Journal of Neurology, Neurosurgery, and Psychiatry, 1980, 43, 118-126 Is ideomotor apraxia the outcome of damage to well-defined regions of the left hemisphere? Neuropsychological study of CAT correlation A BASSO, C LUZZATTI, H SPINNLER From the Neuropsychology Centre ofMilan University, Milan, Italy SUMMARY A CAT scan was recorded from 123 patients with left hemisphere damage from stroke. They were divided into four groups according to presence or absence of ideomotor apraxia and length of illness (15 to 90 days and over 90 days). The lesions were mapped and compared in the four experimental groups for anteroposterior dimension, lesion depth-deep-seated lesions deing separated from lesions with a superficial component-and position with respect to the Sylvian fissure for lesions encroaching on the surface. In the anteroposterior dimension there is no material bifference in the distribution of the lesions with respect to length of illness. Moreover, any difference is hardly detectable between the profiles for patients with and without ideomotor apraxia except for the higher frequency of deep lesions in the non-apraxic group. The same holds true for "small" lesions. One of the oldest and most fascinating aims of clinical neuropsychology is to establish anatomo- psychological correlations. The classical approach based on single necropsy cases selected for be- havioural impairment-that is, for the presence of an outstanding neuropsychological impairment -supplied very precise information on the anatomy of the lesions but, by definition, could not furnish inferential data. Another approach has been to take large series of unselected hemi- sphere-damaged patients, divide them into groups according to the topography suggested by their neurological or instrumental signs, put them through standard tests, and subject the group results to statistical analysis. Nowadays CAT scanning permits a check on the putative lesion area, and its systematic use enables us to con- sider the crucial problem raised by von Monakov' and by Brun2 of the "negative" cases-that is, those in which the presumed critical area does not fit the impaired ability. We have attempted a retrospective study of the records of our Aphasia Unit (this on left hemisphere-damaged Address for reprint requests: Dr A Basso, Neuropsychology Centre of Milan University, Via F. Sforza, 35, 20122 Milano, Italy. Accepted 12 June 1979 ratients only), focusing our attention on ideo- motor apraxia. We are well aware that CAT localisation of a cerebrovascular lesion cannot be anything like as accurate as histological localis- ation, for only occasionally does a CAT assess- ment give sufficient information on the extent of a lesicn in the grey and white matter structures regarded as functionally important for the ability in question. But we thought it would be worth attempting a generalisation of the information drawn by Liepmann,3 4 Niessl von Mayendorff, I Heilbronner,6 and more recently by Ajuriaguerra et al,7 Heilman et al.s and Gc.chwind,9 from a few selected cases to a large series of strictly unselected cases. The aims of the study were two. The first was to ascertain whether the presence or absence of ideomotor apraxia in left hemisphere-damaged (L/pts) is related to the CAT locus of a cerebro- vascular lesion. Here two points were considered: (1) the anteroposterior dimension of the left hemisphere lesion and its depth, and (2) the lesions encroaching on the surface of the hemi- sphere with respect to the Sylvian fissure. The second aim was to establish whether the presence/ absence of ideomotor apraxia is related to a CAT index representing the volume of destroyed cerebral tissue. 118

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Journal of Neurology, Neurosurgery, and Psychiatry, 1980, 43, 118-126
Is ideomotor apraxia the outcome of damage towell-defined regions of the left hemisphere?Neuropsychological study of CAT correlation
A BASSO, C LUZZATTI, H SPINNLER
From the Neuropsychology Centre ofMilan University, Milan, Italy
SUMMARY A CAT scan was recorded from 123 patients with left hemisphere damage fromstroke. They were divided into four groups according to presence or absence of ideomotor apraxiaand length of illness (15 to 90 days and over 90 days). The lesions were mapped and comparedin the four experimental groups for anteroposterior dimension, lesion depth-deep-seated lesionsdeing separated from lesions with a superficial component-and position with respect to the Sylvianfissure for lesions encroaching on the surface. In the anteroposterior dimension there is no materialbifference in the distribution of the lesions with respect to length of illness. Moreover, any differenceis hardly detectable between the profiles for patients with and without ideomotor apraxia exceptfor the higher frequency of deep lesions in the non-apraxic group. The same holds true for "small"lesions.
One of the oldest and most fascinating aims ofclinical neuropsychology is to establish anatomo-psychological correlations. The classical approachbased on single necropsy cases selected for be-havioural impairment-that is, for the presenceof an outstanding neuropsychological impairment-supplied very precise information on theanatomy of the lesions but, by definition, couldnot furnish inferential data. Another approachhas been to take large series of unselected hemi-sphere-damaged patients, divide them into groupsaccording to the topography suggested by theirneurological or instrumental signs, put themthrough standard tests, and subject the groupresults to statistical analysis. Nowadays CATscanning permits a check on the putative lesionarea, and its systematic use enables us to con-sider the crucial problem raised by von Monakov'and by Brun2 of the "negative" cases-that is,those in which the presumed critical area doesnot fit the impaired ability. We have attempteda retrospective study of the records of ourAphasia Unit (this on left hemisphere-damaged
Address for reprint requests: Dr A Basso, NeuropsychologyCentre of Milan University, Via F. Sforza, 35, 20122 Milano,Italy.
