1 Critical Access and Rural Hospital Workgroup: Post-Sepsis Syndrome and Driving Improvement in Sepsis Outcomes Geoff Granseth, MPH, CIC Rebecca Sparks, MA, RN, LNC, CPPS HSAG HIIN Quality Advisors June 20, 2019

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Critical Access and Rural Hospital Workgroup:
Post-Sepsis Syndrome and Driving Improvement in Sepsis Outcomes
Geoff Granseth, MPH, CICRebecca Sparks, MA, RN, LNC, CPPS
HSAG HIIN Quality AdvisorsJune 20, 2019

Critical Access and Rural Hospital Webinar: Leadership Team
2
Geoff Granseth, MPH, CICQuality Advisor, HSAG HIIN602.801.6898 | [email protected]
Rebecca Sparks, MA, RN, LNC, CPPSQuality Advisor, HSAG HIIN916.621.9885 | [email protected]

HSAG HIIN Sepsis Subject Matter Expert
3
Trish Cruz, MBA, RN, PHNQuality Advisor, HSAG HIIN916.717.5443 | [email protected]
4
Agenda
Critical Access and Rural Hospital WorkgroupJune 20, 2019
12 noon–1p.m. Pacific Time (PT)
Discussion Points
Objectives
Participation and sharing among the CAH/Rural participants to:• Review the current progress of our CAH/Rural hospitals in the reduction of
sepsis outcomes• Understand basic pathophysiology of sepsis and recognize post-sepsis
syndrome (PSS) symptoms• Describe best practices to support someone with PSS• Discuss strategies for reducing sepsis mortality and sepsis readmissions in
CAH/Rural settings by networking and spreading of best practices • Discover new tools that can aide your sepsis work • Take home innovative ways to improve care for sepsis patients and identify
ways to sustain improvements
12:00 p.m. Opening Remarks/Introductions…..…………….………………………………..........................................Rebecca Sparks, QA12:05 p.m. Overview of Call Format and Objectives …...............……………………….......................................Geoff/Rebecca, QAs12:10 p.m. HSAG HIIN Sepsis Data Review: Where do we stand?.............................................................Geoff Granseth, QA12:20 p.m. PSS……………………………..………………………………………………….……………………………………………………….…....Trish Cruz, QA12:40 p.m. Discussion and Peer Sharing……...………………………………………………………………………………………………………………..…All12:50 p.m. HSAG HIIN Tools, Resources, and Wrap Up…………………………………………..………...………………….Geoff/Rebecca, QAs
Who Is on the Line?
• Bear Valley Community Hospital• Community Memorial
Health System• Fairchild Medical Center• Healdsburg District Hospital• Hi Desert Medical Center• John C. Fremont
Healthcare District• Kaiser Permanente Downey• La Paz Regional Hospital• Memorial Care Long Beach
Medical Center• Modoc Medical Center
• Mountains Community Hospital• Oroville Hospital• Plumas District Hospital• Ridgecrest Regional Hospital• Saint Agnes Medical Center• San Antonio Regional Hospital• Southern Humboldt Community
Healthcare District• Stanford Healthcare Valley Care• Tri-City Medical Center• Trinity Hospital
5

Overall Sepsis
6
CAHs• Baseline: 29.85%• Q1–Q4 2018: 31.16%• RIR1: -4.4%
HSAG HIIN• Baseline: 9.36%• Q1–Q4 2018: 8.80%• RIR: 6.0%
Rurals• Baseline: 4.95%• Q1–Q4 2018: 4.45%• RIR: 10.1%
1. RIR = Relative Improvement Rate

Sepsis Mortality
7
CAHs• Baseline: 23.23%• Q1–Q4 2018: 18.45%• RIR: 20.6%
HSAG HIIN• Baseline: 24.70%• Q1–Q4 2018: 21.83%• RIR: 11.6%
Rurals• Baseline: 15.95%• Q1–Q4 2018: 15.82%• RIR: 0.8%

