Heart and Lung Center Cardiovascular Outcomes 2014

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Heart and Lung Center
Cardiovascular Outcomes 2014
Dear Colleague,
Deborah Heart and Lung Center is pleased to share with you our most recent outcomesdata. We have included the results produced by our cardiology, electrophysiology andvascular surgery divisions, in addition to cardiac surgery outcomes. At Deborah we believe that integration of different specialties–treating similar disease conditions–leadsnot only to optimal results, but provides the best and most efficient model of delivering
health care. Our commitment to excellence and providingcompassionate state-of-the-art care have been recognized
by many publically reported surveys and rankings. The most recent government HCAHPS (Hospital
Consumer Assessment of Healthcare Providers andSystems) report recognizes Deborah as the topoverall rated hospital in New Jersey! We remainappreciative of your ongoing support of Deborah’smission and look forward to providing the highestquality of care for you and your patients in
the future.
Paul Burns, MDChair of Surgery
1
Deborah is an extraordinary story, with beginningstraced to its founding in 1922 as a tuberculosissanatorium and pulmonary center. According tolegend, the therapeutic pine barren air of ruralBurlington County was key to patient recovery. Inreality, thousands of TB patients were medicallytreated and successfully cured by a heroic team ofDeborah physicians. The heart of the DeborahMission has always been compassion.
Historic Leadership.
With the development of antibiotic medicationsleading to the eradication of TB, Deborah beganexpanding its focus to other chest diseases. Dr.Charles Bailey, a pioneer in heart surgery, performedDeborah’s first open heart surgery. The specialty ofcardiac diseases was immediately embraced,transforming Deborah into New Jersey’s onlycardiac and pulmonary specialty hospital.
Next-Generation Healing.
Today, Deborah offers leading-edge surgicaltechniques and non-surgical alternatives fordiagnosing and treating all forms of cardiac, vascularand pulmonary diseases in adults, includingcongenital heart defects in children.
Deborah is consistently recognized as a leader inpatient care and innovative healing.
New advances in cardiac, pulmonary, and vascularcare for patients are almost always available first atDeborah. Among the new procedures andtechnologies first brought to the region by thehospital are: Bronchial Thermoplasty for treatingsevere asthma; Orbital Atherectomy for clearingcalcified blockages in the coronary arteries; radialartery (or wrist) catheterizations; new percutaneousinterventional abdominal aortic stent graft repair;construction of the county’s first hybrid OR, whereTranscatheter Aortic Valve Replacement (TAVR) isperformed percutaneously; and construction of thearea’s first Wound Care Center with hyperbaricchambers for intense oxygen therapy to promotewound healing. These are just some of the recentadvances in the past few months. Deborah’scompanion Clinical Research Department keeps thehospital in the loop on the most promising newtreatments and technologies.
When it’s your family’s health, don’t settle. Demand DeborahSM.
2
The Deborah Story
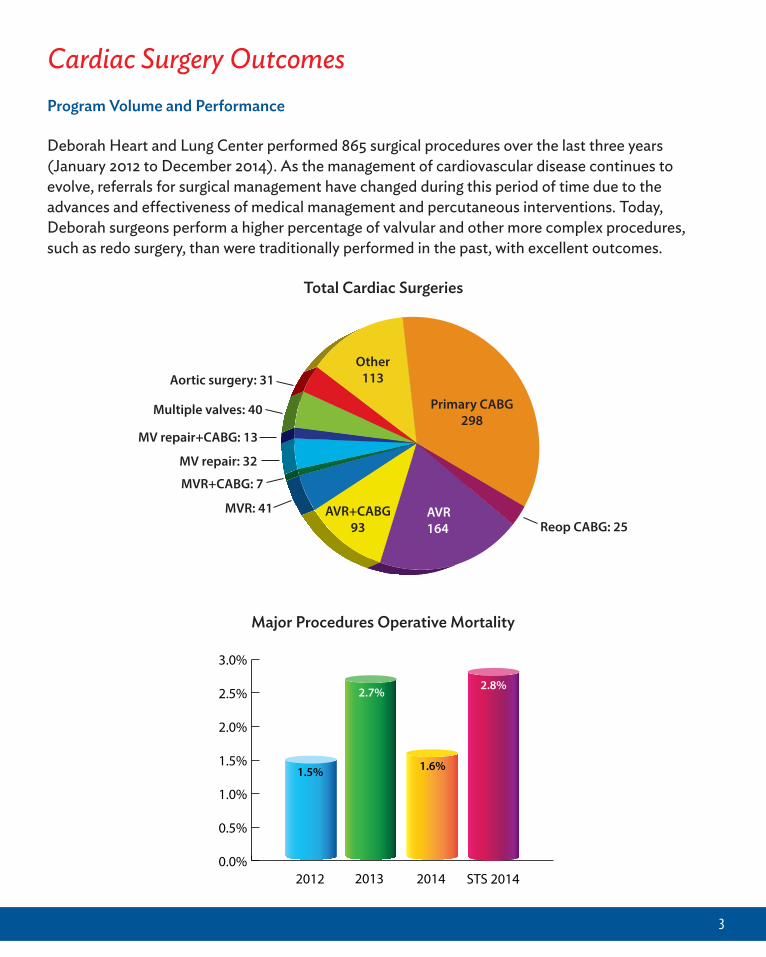
Cardiac Surgery OutcomesProgram Volume and Performance
Deborah Heart and Lung Center performed 865 surgical procedures over the last three years(January 2012 to December 2014). As the management of cardiovascular disease continues toevolve, referrals for surgical management have changed during this period of time due to theadvances and effectiveness of medical management and percutaneous interventions. Today,Deborah surgeons perform a higher percentage of valvular and other more complex procedures,such as redo surgery, than were traditionally performed in the past, with excellent outcomes.
3
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
STS 2014201420132012
1.5%
2.7%
1.6%
2.8%
Major Procedures Operative Mortality
Primary CABG298
Other113
AVR164
AVR+CABG93 Reop CABG: 25
MVR: 41
MVR+CABG: 7
MV repair: 32
MV repair+CABG: 13
Multiple valves: 40
Aortic surgery: 31
Total Cardiac Surgeries
Cardiac Surgery Outcomes (continued)
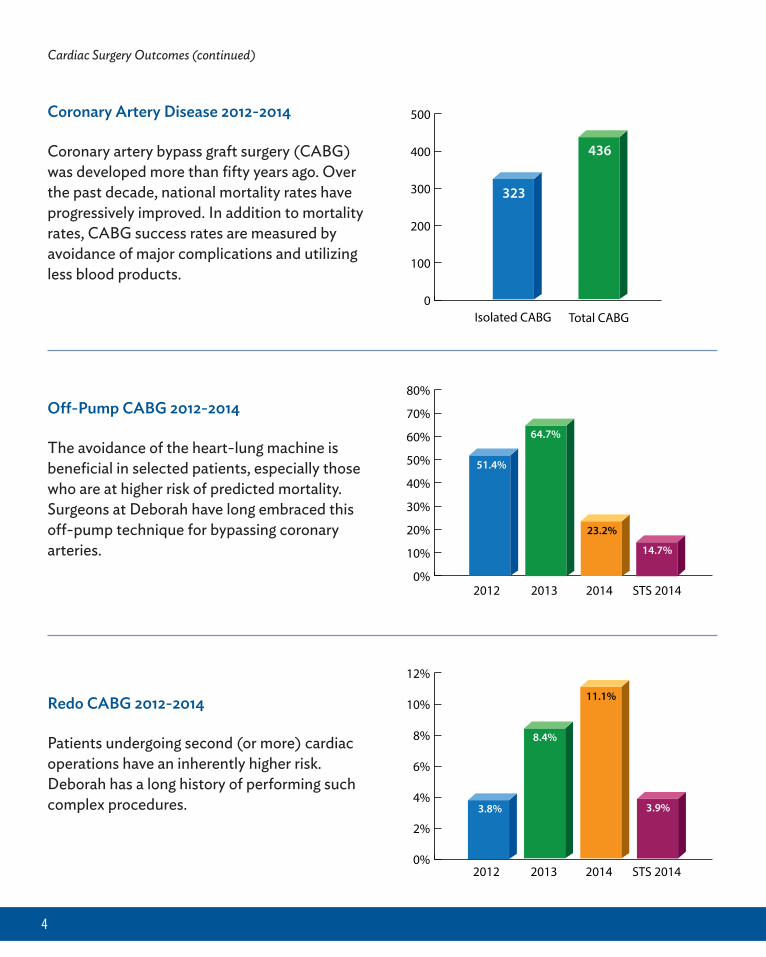
Coronary Artery Disease 2012-2014
Coronary artery bypass graft surgery (CABG)was developed more than fifty years ago. Overthe past decade, national mortality rates haveprogressively improved. In addition to mortalityrates, CABG success rates are measured byavoidance of major complications and utilizingless blood products.
Off-Pump CABG 2012-2014
The avoidance of the heart-lung machine isbeneficial in selected patients, especially thosewho are at higher risk of predicted mortality.Surgeons at Deborah have long embraced thisoff-pump technique for bypassing coronaryarteries.
Redo CABG 2012-2014
Patients undergoing second (or more) cardiacoperations have an inherently higher risk.Deborah has a long history of performing suchcomplex procedures.