Accepted 12 June 1979
ratients only), focusing our attention on ideo-motor apraxia. We are well aware that CATlocalisation of a cerebrovascular lesion cannot beanything like as accurate as histological localis-ation, for only occasionally does a CAT assess-ment give sufficient information on the extent ofa lesicn in the grey and white matter structuresregarded as functionally important for the abilityin question. But we thought it would be worthattempting a generalisation of the informationdrawn by Liepmann,3 4 Niessl von Mayendorff, I
Heilbronner,6 and more recently by Ajuriaguerraet al,7 Heilman et al.s and Gc.chwind,9 froma few selected cases to a large series of strictlyunselected cases.The aims of the study were two. The first was
to ascertain whether the presence or absence ofideomotor apraxia in left hemisphere-damaged(L/pts) is related to the CAT locus of a cerebro-vascular lesion. Here two points were considered:(1) the anteroposterior dimension of the lefthemisphere lesion and its depth, and (2) thelesions encroaching on the surface of the hemi-sphere with respect to the Sylvian fissure. Thesecond aim was to establish whether the presence/absence of ideomotor apraxia is related to a CATindex representing the volume of destroyedcerebral tissue.
118
Is ideomotor apraxia the outcome of damage to well-defined regions of the left hemisphere? 119
Subjects and methods
The cases were drawn from a continuous seriesof 279 left hemisphere-damaged patients whosuffered their first stroke (either haemorrhagic orischaemic), entering the wards of the Neuro-logical Department of Milan University (163) orexamined as outpatients (116) in our AphasiaUnit during the peri,od from January 1977 toJune 1978. We excluded 124 L/pts for thefollowing reasons: 15 because of more than 20%left handedness on the Edinburgh inventory, 59because of clinical or CAT scan evidence ofbilateral lesions, 20 because of unwillingness tobe tested, 25 because of movement artefacts onthe CAT scan, two because of the presence ofa crossed aphasia, and three for concomitantepilepsy. Another 32 were excluded on the fol-lowing grounds: five had negative CAT scan and27 underwent CAT scanning and apraxia testingless than 15 days after the stroke. When CATscanning is done in the first days and the cerebro-vascular lesion is ischaemic, it may be normal(neither hypodense nor hyperdense) or showoedema and it can be difficult to localise the realextent of the lesion; finally, patients might notlie still and the scan would be blurred. Moreover,major or minor vigilance impairments, oftenpresent in the first 15 days, can make formaltesting for apraxia unreliable. Table 1 gives thecurrent data for L/pts entering this study.The 123 L/pts entering the study were divided
into two groups according to the interval betweenstroke and examination: 15 to 90 days (65patients) and over 90 days (58 patients). Thepurpose of this was to take into account therelationship between the CAT localisation andthe possible ultimate functional recovery, for itis well known that apraxia may be clinicallyapparent within a few days of a brain lesion andthen disappear. The groups were then dividedaccording t-o performance on the tests. Thus,
four experimental groups were formed (table 1).It is worth noting that the lesion localisationswere compared between patients with and with-out ideomotor apraxia divided by illness length(as detailed above) and between severe and mildapraxic patients.
TESTING PROCEDURES FOR IDEOMOTOR APRAXIA
All L/pts underwent testing for ideomotorapraxia according to the routine of our AphasiaUnit.'t They were asked to imitate (with the arm-hand ipsilateral to the damaged hemisphere) 10different single gestures. Each item scored twopoints (immediate correct response), one point(correct response preceded by hesitation and pro-tracted latency during which wrong or unsuc-cessful movements may be made, or performanceconceptually correct, bu-t actual movements some-what inaccurate or awkward) and no points (anyother type of error). The best score is thus 20.Patients with scores below a cut-off score of 17(obtained by De Renzi et al, on 40 control sub-jects and 45 right hemisphere-damaged patien.ts)are considered to be apraxic. Apraxic patientswere further divided into mildly and severelyapraxic according to whether their score on ourapraxia scale fell over or under the median value(12). Table 2 shows the distribu,tion of the 123L/pts entering the study on our 0-20 apraxiascale as well as their distribution according to theapraxia cut-off score (17) and the median value(12).
