvieron presentes
en el 100% de los pacientes con asma grave, y en el 88% de aquellos con asma
leve a moderada. Las escalas de puntuación clínica y tomográfica también fueron
más altas en aquellos con asma grave.
Otro aspecto importante relacionado con la afectación nasosinusal y por
ende con la gravedad del asma es la presencia de intolerancia a los AINEs, la cual
se manifiesta en un 10% de los pacientes asmáticos,80 pero puede afectar hasta
más de un 90% de los enfermos que presenten rinosinusitis crónica con pólipos
nasales.79 Estos últimos pacientes padecen un síndrome denominado tríada de
Vidal o tríada-ASA y generalmente se trata de individuos con asma de muy difícil
control.
I. Parte Teórica Tesis Doctoral
44
2.2.1 Efecto de los corticoides nasales en el asma. El interés por el vínculo
asma-sinusitis comenzó hacia 1978 cuando Rachelefsky et al. describieron en un
estudio que el 53% de los niños asmáticos mostraban opacificación de los senos
maxilares en sus radiografías.81 Desde entonces numerosos autores han
investigado el efecto del tratamiento médico de la rinosinusitis en el asma.
Businco et al.82 realizaron un estudio con 80 niños asmáticos, 55 con ocupación
maxilar en radiografías de senos y 25 con radiografías normales. Los pacientes
fueron tratados durante 30 días con corticoides tópicos nasales más un
antihistamínico-descongestionante, o con ampicilina más antihistamínico-
descongestionante, disminuyendo la gravedad del asma y mejorando los
hallazgos radiográficos después de tratamiento.
Posteriormente, Rachelefsky et al.83 observaron 48 niños asmáticos, cuya
hiperreactividad bronquial (HRB) mejoró significativamente después del
tratamiento de su rinosinusitis (diagnosticada por historia clínica y radiografía de
senos). El tratamiento consistió en antibióticos orales de 2 a 5 semanas; 18 de los
pacientes estaban recibiendo o habían recibido corticoides orales y en 9 niños se
realizaron lavado nasales. De los 48 sujetos, 38 (79%) fueron capaces de
interrumpir el uso de broncodilatadores con la resolución de su rinosinusitis. El
seguimiento posterior de estos pacientes demostró que cuando la rinosinusitis
recurría, también lo hacía el asma; este hallazgo fue corroborado en dos estudios
posteriores que reportaron un empeoramiento del asma en niños después de un
episodio de rinosinusitis.84,85
Oliviera et al.86 evaluaron 46 niños atópicos y 20 controles normales. De
los niños con rinitis 28 eran asmáticos (15 con opacificación total de senos
maxilares), tratados con 21 días de trimetoprim-sulfametoxazol, antihistamínicos,
descongestionantes, lavados nasales y 5 días de prednisona oral. Las pruebas de
provocación con metacolina y las mediciones de volumen espiratorio forzado en
el primer segundo (VEMS) mejoraron sólo en 8 de los niños en los que las

Tesis Doctoral I. Parte Teórica
45
evidencias radiológicas de rinosinusitis se habían resuelto al momento de
finalizar el tratamiento.
En todos estos estudios se utilizaron terapias múltiples o combinadas con
diferentes tipos de medicamentos sistémicos, de manera que no sabemos con
certeza cuál es el medicamento que actúa sobre el asma o si el tratamiento actúa
directamente sobre las vías respiratorias inferiores, en vez de ejercer un efecto
secundario a través de la disminución de la inflamación nasosinusal. Además
estos estudios utilizaron los hallazgos radiológicos para el diagnóstico y la
valoración de los resultados en la rinosinusitis, pero posteriormente se ha
observado que la opacificación radiológica de senos no se correlaciona con la
gravedad de los síntomas nasales y es de uso limitado para demostrar el efecto de
los corticoides en la PN, ningún estudio utilizó la endoscopia nasal ni especificó
si la RSC se acompañaba o no de PN.
Benitez et al.87 comprobaron en un estudio prospectivo, aleatorizado y
controlado que un curso corto de prednisona oral seguido de budesonida
intranasal mantenida es un tratamiento efectivo en la poliposis nasal grave. A
pesar de que este tratamiento particular ha sido utilizado ampliamente a través de
los años por muchos rinólogos, ningún estudio ha investigado su efecto sobre las
vías respiratorias inferiores.
Hasta la fecha no existen estudios clínicos bien conducidos que estudien
los efectos del tratamiento médico de la PN sobre el asma bronquial.
2.2.2 Efecto de la cirugía endoscópica nasosinusal (CENS) en el asma.
Voltolini, en 1871, fue el primero en reportar la mejoría del asma después de una
polipectomía nasal.88 Posteriormente muchos autores intentaron rebatir o
corroborar su hipótesis.
La cirugía podía tener un efecto negativo sobre el asma en un pequeño
subgrupo de pacientes con PN cuyas características no habían podido ser
determinadas. Hace muchos años algunos autores objetivaron un empeoramiento
I. Parte Teórica Tesis Doctoral
46
subjetivo del 18 al 40%, o precipitación de la primera crisis asmática después de
la cirugía tradicional,89,90 sin embargo, desde su introducción en la medicina por
Stammberger en 1984, las técnicas funcionales de la CENS han sido ampliamente
aceptadas y aplicadas a enfermedades inflamatorias de los senos paranasales.
Nishioka et al.91 estudiaron el efecto de la CENS en 20 pacientes con
RSC y asma, de los cuales 25% habían sido hospitalizados para el tratamiento del
asma en los 12 meses previos a la cirugía. Un 85% de los pacientes reportaron, en
un cuestionario subjetivo, mejoría de su asma después de la CENS; 7 pacientes
(53,8%) fueron capaces de interrumpir algunos de sus medicamentos sistémicos
para el asma. Los 18 pacientes (90%) que habían acudido al servicio de urgencias
en el año previo a la CENS redujeron el número de estas visitas y de las
hospitalizaciones. Manning et al. estudiaron 14 pacientes pediátricos con
rinosinusitis y asma grave que requerían corticoides orales como mínimo de
forma intermitente, en los cuales el tratamiento médico de su rinosinusitis había
fracasado. Todos se sometieron a etmoidectomía total y meatotomía media. De
los 14 pacientes, 11 tenían una reducción significativa en las hospitalizaciones
por asma, 12 tenían una reducción significativa en las necesidades de
glucocorticoides (la disminución total no se cuantificó), y 11 mejoría en la
puntuación subjetiva del asma comparando 12 meses pre y postoperatorios. Sin
embargo, no se observó una diferencia significativa en los resultados de las
pruebas de función pulmonar.92 Dinis y Gomez93 encontraron resultados similares
al comparar 43 pacientes asmáticos con RSC refractaria al tratamiento médico,
seleccionados para CENS, con un grupo control de 93 pacientes no asmáticos
sometidos a CENS, antes y 12 meses después de la cirugía. Desarrollaron un
sistema de clasificación sinusal por grados (de 0 a 4) utilizando hallazgos
endoscópicos y radiológicos por la tomografía computarizada (TC). Se encontró
una PN difusa (enfermedad grado 4) en cerca del 30% de los pacientes. También
se empleó una escala de clasificación de la gravedad del asma, en base a las
necesidades terapéuticas y teniendo en cuenta las tendencias predominantes en el

Tesis Doctoral I. Parte Teórica
47
tratamiento del asma. Esto permitió la descripción de la enfermedad en cuatro
grados dependientes de corticoides sistémicos (I, leve, al grado IV). También se
les preguntó a los pacientes cuántas visitas al servicio de urgencias se produjeron
debido al asma en los últimos 12 meses, y si los síntomas nasales
desencadenaban las crisis asmáticas. Se realizaron pruebas de función pulmonar
pre y postoperatoriamente en 27 pacientes. El número de pacientes que
requirieron más de 6 visitas se redujo de 23,3% al 4,7% y el número de pacientes
que referían que los síntomas nasales desencadenaban las crisis de asma
descendió del 83,7% antes de la cirugía a 46,5% después de la cirugía. En la
evaluación subjetiva de los efectos de la cirugía sobre la gravedad del asma, el
81,4% de los sujetos refirieron algún beneficio, desde leve (30,2%) a marcado
(51,2%), mientras que un 18,7% negó cualquier tipo de beneficio. No se
detectaron diferencias en la función pulmonar pre y postoperatoria, posiblemente,
por el hecho de que el 74% de los sujetos tenían VEMS normales antes de la
cirugía. En un estudio similar Goldstein et al.94 analizaron retrospectivamente los
registros médicos de 13 pacientes que tenían RSC resistente a la medicación (9
con PN) y asma bronquial, y que fueron sometidos a CENS por primera vez. Las
comparaciones de las medias grupales antes y después de la CENS revelaron que
no hubo cambios estadísticamente significativos en las puntuaciones de las
escalas de los síntomas pulmonares, en el uso de medicación para el asma, en las
pruebas de función pulmonar, y en el número de visitas al departamento de
urgencias o ingresos hospitalarios. Ninguno de los dos estudios evaluó los
cambios de dosis de esteroides individualmente.
McFadden et al.95 revisaron retrospectivamente 80 pacientes con RSC
que habían sido sometidos a cirugía de senos mediante la técnica de Caldwell-
Luc, de los cuales 25 pacientes tenían asma dependiente de corticoides y otros 40
requerían uso intermitente de corticoides orales para controlar su asma. Se
observó que 68 pacientes (85%) tuvieron una mejoría significativa de síntomas
nasales y 67 pacientes (83%) refirieron alivio de sus síntomas asmáticos con

I. Parte Teórica Tesis Doctoral
48
disminución del número y/o la dosis necesaria de medicamentos para controlar su
enfermedad. Sólo 9 pacientes seguían siendo dependientes de corticoides, sin
embargo, requerían menor dosis para controlar sus síntomas. En un estudio
retrospectivo de 79 pacientes (73% con PN), con asma y sinusitis refractaria al
tratamiento médico, en los que se realizó CENS, Park et al.96 encontraron que el
80% de los pacientes que se quejaban de que la rinosinusitis empeoraba el asma,
tuvieron mejoría después de la CENS. Se redujeron significativamente el número
de hospitalizaciones, visitas a urgencias, y el uso de corticoides.
Debido a las controversias creadas por los estudios previos, en 1999 se
intensificaron los esfuerzos por encontrar una relación causa-efecto definitiva.
Ikeda et al.97 estudiaron 21 pacientes después de CENS e hicieron comparaciones
de los 6 meses previos y 6 meses posteriores a la cirugía, obteniendo mejoría
significativa en los síntomas nasales y el flujo espiratorio máximo (FEM) en el
grupo de CENS. En un intento por disminuir los efectos de la variación
estacional, se midieron los valores del FEM, que mostraron mejoría un mes antes
y un mes después de la cirugía. Sin embargo, no hubo cambios significativos en
el uso de prednisona en esta serie.
Dunlop et al.98 evaluaron retrospectivamente la eficacia de la CENS sobre
el asma, usando un cuestionario en 50 pacientes adultos con RSC, 34 de ellos con
PN. Un total de 20 pacientes (40%) refirieron mejoría postoperatoria del control
del asma, 20% requirió menos esteroides inhalados, mientras que el 28% necesitó
menos broncodilatadores. También se observó una reducción estadísticamente
significativa en el uso de corticoides orales y el número de ingresos hospitalarios
por asma. Se tomaron mediciones de la FEM en 23 pacientes, 7 de los cuales
evidenciaron niveles más altos. Aunque el efecto del asma en la vida cotidiana
parece ser más grave en el subgrupo con PN, no se observaron diferencias en los
resultados de la CENS sobre el asma entre los grupos de RSC con y sin PN.
Senior et al.99 llevaron a cabo un seguimiento a largo plazo (media de 6,5
años) de 120 pacientes con RSC y asma que se sometieron a CENS. Mediante un
Tesis Doctoral I. Parte Teórica
49
cuestionario los pacientes, proporcionaron información subjetiva en relación a la
mejoría del asma y, si procedía, el grado de mejoría, junto con los cambios en la
medicación antes y después de la intervención. A los 1,1 años después de la
cirugía el 78% de los pacientes informaron de una mejoría del 49% en el asma
respecto a antes de la cirugía. A los 6,5 años después de la cirugía el 90% mostró
mejoría en el asma y el 74,1% de los pacientes disminuyeron las crisis de asma.
De los 20 pacientes que refirieron uso crónico de corticoides orales antes de la
cirugía, 13 (65%) informaron disminución de la necesidad de corticoides. Para 26
de los pacientes que usaban corticoides inhalados antes de la cirugía, 12 (46%)
reportaron disminución de uso. Los autores concluyen que una combinación de
CENS, unos correctos cuidados postoperatorios, y un tratamiento médico
adecuado de la enfermedad sinonasal puede tener un impacto positivo en la
enfermedad de las vías respiratorias inferiores a largo plazo.
Palmer et al.100 estudiaron la necesidad de medicación para controlar el
asma tras CENS. Se seleccionó a 15 pacientes que requerían corticoides
inhalados y como mínimo prednisona oral intermitente para el control del asma.
Compararon el número de días y el total de dosis de prednisona como medidas
objetivas de control del asma un año antes y un año después de la cirugía. La
media grupal para los días de ingesta de prednisona preoperatoria fue de 84,
mientras que tras la cirugía fue de 63, lo que refleja una disminución
estadísticamente significativa del 25% (p<0,0001). La media grupal para el total
de dosis de prednisona preoperatoria en el año fue de 3094, mientras que tras la
cirugía fue de 1780, mostrando una disminución estadísticamente significativa
del 50% (p <0,03). Tanto la dosis total como el número de días de uso de
corticoides disminuyeron en el año postoperatorio en este grupo de pacientes. El
uso de antibióticos fue también comparado y expresado en semanas de uso.
Preoperatoriamente, los pacientes utilizaron antibióticos un promedio de nueve
semanas, mientras que en el año después de la CENS, los pacientes sólo los

I. Parte Teórica Tesis Doctoral
50
tomaron un promedio de siete semanas, disminución que fue estadísticamente
significativa (p<0,045).
Uri et al.101 examinaron a 34 pacientes asmáticos con PN masiva en los
que se realizó CENS, y realizaron seguimiento a 13 pacientes en la clínica de
asma. Se presentó a los pacientes un cuestionario sobre evaluación subjetiva de
asma y estado nasosinusal y se realizaron evaluaciones objetivas incluyendo
endoscopia nasal y espirometría. Se pudo documentar una disminución
estadísticamente significativa en el uso de prednisona y broncodilatadores, sin
embargo, nuevamente no se observó diferencia en la condición asmática pre y
postoperatoria. Siete pacientes tuvieron una mínima mejoría y seis observaron un
empeoramiento de su asma.
Más recientemente, Dejima et al.102 realizaron un análisis prospectivo de
28 pacientes con asma bronquial (22 con PN) que se sometieron a CENS. Como
grupo control, se utilizaron 57 pacientes con rinosinusitis crónica, pero sin asma.
Los pacientes fueron observados por un período medio de 37,4 meses. En el
análisis se evaluó la mejoría postoperatoria de los síntomas asmáticos, el FEM y
el uso de medicamentos, utilizando los criterios de la Food and Drug
Administration (FDA). Se observó una mejoría subjetiva del asma bronquial y
aumento del FEM en 21 pacientes (75%). El promedio de uso de la medicación
para el asma, según la puntuación de la escala de la FDA, disminuyó
significativamente de 2,3 a 1,8 después de la CENS. En el grupo en el que la
sintomatología nasal había mejorado tras CENS se observó mejoría significativa
en el asma, sin embargo, no fueron significativas en el grupo sin mejoría de los
síntomas nasales tras CENS. La valoración subjetiva del asma después de la
CENS mostró que 15 pacientes (88%) se encontraban satisfechos en el grupo de
mejoría nasal tras CENS y 6 (60%) se mostraron satisfechos en el grupo de no
mejoría nasal tras CENS.
Tesis Doctoral I. Parte Teórica
51
Existen pocas publicaciones donde se evalúe la tolerancia
(ATA)/intolerancia a la aspirina (AIA) cuando se estudia sobre el efecto de la
cirugía de la PN sobre el asma. Nakamura et al.103 evaluaron retrospectivamente
el componente asmático de 22 pacientes con AIA un año después de CENS y
cirugía sinusal tradicional. Se encontró que el 90,9% de los pacientes presentaban
una mejoría subjetiva y que las pruebas de función pulmonar mejoraron
significativamente. La aplicación clínica de este estudio es limitada debido a que
el estudio combinó abordajes quirúrgicos diferentes como el de Caldwell-Luc y
la CENS, además no se incluyó un grupo de comparación y el seguimiento se
limitó a un año.
Otro estudio muestra que los pacientes con AIA no se benefician de la
CENS en la misma medida que otros pacientes asmáticos con RSC. Batra y
cols.104 estudiaron 17 pacientes con PN y asma corticodependiente, 9 de ellos con
AIA y 8 con ATA. Si bien en los pacientes con ATA el VEMS mejoró de 81% a
86% (p<0,047) y en los pacientes con AIA el VEMS pasó de 85% a 92%
(p>0,08), la diferencia no fue estadísticamente significativa. En cuanto al uso de
corticoides no hubo cambios en ninguno de los dos grupos. Loehrl et al.105
llevaron a cabo un seguimiento retrospectivo medio de 10 años en 34 pacientes
con tríada ASA que fueron sometidos a CENS, de los cuales, 29% notaron
mejoría subjetiva del asma en el primer año postcirugía, y de éstos, 68%
reportaron mejoría persistente después del primer año de seguimiento. El número
de visitas al servicio de urgencias, ingresos hospitalarios y crisis asmáticas
disminuyeron significativamente en los últimos 12 meses de seguimiento.
Además los valores de FEM mejoraron en una media de 60% del valor predictivo
preoperatoriamente a 86% en la última visita de seguimiento.
Recientemente, Awad et al.106 realizaron una revisión retrospectiva de 91
pacientes asmáticos (41 con AIA y 50 con ATA) con RSC médicamente
refractaria, que fueron evaluados inmediatamente antes de la cirugía y a los 6 y
12 meses de la misma. Dentro del grupo de pacientes con AIA habían más
I. Parte Teórica Tesis Doctoral
52
sujetos con PN que en el grupo de los con ATA (41 y 25 respectivamente). La
gravedad del asma, valorada según los criterios de la guía NIH (National Institute
of Health), mejoró en ambos grupos de pacientes después de la CENS. La
diferencia entre la mejoría de los dos grupos a los 6 meses no fue
estadísticamente significativa, sin embargo, a los 12 meses, la mejoría fue
mantenida en 58,5% de los pacientes con AIA y sólo en 30.0% de los pacientes
con ATA (p<0.01). Con respecto al VEMS, no hubo diferencias estadísticamente
significativas en ninguno de los dos grupos. Hubo una disminución
estadísticamente significativa en el uso de corticoides inhalados en ambos
grupos, con una mejoría predominante en el grupo con ATA sobre el grupo con
AIA (34,1% versus 16% a los 6 meses, y 34,1% versus 8% a los 12 meses
respectivamente). Ambos grupos disminuyeron significativamente el uso de
esteroides orales y el número de visitas al servicio de urgencias, sin producirse
diferencias estadísticamente significativas entre ambos grupos.
Todos los estudios coinciden en que hay una mejoría subjetiva del asma
tras la cirugía y esta parece ser mayor en los pacientes con ATA. En las pruebas
de función pulmonar hay inconsistencias, pero hay que tener en cuenta que se
trata de estudios retrospectivos, con todas las limitaciones que ello implica, por lo
que es difícil llegar a una conclusión al respecto.
Actualmente no existen estudios que evalúen como la influencia de la
tolerancia a la aspirina sobre el efecto del tratamiento médico de la PN sobre el
asma.
2.2.3 Estudios Comparativos. En la literatura tan sólo existen dos estudios que
comparan los efectos del tratamiento médico y quirúrgico de la PN en el asma
bronquial.
Lamblin et al.107 dividieron los pacientes con PN en dos grupos
diferentes, basados en su capacidad de respuesta a la beclometasona intranasal.
Encontraron que en los respondedores a corticoides (18 pacientes que
Tesis Doctoral I. Parte Teórica
53
disminuyeron 4 de 15 síntomas nasales después de 6 semanas de tratamiento con
corticoides tópicos), la prueba de provocación con metacolina y el VEMS, así
como los síntomas pulmonares y la gravedad del asma, se mantuvieron sin
cambios durante un período de 4 años. En los 28 pacientes no respondedores a
corticoides, que fueron sometidos a etmoidectomía intranasal, se observó un
descenso estadísticamente significativo del VEMS, manteniéndose estables los
síntomas pulmonares y la gravedad del asma en el seguimiento durante 4 años.
La aplicación clínica de este estudio es limitada, debido a que es un estudio con
una muestra no aleatoria que, además, no incluye un grupo control sin PN para
comparación.
Recientemente, Ragab et al.108 estudiaron una muestra de 43 pacientes
asmáticos con RSC dividida aleatoriamente en dos grupos: 23 pacientes
sometidos a CENS y 20 pacientes que recibieron sólo tratamiento médico
(lavados nasales con solución alcalina, corticoides intranasales y 12 semanas de
eritromicina oral). Sólo se observó una clara mejoría subjetiva del asma en el
grupo tratado médicamente. En el grupo de CENS no se observaron diferencias
significativas; un paciente sin PN desarrolló nuevos síntomas asmáticos después
de la cirugía, mientras que otro paciente con PN el asma estaba “peor que nunca”
después de la CENS. Sin embargo, el único paciente en el grupo de CENS que
refirió mejoría importante de su asma no tenía PN. Se observó una disminución
significativa de los requerimientos de broncodilatadores inhalados, corticoides
sistémicos y número de hospitalizaciones necesarias para el control del asma en
ambos grupos sin diferencias significativas entre los pacientes con y sin PN. Los
niveles de óxido nítrico exhalado (parámetro de inflamación de vías aéreas
inferiores que se ha correlacionado con las exacerbaciones del asma y el número
de eosinófilos en secreciones bronquiales) y el VEMS mejoraron
significativamente en ambos grupos con un predominio en el grupo de
tratamiento médico y aún más en el subgrupo de pacientes con PN. Los autores
concluyen que tanto el tratamiento médico como el quirúrgico de la RSC mejora
I. Parte Teórica Tesis Doctoral
54
el curso clínico del asma, siendo el tratamiento médico superior al quirúrgico en
la RSC con PN. Una vez más, podría deberse a un efecto directo del tratamiento
sistémico sobre las vías respiratorias inferiores, pues los macrólidos han probado
tener un efecto benéfico directo sobre el asma, a través de sus propiedades
antibacterianas, antiinflamatorias, mucolíticas, así como la disminución del
aclaramiento bronquial de glucocorticoides.
En resumen, los datos anteriores sugieren que la afectación de la nariz
(rinitis alérgica, rinosinusitis crónica y/o poliposis nasal) se relaciona
directamente con la aparición y la gravedad del asma.
2.3 Rinosinusitis crónica y EPOC. Existe poca información publicada al
respecto, existe un aumento de los síntomas nasales en los pacientes con EPOC y
estos provocan un empeoramiento de la calidad de vida de los pacientes.109
También se ha observado un aumento de la inflamación nasal en los pacientes
con EPOC.110
Capítulo 4. Rinosinusitis crónica sin pólipos

Tesis Doctoral I. Parte Teórica
57
1. Definición de rinosinusitis crónica
La rinosinusitis crónica (RSC), incluyendo la poliposis nasal, se
define como aquella inflamación nasosinusal que dura más de 12 semanas
y se caracteriza por la presencia de 2 ó más síntomas nasales, en que al
menos uno de ellos ha de ser congestión / obstrucción / bloqueo nasal o
rinorrea anterior y/o posterior; además de dolor o presión facial y pérdida
total o parcial del olfato.111
La RSC con o sin pólipos nasales se considera aún como una
única entidad debido a la dificultad en diferenciarlas claramente. La razón
por la que unos pacientes desarrollan pólipos permanece desconocida, por
lo que la RSC con pólipos se considera un subgrupo de las RSC (Figura 5).
Figura 5. La poliposis nasal se considera un subgrupo dentro de la rinosinusitis crónica, por lo
tanto existen pacientes con rinosinusitis crónica sin pólipos y otros con pólipos nasales.
El diagnóstico clínico de la RSC se basa en la historia clínica
(síntomas), la exploración endoscópica nasal y el diagnóstico por la imagen
(tomografía computerizada). Debe realizarse siempre un cuestionario para
determinar la posible presencia de alergia. La exploración de las fosas
nasales debe realizarse idealmente mediante endoscopia nasal. La prueba
PPóólliippooss nnaassaalleess
RRSSCC
I. Parte Teórica Tesis Doctoral
58
de imagen más fidedigna para la patología nasosinusal es la tomografía
computerizada que revela los cambios de la mucosa en el complejo
ostiomeatal e identifica la extensión de la enfermedad en los diferentes
senos paranasales. Además, es de indicación obligatoria para la cirugía. En
la poliposis nasal la pérdida del olfato aparece precozmente, muchas veces
incluso antes de que los pólipos sean visibles en las fosas nasales.112
Siempre debe realizarse una evaluación del sentido del olfato ya sea
mediante anamnesis o olfatometría subjetiva (UPSIT, BAST-24). La RSC
se divide según criterios de gravedad en leve, moderada y grave siguiendo
la escala visual analógica (EVA: 0-3 leve, >3-7 moderada, >7-10 grave)
2. Rinosinusitis crónica sin pólipos
2.1 Epidemiología y comorbilidades. La falta de información
epidemiológica, tanto en RSC con pólipos como sin pólipos, contrasta con
la abundante información en microbiología, diagnóstico y tratamiento. En
una encuesta de la prevalencia de RSC, definida como tener “problemas en
los senos” durante más de 3 meses en el año previo a la entrevista, cifró en
un 15,5% la prevalencia de RSC en EEUU.113 Posiblemente el diagnóstico
de RSC está sobredimensionado, ya que habitualmente es sólo clínico,
dejando aparte las alteraciones del olfato; y falta su corroboración con la
endoscopia nasal y la TC nasosinusal. Además, los médicos de atención
primaria carecen del entrenamiento y del equipamiento para realizar una
endoscopia nasal.
Los factores asociados a una RSC sin pólipos son:
2.1.1 Alteraciones ciliares. La función ciliar juega un importante
papel en la limpieza de los senos y la prevención de la inflamación crónica
nasosinusal. En condiciones normales cada célula ciliada consta de 200-
Tesis Doctoral I. Parte Teórica
59
300 cilios que baten con una frecuencia de 500 ciclos por minuto. La
discinesia ciliar primaria predispone a infecciones respiratorias como la
RSC.114 En pacientes con RSC existe además una discinesia ciliar
secundaria. En los pacientes con fibrosis quística la imposibilidad de
transporte del moco viscoso causa alteraciones en la función ciliar y por lo
tanto también RSC. La prevalencia de poliposis nasal en la FQ varía según
la edad, siendo un 10% en niños, llegando hasta un 40% en adultos.115
2.1.2 Alergia. Existen estudios que correlacionan la inflamación de
tipo alérgico con el desarrollo de RSC,116 y en los que los marcadores de
atopia son más prevalentes. El 54% de los pacientes con RSC presentan un
prick test positivo.117 Entre los pacientes operados por RSC se observa una
prevalencia de prick test positivo de un 50% al 84%, de los que un 60%
presenta múltiples sensibilizaciones.
2.1.3 Asma. La RSC y el asma tienen una gran interrelación, más
ampliamente estudiada en los pacientes RSC con PN. Los estudios
radiológicos nasosinusales en pacientes asmáticos demuestran una alta
prevalencia de sinusopatía crónica. Todos los pacientes que requieren
tratamiento corticoideo oral para control de su asma presentan ocupación
sinusal en la TC de senos.79,118,119
2.1.4 Inmunodeficiencias. En estudios realizados en pacientes con
RSC refractarias al tratamiento médico se encontraron una elevada
incidencia de alteraciones inmunes. De 60 pacientes con pruebas in vitro de
funcionalidad de sus linfocitos T, el 55% presentan una proliferación
anormal en respuesta a antígenos. Se encontraron niveles bajos de IgG, A y
M en el 18%, 17% y el 5% respectivamente. Inmunodeficiencia común
variable se observa en un 10% y la deficiencia selectiva de IgA en un 6%
de los pacientes.120
Más de un 50% de los pacientes con infección por VIH121 presentan
RSC, siendo ésta una de las enfermedades más persistentes en estos
I. Parte Teórica Tesis Doctoral
60
pacientes. En un estudio más detallado la cifra de RSC en pacientes con
VIH es más baja (34%), pero con una buena correlación entre el número de
células CD4+ y la probabilidad de tener una RSC. También cabe
mencionar que microorganismos atípicos como el Aspergillus spp, la
Pseudomona aeruginosa y la microsporidiasis se pueden aislar de los senos
afectados y neoplasias como el linfoma no Hodgkin y el sarcoma de Kaposi
pudiendo simular síntomas de RSC.122
2.1.5 Factores genéticos. A pesar de que existen casos de RSC en
miembros de una misma familia, no se han encontrado, generalmente
alteraciones genéticas que se relacionen con la RSC.123 El papel de los
factores genéticos en la RSC se ha implicado en los pacientes con fibrosis
quística y con discinesia ciliar primaria.115
2.1.6 Embarazo y transtornos endocrinos. El 20-30% de las
embarazadas sufren de obstrucción nasal, estornudos y rinorrea, sobre todo
a partir del primer trimestre.124 Se cree que esta condición es causada por
los cambios en los niveles hormonales durante el embarazo, si bien aún no
se ha podido determinar la causa exacta de la rinitis del embarazo, que
puede abocar en una rinosinusitis. Sobol et al.125 demuestran que el 61% de
las embarazadas tienen congestión nasal durante el primer trimestre
mientras que sólo el 3% desarrollan sinusitis.Además, existe una relación
entre el hipotiroidismo y la RSC aunque con estudios muy limitados.126
2.1.7 Factores locales. Se ha sugerido que ciertas variaciones
anatómicas (concha bullosa, dismorfia septal, unciforme desplazada)
pueden ser precursoras de una RSC.127 Los estudios que han defendido este
supuesto han identificado una hipertrofia de la mucosa intrasinusal en la
TC. En contra de este supuesto hay que aclarar que un 30% de la población
general presenta una hipertrofia de la mucosa sin presentar síntomas.
Además, no se ha aclarado como una variación anatómica en particular
puede alterar el drenaje del complejo ostiomeatal per se. Muchos estudios

Tesis Doctoral I. Parte Teórica
61
muestran que la prevalencia de anomalias anatómicas no es más común en
los pacientes con RSC que en los controles.128
2.1.8 Microorganismos
a) Bacterias. El papel de las bacterias en la patogenia de la RSC no
está suficientemente aclarado. Ningún estudio ha probado que la RSC
provenga de una rinosinusitis aguda. Se han cultivado similares patógenos
aerobios y anaerobios en pacientes con RSC, tanto de los senos ocupados
como de los sanos. En personas sanas los Staphylococcus coagulasa-
negativos (56%), Staphylococcus aureus (39%) y Streptococus pneumoniae
(9%) son los gérmenes más frecuentes. Los cultivos de meato medio y de
seno maxilar coinciden en un 80% de los pacientes. En pacientes con RSC,
Arouja et al.129 aisló aerobios en meato medio, en el 86% y anaerobios en el
8%. Staphylococcus aureus (36%), Staphylococcus coagulasa-negativos
(20%), y Streptococus pneumoniae (17%). Algunos autores sugieren que
la cronicidad desarrolla un reemplazamiento y aumento gradual de
gérmenes anaerobios. Los gérmenes anaerobios sólo son más frecuentes en
las infecciones secundarias a problemas odontógenos.130
b) Hongos. Generalmente los hongos se encuentran a nivel sinusal
de manera asintomática131. Las formas sintomáticas van desde formas no
invasivas como la bola fúngica a formas invasivas como una sinusitis
fúngica aguda en la que la vida del paciente corre un gran riesgo.132 Como
ocurre con las bacterias la presencia de hongos a nivel nasosinusal no
prueba que su presencia origine o perpetue una RSC. De hecho el
tratamiento con antimicóticos tópicos y sistémicos no mejora los síntomas
en dichos pacientes.133
2.1.9 Otros factores. Existen dudas sobre el aumento de RSC entre
los pacientes fumadores. En un estudio en Canada134 se vió asociado, pero
ésto no se confirmó con otro realizado en Corea.135 El bajo salario está
asociado a una mayor prevalencia de RSC. No existen trabajos sobre el
I. Parte Teórica Tesis Doctoral
62
papel etiológico de la polución y tóxicos como sería el ozono.134 En el 11-
33% de pacientes con RSC se ha encontrado ADN intrasinusal de
Helicobacter pylori comparado con un 0% en los controles,136 lo cual
tampoco prueba que sea un agente causante.
2.2 Histopatología de la RSC sin pólipos. En la RSC sin pólipos hay
una inflamación difusa de la mucosa de las fosas nasales y senos paranasales
con una gran cantidad de células inflamatorias, predominantemente
neutrófilos (como en la RSA) junto a eosinófilos, mastocitos y basófilos.
La mucosa nasal se caracteriza por una membrana basal engrosada,
hiperplasia de células caliciformes, edema subepitelial e infiltrado
mononuclear.
2.2.1 Células inflamatorias.
a) Linfocitos. Los linfocitos T CD4+ están presentes en la
patofisiología de la RSC, siendo predominantes en el inicio y regulación de
la inflamación.137
b) Eosinófilos. La infiltración de la mucosa por eosinófilos en la
RSC es un marcador de inflamación,138 que también muestra relación con
la gravedad139 y el pronóstico,140 La RSC sin pólipos presenta niveles
menores de marcadores eosinofílicos (eosinófilos, eotaxina, proteina
catiónica eosinófila) que los pacientes con poliposis nasal.141,142 Estos
hallazgos pueden sugerir que la RSC con o sin pólipos sean diferentes
entidades, aunque también se podrían interpretar como diferentes grados de
la misma.
c) Macrófagos. La RSC, con o sin pólipos, presenta una elevada
infiltración por macrófagos.142 El receptor de manosa macrofágico (RMM),
que se encarga de los procesos fagocíticos y de la transducción de la señal
para la activación de mecanismos proinflamatorios, se encuentra más

Tesis Doctoral I. Parte Teórica
63
expresado en los pacientes con RSC sin pólipos que en la poliposis nasal y
los controles.143
d) Mastocitos. Tanto los mastocitos como los eosinófilos se
encuentran involucrados en los procesos inflamatorios crónicos de la mucosa
nasal, incluyendo la RSC.144 En la RSC los mastocitos, eosinófilos y las
células IgE+ están aumentadas comparadas con los controles.145
e) Neutrófilos. El infiltrado tisular presente en la RSC está dominado
por la presencia de linfocitos y de neutrófilos.146 Los eosinófilos
predominaron en los líquidos de lavado de los meatos medios de pacientes
asmáticos, mientras que los neutrófilos lo hicieron en las citologías nasales
de pacientes con afectación patológica de las vías aéreas de pequeño
calibre. Su correlación con la función pulmonar sugiere que en la RSC
estaría implicada la vía aérea inferior.147
2.2.2 Citoquinas y mediadores. Se ha descrito que las
concentraciones de diversos mediadores y citoquinas (IL-1, IL-6, IL-8,
TNF-α, IL-3, GM-CSF, molécula de adhesión intercelular (ICAM-1),
mieloperoxidasa (MPO), y proteína catiónica eosinófila (PCE) son mayores
en el tejido afectado por una RSC que en el de los controles (en la mayoría
de los casos, en los cornetes inferiores).148-151 Curiosamente, se ha
observado que los niveles de la molécula de adhesión celular vascular
(VCAM-1), implicada en el reclutamiento selectivo de los eosinófilos, y de
la IL-5, citoquina clave para la supervivencia y actividad de los eosinófilos,
no están aumentadas.148,150 Este perfil de citoquinas y mediadores se parece
al que se observa en la rinitis vírica y en la RSA, con la excepción del
discreto, pero significativo aumento de la PCE.
a) Citoquinas. Se ha detectado la presencia de IL-8, un potente
factor quimiotáctico para los neutrófilos en los tejidos afectados por una
I. Parte Teórica Tesis Doctoral
64
RSC. En un estudio en el que se determinaron las concentraciones de
proteína de diversas citoquinas (IL-3, IL-4, IL-5, IL-8, y GM-CSF) en
homogeneizados de tejido, se observó que las cifras de IL-8 en la RSA y
las de IL-3 en la RSC eran significativamente mayores en la mucosa
sinusal que en las muestras de control procedentes del cornete inferior.148
La IL-3 podría estar implicada en la defensa local y en la reparación de la
mucosa sinusal afectada por un proceso inflamatorio crónico, ya que
estimula a diversas poblaciones celulares y participa de forma indirecta en
la fibrosis y en el engrosamiento de la mucosa.152 En pacientes con RSC, la
expresión de IL-5, IL-6, y IL-8 está aumentada en comparación con los
sujetos sanos.153 Las comunicaciones sobre la presencia de diferentes tipos
y cantidades de mediadores inflamatorios también respalda la hipótesis de
que la RSC y la PN podrían ser dos entidades patológicas distintas. Las
concentraciones de albúmina y de IL-5, pero no las de IL-8, son inferiores
en los pacientes con RSC sin PN que en los que presentan PN.154 La RSC
sin PN se caracteriza por una polarización de los linfocitos TH1 y
concentraciones elevadas de IFN-γ y TGF-β, mientras la RSC con PN lo
está por una polarización de TH2 con concentraciones elevadas de IL-5 e
IgE.142 En trabajos que intentaban identificar perfiles de marcadores
biológicos característicos de la enfermedad, se observó que las
concentraciones de IgE e IL-5 eran inferiores en la RSC que en la PN.155
Aunque no hubo diferencias en relación con IL-6, IL-8, y IL-11, los niveles
de TGF-β fueron tres veces superiores y respondieron más a la IL-4 en
pacientes con PN que cuando sólo existía afectación por RSC.156 Las
concentraciones de IL-5 y PCE fueron menores en la RSC que en la PN, y
correlacionaron directamente con las de leucotrienos peptídicos e
inversamente con las de PGE2.157
b) Quimioquinas. Su expresión es diferente en los pacientes con
RSC atópicos (aumento de las células CCR4+ y EG2+) y en los no atópicos
Tesis Doctoral I. Parte Teórica
65
(descenso de las células CCR5+), lo cual sugiere que en la rinosinusitis
atópica existe una posible asociación entre la infiltración por eosinófilos y
por linfocitos TH2.158 Otras quimioquinas, como el oncogén alfa,
relacionado con el crecimiento (GRO-alfa), y la proteína quimiotáctica-2
de los granulocitos (GCP-2), producidas principalmente por las células
glandulares y epiteliales, contribuyen a la quimiotaxis de los neutrófilos en
la RSC, mientras que la IL-8 y la ENA-78 tienen una importancia
secundaria.154
c) Moléculas de adhesión. En pacientes con RSC maxilar se registró
un mayor grado de eosinofilia y de proliferación de vasos que expresan
ligandos de la selectina L endotelial que en los sujetos de control, y estos
factores correlacionaron con la gravedad de la inflamación.159
d) Eicosanoides. Se ha observado que las concentraciones de PGE2
y del ARNm de COX-2 son mayores en los pacientes con RSC con PN que
en los pacientes con RSC sin PN, y que las de 15-lipooxigenasa y de
lipoxina A4 son mayores en todos los grupos de pacientes con RSC que en
la mucosa sana. Las cifras de sintasa de LTC4, ARNm de 5-lipoxigenasa, y
de LT peptídicos aumentan en proporción con la gravedad de la
enfermedad.157 La expresión del receptor de CisLT1 es menor en la RSC
que en la PN, mientras que la de CisLT2 está aumentada en ambos grupos
en comparación con los sujetos de control sanos.160
e) Metaloproteinasas y TGF-β. La expresión del factor de
crecimiento transformador beta-1 (TGF-β1), tanto a nivel de la proteína
como de su ARN, es significativamente mayor en la RSC sin PN que en la
RSC con PN y se asocia a la presencia de fibrosis.161 Algunos datos
también sugieren que la RSC y la PN difieren en sus características
histopatológicas. Histopatológicamente, la RSC cursa con fibrosis, y ello se
refleja en forma de un aumento de la expresión del TGF-β1 en relación con
la PN. Esto podría distinguir ambas entidades.162
I. Parte Teórica Tesis Doctoral
66
f) Inmunoglobulinas. En los pacientes con RSC de origen alérgico,
fúngico y eosinofílico los recuentos de células IgE+ son mayores que en los
sujetos de control.145 En un ensayo clínico, las concentraciones
preoperatorias de IgE totales correlacionaron de forma significativa con el
grado de afectación según la TC sinusal y no cambiaron al cabo de un año
de la intervención quirúrgica.163 Los anticuerpos de tipo IgG dirigidos
contra microorganismos de los géneros Alternaria y Cladosporium están
claramente aumentados en los pacientes con RSC en comparación con los
individuos normales, pero en menos del 30% de los pacientes con RSC se
detectan anticuerpos específicos de tipo IgG contra microorganismos de los
géneros Alternaria y Cladosporium.164 Las concentraciones de IgA e IgG
(IgG3) específicas contra hongos (Alternaria alternata y Aspergillus
fumigatus), pero no las de sus IgE, son mayores en la RSC con moco
eosinofílico que en los voluntarios sanos, lo cual pone en duda la
presunción de que exista un único mecanismo patogénico de alergia
fúngica en las "sinusitis fúngica alérgica".165
g) Óxido nítrico nasal (ONn). En un ensayo clínico prospectivo y
aleatorizado en pacientes con RSC sin mejoría tras un tratamiento inicial
con corticoides nasales, el aumento en el ONn observado tras el
tratamiento, tanto médico como quirúrgico, correlacionó con la puntuación
en las escalas de evaluación de síntomas, el tiempo de aclaramiento de
sacarina, los cambios endoscópicos y el tamaño de los pólipos. Estos
resultados sugieren que el ONn se podría utilizar como un indicador no
invasivo de la respuesta de la RSC al tratamiento.166 No obstante, se han
estudiado recientemente algunos resultados contradictorios sobre el papel
del ONn en la inflamación nasal.167
h) Neuropéptidos. La inflamación neurógena puede desempeñar un
papel potencial en la sintomatología de la rinosinusitis crónica.168 Las
concentraciones de CGRP (trigémino sensitivo) y de VIP (parasimpático)

Tesis Doctoral I. Parte Teórica
67
en saliva se encontraron significativamente elevadas entre crisis en
pacientes con el diagnóstico de RSC alérgica y migrañas en comparación
con los sujetos control y, únicamente en el caso de los pacientes con RSC,
volvieron a sus valores basales después del tratamiento con
pseudoefedrina.169
i) Mucinas. En la RSC existe una cantidad de moco superior a la
normal. Las mucinas son el principal componente del moco de las vías
aéreas. Las concentraciones de MUC5AC y MUC5B son mayores en la
mucosa de los pacientes con RSC que en la de los individuos sanos.170,171
MUC5AC y MUC5B son el principal componente de la mucina en los
senos, mientras que MUC5B y MUC2 predominan en la mucosa sana. En
los pacientes con RSC la producción de MUC5AC fue mayor y la de
MUC2 menor, mientras en los individuos sanos sucedió a la inversa.172 La
expresión de MUC8 está también aumentada en la RSC en comparación
con la mucosa sinusal maxilar sana.173 En un estudio comparativo entre
diferentes patologías de las vías respiratorias superiores, la RSC con PN
cursó con un patrón distinto de expresión de mucinas (mayor la de MUC1 y
MUC4, y menor la de MUC5AC) en comparación con la mucosa sana;
también hubo diferencias en comparación con la FQ (mayor expresión de
MUC5B) y con los pólipos antrocoanales (mayor expresión de
MUC2).174,175 El número de células caliciformes que expresan MUC5AC
no difiere entre niños con y sin RSC.176
j) Biopelículas. La conversión de formas bacterianas planctónicas
que flotan libremente en comunidades sésiles complejas ha sido objeto de
investigaciones exhaustivas. Las biopelículas son comunidades
estructuradas y especializadas de microorganismos con capacidad adhesiva
que se encuentran englobados en una sustancia extracelular polimérica
(SEP) compleja.177 Aunque las bacterias aisladas pueden ser sensibles a los
antibióticos, su organización en biopelículas las protege y puede dar origen

I. Parte Teórica Tesis Doctoral
68
a procesos infecciosos crónicos y recalcitrantes. Se han observado
biopelículas en pacientes con otitis media, colesteatoma o amigdalitis.178 Su
papel en la fisiopatología es todavía desconocido.
2.3 Tratamiento de la rinosinusitis crónica sin pólipos (Tabla 2,
Figura 6).
2.3.1 Corticoides intranasales. En un reciente ensayo multicéntrico
a doble ciego, controlado con placebo y con asignación al azar, se estudió a
134 pacientes con RSC sin PN. El tratamiento con budesonida nasal
durante 20 semanas mejoró significativamente diversos parámetros
(puntuación de síntomas, flujo inspiratorio nasal máximo o FINM).179 No
obstante, la valoración de la calidad de vida no se modificó. Se dispone de
algunas pruebas científicas que respaldan que los corticoides tópicos
nasales ejercen efectos en la RSC, en particular cuando se instilan por vía
intramaxilar. No se registraron efectos colaterales, ni siquiera en forma de
un aumento de los signos de infección, con la administración de corticoides
intranasales. No se dispone de datos que demuestren la eficacia de los
corticoides orales en la RSC sin PN.
2.3.2 Antibióticos. Es mucho más difícil evaluar la eficacia del
tratamiento con antibióticos en la RSC que en la RSA, debido a los
conflictos acerca de la terminología y la definición del cuadro clínico en la
literatura. En la mayoría de los estudios no se ha llevado a cabo una
exploración radiológica (p. ej., mediante TC) para confirmar el diagnóstico
de RSC. Los datos que respaldan el uso de antibióticos en esta afección son
escasos y, en general, no proceden de ensayos clínicos controlados con
placebo y con asignación al azar.
a) Tratamiento antibiótico de corta duración. Por el momento no
se dispone de estudios controlados sobre los efectos del tratamiento de
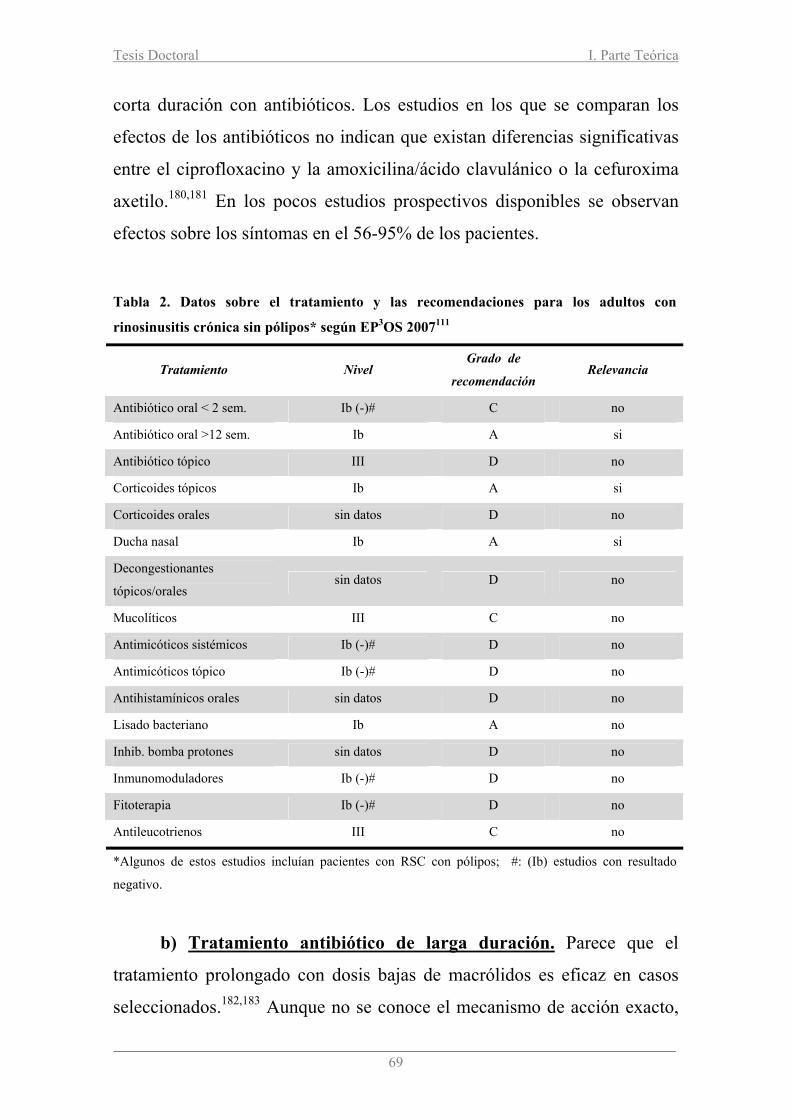
Tesis Doctoral I. Parte Teórica
69
corta duración con antibióticos. Los estudios en los que se comparan los
efectos de los antibióticos no indican que existan diferencias significativas
entre el ciprofloxacino y la amoxicilina/ácido clavulánico o la cefuroxima
axetilo.180,181 En los pocos estudios prospectivos disponibles se observan
efectos sobre los síntomas en el 56-95% de los pacientes.
b) Tratamiento antibiótico de larga duración. Parece que el
tratamiento prolongado con dosis bajas de macrólidos es eficaz en casos
seleccionados.182,183 Aunque no se conoce el mecanismo de acción exacto,
Tabla 2. Datos sobre el tratamiento y las recomendaciones para los adultos con
rinosinusitis crónica sin pólipos* según EP3OS 2007111
Tratamiento Nivel Grado de
recomendación Relevancia
Antibiótico oral < 2 sem. Ib (-)# C no
Antibiótico oral >12 sem. Ib A si
Antibiótico tópico III D no
Corticoides tópicos Ib A si
Corticoides orales sin datos D no
Ducha nasal Ib A si
Decongestionantes
tópicos/orales sin datos D no
Mucolíticos III C no
Antimicóticos sistémicos Ib (-)# D no
Antimicóticos tópico Ib (-)# D no
Antihistamínicos orales sin datos D no
Lisado bacteriano Ib A no
Inhib. bomba protones sin datos D no
Inmunomoduladores Ib (-)# D no
Fitoterapia Ib (-)# D no
Antileucotrienos III C no
*Algunos de estos estudios incluían pacientes con RSC con pólipos; #: (Ib) estudios con resultado
negativo.

