of June 26, 2018. This information is current as Fibrosis Lung Disease Infection in Cystic Pseudomonas aeruginosa Suppressor Cells: Implications for Flagellin Induces Myeloid-Derived Kormann and Dominik Hartl Hogardt, Gerd Döring, Joachim Riethmüller, Michael Jörg Fuchs, Rupert Handgretinger, Martin Stern, Michael Davide Neri, Andreas Wirth, Lauren Mays, Sabine Zundel, Graepler-Mainka, Michael Ost, Iris Schäfer, Irene Wecker, Nikolaus Rieber, Alina Brand, Andreas Hector, Ute http://www.jimmunol.org/content/190/3/1276 doi: 10.4049/jimmunol.1202144 December 2012; 2013; 190:1276-1284; Prepublished online 31 J Immunol Material Supplementary 4.DC1 http://www.jimmunol.org/content/suppl/2013/01/04/jimmunol.120214 References http://www.jimmunol.org/content/190/3/1276.full#ref-list-1 , 15 of which you can access for free at: cites 50 articles This article average * 4 weeks from acceptance to publication Fast Publication! • Every submission reviewed by practicing scientists No Triage! • from submission to initial decision Rapid Reviews! 30 days* • Submit online. ? The JI Why Subscription http://jimmunol.org/subscription is online at: The Journal of Immunology Information about subscribing to Permissions http://www.aai.org/About/Publications/JI/copyright.html Submit copyright permission requests at: Email Alerts http://jimmunol.org/alerts Receive free email-alerts when new articles cite this article. Sign up at: Print ISSN: 0022-1767 Online ISSN: 1550-6606. Immunologists, Inc. All rights reserved. Copyright © 2013 by The American Association of 1451 Rockville Pike, Suite 650, Rockville, MD 20852 The American Association of Immunologists, Inc., is published twice each month by The Journal of Immunology by guest on June 26, 2018 http://www.jimmunol.org/ Downloaded from by guest on June 26, 2018 http://www.jimmunol.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

of June 26, 2018.This information is current as
Fibrosis Lung Disease Infection in CysticPseudomonas aeruginosa
Suppressor Cells: Implications for Flagellin Induces Myeloid-Derived
Kormann and Dominik HartlHogardt, Gerd Döring, Joachim Riethmüller, MichaelJörg Fuchs, Rupert Handgretinger, Martin Stern, Michael Davide Neri, Andreas Wirth, Lauren Mays, Sabine Zundel,Graepler-Mainka, Michael Ost, Iris Schäfer, Irene Wecker, Nikolaus Rieber, Alina Brand, Andreas Hector, Ute
http://www.jimmunol.org/content/190/3/1276doi: 10.4049/jimmunol.1202144December 2012;
2013; 190:1276-1284; Prepublished online 31J Immunol
MaterialSupplementary
4.DC1http://www.jimmunol.org/content/suppl/2013/01/04/jimmunol.120214
Referenceshttp://www.jimmunol.org/content/190/3/1276.full#ref-list-1
, 15 of which you can access for free at: cites 50 articlesThis article
average*
4 weeks from acceptance to publicationFast Publication! •
Every submission reviewed by practicing scientistsNo Triage! •
from submission to initial decisionRapid Reviews! 30 days* •
Submit online. ?The JIWhy
Subscriptionhttp://jimmunol.org/subscription
is online at: The Journal of ImmunologyInformation about subscribing to
Permissionshttp://www.aai.org/About/Publications/JI/copyright.htmlSubmit copyright permission requests at:
Email Alertshttp://jimmunol.org/alertsReceive free email-alerts when new articles cite this article. Sign up at:
Print ISSN: 0022-1767 Online ISSN: 1550-6606. Immunologists, Inc. All rights reserved.Copyright © 2013 by The American Association of1451 Rockville Pike, Suite 650, Rockville, MD 20852The American Association of Immunologists, Inc.,
is published twice each month byThe Journal of Immunology
by guest on June 26, 2018http://w
ww
.jimm
unol.org/D
ownloaded from
by guest on June 26, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from
The Journal of Immunology
Flagellin Induces Myeloid-Derived Suppressor Cells:Implications for Pseudomonas aeruginosa Infection in CysticFibrosis Lung Disease
Nikolaus Rieber,* Alina Brand,* Andreas Hector,* Ute Graepler-Mainka,*
Michael Ost,* Iris Schafer,* Irene Wecker,* Davide Neri,* Andreas Wirth,*
Lauren Mays,* Sabine Zundel,† Jorg Fuchs,† Rupert Handgretinger,* Martin Stern,*
Michael Hogardt,‡ Gerd Doring,x Joachim Riethmuller,* Michael Kormann,*,1 and
Dominik Hartl*,1
Pseudomonas aeruginosa persists in patients with cystic fibrosis (CF) and drives CF lung disease progression. P. aeruginosa
potently activates the innate immune system, mainly mediated through pathogen-associated molecular patterns, such as flagellin.
However, the host is unable to eradicate this flagellated bacterium efficiently. The underlying immunological mechanisms are
incompletely understood. Myeloid-derived suppressor cells (MDSCs) are innate immune cells generated in cancer and proin-
flammatory microenvironments and are capable of suppressing T cell responses. We hypothesized that P. aeruginosa induces
MDSCs to escape T cell immunity. In this article, we demonstrate that granulocytic MDSCs accumulate in CF patients chronically
infected with P. aeruginosa and correlate with CF lung disease activity. Flagellated P. aeruginosa culture supernatants induced the
generation of MDSCs, an effect that was 1) dose-dependently mimicked by purified flagellin protein, 2) significantly reduced using
flagellin-deficient P. aeruginosa bacteria, and 3) corresponded to TLR5 expression on MDSCs in vitro and in vivo. Both purified
flagellin and flagellated P. aeruginosa induced an MDSC phenotype distinct from that of the previously described MDSC-inducing
cytokine GM-CSF, characterized by an upregulation of the chemokine receptor CXCR4 on the surface of MDSCs. Functionally,
P. aeruginosa–infected CF patient ex vivo–isolated as well as flagellin or P. aeruginosa in vitro–generated MDSCs efficiently
suppressed polyclonal T cell proliferation in a dose-dependent manner and modulated Th17 responses. These studies demonstrate
that flagellin induces the generation of MDSCs and suggest that P. aeruginosa uses this mechanism to undermine T cell–mediated
host defense in CF and other P. aeruginosa–associated chronic lung diseases. The Journal of Immunology, 2013, 190: 1276–1284.
Pseudomonas aeruginosa, a gram-negative flagellated bac-terium, acts as opportunistic pathogen in immunocompro-mised hosts or compartments in which the local host
defense is impaired. P. aeruginosa potently activates the innate armof the immune system, an effect mainly mediated through pathogen-associated molecular patterns (PAMPs) and pattern recognitionreceptors. Among those, the TLR 5 ligand flagellin was found to play
a key role in the recognition of P. aeruginosa (1–5). However,patients with chronic lung diseases, prototypically cystic fibrosis(CF) patients (6), are unable to eradicate the bacterium efficiently.The underlying immunological mechanisms are poorly understood.P. aeruginosa is known to suppress T cell responses in vivo,
and lymphocytes isolated from P. aeruginosa–infected CF patientsshow a blunted T cell proliferation capability ex vivo (7, 8). Beyonddirect effects of P. aeruginosa on T cells (7, 8), this flagellatedbacterium activates TLR5 on innate myeloid cells. Myeloid-derivedsuppressor cells (MDSCs) represent a novel innate immune cellsubset generated in tumor, infective, and proinflammatory micro-environments (9, 10). These specialized innate immune cells arecharacterized by their capacity to suppress T cell responses andthereby modulate the cellular arm of adaptive immunity (10). Con-sequently, MDSCs are considered a key intermediary in balancinginnate and adaptive immune responses, particularly under chronicdisease conditions. In mice, in which MDSCs have been studiedextensively, these cells constitute both a neutrophilic and a mono-cytic MDSC subphenotype (10–12); studies on MDSCs in humandisease conditions are scarce. Recent evidence suggests that neu-trophilic MDSCs accumulate in malignancy and systemic inflam-mation and are capable of suppressing T cell responses (13–15), buttheir role in host–pathogen interactions is, so far, poorly understood.On the basis of the fact that CF patients are unable to eradicate
P. aeruginosa infections and show impaired T cell proliferation, wehypothesized that P. aeruginosa induces MDSCs to escape T cellimmunity. Our studies demonstrate that neutrophilic MDSCs areinduced in P. aeruginosa–infected CF patients and correlate with
*Department of Pediatrics I, University of Tubingen, Tubingen, 72076 Germany;†Department of Pediatric Surgery, University of Tubingen, Tubingen, 72076 Ger-many; ‡Institute of Medical Microbiology and Hygiene, University of Frankfurt,Frankfurt, 60486 Germany; and xInstitute of Medical Microbiology and Hygiene,University of Tubingen, Tubingen, 72076 Germany
1M.K. and D.H. contributed equally to this work.