4
0
100
200
300
400
500
Total CABGIsolated CABG
323
436
0%
10%
20%
30%
40%
50%
60%
70%
80%
STS 2014201420132012
51.4%
64.7%
23.2%
14.7%
0%
2%
4%
6%
8%
10%
12%
STS 2014201420132012
3.8%
8.4%
11.1%
3.9%
Cardiac Surgery Outcomes (continued)
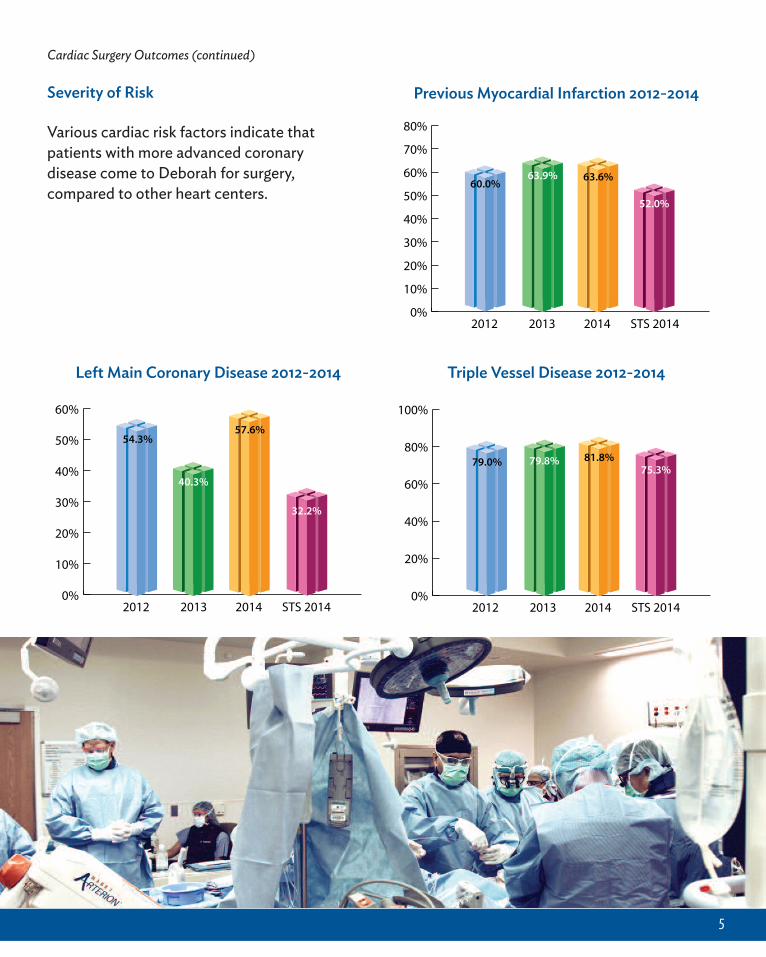
Severity of Risk
Various cardiac risk factors indicate thatpatients with more advanced coronarydisease come to Deborah for surgery,compared to other heart centers.
5
0%
10%
20%
30%
40%
50%
60%
70%
80%
STS 2014201420132012
60.0%63.9% 63.6%
52.0%
0%
10%
20%
30%
40%
50%
60%
STS 2014201420132012
54.3%
40.3%
57.6%
32.2%
0%
20%
40%
60%
80%
100%
STS 2014201420132012
75.3%79.0% 79.8% 81.8%
Previous Myocardial Infarction 2012-2014
Left Main Coronary Disease 2012-2014 Triple Vessel Disease 2012-2014
Cardiac Surgery Outcomes (continued)
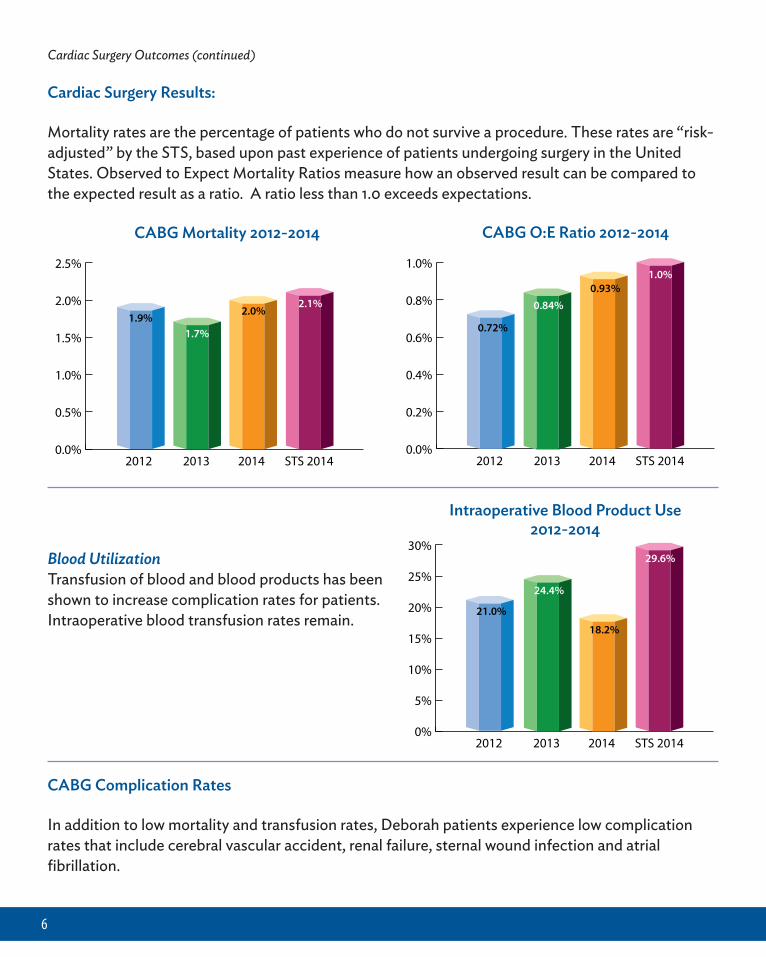
Cardiac Surgery Results:
Mortality rates are the percentage of patients who do not survive a procedure. These rates are “risk-adjusted” by the STS, based upon past experience of patients undergoing surgery in the UnitedStates. Observed to Expect Mortality Ratios measure how an observed result can be compared tothe expected result as a ratio. A ratio less than 1.0 exceeds expectations.
Blood UtilizationTransfusion of blood and blood products has beenshown to increase complication rates for patients.Intraoperative blood transfusion rates remain.
6
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
STS 2014201420132012
1.9%1.7%
2.0%2.1%
0.0%
0.2%
0.4%
0.6%
0.8%
1.0%
STS 2014201420132012
0.72%
0.84%0.93%
1.0%
0%
5%
10%
15%
20%
25%
30%
STS 2014201420132012
21.0%
24.4%
18.2%
29.6%
CABG Mortality 2012-2014 CABG O:E Ratio 2012-2014
Intraoperative Blood Product Use2012-2014
CABG Complication Rates
In addition to low mortality and transfusion rates, Deborah patients experience low complicationrates that include cerebral vascular accident, renal failure, sternal wound infection and atrialfibrillation.
Cardiac Surgery Outcomes (continued)
7
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
0%
STS 2014201420132012
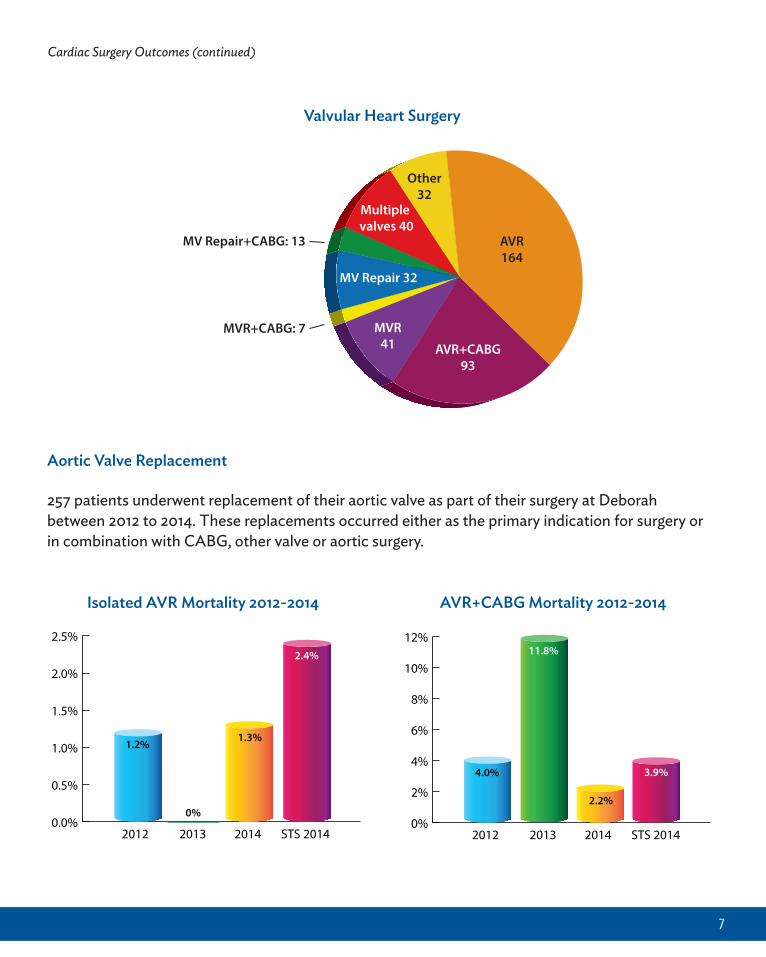
1.2%1.3%
2.4%
0%
2%
4%
6%
8%
10%
12%
STS 2014201420132012
4.0%
11.8%
2.2%
3.9%
Other32
Multiple valves 40
AVR164
AVR+CABG93
MVR41
MV Repair 32
MV Repair+CABG: 13
MVR+CABG: 7
AVR+CABG Mortality 2012-2014Isolated AVR Mortality 2012-2014
Aortic Valve Replacement
257 patients underwent replacement of their aortic valve as part of their surgery at Deborahbetween 2012 to 2014. These replacements occurred either as the primary indication for surgery orin combination with CABG, other valve or aortic surgery.
Valvular Heart Surgery
Cardiac Surgery Outcomes (continued)
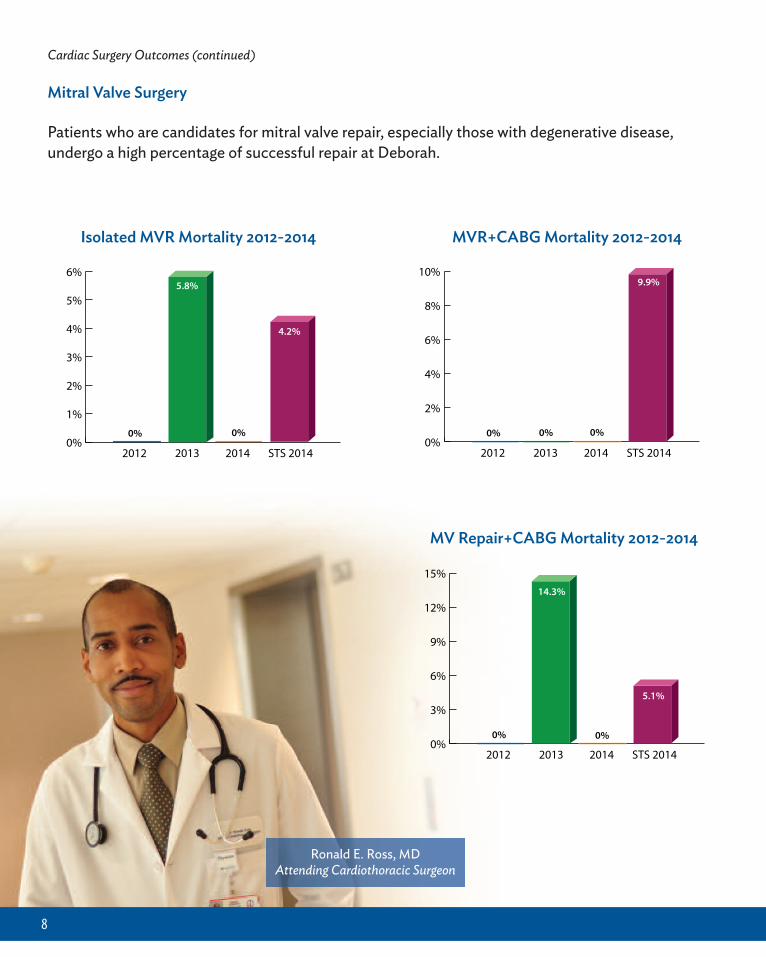
Mitral Valve Surgery
Patients who are candidates for mitral valve repair, especially those with degenerative disease,undergo a high percentage of successful repair at Deborah.