I. Parte Teórica Tesis Doctoral
70
probablemente se produce un descenso de la respuesta inmunitaria del
huésped y una disminución de la virulencia de las bacterias colonizadoras.
Si se pretende aceptar este tratamiento según los criterios de la medicina
basada en pruebas científicas, es necesario que se lleven a cabo estudios
controlados con placebo para establecer la eficacia de los macrólidos.
2.3.3 Tratamiento quirúrgico. El tratamiento quirúrgico se ha de
reservar a los pacientes que no responden a tratamiento médico.104 Realizar
una cirugía endoscópica nasosinusal (CENS) favorece la recuperación
clínica del paciente a largo plazo. La CENS es muy superior a ciertos
procedimientos poco invasivos como sería la polipectomía (en el caso de
RSC con pólipos) o las irrigaciones astrales.184 Aparecen complicaciones
graves en menos del 1% de los casos y se tienen que llevar a cabo
revisiones quirúrgicas en aproximadamente un 10% de los pacientes en los
tres años siguientes a la intervención.
Figura 8. Esquema de tratamiento de la RSC sin pólipos para adultos (documento EP3OS).111
LLeevvee EVA 0-3
Corticoides tópicos Ducha/lavado nasal
Seguimiento + Ducha nasal
Corticoides tópicos ± Macrólidos (pauta
larga)
Mejoría
MMooddeerraaddaa//ggrraavveeEVA >3-10
Corticoides tópicosDucha nasal
cultivo Macrólidos (pauta
larga)
Fallo a los3 meses
Fallo a los 3 meses
realizar TC
Cirugía
Capítulo 5. Rinosinusitis crónica con pólipos


Tesis Doctoral I. Parte Teórica
73
Capítulo 5. Rinosinusitis crónica con pólipos
1. Epidemiología y comorbilidades.
1.1 Poliposis nasal (Figura 7). Según datos publicados por la
American General Health Survey las consultas por síntomas relacionados
con sinusopatía crónica llegan a englobar a un 14,7% de la población
americana, aunque la poliposis nasosinusal afectaría sólo a un 2-5% de la
población general.185 Otras publicaciones citan una prevalencia de la
poliposis nasosinusal del 4,3% en la población general.186 Desde el punto
de vista del especialista el 5% de las consultas otorrinolaringológicas y el
4% de las del alergólogo están en relación con los pólipos nasales.187 La
distribución por sexos es de 2 a 3 hombres por cada mujer y suele
manifestarse por encima de los 40 años.188 La poliposis nasosinusal es
excepcional en los menores de 10 años, debiéndose pensar a esta edad en
una fibrosis quística.
Figura 7. Poliposis nasal en FND. U: Apófisis unciforme, MM: Meato medio, P: pólipo
nasal, CM: cornete medio, S: septo nasal.
U CM
P
MM
S

I. Parte Teórica Tesis Doctoral
74
1.2 Asma. La poliposis nasosinusal está claramente asociada al asma.
Sobre 6.000 pacientes el 12,5% de los asmáticos sin alergia demostrable,
especialmente mayores de 40 años, tienen pólipos nasales, aunque sólo el
2,2% de los pacientes con asma extrínseca presentan pólipos nasales. La
media de éstos valores (7%) conforma la incidencia clásica de la poliposis
nasosinusal en los pacientes asmáticos.23
Otros autores presentan valores diferentes en la población general
dependiendo de si los sujetos tienen un asma diagnosticada o no. Sobre
4.300 pacientes la prevalencia de la poliposis nasosinusal es mayor en los
sujetos con asma diagnosticada (16,5%) frente a pacientes sin diagnóstico
de asma (3,7%).186 El asma bronquial afecta entre el 3 y el 7% de la
población general catalana y aumentan hasta un 30% en la población con
poliposis nasal.189 La PN tiene un considerable impacto en la calidad de
vida de los pacientes afectos. El asma tiene un impacto negativo adicional
en la calidad de vida de los pacientes con PN.190
1.3 Intolerancia a los AINEs. De todos los pacientes asmáticos un
10% son intolerantes al ácido acetil-salicílico (AAS) y otros AINEs, pero
en el grupo de asmáticos graves este porcentaje se eleva al 20%.191 La
prevalencia de pólipos nasales es de más del 90% en los pacientes con
asma inducida por AAS, lo que contrasta con el 10% en los pacientes con
asma tolerante.192 Por último, en los pacientes con rinosinusitis crónica
sometidos a cirugía endoscópica, la prevalencia de intolerancia al AAS es
de un 11-20%, siendo un claro indicador indirecto de gravedad de la
poliposis.193 El asma, pero no la intolerancia a la aspirina tienen un impacto
negativo adicional en la calidad de vida de los pacientes con PN.190
1.4 Rinitis alérgica. Las manifestaciones clínicas de la poliposis
nasal y de la rinitis alérgica pueden ser parecidas, lo que hizo sugerir
inicialmente que la poliposis nasosinusal era una enfermedad alérgica.

Tesis Doctoral I. Parte Teórica
75
Entre un 0,5% - 1,5% de pacientes con rinitis alérgica presenta pólipos
nasales. La atopia tiene un impacto negativo adicional en la calidad de vida
de los pacientes con PN.194 En los pacientes con rinitis no alérgica el
porcentaje se eleva al 5%.188,192
1.5 Otras asociaciones. En los pacientes afectos de fibrosis quística la
poliposis nasosinusal se presenta con mayor frecuencia que en la población
general, habiéndose descrito prevalencias que oscilan entre el 6-48%.195
Otras patologías que presentan pólipos nasales son la discinesia ciliar
primaria, el síndrome de Young y las inmunodeficiencias.
2. Histopatología de los pólipos nasales. En la poliposis nasosinusal
hay una inflamación difusa de la mucosa de las fosas nasales y senos
paranasales.196,197 Los pólipos nasales contienen una gran cantidad de
células inflamatorias, sobre todo eosinófilos, linfocitos y mastocitos. Existe
un predominio de linfocitos T sobre los B, predominando los T supresores
(CD8+) sobre los cooperadores (CD4+). Estas células, además de las células
estructurales (fibroblastos y células epiteliales) liberan moléculas que
actúan como mediadores inflamatorios, como son histamina, citoquinas,
quimioquinas y eicosanoides.
En los pólipos nasales se han distinguido cuatro tipos histológicos
diferentes, el que caracteriza a la poliposis nasosinusal es el incorrectamente
llamado pólipo “alérgico”.198 Es edematoso, eosinofílico y el tipo más común.
Sus características son el edema del estroma, hiperplasia de las células
caliciformes, gran cantidad de eosinófilos y mastocitos en el estroma y, por
último, una finísima membrana basal que separa el epitelio del estroma. Son
bilaterales y representan alrededor de un 80% de los pólipos nasosinusales.199
La poliposis antrocoanal es una patología totalmente diferente, ya que es
unilateral y proviene de la mucosa del seno maxilar, creciendo dentro del
I. Parte Teórica Tesis Doctoral
76
mismo hasta salir a la fosa nasal alcanzando la coana ipsilateral. El síntoma
más frecuente en estos pacientes es la obstrucción nasal unilateral.200
2.1 Células inflamatorias (Figura 8).
a) Mastocitos. Los pólipos nasales contienen un gran número de
mastocitos.201,202 Cuando éstos se activan se produce la degranulación con
secreción de histamina, serotonina, PAF, leucotrienos y prostaglandinas. Los
mastocitos también producen citoquinas (IL-1β, TNF-α, IFN-γ, IL-4, IL-5 y
IL-6) que, mediante la activación de moléculas de adhesión, inducirían la
infiltración eosinófila perpetuando la inflamación.
b) Eosinófilos. Una de las características más comunes de la
poliposis nasosinusal es la infiltración de la mucosa por eosinófilos.203 El
infiltrado eosinófilo es el resultado de varios fenómenos: a) aumento de la
producción de eosinófilos en la médula ósea por factores de crecimiento; b)
quimiotaxis hacia la mucosa bronquial o nasosinusal desde los vasos por
citoquinas, moléculas de adhesión y factores quimiotácticos, y c) activación
in situ para que los eosinófilos liberen sus productos.
La liberación de citoquinas y otros mediadores provoca la
diferenciación y migración de los eosinófilos al lugar de la inflamación. La
migración de los eosinófilos se produce desde la submucosa a la membrana
basal y de allí a la zona epitelial. Una vez en el tejido, el efecto de otras
citoquinas aumentará la supervivencia y activación de los eosinófilos.204,205
La efectividad de los corticoides sobre los pólipos nasales se debe, en parte,
a su efecto inductor de la muerte celular programada o apoptosis de los
eosinófilos y al efecto de inhibición de factores activadores y
quimiotácticos.206
Uno de los motivos del aumento de los eosinófilos en los pólipos
nasales es la estimulación del receptor transmembrana alfa de la IL-5. Esto
condiciona, gracias a la liberación de IL-5 y GM-CSF por el propio

Tesis Doctoral I. Parte Teórica
77
eosinófilo, un mecanismo de autosupervivencia fundamental para la
inflamación eosinofílica crónica en la poliposis nasosinusal.
Figura 8. Infiltrado celular inflamatorio. A) Pólipo nasal poco infiltrado. Eos: eosinófilos, L:
linfocitos, PMN: polimorfonucleares, M: mastocitos, CP: células plasmáticas. B) Infiltración
masiva en pólipo nasal. Tinción con Hematoxilina-Eosina (400x).
c) Linfocitos T. En el asma los linfocitos T CD4+ están presentes en
la mucosa respiratoria y se caracterizan por elaborar las citoquinas (IL-3,
IL-5 y GM-CSF) que atraen y activan a los eosinófilos. Estudios muy
recientes han permitido clasificar los linfocitos T en dos grupos
denominados TH1 y TH2. Los últimos parecen estar involucrados en las
reacciones inmunológicas que participan en la inflamación del asma, ya
que son los que segregan las citoquinas más activas sobre los eosinófilos y
elaboran la IL-4, la cual es la responsable de la activación de los linfocitos
B y su cambio fenotípico a células productoras de IgE.
d) Linfocitos B. Son los responsables de la fabricación de la IgE
implicada en la reacción alérgica inmediata. La infiltración por eosinófilos
en los pólipos nasales y la mucosa nasosinusal de los pacientes con tríada
Widal/Samter es, en la mayoría de casos, mayor que en los pacientes con
poliposis nasosinusal con tolerancia al AAS.198 Un estudio reciente del
EosPMN
CP
M L
A B
I. Parte Teórica Tesis Doctoral
78
infiltrado eosinofílico en biopsias bronquiales demuestra como en los
pólipos de los pacientes intolerantes al AAS hay más eosinófilos (37%) que
en los tolerantes (11%).207
2.2 Mediadores inflamatorios.
a) Histamina. La histamina es un mediador liberado tras la
activación de los mastocitos con potentes efectos de constricción del
músculo liso, aumento de la permeabilidad vascular y edema. Aún
existiendo en los pólipos nasales una gran presencia de histamina, los
antihistamínicos no han demostrado ninguna eficacia clínica en su
tratamiento.208
b) Citoquinas. Las citoquinas son responsables de la comunicación
intercelular ejerciendo, mediante la activación de receptores específicos de
membrana, funciones de proliferación y diferenciación celular, quimiotaxis
celular, crecimiento y modulación de la secreción de inmunoglobulinas. El
efecto antiinflamatorio de los corticoides sobre los pólipos nasales se
consigue tanto induciendo la apoptosis de los eosinófilos como inhibiendo
la secreción de citoquinas reguladoras de los eosinófilos.204,206,209-211
c) Quimiocinas. Las quimioquinas regulan la quimiotaxis de células
inflamatorias como linfocitos T, monocitos y eosinófilos. Existen varias
familias, entre las que destacan las C, CC, CXC, CX3C. De la familia CC
destacan las quimioquinas RANTES, eotaxina-1, -2 y -3, y MCP-2, -3 y –4
en los pólipos nasales.212,213
d) Factores de transcripción. Son proteínas que, tras unirse a
secuencias específicas de la región promotora de los genes, facilitan o
reprimen la transcripción de ADN a ARN y, por tanto, la producción de
proteínas. De todas las descritas en la poliposis nasal ocupan un papel
destacado el c-fos, AP-1 y NFкB.214

Tesis Doctoral I. Parte Teórica
79
e) Eicosanoides. Los eicosanoides son productos del metabolismo
del ácido araquidónico (AA) libre e incluyen dos grandes familias de
mediadores, los leucotrienos (LTs) y las prostaglandinas (PGs). Ante una
exagerada producción o por fallo de los mecanismos de degradación, los
eicosanoides pueden acumularse e influir en la patogénesis de la poliposis
nasosinusal.215 La ciclooxigenasa (Cox) metaboliza el AA a PGH2, origen
común de PGs, prostaciclina y tromboxanos.216 Las lipoxigenasas
metabolizan el AA a leucotrienos, lipoxinas y ácidos
hidroxieicosatetraenoicos (HETEs).217 Se han encontrado disminuidos la
Cox-2 y la PGE2 en las poliposis nasales de pacientes con asma
intolerante.157
3. Tratamiento de la rinosinusitis crónica con pólipos (Tabla 3, Figura
11)
Los objetivos del tratamiento, médico o quirúrgico, van destinados a
reducir o eliminar los pólipos, restablecer la respiración nasal, restaurar el
sentido del olfato, reducir los síntomas de la rinosinusitis y, por último,
prevenir las recurrencias de los pólipos nasales. Los corticoides
intranasales constituyen la piedra angular debido a su probado efecto
terapéutico.
3.1 Tratamiento médico con glucocorticoides (GC). Constituyen el
tratamiento más efectivo en la prevención y la supresión de la inflamación
a nivel de la mucosa nasosinusal. Los GC inhiben la inflamación mediante
la transrepresión de los factores de transcripción y, por lo tanto, de la
expresión de mediadores, receptores, moléculas de adhesión, y citoquinas
que participan en el proceso inflamatorio.218,219
Los principales efectos antiinflamatorios se basan en su capacidad de
reducir la síntesis de citoquinas (IL-1, IL-2, IL-3, IL-4, IL-5, IL-6, IL-8,

I. Parte Teórica Tesis Doctoral
80
TNF-α, IFN-γ, GM-CSF) y de células (macrófagos, monocitos, linfocitos, y
células epiteliales y endoteliales), al inhibir la transcripción genética
interactuando con los “elementos de respuesta a los GC” (ERG), por
transrepresión con factores de transcripción o al no permitir la traducción
de proteínas eliminando los ARNm.220,221 Este hecho afecta al
reclutamiento, localización, síntesis proteica y supervivencia de células
proinflamatorias, como los eosinófilos. El reclutamiento de células
inflamatorias también disminuye por la inhibición en la expresión de
moléculas de adhesión como ICAM-1 y VCAM-1222, que afectan el flujo
de basófilos y mastocitos en el epitelio de la mucosa nasal. Los GC
también actuan en el ciclo del ácido araquidónico, inhibiendo directamente
la fosfolipasa A2 (PLA2) y la expresión de la COX-2.223-225 Esto último no
está claro, ya que existen pruebas de que el tratamiento corticoideo produce
un aumento de la expresión de la Cox-2 in vivo en pacientes con poliposis
nasal.226 Además, los GC reducen la supervivencia de los eosinófilos ya sea
por inhibición de la expresión de citoquinas por otras células, o por bloqueo
de la acción de las citoquinas en los eosinófilos por activación de
endonucleasas y de la apoptosis o muerte celular programada.227,228
La corticoterapia intranasal, y a veces sistémica, es el tratamiento
recomendado para la poliposis nasal. Tanto el tratamiento médico como el
tratamiento quirúrgico alcanzan una mejoría de la calidad de vida similar
en los pacientes con RSC con pólipos.112 La eficacia de los corticoides
intranasales se observa a todos los niveles:
a) Síntomas. Existe una reducción de la obstrucción nasal, la rinorrea
y los estornudos con un incremento significativo del flujo aéreo nasal. Esta
eficacia se mantiene mientras dura el tratamiento, pero al abandonarse
recurren los síntomas de forma lenta cuando la poliposis es leve y rápida
cuando es grave. Los corticoides intranasales tienen un efecto limitado en
la recuperación de la pérdida de olfato en los pacientes con poliposis
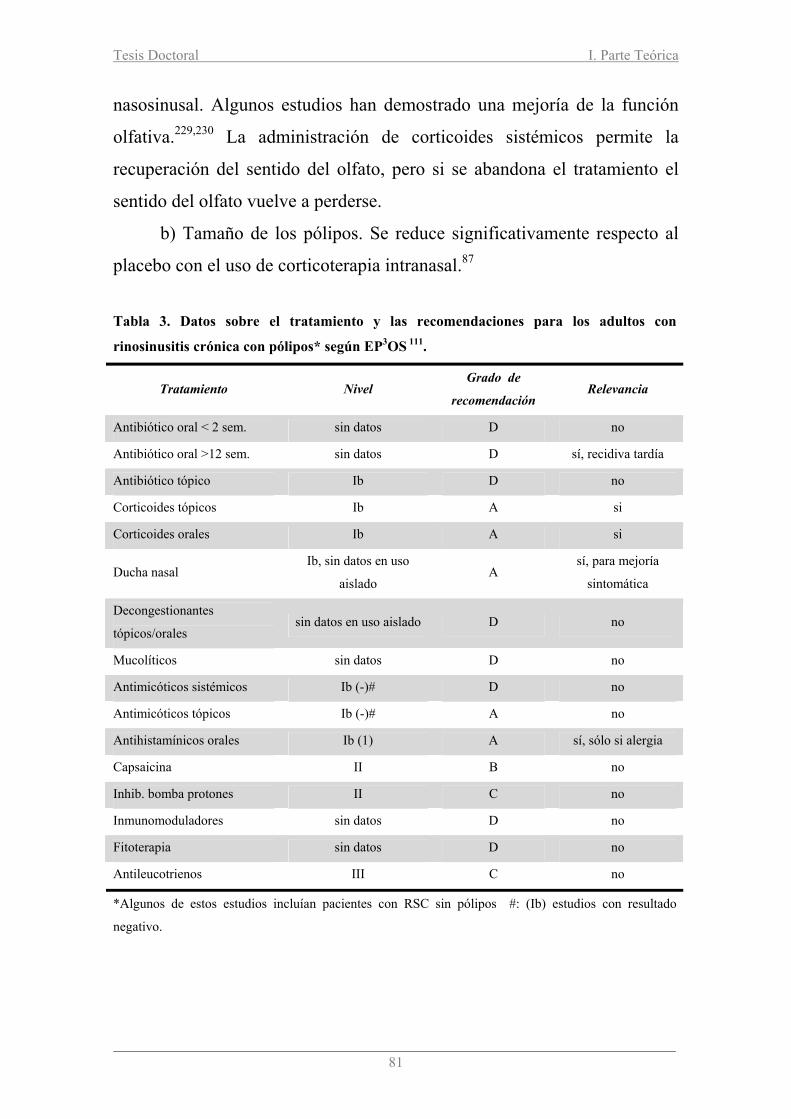
Tesis Doctoral I. Parte Teórica
81
nasosinusal. Algunos estudios han demostrado una mejoría de la función
olfativa.229,230 La administración de corticoides sistémicos permite la
recuperación del sentido del olfato, pero si se abandona el tratamiento el
sentido del olfato vuelve a perderse.
b) Tamaño de los pólipos. Se reduce significativamente respecto al
placebo con el uso de corticoterapia intranasal.87
Tabla 3. Datos sobre el tratamiento y las recomendaciones para los adultos con
rinosinusitis crónica con pólipos* según EP3OS 111.
Tratamiento Nivel Grado de
recomendación Relevancia
Antibiótico oral < 2 sem. sin datos D no
Antibiótico oral >12 sem. sin datos D sí, recidiva tardía
Antibiótico tópico Ib D no
Corticoides tópicos Ib A si
Corticoides orales Ib A si
Ducha nasal Ib, sin datos en uso
aislado A
sí, para mejoría
sintomática
Decongestionantes
tópicos/orales sin datos en uso aislado D no
Mucolíticos sin datos D no
Antimicóticos sistémicos Ib (-)# D no
Antimicóticos tópicos Ib (-)# A no
Antihistamínicos orales Ib (1) A sí, sólo si alergia
Capsaicina II B no
Inhib. bomba protones II C no
Inmunomoduladores sin datos D no
Fitoterapia sin datos D no
Antileucotrienos III C no
*Algunos de estos estudios incluían pacientes con RSC sin pólipos #: (Ib) estudios con resultado
negativo.
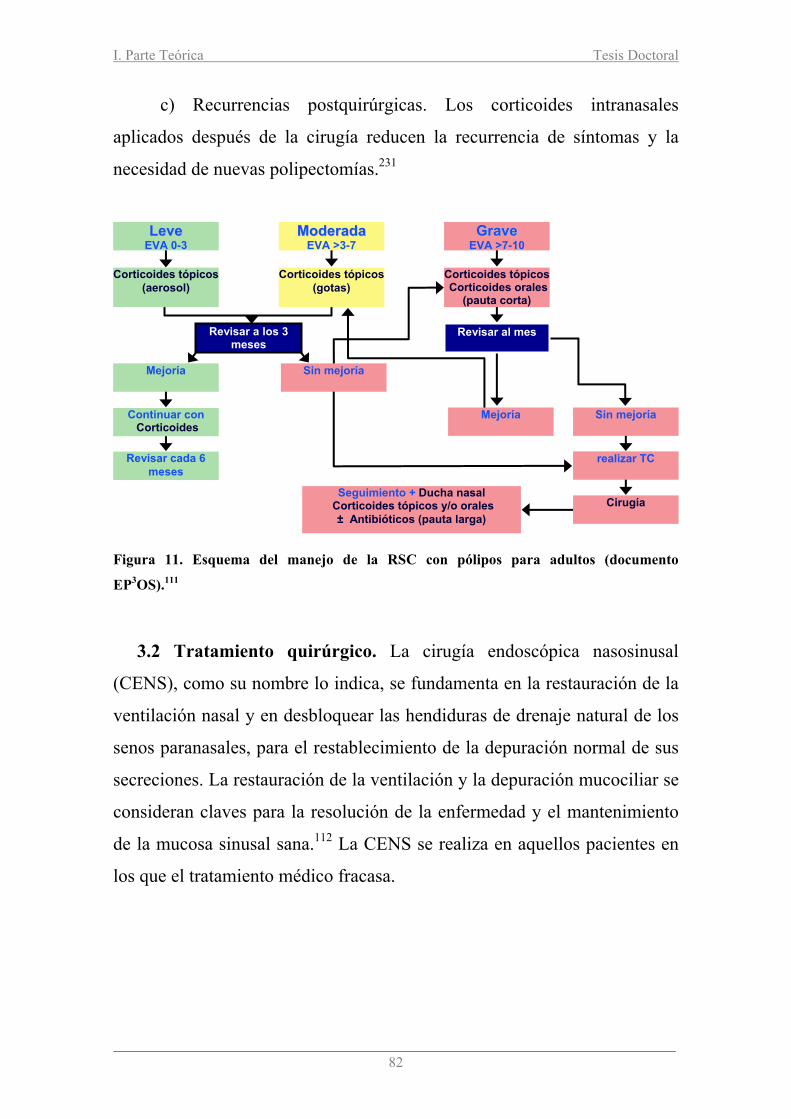
I. Parte Teórica Tesis Doctoral
82
c) Recurrencias postquirúrgicas. Los corticoides intranasales
aplicados después de la cirugía reducen la recurrencia de síntomas y la
necesidad de nuevas polipectomías.231
Figura 11. Esquema del manejo de la RSC con pólipos para adultos (documento
EP3OS).111
3.2 Tratamiento quirúrgico. La cirugía endoscópica nasosinusal
(CENS), como su nombre lo indica, se fundamenta en la restauración de la
ventilación nasal y en desbloquear las hendiduras de drenaje natural de los
senos paranasales, para el restablecimiento de la depuración normal de sus
secreciones. La restauración de la ventilación y la depuración mucociliar se
consideran claves para la resolución de la enfermedad y el mantenimiento
de la mucosa sinusal sana.112 La CENS se realiza en aquellos pacientes en
los que el tratamiento médico fracasa.
LLeevvee EVA 0-3
Seguimiento + Ducha nasal Corticoides tópicos y/o orales
± Antibióticos (pauta larga)
MMooddeerraaddaa EVA >3-7
Corticoides tópicos(aerosol)
Mejoría
Continuar con Corticoides
ó iRevisar cada 6
meses
Corticoides tópicos(gotas)
GGrraavvee EVA >7-10
Sin mejoría
Corticoides tópicos Corticoides orales
(pauta corta)
Mejoría Sin mejoría
realizar TC
Cirugía
Revisar a los 3 meses
Revisar al mes

Capítulo 6. Bronquiectasias


Tesis Doctoral I. Parte Teórica
85
Capítulo 7. Bronquiectasias
1. Definición. La bronquiectasia (BQ) es la destrucción y la dilatación
anormal, permanente e irreversible de uno o más bronquios medianos y
pequeños, producidas por la pérdida de los componentes musculares y
elásticos de la pared bronquial.232 Laennec (1819) fue quien describió la
BQ y sugirió que se debía a retención de secreciones bronquiales con
destrucción secundaria de la pared, debilitamiento y ulterior dilatación233
(Figura 12). Esta interpretación es totalmente válida actualmente y se
considera que la inflamación bronquial juega un papel central. La BQ causa
sobreinfecciones pulmonares graves junto a colonización de las mismas y
pérdida de capacidad y función pulmonar, por lo que presenta una elevada
morbilidad y contribuye a una mortalidad prematura en el paciente que las
presenta.234
Figura 12. Tomografía pulmonar de alta resolución donde se objetivan bronquiectasias
a nivel bilateral.

I. Parte Teórica Tesis Doctoral
86
2. Epidemiología. Según las compañías aseguradoras de Estados
Unidos se estima que existen al menos 110.000 personas tratadas en este
país por presentar BQ no quísticas.235 El coste medio anual por paciente es
de 13244 dólares, ligeramente superior al de los pacientes con enfermedad
pulmonar obstructiva crónica siendo el 25% de ellos responsables del 80%
del coste total. La prevalencia a nivel mundial se desconoce. Estudios
epidemiológicos en Auckland (Nueva Zelanda) y Hong Kong dieron una
prevalencia de 1 por cada 6.000 y de 16,4 por cada 100.000 personas,
respectivamente.236
3. Etiología (Tabla 4). Establecer la etiología de las BQ es un
trabajo árduo, dificultoso y sin éxito la mayoría de las veces. A pesar de
una exhaustiva investigación, del 50 al 80% de las BQ se acaban
diagnosticando como idiopáticas. Así pues, las BQ pueden ser idiopáticas,
pos-infecciosas, debidas a defectos anatómicos o asociadas a una larga lista
de enfermedades sistémicas. Las bronquiectasias idiopáticas representan
una parte muy importante de las BQ de origen desconocido debidas a
alteraciones indetectables a nivel inmunológico o a anormalidades
autoinmunes. Nicotra et al.237 revisaron 123 pacientes afectos de BQ,
encontrando que un 30% de los pacientes no tenían ningún antecedente y
un 35% refieren una historia de neumonía previa. Sólo un 11% presentaron
algún antecedente de infección en la infancia. Pasteur et al.238 evaluó 150
pacientes adultos, muchos de los cuales fueron catalogados de tener BQ
idiopáticas (35,3%). Entre los pacientes en los que encontró una causa,
destacan las inmunodeficiencias humorales, la aspiración, la aspergilosis
broncopulmonar alérgica (ABPA), la colitis ulcerosa, la discinesia ciliar, la
fibrosis quística y el déficit de α1-antitripsina. Un estudio realizados por

Tesis Doctoral I. Parte Teórica
87
Shoemark et al.239 muestra unos datos muy similares a los de Pasteur et
al.238.
Las bronquiectasias localizadas suelen estar motivadas por estenosis
de algún bronquio debido a procesos inflamatorios, neoformativos o
cuerpos extraños.240 Cualquier condición que produzca colapso por
absorción en la zona y fibrosis del tejido pulmonar adyacente, contribuye a
la formación de bronquiectasias por dilatación compensadora del bronquio.
Las bronquiectasias difusas pueden ser debidas a múltiples causas
(Tabla 4) entre las que destacan las enfermedades congénitas que afectan la
función mucociliar, como son la fibrosis quística o las discinesias
(síndrome de Kartagener, síndrome de Young). En otras ocasiones se
asocian a defectos en los mecanismos de defensa que favorecen el
desarrollo de infecciones bronquiales repetidas (inmunodeficiencia común
Tabla 4. Etiologia de las bronquiectasias.234
Postinfección Bacterias: neumonía necrosante Micobacterias: tuberculosis, micobacterias no tuberculosas Virus: adenovirus, sarampión Hongos
Obstrucción bronquial
Intrínseca: estenosis cicatricial, broncolitiasis, cuerpo extraño, tumor Extrínseca: adenopatías, tumor, aneurisma
Inmunodeficiencias Primarias: déficit de anticuerpos, inmunodeficiencias combinadas Secundarias: quimioterapia, trasplante, neoplasias hematológicas, VIH
Alteración mucociliar Fibrosis quística Discinesia ciliar primaria Síndrome de Young
Neumonitis inflamatoria
Aspiración, reflujo gastroesofágico Inhalación de tóxicos (drogas, gases)
Anormalidad árbol traqueobronquial
Traqueobroncomegalia (síndrome de Mounier-Kuhn) Defectos del cartílago (síndrome de Williams-Campbell) Secuestro pulmonar Traqueobroncomalacia Bronquio traqueal
Asociada a otras enfermedades
Enfermedades sistémicas: artritis reumatoide, lupus, síndrome de Sjögren, síndrome de Marfan, policondritis recidivante, espondilitis anquilosante, sarcoidosis Enfermedad inflamatorio intestinal: colitis ulcerosa, enfermedad de Crohn Otras enfermedades respiratorias: asma, EPOC, síndroma de Swyer-James Déficit de alfa1-antitripsina, síndrome de la uñas amarillas
Aspergilosis o ABPA Panbronquiolitis difusa No conocida

I. Parte Teórica Tesis Doctoral
88
variable, deficiencias de la formación de anticuerpos). Algunas
bronquiectasias parecen haberse desarrollado a raíz de una bronquiolitis
infecciosa en la infancia (sarampión, virus respiratorio sincitial). También
pueden presentarse asociadas a enfermedades sistémicas (artritis
reumatoide, síndrome de Sjögren) o a enfermedades inflamatorias
intestinales (colitis ulcerosa, enfermedad de Crohn). En un número
reducido de casos pueden ser consecuencia de la aspiración de sustancias
tóxicas que lesionan los bronquios.
Entre las enfermedades que ocasionan bronquiectasias y patología
nasosinusal debemos destacar:
3.1 Fibrosis quística (FQ). Es la alteración genética de tipo
autosómico recesivo más común en la población de tipo caucásico. Uno de
cada 25 individuos es portador del gen.241,242 Se calcula que afecta
aproximadamente a 1 de cada 3.000-10.000 nacidos vivos por año. El gen
responsable de la FQ se encuentra en el locus simple del brazo largo del
cromosoma 7. La deleción de tres pares de bases o mutación Delta F508
acontece aproximadamente en el 70% de todos los cromosomas de la FQ.
La proteína defectuosa, codificada por este gen anormal, tiene una
estructura similar a una clase de proteínas conocida por ser activa en el
transporte epitelial y ha sido denominada Cystic Fibrosis Transmembrane
Regulator (CFTR).243 Esta proteína defectuosa contribuye a un mal
funcionamiento de las canales del cloro que provoca un aumento de la
viscosidad del moco dificultando su eliminación y favoreciendo la
colonización por Stafilococus aureus y Pseudomona mucoide.
Otras mutaciones han sido identificadas cerca del locus afectado. Los
pacientes afectos de FQ se caracterizan por presentar infecciones repetidas
en el tracto respiratorio, insuficiencia pancreática exocrina e infertilidad. La
radiografía de tórax244 muestra afectación de los lóbulos superiores en
estados precoces, que se vuelven difusos con la progresión de la
Tesis Doctoral I. Parte Teórica
89
enfermedad. La función pulmonar puede ser normal o presentar un patrón
de tipo obstructivo o mixto. En la presentación adulta los síntomas han
estado usualmente presentes por años, pero muchas veces no son tomados
en cuenta al ser moderados. El adulto puede presentar bronquiectasias,
rinosinusitis, insuficiencia pancreática, pancreatitis aguda, colelitiasis e
infertilidad. La obstrucción nasal es el síntoma más frecuente entre los
pacientes con FQ. La incidencia de poliposis nasal es de más del 20% de
los pacientes. Encontramos diferentes patrones de rinosinusitis: pólipos
nasales, rinosinusitis crónica purulenta y mucopiosinusitis del antro del
seno maxilar con protusión de la pared nasal lateral.245 Esta última entidad
recibe el nombre de pseudomucocele maxilar. En el diagnóstico de la FQ es
importante el test del sudor246 (en la enfermedad las concentraciones de
sodio o cloro son de 60 mmol/l o superior, siendo en individuos normales y
portadores del gen FQ de hasta 30 mmol/l), el estudio genotípico y la TC
torácica y nasosinusal. Los objetivos del tratamiento de la FQ son: reducir
la obstrucción, controlar las infecciones, disminuir la inflamación y mejorar
el estado nutricional. A nivel nasal el tratamiento consiste en lavados
nasales con suero fisiológico, corticoterapia intranasal, antibioticoterapia y,
en caso necesario, la cirugía endoscópica nasosinusal (CENS).
3.2 Discinesia ciliar primaria (DCP). Es una enfermedad congénita
en la que existe una alteración total o parcial en la función de las células
ciliadas.247 La DCP es una enfermedad autosómica recesiva que afecta a
uno de cada 16.000 nacidos vivos, presentándose clínicamente con
rinosinusitis y bronquiectasias y, de forma menos frecuente, esterilidad en
los varones. En el síndrome de discinesia (dificultad para el movimiento)
ciliar primaria existen alteraciones estructurales o funcionales en los
microtúbulos de los cilios que son responsables del movimiento de los
mismos. Estas alteraciones originan un mal aclaramiento del moco de los
cilios, con las consiguientes infecciones bronquiales supurativas y

I. Parte Teórica Tesis Doctoral
90
bronquiectasias. Se alteran todas las estructuras donde existen cilios:
epitelios de las vías respiratorias, senos paranasales, trompa de Eustaquio, y
espermatozoides (astenospermia).248
Entre los individuos afectados, el 50% presenta el síndrome de
Kartagener caracterizado por la triada de bronquiectasias, rinosinusitis
crónica y situs inversus (dextrocardia).249 Una rinitis con presencia de
rinorrea anterior se encuentra en todos los pacientes afectos de DCP,
acompañados en algunos casos de pólipos nasales y disminución o pérdida
parcial o completa del olfato. En la TC de senos es típico encontrar
ocupación de los senos etmoidales y maxilares, junto a hipoplasia de seno
frontal. El diagnóstico se realiza mediante una combinación de pruebas
como son: tiempo de sacarina, ON nasal, biopsia nasal en la que se puede
observar la frecuencia de batida de los cilios y la densidad de los mismos
mediante microscopía electrónica.250 En el manejo del paciente con DCP
resulta de gran importancia la fisioterapia respiratoria con drenaje postural
y el uso de antibióticos en las agudizaciones por infecciones respiratorias.
La realización de una polipectomía endoscópica o una CENS es
beneficiosa en aquellos pacientes con una rinosinusitis crónica rebelde al
tratamiento.
El diagnóstico se establece por estudio ultraestructural de muestras
obtenidas de mucosa nasal, en las que se suele observar la ausencia de los
brazos de la dineína o disposición anómala de los microtúbulos. Estudios
recientes han demostrado unos niveles bajos de ON nasal en los pacientes
afectos,251 considerándose diagnóstico niveles de ON inferiores a 100 ppb.
3.3 Síndrome de Young. Consiste en la presencia de la triada:
bronquiectasias, rinosinusitis crónica e infertilidad. En estos pacientes la
actividad ciliar es normal siendo el moco muy viscoso. La biopsia nasal
estudiada bajo microscopía electrónica no muestra cambios en la estructura
de los cilios en estos pacientes.252 La azoespermia causante de la

