Br Heart J 1987;58:518-24 Conjoined twins, right atrial isomerism, and sequential segmental analysis MARINEZ BARRA ROSSI, JOHN BURN, SIEW YEN HO, GAETANO THIENE, WILLIAM A DEVINE, ROBERT H ANDERSON From the Department of Paediatrics, Cardiothoracic Institute, Brompton Hospital, London; Department of Human Genetics, University of Newcastle upon Tyne; Division of Pathology, Children's Hospital of Pittsburgh, Pittsburgh, Pennsylvania, USA; and Department of Pathology, University of Padua, Padua, Italy SUMMARY Three cases of twins conjoined across the chest were examined. In one set, one twin showed right atrial isomerism and the other showed the usual atrial arrangement. The other two sets showed the usual atrial arrangement in both twins. The associated cardiac anomalies were diverse, ranging from atrioventricular septal defects to absent atrioventricular connections. Sequential segmental analysis was used successfully in each case to classify the complex cardiac anomalies. The first step was the recognition of the atrial arrangement. This was easily achieved despite the complexity of the intracardiac morphology. Conjoined twins have a high incidence of cardiac anomalies particularly when, as occurs most fre- quently, they are joined across the chest.' We report here three sets of conjoined hearts from twins joined at the chest. In the first set, one twin had right atrial isomerism and showed the cardiac anomalies which accompany this atrial arrangement. In the other two sets, both twins had the usual atrial arrangement together with other cardiac anomalies. Our experi- ence emphasises the importance of accurate recog- nition of atrial arrangement as the first step in sequential segmental analysis and subsequent classification of associated anomalies. Case reports The three sets of twins were all female and all were joined at their thoracic and abdominal regions. Since there were considerable differences in the specific morphology of the various twins, we need to dis- tinguish the individual members of each pair. This is conventionally done by calling them twins A and B, as shown in fig 1. Thus two sets of twins were joined more or less in side by side fashion. This arrangement can be likened to an opened book, the Requests for reprints to Dr Siew Yen Ho, Department of Pae- diatrics, The Cardiothoracic Institute, Fulham Road, London SW3 6HP. Accepted for publication 23 June 1987 junctional line representing the spine of the book and the bodies of each twin the book pages. In such book-leaf fusion the anterior surfaces of the twins can be viewed by the observer and the twin on the observer's left-hand side is called twin B. The third set of twins was fused in a face to face arrangement Twin B Twin A Twin B Twin A Fig 1 Diagram showing the side by side and face to face arrangement of two sets of thoracopagus twins. The twins are placed in a position that best approximates an open book facing the observer for the designation of A (to the observer's right hand) and B (to the observer's left hand). 518 copyright. on November 27, 2020 by guest. Protected by http://heart.bmj.com/ Br Heart J: first published as 10.1136/hrt.58.5.518 on 1 November 1987. Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Br Heart J 1987;58:518-24
Conjoined twins, right atrial isomerism, andsequential segmental analysisMARINEZ BARRA ROSSI, JOHN BURN, SIEW YEN HO, GAETANO THIENE,WILLIAM A DEVINE, ROBERT H ANDERSON
From the Department of Paediatrics, Cardiothoracic Institute, Brompton Hospital, London; Department ofHuman Genetics, University of Newcastle upon Tyne; Division of Pathology, Children's Hospital ofPittsburgh, Pittsburgh, Pennsylvania, USA; and Department of Pathology, University of Padua, Padua, Italy
SUMMARY Three cases of twins conjoined across the chest were examined. In one set, one twinshowed right atrial isomerism and the other showed the usual atrial arrangement. The other twosets showed the usual atrial arrangement in both twins. The associated cardiac anomalies were
diverse, ranging from atrioventricular septal defects to absent atrioventricular connections.Sequential segmental analysis was used successfully in each case to classify the complex cardiacanomalies. The first step was the recognition of the atrial arrangement. This was easily achieveddespite the complexity of the intracardiac morphology.