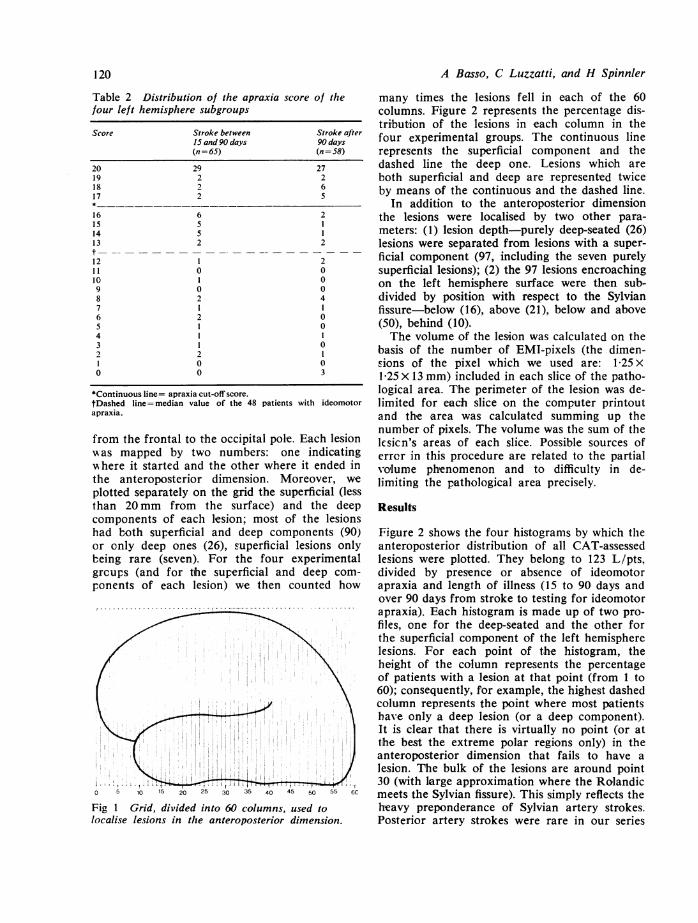
CAT SCAN INVESTIGATIONSWithin 10 days of testing for ideomotor apraxia,all patients underwent a CAT scan. The lesionswere mapped by the method of Luzzatti et al.12We decided to read the maximum anteroposterior(AP) dimension of the lesion on a grid of sizeequal to that of the lateral diagram used formapping the lesion. These grids are divided into60 equal columns, numbered 1 to 60 (see fig 1)
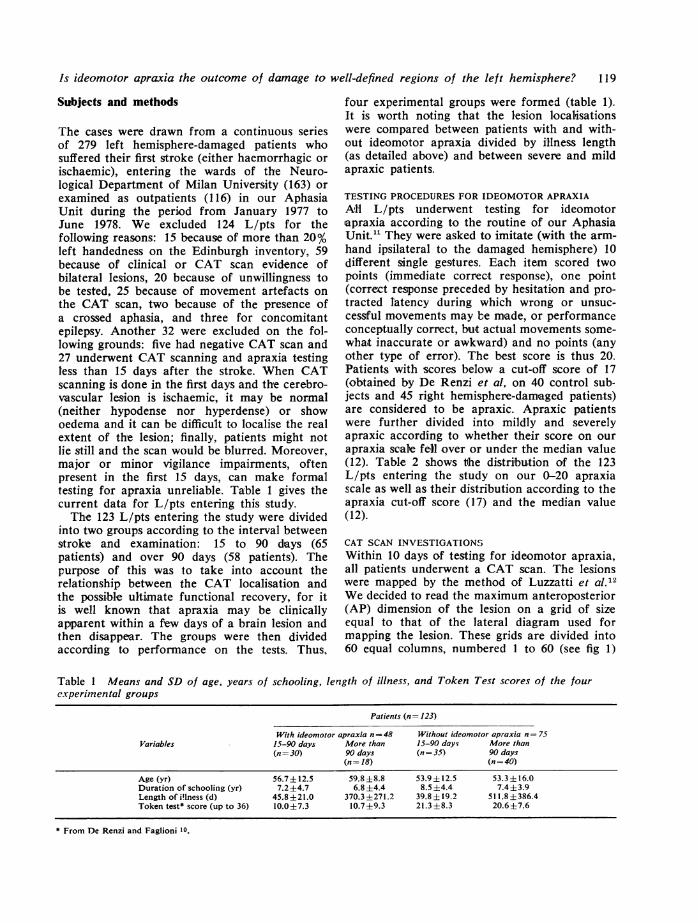
Table 1 Means and SD of age, years of schooling, length of illness, and Token Test scores of the fourcxperiniental groups
Patients (n= 123)
With ideomotor apraxia n=48 Without ideomotor apr-axia n = 75Variables 15-90 days More than 15-90 days More than
(n= 30) 90 days (n= 35) 90 days(n= 18) (n= 40)
Age (yr) 56.7±12.5 59.8 ±8.8 53.9±12.5 53.3 ±16.0Duration of schooling (yr) 7.2±4.7 6.8±4.4 8.5 ±4.4 7.4±3.9Length of illness (d) 45.8±21.0 370.3±271.2 39.8±19.2 511.8±386.4Token test* score (up to 36) 10.0±7.3 10.7±9.3 21.3±8.3 20.6±7.6
* From De Renzi and Faglioni 10.
