Menu Diseases of the Adrenal Gland Adriana G. Ioachimescu Amir H. Hamrahian Back to Top Anatomy and Physiology of the Adrenal Glands Each adrenal consists of two functionally distinct endocrine glands: the cortex, derived from mesenchymal cells, and the medulla, derived from neuroectodermal cells. The adrenal cortex consists of three concentric zones: The outer glomerulosa secretes the mineralocorticoid aldosterone, the intermediate fasciculata secretes cortisol, and the inner reticularis secretes androgens. The endocrine cells of the adrenal medulla are the chromaffin cells, which are part of the sympathetic nervous system and produce the catecholamine epinephrine. Back to Top Adrenal Insufficiency Etiology Glucocorticoid insufficiency can be primary, resulting from the direct insult to the adrenal cortex, or secondary, from adrenocorticotropic hormone (ACTH) or corticotropin-releasing hormone (CRH) hyposecretion as a result of pituitary or hypothalamic dysfunctions. Primary adrenal insufficiency affects glucocorticoid and mineralocorticoid secretion and may be fatal if untreated. Autoimmune destruction of the adrenal glands (Addison’s disease) is the most common cause of primary adrenal insufficiency in United States (70%-90%), whereas tuberculosis is now the second most common cause worldwide. Some other causes of primary adrenal insufficiency include bilateral adrenal hemorrhage, drugs (e.g., mitotane, etomidate, ketoconazole) and other infectious diseases (e.g., HIV infection, disseminated histoplasmosis, paracoccidiomycosis). HIV infection may result in both primary and secondary adrenal insufficiencies (AI). Addison’s disease may coexist with other autoimmune conditions, such as type 1 diabetes, hypothyroidism, or hypoparathyroidism. Secondary and tertiary adrenal insufficiencies occur commonly after the discontinuation of glucocorticoids. Less frequently, ACTH deficiency may be caused by pituitary macroadenomas, pituitary surgery or radiation, and parasellar diseases. Megestrol acetate, an appetite stimulator used in some patients with advanced cancer or cachexia related to AIDS may be associated with secondary AI. Tertiary adrenal insufficiency results from the inadequate secretion of CRH. Secondary and tertiary adrenal insufficiencies only affect cortisol secretion, because ACTH has only a minor role in regulation of aldosterone secretion. Manifestations Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement... 1 of 25 11/12/2013 5:35 PM

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Menu
Diseases of the Adrenal GlandAdriana G. IoachimescuAmir H. Hamrahian
Back to Top
Anatomy and Physiology of the Adrenal Glands
Each adrenal consists of two functionally distinct endocrine glands: the cortex, derived from mesenchymalcells, and the medulla, derived from neuroectodermal cells. The adrenal cortex consists of three concentriczones: The outer glomerulosa secretes the mineralocorticoid aldosterone, the intermediate fasciculata secretescortisol, and the inner reticularis secretes androgens. The endocrine cells of the adrenal medulla are thechromaffin cells, which are part of the sympathetic nervous system and produce the catecholamineepinephrine.
Back to Top
Adrenal Insufficiency
Etiology
Glucocorticoid insufficiency can be primary, resulting from the direct insult to the adrenal cortex, orsecondary, from adrenocorticotropic hormone (ACTH) or corticotropin-releasing hormone (CRH)hyposecretion as a result of pituitary or hypothalamic dysfunctions.
Primary adrenal insufficiency affects glucocorticoid and mineralocorticoid secretion and may be fatal ifuntreated. Autoimmune destruction of the adrenal glands (Addison’s disease) is the most common cause ofprimary adrenal insufficiency in United States (70%-90%), whereas tuberculosis is now the second mostcommon cause worldwide. Some other causes of primary adrenal insufficiency include bilateral adrenalhemorrhage, drugs (e.g., mitotane, etomidate, ketoconazole) and other infectious diseases (e.g., HIVinfection, disseminated histoplasmosis, paracoccidiomycosis). HIV infection may result in both primary andsecondary adrenal insufficiencies (AI). Addison’s disease may coexist with other autoimmune conditions,such as type 1 diabetes, hypothyroidism, or hypoparathyroidism.
Secondary and tertiary adrenal insufficiencies occur commonly after the discontinuation of glucocorticoids.Less frequently, ACTH deficiency may be caused by pituitary macroadenomas, pituitary surgery or radiation,and parasellar diseases. Megestrol acetate, an appetite stimulator used in some patients with advanced canceror cachexia related to AIDS may be associated with secondary AI. Tertiary adrenal insufficiency results fromthe inadequate secretion of CRH. Secondary and tertiary adrenal insufficiencies only affect cortisol secretion,because ACTH has only a minor role in regulation of aldosterone secretion.
Manifestations
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
1 of 25 11/12/2013 5:35 PM
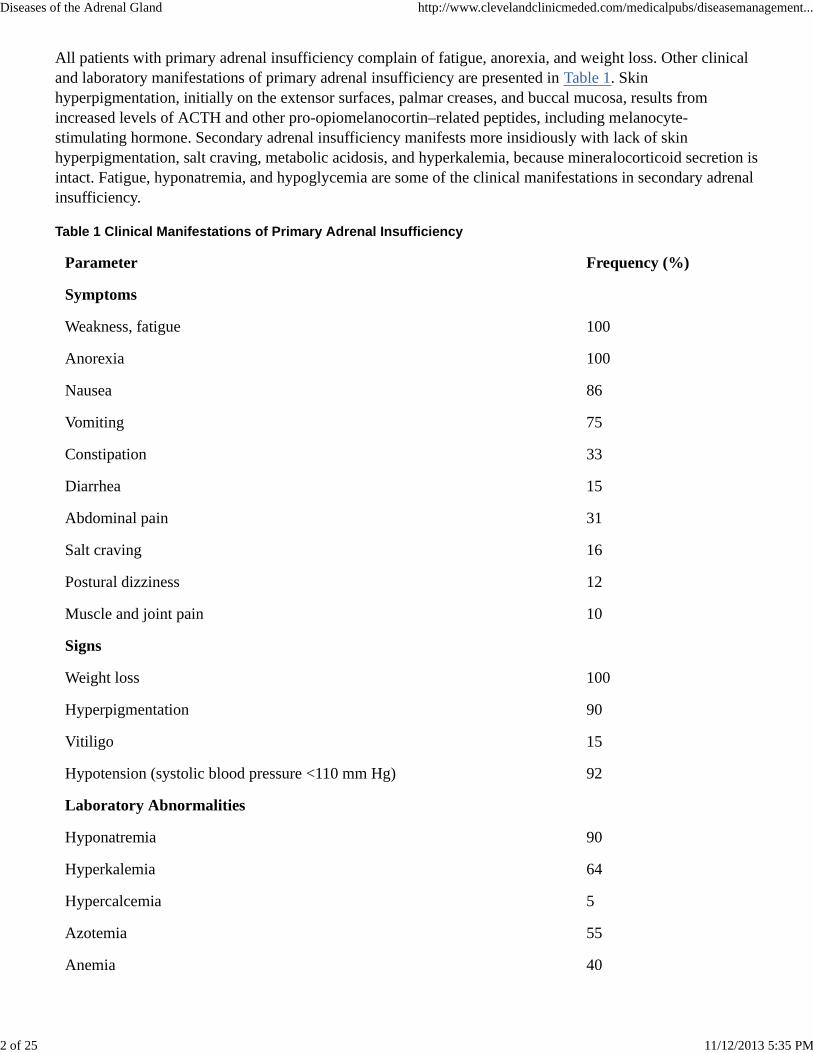
All patients with primary adrenal insufficiency complain of fatigue, anorexia, and weight loss. Other clinicaland laboratory manifestations of primary adrenal insufficiency are presented in Table 1. Skinhyperpigmentation, initially on the extensor surfaces, palmar creases, and buccal mucosa, results fromincreased levels of ACTH and other pro-opiomelanocortin–related peptides, including melanocyte-stimulating hormone. Secondary adrenal insufficiency manifests more insidiously with lack of skinhyperpigmentation, salt craving, metabolic acidosis, and hyperkalemia, because mineralocorticoid secretion isintact. Fatigue, hyponatremia, and hypoglycemia are some of the clinical manifestations in secondary adrenalinsufficiency.
Table 1 Clinical Manifestations of Primary Adrenal Insufficiency
Parameter Frequency (%)
Symptoms
Weakness, fatigue 100
Anorexia 100
Nausea 86
Vomiting 75
Constipation 33
Diarrhea 15
Abdominal pain 31
Salt craving 16
Postural dizziness 12
Muscle and joint pain 10
Signs
Weight loss 100
Hyperpigmentation 90
Vitiligo 15
Hypotension (systolic blood pressure <110 mm Hg) 92
Laboratory Abnormalities
Hyponatremia 90
Hyperkalemia 64
Hypercalcemia 5
Azotemia 55
Anemia 40
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
2 of 25 11/12/2013 5:35 PM
Eosinophilia 17
Evaluation
Evaluating a patient with suspected adrenal insufficiency is a three-step process: establishing the diagnosis,differentiating between primary and secondary adrenal insufficiencies, and looking for the cause of adrenalinsufficiency.
Establishing the Diagnosis. Because of circadian secretion of cortisol and overlap among patients withadrenal insufficiency and those with normal adrenal function, determining the random serum cortisol level isonly of value during stress (see later, “Adrenal Insufficiency in the Critically Ill Patient”). An algorithm forthe evaluation of adrenal function is shown in Figure 1. An early morning (8 am) plasma cortisol level lowerthan 3 μg/dL confirms adrenal insufficiency, whereas a value higher than 15 μg/dL makes the diagnosishighly unlikely. Cortisol levels in the range of 3 to 15 μg/dL may be seen in patients with primary, secondary,or tertiary adrenal insufficiency.
