children Article Evaluating and Enhancing the Preparation of Patients and Families before Pediatric Surgery Christopher Newell 1, * , † , Heather Leduc-Pessah 1, † , Lisa Bell-Graham 2 , Nivez Rasic 3,4 and Kerryn Carter 4 1 Cumming School of Medicine, University of Calgary, Calgary, AB T2N 4N1, Canada; [email protected] 2 Alberta Children’s Hospital, Calgary, AB T3B 6A8, Canada; [email protected] 3 Alberta Children’s Hospital Research Institute, Calgary, AB T3B 6A8, Canada; [email protected] 4 Section of Pediatric Anesthesiology, Department of Anesthesiology, Perioperative and Pain Medicine, University of Calgary, Calgary, AB T3B 6A8, Canada; [email protected] * Correspondence: [email protected] † These authors contributed equally to the manuscript. Received: 14 June 2020; Accepted: 31 July 2020; Published: 5 August 2020 Abstract: Surgery can be a difficult and unfamiliar experience for children and their families. We examined the ability of existing information to help families feel better prepared for surgery at the Alberta Children’s Hospital (ACH) and evaluated the best way to enhance its content and accessibility. We developed an online survey for families who have had surgery at ACH. Participants were recruited through pre-existing patient networks and from the ACH Short Stay Unit (SSU) between October 2018 and October 2019. The survey asked participants to evaluate the information available to prepare them for surgery and requested suggestions for improvement. Our survey results show that those who completed the in-person Surgery 101 program felt significantly more prepared for surgery. Of those who did not attend; 40% would have been interested in participating but were unaware that the program existed; and 17% planned to attend but were unable to; due to work or travel distance. Participants felt additional resources via online content or paper handouts would be most valuable. We used this information to prepare an online accessible summary of the Surgery 101 program and tour in the form of a video to reach more Albertan families preparing for surgery for their children Keywords: pediatric surgery; patient education; patient-centered care; pre-operative anxiety 1. Introduction More than one million patients undergo a surgical procedure in Canada annually [1], with at least 64,000 being pediatric cases [2]. Surgery can be a difficult and unfamiliar experience for both children and their families, which can be influenced by parental and child stress, anxiety, and catastrophizing [3]. Data suggests that up to 60% of pediatric patients experience high levels of pre-operative anxiety [4], which can lead to increased levels of post-operative pain, analgesic consumption, and general anxiety [5]. To address these concerns, many hospitals provide access to pre-operative resources aimed at alleviating pre-operative stressors. Existing information to help prepare families for surgery at the Alberta Children’s Hospital (ACH) includes paper handouts, the ACH website, the Family and Community Resource Centre (FCRC), and the Surgery 101 program. The FCRC is a dedicated service within ACH which aims to provide credible health information, family support, and resources to the surrounding community. Surgery 101 is a specialized program run by Child Life Specialists at ACH providing in-hospital sessions to orient patients and families on what to expect when preparing to undergo surgical intervention. Children 2020, 7, 90; doi:10.3390/children7080090 www.mdpi.com/journal/children

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

children
Article
Evaluating and Enhancing the Preparation of Patientsand Families before Pediatric Surgery
Christopher Newell 1,*,† , Heather Leduc-Pessah 1,†, Lisa Bell-Graham 2, Nivez Rasic 3,4 andKerryn Carter 4
1 Cumming School of Medicine, University of Calgary, Calgary, AB T2N 4N1, Canada; [email protected] Alberta Children’s Hospital, Calgary, AB T3B 6A8, Canada; [email protected] Alberta Children’s Hospital Research Institute, Calgary, AB T3B 6A8, Canada;
[email protected] Section of Pediatric Anesthesiology, Department of Anesthesiology, Perioperative and Pain Medicine,
University of Calgary, Calgary, AB T3B 6A8, Canada; [email protected]* Correspondence: [email protected]† These authors contributed equally to the manuscript.
Received: 14 June 2020; Accepted: 31 July 2020; Published: 5 August 2020�����������������
Abstract: Surgery can be a difficult and unfamiliar experience for children and their families.We examined the ability of existing information to help families feel better prepared for surgery at theAlberta Children’s Hospital (ACH) and evaluated the best way to enhance its content and accessibility.We developed an online survey for families who have had surgery at ACH. Participants were recruitedthrough pre-existing patient networks and from the ACH Short Stay Unit (SSU) between October2018 and October 2019. The survey asked participants to evaluate the information available toprepare them for surgery and requested suggestions for improvement. Our survey results show thatthose who completed the in-person Surgery 101 program felt significantly more prepared for surgery.Of those who did not attend; 40% would have been interested in participating but were unaware thatthe program existed; and 17% planned to attend but were unable to; due to work or travel distance.Participants felt additional resources via online content or paper handouts would be most valuable.We used this information to prepare an online accessible summary of the Surgery 101 program andtour in the form of a video to reach more Albertan families preparing for surgery for their children
Keywords: pediatric surgery; patient education; patient-centered care; pre-operative anxiety
1. Introduction
More than one million patients undergo a surgical procedure in Canada annually [1], withat least 64,000 being pediatric cases [2]. Surgery can be a difficult and unfamiliar experience forboth children and their families, which can be influenced by parental and child stress, anxiety,and catastrophizing [3]. Data suggests that up to 60% of pediatric patients experience high levelsof pre-operative anxiety [4], which can lead to increased levels of post-operative pain, analgesicconsumption, and general anxiety [5].
To address these concerns, many hospitals provide access to pre-operative resources aimedat alleviating pre-operative stressors. Existing information to help prepare families for surgery atthe Alberta Children’s Hospital (ACH) includes paper handouts, the ACH website, the Family andCommunity Resource Centre (FCRC), and the Surgery 101 program. The FCRC is a dedicated servicewithin ACH which aims to provide credible health information, family support, and resources to thesurrounding community. Surgery 101 is a specialized program run by Child Life Specialists at ACHproviding in-hospital sessions to orient patients and families on what to expect when preparing toundergo surgical intervention.
Children 2020, 7, 90; doi:10.3390/children7080090 www.mdpi.com/journal/children

Children 2020, 7, 90 2 of 10
Internal ACH data report that approximately 10,000 surgeries take place annually. The existingSurgery 101 program receives approximately 50 families per year, reaching only 0.5% of potentialpatients. We hypothesized that the existing Surgery 101 program is valuable in preparing families forsurgery but that its accessibility and enrollment may be improved upon. Therefore, we developedan online survey for families who have had surgery at ACH. Participants were asked to evaluate theinformation that was available to prepare them for surgery and specifically highlighted participantawareness of the Surgery 101 program. The study presented here was designed to improve the surgicalexperience for pediatric patients and their families from across Alberta who were coming to ACH forsurgery and may serve as an example to other hospitals caring for children.