Tesis Doctoral I. Parte Teórica
91
infertilidad es debida a la obstrucción del epidídimo, ya que la
espermiogénesis es totalmente normal. El diagnóstico se basa en la clínica
(enfermedad sinopulmonar crónica, azoespermia), así como en la exclusión
de fibrosis quística y de síndromes de inmovilidad ciliar.253
3.4 Deficiencia de alfa1-antitripsina (ATT). Esta es una
glicoproteína producida por los hepatocitos, cuya función es la de inhibir
las proteasas (elastasa), en particular las liberadas por los neutrófilos, en su
misión reparadora y de limpieza de agentes externos a nivel pulmonar. Al
inhabilitar las proteasas evita la destrucción de tejidos sanos en nuestro
organismo.254 El gen que la codifica está situado en el cromosoma 14. En el
pulmón el déficit de ATT produce enfisema por una destrucción progresiva
de los alveolos en la tercera y cuarta década de la vida. El humo del tabaco
contribuye a la destrucción pulmonar, dado que aumenta la actividad de la
elastasa, disminuye la actividad de la ATT por su oxidación e inactiva la
síntesis de elastina, interfiriendo en la reparación pulmonar; por lo que
dejar de fumar debe ser la principal prioridad del paciente diagnosticado
con déficit de ATT.255
El enfisema producido por el déficit de ATT es panacinar, donde
existe destrucción de todo el acini. Se localiza frecuentemente en las bases,
existiendo un aumento de la distensibilidad “compliance" pulmonar. La
disminución de los niveles de ATT produce un desequilibrio entre esta
proteína (antiproteasa) y la elastasa (proteasa). Al no existir suficiente
cantidad de ATT, las elastasas siguen destruyendo progresivamente la
elastina de las paredes alveolares.256 Se consideran como niveles normales
de la proteína ATT en sangre los comprendidos entre 150 a 350 mg/dl ó
20-53 µM. Niveles por debajo de los 80 mg/dl u 11 µM ponen en riesgo al
individuo de padecer alguna de las enfermedades relacionadas con su
déficit. A nivel pulmonar se observan enfisema, bronquitis crónica,
bronquiectasias, asma de difícil tratamiento y neumonías de repetición. Las
I. Parte Teórica Tesis Doctoral
92
recomendaciones para realizar mediciones cuantitativas de ATT son:
enfisema precoz, antecedentes familiares, disnea o tos en varios miembros
de una misma familia de las mismas o diferentes generaciones, adultos con
bronquiectasias sin etiología evidente, todos los pacientes con enfermedad
obstructiva pulmonar, enfermedad hepática de causa desconocida,
pacientes asmáticos que no responden a tratamiento o padecen paniculitis
inexplicable.257 La rinitis alérgica y las rinosinusitis de repetición también
constituyen una manifestación frecuente en estos pacientes, incluso en
ausencia de enfermedad obstructiva pulmonar.258
4. Histopatología. La bronquiectasia (BQ) es la destrucción y la
dilatación anormal, permanente e irreversible de uno o más bronquios
medianos y pequeños, producidas por la pérdida de los componentes
musculares y elásticos de la pared bronquial. En las bronquiectasias se
encuentran áreas de la pared bronquial destruidas e inflamadas
crónicamente constituyendo un círculo vicioso; las células ciliadas están
dañadas o destruidas y la producción de moco está aumentada, perdiéndose
el tono normal de la pared.259 El aumento de la producción de moco facilita
el crecimiento de las bacterias, obstruye los bronquios y favorece el
estancamiento de las secreciones infectadas, con un daño posterior de la
pared bronquial.260 La inflamación puede extenderse a los alvéolos y
producir bronconeumonía, formación de tejido cicatricial y pérdida del
tejido pulmonar sano. Además, la inflamación de los vasos sanguíneos de
la pared bronquial puede ocasionar expectoración hemoptóica o hemoptisis
franca. En el examen anatomopatológico se observan dilataciones
bronquiales, hipertrofia de la mucosa, en ocasiones con metaplasia
escamosa, infiltrado linfocítario de la pared bronquial y desaparición de
cartílago, músculo y fibras elásticas que son substituidas por tejido
cicatricial.261 El análisis del esputo y las biopsias de la mucosa bronquial
han mostrado un aumento de la concentración de la elastasa, IL-8, TNF-α y

Tesis Doctoral I. Parte Teórica
93
prostanoides.262,263 Los marcadores de inflamación sistémica también estan
elevados en los pacientes con BQ en fase estable.263
5. Aspectos clínicos y diagnóstico. El curso clínico de las BQ no
quísticas es muy variable. Algunos pacientes no tienen síntomas o son muy
leves, mientras que otros los presentan a diario con progresiva pérdida de
funcionalidad pulmonar y por consiguiente de calidad de vida. El síntoma
que caracteriza a esta enfermedad es la tos productiva crónica ó broncorrea
mucopurulenta y maloliente. Es típico que la tos sea intermitente durante el
día y que predomine por las mañanas al levantarse, debido a la retención de
las secreciones durante la noche y que, a su vez, aumente con las
infecciones agudas. En ocasiones no existe ningún síntoma evidente o una
simple tos seca. En un 50-70% de los casos hay esputo sanguinolento
(hemoptoico). Con frecuencia suelen haberse padecido neumonías de
repetición o crisis de disnea (dificultad para respirar) antes de ser
diagnosticados de esta enfermedad. No es rara la presencia de episodios
febriles, deterioro del estado general, adelgazamiento del paciente y, en
ocasiones, olor nauseabundo de las secreciones y, en consecuencia, del
paciente.
Actualmente, el manejo apropiado (fundamentalmente por el
correcto uso de los antibióticos) de las bronquiectasias ha conseguido
reducir o hacer desaparecer las complicaciones que tradicionalmente
presentaban éstos pacientes debidas a la extensión local o a distancia de la
infección (abscesos cerebrales, abscesos pulmonares). Por este motivo, las
complicaciones más frecuentes son: hemoptisis, obstrucción crónica al
flujo aéreo, acropaquia, insuficiencia respiratoria crónica y el cor
pulmonale.
El diagnóstico de las BQ es clínico-radiológico.264 En la auscultación
pulmonar pueden encontrarse crepitantes, roncus y/o sibilancias, todos
I. Parte Teórica Tesis Doctoral
94
ellos indicativos de abundante secreción bronquial. Inicialmente en las
bronquiectasias difusas puede haber un patrón obstructivo moderado-
severo y al avanzar la enfermedad aparecer un patrón restrictivo. Es
bastante frecuente la hiperreactividad bronquial. La placa de tórax y la TC
pulmonar convencional no son suficientemente sensibles en el diagnóstico
de BQ. Actualmente la confirmación de las mismas es por la TC de alta
resolución pulmonar, que ha desplazado a la broncografía con contraste. La
extensión de las BQ en la TC de alta resolución está correlacionada con
cambios funcionales y pronóstico del paciente. Otras pruebas
complementarias van encaminadas a demostrar la causa de las
bronquiectasias.
6. Microbiología. La complicación más frecuente de las BQs es la
sobreinfección.265 La colonización más frecuente en estos pacientes es por
Haemophilus Influenzae (55%), Pseudomona spp (26%), Staphilococus
aureus y Streptococus pneumoniae.237 Resulta de gran importancia conocer
que tipo de bacterias colonizan las vías distales, ya que dicha colonización
produce gran cantidad de mediadores de la inflamación que conducen a un
daño progresivo en el tejido pulmonar y obstrucción a nivel bronquial.266
7. Tratamiento
7.1 Tratamiento médico. El principal objetivo va encaminado a
tratar la causa siempre que sea posible y si no se encuentra, el tratamiento
es sintomático a fin de mejorar la clínica y prevenir la progresión de la
enfermedad. Resulta primordial controlar las infecciones y las secreciones,
evitando la obstrucción de las vías aéreas y sus complicaciones.
a) Tratamiento de la agudización. Los antibióticos, facilitar la
eliminación de las secreciones y el tratamiento del broncoespasmo asociado
constituyen la base del tratamiento de las agudizaciones. La elección del

Tesis Doctoral I. Parte Teórica
95
antibiótico depende de la presencia o no de una colonización o infección
bronquial crónica conocida. En el primer caso hay que adecuar el
antibiótico a los microorganismos previamente aislados; en el segundo,
debe iniciarse un tratamiento empírico. Siempre ha de tenerse en cuenta el
riesgo de colonización por Pseudomona aeruginosa.267 Hay que usar
antibióticos con alto grado de penetración en las secreciones bronquiales, a
dosis elevadas y administrarlos hasta que el esputo deje de ser purulento,
con un mínimo de 10 días, y en casos de infección por Pseudomona,
durante 14-21 días.266,268 Añadir tratamiento por vía inhalada al tratamiento
antibiótico oral o intravenoso no ha demostrado reportar beneficios
clínicos.
b) Tratamiento de la colonización. En la colonización bronquial
inicial no existe evidencia para indicar tratamiento antibiótico, excepto en
el primer aislamiento de Pseudomona en BQ debidas a FQ.266 Cuando
existe infección bronquial crónica el tratamiento se basa en la
administración prolongada de antibióticos269 y en facilitar el drenaje de las
secreciones, intentando romper el círculo vicioso de infección-inflamación
reduciendo tanto la carga bacteriana como la respuesta inflamatoria.
c) Tratamiento de la inflamación bronquial. Los macrólidos
disminuyen el número de agudizaciones.270,271 Su efecto probablemente se
debe a su acción moduladora de la respuesta inflamatoria y a la capacidad
en interferir en la formación de biopelículas. Los corticoides inhalados
están indicados especialmente en los pacientes con clínica de
hiperreactividad bronquial.
d) Tratamiento de la hiperreractividad bronquial. Se utilizarán
broncodilatadores y corticoides inhalados. Los broncodilatadores también
mejoran la movilidad ciliar y facilitan el aclaramiento de secreciones.272
I. Parte Teórica Tesis Doctoral
96
7.2 Tratamiento quirúrgico. Las indicaciones son: 1) enfermedad
localizada y que pueda ser extirpada totalmente sin que ello implique
eliminar grandes cantidades de pulmón funcionante. Solamente a
considerar si fracasa el tratamiento médico y fisioterápico; 2) hemoptisis
masiva con embolización inefectiva; y 3) zonas abscesificadas no curables
con tratamiento antibiótico.273
7.3 Otros tratamientos. Las medidas preventivas más importantes
serían: abandono del hábito tábaquico, evitar la contaminación, mantener
una correcta hidratación para hacer las secreciones bronquiales más fluidas,
mucolíticos, consejo dietético individualizado, incrementar el ejercicio
aeróbico, vacunación contra el neumococo y el haemophilus y la
vacunación anual contra el virus de la gripe contribuyen muy
probablemente a disminuir el número de episodios infecciosos graves,
fisioterapia respiratoria, mediante drenaje postural de forma correcta y
mantenida un mínimo de dos veces al día. En el tratamiento es fundamental
la fisioterapia respiratoria efectiva, con el fin de expulsar las secreciones
bronquiales.

II. HIPÓTESIS Y OBJETIVOS


Tesis Doctoral II. Hipótesis y Objetivos
99
HIPÓTESIS Y OBJETIVOS
Hipótesis.
Se ha demostrado por otras enfermedades, como la asociación de
asma/rinitis alérgica, que existe una relación entre las vías aérea superior e
inferior bajo el concepto de “una vía, una enfermedad”. La experiencia
clínica en el servicio de ORL y Neumología nos ha llevado a observar que
en los pacientes con BQs existe una asociación con rinosinusitis crónica
(RSC). La hipótesis de nuestro estudio establece que las BQs y la patología
nasosinusal acompañante formarían parte de una misma enfermedad y, por
tanto, los mecanismos de producción a nivel inflamatorio e infeccioso que
modulan la formación de las bronquiectasias serían los mismos que
modulan la enfermedad a nivel nasosinusal. La demostración de la
existencia de un aumento de patología nasosinusal en estos pacientes y su
caracterización sería el paso previo que permitirá realizar estudios
encaminados a aclarar los mecanismos responsables de su origen.
Objetivo general.
Demostrar que en los pacientes con BQs existe una asociación de
patología inflamatoria nasosinusal en forma de RSC con o sin pólipos
nasales que estarían ligadas de forma epidemiológica, fisiopatológica y de
impacto en la calidad de vida.
Objetivos específicos.
Estudio 1: Una única vía aérea: alta prevalencia de rinosinusitis y poliposis
nasal en bronquiectasias.
• Demostrar que los pacientes con bronquiectasias presentan un alto
índice de patología nasosinusal: rinosinusitis crónica con / sin
pólipos

II. Hipótesis y Objetivos Tesis Doctoral
100
• Medir la afectación semiológica, endoscópica nasal y radiológica
nasosinusal en pacientes con bronquiectasias.
• Investigar, comparar y correlacionar si la inflamación a nivel
pulmonar es similar a la existente a nivel nasosinusal mediante
técnicas no invasivas (NO exhalado y nasal).
• Estudiar la existencia de correlación entre la afectación radiológica
nasal y pulmonar mediante TC pulmonar de alta resolución y TC de
senos paranasales.
• Investigar si la alteración de la función pulmonar (espirometría) se
corresponde con la alteración de la función nasal (rinomanometría y
rinometria acústica).
• Analizar la posible relación entre la patología nasosinusal y la
etiología de las bronquiectasias (postinfecciosa vs. idiopática).
Estudio 2: Impacto de las bronquiectasias asociadas a patología
nasosinusal en la calidad de vida.
• Estudiar si los pacientes afectos de bronquiectasias con patología a
nivel nasal presentan una peor calidad de vida comparado con la
población general española utilizando un cuestionario genérico de
calidad de vida (SF-36).
• Valorar si la presencia de poliposis nasal empeora más la calidad de
vida de los pacientes con BQs.
Estudio 3: Vía aérea única: el impacto de la rinosinusitis crónica y la
poliposis nasal en la calidad de vida de los pacientes con bronquiectasias.

Tesis Doctoral II. Hipótesis y Objetivos
101
• Evaluar el impacto de la rinosinusitis crónica con o sin pólipos en la
calidad de vida empleando cuestionarios específicos / genéricos (SF-
36, SNOT-20, SGRQ) de los pacientes con bronquiectasias.
• Correlacionar dicho impacto en la calidad de vida con los síntomas
nasales, función pulmonar y el estado de la salud en general.
Interés asistencial y aplicabilidad La demostración de patología nasosinusal asociada a las BQs llevaría a:
1. Incorporar visitas rutinarias por parte del ORL en los pacientes
con bronquiectasias a fin de evaluar la existencia concomitante de una
rinosinusitis crónica con o sin pólipos.
2. Mejorar el manejo de las vías aéreas altas, tanto mediante el
diagnóstico como el tratamiento, y la evolución de las bronquiectasias
(disminución de ingresos hospitalarios, mejoría de calidad de vida) en una
visión unificada.
3. Dada la mejor accesibilidad de la nariz en la realización de
exploraciones (endoscopia nasal, biopsia, recogida de secreciones nasales)
en comparación a las vías inferiores (fibrobroncoscopia), el control
evolutivo de la patología pulmonar podría mejorar y ser menos invasivo.
4. Se lograría un diagnóstico y tratamiento común mediante la
creación de unidades multidisciplinares: Alergia-Neumología-ORL.


III. PARTE EXPERIMENTAL

Tesis Doctoral III. Trabajo Experimental
105
RESUMEN DE LOS ARTÍCULOS ORIGINALES
Estudio 1: United airway again: high prevalence of rhinosinusitis and
nasal polyps in bronchiectasis. Allergy 2009;64:790-7. DOI: 10.111/j.1398-9995.2008.01892.x
Introducción: a pesar de las múltiples relaciones entre patología de la vía
aérea superior e inferior, la asociación de BQs con RSC con o sin pólipos
no ha sido del todo evaluada.
Objetivo: investigar la patología nasosinusal que se asocia a los pacientes
con bronquiectasias.
Metodología: en este estudio prospectivo se estudiaron 88 pacientes con
BQs (56 pacientes con BQs idiopáticas y 32 con BQs post-infecciosas). En
ellos se evaluó la posible existencia de RSC con o sin pólipos nasales
aplicando los criterios EP3OS. Se empleo: puntuación de síntomas nasales
(obstrucción, rinorrea anterior, rinorrea posterior, dolor facial, estornudos,
picor nasal, pérdida de olfato, RASP: 0-3), endoscopia nasal (Lildholdt: 0-
3) , TC nasosinusal (Lund&Mackay: 0-24), TC pulmonar de alta resolución
(0-18), función nasal (rinomanometría: cm3/sec.; rinometría acústica: ATM,
cm2; Volumen: cm3) /pulmonar (espirometría: l) y NO nasal (ppb) y
exhalado (ppb).
Resultados: la mayoria de los pacientes (n=68; 77%) con bronquiectasias
en fase estable cumplieron criterios EP3OS para RSC, presentando como
síntomas nasales predominantes: rinorrea anterior (98,5%) y rinorrea
posterior (91%) y obstrucción nasal (90%). Además, la pérdida de olfato
fué uno de los síntomas más frecuentes (77,2%) en los pacientes con RSC
con pólipos. El tamaño de los pólipos fué de leve a moderado (1,6±0,1)
encontrándose en el 25% de los pacientes. Los pacientes con RSC
presentaron en la TC una mayor frecuencia de ocupación de los senos

III. Trabajo Experimental Tesis Doctoral
106
maxilares, etmoidales y complejo ostiomeatal (puntuación total: 8,4±0,4).
También se observó una mayor afectación en la rinomanometría entre los
pacientes con (590±37 cm3/s) y sin RSC (854±81,5 cm3/s), y en la
rinometría acústica entre los pacientes con RSC, con o sin pólipos nasales.
El óxido nítrico nasal está disminuido en los pacientes con RSC con
pólipos (347±62 ppb; p<0,001) comparado con los que no tienen pólipos
(683±76 ppb). Se observó una correlación inversa entre la puntuación del
complejo ostiomeatal y el NO nasal (R= -0,36; p<0,01). El óxido nítrico
exhalado está incrementado en los pacientes con poliposis nasal (11,1±2
ppb), pero sin significancia estadística. A nivel sistémico, la PCR está más
elevada en los paciente que cumplen criterios de rinosinusitis crónica. Los
pacientes con RSC (7,2±0,5; p<0,001) presentan un mayor índice de
extensión de BQs que los pacientes sin RSC (3,7±0,7). La prevalencia de
patología nasosinusal es similar entre los pacientes con bronquiectasias de
origen postinfeccioso e idiopático.
Conclusiones: Los pacientes con BQs presentaron una alta prevalencia de
rinosinusitis crónica (77%) y poliposis nasal (25%). La PCR está
significativamente elevada en los pacientes con RSC comparada con los
pacientes sin patología nasosinusal. Los pacientes con BQs, los senos
maxilares y los etmoidales, junto a obliteración del complejo ostiomeatal
fueron los más afectados entre los pacientes con RSC con o sin pólipos,
mientras que los pacientes con RSC sin PN tienen una puntuación total
inferior en la TC nasosinusal que los pacientes con RSC con PN.
La gravedad de las BQs se relaciona con la presencia de RSC o PN.
Los pacientes con RSC presentaron una mayor afectación pulmonar
evaluada mediante la TC pulmonar de alta resolución en comparación con
los pacientes sin RSC, sin existir diferencias entre pacientes con o sin PN.

Tesis Doctoral III. Trabajo Experimental
107
La prevalencia de RSC y de PN es alta en los pacientes con BQs,
independientemente de que la causa sea post-infecciosa o idiopática.
El ON nasal está disminuido en los pacientes con RSC con PN y su
valor disminuye conforme aumenta la afectación del complejo ostiomeatal.
Las concentraciones de ON nasal fueron similares en los diferentes grupos,
excepto en los pacientes con PN, en los cuales el NO nasal se encontró en
concentraciones menores que en los pacientes sin RSC y sin pólipos.
También se observó que el ON nasal estaba más bajo conforme aumentaba
la puntuación del complejo ostiomeatal en la TC nasosinusal.
Conclusión general: los pacientes con BQs deberían ser evaluados
siempre a fin de descartar una RSC con o sin pólipos, y a su vez los
pacientes con RSC con o sin pólipos deberían ser estudiados para
enfermedades de la vía aérea inferior, incluyendo BQs.


Tesis Doctoral III. Trabajo Experimental
109
Estudio 2: The impact of bronchiectasis associated to sinonasal disease
on quality of life. Respir Med 2006;100:1997-2003. DOI: 10.1016/j.rmed.2006.02.016
Introducción: los pacientes afectos de BQs se caracterizan por presentar
tos productica crónica lo cual supone un empeoramiento de su calidad de
vida. No se han realizado estudios sobre la afectación de la calidad de vida
en pacientes con BQs y patologia nasosinusal.
Objetivos: se estudió si los pacientes afectos de bronquiectasias con
patología a nivel nasal presentan una peor calidad de vida comparado con
la población general española utilizando un cuestionario genérico de
calidad de vida (SF-36).
Métodos: se incluyeron 60 pacientes con BQs y patología nasosinusal que
fueron evaluados por: síntomas nasales (obstrucción, rinorrea anterior,
rinorrea posterior, dolor facial, estornudos, picor nasal, pérdida de olfato;
RASP: 0-3), tamaño de los pólipos (Lildholdt: 0-3) y calidad de vidad (SF-
36: 0-100).
Resultados: La edad media de los pacientes con BQs fué de 52±16 años
(rango: 18-78 años). 39 pacientes (65%) fueron mujeres. Los pacientes con
BQs presentaban predominantemente rinorrea anterior (1,9±0,9) y posterior
(1,8±0,9), pérdida del olfato (0,9±1), obstrucción nasal (1,65±0,9) y
estornudos (1,2±1). Veinticinco pacientes (41,6%) con BQs presentaban
pólipos nasales en la endoscopia con un tamaño medio de Lildholdt:
1,5±0,4 (rango:1–2). Los pacientes con BQ y PN tenían puntuaciones
mayores (P<0,05) de obstrucción nasal (2,05±0,8) y pérdida del olfato
(1,4±1) que los pacientes con BQs sin pólipos (1,4±0,8; 0,5±0,8)
respectivamente. En comparación con la población general española, los
pacientes con BQs presentaban peor calidad de vida en todos los dominios
del SF-36 (Función física: 90,3±17,1 vs. 76±22; Rol físico: 87,6±30,4 vs.
III. Trabajo Experimental Tesis Doctoral
110
71±42; Dolor corporal: 81,9±26 vs. 62,3±24,9; Salud general: 70,9±19,6
vs. 35,5±18; Vitalidad: 71,6±21 vs. 48,7±17,3; Rol emocional: 94,6±21,8
vs. 71,3±42,5; Función social: 94,1±15,6 vs. 75,2±28,3; Salud mental:
77,7±18,7 vs. 65,4±21,4; Sumario físico: 82,7±23,3 vs. 46,5±26,7; Sumario
mental: 84,5±19,3 vs. 39,7±27,3). No existen diferencias significativas
entre la calidad de vida de los pacientes con BQs con o sin PN.
Las mujeres mostraron peor función física (diferencia: 13,1; P<0,05
y 95%IC: 1,7–24,5) y peor función social (diferencia: 15,7; P<0,05 y
95%IC: 0,4–31) que los hombres. Las mujeres con BQs tenían peores
puntuaciones de calidad de vida (P<0,05) que las mujeres de la población
general española en la función física, dolor corporal, salud general,
vitalidad, función social y el rol emocional. Los hombres también
mostraron peores puntuaciones de calidad de vida (P<0,05) que los
hombres de la población general española en el dolor corporal, salud
general y vitalidad. No existen diferencias significativas entre mujeres y
hombres en cuanto a la edad, función pulmonar, presencia de pólipos
nasales, síntomas nasales, tabaco y duración de la enfermedad.
Los pacientes mostraron una VEMS% de 81±3,4. No existía
correlación entre los 2 sumarios de calidad de vida y la función pulmonar:
SF (r: 0,21; P=0,242) y SM (r: 0,095; P=0,599).
Conclusiones: en comparación con la población general española, los
pacientes afectos de BQs presentaron peor puntuación (p<0,05) en todos
los dominios del SF-36. Los hombres presentaron puntuaciones más altas
en función física y social que las mujeres. La afectación en la calidad de
vida resultó ser independiente de la edad, función pulmonar, síntomas
nasales, tabaquismo y duración de la enfermedad. En el sexo masculino, los
pacientes con BQs presentaron peor calidad de vida que los de la población
general española en dolor corporal, salud general y vitalidad. En el sexo
femenino, las pacientes con BQs presentaron peor calidad de vida que las

Tesis Doctoral III. Trabajo Experimental
111
de la población general española, además de los dominios anteriores, en
función física, función social y rol emocional.
Conclusión general: estos resultados sugieren que las BQs con RSC
producen una importante impacto en la calidad de vida, sin que exista un
impacto adicional en los pacientes con RSC y pólipos nasales.


Tesis Doctoral III. Trabajo Experimental
113
Estudio 3. United airways: the impact of chronic rhinosinusitis and nasal
polyps in bronchiectasic patient’s quality of life. Allergy 2009;64:1524-9. DOI:10.1111/j.1398-9995.2009.02011.x
Introducción: resultados anteriores sugieren que las BQs con RSC
producen una importante impacto en la calidad de vida, sin que exista un
impacto añadido en los pacientes con RSC y pólipos nasales. No obstante,
no se han realizado estudios comparativos sobre calidad de vida en
pacientes con BQs con o sin patologia nasosinusal.
Objetivos: se evaluó el impacto de la CRS con o sin pólipos en la calidad
de vida de los pacientes con BQs, y a su vez si existía correlación en la
calidad de vida entre la vía aérea superior e inferior y a nivel general.
Métodos: se estudiaron prospectivamente 80 pacientes con BQs, de los
cuales 60 presentaban RSC según los criterios EP3OS. Los pacientes
realizaron cuestionarios de calidad de vida específicos de vía superior
(SNOT-20), de vía inferior (SGRQ) y genéricos (SF-36).
Resultados: los pacientes con RSC presentaron unos valores superiores del
SNOT-20 total (2,1±0,1; p<0,001) que los pacientes sin patología nasal
(0,4±0,06). Los pacientes con RSC presentaron también valores superiores
del SGRQ total (43,7±2,2; p<0,001) que los pacientes sin patología
nasosinusal (24,7±2,5). En el SF-36, los pacientes con RSC presentaron
una peor calidad de vida tanto en el sumario mental (65,5±4,7; p<0,05)
como en el físico (64±3,4; p<0,05) en comparación a los pacientes sin
patología nasosinusal (SM: 78,3±5,3; SF: 76,2±3,3; respectivamente). La
puntuación total del SNOT-20 se correlacionó tanto con la puntuación total
del SGRQ (r:0,72; p<0,01) como con el componente físico del SF-36 (r:-
0,63; p<0,01). La puntuación total del SGRQ se correlacionó con el
componente físico del SF-36 (r:-0,58; p<0,05) y con el VEMS (r:-
0,41;p<0,05).

III. Trabajo Experimental Tesis Doctoral
114
Conclusiones: La RSC con o sin pólipos tiene un considerable impacto en
la calidad de vida de los pacientes con BQs. La puntuación global del
SNOT-20 en pacientes con BQ que presentaban criterios de RSC, con o sin
pólipos, fue de 2,1. A su vez, la puntuación en los pacientes con BQs sin
RSC fue de 0,4. Así pues, en nuestro estudio en la calidad de vida, no
existen diferencias medidas por SNOT-20 entre pacientes con RSC con o
sin pólipos.
Los pacientes con BQs mostraban una importante reducción de su
calidad de vida cuando presentaban RSC asociada, sin existir una
repercusión añadida por tener PN. En los pacientes afectados de EPOC con
síntomas nasales, no se ha observado ninguna correlación entre el SNOT-
20 y el SGRQ total, o alguno de sus dominios (impacto, actividades o
síntomas). Sin embargo, en los pacientes con BQ sí que hay correlación
entre el SNOT-20, el SGRQ y el SF-36, asociándose la intensidad de los
síntomas nasales con el empeoramiento de la calidad de vida tanto en el
SNOT-20 y el SGRQ como en el SF-36. Los pacientes con RSC con PN
presentaron una mayor pérdida de olfato que los pacientes con RSC sin PN,
pero sin provocar un empeoramiento de la calidad de vida de los pacientes
(SNOT-20, SGRQ, y SF-36).
Conclusión general: estos resultados sugieren que la RSC evaluada, tanto
mediante cuestionarios específicos como genéricos, tiene un considerable
impacto sobre la calidad de vida de los pacientes con BQs.
Tesis Doctoral III. Trabajo Experimental
115
Estudio 1. United airway again: high prevalence of rhinosinusitis and nasal
polyps in bronchiectasis. Allergy 2009;64:790-7. DOI: 10.111/j.1398-9995.2008.01892.x

Original article
United airways again: high prevalence of rhinosinusitis and nasal
polyps in bronchiectasis
Bronchiectasis (BQ) is a chronic bronchial disease with astructural derangement of the bronchial wall, withpermanent and irreversible destruction and dilatation,retained secretions and recurrent infections that causeinflammation, obstruction, damage of the lower airway,significant impact on health care and impairment of thequality of life (1, 2). BQ are a consequence of a variety ofdifferent diseases where infection and excessive mucousproduction appear to be the most important contributoryfactors. Although more than 50% of BQ cases are stillconsidered idiopathic, the study of contributing potentialcauses may have important implications for the manage-ment of the disease (3).Chronic rhinosinusitis (CRS) is an inflammatory dis-
ease of the nose and sinus mucosa that, despite differenthypotheses about its cause, remains poorly understood
(4). CRS has become one of the most common chronicdiseases (5), with studies reporting that in the generalpopulation up to 6% of subjects suffered from chronicnasal discharge (6). Nasal polyps (NP) are smooth, grape-like structures that arise from the inflamed nasal mucosa.NP usually occurs in association with CRS. Smelldisorders are more prevalent in patients with NP thanin CRS patients with no NP (7).
The recently coined concept �united airways�, alsoknown as �one airway, one disease�, maintains thatinflammatory processes of the upper and lower airwayoften co-exist and share common etiopathogenic mech-anisms. It has been mainly explored with reference toasthma and rhinitis. Epidemiological data indicate thatasthma and rhinitis frequently occur in the same patient.It has also been reported that the severity of rhinitis
Background: Although various relationships between the lower and upperairways have been found, the association of bronchiectasis with chronic rhin-osinusitis and nasal polyps has not been thoroughly evaluated. This study wasundertaken to examine the association of idiopathic and postinfective bronchi-ectasis with chronic rhinosinusitis and nasal polyposis.Methods: In a prospective study, 56 patients with idiopathic and 32 withpostinfective bronchiectasis were evaluated for chronic rhinosinusitis and nasalpolyposis by using EP3OS criteria and assessing: symptoms score, nasal endos-copy, sinonasal and chest CT scan, nasal and lung function and nasal andexhaled NO.Results: Most bronchiectasis patients (77%) satisfied the EP3OS criteria forchronic rhinosinusitis, with anterior (98.5%) and posterior (91%) rhinorrheaand nasal congestion (90%) being the major symptoms. Patients presentedmaxillary, ethmoidal and ostiomeatal complex occupancy with a total CT scoreof 8.4 ± 0.4 (0–24). Using endoscopy, nasal polyps with a moderate score of1.6 ± 0.1 (0–3) were found in 25% of patients. Nasal NO was significantlylower in patients with nasal polyposis (347 ± 62 ppb) than in those withoutthem (683 ± 76 ppb; P < 0.001), and inversely correlated (R = )0.36;P < 0.01) with the ostiomeatal complex occupancy. In the chest CT scan,patients with chronic rhinosinusitis showed a higher bronchiectasis severityscore (7.2 ± 0.5; P < 0.001) than patients without (3.7 ± 0.7). The prevalenceof chronic rhinosinusitis, nasal polyps and other outcomes were similar inidiopathic and postinfective bronchiectasis.Conclusions: The frequent association of chronic rhinosinusitis and nasalpolyposis with idiopathic and postinfective BQ supports the united airwaysconcept, and it suggests that the two type of bronchiectasis share commonetiopathogenic mechanisms.
J. M. Guilemany1,4, J. Angrill2,I. Alobid1,4, S. Centellas1,4,L. Pujols3,4, J. Bartra2,4,M. Bernal-Sprekelsen1,4, A. Valero2,4,C. Picado2,3,4, J. Mullol1,3,4
1Department of Otorhinolaryngology, Rhinology Unitand Smell Clinic; 2Department of Medicine,Pneumology and Respiratory Allergy, Hospital Cl�nic,University of Barcelona; 3Institut d�InvestigacionsBiom�diques August Pi i Sunyer (IDIBAPS); 4Centrode Investigaci�n Biom�dica en Red deEnfermedades Respiratorias (CIBERes), Barcelona,Catalonia, Spain
Key words: bronchiectasis; chronic rhinosinusitis; nasalpolyposis.
Joaquim MullolRhinology Unit & Smell ClinicDepartment of OtorhinolaryngologyHospital Cl�nic i Universitaric/ Villarroel 17008036 BarcelonaCataloniaSpain
Accepted for publication 4 August 2008
Allergy 2009: 64: 790–797 � 2009 The AuthorsJournal compilation � 2009 Blackwell Munksgaard
DOI: 10.1111/j.1398-9995.2008.01892.x
790

directly correlates with asthma severity. NP are alsofrequently associated with asthma. Over 84% of sino-nasal CT scans have been found to be abnormal in severeasthmatic patients, with a correlation between the CTscores, sputum eosinophilia and pulmonary function (8).In addition, both the medical and surgical treatments ofCRS and NP may benefit concomitant asthma (9).Upper airway symptoms are also frequent in patients
with chronic obstructive pulmonary disease (COPD) andcause impairment in patients� quality of life (10).Increased nasal inflammation has also been reported inCOPD patients (11). Patients with allergic and nonaller-gic asthma and COPD show increased nasal symptomsand more nasal inflammation (12).CRS and NP frequently occur in cystic fibrosis and
primary ciliary dyskinesia. Both are distinguish diseaseswith clear pathological mechanisms and with a conse-quence of pulmonary pathology due to recurrent airwayinfections (13). However, few studies have addressed thepotential co-morbidity between noncystic BQ and upperairway disease, including CRS and NP. We hypothesizethat, according to the �united airway� concept, mostso-called idiopathic bronchiectasis should be the conse-quence of a process affecting the entire airways, includingthe nose and the paranasal sinuses. In contrast, BQconsidered secondary to infectious insults of the lowerairways (postinfective BQ) usually occurring in early years,such as after pneumonia or in whooping cough, should notbe necessarily associatedwithCRS. If this hypothesis holdstrue, most patients with idiopathic bronchiectasis shouldsuffer from nasal and sinus diseases, and the severity ofCRS and bronchiectasis should also be correlated. Incontrast, in postinfective BQ, the upper airway shouldrarely be involved. To test this hypothesis, we: (1) examinedthe association of idiopathic and postinfective BQ andCRS with and without NP and (2) assessed the prevalenceof symptoms, sinusal occupancy, nasal polyp size, nasaland lung function and inflammation in patients with BQand concomitant CRS and NP.
Methods
Study subjects
Eighty-eight consecutive patients with idiopathic and postinfectiveBQ, diagnosed in the pneumology clinic, were included in a pro-spective study from April 2004–June 2006. The diagnosis of BQ wasperformed on the basis of characteristic clinical symptoms and CTscanning. The Ethics Committee of our institution approved thestudy and signed informed consent was obtained from all patients.
Diagnosis and extent of BQ
BQ predisposing factors were assessed: serum immunoglobulin (Ig),IgG, IgA, IgM, IgG subclasses, specific antibody response topneumococal antigens, alpha1-antitrypsin deficiency, cystic fibrosis(sweat test and genotyping), allergic bronchopulmonary aspergil-losis and ciliary dysfunction. A high resolution CT (HRCT) scan of
the chest was performed during the 3-month period prior to thesinonasal examination and the extent of BQ in each lobe was gra-ded, using a scale from 0 to 3 (0, no involvement; 1, segmentinvolved; 2, more than one segment involved and 3, gross cystic BQinvolving the entire lobe) (14). Forced spirometry was performedaccording to standard methods and percent-predicted FEV1
(FEV1%), FVC and FEV1/FVC was chosen for analysis, as previ-ously reported. Exhaled nitric oxide (eNO) was measured accordingto standardized methods (15).Postinfective BQ was diagnosed when the patient reported a
history of symptoms appearing immediately after a severe infection,such as pneumonia, tuberculosis or whooping cough. Idiopathic BQwas diagnosed when known causes of BQ had been ruled-out.
Diagnosis and extent of sinusitis and nasal polyps
Patients with BQ were evaluated for CRS and NP following EP3OSguidelines (4). The diagnosis of NP was based on the visualizationof nasal polyps under endoscopic examination. To characterize theinvolvement of upper airway disease in patients with BQ, the fol-lowing diagnostic tools were used: nasal symptom score, nasalendoscopy, sinonasal CT-scan, nasal function and nasal NO.Nasal congestion/obstruction/blockage, reduction or loss of the
sense of smell, anterior rhinorrhea, postnasal drip, facial pain/pressure, itching and sneezing were scored using the Rasp classifi-cation (0–3) (16). Polyp size was scored from 0 to 3 for each nasalcavity using nasal endoscopy, following Lildholdt�s classification(17). A radiologist blindly staged sinus occupation for each patient,using CT scanning and the Lund-MacKay score system (0–24) (18).Nasal airflow was measured by active anterior rhinomanometry andexpressed as the flow generated at a pressure of 150 Pa (cm3/s).Nasal volume within the distance of 6 cm from the nostrils (volume0–6 cm3) was measured using acoustic rhinometry, according to amethod previously reported (15). nNO was obtained from onenostril using a negative pressure pump with a flow rate of 3 l/min, asreported elsewhere (15).
Other studies
Skin prick testing to most common allergens, nasal eosinophilia,blood eosinophil counts and serum total and specific IgE levels werecarried out, using previously reported standard methods.
Statistical analysis
Data analysis and statistics were performed using spss for Windows(SPSS 12.0, Chicago, IL, USA). Comparisons between categoricalvariables used the Pearson�s v2 statistic (or the Fisher�s exact test forsmall samples). When comparing continuous variables with cate-gorical predictors, the Student�s t-test was used. Pearson correlationcoefficients were used to examine the association between gender,age, nasal symptoms, nasal polyps, CT opacification, lung function,nasal patency and nasal/exhaled nitric oxide. Values of P < 0.05were considered statistically significant.
Results
Demographic data
Fifty-six of the 88 patients (64%) were classified as havinga postinfective disease, while 32 (36%) were classified ashaving an idiopathic disease, of those one had an
Upper airway disease in bronchiectasis
� 2009 The AuthorsJournal compilation � 2009 Blackwell Munksgaard Allergy 2009: 64: 790–797 791

inflammatory bowel disease, and another rheumatoidarthritis. The mean age was 55 ± 2 years (ranging from21 years to 78 years), 6% were current smokers and 24%were ex-smokers. The mean age at BQ diagnosis was40 ± 2 years. Patients with NP (36.5 ± 5 years) werediagnosed with BQ earlier than patients with no sinonasalpathology (47 ± 4 years). Patients with CRS, 69% ofthem female, had a significantly higher female ratio(3 : 1), and this was even higher in patients with CRS-NP(5.6 : 1), compared to patients with no CRS (1 : 1)(Table 1).
Allergic and immunologic studies
C-reactive protein level was significantly increased inpatients with CRS (1.3 ± 0.2 mg/dl; P < 0.05) com-pared with patients with no CRS (0.6 ± 0.2 mg/dl). Themain allergic and immunologic characteristics aredescribed and compared with normal values in Table 2.No significant differences between groups (including CRSvs No CRS) were found.
Lung function
Mean FEV1 was 83 ± 3% predicted. FEV1 in patientswith CRS (81 ± 3%) was lower than in those with noCRS (90 ± 4%) but the difference did not reach statis-tical significance (P = 0.06). No other differences werefound in spirometry between groups, and no correlationwas observed with nasal symptoms, nasal polyposis orCT scores (Table 1).
Chest CT-scan
Patients with CRS (7.2 ± 0.5; P < 0.001) showed ahigher BQ severity score than patients with no CRS(3.7 ± 0.7) (Fig. 1). No differences were observedbetween patients with and without NP.
Sinonasal symptoms
Seventy-seven percent of patients fulfilled the EP3OScriteria for CRS. Anterior rhinorrhea (89%), postnasaldrip (77%) and nasal congestion (77%) were scored bypatients as major complaints, while sneezing (59%), facialpain (40%), reduction/loss of smell (39%) and itching(36%) were less frequent. Patients with CRS reportedanterior rhinorrhea (98.5%), postnasal drip (91%) andnasal congestion (90%), with significant differences(P < 0.001) in all symptoms except sneezing, comparedto patients with no CRS. Patients with CRS hadsignificant higher scores (P < 0.001) in total symptom
Table 1. Epidemiological characteristics of BQ patients included in the study
All BQ patients No CRS CRS CRS without NP CRS with NP ID PI
Patients, n (%) 88 20 (23) 68 (77) 46 (52) 22 (25) 32 (37) 56 (63)Age (years)� 55 € 2 59 € 3 54 € 2 56 € 2 49 € 4* 53 € 3 58 € 1BQ age diagnosis (years)� 40 € 2 47 € 4 38 € 2.5 39 € 3 36.5 € 5* 45 € 3 40 € 3Female (%) 69 50 75* 87* 50** 84* 68F/M ratio 2.3 : 1 1 : 1 3 : 1 5.6 : 1 1 : 1 5.2 : 1 2.1 : 1Smoking habit
Ex-smokers (%) 24 50 16 13 23 16 26Smokers (%) 6 0 7 9 4.5 7 5Packs/year� 23 € 3 25.5 € 5 22 € 4 20 € 4 27 € 9 22.5 € 3 25 € 4
Lung functionFEV1 (%)� 83 € 3 90 € 4 81 € 3 81 € 4 80 € 6 85 € 5 82.5 € 3FEV1/FVC (%)� 93 € 1.5 96 € 3 92 € 2 92 € 2 92 € 3.5 93.3 € 4 93.3 € 2
BQ, bronchiectasis; CRS, chronic rhinosinusitis; NP, nasal polyposis; ID, idiopathic BQ; PI, postinfectious BQ; SEM, standard error of the mean; M, male; F, female; FEV1, forcedexpiratory volume at 1 s; FVC, forced vital capacity. Unpaired Student�s t-test: *P < 0.05, compared to CRS– patients; **P < 0.05, compared to patients with CRS without NP.�Data presented as mean € SEM.
Table 2. Allergic and immunologic outcomes of BQ patients
BQ patients Normal values
OutcomesPositive nasal eosinophilia, n (%) 3 <1�Positive skin prick test to allergen, n (%) 20 20–30�Positive prick test to moulds, n (%) 9 6–12�Positive Aspergillus recombinant
allergens, n (%)3 Not described
Positive IgE to mould, n (%) 7 Not describedBlood eosinophils (%)� 3.5 € 0.3 <5�Blood eosinophils (cells/vol)� 0.26 € 0.02 <0.5�Positive AspergillusPrecipitins (%) 4.5 Not described
ImmunoglobulinsIgE (KU/l) 114 € 23 <100IgA (g/l) 2.341 € 119 0.66–3.650IgM (g/l) 1.352 € 179 0.36–2.610IgG (g/l) 11.519 € 367 6.800–15.300IgG1 (g/l) 7.186 € 260 4.900–11.400IgG2 (g/l) 3.537 € 156 1.500–6.400IgG3 (g/l) 0.51 € 0.03 0.2–1.100IgG4 (g/l) 0.67 € 0.08 0.08–1.400
�Normal values in the Spanish general population from Alergol�gica 2006 (32).�Data presented as mean € SEM.
Guilemany et al.
� 2009 The Authors792 Journal compilation � 2009 Blackwell Munksgaard Allergy 2009: 64: 790–797

score (8.4 ± 0.4), especially for anterior rhinorrhea(1.9 ± 0.1), postnasal drip (1.8 ± 0.1) and nasalobstruction (1.6 ± 0.1), than patients with no CRS.
Patients with NP reported more reduction/loss of smell(77%; P < 0.001) compared to patients with no NP(30%), as well as higher total symptom scores, nasalobstruction and itching (Fig. 2).
Nasal polyp size
By nasal endoscopy, 22 patients (26%) with BQs hadmild-moderate nasal polyps (1.6 ± 0.1), of whom only32% of patients with NP had previously been diagnosed.The diagnosis of BQs had been performed 9 years earlierin patients with CRS (38 ± 2.5 years) than in thosewithout CRS (47 ± 4 years).
Sinusal occupancy
CT scan was affected in 66 patients (86%), with a score of6.6 ± 0.5, and a predominance of maxillary sinus(1.8 ± 0.1), ostiomeatal complex (1.7 ± 0.2) and ante-rior ethmoid sinus (1.5 ± 0.1). Patients that fulfilled theEP3OS criteria of CRS showed a total CT score of8.4 ± 0.4 (Fig. 3).
Che
st C
T-sc
an s
core
0
2
4
6
8
10
12
14
16
18
CRS – CRS + CRS – CRS +
Idiopathic Post-infectious
P < 0.001
*** ***
P < 0.001
Figure 1. Chest HRCT scan score (BQ severity) in patients withidiopathic or postinfectious bronchiectasis without (CRS–) andwith (CRS+) chronic rhinosinusitis. Unpaired Student�s t-test:***P < 0.001 compared to CRS– patients.
A B C
D E F
* * * * * *
* * * * * * * * * * * *
* * * * * *
* * *
P < 0.001
3 3
2 2 * * * * * *
* * *
* * *
P < 0.01 P < 0.001
Sco
re (
0 -
3)
Sco
re (
0 -
3)
0
1
0
1
3
2
Sco
re (
0 -
3)
0
1
3
2
Sco
re (
0 -
3)
0
1
3
2
Sco
re (
0 -
3)
0
1 6
9
12
15
Sco
re (
0 -
15)
0
3
* * * * * * * * *
All CRS– CRS+ NP– NP+ All CRS– CRS+ NP– NP+ All CRS– CRS+ NP– NP+
All CRS– CRS+ NP– NP+ All CRS– CRS+ NP– NP+ All CRS– CRS+ NP– NP+
Figure 2. Nasal symptom scores (Table 1in patients with bronchiectasis without (CRS–) and with (CRS+) chronic rhinosinusitis,and without (NP–) or with (NP+) nasal polyposis. (A) Total symptom score (TSS5), (B) anterior rhinorrhea, (C) postnasal drip, (D)nasal congestion/blockage, (E) loss of sense of smell and (F) facial pain/pressure. Unpaired Student�s t-test: *P < 0.05, **P < 0.01,***P < 0.001, compared to CRS– patients.
Upper airway disease in bronchiectasis
� 2009 The AuthorsJournal compilation � 2009 Blackwell Munksgaard Allergy 2009: 64: 790–797 793

