Int J Intg Med Sci 2015;2(10):170-74. ISSN 2394 - 4137 170 Case Report Conjoined Twins (Thoraco-Omphalopagus) Prasad Arun * 1 , Kapoor Kanchan 2 , Sharma Anshu 3 , Abraham Joseph 4 . * 1 Department of Anatomy, Andaman Nicobar Islands Institute of Medical Sciences, Port Blair, India. 2,3,4 Department of Anatomy, Government Medical College, Chandigarh, India. Conjoined twins are a rarely seen congenital anomaly with severe mortality. Among the different variety of conjoined twins, Thoraco-omphalopagus is the most common type, wherein the two foetuses are joined at thorax and upper abdomen region. In this type of twins usually there is single heart, but lungs will be separate. In GIT, the foregut will be separate, but midgut may be shared by both twins. Hindgut will be separate. The exact cause is unknown, but it is mostly considered to be an irregular division of the zygote. One such case was observed during routine foetal autopsy performed in Dept of Anatomy, GMCH-32, and Chandigarh. The mother was 21yrs old prime gravida and the condition was diagnosed at the time of USG examination at 13+6 weeks of gestational age. Autopsy was performed after taking full consent. The foetuses had single umbilical cord and sex of both the foetuses was male. After autopsy it was found that both foetuses shared single heart, stomach, small intestine, large intestine, liver and spleen. However there was development of separate lungs and organs of Genito-urinary system. There are two theory proposed for the formation of the conjoined twins. A fusion theory which is more accepted and other one is fission theory. The exact mechanism of formation of twins, obstetrical and surgical importance and other details will be discussed in detail with the available literature. KEY WORDS: Conjoined Twins, Thoraco-ompahlopagus, Congenital Anomaly. Online Access and Article Informtaion International Journal of Integrative Medical Sciences www.imedsciences.com ABSTRACT INTRODUCTION Address for correspondence: Dr. Arun Prasad, Department of Anatomy, Andaman Nicobar Island Institute of Medical Sciences, Port Blair, Andaman Nicobar Islands, India. E-Mail: [email protected] International Journal of Integrative Medical Sciences, Int J Intg Med Sci 2015, Vol 2(10):170-74. ISSN 2394 - 4137 DOI: http://dx.doi.org/10.16965/ijims.2015.130 Quick Response code Received: 12-10-2015 Reviewed: 12-10-2015 Accepted: 02-11-2015 Published: 10-11-2015 Source of Funding: Self Conflicts of interest: None DOI: 10.16965/ijims.2015.130 Babies come into the world heralding the good news that the human species with all its diversit- ies and complexities is still going good. Though a new-born brings in its wake untold happiness to those around, there are some unfortunate babies whose birth is clouded with sadness and worry for the parents because of the birth defects [1] in them that are manifest either immediately defects like cleft lip, cleft palate, Down syndrome, autism, muscular dystrophy, neural tube defects, congenital heart disorders to rare birth defects such as cleft foot and hand, club foot, aglossia and albinism, to name a few after birth or after a while, depending on the nature of the congenital abnormality. Birth defects include abnormalities in the new born baby’s (structure, function or body metabolism), which usually lead to physical and mental disabilities and can even be fatal sometimes. There are many causes for birth defects involving a wide range of factors some due to hereditary abnormality, some caused by chromosomal disorders or genetic disorder and some others caused by environmental agents. All over the world as per the 2015 studies Congenital anomalies affect approximately 1 in 33 infants leading to 6.6% deaths in infants and

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Int J Intg Med Sci 20152(10)170-74 ISSN 2394 - 4137 170
Case Report
Conjoined Twins (Thoraco-Omphalopagus)Prasad Arun 1 Kapoor Kanchan 2 Sharma Anshu 3 Abraham Joseph 41 Department of Anatomy Andaman Nicobar Islands Institute of Medical Sciences Port BlairIndia234 Department of Anatomy Government Medical College Chandigarh India
Conjoined twins are a rarely seen congenital anomaly with severe mortality Among the different variety ofconjoined twins Thoraco-omphalopagus is the most common type wherein the two foetuses are joined atthorax and upper abdomen region In this type of twins usually there is single heart but lungs will be separateIn GIT the foregut will be separate but midgut may be shared by both twins Hindgut will be separate The exactcause is unknown but it is mostly considered to be an irregular division of the zygote One such case wasobserved during routine foetal autopsy performed in Dept of Anatomy GMCH-32 and Chandigarh The motherwas 21yrs old prime gravida and the condition was diagnosed at the time of USG examination at 13+6 weeks ofgestational age Autopsy was performed after taking full consent The foetuses had single umbilical cord andsex of both the foetuses was male After autopsy it was found that both foetuses shared single heart stomachsmall intestine large intestine liver and spleen However there was development of separate lungs and organsof Genito-urinary system There are two theory proposed for the formation of the conjoined twins A fusiontheory which is more accepted and other one is fission theory The exact mechanism of formation of twinsobstetrical and surgical importance and other details will be discussed in detail with the available literatureKEY WORDS Conjoined Twins Thoraco-ompahlopagus Congenital Anomaly
Online Access and Article Informtaion
International Journal of Integrative Medical Sciences
wwwimedsciencescom
ABSTRACT
INTRODUCTION
Address for correspondence Dr Arun Prasad Department of Anatomy Andaman Nicobar IslandInstitute of Medical Sciences Port Blair Andaman Nicobar Islands IndiaE-Mail drprasadarungmailcom
International Journal of Integrative Medical SciencesInt J Intg Med Sci 2015 Vol 2(10)170-74 ISSN 2394 - 4137
DOI httpdxdoiorg1016965ijims2015130
Quick Response code
Received 12-10-2015 Reviewed 12-10-2015
Accepted 02-11-2015Published 10-11-2015
Source of Funding Self Conflicts of interest NoneDOI 1016965ijims2015130
