Inhibition of Protein-protein Interactions in Mycobacterium Tuberculosis through Drug Screening Team Mycobacterium Tuberculosis (MTB) Authors: Pradip Ramamurti, Malik Antoine, Paige Chan, He Chun, Elizabeth Corley, Isaac Jeong, Christopher Kim, Carolyn Lane, Ari Mandler, Nathaniel Nenortas, Michelle Nguyen, Ian Qian, James Tuo, Jimmy Zhang Mentor: Volker Briken Abstract The bacterium Mycobacterium tuberculosis (Mtb) is the main causative agent of human tuberculosis (TB). TB is typically characterized by large granulomas on the lungs where the bacteria reside. Mtb is transmitted between humans through aerosol droplets released when an infected individual coughs or expels fluid from their lungs. This has led to an estimate that one in every three people in the world are infected with some form of the disease. TB may remain in its latent form for the entirety of the patient’s life span. If the infection progresses to active disease, the patient will have few viable options for effective treatment, which is a large reason for the disease killing 1.3 million people annually. Many of these people are located in developing countries and mortality rate is increased in immunocompromised communities. Current treatments have been rendered ineffective by the emergence of drug resistant strains of the pathogen. The type VII secretion systems and signal transduction pathways of Mtb have been shown to be vital to its virulence in the human body. Inhibition of the protein-protein interactions in these pathways has been shown to result in attenuation of the pathogen. The mycobacterial protein fragment complementation (M-PFC) assay has been shown to be an accurate method to quantify the degree of interaction between a specific pair of proteins in Mtb. Using the M-PFC assay, a drug panel can be screened to identify inhibitors of protein-protein interactions important to virulence. By inhibiting these specific interactions, a possible new treatment for TB can be identified. This new treatment will has the potential to advance to clinical trials and eventually to patient treatment. Introduction Tuberculosis, caused by the bacillus, Mycobacterium tuberculosis, is a highly contagious and infectious disease that kills about 1.3 million people annually Despite current research and treatments, TB is the second leading cause of death in several regions, mainly in East Asia and Africa, and worldwide, one in three people are carriers for the disease. The TB epidemic is magnified by the emergence of multidrug resistant strains such as mycobacteria MDR-TB and XDR-TB, which are resistant to rifampicin and isoniazid, two of the leading treatments. Specific Aims 1. Establish a High-Throughput Liquid Screening Assay 2. Construct Desired Fusion Proteins for the Mycobacterial Protein Fragment Complementation (MPFC) System to Test for Protein-protein Interaction 3. Perform drug screenings on a multi-compound drug panel with our MPFC assay. 4. Validate our results by testing for potential false negatives and false positives. Research Question What established drugs can be repurposed to disrupt vital virulence pathways within Mycobacterium tuberculosis ? Use of M. smegmatis Model System Mycobacterium smegmatis (Msm) was chosen to be the model organism because it shares similar biosynthetic pathways and cell membrane types with Mycobacterium tuberculosis (Mtb). Msm replicates much faster than Mtb and takes up DNA more efficiently. While a colony of Mtb requires about three weeks to grow, a colony of Msm requires only four days. A shorter doubling time and quicker transformation means these assays will take less time to complete. Msm is nonpathogenic in humans and can therefore be safely handled in Biosafety Level (BSL)-2 labs, while Mtb must be handled in a BSL-3 lab. Methodology Compound Drug Library The National Institute of Health’s Clinical Collection will provide the drug library that will be used for this experiment. This library includes plated arrays of 446 small molecules with known health benefits that were originally designed for other diseases, but may have untapped potential in disrupting mycobacterial biological pathways. As these drugs have already passed clinical testing, they can be implemented more easily than new compounds. Expected Results We hope that one or more of our drugs tested will give us a positive hit. After analyzing and collecting all of our positive hits, we could perform a cytotoxicity screen against HEPG2 and HEK293 human cell lines for liver and kidney cells, respectively. It is