These patients should be further evaluated by the cosyntropin (Cortrosyn) stimulation test (CST), which canbe performed at any time during the day. The standard-dose CST uses an intravenous or intramuscularinjection of 250 μg cosyntropin with plasma cortisol before and 30 and 60 minutes after the injection. Anormal response is a plasma cortisol concentration higher than 18 μg/dL at 30 minutes. Most individuals withnormal adrenal function achieve much higher cortisol levels at 60 minutes after cosyntropin injection. For thisreason, the 18 μg/dL cutoff value should be applied only for the 30-minute cortisol level. The standard-doseCST is excellent for excluding primary adrenal insufficiency. However, patients with mild partial orrecent-onset pituitary ACTH or hypothalamic CRH deficiency (e.g., within 2-4 weeks after pituitary surgery)may have a normal response to 250 μg of cosyntropin in the CST, because the adrenal glands have notundergone significant atrophy and will still respond to very high concentrations of ACTH stimulation. Thesensitivity of CST to pick up mild adrenal insufficiency improves when using the low-dose CST (1 μgACTH1-2 given intravenously); however, this may result in a higher false-positive rate. The lack of acommercially available 1-μg cosyntropin dose may be a potential for error. In most clinical situations, the30-minute cortisol value during a standard-dose CST has a diagnostic accuracy close to that of a low-doseCST.1
The insulin tolerance test (ITT) and metyrapone test are generally used for the evaluation of patientssuspected to have secondary adrenal insufficiency. ITT is considered the gold standard test for the evaluationof hypothalamic-pituitary-adrenal (HPA) axis. The ITT is contraindicated in older patients (>65 years) andthose with acute illness, seizure disorders, or cardiovascular-cerebrovascular disease. The result of themetyrapone test has been validated compared with the ITT. Metyrapone blocks the final step in cortisolbiosynthesis, resulting in a reduction in cortisol secretion, which in turn stimulates ACTH secretion. Thisleads to higher levels of 11-deoxycortisol, which is the precursor to cortisol.
The CRH stimulation test requires intact pituitary and adrenal glands for a response. The test has not beenwell validated for the evaluation of adrenal function and its current role in the evaluation of adrenal functionis limited to research protocols.
Differentiation Between Primary and Secondary Adrenal Insufficiencies. This is done through themeasurement of the basal plasma ACTH level. An elevated ACTH level is consistent with primary adrenalinsufficiency. A low or normal-range ACTH level, with a low cortisol level, confirms the diagnosis ofsecondary or tertiary adrenal insufficiency.
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
3 of 25 11/12/2013 5:35 PM
Determining the Cause of Adrenal Insufficiency. When the biochemical workup is consistent with primaryadrenal insufficiency, computed tomography (CT) scanning of the adrenal glands may help with thedifferential diagnosis. Enlarged adrenal glands or calcifications suggest an infectious, hemorrhagic, ormetastatic cause. In rare circumstances, CT-guided percutaneous fine-needle aspiration of enlarged adrenalglands may help establish the diagnosis. Patients with tuberculous adrenal insufficiency usually haveevidence of active systemic disease. When the biochemical work up suggests secondary or tertiary adrenalinsufficiency, magnetic resonance imaging (MRI) of the pituitary gland is indicated if glucocorticoid therapyas the cause of the secondary adrenal insufficiency has been ruled out.
Treatment
Patients with Addison’s disease require lifelong replacement with glucocorticoids and mineralocorticoids.The minimal dosage to treat symptoms should be used, starting with hydrocortisone, 12.5 to 15 mg in themorning, and 2.5 to 5 mg at noon to mimic the physiologic pattern. Some patients may need another dose of2.5 to 5 mg hydrocortisone at about 6 pm if fatigue continues later in the day. Patients require fludrocortisone,0.05 to 0.2 mg, for mineralocorticoid replacement. The dose is adjusted based on clinical status, including thepresence or absence of orthostatic hypotension, hypertension, and electrolyte imbalance. Patients may need todouble the dose of fludrocortisone or increase salt intake during the summer, when the weather is hot. Patientswith secondary or tertiary adrenal insufficiency do not need mineralocorticoid replacement.
During minor illness (e.g., flu or fever >38° C [100.4° F]) the hydrocortisone dose should be doubled for 2 or3 days. The inability to ingest hydrocortisone tablets warrants parenteral administration. Most patients can beeducated to self administer hydrocortisone, 100 mg IM, and reduce the risk of an emergency room visit.Hydrocortisone, 75 mg/day, provides adequate glucocorticoid coverage for outpatient surgery. Parenteralhydrocortisone, 150 to 200 mg/day (in three or four divided doses), is needed for major surgery, with a rapidtaper to normal replacement during the recovery. Patients taking more than 100 mg hydrocortisone/day do notneed any additional mineralocorticoid replacement. All patients should wear some form of identificationindicating their adrenal insufficiency status.
Adrenal Crisis
Acute adrenal insufficiency (adrenal crisis) is a life-threatening emergency, which usually manifests withnausea, vomiting, abdominal pain, and shock. Patients may be previously undiagnosed or have chronicprimary adrenal insufficiency, with no or inadequate glucocorticoid replacement. Abdominal tenderness andfever are common findings, and adrenal crisis may manifest as an acute abdomen. In these cases, surgicalexploration without glucocorticoid coverage can be lethal. The major hormonal factor precipitating adrenalcrisis is mineralocorticoid deficiency. Therefore, adrenal crisis rarely occurs with secondary adrenalinsufficiency.
Treatment of adrenal crisis should not be delayed. Diagnostic workup in a patient with no history of AIshould include a plasma sample for cortisol and ACTH level determination, immediately followed by an IVbolus of hydrocortisone, 100 mg, and adequate fluid replacement (normal saline). Hydrocortisone should becontinued, 50 mg every 8 hours, while awaiting laboratory results.
Adrenal Insufficiency in the Critically Ill Patient
The overall incidence of AI in critically ill patients is less than 10%, but an incidence as high as 50% in apatient with septic shock has been reported. The concept of total adrenal insufficiency has gradually been
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
4 of 25 11/12/2013 5:35 PM
replaced by relative adrenal insufficiency, which may be fatal in critically ill patients. Hypotension in patientswith adrenal insufficiency may mimic hypovolemic or septic shock and should be considered in thedifferential diagnosis. Serial follow-up of adrenal function in critically patients with clinical featuressuggestive of AI is recommended.
Intensive care unit (ICU) patients with hemodynamic instability, despite fluid resuscitation (especially in thepresence of shock), should be tested for AI. A random serum cortisol level determination and the standardCST are the two commonly used tests for evaluating adrenal function in these patients. However, the cortisollevel that reflects an adequate response is uncertain. In critically ill patients with near-normal albumin levels(>2.5 g/dL), a random plasma cortisol level lower than 15 μg/dL, and a maximum cortisol level lower than20 μg/dL during the CST strongly suggest adrenal insufficiency. In patients with equivocal biochemicalresults, a trial of 2 or 3 days of stress dosage glucocorticoids is appropriate, as long as it will be discontinuedin the absence of any significant hemodynamic improvement. The value of the delta cortisol during the CST(stimulated minus basal cortisol levels) of 9 μg/dL or lower as an indicator of partial AI during septic shock isa matter of debate and does not have strong literature support.
More than 90% of circulating cortisol is bound to cortisol- binding globulin (CBG) and albumin. Free cortisolis biologically active. During severe illness caused by a marked decrease in the CBG level, albumin has amore significant influence on the total concentration of cortisol. Critically ill patients with significanthypoalbuminemia (albumin level >2.5 g/dL) have subnormal serum total cortisol concentrations, but theirbaseline or cosyntropin-stimulated serum free cortisol level is in the high-normal range or elevated.3 Inpatients with hypoalbuminemia, total serum cortisol is a poor indicator of glucocorticoid activity. Studies areneeded to establish normative ranges for free cortisol for different levels of stress, including septic shock.3
Hydrocortisone, 50 mg IV every 6 to 8 hours is an adequate replacement dose for critically ill patients withsuspected adrenal insufficiency. Treatment with this dose should be continued for 2 or 3 days. Afterhemodynamic improvement, a gradual taper of hydrocortisone, depending on the patient’s condition, shouldbe instituted. A subset of patients with septic shock may benefit from physiologic stress dose glucocorticoids.Such therapy has not yet been proven to be effective and safe in all patients with septic shock. Lifelongglucocorticoid replacement therapy should not be sanctioned on the basis of an equivocal biochemical testresult in an acutely ill patient. Adrenal function should be re-evaluated after recovery from acute illness.
Summary
Autoimmune destruction of the adrenal glands is the most common cause of primary adrenalinsufficiency in the United States.Almost all patients with primary adrenal insufficiency present with fatigue, anorexia, and weight loss.Primary and secondary adrenal insufficiencies are differentiated through measurement of the plasmaACTH level.Acute adrenal insufficiency is a medical emergency that should be treated with IV hydrocortisone andfluids as soon as the diagnosis is suspected.Adrenal insufficiency should be suspected in critically ill patients with septic shock or hypotensionrefractory to intravenous fluids and pressors.
Back to Top
Syndromes of Adrenal Hyperfunction
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
5 of 25 11/12/2013 5:35 PM
Diseases related to adrenal hyperfunction are relatively rare, but they have significant mortality and morbidityif untreated. In the following sections, Cushing’s syndrome, primary hyperaldosteronism,pheochromocytoma, and androgen-producing adrenal tumors are reviewed.
Cushing’s Syndrome
Definition and Classification
Cushing’s syndrome (CS) is composed of symptoms and signs associated with prolonged exposure toinappropriately high levels of plasma glucocorticoids. Exogenous glucocorticoid intake is the most commoncause of CS. The endogenous causes are divided into ACTH-dependent and ACTH-independent CS, asshown in Box 1.
Box 1 Etiology of Endogenous Cushing’s Syndrome
ACTH-Dependent
Cushing's syndrome (67%)
Ectopic ACTH secretion (12%)
Ectopic CRH secretion (<1%)
ACTH-Independent
Adrenal adenoma (10%)
Adrenal carcinoma (8%)
Micro-and macronodular adrenal hyperplasias (1%)
ACTH, adrenocorticotropic hormone; CRH, corticotropin-releasing hormone.
Clinical Features
Harvey Cushing initially described the clinical features of CS in the early 20th century, including centripetalobesity, moon face, hirsutism, and plethora; however, such a classic clinical picture is not always present anda high index of suspicion is usually required. Box 2 describes some of the clinical features suggestive of CS.Weight gain is almost always present, except in ectopic ACTH secretion (EAS) caused by malignancy. Thestriae in CS are red-purple and usually wider than 1 cm. The skin is thin and minimal trauma results in easybruising. Patients have a plethoric appearance and acne may be present. Proximal myopathy involving thelower limb and shoulder girdle may be present. Moon face and supraclavicular and dorsocervical fat pads(buffalo hump) are nonspecific and accompany obesity from other causes.