2. Materials and Methods
2.1. Study Design, Setting, Survey Participants and Size
This study employed a retrospective cohort study design using an online survey. Designed tobe completed by patients and/or their parents, this open survey was comprised of 24 questions or30 questions if they had participated in Surgery 101. For a full list of survey questions, see SupplementaryFile S1. A 10-point Likert scale was used for ranking. All survey questions were reviewed and approvedby all members of the research team. No incentives were offered for completion of the survey. The surveywas conducted through the Alberta Health Services approved online survey platform (Select Survey).Patients and/or their parents were asked to provide consent online through Select Survey and allconsent documents were provided through the Select Survey platform. The site was not passwordprotected but a link or information with the survey ID was helpful to locate it. Since families mayhave multiple children or experiences, we did not limit responses by IP address or computer, and weasked families to report only their most recent experience. At initiation of the survey, participants wereprovided with a Select Survey code through which they could modify or delete their responses atany time.
We surveyed pediatric patients, age 0–18 years, who have had surgery at ACH and parents ofpediatric patients who have had surgery at ACH. Past participants of the Surgery 101 in-hospitalprogram during the past two years (2017–2019) were contacted via e-mail. Participants who did notparticipate in Surgery 101 were recruited through the ACH Patient and Family Centered Care Network(e-mail list of families willing to receive information about research), the Day Surgery Unit at ACH(poster and optional access to survey link), and through approved posters displayed throughout ACH.Although general demographic data were collected, patient or family names and contact informationwere not collected and all data was anonymized upon receipt by the investigators. Only anonymizeddata were stored on the secure Select Survey platform.
A sample size of 96 participants was calculated prior to survey implementation using a populationof 10,000 pediatric surgical cases per year at ACH, a margin of error of 10%, a 95% confidenceinterval, and a response distribution of 50:50. This study was carried out in accordance with theregulations of the University of Calgary’s Conjoint Health Research Ethics Board and the Declarationof Helsinki (REB18-0272).
2.2. Thematic Analysis
A qualitative deductive thematic analysis was conducted of the free text reported in the survey.The global themes from this data were separated into Surgery 101 specific feedback and generalfeedback. The most common re-occurring codes were identified on qualitative analysis of the text andgrouped into themes. Codes and themes are reported in Figure 1. Direct participant comments areanonymously reported within the text.

Children 2020, 7, 90 3 of 10Children 2020, 7, x FOR PEER REVIEW 3 of 10
Figure 1. Thematic Analysis Summary of Participant Free Text Responses. A qualitative deductive
thematic analysis was conducted of the free text participants responses to the questions (1) “Is there
any further information you wish to share regarding your and/or your child’s experience at Alberta
Children’s Hospital?”, (2) “What was something you learned from the Surgery 101 Program?” and
(3) “What was something you wished you learned from the Surgery 101 Program?” All responses
were analyzed into global themes and organizing themes with code words for each organizing theme
displayed here.
2.3. Statistical Analysis
Statistical analysis was performed using GraphPad Prism for Windows, Version 6.0.7
(GraphPad Software Inc., La Jolla, CA, USA). Differences between groups were determined by
Student’s t-tests, where p < 0.05 was significant. Data are expressed as mean ± SEM.
3. Results
Participant recruitment occurred between October 2018 and October 2019, with each participant
being represented only once (Table 1). A total of 140 responses to the survey were collected, of which
97 were completed and used for analysis. Four of the responses were completed by the patient and
the remaining 93 by a parent. Hereafter, patient and/or parent survey responses will be referred to as
participants. A total of 32 (33.0%) survey participants completed the Surgery 101 program and 65
(67.0%) participants did not complete Surgery 101. When examining all responses, the age of
participants ranged from <1 to 16 years of age. Males comprised 60.8% of participants. Of surgical
patients, 64.9% spent at least one night in the hospital. The three most common types of surgical
procedures were ENT, GI, and Urology/Gynecology. The amount of time between surgery being
planned and the surgical intervention was typically >28 days (55.7%); however, Non-Surgery 101
participants more frequently experienced <7 days’ notice (20.0% vs. 6.2%, respectively). Most
participants travelled from within Calgary to attend their surgical procedure (74.3%). A complete
Figure 1. Thematic Analysis Summary of Participant Free Text Responses. A qualitative deductivethematic analysis was conducted of the free text participants responses to the questions (1) “Is thereany further information you wish to share regarding your and/or your child’s experience at AlbertaChildren’s Hospital?”, (2) “What was something you learned from the Surgery 101 Program?” and(3) “What was something you wished you learned from the Surgery 101 Program?” All responseswere analyzed into global themes and organizing themes with code words for each organizing themedisplayed here.
2.3. Statistical Analysis
Statistical analysis was performed using GraphPad Prism for Windows, Version 6.0.7 (GraphPadSoftware Inc., La Jolla, CA, USA). Differences between groups were determined by Student’s t-tests,where p < 0.05 was significant. Data are expressed as mean ± SEM.