Babies come into the world heralding the goodnews that the human species with all its diversit-ies and complexities is still going good Thougha new-born brings in its wake untold happinessto those around there are some unfortunatebabies whose birth is clouded with sadness andworry for the parents because of the birthdefects [1] in them that are manifest eitherimmediately defects like cleft lip cleft palateDown syndrome autism muscular dystrophyneural tube defects congenital heart disordersto rare birth defects such as cleft foot and handclub foot aglossia and albinism to name a few
after birth or after a while depending on thenature of the congenital abnormality Birthdefects include abnormalities in the new bornbabyrsquos (structure function or body metabolism)which usually lead to physical and mentaldisabilities and can even be fatal sometimesThere are many causes for birth defects involvinga wide range of factors some due to hereditaryabnormality some caused by chromosomaldisorders or genetic disorder and some otherscaused by environmental agentsAll over the world as per the 2015 studiesCongenital anomalies affect approximately 1 in33 infants leading to 66 deaths in infants and
Int J Intg Med Sci 20152(10)170-74 ISSN 2394 - 4137 171
causing significant morbidity in children Birthdefects are present in about 3 of new-borns[2] Congenital anomalies resulted in about632000 deaths per year in 2013 down from751000 in 1990 [3-6] The type with the greatestdeath are congenital heart disease (323000)followed by neural tube defects (69000) [7]Many studies have found that the frequency ofoccurrence of certain congenital malformationsdepends on the sex of the child [4-8] Nowvarious techniques are available to detectcongenital anomalies in fetus before birth About3 of new-borns have a ldquomajor physicalanomalyrdquo meaning a physical anomaly that hascosmetic or functional significance [9] Physicalcongenital abnormalities are the leading causeof infant mortality in the United Statesaccounting for more than 20 of all infantdeaths Seven to ten present of all children willrequire extensive medical care to diagnose ortreat a birth defect [10] Among new-borns isbetween 2-3 that is similar to that found inthe industrialized world (ICBDMS 1991)Congenital anomalies account3 for 8-15 ofperinatal deaths and 13-16 of neonatal deathsin IndiaConjoined twins are rarely seen congenitalanomaly with severe mortality occurring in150000 - 160000 live births Among thedifferent variety of conjoined twins Thoraco-ompholopagus is the most common typewherein the two foetuses are joined at thoraxand upper abdomen region Teratologists haveproved that congenital abnormalities in animalscan be induced but no one has been able toprevent the occasional occurrence of conjoinedtwins Untill this is achieved surgeons will beconcerned with repair procedures primarilydepending upon the morphology of theabnormality The opportunity to dissectischiopagus whose incidence among conjoinedtwins is very low (6) is worth reporting [11]Case Report
The different variety of conjoined twins Thoraco-ompholopagus is the most common typewherein the two foetuses are joined in the thoraxand upper abdomen region In this type of twinsusually they will share a single heart but lungswill be separate The GIT system the foregut part
will be separate but midgut may be shared byboth twins Hindgut will be separate The exactcause is unknown but it is mostly considered tobe irregular division of the zygote Here we arereporting a case of Thoraco-ompholopagusDuring a routine foetal autopsy a foetus wasfound to have a thoracophagus in the Dept ofanatomy GMCH-32 Chandigarh The motherwas 21yrs old primi-gravida and the conditionwas diagnosed at the time of USG examinationat 13+6 weeks of gestational age A primigravidwas diagnosed thru USG as Thoracophagus andpregnancy was terminated and abortus was sentto our department for autopsy Antenatal historywas normal with routine check-ups and intakeof vit-B12 and folic acid tablets Medical andpast history was not significant No significantfamily history Autopsy was performed aftertaking full consentOBSERVATIONSExternal examinationmiddot Both were male foetusmiddot Foetuses were fused at thorax and upperabdomen regionmiddot Both foetuses had separate urogenitalopeningsmiddot Both foetuses had imperforate anusmiddot Limbs were separatemiddot Left side foetus showed amniotic bands atmidthigh level on left sidemiddot They had single umbilical cordInternal Examinationmiddot Incision was given to open the fused regionmiddot The thoracic and abdominal cavities wereopenedmiddot Following observations were seenmiddot Single heartmiddot Trachea fused in the middle region In upperand lower part they were separate to bothfoetuses They both had separate lungsmiddot In GIT both foetuses had separate oesophaguswhich opened into common stomach Smallintestine and large intestine were shared insideboth foetuses Sigmoid colon was seen on rightside onlymiddot Liver was present on right foetus and spleenin left foetus
Prasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph Conjoined Twins (Thoraco-Omphalopagus) A Case Report
Int J Intg Med Sci 20152(10)170-74 ISSN 2394 - 4137 172
Prasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph Conjoined Twins (Thoraco-Omphalopagus) A Case Report
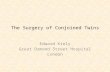
middot In Gentio-Urinary system Both foetuses hadtheir own gentio-urinary systemFig 1 Showing the Internal Examination of theConjoined Twins (Thoraco-Omphalopagus)
Fig 2 Showing the External Examination of the ConjoinedTwins (Thoraco-Omphalopagus)
Fig 3 X-Ray showingthe External Examina-tion of the ConjoinedTwins (Thoraco-Omphalopagus)
DISCUSSIONConjoined twinning was first described in1100AD The first case diagnosed by USG wasreported in 1977 It is rare abnormality estimatedto occur in about 1 of monozygotic twinsDepending upon the site of fusion it is dividedinto different types of conjoined twins Robertson