Patients with CRS mainly presented maxillary andethmoid opacification. Patients with CRS reported signif-icantly higher CT scores (P < 0001) than patients withoutCRS in: total score (8.4 ± 0.4 vs 0.7 ± 0.2), maxillary(2.1 ± 0.1 vs 0.4 ± 0.1), ostiomeatal complex (2.2 ± 0.2vs 0), anterior ethmoid (1.9 ± 0.1 vs 0.1 ± 0.1), posteriorethmoid (0.8 ± 0.1 vs 0.1 ± 0), frontal (0.5 ± 0.1 vs0.1 ± 0.1) and sphenoid (0.8 ± 0.1 vs 0) sinuses.Patients with NP presented significantly higher CT
scores (P < 0.05) than patients with no NP in: total score(10.8 ± 0.7 vs 7.3 ± 0.4), ostiomeatal complex(3.1 ± 0.2 vs 1.8 ± 0.2), posterior ethmoid (1.2 ± 0.2vs 0.7 ± 0.1), frontal (1 ± 0.2 vs 0.3 ± 0.1) andsphenoid (1.2 ± 0.2 vs 0.7 ± 0.1) sinuses.
Nasal function
Using anterior rhinomanometry, patients with CRSshowed a greater nasal obstruction (590 ± 37 cm3/s)compared to those with no CRS (854 ± 81.5 cm3/s;P < 0.01) (Fig. 4A) Acoustic rhinometry carried out onpatients with NP showed a significantly lower nasalvolume (13 ± 0.7 cm3) than those with no CRS(15 ± 0.8 cm3, P < 0.05) (Fig. 4B).
Inflammation markers
nNO was significantly lower in patients with NP(347 ± 62 ppb) compared to those with no CRS(683 ± 76 ppb, P < 0.001) and CRS with no NP(620 ± 47 ppb) (Fig. 4C). Nasal NO was inversely cor-related with the occupancy of the ostiomeatal complex
(R = )0.36; P < 0.01) in patients with NP. No differ-ences between groups were found on exhaled NOproduction (Fig. 4D).
CRS and nasal polyps in idiopathic vs postinfective bronchiectasis
We were interested in contrasting the results of patientswith postinfective with those classified as idiopathic. Nosignificant differences were observed between patientsdiagnosed with idiopathic and postinfective BQs, intotal symptoms score (6.9 ± 0.8 vs 7 ± 0.5), nasalpolyp prevalence (25% vs 25%) and the sinonasaloccupancy, as detected by the CT score (6.7 ± 1.1 vs6.0 ± 0.5). The only exception was olfaction, whichwas more affected in idiopathic bronchiectasis(1.08 ± 0.2 vs 0.5 ± 0.1). No significant differencesbetween idiopathic and postinfective BQs were found inallergic and immunologic studies, lung function, chestCT-scan, nasal function and inflammation markers(data not shown).
Discussion
The main findings of the present study are: (1) there is ahigh prevalence of CRS (77%) and NP (26%) in BQpatients (postinfective and idiopathic), (2) the severity ofBQ is related to the presence of CRS and NP, (3) thepercentage of patients with CRS and NP is similar inpostinfective and idiopathic BQ and (4) nasal NO isinversely correlated to the severity of CRS and thepresence of NP.
9
12
15A
E F G
B C D
* * *
* * * * * * * * *
* * * * * *
* * * * * *
* * *
* * *
* * * * * *
P < 0.001 P < 0.001
Sco
re (
0 -
15)
0
3
6
2
3
4
* * *
P < 0.05 P < 0.05 P < 0.01
Sco
re (
0 -
4)
0
1
2
3
4
Sco
re (
0 -
4)
0
1
2
3
4
Sco
re (
0 -
4)
0
1
2
3
4
Sco
re (
0 -
4)
0
1
2
3
4
Sco
re (
0 -
4)
0
1
2
3
4
Sco
re (
0 -
4)
0
1
All CRS– CRS+ NP– NP+ All CRS– CRS+ NP– NP+ All CRS– CRS+ NP– NP+
All CRS– CRS+ NP– NP+ All CRS– CRS+ NP– NP+ All CRS– CRS+ NP– NP+ All CRS– CRS+ NP– NP+
* * * * * * * * *
* * *
* * *
* *
* * * * * *
Figure 3. Sinonasal CT occupancy in patients with bronchiectasis without (CRS–) and with (CRS+) chronic rhinosinusitis, andwithout (NP–) and with (NP+) nasal polyposis. (A) Total CT score, (B) maxillary sinus, (C) ostiomeatal complex, (D) anteriorethmoid sinus, (E) posterior ethmoid sinus, (F) sphenoid sinus and (G) frontal sinus. Unpaired Student�s t-test: **P < 0.01,***P < 0.001, compared to CRS– patients.
Guilemany et al.
� 2009 The Authors794 Journal compilation � 2009 Blackwell Munksgaard Allergy 2009: 64: 790–797
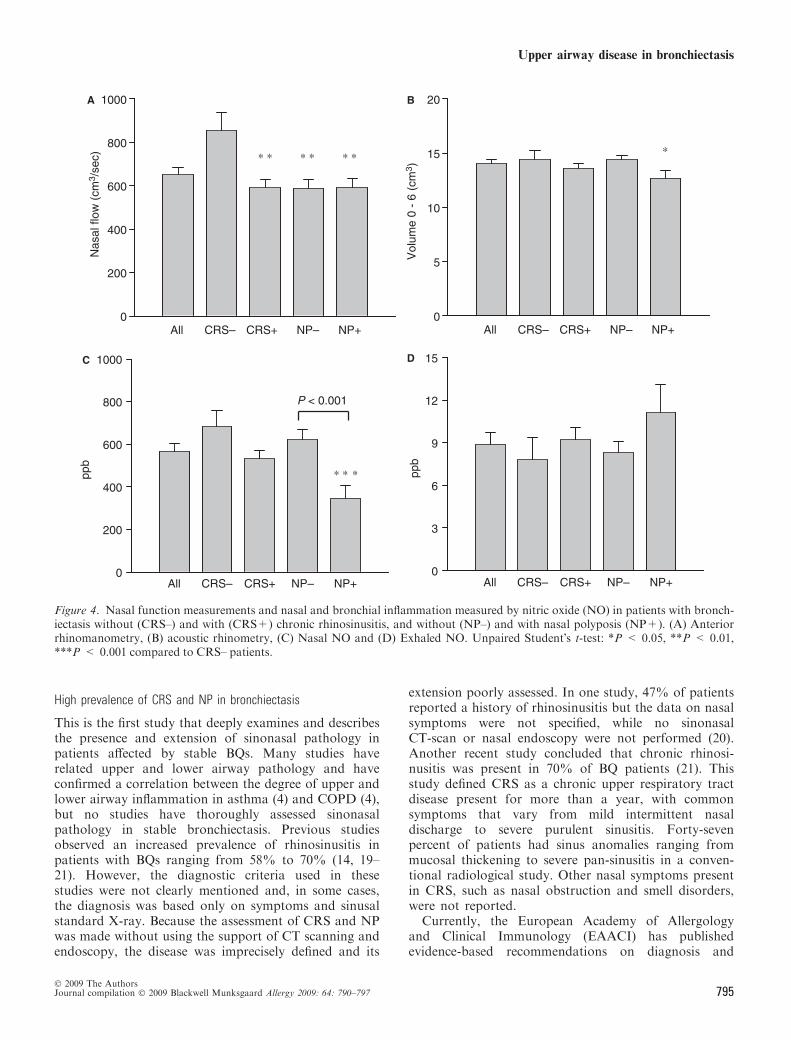
High prevalence of CRS and NP in bronchiectasis
This is the first study that deeply examines and describesthe presence and extension of sinonasal pathology inpatients affected by stable BQs. Many studies haverelated upper and lower airway pathology and haveconfirmed a correlation between the degree of upper andlower airway inflammation in asthma (4) and COPD (4),but no studies have thoroughly assessed sinonasalpathology in stable bronchiectasis. Previous studiesobserved an increased prevalence of rhinosinusitis inpatients with BQs ranging from 58% to 70% (14, 19–21). However, the diagnostic criteria used in thesestudies were not clearly mentioned and, in some cases,the diagnosis was based only on symptoms and sinusalstandard X-ray. Because the assessment of CRS and NPwas made without using the support of CT scanning andendoscopy, the disease was imprecisely defined and its
extension poorly assessed. In one study, 47% of patientsreported a history of rhinosinusitis but the data on nasalsymptoms were not specified, while no sinonasalCT-scan or nasal endoscopy were not performed (20).Another recent study concluded that chronic rhinosi-nusitis was present in 70% of BQ patients (21). Thisstudy defined CRS as a chronic upper respiratory tractdisease present for more than a year, with commonsymptoms that vary from mild intermittent nasaldischarge to severe purulent sinusitis. Forty-sevenpercent of patients had sinus anomalies ranging frommucosal thickening to severe pan-sinusitis in a conven-tional radiological study. Other nasal symptoms presentin CRS, such as nasal obstruction and smell disorders,were not reported.
Currently, the European Academy of Allergologyand Clinical Immunology (EAACI) has publishedevidence-based recommendations on diagnosis and
600
800
1000C D
P < 0.001
ppb
ppb
200
400* * *
0
9
12
15
3
6
0All CRS– CRS+ NP+NP–All CRS– CRS+ NP+NP–
600
800
1000A B
* * * * * *
Nas
al fl
ow (
cm3 /
sec)
200
400
0
15
20
*
Vol
ume
0 -
6 (c
m3 )
5
10
0All CRS– CRS+ NP+NP–All CRS– CRS+ NP+NP–
Figure 4. Nasal function measurements and nasal and bronchial inflammation measured by nitric oxide (NO) in patients with bronch-iectasis without (CRS–) and with (CRS+) chronic rhinosinusitis, and without (NP–) and with nasal polyposis (NP+). (A) Anteriorrhinomanometry, (B) acoustic rhinometry, (C) Nasal NO and (D) Exhaled NO. Unpaired Student�s t-test: *P < 0.05, **P < 0.01,***P < 0.001 compared to CRS– patients.
Upper airway disease in bronchiectasis
� 2009 The AuthorsJournal compilation � 2009 Blackwell Munksgaard Allergy 2009: 64: 790–797 795

treatment: the EP3OS consensus (4). Clinical symptoms,endoscopic signs and/or CT changes persisting morethan 12 weeks define CRS, including nasal polyps. Inour study, 98% of patients with bronchiectasispresented nasal symptoms. Patients with BQs pre-sented anterior rhinorrhea, postnasal drip and nasalblockage as the major complaints, in accordance withthe major symptoms reported in EP3OS. An importantendoscopic sign, observed in more than 60% ofpatients, was mucous discharge from the middlemeatus. Using EP3OS criteria, 77% of patients withBQ presented CRS, while 25% presented mild tomoderate NP.C-reactive protein level was significantly increased in
patients with CRS, compared with patients with no CRS.Patients with NP were diagnosed with BQs more than10 years earlier than patients with no sinonasal pathol-ogy. Maxillary and ethmoid sinuses were mostly affectedin patients with CRS, either with or without NP, whilepatients with no NP had significant lower scores in CTthan patients with NP. Chest imaging (HRCT) is thegold-standard method for diagnosing BQ (22), and in ourstudy patients with CRS presented a significant increasein BQ imaging score, with no differences between CRS,with or without NP.All in all, these findings suggest that the presence of
CRS and NP in a patient with BQ is a marker of a moreactive and extended airway inflammatory process.
CRS and NP occur with similar frequency in idiopathic andpostinfectious bronchiectasis
A number of bronchiectasis is commonly consideredpostinfectious, mostly on the basis of a previous historyof severe pulmonary infections preceding the symptomsof bronchiectasis and radiological abnormalities. How-ever, the existence of either permanent bronchialdilatations before the infective episode or a defectivedefensive mechanism that precedes and/or accounts forboth the infective episode and the posterior develop-ment of bronchiectasis cannot be excluded as the originof some of these supposedly postinfective BQs. Weassumed that in the case of bronchiectasis resultingfrom a direct injury to the lower airways, the upperairways should remain preserved from any nasal andsinusal process. Conversely, and according to the unitedairway theory, most idiopathic BQs resulting from asyet unknown airway defensive or metabolic deficiencyshould be associated with upper airway diseases. Sincewe could not find significant differences between post-infectious and idiopathic bronchiectasis, in either theprevalence or the extension of CRS and NP, our resultssuggest that most of BQs considered as secondary todirect infectious injuries of the lower airways sharecommon mechanisms with idiopathic BQs.Nasal NO is inversely correlated to the occupation of
the ostiomeatal complex. In asthma patients, the ethmoi-
dal sinus is the most severely involved when CRS ispresent (23), while in our study, BQ patients show apredominant maxilo-ethmoidal involvement withobstruction of the ostiomeatal complex.
In healthy upper airways, nitric oxide is continuouslygenerated and secreted by the maxillary sinus through theostiomeatal complex and then diffuses into the nasalcavities (24). The ostiomeatal complex is a functional unitthat comprises maxillary sinus ostia, anterior ethmoidcells and their ostia, ethmoid infundibulum, hiatussemilunaris and middle meatus. NO has antiviral andantibacterial properties and plays a major role in innateimmunity.
It is known that nasal NO is increased in allergicrhinitis but the data on CRS and NP are controversial(25). A previous study found lower levels of nNO in CRSpatients than in healthy controls (26). Other studies alsoshow that nasal NO levels are inversely correlated withthe extent of NP, possibly related to the blockage of theostiomeatal complex (27, 28). nNO levels have also beenshown to inversely correlate with both the extent of theCT scan and the number of occluded paranasal sinuses(25, 27). In our study, nasal NO concentrations did notdiffer between groups, except in patients with NP, inwhom the nNO was found at lower concentrations, withan inverse correlation with the ostiomeatal complex CTscore.
Kharitonov et al. (29) have reported increased exhaledNO concentrations in BQ, in contrast with findings inother studies (30, 31). Our results concur with thosereporting no increase in exhaled NO in BQ.
In summary, almost four out of five patients with BQ(77%) presented criteria for CRS, and one out of everyfour patients had NP at nasal endoscopy (25%). Theseresults support the �united airways� concept and suggestthat most of the so-called postinfective bronchiectasisprobably result from as yet unknown processes thataffect the entire airways, rather than being the conse-quence of an injury (postinfectious and others) specifi-cally affecting only the lower airways. Finally, ourfindings also suggest that patients with BQ shouldalways be evaluated for CRS and NP, while patientswith CRS and NP should also be assessed for lowerairway diseases, including BQ.
Acknowledgments
Josep M Guilemany has been supported by the National Plan forScientific Research, Development and Technologic Innovation ofthe Health�s Institute Carlos III – Health Research Fund (CM06/00071), and the Spanish Society of Oto-Rhino-Laryngology, Head& Neck Pathology. The study has been partially sponsored by theFundacio Catalana de Pneumologia (FUCAP). Josep M Guilemanyand co-workers were awarded with the first prize on JMA posterpresentation for this study during the annual EAACI congress heldin Goteborg on June 2007.
Guilemany et al.
� 2009 The Authors796 Journal compilation � 2009 Blackwell Munksgaard Allergy 2009: 64: 790–797

References
1. Barker AF. Bronchiectasis. N Engl JMed 2002;346:1383–1393.
2. Guilemany JM, Alobid I, Angrill J,Ballesteros F, Bernal-Sprekelsen M,Picado C et al. The impact of bronchi-ectasis associated to sinonasal disease onquality of life. Respir Med 2006;100:1997–2003.
3. King P, Holdsworth S, Freezer N,Holmes P. Bronchiectasis. Intern Med J2006;36:729–737.
4. Fokkens W, Lund V, Mullol J, BachertC, Cohen N, Cobo R et al. EP3OS 2007:European position paper on rhinosi-nusitis and nasal polyps. Rhinology2007;20:1–136.
5. Kaliner MA, Osguthorpe JD, FiremanP, Anon J, Georgitis J, Davis ML et al.Sinusitis: bench to bedside. Currentfindings, future directions. J Allergy ClinImmunol 1997;99:s829–s848.
6. Gordts F, Clement PAR, Buisseret T.Prevalence of sinusitis signs in a non-ENT population. Otorhinolaringology1996;58:315–319.
7. Benitez P, Alobid I, de Haro J,Berenguer J, Bernal-Sprekelsen M,Pujols L et al. A short course of oralprednisone followed by intranasalbudesonide is an effective treatment ofsevere nasal polyps. Laryngoscope2006;116:770–775.
8. ten Brinke A, Grootendorst DC,Schmidt JT, De Bruine FT, van BuchemMA, Sterk PJ et al. Chronic sinusitis insevere asthma is related to sputumeosinophilia. J Allergy Clin Immunol2002;109:621–626.
9. Alobid I, Benıtez P, Bernal-SprekelsenM, Roca J, Alonso J, Picado C et al.Nasal polyposis and its impact onquality of life. Comparison between theeffects of medical and surgical treat-ments. Allergy 2005;60:452–458.
10. Haave E, Hyland ME, Skumlien S. Therelation between measures of healthstatus and quality of life in COPD.Chron Respir Dis 2006;3:195–199.
11. Roberts NJ, Lloyd-Owen SJ, Rapado F,Patel IS, Wilkinson TM, Donaldson GCet al. Relationship between chronicnasal and respiratory symptoms inpatients with COPD. Respir Med 2003;97:909–914.
12. Hens G, Vanaudenaerde BM, BullensDM, Piessens M, Decramer M, DupontLJ et al. Allergy 2008;63:261–267.
13. Guilemany JM, Mullol J, Picado C.Relation between rhinosinusitis andbronchiectasis. Arch Bronconeumol2006;42:135–140.
14. Angrill J, Agusti C, de Celis R, Rano A,Gonzalez J, Sole T et al. Bacterial col-onisation in patients with bronchiecta-sis: microbiological pattern and riskfactors. Thorax 2002;57:15–19.
15. Valero A, Serrano C, Valera JL,Barbera A, Torrego A, Mullol J et al.Nasal and bronchial response to exercisein patients with asthma and rhinitis: therole of nitric oxide. Allergy 2005;60:1126–1131.
16. Rasp G, Schuk A, Kastenbauer ER. Anew grading system for nasal polyps ofthe ethmoid bone. HNO-online 1996.http://www.link.springer.de/link//service//journals/00106.
17. Lildholdt T, Rundcrantz H, LindqvistN. Efficacy of topical corticosteroidpowder for nasal polyps: a double-blind,placebo-controlled study of budesonide.Clin Otolaryngol 1995;20:26–30.
18. Lund VJ, MacKay IS. Staging in rhino-sinusitus. Rhinology 1993;31:183–184.
19. King PT, Holdsworth SR, Freezer NJ,Villanueva E, Holmes PW. Characteri-sation of the onset and presenting clini-cal features of adult bronchiectasis.Respir Med 2006;100:2183–2189.
20. Pasteur MC, Helliwell SM, HoughtonSJ, Webb SC, Foweraker JE, CouldenRA et al. An investigation into causa-tive factors in patients with bronchiec-tasis. Am J Respir Crit Care Med2000;162:1277–1284.
21. Smith IE, Jurriaans E, Diederich S, AliN, Shneerson JM, Flower CD. Chronicsputum production: correlationsbetween clinical features and findings onhigh resolution computed tomographicscanning of the chest. Thorax 1996;51:914–918.
22. Judge EP, Dodd JD, Masterson JB,Gallagher CG. Pulmonary abnormali-ties on high-resolution CT demonstratemore rapid decline than FEV1 in adultswith cystic fibrosis. Chest 2006;130:1424–1432.
23. Hun-Jong D, Hyo Yeol K, Young-JunC, Tae Wook K, Joon Ho K, Seung-Kyu C et al. Computed tomographicassessment of chronic rhinosinusitis withasthma. Am J Rhinol 2006;5:450–452.
24. Lundberg JO, Rinder J, Weitzberg E,Lundberg JM, Alving K. Nasallyexhaled nitric oxide in humans origi-nates mainly in the paranasal sinuses.Acta Physiol Scand 1994;152:431–432.
25. Ragab SM, Lund VJ, Saleh HA,Scadding G. Nasal nitric oxide inobjective evaluation of chronic rhino-sinusitis therapy. Allergy 2006;61:717–724.
26. Lindberg S, Cervin A, Runer T. Nitricoxide (NO) production in the upperairways is decreased in chronic sinusitis.Acta Otolaryngol 1997;117:113–117.
27. Arnal JF, Flores P, Rami J, Murris-Espin M, Bremont F, Pasto I et al.Nasal nitric oxide concentration inparanasal sinus inflammatory diseases.Eur Respir J 1999;13:307–312.
28. Colantonio D, Brouillette A, Parikh A,Scadding GK. Paradoxical low nasalnitric oxide in nasal polyposis. Clin ExpAllergy 2002;32:698–701.
29. Kharitonov SA, Wells AU, O¢ConnorBJ, Cole PJ, Hansell DM, Logan-Sinclair RB et al. Elevated levels ofexhaled nitric oxide in bronchiectasis.Am J Respir Crit Care Med 1995;151:1889–1893.
30. Narang I, Ersu R, Wilson NM, Bush A.Nitric oxide in chronic airway inflam-mation in children: diagnostic use andpathophysiological significance. Thorax2002;57:586–589.
31. Foley SC, Hopkins NO, Fitzgerald MX,Donnelly SC, McLoughlin P. Airwaynitric oxide output is reduced in bron-chiectasis. Respir Med 2007;101:1549–1555.
32. Colas C, Chivato T, Dıaz de Rojas F,Lleonart R, Nieto A, Pelaez Aet al. Alergologica 2005. Factoresepidemiologicos, clınicos ysocioeconomicos de las enfermedadesalergicas en Espana en 2005 (SEAIC).Vol. 5. Madrid: ed. Luzan, 2006.
Upper airway disease in bronchiectasis
� 2009 The AuthorsJournal compilation � 2009 Blackwell Munksgaard Allergy 2009: 64: 790–797 797

Tesis Doctoral III. Trabajo Experimental
123
Estudio 2. The impact of bronchiectasis associated to sinonasal disease on
quality of life. Respir Med 2006;100:1997-2003. DOI: 10.1016/j.rmed.2006.02.016


ARTICLE IN PRESS
Respiratory Medicine (2006) 100, 1997–2003
0954-6111/$ - sdoi:10.1016/j.r
�CorrespondiE-mail addr
The impact of bronchiectasis associated tosinonasal disease on quality of life
J.M. Guilemanya,�, I. Alobida,b, J. Angrillc, F. Ballesterosa,M. Bernal-Sprekelsena, C. Picadoc, J. Mullola,d
aRhinology Unit, Department of Otorhinolaryngology, Hospital Clinic de Barcelona, ENT, Barcelona, SpainbDepartment of Otorhinolaryngology, Hospital Municipal de Badalona, Badalona, SpaincDepartment of Pneumology, Hospital Clınic, Department of Medicine, University of Barcelona, SpaindInstitut d’Investigacions Biomediques August Pi i Sunyer (IDIBAPS), Barcelona, Spain
Received 20 September 2005; accepted 19 February 2006
KEYWORDSBronchiectasis;Nasal polyposis;Quality of life;SF-36 questionnaire
ee front matter & 2006med.2006.02.016
ng author. Tel.: +34 932ess: [email protected]
SummaryBackground: Bronchiectasis (BQs) is an uncommon disease with the potential tocause devastating complications. All patients with BQs have cough and chronicsputum production that may have a great impact on patient’s quality of life. Upperairway symptoms are also frequent in patients with BQs. Associations between upperand lower airways diseases have been demonstrated in allergic rhinitis and asthma,nasal polyposis and asthma, chronic obstructive lung disease and chronicrhinosinusitis.Objective: (1) To investigate the impact of bronchiectasis and nasal symptoms onquality of life. (2) To evaluate the added impact of nasal polyposis on quality of lifein patients with BQs.Methods: Sixty patients with bronchiectasis and upper airway symptoms wereincluded. Patients were evaluated for nasal symptoms, nasal polyp size byendoscopy, and quality of life using the SF-36 generic questionnaire.Results: In comparison with the Spanish general population, patients with BQs hadworse scores in all SF-36 domains (Po0.05). Males reported significantly higherquality of life scores on physical functioning and social functioning than females did.Although the age, pulmonary function, presence of nasal polyps, upper airwaysymptoms, tobacco smoking history, and disease duration was similar between them.Males with BQs had worse quality of life than males from the Spanish generalpopulation on body pain, general health, and vitality (Po0.05). Females with BQshad worse quality of life than females from the Spanish general population onphysical function, body pain, general health, vitality, social function, and emotionalrole (Po0.05). Nasal polyps were found in 25 (41.6%) of 60 patients with BQs.
Elsevier Ltd. All rights reserved.
279 872; fax: +34 932 275 454.(J.M. Guilemany).

ARTICLE IN PRESS
J.M. Guilemany et al.1998
No significant differences were observed on quality of life outcomes betweenpatients with BQs with and without nasal polyposis.Conclusion: These results suggest that BQs has a considerable impact on quality oflife while nasal polyposis has no additional impact on the quality of life of patientswith BQs.& 2006 Elsevier Ltd. All rights reserved.
Introduction
Bronchiectasis (BQs) consists of a permanent andirreversible destruction and dilatation of bronchiand bronchioles due to retained secretions andrecurrent infections that cause inflammation, ob-struction, and damage of the lower airway. BQs area consequence of a variety of different diseaseswhere infection and obstruction appears to be themost important contributory factors. BQs arefrequently associated with cystic fibrosis, primaryciliary dyskinesia, immunodeficiency, rheumatoidarthritis, and inflammatory bowel disease.1
Nasal polyposis (NP) is a chronic inflammatorydisease of the nose and sinus mucosa that, despitediffering hypotheses of its cause, remains poorlyunderstood.2,3 NP can lead to progressive nasalobstruction, loss of smell, rhinorrhea, and sneez-ing. NP is frequently associated with asthma andother pulmonary disorders such as cystic fibrosis,primary ciliary dyskinesia, and aspirin sensitivity.4,5
BQs is a disease with the potential to causedevastating complications. The patients with BQshave cough and chronic sputum production thathave a great impact on patient’s quality of life(QoL). Most patients undergo slow and progressivehealth deterioration over decades. It can havedetrimental effects on physical, psychological, andsocial aspects of the patient0s life, significantlyworsening the patient’s QoL. The lung functiondoes not reflect the impact of the disease in thepatient0s health status and thus should be supple-mented using QoL questionnaires.6 However, theimpact of BQs to patients’ general health status hasnot been reported for the Spanish patients. Gen-erally, there are two major types of QoL instru-ments used in clinical trials: specific and generic.Specific questionnaires are usually focused on oneparticular area such as a disease state, a selectedpopulation, or a certain function or problem. TheSt. George Respiratory Questionnaire (SGRQ) hasbeen used to assess the QoL in patients withasthma, COPD, a1-antitrypsin deficiency, intersti-cial lung diseases and BQ.7
Generic QoL questionnaires are also availableand may be administrated to any individual,
thereby making it possible to assess the burden ofillness in different conditions. The Short Form-36Health Survey (SF-36) is the most widely usedgeneric instrument to measure health status. Thisquestionnaire has been recently adapted for theSpanish-speaking general population according tothe International Quality of Life Assessment (IQO-LA) project showing a good reproducibility andvalidity.8–10
The aims of this study were: (1) to investigatethe impact of BQs and nasal symptoms on QoLcompared with the Spanish general populationusing the SF-36 questionnaire; and (2) to evaluatethe additional impact of mild-moderate nasalpolyposis on QoL in patients with BQs.
Material and methods
Study population: sixty patients with non-cysticfibrosis BQs in a stable phase of their illnes withupper airways symptoms were included in thisprospective study from April 2002 to July 2004.
Design: the diagnosis of BQs was based onsymptoms, physical findings, and thoracic high-resolution CT scan. Stability of the BQs conditionwas assessed with a complete clinical evaluation, aforced spirometry, and if is necessary a thoraxradiology. Stable BQs condition was defined as theabsence of fever, no impairment of airflow limita-tion, no increase in sputum overproduction orchange of the macroscopic characteristics (puru-lent), and no increase in chronic cough. Insummary, no increase in respiratory symptoms ormodifications in the treatment over the previous 6weeks. The day of the study, a complete clinicalevaluation and a forced spirometry (Collins SurveyIII, plus, USA) were performed. Exclusion criteriawere hospitalization in the previous 2 months, useof antibiotics in the last 4 weeks or presence of aserious concomitant illness.
The diagnosis of nasal polyposis was based on thevisualization of bilateral polyps under nasal endo-scopic examination. Approval for the study wasobtained from the Ethic’s Committee of ourinstitution and a signed informed consent wasobtained from all patients.

ARTICLE IN PRESS
The impact of bronchiectasis 1999
After a 4-week washout period of oral andintranasal steroids, all patients with BQs completedthe SF-36 survey. Nasal symptoms and nasalendoscopy were also scored. Most of experimentalstudies and clinical trails investigating nasal poly-posis consider adequate a washout period of 4weeks since patients with sinonasal pathology oftenfollow treatments with oral antihistamines, oraland intranasal corticosteroids, oral antibiotics, andnasal lavages that may improve the clinicalsymptoms.11,12
Quality of life: the Health Survey SF-36 consistsof 36 self-administered questions and was devel-oped to measure eight health domains: physicalfunctioning (PF), role physical (RP), bodily pain(BP), general health (GH), vitality (VT), roleemotional (RE), social functioning (SF), and mentalhealth (MH). Two summary scales are also included:the physical component summary (PCS) and themental component summary (MCS). Spanish versionof the SF-36 Health Survey was used. This version isvery similar to the original US questionnaire inabsolute values, age and gender. We needed ageneric questionnaire to assess QoL in pathologypotentially involved both upper and lower airways:bronchiectasis and sinonasal pathology (with orwithout nasal polyposis). Scale scores in eachdomain and summaries range from 0 to 100, higherscores indicating better QoL.13
Nasal symptoms: obstruction, loss of the sense ofsmell, rhinorrhea (anterior and posterior), facialpain, itching, and sneezing was scored. The severityof nasal symptoms was assessed and scored, follow-ing the system designed by Rasp et al.,14 andpublished before11,12 by our group, as follows: 0, nosymptom; 1, mild but not troublesome symptom; 2,moderate symptom somewhat troublesome but notenough to interfere with daily activities or sleep;and 3, severe and troublesome symptom thatinterferes with daily activities or sleep.
Nasal endoscopy: polyp size was scored from 0 to3 for each nasal cavity following Lildholdt0sclassification: 0, no polyps; 1, mild polyposis (smallpolyps not reaching the upper edge of the inferiorturbinate); 2, moderate polyposis (polyps betweenthe upper and lower edges of the inferior turbi-nate); 3, severe polyposis (large polyps reachingthe lower edge of the inferior turbinate).15,16 Allpatients had upper airway symptoms and wereexamined by the same otorhinolaryngologist at theDepartment of Otolaryngology of our Hospital.
Lung function: evaluated by forced spirometryaccording to standard methods. The best one-second forced expiratory volume (FEV1) was chosenfor analysis and expressed as percent predictedFEV1 (FEV1%).
Statistical analysis: was performed using SPSS forWindows (SPSS 11.0, Chicago, IL, USA). All analyseswere performed using two-tailed tests significanceat the 0.05 level. The data are presented asmean7SD (standard deviation). All data wereassesed for normal distribution and the Bonferronicorrection for multiple comparisons was used. Ourfirst objective was to investigate the impact of BQsand nasal symptoms on QoL compared with theSpanish general population using the SF-36 ques-tionnaire. A study population size of 29 patients pergroup, achieves 95% power to detect a differenceof 20% between the null hypothesis mean of 82.7(PCS) and the alternative hypothesis mean of 66.4with an estimated standard deviation of 23.3 andwith a significance level (alpha) of 0.05 using a two-sided one-sample t-test.
Unpaired Student’s t test was used to comparenasal symptoms and SF-36 scores of patients withBQs with those from the Spanish general popula-tion, and between patients with or without NP. SF-36 scores for healthy control subjects from theSpanish population used in comparative analyseswere derived from a sample of 9984 people ofwhom 51.8% were females. Males of the Spanishgeneral population have demonstrated significanthigher scores than females in all SF-36 dimensions.7
After analyzing matching for age, no significantdifference on the mean age between patients ofour study and the Spanish general population.
Pearson correlation coefficients were used toexamine the association between QoL scores andgender, age, nasal symptoms, nasal polyps, andlung function. Multiple linear regression analysiswith SF-36 scores were used, alternatively the PCSand MCS scores as the dependent variable and age,sex, nasal polyps size as independent variables.Internal consistency was calculated by Cronbach’s acoefficient for each SF-36 scale. This coefficientranges from 0 to 1, and a minimum coefficient of0.7 is recommended to ensure a good internalconsistency.17
Results
The mean age of patients with BQs was 52716years (ranging from 18 to 78 years). Thirty-ninepatients (65%) were female (Table 1). Patients withBQs scored anterior and posterior rhinorrhea, lossof the sense of smell, and nasal obstruction as themajor complaints, while itching, facial pain andsneezing were much less frequent and discomfort-ing (Table 2).
Twenty-five patients (41.6%) with BQs had nasalpolyps with a size score of 1.570.4 with a range(1–2).15 The patients distribution by lildholdt is:

ARTICLE IN PRESS
Table 1 Characteristics of patients with bronchiectasis (BQs).
N Age (yr) Gender(M/F)
Diseaseduration (yr)
Smoking habit FEV1% FEV1 FVC
All patientsBQs
60 52716 21/39 1570.7 15 8173.4 2.570.2 8974
BQs without NP 35 55713 9/26 1670.7 6 (5 ex-smokers) 8276 2.870.6 9076.1BQs with NP 25 48718 12/13 1370.7 9 (7 ex-smokers) 80.674.2 2.370.2 88.476
Table 2 Nasal symptoms in patients with bronchiectasis (BQs).
N Nasalobstruction
Loss of sense ofsmell
Anteriorrhinorrhea
Posteriorrhinorrhea
Sneezing
All patientswith BQs
60 1.6570.9 0.971 1.970.9 1.870.9 1.271
BQs without NP 35 1.470.8 0.570.8 1.870.9 1.970.9 1.270.9BQs with NP 25 2.0570.8y 1.471.0y 270.8 1.770.9 1.271
Nasal symptoms and polyp size were scored from 0 to 3. yPo0.05, compared to patients with bronchiectasis without nasalpolyposis.
0
20
40
60
80
100
PF RP BP GH VT SF RE MH PCS MCS
Spanish population
All BQs
without NP
with NP
**
**
**
*
*
*
*
SF-36 domains
Scor
e
Figure 1 Quality of life in patients with bronchiectasisand sinonasal disease compared to the Spanish generalpopulation. Physical functioning (PF), role physicalfunctioning (RP), bodily pain (BP), general health (GH),vitality (VT), social functioning (SF), role emotionalfunctioning (RE), mental health (MH), mental componentsummary (MCS), and physical component summary (PCS).All patients (with and without polyps) had significantlyworse scores in all SF-36 domains. Unpaired student’s ttest was used, *Po0.05.
J.M. Guilemany et al.2000
Lildholdt 1: 8 patients; Lildholdt 1.5: 10 patients(a NP punctuation of 2 in a fossa and 1 in the other);Lildholdt 2: 7 patients. Patients with BQ and NPhad higher scores (Po0.05) of nasal obstructionand loss of sense of smell than patients with BQwithout NP.
In comparison with the Spanish general popula-tion,8 patients with BQs had significantly (Po0.05)worse QoL scores in all SF-36 domains (Fig. 1) aswell as in MCS and PCS (Table 3). No significantdifferences on QoL of patients with BQs and NP orwithout NP were observed.
Females showed lower physical functioning (dif-ference: 13.1, Po0.05 and 95%CI: 1.7–24.5), andlower social functioning (difference: 15.7, Po0.05and 95%CI: 0.4–31) than males. Females withBQs had lower scores of QoL (Po0.05) thanfemales from the Spanish general population onphysical functioning, body pain, general health,vitality, social functioning, and role emotional.Males with BQs also showed lower scores of QoL(Po0.05) than males from the Spanish generalpopulation on body pain, general health, andvitality. No significant differences were observedbetween males and females on age, pulmonaryfunction, presence of nasal polyps, upper airwaysymptoms, tobacco smoking history, and diseaseduration. Analysis of internal consistencies for allSF-36 domains showed a Cronbach’s a value higherthan 0.7 (0.75–0.91). Age, nasal symptoms, andpolyp size score were not statistically correlated toSF-36 scores.
Patients showed a degree of pulmonary functionimpairment on the FEV1% (8173.4). There were nosignificant correlation between the two QoL sum-maries and the degree of pulmonary function are:SCF (r: 0.21; P ¼ 0:242) and SCM (r: 0.095;P ¼ 0:599). Multiple linear regression analysis with

ARTICLE IN PRESS
Table 3 Quality of life domains and summary data of patients with bronchiectasis and sinonasal disease.
Spanish general population7 All patients with BQs
Physical functioning (PF) 90.3717.1 76722�
Role physical (RP) 87.6730.4 71742�
Body pain (BP) 81.9726 62.3724.9�
General health (GH) 70.9719.6 35.5718�
Vitality (VT) 71.6721 48.7717.3�
Role emotional (RE) 94.6721.8 71.3742.5�
Social functioning (SF) 94.1715.6 75.2728.3�
Mental health (MH) 77.7718.7 65.4721.4�
Physical component summary (PCS) 82.7723.3 46.5726.7�
Mental component summary (MCS) 84.5719.3 39.7727.3�
�Po0.05 bronchiectasis with nasal pathology compared to the Spanish general population.
The impact of bronchiectasis 2001
SF-36 scores were used, alternatively the PCS andMCS scores as the dependent variable and age, sex,nasal polyps size as independent variables withoutsignificant results.
Discussion
No studies have reported the impact of BQ andupper airway disease on QoL using the SF-36questionnaire. The main findings of our study were:(1) patients with BQ have an impaired QoL whencompared to the Spanish general population; (2)nasal polyposis has no additional impact on QoL inpatients with BQs.
This study demonstrates that QoL in patients withBQ is impaired compared to the general populationsin all SF-36 domains. No associations between QoLand age, nasal symptoms, and polyp size wereobserved. Furthermore, our findings supported thedeveloper’s claim of internal consistency for the SF-36 questionnaire since all the coefficients were atvalues above those recommended.
This study also demonstrates that women withBQ report poorer QoL scores on physical functioningand social functioning than males. Using the SF-36questionnaire, Bousquet et al. have observed thatmales with asthma report higher QoL scores thanfemales with asthma.18 Gender-related differencesin response to a chronic disease such as asthma isimportant in tailoring an education and manage-ment plan to each individual patient.19 Allergicrhinitis and asthma usually coexist. Patients withboth diseases experience more physical limitationsthan patients with allergic rhinitis alone, but nodifferences were found between these two groupsfor concepts related to social/mental health.20
Cystic fibrosis is the most common autosomalrecessive disease with fatal outcome in Caucasians
due to chronic infection of the lung resulting infibrosis and bronchiectasis followed by respiratoryinsufficiency. Some differences emerged betweenmales and females, with females generally report-ing poorer QoL scores. Evidence indicated thatmales and females perceived their health statusdifferently, with females having a more accurateperception of objective clinical health status.21
The St. George Respiratory Questionnaire (SGRQ)is a self-administrated health-related QoL measurecontaining 50 items and 76 weighted responsesdivided into three components: symptoms, activity,and impacts. The SGRQ has been used to assess theQoL in patients with asthma, COPD, a1-antitrypsindeficiency,22–25 and more recently BQ.26 Anxietyand depression are quite common in patients withBQ.27 QoL measured by the SGRQ in patients withBQ assessing the pulmonary function and thepresence of colonization (with pseudomonas orother microorganisms) shows that patients with BQcolonized with pseudomonas have worse pulmonaryfunction and QoL than uncolonized patients. More-over, patients having microorganisms other thanpseudomonas have a worse QoL than those withoutmicroorganisms.28 Pseudomonas aeruginosa is themost relevant pathogen producing chronic lunginfections in patients with chronic underlyingdiseases such as cystic fibrosis (CF), bronchiectasis,and chronic obstructive pulmonary disease (COPD).Hypermutation of pseudomona is found to be a keyfactor for the development of multiple-antimicro-bial resistance, and therefore these findings areexpected to have important consequences for thetreatment of chronic infections.29,30
Chronic rhinosinusitis (CRS) is an inflammatorydisease of the mucosa of the nasal cavity andparanasal sinuses with symptoms lasting longerthan 12 weeks. Currently, it is unclear, whetherCRS with NP and CRS without NP represent different