3. Results
Participant recruitment occurred between October 2018 and October 2019, with each participantbeing represented only once (Table 1). A total of 140 responses to the survey were collected, of which97 were completed and used for analysis. Four of the responses were completed by the patient andthe remaining 93 by a parent. Hereafter, patient and/or parent survey responses will be referred to asparticipants. A total of 32 (33.0%) survey participants completed the Surgery 101 program and 65 (67.0%)participants did not complete Surgery 101. When examining all responses, the age of participantsranged from <1 to 16 years of age. Males comprised 60.8% of participants. Of surgical patients,64.9% spent at least one night in the hospital. The three most common types of surgical procedureswere ENT, GI, and Urology/Gynecology. The amount of time between surgery being planned and thesurgical intervention was typically >28 days (55.7%); however, Non-Surgery 101 participants morefrequently experienced <7 days’ notice (20.0% vs. 6.2%, respectively). Most participants travelledfrom within Calgary to attend their surgical procedure (74.3%). A complete comparison of patient
Children 2020, 7, 90 4 of 10
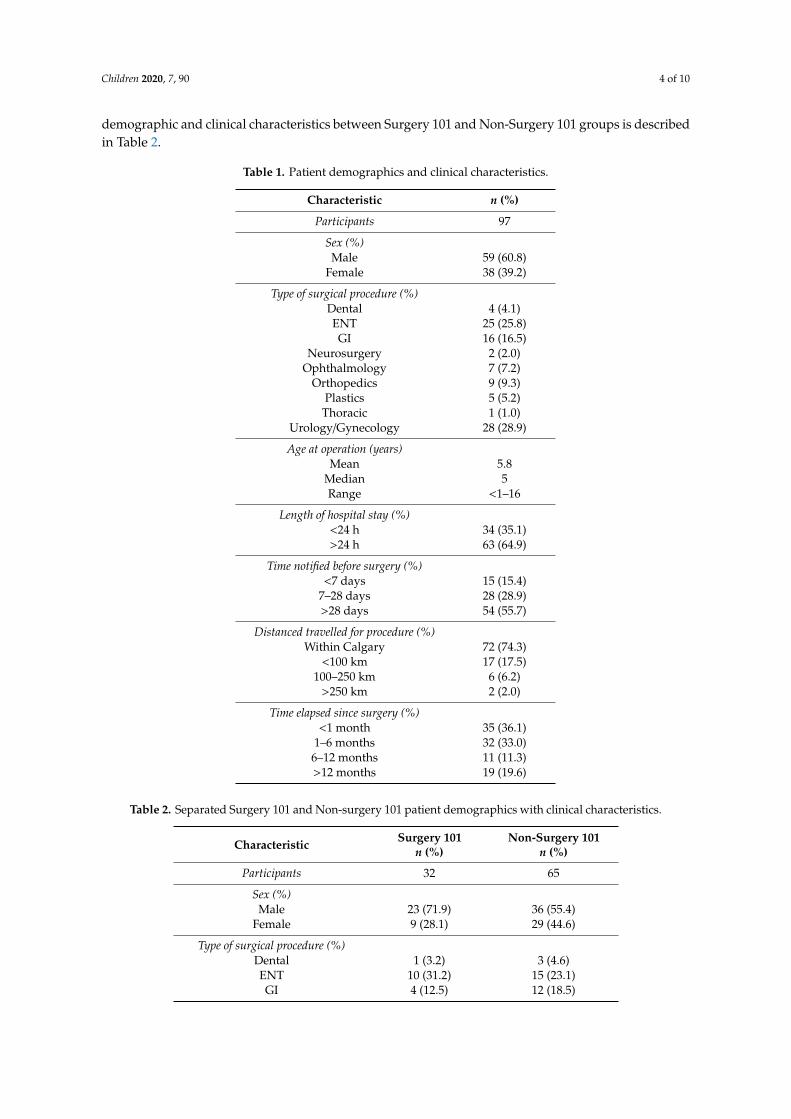
demographic and clinical characteristics between Surgery 101 and Non-Surgery 101 groups is describedin Table 2.
Table 1. Patient demographics and clinical characteristics.
Characteristic n (%)
Participants 97
Sex (%)Male 59 (60.8)
Female 38 (39.2)
Type of surgical procedure (%)Dental 4 (4.1)ENT 25 (25.8)GI 16 (16.5)
Neurosurgery 2 (2.0)Ophthalmology 7 (7.2)
Orthopedics 9 (9.3)Plastics 5 (5.2)
Thoracic 1 (1.0)Urology/Gynecology 28 (28.9)
Age at operation (years)Mean 5.8
Median 5Range <1–16
Length of hospital stay (%)<24 h 34 (35.1)>24 h 63 (64.9)
Time notified before surgery (%)<7 days 15 (15.4)
7–28 days 28 (28.9)>28 days 54 (55.7)
Distanced travelled for procedure (%)Within Calgary 72 (74.3)
<100 km 17 (17.5)100–250 km 6 (6.2)
>250 km 2 (2.0)
Time elapsed since surgery (%)<1 month 35 (36.1)
1–6 months 32 (33.0)6–12 months 11 (11.3)>12 months 19 (19.6)
Table 2. Separated Surgery 101 and Non-surgery 101 patient demographics with clinical characteristics.
Characteristic Surgery 101n (%)
Non-Surgery 101n (%)
Participants 32 65
Sex (%)Male 23 (71.9) 36 (55.4)
Female 9 (28.1) 29 (44.6)
Type of surgical procedure (%)Dental 1 (3.2) 3 (4.6)ENT 10 (31.2) 15 (23.1)GI 4 (12.5) 12 (18.5)
Children 2020, 7, 90 5 of 10
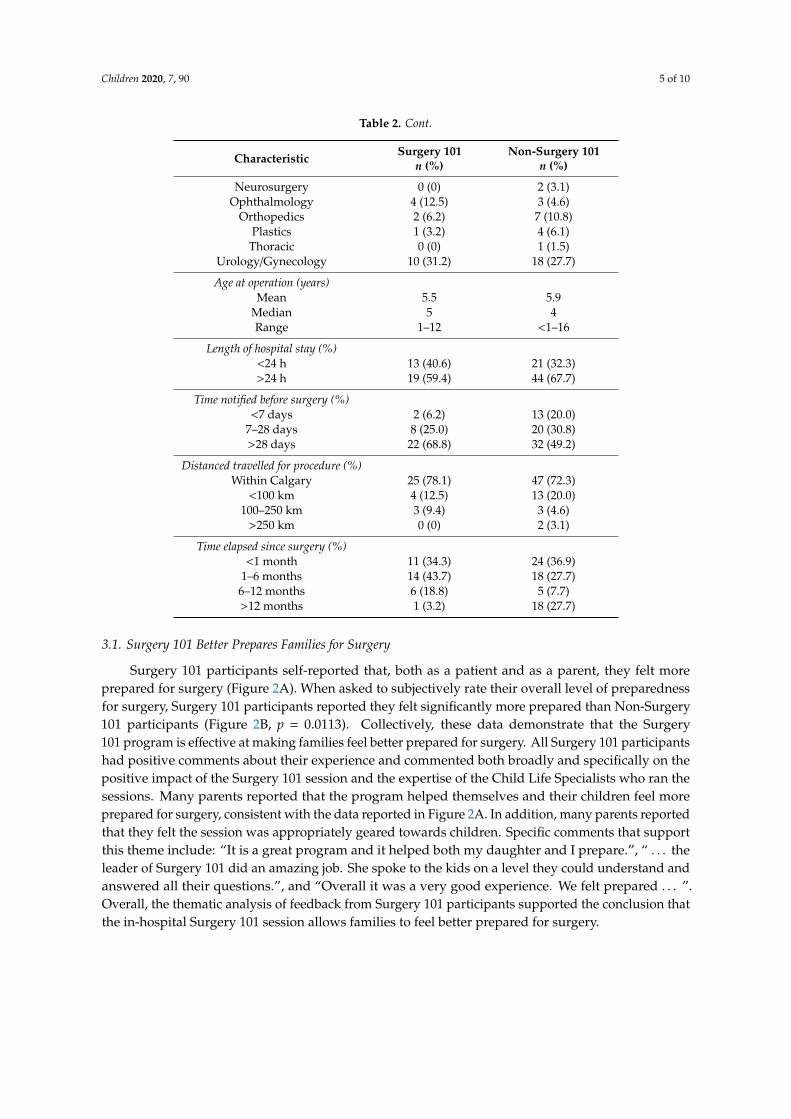
Table 2. Cont.
