Metastatic Colorectal Cancer Britt MacArthur Dietetic Intern: Case Study Presentation Spring 2012

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Metastatic Colorectal Cancer
Britt MacArthurDietetic Intern: Case Study Presentation Spring 2012

What I learned in MSS with Susan & Leah
SennaColaceMiralax
SuppositoryEnemaCoLyte

Colorectal Cancer Review◦ Statistics◦ Function of Colon◦ Understanding Cancer◦ Causes & Risk Factors◦ Screenings/Tests◦ How Cancer Spreads◦ Treatments
Case Study◦ Pt. Profile◦ Past Medical Hx.◦ Background Research◦ Nutritional Status◦ Prognosis
Outline
Cancer that begins in the colon is called colon cancer, and cancer that begins in the rectum is called rectal cancer
Cancer that starts in either of these organs may also be called colorectal cancer
In 2012, more than 143,000 people in the United States will be diagnosed with colorectal cancer◦ It is the 4th most common cancer in men, after skin,
prostate, and lung cancer◦ It is also the 4th most common cancer in women, after
skin, breast, and lung cancer
Colorectal CancerDefinition & Statistics
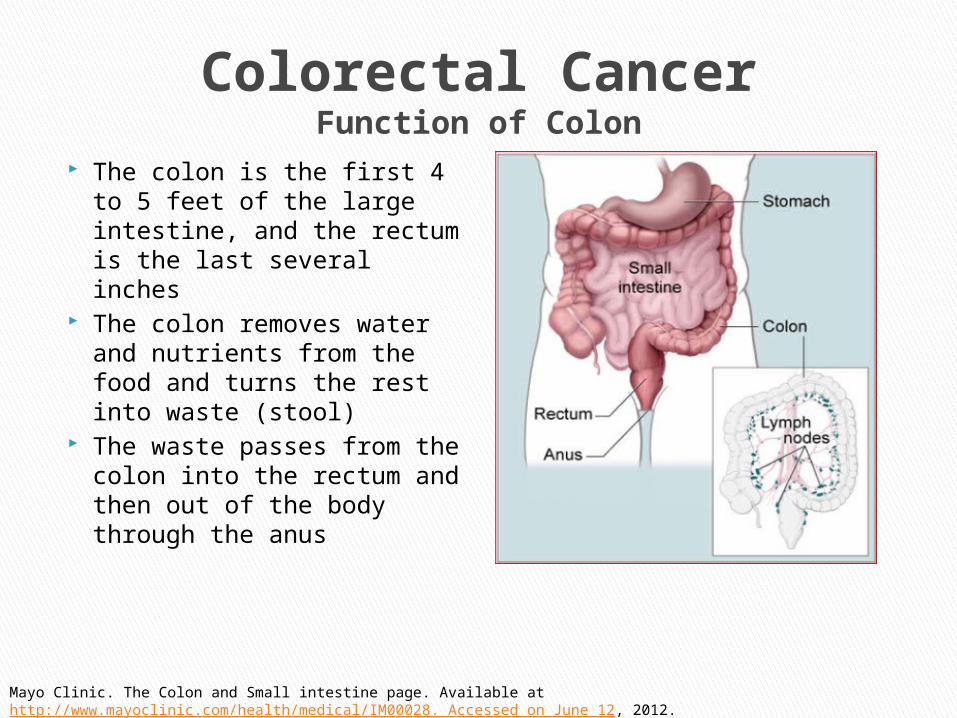
Colorectal CancerFunction of Colon
The colon is the first 4 to 5 feet of the large intestine, and the rectum is the last several inches
The colon removes water and nutrients from the food and turns the rest into waste (stool)
The waste passes from the colon into the rectum and then out of the body through the anus
Mayo Clinic. The Colon and Small intestine page. Available at http://www.mayoclinic.com/health/medical/IM00028. Accessed on June 12, 2012.