8
0%
1%
2%
3%
4%
5%
6%
0% 0%
STS 2014201420132012
4.2%
5.8%
0%
2%
4%
6%
8%
10%
0% 0% 0%
STS 2014201420132012
9.9%
0%
3%
6%
9%
12%
15%
0% 0%
STS 2014201420132012
14.3%
5.1%
MV Repair+CABG Mortality 2012-2014
MVR+CABG Mortality 2012-2014Isolated MVR Mortality 2012-2014
Ronald E. Ross, MDAttending Cardiothoracic Surgeon
9
Cardiac Surgery Outcomes (continued)
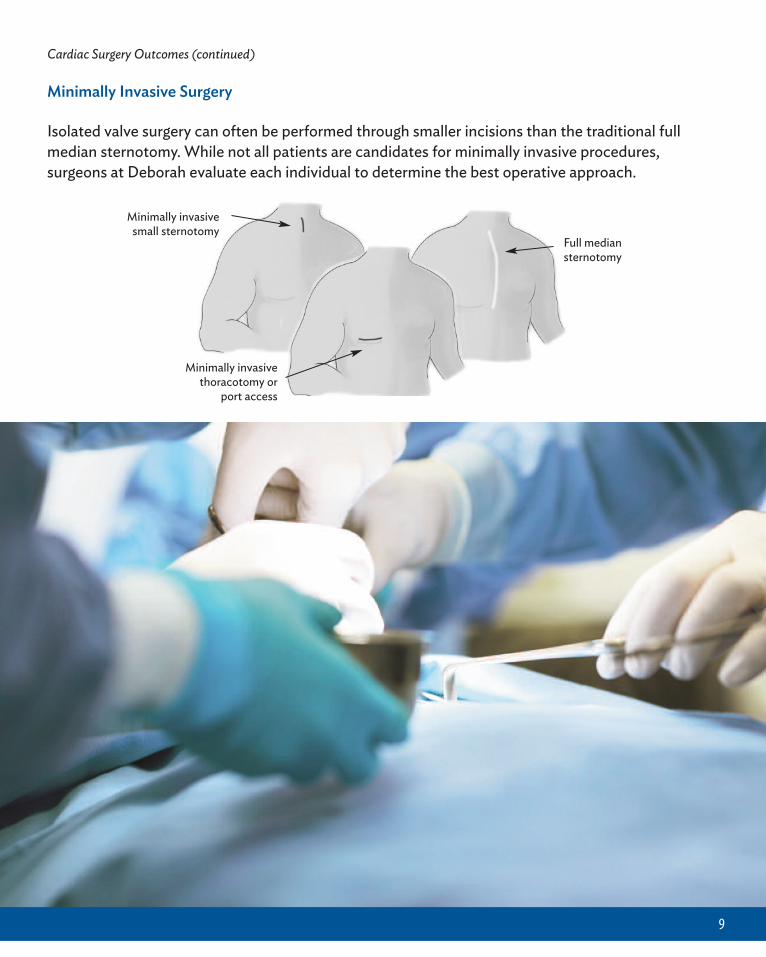
Minimally Invasive Surgery
Isolated valve surgery can often be performed through smaller incisions than the traditional fullmedian sternotomy. While not all patients are candidates for minimally invasive procedures,surgeons at Deborah evaluate each individual to determine the best operative approach.
Minimally invasivesmall sternotomy
Full mediansternotomy
Minimally invasivethoracotomy or
port access
10
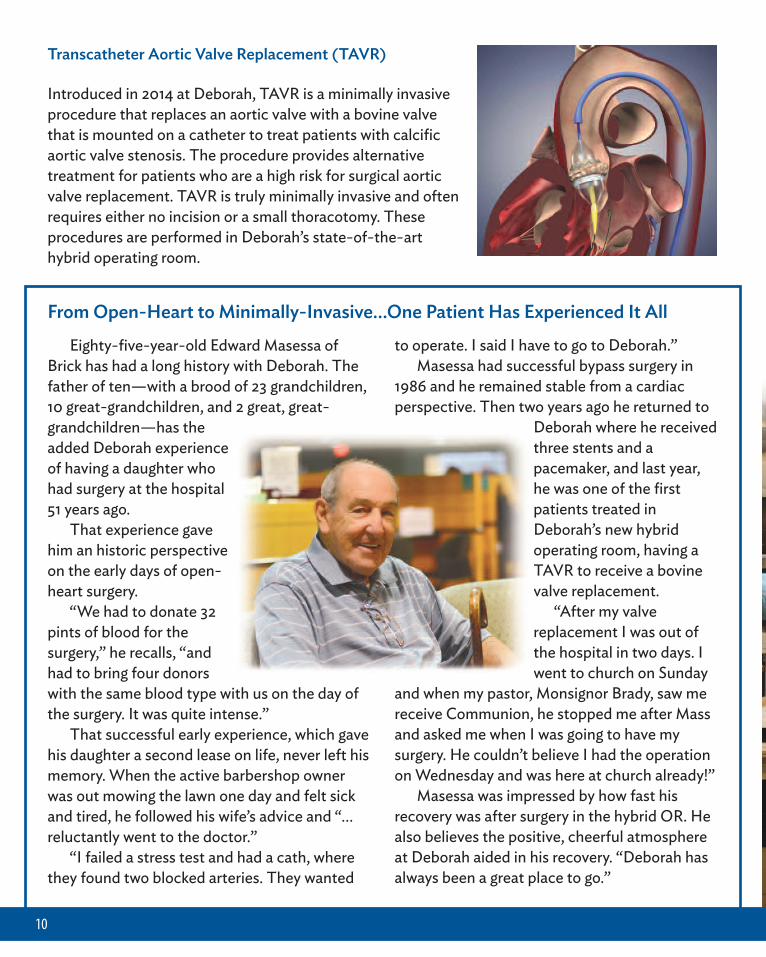
Transcatheter Aortic Valve Replacement (TAVR)
Introduced in 2014 at Deborah, TAVR is a minimally invasiveprocedure that replaces an aortic valve with a bovine valvethat is mounted on a catheter to treat patients with calcificaortic valve stenosis. The procedure provides alternativetreatment for patients who are a high risk for surgical aorticvalve replacement. TAVR is truly minimally invasive and oftenrequires either no incision or a small thoracotomy. Theseprocedures are performed in Deborah’s state-of-the-arthybrid operating room.
Eighty-five-year-old Edward Masessa ofBrick has had a long history with Deborah. Thefather of ten—with a brood of 23 grandchildren,10 great-grandchildren, and 2 great, great-grandchildren—has theadded Deborah experienceof having a daughter whohad surgery at the hospital51 years ago. That experience gavehim an historic perspectiveon the early days of open-heart surgery. “We had to donate 32pints of blood for thesurgery,” he recalls, “andhad to bring four donorswith the same blood type with us on the day ofthe surgery. It was quite intense.” That successful early experience, which gavehis daughter a second lease on life, never left hismemory. When the active barbershop ownerwas out mowing the lawn one day and felt sickand tired, he followed his wife’s advice and “…reluctantly went to the doctor.” “I failed a stress test and had a cath, wherethey found two blocked arteries. They wanted
to operate. I said I have to go to Deborah.” Masessa had successful bypass surgery in1986 and he remained stable from a cardiacperspective. Then two years ago he returned to
Deborah where he receivedthree stents and apacemaker, and last year,he was one of the firstpatients treated inDeborah’s new hybridoperating room, having aTAVR to receive a bovinevalve replacement.
“After my valvereplacement I was out ofthe hospital in two days. Iwent to church on Sunday
and when my pastor, Monsignor Brady, saw mereceive Communion, he stopped me after Massand asked me when I was going to have mysurgery. He couldn’t believe I had the operationon Wednesday and was here at church already!” Masessa was impressed by how fast hisrecovery was after surgery in the hybrid OR. Healso believes the positive, cheerful atmosphereat Deborah aided in his recovery. “Deborah hasalways been a great place to go.”
From Open-Heart to Minimally-Invasive…One Patient Has Experienced It All
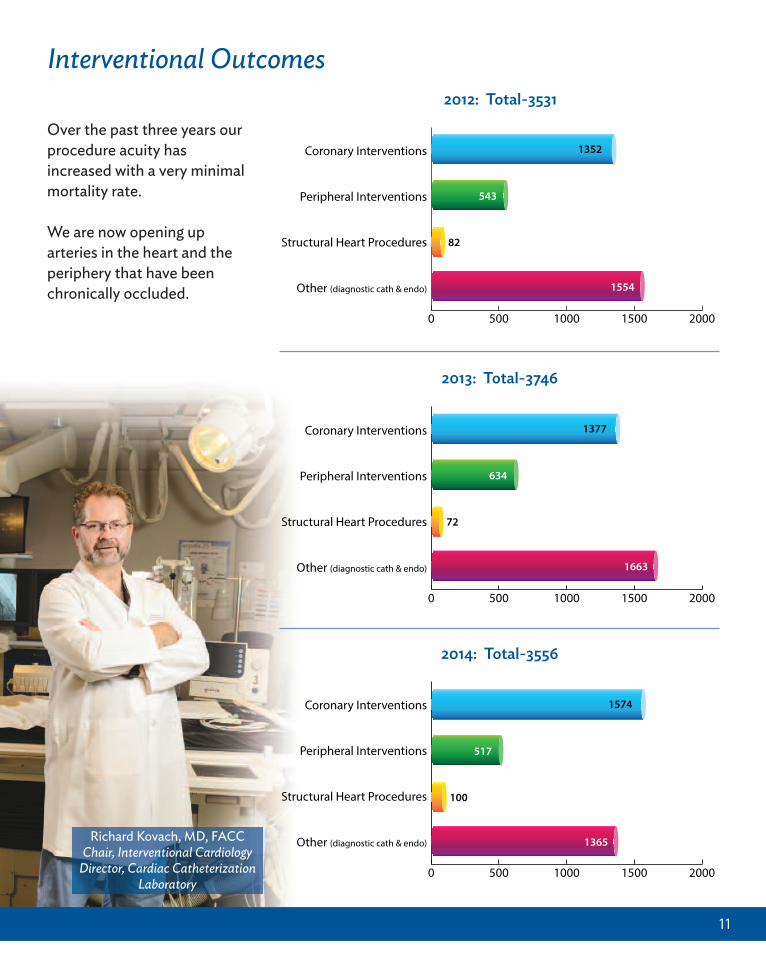
Over the past three years ourprocedure acuity hasincreased with a very minimalmortality rate.