ARTICLE IN PRESS
J.M. Guilemany et al.2002
disease entities or just different stages of onesingle disease. Recent evidence suggests that,despite clinical similarities, CRS with and withoutNP have different inflammatory pathways andcytokine profiles. Although the similar clinicalsymptoms found in these patients, the greatclinical differences probably remains in the inten-sity on nasal obstruction and smell disorders.31
Nasal polyps are often an indicative of airwaydisease involving both the upper and lower respira-tory tracts.32 Radenne et al.33 has investigated theimpact of NP in QoL demonstrating that nasal polypsimpaired QoL in all SF-36 domains. More recently ourgroup demonstrated that asthma but not aspirinsensitivity has an additional negative impact on theQoL of patients with NP.11 QoL improved after NPtreatment, the improvement being related to nasalsymptoms. Both medical and surgical treatment ledto similar effects in improving QoL.12,34 Gliklich andMetson35 assessed the burden of chronic rhinosinusitisby using the SF-36 questionnaire and demonstrated asignificant decrease in body pain, general health,vitality, and social functioning domains comparedwith the American general population. Using the SF-36, other studies have also demonstrated thatchronic rhinosinusitis has a considerable impact onall SF-36 domains except for physical functioning andcompared with a healthy population.36–38
Patients with NP had lower scores in all SF-36domains except for physical functioning and roleemotional than patients with coronary arterydisease,39 chronic obstructive pulmonary disease,9
and asthma.40
In the present study patients with BQ and mild-moderate NP (Lildholdt classification o1.5), showedno further negative impact on QoL. The three mostdisabling symptoms were anterior rhinorrhea, pos-terior rhinorrhea and nasal obstruction. This studyprovides additional evidence that the degree ofabnormality on nasal symptoms is not associatedwith impairment of QoL. Patients with nasal polypshad a higher nasal obstruction and loss of sense ofsmell that did provoke no significant differences onQoL compared to patients without NP.
In conclusion, these results suggest that BQ has aconsiderable impact on QoL, but that nasal polypshave no additional impact on QoL of patients withBQ. Further studies are needed to better under-standing of the association between the upper andlower airways diseases.
Acknowledgements
The authors are grateful for Dr. Jordi Alonso of theHealth Services Research Unit, Institut Municipald0Investigacio Medica (IMIM-IMAS) of Barcelona, and
for Llorenc- Quinto of the Statistic Department inour Hospital, for their comments that greatlyimproved the presentation of the paper.
References
1. Barker AL. Bronchiectasis. N Engl J Med 2002;346:1383–93.2. Larsen PL, Tos M. Origin and structure of nasal polyps. In:
Mygind N, Lildholdt T, editors. Nasal polyposis: an inflam-matory disease and its treatment. Copenhagen: Munks-gaard; 1997. p. 17–30.
3. Fokkens W, Lund V, Bachert C, Clement P, Helllings P,Holmstrom M, et al. EAACI. EAACI position paper onrhinosinusitis and nasal polyps executive summary. Allergy2005;60(5):583–601.
4. Settipane GA. Epidemiology of nasal polyps. Allergy AsthmaProc 1996;17:231–6.
5. Widal MF, Abrani P, Lermoyez J. Anaphylaxie et idiosyncra-sie. Presse Med 1922;30:189–92.
6. Jones PW, Quirk FH, Baveystock CM. Why quality of lifemeasures should be used in the treatment of patients withrespiratory illness. Monaldi Arch Chest Dis 1994;49:79–82.
7. Chan SL, Chan-Yeung MM, Ooi GC, Lam CL, Cheung TF, LamWK, et al. Validation of the Hong Kong Chinese version of theSt. George Respiratory Questionnaire in patients withbronchiectasis. Chest 2002;122:2030–7.
8. Alonso J, Regidor E, Barrio G, Prieto L, Rodriguez C, de laFuente L. Population reference values of the Spanish versionof the Health Questionnaire SF-36. Med Clin (Barc) 1998;111:410–6.
9. Alonso J, Prieto L, Ferrer M, Vilagut G, Broquetas JM, Roca J,et al. Testing the measurement properties of the Spanishversion of the SF-36 Health Survey among male patients withchronic obstructive pulmonary disease. Quality of life inCOPD study group. J Clin Epidemiol 1998;51:1087–94.
10. Alonso J, Ferrer M, Gandek B, Ware Jr JE, Aaronson NK,Mosconi P, et al. IQOLA Project Group. Health-relatedquality of life associated with chronic conditions in eightcountries: results from the International Quality of LifeAssessment (IQOLA) Project. Qual Life Res 2004;13:283–98.
11. Alobid I, Benıtez P, Bernal-Sprekelsen M, Guilemany JM,Picado C, Mullol J. The impact of asthma and aspirinsensitivity on quality of life of patients with nasal polyposis.Qual Life Res 2005;14:789–93.
12. Alobid I, Benıtez P, Bernal M, Roca J, Alonso J, Picado C,et al. Nasal polyposis and its impact on quality of life.Comparison between the effects of medical and surgicaltreatments. Allergy 2005;60:452–8.
13. Ware JE, Konsinski M, Keller SD. SF-36 Physical and mentalhealth summary scales: a user’s manual. Boston, MA: TheHealth Institute, New England Medical Center; 1994.
14. Rasp G, Schuk A, Kastenbauer ER. A new grading system fornasal polyps of the ethmoid bone. HNO-on line, 1996.http://www.link.springer.de/link/service/journals/00106
15. Lildholdt T, Rundcrantz H, Lindqvist N. Efficacy of topicalcorticosteroid powder for nasal polyps: a double-blind,placebo-controlled study of budesonide. Clin Otolaryngol1995;20:26–30.
16. Johansen LV, Illum P, Kristensen S, Winther L, Petersen SV,Synnerstad B. The effect of Budesonide (Rhinocorts) in thetreatment of small and medium sized nasal polyps. ClinOtolaryngol 1993;18:524–7.
17. Cronbach LJ. Coefficient alpha and internal structure of atest. Psychometrika 1951;16:297–334.
18. Bousquet J, Knani J, Dhivert H, Richard A, Chicoye A, WareJr JE, et al. Quality of life in asthma. I. Internal consistency

ARTICLE IN PRESS
The impact of bronchiectasis 2003
and validity of the SF-36 questionnaire. Am J Respir CritCare Med 1994;149:371–5.
19. Osborne ML, Vollmer WM, Linton KL, Buist AS. Character-istics of patients with asthma within a large HMO: acomparison by age and gender. Am J Respir Crit Care Med1998;157:123–8.
20. Leynaert B, Neukirch C, Liard R, Bousquet J, Neukirch F.Quality of life in allergic rhinitis and asthma. A population-based study of young adults. Am J Respir Crit Care Med2000;162:1391–6.
21. Gee L, Abbott J, Conway SP, Etherington C, Webb AK.Quality of life in cystic fibrosis: the impact of gender,general health perceptions and disease severity. J CystFibros 2003;2:206–13.
22. Engstrom CP, Persson LO, Larsson S, Sullivan M. Reliabilityand validity of a Swedish version of the St. George’sRespiratory Questionnaire. Eur Respir J 1998;11:61–6.
23. Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A self-complete measure of health status for chronic airflowlimitation: the St. Georges’s Respiratory Questionnaire. AmRev Respir Dis 1992;145:1321–7.
24. Knebel AR, Leidy NK, Sherman S. Health related quality oflife and disease severity in patients with alpha-1 antitrypsindeficiency. Qual Life Res 1999;8:385–91.
25. Chang JA, Curtis R, Patrick DL, Raghu G. Assessment ofhealth-related quality of life in patients with interstitiallung disease. Chest 1999;116:1175–82.
26. Wilson CB, Jones PW, O’Leary CJ, Cole PJ, Wilson R.Validation of the St. George’s Respiratory Questionnaire inbronchiectasis. Am J Respir Crit Care Med 1997;156:536–41.
27. O’Leary CJ, Wilson CB, Hansell DM, Cole PJ, Wilson R, JonesPW. Relationship between psychological well-being and lunghealth status in patients with bronchiectasis. Respir Med2002;96:686–92.
28. Hernandez C, Abreu J, Jimenez A, Fernandez R, Martin C.Pulmonary function and quality of life in relation tobronchial colonization in adults with bronchiectasis notcaused by cystic fibrosis. Med Clin (Barc) 2002;118:130–4.
29. Macia MD, Blanquer D, Togores B, Sauleda J, Perez JL, OliverA. Hypermutation is a key factor in development of
multiple-antimicrobial resistance in Pseudomonas aerugino-sa strains causing chronic lung infections. Antimicrob AgentsChemother 2005;49:3382–6.
30. Rosell A, Monso E, Soler N, Torres F, Angrill J, Riise G, et al.Microbiologic determinants of exacerbation in chronicobstructive pulmonary disease. Arch Intern Med 2005;165:891–7.
31. Gillespie MB, Osguthorpe JD. Pharmacologic management ofchronic rhinosinusitis, alone or with nasal polyposis. CurrAllergy Asthma Rep 2004;4:478–85.
32. Johansson L, Bramerson A, Holmberg K, Melen I, Akerlund A,Bende M. Clinical relevance of nasal polyps in individualsrecruited from a general population-based study. ActaOtolaryngol 2004;124:77–81.
33. Radenne F, Lamblin C, Vandezande LM, Tillie-Leblond I,Darras J, Tonnel AB, et al. Quality of life in nasal polyposis. JAllergy Clin Immunol 1999;104:79–84.
34. Alobid I, Benıtez P, Pujols L, Maldonado M, Bernal-Sprekelsen M, Morello A, et al. Severe nasal polyposis andits impact on quality of life. The effect of short course oforal steroids followed by long term intranasal steroidstreatment. Rhinology 2006;44:8–13.
35. Gliklich RE, Metson R. Effect of sinus surgery on quality oflife. Otolaryngol Head Neck Surg 1997;117:12–7.
36. Winstead W, Barnett S. Impact of endoscopic sinus surgeryon global health perception: an outcomes study. OtolaryngolHead Neck Surg 1998;119:486–91.
37. Durr DG, Desrosiers MY, Dassa C. Quality of life in patientswith rhinosinusitis. J Otolaryngol 1999;28:108–11.
38. Wang PC, Tai CJ, Lin MS, Chu CC, Liang SC. Quality of life inTaiwanese adults with chronic rhino-sinusitis. Qual Life Res2003;12:443–8.
39. Failde I, Ramos I. Validity and reliability of the SF-36 healthsurvey questionnaire in patients with coronary arterydisease. J Clin Epidemiol 2000;53:359–65.
40. Espinosa De Los Monteros MJ, Alonso J, Ancochea J,Gonzalez A. Quality of life in asthma: reliability and validityof the short form generic questionnaire (SF-36) applied tothe population of asthmatics in a public health area. ArchBronconeumol 2002;38:4–9.

Tesis Doctoral III. Trabajo Experimental
133
Estudio 3. United airways: the impact of chronic rhinosinusitis and nasal
polyps in bronchiectasic patient’s quality of life. Allergy 2009;64:1524-9. DOI:10.1111/j.1398-9995.2009.02011.x

Original article
United airways: the impact of chronic rhinosinusitis and nasal
polyps in bronchiectasic patient�s quality of life
Bronchiectasis (BQ) consists of a permanent and irrevers-ible dilatation of bronchi and bronchioles caused byretained secretions and recurrent infections that causeinflammation, obstruction, and damage of the lowerairway. Bronchiectasis is a consequence of a variety ofdifferent diseases inwhich airway infection andobstructionappear to be the most important contributory factors.Bronchiectasis is frequently associated with cystic fibrosis,primary ciliary dyskinesia, immunodeficiency, rheumatoidarthritis, and inflammatory bowel diseases (1).Chronic rhinosinusitis (CRS), one of the most common
chronic diseases (2), is an inflammatory disease of the
nose and sinus mucosa that is still little understood,despite various hypotheses about its cause (3). Chronicrhinosinusitis with nasal polyps (NP) is considered asubgroup of CRS. Chronic rhinosinusitis with or withoutNP is often taken together as one disease entity, becauseit seems impossible to clearly differentiate both entities(4–6). The reason why polyps develop in some patientsand not in others remains unknown. In the generalpopulation, the prevalence of NP is 4%. Although thecause of NPs is still unknown, it has been reported to beassociated with asthma and other pulmonary disorders,such as cystic fibrosis, primary ciliary dyskinesia, aspirin
Background: The nose and the bronchi belong, in anatomical and physiopath-ological terms, to the concept of united airways. Associations between upper andlower airways diseases have been demonstrated in allergic rhinitis and asthma,nasal polyposis (NP) and asthma, chronic rhinosinusitis (CRS) and chronicobstructive pulmonary disease, and more recently CRS/NP and bronchiectasis(BQ).Objective: To evaluate the impact of CRS on quality of life (QoL) of patientswith BQ, and to correlate these findings with the pulmonary status, nasalsymptoms, and general health status.Methods: In a prospective study, patients with BQ (n = 80) were evaluated forCRS and NP using EP3OS criteria, and severity of BQ using chest highresolution computed tomography (HRCT)-scan. Quality of life was assessed inall patients by using specific [Sinonasal Outcome Test-20 (SNOT-20), St GeorgeRespiratory Questionnaire (SGRQ)], and generic (Short Form-36; SF-36)questionnaires.Results: Using SNOT-20, patients with CRS had worse QoL (2.1 ± 0.1;P < 0.001) than patients without CRS (0.4 ± 0.06). Using SGRQ total score,patients with CRS had worse QoL (43.7 ± 2.2; P < 0.001) than patientswithout CRS (24.7 ± 2.5). Using SF-36, patients with CRS had worse QoL,both in the physical summary (64 ± 3.4; P < 0.05) and the mental summary(65.5 ± 4.7; P < 0.05), than patients without CRS (physical summary [PS]:76.2 ± 3.3; mental summary [MS]: 78.3 ± 5.3, respectively). SinonasalOutcome Test-20 was correlated with SGRQ total score (r = 0.72; P < 0.01),and SF-36 physical summary (r = )0.63; P < 0.01). St George RespiratoryQuestionnaire was correlated with SF-36 on physical summary (r = )0.58;P < 0.05) and with forced expiratory volume in 1 s (r = )0.41; P < 0.05).Conclusion: These results suggested that CRS, measured by both specific andgeneric questionnaires, has a considerable impact on the QoL of patients withBQ.
J. M. Guilemany1,5, J. Angrill2,I. Alobid1,5, S. Centellas1,5, E. Prades1,J. Roca1,4,5, L. Pujols1,5, M. Bernal-Sprekelsen1,5, C. Picado2,3,5,*,J. Mullol1,3,4,5,*1Rhinology Unit and Smell Clinic, Department ofOtorhinolaryngology, Hospital Cl�nic i Universitari,Barcelona; 2Pneumology and Respiratory Allergy,Hospital Cl�nic, Barcelona; 3Department ofMedicine, University of Barcelona, Barcelona;4Institut d�Investigacions Biom�diques August Pi iSunyer (IDIBAPS), Barcelona; 5Centro deInvestigaci�n Biom�dica en Red de EnfermedadesRespiratorias (CIBERes), Barcelona, Spain
Key words: bronchiectasis; chronic rhinosinusitis; nasalpolyposis; quality of life; Short Form-36 questionnaire;St George Respiratory Questionnaire; SinonasalOutcome Test-20.
Jos� Mara Guilemany TosteDepartment of OtorhinolaryngologyHospital Cl�nic i Universitaric/Villarroel, 17008036 BarcelonaCataloniaSpain
*Both senior investigators participated with equalresponsibilities.Hospital Cl�nic – IDIBAPS is a partner center ofGA2LEN (Global Allergy and Asthma EuropeanNetwork).
Accepted for publication 29 January 2009
Allergy 2009: 64: 1524–1529 � 2009 John Wiley & Sons A/S
DOI: 10.1111/j.1398-9995.2009.02011.x
1524

sensitivity (7, 8), and more recently BQ (9). Almost fourout of five patients with BQ (77%) presented criteria forCRS, and one out of every four patients had NP on nasalendoscopy (25%) (9).Bronchiectasis is a disease with the potential to cause
devastating complications. The patients with BQ presentcough and chronic sputum production, which have agreat impact on patient�s quality of life (QoL) (10). Mostpatients undergo slow and progressive health deteriora-tion over decades. Chronic rhinosinusitis and BQ canhave detrimental effects on physical, psychological, andsocial aspects of patients� lives, significantly worseningtheir QoL. Symptoms and lung function do not reflect theimpact of the disease on the patient�s health status, whichshould be supplemented by the use of QoL questionnaires(11). Studies have reported that patients with CRS havemore bodily pain (BP) and worse social functioning (SF)than for example patients with chronic obstructivepulmonary disease (COPD), congestive heart failure,diabetes, and back pain (12, 13).There are two major types of QoL instruments used in
clinical trials: specific and generic questionnaires (14, 15).Specific questionnaires are usually focussed on oneparticular area such as a disease state, a selectedpopulation, or a certain function or problem. The StGeorge Respiratory Questionnaire (SGRQ) has beenused to assess the QoL in patients with asthma, COPD,a1-antitrypsin deficiency, interstitial lung diseases, andBQ (16). The Sinonasal Outcome Test (SNOT-20) is alsoa validated, disease-specific, health-related QoL question-naire for upper airway pathology (17). This has been usedin a number of studies of CRS (18, 19). Rhinosinusitis-related impairment of QoL was assessed with theSNOT-20 questionnaire in allergic asthmatic, nonallergicasthmatic, and COPD patients. Patients with allergic andnonallergic asthma and COPD show increased nasalsymptoms, more nasal inflammation, and significantimpairment of their QoL related to rhinosinusitis (20).No studies have reported the impact of upper airwaydisease on QoL in patients affected by BQ on the basis ofspecific questionnaires such as SNOT-20 and SGRQ.Generic QoL questionnaires are also available and
may be administrated to any individual, thereby makingit possible to assess the burden of illness in variousconditions. The Short Form-36 Health Survey (SF-36) isthe most widely used generic instrument for measuringhealth status. This questionnaire has been adapted forthe Spanish-speaking general population in accordancewith the International Quality of Life Assessmentproject and has demonstrated a good reproducibilityand validity (21–23). In a previous study performed byour group with SF-36, we demonstrated that patientswith BQ and CRS have a significantly impaired QoLcompared with the Spanish general population with nodifferences between CRS, either with or without NP(24). The aim of this study was to evaluate the impact ofCRS, with or without NP, on the QoL of patients with
BQ using a specific QoL questionnaire (SNOT-20,SGRQ), and to correlate the findings with: SF-36, nasalsymptoms, and lung function.
Material and methods
Study population
Patients with noncystic fibrosis BQ in a stable phase of their illness(n = 80) were included in this prospective study from January 2005to February 2006. Sixty patients fulfilled EP3OS criteria (2) forCRS, 20 of whom with NP (9).
Design
The diagnosis of BQ was performed on the basis of characteristicclinical symptoms and chest-CT scanning (Siemens Emotion DuoTwo-slice 5 mm with high resolution slices 1 mm for pulmonaryparenchyma; Siemens, Munich, Germany). The stability of the BQcondition was assessed with a complete clinical evaluation, a forcedspirometry, and wherever necessary also with a thorax radiology.Stable BQ condition was defined as the absence of fever, no impair-ment of airflow limitation, no increase in sputum overproduction orchange in the macroscopic characteristics (purulence), and noincrease in chronic cough. In summary, no increase in respiratorysymptoms or modifications in the treatment over the previous6 weeks. The Ethics Committee of our institution approved the studyand signed informed consent was obtained from all the patients.Exclusion criteria were hospitalization in the previous 2 months,
use of antibiotics in the last 4 weeks, pseudomonas colonization, orpresence of a serious concomitant illness.To characterize the involvement of upper airway disease in
patients with BQ, the following diagnostic tools were used in thestudy: nasal symptom score, nasal endoscopy, sinonasal CT-scan(Siemens Somaton P4 Unislice 3 mm). Nasal congestion/obstruc-tion/blockage, reduction or loss of the sense of smell, anteriorrhinorrhea, postnasal drip, facial pain/pressure, itching, andsneezing were scored using the Rasp classification (0–3) (25). Polypsize was scored from 0 to 3 for each nasal cavity using nasalendoscopy, following Lildholdt�s classification (26). A radiologistblindly staged sinus occupation for each patient, using CT scanningand the Lund-MacKay score system (0–24) (27). All these resultshave been already published in a previous study (9).To characterize the involvement of lower airway disease, a chest
HRCT-scan was performed during the 3-month period prior to thesinonasal examination and the extent of BQ in each lobe wasgraded, using a scale from 0 to 3 (0, no involvement; 1, segmentinvolved; 2, more than one segment involved; and 3, gross cystic BQinvolving the entire lobe) (28).After a 4-week washout period for oral and intranasal steroids,
SNOT-20, SGRQ, and SF-36 questionnaires were completed by allpatients (29, 30).
Quality of life
1 The SNOT-20 comprises 20 items that assess symptoms ofCRS and the impact that they have on health status. Each itemis graded from 0 to 5. Higher scores represented a worseimpairment of health status because of upper airway symp-toms. A control group without CRS, studied to validate thequestionnaire, had a mean score of 0.6 (17).
QoL in bronchiectasis
� 2009 John Wiley & Sons A/S Allergy 2009: 64: 1524–1529 1525

2 The SGRQ is a disease-specific instrument designed to measureimpact on overall health, daily life, and perceived well-being.The SGRQ was developed for use by patients with fixed andreversible airway obstruction, and has been widely used inCOPD, asthma and more recently in BQ research, including 56items (76 weighted responses) across three domains: symptoms(frequency and severity), activity (activities that cause or arelimited by breathlessness), and impact (SF, psychologicaldisturbances resulting from airways disease). Scores range from0 to 100, with higher scores indicating poorer QoL.
3 The Medical Outcomes Study SF-36 consists of 36 self-administered questions and was developed to measure eighthealth domains: physical functioning (PF), role physical, BP,general health (GH), vitality, role emotional (RE), SF, andmental health. Two summary scales are also included: thephysical component summary (PCS) and the mental compo-nent summary (MCS). We needed a generic questionnaire toassess QoL in pathology potentially involving both upper andlower airways: BQ and CRS (with or without NP). The Spanishversion of the SF-36 Health Survey was used (21). This versionis very similar to the original US questionnaire in absolutevalues, age, and gender. Scale scores in each domain andsummaries range from 0 to 100, higher scores indicating betterQoL (31). Data on SF-36 has already been published and willbe used here only to correlate with specific QoL questionnaires,and to support our objectives including a subgroup of patientswith BQ with no nasal pathology; given that only the PCS andthe MCS will be reported here.
Statistical analysis
Statistics were performed using spss for Windows (spss 11.0; SPSSInc., Chicago, IL, USA). All analyses were performed using two-tailed tests significance at the 0.05 level. The data are presented asmean ± SEM. All data were assessed for normal distribution andthe Bonferroni correction for multiple comparisons was used.Unpaired Student�s t-test was used to compare SNOT-20, SGRQ,and SF-36 of patients with BQ with and without CRS, and betweenpatients with or without NP. Pearson correlation coefficients wereused to examine the association between QoL scores (SNOT-20,SGRQ, SF-36) with nasal symptoms, and lung function.
Results
Demographic data
The mean age of BQ patients was 56.6 ± 1.8 years, 8%were smokers and 27% ex-smokers. No significantdifferences exist on the presence of CRS depending on
smoking history. Patients with CRS (81% female sub-jects) had a significantly higher female ratio (4.4 : 1), andthis was even higher in patients with CRS without NP(8.3 : 1), when compared with patients without CRS(1 : 1) (Table 1).
Quality of life
1 SNOT-20. Patients with CRS had significantly highertotal scores (2.1 ± 0.1; P < 0.001) than patientswithout CRS (0.4 ± 0.06) (Fig. 1). No significantdifferences were observed between patients with orwithout NP and depending on the BQ aetiology(idiopathic vs postinfectious).
2 SGRQ. Patients with CRS had significantly higherscores in total score (43.7 ± 2.2; P < 0.001), symp-toms (56.7 ± 3; P < 0.001), activities (41.6 ± 2.4;P < 0.001), and impact (33 ± 2.5; P < 0.001), thanpatients with no CRS (total: 24.7 ± 2.5; symptoms:35.9 ± 3.2; activities: 18.2 ± 3; impact: 19.9 ± 2.7)respectively (Fig. 1). No significant differences werefound between patients with or without NP or be-tween those with a different BQ aetiology (idiopathicvs postinfectious).
St George Respiratory Questionnaire total score (r =0.72; P < 0.01), symptoms (r = 0.56; P < 0.01), activ-ities (r = 0.72; P < 0.01), and impact (r = 0.64;P < 0.01) were correlated with the SNOT-20 totalscore.
3 SF-36. Patients with CRS had significantly lowerscores in PCS (64 ± 3.4; P < 0.05), and MCS(65.5 ± 4.7; P < 0.05) than patients with no CRS(PS: 76.2 ± 3.3; MS: 78.3 ± 5.3) respectively(Fig. 1). No significant differences were foundbetween patients with or without NP and dependingon the BQ aetiology (idiopathic vs postinfectious).
SF-36 PCS (r = )0.63; P < 0.01), and SF-36 MCS(r = )0.43; P < 0.01) correlated with SNOT-20 totalscore, while only PCS (r = )0.58; <0.05) correlated withSGRQ total score.
4 Correlation of QoL questionnaires (SNOT-20,SGRQ, SF-36) with nasal symptoms, lung function
Table 1. Epidemiologic characteristics of BQ patients included in the study
All BQ patients Non-CRS CRS CRS without NP CRS with NP
Patients, n (%) 80 20 (25) 60 (75) 40 (50) 20 (25)Age (years)� 56.6 € 1.8 58.7 € 3.2 55.5 € 2.1 57 € 2.5 51.2 € 4Female subjects, % F/M ratio 71
2.4 : 150
1 : 181*
4.4 : 189*
8.3 : 160**
1.5 : 1FEV1, %� 80.8 € 2.8 90 € 4 75.8 € 3* 77.6 € 3.6* 71 € 8*
BQ, bronchiectasis; CRS, chronic rhinosinusitis; NP, nasal polyposis; M, male; F, female; FEV1, forced expiratory volume in 1 s.Unpaired Student�s t test: *P < 0.05, when compared with non-CRS patients; **P < 0.05, when compared with patients with CRS without NP.�Data presented as mean € SEM.
Guilemany et al.
1526 � 2009 John Wiley & Sons A/S Allergy 2009: 64: 1524–1529

(forced expiratory volume in 1 s; FEV1), and BQseverity (chest HRCT-scan).
(i) Nasal symptoms. Total nasal symptom scorecorrelated with SNOT-20 total score (r = 0.8;P < 0.01), SGRQ total score (r = 0.67;P < 0.01), as well as with the SF-36 PCS(r = )0.72; P < 0.01), and MCS (r = )0.48;P < 0.01).
(ii) Lung function. A mild but significant correla-tion was observed between FEV1 and SGRQtotal score (r = )0.41; P < 0.05), but notwith SGRQ total score and SF-36 componentsummaries.
(iii) Chest HRCT-scan. Patients with CRS(6.2 ± 0.5; P < 0.001) showed a higher BQseverity score than patients with no CRS(4.2 ± 0.7). No differences were observed be-tween patients with and without NP. Amild butsignificant correlation was observed betweenextension ofBQandSGRQ total score (r = 0.4;P < 0.05), but not with SNOT-20 total scoreand SF-36 component summaries.
Discussion
The main findings of our study were: (i) patients with BQand CRS had an impaired QoL when compared with BQ
patients with no CRS measured by SNOT-20, SGRQ,and SF-36; (ii) NP had no additional impact on QoL inpatients with BQs; (iii) upper airway QoL (SNOT-20)have been shown to correlate with both the lower airwaysQoL (SGRQ) and the GH QoL (SF-36). This studydemonstrates that CRS contributed to the impairment ofhealth status in patients with BQ.
The mean SNOT-20 score in patients with BQ whofulfill EP3OS criteria for CRS, with or without NP, was2.1. This was higher than the score registered in apopulation of patients with CRS, studied during thevalidation of the SNOT-20 questionnaire, who had amean score of 1.9 (17). Moreover, the SNOT-20 score inpatients with BQ without CRS (0.4) was similar to thatpreviously reported in normal control patients (0.6) (17).There were no differences between patients with CRSwith or without NP, although the SNOT-20 question-naire does not include sections on nasal congestion orsmell disorders. Although SNOT-22, which includes bothitems, could be more adequate for differentiating betweenCRS with NP and CRS without NP, this questionnairehas not yet been validated. The absence of a relationshipbetween current smoking status and the nasal or SNOT-20 scores is interesting as active smoking is known to beassociated with symptoms of CRS (32).
Quality of life measured by the SGRQ in patients withBQ assessing the pulmonary function and the presence ofcolonization (with pseudomonas or other microorganisms)
5SNOT-20 (total) SGRQ (total)
SF-36
001
2
3
4
ore
(0-5
)
P < 0.05 P < 0.05
P < 0.001P < 0.001
orse
QoL
05
57
ore
(0-1
00)
orse
QoL
0
1
2
Sco
wo
0
52Sco w
o
+SRC–SRC+SRC–SRC
09
001
05
06
07
08
(0-1
00)
rse
QoL
01
02
03
04
Scor
e(
wor
0
01
+SRC–SRC+SRC–SRCSCM SCP
Figure 1. Quality of life depending on the existence (CRS+, gray bars) or absence (CRS), white bars) of chronic rhinosinusitis,measured by SNOT-20, SGRQ, and SF-36 (MCS, PCS) questionnaires.
QoL in bronchiectasis
� 2009 John Wiley & Sons A/S Allergy 2009: 64: 1524–1529 1527

has shown that patients with BQ colonized with pseudo-monas have worse pulmonary function and QoL thanuncolonized patients. Moreover, patients having microor-ganisms other than pseudomonas have a worse QoL thanthose without microorganisms (33). In our study, none ofthe patients with BQwere colonized by pseudomonas. Withrespect to the aetiology (idiopathic vs postinfectious), nodifferences in QoL were found in patients with BQ.Patients with NP have shown lower scores in all SF-36
domains except for PF and RE than patients withcoronary artery disease (34), COPD (22), and asthma(35). Nasal polyps are often an indicator of airway diseaseinvolving both the upper and lower respiratory tracts(36). Radenne et al. (37) have investigated the impact ofNP on QoL demonstrating that NPs impaired QoL in allSF-36 domains. Other studies have shown statisticallysignificant differences in seven of the eight domains of theSF-36, the exception being PF (12, 28, 38). More recentlyour group has demonstrated that asthma – but notaspirin sensitivity – has an additional negative impact onthe QoL of patients with NP (29).A previous study by our group demonstrated that
patients with BQ and CRS present a significantlyimpaired QoL when compared with the Spanish generalpopulation with no differences between CRS with NP andCRS without NP (24). In this study, patients with BQwith CRS showed an important negative impact on QoLwhen compared with patients with BQ without CRS, withno additional impact from the presence of NPs. Upperairway QoL (SNOT-20) have been shown to correlatewith both the lower airways QoL (SGRQ) and the GH
QoL (SF-36). This study provides additional evidencethat the degree of abnormality in nasal symptoms isassociated with the impairment of QoL in SNOT-20,SGRQ, and SF-36. Patients of the group CRS with NPhad a higher loss of sense of smell, without provoking anysignificant differences in QoL (SNOT-20, SGRQ, and SF-36), when compared with patients of the group CRSwithout NP. Otherwise, there was no significant correla-tion between the SNOT-20 and SGRQ total score(r = 0.21, P < 0.09), or between the SNOT-20 and theindividual impact, activity, or symptoms domains of theSGRQ in patients with upper airway symptoms andCOPD (39).
In conclusion, these results are the first to suggest thatCRS with and without NP have a considerable impact onthe QoL of patients with BQ. Hence, our data alsoconfirm that the �united airway� concept goes beyond thescope of asthma and COPD. In addition, treating thenose might also have beneficial effects on the health statusof patients with BQ.
Acknowledgments
Jose M. Guilemany has been supported by the National Plan forScientific Research, Development and Technologic Innovation ofthe Health�s Institute Carlos III – Health Research Fund (CM06/00071), and the Spanish Society of Oto-Rhino-Laryngology, Head& Neck Pathology. This study has been partially sponsored by theFundacio Catalana de Pneumologia (FUCAP).
References
1. Guilemany JM, Mullol J, Picado C.Relation between rhinosinusitis andbronchiectasis. Arch Bronconeumol2006;42:135–140.
2. Kaliner MA, Osguthorpe JD, FiremanP, Anon J, Georgitis J, Davis ML et al.Sinusitis: bench to bedside. Currentfindings, future directions. J Allergy ClinImmunol 1997;99:s829–s848.
3. Fokkens W, Lund V, Mullol J, Onbehalf of the European Position Paperon Rhinosinusitis and Nasal PolypsGroup. EP3OS 2007: European positionpaper on rhinosinusitis and nasal polyps2007. Rhinol Suppl 2007;20:1–136.
4. Steinke JW, Bradley D, Arango P,Crouse CD, Frierson H, Kountakis SEet al. Cysteinyl leukotriene expression inchronic hyperplastic sinusitis-nasalpolyposis: importance to eosinophiliaand asthma. J Allergy Clin Immunol2003;111:342–349.
5. Ichimura K, Shimazaki Y, Ishibashi T,Higo R. Effect of new macrolide roxi-thromycin upon nasal polyps associatedwith chronic sinusitis. Auris NasusLarynx 1996;23:48–56.
6. Dykewicz MS. 7. Rhinitis and sinusitis.J Allergy Clin Immunol 2003;111:S520–S529.
7. Settipane GA. Epidemiology of nasalpolyps. Allergy Asthma Proc1996;17:231–236.
8. Widal MF, Abrani P, Lermoyez J.Anaphylaxie et idiosyncrasie. PresseMed 1922;30:189–192.
9. Guilemany JM, Angrill J, Alobid I,Centellas S, Pujols L, Bartra J et al.United airways again: high pre-valence of rhinosinusitis and nasalpolyps in bronchiectasis. Allergy2009;64:790–797.
10. Polley L, Yaman N, Heaney L, CardwellC, Murtagh E, Ramsey J et al. Impactof cough across different chronic respi-ratory diseases: comparison of twocough-specific health-related quality oflife questionnaires. Chest 2008;134:295–302.
11. Jones PW, Quirk FH, Baveystock CM.Why quality of life measures should beused in the treatment of patients withrespiratory illness. Monaldi Arch ChestDis 1994;49:79–82.
12. Van Agthoven M, Fokkens WJ, van deMerwe JP, Marijke van Bolhuis E, Uyl-de Groot CA, Busschbach JJ. Quality oflife of patients with refractory chronicrhinosinusitis: effects of filgrastim treat-ment. Am J Rhinol 2001;15:231–237.
13. Gliklich RE, Metson R. The healthimpact of chronic sinusitis in patientsseeking otolaryngologic care. Otolaryn-gol Head Neck Surg 1995;113:104–109.
Guilemany et al.
1528 � 2009 John Wiley & Sons A/S Allergy 2009: 64: 1524–1529

14. Alobid I, Guilemany JM, Mullol J. Theimpact of chronic rhinosinusitis andnasal polyposis in quality of life. FrontBiosci 2009, in press.
15. Alobid I, Bernal-Sprekelsen M, MullolJ. Chronic rhinosinusitis and nasal pol-yps: the role of generic and specificquestionnaires on assessing its impact onpatient�s quality of life. Allergy2008;63:1267–1279.
16. Chan SL, Chan-Yeung MM, Ooi GC,Lam CL, Cheung TF, Lam WK et al.Validation of the Hong Kong Chineseversion of the St. George RespiratoryQuestionnaire in patients with bronchi-ectasis. Chest 2002;122:2030–2037.
17. Piccirillo JF, Merritt MG Jr, RichardsML. Psychometric and clinimetricvalidity of the 20-Item Sino-NasalOutcome Test (SNOT-20). OtolaryngolHead Neck Surg 2002;126:41–47.
18. Ragab SM, Lund VJ, Scadding G.Evaluation of the medical and surgicaltreatment of chronic rhinosinusitis: aprospective, randomised, controlledtrial. Laryngoscope 2004;114:923–930.
19. Hopkins C, Browne JP, Slack R, LundV, Topham J, Reeves B et al. The na-tional comparative audit of surgery fornasal polyposis and chronic rhinosinus-itis. Clin Otolaryngol 2006;31:390–398.
20. Hens G, Vanaudenaerde BM, BullensDM, Piessens M, Decramer M, DupontLJ et al. Sinonasal pathology in nonal-lergic asthma and COPD: �united airwaydisease� beyond the scope of allergy.Allergy 2008;63:261–267.
21. Alonso J, Regidor E, Barrio G, Prieto L,Rodriguez C, de la Fuente L. Popula-tion reference values of the Spanishversion of the Health QuestionnaireSF-36. Med Clin (Barc) 1998;111:410–416.
22. Alonso J, Prieto L, Ferrer M, Vilagut G,Broquetas JM, Roca J et al. Testing themeasurement properties of the Spanishversion of the SF-36 Health Surveyamong male patients with chronicobstructive pulmonary disease. Qualityof life in COPD study group. J ClinEpidemiol 1998;51:1087–1094.
23. Alonso J, Ferrer M, Gandek B, Ware JEJr, Aaronson NK, Mosconi P et al.Health-related quality of life associatedwith chronic conditions in eight coun-tries: results from the InternationalQuality of Life Assessment (IQOLA)Project. Qual Life Res 2004;13:283–298.
24. Guilemany JM, Alobid I, Angrill J,Ballesteros F, Bernal-Sprekelsen M,Picado C et al. The impact of bronchi-ectasis associated to sinonasal disease onquality of life. Respir Med2006;100:1997–2003.
25. Rasp G, Kramer MF, Ostertag P,Kastenbauer E. A new system for theclassification of ethmoid polyposis.Effect of combined local and systemicsteroid therapy. Laryngorhinootologie2000;79:266–272.
26. Lildholdt T, Rundcrantz H, LindqvistN. Efficacy of topical corticosteroidpowder for nasal polyps: a double-blind,placebo-controlled study of budesonide.Clin Otolaryngol 1995;20:26–30.
27. Lund VJ, MacKay IS. Staging inrhinosinusitus. Rhinology 1993;31:183–184.
28. Angrill J, Agusti C, de Celis R, Rano A,Gonzalez J, Sole T et al. Bacterial col-onisation in patients with bronchiecta-sis: microbiological pattern and riskfactors. Thorax 2002;57:15–19.
29. Alobid I, Benıtez P, Bernal-SprekelsenM, Guilemany JM, Picado C, Mullol J.The impact of asthma and aspirin sen-sitivity on quality of life of patients withnasal polyposis. Qual Life Res2005;14:789–793.
30. Alobid I, Benıtez P, Bernal M, Roca J,Alonso J, Picado C et al. Nasal polyp-osis and its impact on quality of life.Comparison between the effects ofmedical and surgical treatments. Allergy2005;60:452–458.
31. Ware JE, Konsinski M, Keller SD.SF-36 Physical and Mental HealthSummary Scales: a user�s manual.Boston, MA: The Health Institute, NewEngland Medical Center, 1994.
32. Benninger MS. The impact of cigarettesmoking and environmental tobaccosmoke on nasal and sinus disease: areview of the literature. Am J Rhinol1999;13:435–438.
33. Hernandez C, Abreu J, Jimenez A,Fernandez R, Martin C. Pulmonaryfunction and quality of life in relation tobronchial colonization in adults withbronchiectasis not caused by cysticfibrosis. Med Clin (Barc) 2002;118:130–134.
34. Failde I, Ramos I. Validity and reli-ability of the SF-36 health survey ques-tionnaire in patients with coronaryartery disease. J Clin Epidemiol2000;53:359–365.
35. Espinosa De Los Monteros MJ,Alonso J, Ancochea J, Gonzalez A.Quality of life in asthma: reliabilityand validity of the short form genericquestionnaire (SF-36) applied to thepopulation of asthmatics in a publichealth area. Arch Bronconeumol2002;38:4–9.
36. Johansson L, Bramerson A, HolmbergK, Melen I, Akerlund A, Bende M.Clinical relevance of nasal polyps inindividuals recruited from a generalpopulation-based study. Acta Otolar-yngol 2004;124:77–81.
37. Radenne F, Lamblin C, VandezandeLM, Tillie-Leblond I, Darras J, TonnelAB et al. Quality of life in nasal polyp-osis. J Allergy Clin Immunol1999;104:79–84.
38. Dur DG, Desrosiers MY, Dassa C.Quality of life in patients with rhinosi-nusitis. J Otolarymgol 1999;28:108–111.
39. Hurst JR, Wilkinson TM, DonaldsonGC, Wedzicha JA. Upper airwaysymptoms and quality of life in chronicobstructive pulmonary disease (COPD).Respir Med 2004;98:767–770.
QoL in bronchiectasis
� 2009 John Wiley & Sons A/S Allergy 2009: 64: 1524–1529 1529

Tesis Doctoral III. Trabajo Experimental
141
Revisión 1. Relation between rhinosinusitis and bronchiectasis. Arch
Bronconeumol 2006;42:135-40.