Box 2 Clinical Features Suggestive of Cushing’s Syndrome
Central obesity
Proximal myopathy
Spontaneous bruising
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
6 of 25 11/12/2013 5:35 PM
Facial plethora
Wide purplish striae (>1 cm)
Changes in serial photographs
Hypokalemia
Osteoporosis
Women have menstrual irregularity and hirsutism. Men and women exhibit loss of libido. Agitated depressionand lethargy are among the most common psychiatric abnormalities seen in CS patients, but paranoia andovert psychosis may occur. Irritability is an early symptom and insomnia is common. CS has profound effectson bone, causing poor linear growth in children and osteoporotic vertebral collapse and pathologic fracturesin adults.
Patients with ectopic ACTH syndrome caused by small cell lung carcinoma lack many of the typical clinicalfeatures. The rapid course and high levels of ACTH and cortisol often result in hyperpigmentation, myopathy,peripheral edema, glucose intolerance, and hypokalemic alkalosis. Female patients with adrenal carcinomasoften present with signs and symptoms of virilization (hirsutism and acne), breast atrophy, deepening of thevoice, temporal hair recession, and clitoromegaly caused by hypersecretion of androgens, along with thecortisol.
Pseudo-Cushing’s syndrome refers to features of CS combined with some features of hypercortisolism thatresolve after resolution of the underlying cause, such as psychiatric disorders (e.g., major depression, anxietydisorder, obsessive-compulsive disorder, anorexia nervosa), morbid obesity, poorly controlled diabetes, andchronic alcoholism.
CS as a result of exogenous administration of glucocorticoids must be excluded. The diagnosis of Cushing’ssyndrome then involves two steps: demonstration of inappropriate cortisol secretion and localization of itscause.
Establishing the Diagnosis
Screening for CS may be done by a 24-hour urinary free cortisol (UFC) determination, 1-mg dexamethasonesuppression test (DST), or midnight salivary cortisol test (Fig. 2). Currently, a 24-hour UFC test (withsimultaneous urinary creatinine level measurement) is the most widely used initial screening test but amidnight salivary cortisol determination is becoming a good alternative. An elevated salivary cortisol level inmost cases should be confirmed by a 24-hour UFC test before referral to surgery. A normal sleeping pattern isnecessary for an accurate salivary cortisol level measurement for the evaluation of CS. Values of UFC abovethree or four times upper normal for the assay are usually diagnostic for CS, especially when repeated andconfirmed. In patients with a glomerular filtration rate lower than 20 mL/min, urinary cortisol excretion issignificantly decreased and may thus be normal, despite excessive cortisol production. On the other hand,normal individuals with excess fluid intake (>4 L/day) may have a false elevation of the UFC.
The 1-mg DST is performed by the administration of dexamethasone, 1 mg at 11 pm, followed bymeasurement of the plasma cortisol level at 8 am. A cortisol level lower than 1.8 μg/dL is a normal response.It is an excellent test to rule out CS, with less than a 2% false-negative test result; however, because of a highfalse-positive rate (≤40%), a positive test result needs to be further confirmed by other tests, such as a
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
7 of 25 11/12/2013 5:35 PM
24-hour UFC assay.
During the low-dose DST, dexamethasone, 0.5 mg, is taken orally every 6 hours, for a total of eight doses,starting at 6 am. A cutoff cortisol value of 1.8 μg/dL in the morning (at 7 or 8 am), after the last dose ofdexamethasone at midnight, has been reported to have an excellent sensitivity and specificity of about 98% inthe evaluation of patients suspected to have CS. Measurement of the 24-hour UFC during the second day ofthe low-dose DST is of lesser value, and usually does not add any further to the diagnostic accuracy of thebaseline 24-hour UFC test.
The combined DST-CRH stimulation test may be used for differentiating between CS and pseudo-Cushing’ssyndrome. The test consists of the oral administration of 0.5 mg dexamethasone every 6 hours for eight doses,starting at noon, followed by the IV administration of 100 μg CRH at 8 am (2 hours after the last dose ofdexamethasone). A plasma cortisol level higher than 1.4 μg/dL 15 minutes after the CRH injection stronglysuggests CS.
Certain drugs, such as phenytoin, phenobarbitals, and rifampin, increase the clearance rate of dexamethasone,resulting in false- positive results during a DST. In these cases, it may be necessary to measure the plasmadexamethasone level. It is always important to remember the effect of increased levels of CBG on serumcortisol levels during pregnancy or in women taking estrogens. These states do not affect the 24-hour UFC ormidnight salivary cortisol levels.
Because of the challenging nature of CS, reaching the proper diagnosis requires a stepwise evaluation,knowledge of the limitations of each test, and avoidance of shortcuts (see Fig. 2). Discrepant or inconclusivetest results require re-evaluation of the entire clinical picture and a biochemical workup, because CS is almostalways a progressive disease. Another clinical scenario that may be associated with normal screening tests iscyclic CS, which needs to be ruled out by periodic evaluation. Fortunately, true cyclic CS is a rare condition.
Differential Diagnosis: ACTH-Dependent Versus Primary Adrenal Disease
Once Cushing’s syndrome is biochemically confirmed, the plasma ACTH level should be measured,preferably in the morning. Normal values typically range between 5 and 50 pg/mL. A suppressed or lowACTH level (<10 pg/mL) is consistent with ACTH-independent CS and should be followed by adrenal CTscanning. ACTH values of 10 to 20 pg/mL may be seen in patients with both adrenal and pituitary causes forCS; these patients should undergo a CRH stimulation test. A flat response of ACTH to CRH during the testsuggests an adrenal cause, but a more than 50% increase in the ACTH level during the test is consistent withCushing’s disease. ACTH levels higher than 20 pg/mL suggest ACTH-dependent CS. About 90% of patientswith ACTH-dependent CS have a pituitary cause and the rest are ectopic in origin. Pituitary MRI withgadolinium enhancement should be performed. In patients with ACTH-dependent CS, the presence of apituitary adenoma larger than 6 mm strongly suggests a pituitary origin, but 50% of CS patients do not haveany abnormality on MRI.4 ACTH levels tend to be higher in ectopic CS compared with Cushing’s disease,but there is significant overlap.
A combination of the CRH stimulation test and an overnight high-dose DST are used to differentiate ectopicCS from Cushing’s disease. A more than 50% increase in the ACTH level after the CRH test and more thanan 80% reduction in the morning cortisol level (8-9 am) after taking 8 mg dexamethasone at 11 pm during ahigh-dose DST is consistent with a pituitary source, and in the presence of a pituitary adenoma, almostestablishes the definitive diagnosis of CS. If the CRH stimulation test and DST results are not concordant andMRI does not show a pituitary adenoma, then inferior petrosal sinus sampling to distinguish ectopic fromCushing’s disease is indicated. Localizing tumors that produce ectopic ACTH is accomplished by chest and
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
8 of 25 11/12/2013 5:35 PM
abdominal CT studies, followed by neck CT if no source is found. An octreotide scan may be of some valuein patients with ectopic CS and negative imaging studies.
Treatment
Surgical (trans-sphenoidal) removal of the ACTH-secreting pituitary tumor is the treatment of choice.Experienced neurosurgeons usually achieve 70% to 80% long-term remission rates following surgery. Anundetectable cortisol level postoperatively, when the patient is off glucocorticoids, is considered to be anexcellent indication of long-term cure.
Cushing’s syndrome caused by an adrenal adenoma is usually cured by laparoscopic unilateral adrenalectomy.Adrenal carcinoma is typically an aggressive tumor with a poor prognosis; surgical resection at an early stage,along with lifelong mitotane therapy started soon after surgery, offers the only chance for cure or long-termremission.
Surgical removal of an ectopic ACTH-producing tumor, if possible, results in cure. When the tumor is notresectable, bilateral adrenalectomy is performed to correct hypercortisolemia. Medical therapy withketoconazole, metyrapone, aminoglutethimide, or mitotane may be considered for patients with a limited lifeexpectancy or for alleviation of hypercortisolemic symptoms before surgery.
National Guidelines
During an international workshop in Italy, in October 2002, a relatively comprehensive consensus statementabout the diagnosis and complications of Cushing’s syndrome was published.4 The workshop recommended alow threshold for screening patients for CS, including patients with metabolic syndrome, especially if youngand resistant to conventional treatment. The consensus emphasized that if the diagnosis of Cushing’s issuspected clinically but initial screening tests are normal, the patient should be re-evaluated at a later date andinvasive procedures postponed. A 24-hour UFC assay, overnight 1-mg DST, and midnight salivary cortisoldetermination were described as first-line screening tests for CS. The workshop briefly discussed thepromising results from the midnight salivary cortisol test, which we believe should be part of the diagnosticworkup for most patients suspected to have CS, particularly if early disease is suspected.
Evaluation for the plasma circadian rhythm, midnight plasma cortisol level, 2-day low-dose dexamethasonesuppression test (LDDST), and combined LDDST-CRH test were described by the workshop as second-linescreening tests. In our experiences and in spite of being labor intensive, the combined LDDST-CRH test is ofsignificant value in differentiating CS from pseudo-Cushing’s syndrome. The workshop recommended theuse of bilateral inferior petrosal sinus sampling (BIPSS) in patients whose clinical, biochemical, or radiologicstudy results are discordant or equivocal. We usually carry out BIPSS in most of our patients with ACTH-dependent CS who have no clear adenoma on pituitary MRI. After pituitary tumors are treated, lifelongmedical follow-up is necessary to detect early recurrence, monitor hormone replacement, and treat anycomplications related to the tumor.
Summary
Screening for Cushing’s syndrome may be done by a midnight salivary cortisol level assay, 1-mg DST,or 24-hour urinary free cortisol test.Certain drugs, such as phenytoin, phenobarbitals and rifampin, increase the clearance rate ofdexamethasone, resulting in false-positive results during DSTs.Because of the challenging nature of Cushing’s syndrome, obtaining a proper diagnosis requires a
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
9 of 25 11/12/2013 5:35 PM
stepwise evaluation, knowledge of the limitations of each test, and avoidance of shortcuts.Once Cushing’s syndrome has been biochemically confirmed, the plasma ACTH level should bemeasured to differentiate between ACTH-dependent and ACTH-independent CS.
Primary Hyperaldosteronism
Prevalence and Etiology
Conn first described primary hyperaldosteronism in 1955 in a patient with an adrenal adenoma.Hyperaldosteronism may be more common than once believed. Some investigators have proposed aprevalence as high as 10% in hypertensive patients.5 Women in their fourth to sixth decade of life are affectedmore often than men. A solitary aldosterone-producing adenoma (65%) and bilateral idiopathic hyperplasia(30%) are the most common subtypes of primary aldosteronism. The adenomas are usually benign andsmaller than 2 cm in diameter. Idiopathic adrenal hyperplasia may be accompanied by adrenocortical nodulesand is associated with lower aldosterone levels and less severe hypertension, compared with adenomas.