We are now opening uparteries in the heart and theperiphery that have beenchronically occluded.
11
0 500 1000 1500 2000
Other (diagnostic cath & endo)
Structural Heart Procedures
Peripheral Interventions
Coronary Interventions 1352
543
82
1554
2
0 500 1000 1500 2000
Other (diagnostic cath & endo)
Structural Heart Procedures
Peripheral Interventions
Coronary Interventions 1377
634
72
1663
2
0 500 1000 1500 2000
Other (diagnostic cath & endo)
Structural Heart Procedures
Peripheral Interventions
Coronary Interventions 1574
517
100
1365
2012: Total-3531
2013: Total-3746
2014: Total-3556
Interventional Outcomes
Richard Kovach, MD, FACCChair, Interventional Cardiology
Director, Cardiac CatheterizationLaboratory
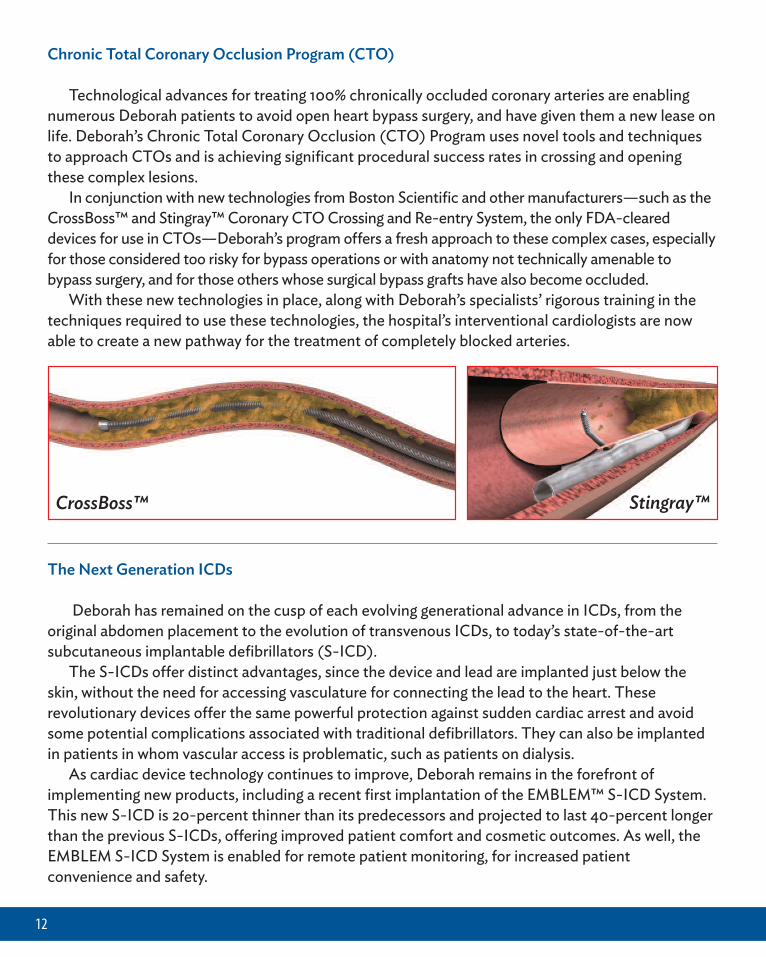
Chronic Total Coronary Occlusion Program (CTO)
Technological advances for treating 100% chronically occluded coronary arteries are enablingnumerous Deborah patients to avoid open heart bypass surgery, and have given them a new lease onlife. Deborah’s Chronic Total Coronary Occlusion (CTO) Program uses novel tools and techniquesto approach CTOs and is achieving significant procedural success rates in crossing and openingthese complex lesions.
In conjunction with new technologies from Boston Scientific and other manufacturers—such as theCrossBoss™ and Stingray™ Coronary CTO Crossing and Re-entry System, the only FDA-cleareddevices for use in CTOs—Deborah’s program offers a fresh approach to these complex cases, especiallyfor those considered too risky for bypass operations or with anatomy not technically amenable tobypass surgery, and for those others whose surgical bypass grafts have also become occluded.
With these new technologies in place, along with Deborah’s specialists’ rigorous training in thetechniques required to use these technologies, the hospital’s interventional cardiologists are nowable to create a new pathway for the treatment of completely blocked arteries.
12
CrossBoss™ Stingray™
The Next Generation ICDs
Deborah has remained on the cusp of each evolving generational advance in ICDs, from theoriginal abdomen placement to the evolution of transvenous ICDs, to today’s state-of-the-artsubcutaneous implantable defibrillators (S-ICD).
The S-ICDs offer distinct advantages, since the device and lead are implanted just below theskin, without the need for accessing vasculature for connecting the lead to the heart. Theserevolutionary devices offer the same powerful protection against sudden cardiac arrest and avoidsome potential complications associated with traditional defibrillators. They can also be implantedin patients in whom vascular access is problematic, such as patients on dialysis.
As cardiac device technology continues to improve, Deborah remains in the forefront ofimplementing new products, including a recent first implantation of the EMBLEM™ S-ICD System.This new S-ICD is 20-percent thinner than its predecessors and projected to last 40-percent longerthan the previous S-ICDs, offering improved patient comfort and cosmetic outcomes. As well, theEMBLEM S-ICD System is enabled for remote patient monitoring, for increased patientconvenience and safety.
Team Approach to Structural Heart Procedures
Deborah’s innovative multidisciplinary approach for patients with advanced and complexstructural heart disease now offers patients considered too risky for conventional open-heartsurgery non-surgical alternatives with very effective long-term results.
Deborah’s team—including cardiologists, interventional cardiologists, surgeons, imagingspecialists, and anesthesiologists—works as a coordinated unit in the hospital’s state-of-the-arthybrid operating room, where these complex catheter-based, or minimally-invasive, procedures canbe performed with far less pain, and a quicker recovery than conventional open surgical procedures.
Deborah has performed over 254 minimally-invasive structural heart procedures from 2012 to 2014.
13
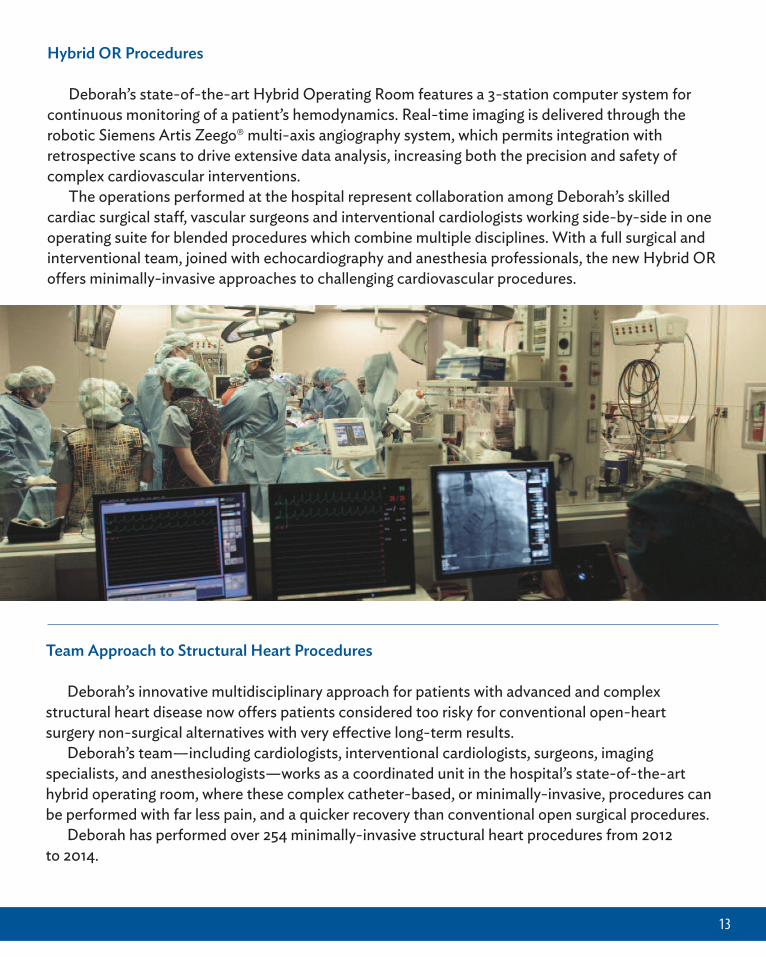
Hybrid OR Procedures
Deborah’s state-of-the-art Hybrid Operating Room features a 3-station computer system forcontinuous monitoring of a patient’s hemodynamics. Real-time imaging is delivered through therobotic Siemens Artis Zeego® multi-axis angiography system, which permits integration withretrospective scans to drive extensive data analysis, increasing both the precision and safety ofcomplex cardiovascular interventions.
The operations performed at the hospital represent collaboration among Deborah’s skilledcardiac surgical staff, vascular surgeons and interventional cardiologists working side-by-side in oneoperating suite for blended procedures which combine multiple disciplines. With a full surgical andinterventional team, joined with echocardiography and anesthesia professionals, the new Hybrid ORoffers minimally-invasive approaches to challenging cardiovascular procedures.