Readmissions: Disease State
8
Combined CAH & Rural
Disease30-Day
Readmit Rate
Discharges30-Day
Readmissions
30-Day Readmits to Same Hospital
30-Day Readmissions to Different Hospital
0–3 days to readmission 4–7 days 8–14 days 15–21 days 22–30 days
Count Rate Count Rate N % N % N % N % N %
AMI 20.69% 348 72 44 61.11% 28 38.89% 22 30.56% 14 19.44% 14 19.44% 16 22.22% 6 8.33%
HF 22.95% 1760 404 283 70.05% 121 29.95% 80 19.80% 74 18.32% 106 26.24% 65 16.09% 79 19.55%
CABG 66.67% 6 4 4 100.00% 0 0.00% 2 50.00% 0 0.00% 2 50.00% 0 0.00% 0 0.00%
PNE 18.26% 2985 545 415 76.15% 130 23.85% 113 20.73% 97 17.80% 145 26.61% 98 17.98% 92 16.88%
COPD 18.57% 1551 288 203 70.49% 85 29.51% 49 17.01% 50 17.36% 69 23.96% 52 18.06% 68 23.61%
THA/TKA 3.45% 1131 39 26 66.67% 13 33.33% 10 25.64% 6 15.38% 8 20.51% 7 17.95% 8 20.51%
Sepsis 21.02% 5294 1113 906 81.40% 207 18.60% 220 19.77% 206 18.51% 264 23.72% 214 19.23% 209 18.78%
* Medicare Fee-for-Service (FFS) Hospital Readmissions

Sepsis Readmissions
9
Combined CAH & Rural
Setting Discharged
To
30-Day Readmit Rate Discharges
30-Day Readmis
sions
30-Day Readmits to Same Hospital
30-Day Readmissions to Different Hospital
0–3 days to readmission 4–7 days 8–14 days 15–21 days 22–30 days
Count Rate Count Rate N % N % N % N % N %
Home 20.54% 2814 578 510 88.24% 68 11.76% 107 18.51% 114 19.72% 131 22.66% 121 20.93% 105 18.17%
SNF* 20.40% 1191 243 196 80.66% 47 19.34% 36 14.81% 46 18.93% 62 25.51% 41 16.87% 58 23.87%
HHA** 23.72% 666 158 120 75.95% 38 24.05% 26 16.46% 27 17.09% 46 29.11% 31 19.62% 28 17.72%
Hospice 2.54% 197 5 4 80.00% 1 20.00% 2 40.00% 2 40.00% 0 0.00% 1 20.00% 0 0.00%
Other 30.28% 426 129 76 58.91% 53 41.09% 49 37.98% 17 13.18% 25 19.38% 20 15.50% 18 13.95%
Total 21.02% 5294 1113 906 81.40% 207 18.60% 220 19.77% 206 18.51% 264 23.72% 214 19.23% 209 18.78%
SNF = Skilled Nursing FacilityHHA = Home Health Agency
* Medicare Fee-for-Service (FFS) Hospital Readmissions

Life After SepsisPost-Sepsis Syndrome (PSS)
10
Trish Cruz, MBA, RN, PHNHSAG HIIN Quality Advisor