Colorectal CancerUnderstanding Cancer
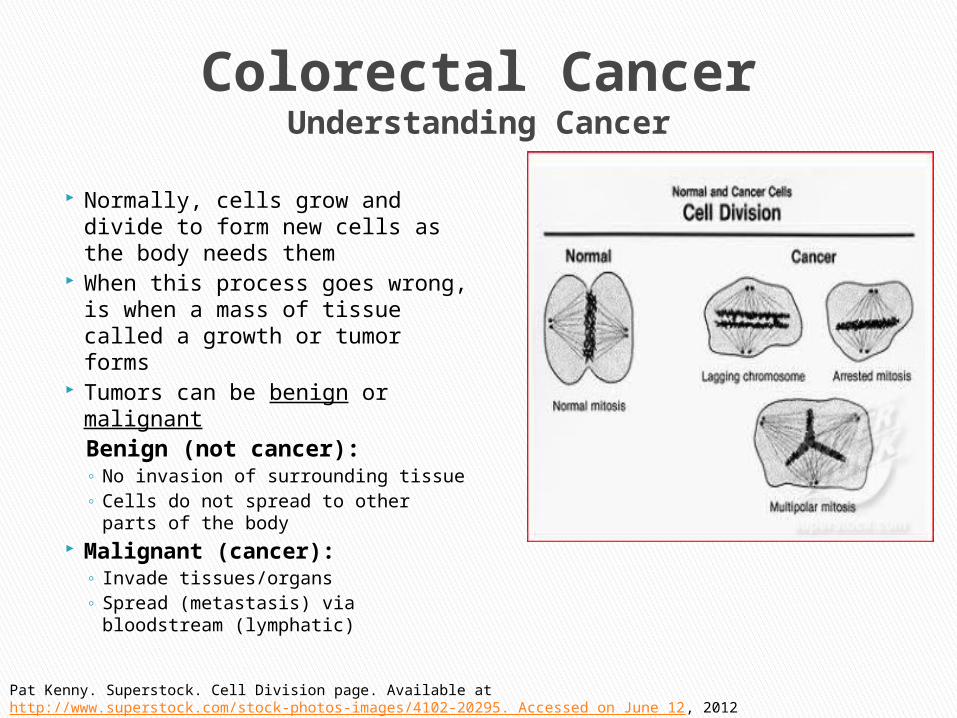
Normally, cells grow and divide to form new cells as the body needs them
When this process goes wrong, is when a mass of tissue called a growth or tumor forms
Tumors can be benign or malignantBenign (not cancer):◦ No invasion of surrounding tissue◦ Cells do not spread to other parts
of the body Malignant (cancer):
◦ Invade tissues/organs◦ Spread (metastasis) via
bloodstream (lymphatic)
Pat Kenny. Superstock. Cell Division page. Available at http://www.superstock.com/stock-photos-images/4102-20295. Accessed on June 12, 2012

Causes◦ Unknown?◦ Begins as a polyp
Risks Factors◦ > 50 yrs◦ African American/Black◦ Eat a diet high in red or processed meats◦ Have cancer elsewhere in the body◦ Have cororectal polyps◦ Have inflammatory bowel disease (Chron’s or ulcerative colities)◦ Family history of colon cancer◦ Personal history of breast cancer◦ Inherited gene mutations (rare)
Familial adenomatous polyposis (FAP) Hereditary nonpolyposis colorectal cancer (HNPCC)
◦ Smoking◦ Sedentary life-style◦ Obesity
Colorectal CancerCauses & Risk Factors

◦ Abdominal pain & tenderness in the lower abdomen◦ Blood in the stool◦ Diarrhea, constipation, or other change in bowel habits◦ Narrow stools◦ Weight loss with no known reason
Colorectal CancerSigns/Symptoms
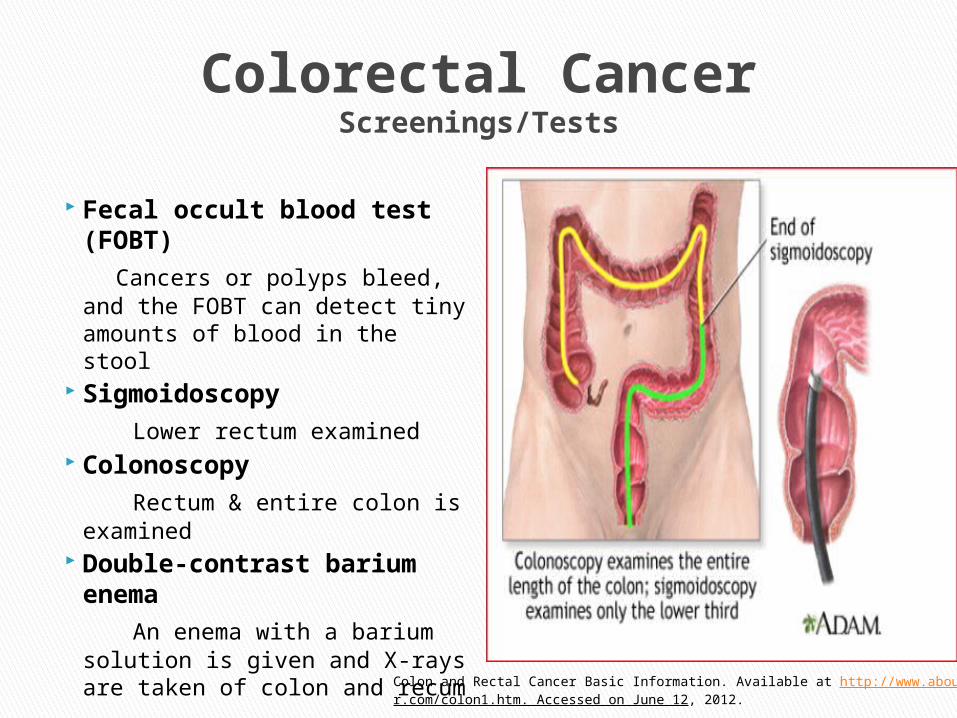
Colorectal CancerScreenings/Tests
Fecal occult blood test (FOBT)
Cancers or polyps bleed, and the FOBT can detect tiny amounts of blood in the stool
Sigmoidoscopy Lower rectum examined Colonoscopy Rectum & entire colon is
examined Double-contrast
barium enema An enema with a barium
solution is given and X-rays are taken of colon and recum
Colon and Rectal Cancer Basic Information. Available at http://www.aboutcancer.com/colon1.htm. Accessed on June 12, 2012.