14
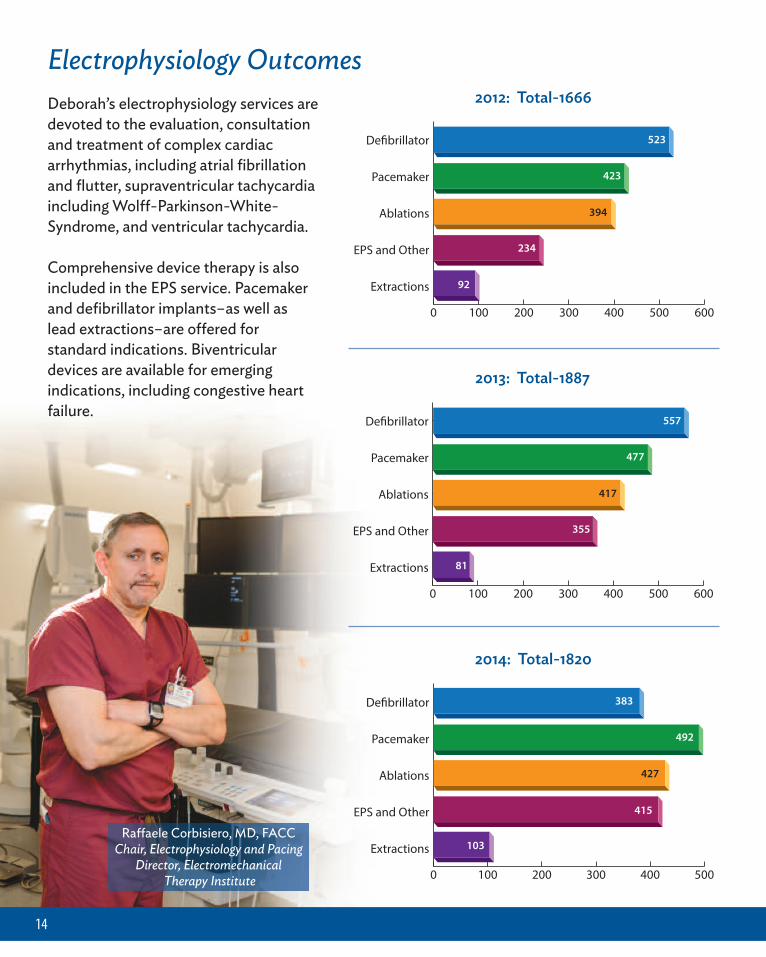
Electrophysiology Outcomes
0 100 200 300 400 500
Extractions
EPS and Other
Ablations
Pacemaker
De!brillator 383
492
427
415
103
2014: Total-1820
0 100 200 300 400 500 600
Extractions
EPS and Other
Ablations
Pacemaker
De!brillator 557
477
417
355
81
2013: Total-1887
0 100 200 300 400 500 600
Extractions
EPS and Other
Ablations
Pacemaker
De!brillator 523
423
394
234
92
2012: Total-1666
Raffaele Corbisiero, MD, FACCChair, Electrophysiology and Pacing
Director, ElectromechanicalTherapy Institute
Deborah’s electrophysiology services aredevoted to the evaluation, consultationand treatment of complex cardiacarrhythmias, including atrial fibrillationand flutter, supraventricular tachycardiaincluding Wolff-Parkinson-White-Syndrome, and ventricular tachycardia.
Comprehensive device therapy is alsoincluded in the EPS service. Pacemakerand defibrillator implants–as well aslead extractions–are offered forstandard indications. Biventriculardevices are available for emergingindications, including congestive heartfailure.
15
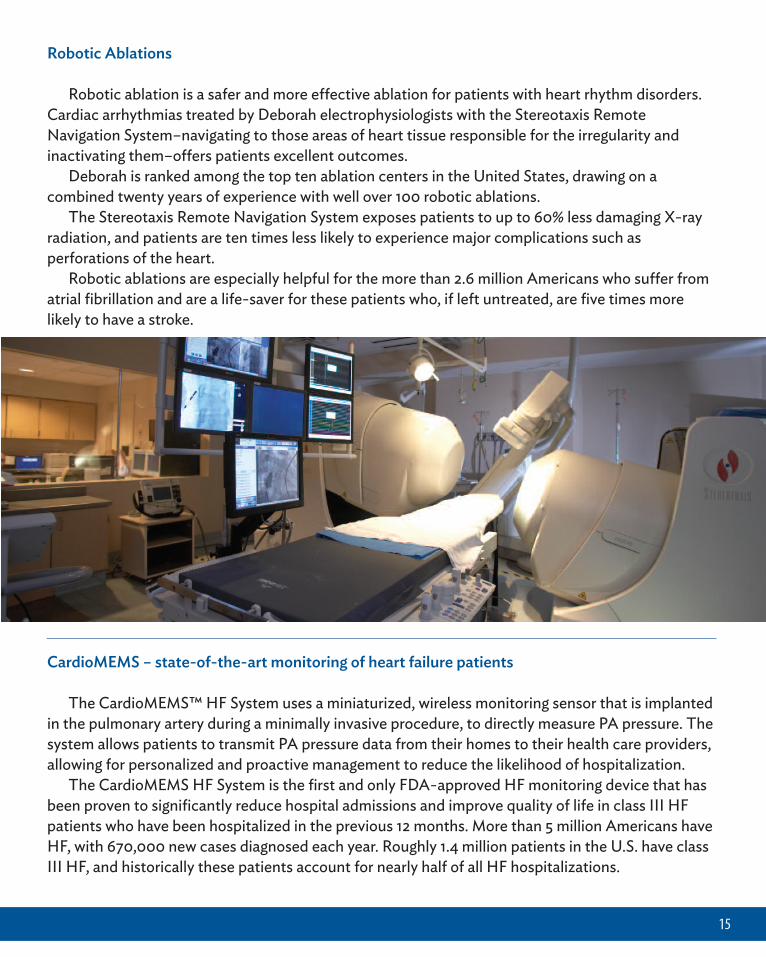
Robotic Ablations
Robotic ablation is a safer and more effective ablation for patients with heart rhythm disorders.Cardiac arrhythmias treated by Deborah electrophysiologists with the Stereotaxis RemoteNavigation System–navigating to those areas of heart tissue responsible for the irregularity andinactivating them–offers patients excellent outcomes.
Deborah is ranked among the top ten ablation centers in the United States, drawing on acombined twenty years of experience with well over 100 robotic ablations.
The Stereotaxis Remote Navigation System exposes patients to up to 60% less damaging X-rayradiation, and patients are ten times less likely to experience major complications such asperforations of the heart.
Robotic ablations are especially helpful for the more than 2.6 million Americans who suffer fromatrial fibrillation and are a life-saver for these patients who, if left untreated, are five times morelikely to have a stroke.
CardioMEMS – state-of-the-art monitoring of heart failure patients
The CardioMEMS™ HF System uses a miniaturized, wireless monitoring sensor that is implantedin the pulmonary artery during a minimally invasive procedure, to directly measure PA pressure. Thesystem allows patients to transmit PA pressure data from their homes to their health care providers,allowing for personalized and proactive management to reduce the likelihood of hospitalization.
The CardioMEMS HF System is the first and only FDA-approved HF monitoring device that hasbeen proven to significantly reduce hospital admissions and improve quality of life in class III HFpatients who have been hospitalized in the previous 12 months. More than 5 million Americans haveHF, with 670,000 new cases diagnosed each year. Roughly 1.4 million patients in the U.S. have classIII HF, and historically these patients account for nearly half of all HF hospitalizations.
16
ICD Lead Extraction
Implantable cardioverter defibrillators (ICDs) have been in use since the 1980s. Since thetechnology’s introduction, ICDs have saved and prolonged thousands of lives. A side consequence,however, is that over time the leads can become infected or ineffective and need to be extractedand replaced. Deborah stands as a regional leader in this advanced procedure.
Deborah’s extraction techniques adhere to the Heart Rhythm Society’s recommendations. Inaddition, the hospital uses Cook Medical’s lead extraction tools, backed by 25 years of extractionexperience. The extraction system relies primarily on a locking stylet and the concept ofcountertraction, as well as a telescoping sheath — a vast improvement from the early days of leadextraction when physicians tried various methods of pulling leads out using a weighted pulleysystem, or resorting to open heart surgery.
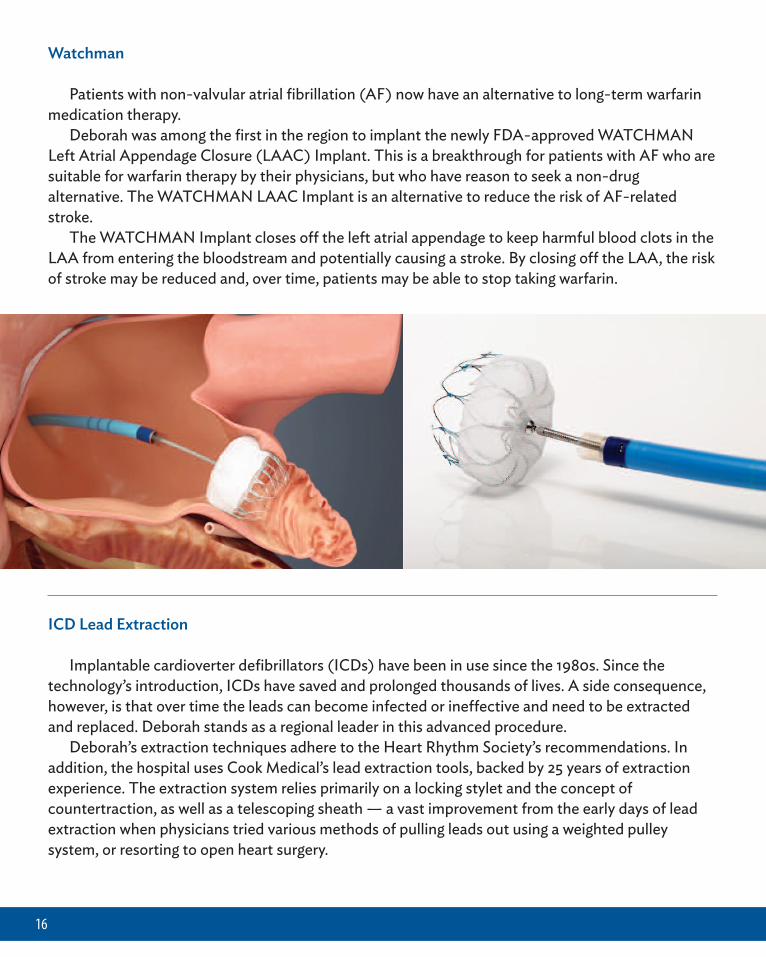
Watchman
Patients with non-valvular atrial fibrillation (AF) now have an alternative to long-term warfarinmedication therapy.