Simplified Sepsis Pathophysiology
1. Immune response triggered2. White blood cells increase3. Vasodilation, capillary leak, blood clotting4. Insufficient blood flow to organs5. Metabolic acidosis6. Septic shock7. Multiple organ dysfunction syndrome
(MODS)
11
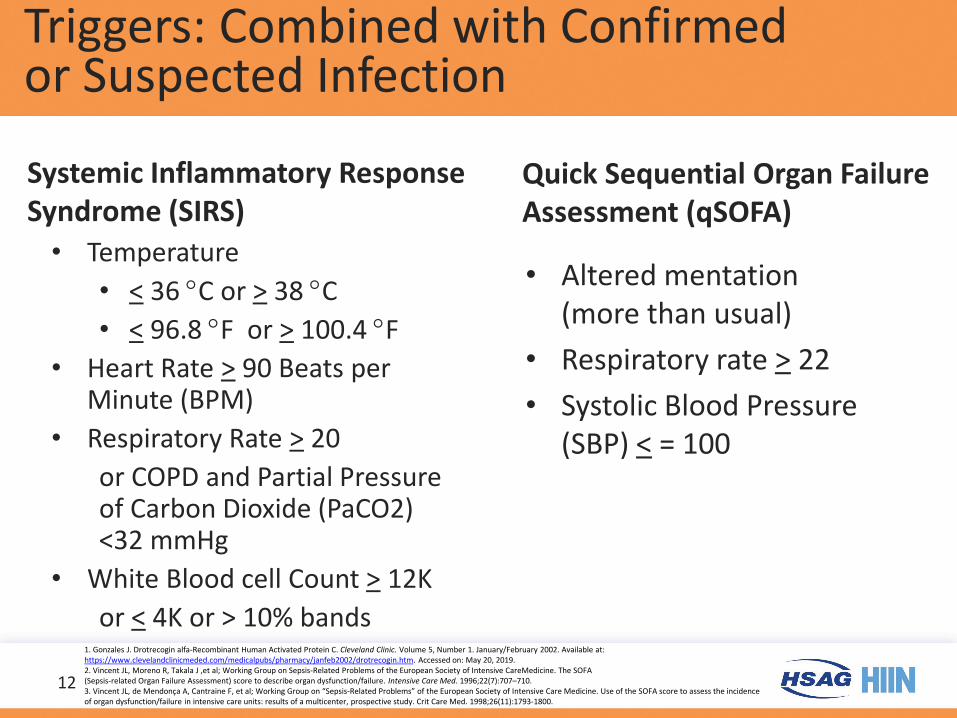
Triggers: Combined with Confirmed or Suspected Infection
Systemic Inflammatory Response Syndrome (SIRS)
• Temperature • < 36 °C or > 38 °C • < 96.8 °F or > 100.4 °F
• Heart Rate > 90 Beats per Minute (BPM)
• Respiratory Rate > 20 or COPD and Partial Pressure of Carbon Dioxide (PaCO2) <32 mmHg
• White Blood cell Count > 12K or < 4K or > 10% bands
Quick Sequential Organ Failure Assessment (qSOFA)
• Altered mentation (more than usual)
• Respiratory rate > 22• Systolic Blood Pressure
(SBP) < = 100
12
1. Gonzales J. Drotrecogin alfa-Recombinant Human Activated Protein C. Cleveland Clinic. Volume 5, Number 1. January/February 2002. Available at: https://www.clevelandclinicmeded.com/medicalpubs/pharmacy/janfeb2002/drotrecogin.htm. Accessed on: May 20, 2019. 2. Vincent JL, Moreno R, Takala J ,et al; Working Group on Sepsis-Related Problems of the European Society of Intensive CareMedicine. The SOFA(Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intensive Care Med. 1996;22(7):707–710.3. Vincent JL, de Mendonça A, Cantraine F, et al; Working Group on “Sepsis-Related Problems” of the European Society of Intensive Care Medicine. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Crit Care Med. 1998;26(11):1793-1800.

Most Up-To-Date Sepsis Definition
• Sepsis = a life-threatening organ dysfunction caused by a dysregulated host response to infection– Used to be called severe sepsis
• Organ dysfunction identification: acute change in Sequential Organ Failure Assessment (SOFA) score > 2
• Septic shock = a subset of sepsis where underlying circulatory and cellular/metabolic abnormalities are profound enough to substantially increase mortality
• Blood pressure and lactate
13
1. O’Brien J. Sepsis: A Medical Emergency. Ohio Health. April 24, 2017. Available at: https://www.ohiohospitals.org/OHA/media/OHA-Media/Documents/Patient%20Safety%20and%20Quality/Sepsis/Webinars/4-24-17-Sepsis-A-Medical-Emergency-j-obrien.pdf. Accessed on: May 20, 2019.
2. Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287. Available at: https://jamanetwork.com/journals/jama/fullarticle/2492881. Accessed on: May 20, 2019.

Readmission Prevention Bundle
1. Comprehensive discharge summary completed and sent to post care provider/primary care physician (PCP) within 48 hours of discharge
2. Follow-up appointment scheduled within seven days post discharge with PCP and/or specialist
3. Discharge phone call by clinician within 48 hours4. Involve pharmacy in medication reconciliation before discharge5. Use Teach-Back (or health literacy tool) to give all
patient education6. Partner with community organizations
– Skilled Nursing Facilities (SNFs), Transition Clinics, Home Health, Telemonitoring, Hospice, Palliative Care, Call Centers, and etc.
14