in 1953 studied conjoined twins and determinedthe incidence of various types as being 73thoracophagus 19 Pygopagus 6 ischiopagusand 2 craniopagus The female conjoined twinsare two to three times more common than maletwins Higher incidence of anomalies in stillbirths [12] and the incidence of congenitalanomalies were significantly higher in pretermbabies [13] low birth weight infants [14]motherrsquos age above 35 years [15] increasedmaternal age [16] and increased birth order Thefactors that significantly increase the risk ofcongenital malformations to be presence ofhydramnios maternal febrile illness in the firsttrimester past history of abortions diabeticmother eclampsia previous abortion and historyof congenital heart disease in previous child ormalformed babies Mother having diabetesmellitus arterial hypertension andhypothyroidism shows a positive association[17] with congenital malformations The annualreport of Indian Council of Medical Research [18]says that the commonest congenitalmalformations are cardiac in natureCardiovascular musculoskeletal and genito-urinary were the most commonly affectedsystems in a descending order of frequencyWith special reference to the neural tube defect(NTD) [19] the incidence of NTD has markedlyreduced in the developed countries followingmass promotion and mandatory prescription offolic acid for pregnant mothers The incidenceof congenital heart disease was the leadingcongenital malformation followed bymusculoskeletal systemTypes of Conjoined TwinsInferior Conjunction Lower body is single or twins joined by some lower portion of body
Diprosopus Two faces with one head and body
Dicephalus Two heads with one body
Ischiopagus Joined by inferior sacrum and coccyx
Pygopagus Joined by posterolateral sacrum and coccyx
Superior Conjunction Upper body is single or twins joined by some upper body portion
Dipygus Single head thorax abdomen with two pelves and four legs
Syncephalus Facial fusion wi th or wi thout thoracic fusion
Craniopagus Joined at the head
Middle Conjunction Fusion of the midportion of the body separate above and below
Thoracopagus Thoracic fusionOmphalopagus (Xiphopagus) Joined from umbi licus to xiphoid carti lage
Thoraco-omphalopagus Thoracic and abdominal fusion
Rachipagus Vertebral fusion above the sacrum
Int J Intg Med Sci 20152(10)170-74 ISSN 2394 - 4137 173
The exact aetiology for the occurrence of twinsis unclear But two theories have been proposedto explain this phenomenon The traditionaltheory is fission theory in which the fertilizedegg splits partially and conjoined twins representdelayed separation of the embryonic mass afterday 12 of fertilization The second theory isfusion in which a fertilized egg completelyseparates but stem cells (which search forsimilar cells) find like stem cells on the othertwin and fuse the twins together Generally thistype of cases normal delivery is not possible ifthe fetuses survive up to termPrenatal ultrasonography leads to early detectionof malformations and facilitates early surgicalintervention Ultrasound at around 20 - 21 weekshas long been considered for screeningpregnancies for structural malformations Useof second trimester ultrasound for detection ofchromosomal anomalies was first suggested in1985 [20] Chromosomal defects wereprogressively found to be associated with certainsonographic features including biometricparameters (eg short length of femur andhumerus pyelectasis large nuchal foldventriculomegaly early fetal growth restriction)and morphologic signs (eg choroids plexuscysts echogenic bowel echogenic intracardiacfocus) Data on the validity of those markers aspredictors of chromosomal anomalies (mostlyrelated to Down syndrome) are at variancedepending upon the author [22] There may bemulti factorial reasons for these namely lack ofawareness among people to get level 3ultrasound during antenatal period poverty lackof proper health services in periphery The mainpurpose of the study is we need to involve andmake aware all the health care workers who areproviding maternal and child health care workingin government or private sector so as to quantifyexact prevalence rate of congenitalmalformations involving any particular systemMortality and morbidity can be because ofsepsis infections prematurity or delay intreatment due to late admissions after diagnosisdue lack of money poor background and lack ofawareness This study definitely helps to knowthe pattern of congenital anomalies and theiroutcome in this area so that strategies forprevention early detection and timely manage-
ment can be sort outManagement Prenatal diagnosis by USG shouldbe done Surgery to separate conjoined twinsmay vary from relatively simple to extremelycomplex depending on point of attachment andthe internal organs that are shared but it is lifethreatening
CONCLUSION
The prognosis of this type of twins is generallypoor Once conjoined twins have been diagno-sed characterization of the type and severity ofthe abnormality should be assed using three-dimensional USG or MRI Termination ofpregnancy should be suggested to the family
REFERENCES
[1] Medindia Birth Defects Registry of India A lsquoSavingBabiesrsquo Project Available at httpwwwmedindianetnewshealth watchBirthDefects Registry of India A Saving Babies Project78389 1 htmixzz2GtO6Ld5M
[2] ldquoBirth Defectsrdquo (httpwwwcdcgovncbdddbirthdefectsindexhtml) March 16 2015 Retrieved8 May 2015
[3] GBD 2013 Mortality and Causes of DeathCollaborators (17 December 2014) ldquoGlobalregional and national agesex specific allcause andcausespecific mortality for 240 causes of death1990ndash2013 a systematic analysis for the GlobalBurden of Disease Study 2013rdquo (httpsw w w n c b i n l m n i h g o v p m c a r t i c l e s PMC4340604) Lancet 385 (9963) 117ndash71
[4] Gittelsohn A Milham S Statistical study of twinsmdashmethods Am J Public Health Nations Health 196454286ndash294
[5] Fernando J Arena P Smith D W Sex liability tosingle structural defects Am J DisChild1978132970ndash972
[6] Lubinsky M S Classifying sex biased congenitalanomalies Am J Med Genet199769225ndash228
[7] Lary J M Paulozzi L J Sex differences in theprevalence of human birth defects apopulationbased study Teratology200164237ndash251
[8] Wei Cui ChangXing Ma Yiwei Tang e a SexDifferences in Birth Defects A Study of OppositeSexTwins Birth Defects Research (Part A)200573876ndash880
[9] Kumar Abbas and Fausto eds Robbins and CotranrsquosPathologic Basis of Disease 7th edition p470
[10] Dicke JM ldquoTeratology principles and practicerdquoMed Clin North Am 19893 (3) 567-82
[11] Sangari SK Khatri K Pradhan S OmphalopagusIschiopagus Tetrapus Conjoined Twins mdash A CaseReport J Anat Soc India200150(1)40-42
Prasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph Conjoined Twins (Thoraco-Omphalopagus) A Case Report
Int J Intg Med Sci 20152(10)170-74 ISSN 2394 - 4137 174
Prasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph Conjoined Twins (Thoraco-Omphalopagus) A Case Report
How to cite this articlePrasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph ConjoinedTwins (Thoraco-Omphalopagus) A Case Report Int J Intg Med Sci20152(10)170-174 DOI 1016965ijims2015130