Deborah was among the first in the region to implant the newly FDA-approved WATCHMANLeft Atrial Appendage Closure (LAAC) Implant. This is a breakthrough for patients with AF who aresuitable for warfarin therapy by their physicians, but who have reason to seek a non-drugalternative. The WATCHMAN LAAC Implant is an alternative to reduce the risk of AF-relatedstroke.
The WATCHMAN Implant closes off the left atrial appendage to keep harmful blood clots in theLAA from entering the bloodstream and potentially causing a stroke. By closing off the LAA, the riskof stroke may be reduced and, over time, patients may be able to stop taking warfarin.
17
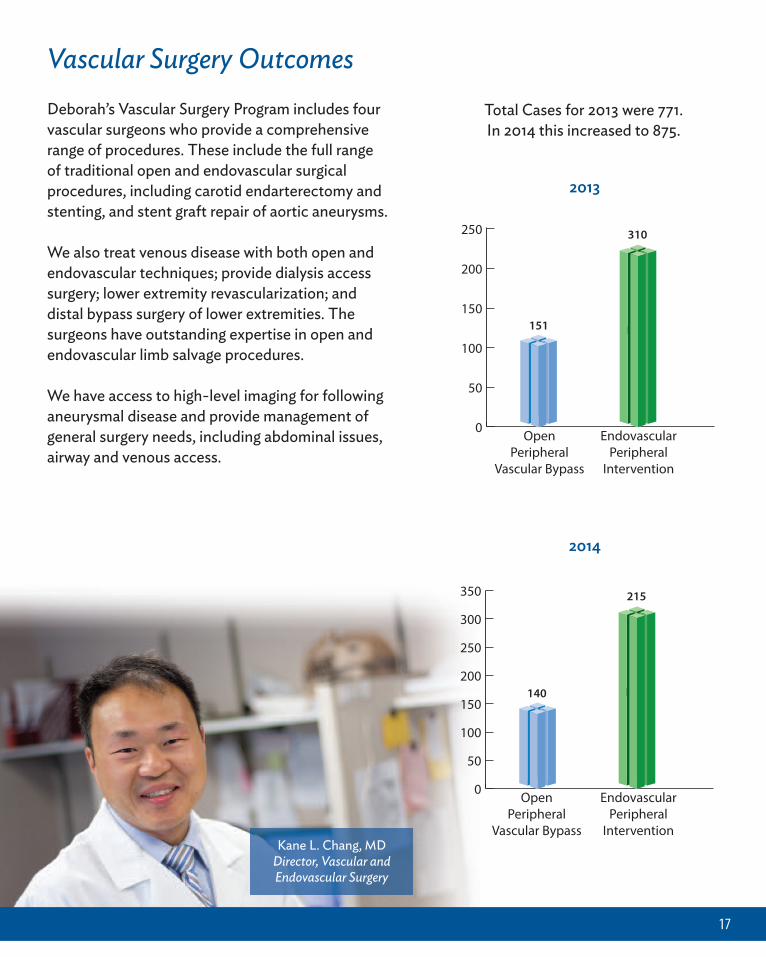
Kane L. Chang, MDDirector, Vascular and Endovascular Surgery
Vascular Surgery OutcomesTotal Cases for 2013 were 771.In 2014 this increased to 875.
0
50
100
150
200
250
EndovascularPeripheral
Intervention
OpenPeripheral
Vascular Bypass
151
310
151
0
50
100
150
200
250
300
350
EndovascularPeripheral
Intervention
OpenPeripheral
Vascular Bypass
151
215
140
2013
2014
Deborah’s Vascular Surgery Program includes fourvascular surgeons who provide a comprehensiverange of procedures. These include the full rangeof traditional open and endovascular surgicalprocedures, including carotid endarterectomy andstenting, and stent graft repair of aortic aneurysms.
We also treat venous disease with both open andendovascular techniques; provide dialysis accesssurgery; lower extremity revascularization; anddistal bypass surgery of lower extremities. Thesurgeons have outstanding expertise in open andendovascular limb salvage procedures.
We have access to high-level imaging for followinganeurysmal disease and provide management ofgeneral surgery needs, including abdominal issues,airway and venous access.
18
0
20
40
60
80
100
CarotidStent
CarotidEndarterectomy
12
88
0
20
40
60
80
100
CarotidStent
CarotidEndarterectomy
9
86
2013 2014
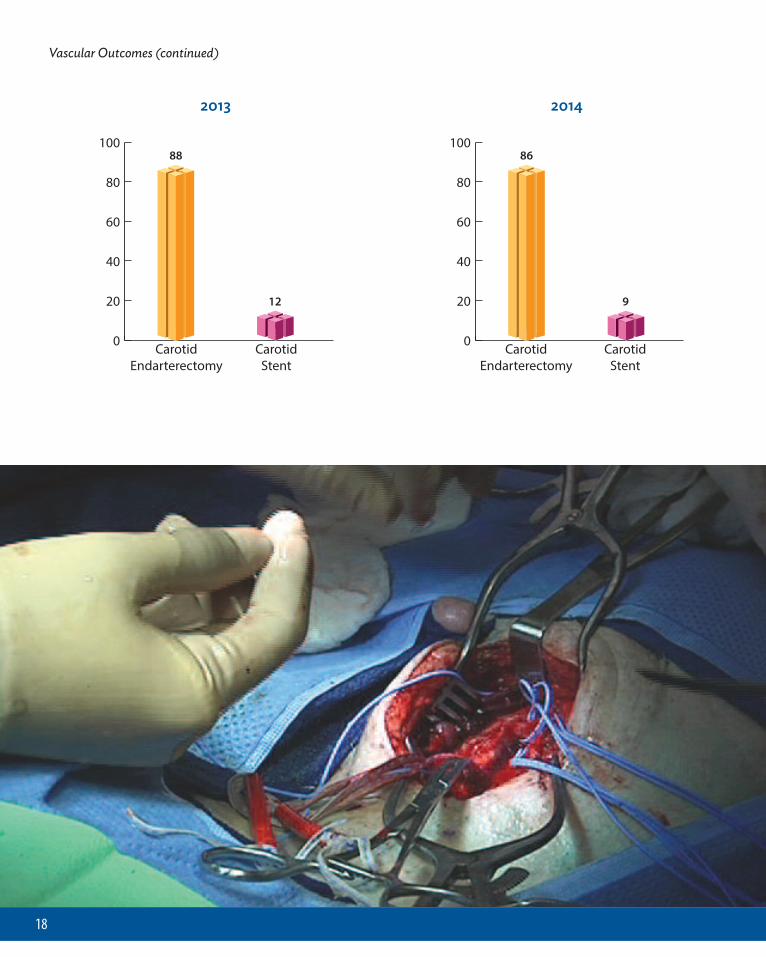
Vascular Outcomes (continued)
19
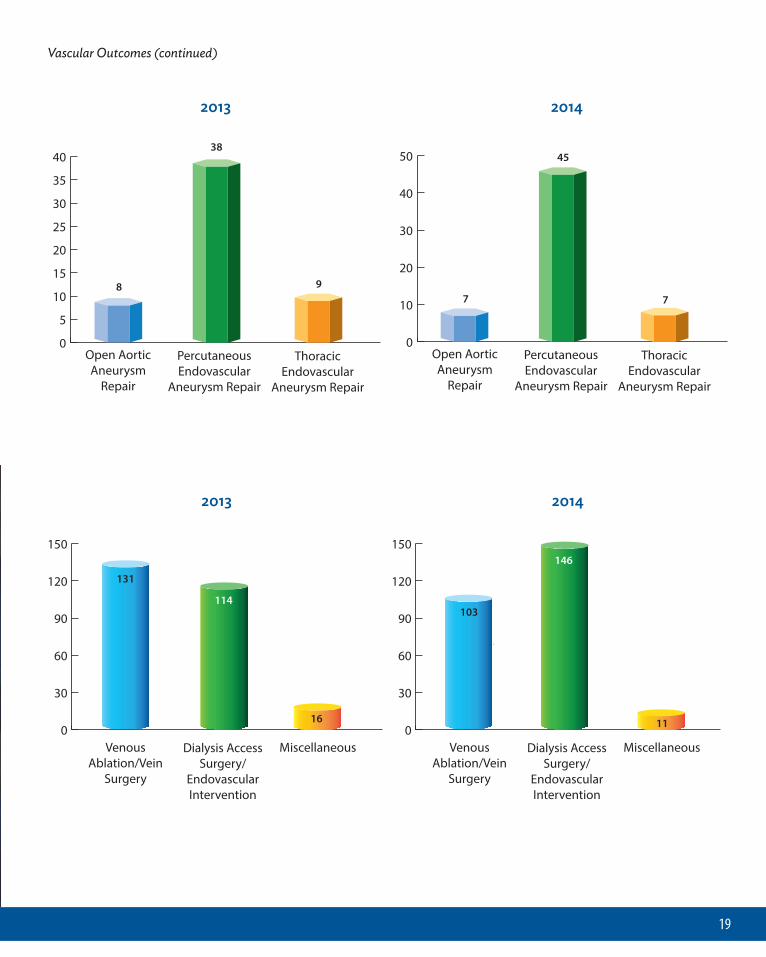
Vascular Outcomes (continued)
0
5
10
15
20
25
30
35
40
ThoracicEndovascular
Aneurysm Repair
PercutaneousEndovascular
Aneurysm Repair
Open AorticAneurysm
Repair
8
38
9
2013 2014
0
10
20
30
40
50
7
45
7
ThoracicEndovascular
Aneurysm Repair
PercutaneousEndovascular
Aneurysm Repair
Open AorticAneurysm
Repair
2013 2014
0
30
60
90
120
150
131
114
16
MiscellaneousDialysis AccessSurgery/
EndovascularIntervention
VenousAblation/Vein
Surgery
0
30
60
90
120
150
103
146
11
MiscellaneousDialysis AccessSurgery/
EndovascularIntervention
VenousAblation/Vein
Surgery
The Vein Center
Deborah’s Vein Center looks below the surface of unsightly spider and varicose veins, todetermine whether these unattractive – and easily removed – veins are a sign of a deeper circulationproblem or more severe condition.
Deborah’s highly qualified staff is able to appropriately diagnose and treat these vein conditions.If the veins are superficial, recommendations including the use of compression stockings andelevating legs while sitting, can offer conservative management. If they need treatment, Deborah’sVein Center specialists have a range of tools in their arsenal, including: radiofrequency ablation, theVenefit Closure, sclerotherapy, and phlebectomy, among other treatments.