Introducción
En los últimos años se ha demostrado que enferme-dades que se suponía exclusivamente pulmonares obronquiales suelen asociarse a afección nasal y parana-sal. El concepto de rinobronquitis1 ha suscitado la ideade que las vías respiratorias superior e inferior constitu-yen una única vía, con una enfermedad común que afec-ta a todo el aparato respiratorio. Esto se ha demostrado yconfirmado en múltiples estudios epidemiológicos, conlo que ha aparecido el concepto de “una única vía, unaúnica enfermedad” (fig. 1). El ejemplo más claro de di-cha asociación es la rinitis y el asma2, pues se ha de-mostrado que ambas se dan de forma conjunta en la ma-yoría de los asmáticos y que el tratamiento de la rinitispuede tener efectos beneficiosos en el curso del asma3.
Las vías respiratorias superiores e inferiores tienencomo función común la de acondicionar y canalizar elaire del exterior al interior de los pulmones. Dentro deesta función común existen unas funciones especializa-das propias de las diferentes áreas que la forman: humi-dificación, calentamiento, filtración, fonación e inter-cambio gaseoso4.
Mucosas nasal y bronquial
Las mucosas nasal y bronquial tienen una estructurasimilar en el epitelio y la lámina propia. Una de las fun-
ciones más importantes de la nariz es actuar como ba-rrera para evitar la inhalación de sustancias nocivas tan-to infecciosas como de naturaleza no infecciosa. La na-riz actúa, además, como acondicionador del airerespirado calentándolo y humidificándolo. La funciónque más diferencia la nariz de las vías aéreas inferioreses sin duda la olfativa, que le es propia y tiene su baseen la pituitaria, situada en el techo de la fosa nasal5.
El epitelio escamoso que se encuentra en la válvulanasal se transforma en el resto de la nariz en un epiteliorespiratorio columnar ciliado seudoestratificado. En lanariz dicho epitelio columnar está formado por célulasciliadas, células no ciliadas, células basales, células ca-liciformes o goblet, y se diferencia del epitelio respira-torio bajo porque no existen células serosas, células deClara y células en cepillo6. La membrana basal estácompuesta por colágeno tipo IV, proteoglucanos, lami-nina y fibronectina. Debajo de ésta existe la denomina-da lamina reticularis, que se encuentra engrosada demanera difusa en los pacientes asmáticos7. Se observanengrosamientos focales de dicha membrana en los pa-cientes afectados de bronquiectasias, tuberculosis y ri-nosinusitis crónica8. En los pacientes con rinitis no sehan detectado cambios en esta zona9.
En la submucosa hay glándulas, vasos sanguíneos,nervios, células extravasculares y matriz extracelular.Una de las grandes diferencias se encuentran aquí, yaque el músculo liso se halla en la capa submucosa delbronquio, pero no en la submucosa de la nariz6.
En la nariz predominan las glándulas y los vasos.Aparte de los vasos arteriales, la vascularización nasalestá formada por lechos capilares, cortocircuitos arte-
Correspondencia: Dr. J.M. Guilemany.Servei d’ORL. Hospital Clínic.Villarroel, 170, esc. 8, pl. 2. 08015. Barcelona. España.Correo electrónico:[email protected]
Recibido: 15-3-2005; aceptado para su publicación: 5-4-2005.
Arch Bronconeumol. 2006;42(3):135-40 135
REVISIÓN
Relaciones entre rinosinusitis y bronquiectasias
J.M. Guilemanya, J. Mullola y C. Picadob
aUnitat de Rinologia. Servei d’ORL (ICEMEQ). Hospital Clínic. Universitat de Barcelona. Barcelona. España.bServei de Pneumologia (ICPCT). Hospital Clínic. Universitat de Barcelona. Barcelona. España.
La nariz y el bronquio presentan similitudes y diferenciastanto histológicas como funcionales. Son muchas las enfer-medades en que se asocian la afección nasosinusal y la bron-quial. La fibrosis quística, la discinesia ciliar primaria, elsíndrome de Young y el déficit de alfa-1-antitripsina son en-fermedades en las que se asocian bronquiectasias y rinosinu-sitis. En este artículo se realiza una revisión de las bron-quiectasias y de las enfermedades que las asocian junto aafección nasosinusal. El propósito es dar un nuevo enfoquede la patología nasosinusal observada en los pacientes afec-tados de bronquiectasias.
Palabras clave: Rinitis. Sinusitis. Bronquiectasias.
Relation Between Rhinosinusitis and Bronchiectasis
The nose and lungs have both histological and functionalsimilarities and differences. Sinonasal and bronchialinvolvement are associated in many diseases. Cystic fibrosis,primary ciliary dyskinesia, Young’s syndrome, and α-1antitrypsin deficiency are diseases in which bronchiectasisand rhinosinusitis are both present. This review considersthe diseases in which bronchiectasis occurs along withsinonasal manifestations. We propose examining sinonasaldisease from a new perspective by observing it in patientswith bronchiectasis.
Key words: Rhinitis. Sinusitis. Bronchiectasis.
111.282
08 135-140 REV 4916 1/3/06 16:13 Página 135
Documento descargado de http://www.elsevier.es el 27/10/2009. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

riovenosos, sinusoides y vasos venosos. Las venas quedrenan los sinusoides contienen músculo liso. Cuandodichas venas se contraen, se produce una expansión delos sinusoides, por lo que se incrementa el tamaño delos cornetes (tejido eréctil) y se refleja en los flujos na-sales. Esto no sucede en los bronquios, donde los cam-bios de resistencia al flujo se deben a la contracción dela musculatura lisa.
Transporte mucociliar
El aparato mucociliar está formado por los numero-sos cilios que emergen de la superficie de las célulasepiteliales columnares seudoestratificadas. Cada célulaciliada contiene alrededor de 200-300 cilios que reali-zan unas 500 batidas por minuto. La frecuencia de bati-das disminuye distalmente10, de modo que en las víasmedias la frecuencia es menor. Su alteración en estazona puede conducir al estancamiento de secreciones ypredisposición a padecer infecciones locales, lo que po-siblemente contribuya al desarrollo de bronquiectasiasen esa parte de las vías respiratorias11. El defecto en laultraestructura de los cilios, que altera y evita su normalmotilidad, predispone a las infecciones crónicas y recu-rrentes (rinosinusitis crónica), infecciones pulmonaresque provocan la aparición de bronquiectasias.
Aproximadamente, el 70-80% de los asmáticos pre-sentan rinitis y, según estudios recientes, la rinitis es unfactor que predispone al desarrollo ulterior de asma12.Este hecho ha llevado a la realización de estudios confinalidad preventiva dirigidos a tratar precozmente la ri-nitis para evitar el asma.
La poliposis nasal se detecta en el 2-4% de la pobla-ción, mientras que en los pacientes asmáticos la prevalen-cia llega al 7%. En quienes padecen asma leve es pocohabitual encontrar poliposis; a medida que aumenta lagravedad de la enfermedad, aparecen sinusopatía y poli-posis nasal con mucha mayor frecuencia, hasta el puntode que es excepcional que entre los pacientes con asma eintolerancia a la aspirina no se observe poliposis nasal13.
También se ha observado que existe relación entre laenfermedad pulmonar obstructiva crónica (EPOC) y la
rinitis14, pues en las biopsias de mucosa nasal de los in-dividuos con EPOC se han apreciado alteraciones infla-matorias similares a las halladas en las biopsias bron-quiales de estos mismos pacientes15.
La asociación de la rinorrea anterior y posterior, delos estornudos, de la congestión nasal y de la pérdidadel olfato con los síntomas respiratorios induce asimis-mo a pensar en la relación entre las vías respiratorias al-tas y bajas16.
Bronquiectasias
La bronquiectasia es la destrucción y dilatación anor-mal, permanente e irreversible de uno o más bronquiosmedianos y pequeños (de la cuarta a la novena genera-ción), producida, por destrucción de los componentesmusculares y elásticos de la pared bronquial. Se ignoracuál es su prevalencia en la población general y tampo-co se conoce bien la historia natural de la enfermedad,ya que no se han realizado estudios desde el inicio delproceso y con posterior análisis de su evolución17.
Laennec18 (1819) fue quien describió la bronquiecta-sia y señaló que se debía a la retención de secrecionesbronquiales con destrucción secundaria de la pared yposterior debilitamiento y dilatación de la misma. Estainterpretación es aún válida y se considera que la infla-mación bronquial desempeña un papel central. En 1922,con la introducción de la broncografía con contraste porSicard, se pudo observar con mejor precisión la imagende las bronquiectasias19.
Etiopatogenia
La bronquiectasia no es en sí misma una única en-fermedad, sino que puede ser el resultado de diversasenfermedades que lesionan la pared bronquial e inter-fieren así en sus defensas, ya sea de forma directa o in-directa. La afección puede ser difusa o local. Es típicala dilatación de los bronquios de tamaño medio, pero amenudo los bronquios pequeños también presentan en-grosamiento u obliteración. En las bronquiectasias seencuentran áreas de la pared bronquial destruidas e in-
GUILEMANY JM ET AL. RELACIONES ENTRE RINOSINUSITIS Y BRONQUIECTASIAS
136 Arch Bronconeumol. 2006;42(3):135-40
Fig. 1. Rinosinusopatía crónica en laregión maxiloetmoidal bilateral (tomo-grafía axial computarizada de senos)junto a bronquiectasias bilaterales (to-mografía pulmonar) en un mismo pa-ciente.
08 135-140 REV 4916 1/3/06 16:13 Página 136
Documento descargado de http://www.elsevier.es el 27/10/2009. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

flamadas crónicamente; las células ciliadas están daña-das o destruidas y la producción de moco está aumen-tada, con lo que se pierde el tono normal de la pared.El aumento de la producción de moco facilita el creci-miento de las bacterias, obstruye los bronquios y favo-rece el estancamiento de las secreciones infectadas,con lesión posterior de la pared bronquial20. La infla-mación puede extenderse a los alveolos y producirbronconeumonía, formación de tejido cicatrizal y pér-dida del tejido pulmonar sano. Además, la inflamaciónde los vasos sanguíneos de la pared bronquial puedeocasionar expectoración hemoptoica o hemoptisis fran-ca. En el examen anatomopatológico se observan dila-taciones bronquiales, hipertrofia de la mucosa, en oca-siones con metaplasia escamosa, infiltrado linfocitariode la pared bronquial y desaparición de cartílago, mús-culo y fibras elásticas, que son sustituidas por tejido ci-catrizal21.
Las bronquiectasias localizadas suelen estar motiva-das por estenosis de algún bronquio debido a procesosinflamatorios, neoformativos o cuerpos extraños22.Cualquier circunstancia que produzca colapso por ab-sorción en la zona y fibrosis del tejido pulmonar adya-cente contribuye a la formación de bronquiectasias pordilatación compensadora del bronquio.
Las bronquiectasias difusas pueden deberse a múlti-ples causas (tabla I), entre las que destacan las enferme-dades congénitas que afectan a la función mucociliar,como son la fibrosis quística o las discinesias (síndromede Kartagener, síndrome de Young). En otras ocasionesse asocian a defectos en los mecanismos de defensa quefavorecen el desarrollo de infecciones bronquiales repe-tidas (inmunodeficiencia común variable, deficienciasde la formación de anticuerpos). Algunas bronquiecta-sias parecen haberse desarrollado a raíz de una bron-quiolitis infecciosa en la infancia (sarampión, virus res-piratorio sincitial). También pueden presentarse aso-ciadas a enfermedades sistémicas (artritis reumatoide,síndrome de Sjögren) o a enfermedades inflamatoriasintestinales (colitis ulcerosa, enfermedad de Crohn). Enun número reducido de casos pueden ser la consecuen-cia de la aspiración de sustancias tóxicas que lesionanlos bronquios.
Según su forma, existen 3 tipos de bronquiectasias:cilíndricas, varicosas y saculares (las 2 últimas suelenser las más graves clínicamente).
La biopsia de la mucosa bronquial revela la infiltra-ción por neutrófilos y linfocitos T21, además de un au-mento del contenido de elastasa en el esputo23 y un in-cremento de las concentraciones de interleucina 824,factor de necrosis tumoral alfa25 y prostanoides26.
La complicación más frecuente de las bronquiecta-sias es la sobreinfección27. La colonización más fre-cuente en estos pacientes es por Haemophilus influen-zae (55%) y Pseudomonas spp. (26%)28. Menosfrecuentes son el desarrollo de abscesos metastásicos depredomino en el sistema nervioso central (12-16%) ylas acumulaciones de amiloide tipo AA (6%). Otrascomplicaciones son la hipertensión pulmonar y el corpulmonale crónico. En las bronquiectasias saculares esmás frecuente encontrar los dedos en palillo de tambor.
Clínica
A pesar de que las bronquiectasias pueden producirsea cualquier edad, la enfermedad se inicia con mayor fre-cuencia en las primeras 2 décadas de la vida. Dado quelos síntomas pueden no manifestarse hasta mucho mástarde o incluso nunca, en algunas ocasiones se realiza eldiagnóstico radiológico cuando las bronquiectasias aúnson asintomáticas. La clínica más frecuente suele con-sistir en tos con expectoración abundante (broncorrea) yocasionalmente hemoptoica. La cantidad y el tipo de es-puto dependen de lo extensa que sea la enfermedad y dela presencia de una infección activa. En algunas ocasio-nes puede producirse hemoptisis masiva. Las neumo-nías son relativamente frecuentes y en algunos casos sepresentan de forma repetida. Las bronquiectasias exten-sas pueden llegar a ocasionar insuficiencia respiratoria,hipertensión pulmonar y cor pulmonale29.
Diagnóstico
El diagnóstico se realiza por historia clínica y radiolo-gía. La radiografía simple de tórax puede mostrar imá-genes muy indicativas de bronquiectasias como las de-nominadas en “raíl de tren”, quistes y bronquios rellenosde moco (imagen en dedos de guante), aunque lo másfrecuente es que sea normal o muestre cambios inespecí-ficos como el aumento de las marcas broncovasculares.Hoy día, la tomografía axial computarizada (TAC) de tó-rax permite diagnosticar la enfermedad con certeza altiempo que evalúa su localización y extensión30. Labroncografía, técnica usada en el diagnóstico antes de laintroducción de la TAC, ya no se utiliza.
El examen de la función pulmonar puede mostrar unpatrón obstructivo de grado diverso según la extensiónde la enfermedad, aunque no es infrecuente observar
GUILEMANY JM ET AL. RELACIONES ENTRE RINOSINUSITIS Y BRONQUIECTASIAS
Arch Bronconeumol. 2006;42(3):135-40 137
TABLA IEtiología de las bronquiectasias
Bronquiectasias localizadasObstrucción bronquial: aspiración de cuerpo extraño,
adenopatías, tumores pulmonares, tapón de moco
Bronquiectasias generalizadasCongénitas: discinesia ciliar primaria (síndrome de Kartagener),
fibrosis quística, deficiencia de alfa-1-antitripsina,traqueobroncomegalia (síndrome de Mounier-Kühn),deficiencia del cartílago (síndrome de Williams-Campbell),síndrome de Marfan, secuestro pulmonar
Postinfecciosa: viral (paramyxovirus, adenovirus,influenzavirus, virus de la inmunodeficiencia humana),bacteriana (Haemophilus, Pseudomonas, Klebsiella,Staphylococcus, Bordetella, Mycobacterium [M. tuberculosis]Mycoplasma [M. pneumoniae]), hongos (Aspergillus)
Alteraciones del sistema inmunitario: primaria(hipogammaglobulinemia, deficiencias del complemento),secundaria (leucemia linfocítica crónica, quimioterapia)
Tóxicos: inhalación de vapores tóxicos, aspiración de contenidogástrico
Enfermedades sistémicas: artritis reumatoide, lupus eritematososistémico, síndrome de Sjögren, policondritis recidivante
Otras: enfermedades inflamatorias intestinales (colitis ulcerosa,enfermedad de Crohn), síndrome de las uñas amarillas
08 135-140 REV 4916 1/3/06 16:13 Página 137
Documento descargado de http://www.elsevier.es el 27/10/2009. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

patrones mixtos ocasionados por la frecuente pérdida devolumen por colapso de algunos lóbulos asociada a laobstrucción. El intercambio de gases puede estar muyalterado debido a la presencia de zonas de cortocircuitoque causan en ocasiones hipoxemia acentuada31.
Tratamiento
El objetivo principal del tratamiento es controlar lasinfecciones y las secreciones, evitando la obstrucciónde las vías aéreas y sus complicaciones. Es fundamentalla fisioterapia respiratoria efectiva, con el fin de expul-sar las secreciones bronquiales. La disminución de al-gunas infecciones virales en la infancia gracias a la va-cunación ha permitido reducir el riesgo de desarrollarbronquiectasias. La vacunación contra el neumococo yHaemophilus y la vacunación anual contra el virus de lagripe contribuyen muy probablemente a disminuir elnúmero de episodios infecciosos graves32.
Enfermedades que ocasionan bronquiectasias y afección nasal asociada
Fibrosis quística
La fibrosis quística (FQ) es la alteración genética detipo autosómico recesivo más común en la poblacióncaucásica. Uno de cada 25 individuos es portador delgen33,34. Se calcula que afecta aproximadamente a unode cada 3.000-10.000 nacidos vivos por año. El gen res-ponsable de la FQ se encuentra en el locus simple delbrazo largo del cromosoma 7. La deleción de 3 pares debases o mutación delta F508 acontece aproximadamen-te en el 70% de todos los cromosomas de la FQ. La pro-teína defectuosa codificada por este gen anormal tieneuna estructura similar a la de una clase de proteínas co-nocidas por ser activas en el transporte epitelial y se hadenominado CFTR (cystic fibrosis transmembrane re-gulator)35. Esta proteína defectuosa contribuye al malfuncionamiento de los canales del cloro, lo cual provocaun aumento de la viscosidad del moco que dificulta sueliminación y favorece la colonización por Staphylococ-cus aureus y Pseudomonas mucoide.
Se han identificado muchas otras mutaciones cercadel locus afectado. Los pacientes con FQ se caracteri-zan por presentar infecciones repetidas en el tracto res-piratorio, insuficiencia pancreática exocrina e infertili-dad. En estadios tempranos la radiografía de tórax36
muestra afectación de los lóbulos superiores, que sevuelven difusos con la progresión de la enfermedad. Lafunción pulmonar puede ser normal o presentar un pa-trón de tipo obstructivo o mixto. En la presentaciónadulta de la enfermedad, los síntomas normalmente hanestado presentes durante años, pero muchas veces no setienen en cuenta al ser moderados. El adulto puede pre-sentar bronquiectasias, rinosinusitis, insuficiencia pan-creática, pancreatitis aguda, colelitiasis e infertilidad.La obstrucción nasal es el síntoma más frecuente entrelos pacientes con FQ. La incidencia de poliposis nasales de más del 20% de los pacientes. Hay diferentes pa-trones de rinosinusitis: pólipos nasales, rinosinusitiscrónica purulenta y mucopiosinusitis del antro del seno
maxilar con protrusión de la pared nasal lateral37. Estaúltima entidad recibe el nombre de seudomucocele ma-xilar. En el diagnóstico de la FQ es importante la prue-ba del sudor38 (las concentraciones de sodio o cloro sonde 60 mmol/l, mientras que en individuos sanos y porta-dores del gen de la FQ son de 30 mmol/l), el estudio ge-notípico y la TAC pulmonar y sinusal. Los objetivos deltratamiento son: reducir la obstrucción, controlar las in-fecciones39, disminuir la inflamación y mejorar el esta-do nutricional. El tratamiento nasal consiste en lavadoscon suero fisiológico, corticoterapia intranasal, antibio-terapia y, en caso necesario, cirugía endoscópica funcio-nal de senos.
Discinesia ciliar primaria
La discinesia ciliar primaria (DCP) es una enferme-dad congénita en la que existe una alteración total oparcial de la función de las células ciliadas40. Es una en-fermedad autosómica recesiva que afecta a uno de cada16.000 nacidos vivos y se presenta clínicamente con ri-nosinusitis, bronquiectasias y, de forma menos frecuen-te, esterilidad en los varones. En el síndrome de discine-sia (dificultad para el movimiento) ciliar primariaexisten alteraciones estructurales o funcionales en losmicrotúbulos de los cilios que son responsables del mo-vimiento de éstos. Tales alteraciones originan un malaclaramiento del moco de los cilios, con las consiguien-tes infecciones bronquiales supurativas y bronquiecta-sias. Se alteran todas las estructuras donde existen cilios: epitelios de las vías respiratorias, senos paranasa-les, trompa de Eustaquio y espermatozoides (astenos-permia)41.
El 50% de los individuos afectados presenta síndro-me de Kartagener, que se caracteriza por la tríada debronquiectasias, rinosinusitis crónica y situs inversus(dextrocardia)42,43. La rinitis con presencia de rinorreaanterior se encuentra en todos los enfermos afectadosde DCP, y en algunos casos se acompañan de póliposnasales y disminución o pérdida completa del olfato. Enla TAC de senos es típico observar ocupación de los se-nos etmoidales y maxilares, junto a hipoplasia del senofrontal. El diagnóstico se realiza mediante una combi-nación de pruebas, como son: tiempo de sacarina, óxidonítrico nasal, biopsia nasal, en la que se observa la fre-cuencia de batida de los cilios y la densidad de éstosmediante microscopia electrónica44. En el tratamientodel paciente con DCP resulta de gran importancia la fi-sioterapia respiratoria con drenaje postural y la antibio-terapia en las agudizaciones por infecciones respirato-rias. La realización de polipectomía endoscópica o decirugía endoscópica funcional de senos es beneficiosaen los pacientes con rinosinusitis crónica rebelde al tra-tamiento.
El diagnóstico se establece por el estudio ultraestruc-tural de muestras obtenidas de la mucosa nasal, en lasque se suele observar la ausencia de los brazos de la di-neína o la disposición anómala de los microtúbulos. Es-tudios recientes han demostrado concentraciones bajasde óxido nítrico nasal en los pacientes afectados de di-cha enfermedad45.
GUILEMANY JM ET AL. RELACIONES ENTRE RINOSINUSITIS Y BRONQUIECTASIAS
138 Arch Bronconeumol. 2006;42(3):135-40
08 135-140 REV 4916 1/3/06 16:13 Página 138
Documento descargado de http://www.elsevier.es el 27/10/2009. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

Síndrome de Young
El síndrome de Young se caracteriza por la tríada:bronquiectasias, rinosinusitis crónica e infertilidad. Enlos pacientes que lo presentan la actividad ciliar es nor-mal y el moco, muy viscoso. La biopsia nasal bajo mi-croscopia electrónica no muestra cambios en la estruc-tura de los cilios46. La azoospermia causante de lainfertilidad se debe a la obstrucción del epidídimo, yaque la espermiogénesis es totalmente normal. El diag-nóstico se basa en la clínica (enfermedad sinopulmonarcrónica, azoospermia), así como en la exclusión de FQy de síndromes de inmovilidad ciliar47.
Deficiencia de alfa-1-antitripsina
La alfa-1-antitripsina es una glucoproteína producidapor los hepatocitos, cuya función es inhibir las protea-sas (elastasa), en particular las liberadas por los neutró-filos, en su misión reparadora y de limpieza de agentesexternos en el pulmón. Al inhabilitar las proteasas, evitala destrucción de tejidos sanos en el organismo48. El genque la codifica está situado en el cromosoma 14. El dé-ficit pulmonar de alfa-1-antitripsina produce enfisemapor la destrucción progresiva de los alveolos en la terce-ra y cuarta décadas de la vida. El humo del tabaco con-tribuye a la destrucción pulmonar, ya que aumenta laactividad de la elastasa, disminuye la actividad de laalfa-1-antitripsina por su oxidación e inactiva la síntesisde elastina, lo que interfiere en la reparación pulmonar;por lo tanto, dejar de fumar debe ser la principal priori-dad del paciente diagnosticado de déficit de alfa-1-anti-tripsina49.
El enfisema producido por el déficit de alfa-1-anti-tripsina es paracinar, con destrucción de todo el ácino.Se localiza frecuentemente en las bases y existe un au-mento de la distensibilidad (compliance) pulmonar. Ladisminución de las concentraciones de alfa-1-antitripsi-na produce un desequilibrio entre esta proteína (antipro-teasa) y la elastasa (proteasa). Al no existir suficientecantidad de alfa-1-antitripsina, las elastasas siguen des-truyendo progresivamente la elastina de las paredes al-veolares50. Se consideran valores normales de proteínaalfa-1-antitripsina en sangre los comprendidos en el in-tervalo de 150 a 350 mg/dl o 20-53 µM. Con concentra-ciones inferiores a 80 mg/dl u 11 µM existe el riesgo depadecer alguna de las enfermedades relacionadas con sudéficit51. El segundo órgano más afectado es el hígado,afectando más frecuentemente a recién nacidos y niños.Los pacientes afectados presentan historia previa de dé-ficit de alfa-1-antitripsina o de enfermedad pulmonar.En el pulmón se observan enfisema, bronquitis crónica,bronquiectasias, asma de difícil tratamiento y neumo-nías de repetición. Se recomienda realizar medicionescuantitativas de alfa-1-antitripsina en los siguientes ca-sos: enfisema precoz, antecedentes familiares, disnea otos en varios miembros de una misma familia o diferen-tes generaciones, adultos con bronquiectasias sin etiolo-gía evidente, pacientes con enfermedad obstructiva pul-monar, enfermedad hepática de causa desconocida,pacientes asmáticos que no responden a tratamiento yen la paniculitis inexplicable52. La rinitis alérgica y las
rinosinusitis de repetición también constituyen una ma-nifestación frecuente en estos pacientes incluso en au-sencia de enfermedad obstructiva pulmonar53.
Conclusiones
De acuerdo con el concepto de “una única vía, unasola enfermedad”, los pacientes afectados de bronquiec-tasias presentan en muchos casos afectación nasosinu-sal. Se desconoce la frecuencia de esta asociación, yaque no se ha realizado un estudio sistemático de afecta-ción nasosinusal en pacientes con bronquiectasias. Nose sabe, por ejemplo, si los gérmenes que colonizan lasvías inferiores son los responsables del proceso nasal.Tampoco se ha investigado si las características de larespuesta inflamatoria de las vías bajas son similares alas nasales y sinusales. Dada la mejor accesibilidad dela nariz en la realización de exploraciones (endoscopia,biopsia, recogida de secreciones nasales) en compara-ción con las vías inferiores (fibrobroncoscopia), el con-trol evolutivo de la enfermedad pulmonar podría mejo-rar y ser menos invasivo. Se ha demostrado que eltratamiento de la rinitis alérgica y la poliposis nasal me-jora la evolución del paciente con asma, pero se desco-noce si algo similar puede ocurrir entre la sinusitis y lasbronquiectasias. La demostración de la presencia de unproceso infeccioso e inflamatorio similar de las vías aé-reas superiores e inferiores de los pacientes con bron-quiectasias permitirá realizar estudios encaminados aaclarar los mecanismos responsables de su origen.
BIBLIOGRAFÍA
1. Simons FE. Allergic rhinobronchitis: the asthma-allergic rhinitislink. J Allergy Clin Immunol. 1999;104:534-40.
2. Bachert C, Vignola AM, Gevaert P, Leynaert B, Van Cauwenber-ge P, Bousquet J. Allergic rhinitis, rhinosinusitis, and asthma: oneairway disease. Immunol Allergy Clin Am. 2004;24:19-43.
3. Bousquet J, Van Cauwenberge P, Khaltaev N; Aria WorkshopGroup; World Health Organization. Allergic rhinitis and its im-pact on asthma. J Allergy Clin Immunol. 2001;108:S147-334.
4. Proctor DF. The upper airways. Nasal physiology and defense ofthe lungs. Am Rev Respir Dis. 1977;115:97-119.
5. Zhao K, Scherer PW, Hajiloo SA, Dalton P. Effect of anatomy onhuman nasal air flow and odorant transport patterns: implicationsfor olfaction. Chem Senses. 2004;29:365-79.
6. Gaga M, Vignola AM, Chánez P. Upper and lower airways: simi-larities and differences. En: Wallaërt B, Chánez P, Godard P, edi-tors. The nose and lung diseases. Eur Respir Mon. 2001;6 Mon18:10-5.
7. Roche WR, Beasley R, Williams JH, Holgate ST. Subepithelial fi-brosis in the bronchi of asthmatics. Lancet. 1989;11;1:520-4.
8. Martínez-Hernandez A, Amenta PS. The basement membrane in pathology. Lab Invest. 1983;48:656-77.
9. Chánez P, Vignola AM, Vic P, Guddo F, Bonsignore G, GodardP, et al. Comparison between nasal and bronchial inflammation inasthmatic and control subjects. Am J Respir Crit Care Med. 1999;159:588-95.
10. Rutland J, Griffin WM, Cole PJ. Human ciliary beat frequency inepithelium from intrathoracic and extrathoracic airways. Am RevRespir Dis. 1982;125:100-5.
11. Owen CA, Campbell EJ, Hill SL, Stockley RA. Increased adhe-rence of monocytes to fibronectin in bronchiectasis. Am Rev Res-pir Dis. 1992;146:626-31.
12. Leynaert B, Neukirch F, Demoly P, Bousquet J. Epidemiologicevidence for asthma and rhinitis comorbidity. J Allergy Clin Im-munol. 2000;106:201-5.
GUILEMANY JM ET AL. RELACIONES ENTRE RINOSINUSITIS Y BRONQUIECTASIAS
Arch Bronconeumol. 2006;42(3):135-40 139
08 135-140 REV 4916 1/3/06 16:13 Página 139
Documento descargado de http://www.elsevier.es el 27/10/2009. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

13. Settipane GA, Chafee FH. Nasal polyps in asthma and rhinitis. Areview of 6,037 patients. J Allergy Clin Immunol. 1977;59:17-21.
14. Hurd S. The impact of COPD on lung health worldwide: epide-miology and incidence. Chest. 2000;117:1S-4S.
15. Vachier I, Vignola AM, Chiappara G, Bruno A, Meziane H, Go-dard P, et al. Inflammatory features of nasal mucosa in smokerswith and without COPD. Thorax. 2004;59:303-7.
16. Roberts NJ, Lloyd-Owen SJ, Rapado F, Patel IS, Wilkinson TM, Do-naldson GC, et al. Relationship between chronic nasal and respiratorysymptoms in patients with COPD. Respir Med. 2003;97:909-14.
17. Angrill J, Agustí C, Torres A. Bronchiectasis. Curr Opin InfectDis. 2001;14:193-7.
18. Laennec RTH. A treatise on the disease of the chest. New York:Library of the New York Academy of Medicine, Hafner Publis-hing; 1962. p. 78.
19. Reid LM. Reduction in bronchial subdivision in bronchiectasis.Thorax. 1950;5:233-47.
20. Cole PJ. Inflammation: a two-edged sword –the model of bron-chiectasis. Eur J Respir Dis Suppl. 1986;147:6-15.
21. Gaga M, Bentley AM, Humbert M, Barkans J, O’Brien F, WathenCG, et al. Increases in CD4+ T lymphocytes, macrophages, neu-trophils and interleukin 8 positive cells in the airways of patientswith bronchiectasis. Thorax. 1998;53:685-91.
22. Limper AH, Prakash UB. Tracheobronchial foreign bodies inadults. Ann Intern Med. 1990;15:604-9.
23. Tsang KW, Chan K, Ho P, Zheng L, Ooi GC, Ho JC, et al. Sputumelastase in steady-state bronchiectasis. Chest. 2000;117:420-6.
24. Richman-Eisenstat JB, Jorens PG, Hebert CA, Ueki I, Nadel JA.Interleukin-8: an important chemoattractant in sputum of patientswith chronic inflammatory airway diseases. Am J Physiol. 1993;264:L413-8.
25. Shum DK, Chan SC, Ip MS. Neutrophil-mediated degradation oflung proteoglycans: stimulation by tumor necrosis factor-alpha insputum of patients with bronchiectasis. Am J Respir Crit CareMed. 2000;162:1925-31.
26. Tamaoki J, Chiyotani A, Kobayashi K, Sakai N, Kanemura T, Ta-kizawa T. Effect of indomethacin on bronchorrhea in patients withchronic bronchitis, diffuse panbronchiolitis, or bronchiectasis. AmRev Respir Dis. 1992;145:548-52.
27. Angrill J, Agustí C, De Celis R, Rano A, González J, Solé T, et al.Bacterial colonisation in patients with bronchiectasis: microbiolo-gical pattern and risk factors. Thorax. 2002;57:15-9.
28. Nicotra MB, Rivera M, Dale AM, Shepherd R, Carter R. Clinical,pathophysiologic, and microbiologic characterization of bron-chiectasis in an aging cohort. Chest. 1995;108:955-61.
29. Barker AF. Bronchiectasis. N Engl J Med. 2002;346:1383-93.30. Hansell DM. Bronchiectasis. Radiol Clin North Am. 1998;36:107-28.31. Patel IS, Vlahos I, Wilkinson TM, Lloyd-Owen SJ, Donaldson
GC, Wilks M, et al. Bronchiectasis, exacerbation indices, and in-flammation in chronic obstructive pulmonary disease. Am J Res-pir Crit Care Med. 2004;170:400-7.
32. Keistinen T, Saynajakangas O, Tuuponen T, Kivela SL. Bron-chiectasis: an orphan disease with a poorly understood prognosis.Eur Respir J. 1997;10:2784-7.
33. Rommens JM, Iannuzzi MC, Kerem B, Drumm ML, Melmer G,Dean M, et al. Identification of the cystic fibrosis gene: chromoso-me walking and jumping. Science. 1989;245:1059-65.
34. Collins FS. Cystic fibrosis: molecular biology and therapeutic im-plications. Science. 1992;256:774-9.
35. Gilljam M, Ellis L, Corey M, Zielenski J, Durie P, Tullis DE. Cli-nical manifestations of cystic fibrosis among patients with diagno-sis in adulthood. Chest. 2004;126:1215-24.
36. Wood B. Cystic fibrosis: 1997. Radiology. 1977;204:1-10.37. Yung MW, Gould J, Upton GJ. Nasal polyposis in children with
cystic fibrosis: a long-term follow-up study. Ann Otol RhinolLaryngol. 2002;111:1081-6.
38. Wang L, Freedman SD. Laboratory tests for the diagnosis of cys-tic fibrosis. Am J Clin Pathol. 2002;117:109-15.
39. Salcedo A, Girón RM, Beltrán B, Martínez A, Máiz L, Suárez L;Fundación Sira Carrasco. Conferencia de consenso. Tratamientoantibiótico intravenoso domiciliario en la fibrosis quística; 2002,abril 26. Arch Bronconeumol. 2003;39:469-75.
40. Bush A, O’Callaghan C. Primary ciliary dyskinesia. Arch DisChild. 2002;87:363-5.
41. Coren ME, Meeks M, Morrison I, Buchdahl RM, Bush A. Primaryciliary dyskinesia: age at diagnosis and symptom history. Acta Pa-ediatr. 2002;91:667-9.
42. Chin GY, Karas DE, Kashgarian M. Correlation of presentationand pathologic condition in primary ciliary dyskinesia. Arch Oto-laryngol Head Neck Surg. 2002;128:1292-4.
43. Armengot M, Carda C, Escribano A, Samper GJ. Estudio deltransporte mucociliar y de la ultraestructura ciliar nasales en pa-cientes con síndrome de Kartagener. Arch Bronconeumol. 2005;41:11-5.
44. Noone PG, Leigh MW, Sannuti A, Minnix SL, Carson JL, Hazu-cha M, et al. Primary ciliary dyskinesia: diagnostic and phenoty-pic features. Am J Respir Crit Care Med. 2004;169:459-67.
45. Corbelli R, Bringolf-Isler B, Amacher A, Sasse B, Spycher M,Hammer J. Nasal nitric oxide measurements to screen children forprimary ciliary dyskinesia. Chest. 2004;126:1054-9.
46. Domingo C, Mirapeix RM, Encabo B, Roig J, López D, Ruiz J.Hallazgos clínicos y ultraestructura de la discinesia ciliar primariay el síndrome de Young. Rev Clin Esp. 1997;197:100-3.
47. Handelsman DJ, Conway AJ, Boylan LM, Turtle JR. Young’ssyndrome: Obstructive azoospermia and chronic sinopulmonaryinfections. N Engl J Med. 1984;310:3-9.
48. Tomashefski JF Jr, Crystal RG, Wiedemann HP, Mascha E, Sto-ller JK; Alpha 1-Antitrypsin Deficiency Registry Study Group.The bronchopulmonary pathology of alpha-1 antitrypsin (AAT)deficiency: findings of the Death Review Committee of the natio-nal registry for individuals with Severe Deficiency of Alpha-1 An-titrypsin. Hum Pathol. 2004;35:1452-61.
49. Hutchison DC, Cooper D; British Thoracic Society. Alpha-1-an-titrypsin deficiency: smoking, decline in lung function and impli-cations for therapeutic trials. Respir Med. 2002;96:872-80.
50. Lomas DA, Parfrey H. Alpha1-antitrypsin deficiency. 4: Molecu-lar pathophysiology. Thorax. 2004;59:529-35.
51. De la Roza C, Costa X, Vidal R, Vila S, Rodríguez-Frías F, JardíR, et al. Programa de cribado para el déficit α 1-antitripsina en pa-cientes con EPOC mediante el uso de gota de sangre en papel se-cante. Arch Bronconeumol. 2003;39:8-12.
52. Strange C, Dickson R, Carter C, Carpenter MJ, Holladay B, Lund-quist R, et al. Genetic testing for alpha1-antitrypsin deficiency.Genet Med. 2004;6:204-10.
53. American Thoracic Society/European Respiratory Society State-ment. Standards for the diagnosis and management of individualswith alpha-1 antitrypsin deficiency. Am J Respir Crit Care Med.2003;168:818-900.
GUILEMANY JM ET AL. RELACIONES ENTRE RINOSINUSITIS Y BRONQUIECTASIAS
140 Arch Bronconeumol. 2006;42(3):135-40
08 135-140 REV 4916 1/3/06 16:13 Página 140
Documento descargado de http://www.elsevier.es el 27/10/2009. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

Tesis Doctoral III. Trabajo Experimental
149
Cartas al Editor 1. "Una vía respiratoria unificada": las bronquiectasias
también se asocian a rinosinusitis crónica y pólipos nasales. Arch
Bronconeumol 2009 (en prensa). DOI:10.1016/j.arbres.2009.03.006


ARTICLE IN PRESS
Arch Bronconeumol. ]]]];](]):]]]–]]]
0300-28
doi:10.1
Comrinos
www.archbronconeumol.org
Carta al Director
Una vıa respiratoria unificada: las bronquiectasias tambien seasocian a rinosinusitis cronica y polipos nasales
A United Airway: Bronchiectasis Is Also Associated With ChronicRhinosinusitis and Nasal Polyps
Sr. Director:
En noviembre de 2008, ARCHIVOS DE BRONCONEUMOLOGIA publico lanormativa de la Sociedad Espanola de Neumologıa y CirugıaToracica (SEPAR) sobre el diagnostico y tratamiento de lasbronquiectasias1. Aunque de enorme importancia para el diag-nostico y tratamiento de las bronquiectasias, el documento nomenciona en absoluto el impacto que dicha enfermedad tiene enla vıa respiratoria superior en forma de rinosinusitis cronica con ysin polipos nasales, hecho que ya se habıa puntualizado en unartıculo de revision publicado en esta Revista en 20062.
El concepto de ‘‘una vıa unica’’ se ha demostrado mediante laasociacion epidemiologica, fisiopatologica, de diagnostico ytratamiento de la enfermedad broncopulmonar con la nasosinu-sal: asma con rinitis alergica3, asma con poliposis nasal4, asma noalergica y enfermedad pulmonar obstructiva cronica con rinosi-nusitis cronica5. La experiencia clınica en los Servicios deOtorrinolaringologıa y Neumologıa del Hospital Clınic de Barce-lona ha llevado a investigar desde hace varios anos la asociacionde enfermedad nasosinusal en pacientes con bronquiectasias.
Como fruto de esta investigacion, contamos hoy dıa con 2artıculos publicados6,7 y uno actualmente en prensa sobre laasociacion de bronquiectasias y rinosinusitis cronica con o sinpoliposis nasal. Entre sus conclusiones, debemos destacar que 3de cada 4 (77%) pacientes con bronquiectasias reunen criteriosclınicos y radiologicos de rinosinusitis cronica, mientras uno decada 4 (25%) presenta polipos nasales en la endoscopia nasal7.Dichos resultados apoyan el concepto de ‘‘una unica vıa aerea’’ eindican que en las llamadas bronquiectasias postinfecciosaspodrıa haber algun proceso todavıa desconocido que afectara atoda la vıa aerea. Ademas, los pacientes con bronquiectasias yrinosinusitis cronica tienen una peor calidad de vida, medidatanto con cuestionarios genericos como especıficos, que losafectados de bronquiectasias sin sinusopatıa cronica6.
De estos resultados se puede concluir que los pacientes conbronquiectasias deberıan evaluarse siempre, tanto clınicamentocomo mediante endoscopia nasal y/o tomografıa computarizada
96/$ - see front matter & 2009 SEPAR. Publicado por Elsevier Espana, S.L. Todo
016/j.arbres.2009.03.006
o citar este artıculo: Guilemany Toste JM, et al. Una vıa resinusitis cronica y polipos nasales. Arch Bronconeumol. 2009. d
nasosinusal, a fin de diagnosticar una posible rinosinusitis cronica,con o sin polipos nasales. Ası pues, a todos los pacientes conbronquiectasias, ademas de aquellos con asma y enfermedadpulmonar obstructiva cronica, se les deberıa realizar un estudiootorrinolaringologico, idealmente en unidades multidisciplinarias,con el objetivo de mejorar su diagnostico, tratamiento yseguimiento tanto de la enfermedad broncopulmonar como dela nasosinusal.
Bibliografıa
1. Vendrell M, De Gracia J, Oliveira C, Martınez MA, Giron R, Maiz L, et al. ArchBronconeumol. 2008;44:629–40.
2. Guilemany JM, Mullol J, Picado C. Rlation between rhinosinusitis andbronchiectasis. Ach Bronconeumol. 2006;42:135–40.
3. Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, Togias A, et al. AlergicRhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration withthe World Health Organization, GA2LEN and AllerGen). Allergy. 2008;63(Suppl86):8–160.
4. Fokkens W, Lund V, Mullol J, European Position Paper on Rhinosinusitis andNasal Polyps group. European position paper on rhinosinusitis and nasal polyps2007. Rhinology. 2007(20):1–136.
5. Hens G, Vanaudenaerde BM, Bullens DM, Piessens M, Decramer M, Dupont LJ,et al. Sinonasal pathology in nonallergic asthma and COPD: ‘‘united airwaydisease’’ beyond the scope of allergy. Allergy. 2008;63:261–7.
6. Guilemany JM, Alobid I, Angrill J, Ballesteros F, Bernal-Sprekelsen M, Picado C,et al. The impact of bronchiectasis associated to sinonasal disease on quality oflife. Respir Med. 2006;100:1997–2003.
7. Guilemany JM, Angrill J, Alobid I, Centellas S, Pujols L, Bartra J, et al. Unitedairway again: high prevalence of rhinosinusitis and nasal polyps in bronch-iectasis. Allergy. 2009;64:790–7.
Josep Maria Guilemany Toste a,b,c, Cesar Picado Valles b,c,d yJoaquim Mullol i Miret a,b,c,�
aUnitat de Rinologia i Clınica de l’Olfacte, Servei d’Otorrino-
laringologia, Hospital Clınic, Barcelona, EspanabCentro de Investigacion Biomedica en Red de Enfermedades
Respiratorias (CibeRes)cImmunoal � lergia Respiratoria Clınica i Experimental, IDIBAPS,
Barcelona, EspanadServei de Pneumologia i Al � lergia Respiratoria, Institut Clınic del
Torax, Hospital Clınic, Barcelona, Espana
�Autor para correspondencia.Correo electronico: [email protected] (J. Mullol i Miret)
s los derechos reservados.
piratoria unificada: las bronquiectasias tambien se asocian aoi:10.1016/j.arbres.2009.03.006


IV. DISCUSIÓN

Tesis Doctoral IV. Discusión
155
DISCUSIÓN GENERAL
Los principales hallazgos de los diferentes estudios que conforman esta
tesis doctoral son: 1º) Existe una alta prevalencia de RSC (77%) y PN
(25%) en los pacientes con BQ; 2º) la gravedad de las BQs está relacionada
con la presencia de RSC ó PN; 3º) El porcentaje de RSC ó PN es similar
entre los pacientes con BQs independientemente de que la causa sea post-
infecciosa o idiopática; 4º) El ON nasal está disminuido en los pacientes
con PN, disminuyendo conforme aumenta la afectación del complejo
ostiomeatal; 5º) Las BQs con RSC tienen una repercusión considerable en
la calidad de vida de los pacientes, no existiendo un aumento de esta
repercusión en los pacientes con RSC con pólipos nasales; y 6º) La RSC
con o sin pólipos tiene un considerable impacto en la calidad de vida de los
pacientes con BQs.
1º) Los pacientes con BQs presentaron una alta prevalencia de
rinosinusitis crónica (77%) y poliposis nasal (25%) (Estudio 1).
El reciente concepto de “una vía aérea unificada” también conocido
por “una vía, una patología” sostiene que los procesos inflamatorios de la
vía aérea superior e inferior a menudo coexisten y muestran mecanismos
etiopatogénicos similares, con lo que recomienda un diagnóstico,
tratamiento y seguimiento unificados. Esta coexistencia está ampliamente
demostrada en patologías como la rinitis y el asma.3,55 Este es el primer
estudio que examina y describe en profundidad la presencia y extensión de
la patología nasosinusal en los pacientes afectos de BQs en fase estable.
Muchos estudios han relacionado la patología de la vía aérea superior e
inferior, confirmando la existencia de una correlación entre el grado de
inflamación de la vía aérea superior e inferior en pacientes afectos de asma

IV. Discusión Tesis Doctoral
156
y EPOC.110 Estudios previos observaron una alta prevalencia de
rinosinusitis (58-70%) en pacientes con BQs.232,265,274,275 Los criterios
diagnósticos utilizados en estos estudios no están claramente mencionados
y en algunos casos el diagnóstico se basaba en síntomas y radiografia
simple de senos. Debido a que en ningún estudio se utilizó la TC
nasosinusal y la endoscopia nasal para el diagnóstico de RSC con o sin
pólipos, dichas enfermedades están definidas de manera poco precisa y sin
estudios de extensión. Pasteur et al. publicaron que el 31% de los pacientes
con BQs tenían historia de rinosinusitis sin aportar datos sobre síntomas
nasales, TC nasosinusal ni endoscopia nasal.232 En otro estudio Smith et al.
concluyeron que casi el 70% de los pacientes con BQs presentaban
rinitis.275 En un estudio más reciente, King et al. mostraba que los síntomas
más frecuentes en los pacientes con BQs eran la tos productiva crónica
(98%), la RSC (70%), la disnea (62%) y la fatiga (74%).274 Este estudio
definía la RSC como una enfermedad crónica de la vía aérea superior de
más de un año de duración, cuyos síntomas variaban desde una rinorrea
leve e intermitente hasta una sinusitis purulenta grave. El 47% de estos
pacientes presentaban alteraciones sinusales desde una hipertrofía mucosa
hasta la ocupación completa de los senos (pansinusitis) en el estudio
radiológico convencional. Otros síntomas nasales presentes en la RSC
como la obstrucción nasal y la alteración del sentido del olfato no fueron
estudiados.
Recientemente se ha publicado la actualización de las
recomendaciones basadas en evidencias en el diagnóstico y tratamiento de
la rinosinusitis: el documento EP3OS.111 La rinosinusitis crónica se define
clínicamente con la presencia de dos o más síntomas nasales que persisten
más de 12 semanas con signos endoscópicos y/o cambios en la TC
nasosinusal definen la RSC, incluyendo los pólipos nasales. Los pacientes
con BQs presentan como síntomas más frecuentes la rinorrea anterior,

Tesis Doctoral IV. Discusión
157
rinorrea posterior y obstrucción nasal, lo cual está de acuerdo con los
síntomas más frecuentemente hallados en los pacientes con RSC según los
criterios EP3OS. Un importante hallazgo endoscópico observado en más del
60% de los pacientes es la descarga mucosa a nivel de meato medio.
Utilizando criterios EP3OS, el 77% de los pacientes con BQ presentaban
RSC, mientras que el 25% presentaban poliposis nasal leve-moderada. Los
pacientes con PN fueron diagnosticados de BQs más de 10 años antes que
los pacientes sin patología nasal.
La proteína C reactiva (PCR) se produce en el hígado y su nivel se
eleva cuando hay alguna inflamación en el cuerpo. Entre los pacientes con
BQs, la PCR está significativamente elevada en los pacientes con RSC
comparado con los pacientes sin patologia nasosinusal. La afectación a
nivel sistémico es mayor si el paciente afecto de BQs asocia patologia
nasosinusal.
En los pacientes asmáticos, el seno etmoidal es el más afectado
cuando existe RSC276 mientras que en los pacientes con BQs, los senos
maxilares y los etmoidales, junto a obliteración del complejo ostiomeatal
fueron los más afectados entre los pacientes con RSC con o sin pólipos,
mientras que los pacientes con RSC sin PN tienen una puntuación total
inferior en la TC nasosinusal que los pacientes con RSC con PN. El 30% de
los pacientes con asma presentan poliposis nasal. En términos generales, la
RSC de los pacientes asmáticos es más grave, más extensa y de peor
control que la de los pacientes sin asma.
2º) La gravedad de las BQs se relaciona con la presencia de RSC o PN
(Estudio 1).
Diversos estudios han demostrado la relación entre RSC y asma,111
teniendo la mayoría de los pacientes con asma grave síntomas