[12]Amar Taksande Krishna V i lhekar PushpaChaturvedi et al Congenital malformations at birthin Central India A rural medical college hospitalbased data Indian J Hum Genet 20103 159ndash163
[13] Mathur BC Karan S V ijaya Devi KKCongenitalmalformations in the newbornIndian Pediatr197512179-83
[14] Mohanty C Mishra OP Das BK Bhatia BD Singh Get al Congenital malformation in newborn A studyof 10874 consecutive births J Anat Soc India 198938101ndash11
[15] Suguna Bai NS Mascarene M et al An etiologicalstudy of congenital malformation in the newbornIndian Pediatr 1982 Dec 191003-7
[16]Dutta V Chaturvedi P et al Congenit-almalformations in rural Maharashtra IndianPediatr 200037998-1001
[17] Ordoacutentildeez MP Nazer J Aguila A Cifuentes et alCongenitalmalformations and chronic diseases ofthe mother Latin American Collaborative Study ofCongenitalMalformations (ECLAMC) 1971-1999LRev Med Chil 2003131404-11
[18] New DelhiReproductive health Annual report2002-03 Indian Council of Medical Research p91
[19] OrsquoDowd MJ Connolly K Ryan A et al Neural tubedefects in rural Ireland Arch D is Child 1987 Mar62(3)297-8
[20] Benacerraf B Barss V Laboda L A sonographic signfor the detection in the second trimester of the fetuswith Downrsquos syndrome Am J Obstet Gynecol1985~1511078ndash1079
[21] Snijders RJM Nicolaides KH In Ultrasound markersfor fetal chromosome defects Canforth UKParthenon Publishing~ 1996 Assessment of risks~pp 63ndash120

Int J Intg Med Sci 20152(10)170-74 ISSN 2394 - 4137 171
causing significant morbidity in children Birthdefects are present in about 3 of new-borns[2] Congenital anomalies resulted in about632000 deaths per year in 2013 down from751000 in 1990 [3-6] The type with the greatestdeath are congenital heart disease (323000)followed by neural tube defects (69000) [7]Many studies have found that the frequency ofoccurrence of certain congenital malformationsdepends on the sex of the child [4-8] Nowvarious techniques are available to detectcongenital anomalies in fetus before birth About3 of new-borns have a ldquomajor physicalanomalyrdquo meaning a physical anomaly that hascosmetic or functional significance [9] Physicalcongenital abnormalities are the leading causeof infant mortality in the United Statesaccounting for more than 20 of all infantdeaths Seven to ten present of all children willrequire extensive medical care to diagnose ortreat a birth defect [10] Among new-borns isbetween 2-3 that is similar to that found inthe industrialized world (ICBDMS 1991)Congenital anomalies account3 for 8-15 ofperinatal deaths and 13-16 of neonatal deathsin IndiaConjoined twins are rarely seen congenitalanomaly with severe mortality occurring in150000 - 160000 live births Among thedifferent variety of conjoined twins Thoraco-ompholopagus is the most common typewherein the two foetuses are joined at thoraxand upper abdomen region Teratologists haveproved that congenital abnormalities in animalscan be induced but no one has been able toprevent the occasional occurrence of conjoinedtwins Untill this is achieved surgeons will beconcerned with repair procedures primarilydepending upon the morphology of theabnormality The opportunity to dissectischiopagus whose incidence among conjoinedtwins is very low (6) is worth reporting [11]Case Report
The different variety of conjoined twins Thoraco-ompholopagus is the most common typewherein the two foetuses are joined in the thoraxand upper abdomen region In this type of twinsusually they will share a single heart but lungswill be separate The GIT system the foregut part
will be separate but midgut may be shared byboth twins Hindgut will be separate The exactcause is unknown but it is mostly considered tobe irregular division of the zygote Here we arereporting a case of Thoraco-ompholopagusDuring a routine foetal autopsy a foetus wasfound to have a thoracophagus in the Dept ofanatomy GMCH-32 Chandigarh The motherwas 21yrs old primi-gravida and the conditionwas diagnosed at the time of USG examinationat 13+6 weeks of gestational age A primigravidwas diagnosed thru USG as Thoracophagus andpregnancy was terminated and abortus was sentto our department for autopsy Antenatal historywas normal with routine check-ups and intakeof vit-B12 and folic acid tablets Medical andpast history was not significant No significantfamily history Autopsy was performed aftertaking full consentOBSERVATIONSExternal examinationmiddot Both were male foetusmiddot Foetuses were fused at thorax and upperabdomen regionmiddot Both foetuses had separate urogenitalopeningsmiddot Both foetuses had imperforate anusmiddot Limbs were separatemiddot Left side foetus showed amniotic bands atmidthigh level on left sidemiddot They had single umbilical cordInternal Examinationmiddot Incision was given to open the fused regionmiddot The thoracic and abdominal cavities wereopenedmiddot Following observations were seenmiddot Single heartmiddot Trachea fused in the middle region In upperand lower part they were separate to bothfoetuses They both had separate lungsmiddot In GIT both foetuses had separate oesophaguswhich opened into common stomach Smallintestine and large intestine were shared insideboth foetuses Sigmoid colon was seen on rightside onlymiddot Liver was present on right foetus and spleenin left foetus
Prasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph Conjoined Twins (Thoraco-Omphalopagus) A Case Report
Int J Intg Med Sci 20152(10)170-74 ISSN 2394 - 4137 172
Prasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph Conjoined Twins (Thoraco-Omphalopagus) A Case Report
middot In Gentio-Urinary system Both foetuses hadtheir own gentio-urinary systemFig 1 Showing the Internal Examination of theConjoined Twins (Thoraco-Omphalopagus)
Fig 2 Showing the External Examination of the ConjoinedTwins (Thoraco-Omphalopagus)
Fig 3 X-Ray showingthe External Examina-tion of the ConjoinedTwins (Thoraco-Omphalopagus)
DISCUSSIONConjoined twinning was first described in1100AD The first case diagnosed by USG wasreported in 1977 It is rare abnormality estimatedto occur in about 1 of monozygotic twinsDepending upon the site of fusion it is dividedinto different types of conjoined twins Robertson