Characteristic Surgery 101n (%)
Non-Surgery 101n (%)
Neurosurgery 0 (0) 2 (3.1)Ophthalmology 4 (12.5) 3 (4.6)
Orthopedics 2 (6.2) 7 (10.8)Plastics 1 (3.2) 4 (6.1)
Thoracic 0 (0) 1 (1.5)Urology/Gynecology 10 (31.2) 18 (27.7)
Age at operation (years)Mean 5.5 5.9
Median 5 4Range 1–12 <1–16
Length of hospital stay (%)<24 h 13 (40.6) 21 (32.3)>24 h 19 (59.4) 44 (67.7)
Time notified before surgery (%)<7 days 2 (6.2) 13 (20.0)
7–28 days 8 (25.0) 20 (30.8)>28 days 22 (68.8) 32 (49.2)
Distanced travelled for procedure (%)Within Calgary 25 (78.1) 47 (72.3)
<100 km 4 (12.5) 13 (20.0)100–250 km 3 (9.4) 3 (4.6)
>250 km 0 (0) 2 (3.1)
Time elapsed since surgery (%)<1 month 11 (34.3) 24 (36.9)
1–6 months 14 (43.7) 18 (27.7)6–12 months 6 (18.8) 5 (7.7)>12 months 1 (3.2) 18 (27.7)
3.1. Surgery 101 Better Prepares Families for Surgery
Surgery 101 participants self-reported that, both as a patient and as a parent, they felt moreprepared for surgery (Figure 2A). When asked to subjectively rate their overall level of preparednessfor surgery, Surgery 101 participants reported they felt significantly more prepared than Non-Surgery101 participants (Figure 2B, p = 0.0113). Collectively, these data demonstrate that the Surgery101 program is effective at making families feel better prepared for surgery. All Surgery 101 participantshad positive comments about their experience and commented both broadly and specifically on thepositive impact of the Surgery 101 session and the expertise of the Child Life Specialists who ran thesessions. Many parents reported that the program helped themselves and their children feel moreprepared for surgery, consistent with the data reported in Figure 2A. In addition, many parents reportedthat they felt the session was appropriately geared towards children. Specific comments that supportthis theme include: “It is a great program and it helped both my daughter and I prepare.”, “ . . . theleader of Surgery 101 did an amazing job. She spoke to the kids on a level they could understand andanswered all their questions.”, and “Overall it was a very good experience. We felt prepared . . . ”.Overall, the thematic analysis of feedback from Surgery 101 participants supported the conclusion thatthe in-hospital Surgery 101 session allows families to feel better prepared for surgery.
Children 2020, 7, 90 6 of 10
Children 2020, 7, x FOR PEER REVIEW 5 of 10
Plastics 1 (3.2) 4 (6.1)
Thoracic 0 (0) 1 (1.5)
Urology/Gynecology 10 (31.2) 18 (27.7)
Age at operation (years)
Mean 5.5 5.9
Median 5 4
Range 1–12 <1–16
Length of hospital stay (%)
<24 h 13 (40.6) 21 (32.3)
>24 h 19 (59.4) 44 (67.7)
Time notified before surgery (%)
<7 days 2 (6.2) 13 (20.0)
7–28 days 8 (25.0) 20 (30.8)
>28 days 22 (68.8) 32 (49.2)
Distanced travelled for procedure (%)
Within Calgary 25 (78.1) 47 (72.3)
<100 km 4 (12.5) 13 (20.0)
100–250 km 3 (9.4) 3 (4.6)
>250 km 0 (0) 2 (3.1)
Time elapsed since surgery (%)
<1 month 11 (34.3) 24 (36.9)
1–6 months 14 (43.7) 18 (27.7)
6–12 months 6 (18.8) 5 (7.7)
>12 months 1 (3.2) 18 (27.7)
3.1. Surgery 101 Better Prepares Families for Surgery
Surgery 101 participants self-reported that, both as a patient and as a parent, they felt more
prepared for surgery (Figure 2A). When asked to subjectively rate their overall level of preparedness
for surgery, Surgery 101 participants reported they felt significantly more prepared than Non-
Surgery 101 participants (Figure 2B, p = 0.0113). Collectively, these data demonstrate that the Surgery
101 program is effective at making families feel better prepared for surgery. All Surgery 101
participants had positive comments about their experience and commented both broadly and
specifically on the positive impact of the Surgery 101 session and the expertise of the Child Life
Specialists who ran the sessions. Many parents reported that the program helped themselves and
their children feel more prepared for surgery, consistent with the data reported in Figure 2A. In
addition, many parents reported that they felt the session was appropriately geared towards children.
Specific comments that support this theme include: “It is a great program and it helped both my
daughter and I prepare.”, “…the leader of Surgery 101 did an amazing job. She spoke to the kids on
a level they could understand and answered all their questions.”, and “Overall it was a very good
experience. We felt prepared…”. Overall, the thematic analysis of feedback from Surgery 101
participants supported the conclusion that the in-hospital Surgery 101 session allows families to feel
better prepared for surgery.