Received for publication August 3, 2012. Accepted for publication November 27,2012.
This work was supported by the German Research Foundation, Emmy Noether Pro-gramme HA 5274/3-1, the German Society of Pediatric Pneumonology, Praventions-und Informationsnetzwerk Allergie/Asthma, the Novartis Foundation, and the Ernest-Solvay-Foundation (all to D.H.).
Address correspondence and reprint requests to Dr. Nikolaus Rieber and Prof. Dr.Dominik Hartl, Department of Pediatrics I, University Hospital Tubingen, Hoppe-Seyler-Strasse 1, Tubingen, 72076 Germany. E-mail addresses: [email protected] (N.R.) and [email protected] (D.H.)
The online version of this article contains supplemental material.
Abbreviations used in this article: CF, cystic fibrosis; CFTR, cystic fibrosis trans-membrane conductance regulator; FEV1, forced expiratory volume in 1 s; MDSC,myeloid-derived suppressor cell; MEF25, maximum expiratory flow rate at 25% ofvital capacity; PAMP, pathogen-associated molecular pattern.
Copyright� 2013 by TheAmericanAssociation of Immunologists, Inc. 0022-1767/13/$16.00
www.jimmunol.org/cgi/doi/10.4049/jimmunol.1202144
by guest on June 26, 2018http://w
ww
.jimm
unol.org/D
ownloaded from
pulmonary disease. Flagellated P. aeruginosa culture supernatants aswell as purified flagellin dose-dependently and efficiently inducedMDSC generation, corresponding to TLR5 expression on MDSCs.Functionally, both CF patient–isolated and flagellin-induced MDSCssuppressed T cell proliferation and modulated Th17 cells, as keyantibacterial T cell populations in CF. This study highlights a novelmechanism by which the flagellated bacterium P. aeruginosa subvertshost defense by inducing T cell–suppressive MDSCs. Given the well-documented role of this cell type in immune regulation, MDSCscould therefore represent a novel therapeutic target in CF and otherdiseases characterized by infections with flagellated bacteria.
Materials and MethodsStudy subjects
The study was conducted at the University Children’s Hospital Tubingen(Tubingen, Germany). MDSCs were analyzed in the peripheral blood ofpatients with CF (n = 75) and age-matched pediatric non-CF controlsubjects without infections, malignancies, or inflammation (n = 37) (TableI). Informed written consent was obtained from all subjects included in thestudy or their legal representatives, and all study methods were approvedby the local ethics committee. Inclusion criteria were the diagnosis of CFby clinical symptoms and positive sweat tests (sweat Cl2 concentration. 60mmol/l) or disease-causing mutations in the cystic fibrosis transmembraneconductance regulator (CFTR) gene. Chronic P. aeruginosa infection wasdiagnosed if the organism was isolated in at least two consecutive sputumsamples with a minimum interval of 6 mo. For lung function analyses,forced expiratory volume in 1 s (FEV1) and maximum expiratory flow rateat 25% of vital capacity (MEF25) were acquired and calculated. For thenon–lung disease control group, samples were taken from children beforethey underwent elective surgery for multiple diagnoses. At the time ofblood sampling, all control subjects were without any signs of infection,inflammation, or respiratory symptoms.
Cell isolation and flow cytometry
PBMCs were prepared from blood samples by Ficoll density gradient sed-imentation (Lymphocyte Separation Medium; Biochrom) and washed twice
in RPMI 1640 medium. Trypan blue staining solution at 0.5% differentiatedbetween viable and nonviable cells and showed viability of .90% for allcells used in this study. After Ficoll density gradient sedimentation, MDSCswere characterized as CD33highCD66bhighIL-4RainterHLA-DRdim neutro-philic cells in the PBMC fraction, according to previously established hu-man MDSC analysis methods (13, 15) (Fig. 1). For MDSC isolation, cellswere obtained from the PBMC fraction and labeled with anti–CD66b-FITC,followed by two sequential anti-FITC magnetic bead separation steps(Miltenyi Biotec), per the manufacturer’s protocol. Purity of CD66b+ cellsafter separation was .95%, as assessed by flow cytometry. Morphology ofthe cells (MDSCs and conventional neutrophils isolated from healthy con-trol individuals) was performed by staining of cytospins. Isolated MDSCsshowed typical morphological characteristics of neutrophils, marking themas neutrophilic MDSCs (see supplementary material). For cytospin stain-ings, 5 3 104 cells were centrifuged in a Cytospin 3 Centrifuge (Shandon)at 800 rpm for 15 min and stained after with May–Grunwald–Giemsa. Absagainst CD3, CD4, CD8, CD14, CD16, CD66b, HLA-DR, and CD124 (IL-4Ra) were purchased from BD Pharmingen. Abs against CD11b and CD33were purchased from Miltenyi Biotec. Anti-human CXCR4 (clone 12G5)was obtained from eBioscience (San Diego, CA). Abs against TLR5 werepurchased from Santa Cruz Biotechnology. Mouse IgG1-FITC, Mouse IgM-FITC, Mouse IgG1-PE, and Mouse IgG1-APC (BD Pharmingen) were usedas isotype controls. Results were expressed as percent of positive cells andmean fluorescence intensity. Calculations were performed with BD Cell-Quest analysis software. For Th17 cell staining, 2.5 3 106 PBMCs werestimulated overnight with 10 ng/ml PMA and 1 mg/ml ionomycin (Sigma-Aldrich, St Louis, MO) in the presence of GolgiPlug (BD Biosciences, SanJose, CA). After cell surface staining with PE-conjugated anti-CD4(eBioscience), cells were fixed and permeabilized (Cytofix/Cytoperm;BD Biosciences) and stained with Alexa Fluor 647–conjugated anti–IL-17A (eBioscience). As a control for cellular activation and intracellularstaining, CD4+ T cells were also evaluated for IFN-g production (FITC–conjugated; eBioscience). For all in vitro FACS assays, three independentexperiments were performed.
In vitro generation and isolation of human MDSCs
HumanMDSCs were generated in vitro according to a previously publishedprotocol (16). Isolated human PBMCs were cultured in 12-well flat-bottomplates (Corning) or 25-cm2 flasks (Greiner Bio-One) at 53 105 cells/ml incomplete medium for 6 d, and GM-CSF (10 ng/ml; Genzyme), P. aeruginosa
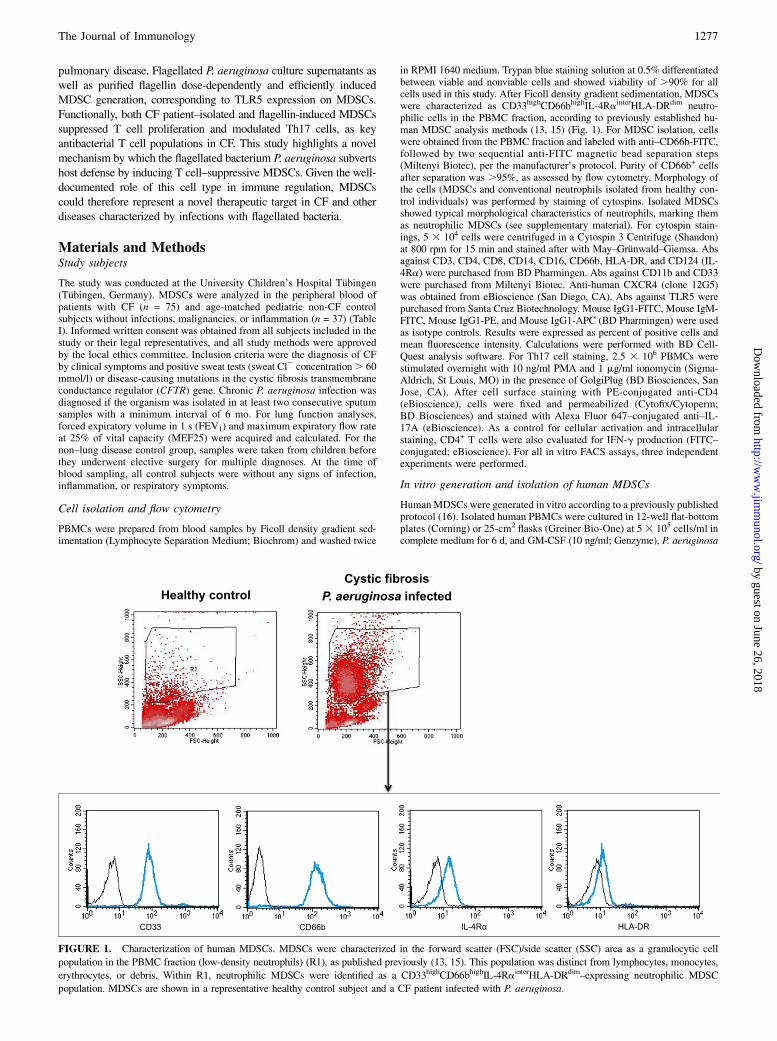
FIGURE 1. Characterization of human MDSCs. MDSCs were characterized in the forward scatter (FSC)/side scatter (SSC) area as a granulocytic cell
population in the PBMC fraction (low-density neutrophils) (R1), as published previously (13, 15). This population was distinct from lymphocytes, monocytes,
erythrocytes, or debris. Within R1, neutrophilic MDSCs were identified as a CD33highCD66bhighIL-4RainterHLA-DRdim–expressing neutrophilic MDSC
population. MDSCs are shown in a representative healthy control subject and a CF patient infected with P. aeruginosa.