in 1953 studied conjoined twins and determinedthe incidence of various types as being 73thoracophagus 19 Pygopagus 6 ischiopagusand 2 craniopagus The female conjoined twinsare two to three times more common than maletwins Higher incidence of anomalies in stillbirths [12] and the incidence of congenitalanomalies were significantly higher in pretermbabies [13] low birth weight infants [14]motherrsquos age above 35 years [15] increasedmaternal age [16] and increased birth order Thefactors that significantly increase the risk ofcongenital malformations to be presence ofhydramnios maternal febrile illness in the firsttrimester past history of abortions diabeticmother eclampsia previous abortion and historyof congenital heart disease in previous child ormalformed babies Mother having diabetesmellitus arterial hypertension andhypothyroidism shows a positive association[17] with congenital malformations The annualreport of Indian Council of Medical Research [18]says that the commonest congenitalmalformations are cardiac in natureCardiovascular musculoskeletal and genito-urinary were the most commonly affectedsystems in a descending order of frequencyWith special reference to the neural tube defect(NTD) [19] the incidence of NTD has markedlyreduced in the developed countries followingmass promotion and mandatory prescription offolic acid for pregnant mothers The incidenceof congenital heart disease was the leadingcongenital malformation followed bymusculoskeletal systemTypes of Conjoined TwinsInferior Conjunction Lower body is single or twins joined by some lower portion of body
Diprosopus Two faces with one head and body
Dicephalus Two heads with one body
Ischiopagus Joined by inferior sacrum and coccyx
Pygopagus Joined by posterolateral sacrum and coccyx
Superior Conjunction Upper body is single or twins joined by some upper body portion
Dipygus Single head thorax abdomen with two pelves and four legs
Syncephalus Facial fusion wi th or wi thout thoracic fusion
Craniopagus Joined at the head
Middle Conjunction Fusion of the midportion of the body separate above and below
Thoracopagus Thoracic fusionOmphalopagus (Xiphopagus) Joined from umbi licus to xiphoid carti lage
Thoraco-omphalopagus Thoracic and abdominal fusion
Rachipagus Vertebral fusion above the sacrum
Int J Intg Med Sci 20152(10)170-74 ISSN 2394 - 4137 173
The exact aetiology for the occurrence of twinsis unclear But two theories have been proposedto explain this phenomenon The traditionaltheory is fission theory in which the fertilizedegg splits partially and conjoined twins representdelayed separation of the embryonic mass afterday 12 of fertilization The second theory isfusion in which a fertilized egg completelyseparates but stem cells (which search forsimilar cells) find like stem cells on the othertwin and fuse the twins together Generally thistype of cases normal delivery is not possible ifthe fetuses survive up to termPrenatal ultrasonography leads to early detectionof malformations and facilitates early surgicalintervention Ultrasound at around 20 - 21 weekshas long been considered for screeningpregnancies for structural malformations Useof second trimester ultrasound for detection ofchromosomal anomalies was first suggested in1985 [20] Chromosomal defects wereprogressively found to be associated with certainsonographic features including biometricparameters (eg short length of femur andhumerus pyelectasis large nuchal foldventriculomegaly early fetal growth restriction)and morphologic signs (eg choroids plexuscysts echogenic bowel echogenic intracardiacfocus) Data on the validity of those markers aspredictors of chromosomal anomalies (mostlyrelated to Down syndrome) are at variancedepending upon the author [22] There may bemulti factorial reasons for these namely lack ofawareness among people to get level 3ultrasound during antenatal period poverty lackof proper health services in periphery The mainpurpose of the study is we need to involve andmake aware all the health care workers who areproviding maternal and child health care workingin government or private sector so as to quantifyexact prevalence rate of congenitalmalformations involving any particular systemMortality and morbidity can be because ofsepsis infections prematurity or delay intreatment due to late admissions after diagnosisdue lack of money poor background and lack ofawareness This study definitely helps to knowthe pattern of congenital anomalies and theiroutcome in this area so that strategies forprevention early detection and timely manage-
ment can be sort outManagement Prenatal diagnosis by USG shouldbe done Surgery to separate conjoined twinsmay vary from relatively simple to extremelycomplex depending on point of attachment andthe internal organs that are shared but it is lifethreatening
CONCLUSION
The prognosis of this type of twins is generallypoor Once conjoined twins have been diagno-sed characterization of the type and severity ofthe abnormality should be assed using three-dimensional USG or MRI Termination ofpregnancy should be suggested to the family
REFERENCES
[1] Medindia Birth Defects Registry of India A lsquoSavingBabiesrsquo Project Available at httpwwwmedindianetnewshealth watchBirthDefects Registry of India A Saving Babies Project78389 1 htmixzz2GtO6Ld5M
[2] ldquoBirth Defectsrdquo (httpwwwcdcgovncbdddbirthdefectsindexhtml) March 16 2015 Retrieved8 May 2015
[3] GBD 2013 Mortality and Causes of DeathCollaborators (17 December 2014) ldquoGlobalregional and national agesex specific allcause andcausespecific mortality for 240 causes of death1990ndash2013 a systematic analysis for the GlobalBurden of Disease Study 2013rdquo (httpsw w w n c b i n l m n i h g o v p m c a r t i c l e s PMC4340604) Lancet 385 (9963) 117ndash71
[4] Gittelsohn A Milham S Statistical study of twinsmdashmethods Am J Public Health Nations Health 196454286ndash294
[5] Fernando J Arena P Smith D W Sex liability tosingle structural defects Am J DisChild1978132970ndash972
[6] Lubinsky M S Classifying sex biased congenitalanomalies Am J Med Genet199769225ndash228
[7] Lary J M Paulozzi L J Sex differences in theprevalence of human birth defects apopulationbased study Teratology200164237ndash251
[8] Wei Cui ChangXing Ma Yiwei Tang e a SexDifferences in Birth Defects A Study of OppositeSexTwins Birth Defects Research (Part A)200573876ndash880
[9] Kumar Abbas and Fausto eds Robbins and CotranrsquosPathologic Basis of Disease 7th edition p470
[10] Dicke JM ldquoTeratology principles and practicerdquoMed Clin North Am 19893 (3) 567-82
[11] Sangari SK Khatri K Pradhan S OmphalopagusIschiopagus Tetrapus Conjoined Twins mdash A CaseReport J Anat Soc India200150(1)40-42
Prasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph Conjoined Twins (Thoraco-Omphalopagus) A Case Report