important to test cytotoxicity toward human cells because if a drug is effective against our protein interaction but is toxic toward human cells, it is not a viable candidate for future clinical testing. We will be using liver and kidney cell lines because those organs are responsible for filtering toxins from the blood, which means that they will be exposed to our drugs in the highest concentrations in the body. Future Testing Compound Structure Analysis • Any drugs which result in a positive hit or exhibit toxicity toward human cells should be analyzed on a structural basis to determine if there are any other compounds that exist in the same family. A drug family is categorized by a group of compounds that share many similar structural characteristics • If any compounds like this can be identified, we can look into possibly requesting to have those sent to us by NIH or synthesized for us by an organic chemist. By further analyzing drug families similar to molecules already found to be effective, we would hope to find a plethora of possible drugs based on structural similarities to already defined positive hits. Dose- Response Relationship • If a compound yields a positive result and we have enough of it for further testing after our cytotoxicity assay, we could try and develop a dose-response relationship • Testing in virulent Mtb to ensure that the drugs are effective in the true disease causing bacteria. References Abate, G., Mshana, R. N., & Miörner, H. (1998). Evaluation of a colorimetric assay based on 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyl tetrazolium bromide (MTT) for rapid detection of rifampicin resistance in Mycobacterium tuberculosis. International Journal of Tuberculosis and Lung Disease 2(12), 1011-6.Clark, K. L., Larsen, P. B., Wang, X., & Chang, C. (1998). Association of the Arabidopsis CTR1 Raf-like kinase with the ETR1 and ERS ethylene receptors. PNAS, 95(9), 5401-5406.Dziedzic, R., Kiran, M., Plocinski, P., Ziolkiewicz, M., Brzostek, A., Moomey, M., & Rajagopalan, M. (2010). Mycobacterium tuberculosis ClpX interacts with FtsZ and interferes with FtsZ assembly. PloS one, 5(7). Mai, D., Jones, J., Rodgers, J.W., Hartman IV, J.L., Kutsch, O., & Steyn, A.J. (2011). A screen to identify small molecule inhibitors of protein-protein interactions in mycobacteria. Assay and drug development technologies, 9(3), 299-310.New England BioLab Inc. (2014). Molecular Cloning Technical Guide. Retrieved from http://www.neb.com/~/media/NebUs/Files/Brochures/Cloning_Guide_1113.pdfPeñuelas-Urquides, K., Silva-Ramírez, B., Rivadeneyra-Espinoza, L., & Said-Fernández, S. (2013) Measuring of Mycobacterium tuberculosis growth. A correlation of the optical measurements with colony forming units. Brazilian Journal of Microbiology, 44(1), 287–290.Singh, A., Mai, D., Kumar, A., & Steyn, A. (2006). Dissecting virulence pathways of Mycobacterium tuberculosis through protein-protein association. Proceedings of the National Academy of Sciences, 103(30), 11346-11351.Tiwari, B. M., Kannan, N., Vemu, L., & Raghunand, T. R. (2012). The Mycobacterium tuberculosis PE proteins Rv0285 and Rv1386 modulate innate immunity and mediate bacillary survival in macrophages. PloS one, 7(12). Velmurugan, K., Chen, B., Miller, J., Azogue, S., Gurses, S., Hsu, T., Briken, V. (2010). Mycobacterium tuberculosis nuoG is a virulence gene that inhibits apoptosis of infected host cells. PLoS Pathogens, 3(7). The M-PFC assay is specifically designed to detect cytoplasmic and membrane-bound protein interactions within mycobacterium cells Using M-PFC plasmids containing mDHFR domain genes, the plasmids can be digested producing sticky ends, which can then be combined and ligated together to produce an assembled vector Using the M-PFC assay, we will be able to detect whether the drugs used interact with the proteins, preventing the protein-protein interaction, and expressing a blue color In order to disprove false positive and negative results, we will perform a screen that involves testing compounds with the M-PFC assay and no TRIM in triplicate form

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Inhibition of Protein-protein Interactions in Mycobacterium Tuberculosis through Drug Screening
Team Mycobacterium Tuberculosis (MTB)Authors: Pradip Ramamurti, Malik Antoine, Paige Chan, He Chun, Elizabeth Corley, Isaac Jeong, Christopher
Kim, Carolyn Lane, Ari Mandler, Nathaniel Nenortas, Michelle Nguyen, Ian Qian, James Tuo, Jimmy ZhangMentor: Volker Briken