The Journal of Immunology 1277
by guest on June 26, 2018http://w
ww
.jimm
unol.org/D
ownloaded from
culture supernatants (0.1–1%), flagellin (0.0001–0.1 mg/ml; Invivogen), orthe CFTR inhibitors CFTRinh-172 (10 mM; Tocris) or GlyH-101 (10 mM;Merck, Millipore) were added as indicated in the respective figures. Forall assays, at least three independent experiments were performed.P. aeruginosa culture supernatants were generated from two flagellated
(PAO1 and PA14) strains or from a flagellin-deficient (PAO1 fliM) strainaccording to standard protocols. PBMCs cultured in medium alone wererun in parallel as a control for each donor. Medium and supplements wererefreshed after 3 d. After 6 d, all cells were collected from PBMC cultures.Adherent cells were removed using the nonprotease cell detachment so-
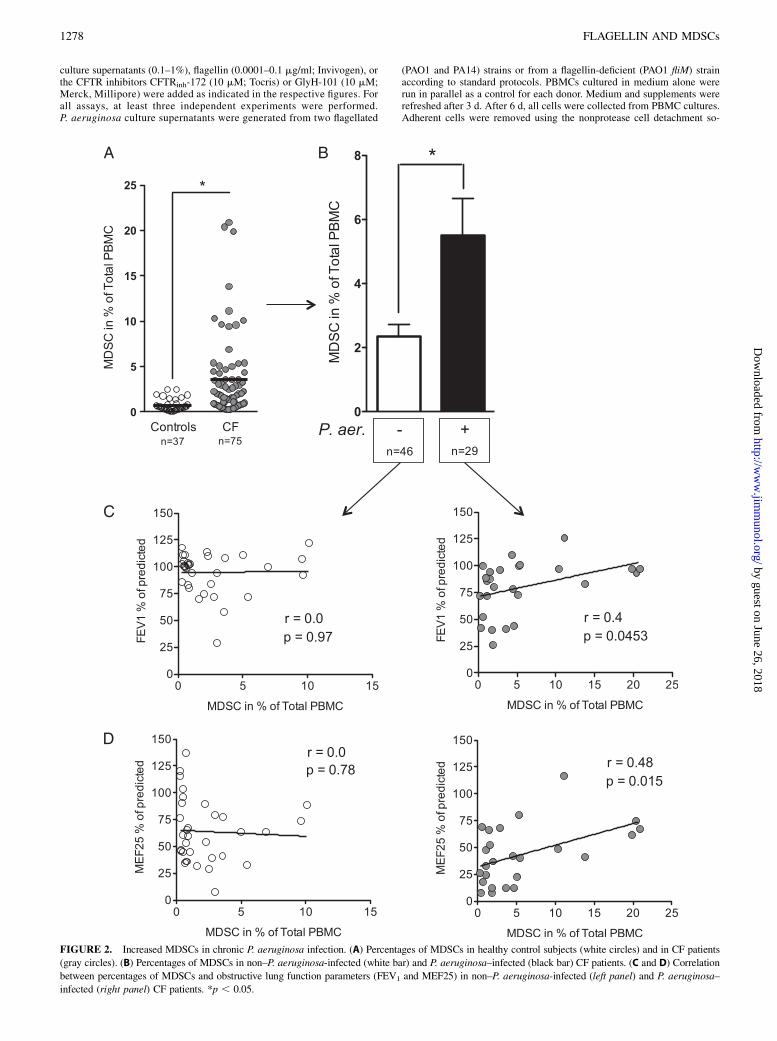
FIGURE 2. Increased MDSCs in chronic P. aeruginosa infection. (A) Percentages of MDSCs in healthy control subjects (white circles) and in CF patients
(gray circles). (B) Percentages of MDSCs in non–P. aeruginosa-infected (white bar) and P. aeruginosa–infected (black bar) CF patients. (C and D) Correlation
between percentages of MDSCs and obstructive lung function parameters (FEV1 and MEF25) in non–P. aeruginosa-infected (left panel) and P. aeruginosa–
infected (right panel) CF patients. *p , 0.05.
1278 FLAGELLIN AND MDSCs
by guest on June 26, 2018http://w
ww
.jimm
unol.org/D
ownloaded from

lution Detachin (Genlantis). CD33+ cells were isolated from each culture,using anti-CD33 magnetic microbeads and LS column separation (Milte-nyi Biotec) according to the manufacturer’s instructions. The purity ofisolated cell populations was .90% by flow cytometry.
T cell suppression assay
Responder PBMCs were obtained from healthy volunteers and stained withCFSE according to the manufacturer’s protocol (Invitrogen). PBMCs werestimulated with 100 U/ml IL-2 (R&D Systems) and 1 mg/ml OKT3(Janssen-Cilag). In a standardized way, 60,000 PBMCs per well in RPMI1640 (Biochrom) were seeded in a 96-well microtiter plate, and 10,000–30,000 MDSCs in RPMI 1640 or, as control, isolated conventional non-MDSC neutrophils in RPMI 1640 or RPMI1640 only was added. The cellculture was supplemented with 10% heat-inactivated human serum, 2 mMglutamine, 100 IU/ml penicillin, and 100 mg/ml streptomycin. After 96 hof incubation in a humidified atmosphere at 37˚C and 5% CO2, cells wereharvested and supernatants were frozen in 220˚C. CFSE-fluorescenceintensity was analyzed by flow cytometry to determine polyclonal T cellproliferation. For all assays, at least three independent experiments wereperformed. CD4 or CD8 T cells, respectively, were gated out for CFSEdilution after polyclonal stimulation. Only propidium iodide–negative cellswere considered for analysis. Where indicated (Supplemental Fig. 3),dose-dependent MDSC–T cell experiments were performed. Where indi-cated, the effect of CXCR4 inhibition, using the small-molecule inhibitorAMD3100 (2 mM; Sigma-Aldrich), on MDSC-mediated suppression ofCD4 and CD8 T cell proliferation was analyzed (Supplemental Fig. 2C).
Quantitative PCR
Quantitative RT-PCR was performed in MACS-isolated human MDSCs.mRNA was isolated with the NucleoSpin RNA II kit (Macherey & Nagel,Duren, Germany), cDNA was synthesized with the iScript AdvancedSynthesis Kit (Bio-Rad, Munich, Germany), and real-time RT-PCR wasperformed using the Power SYBR Green Master Mix (Applied Bio-systems, Darmstadt, Germany) and a ViiA7 Real-Time PCR cycler (Ap-plied Biosystems) according to the manufacturer’s protocols. Results werecalculated by the 2(2DDCT) method and are given as relative expression incomparison with the housekeeping gene b-actin. The following primerswere used:
G-CSF, forward: 59-TAGAGCAAGTGAGGAAGATCAGG-39,
reverse: 59-AGTTCTTCCATCTGCTGCCAGATG-39;
b-actin: forward: 59-CATGTACGTTGCTATCCAGGC-39,
reverse: 59-CTCCTTAATGTCACGCACGAT-39.
Cytokine analysis in culture supernatants
Multiplex cytokine array analysis in supernatants was performed usingthe Bio-Plex protein multiarray system (Bio-Plex Pro Human CytokineArray, Bio-Rad Laboratories). For the current experiments, a human 27-plexassay was used according to the recommendations of the manufacturer(Bio-Rad).
Statistical analysis
Statistical analysis was accomplished using GraphPad Prism 5.0 (GraphPadSoftware). Differences between the groups were determined by a Studentt test. A p value , 0.05 was considered significant.