Int J Intg Med Sci 20152(10)170-74 ISSN 2394 - 4137 174
Prasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph Conjoined Twins (Thoraco-Omphalopagus) A Case Report
How to cite this articlePrasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph ConjoinedTwins (Thoraco-Omphalopagus) A Case Report Int J Intg Med Sci20152(10)170-174 DOI 1016965ijims2015130
[12]Amar Taksande Krishna V i lhekar PushpaChaturvedi et al Congenital malformations at birthin Central India A rural medical college hospitalbased data Indian J Hum Genet 20103 159ndash163
[13] Mathur BC Karan S V ijaya Devi KKCongenitalmalformations in the newbornIndian Pediatr197512179-83
[14] Mohanty C Mishra OP Das BK Bhatia BD Singh Get al Congenital malformation in newborn A studyof 10874 consecutive births J Anat Soc India 198938101ndash11
[15] Suguna Bai NS Mascarene M et al An etiologicalstudy of congenital malformation in the newbornIndian Pediatr 1982 Dec 191003-7
[16]Dutta V Chaturvedi P et al Congenit-almalformations in rural Maharashtra IndianPediatr 200037998-1001
[17] Ordoacutentildeez MP Nazer J Aguila A Cifuentes et alCongenitalmalformations and chronic diseases ofthe mother Latin American Collaborative Study ofCongenitalMalformations (ECLAMC) 1971-1999LRev Med Chil 2003131404-11
[18] New DelhiReproductive health Annual report2002-03 Indian Council of Medical Research p91
[19] OrsquoDowd MJ Connolly K Ryan A et al Neural tubedefects in rural Ireland Arch D is Child 1987 Mar62(3)297-8
[20] Benacerraf B Barss V Laboda L A sonographic signfor the detection in the second trimester of the fetuswith Downrsquos syndrome Am J Obstet Gynecol1985~1511078ndash1079
[21] Snijders RJM Nicolaides KH In Ultrasound markersfor fetal chromosome defects Canforth UKParthenon Publishing~ 1996 Assessment of risks~pp 63ndash120

Int J Intg Med Sci 20152(10)170-74 ISSN 2394 - 4137 172
Prasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph Conjoined Twins (Thoraco-Omphalopagus) A Case Report
middot In Gentio-Urinary system Both foetuses hadtheir own gentio-urinary systemFig 1 Showing the Internal Examination of theConjoined Twins (Thoraco-Omphalopagus)
Fig 2 Showing the External Examination of the ConjoinedTwins (Thoraco-Omphalopagus)
Fig 3 X-Ray showingthe External Examina-tion of the ConjoinedTwins (Thoraco-Omphalopagus)
DISCUSSIONConjoined twinning was first described in1100AD The first case diagnosed by USG wasreported in 1977 It is rare abnormality estimatedto occur in about 1 of monozygotic twinsDepending upon the site of fusion it is dividedinto different types of conjoined twins Robertson
in 1953 studied conjoined twins and determinedthe incidence of various types as being 73thoracophagus 19 Pygopagus 6 ischiopagusand 2 craniopagus The female conjoined twinsare two to three times more common than maletwins Higher incidence of anomalies in stillbirths [12] and the incidence of congenitalanomalies were significantly higher in pretermbabies [13] low birth weight infants [14]motherrsquos age above 35 years [15] increasedmaternal age [16] and increased birth order Thefactors that significantly increase the risk ofcongenital malformations to be presence ofhydramnios maternal febrile illness in the firsttrimester past history of abortions diabeticmother eclampsia previous abortion and historyof congenital heart disease in previous child ormalformed babies Mother having diabetesmellitus arterial hypertension andhypothyroidism shows a positive association[17] with congenital malformations The annualreport of Indian Council of Medical Research [18]says that the commonest congenitalmalformations are cardiac in natureCardiovascular musculoskeletal and genito-urinary were the most commonly affectedsystems in a descending order of frequencyWith special reference to the neural tube defect(NTD) [19] the incidence of NTD has markedlyreduced in the developed countries followingmass promotion and mandatory prescription offolic acid for pregnant mothers The incidenceof congenital heart disease was the leadingcongenital malformation followed bymusculoskeletal systemTypes of Conjoined TwinsInferior Conjunction Lower body is single or twins joined by some lower portion of body
Diprosopus Two faces with one head and body
Dicephalus Two heads with one body
Ischiopagus Joined by inferior sacrum and coccyx
Pygopagus Joined by posterolateral sacrum and coccyx
Superior Conjunction Upper body is single or twins joined by some upper body portion
Dipygus Single head thorax abdomen with two pelves and four legs
Syncephalus Facial fusion wi th or wi thout thoracic fusion
Craniopagus Joined at the head
Middle Conjunction Fusion of the midportion of the body separate above and below
Thoracopagus Thoracic fusionOmphalopagus (Xiphopagus) Joined from umbi licus to xiphoid carti lage
Thoraco-omphalopagus Thoracic and abdominal fusion
Rachipagus Vertebral fusion above the sacrum
Int J Intg Med Sci 20152(10)170-74 ISSN 2394 - 4137 173
The exact aetiology for the occurrence of twinsis unclear But two theories have been proposedto explain this phenomenon The traditionaltheory is fission theory in which the fertilizedegg splits partially and conjoined twins representdelayed separation of the embryonic mass afterday 12 of fertilization The second theory isfusion in which a fertilized egg completelyseparates but stem cells (which search forsimilar cells) find like stem cells on the othertwin and fuse the twins together Generally thistype of cases normal delivery is not possible ifthe fetuses survive up to termPrenatal ultrasonography leads to early detectionof malformations and facilitates early surgicalintervention Ultrasound at around 20 - 21 weekshas long been considered for screeningpregnancies for structural malformations Useof second trimester ultrasound for detection ofchromosomal anomalies was first suggested in1985 [20] Chromosomal defects wereprogressively found to be associated with certainsonographic features including biometricparameters (eg short length of femur andhumerus pyelectasis large nuchal foldventriculomegaly early fetal growth restriction)and morphologic signs (eg choroids plexuscysts echogenic bowel echogenic intracardiacfocus) Data on the validity of those markers aspredictors of chromosomal anomalies (mostlyrelated to Down syndrome) are at variancedepending upon the author [22] There may bemulti factorial reasons for these namely lack ofawareness among people to get level 3ultrasound during antenatal period poverty lackof proper health services in periphery The mainpurpose of the study is we need to involve andmake aware all the health care workers who areproviding maternal and child health care workingin government or private sector so as to quantifyexact prevalence rate of congenitalmalformations involving any particular systemMortality and morbidity can be because ofsepsis infections prematurity or delay intreatment due to late admissions after diagnosisdue lack of money poor background and lack ofawareness This study definitely helps to knowthe pattern of congenital anomalies and theiroutcome in this area so that strategies forprevention early detection and timely manage-