IV. Discusión Tesis Doctoral
158
nasosinusales, frecuentemente dentro del contexto de una RSC. El 30% de
los pacientes con RSC con pólipos nasales presentan asma. La frecuencia
de hiperreactividad bronquial en la población general es de 12-14%,
mientras que en los pacientes con poliposis nasal es del 53-55%.111
La TC pulmonar de alta resolución constituye el gold-standard en el
diagnóstico de las BQs.277 En nuestro estudio los pacientes con RSC
presentaron una mayor afectación pulmonar evaluada mediante la TC
pulmonar de alta resolución en comparación con los pacientes sin RSC, sin
existir diferencias entre pacientes con o sin PN.
Este hallazgo sugiere que la presencia de RSC con o sin pólipos en
los pacientes con BQs constituye un marcador de mayor actividad y
extensión de la patología a nivel de la vía aérea inferior.
3º) La prevalencia de RSC y de PN es alta en los pacientes con BQs,
independientemente de que la causa sea post-infecciosa o idiopática
(Estudio 1).
Una gran parte de casos de BQs se consideran post-infecciosas
debido a un episodio infeccioso pulmonar grave que precede los síntomas
de las BQs y las anomalías radiológicas. La existencia de dilataciones
bronquiales permanentes antes del episodio infeccioso o un deficitario
sistema defensivo que preceda tanto el episodio infeccioso inicial como el
posterior desarrollo completo de la BQ no ha podido ser excluido como el
origen de algunas de dichas supuestas BQs post-infecciosas. Asumimos
que en el caso de las BQs debidas a una lesión directa de las vías aéreas
inferiores, la vía aérea superior debería permanecer intacta de algún
proceso nasal y sinusal. Contrariamente pero de acuerdo con la teoría de la
“única vía aérea” la mayoría de las BQs idiopáticas debidas a algún déficit
defensivo o a alguna alteración metabólica desconocidos debería asociarse
Tesis Doctoral IV. Discusión
159
a patología de la vía aérea superior. El hecho de que en nuestra serie no
encontramos diferencias significativas entre la causa post-infecciosa y la
idiopática, tanto en prevalencia como en extensión de la RSC con o sin
pólipos, sugiere que la mayoría de las BQs consideradas como secundarias
a daño infeccioso directo comparten mecanismos comunes con las BQs
idiopáticas.
4º) El ON nasal está disminuido en los pacientes con RSC con PN y su
valor disminuye conforme aumenta la afectación del complejo ostiomeatal
(Estudio 1).
En la vía aérea superior sana, el óxido nítrico (ON) esta siendo
continuamente producido por el seno maxilar y, a través del complejo
ostiomeatal, liberado posteriormente a las fosas nasales.278 El complejo
ostiomeatal es una unidad funcional que comprende el ostium del seno
maxilar, las celdas etmoidales anteriores y su ostium, el infundíbulo
etmoidal, el hiatus semilunaris y el meato medio. El ON presenta
propiedades antivirales y antibacterianas, jugando un papel clave en la
inmunidad.
Actualmente sabemos que el ON nasal está elevado en los pacientes
con rinitis alérgica, mientras que persiste cierta controversia en sus datos
para la RSC con o sin pólipos.166 Lindberg et al.279 encontró bajos los
niveles de ON nasal en pacientes con RSC comparado con los controles
sanos. Otros estudios también muestran que los niveles de ON nasal estan
inversamente correlacionados con la extensión de la PN, probablemente
relacionado con el bloqueo del complejo ostiomeatal.280,281 También se han
observado niveles de ON nasal más reducidos cuanta más extensa es la
afectación de la TC nasosinusal y mayor es el número de senos
ocupados.166,280 En nuestro estudio, las concentraciones de ON nasal fueron
IV. Discusión Tesis Doctoral
160
similares en los diferentes grupos, excepto en los pacientes con PN, en los
cuales el ON nasal se encontró en concentraciones menores que en los
pacientes sin RSC y sin pólipos. También se observó que el ON nasal
estaba más bajo conforme aumentaba la puntuación del complejo
ostiomeatal en la TC nasosinusal.
El ON exhalado se considera un marcador no invasivo de la
inflamación a nivel de la vía aérea inferior. Se han encontrado niveles altos
de ON exhalado en pacientes con asma no tratado que disminuye con el
tratamiento antiinflamatorio e incluso constituye un marcador de gravedad
en su seguimiento. No obstante en otras enfermedades pulmonares como la
fibrosis quística, a pesar de existir niveles muy altos de inflamación, los
niveles de ON exhalado son inferiores que los de la población general sana.
Por lo tanto, no está claro que el ON exhalado sirva de marcador
inflamatorio en todas las enfermedades inflamatorias de la vía aérea
inferior. Kharitonov et al.282 han publicado la existencia de niveles elevados
de ON exhalado en las BQs, en contraste con lo hallado en otros estudios
en los que se encontraron valores normales283 e incluso disminuidos.284
Nuestros resultados coinciden con el trabajo de Narang et al.283 en el que no
se observa un incremento significativo del ON exhalado.
5º) Los pacientes con BQs y RSC tienen una importante repercusión en su
calidad de vida que no se ve aumentada en los pacientes con RSC con
pólipos (Estudio 2).
Este constituye el primer estudio sobre la repercusión de la patología
nasosinusal sobre la calidad de vida en pacientes con BQ utilizando el
cuestionario genérico SF-36. Este estudio demostró que la calidad de vida
en los pacientes con BQs y RSC está peor en todos los dominios del SF-36
comparado con la población general, no existiendo una clara relación
asociación entre la calidad de vida y la edad, los síntomas nasales o el
Tesis Doctoral IV. Discusión
161
tamaño de los pólipos. También pudimos observar que las mujeres con
BQs presentaban peor calidad de vida en la función física y la función
social que los hombres. Utilizando también el SF-36, Bousquet et al. ya
habían observado que los hombres con asma presentan una mejor calidad
de vida que las mujeres asmáticas.285 Las diferencias en calidad de vida
derivadas del género del paciente en una enfermedad crónica como el asma
son importantes para saber adaptar el manejo de cada paciente a un nivel
individual.286 Las mujeres afectas de fibrosis quística (FQ) presentan
también una peor puntuación en calidad de vida que los hombres. Los
estudios parecen concluir que los hombres y las mujeres percibimos
nuestro estado de salud de manera diferente, teniendo las mujeres una
percepción más objetiva sobre el estado de salud propio.287
El SGRQ se ha utilizado para evaluar la calidad de vida en los
pacientes con patología pulmonar como el asma, la EPOC, el déficit de α1-
antitripsina,288-291 y más recientemente con las BQ. Además se ha
observado que la ansiedad y la depresión son muy frecuentes en los
pacientes con BQs.292 La Pseudomona auruginosa es el microorganismo
más relevante causando infecciones crónicas a nivel pulmonar en pacientes
con patologías crónicas como sería la FQ, BQs y EPOC. Las
hipermutaciones de la pseudomona serían el factor clave para el desarrollo
de su resistencia a los antibióticos, lo cual tiene consecuencias importantes
en el tratamiento de estas infecciones.293,294 La calidad de vida de pacientes
con BQs medida con SGRQ, junto a la función pulmonar y la colonización
(por pseudomonas u otros microorganismos) demuestran que los pacientes
colonizados por pseudomonas presentan una peor función pulmonar y
calidad de vida que los pacientes no colonizados. Además los pacientes
colonizados por otros microorganismos, exceptuando la pseudomona,
presentan también una peor calidad de vida que los no colonizados.295

IV. Discusión Tesis Doctoral
162
La RSC es una enfermedad inflamatoria crónica de la mucosa
nasosinusal cuyos síntomas duran más de 12 semanas. Actualmente, no
está todavía claro si la RSC con o sin pólipos son diferentes estadios de una
misma enfermedad o constituyen diferentes enfermedades. Los síntomas
que más diferenciarían la RSC con o sin pólipos serían una mayor
intensidad de la obstrucción nasal y de la alteración del olfato,296 aunque
también por diferencias a nivel de expresión de marcadores
inflamatorios.297.
Radenne et al. han investigado la repercusión de los pólipos nasales en
la calidad de vida, demostrando un empeoramiento en todos los dominios
del SF-36.298 Más recientemente nuestro grupo ha demostrado que el
asma190 y la atopia,194 pero no la intolerancia a la aspirina, tiene un impacto
negativo en la calidad de vida de los pacientes con pólipos.190 La calidad de
vida mejora después del tratamiento de la PN, asociandose a la mejoría
clínica, y tanto el tratamiento médico como el quirúrgico tienen similares
efectos mejorando la calidad de vida.112 Los pacientes en los que la rinitis
alérgica y el asma coexisten presentan más limitaciones físicas que los
pacientes con rinitis alérgica sólo.299 Gliklich y Metson investigaron la
importancia de la RSC sobre la calidad de vida utilizando el SF-36,
demostrando un descenso significativo en los dominios del dolor corporal,
salud general, vitalidad y función social comparados con la población
general americana.300 Utilizando el SF-36, otros estudios también han
demostrado que la RSC tiene un considerable impacto en todos los
dominios del SF-36 excepto en la función física, comparado con la
población sana.301-303 Alobid et al. concluyeron que no existen correlaciones
entre la calidad de vida y los síntomas nasales, tamaño de los pólipos,
ocupación en la TC de senos, permeabilidad nasal y atopia en pacientes con
poliposis nasal masiva.194
Tesis Doctoral IV. Discusión
163
Es interesante destacar como los pacientes con PN presentan peores
puntuaciones en todos los dominios del SF-36 excepto en la función física
y el rol emocional comparado con los pacientes afectos de cardiopatía
isquémica,304 EPOC,305 y asma306.
En nuestro estudio los pacientes con BQs y PN leve-moderada
(Clasificación Lildholdt <1,5) no mostraron una mayor repercusión en la
calidad de vida. Los síntomas más invalidantes fueron la rinorrea anterior,
la rinorrea posterior y la obstrucción nasal. Los pacientes con PN
presentaron además una mayor obstrucción nasal y pérdida de olfato pero
sin presentar diferencias en la calidad de vida.
6º) La RSC con o sin pólipos tiene un considerable impacto en la calidad
de vida de los pacientes con BQs (Estudio 3).
La puntuación global del SNOT-20 en pacientes con BQ que
presentaban criterios de RSC, con o sin pólipos, fue de 2,1. Esta puntuación
fue ligeramente superior al registrado en los pacientes con RSC durante la
validación del SNOT-20, que había sido de 1,9.307 A su vez, la puntuación
en los pacientes con BQs sin RSC (0,4) fue similar a la hallada en el grupo
control de la validación del test (0,6).307 Así pues, en nuestro estudio en la
calidad de vida, no existen diferencias medidas por SNOT-20 entre
pacientes con RSC con o sin pólipos. No obstante, SNOT-20 no presenta
preguntas sobre la obstrucción nasal y la pérdida de olfato y esto puede ser
determinante en la repercusión sobre la calidad de vida.
Los pacientes con BQs mostraban una importante reducción de su
calidad de vida cuando presentaban RSC asociada, sin existir una
repercusión añadida por tener PN. En los pacientes afectados de EPOC con
síntomas nasales, no se ha observado ninguna correlación entre el SNOT-
20 y el SGRQ total (r: 0.21, p<0.09), o alguno de sus dominios (impacto,
actividades o síntomas).109 Sin embargo, en los pacientes con BQ sí que

IV. Discusión Tesis Doctoral
164
hay correlación entre el SNOT-20, el SGRQ y el SF-36, asociándose la
intensidad de los síntomas nasales con el empeoramiento de la calidad de
vida tanto en el SNOT-20 y el SGRQ como en el SF-36. Los pacientes con
RSC con PN presentaron una mayor pérdida de olfato que los pacientes con
RSC sin PN, pero sin provocar un empeoramiento de la calidad de vida de
los pacientes (SNOT-20, SGRQ, y SF-36).
7º) Diferenciación entre RSC con y sin pólipos
A menudo la poliposis nasal (RSC con pólipos) y la RSC sin pólipos
se integran en una sola enfermedad. El documento EP3OS habla de la
poliposis nasal como un subgrupo de pacientes dentro de la familia de la
RSC.111 Actualmente no está claro si la poliposis nasal refleja un estadio
más avanzado de una RSC o si, por lo contrario, estamos hablando de
patologías diferentes.308 A pesar que los síntomas de ambas supuestas
patologías se superponen, la PN provoca una mayor pérdida de olfato
mientras que en la RSC suele predominar la rinorrea posterior.
Posiblemente el síntoma que realmente nos ayudaría más en la
diferenciación de ambas patologías sería la pérdida del olfato.
Nuestros resultados son totalmente compatibles con estos hallazgos
previos. Existen diferencias en la puntuación total de síntomas, la
obstrucción nasal y sobretodo en la intensidad de la pérdida del olfato entre
los pacientes con RSC con o sin pólipos nasales.
En la TC nasosinusal, Deal and Kountakis,309 utilizando la escala de
Lund&Mackay, observaron que los pacientes con PN presentaban una
mayor ocupación de los senos paranasales, siendo nuestros resultados
compatibles con estos hallazgos. Además, la ocupación sinusal en la TC en
los pacientes con PN fué más elevada que en los pacientes con RSC sin
pólipos, así como en la puntuación del complejo ostiomeatal, etmoides
posterior, esfenoides y frontal. Todo ello nos confirma una afectación

Tesis Doctoral IV. Discusión
165
mucho más extensa de la TC nasosinusal en los pacientes con RSC y
pólipos nasales que en aquellos sin pólipos nasales.


V. INVESTIGACIÓN FUTURA


Tesis Doctoral V. Investigación Futura
169
INVESTIGACIÓN FUTURA 1. Investigar el papel del tratamiento de la rinosinusitis crónica con o sin
pólipos, tanto médico como quirúrgico, en la función pulmonar,
necesidades de tratamiento y evolución de los pacientes con
bronquiectasias.
2. Investigar el olfato en los pacientes con bronquiectasias mediante
olfatometría subjetiva (BAST-24).
3. Investigar si la colonización bacteriana y fúngica de la mucosa
nasosinusal y de la mucosa bronquial se parecen o difieren.
4. Estudiar si la inflamación subyacente, tanto celularidad como
marcadores inflamatorios, de la patología nasosinusal y pulmonar es
parecida o diferente.

VI. CONCLUSIONES
Tesis Doctoral VI. Conclusiones
173
CONCLUSIONES
Estudio 1. Prevalencia de rinosinusitis crónica con / sin pólipos nasales
en bronquiectasias.
1. Tres de cada cuatro pacientes (77%) afectados de bronquiectasias reunen
criterios para rinosinusitis crónica, mientras que uno de cada cuatro (25%)
tienen además pólipos nasales.
2. Los síntomas nasales predominantes en los pacientes con bronquiectasias
son la rinorrea antero-posterior y la obstrucción nasal.
3. En los pacientes con rinosinusitis crónica con pólipos, el tamaño de los
mismos en de leve a moderado. Además la pérdida de olfato fué uno de los
síntomas más frecuentes en dichos pacientes.
4. La tomografia computerizada nasosinusal de los pacientes con
rinosinusitis crónica presenta una ocupación predominantemente de los
senos maxilares, etmoidales y complejo ostiomeatal.
5. Existe una mayor afectación de la rinomanometría entre los pacientes
con y sin rinosinusitis crónica, y una mayor afectación en la rinometría
acústica entre los pacientes con rinosinusitis crónica con y sin pólipos
nasales.
6. El óxido nítrico nasal esta disminuido en los pacientes con rinosinusitis
crónica con pólipos nasales. Se observó una correlación inversa entre la

VI. Conclusiones Tesis Doctoral
174
puntuación radiológica por tomografía del complejo ostiomeal y el óxido
nítrico nasal. El óxido nítrico exhalado esta más elevado en los pacientes
con RSC con pólipos sin lograr significancia estadística.
7. En los pacientes afectos de bronquiectasias, la proteina C reactiva está
más elevada en aquellos que tienen rinosinusitis crónica.
8. Los pacientes con rinosinusitis crónica presentan una mayor extensión de
las bronquiectasias.
9. La prevalencia de patología nasosinusal es similar entre los pacientes
con bronquiectasias tanto de origen postinfeccioso como idiopático.
10. Estos resultados apoyan el concepto de “una única vía aérea” y sugiere
que en las llamadas bronquiectasias post-infecciosas podría existir algún
proceso todavía desconocido que afecta a toda la vía aérea.
Estudio 2. Calidad de vida.
1. En comparación con la población general española, los pacientes afectos
de bronquiectasias presentaron peor puntuación en todos los dominios del
SF-36.
2. Los hombres afectos de bronquiectasias presentaron mejor calidad de
vida que las mujeres.

Tesis Doctoral VI. Conclusiones
175
3. En el sexo masculino, los pacientes con bronquiectasias presentaron peor
calidad de vida que los de la población general española en dolor corporal,
salud general y vitalidad. En el sexo femenino, las pacientes con
bronquiectasias presentaron peor calidad de vida que las de la población
general española, además de los dominios anteriores, en función física,
función social y rol emocional.
4. Las bronquiectasias con rinosinusitis crónica producen una importante
impacto en la calidad de vida, sin que exista un impacto adicional en los
pacientes con rinosinusitis crónica y pólipos nasales.
Estudio 3. Calidad de vida.
1. Los pacientes con bronquiectasias y rinosinusitis crónica tienen una peor
calidad de vida que los pacientes con bronquiectasias sin rinosinusitis
crónica.
2. En los pacientes con bronquiectasias y rinosinusitis crónica, la presencia
de pólipos nasales no empeora la calidad de vida en comparación a los
pacientes sin pólipos.
3. En términos de calidad de vida, existe una correlación clara entre la vía
aérea superior (SNOT-20), la via aérea inferior (SGRQ) y la salud en
general (SF-36).
4. La rinosinusitis crónica evaluada tanto mediante cuestionarios
específicos como genéricos tiene un considerable impacto sobre la calidad
de vida de los pacientes con bronquiectasias.

VI. Conclusiones Tesis Doctoral
176
CONCLUSIONES FINALES
1. Se confirma que el concepto de “una única vía aérea” va más allá del
ámbito del asma y las enfermedades pulmonares obstructivas crónicas.
2. La alta prevalencia de patología nasosinusal en los pacientes con
bronquiectasias nos hace concluir que estos pacientes deberían ser siempre
evaluados a fin de descartar una rinosinusitis crónica con o sin pólipos. A
su vez los pacientes con rinosinusitis crónica con o sin pólipos, además de
rinitis alérgica y no alérgica deberían ser estudiados para enfermedades de
la vía aérea inferior como el asma y el EPOC, pero incluyendo también
ahora bronquiectasias.
3. Estos estudios sugieren que la rinosinusitis crónica con o sin pólipos
tienen una considerable repercusión en la calidad de vida de los pacientes
con bronquiectasias.
4. En un futuro se requerirán más estudios para el mejor entendimiento de
la asociación de la via aérea inferior y superior en los pacientes con
bronquiectasias tanto en epidemiología, fisiopatología, diagnóstico,
tratamiento y seguimiento.

VII. BIBLIOGRAFÍA


Tesis Doctoral VII. Bibliografía
179
1. VII. Bibliografía
2. Simons FE. Allergic rhinobronchitis: the asthma-allergic rhinitis link. J Allergy
Clin Immunol 1999;104:534-40.
3. Bachert C, Vignola AM, Gevaert P, Leynaert B, Van Cauwenberge P, Bousquet
J. Allergic rhinitis, rhinosinusitis, and asthma: one airway disease. Immunol
Allergy Clin Am 2004;24:19-43.
4.Bousquet J, Van Cauwenberge P, Khaltaev N; Aria Workshop Group; World Health
Organization. Allergic rhinitis and its impact on asthma. J Allergy Clin
Immunol 2001;108: 147-334.
5.Vignola A, Bousquet J. Rhinitis and asthma: a continuum of disease? Clin Exp
Allergy2001;31:674-7.
6.Haave E, Hyland ME, Skumlien S. The relation between measures of health status
and quality of life in COPD. Chron Respir Dis 2006;3:195-9.
7.Nouraei SA, Elisay AR, Dimarco A, Abdi R, Majidi H, Madani SA, Andrews PJ.
Variations in paranasal sinus anatomy: implications for the pathophysiology of
chronic rhinosinusitis and safety of endoscopic sinus surgery. J Otolaryngol
Head Neck Surg 2009;38:32-7.
8.Proctor DF. The upper airways. Nasal physiologyc and defense of the lungs. Am Rev
Respir Dis 1977;115:97-119.
9. Elad D, Wolf M, Keck T. Air-conditioning in the human nasal cavity. Respir
Physiol Neurobiol 2008;163:121-7.
10. Frank H. Netter, M. D. Atlas de Anatomía Humana. Barcelona: Masson, 1996.
Rouvière, H. y Delmas, A. Anatomía Humana. Barcelona: Masson, 9ª ed., 1996.
Warwick, Williams. Gray: Anatomía. Madrid: Editorial Harcourt, 36ª ed., 1995.
11. Boyden EA. Developmental anomalies of the lungs. Am J Surg 1955;89:79-89.
12. West JB. Distribution of blood and gas in lungs. Phys Med Biol 1966;11:357-
70.
13. Mason RJ, Broaddus VC, Murray JF, Nadel JA. Murray and Nadel's Textbook
of Respiratory Medicine. 4th ed. Philadelphia, Pa: Saunders; 2005.
14. Martínez-Antón A, Debolós C, Garrido M, Roca-Ferrer J, Barranco C, Alobid I,
Xaubet A, Picado C, Mullol J. Mucin genes have different expression patterns

VII. Bibliografía Tesis Doctoral
180
in healthy and diseased upper airway mucosa. Clin Exp Allergy 2006;36:448-
57.
15. Rouadi P, Baroody FM, Abbott D, Naureckas E, Solway J, Naclerio RM. A
technique to measure the ability of the human nose to warm and humidify air. J
Appl Physiol 1999;87:400-6.
16. Doty RL. The olfactory system and its disorders. Semin Neurol 2009 ;29:74-81.
17. Gaga M, Vignola AM, Chanez P. Upper and lower airways: similarities and
differences. En: The Nose and Lung diseases. Wallaërt B, Chanez P, Godard P,
eds. Eur Respir Mon 2001;6:10-15.
18. Tos M, Mogensen C. Mucus production in chronic maxillary sinusitis. A
quantitative histopathological study. Acta Otolaryngol 1984;97:151-9.
19. Roche WR, Beasley R, Williams JH, Holgate ST. Subepithelial fibrosis in the
bronchi of asthmatics. Lancet 1989 11;1:520-4.
20. Crepea SB, Harman A, Amenta PS. The basement membrana pathology. Lab
Invest 1983;48:656-77.
21. Bousquet J, Jacot W, Vignola AM, Bachert C, Van Cauwenberge P. Allergic
rhinitis: a disease remodeling the upper airways? J Allergy Clin Immunol
2004;113:43-9
22. Rutland, J; Griffin, WM y Cole, PJ. Human ciliary beat frequency in epithelium
from intrathoracic and extrathoracic airways. Am Rev Respir Dis
1982;125:100-5.
23. Leynaert B, Neukirch F, Demoly P, Bousquet J. Epidemiologic evidence for
asthma and rhinitis comorbidity. J Allergy Clin Immunol 2000;106:201-5.
24. Settipane GA, Chafee FH. Nasal polyps in asthma and rhinitis. A review of
6,037 patients. J Allergy Clin Immunol 1977;59:17-21.
25. Corren J, Adinoff A, Irvin C, Changes in bronquial responsiveness following
nasal provocacation con allergen. J Allergy Clin Immunol 1992; 89: 611-618.
26. Schumacher M, Cota K, Taussig L. Pulmonary response to nasal-challenge
testing of atopic subjects with stable asthma. J Allergy Clin Immunol 1986; 78:
30-35.
27. Littell N, Carlisle C, Millman R, Braman S. Changes in airway resistance
following nasal provocation. Am Rev Respir Dis 1990; 141: 580-583.
28. Prieto L, Uixera S, Gutiérrez V, Bruno L. Modifications of airway
responsiveness to adenosine 5'-monophosphate and exhaled nitric oxide
Tesis Doctoral VII. Bibliografía
181
concentrations after the pollen season in subjects with pollen-induced rhinitis.
Chest 2002;122:940-7.
29. Braunstahl GJ, KleinJan A, Overbeek SE, , Prins JB, Hoogsteden HC, Fokkens
WJ. Segmental bronchial provocation induces nasal inflammation in allergic
rhinitis patients. Am J Respir Crit Care Med 2000;161:2051-7.
30. Braunstahl GJ, Overbeek SE, Fokkens WJ, KleinJan A, McEuen AR, Walls AF,
Hoogsteden HC, Prins JB. Segmental bronchoprovocation in allergic rhinitis
affects mast cell and basophil numbers in nasal and bronchial mucosa. Am
Respir Crit Care Med 2001;164:858-65.
31. Togias A. Rhinitis and asthma: Evidence for respiratory system integration. J
Allergy Clin Immunol 2003;111:1171-83.
32. Bousquet J, Vignola A, Leynaert B, Demoly P. Links between rhinitis and
asthma. Allergy 2003;58:733– 41.
33. Chanez P, Vignola AM, Vic P, Guddo F, Bonsignore G, Godard P, et al.
Comparison between nasal and bronchial inflammation in asthmatic and control
subjects. Am J Respir Crit Care Med 1999;159:588–95.
34. Gaga M, Lambrou P, Papageorgiou N, Koulouris N, Kosmas E, Fragakis S, et
al. Eosinophils are a feature of upper and lower airway pathology in non-atopic
asthma, irrespective of the presence of rhinitis. Clin Exp Allergy 2000;30:663-9.
35. Watelet JB, Van Zele T, Gjomarkaj M, Canonica GW, Dahlen SE, Fokkens W,
Lund VJ, Scadding GK, Mullol J, Papadopoulos N, Bonini S, Kowalski ML,
Van Cauwenberge P, Bousquet J; GA(2)LEN Workpackage Members 2.7.
Tissue remodelling in upper airways: where is the link with lower airway
remodelling?. Allergy 2006;61:1249-58.
36. Togias A. Systemic immunologic and inflammatory aspects of allergic rhinitis.
J Allergy Clin Immunol 2000;106:S247-250.
37. McCusker C, Chicoine M, Hamid D, Mazer B. Site-specific sensitization in a
murine model of allergic rhinitis: role of the upper airway in lower airway
disease. J Allergy Clin Immunol 2002;110:891-8.
38. Braunstahl GJ, Overbeek SE, KleinJan A, Prins JB, Hoogsteden HC, Fokkens
WJ. Nasal allergen provocation induces adhesion molecule expression and
tissue eosinophilia in upper and lower airways. J Allergy Clin Immunol
2001;107:469-76.

VII. Bibliografía Tesis Doctoral
182
39. Beeh KM, Beier J, Kornmann O, Meier C, Taeumer T, Buhl R. A single nasal
allergen challenge increases induced sputum inflammatory markers in non-
asthmatic with seasonal allergic rhinitis: correlation with plasma interleukin-5.
Clin Exp Allergy 2003;33:475-82.
40. Chakir J, Laviolette M, Turcotte H, Boutet M, Boulet LP. Cytokine expression
in the lower airways of nonasthmatics subjects with allergic rhinitis: Influence
of natural allergen exposure. J Allergy Clin Immunol 2000;106:904-10.
41. Boulay ME, Boulet LP. Influence of natural exposure to pollen and domestic
animals on airway responsiveness and inflammation in sensitized non-
asthmatics subjects. Int Arch Allergy Immunol 2002;128:336-43.
42. Braunstahl GJ, Fokkens WJ, Overbeek SE, KleinJan A, Hoogsteden HC, Prins
JB. Mucosal and systemic inflammatory changes in allergic rhinitis and asthma:
A comparison between upper and lower airways. Clin Exp Allergy
2003;33:579-87.
43. Boulay ME, Boulet LP. Lower airway inflammatory responses to repeated very
low dose allergen challenge in allergic rhinitis and asthma. Clin Exp Allergy
2002;32:1441-47.
44. Mc Fadden Jr ER.: Exercise-induced airway narrowing. En: Adkinson NF,
Yunginger JW, Busse WW, Bochner BS, Holgate ST, Simons FE. Middleton`s
Allergy Principles and Practice. Mosby Inc. 2003:1323-32.
45. Richardson HB, Slebohm PM. Nasal airway response to exercise. J Allergy
1968;41:269-284.
46. Syabbalo NC, Bundgaard A, Widdicombe JG. Effect of exercise on nasal
airflow resistance in healthy subjects and in patients with asthma and rhinitis.
Bull Eur Physiopathol Respir 1985;21:507-513.
47. Olson LG, Strohl KP. The response of the nasal airway to exercise. Am Rev
Respir Dis 1987;135:356-359.
48. Serra-Batlles J, Montserrat JM, Mullol J, Ballester E, Xaubet A, Picado C.
Response of the nose to exercise in healthy subjects and in patients with rhinitis
and asthma. Thorax 1994; 49:128-32.
49. Jang YJ, Lee JH, Jang JY. Acoustic rhinometric evaluation of the nasal response
to exercise in patients with nasal septal deviation. Clin Otolaryngol
2000;25:423-427.
Tesis Doctoral VII. Bibliografía
183
50. Strohl KP, Arnold JL, Decker MJ, Hooekje PL, Doershuk CF, Stern RC. The
nasal response to exercise in patients with cistic fibrosis.Rhinology
1992;30:241-248.
51. Strohl KP, Decker MJ, Olson LG, Flak TA, Hoekje PL. The nasal response to
exercise and exercise induced bronchoconstriction in normal and asthmatic
subjects. Thorax 1988;43:890-5.
52. Bardin P, VanHeerden B, Joubert J. Absence of pulmonary aspiration of sinus
contents in patients with asthma and sinusitis. J Allergy Clin Immunol
1990;86:82-8.
53. Csoma Z, Kharitonov S, Balint B, Bush A, Wilson N, Barnes P. Increased
leukotrienes in exhaled breath condensate in childhood asthma. Am J Respir
Crit Care Med 2002;166:1345-9.
54. Togias A, Bieneman A, Bloom D, Schleimer R, Lezzoni D, Harris A, et al.
Changes in blood leucocyte cytokine expression following repeated nasal
allergen provocation: evidence for systemic manifestations [abstract]. J Allergy
Clin Immunol 2002;109:S262.
55. Magnusson J, Ping Lin X, Dahlman-Höglund A, Hanson LA, Telemo E,
Magnusson O, et al. Seasonal intestinal inflammation in patients with birch
pollen allergy. J Allergy Clin Immunol 2003;112:45-51.
56. Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, Togias A,
Zuberbier T, Baena-Cagnani CE, Canonica GW, van Weel C, Agache I, Aït-
Khaled N, Bachert C, Blaiss MS, Bonini S, Boulet LP, Bousquet PJ, Camargos
P, Carlsen KH, Chen Y, Custovic A, Dahl R, Demoly P, Douagui H, Durham
SR, van Wijk RG, Kalayci O, Kaliner MA, Kim YY, Kowalski ML, Kuna P, Le
LT, Lemiere C, Li J, Lockey RF, Mavale-Manuel S, Meltzer EO, Mohammad
Y, Mullol J, Naclerio R, O'Hehir RE, Ohta K, Ouedraogo S, Palkonen S,
Papadopoulos N, Passalacqua G, Pawankar R, Popov TA, Rabe KF, Rosado-
Pinto J, Scadding GK, Simons FE, Toskala E, Valovirta E, van Cauwenberge P,
Wang DY, Wickman M, Yawn BP, Yorgancioglu A, Yusuf OM, Zar H,
Annesi-Maesano I, Bateman ED, Ben Kheder A, Boakye DA, Bouchard J,
Burney P, Busse WW, Chan-Yeung M, Chavannes NH, Chuchalin A, Dolen
WK, Emuzyte R, Grouse L, Humbert M, Jackson C, Johnston SL, Keith PK,
Kemp JP, Klossek JM, Larenas-Linnemann D, Lipworth B, Malo JL, Marshall
GD, Naspitz C, Nekam K, Niggemann B, Nizankowska-Mogilnicka E,

VII. Bibliografía Tesis Doctoral
184
Okamoto Y, Orru MP, Potter P, Price D, Stoloff SW, Vandenplas O, Viegi G,
Williams D; World Health Organization; GA(2)LEN; AllerGen. Allergic
Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with
the World Health Organization, GA(2)LEN and AllerGen). Allergy 2008;63:8-
160.
57. Beasley R, Keil U, von Mutius E, Pearce N. World wide variation in prevalence
of symptoms of asthma, allergic rhinoconjunctivitis and atopic eczema: ISAAC.
Lancet 1998;351:1225-32.
58. Van Cauwenberge P, Watelet JB, Van Zele T, Wang DY, Toskala E, Durham S,
Fokkens W, Lau S, Leynaert B, Wickman M, Salapatas M, Burney P, Mullol J;
GA2LEN workpackages 3.2 and 3.3. Does rhinitis lead to asthma? Rhinology.
2007;45:112-21.
59. Navarro A, Valero A, Juliá B, Quirce S. Coexistence of asthma and allergic
rhinitis in adult patients attending allergy clinics: ONEAIR study. J Investig
Allergol Clin Immunol 2008;18:233-8.
60. Mullol J, Valero A, Alobid I, Bartra J, Navarro AM, Chivato T, Khaltaev N,
Bousquet J. Allergic Rhinitis and its Impact on Asthma update (ARIA 2008).
The perspective from Spain. J Investig Allergol Clin Immunol 2008;18:327-34.
61. Wright AL, Holberg CJ, Martinez FD, Halonen M, Morgan W, Taussig LM.
Epidemiology of physician-diagnosed allergic rhinitis in childhood. Pediatrics
1994;94:895–901.
62. Settipane RJ, Hagy GW, Settipane GA. Long-term risk factors for developing
asthma and allergic rhinitis: a 23-year follow-up study of college students.
Allergy Proc 1994;15:21–5.
63. Guerra S, Sherrill DL, Martinez FD, Barbee RA. Rhinitis as an independent risk
factor for adult-onset asthma. J Allergy Clin Immunol 2002;109:419–25.
64. Peat JK, Salome CM, Woolcock AJ. Longitudinal changes in atopy during a 4-
year period: relation to bronchial hyperresponsiveness and respiratory
symptoms in a population sample of Australian schoolchildren. J Allergy Clin
Immunol 1990; 85: 65–74.
65. Sandrini A, Ferreira IM, Jardim JR, Zamel N, Chapman KR. Effect of nasal
triamcinolone acetonide on lower airway inflammatory markers in patients with
allergic rhinitis. J Allergy Clin Immunol 2003;111:313-20.

Tesis Doctoral VII. Bibliografía
185
66. Pedersen B, Dahl R, Lindqvist N, Mygind N. Nasal inhalation of the
glucocorticoid budesonide from a spacer for the treatment of patients with
pollen rhinitis and asthma. Allergy 1990; 45: 451–6.
67. Watson WT, Becker AB, Simons FE. Treatment of allergic rhinitis with
intranasal corticosteroids in patients with mild asthma: effect on lower airway
responsiveness. J Allergy Clin Immunol 1993; 91: 97–101.
68. Adams RJ, Fuhlbrigge AL, Finkelstein JA, Weiss ST. Intranasal steroids and the
risk of emergency department visits for asthma. J Allergy Clin Immunol 2002;
109: 636-42.
69. Crystal-Peters J, Neslusan C, Crown WH, Torres A. Treating allergic rhinitis in
patients with comorbid asthma: the risk of asthma related hospitalizations and
emergency department visits. J Allergy Clin Immunol 2002; 109: 57-62.
70. Taramarcaz P, Gibson PG. Intranasal corticosteroids for asthma control in
people with coexisting asthma and rhinitis. Cochrane Database Syst Rev.
2003;(4):CD003570.
71. Grant JA, Nicodemus CF, Findlay SR, Glovsky MM, Grossman J, Kaiser h, et
al. Cetirizine in patients with seasonal rhinitis and concomitant asthma:
prospective, randomized controlled trial. J Allergy Clin Immunol 1995;95:923-
32.
72. Ciprandi G, Tosca MA, Passalacqua G, Canonica GW. Long-term cetirizine
treatment reduces allergic symptoms and drug prescriptions in children with
mite allergy. Ann Allergy Asthma Immunol 2001; 87: 222-6.
73. Baena-Cagnani CE, Berger WE, DuBuske LM, Gume SE, Stryszak P, Lorber R,
et al. Comparative effects of desloratadine versus montelukast on asthma
symptoms and use of beta 2-agonists in patients with seasonal allergic rhinitis
and asthma. Int Arch Allergy Immunol 2003; 130: 307-13.
74. Davis BE, Todd DC, Cockcroft DW. Effect of combined montelukast and
desloratadine on the early asthmatic response to inhaled allergen. J Allergy Clin
Immunol 2005 ;116:768-72.
75. Moller C, Dreborg S, Ferdousi HA, Halken S, Host A, Jacobsen L, et al. Pollen
immunotherapy reduces the development of asthma in children with seasonal
rhinoconjunctivitis (the PAT-study). J Allergy Clin Immunol 2002;109:251-6.
76. Passalacqua G, Canonica GW. Treating the allergic patient: think globally, treat
globally. Allergy 2002;57:876-83.

VII. Bibliografía Tesis Doctoral
186
77. Philip G, Nayak AS, Berger WE, Leynadier F, Vrijens F, Dass SB, Reiss TF.
The effect of montelukast on rhinitis symptoms in patients with asthma and
seasonal allergic rhinitis. Curr Med Res Opin 2004;20:1549-58.
78. Perry TT, Corren J, Philip G, Kim EH, Conover-Walker MK, Malice MP,
Massaad R, Dass SB, Reiss TF, Wood RA. Protective effect of montelukast on
lower and upper respiratory tract responses to short-term cat allergen exposure.
Ann Allergy Asthma Immunol 2004;93:431-8.
79. Dixon AE, Kaminsky DA, Holbrook JT, Wise RA, Shade DM, Irvin CG.
Allergic rhinitis and sinusitis in asthma: differential effects on symptoms and
pulmonary function. Chest. 2006;130:429-35.
80. Bresciani M, Paradis L, Des Roches A, Vernhet H, Vachier I, Godard P,
Bousquet J, Chanez P. Rhinosinusitis in severe asthma. J Allergy Clin Immunol
2001;107:73-80.
81. Kowalski ML. Aspirin-sensitive rhinosinusitis and asthma. Clin Allergy
Immunol. 2007;19:147-75.
82. Rachelefsky GS, Goldberg M, Katz RM. Sinus disease in children with
respiratory allergy. Allergy Clin Immunol 1978;61:310-14.
83. Businco L, Fiore L, Frediani T, Artuso A, Difazio a, Bellioni P. Clinical and
therapeutic aspects of sinusitis in children with bronchial asthma. Int J Pediatr
Otorhinolaryngol 1981;3:277-284.
84. Rachelefsky GS, Katz RM, Siegel SC. Chronic sinus disease with associated
reactive airway disease in children. Pediatrics 1984;73:526-9.
85. Richards W, Roth RM, Church JA. Underdiagnosis and undertreatment of
chronic sinusitis in children. Clin Ped 1991;30:88-92.
86. Freedman R, Ackerman M, Wald E, y col. Asthma and bacterial sinusitis in
children. J Allergy Clin Immunol 1984;74:185-9.
87. Oliveira CA, Solé D, Naspitz CK, Rachelefsky GS. Improvement of bronchial
hyperresponsiveness in asthmatic children treated for concomitant sinusitis. Ann
Allergy Asthma Immunol 1997;79:70-4.
88. Benítez P, Alobid I, de Haro J, Berenguer J, Bernal-Sprekelsen M, Pujols L et
al. A short course of oral prednisone followed by intranasal budesonide is an
effective treatment of severe nasal polyps. Laryngoscope 2006;116:770-5.
89. English G. Nasal polypectomy and sinus surgery in patients with asthma and
aspirin idiosyncrasy. Laryngoscope 1986;96:374-80.

Tesis Doctoral VII. Bibliografía
187
90. Francis C. Prognosis of operations for removal of nasal polyps in asthma.
Practitioner. 1929;123:272-8.
91. Samter M, Lederer FL. Nasal polyps: their relationship to allergy, particulary
bronchial asthma. Med Clin N Am. 1958;42:175-9.
92. Nishioka GJ, Cook PR, Davis WE, McKinsey JP. Functional endoscopic sinus
surgery in patients with chronic sinusitis and asthma. Otolaryngol Head Neck
Surg 1994;110:494–500.
93. Manning SC, Wasserman RL, Silver R, Phillips DL. Results of endoscopic
sinus surgery in paediatric patients with chronic sinusitis and asthma. Arch
Otolaryngol Head Neck Surg.1994;120:1142-5.
94. Dinis PB, and Gomez A. Sinusitis and Asthma. How do they interrelate in sinus
surgery? Am J Rhinol. 1997;11:421-8.
95. Goldstein MF, Grundfast SK, Dunsky EH, Dvorin DJ, Lesser R. Effect of
functional endoscopic sinus surgery on bronchial asthma outcomes. Arch
Otolaryngol Head Neck Surg. 1999;125:314-9.
96. McFadden EA, Woodson BT, Fink JN, Toohill JT. Surgical treatment of aspirin
triad patients. Am J Rhinol. 1997;11:263–270.
97. Park AH;Lau J; Stankiewicz J; Chow J. The role of functional endoscopic sinus
surgery in asthmatic patients. The Journal of Otolaryngology. 1998;27:275-
280.
98. Ikeda K, Tanno N, Tamura G, y col. Endoscopic sinus surgery improves
pulmonary function in patients with asthma associated with chronic sinusitis.
Ann Otol Rhinol Laryngol. 1999;108:355-359.
99. Dunlop G, Scadding GK, Lund VJ. The effect of endoscopic sinus surgery on
asthma: management of patients with chronic rhinosinusitis, nasal polyposis and
asthma. Am J Rhinol 1999;13:261–5.
100. Senior Ba, Kennedy Dw, Tanabodee J, Kroger H, Hassab M, Lanza Dc. Long-
term impact of functional endoscopic sinus surgery on asthma. Otolaryngol
Head Neck Surg 1999; 121:66-8.
101. Palmer JN, Conley DB, Dong RG, et al. Efficacy of endoscopic sinus surgery in
the management of patients with asthma and chronic sinusitis. Am J Rhinol
2001;15:49-53.
VII. Bibliografía Tesis Doctoral
188
102. Uri N, Cohen-Kerem R, Barzilai G, et al. Functional endoscopic sinus surgery
in the treatment of massive polyposis in asthmatic patients. J Laryngol Otol
2002;116:185–9
103. Dejima K, Hama T, Miyazaki M, Yasuda S, Fukushima K, Oshima A et al. A
Clinical Study of Endoscopic Sinus Surgery for Sinusitis in Patients with
Bronchial Asthma. Int Arch Allergy Immunol 2005;138:97-104.
104. Nakamura H, Kawasaki M, Higuuchi Y, Takahashi S. Effects of sinus surgery
on asthma in aspirin triad patients. Acta otolaryngol 1999;119:592-8.
105. Batra PS, Kern RC, Tripathi A, Conley DB, Ditto AM, Haines GK, Yarnold PR,
Grammar L. Outcome Analysis of Endoscopic Sinus Surgery in Patients with
Nasal Polyps and Asthma. Laryngoscope 2003;113:1703-6.
106. Loehrl TA, Toohill RJ, Ferre R, Smith TL. Long-term Asthma Outcomes After
Endoscopic Sinus Surgery in Patients with Aspirin Triad Disease. American
Journal of Otolaryngology 2006;27:154-60.
107. Awad OG, Lee JH, Fasano MB, Graham SM. Sinonasal outcomes after
endoscopic sinus surgery in asthmatic patients with nasal polyps: a difference
between aspirin-tolerant and aspirin-induced asthma? Laryngoscope
2008;118:1282-6.
108. Lamblin C, Brichet A, Perez T, Darras J, Tonnel Ab, Wallaert B. Long-term
Follow-up of Pulmonary Function in Patients with Nasal Polyposis. Am J
Respir Crit. Care Med 2000;161: 406-13.
109. Ragab S, Scadding GK, Lund V J Saleh H. Treatment of chronic rhinosinusitis
and its effects on asthma. Eur Respir J 2006;28:68-74.
110. Hurst JR, Wilkinson TM, Donaldson GC, Wedzicha JA. Upper airway
symptoms and quality of life in chronic obstructive pulmonary disease (COPD).
Respir Med 2004 ;98:767-70.
111. Hens G, Vanaudenaerde BM, Bullens DM, Piessens M, Decramer M, Dupont
LJ, Ceuppens JL, Hellings PW. Sinonasal pathology in nonallergic asthma and
COPD: 'united airway disease' beyond the scope of allergy. Allergy
2008;63:261-7.
112. Fokkens W, Lund V, Mullol J. On behalf of the European position paper on
rhinosinusitis and nasal polyps group. EP3OS 2007: European position paper on
rhinosinusitis and nasal polyps 2007. A summary for otorhinolaryngologists.
Rhinology. 2007;45:97-101.
Tesis Doctoral VII. Bibliografía
189
113. Alobid I, Benítez P, Bernal-Sprekelsen M, Roca J, Alonso J, Picado C, Mullol J.
Nasal polyposis and its impact on quality of life: comparison between the
effects of medical and surgical treatments. Allergy 2005;60:452-8.
114. Collins JG. Prevalence of selected chronic conditions: United States, 1990-
1992. Vital Health Stat 10. 1997;194:1-89.
115. Coren ME, Meeks M, Morrison I, Buchdahl RM, Bush A. Primary ciliary
dyskinesia: age at diagnosis and symptom history. Acta Paediatr 2002;91:667-9.
116. Hadfield PJ, Rowe-Jones JM, Mackay IS. The prevalence of nasal polyps in
adults with cystic fibrosis. Clin Otolaryngol Allied Sci 2000;25:19-22.
117. Kaliner M. Treatment of sinusitis in the next millennium. Allergy Asthma Proc.
1998;19:181-4.
118. Beninger M. Rhinitis, sinusitis and their relationship to allergies. Am J Rhinol
1992;6:37-43.
119. Salvin RG, Cannon RE, Friedman WH, Palitang E, Sundaram M. Sinusitis and
bronchial asthma. J Allergy Clin Immunol 1980;66:250-7.
120. Schwartz HJ, Thompson JS, Sher TH, Ross RJ. Occult sinus abnormalities in
the asthmatic patient. Arch Intern Med 1987;147:2194-6.
121. Chee L, Graham SM, Carothers DG, Ballas ZK. Immune dysfunction in
refractory sinusitis in a tertiary care setting. Laryngoscope. 2001;111:233-5.
122. Porter JP, Patel AA, Dewey CM, Stewart MG. Prevalence of sinonasal
symptoms in patients with HIV infection. Am J Rhinol 1999;13:203-8.
123. Sabini P, Josephson GD, Reisacher WR, Pincus R. The role of endoscopic sinus
surgery in patients with acquired immune deficiency syndrome. Am J
Otolaryngol 1998;19:351-6.
124. Cuppens H, Marynen P, De Boeck C, Cassiman JJ. Detection of 98.5% of the
mutations in 200 Belgian cystic fibrosis alleles by reverse dot-blot and
sequencing of the complete coding region and exon/intron junctions of the
CFTR gene. Genomics. 1993;18:693-7.
125. Ellegard EK. Pregnancy rhinitis. Immunol Allergy Clin North Am 2006;26:119-
35.
126. Sobol SE, Frenkiel S, Nachtigal D, Wiener D, Teblum C. Clinical
manifestations of sinonasal pathology during pregnancy. J Otolaryngol
2001;30:24-8.