ResultsNeutrophilic MDSCs accumulate in Pseudomonas aeruginosa–infected CF patients
We studied patients with CF lung disease, characterized byP. aeruginosa infections. In a large cross-sectional CF patient cohort,percentages of MDSCs (Fig. 1) were significantly increased com-pared with percentages in age-matched healthy control subjects (Fig.2A). This accumulation of MDSCs was not due to relative changesin peripheral blood mononuclear, polymorphonuclear cell counts, orband cells. Scatter plot analyses further revealed a high interpatientvariability, ranging fromMDSC percentages in CF patients similar tothose in control individuals (,1% of PBMCs) to CF patients with upto 20% MDSCs (of PBMCs gated), suggesting underlying disease-associated factors regulating MDSC generation in CF patients.
Patient stratification showed that, in particular, CF patientschronically infected with P. aeruginosa showed significantly in-creased MDSC percentages over those in CF patients withoutP. aeruginosa infection (Figs. 1, 2B). The majority of P. aeruginosa–infected CF patients had a nonmucoid Pseudomonas phenotype(86%), and percentages of MDSCs tended to be higher in CFpatients with nonmucoid than in patients with mucoid P. aerugi-nosa isolates (Supplemental Fig. 1A). Importantly, percentages ofMDSCs correlated positively with obstructive pulmonary functionparameters (FEV1: r = 0.4, p = 0.0045; MEF25: r = 0.48, p =0.015) in chronically P. aeruginosa–infected, but not in non–Pseudomonas-infected CF patients (Fig. 2C, 2D). Longitudinalfollow-up of individual CF patients indicated that percentages ofMDSCs increased in P. aeruginosa–infected, but not in non–P. aeruginosa–infected, conditions, and also suggested thatMDSCs correlate with lung function over time (Supplemental Fig.1B). No statistical association of antibiotics with MDSCs wasfound. Despite a substantial number of CF patients coinfected withP. aeruginosa and Staphylococcus aureus (15 of 29, see Table Ifor details), no statistical associations were found between MDSCpercentages and the detection of S. aureus or Aspergillus fumigatus,as other characteristic pathogens in CF lung disease, suggestingthat the accumulation of MDSCs in CF patients is not due to in-fection in general but indicates that P. aeruginosa–associated fac-tors induce MDSCs and thereby modulate lung disease severityin CF.
Flagellated Pseudomonas aeruginosa and purified flagellininduce CXCR4high MDSCs
To test our hypothesis that P. aeruginosa–derived factors, such asmicrobe-associated or shedded PAMPs (6), in CF patients drivethe generation of MDSCs, we first used P. aeruginosa culturesupernatants from two different P. aeruginosa strains and testedtheir capacity to induce MDSC generation in vitro. These studiesdemonstrated that P. aeruginosa culture supernatants harvestedfrom two different flagellated P. aeruginosa strains efficiently in-duced MDSCs to a similar extent as GM-CSF did, which is wellknown to induce MDSCs in this setting in vitro (16) (Fig. 3A).
Table I. CF patient and control group
Parameters Cystic Fibrosis Controls
N 75 37Age (y) 16 6 10 14 6 12Sex (m/f) 38/37 21/16WBC (109/l) 8 6 2 NDCRP (mg/dl) 0.41 6 0.76 NDFVC (% pred.) 98 6 18 ND.FEV1 (% pred.) 89 6 22 NDMEF25 (% pred.) 56 6 30 NDP. aeruginosaa 29 NDS. aureusb 49 NDP. aeruginosa/S. aureus coinfection 15Age P. aeruginosa 22 6 11Age S. aureus 16 6 9Age P. aeruginosa/S. aureus coinfection 21 6 11Antibiotics inhaled 35 NDAntibiotics systemic 14 NDdF508homozygous/heterozygous/other 29/31/15 ND
Results are expressed as means 6 SD.aP. aeruginosa bacteria isolated in at least two consecutive sputum samples or
throat swabs with a minimum interval of 6 mo.bS. aureus bacteria isolated in at least two consecutive sputum samples or throat
swabs with a minimum interval of 6 mo.% pred., % of predicted; CRP, C-reactive protein; f, female; FVC, forced vital
capacity; m, male.
The Journal of Immunology 1279
by guest on June 26, 2018http://w
ww
.jimm
unol.org/D
ownloaded from
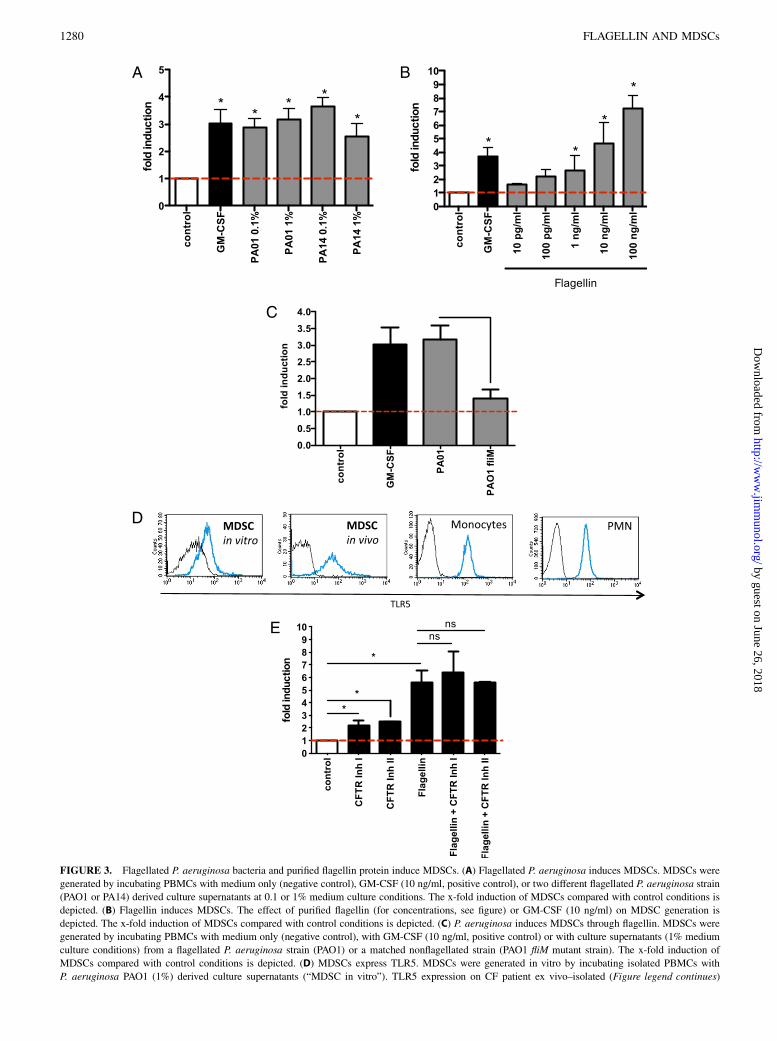
FIGURE 3. Flagellated P. aeruginosa bacteria and purified flagellin protein induce MDSCs. (A) Flagellated P. aeruginosa induces MDSCs. MDSCs were
generated by incubating PBMCs with medium only (negative control), GM-CSF (10 ng/ml, positive control), or two different flagellated P. aeruginosa strain
(PAO1 or PA14) derived culture supernatants at 0.1 or 1% medium culture conditions. The x-fold induction of MDSCs compared with control conditions is
depicted. (B) Flagellin induces MDSCs. The effect of purified flagellin (for concentrations, see figure) or GM-CSF (10 ng/ml) on MDSC generation is
depicted. The x-fold induction of MDSCs compared with control conditions is depicted. (C) P. aeruginosa induces MDSCs through flagellin. MDSCs were
generated by incubating PBMCs with medium only (negative control), with GM-CSF (10 ng/ml, positive control) or with culture supernatants (1% medium
culture conditions) from a flagellated P. aeruginosa strain (PAO1) or a matched nonflagellated strain (PAO1 fliM mutant strain). The x-fold induction of
MDSCs compared with control conditions is depicted. (D) MDSCs express TLR5. MDSCs were generated in vitro by incubating isolated PBMCs with
P. aeruginosa PAO1 (1%) derived culture supernatants (“MDSC in vitro”). TLR5 expression on CF patient ex vivo–isolated (Figure legend continues)
1280 FLAGELLIN AND MDSCs
by guest on June 26, 2018http://w
ww
.jimm
unol.org/D
ownloaded from

To dissect which mechanism(s) induce(s) MDSCs in chronicP. aeruginosa infection, we focused on flagellin because 1) infec-tion with flagellated P. aeruginosa was associated with MDSCinduction in our CF patient cohort, whereas nonflagellated mi-crobes did not show any association with MDSCs in vivo; and 2)previous studies showed that among different PAMPs, flagel-lin recognition through TLR5 in particular plays a key role inleukocyte–P. aeruginosa interactions in CF lung disease (4, 5, 17, 18).Our studies demonstrated that flagellin efficiently and dose-depen-dently induced MDSCs with a more potent capacity than GM-CSFdid (Fig. 3B). Further studies also showed that flagellin upregulatedG-CSF, but had no effect on GM-CSF expression in MDSCs(Supplemental Fig. 2A and data not shown). P. aeruginosa–inducedMDSC generation was significantly reduced using a flagellin-defi-cient P. aeruginosa strain (Fig. 3C). Because flagellin acts mainlythrough TLR5, we analyzed TLR5 surface expression on MDSCsand found that both in vitro–generated and P. aeruginosa CF patientin vivo/ex vivo isolated MDSCs expressed TLR5 (Fig. 3D). To as-sess the effect of the CFTR in MDSC generation, we used a small-molecule CFTR inhibitor. These studies demonstrated that CFTRinhibition slightly increased the generation of MDSCs but had nosignificant effect on flagellin-induced MDSC generation (Fig. 3E).These findings were not due to toxic or proapoptotic effects of theCFTR inhibitor and could be reproduced using a second dif-ferent CFTR inhibitor (Fig. 3E).Next, we characterized the immunological phenotype of
P. aeruginosa– and flagellin-induced MDSCs compared with canon-ical GM-CSF–induced MDSCs. These studies demonstrated that bothflagellated P. aeruginosa bacteria and purified flagellin protein upre-gulated surface expression levels of the homeostatic chemokine re-ceptor and HIV coreceptor CXCR4 on MDSCs, whereas GM-CSFtreatment had no significant effect on the expression of these surfaceproteins (Fig. 4). When viewed in combination, these studies indi-cate that flagellated P. aeruginosa strains and purified flagellinprotein potently induce MDSCs with a distinct CXCR4high MDSCphenotype.