120
Table 2 Distribution of the apraxia score of thefour left hemisphere subgroups
Score Stroke between Stroke after15 and 90 days 90 days(n=65) (n=58)
20 29 2719 2 218 2 617 2 5
16 6 215 5 114 5 113 2 2
12 1 211 0 010 1 09 0 08 2 47 1 16 2 05 1 04 13 02 2 1l 0 00 0 3
*Continuous line= apraxia cut-off score.tDashed line= median value of the 48 patients with ideomotorapraxia.
from the frontal to the occipital pole. Each lesionwas mapped by two numbers: one indicating,-here it started and the other where it ended inthe anteroposterior dimension. Moreover, weplotted separately on the grid the superficial (lessthan 20 mm from the surface) and the deepcomponents of each lesion; most of the lesionshad both superficial and deep components (90)or only deep ones (26), superficial lesions onlybeing rare (seven). For the four experimentalgrcups (and for the superficial and deep com-ponents of each lesion) we then counted how
0 5 10 15 20 25 30 35 40 45 50 55 6C
Fig 1 Grid, divided into 60 columns, used tolocalise lesions in the anteroposterior dimension.
A Basso, C Luzzatti, and H Spinnler
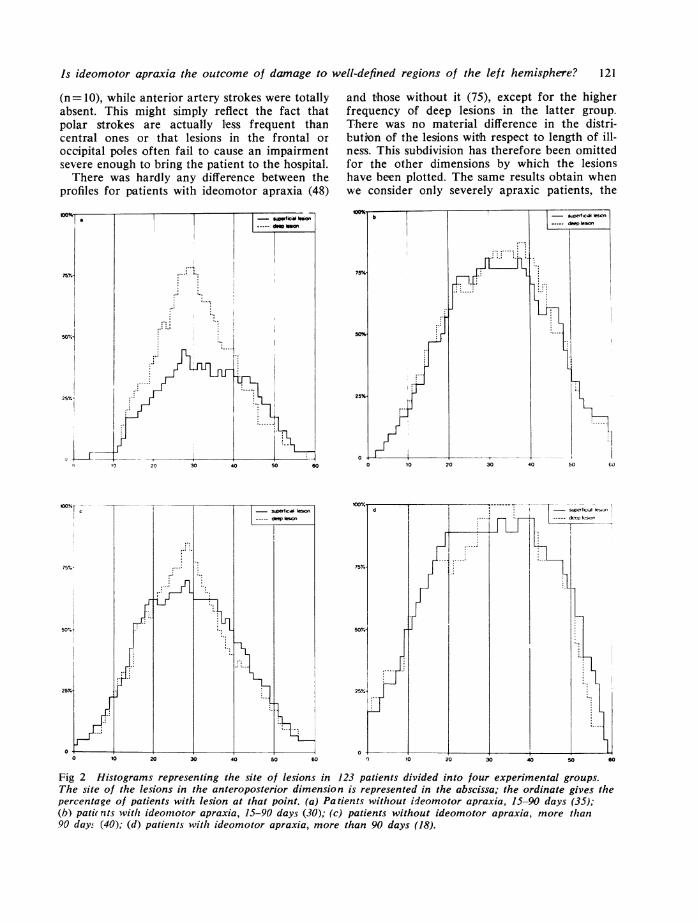
many times the lesions fell in each of the 60columns. Figure 2 represents the percentage dis-tribution of the lesions in each column in thefour experimental groups. The continuous linerepresents the superficial component and thedashed line the deep one. Lesions which areboth superficial and deep are represented twiceby means of the continuous and the dashed line.
In addition to the anteroposterior dimensionthe lesions were localised by two other para-meters: (1) lesion depth-purely deep-seated (26)lesions were separated from lesions with a super-ficial component (97, including the seven purelysuperficial lesions); (2) the 97 lesions encroachingon the left hemisphere surface were then sub-divided by position with respect to the Sylvianfissure-below (16), above (21), below and above(50), behind (10).The volume of the lesion was calculated on the
basis of the number of EMI-pixels (the dimen-sions of the pixel which we used are: 1-25 x1-25 x 13 mm) included in each slice of the patho-logical area. The perimeter of the lesion was de-limited for each slice on the computer printoutand the area was calculated summing up thenumber of pixels. The volume was the sum of thelcsicn's areas of each slice. Possible sources oferror in this procedure are related to the partialvolume phenomenon and to difficulty in de-limiting the pathological area precisely.