ment can be sort outManagement Prenatal diagnosis by USG shouldbe done Surgery to separate conjoined twinsmay vary from relatively simple to extremelycomplex depending on point of attachment andthe internal organs that are shared but it is lifethreatening
CONCLUSION
The prognosis of this type of twins is generallypoor Once conjoined twins have been diagno-sed characterization of the type and severity ofthe abnormality should be assed using three-dimensional USG or MRI Termination ofpregnancy should be suggested to the family
REFERENCES
[1] Medindia Birth Defects Registry of India A lsquoSavingBabiesrsquo Project Available at httpwwwmedindianetnewshealth watchBirthDefects Registry of India A Saving Babies Project78389 1 htmixzz2GtO6Ld5M
[2] ldquoBirth Defectsrdquo (httpwwwcdcgovncbdddbirthdefectsindexhtml) March 16 2015 Retrieved8 May 2015
[3] GBD 2013 Mortality and Causes of DeathCollaborators (17 December 2014) ldquoGlobalregional and national agesex specific allcause andcausespecific mortality for 240 causes of death1990ndash2013 a systematic analysis for the GlobalBurden of Disease Study 2013rdquo (httpsw w w n c b i n l m n i h g o v p m c a r t i c l e s PMC4340604) Lancet 385 (9963) 117ndash71
[4] Gittelsohn A Milham S Statistical study of twinsmdashmethods Am J Public Health Nations Health 196454286ndash294
[5] Fernando J Arena P Smith D W Sex liability tosingle structural defects Am J DisChild1978132970ndash972
[6] Lubinsky M S Classifying sex biased congenitalanomalies Am J Med Genet199769225ndash228
[7] Lary J M Paulozzi L J Sex differences in theprevalence of human birth defects apopulationbased study Teratology200164237ndash251
[8] Wei Cui ChangXing Ma Yiwei Tang e a SexDifferences in Birth Defects A Study of OppositeSexTwins Birth Defects Research (Part A)200573876ndash880
[9] Kumar Abbas and Fausto eds Robbins and CotranrsquosPathologic Basis of Disease 7th edition p470
[10] Dicke JM ldquoTeratology principles and practicerdquoMed Clin North Am 19893 (3) 567-82
[11] Sangari SK Khatri K Pradhan S OmphalopagusIschiopagus Tetrapus Conjoined Twins mdash A CaseReport J Anat Soc India200150(1)40-42
Prasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph Conjoined Twins (Thoraco-Omphalopagus) A Case Report
Int J Intg Med Sci 20152(10)170-74 ISSN 2394 - 4137 174
Prasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph Conjoined Twins (Thoraco-Omphalopagus) A Case Report
How to cite this articlePrasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph ConjoinedTwins (Thoraco-Omphalopagus) A Case Report Int J Intg Med Sci20152(10)170-174 DOI 1016965ijims2015130
[12]Amar Taksande Krishna V i lhekar PushpaChaturvedi et al Congenital malformations at birthin Central India A rural medical college hospitalbased data Indian J Hum Genet 20103 159ndash163
[13] Mathur BC Karan S V ijaya Devi KKCongenitalmalformations in the newbornIndian Pediatr197512179-83
[14] Mohanty C Mishra OP Das BK Bhatia BD Singh Get al Congenital malformation in newborn A studyof 10874 consecutive births J Anat Soc India 198938101ndash11
[15] Suguna Bai NS Mascarene M et al An etiologicalstudy of congenital malformation in the newbornIndian Pediatr 1982 Dec 191003-7
[16]Dutta V Chaturvedi P et al Congenit-almalformations in rural Maharashtra IndianPediatr 200037998-1001
[17] Ordoacutentildeez MP Nazer J Aguila A Cifuentes et alCongenitalmalformations and chronic diseases ofthe mother Latin American Collaborative Study ofCongenitalMalformations (ECLAMC) 1971-1999LRev Med Chil 2003131404-11
[18] New DelhiReproductive health Annual report2002-03 Indian Council of Medical Research p91
[19] OrsquoDowd MJ Connolly K Ryan A et al Neural tubedefects in rural Ireland Arch D is Child 1987 Mar62(3)297-8
[20] Benacerraf B Barss V Laboda L A sonographic signfor the detection in the second trimester of the fetuswith Downrsquos syndrome Am J Obstet Gynecol1985~1511078ndash1079
[21] Snijders RJM Nicolaides KH In Ultrasound markersfor fetal chromosome defects Canforth UKParthenon Publishing~ 1996 Assessment of risks~pp 63ndash120

Int J Intg Med Sci 20152(10)170-74 ISSN 2394 - 4137 173
The exact aetiology for the occurrence of twinsis unclear But two theories have been proposedto explain this phenomenon The traditionaltheory is fission theory in which the fertilizedegg splits partially and conjoined twins representdelayed separation of the embryonic mass afterday 12 of fertilization The second theory isfusion in which a fertilized egg completelyseparates but stem cells (which search forsimilar cells) find like stem cells on the othertwin and fuse the twins together Generally thistype of cases normal delivery is not possible ifthe fetuses survive up to termPrenatal ultrasonography leads to early detectionof malformations and facilitates early surgicalintervention Ultrasound at around 20 - 21 weekshas long been considered for screeningpregnancies for structural malformations Useof second trimester ultrasound for detection ofchromosomal anomalies was first suggested in1985 [20] Chromosomal defects wereprogressively found to be associated with certainsonographic features including biometricparameters (eg short length of femur andhumerus pyelectasis large nuchal foldventriculomegaly early fetal growth restriction)and morphologic signs (eg choroids plexuscysts echogenic bowel echogenic intracardiacfocus) Data on the validity of those markers aspredictors of chromosomal anomalies (mostlyrelated to Down syndrome) are at variancedepending upon the author [22] There may bemulti factorial reasons for these namely lack ofawareness among people to get level 3ultrasound during antenatal period poverty lackof proper health services in periphery The mainpurpose of the study is we need to involve andmake aware all the health care workers who areproviding maternal and child health care workingin government or private sector so as to quantifyexact prevalence rate of congenitalmalformations involving any particular systemMortality and morbidity can be because ofsepsis infections prematurity or delay intreatment due to late admissions after diagnosisdue lack of money poor background and lack ofawareness This study definitely helps to knowthe pattern of congenital anomalies and theiroutcome in this area so that strategies forprevention early detection and timely manage-