Colorectal CancerHow Colorectal Cancer Spreads & Staging
How colorectal cancer spreads◦ Colorectal cancer cells most
often spread to the liver, where the disease is dx. as metastatic colorectal cancer, not liver cancer
Staging◦ Stage 0: Polyp, localized to
colon◦ Stage 1: Spread to inner linings
of colon◦ Stage 2: Extends through the
muscular wall of colon◦ Stage 3: Spread outside colon
to lymph nodes◦ Stage 4: Other organs such as
liver or lungs
Mayo Clinic. Staging of Colon Cancer. Available at http://www.mayoclinic.com/health/medical/IM01892. Accessed on June 12, 2012.

◦ Surgery (most often a colectomy)- removes cancer cells
◦ Chemotherapy-kills cancer cells◦ Radiation therapy-destroys cancerous tissue
Colorectal CancerTreatments
Case Study
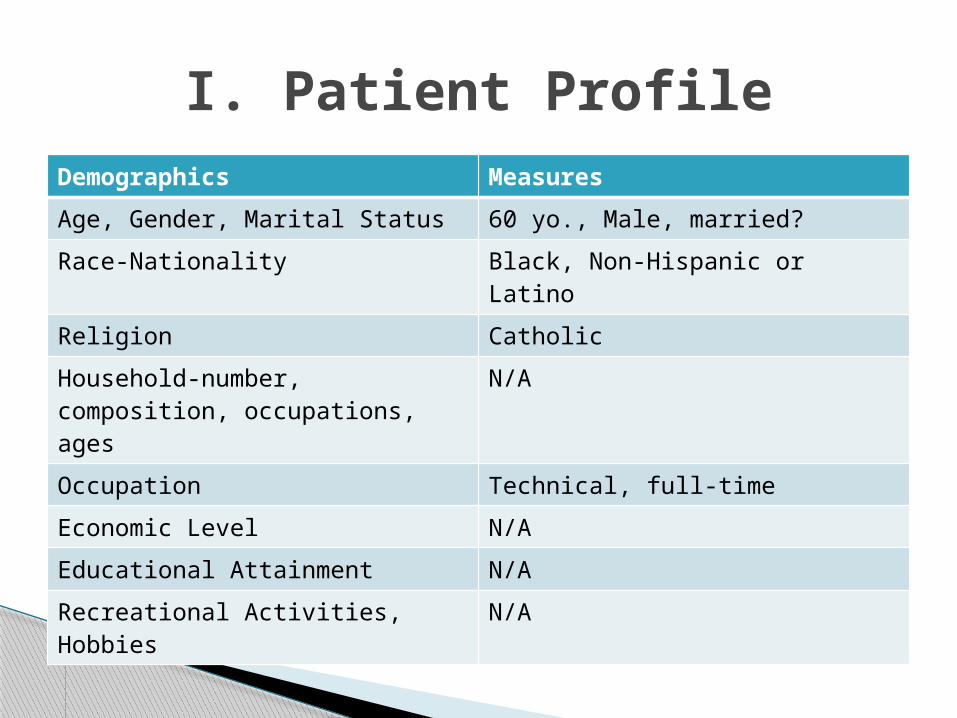
Demographics Measures
Age, Gender, Marital Status 60 yo., Male, married?
Race-Nationality Black, Non-Hispanic or Latino
Religion Catholic
Household-number, composition, occupations, ages
N/A
Occupation Technical, full-time
Economic Level N/A
Educational Attainment N/A
Recreational Activities, Hobbies N/A
I. Patient Profile

Medical Condition Symptoms of Condition
Cardiac: HTN, CHF, Hyperlipidemia
Respiratory: COPD
GI: GERD
Surgical Hx.: Herniorrhaphy
Family Hx.: CAD, HTN
Social Hx.: ETOH use: Occasionally; Tobacco use: Regular; Drug use: Denies
Allergies: N/A
II. Past Medical History( Hx)

5/7: OSH◦ Pt. presented to OSH with N/V, and abdominal pain, had a
cholecystectomy 5/14: OSH
◦ Pt presented back to OSH shortly after with intense N/V and abdominal pain.