Results
Figure 2 shows the four histograms by which theanteroposterior distribution of all CAT-assessedlesions were plotted. They belong to 123 L/pts,divided by presence or absence of ideomotorapraxia and length of illness (15 to 90 days andover 90 days from stroke to testing for ideomotorapraxia). Each histogram is made up of two pro-files, one for the deep-seated and the other forthe superficial component of the left hemispherelesions. For each point of the histogram, theheight of the column represents the percentageof patients with a lesion at that point (from 1 to60); consequently, for example, the highest dashedcolumn represents the point where most patientshave only a deep lesion (or a deep component).It is clear that there is virtually no point (or atthe best the extreme polar regions only) in theanteroposterior dimension that fails to have alesion. The bulk of the lesions are around point30 (with large approximation where the Rolandicmeets the Sylvian fissure). This simply reflects theheavy preponderance of Sylvian artery strokes.Posterior artery strokes were rare in our series
Is ideomotor apraxia the outcome of damage to well-defined regions of the left hemisphere? 121
(n=10), while anterior artery strokes were totallyabsent. This might simply reflect the fact thatpolar strokes are actually less frequent thancentral ones or that lesions in the frontal oroccipital poles often fail to cause an impairmentsevere enough to bring the patient to the hospital.There was hardly any difference between the
profiles for patients with ideomotor apraxia (48)
and those without it (75), except for the higherfrequency of deep lesions in the latter group.There was no material difference in the distri-bution of the lesions witih respect to length of ill-ness. This subdivision has therefore been omittedfor the other dimensions by which the lesionshave been plotted. The same results obtain whenwe consider only severely apraxic patients, the
Fig 2 Histograms representing the site of lesions in 123 patients divided into four experimental groups.The site of the lesions in the anteroposterior dimension is represented in the abscissa; the ordinate gives thepercentage of patients with lesion at that point. (a) Patients without ideomotor apraxia, 15-90 days (35);(b) pati( nts with ideomnotor apraxia, 15-90 days (30); (c) patients without ideomotor apraxia, more than90 days (40); (d) patients with ideomotor apraxia, more than 90 days (18).
122
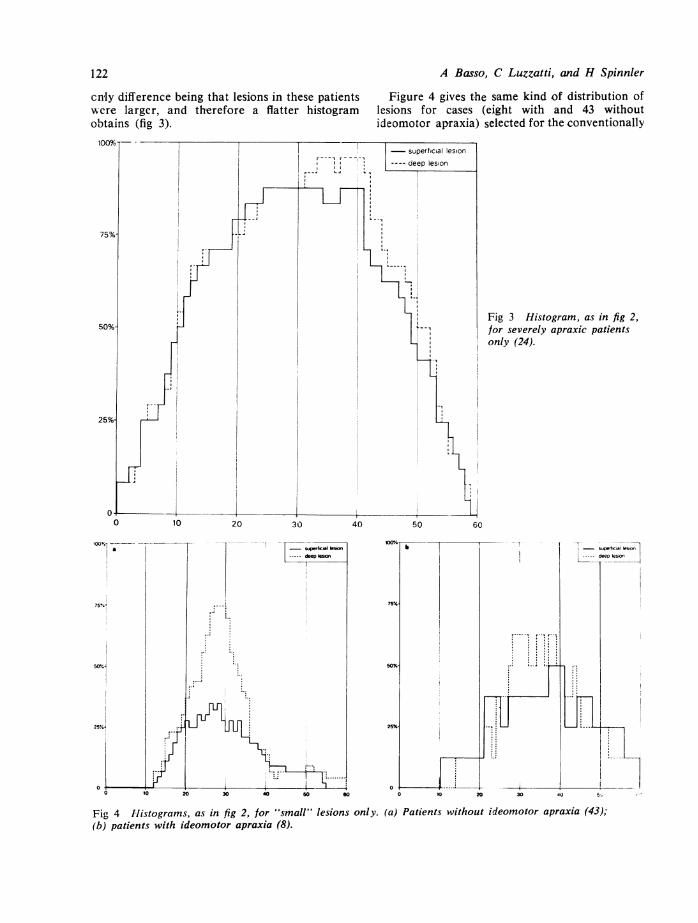
cnly difference being that lesions in these patientswere larger, and therefore a flatter histogramobtains (fig 3).
A Basso, C Luzzatti, and H Spinnler
Figure 4 gives the same kind of distribution oflesions for ca.ses (eight with and 43 withoutideomotor apraxia) selected for the conventionally
Fig 3 Histogram, as in fig 2,for severely apraxic patientsonly (24).
Fig 4 Histograms, as in fig 2, for "small" lesions only. (a) Patients without ideomotor apraxia (43);(b) patients with ideomotor apraxia (8).