Two forms of familial hyperaldosteronism (FH) have been described: FH type I and FH type II. FH type I, orglucocorticoid-remediable hyperaldosteronism (GRH), is an autosomal dominant disease characterized by achimeric gene between the 11β-hydroxylase and aldosterone synthase, with varying degrees ofhyperaldosteronism, which responds to exogenous glucocorticoids. FH type II is an autosomal dominantdisorder of both the aldosterone-producing adenoma (APA) and idiopathic hyperaldosteronism (IHA).
Clinical Presentation
The clinical picture varies from asymptomatic to symptoms related to hypertension, hypokalemia, or both.Patients may have headaches, polyuria, nocturia, polydipsia, parasthesias, weakness, and muscle cramps.There are no specific physical findings. The degree of hypertension is usually moderate to severe, and may berefractory to conventional antihypertensive agents. Malignant hypertension and leg edema are rare. The leftventricular hypertrophy is disproportionate to the level of blood pressure and improves after treatment ofhyperaldosteronism, even if hypertension persists.
Routine laboratory tests may show slightly high serum sodium levels (143-147 mEq/L), hyperglycemia,hypokalemia, metabolic alkalosis, and hypomagnesemia. Although most patients with hyperaldosteronism arenot hypokalemic, a low serum potassium level may be noted, either spontaneously or after thiazide or loopdiuretic use. Hypokalemia may be severe and difficult to correct. Its presence reduces the secretion ofaldosterone and thus should be corrected before the laboratory evaluation of hyperaldosteronism.
Diagnosis
The workup of a patient for primary hyperaldosteronism involves the following steps: screening tests forprimary hyperaldosteronism, establishing the autonomy of aldosterone secretion, and determination of thesource of hyperaldosteronism (Fig. 3).
The following categories of patients should be tested with priority for primary hyperaldosteronism:
Hypertensive patients with spontaneous or thiazide-induced hypokalemiaHypertensive patients resistant to therapyHypertensive patients with adrenal incidentalomas
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
10 of 25 11/12/2013 5:35 PM
Screening Tests
Although hypokalemia in a hypertensive patient is suggestive of hyperaldosteronism, normokalemia does notexclude the diagnosis. Up to 60% of patients with hyperaldosteronism do not have hypokalemia. Adequatesodium intake may be necessary to unmask the hypokalemia. Measurement of the 24-hour urinary potassiumlevel can be useful in assessing the cause of a low potassium level, including surreptitious vomiting orlaxative abuse. Inappropriate urinary potassium excretion of more than 30 mEq/24 hours in a patient withhypokalemia suggests primary hyperaldosteronism, especially if plasma renin activity (PRA) is low.
The ratio of the plasma aldosterone concentration (PAC) to PRA (PAC/PRA) is the best screening test forprimary hyperaldosteronism. The test can be done while the patient is on antihypertensive medications(except spironolactone and eplerenone), without requiring postural stimulation. Both spironolactone andeplerenone should be discontinued for 6 weeks before biochemical testing and after the potassium levelreaches the normal range. A PAC/PRA above 20, with a concomitant PAC above 10 ng/dL, needs to bepursued by confirmatory tests (see Fig. 3). Low or suppressed PRA during therapy with angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs) suggests hyperaldosteronism.
Establishing Autonomous Aldosterone Secretion. An elevated PAC/PRA by itself is not diagnostic forhyperaldosteronism and must be confirmed by a 24-hour urinary aldosterone level determined during 4 daysof oral salt loading by adding one flat teaspoon of salt to the meals every day. Diuretics, ACE inhibitors, andARBs should be discontinued for 2 weeks before the tests and potassium needs to be replaced to the normalrange. Hypertension may be controlled by calcium channel blockers, beta blockers, or α1-adrenergic receptorblockers, which do not significantly affect the biochemical workup for hyperaldosteronism. Potassiumsupplementation is stopped in most patients without any underlying heart disease at the beginning of thesalt-loading test. During day 4 of salt loading, a 24-hour urine sample must be collected by the patient foraldosterone, sodium, potassium, and creatinine level testing. A urinary sodium level higher than 200 mEq/24hours confirms an adequate salt load. An aldosterone level higher than 12 μg/day during salt loading is almostalways diagnostic of hyperaldosteronism. Hypokalemia with an inappropriately high urine potassium losssupports the diagnosis. Another supportive measure is correction of hypokalemia with the addition ofaldactone at the end of biochemical workup.
IV administration of 2 L of isotonic saline over 4 hours in the recumbent patient is a less favored way toestablish the diagnosis. A plasma aldosterone level higher than 10 ng/dL at the end of the infusion supportsthe diagnosis of primary hyperaldosteronism. The test may entail risk in older patients, those withuncontrolled hypertension, or those with decompensated heart disease.
Establishing the Source of Aldosterone Excess. Because of differences in therapy, distinguishing analdosterone-producing adenoma APA and idiopathic hyperaldosteronism is important (Table 2). Patients withan APA generally have more severe hypertension, more frequent hypokalemia, higher plasma (>25 ng/dL)and urinary (>30 μg/24 hr) aldosterone levels, and are younger (<50 years). The APA is typically hypodenseand smaller than 2 cm on a CT scan of the adrenals. The presence of a solitary adrenal tumor with a normalcontralateral adrenal gland is usually consistent with an APA. Determination of plasma aldosterone levelsbefore and 2 hours after an upright posture (with ambulation) and a plasma 18-hydroxycorticosterone levelcan further help distinguish APA from IHA. Patients with a solitary adrenal tumor, a plasma18-hydroxycorticosterone level higher than 100 ng/dL, and no significant increase (less than 30%) or aparadoxical decrease in the aldosterone level during a posture test are presumed to have an APA and shouldbe referred for surgery. Patients with an inconclusive adrenal CT scan or discordant results are referred foradrenal venous sampling.
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
11 of 25 11/12/2013 5:35 PM
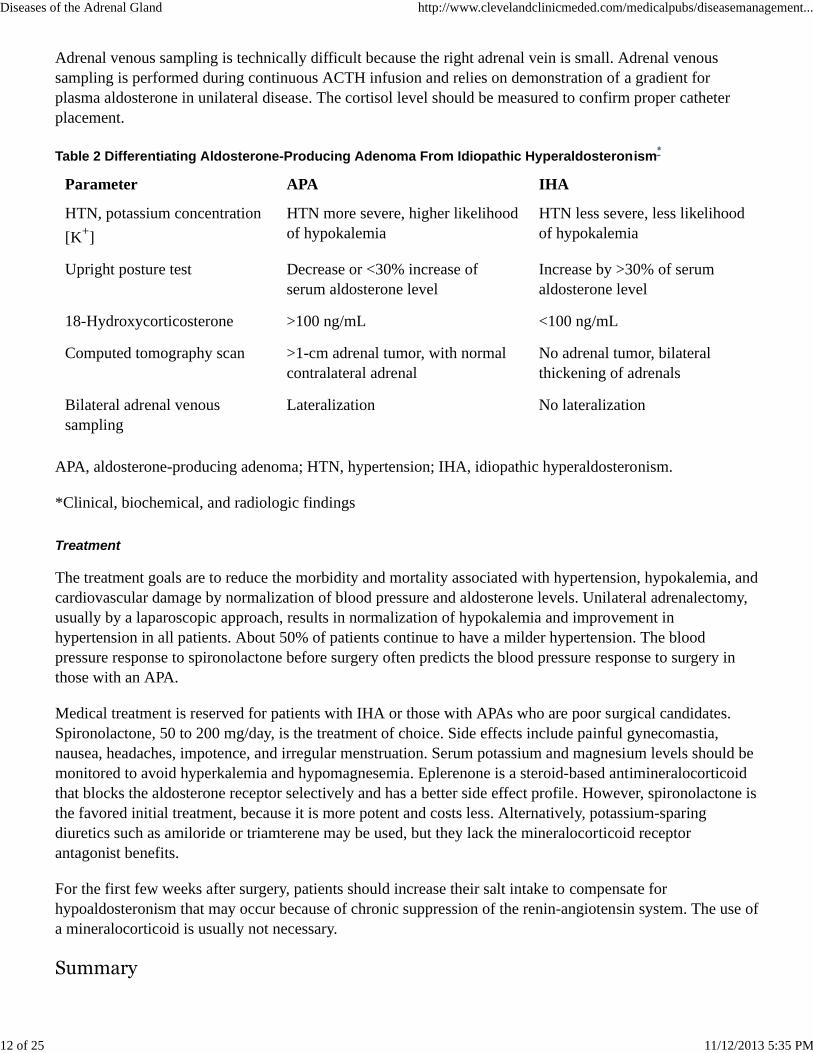
Adrenal venous sampling is technically difficult because the right adrenal vein is small. Adrenal venoussampling is performed during continuous ACTH infusion and relies on demonstration of a gradient forplasma aldosterone in unilateral disease. The cortisol level should be measured to confirm proper catheterplacement.
Table 2 Differentiating Aldosterone-Producing Adenoma From Idiopathic Hyperaldosteronism*
Parameter APA IHA
HTN, potassium concentration[K+]
HTN more severe, higher likelihoodof hypokalemia
HTN less severe, less likelihoodof hypokalemia
Upright posture test Decrease or <30% increase ofserum aldosterone level
Increase by >30% of serumaldosterone level
18-Hydroxycorticosterone >100 ng/mL <100 ng/mL
Computed tomography scan >1-cm adrenal tumor, with normalcontralateral adrenal
No adrenal tumor, bilateralthickening of adrenals
Bilateral adrenal venoussampling
Lateralization No lateralization
APA, aldosterone-producing adenoma; HTN, hypertension; IHA, idiopathic hyperaldosteronism.
*Clinical, biochemical, and radiologic findings
Treatment
The treatment goals are to reduce the morbidity and mortality associated with hypertension, hypokalemia, andcardiovascular damage by normalization of blood pressure and aldosterone levels. Unilateral adrenalectomy,usually by a laparoscopic approach, results in normalization of hypokalemia and improvement inhypertension in all patients. About 50% of patients continue to have a milder hypertension. The bloodpressure response to spironolactone before surgery often predicts the blood pressure response to surgery inthose with an APA.