If, however, the veins are the sign of a more serious condition such as deep vein thrombosis(DVT), Deborah’s team is highly skilled in appropriate surgical options.
Abdominal Aortic Aneurysms
More than one million people are living with undiagnosed Abdominal Aortic Aneurysms (AAA).An estimated 95% of all AAAs can be successfully treated if detected prior to rupture, but ifundetected until rupture, only 10-25% of patients survive.
Deborah is expert in diagnosing and treating AAAs, a weakening and bulging of the aorta.Despite the fact that this condition is the third leading cause of sudden death in men over 60 yearsof age, when detected, Deborah’s surgical/interventional team has a very successful track recordover the years in repairing AAAs.
Early detection is key for successful repair. Men with a history of smoking, high blood pressure,high cholesterol, family history of the disease, and those who have undergone bypass surgery arerecommended for an ultrasound. If an aneurysm is detected, the skilled surgical/interventional teamat Deborah can offer a life-saving repair.
20
21
The Women’s Heart Center
Deborah’s Women’s Heart Center is focused on closing the healthcare gap for women who toooften miss the early warning signs of heart disease, the number one killer among American women.
The Women’s Heart Center team blends multi-disciplinary expertise in the areas of cardiology,endocrinology, pulmonology, imaging, congestive heart failure and diabetes. The program also has
extended Deborah resources from its Institute forSleep Medicine; the Joslin Diabetes CenterAffiliate at Deborah; and on-site, highly-skillednutritionists. Deborah’s female physicianspecialists offer dedicated women’s clinic time tofocus on their patients and build an overall healthprofile. With this “big picture” in mind, Deborah’sspecialists can then recommend a pro-active planfor reducing stress, losing weight, quittingsmoking, eating better, sleeping more soundly,managing diabetes, and teaching about the earlysigns and symptoms of heart disease.
Heart Failure Experts
More than two-thirds of heart failure patientsare under the care of a primary care physician.Assessing a patient’s level of heart failure via theAmerican Heart Association and AmericanCollege of Cardiology (AHA/ACC)s’ levels ofheart failure– Stages A-D – offers excellentguidelines for when to bring Deborah’s specialtyexpertise into play.
In Stage A, patients are symptomless, but atrisk. Here a primary care physician can havetremendous impact on a patient with lifestyle modifications such as quitting smoking and exercising.Medications are helpful at this point if a patient has hypertension or other early signs of heartdisease.
In Stage B, when an initial diagnosis of heart failure is determined by a reduced ejection fraction,a cardiology consult is warranted. Deborah’s Electromechanical Therapy Institute can evaluate earlyprocedural interventions with the goal of preventing future heart damage.
As heart failure progresses through Stage C and into Stage D – advanced heart failure – patientsshould be fully transitioned into a specialty program such as Deborah’s for consistent monitoring,aggressive medication, and state-of-the-art treatment opportunities.

Clinical Research
Deborah’s innovative Clinical Research Departmentis currently involved in over 30 innovative trialsexploring new treatments and procedures inElectrophysiology, Interventional Cardiology,Peripheral Vascular Disease, and PreventiveCardiology. In addition to highly committed andtalented Principal Investigators, the Clinical ResearchTeam at Deborah provides superior patient supportthrough its research associates, who keep bothreferring physicians and patients apprised of not onlytheir progress, but that of the clinical research study,at each step of the way.
22
Parachute® Ventricular Partitioning Device
Patients at Deborah now have access to a new clinical research device whichoffers hope to those suffering from heart failure caused by damage to and
weakening of the heart muscle following a heart attack.Deborah is the first investigational site in New Jersey, New York, and
Eastern Pennsylvania to implant the Parachute Ventricular PartitioningDevice, which is a minimally-invasive approach to this life-threatening
condition.Through a catheter inserted in the femoral artery, the Parachuteimplant is deployed in the left ventricle to partition the damagedmuscle, excluding the non-functional heart segment from the healthy,functional segment to decrease the overall volume of the left ventricleand restore its geometry and functionality.
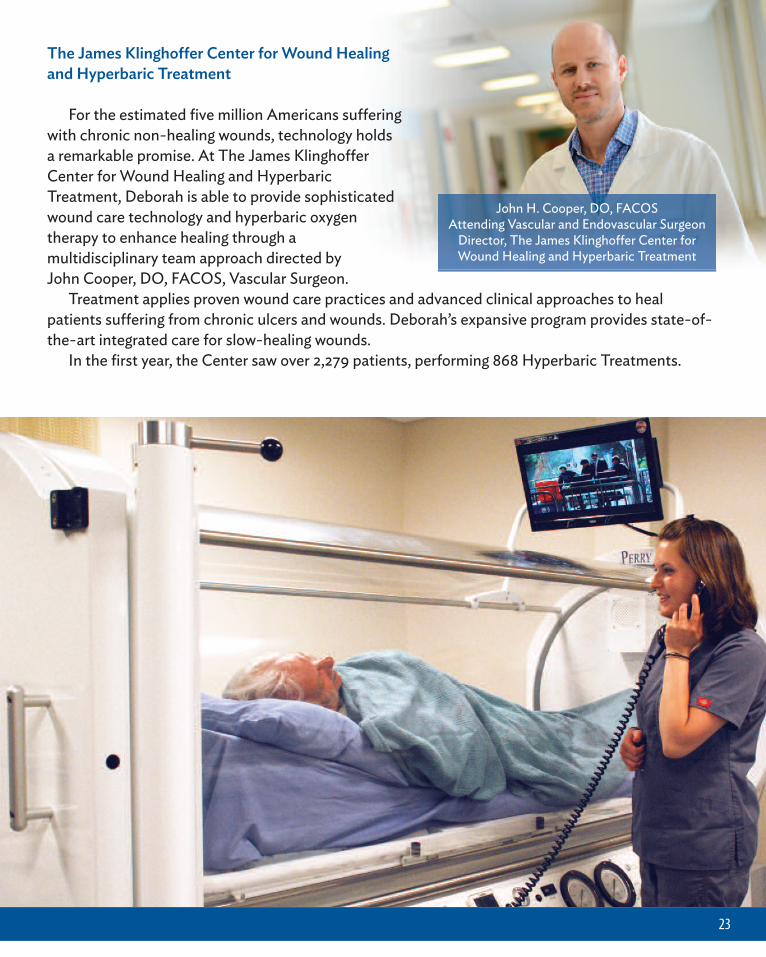
The James Klinghoffer Center for Wound Healingand Hyperbaric Treatment
For the estimated five million Americans sufferingwith chronic non-healing wounds, technology holdsa remarkable promise. At The James KlinghofferCenter for Wound Healing and HyperbaricTreatment, Deborah is able to provide sophisticatedwound care technology and hyperbaric oxygentherapy to enhance healing through amultidisciplinary team approach directed by John Cooper, DO, FACOS, Vascular Surgeon.
Treatment applies proven wound care practices and advanced clinical approaches to healpatients suffering from chronic ulcers and wounds. Deborah’s expansive program provides state-of-the-art integrated care for slow-healing wounds.
In the first year, the Center saw over 2,279 patients, performing 868 Hyperbaric Treatments.
23
John H. Cooper, DO, FACOSAttending Vascular and Endovascular Surgeon
Director, The James Klinghoffer Center forWound Healing and Hyperbaric Treatment
Walter Boris, DO, FACOSAttending Thoracic SurgeonAttending Thoracic Surgeon,Robert Wood Johnson UniversityHospital HamiltonClinical Assistant Professor,Philadelphia College ofOsteopathic Medicine
Dr. Boris joined Deborah’ssurgical staff following a distinguished military medicalcareer as an officer in the United States Army. Doubleboard certified in both general surgery and thoraciccardiovascular surgery, Dr. Boris completed his training ingeneral surgery at Community General Hospital inHarrisburg, Pennsylvania, and his specialized training inthoracic cardiovascular surgery was completed atDeborah Heart and Lung Center. Clinical assistantprofessor at Philadelphia College of OsteopathicMedicine, Dr. Boris additionally serves as adjunct thoracicsurgeon at Robert Wood Johnson University HospitalHamilton. Published in eminent medical journals andassociations, Dr. Boris is also on the Board of Directors,Cardiothoracic Section Chair, of the AmericanOsteopathic Board of Surgery, also serving as a BoardExaminer. Dr. Boris’ special interests include cardiacsurgery, thoracic surgery, vascular surgery and surgicalcritical care.
Ronald E. Ross, MDAttending CardiothoracicSurgeon*Services provided under contractby Mid-Atlantic Surgical Associates
Dr. Ross is board certified ingeneral surgery and thoracicsurgery. He joined Deborah aftercompleting his cardiothoracic
surgery fellowship at Strong Memorial Hospital inRochester, NY, which is ranked by U.S. News & WorldReport in the highest category for cardiology and heartsurgery volume, advanced technologies and patientservices. Dr. Ross has written extensively for peer-reviewed publications, such as the American Journal ofSurgery, among others. His interests include all aspects ofadult cardiac surgery.
SURGERY
Paul Gerard Burns, MDChair, Department of Surgery*Services provided under contractby Mid-Atlantic Surgical Associates
Dr. Burns is board certified insurgery and thoracic surgery. Hehas practiced cardiac surgery inNJ for over fourteen years withexceptional outcomes. Since
beginning his general surgical residency at HarvardMedical School Deaconess Hospital over 25 years ago, hispersonal achievements include several distinguishedawards, also named a “Top Doctor” numerous times bystate and national magazines, including U.S. News &World Report for the years 2011-2014. He is widelypublished in well-known medical and scientific journals,and has a special interest in minimally invasivecardiothoracic surgery.