50 eo
Is ideornotor apraxia the outcome of damage to we!l-defined regions of the left hemisphere? 123
defined "smallness" of their lesions (less than40% of the anteroposterior index). There is againan impressive similarity of profile between thosewith and without the disorder, which is clearlyat variance with the view that one or more areascritical for ideomotor apraxia lie in highlypredictable regions.
Table 3 shows the L/pts (123) divided bypresence or absence of ideomotor apraxia andencroachment or not of the lesion on the cerebralsurface. Purely deep lesions were rarely as-sociated with ideomotor apraxia (x2=7-743,df=l,,p <001).
Table 3 Distribution of patients with and withoutideomotor apraxia according to location of lesions
Level oJ lesion Patients Patientswithout withideomotor apraxia ideomotor apraxia(n= 75) (n= 48)
Only deep lesions (n= 26) 22 4Lesions encroaching on thesurface (n=97) 53 44
20 Ie oor°° °° °°2
17 -17
-
0 164--
10
5
0
Table 4 concerns the 97 L/pts with lesionsencroaching on the cerebral surface. They aredivided by position of the lesion with respect tothe Sylvian fissure (below, above, below andabove, behind) and presence or absence of ideo-motor apraxia. It turns out that none of theseanatomical positions fits the behavioural sub-division onto patients with and without apraxia(x2=5 177, df= 3, P: NS).
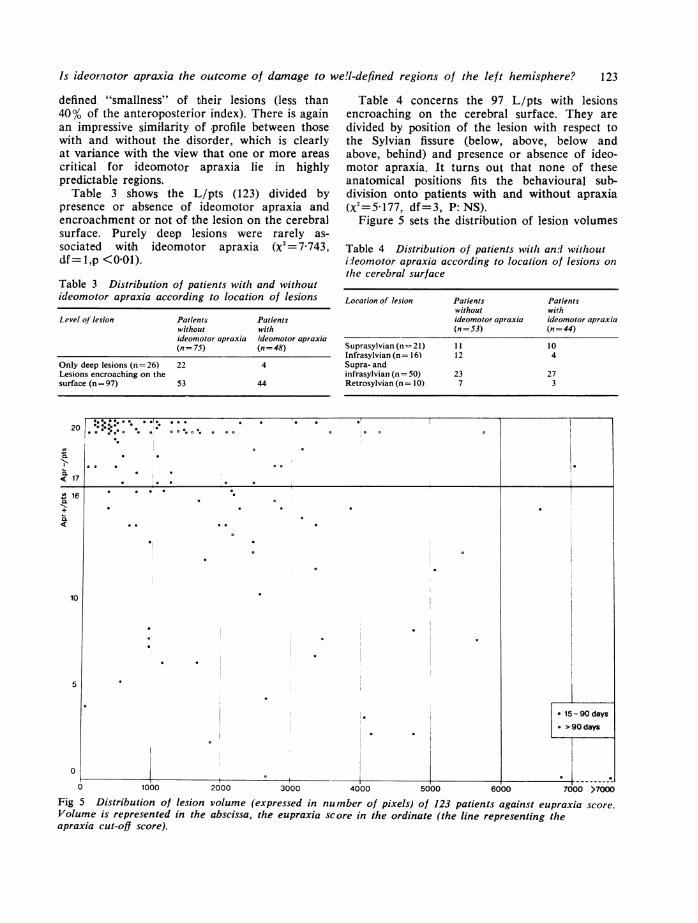
Figure 5 sets the distribution of lesion volumes
Table 4 Distribution of patients with an.d withoutideomotor apraxia according to location of lesions onithe cerebral surface
Location of lesion Patients Patientswithout withideomotor apraxia ideomotor apraxia(n=3) (n= 44)
Suprasylvian (n-=21) I I 10Infrasylvian (n= 16) 12 4Supra- andinfrasylviazn (n= 50) 23 27Retrosylvian (n= 10) 7 3
15-90 days
e >90days
0,---r- -,
0 1000 2000 3000 4000 5000 6000 7000 >7000
Fig 5 Distribution of lesion volume (expressed in number of pixels) of 123 patients against eupraxia score.Volume is represented in the abscissa, the eupraxia score in the ordinate (the line representing theapraxia cut-off score).
1-
0
-

124
of all L/pts against the apraxia scores. As it canbe seen there is no easily detectable relationshipbetween apraxia score and lesion volume.
Discussion
The main value of atte.m,pts like ours to correlatethe locus and extent of a hemisphere lesion andthe presence or absence of a neuropsychologicaldefect is the absence of nearly any neuropsy-chological selection of the patients entering thestudy, an approach diametrically opposed to theclassical one.