◦ CT scan was ordered, pt. was dx. to have an ileus and large liver mass on rt. lobe
◦ A liver biopsy was performed, pt was started on TPN and then sent to UTMCK
◦ Biopsy + for cancer (CA), 5/21/12; ICU
◦ At UTMCK, pt presented with +BMs◦ D/c’s TPN◦ Waited 36 hrs, gave pt. Reglan, with clears, and then initiated TFs
with NGT to suction◦ Since + biopsy for liver CA, was decided to scope pt. via colonoscopy
to determine 1° CA site to determine if the liver mass was 2° to colorectal CA
III. Background ResearchCourse of Hospitalization
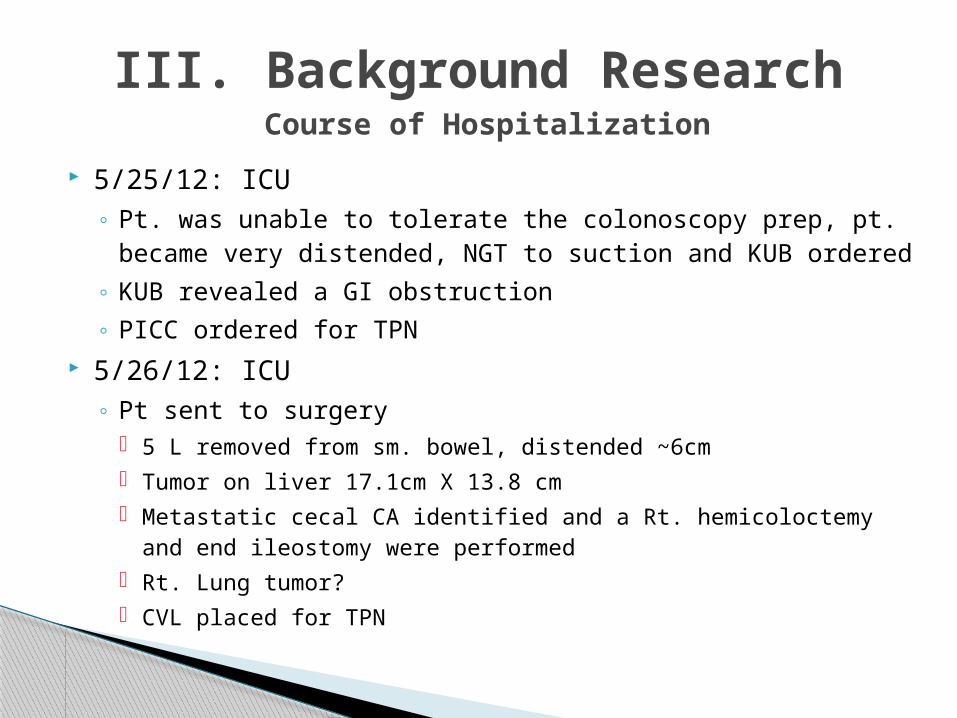
5/25/12: ICU◦ Pt. was unable to tolerate the colonoscopy prep, pt.
became very distended, NGT to suction and KUB ordered◦ KUB revealed a GI obstruction◦ PICC ordered for TPN
5/26/12: ICU◦ Pt sent to surgery
5 L removed from sm. bowel, distended ~6cm Tumor on liver 17.1cm X 13.8 cm Metastatic cecal CA identified and a Rt. hemicoloctemy and
end ileostomy were performed Rt. Lung tumor? CVL placed for TPN
III. Background Research Course of Hospitalization

Right Hemicoloctemy
Right hemicolectomy
Mayo Clinic. Colectomy. Available at http://www.mayoclinic.com/health/medical/IM00231. Accessed on June 12, 2012.

End Ileostomy
End Ileostomy
Irish Stoma Care and Colrectal Nurses Association. Available at http://www.isccna.org/ileostomy.htm. Accessed on June 12, 2012.
5/31-6/6: Floor ◦ S/P colonic resection and end ileostomy, has developed
PNA, Resp. Failure, COPD, now on BiPAP, edema, pulmonary effusion with mucus plugging, but unable to tolerate thoracentesis as yet.