AbstractThe bacterium Mycobacterium tuberculosis (Mtb) is the main causative agent of human tuberculosis (TB). TB is typically characterized by large granulomas on the lungs where the bacteria reside. Mtb is transmitted between humans through aerosol droplets released when an infected individual coughs or expels fluid from their lungs. This has led to an estimate that one in every three people in the world are infected with some form of the disease. TB may remain in its latent form for the entirety of the patient’s life span. If the infection progresses to active disease, the patient will have few viable options for effective treatment, which is a large reason for the disease killing 1.3 million people annually. Many of these people are located in developing countries and mortality rate is increased in immunocompromised communities. Current treatments have been rendered ineffective by the emergence of drug resistant strains of the pathogen. The type VII secretion systems and signal transduction pathways of Mtb have been shown to be vital to its virulence in the human body. Inhibition of the protein-protein interactions in these pathways has been shown to result in attenuation of the pathogen. The mycobacterial protein fragment complementation (M-PFC) assay has been shown to be an accurate method to quantify the degree of interaction between a specific pair of proteins in Mtb. Using the M-PFC assay, a drug panel can be screened to identify inhibitors of protein-protein interactions important to virulence. By inhibiting these specific interactions, a possible new treatment for TB can be identified. This new treatment will has the potential to advance to clinical trials and eventually to patient treatment.
IntroductionTuberculosis, caused by the bacillus, Mycobacterium tuberculosis, is a highly contagious and infectious disease that kills about 1.3 million people annually Despite current research and treatments, TB is the second leading cause of death in several regions, mainly in East Asia and Africa, and worldwide, one in three people are carriers for the disease. The TB epidemic is magnified by the emergence of multidrug resistant strains such as mycobacteria MDR-TB and XDR-TB, which are resistant to rifampicin and isoniazid, two of the leading treatments.
Specific Aims1. Establish a High-Throughput Liquid Screening Assay2. Construct Desired Fusion Proteins for the Mycobacterial Protein Fragment
Complementation (MPFC) System to Test for Protein-protein Interaction3. Perform drug screenings on a multi-compound drug panel with our MPFC assay.4. Validate our results by testing for potential false negatives and false positives.
Research QuestionWhat established drugs can be repurposed to disrupt vital virulence pathways within Mycobacterium tuberculosis?
Use of M. smegmatis Model SystemMycobacterium smegmatis (Msm) was chosen to be the model organism because it shares similar biosynthetic pathways and cell membrane types with Mycobacterium tuberculosis (Mtb). Msm replicates much faster than Mtb and takes up DNA more efficiently. While a colony of Mtb requires about three weeks to grow, a colony of Msm requires only four days. A shorter doubling time and quicker transformation means these assays will take less time to complete. Msm is nonpathogenic in humans and can therefore be safely handled in Biosafety Level (BSL)-2 labs, while Mtb must be handled in a BSL-3 lab.
Methodology
Compound Drug LibraryThe National Institute of Health’s Clinical Collection will provide the drug library that will be used for this experiment. This library includes plated arrays of 446 small molecules with known health benefits that were originally designed for other diseases, but may have untapped potential in disrupting mycobacterial biological pathways. As these drugs have already passed clinical testing, they can be implemented more easily
than new compounds.
Expected Results
We hope that one or more of our drugs tested will give us a positive hit. After analyzing and collecting all of our positive hits, we could perform a cytotoxicity screen against HEPG2 and HEK293 human cell lines for liver and kidney cells, respectively. It is important to test cytotoxicity toward human cells because if a drug is effective against our protein interaction but is toxic toward human cells, it is not a viable candidate for future clinical testing. We will be using liver and kidney cell lines because those organs are responsible for filtering toxins from the blood, which means that they will be exposed to our drugs in the highest concentrations in the body.