Flagellin-induced MDSCs functionally suppress T cellproliferation ex vivo and in vitro
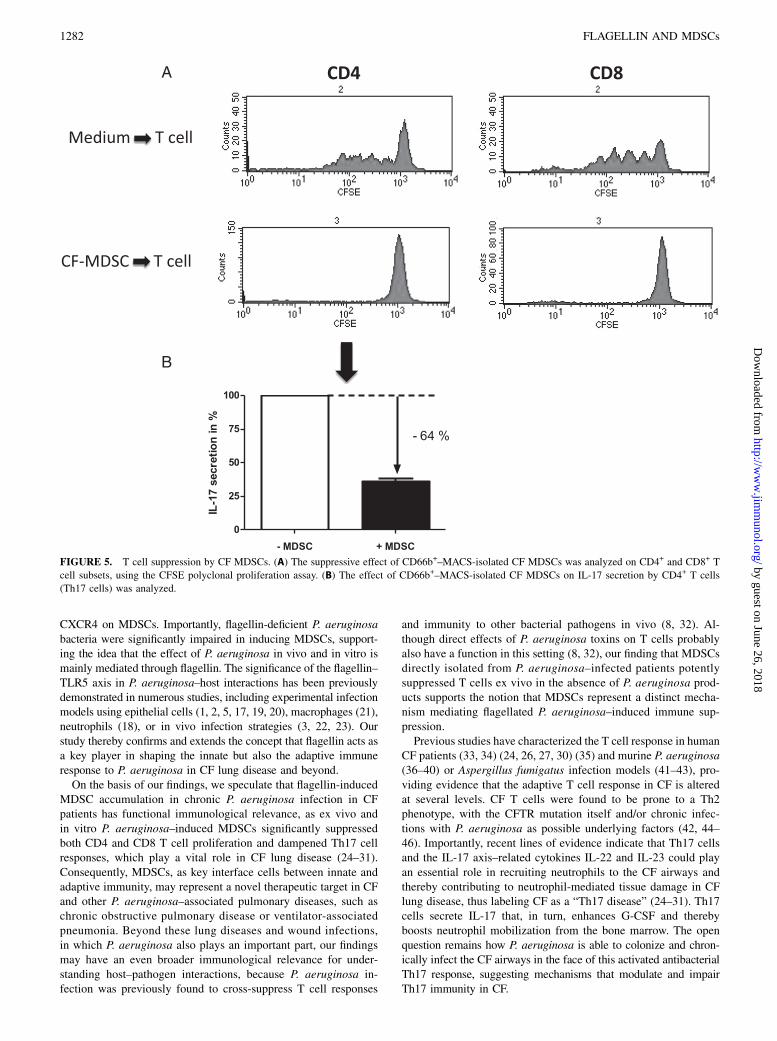
To assess the functional capacities of flagellated P. aeruginosa–induced phenotypic MDSCs and to corroborate their role as aT cell suppressive cell type, we isolated MDSCs from P. aeruginosa–infected CF patients, using gradient centrifugation and sequentialmagnetic bead isolation, and studied MDSC–T cell interactions exvivo. These studies using T cell CFSE labeling demonstrated thatP. aeruginosa–infected CF patient–derived MDSCs efficientlysuppressed polyclonal T cell proliferation of both CD4+ and CD8+
T cell subsets in a dose-dependent fashion (Fig. 5A, SupplementalFig. 2B). As flagellin induced CXCR4high MDSCs, we investi-gated whether inhibiting CXCR4 functionality using the small-molecule inhibitor AMD3100 has an effect on MDSC-mediatedT cell suppression. These studies showed that CXCR4 inhibition hadno effect on MDSC-mediated T cell suppression (SupplementalFig. 2C).Because IL-17–producing T cells have been previously de-
scribed as playing a pivotal role in the pathogenesis of chronicinfective CF lung disease, we investigated whether CF-isolatedMDSCs are capable of modulating IL-17 protein production by
CD4+ T cells. These studies demonstrated that MDSCs derivedfrom P. aeruginosa–infected CF patients substantially dampenedreleased IL-17 protein (64% reduction of IL-17 protein) (Fig. 5B).These findings on IL-17 cytokine production, quantified in cellculture supernatants, were confirmed by intracellular flow cytom-etry stainings, showing that MDSCs suppressed IL-17 protein ex-pression in T cells (Supplemental Fig. 2D). In addition to IL-17,MDSCs had an effect on several other cytokines, chemokines, andgrowth factors, as analyzed by a high-throughput bioplex array(Supplemental Fig. 3).Finally, we investigated whether P. aeruginosa– or flagellin-
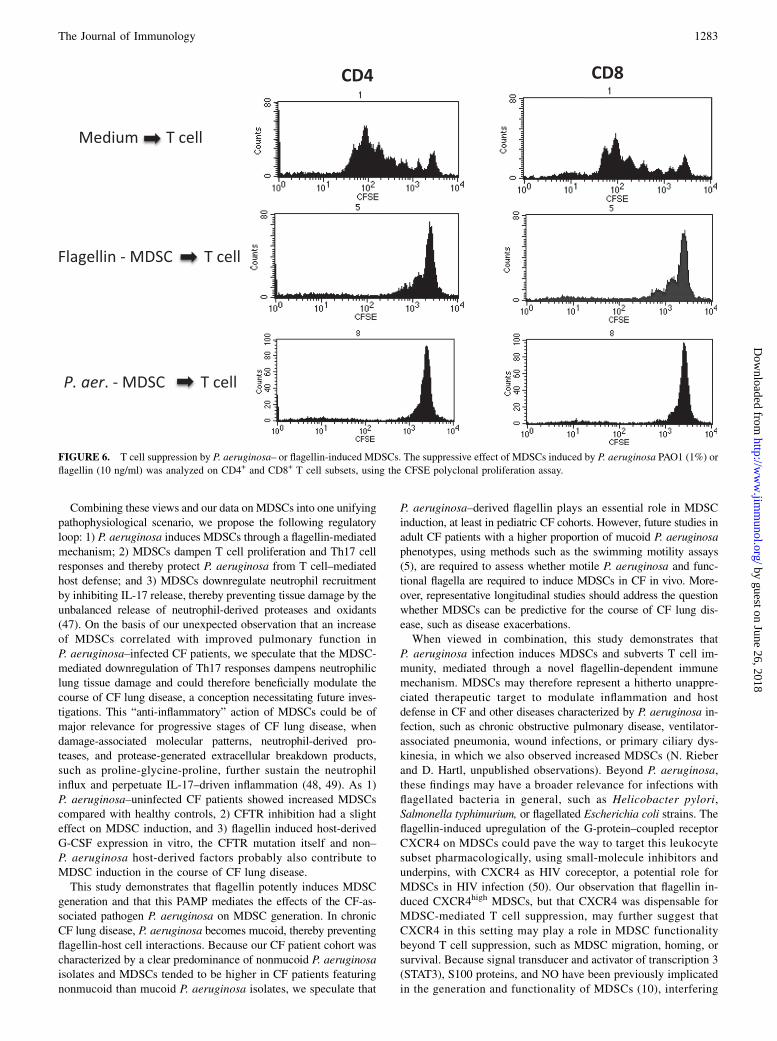
induced MDSCs feature a similar T cell–suppressive phenotype.These studies showed that flagellated P. aeruginosa–or purifiedflagellin-induced MDSCs mimicked the T cell–suppressive char-acteristics of CF patient ex vivo–isolated MDSCs in potentlysuppressing both CD4 and CD8 T cell proliferation (Fig. 6). Whenviewed in combination, these studies demonstrate that both exvivo CF patient–isolated and in vitro P. aeruginosa–/flagellin-induced MDSCs suppress CD4+ and CD8+ T cell proliferationand modulate Th17 responses.