◦ Metabolic acidosis 2° to acute kidney failure, nephrology consulted, pt. given Bumex + Albumen
◦ + ostomy output,+ UOP◦ Pt. voices no complaints, denies pain◦ Pt. is DNR/DNI◦ Prognosis poor◦ Nutrition: TFs
III. Background ResearchCourse of Hospitalization
III. Background ResearchLabs
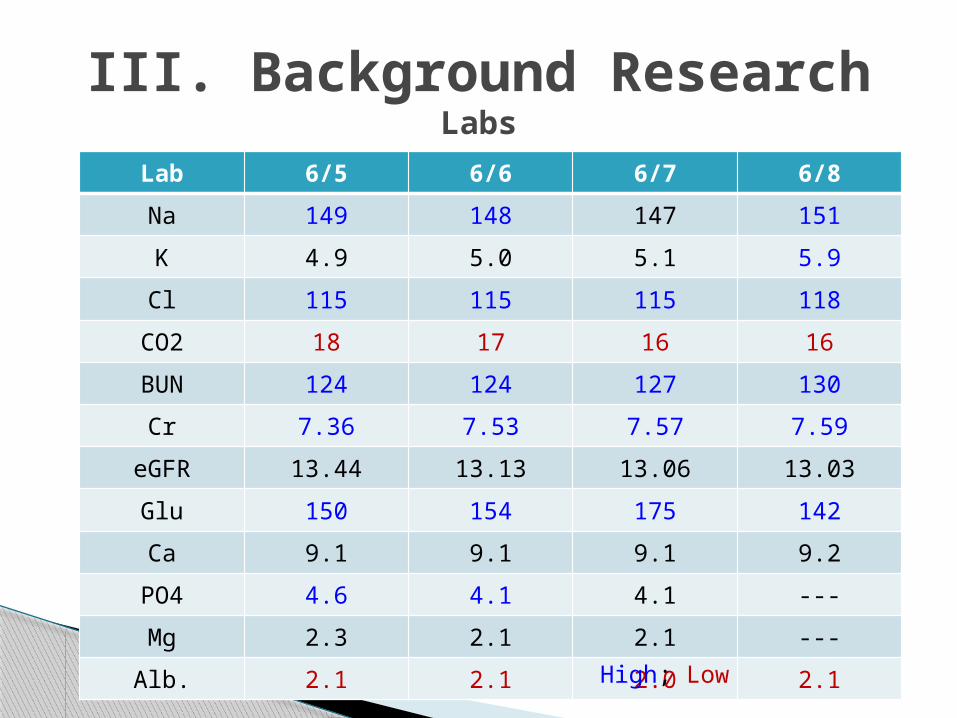
Lab 6/5 6/6 6/7 6/8
Na 149 148 147 151
K 4.9 5.0 5.1 5.9
Cl 115 115 115 118
CO2 18 17 16 16
BUN 124 124 127 130
Cr 7.36 7.53 7.57 7.59
eGFR 13.44 13.13 13.06 13.03
Glu 150 154 175 142
Ca 9.1 9.1 9.1 9.2
PO4 4.6 4.1 4.1 ---
Mg 2.3 2.1 2.1 ---
Alb. 2.1 2.1 2.0 2.1
High; Low
III. Background ResearchLabs
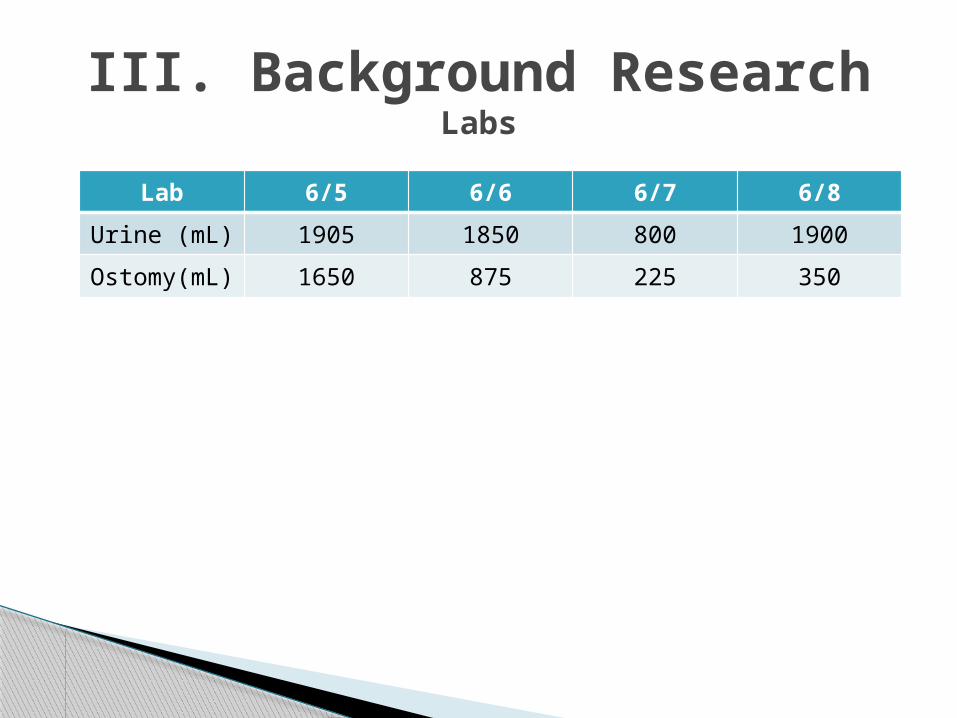
Lab 6/5 6/6 6/7 6/8
Urine (mL) 1905 1850 800 1900
Ostomy(mL)
1650 875 225 350
6/6-6/8: Floor ◦ S/P colonic resection and end ileostomy, PNA, Resp. Failure,
COPD, off BiPAP only PRN, edema, pulmonary effusion with mucus plugging
◦ Metabolic acidosis 2° to acute kidney failure, nephrology consulted,
◦ + ostomy output,+ UOP◦ Pt. voices no complaints, depressed, wants to go home, Pallative
Care discussed with family re: SNF and/or Hospice options◦ Pt. is DNR/DNI◦ Prognosis poor◦ Nutrition: Soft FT d/c’d, Renal diet, Megace and Boost ordered◦ d/c’d Bumex + Albumen
6/10:◦ Pt. d/c’d with Hospice◦ LOS: 20.0 days
III. Background ResearchCourse of Hospitalization
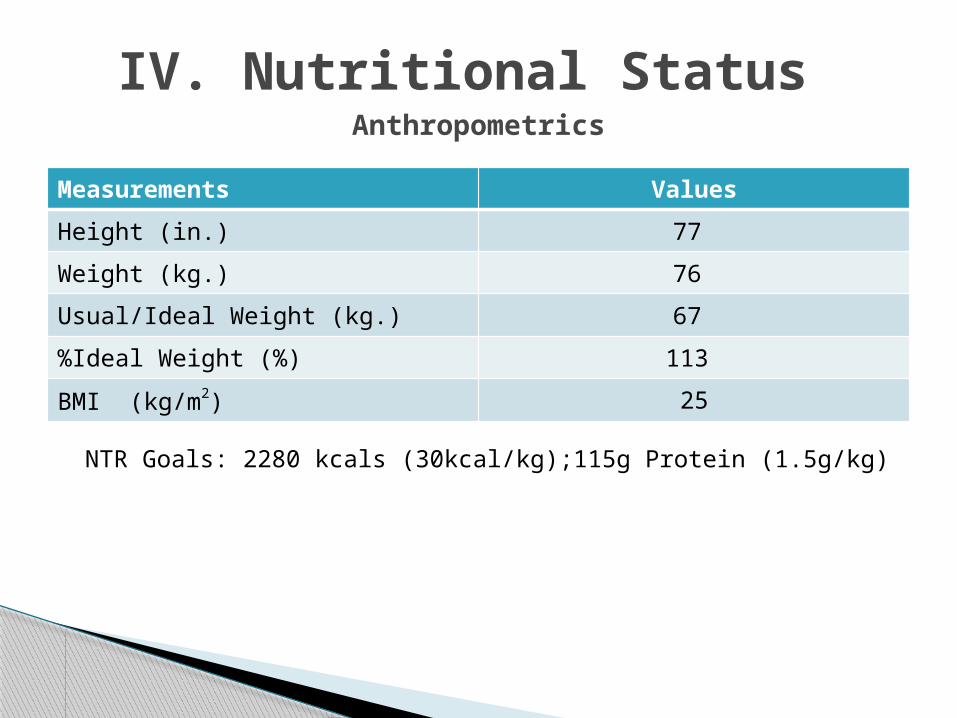
Measurements Values
Height (in.) 77
Weight (kg.) 76
Usual/Ideal Weight (kg.) 67
%Ideal Weight (%) 113
BMI (kg/m2) 25
IV. Nutritional Status Anthropometrics
NTR Goals: 2280 kcals (30kcal/kg);115g Protein (1.5g/kg)
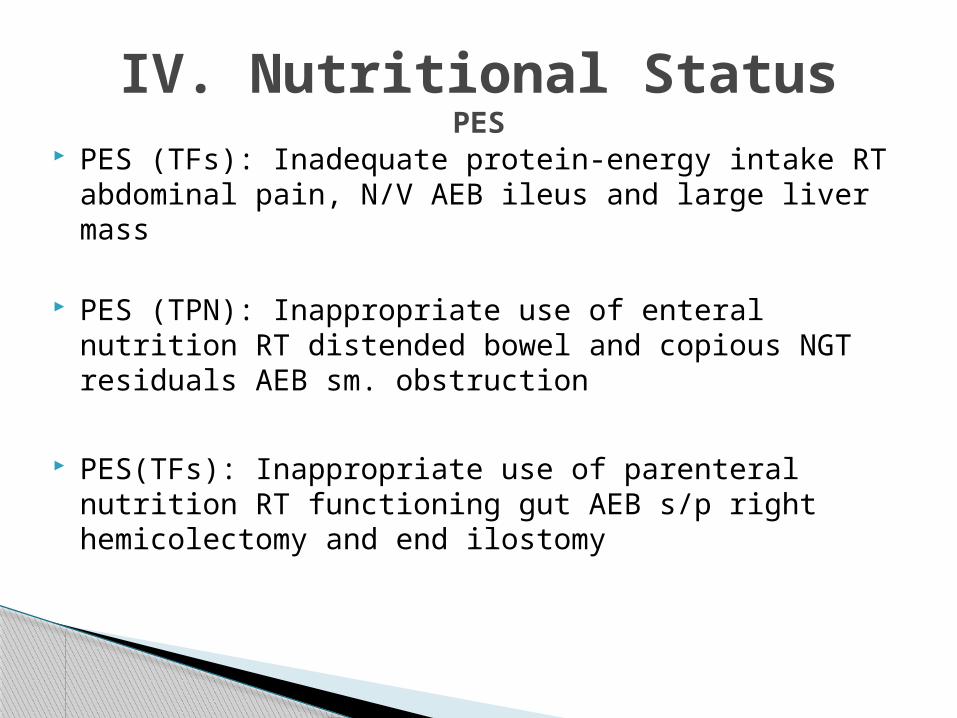
IV. Nutritional StatusPES