Teach-Back/Show Me
1. Plain language2. Plan your approach3. This tests how well you taught the information4. Chunk and check5. Clarify and check again6. Show me method7. Use handouts
15Agency for Healthcare Research and Quality (AHRQ). Health Literacy Universal Precautions Toolkit, Second Edition. https://www.ahrq.gov/professionals/quality-patient-safety/quality-resources/tools/literacy-toolkit/healthlittoolkit2-tool5.html. Accessed on May 20, 2019.
Sepsis Patient Education
• What is sepsis?• Common sources of sepsis• Who is at risk for developing sepsis?• How do we care for patients with sepsis?
16

Sepsis Patient Education (cont.)
• Patients and families should be involved in decisions regarding care
• Usual course of treatment: emergency (ED), within 12–24 hours, during the hospitalization
• Who is the healthcare team?• Planning for post-hospital care• Sepsis resources
17

18

Sepsis Staff Member Education
• Simulation labs– Role play the patient, doctor, and nurse
• Games– Escape room based upon sepsis questions
19

PSS
20
Sepsis Survivors
Mortality first year post discharge 28–40%
(13 times higher than patient without sepsis)
30%–60% high rates of neuro/muscular debility
High rate of depression/post-traumatic
stress disorder (PTSD)
25%, 50% readmission within 30, 90 days. Readmitted
patient with higher mortality and cost
70% readmitted for infection/sepsis
Patient with second infection in sepsis has two times higher
readmission rate
Andre Vovan, MD. St. Joseph Health. Shared with permission.
Life After Sepsis
• 20,000 new cases of cognitive dysfunction per year among survivors of sepsis1
• 74% with functional disabilities after three years2
• Approximately 60% with symptoms of depression and/or anxiety and/or post-traumatic stress disorder (PTSD)3
• Brain atrophy and low-frequency on EEG 6–24 months after discharge4
21
1. Iwashyna TJ, Ely EW, Smith DM, Langa KM. Long-term Cognitive Impairment and Functional Disability Among Survivors of Severe Sepsis. JAMA. 2010;304(16):1787–1794. doi:10.1001/jama.2010.1553. Available at: https://jamanetwork.com/journals/jama/fullarticle/186769. Accessed on: May 20, 2019.
2. Iwashyna TJ et al. Population burden of long-term survivorship after severe sepsis in older Americans. J Am Geriatr Soc. 2012 Jun;60(6):1070–7. doi: 10.1111/j.1532-5415.2012.03989.x. Epub 2012 May 29. Available at: https://www.ncbi.nlm.nih.gov/pubmed/22642542. Accessed on: May 20, 2019.
3. Rosendahl J. et al. Physical and mental health in patients and spouses after intensive care of severe sepsis: a dyadic perspective on long-term sequelae testing the Actor-Partner Interdependence Model. CritCare Med 2013 Jan; 41(1):69-75. doi: 10.1097/CCM.0b013e31826766b0. Available at: https://www.ncbi.nlm.nih.gov/pubmed/23222259. Accessed on: May 20, 2019.
4. Semmier A. et al. Persistent cognitive impairment, hippocampal atrophy and EEG changes in sepsis survivors. J NeurolNeurosurgPsych 2013 Jan; 84(1): 62–9. doi: 10.1136/jnnp-2012-302883. Epub 2012 Nov 7. Available at: https://www.ncbi.nlm.nih.gov/pubmed/23134661. Accessed on: May 20, 2019.

Life After Sepsis (cont.)
• Wives of sepsis survivors four times more likely to experience depressive symptoms1
• One-quarter of relatives of survivors with anxiety and one-half with PTSD symptoms at six months post ICU2
• More than 30% of pediatric sepsis survivors are discharged with some disability such as cognitive or physical impairments, skin grafts, amputation, or hearing loss3
22
1. Davydow DS et al. Depressive symptoms in spouses of older patients with severe sepsis. CrtiCare Med. 2012 Aug; 40(8): 2335–41. doi: 10.1097/CCM.0b013e3182536a81. Available at: https://www.ncbi.nlm.nih.gov/pubmed/22635049. Accessed on: May 20, 2019.
2. Jones C. et al. Post-traumatic stress disorder-related symptoms in relatives of patients following intensive care. Intensive Care Med 2004 Mar; 30(3): 456–60. Epub 2004 Feb 4. Available at: https://www.ncbi.nlm.nih.gov/pubmed/14767589. Accessed on: May 20, 2019.
3. Boeddha NP, et al. Mortality and morbidity in community-acquired sepsis in European pediatric intensive care units: a prospective cohort study from the European Childhood Life-threatening Infectious Disease Study (EUCLIDS). Crit Care. 2018;22(1):143. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5984383/. Accessed on: May 20, 2019.