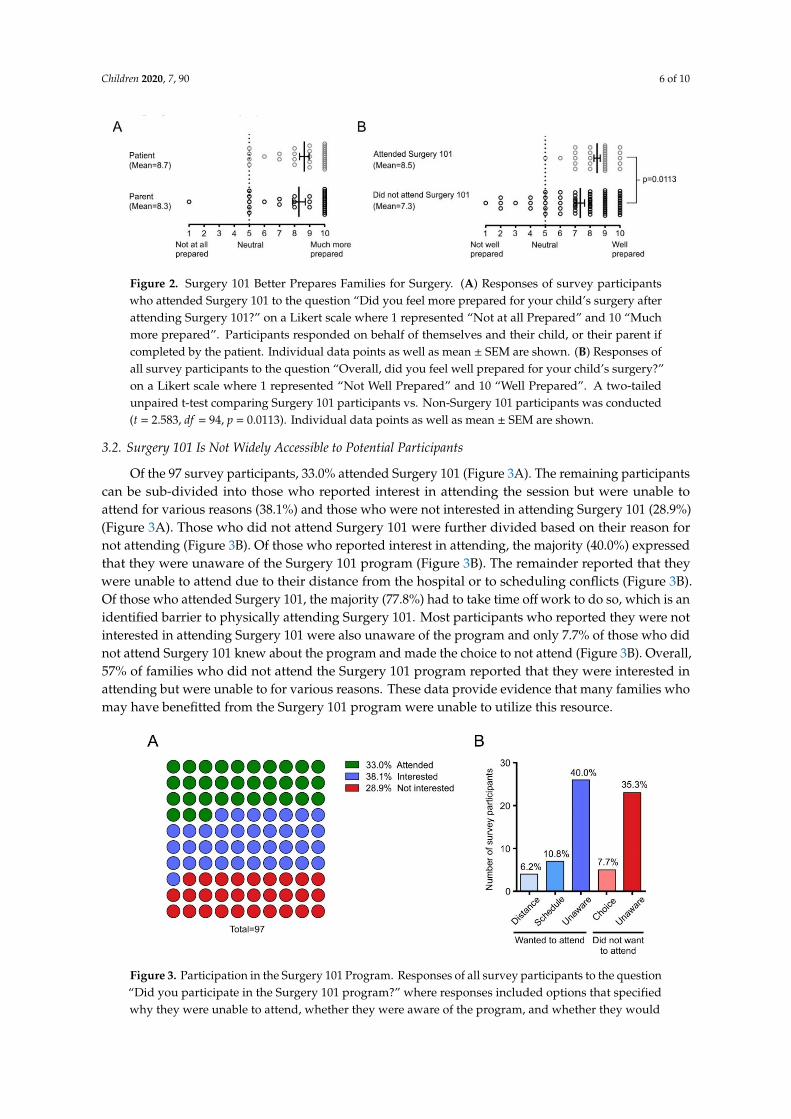
Figure 2. Surgery 101 Better Prepares Families for Surgery. (A) Responses of survey participants who
attended Surgery 101 to the question “Did you feel more prepared for your child’s surgery after
attending Surgery 101?” on a Likert scale where 1 represented “Not at all Prepared” and 10 “Much
Figure 2. Surgery 101 Better Prepares Families for Surgery. (A) Responses of survey participantswho attended Surgery 101 to the question “Did you feel more prepared for your child’s surgery afterattending Surgery 101?” on a Likert scale where 1 represented “Not at all Prepared” and 10 “Muchmore prepared”. Participants responded on behalf of themselves and their child, or their parent ifcompleted by the patient. Individual data points as well as mean ± SEM are shown. (B) Responses ofall survey participants to the question “Overall, did you feel well prepared for your child’s surgery?”on a Likert scale where 1 represented “Not Well Prepared” and 10 “Well Prepared”. A two-tailedunpaired t-test comparing Surgery 101 participants vs. Non-Surgery 101 participants was conducted(t = 2.583, df = 94, p = 0.0113). Individual data points as well as mean ± SEM are shown.
3.2. Surgery 101 Is Not Widely Accessible to Potential Participants
Of the 97 survey participants, 33.0% attended Surgery 101 (Figure 3A). The remaining participantscan be sub-divided into those who reported interest in attending the session but were unable toattend for various reasons (38.1%) and those who were not interested in attending Surgery 101 (28.9%)(Figure 3A). Those who did not attend Surgery 101 were further divided based on their reason fornot attending (Figure 3B). Of those who reported interest in attending, the majority (40.0%) expressedthat they were unaware of the Surgery 101 program (Figure 3B). The remainder reported that theywere unable to attend due to their distance from the hospital or to scheduling conflicts (Figure 3B).Of those who attended Surgery 101, the majority (77.8%) had to take time off work to do so, which is anidentified barrier to physically attending Surgery 101. Most participants who reported they were notinterested in attending Surgery 101 were also unaware of the program and only 7.7% of those who didnot attend Surgery 101 knew about the program and made the choice to not attend (Figure 3B). Overall,57% of families who did not attend the Surgery 101 program reported that they were interested inattending but were unable to for various reasons. These data provide evidence that many families whomay have benefitted from the Surgery 101 program were unable to utilize this resource.
Children 2020, 7, x FOR PEER REVIEW 6 of 10
more prepared”. Participants responded on behalf of themselves and their child, or their parent if
completed by the patient. Individual data points as well as mean ± SEM are shown. (B) Responses of
all survey participants to the question “Overall, did you feel well prepared for your child’s surgery?”
on a Likert scale where 1 represented “Not Well Prepared” and 10 “Well Prepared”. A two-tailed
unpaired t-test comparing Surgery 101 participants vs. Non-Surgery 101 participants was conducted
(t = 2.583, df = 94, p = 0.0113). Individual data points as well as mean ± SEM are shown.
3.2. Surgery 101 is Not Widely Accessible to Potential Participants
Of the 97 survey participants, 33.0% attended Surgery 101 (Figure 3A). The remaining
participants can be sub-divided into those who reported interest in attending the session but were
unable to attend for various reasons (38.1%) and those who were not interested in attending Surgery
101 (28.9%) (Figure 3A). Those who did not attend Surgery 101 were further divided based on their
reason for not attending (Figure 3B). Of those who reported interest in attending, the majority (40.0%)
expressed that they were unaware of the Surgery 101 program (Figure 3B). The remainder reported
that they were unable to attend due to their distance from the hospital or to scheduling conflicts
(Figure 3B). Of those who attended Surgery 101, the majority (77.8%) had to take time off work to do
so, which is an identified barrier to physically attending Surgery 101. Most participants who reported
they were not interested in attending Surgery 101 were also unaware of the program and only 7.7%
of those who did not attend Surgery 101 knew about the program and made the choice to not attend
(Figure 3B). Overall, 57% of families who did not attend the Surgery 101 program reported that they
were interested in attending but were unable to for various reasons. These data provide evidence that
many families who may have benefitted from the Surgery 101 program were unable to utilize this
resource.