PES (TFs): Inadequate protein-energy intake RT abdominal pain, N/V AEB ileus and large liver mass
PES (TPN): Inappropriate use of enteral nutrition RT distended bowel and copious NGT residuals AEB sm. obstruction
PES(TFs): Inappropriate use of parenteral nutrition RT functioning gut AEB s/p right hemicolectomy and end ilostomy
Prevent Malnutrition
Ensure pt.’s est. needs are always met
Ensure pt. is tolerating chosen TF formula
Practicing evidenced-based guidelines to better ensure pt. receives the most up-to date care as practiced in the field
IV. Nutritional Status: Nutrition Care Goals
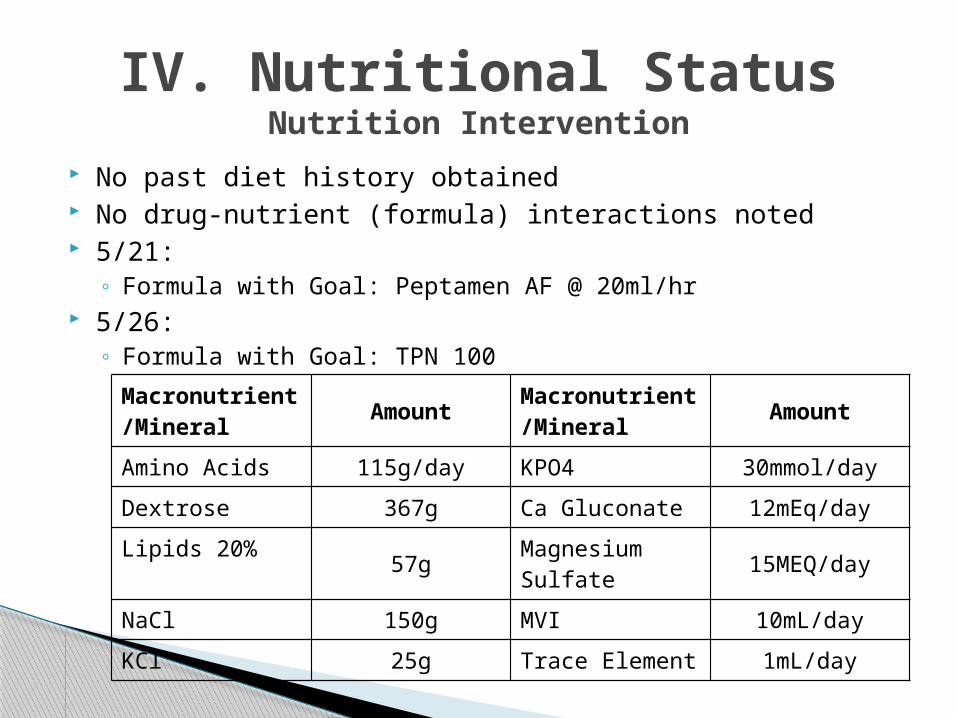
IV. Nutritional StatusNutrition Intervention
No past diet history obtained No drug-nutrient (formula) interactions noted 5/21:
◦ Formula with Goal: Peptamen AF @ 20ml/hr 5/26:
◦ Formula with Goal: TPN 100
Macronutrient/Mineral
AmountMacronutrient/Mineral
Amount
Amino Acids 115g/day KPO4 30mmol/day
Dextrose 367g Ca Gluconate 12mEq/day
Lipids 20%57g
Magnesium Sulfate
15MEQ/day
NaCl 150g MVI 10mL/day
KCl 25g Trace Element 1mL/day
IV. Nutritional Statues:Nutrition Intervention
5/28: ◦ TPN at 100ml/hr decreased rate to 85 ml/hr 2° to volume overload
5/31:◦ Formula with Goal: Peptamen AF @ 20ml/hr
6/5:◦ D/c’d Peptmen AF changed to Peptamen 1.5@ 65 ml/hr

IV. Nutritional Status:Nutrition Intervention
6/6:◦ Novasource Renal @ 40ml/hr was suggested d/t pt’s renal status
Despite pt’s AFR and related lab values, I do not feel as if Novasource Renal is an appropriate formula for the following reasons:
Protein needs will not be met Electrolytes are stable-not dehydrated + UOP and ostomy output Pt is tolerating current formula Looking at the pt as a whole, very sick. No escalading measures are to
be taken; therefore, best leave pt on formula that can tolerate 6/8:
◦ TFs d/c’d on Renal diet 6/10:
◦ Pt. d/c’d with Hospice
IV. Nutritional Status:Evaluation of Nutrition Intervention
Prevent Malnutrition
Ensure pt.’s est. needs are always met
Ensure pt. is tolerating chosen TF formula
Practicing evidenced-based guidelines to ensure the pt. receives the most up-to date care as practiced within the field

Medication Function/Purpose
Acetaminophen-oxyCodone-1 tab Pain relief
Asprin-81mg 1x/d Antiplatelet
Bumetanide (Bumex) -2mg- 1x/d Loop diuretic for heart failure & volume overload
Carvedilol-12.5mg-2x/d No selective beta 1/alpha blocker used to treat heart failure
Lansoprazole-30mg-1x/d Proton pump inhibitor
Omeprazole-20mg-1x/d Proton pump inhibitor
Ondansetron-(zofran)-4mg-1tab-1x/d
Antiemetic
OxyCodone-15mg q 4 hrs PRN Narcotic
Spirenolotone-25mg-2x/d Sparing diuretic
IV. Nutritional Status:Medications for D/C
IV. Nutritional Status: Effects of Disease on Nutritional Status
Looking just at the pt.’s surgery re: the right hemicoloctomy and end ileostomy◦ Cancer treatments will not be initiated on the patient
Greatest Concern: blockage of stoma & dehydration
Foods to Avoid: f &v skins and seeds, raw veggies, nuts, popcorn, corn, salads and dried fruit
Diet Alterations: refined breads, cereals and pastas are recommended over whole grains due to extra fiber in unrefined grains can cause digestion problems or stoma blockage
Diet Modifications: eat smaller, more frequent meals on a consistent schedule to promote regular digestion and stool output