Future TestingCompound Structure Analysis• Any drugs which result in a positive hit or exhibit toxicity toward human cells should be analyzed on a
structural basis to determine if there are any other compounds that exist in the same family. A drug family is categorized by a group of compounds that share many similar structural characteristics
• If any compounds like this can be identified, we can look into possibly requesting to have those sent to us by NIH or synthesized for us by an organic chemist. By further analyzing drug families similar to molecules already found to be effective, we would hope to find a plethora of possible drugs based on structural similarities to already defined positive hits.
Dose- Response Relationship • If a compound yields a positive result and we have enough of it for further testing after our cytotoxicity assay,
we could try and develop a dose-response relationship• Testing in virulent Mtb to ensure that the drugs are effective in the true disease causing bacteria.
ReferencesAbate, G., Mshana, R. N., & Miörner, H. (1998). Evaluation of a colorimetric assay based on 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyl tetrazolium bromide (MTT) for rapid detection of rifampicin resistance in Mycobacterium tuberculosis. International Journal of Tuberculosis and Lung Disease 2(12), 1011-6.Clark, K. L., Larsen, P. B., Wang, X., & Chang, C. (1998). Association of the Arabidopsis CTR1 Raf-like kinase with the ETR1 and ERS ethylene receptors. PNAS, 95(9), 5401-5406.Dziedzic, R., Kiran, M., Plocinski, P., Ziolkiewicz, M., Brzostek, A., Moomey, M., & Rajagopalan, M. (2010). Mycobacterium tuberculosis ClpX interacts with FtsZ and interferes with FtsZ assembly. PloS one, 5(7).Mai, D., Jones, J., Rodgers, J.W., Hartman IV, J.L., Kutsch, O., & Steyn, A.J. (2011). A screen to identify small molecule inhibitors of protein-protein interactions in mycobacteria. Assay and drug development technologies, 9(3), 299-310.New England BioLab Inc. (2014). Molecular Cloning Technical Guide. Retrieved from http://www.neb.com/~/media/NebUs/Files/Brochures/Cloning_Guide_1113.pdfPeñuelas-Urquides, K., Silva-Ramírez, B., Rivadeneyra-Espinoza, L., & Said-Fernández, S. (2013) Measuring of Mycobacterium tuberculosis growth. A correlation of the optical measurements with colony forming units. Brazilian Journal of Microbiology, 44(1), 287–290.Singh, A., Mai, D., Kumar, A., & Steyn, A. (2006). Dissecting virulence pathways of Mycobacterium tuberculosis through protein-protein association. Proceedings of the National Academy of Sciences, 103(30), 11346-11351.Tiwari, B. M., Kannan, N., Vemu, L., & Raghunand, T. R. (2012). The Mycobacterium tuberculosis PE proteins Rv0285 and Rv1386 modulate innate immunity and mediate bacillary survival in macrophages. PloS one, 7(12).Velmurugan, K., Chen, B., Miller, J., Azogue, S., Gurses, S., Hsu, T., Briken, V. (2010). Mycobacterium tuberculosis nuoG is a virulence gene that inhibits apoptosis of infected host cells. PLoS Pathogens, 3(7).