If we consider the map of lesions in patientswit!h ideomotor apraxia, we find somethingapproximating to the classical notion of apraxialocalisation within the left hemisphere-namely,in the anterior, central, and suprasylvian re-
trorolandic areas,14 disconnection of which fromthe central executor region has been regarded asresponsible for apraxia. So the correlations ofpatients with ideomotor apraxia tally with the"positive" clinico-anatomical correlations foundby von Monakov' for his 10 apraxia cases(". . . in Bezug auf die Lokalisation der Apraxiakame jeder Vertreter einer besonderen Lokal-isationsweise auf seine Rechnung"). Thesame is true if we consider the maps of severelyapraxic patients-that is, of patients whose be-havioural impairment is probably more similarto that of the single necropsy cases (fig 3).Turning to the patients who did not have ideo-
motor apraxia, we find a pattern of lesion dis-tribution similar to that for those with the dis-order which also agrees pretty well with vonMonakov's rather sceptical conclusions. Thereis no such agreement in the case of deep-seatedlesions which are often unrelated to apraxia (butsee Kimura"5). These usually lie either withinthe striatum or, more often, deeper, and theynearly always encroach on the inner capsule.Since the connections classically regarded asbearing on apraxia are more superficial, thedisagreement may be more apparent than real.A similar situation arises when "small" lesionsbelonging to patients either with or without ideo-motor apraxia are considered separately. Suchlesions have been regarded hypothetically ascapable of affecting very circumscribed crucialstructures almost selectively.To illustrate our findings better we selected
six patients with and six without ideomotorapraxia, all of whom had small scattered andtopographically equivalent lesions; fig 6 showshow similar lesions can cause or not cause anapraxic behaviour. Pure small frontal lesions are
A Basso, C Luzzatti, and H Spinnler
not illustrated here as they were not present inour series.Although our routine testing for ideomotor
apraxia is only a rough guide to apraxia, mainlybecause there is no evaluation of gesturesequencing, we do not think it is responsible forthe negative outcome of our study. This issupported by the conclusions of De Renzi et al6who query the paramount value of motorsequence tasks"7 in detecting apraxia. We do notmean that a more flexible assessment of a.praxia,perhaps with allowance for a different classifi-cation of apraxia syndromes, would not providesomewhat different results, as was the case withaphasia localisations.13 However, this is hypo-thetical and calls for a prospective study whichis in progress.Our findings need checking because they cast
doubt on any strictly localising approach toideomotor apraxia and at the same time fail tosuggest what is the anatomical difference betweenapraxic and non-apraxic patients. Our feeling isthat apraxia is the outco.me of widespread dis-ruption in the left hemisphere and in somecallosal connections or even in the right hemi-sphere. The CAT scan approach of lumping thelesions together and localising them in one ormore leftsided regions failed to elicit the crucialtopography, whether because the network ofcritical connections is too diffuse (that is, theopposite of what is meant by a "centre") orbecause CAT scanning is not yet suitable fordemonstrating the relevant highly circumscribedregions, we do not know. Since the question isopen, we may discuss three possible explanationsof our findings.
1. Although there may be circumscribed"centres" for eupraxia in the left hemisphere(for example, parietal inferior and premotorcentres), their location probably varies or, if thelocation is the same, it will rarely show up onthe routine CAT map at the same point. There-fore the "critical areas" are hit unpredictablyby a single stroke with a known CAT localisation,a supposition that would tie in surprisingly wellwith "negative" correlations (tha-t is, absence ofapraxia in presence of a lesion in the areaspredicted by the "positive" cases) contributedmore than half a century ago and stronglyemphasised by von Monakov1 in his thoughtfuldispute against what he called the "anatomicalpsychology" of Wernicke's school.
2. Discrete interruptions of fibres from theright hemisphere may deprive the damaged lefthemisphere of some form of aid, thereby causingapraxia. That the right hemisphere is in some

regions of the left hemisphere? 125G A
<-<37 54
G R
37sc. 20
S F A R
13 25 30 59sc. 16 Li.35 Sc. 15 I.i.32
CS L
2
I.i. 121 sc. 7
I.i. 47 sc. 18 Ii. 24
N S
55 44 60I.i. 31 sc. 20 I.i. 25
G F
44 55sc. 15 I.i. 21
MG
38 60sc. 14 1.1.30
E Superficial lesion
Fig 6 Locus, extent, and anteroposterior diameter of brain lesions in six patients without (upper diagram)and six patients with (lower diagram) ideomotor apraxia. Maps reconstructed from CAT scans. sc=apraxiascore, li=length of illness in days.
measure involved in eupraxia is supported by thefindings of von Monakov1 and Morlaas"8 as wellas by the more recent work of Dee et al9and De Renxi et al."6 It may be that what iscritical for apraxia is not so much the localisationof the bulk of the lesions as of a portion of it(which could be tiny) that disrupts midcallosalfibres. Our plotting could yield little informationon such minute but critical damage and on howit is related to the presence or absence of ideo-motor apraxia. In our prospective study, whichincludeF right hemisphere-damaged patients anduses a more suitable CAT scan a.pproach (for
example, frontal cuts), we are considering therelative importance of remaining sound todamaged parenchyma.