DiscussionP. aeruginosa survives in immunocompromised individuals andpatients with chronic pulmonary diseases, such as CF, owing tothe inability of the host to clear this pathogen efficiently. However,the underlying immune mechanisms remain poorly understood(6). This study reveals a novel mechanism by which flagellatedP. aeruginosa bacteria subvert the host defense by inducingT cell–suppressive MDSCs. MDSCs could therefore representa novel therapeutic target in CF and other diseases characterizedby infections with P. aeruginosa or other flagellated bacteria.MDSCs represent an innate immune cell subset that efficiently
controls adaptive T cell inflammation (9, 10). Our studies provideevidence that granulocytic/neutrophilic MDSCs, regularly absent oronly marginally present in healthy control individuals, accumulatein P. aeruginosa–infected CF patients. We further show that flag-ellated P. aeruginosa bacteria or the purified TLR5 ligand flagellinpotently induces T cell–suppressive MDSCs and upregulates
MDSCs (“MDSC ex vivo”). As control immune cells, peripheral blood monocytes and neutrophils (PMNs) were stained for TLR5. TLR5 surface ex-
pression (blue line) versus unstained control (black line) is shown. (E) MDSC induction and CFTR. MDSCs were generated in vitro by incubating
isolated PBMCs with purified flagellin (10 ng/ml), with or without pretreatment of PBMCs with two different small-molecule CFTR inhibitors (CFTRinh-
172, 10mM; GlyH-101, 10mM). For all assays, at least three independent experiments were performed. *p , 0.05. ns, Not significant.
FIGURE 4. P. aeruginosa and flagellin upregulate CXCR4 expression on
MDSCs. CXCR4 surface expression levels were quantified on GM-CSF, P.
aeruginosa PAO1 (1%), or flagellin (10 ng/ml) in vitro–generated MDSCs.
For all assays, three independent experiments were performed. Where in-
dicated, the small-molecule CFTR inhibitor CFTRinh-172 (10 mM) was
used. *p , 0.05.
The Journal of Immunology 1281
by guest on June 26, 2018http://w
ww
.jimm
unol.org/D
ownloaded from
CXCR4 on MDSCs. Importantly, flagellin-deficient P. aeruginosabacteria were significantly impaired in inducing MDSCs, support-ing the idea that the effect of P. aeruginosa in vivo and in vitro ismainly mediated through flagellin. The significance of the flagellin–TLR5 axis in P. aeruginosa–host interactions has been previouslydemonstrated in numerous studies, including experimental infectionmodels using epithelial cells (1, 2, 5, 17, 19, 20), macrophages (21),neutrophils (18), or in vivo infection strategies (3, 22, 23). Ourstudy thereby confirms and extends the concept that flagellin acts asa key player in shaping the innate but also the adaptive immuneresponse to P. aeruginosa in CF lung disease and beyond.On the basis of our findings, we speculate that flagellin-induced
MDSC accumulation in chronic P. aeruginosa infection in CFpatients has functional immunological relevance, as ex vivo andin vitro P. aeruginosa–induced MDSCs significantly suppressedboth CD4 and CD8 T cell proliferation and dampened Th17 cellresponses, which play a vital role in CF lung disease (24–31).Consequently, MDSCs, as key interface cells between innate andadaptive immunity, may represent a novel therapeutic target in CFand other P. aeruginosa–associated pulmonary diseases, such aschronic obstructive pulmonary disease or ventilator-associatedpneumonia. Beyond these lung diseases and wound infections,in which P. aeruginosa also plays an important part, our findingsmay have an even broader immunological relevance for under-standing host–pathogen interactions, because P. aeruginosa in-fection was previously found to cross-suppress T cell responses
and immunity to other bacterial pathogens in vivo (8, 32). Al-though direct effects of P. aeruginosa toxins on T cells probablyalso have a function in this setting (8, 32), our finding that MDSCsdirectly isolated from P. aeruginosa–infected patients potentlysuppressed T cells ex vivo in the absence of P. aeruginosa prod-ucts supports the notion that MDSCs represent a distinct mecha-nism mediating flagellated P. aeruginosa–induced immune sup-pression.Previous studies have characterized the T cell response in human
CF patients (33, 34) (24, 26, 27, 30) (35) and murine P. aeruginosa(36–40) or Aspergillus fumigatus infection models (41–43), pro-viding evidence that the adaptive T cell response in CF is alteredat several levels. CF T cells were found to be prone to a Th2phenotype, with the CFTR mutation itself and/or chronic infec-tions with P. aeruginosa as possible underlying factors (42, 44–46). Importantly, recent lines of evidence indicate that Th17 cellsand the IL-17 axis–related cytokines IL-22 and IL-23 could playan essential role in recruiting neutrophils to the CF airways andthereby contributing to neutrophil-mediated tissue damage in CFlung disease, thus labeling CF as a “Th17 disease” (24–31). Th17cells secrete IL-17 that, in turn, enhances G-CSF and therebyboosts neutrophil mobilization from the bone marrow. The openquestion remains how P. aeruginosa is able to colonize and chron-ically infect the CF airways in the face of this activated antibacterialTh17 response, suggesting mechanisms that modulate and impairTh17 immunity in CF.
FIGURE 5. T cell suppression by CF MDSCs. (A) The suppressive effect of CD66b+–MACS-isolated CF MDSCs was analyzed on CD4+ and CD8+ T
cell subsets, using the CFSE polyclonal proliferation assay. (B) The effect of CD66b+–MACS-isolated CF MDSCs on IL-17 secretion by CD4+ T cells
(Th17 cells) was analyzed.