ment can be sort outManagement Prenatal diagnosis by USG shouldbe done Surgery to separate conjoined twinsmay vary from relatively simple to extremelycomplex depending on point of attachment andthe internal organs that are shared but it is lifethreatening
CONCLUSION
The prognosis of this type of twins is generallypoor Once conjoined twins have been diagno-sed characterization of the type and severity ofthe abnormality should be assed using three-dimensional USG or MRI Termination ofpregnancy should be suggested to the family
REFERENCES
[1] Medindia Birth Defects Registry of India A lsquoSavingBabiesrsquo Project Available at httpwwwmedindianetnewshealth watchBirthDefects Registry of India A Saving Babies Project78389 1 htmixzz2GtO6Ld5M
[2] ldquoBirth Defectsrdquo (httpwwwcdcgovncbdddbirthdefectsindexhtml) March 16 2015 Retrieved8 May 2015
[3] GBD 2013 Mortality and Causes of DeathCollaborators (17 December 2014) ldquoGlobalregional and national agesex specific allcause andcausespecific mortality for 240 causes of death1990ndash2013 a systematic analysis for the GlobalBurden of Disease Study 2013rdquo (httpsw w w n c b i n l m n i h g o v p m c a r t i c l e s PMC4340604) Lancet 385 (9963) 117ndash71
[4] Gittelsohn A Milham S Statistical study of twinsmdashmethods Am J Public Health Nations Health 196454286ndash294
[5] Fernando J Arena P Smith D W Sex liability tosingle structural defects Am J DisChild1978132970ndash972
[6] Lubinsky M S Classifying sex biased congenitalanomalies Am J Med Genet199769225ndash228
[7] Lary J M Paulozzi L J Sex differences in theprevalence of human birth defects apopulationbased study Teratology200164237ndash251
[8] Wei Cui ChangXing Ma Yiwei Tang e a SexDifferences in Birth Defects A Study of OppositeSexTwins Birth Defects Research (Part A)200573876ndash880
[9] Kumar Abbas and Fausto eds Robbins and CotranrsquosPathologic Basis of Disease 7th edition p470
[10] Dicke JM ldquoTeratology principles and practicerdquoMed Clin North Am 19893 (3) 567-82
[11] Sangari SK Khatri K Pradhan S OmphalopagusIschiopagus Tetrapus Conjoined Twins mdash A CaseReport J Anat Soc India200150(1)40-42
Prasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph Conjoined Twins (Thoraco-Omphalopagus) A Case Report
Int J Intg Med Sci 20152(10)170-74 ISSN 2394 - 4137 174
Prasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph Conjoined Twins (Thoraco-Omphalopagus) A Case Report
How to cite this articlePrasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph ConjoinedTwins (Thoraco-Omphalopagus) A Case Report Int J Intg Med Sci20152(10)170-174 DOI 1016965ijims2015130
[12]Amar Taksande Krishna V i lhekar PushpaChaturvedi et al Congenital malformations at birthin Central India A rural medical college hospitalbased data Indian J Hum Genet 20103 159ndash163
[13] Mathur BC Karan S V ijaya Devi KKCongenitalmalformations in the newbornIndian Pediatr197512179-83
[14] Mohanty C Mishra OP Das BK Bhatia BD Singh Get al Congenital malformation in newborn A studyof 10874 consecutive births J Anat Soc India 198938101ndash11
[15] Suguna Bai NS Mascarene M et al An etiologicalstudy of congenital malformation in the newbornIndian Pediatr 1982 Dec 191003-7
[16]Dutta V Chaturvedi P et al Congenit-almalformations in rural Maharashtra IndianPediatr 200037998-1001
[17] Ordoacutentildeez MP Nazer J Aguila A Cifuentes et alCongenitalmalformations and chronic diseases ofthe mother Latin American Collaborative Study ofCongenitalMalformations (ECLAMC) 1971-1999LRev Med Chil 2003131404-11
[18] New DelhiReproductive health Annual report2002-03 Indian Council of Medical Research p91
[19] OrsquoDowd MJ Connolly K Ryan A et al Neural tubedefects in rural Ireland Arch D is Child 1987 Mar62(3)297-8
[20] Benacerraf B Barss V Laboda L A sonographic signfor the detection in the second trimester of the fetuswith Downrsquos syndrome Am J Obstet Gynecol1985~1511078ndash1079
[21] Snijders RJM Nicolaides KH In Ultrasound markersfor fetal chromosome defects Canforth UKParthenon Publishing~ 1996 Assessment of risks~pp 63ndash120

Int J Intg Med Sci 20152(10)170-74 ISSN 2394 - 4137 174
Prasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph Conjoined Twins (Thoraco-Omphalopagus) A Case Report
How to cite this articlePrasad Arun Kapoor Kanchan Sharma Anshu Abraham Joseph ConjoinedTwins (Thoraco-Omphalopagus) A Case Report Int J Intg Med Sci20152(10)170-174 DOI 1016965ijims2015130
[12]Amar Taksande Krishna V i lhekar PushpaChaturvedi et al Congenital malformations at birthin Central India A rural medical college hospitalbased data Indian J Hum Genet 20103 159ndash163
[13] Mathur BC Karan S V ijaya Devi KKCongenitalmalformations in the newbornIndian Pediatr197512179-83
[14] Mohanty C Mishra OP Das BK Bhatia BD Singh Get al Congenital malformation in newborn A studyof 10874 consecutive births J Anat Soc India 198938101ndash11
[15] Suguna Bai NS Mascarene M et al An etiologicalstudy of congenital malformation in the newbornIndian Pediatr 1982 Dec 191003-7
[16]Dutta V Chaturvedi P et al Congenit-almalformations in rural Maharashtra IndianPediatr 200037998-1001
[17] Ordoacutentildeez MP Nazer J Aguila A Cifuentes et alCongenitalmalformations and chronic diseases ofthe mother Latin American Collaborative Study ofCongenitalMalformations (ECLAMC) 1971-1999LRev Med Chil 2003131404-11
[18] New DelhiReproductive health Annual report2002-03 Indian Council of Medical Research p91
[19] OrsquoDowd MJ Connolly K Ryan A et al Neural tubedefects in rural Ireland Arch D is Child 1987 Mar62(3)297-8
[20] Benacerraf B Barss V Laboda L A sonographic signfor the detection in the second trimester of the fetuswith Downrsquos syndrome Am J Obstet Gynecol1985~1511078ndash1079
[21] Snijders RJM Nicolaides KH In Ultrasound markersfor fetal chromosome defects Canforth UKParthenon Publishing~ 1996 Assessment of risks~pp 63ndash120
Related Documents