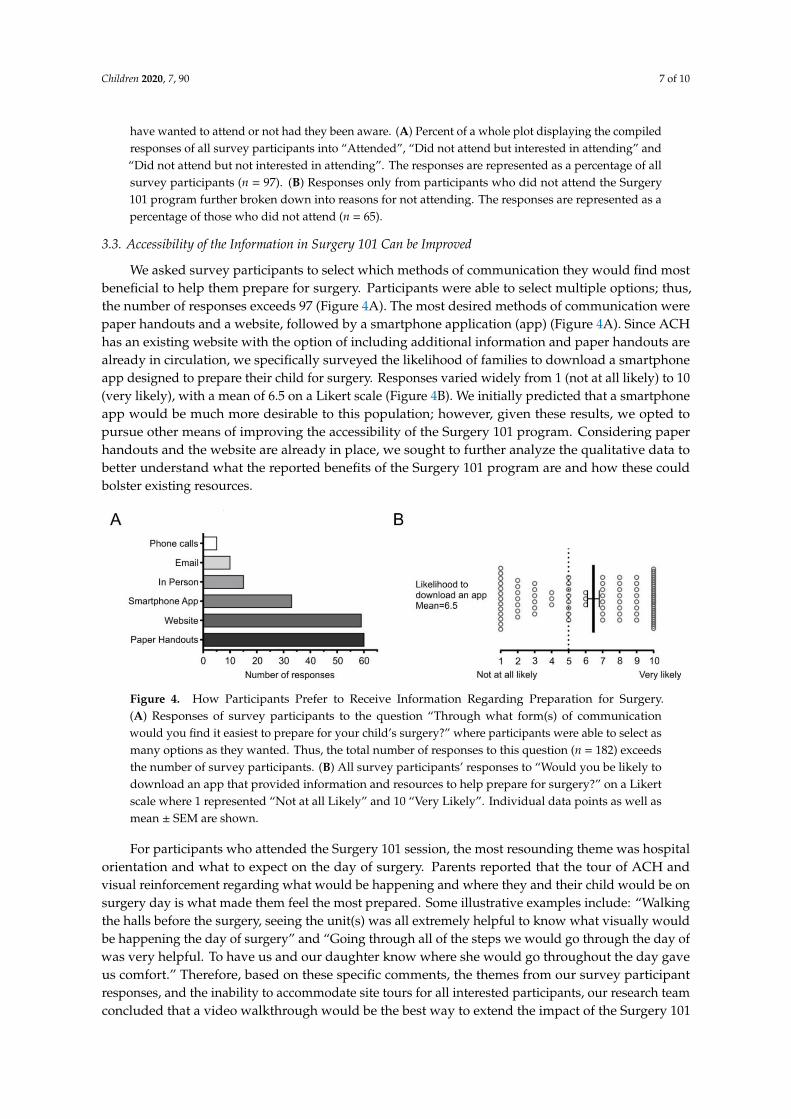
Figure 3. Participation in the Surgery 101 Program. Responses of all survey participants to the
question “Did you participate in the Surgery 101 program?” where responses included options that
specified why they were unable to attend, whether they were aware of the program, and whether
they would have wanted to attend or not had they been aware. (A) Percent of a whole plot displaying
the compiled responses of all survey participants into “Attended”, “Did not attend but interested in
attending” and “Did not attend but not interested in attending”. The responses are represented as a
percentage of all survey participants (n = 97). (B) Responses only from participants who did not attend
the Surgery 101 program further broken down into reasons for not attending. The responses are
represented as a percentage of those who did not attend (n = 65).
3.3. Accessibility of the Information in Surgery 101 Can be Improved
We asked survey participants to select which methods of communication they would find most
beneficial to help them prepare for surgery. Participants were able to select multiple options; thus,
the number of responses exceeds 97 (Figure 4A). The most desired methods of communication were
Figure 3. Participation in the Surgery 101 Program. Responses of all survey participants to the question“Did you participate in the Surgery 101 program?” where responses included options that specifiedwhy they were unable to attend, whether they were aware of the program, and whether they would
Children 2020, 7, 90 7 of 10
have wanted to attend or not had they been aware. (A) Percent of a whole plot displaying the compiledresponses of all survey participants into “Attended”, “Did not attend but interested in attending” and“Did not attend but not interested in attending”. The responses are represented as a percentage of allsurvey participants (n = 97). (B) Responses only from participants who did not attend the Surgery101 program further broken down into reasons for not attending. The responses are represented as apercentage of those who did not attend (n = 65).
3.3. Accessibility of the Information in Surgery 101 Can be Improved
We asked survey participants to select which methods of communication they would find mostbeneficial to help them prepare for surgery. Participants were able to select multiple options; thus,the number of responses exceeds 97 (Figure 4A). The most desired methods of communication werepaper handouts and a website, followed by a smartphone application (app) (Figure 4A). Since ACHhas an existing website with the option of including additional information and paper handouts arealready in circulation, we specifically surveyed the likelihood of families to download a smartphoneapp designed to prepare their child for surgery. Responses varied widely from 1 (not at all likely) to 10(very likely), with a mean of 6.5 on a Likert scale (Figure 4B). We initially predicted that a smartphoneapp would be much more desirable to this population; however, given these results, we opted topursue other means of improving the accessibility of the Surgery 101 program. Considering paperhandouts and the website are already in place, we sought to further analyze the qualitative data tobetter understand what the reported benefits of the Surgery 101 program are and how these couldbolster existing resources.
Children 2020, 7, x FOR PEER REVIEW 7 of 10
paper handouts and a website, followed by a smartphone application (app) (Figure 4A). Since ACH
has an existing website with the option of including additional information and paper handouts are
already in circulation, we specifically surveyed the likelihood of families to download a smartphone
app designed to prepare their child for surgery. Responses varied widely from 1 (not at all likely) to
10 (very likely), with a mean of 6.5 on a Likert scale (Figure 4B). We initially predicted that a
smartphone app would be much more desirable to this population; however, given these results, we
opted to pursue other means of improving the accessibility of the Surgery 101 program. Considering
paper handouts and the website are already in place, we sought to further analyze the qualitative
data to better understand what the reported benefits of the Surgery 101 program are and how these
could bolster existing resources.
Figure 4. How Participants Prefer to Receive Information Regarding Preparation for Surgery. (A)
Responses of survey participants to the question “Through what form(s) of communication would
you find it easiest to prepare for your child’s surgery?” where participants were able to select as many
options as they wanted. Thus, the total number of responses to this question (n = 182) exceeds the
number of survey participants. (B) All survey participants’ responses to “Would you be likely to
download an app that provided information and resources to help prepare for surgery?” on a Likert
scale where 1 represented “Not at all Likely” and 10 “Very Likely”. Individual data points as well as
mean ± SEM are shown.
For participants who attended the Surgery 101 session, the most resounding theme was hospital
orientation and what to expect on the day of surgery. Parents reported that the tour of ACH and
visual reinforcement regarding what would be happening and where they and their child would be
on surgery day is what made them feel the most prepared. Some illustrative examples include:
“Walking the halls before the surgery, seeing the unit(s) was all extremely helpful to know what
visually would be happening the day of surgery” and “Going through all of the steps we would go
through the day of was very helpful. To have us and our daughter know where she would go
throughout the day gave us comfort.” Therefore, based on these specific comments, the themes from
our survey participant responses, and the inability to accommodate site tours for all interested
participants, our research team concluded that a video walkthrough would be the best way to extend
the impact of the Surgery 101 program. We created a video depicting a family’s experience on surgery
day, which is now available on the ACH website (https://youtu.be/RQ5Xl6EDOlw). We believe that
this video will be one of the first steps in improving patient and family’s experiences and reducing
pre-operative anxiety.