1282 FLAGELLIN AND MDSCs
by guest on June 26, 2018http://w
ww
.jimm
unol.org/D
ownloaded from
Combining these views and our data on MDSCs into one unifyingpathophysiological scenario, we propose the following regulatoryloop: 1) P. aeruginosa induces MDSCs through a flagellin-mediatedmechanism; 2) MDSCs dampen T cell proliferation and Th17 cellresponses and thereby protect P. aeruginosa from T cell–mediatedhost defense; and 3) MDSCs downregulate neutrophil recruitmentby inhibiting IL-17 release, thereby preventing tissue damage by theunbalanced release of neutrophil-derived proteases and oxidants(47). On the basis of our unexpected observation that an increaseof MDSCs correlated with improved pulmonary function inP. aeruginosa–infected CF patients, we speculate that the MDSC-mediated downregulation of Th17 responses dampens neutrophiliclung tissue damage and could therefore beneficially modulate thecourse of CF lung disease, a conception necessitating future inves-tigations. This “anti-inflammatory” action of MDSCs could be ofmajor relevance for progressive stages of CF lung disease, whendamage-associated molecular patterns, neutrophil-derived pro-teases, and protease-generated extracellular breakdown products,such as proline-glycine-proline, further sustain the neutrophilinflux and perpetuate IL-17–driven inflammation (48, 49). As 1)P. aeruginosa–uninfected CF patients showed increased MDSCscompared with healthy controls, 2) CFTR inhibition had a slighteffect on MDSC induction, and 3) flagellin induced host-derivedG-CSF expression in vitro, the CFTR mutation itself and non–P. aeruginosa host-derived factors probably also contribute toMDSC induction in the course of CF lung disease.This study demonstrates that flagellin potently induces MDSC
generation and that this PAMP mediates the effects of the CF-as-sociated pathogen P. aeruginosa on MDSC generation. In chronicCF lung disease, P. aeruginosa becomes mucoid, thereby preventingflagellin-host cell interactions. Because our CF patient cohort wascharacterized by a clear predominance of nonmucoid P. aeruginosaisolates and MDSCs tended to be higher in CF patients featuringnonmucoid than mucoid P. aeruginosa isolates, we speculate that
P. aeruginosa–derived flagellin plays an essential role in MDSCinduction, at least in pediatric CF cohorts. However, future studies inadult CF patients with a higher proportion of mucoid P. aeruginosaphenotypes, using methods such as the swimming motility assays(5), are required to assess whether motile P. aeruginosa and func-tional flagella are required to induce MDSCs in CF in vivo. More-over, representative longitudinal studies should address the questionwhether MDSCs can be predictive for the course of CF lung dis-ease, such as disease exacerbations.When viewed in combination, this study demonstrates that
P. aeruginosa infection induces MDSCs and subverts T cell im-munity, mediated through a novel flagellin-dependent immunemechanism. MDSCs may therefore represent a hitherto unappre-ciated therapeutic target to modulate inflammation and hostdefense in CF and other diseases characterized by P. aeruginosa in-fection, such as chronic obstructive pulmonary disease, ventilator-associated pneumonia, wound infections, or primary ciliary dys-kinesia, in which we also observed increased MDSCs (N. Rieberand D. Hartl, unpublished observations). Beyond P. aeruginosa,these findings may have a broader relevance for infections withflagellated bacteria in general, such as Helicobacter pylori,Salmonella typhimurium, or flagellated Escherichia coli strains. Theflagellin-induced upregulation of the G-protein–coupled receptorCXCR4 on MDSCs could pave the way to target this leukocytesubset pharmacologically, using small-molecule inhibitors andunderpins, with CXCR4 as HIV coreceptor, a potential role forMDSCs in HIV infection (50). Our observation that flagellin in-duced CXCR4high MDSCs, but that CXCR4 was dispensable forMDSC-mediated T cell suppression, may further suggest thatCXCR4 in this setting may play a role in MDSC functionalitybeyond T cell suppression, such as MDSC migration, homing, orsurvival. Because signal transducer and activator of transcription 3(STAT3), S100 proteins, and NO have been previously implicatedin the generation and functionality of MDSCs (10), interfering
FIGURE 6. T cell suppression by P. aeruginosa– or flagellin-induced MDSCs. The suppressive effect of MDSCs induced by P. aeruginosa PAO1 (1%) or
flagellin (10 ng/ml) was analyzed on CD4+ and CD8+ T cell subsets, using the CFSE polyclonal proliferation assay.
The Journal of Immunology 1283
by guest on June 26, 2018http://w
ww
.jimm
unol.org/D
ownloaded from
with these pathways might represent a future therapeutic strategyin CF lung disease and other pathological conditions associatedwith flagellated bacteria
DisclosuresThe authors have no financial conflicts of interest.
References1. Zhang, Z., J. P. Louboutin, D. J. Weiner, J. B. Goldberg, and J. M. Wilson.
2005. Human airway epithelial cells sense Pseudomonas aeruginosa infectionvia recognition of flagellin by Toll-like receptor 5. Infect. Immun. 73: 7151–7160.
2. Hybiske, K., J. K. Ichikawa, V. Huang, S. J. Lory, and T. E. Machen. 2004.Cystic fibrosis airway epithelial cell polarity and bacterial flagellin determinehost response to Pseudomonas aeruginosa. Cell. Microbiol. 6: 49–63.
3. Morris, A. E., H. D. Liggitt, T. R. Hawn, and S. J. Skerrett. 2009. Role of Toll-like receptor 5 in the innate immune response to acute P. aeruginosa pneumonia.Am. J. Physiol. Lung Cell. Mol. Physiol. 297: L1112–L1119.
4. Blohmke, C. J., J. Park, A. F. Hirschfeld, R. E. Victor, J. Schneiderman,D. Stefanowicz, M. A. Chilvers, P. R. Durie, M. Corey, J. Zielenski, et al. 2010.TLR5 as an anti-inflammatory target and modifier gene in cystic fibrosis.J. Immunol. 185: 7731–7738.
5. Blohmke, C. J., R. E. Victor, A. F. Hirschfeld, I. M. Elias, D. G. Hancock,C. R. Lane, A. G. Davidson, P. G. Wilcox, K. D. Smith, J. Overhage, et al. 2008.Innate immunity mediated by TLR5 as a novel antiinflammatory target for cysticfibrosis lung disease. J. Immunol. 180: 7764–7773.
6. Cohen, T. S., and A. Prince. 2012. Cystic fibrosis: a mucosal immunodeficiencysyndrome. Nat. Med. 18: 509–519.
7. Sorensen, R. U., R. C. Stern, and S. H. Polmar. 1978. Lymphocyte responsive-ness to Pseudomonas aeruginosa in cystic fibrosis: relationship to status ofpulmonary disease in sibling pairs. J. Pediatr. 93: 201–205.
8. Sorensen, R. U., R. L. Waller, and J. D. Klinger. 1991. Cystic fibrosis. Infectionand immunity to Pseudomonas. Clin. Rev. Allergy 9: 47–74.
9. Youn, J. I., and D. I. Gabrilovich. 2010. The biology of myeloid-derived sup-pressor cells: the blessing and the curse of morphological and functional het-erogeneity. Eur. J. Immunol. 40: 2969–2975.
10. Gabrilovich, D. I., and S. Nagaraj. 2009. Myeloid-derived suppressor cells asregulators of the immune system. Nat. Rev. Immunol. 9: 162–174.
11. Ribechini, E., V. Greifenberg, S. Sandwick, and M. B. Lutz. 2010. Subsets,expansion and activation of myeloid-derived suppressor cells. Med. Microbiol.Immunol. (Berl.) 199: 273–281.
12. Gabrilovich, D. I., V. Bronte, S. H. Chen, M. P. Colombo, A. Ochoa, S. Ostrand-Rosenberg, and H. Schreiber. 2007. The terminology issue for myeloid-derivedsuppressor cells. Cancer Res. 67: 425, author reply 426.
13. Rodriguez, P. C., M. S. Ernstoff, C. P. Hernandez, M. Atkins, J. Zabaleta,R. A. Sierra, and A. C. Ochoa. 2009. Arginase I producing myeloid derivedsuppressor cells (MDSC) in renal cell carcinoma are a subpopulation of activatedgranulocytes. Cancer Res. 69: 1553–1560.
14. Pillay, J., V. M. Kamp, E. van Hoffen, T. Visser, T. Tak, J. W. Lammers,L. H. Ulfman, L. P. Leenen, P. Pickkers, and L. Koenderman. 2012. A subset ofneutrophils in human systemic inflammation inhibits T cell responses throughMac-1. J. Clin. Invest. 122: 327–336.
15. Brandau, S., S. Trellakis, K. Bruderek, D. Schmaltz, G. Steller, M. Elian,H. Suttmann, M. Schenck, J. Welling, P. Zabel, and S. Lang. 2011. Myeloid-derived suppressor cells in the peripheral blood of cancer patients containa subset of immature neutrophils with impaired migratory properties. J. Leukoc.Biol. 89: 311–317.
16. Lechner, M. G., D. J. Liebertz, and A. L. Epstein. 2010. Characterization ofcytokine-induced myeloid-derived suppressor cells from normal human periph-eral blood mononuclear cells. J. Immunol. 185: 2273–2284.
17. Adamo, R., S. Sokol, G. Soong, M. I. Gomez, and A. Prince. 2004. Pseudomonasaeruginosa flagella activate airway epithelial cells through asialoGM1 and toll-like receptor 2 as well as toll-like receptor 5. Am. J. Respir. Cell Mol. Biol. 30:627–634.
18. Koller, B., M. Kappler, P. Latzin, A. Gaggar, M. Schreiner, S. Takyar,M. Kormann, M. Kabesch, D. Roos, M. Griese, and D. Hartl. 2008. TLR ex-pression on neutrophils at the pulmonary site of infection: TLR1/TLR2-mediatedup-regulation of TLR5 expression in cystic fibrosis lung disease. J. Immunol.181: 2753–2763.
19. Tseng, J., J. Do, J. H. Widdicombe, and T. E. Machen. 2006. Innate immuneresponses of human tracheal epithelium to Pseudomonas aeruginosa flagellin,TNF-alpha, and IL-1beta. Am. J. Physiol. Cell Physiol. 290: C678–C690.
20. Pena, J., Z. Fu, C. Schwarzer, and T. E. Machen. 2009. Pseudomonas aeruginosainhibition of flagellin-activated NF-kappaB and interleukin-8 by human airwayepithelial cells. Infect. Immun. 77: 2857–2865.