24
Kane L. Chang, MDDirector, Vascular andEndovascular Surgery
Dr. Chang joined Deborah in2006 and helped propel theexpansion of the hospital’svascular surgery department intoone of the leading vascularsurgery departments in New
Jersey. He is double board certified by the AmericanCollege of Surgeons in general and vascular surgery, witha special interest in vascular and endovascular surgery.Dr. Chang has presented at various professionalgatherings, such as the New York Vascular SocietyMeeting and the Eastern Vascular Society, and hasconducted scientific research. Dr. Chang received hismedical degree from New York University School ofMedicine and has been recognized as a “Top Doc” by SJMagazine and “Rising Star Top Doc” by PhiladelphiaMagazine. Notably, Dr. Chang is on the cutting edge of

Matthew S. Samra, DOAttending Vascular andEndovascular SurgeonDirector, Vein Center
Dr. Samra joined Deborah in2004, where he began his sub-specialty training in cardiac andthoracic surgery fellowship,followed by a vascular and
endovascular fellowship. He is triple-board certified ingeneral, vascular and cardiothoracic surgery and is amember of the American Osteopathic Association. He isalso the Chief of Vascular Surgery at Southern OceanMedical Center in Manahawkin, NJ and is a clinicalinstructor for multiple medical schools. He carriesexpertise in all aspects of vascular and endovascularsurgery as well as treatment and repair of thoracic andabdominal aneurysms, arterial blockages, venous disease,treatment of varicose and spider veins, and carotidstenosis. Dr. Samra is involved in multiple trials evaluatingthe latest vascular and endovascular technologies. He hasreceived multiple “Patient Choice” and “Best Physician”awards over the years including the prestigiousCompassionate Doctor Recognition, of which only a smallpercentage of physicians nationwide are accorded thishonor. Dr. Samra’s special interests lie in the areas ofendovascular treatments of vascular disease, venousdisease, and new technologies and techniques in theareas of vascular and endovascular diseases.
Vijay Kamath, MDAttending Vascular Surgeon
Dr. Kamath completed hisvascular surgery training at JobstVascular Institute in Toledo, OHand joined Deborah’s vascularsurgical team in September 2014.He has a special interest inperipheral vascular disease,
venous disease and cerebrovascular disease. Dr. Kamathis a member of several professional societies including theSociety of Vascular Surgeons, the American College ofSurgeons, the American Venous Forum, Society ofClinical Vascular Surgery, and is a Registered Physician inVascular Interpretation. He has presented at symposiumsand lectures, and is published in various peer-reviewedmedical and scientific journals as well as contributed tochapters in medical textbooks.
John H. Cooper, DO, FACOSAttending Vascular andEndovascular SurgeonDirector, Vascular SurgeryFellowship ProgramDirector, The James KlinghofferCenter for Wound Healing andHyperbaric Treatment
Having graduated from theUniversity of Medicine and Dentistry of New Jersey,School of Osteopathic Medicine, where he also receivedspecialty training in open and endovascular surgery, Dr.Cooper continues as Chief Clinical Faculty Advisor forClinically Integrated Human Anatomy at this prestigiousschool. He is double board certified by the AmericanOsteopathic Board of Vascular Surgery and the AmericanOsteopathic Board of General Surgery, and is a memberof the International Society of Vascular Surgery, AmericanCollege of Osteopathic Surgeons, American OsteopathicBoard of Surgeons, Osteopathic Political ActionCommittee and the American Osteopathic Association.He has been recognized by his peers and patients alike asa “Top Doc,” “Top Physician,” Surgery Mentor of the Year,and has received such prominent awards as The FrederickG. Meoli Scientific Paper Award and The Elmer GrimesMemorial Award. Dr. Cooper specializes in endovascularsurgery, venous disease, complex lower extremityrevascularization, wound care and holds a special interestin endovascular surgery and medical illustration.
25
the latest minimally invasive surgical techniques fortreating patients with vascular diseases, particularlyendovascular treatment for abdominal and thoracic aorticaneurysms and peripheral arterial diseases.

26
ELECTROPHYSIOLOGY
Raffaele Corbisiero, MD, FACCChair, Electrophysiology andPacingDirector, ElectromechanicalTherapy Institute
Dr. Corbisiero began his careerwith Deborah in 1997 as anAssociate in the Department ofElectrophysiology, where in 2007
he was appointed Chair of that department as well asDirector of our EMTI. He serves as a Clinical Professor atthe Philadelphia College of Medicine’s Division ofCardiology. Dr. Corbisiero is triple board certified ininternal medicine, cardiovascular diseases and clinicalcardiac electrophysiology. His memberships include theHeart Failure Society of America; Heart Rhythm Society;American College of Cardiology, of which he is also aFellow; North American Society of Pacing andElectrophysiology; and he is a committee member of theInternational Multi-Site Left Ventricular PacingCommittee. Dr. Corbisiero has been invited to lecture atnumerous national and international symposiums, and isthe primary investigator in several ongoing researchprojects, as well as various concluded research trials. Inaddition, he has contributed to and has been extensivelypublished in numerous and diverse peer-reviewedjournals and publications. In addition to taking a specialinterest in device therapy (pacemakers, defibrillators),heart failure therapy, resynchronization therapy andcomplex ablation, Dr. Corbisiero has been recognized andawarded on many occasions as a “Top Doc,” “BestPhysician,” and “Readers Choice” doctor.
Pedram Kazemian, MD, MSc,FRCPC, FACC, FACPAttending CardiacElectrophysiologist
Dr. Kazemian joined Deborah in2014, bringing with him hisexpertise in catheter-basedtherapies for atrial fibrillation,ventricular tachycardia, and
device-based therapies for heart failure. He is tripleboard certified in internal medicine, cardiovascularmedicine and cardiac electrophysiology, and completed afellowship in advanced cardiac electrophysiology trainingat Tufts University, Steward St. Elizabeth’s MedicalCenter in Boston. Dr. Kazemian is a member of theAmerican Board of Internal Medicine and the AmericanBoard of Cardiovascular Medicine. He holds a specialinterest in atrial fibrillation and heart failure, and iswidely published in these areas, as well as othercardiovascular-related areas. Additionally, Dr. Kazemianhas extensive research-related experience. Hiselectrophysiology experience as first operator numbers inthe hundreds in the areas of atrial fibrillation ablation,supraventricular tachycardia, ventricular tachycardia,ICD/pacemaker implantation, lead extraction and BiVpacemaker/CRT-D. He has taught at such prestigiousschools as Harvard Medical School and the University ofAlberta. He is the recipient of many esteemed awardsand has presented both nationally and internationally inhis area of expertise.
Safi U. Ahmed, MDAttending Electrophysiologist
Dr. Ahmed is double boardcertified in internal medicine andcardiovascular disease.Completing his residency ininternal medicine at HahnemannUniversity and Medical College ofPennsylvania Hospitals,
Philadelphia, Dr. Ahmed received specialized training incardiac electrophysiology at Drexel University atHahnemann University and Medical College andAbington Memorial Hospitals, Philadelphia. Additional
training in cardiology was also completed at HahnemannUniversity and Medical College and Abington MemorialHospitals, Philadelphia, with Dr. Ahmed’s nuclearcardiology training completed at University ofConnecticut at Hartford Hospital, CT. Dr. Ahmed haslectured at various cardiology symposiums, and hisspecial interest is electrophysiology.

Kintur A. Sanghvi, MD, FACC,FASCAIAttending CardiacInterventionalistDirector, Transradial Program
Dr. Sanghvi joined Deborah inSeptember 2010 and commencedDeborah’s Transradial Program,which he propelled into a state-
of-the-art radial training program. Board certified ininterventional cardiology, cardiovascular disease, nuclearcardiology, and internal medicine, Dr. Sanghvi is amember of the Society of Cardiovascular Angiographyand Interventions, the American College of Cardiology,and the American Society of Nuclear Cardiology. Dr.Sanghvi’s special interests lie in sympathetic nervoussystem modulation/renal denervation for treatmentbeyond HTN, transradial catheterization, complexcoronary and endovascular interventions, CTOrevascularization, and structural heart disease. He hasbeen acknowledged for his contributions in thepreparation of the “Patel’s Atlas of TransradialIntervention—The Basics,” a first-ever publishedcomprehensive atlas on transradial intervention. Dr.Sanghvi is extensively published in medical and scientificjournals, and has presented at the Society ofCardiovascular Angiography & Intervention, the AsianPacific Interventional Cardiology Conference, as well asthe Southeast Asian Cardiology Meeting. He hascontributed his expertise in several research projects, andwas awarded second prize for three consecutive years in arow for his research at the Annual Peter Cyrus-RizzoScientific Seminar. Dr. Sanghvi is an Editorial BoardMember of the Journal of Interventional Cardiology.
Harit Desai, DOAttending InterventionalCardiologist
Dr. Desai joined Deborah’sinterventional staff aftercompleting specialized training incardiovascular disease atDeborah Heart and Lung Center.Board certified in internal
medicine, Dr. Desai completed his training and residencyin internal medicine at Mount Clemens Medical Center inMichigan. Published in several peer-reviewed journals, Dr.Desai has a special interest in cardiac interventions.
27
INTERVENTIONAL
Richard Kovach, MD, FACCChair, Interventional CardiologyDirector, Cardiac CatheterizationLaboratory
Dr. Kovach began his esteemedcareer with Deborah in 1988, leftto pursue a career in privatepractice in 1994 and waswelcomed “home” in 2010 as
Chair of Deborah’s Department of EndovascularMedicine, ultimately accepting the positions of Chair ofInterventional Cardiology and Director of the CardiacCatheterization Laboratory. He is a graduate of ThomasJefferson University, where he went on to serve asAssistant Clinical Professor of Medicine at ThomasJefferson University Hospital and Assistant Professor ofMedicine at Hahnemann University. Dr. Kovach leads ateam of highly-skilled Interventional Cardiologists whospecialize in cardiac medicine and endovascularprocedures, providing a comprehensive multi-disciplinaryapproach for testing, diagnosing and treating coronaryartery disease, peripheral arterial disease, venous disease,and structural heart disease. Board certified in internalmedicine, cardiovascular disease and interventionalcardiology, he was recently appointed to the editorialboard of Vascular Disease Management. Dr. Kovach has aspecial interest in endovascular medicine, carotidstenting, endovascular aneurysm repair, peripheralvascular intervention, and limb salvage. Personalachievements include serving as principal investigator ina wide array of laboratory research projects pivotal in thefuture of cardiology diagnosis and treatment. Not onlynamed a “Top Doc” by SJ Magazine, Dr. Kovach is amember of many professional organizations, has beenextensively published in various medical and scientificjournals and he has presented at numerous professionalorganizations and conferences.

28
Vincent Varghese, DO, FACC,FSCAIAttending CardiacInterventionalistDirector, InterventionalCardiology Fellowship Program
Dr. Varghese graduated fromPhiladelphia College ofOsteopathic Medicine in
Philadelphia and is board certified in internal medicine,cardiovascular disease, interventional cardiology, andnuclear cardiology, and serves on the NJ State Board ofExaminers. He was the 2014 recipient of the respectedCompassionate Doctor Recognition. Dr. Varghese isbroadly published in medical and scientific journals, andhas contributed to textbook chapters focusing oninterventional cardiology and endovascular medicine.
Related Documents