Medical treatment is reserved for patients with IHA or those with APAs who are poor surgical candidates.Spironolactone, 50 to 200 mg/day, is the treatment of choice. Side effects include painful gynecomastia,nausea, headaches, impotence, and irregular menstruation. Serum potassium and magnesium levels should bemonitored to avoid hyperkalemia and hypomagnesemia. Eplerenone is a steroid-based antimineralocorticoidthat blocks the aldosterone receptor selectively and has a better side effect profile. However, spironolactone isthe favored initial treatment, because it is more potent and costs less. Alternatively, potassium-sparingdiuretics such as amiloride or triamterene may be used, but they lack the mineralocorticoid receptorantagonist benefits.
For the first few weeks after surgery, patients should increase their salt intake to compensate forhypoaldosteronism that may occur because of chronic suppression of the renin-angiotensin system. The use ofa mineralocorticoid is usually not necessary.
Summary
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
12 of 25 11/12/2013 5:35 PM
Hypokalemia may not be present in up to 60% of patients with primary hyperaldosteronism.The ratio of plasma aldosterone concentration to plasma renin activity (PAC/PRA) is the best screeningtest for primary hyperaldosteronism.Spironolactone and eplerenone should be discontinued for 6 weeks before biochemical testing andpotassium needs to be replaced to the normal range.Adrenal venous sampling is of value in some patients with primary hyperaldosteronism to differentiatebetween an aldosterone-producing adenoma and idiopathic hyperaldosteronism
Glucocorticoid-Remediable Hyperaldosteronism
Familial hyperaldosteronism type I, or glucocorticoid-remediable hyperaldosteronism (GRH), is an autosomaldominant disease in which aldosterone is synthesized in the zona fasciculata of the adrenal gland under thecontrol of ACTH.6 Affected individuals are usually younger than 40 years, exhibit hypertension resistant tostandard therapy, and have a family history of primary hyperaldosteronism or a cerebrovascular accident at ayoung age. Most patients have a normal serum potassium level.
Similar to other causes of primary hyperaldosteronism, the PAC/PRA ratio is higher than 20. A 2-daylow-dose DST (0.5 mg dexamethasone orally, every 6 hours) will suppress aldosterone to levels lower than4 ng/dL. The test is not specific. A very high urinary 18-hydroxycortisol level (>3000 nmol/24 hr) or genetictesting to detect a chimeric gene establishes the diagnosis. Genetic testing for glucocorticoid-remediablealdosteronism (GRA) is available for no charge through the International Registry for Glucocorticoid-Remediable Aldosteronism (available at www.brighamandwomens.org/gra). Affected individuals should haveneurovascular screening for cerebral aneurysms. Treatment with glucocorticoids is effective to normalizeblood pressure. Eplerenone, spironolactone, amiloride, and triamterene have also been used successfully.
National Guidelines
There are no consensus statements for the evaluation and therapy of patients with hyperaldosteronism.Although some experts have advocated screening all hypertensive patients for hyperaldosteronism, werecommend screening only high-risk patients. The PAC/PRA ratio is widely accepted as the best initialscreening test, with some variations in cutoff values because of differences in patient preparation (e.g., diet,medications, position) or assays used.
There is some disagreement about the role of adrenal venous sampling in patients with biochemical proof ofhyperaldosteronism. Adrenal venous sampling is selectively used in some centers, whereas some othercenters perform the test in almost all patients.7 In our opinion, if there is a clear adenoma on CT scan on oneof the adrenals and the results of the posture test also suggest APA, the patient can be assumed to have thedisease and should be referred for surgery. Surgery for APA is more cost-effective than long-term medicaltherapy.8
Pheochromocytoma
Pheochromocytomas (PHEOs) are rare chromaffin cell tumors that may occur at any age. Although their trueprevalence is unknown, they occur in about 0.3% of hypertensive patients. If untreated, the disease can havesevere consequences, such as myocardial infarction, heart failure, cerebrovascular accident, and death.
Anatomic Considerations and Etiology
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
13 of 25 11/12/2013 5:35 PM
Most PHEOs are benign, sporadic, unilateral, and located within the adrenal gland. Extra-adrenalpheochromocytomas (paragangliomas) occur in about 15% of cases in the superior and inferior para-aorticareas, including the Zuckerkandl organ (75%), bladder (10%), thorax (10%), and head, neck, and pelvis (5%).Paragangliomas tend to occur in younger patients <20 years) and are uncommon in those older than 60 years.They are multifocal in about 15% to 30% of cases. Bilateral adrenal pheochromocytomas (5%-10% of cases)are usually seen as part of familial syndromes. Malignant pheochromocytomas (10% of adrenal cases) have ahigher prevalence in ectopic PHEOs and lower prevalence in familial PHEOs. No clinical, imaging, orlaboratory criteria absolutely predict malignancy; tumors larger than 5 cm have a greater potential tometastasize. The diagnosis of malignant pheochromocytoma relies on the presence of metastases and not onthe histology of the tumor.
About 10% to 15% of PHEOs are hereditary in nature. Familial predisposition to pheochromocytoma is seenin patients with multiple endocrine neoplasia (MEN) types IIA and IIB, von Hippel-Lindau disease,neurofibromatosis type 1, and familial paragangliomas. Genetic screening in patients with apparentlysporadic pheochromocytoma is recommended for the following categories of patients: age younger than 20years, bilateral disease, multiple paragangliomas, or family history of pheochromocytoma or paraganglioma.
Clinical Manifestations
Patients with PHEO may have paroxysmal hypertension (48%) or persistent hypertension (29%), or benormotensive (13%).9 Wide fluctuations in blood pressure and resistance to antihypertensive medications aretypical of those with pheochromocytoma. Norepinephrine-secreting tumors are associated with sustainedhypertension and norepinephrine and epinephrine-secreting tumors are associated with labile hypertension.Large cystic PHEOs may not be associated with hypertension because most of the catecholamines aremetabolized within the tumor before being released into circulation. Those with a familial form of PHEO arealso more likely to be normotensive.
The triad of headaches, palpitations, and diaphoresis suggests the diagnosis of PHEO, but absence of thesesymptoms does not exclude the disease. Attacks are usually precipitated by emotional stress, exercise,anesthesia, abdominal pressure, or ingestion of tyramine- containing foods. Both pallor and flushing may beseen in patients. Other symptoms include orthostatic hypotension, weight loss, dyspnea, polyuria, polydipsia,visual blurring, focal neurologic symptoms, and change in mental status.
Diagnosis
Testing for PHEO is indicated for any patient with suggestive clinical manifestations. Priority has to beassigned to monitoring patients with the following:9
Episodic symptoms of headaches, tachycardia, and diaphoresis (with or without hypertension)Family history of PHEO or familial syndromes that may include PHEOAdrenal incidentalomasUnexplained paroxysms of tachyarrythmias or bradyarrythmias or hypertension during intubation,induction of anesthesia, parturition, or prolonged and unexplained postoperative hypotensionAdverse cardiovascular reactions to certain drugs, including anesthetic agents, beta blockers, glucagon,tricyclic antidepressants, histamine, phenothiazine, and tyramine-containing foodsSpells or attacks during exertion, movements of torso, straining, coitus, or micturition
No single test achieves 100% diagnostic accuracy. Plasma-free metanephrines (total free normetanephrine
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
14 of 25 11/12/2013 5:35 PM
and metanephrine) have 99% and 97% sensitivity, respectively, for sporadic and familial PHEOs, but there isapproximately a 10% to 15% false-positive rate for sporadic PHEO. Clinicians should be familiar with theirassay’s diagnostic characteristics. In general, a plasma-free metanephrine level more than three or four timesthe upper normal has 100% specificity for PHEO. Renal failure is only associated with mild increases inplasma-free metanephrine levels. If the plasma-free metanephrine concentration is normal, no otherdiagnostic test is necessary except in those with small tumors found during workup for familial disease,patients with a history of PHEO or, rarely, patients with a dopamine-producing paraganglioma.
Patients with indeterminate levels of plasma-free metanephrines should have their urinary metanephrine andserum catecholamine levels measured (Fig. 4). Urinary total metanephrine levels higher than 1.8 mg/day arediagnostic for PHEO. Total plasma catecholamine (norepinephrine plus epinephrine) concentration higherthan 2000 pg/mL is diagnostic of PHEO, values between 1000 and 2000 pg/mL are highly suggestive of thedisease, and values lower than 1000 pg/mL in a patient with severe signs and symptoms at the time ofsampling almost always rules out the disease. Urinary vanillylmandelic acid (VMA) measurement has a highfalse-negative rate (41%) and should not be used for screening purposes, but a positive result hasapproximately 86% and 99% specificity for sporadic and hereditary PHEOs, respectively.
In patients with nondiagnostic ranges of plasma and urine catecholamine and metanephrine levels, andclinical features suggestive of PHEO, repeating the measurements at the time of symptoms or proceedingwith dynamic testing may be used to support or exclude the diagnosis.10 Clonidine normally suppressesplasma catecholamines, a response that is lost in PHEO. During the clonidine suppression test, clonidine,0.3 mg, is administered orally and plasma catecholamine and metanephrine levels are measured before and 3hours after clonidine is administered. Normalization of the plasma metanephrine level or a decrease in theplasma catecholamine levels by at least 50%, into the normal range for the assay, is considered a normalresponse.
The list of medications and interfering substances varies according to what is measured-plasma or urinecatecholamines or their metabolites-and to the specific assay used. Thus, it is usually more practical to try toavoid all of them (Box 3). Patients should abstain from caffeinated beverages and alcohol for 24 hours andmedications listed in Box 3 for 3 to 5 days before biochemical evaluation. Selective alpha1 blockers (e.g.,doxazosin), calcium channel blockers, and beta blockers such as metoprolol or atenolol can be used for bloodpressure control during biochemical evaluation and do not cause any significant false-positive results.Because of the potential for inducing a hypertensive crisis, beta blockers should never be used withoutsimultaneously using alpha blockers.
Box 3 Medications and Stimulants to Avoid Before Measurement of Plasma and UrinaryCatecholamines and Metanephrines
Tricyclic antidepressants
Acetaminophen
Phenoxybenzamine
Monoamine oxidase inhibitors
Antipsychotics
Buspirone
Sympathomimetics-ephedrine, pseudoephedrine, amphetamines, albuterol
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
15 of 25 11/12/2013 5:35 PM
Stimulants-caffeine, nicotine, theophylline
Miscellanous-levodopa, carbidopa, alcohol, cocaine
Caffeinated beverages and alcohol should preferably be avoided for 24 hours. Medications should be stoppedfor 3 to 5 days, except labetalol, which needs to be discontinued for 2 weeks (causes analytic interferencewith some assays).