PSS Symptoms
• Insomnia, difficulty getting to sleep or staying asleep
• Nightmare, vivid hallucinations, and panic attacks
• Disabling muscle and joint pains• Extreme fatigue• Poor concentration• Decreased mental (cognitive) functioning• Loss of self-esteem and self-belief
23Sepsis Alliance. Post-Sepsis Syndrome—PSS. Available at: https://www.sepsis.org/life-after-sepsis/post-sepsis-syndrome/. Accessed on: May 20, 2019.

PSS Treatment
• Emotional and psychological support– Counseling– Cognitive behavioral therapy– Neuropsychiatric assessment
• Physical support– Physical therapy– Neurorehabilitation
24Sepsis Alliance. Post-Sepsis Syndrome—PSS. Available at: https://www.sepsis.org/life-after-sepsis/post-sepsis-syndrome/. Accessed on: May 20, 2019.

Best Practices
• Educate patient and family regarding PSS• Understand the potential for PSS
– Communicate with the physician– Sometimes letting your loved one/patient
knowing they are not alone helps healing– Sometimes your loved one/patient will need
to talk
• Reinforce patient education provided in the acute care hospital
25

How to Notify the Physician:
• Situation: Patient or family member has symptoms of PSS• Background: A large percentage of sepsis survivors and their
families experience PSS symptoms. • Assessment: The patient is experiencing:
Insomnia, difficulty getting to sleep or staying asleep Nightmares, vivid hallucinations, and/or panic attacks Severe muscle and joint pain Extreme fatigue Poor concentration Decreased cognitive function as evidenced by: _________ Loss of self-esteem and self-belief Expressed feelings of hopelessness or helplessness
• Recommendation: “I think this patient has PSS. Please consider a referral/consult for counseling or physical therapy.”
26
Resources
• HSAG HIIN link to many resources: https://www.hsag.com/en/hiin/tools-and-resources/
• Life After Sepsis fact sheet: https://www.cdc.gov/sepsis/pdfs/life-after-sepsis-fact-sheet.pdf
• Sepsis Alliance: https://www.sepsis.org/
27

Additional Resources for SNFs
• SNFs may be the first to see PSS in our shared patients– Atlantic Quality Innovation Network. SNF Care Pathway
Symptoms of Sepsis and Septic Shock. Available at: https://atlanticquality.org/download/AQIN_Nursing_Facility_Sepsis_Care_Pathway.pdf. Accessed on: May 22, 2019.
– Minnesota Hospital Association. Seeing Sepsis—SNF Sepsis Algorithm for Adults. Available at: https://www.mnhospitals.org/Portals/0/Documents/ptsafety/SeeingSepsisLTC/2.%20Seeing%20Sepsis%20algorithm%20for%20skilled%20nursing%20facility.pdf. Accessed on: May 22, 2019.
28

Discussion/Questions
30
Discussion—What Are Your Experiences?
• Were you previously aware of PSS?• Challenges and barriers you have with your
sepsis program?• How do you track sepsis performance
(HIIN, internally?)• What are your sepsis needs from this group?
31

Sepsis Readmission Interview Tool
32
• This tool focuses on sepsis-related readmissions, meaning patients that are treated and discharged during their index admission with sepsis and readmitted within 30 days for any reason.
Healthcare Communities. Sepsis Readmission Interview Tool. Available at: https://www.healthcarecommunities.org/DesktopModules/Bring2mind/DMX/Download.aspx?portalid=3&EntryId=127947. Accessed on: June 7, 2019.

Listserv Location—Sign up!
33

Best Practices—Share Your Story!
34
Coming Up
• TBD
– Geoff Granseth, [email protected]– Rebecca Sparks, [email protected]
Look for a follow-up email with tools and resources.
35
Please complete the evaluation at:http://bit.ly/2MEMdAE
If you registered online for this event, you will also receive the link via email.
A recording of today’s session will be available at:www.hsag.com/en/hiin/events(Click on today’s event date to
access the recording link)

What are your questions?Thank you!
Geoff Granseth602.801.6898
Rebecca Sparks916.621.9885
37
Related Documents