Pt’s overall prognosis is poor Went home on Hospice care NSG d/c note:
Appears pt may have component of depression, does not wish to participate in exam, keeps
eyes closed, wants to go home [. . .] wife reports he is not wanting to eat much and does not want to interact and not happy when he woke up and saw a bag attached to him. . .
Pt. Prognosis
1. Schluter K, Gassmann P, Enns A, Korb T, Hemping-Bovenkerk A, Holzen J, Haier J. Organ-specific metastic tumor cell ahesion extravasation of colon arcinoma cells with different metastatic potential. American Journal of Pathology. 2006;69: 1064-1073.
2. Mayo Clinic. The Colon and Small intestine page. Available at http://www.mayoclinic.com/health/medical/IM00028. Accessed on June 12, 2012.
3. Pat Kenny. Superstock. Cell Division page. Available at http://www.superstock.com/stock-photos-images/4102-20295. Accessed on June 12, 2012.
4. Colon and Rectal Cancer Basic Information. Available at http://www.aboutcancer.com/colon1.htm. Accessed on June 12, 2012.
5. Mayo Clinic. Staging of Colon Cancer. Available at http://www. mayoclinic.com/health/medical/IM01892. Accessed on June 12, 2012.
6. Mayo Clinic. Colectomy. Available at http://www.mayoclinic.com/health/medical/IM00231. Accessed on June 12, 2012.
7. Irish Stoma Care and Colrectal Nurses Association. Available at http://www.isccna.org/ileostomy.htm. Accessed on June 12, 2012.
8. National Cancer Institue: Colon and rectal cancer page. Available at http://cancer.gov/cancertopics/types/colon-and-rectal. Accessed on June 12, 2012.
References
Who has the first question?
Related Documents