Imaging Studies
PHEO is diagnosed in about 6.5% of incidentally discovered adrenal tumors. PHEOs are usually larger than3 cm in diameter and tend to be cystic, with areas of necrosis with increased size. In a patient suspected tohave PHEO, CT scanning of the abdomen and pelvis should be performed first, followed by CT of the chestand neck if no tumor is found (Fig. 5). An adrenal tumor with a noncontrast Hounsfield unit (HU) lower than10 is extremely unlikely to be PHEO. In a review of more than 30 proven PHEO cases at the ClevelandClinic, all patients had a noncontrast CT scan HU of more than 20.11
Chemical shift MRI has a sensitivity of 93% to 100% and specificity of approximately 50% in detectingpheochromocytomas. The low lipid content of PHEO tumors results in a signal intensity decrease from thein-phase to opposed-phase T1-weighted image. PHEO tumors typically exhibit signal isointensity with theliver, kidneys, and muscle on T1-weighted images and a characteristically bright, high signal intensity onT2-weighted images (Fig. 6). We usually prefer CT scanning over MRI as the initial imaging study with abiochemical workup diagnostic for PHEO because of cost and widespread availability.
Functional imaging using iobenguane sulfate131I (formerly called meta-iodobenzylguanidine [MIBG]) shouldbe used when multiple or metastatic tumors are suspected, such as in younger patients (<20 years), those withfamilial pheochromocytoma, tumors larger than 5 cm, or an extra-adrenal tumor, or when CT and MRI fail tolocalize the tumor despite biochemical evidence supporting the diagnosis of pheochromocytoma (see Fig. 5).The specificity of iobenguane sulfate131I is very high, 95% to 100%, and the sensitivity is about 85%. Nasaldecongestants, some antihypertensives, antidepressants, antipsychotics, and cocaine affect iobenguanesulfate131I uptake and have to be withheld for 1 to 3 days before the study. Labetolol in particular has beenshown to decrease iobenguane sulfate131I uptake. Uptake of iodine by the thyroid gland should be blockedwith potassium iodide (SSKI; five drops three times a day, starting on the day of iobenguane sulfate131I and 3days afterward). If the iobenguane sulfate131I study is negative, fluorodeoxyglucose positron emissiontomography (PET) scanning or oxidronate (Octreoscan) may be used with some success for visualization (seeFig. 5).
Treatment
Surgical resection is the treatment of choice for pheochromocytoma. Adequate medical preparation isessential and usually achieved in 10 to 14 days. α1-Adrenergic receptor blockers (e.g., doxazosin) arefirst-line therapy, with increasing dosage as tolerated. Beta blockers (e.g., metoprolol, atenolol) are added iftachycardia develops while the patient is adequately hydrated. Beta blockers should be added only after alphablockade has been instituted to prevent unopposed alpha receptor activation, which may result in hypertensivecrisis. Calcium channel blockers (CCBs) can be used for medical preparation or may be added if there ispersistent or labile hypertension. The nonspecific α1-adrenergic blocker phenoxybenzamine has a greater side
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
16 of 25 11/12/2013 5:35 PM
effect profile and may result in prolonged hypotension after surgery.
Surgery for PHEO has shifted from the open conventional procedure to the laparoscopic approach over thepast decade. Patients should have electrocardiography and cardiac echocardiography before surgery, withfurther cardiac evaluation if any abnormality is detected. It is preferable that patients be admitted to thehospital 1 day before surgery for close observation. In those with orthostatic hypotension, an isotonic salineinfusion at a rate of 100 to 200 mL/hr should be started. Close blood pressure monitoring is necessary duringsurgery. The anesthesia team should be familiar with the care of patients with PHEO during surgery. Aftersurgery, blood pressure and blood glucose levels need to be closely monitored, antihypertensive agentswithheld, and normal saline infusion continued. Fluid overload should also be avoided. Antihypertensiveagents may be resumed if the patient continues to be hypertensive. Lifelong follow-up is necessary for allpatients, with closer follow-up of those with familial, large, extra-adrenal, or bilateral tumors.
Acute hypertensive crises can be treated with IV nitroprusside, nitroglycerin, the short-acting α-adrenergicblocker phentolamine (competitive α1-adrenergic and weak α2-adrenergic receptor antagonist), magnesiumsulfate, or nicardipine, a calcium channel blocker. Metastatic lesions should also be resected if possible. Inpatients with aggressive tumors, combination chemotherapy (cyclophosphamide, vincristine, dacarbazine) oriobenguane sulfate131I-tagged radiotherapy may be considered, but results have not been promising.
National Guidelines
There are no consensus statements for the evaluation and therapy of PHEO patients. Most experts’ opinionsare based on personal experience in centers with large referral bases. Although there are still disagreementsabout the best initial screening test for PHEO, serum metanephrine or 24-hour urinary metanephrine leveldetermination appears to be the most favored initial test of choice.
Summary
The triad of headaches, palpitations, and diaphoresis suggests the diagnosis of pheochromocytoma, butabsence of these symptoms do not exclude the disease.Beta blockers should not be used in patients with suspected pheochromocytoma until alpha blockadehas been instituted.Plasma-free metanephrines have 99% and 97% sensitivity for sporadic and familialpheochromocytomas, respectively. However, there is approximately a 10% to 15% false-positive ratefor sporadic pheochromocytoma.Adequate medical preparation is essential and should be initiated at least 10 to 14 days before surgery.
Adrenal Hyperandrogenism
The adrenal glands are an important source of androgens, especially in children and women. The primaryadrenal androgens, dehydroepiandrosterone (DHEA) and dehydroepiandrosterone sulfate (DHEAS sulfate),are under ACTH control and have little intrinsic androgenic activity. However, they are converted toandrostenedione and then to testosterone (and estrogen) in both the adrenal gland and peripheral tissues.DHEA and DHEA sulfate are responsible for adrenarche (pubic hair development). Peak levels occur in thethird decade of life and decline progressively to 25% of peak levels around the age of 80 years.
Clinical Manifestations
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
17 of 25 11/12/2013 5:35 PM
Features of adrenal androgen excess differ with age and gender. In female neonates, androgen excess causesfemale pseudohermaphroditism (ambiguous genitalia). Male infants exhibit penile enlargement.
In prepubertal children, boys and girls, androgen excess manifests as increased rate of growth in height andskeletal maturation, leading to premature epiphyseal fusion and short adult height. In addition, boys exhibitpenile enlargement, hair growth in androgen-dependent areas, deepening of the voice, and other secondarysexual characteristics (isosexual precocious puberty). Girls have hirsutism, acne, and clitoromegaly(heterosexual precocious puberty).
Androgen excess with onset at puberty causes premature skeletal maturation and short adult height in boys. Ingirls, it manifests as primary or secondary amenorrhea, different degree of virilization, and increased skeletalmaturation, resulting in short adult height.
Manifestations of androgen excess with onset at adult age are limited in men. A decrease in size of thetesticles, testosterone secretion, and spermatogenesis caused by inhibition of gonadotropin secretion mayoccur. In women, hirsutism, acne, menstrual irregularities, male pattern baldness, infertility, decreased breasttissue, increased muscle mass, android body habitus, and clitoromegaly may occur, depending on the degreeof hyperandrogenism.
Of the various causes of adrenal hyperandrogenism, nonclassic (adult-onset) congenital adrenal hyperplasia(CAH), and androgen-producing adrenal tumors are discussed in this section. Exogenous androgen intake forbody building or to increase erythropoiesis may cause acne, hirsutism, and oligomenorrhea or amenorrhea inwomen and small testes, gynecomastia, and impaired spermatogenesis in men. Hyperprolactinemia may causean increase in serum DHEAS and androstenedione levels by direct stimulation of the adrenal gland.
Nonclassic Congenital Adrenal Hyperplasia
Nonclassic congenital adrenal hyperplasia (NCAH) is an autosomal recessive disorder, with most patientsexhibiting a defect in 21-hydoxlyase enzyme activity, resulting in decreased cortisol production. Theassociated increased ACTH secretion stimulates adrenal steroid production upstream of the defective enzyme,resulting in increased androgen secretion. Hyperandrogenic symptoms are usually diagnosed in late pubertyand early adulthood. NCAH affects from 1% to 10% of hyperandrogenic women, depending on their ethnicbackground. It is rare among African Americans. The main differential diagnosis for NCAH is polycysticovary syndrome (PCOS), which is about 40 to 50 times more common (Table 3).12 Distinguishing the twoonly on clinical grounds is difficult, because both can be associated with varying degrees ofhyperandrogenism and ovulatory dysfunction. (See elsewhere in this text, “Polycystic Ovary Syndrome,” forfurther discussion.) DHEAS and testosterone levels are not reliable in differentiating the two. The diagnosisof NCAH is established based on a basal or post–250-μg cosyntropin-stimulated level of17-hydoxyprogesterone higher than 15 ng/mL (45 nmol/L). Morning basal 17-hydoxyprogesterone levelsduring the follicular phase of the menstrual cycle (shortly after spontaneous or induced vaginal bleeding)lower than 2 ng/mL essentially rules out NCAH. The diagnosis can usually be confirmed by genotyping.