Although not the primary objective, our thematic analysis also generated data on areas for
improvement both within the Surgery 101 program and for the overall surgical process at ACH
(Figure 1). Identified as the main areas of improvement were general post-surgical care, surgery-
specific care, and resources for families within the day surgery unit. The possibility of including post-
surgical care in a smartphone app remains a future goal.
4. Discussion
We found that the in-hospital Surgery 101 program improves family and child preparedness for
surgery at ACH and is well regarded by those who have attended it. With the evolution of patient-
Figure 4. How Participants Prefer to Receive Information Regarding Preparation for Surgery.(A) Responses of survey participants to the question “Through what form(s) of communicationwould you find it easiest to prepare for your child’s surgery?” where participants were able to select asmany options as they wanted. Thus, the total number of responses to this question (n = 182) exceedsthe number of survey participants. (B) All survey participants’ responses to “Would you be likely todownload an app that provided information and resources to help prepare for surgery?” on a Likertscale where 1 represented “Not at all Likely” and 10 “Very Likely”. Individual data points as well asmean ± SEM are shown.
For participants who attended the Surgery 101 session, the most resounding theme was hospitalorientation and what to expect on the day of surgery. Parents reported that the tour of ACH andvisual reinforcement regarding what would be happening and where they and their child would be onsurgery day is what made them feel the most prepared. Some illustrative examples include: “Walkingthe halls before the surgery, seeing the unit(s) was all extremely helpful to know what visually wouldbe happening the day of surgery” and “Going through all of the steps we would go through the day ofwas very helpful. To have us and our daughter know where she would go throughout the day gaveus comfort.” Therefore, based on these specific comments, the themes from our survey participantresponses, and the inability to accommodate site tours for all interested participants, our research teamconcluded that a video walkthrough would be the best way to extend the impact of the Surgery 101

Children 2020, 7, 90 8 of 10
program. We created a video depicting a family’s experience on surgery day, which is now availableon the ACH website (https://youtu.be/RQ5Xl6EDOlw). We believe that this video will be one of thefirst steps in improving patient and family’s experiences and reducing pre-operative anxiety.
Although not the primary objective, our thematic analysis also generated data on areas forimprovement both within the Surgery 101 program and for the overall surgical process at ACH(Figure 1). Identified as the main areas of improvement were general post-surgical care, surgery-specificcare, and resources for families within the day surgery unit. The possibility of including post-surgicalcare in a smartphone app remains a future goal.
4. Discussion
We found that the in-hospital Surgery 101 program improves family and child preparednessfor surgery at ACH and is well regarded by those who have attended it. With the evolution ofpatient-centered care, there has been a major shift to promote education and patient empowerment inthe decision-making process. In pediatric medicine, parental education has traditionally been a focus.However, there is tremendous value in incorporating educational elements, specifically for the child.We identified surgery as an area where family education would be beneficial and effective due to thehigh degree of stress and anxiety [4]. In addition, evidence has shown that patient education prior tosurgery is limited [6,7].
Given that most surgeries are scheduled in advance [8], there is time to improve patient andfamily education pre-operatively, improving the perioperative experience. Several existing studieshave explored specific components of pediatric surgical preparation, including assessing differentmodalities for providing information [9], anesthesiology-specific preparation [10] as well as the impactof pre-operative anxiety [11]. We specifically sought to assess the impact of an in-person orientationsession and collect feedback from families at ACH. Our quantitative and qualitative results supportthe benefit of a program such as Surgery 101 to both parents and patients. This information guided ourdecision to develop additional resources to reach more families; however, it also suggests that similarprograms would be beneficial at other Canadian Pediatric Hospitals.
The major barriers identified to accessing Surgery 101 were a lack of awareness, difficulty withaccess due to parental work schedules, and physical distance from hospital. To address the lack ofawareness, we examined the existing Surgery 101 paper handouts with the Child Life Specialistsat ACH and determined that these pre-operative packages were reaching all clinics in the hospital.We also learned that a revised website was underway for ACH. Therefore, we chose to develop anovel resource that could be electronically distributed and could be used to enhance the new ACHwebsite. This was an online video that provides a walkthrough of what patients and families areto expect when travelling to ACH for surgery (https://youtu.be/RQ5Xl6EDOlw). This video versioncovers key aspects of the Surgery 101 program and confers many advantages. Firstly, it provides acost-effective alternative to families who were not able to attend Surgery 101 due to distance fromthe hospital or who needed to take time off from work. Secondly, an electronic resource can be moreeasily disseminated and may therefore reach families who were not aware of the Surgery 101 program.Finally, this video provides advantages for specific sub-populations of patients. A hypothesis wheninitiating this study was that additional resources would positively impact children with high levels ofanxiety or with existing conditions such as Autism Spectrum Disorder. This theme was also identifiedby survey participants; “[My son] is not an overly anxious child but for children that are, [Surgery 101]would be a must.” We do not anticipate that an online video will discourage families from attendingthe in-hospital Surgery 101 program but believe it will provide an added benefit to review the Surgery101 program at their leisure. Child Life Specialists also reported that older patients typically do notfeel comfortable attending Surgery 101 and our data show that the oldest patient to attend Surgery101 and complete our survey was 12 years old. Child Life offers one-on-one Surgery 101 sessions forteenagers; however, an online video is an additional resource that teenagers can access without unduesocial stressors.

Children 2020, 7, 90 9 of 10
We predicted that a smartphone app would be more desirable to families preparing for surgery.Some of the concerns with the use of a smartphone app included the need to find and downloadthe app for one-time and short-term use, the need to develop it across multiple platforms, and theutility of an app targeted to one centre. Since our thematic analysis identified a major theme of beingable to visually see where to go on the day of surgery, we felt it was appropriate to focus on anACH-specific resource. We found that a variety of generic (non-site specific) applications or onlinevideos are available for surgical preparation [12–14] and we are continuing to explore options forfurther development of a site-specific app. A strength of our study was the ability to directly comparea family’s sense of preparedness for surgery with and without accessing the in-person Surgery 101program. This allowed us to assess the Surgery 101 content as additional valuable content to makemore widely accessible.
Some limitations of our study included a limited sample size as well as targeted recruitmentthrough our e-mail list to families who had agreed in advance to participate in research and maybe more involved with the hospital. However, our posters and recruitment in the day surgery areareached all families. Since the study was voluntary, those who chose to complete it may have beenmore likely to require additional preparation for surgery or have additional perioperative anxiety andmay have been more likely to spend longer times in the hospital contributing to our high numberof patients staying >24 h. The survey tool used in this study was not previously validated and mayhave benefited from specific questions regarding the development of a video. In addition, since 19.6%of participants completed the survey >12 months after their surgery date, their responses may havebeen impacted by recall bias. We were also not able to collect an equal distribution of Surgery 101 andnon-Surgery 101 participants, as indicated in our statistical power calculation.