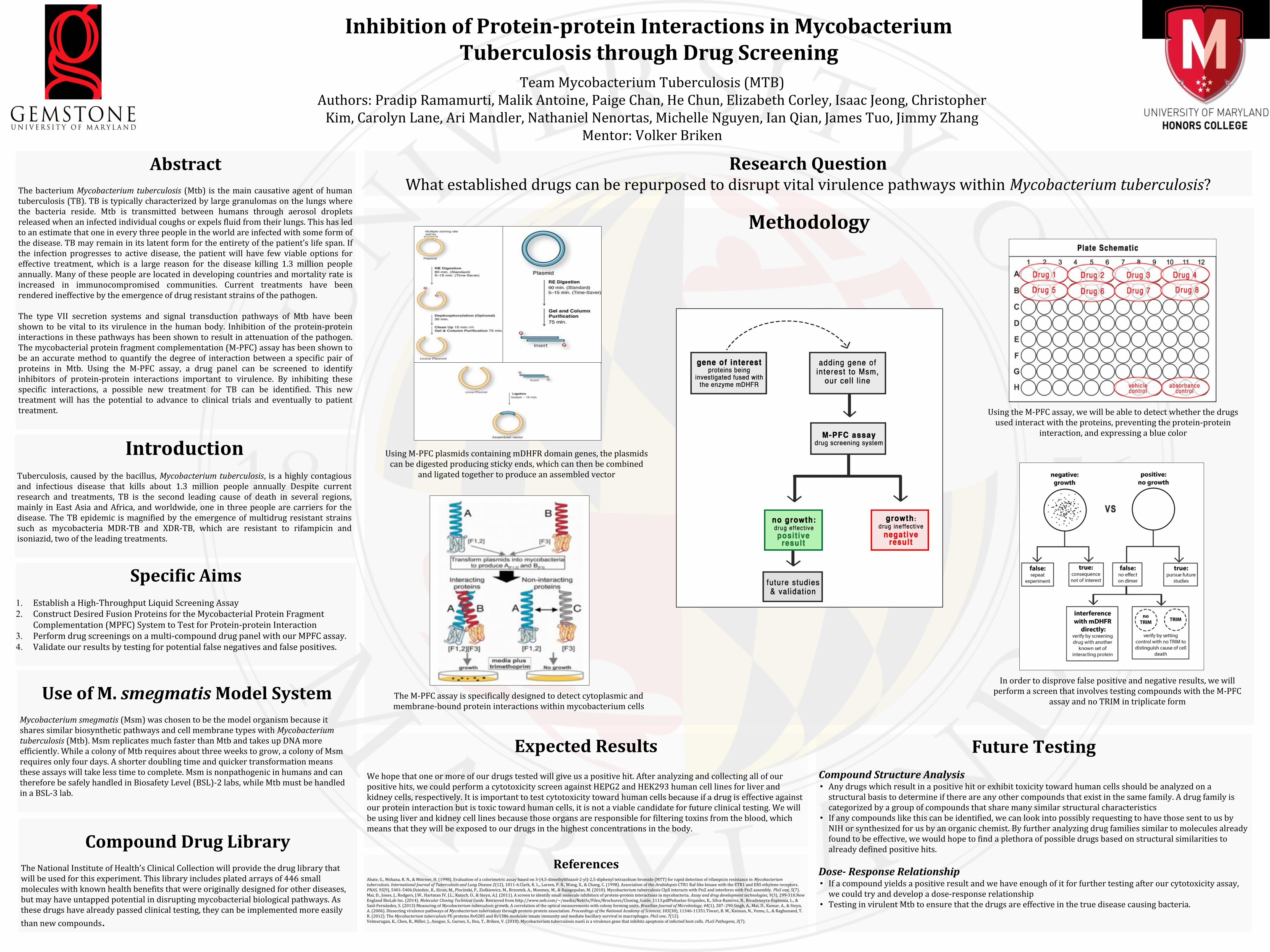
The M-PFC assay is specifically designed to detect cytoplasmic and membrane-bound protein interactions within mycobacterium cells
Using M-PFC plasmids containing mDHFR domain genes, the plasmids can be digested producing sticky ends, which can then be combined
and ligated together to produce an assembled vector
Using the M-PFC assay, we will be able to detect whether the drugs used interact with the proteins, preventing the protein-protein
interaction, and expressing a blue color
In order to disprove false positive and negative results, we will perform a screen that involves testing compounds with the M-PFC
assay and no TRIM in triplicate form

Related Documents