21. Descamps, D., M. Le Gars, V. Balloy, D. Barbier, S. Maschalidi, M. Tohme,M. Chignard, R. Ramphal, B. Manoury, and J. M. Sallenave. 2012. Toll-likereceptor 5 (TLR5), IL-1b secretion, and asparagine endopeptidase are criticalfactors for alveolar macrophage phagocytosis and bacterial killing. Proc. Natl.Acad. Sci. USA 109: 1619–1624.
22. Ramphal, R., V. Balloy, J. Jyot, A. Verma, M. Si-Tahar, and M. Chignard. 2008.Control of Pseudomonas aeruginosa in the lung requires the recognition of ei-ther lipopolysaccharide or flagellin. J. Immunol. 181: 586–592.
23. Ben Mohamed, F., I. Garcia-Verdugo, M. Medina, V. Balloy, M. Chignard,R. Ramphal, and L. Touqui. 2012. A crucial role of Flagellin in the induction ofairway mucus production by Pseudomonas aeruginosa. PLoS ONE 7: e39888.
24. Tan, H. L., N. Regamey, S. Brown, A. Bush, C. M. Lloyd, and J. C. Davies.2011. The Th17 pathway in cystic fibrosis lung disease. Am. J. Respir. Crit. CareMed. 184: 252–258.
25. McAllister, F., A. Henry, J. L. Kreindler, P. J. Dubin, L. Ulrich, C. Steele,J. D. Finder, J. M. Pilewski, B. M. Carreno, S. J. Goldman, et al. 2005. Role ofIL-17A, IL-17F, and the IL-17 receptor in regulating growth-related oncogene-alpha and granulocyte colony-stimulating factor in bronchial epithelium: impli-cations for airway inflammation in cystic fibrosis. J. Immunol. 175: 404–412.
26. Dubin, P. J., F. McAllister, and J. K. Kolls. 2007. Is cystic fibrosis a TH17disease? Inflamm. Res. 56: 221–227.
27. Dubin, P. J., and J. K. Kolls. 2011. IL-17 in cystic fibrosis: more than just Th17cells. Am. J. Respir. Crit. Care Med. 184: 155–157.
28. Decraene, A., A. Willems-Widyastuti, A. Kasran, K. De Boeck, D. M. Bullens,and L. J. Dupont. 2010. Elevated expression of both mRNA and protein levels ofIL-17A in sputum of stable cystic fibrosis patients. Respir. Res. 11: 177.
29. Brodlie, M., M. C. McKean, G. E. Johnson, A. E. Anderson, C. M. U. Hilkens,A. J. Fisher, P. A. Corris, J. L. Lordan, and C. Ward. 2011. Raised interleukin-17 isimmunolocalised to neutrophils in cystic fibrosis lung disease. Eur. Respir. J. 37:1378–1385.
30. Brodlie, M., J. Lordan, and C. Ward. 2011. Can cells other than Th17 lym-phocytes be important sources of IL-17 in the lungs? Thorax 66: 1096, authorreply 1096–1097.
31. Aujla, S. J., P. J. Dubin, and J. K. Kolls. 2007. Interleukin-17 in pulmonary hostdefense. Exp. Lung Res. 33: 507–518.
32. Rubin, H. R., R. U. Sorensen, P. A. Chase, and J. D. Klinger. 1983. Suppressionof in vitro lymphocyte DNA synthesis by killed Pseudomonas aeruginosa.Infect. Immun. 39: 630–637.
33. Moss, R. B., Y. P. Hsu, and L. Olds. 2000. Cytokine dysregulation in activatedcystic fibrosis (CF) peripheral lymphocytes. Clin. Exp. Immunol. 120: 518–525.
34. Kreindler, J. L., C. Steele, N. Nguyen, Y. R. Chan, J. M. Pilewski, J. F. Alcorn,Y. M. Vyas, S. J. Aujla, P. Finelli, M. Blanchard, et al. 2010. Vitamin D3attenuates Th2 responses to Aspergillus fumigatus mounted by CD4+ T cellsfrom cystic fibrosis patients with allergic bronchopulmonary aspergillosis.J. Clin. Invest. 120: 3242–3254.
35. Hartl, D., M. Griese, M. Kappler, G. Zissel, D. Reinhardt, C. Rebhan,D. J. Schendel, and S. Krauss-Etschmann. 2006. Pulmonary T(H)2 response inPseudomonas aeruginosa-infected patients with cystic fibrosis. J. Allergy Clin.Immunol. 117: 204–211.
36. Moser, C., H. K. Johansen, Z. J. Song, H. P. Hougen, J. Rygaard, and N. Høiby.1997. Chronic Pseudomonas aeruginosa lung infection is more severe in Th2responding BALB/c mice compared to Th1 responding C3H/HeN mice. APMIS105: 838–842.
37. Moser, C., P. O. Jensen, O. Kobayashi, H. P. Hougen, Z. Song, J. Rygaard,A. Kharazmi, and N. H by. 2002. Improved outcome of chronic Pseudomonasaeruginosa lung infection is associated with induction of a Th1-dominated cy-tokine response. Clin. Exp. Immunol. 127: 206–213.
38. Moser, C., H. P. Hougen, Z. J. Song, J. Rygaard, A. Kharazmi, and N. Høiby.1999. Early immune response in susceptible and resistant mice strains withchronic Pseudomonas aeruginosa lung infection determines the type of T-helpercell response. APMIS 107: 1093–1100.
39. Dubin, P. J., A. Martz, J. R. Eisenstatt, M. D. Fox, A. Logar, and J. K. Kolls.2012. Interleukin-23-mediated inflammation in Pseudomonas aeruginosa pul-monary infection. Infect. Immun. 80: 398–409.
40. Dubin, P. J., and J. K. Kolls. 2007. IL-23 mediates inflammatory responses tomucoid Pseudomonas aeruginosa lung infection in mice. Am. J. Physiol. LungCell. Mol. Physiol. 292: L519–L528.
41. Mueller, C., S. A. Braag, A. Keeler, C. Hodges, M. Drumm, and T. R. Flotte.2011. Lack of cystic fibrosis transmembrane conductance regulator in CD3+ lym-phocytes leads to aberrant cytokine secretion and hyperinflammatory adaptiveimmune responses. Am. J. Respir. Cell Mol. Biol. 44: 922–929.
42. Moss, R. B. 2010. Allergic bronchopulmonary aspergillosis and Aspergillusinfection in cystic fibrosis. Curr. Opin. Pulm. Med. 16: 598–603.
43. Allard, J. B., M. E. Poynter, K. A. Marr, L. Cohn, M. Rincon, andL. A. Whittaker. 2006. Aspergillus fumigatus generates an enhanced Th2-biasedimmune response in mice with defective cystic fibrosis transmembrane con-ductance regulator. J. Immunol. 177: 5186–5194.
44. Moss, R. B. 2009. Infection, inflammation, and the downward spiral of cysticfibrosis lung disease. J. Pediatr. 154: 162–163.
45. Moss, R. B. 2004. Lymphocytes in cystic fibrosis lung disease: a tale of twoimmunities. Clin. Exp. Immunol. 135: 358–360.
46. Hartl, D. 2009. Immunological mechanisms behind the cystic fibrosis-ABPAlink. Med. Mycol. 47(Suppl 1): S183–S191.
47. Kelly, E., C. M. Greene, and N. G. McElvaney. 2008. Targeting neutrophilelastase in cystic fibrosis. Expert Opin. Ther. Targets 12: 145–157.
48. Gaggar, A., S.M. Rowe, H. Matthew, and J.E. Blalock. 2010. Proline-glycine-proline (PGP) and high mobility group box protein-1 (HMGB1): potentialmediators of cystic fibrosis airway inflammation. Open Respir. Med. J. 4: 32–38.
49. Gaggar, A., Y. Li, N. Weathington, M. Winkler, M. Kong, P. Jackson,J. E. Blalock, and J. P. Clancy. 2007. Matrix metalloprotease-9 dysregulation inlower airway secretions of cystic fibrosis patients. Am. J. Physiol. Lung Cell.Mol. Physiol. 293: L96–L104.
50. Vollbrecht, T., R. Stirner, A. Tufman, J. Roider, R. M. Huber, J. R. Bogner, A. Lechner,C. Bourquin, and R. Draenert. 2012. Chronic progressive HIV-1 infection is associatedwith elevated levels of myeloid-derived suppressor cells. AIDS 26: F31–F37.
1284 FLAGELLIN AND MDSCs
by guest on June 26, 2018http://w
ww
.jimm
unol.org/D
ownloaded from
Related Documents