Table 3 Differences Between Polycystic Ovary Syndrome and 21-Hydroxylase-Deficient NonclassicCongenital Adrenal Hyperplasia
Parameter PCOS NCAH
Prevalence in reproductive age women 4%-6% 0.1%-0.05%
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
18 of 25 11/12/2013 5:35 PM
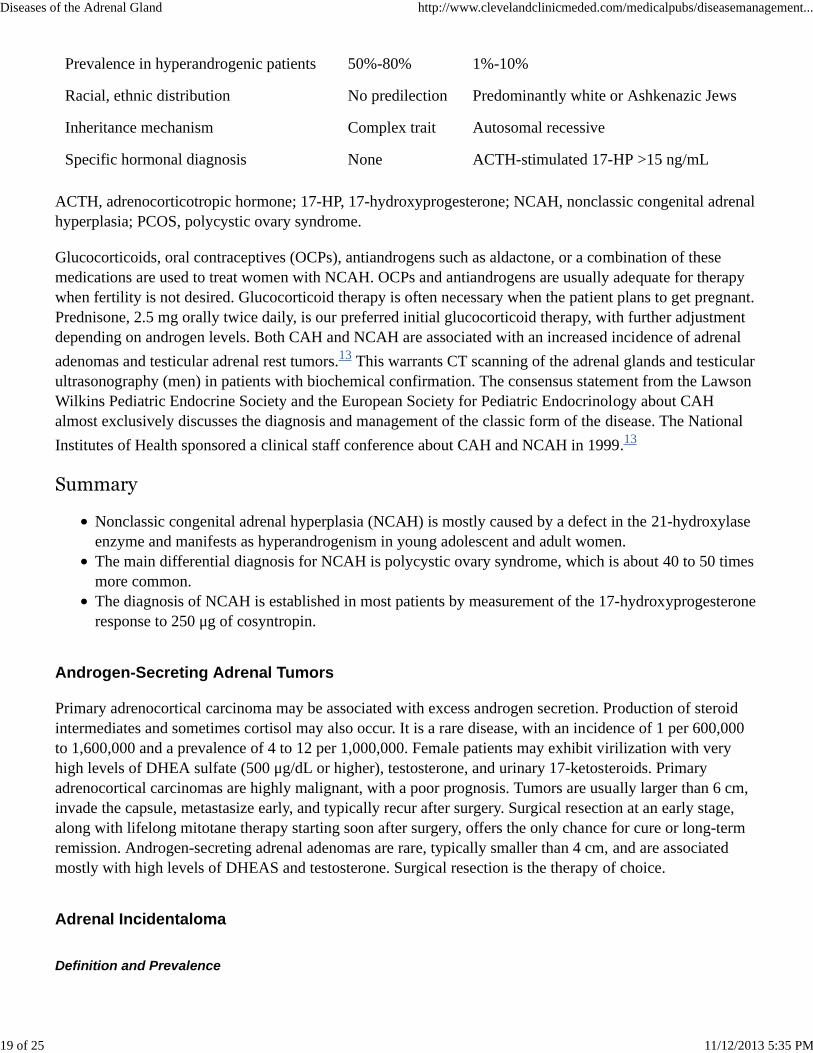
Prevalence in hyperandrogenic patients 50%-80% 1%-10%
Racial, ethnic distribution No predilection Predominantly white or Ashkenazic Jews
Inheritance mechanism Complex trait Autosomal recessive
Specific hormonal diagnosis None ACTH-stimulated 17-HP >15 ng/mL
ACTH, adrenocorticotropic hormone; 17-HP, 17-hydroxyprogesterone; NCAH, nonclassic congenital adrenalhyperplasia; PCOS, polycystic ovary syndrome.
Glucocorticoids, oral contraceptives (OCPs), antiandrogens such as aldactone, or a combination of thesemedications are used to treat women with NCAH. OCPs and antiandrogens are usually adequate for therapywhen fertility is not desired. Glucocorticoid therapy is often necessary when the patient plans to get pregnant.Prednisone, 2.5 mg orally twice daily, is our preferred initial glucocorticoid therapy, with further adjustmentdepending on androgen levels. Both CAH and NCAH are associated with an increased incidence of adrenaladenomas and testicular adrenal rest tumors.13 This warrants CT scanning of the adrenal glands and testicularultrasonography (men) in patients with biochemical confirmation. The consensus statement from the LawsonWilkins Pediatric Endocrine Society and the European Society for Pediatric Endocrinology about CAHalmost exclusively discusses the diagnosis and management of the classic form of the disease. The NationalInstitutes of Health sponsored a clinical staff conference about CAH and NCAH in 1999.13
Summary
Nonclassic congenital adrenal hyperplasia (NCAH) is mostly caused by a defect in the 21-hydroxylaseenzyme and manifests as hyperandrogenism in young adolescent and adult women.The main differential diagnosis for NCAH is polycystic ovary syndrome, which is about 40 to 50 timesmore common.The diagnosis of NCAH is established in most patients by measurement of the 17-hydroxyprogesteroneresponse to 250 μg of cosyntropin.
Androgen-Secreting Adrenal Tumors
Primary adrenocortical carcinoma may be associated with excess androgen secretion. Production of steroidintermediates and sometimes cortisol may also occur. It is a rare disease, with an incidence of 1 per 600,000to 1,600,000 and a prevalence of 4 to 12 per 1,000,000. Female patients may exhibit virilization with veryhigh levels of DHEA sulfate (500 μg/dL or higher), testosterone, and urinary 17-ketosteroids. Primaryadrenocortical carcinomas are highly malignant, with a poor prognosis. Tumors are usually larger than 6 cm,invade the capsule, metastasize early, and typically recur after surgery. Surgical resection at an early stage,along with lifelong mitotane therapy starting soon after surgery, offers the only chance for cure or long-termremission. Androgen-secreting adrenal adenomas are rare, typically smaller than 4 cm, and are associatedmostly with high levels of DHEAS and testosterone. Surgical resection is the therapy of choice.
Adrenal Incidentaloma
Definition and Prevalence
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
19 of 25 11/12/2013 5:35 PM
An adrenal incidentaloma is an adrenal mass larger than 1 cm in diameter discovered during radiologicexamination done for a reason not related to the adrenal gland. The definition of incidentaloma excludespatients undergoing imaging procedures as part of staging and workup for cancer. Incidental adrenal massesare found in 0.5% to 5% of patients undergoing CT of the abdomen and in up to 9% of postmortem autopsiesin unselected populations.
Evaluation
Management decisions are based on the need to address whether the tumor is functional (i.e., producinghormones) or malignant.
Evaluation for Hormonal Hypersecretion. Up to 35% of adrenal incidentalomas may be functional. Allpatients should undergo hormonal evaluation for Cushing’s syndrome and pheochromocytoma, and thosewith hypertension should also be evaluated for hyperaldosteronism. Isolated excess androgen secretion byadrenal adenomas or carcinomas is rare. Thus, only women with an adrenal mass and physical findingssuggestive of hyperandrogenism should have their testosterone and DHEAS levels measured.
Subclinical Cushing’s syndrome (SCS) is a relatively recent and poorly described disorder, occurring in about5% to 24% of patients with adrenal incidentalomas. The prevalence varies greatly, depending on thediagnostic criteria and the screening methods used. Patients do not have the typical signs and symptoms ofCushing’s syndrome, but generally have increased frequency of hypertension, glucose intolerance, diabetes,and possibly osteopenia. We support the 2002 NIH consensus panel recommendation of a 1-mg overnightDST as the initial biochemical evaluation of choice. Some experts have recommended two or more of thefollowing abnormal tests of the HPA axis for the diagnosis of SCS: lack of suppression during 1-mgovernight DST, increased urinary free cortisol levels, loss of diurnal cortisol rhythm, low or suppressedACTH level, and impaired ACTH response to CRH. Development of adrenal insufficiency after surgicalremoval of the adrenal tumor is the best way to confirm the diagnosis.
Evaluation for Malignancy. Adrenal tumor size has been used to differentiate between benign and malignantadrenal masses. Risk of malignancy increases with adrenal tumor size. Cutoff values ranging from 4 to 6 cmhave been proposed by different clinicians for surgical resection of adrenal masses. In spite of a relationshipbetween the risk of malignancy and adrenal tumor size, there is a significant overlap, and even a cutoff valueof 2 cm could not achieve a 100% specificity to rule out a malignant adrenal mass.11
A noncontrast CT attenuation coefficient (in HU) is the most promising imaging tool to differentiate benignadrenal masses from malignant tumors. Intracytoplasmic fat is often abundant in adrenal adenomas, but rarein adrenal metastases, pheochromocytoma, and adrenocortical carcinomas. Adrenal masses with anoncontrast HU of less than 10 are always benign.11 The noncontrast HU is superior to adrenal size indifferentiating benign from malignant adrenal tumors.
Some studies have reported the value of delayed enhancement washout percentage in attenuation value duringCT scanning of the adrenal glands to differentiate lipid-poor adrenal adenomas (noncontrast HU of >10) fromnonadenomas. An absolute enhancement washout percentage of less than 60% at 15 minutes postcontrast had95% to 100% specificity in identifying nonadenomas.14 This needs to be further validated by studies of largenumbers of patients. MRI is another noninvasive method used to differentiate benign and malignant adrenalmasses. Its sensitivity and specificity for diagnosis of a benign adrenal mass seem to be close to thenoncontrast CT attenuation value.
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
20 of 25 11/12/2013 5:35 PM
Algorithm for Evaluation and Treatment of Adrenal Incidentalomas
Our approach to incidentally discovered adrenal masses is shown in Figure 7. We usually do not routinelyobtain any follow-up imaging studies in nonfunctional adrenal masses with a noncontrast HU of less than 10.Such patients undergo annual follow-up evaluations for any excess hormone hypersecretion for 5 years andthen intermittently afterward. We recommend that all adrenal tumors larger than 6 cm be surgically removed;however, myelolipoma is an exception, with a characteristically low attenuation value on noncontrast CTscan. Adrenal masses smaller than 6 cm with a noncontrast HU of more than 10 need to have their absolutepercentage washout calculated at 15 minutes and undergo follow-up imaging studies in 6 to 12 months (seeFig. 7). There is no good evidence supporting continued radiologic surveillance if the follow-up study at 6 to12 months shows no change in adrenal tumor size.
Fine-needle aspiration of an adrenal mass may be done to rule out metastasis once pheochromocytoma hasbeen ruled out. Adrenal biopsy may not differentiate adrenocortical carcinomas from adenomas. Surgicalresection of the adrenal mass is usually considered for patients with functional or malignant adrenal masses.Medical therapy may be acceptable in the case of primary hyperaldosteronism secondary to adrenocorticaladenoma or hyperplasia.
National Guidelines
The National Institute of Health (NIH) held a state-of-the-science conference in February 2002, during whichthe management of adrenal incidentalomas was discussed by a 12-member panel.15 The panel recommendedmeasuring serum aldosterone levels and plasma renin activity only in patients with hypertension and anovernight 1-mg DST and plasma or urine metanephrine levels for all patients with an adrenal incidentaloma.
The panel recommended a noncontrast CT HU threshold of 10 as a reliable radiologic feature to differentiatebenign from malignant adrenal tumors. The panel recommended surgical resection of all adrenal masseslarger than 6 cm and a repeat CT scan in 6 to 12 months for those with adrenal incidentalomas that are notsurgically removed. The panel concluded that there are no data supporting continued radiologic evaluation ifan adrenal mass is stable in size. We usually do not obtain a routine follow-up imaging study in adrenalmasses with a noncontrast CT HU of lower than 10, because the risk of developing a primary adrenocorticalcarcinoma from an adenomatous or hyperplastic adrenal mass is extremely rare.