3. Ideomotor apraxia may be the consequenceof some sort of "mass action" on Lashley'slines,20 in which case only massive left hemispherelesions would be expected to give rise to apraxia.lesions large enough to deprive the lefthemisphere of sufficient healthy tissue to over-come the outcome of the massive lesion.1 HIow-ever, the data in fig 5 do not support thishypothesis, alt-hough there is some evidence for a
sc. 20 I.. 177 sc. 20
CA
116 32sc. 20 I.. 38
sc. 4
0 Deep lesion
Is ideomotor apraxia the outcome ofOG
11 40
damage to well-definedmu
14 26 28 44
126
correlation between large lesions and ideomotorapraxia. Against this, some of our patients hadextremely small lesions and yet their apraxiawas consistently apparent throughout the 12month period of observation.A future task of neuropsychological research
may well be the singling out of the abilities thatdepend strictly on a given region of the brainfrom those with broader and less constantanatomical ties. This differentiation might helpto explain why it is that after some lesions, suchas left temporal lesions, function is slowly andonly partially regained while after others, such asright carrefour lesions, function can be takenover by ipsilateral contralateral structures orboth within a few days. The fact remains that alarge number of stroke patients are permanentlyincapacitated and that so far no anatomicalpeculiarity, apart from bilateral lesions, canexplain why.
We are grateful to Mr Ettore Manacorda whodesigned the illustrations. This work was sup-ported by a grant from the Consiglio Nazionaledelle Ricerche.
References
1 von Monakov C. Die Lokalisation im Grosshirnund der Abbau der Funktion durch kortikaleHerde. Wiesbaden: JF Bergmann, 1914.
2 Brun R. Klinische und anatomische Studien uberA praxie. Zurich: Arbeit des HirnanatomischenInstitut, 1922.
3 Liepmann H. Die linke Hemisphaere und dasHandeln. Munchener medizinische Wochen-schrift 1905; 52:2322-6 and 2375-8.
4 Liepmann H. Der weitere Krankheitsverlauf beidem einseitig Apraktischem und der Gehirnbe-fund auf Grund von Serienschnitten. Monats-schrift fIur Psychiatrie und Neurologie 1906;19:217-43.
5 Niessxl von Mayendorf E. Die Diagnose aufErkrankung der linken Gyrusangularis. Monats-
A Basso, C Luzzatti, and H Spinnier
schrift fiir Psychiatrie und Neurologie 1907;22:145-57 and 225-64.
6 Heilbronner K. Die aphasischen, apraktischenund agnostischen Storungen. In: Handbuch derNeurologie, vol 1. Berlin: Springer, 1910; 982-1093.
7 Ajuriaguerra J, Hdcaen H, Angelergues E. Lesapraxies, varietes cliniques et lateralisationlesionelle. Revue Neurologique 1960; 102:499-566.
8 Heilman KM, Coyle JM, Gonyea EF, GeschwindN. Apraxia and agraphia in a left-hander. Brain1973; 96:21-8.
9 Geschwind N. The apraxias: neural mechanismsof disorders of learned movements. A mericanScientist 1975; 63:188-95.
10 De Renzi E, Faglioni P. Normative data andscreening power of a shortened version of theToken Test. Cortex 1978; 14:41-9.
11 De Renzi E, Pieczuro A, Vignolo LA. Ideationalapraxia: a quantitative study. Neuropsychologia1968; 6:41-52.
12 Luzzatti C, Scotti G, Gettoni A. Further sugges-tions for cerebral CT-localization. Cortex 1979;in press.
13 Basso A, Salvolini U, Vignolo LA. La localizze-zione dei sintomiafasici: prime experienze conl'Emi-scanner. Rivista di Patologia Nervosa eMentale 1979; in press.
14 Faglioni P. Aprassia: In: NeuropsicologiaClinica, Milano: Franco Angeli, 1977: 67-135.
15 Kimura D. Neuromotor mechanisms in the evo-lution of human communication. University ofWestern Ontario, Department of Psychology,Research Bulletin 1978; 454.
16 De Renzi E, Motti F, Nichelli P. Imitating ges-tures: a quantitative approach to ideomotorapraxia. Arch Neurol 1980; in press.
17 Kimura D, Archibald Y. Motor functions of theleft hemisphere. Brain 1974; 97:337-50.
18 Morlaas J. Contribution a' l'etude de l'apraxie.These de Paris, 1928.
19 Dee HL, Benton AL, Van Allen MW. Apraxiain relation to hemispheric locus of lesion andaphasia. Transactions of the American Neuro-logical Association 1970; 95:147-50.
20 Lashley KS. Brain Mechanisms and Intelligence.Chicago: University of Chicago Press, 1929.
Related Documents