To best improve the accessibility of Surgery 101 and reach families who are unable to attend thein-hospital session, we have created a video summary of surgery day, which is available on the ACHwebsite. We believe that this video, as well as ongoing efforts to improve family preparation prior tosurgery, will enhance the experiences of patients and families undergoing surgery.
Supplementary Materials: The following are available online at http://www.mdpi.com/2227-9067/7/8/90/s1,Supplementary Figure S1: Survey Questions.
Author Contributions: Conceptualization, C.N., H.L.-P., L.B.-G., N.R. & K.C.; methodology, C.N., H.L.-P.,L.B.-G., N.R. & K.C.; software, C.N. & H.L.-P.; validation, C.N., H.L.-P., L.B.-G., N.R. & K.C.; formal analysis,C.N. & H.L.-P.; investigation, C.N. & H.L.-P.; resources, C.N., H.L.-P., L.B.-G., N.R. & K.C.; data curation,C.N. & H.L.-P.; writing—original draft preparation, C.N. & H.L.-P.; writing—review and editing, C.N., H.L.-P.,L.B.-G., N.R. & K.C.; visualization, C.N. & H.L.-P.; supervision, N.R. and K.C.; project administration, L.B.-G.;funding acquisition, C.N., H.L.-P., N.R. & K.C. All authors have read and agreed to the published version ofthe manuscript.
Funding: This research was supported by an Alberta Children’s Hospital Research Institute Small Grant (C.N.,H.L.P., L.B.G., N.R. & K.C.). This research was supported by MD/PhD funding to C.N. and H.L.P. from the AlbertaInnovates—Health Solutions MD/PhD Studentship.
Acknowledgments: We thank Karen Stetar for administrative assistance during the study.
Conflicts of Interest: The authors declare no conflict of interest and that the research was conducted in the absenceof any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Canadian Medical Protective Association. Surgical Safety in Canada: A 10-Year Review of CMPA and HIROCMedico-Legal Data. Available online: https://www.patientsafetyinstitute.ca/en/toolsResources/Surgical-Safety-in-Canada/Pages/default.aspx (accessed on 1 June 2020).
2. Wright, J.G.; Menaker, R.J.; Houle, A.M.; Leclerc, S.; Mayer, S.K.; Willis, B.; Corsten, G.; Blair, G.K.; Jones, S.;Hyndman, W.; et al. Waiting for children’s surgery in Canada: The Canadian Paediatric Surgical Wait Timesproject. Can. Med. Assoc. J. 2011, 183, E559–E564. [CrossRef] [PubMed]
3. Visintainer, M.A.; Wolfer, J.A. Psychological Preparation for Surgical Pediatric Patients: The Effect onChildren’s and Parents’ Stress Responses and Adjustment. Pediatrics 1975, 56, 187–202. [CrossRef] [PubMed]
https://www.patientsafetyinstitute.ca/en/toolsResources/Surgical-Safety-in-Canada/Pages/default.aspx
Children 2020, 7, 90 10 of 10
4. Kain, Z.N.; Mayes, L.C.; O’Connor, T.Z.; Cicchetti, D.V. Preoperative anxiety in children: Predictors andoutcomes. Arch. Pediatr. Adolesc. Med. 1996, 150, 1238–1245. [CrossRef] [PubMed]
5. Kain, Z.N.; Mayes, L.C.; Caldwell-Andrews, A.A.; Karas, D.E.; McClain, B.C. Preoperative anxiety,postoperative pain, and behavioral recovery in young children undergoing surgery. Pediatrics 2006,118, 651–658. [CrossRef] [PubMed]
6. Grocott, M.P.W.; Plumb, J.O.M.; Edwards, M.; Fecher-Jones, I.; Levett, D.Z.H. Re-designing the pathway tosurgery: Better care and added value. Perioper. Med. 2017, 6, 1–7. [CrossRef] [PubMed]
7. Rankinen, S.; Salanterä, S.; Heikkinen, K.; Johansson, K.; Kaljonen, A.; Virtanen, H.; Leino-Kilpi, H.Expectations and received knowledge by surgical patients. Int. J. Qual. Health Care 2007, 19, 113–119.[CrossRef] [PubMed]
8. Mullen, M.G.; Michaels, A.D.; Mehaffey, H.J.; Guidry, C.A.; Turrentine, L.E.; Hedrick, T.L.; Friel, C.M.Risk associated with complications and mortality after urgent surgery vs elective and emergency surgery:Implications for defining “quality” and reporting outcomes for urgent surgery. JAMA Surg. 2017, 152,768–774. [CrossRef] [PubMed]
9. Fernandes, S.C.; Arriaga, P.; Esteves, F. Providing preoperative information for children undergoing surgery:A randomized study testing different types of educational material to reduce children’s preoperative worries.Health Educ. Res. 2014, 29, 1058–1076. [CrossRef] [PubMed]
10. Bogusaite, L.; Razlevice, I.; Lukosiene, L.; Macas, A. Evaluation of preoperative information needs in pediatricanesthesiology. Med. Sci. Monit. 2018, 24, 8773–8780. [CrossRef] [PubMed]
11. Kain, Z.N.; Caldwell-Andrews, A.A.; Mayes, L.C.; Weinberg, M.E.; Wang, S.M.; MacLaren, J.E.; Blount, R.L.Family-centered preparation for surgery improves perioperative outcomes in children: A randomizedcontrolled trial. Anesthesiology 2007, 106, 65–74. [CrossRef] [PubMed]
12. Warnock, G.L. The use of apps in surgery. Can. J. Surg. 2012, 55, 77. [CrossRef] [PubMed]13. Stewart, J.J.; Fayed, I.; Henault, S.; Kalantar, B.; Voyadzis, J.-M. Use of a Smartphone Application for Spine
Surgery Improves Patient Adherence with Preoperative Instructions and Decreases Last-minute SurgeryCancellations. Cureus 2019, 11, e4192. [CrossRef] [PubMed]
14. Herrera-Usagre, M.; Santana, V.; Burgos-Pol, R.; Oliva, J.P.; Sabater, E.; Rita-Acosta, M.; Casado, M.A.;Cruces, S.; Pacheco, M.; Perez, C.S. Effect of a mobile app on preoperative patient preparation for majorambulatory surgery: Protocol for a randomized controlled trial. J. Med. Internet Res. 2019, 21, e10938.[CrossRef] [PubMed]
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open accessarticle distributed under the terms and conditions of the Creative Commons Attribution(CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Related Documents