Summary
All patients with adrenal incidentaloma should undergo hormonal evaluation for Cushing’s syndromeand pheochromocytoma and those with hypertension should also be evaluated for hyperaldosteronism.Adrenal masses with a noncontrast CT attenuation coefficient (in HU) of less than 10 are almost alwaysbenign.Fine-needle aspiration of an adrenal mass may be done to rule out metastasis once pheochromocytomahas been ruled out.
Back to Top
Considerations of the Pharmacologic use of Glucocorticoids
Pharmacologic doses of synthetic glucocorticoids are used in a wide variety of diseases for theiranti-inflammatory and immunosuppressive effects.
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
21 of 25 11/12/2013 5:35 PM
Endocrine Problems with Chronic Glucocorticoid Treatment
Two main clinical problems arise with the chronic use of pharmacologic doses of glucocorticoids,iatrogenically induced Cushing’s syndrome and adrenal insufficiency on abrupt cessation of therapy.Cushing’s syndrome may become clinically apparent within 1 month after onset of treatment. The duration ofglucocorticoid therapy, the highest dose, and the total cumulative dose have long been considered importantpredictors of suppression of the HPA axis. Secondary adrenal insufficiency caused by exogenous steroidintake should be anticipated in any patient who takes more than 30 mg of hydrocortisone (or 7.5 mgprednisone) per day for more than 3 weeks.16 Excluding depot glucocorticoid injections, therapy for less than2 weeks rarely results in clinically significant suppression of HPA axis.
Alternate-day therapy and avoidance of nighttime doses are associated with less suppression of the HPA axis.The time to recovery of the HPA axis after discontinuation of glucocorticoid therapy is variable and can be asshort as 2 to 5 days or as long as 9 to 12 months.
Inhaled glucocorticoid use for a long duration may result in suppression of the HPA axis. All topicalglucocorticoids are absorbed to some extent, depending on the area of the body (intertriginous area absorptionhigher than forehead and scalp absorption; least absorption is in the forearm). Inflammation of the skin andapplication of occlusive dressings increase systemic absorption. Case reports have been published, withpatients demonstrating a grossly cushingoid appearance after long-term use of steroid-containing topicalcreams or eye drops.
Recommendations for Glucocorticoid Treatment Withdrawal
There are two important issues that need particular attention when trying to wean a patient from chronicsteroid therapy. First, the underlying condition for which the steroid therapy was initiated should always bekept in mind, and any tapering of the dose should be done accordingly. For example, too rapid tapering ofglucocorticoid therapy in a patient with asthma may result in exacerbation of the underlying condition.Second, if the underlying disorder for which glucocorticoid therapy was initiated has been resolved, then arapid tapering of the glucocorticoid dose to about 2 to 3 times the physiologic replacement dose is safe inmost patients.
Our approach is to change different glucocorticoid preparations to hydrocortisone, 20 mg in the morning and10 mg at noon, which after 2 to 4 weeks is changed to 20 mg hydrocortisone once daily in the morning. Whileon hydrocortisone therapy, patients are advised to double their dose for 2 to 3 days if they develop any acuteillness. Patients are then followed at 1- to 2-month intervals, measuring the serum cortisol level during a CSTafter holding the morning hydrocortisone. A cortisol value higher than 18 μg/dL at 30 minutes during alow-dose (1 μg) or standard-dose (250 μg) CST indicates normal recovery of adrenal function. Those patientswith levels between 14 and 18 μg/dL may only take hydrocortisone during acute illness, with re-evaluation oftheir adrenal axis at 2- to 3-month intervals to ensure full recovery. All patients chronically treated withglucocorticoids should wear medical alert tags and be instructed about supplemental coverage duringinfection or surgery and the need for parenteral glucocorticoid therapy if unable to tolerate oral medications.
Back to Top
Summary
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
22 of 25 11/12/2013 5:35 PM
Secondary adrenal insufficiency caused by exogenous glucocorticoid intake should be anticipated inany patient who takes more 7.5 mg prednisone/day for longer than 3 weeks.Inhaled glucocorticoid use for long periods may result in suppression of the hypothalamic-pituitary-adrenal axis.Morning serum cortisol determination and the CST may be used to evaluate the recovery of adrenalfunction during glucocorticoid taper and withdrawal.
Back to Top
Suggested Readings
Annane D, Sebille V, Charpentier C, et al: Effect of treatment with low doses of hydrocortisone andfludrocortisone on mortality in patients with septic shock. JAMA 2002;288:862-871.
Arnaldi G, Angeli A, Atkinson AB, et al: Diagnosis and complications of Cushing’s syndrome: Aconsensus statement. J Clin Endocrinol Metab 2003;88:5593-5602.
Bravo EL, Tagle R: Pheochromocytoma: State-of-the-art and future prospects. Endocr Rev2003;24:539-553.
Caoili EM, Korobkin M, Francis IR, et al: Delayed enhanced CT of lipid-poor adrenal adenomas. AJRAm J Roentgenol 2000;175:1411-1415.
Cooper MS, Stewart PM: Corticosteroid insufficiency in acutely ill patients. N Engl J Med2003;348:727-734.
Gordon RD, Stowasser M, Rutherford JC: Primary aldosteronism: Are we diagnosing and operating ontoo few patients? World J Surg 2001;25:941-947.
Grumbach MM, Biller BM, Braunstein GD, et al: Management of the clinically inapparent adrenalmass (“incidentaloma”). Ann Intern Med 2003;138:424-429.
Hamrahian AH, Ioachimescu AG, Remer EM, et al: Clinical utility of noncontrast computedtomography attenuation value (Hounsfield units) to differentiate adrenal adenomas/hyperplasias fromnonadenomas: Cleveland Clinic experience. J Clin Endocrinol Metab 2005;90:871-877.
Hamrahian AH, Oseni TS, Arafah BM: Measurements of serum free cortisol in critically ill patients. NEngl J Med 2004;350:1629-1638.
Ilias I, Pacak K: Current approaches and recommended algorithm for the diagnostic localization ofpheochromocytoma. J Clin Endocrinol Metab 2004;89:479-491.
Mayenknecht J, Diederich S, Bahr V, et al: Comparison of low and high dose corticotropin stimulationtests in patients with pituitary disease. J Clin Endocrinol Metab 1998;83:1558-1562.
McMahon GT, Dluhy RG: Glucocorticoid-remediable aldosteronism. Cardiol Rev 2004;12:44-48.
Merke DP, Bornstein SR, Avila NA, Chrousos GP: NIH conference. Future directions in the study andmanagement of congenital adrenal hyperplasia caused by 21-hydroxylase deficiency. Ann Intern Med2002;136:320-334.
Moran C, Azziz R: 21-Hydroxylase-deficient nonclassic adrenal hyperplasia: The great pretender.Semin Reprod Med 2003;21:295-300.
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
23 of 25 11/12/2013 5:35 PM
Sywak M, Pasieka JL: Long-term follow-up and cost benefit of adrenalectomy in patients with primaryhyperaldosteronism. Br J Surg 2002;89:1587-1593.
Young WF Jr: Minireview: Primary aldosteronism-changing concepts in diagnosis and treatment.Endocrinology 2003;144:2208-2213.
Back to Top
References
Mayenknecht J, Diederich S, Bahr V, et al: Comparison of low and high dose corticotropin stimulationtests in patients with pituitary disease. J Clin Endocrinol Metab 1998;83:1558-1562.
1.
Annane D, Sebille V, Charpentier C, et al: Effect of treatment with low doses of hydrocortisone andfludrocortisone on mortality in patients with septic shock. JAMA 2002;288:862-871.
2.
Hamrahian AH, Oseni TS, Arafah BM: Measurements of serum free cortisol in critically ill patients. NEngl J Med 2004;350:1629-1638.
3.
Arnaldi G, Angeli A, Atkinson AB, et al: Diagnosis and complications of Cushing’s syndrome: Aconsensus statement. J Clin Endocrinol Metab 2003;88:5593-5602.
4.
Young WF Jr: Minireview: Primary aldosteronism—changing concepts in diagnosis and treatment.Endocrinology 2003;144:2208-2213.
5.
McMahon GT, Dluhy RG: Glucocorticoid-remediable aldosteronism. Cardiol Rev 2004;12:44-48.6.
Gordon RD, Stowasser M, Rutherford JC: Primary aldosteronism: Are we diagnosing and operating ontoo few patients? World J Surg 2001;25:941-947.
7.
Sywak M, Pasieka JL: Long-term follow-up and cost benefit of adrenalectomy in patients with primaryhyperaldosteronism. Br J Surg 2002;89:1587-1593.
8.
Bravo EL, Tagle R: Pheochromocytoma: State-of-the-art and future prospects. Endocr Rev2003;24:539-553.
9.
Ilias I, Pacak K: Current approaches and recommended algorithm for the diagnostic localization ofpheochromocytoma. J Clin Endocrinol Metab 2004;89:479-491.
10.
Hamrahian AH, Ioachimescu AG, Remer EM, et al: Clinical utility of noncontrast computedtomography attenuation value (Hounsfield units) to differentiate adrenal adenomas/hyperplasias fromnonadenomas: Cleveland Clinic experience. J Clin Endocrinol Metab 2005;90:871- 877.
11.
Moran C, Azziz R: 21-Hydroxylase-deficient nonclassic adrenal hyperplasia: The great pretender.Semin Reprod Med 2003;21:295-300.
12.
Merke DP, Bornstein SR, Avila NA, Chrousos GP: NIH conference. Future directions in the study andmanagement of congenital adrenal hyperplasia due to 21-hydroxylase deficiency. Ann Intern Med2002;136:320-334.
13.
Caoili EM, Korobkin M, Francis IR, et al: Delayed enhanced CT of lipid-poor adrenal adenomas. AJRAm J Roentgenol 2000;175:1411-1415.
14.
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
24 of 25 11/12/2013 5:35 PM
Grumbach MM, Biller BM, Braunstein GD, et al: Management of the clinically inapparent adrenalmass (“incidentaloma”). Ann Intern Med 2003;138:424-429.
15.
Cooper MS, Stewart PM: Corticosteroid insufficiency in acutely ill patients. N Engl J Med2003;348:727-734.
16.
Back to Top
Diseases of the Adrenal Gland http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement...
25 of 25 11/12/2013 5:35 PM
Related Documents