VII. Bibliografía Tesis Doctoral
190
127. Jeevanan J, Gendeh BS, Satpal S. Hashimoto's thyroiditis: a rare cause for
rhinosinusitis. Med J Malaysia 2004;59:428-30.
128. Zinreich SJ, Mattox DE, Kennedy DW, Chisholm HL, Diffley DM, Rosenbaum
AE. Concha bullosa: CT evaluation. J Comput Assist Tomogr 1988;12:778-84.
129. Bolger WE, Butzin CA, Parsons DS. Paranasal sinus bony anatomic variations
and mucosal abnormalities: CT analysis for endoscopic sinus surgery.
Laryngoscope 1991;101:56-64.
130. Araujo E, Palombini BC, Cantarelli V, Pereira A, Mariante A. Microbiology of
middle meatus in chronic rhinosinusitis. Am J Rhinol 2003;17:9-15.
131. Brook I. Microbiology and management of sinusitis. J Otolaryngol
1996;25:249-56.
132. Schubert MS. Fungal rhinosinusitis: diagnosis and therapy. Curr Allergy
Asthma Rep 2001 ;1:268-76.
133. Schubert MS. Allergic fungal sinusitis. Otolaryngol Clin North Am
2004;37:301-26.
134. Ebbens FA, Georgalas C, Luiten S, van Drunen CM, Badia L, Scadding GK,
Hellings PW, Jorissen M, Mullol J, Cardesin A, Bachert C, van Zele TP, Lund
VJ, Fokkens WJ. The effect of topical amphotericin B on inflammatory markers
in patients with chronic rhinosinusitis: a multicenter randomized controlled
study. Laryngoscope 2009;119:401-8.
135. Chen Y, Dales R, Lin M. The epidemiology of chronic rhinosinusitis in
Canadians. Laryngoscope 2003;113:1199-205.
136. Greisner WA 3rd, Settipane GA. Hereditary factor for nasal polyps. Allergy
Asthma Proc 1996;17:283-6.
137. Ozdek A, Cirak MY, Samim E, Bayiz U, Safak MA, Turet S. A possible role of
Helicobacter pylori in chronic rhinosinusitis: a preliminary report.
Laryngoscope 2003 ;113:679-82.
138. Muluk NB, Koç C, Atasoy P. Localization of T cells and subtypes in the
paranasal sinus and turbinate mucosa in patients with chronic sinusitis. J
Otolaryngol 2004;33:235-42.
139. Bhattacharyya N, Vyas DK, Fechner FP, Gliklich RE, Metson R. Tissue
eosinophilia in chronic sinusitis: quantification techniques. Arch Otolaryngol
Head Neck Surg 2001;127:1102-5.

Tesis Doctoral VII. Bibliografía
191
140. Szucs E, Ravandi S, Goossens A, Beel M, Clement PA. Eosinophilia in the
ethmoid mucosa and its relationship to the severity of inflammation in chronic
rhinosinusitis. Am J Rhinol 2002;16:131-4.
141. Zadeh MH, Banthia V, Anand VK, Huang C. Significance of eosinophilia in
chronic rhinosinusitis. Am J Rhinol 2002;16:313-7.
142. Seiberling KA, Conley DB, Tripathi A, Grammer LC, Shuh L, Haines GK 3rd,
Schleimer R, Kern RC. Superantigens and chronic rhinosinusitis: detection of
staphylococcal exotoxins in nasal polyps. Laryngoscope 2005;115:1580-5.
143. Van Zele T, Claeys S, Gevaert P, Van Maele G, Holtappels G, Van
Cauwenberge P, Bachert C. Differentiation of chronic sinus diseases by
measurement of inflammatory mediators. Allergy 2006;61:1280-9.
144. Claeys S, De Belder T, Holtappels G, Gevaert P, Verhasselt B, Van
Cauwenberge P, Bachert C. Macrophage mannose receptor in chronic sinus
disease. Allergy 2004;59:606-12.
145. Kramer MF, Burow G, Pfrogner E, Rasp G. In vitro diagnosis of chronic nasal
inflammation. Clin Exp Allergy 2004;34:1086-92.
146. Carney AS, Tan LW, Adams D, Varelias A, Ooi EH, Wormald PJ. Th2
immunological inflammation in allergic fungal sinusitis, nonallergic
eosinophilic fungal sinusitis, and chronic rhinosinusitis. Am J Rhinol
2006;20:145-9.
147. Rudack C, Sachse F, Alberty J. Chronic rhinosinusitis-need for further
classification? Inflamm Res 2004;53:111-7.
148. Ragab A, Clement P, Vincken W. Correlation between the cytology of the nasal
middle meatus and BAL in chronic rhinosinusitis. Rhinology 2005;43:11-7.
149. Bachert C, Wagenmann M, Rudack C, Höpken K, Hillebrandt M, Wang D, van
Cauwenberge P. The role of cytokines in infectious sinusitis and nasal
polyposis. Allergy 1998;53:2-13.
150. Rhyoo C, Sanders SP, Leopold DA, Proud D. Sinus mucosal IL-8 gene
expression in chronic rhinosinusitis. J Allergy Clin Immunol 1999;103:395-400.
151. Nonoyama T, Harada T, Shinogi J, Yoshimura E, Sakakura Y.
Immunohistochemical localization of cytokines and cell adhesion molecules in
maxillary sinus mucosa in chronic sinusitis. Auris Nasus Larynx 2000;27:51-8.
VII. Bibliografía Tesis Doctoral
192
152. Demoly P, Crampette L, Mondain M, Enander I, Jones I, Bousquet J.
Myeloperoxidase and interleukin-8 levels in chronic sinusitis. Clin Exp Allergy
1997;27:672-5.
153. Persson CG, Erjefält JS, Andersson M, Erjefält I, Greiff L, Korsgren M, Linden
M, Sundler F, Svensson C. Epithelium, microcirculation, and eosinophils--new
aspects of the allergic airway in vivo. Allergy 1997;52:241-55.
154. Xu R, Xu G, Shi J, Wen W. A correlative study of NF-kappaB activity and
citokines expression in human chronic nasal sinusits. J Laryngol Otol
2006;11:1-6.
155. Rudack C, Sachse F, Alberty J. Primary role of growth-related oncogene-alpha
and granulocyte chemotactic protein-2 as neutrophil chemoattractants in chronic
rhinosinusitis. Clin Exp Allergy 2006;36:748-59
156. Riechelmann H, Deutschle T, Rozsasi A, Keck T, Polzehl D, Bürner H. Nasal
biomarker profiles in acute and chronic rhinosinusitis. Clin Exp Allergy
2005;35:1186-91.
157. Bradley DT, Kountakis SE. Role of interleukins and transforming growth
factor-beta in chronic rhinosinusitis and nasal polyposis. Laryngoscope
2005;115:684-6.
158. Pérez-Novo CA, Watelet JB, Claeys C, Van Cauwenberge P, Bachert C.
Prostaglandin, leukotriene, and lipoxin balance in chronic rhinosinusitis with
and without nasal polyposis. J Allergy Clin Immunol 2005;115:1189-96.
159. Elhini A, Abdelwahab S, Ikeda K. Th1 and Th2 cell population in chronic
ethmoidal rhinosinusitis: a chemokine receptor assay. Laryngoscope
2005;115:1272-7.
160. Toppila-Salmi SK, Myller JP, Torkkeli TV, Muhonen JV, Renkonen JA,
Rautiainen ME, Renkonen RL. Endothelial L-selectin ligands in sinus mucosa
during chronic maxillary rhinosinusitis. Am J Respir Crit Care Med
2005;171:1350-7.
161. Pérez-Novo CA, Claeys C, Van Cauwenberge P, Bachert C. Expression of
eicosanoid receptors subtypes and eosinophilic inflammation: implication on
chronic rhinosinusitis. Respir Res 2006;7:75.
162. Watelet JB, Claeys C, Perez-Novo C, Gevaert P, Van Cauwenberge P, Bachert
C. Transforming growth factor beta1 in nasal remodeling: differences between
chronic rhinosinusitis and nasal polyposis. Am J Rhinol 2004;18:267-72.

Tesis Doctoral VII. Bibliografía
193
163. Lu X, Liu Z, Cui Y. The protein expression difference of transforming growth
factor beta1, matrix metalloproteinases 1,7,9 and tissue inhibitors of matrix
metalloproteinases-1 between chronic rhinosinusitis, nasal polyps and normal
mucosa tissues. Lin Chuang Er Bi Yan Hou Ke Za Zhi 2005;19:633-5.
164. Lal D, Baroody FM, Weitzel EK, deTineo M, Naclerio RM. Total IgE levels do
not change 1 year after endoscopic sinus surgery in patients with chronic
rhinosinusitis. Int Arch Allergy Immunol 2006;139:146-8.
165. Shin SH, Ponikau JU, Sherris DA, Congdon D, Frigas E, Homburger HA,
Swanson MC, Gleich GJ, Kita H. Chronic rhinosinusitis: an enhanced immune
response to ubiquitous airborne fungi. J Allergy Clin Immunol 2004;114:1369-
75.
166. Pant H, Kette FE, Smith WB, Wormald PJ, Macardle PJ. Fungal-specific
humoral response in eosinophilic mucus chronic rhinosinusitis. Laryngoscope
2005;115:601-6.
167. Ragab SM, Lund VJ, Saleh HA, Scadding G. Nasal nitric oxide in objective
evaluation of chronic rhinosinusitis therapy. Allergy 2006;61:717-24.
168. Struben VM, Wieringa MH, Feenstra L, de Jongste JC. Nasal nitric oxide and
nasal allergy. Allergy 2006;61:665-70.
169. Baraniuk JN. Neurogenic mechanisms in rhinosinusitis. Curr Allergy Asthma
Rep 2001;1:252-61.
170. Bellamy JL, Cady RK, Durham PL. Salivary levels of CGRP and VIP in
rhinosinusitis and migraine patients. Headache 2006;46:24-33.
171. Kim DH, Chu HS, Lee JY, Hwang SJ, Lee SH, Lee HM. Up-regulation of
MUC5AC and MUC5B mucin genes in chronic rhinosinusitis. Arch
Otolaryngol Head Neck Surg 2004;130:747-52.
172. Viswanathan H, Brownlee IA, Pearson JP, Carrie S. MUC5B secretion is up-
regulated in sinusitis compared with controls. Am J Rhinol 2006;20:554-7.
173. Ali MS, Hutton DA, Wilson JA, Pearson JP. Major secretory mucin expression
in chronic sinusitis. Otolaryngol Head Neck Surg 2005;133:423-8.
174. Lee HM, Kim DH, Kim JM, Lee SH, Hwang SJ. MUC8 mucin gene up-
regulation in chronic rhinosinusitis. Ann Otol Rhinol Laryngol 2004;113:662-6.
175. Martínez-Antón A, Debolós C, Garrido M, Roca-Ferrer J, Barranco C, Alobid I,
Xaubet A, Picado C, Mullol J. Mucin genes have different expression patterns

VII. Bibliografía Tesis Doctoral
194
in healthy and diseased upper airway mucosa. Clin Exp Allergy 2006;36:448-
57.
176. Martínez-Antón A, Roca-Ferrer J, Mullol J. Mucin gene expression in rhinitis
syndromes. Curr Allergy Asthma Rep 2006;6:189-97.
177. Pena A. A medical history of Bernardo O’ Higgins (1778-1842). Rev Med Chil
1999;127:862-8.
178. Hall-Stoodley L, Stoodley P. Biofilm formation and dispersal and the
transmission of human pathogens. Trends Microbiol 2005;13:7-10.
179. Post JC, Stoodley P, Hall-Stoodley L, Ehrlich GD. The role of biofilms in
otolaryngologic infections. Curr Opin Otolaryngol Head Neck Surg
2004;12:185-90.
180. Lund VJ, Black JH, Szabó LZ, Schrewelius C, Akerlund A. Efficacy and
tolerability of budesonide aqueous nasal spray in chronic rhinosinusitis patients.
Rhinology 2004;42:57-62.
181. Legent F, Bordure P, Beauvillain C, Berche P. A double-blind comparison of
ciprofloxacin and amoxycillin/clavulanic acid in the treatment of chronic
sinusitis. Chemotherapy 1994;40:8-15.
182. Namyslowski G, Misiolek M, Czecior E, Malafiej E, Orecka B, Namyslowski P,
Misiolek H. Comparison of the efficacy and tolerability of
amoxycillin/clavulanic acid 875 mg b.i.d. with cefuroxime 500 mg b.i.d. in the
treatment of chronic and acute exacerbation of chronic sinusitis in adults. J
Chemother 2002;14:508-17.
183. Hashiba M, Baba S. Efficacy of long-term administration of clarithromycin in
the treatment of intractable chronic sinusitis. Acta Otolaryngol Suppl
1996;525:73-8.
184. Wallwork B, Coman W, Mackay-Sim A, Greiff L, Cervin A. A double-blind,
randomized, placebo-controlled trial of macrolide in the treatment of chronic
rhinosinusitis. Laryngoscope 2006;116:189-93.
185. Hartog B, van Benthem PP, Prins LC, Hordijk GJ. Efficacy of sinus irrigation
versus sinus irrigation followed by functional endoscopic sinus surgery. Ann
Otol Rhinol Laryngol 1997;106:759-66.
186. American General Health Survey, 1980.

Tesis Doctoral VII. Bibliografía
195
187. Hedman J, Kaprio J, Poussa T, Nieminen MM. Prevalence of asthma, aspirin
intolerance, nasal polyps and chronic obstructive pulmonary disease in a
population-based study. Inter J Epidemiol 1999;28:717-22.
188. Naclerio R, Durham S, Mygind N, Rhinitis. Mechanisms and management.
Marcel Dekker, Inc. New York. 1999.
189. Settipane GA, Lund VJ, Bernstein JM, Tos M. Nasal polyps: epidemiology,
Pathogenesis and Treatment. OceanSide Publications, Inc. Providence, Rhode
Island; 1997.
190. Klossek JM, Neukirch F, Pribil C, Jankowski R, Serrano E, Chanal I, El
Hasnaoui A. Prevalence of nasal polyposis in France: a cross-sectional, case-
control study. Allergy 2005 ;60:233-7.
191. Alobid I, Benítez P, Bernal-Sprekelsen M, Guilemany JM, Picado C, Mullol J.
The impact of asthma and aspirin sensitivity on quality of life of patients with
nasal polyposis. Qual Life Res 2005;14:789-93.
192. Zeitz HJ. Bronchial asthma, nasal polyps, and aspirin sensitivity: Samter's
syndrome. Clin Chest Med 1988; 9: 567-576.
193. Caplin I, Haynes TJ, Sphan J. Are nasal polyps an allergic phenomenon? Ann
Allergy 1971; 29: 631-634.
194. Terries MH, Davidson TM. Review of published results for endoscopic sinus
surgery. Ear Nose Throat J 1994; 73: 574-580.
195. Alobid I, Benítez P, Valero A, Berenguer J, Bernal-Sprekelsen M, Picado C,
Mullol J. The impact of atopy, sinus opacification, and nasal patency on quality
of life in patients with severe nasal polyposis. Otolaryngol Head Neck Surg
2006;134:609-12.
196. Parson DS. Sinusitis and cystic fibrosis. En: Pediatric Sinusitis. Raven Press,
New York.1992.
197. Jordana M, Dolovich J, Ohno I, Finotto S, Denburg J. Nasal polyposis: a model
for chronic inflammation. In: Asthma and Rhinitis. Bisse WW, Holgate ST, eds.
Blackwell Scientific Publications, Boston 1995:156-64.
198. Djukanovic R. Nasal polyps -a model of chronic respiratory mucosal
inflammation. Clin Exp Allergy 1995;25:582-585.
199. Hellquist HB. Nasal polyps update. Histopathology. Allergy Asthma Proc
1996;17:237-42.

VII. Bibliografía Tesis Doctoral
196
200. Davidsson A Hellquist HB. The so-called 'allergic' nasal polyp. J Oto Rhino
Laryngol Relat Spec 1993;55:30-35.
201. Maldonado M, Martínez A, Alobid I, Mullol J. The antrochoanal polyp.
Rhinology 2004;42:178-82.
202. Ruhno J, Andersson B, Denburg J, Hitch D, Lap P, Vanzieleghem M, Dolovich
J. A double-blind comparison of intranasal budesonide with placebo for nasal
polyposis. J Allergy Clin Immunol 1990;86:946-953.
203. Kawabori S, Denburg JA, Schwartz LB, Irani AA, Wong D, Jordana G, Evans
S, Dolovich J. Histochemical and immunohistochemical characteristic of mast
cells in nasal polyps. Am J Respir Cell Mol Biol 1992;6:37-43.
204. Jordana M, Dolovich J. Eosinophils in nasal polyps. En: Settipane GA, Lund
VJ, Bernstein JM, Tos M (eds). Nasal polyps. Epidemiology, pathogenesis, and
treatment. OceanSide Publications Inc, Providence 1997:49-56.
205. Xaubet A, Mullol J, López E, Roca-Ferrer J, Rozman M, Carrión M, Fabra JM,
Picado C. Comparison of the role of nasal polyp and normal nasal mucosal
epithelial cells on in vitro eosinophil survival. Mediation by GM-CSF and
inhibition of dexamethasone. Clin Exp Allergy 1994; 24: 307-317.
206. Mullol J, Xaubet A, López E, Roca-Ferrer J, Carrión T, Rosello-Catafau J,
Picado C. Eosinophil activation by epithelial cells of the respiratory mucosa.
Comparative study of normal mucosa and inflammatory mucosa. Med Clin
1997; 109: 6-11.
207. Mullol J, E López, J Roca-Ferrer, A Xaubet, L Pujols, JC Fernández-Morata,
JM Fabra, C Picado. Effects of topical anti-inflammatory drugs on eosinophil
survival primed by epithelial cells. Additive effect of glucocorticoids and
nedocromil sodium. Clin Exp Allergy 1997; 27: 1432-1441.
208. Nasser SMS, Pfister R, Chistie PE, Sousa AR, Barker J, Schmitz-Schumann M,
Lee TH. Inflammatory cell populations in bronchial biopsies from aspirin-
sensitive asthmatic subjects. Am J Respir Crit Care Med 1996; 153: 90-96.
209. Drake-Lee A, Price J. Mast cell ultrastructure in the inferior turbinate and
stroma of nasal polyps. J Laryngol Otol 1997; 11: 340-345.
210. Roca-Ferrer J, Mullol J, López E, Xaubet A, Pujols L, Fernández-Morata JC,
Fabra JM, Picado C. Effect of topycal anti-inflammatory drugs on epithelial
cell-induced eosinophil survival and GM-CSF secretion. Eur Respir J 1997; 10:
1489-1495.
Tesis Doctoral VII. Bibliografía
197
211. Mullol J, Roca-Ferrer J, Xaubet A, Traserra J, Picado C. Inhibition of GM-CSF
secretion by topical corticosteroids and nedocromil sodium. A comparison study
using nasal polyp epithelial cells. Respir Med 2000; 94: 428-431.
212. Xaubet A, Mullol J, Roca-Ferrer J, Pujols L, Fuentes M, Pérez M, Fabra JM,
Picado C. Effect of budesonide and nedocromil sodium on IL-8 and IL-6 release
from human nasal mucosa and polyp epithelial cells. Respir Med 2001; 95: 408-
414.
213. Beck LA, Stellato C, Beall LD, Schall TJ, Leopold D, Bickel CA, Baroody F,
Bochner BS, Schleimer RP. Detection of chemokine RANTES and endothelial
adhesion molecules in nasal polyps. J Allergy Clin Immunol 1996; 98: 766-780.
214. Hamilos DL, Leung DYM, Huston DP, Kamil A, Wood R, Hamid Q. GM-SCF,
IL-5 and RANTES immunoreactivity and mRNA expression in chronic
hyperplastic sinusitis with nasal polyposis. Clin Exp Allergy 1998; 28: 1145-
1152.
215. Ramis I, Bioque G, Lorente J, Jares P, Quesada P, Rosello-Catafau J, Gelpi E,
Bulbena O. Constitutive nuclear factor-kappa B activity in human upper airway
tissues and nasal epithelial cells. Eur Respir J 2000; 15: 582-589.
216. Picado C, Fernández-Morata JC, Juan M, Roca-Ferrer J, Fuentes M, Xaubet A,
Mullol J. Cyclooxygenase-2 mRNA is downexpressed in nasal polyps from
aspirin-sensitive asthmatics. Am J Respir Crit Care Med 1999; 160: 291-296.
217. Picot D, Loll PJ, Garavito RM. The X-ray cristal structure of the membrane
protein prostaglandin H2 synthase-1. Nature 1994; 367: 243-249.
218. Samuelsson B, Dahlen SE, Lindgren JA, Rouzer CA, Serhan CN. Leukotrienes
and lipoxins: structures, biosynthesis and biological effects. Science 1987; 237:
1171-1176.
219. Pujols L, Mullol J, Torrego A, Picado C. Glucocorticoid receptors in human
airways. Allergy 2004;59:1042-52.
220. Pujols L, Mullol J, Picado C. Alpha and beta glucocorticoid receptors: relevance
in airway diseases. Curr Allergy Asthma Rep 2007;7:93-9.
221. Guyre PM, Girard MT, Morganelli PM, Manganiello PD. Glucocorticoid effects
on the production and actions of immune cytokines. J Steroid Biochem
1988;30:89-93.
VII. Bibliografía Tesis Doctoral
198
222. Kern JA, Lamb RJ, Reed JC, Daniele RP, Nowell PC. Dexamethasone
inhibition of interleukin 1 beta production by human monocytes.
Posttranscriptional mechanisms. J Clin Invest 1988;81:237-44.
223. Cronstein BN, Kimmel SC, Levin RI, Martiniuk F, Weissmann G. A
mechanism for the antiinflammatory effects of corticosteroids: the
glucocorticoid receptor regulates leukocyte adhesion to endothelial cells and
expression of endothelial-leukocyte adhesion molecule-1 and intercellular
adhesion molecule-1. Proc Natl Acad Sci USA 1992;89:9991-5.
224. Schalkwijk C, Vervoordeldonk M, Pfeilschifter J, Marki F, van den Bosch H.
Cytokine- and forskolin-induced synthesis of group II phospholipase A2 and
prostaglandin E2 in rat mesangial cells is prevented by dexamethasone.
Biochem Biophys Res Commun 1991;180:46-52.
225. O’Banian MK, Winn VD, Young DA. cDNA cloning and functional activity of
a glucocorticoid-regulated inflammatory cyclooxigenase. Proc Natl Acad Sci
USA 1992;89:4888-92.
226. Mullol J, Fernàndez-Morata JC, Roca-Ferrer J, Pujols L, Xaubet A, Benitez P,
Picado C. Cyclooxygenase 1 and cyclooxygenase 2 expression is abnormally
regulated in human nasal polyps. J Allergy Clin Immunol 2002;109:824-30.
227. Pujols L, Benitez P, Alobid I, Martinez-Antón A, Roca-Ferrer J, Mullol J,
Picado C. Glucocorticoid therapy increases COX-2 gene expression in nasal
polyps in vivo. Eur Respir J 2009;33:502-8.
228. Mullol J, Xaubet A, López E, Roca-Ferrer J, Carrión T, Rosello-Catafau J,
Picado C. Eosinophil activation by epithelial cells of the respiratory mucosa.
Comparative study of normal mucosa and inflammatory mucosa. Med Clin
1997;109:6-11.
229. Mullol J, E López, J Roca-Ferrer, A Xaubet, L Pujols, JC Fernández-Morata,
JM Fabra, C Picado. Effects of topical anti-inflammatory drugs on eosinophil
survival primed by epithelial cells. Additive effect of glucocorticoids and
nedocromil sodium. Clin Exp Allergy 1997;27:1432-41.
Tesis Doctoral VII. Bibliografía
199
230. Lildholdt T, Rundcrantz H, Lindqvist N. Efficacy of topical corticosteroid
powder for nasal polyps: a double-blind, placebo-controlled study of
budesonide. Clin Otolaryngol 1995; 20: 26-30.
231. El Naggar M, Kale S, Aldren C, Martin F. Effect of beconase nasal spray on
olfactory function in post-nasal polypectomy patients: a prospective controlled
trial. J Laryngol Otol 1995; 109: 941-944.
232. Mygind N. Advances in the medical treatment of nasal polyps. Allergy 1999;
54: 12-16.
233. Angrill. J, Agusti. C, Torres. A. Bronchiectasis. Curr Opin Infect Dis
2001;14:193-7.
234. Laennec RTH. A treatise on the disease of the chest. Forbes J, trans. New York:
Library of the New York Academy of Medicine, Hafner Publishing,1962,
pag.78.
235. Barker AF. Bronchiectasis. N Engl J Med 2002;346:1383-93.
236. Weycker D, Edelsberg J, Oster G, Tino G. Prevalence and economic burden of
bronchiectasis. Clin Pulm Med 2005;4:205-9.
237. Twiss J, Metcalfe R, Edwards E, Byrnes C. New Zealand national incidence of
bronchiectasis "too high" for a developed country. Arch Dis Child.
2005;90:737-40.
238. Nicotra MB, Rivera M, Dale AM, Shepherd R, Carter R. Clinical,
pathophysiologic, and microbiologic characterization of bronchiectasis in an
aging cohort. Chest 1995;108:955-61.
239. Pasteur MC, Helliwell SM, Houghton SJ, Webb SC, Foweraker JE, Coulden
RA, Flower CD, Bilton D, Keogan MT. An investigation into causative factors
in patients with bronchiectasis. Am J Respir Crit Care Med 2000;162:1277-84.
240. Shoemark A, Ozerovitch L, Wilson R. Aetiology in adult patients with
bronchiectasis. Respir Med 2007;101:1163-70.
241. King P, Holdsworth S, Freezer N, Holmes P. Bronchiectasis. Intern Med J
2006;36:729-37.
242. Rommens JM, Iannuzzi MC, Kerem B, Drumm ML, Melmer G, Dean M, et al.
Identification of the cystic fibrosis gene: chromosome walking and jumping.
Science 1989;245:1059-65.
243. Collins FS. Cystic fibrosis: molecular biology and therapeutic implications.
Science 1992;256:774-9.

VII. Bibliografía Tesis Doctoral
200
244. Gilljam M, Ellis L, Corey M, Zielenski J, Durie P, Tullis DE. Clinical
Manifestations of Cystic Fibrosis Among Patients With Diagnosis in
Adulthood. Chest 2004;126:1215-24.
245. Wood, B. Cystic Fibrosis: 1997. Radiology 1977;204:1-10.
246. Yung MW, Gould J, Upton GJ. Nasal polyposis in children with cystic fibrosis:
a long-term follow-up study. Ann Otol Rhinol Laryngol 2002;111:1081-6.
247. Wang L, Freedman SD. Laboratory tests for the diagnosis of cystic fibrosis. Am
J Clin Pathol 2002;117:109-15
248. Bush A, O´Callaghan C. Primary ciliary dyskinesia. Arch Dis Child
2002;87:363-5
249. Coren ME, Meeks M, Morrison I, Buchdahl RM, Bush A. Primary ciliary
dyskinesia: age at diagnosis and symptom history. Acta Paediatr 2002;91:667-9.
250. Armengot M, Carda C, Escribano A, Samper GJ. Estudio del transporte
mucociliar y de la ultraestructura ciliar nasales en pacientes con síndrome de
Kartagener. Arch Bronconeumol 2005;41:11- 15.
251. Noone PG, Leigh MW, Sannuti A, Minnix SL, Carson JL, Hazucha M, et al.
Primary ciliary dyskinesia: diagnostic and phenotypic features. Am J Respir Crit
Care Med 2004;169:459-67.
252. Corbelli R, Bringolf-Isler B, Amacher A, Sasse B, Spycher M, Hammer J. Nasal
Nitric Oxide Measurements To Screen Children for Primary Ciliary Dyskinesia.
Chest 2004;126:1054-9.
253. Domingo C, Mirapeix RM, Encabo B, Roig J, Lopez D, Ruiz J. Clinical features
and ultrastructure of primary ciliary dyskinesia and Young syndrome. Rev Clin
Esp 1997;197:100-3.
254. Handelsman DJ, Conway AJ, Boylan LM, Turtle JR. Young's syndrome.
Obstructive azoospermia and chronic sinopulmonary infections. N Engl J Med
1984;310:3-9.
255. Tomashefski JF Jr, Crystal RG, Wiedemann HP, Mascha E, Stoller JK; Alpha
1-Antitrypsin Deficiency Registry Study Group. The bronchopulmonary
pathology of alpha-1 antitrypsin (AAT) deficiency: findings of the Death
Review Committee of the national registry for individuals with Severe
Deficiency of Alpha-1 Antitrypsin. Hum Pathol 2004;35:1452-61.
Tesis Doctoral VII. Bibliografía
201
256. Hutchison DC, Cooper D; British Thoracic Society. Alpha-1-antitrypsin
deficiency: smoking, decline in lung function and implications for therapeutic
trials. Respir Med 2002;96:872-80.
257. Lomas DA, Parfrey H. Alpha1-antitrypsin deficiency. 4: Molecular
pathophysiology. Thorax 2004;59:529-35.
258. Strange C, Dickson R, Carter C, Carpenter MJ, Holladay B, Lundquist R, et al.
Genetic testing for alpha1-antitrypsin deficiency. Genet Med 2004;6:204-10.
259. American Thoracic Society/European Respiratory Society Statement: Standards
for the Diagnosis and Management of Individuals with Alpha-1 Antitrypsin
Deficiency. Am J Respir Crit Care Med 2003;168:818-900.
260. Wilson R, Roberts D, Cole P. Effect of bacterial products on human ciliary
function in vitro. Thorax 1985;40:125–31.
261. Cole PJ. Inflammation: a two-edged sword – the model of bronchiectasis. Eur J
Respir Dis Suppl 1986; 147: 6–15.
262. Eller J, Lapa e Silva JR, Poulter LW, Lode H, Cole PJ. Cells and cytokines in
chronic bronchial infection. Ann N Y Acad Sci 1994;725:331–45.
263. Woolhouse, I S; Bayley, D L; Stockley, R A. Effect of sputum processing with
dithiothreitol on the detection of inflammatory mediators in chronic bronchitis
and bronchiectasis. Thorax 2002;57:667-71.
264. Gaga, M; Bentley, A M; Humbert, M; Barkans, J; O'Brien, F; Wathen, C G;
Kay A B; Durham, S R. Increases in CD4+ T lymphocytes, macrophages,
neutrophils and interleukin 8 positive cells in the airways of patients with
bronchiectasis. Thorax 1998;53:685-91.
265. Vendrell M, de Gracia J, Olveira C, Martínez MA, Girón R, Máiz L, Cantón R,
Coll R, Escribano A, Solé A. Diagnosis and treatment of bronchiectasis.
Spanish Society of Pneumology and Thoracic Surgery. Arch Bronconeumol
2008;44:629-40.
266. Angrill J, Agusti C, de Celis R, Rano A, Gonzalez J, Sole T, et al. Bacterial
colonisation in patients with bronchiectasis: microbiological pattern and risk
factors. Thorax 2002;57:15-9.
267. Cantón R, Cobos N, de Gracia J, Baquero F, Honorato J, Gartner S, Alvarez A,
Salcedo A, Oliver A, García-Quetglas E; Spanish Consensus Group for
Antimicrobial Therapy in the Cystic Fibrosis Patient. Antimicrobial therapy for

VII. Bibliografía Tesis Doctoral
202
pulmonary pathogenic colonisation and infection by Pseudomonas aeruginosa in
cystic fibrosis patients. Clin Microbiol Infect 2005;11:690-703.
268. Woodhead M, Blasi F, Ewig S, Huchon G, Ieven M, Ortqvist A, Schaberg T,
Torres A, van der Heijden G, Verheij TJ; European Respiratory Society;
European Society of Clinical Microbiology and Infectious Diseases. Guidelines
for the management of adult lower respiratory tract infections. Eur Respir J
2005;26:1138-80.
269. Máiz L, Baranda F, Coll R, Prados C, Vendrell M, Escribano A, Gartner S, de
Gracia S, Martínez M, Salcedo A, Vázquez C; SEPAR (Spanish Society of
Pneumology and Thoracic Surgery). SEPAR (Spanish Society of Pneumology
and Thoracic Surgery) Guidelines. Guideline for diagnosis and treatment of
respiratory involvements in cystic fibrosis. Arch Bronconeumol 2001;37:316-
24.
270. Evans DJ, Bara AI, Greenstone M. Prolonged antibiotics for purulent
bronchiectasis. Cochrane Database Syst Rev. 2003;(4):CD001392.
271. Saiman L, Marshall BC, Mayer-Hamblett N, Burns JL, Quittner AL, Cibene
DA, Coquillette S, Fieberg AY, Accurso FJ, Campbell PW 3rd; Macrolide
Study Group. Azithromycin in patients with cystic fibrosis chronically infected
with Pseudomonas aeruginosa: a randomized controlled trial. JAMA
2003;290:1749-56.
272. Davis G, Wilson R. Prophylactic antibiotic treatment of bronchiectasis with
azithromycin. Thorax 2004;59:540-1.
273. de Gracia J, Máiz L, Prados C, Vendrell M, Baranda F, Escribano A, Gartner S,
López-Andreu JA, Martínez M, Martínez MT, Pérez Frías J, Seculi JL, Sirvent
J. Nebulized antibiotics in patients with cystic fibrosis. Med Clin (Barc)
2001;117:233-7.
274. Lavery K, O'Neill B, Elborn JS, Reilly J, Bradley JM. Self-management in
bronchiectasis: the patients' perspective. Eur Respir J 2007;29:541-7.
275. King PT, Holdsworth SR, Freezer NJ, Villanueva E, Holmes PW.
Characterisation of the onset and presenting clinical features of adult
bronchiectasis. Respir Med 2006;100:2183-89.
276. Smith IE, Jurriaans E, Diederich S, Ali N, Shneerson JM, Flower CD. Chronic
sputum production: correlations between clinical features and findings on high

Tesis Doctoral VII. Bibliografía
203
resolution computed tomographic scanning of the chest. Thorax 1996;51:914-
18.
277. Hun-Jong D, Hyo Yeol K, Young-Jun C, Tae Wook K, Joon Ho K, Seung-Kyu
C et al. Computed tomographic assessment of chronic rhinosinusitis with
asthma. Am J Rhinol 2006;5:450–2.
278. Judge EP, Dodd JD, Masterson JB, Gallagher CG. Pulmonary abnormalities on
high-resolution CT demonstrate more rapid decline than FEV1 in adults with
cystic fibrosis. Chest 2006;130:1424-32.
279. Lundberg JO, Rinder J, Weitzberg E, Lundberg JM, Alving K. Nasally exhaled
nitric oxide in humans originates mainly in the paranasal sinuses. Acta Physiol
Scand 1994;152:431–2.
280. Lindberg S, Cervin A, Runer T. Nitric oxide (NO) production in the upper
airways is decreased in chronic sinusitis. Acta Otolaryngol 1997;117:113-7.
281. Arnal JF, Flores P, Rami J, Murris-Espin M, Bremont F, Pasto I et al. Nasal
nitric oxide concentration in paranasal sinus inflammatory diseases. Eur Respir
J 1999;13:307-12.
282. Colantonio D, Brouillette A, Parikh A, Scadding GK. Paradoxical low nasal
nitric oxide in nasal polyposis. Clin Exp Allergy 2002;32:698–701.
283. Kharitonov SA, Wells AU, O'Connor BJ, Cole PJ, Hansell DM, Logan-Sinclair
RB et al. Elevated levels of exhaled nitric oxide in bronchiectasis. Am J Respir
Crit Care Med 1995;151:1889-93.
284. Narang I, Ersu R, Wilson NM, Bush A. Nitric oxide in chronic airway
inflammation in children: diagnostic use and pathophysiological significance.
Thorax 2002;57:586–9.
285. Foley SC, Hopkins NO, Fitzgerald MX, Donnelly SC, McLoughlin P. Airway
nitric oxide output is reduced in bronchiectasis. Respir Med 2007;101:1549-55.
286. Bousquet J, Knani J, Dhivert H, Richard A, Chicoye A, Ware Jr JE. Quality of
life in asthma. I. Internal consistency and validity of the SF-36 questionnaire.
Am J Respir Crit Care Med 1994;149:371-75.
287. Osborne ML, Vollmer WM, Linton KL, Buist AS. Characteristics of patients
with asthma within a large HMO: a comparison by age and gender. Am J Respir
Crit Care Med 1998;157:123–8.

VII. Bibliografía Tesis Doctoral
204
288. Gee L, Abbott J, Conway SP, Etherington C, Webb AK. Quality of life in cystic
fibrosis: the impact of gender, general health perceptions and disease severity. J
Cyst Fibros 2003;2:206-13.
289. Engstrom CP, Persson LO, Larsson S, Sullivan M. Reliability and validity of a
Swedish version of the St. George’s Respiratory Questionnaire. Eur Respir J
1998;11:61–6.
290. Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A self-complete measure
of health status for chronic airflow limitation: the St. Georges’s Respiratory
Questionnaire. Am Rev Respir Dis 1992; 145:1321–27.
291. Knebel AR, Leidy NK, Sherman S. Health related quality of life and disease
severity in patients with alpha-1 antitrypsin deficiency. Qual Life Res
1999;8:385–91.
292. Chang JA, Curtis R, Patrick DL, Raghu G. Assessment of health-related quality
of life in patients with interstitial lung disease. Chest 1999;116:1175–82.
293. O'Leary CJ, Wilson CB, Hansell DM, Cole PJ, Wilson R, Jones PW.
Relationship between psychological well-being and lung health status in
patients with bronchiectasis. Respir Med 2002;96:686-92.
294. Macia MD, Blanquer D, Togores B, Sauleda J, Perez JL, Oliver A.
Hypermutation is a key factor in development of multiple-antimicrobial
resistance in Pseudomonas aeruginosa strains causing chronic lung infections.
Antimicrob Agents Chemother. 2005;49:3382-6.
295. Rosell A, Monso E, Soler N, Torres F, Angrill J, Riise G, et al. Microbiologic
determinants of exacerbation in chronic obstructive pulmonary disease. Arch
Intern Med 2005;165:891-7.
296. Hernandez C, Abreu J, Jimenez A, Fernandez R, Martin C. Pulmonary function
and quality of life in relation to bronchial colonization in adults with
bronchiectasis not caused by cystic fibrosis. Med Clin (Barc) 2002;118:130-4.
297. Gillespie MB, Osguthorpe JD. Pharmacologic management of chronic
rhinosinusitis, alone or with nasal polyposis. Curr Allergy Asthma Rep
2004;4:478-85.
298. Huvenne W, van Bruaene N, Zhang N, van Zele T, Patou J, Gevaert P, Claeys
S, Van Cauwenberge P, Bachert C. Chronic rhinosinusitis with and without
nasal polyps: what is the difference? Curr Allergy Asthma Rep 2009;9:213-20.

Tesis Doctoral VII. Bibliografía
205
299. Radenne F, Lamblin C, Vandezande LM, Tillie-Leblond I, Darras J, Tonnel AB,
Wallaert B. Quality of life in nasal polyposis, J Allergy Clin Immunol
1999;104:79–84.
300. Leynaert B, Neukirch C, Liard R, Bousquet J, Neukirch F. Quality of life in
allergic rhinitis and asthma. A population-based study of young adults. Am J
Respir Crit Care Med 2000;162:1391-6.
301. Gliklich RE, Metson R. Effect of sinus surgery on quality of life. Otolaryngol
Head Neck Surg 1997;117:12-7.
302. Winstead W, Barnett S. Impact of endoscopic sinus surgery on global health
perception: an outcomes study. Otolaryngol Head Neck Surg 1998;119:486-91.
303. Durr DG, Desrosiers MY, Dassa C. Quality of life in patients with
rhinosinusitis. J Otolaryngol 1999;28:108-11.
304. Wang PC, Tai CJ, Lin MS, Chu CC, Liang SC. Quality of life in Taiwanese
adults with chronic rhino-sinusitis. Qual Life Res 2003;12:443-8.
305. Failde I, Ramos I. Validity and reliability of the SF-36 health survey
questionnaire in patients with coronary artery disease. J Clin Epidemiol
2000;53:359-65.
306. Alonso J, Prieto L, Ferrer M, Vilagut G, Broquetas JM, Roca J, et al. Testing
the measurement properties of the Spanish version of the SF-36 Health Survey
among male patients with chronic obstructive pulmonary disease. Quality of life
in COPD study group. J Clin Epidemiol 1998;51:1087-94.
307. Espinosa De Los Monteros MJ, Alonso J, Ancochea J, Gonzalez A. Quality of
life in asthma: reliability and validity of the short form generic questionnaire
(SF-36) applied to the population of asthmatics in a public health area. Arch
Bronconeumol 2002;38:4-9.
308. Piccirillo JF, Merritt MG Jr, Richards ML. Psychometric and clinimetric
validity of the 20-Item Sino-Nasal Outcome Test (SNOT-20). Otolaryngol Head
Neck Surg 2002 ;126:41-7.
309. Van Zele T, Claeys S, Gevaert P, Van Maele G, Holtappels G, Van
Cauwenberge P, Bachert C. Differentiation of chronic sinus diseases by
measurement of inflammatory mediators. Allergy 2006;61:1280-9.
310. Deal RT, Kountakis SE. Significance of nasal polyps in chronic rhinosinusitis:
symptoms and surgical outcomes. Laryngoscope 2004;114:1932-5.

VII. Bibliografía Tesis Doctoral
206

Tesis Doctoral VII. Bibliografía
207
Related Documents