Conjoined twins have a high incidence of cardiacanomalies particularly when, as occurs most fre-quently, they are joined across the chest.' We reporthere three sets of conjoined hearts from twins joinedat the chest. In the first set, one twin had right atrialisomerism and showed the cardiac anomalies whichaccompany this atrial arrangement. In the other twosets, both twins had the usual atrial arrangementtogether with other cardiac anomalies. Our experi-ence emphasises the importance of accurate recog-nition of atrial arrangement as the first step insequential segmental analysis and subsequentclassification of associated anomalies.
Case reports
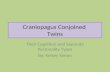
The three sets of twins were all female and all werejoined at their thoracic and abdominal regions. Sincethere were considerable differences in the specificmorphology of the various twins, we need to dis-tinguish the individual members of each pair. Thisis conventionally done by calling them twins A andB, as shown in fig 1. Thus two sets of twins werejoined more or less in side by side fashion. Thisarrangement can be likened to an opened book, the
Requests for reprints to Dr Siew Yen Ho, Department of Pae-diatrics, The Cardiothoracic Institute, Fulham Road, LondonSW3 6HP.
Accepted for publication 23 June 1987
junctional line representing the spine of the bookand the bodies of each twin the book pages. In suchbook-leaf fusion the anterior surfaces of the twinscan be viewed by the observer and the twin on theobserver's left-hand side is called twin B. The thirdset of twins was fused in a face to face arrangement
Twin B Twin A Twin B Twin A
Fig 1 Diagram showing the side by side andface to facearrangement of two sets of thoracopagus twins. The twins areplaced in a position that best approximates an open bookfacing the observer for the designation ofA (to the observer'sright hand) and B (to the observer's left hand).
518
copyright. on N
ovember 27, 2020 by guest. P
rotected byhttp://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.58.5.518 on 1 Novem
ber 1987. Dow
nloaded from

Conjoined twins, right atrial isomerism, and sequential segmental analysisand naming individual members was more difficult,since the pair can be positioned either way up to facethe observer. We arbitrarily positioned the pair mostclosely to approximate the book-leaf arrangement(fig 1). Having designated the twins as "A" and "B"we use the terms "left" and "right" only in respectof the anatomical arrangement in each twin. Thehearts and great vessels were examined in all casesand complementary information obtained as andwhen possible. The table summarises the importantcardiac anomalies. The specific details are as follows:
SET 1The hearts, which were studied in isolation, werejoined at atrial and ventricular levels in book-leaffashion. There were four atrial appendages, Thoseof twin B were both of right morphology (right atrialisomerism) as judged by internal and external fea-tures (fig 2).- The left-sided morphologically right
t.1N2>.t, , . .....
Fig 2 (a) Internal view of the common atrial chambershared by both twins (set 1), showing the septal strand.(b) Anterior external view of the hearts of set 1 showing theconjoined atrium of right morphology.
atrium of twin B was part of a midline atrial chambercommon to both twins, the other component beingthe right-sided morphologically right atrium of twinA. Twin A then had a left-sided atrium of left mor-phology (usual atrial arrangement). The commonatrial chamber was crossed only by a fibrous strandas a remnant of atrial septation. The right side of thecommon atrium received the common pulmonaryvein from twin B while the left side received the sys-temic veins from twin B. The pulmonary venous-return from twin A was to the morphologically leftatrium.The four atrial chambers were connected to one
ventricular mass through a conjoined atrioven-tricular junction (fig 3). The ventricular mass pos-sessed a right-sided morphologically right ventricleand a left-sided morphologically left ventricle. Inaddition, there was a rudimentary right ventricle onthe left anterior shoulder of this dominant leftventricle that was exclusive to twin A. A valve oftricuspid morphology connected the right-sidedatrium of twin B to the morphologically right ventri-cle. This valve overrode and straddled the dominant-morphologically left ventricle, the latter chamberbeing shared by both twins. The right-sided rightventricle supported the subaortic and subpulmonaryoutflow tracts of twin B. The aorta was anterior andto the right while the pulmonary valve was markedlystenotic. The aortic arch was right-sided with a-right-sided arterial duct feeding the conjoined pul-monary arteries. The necropsy report noted thattwin B had no spleen. A common atrioventricularvalve guarded the right and the left atrioventricularjunctions of twin A, together with the junction of theleft-sided morphologically right atrium of twin B tothe morphologically left ventricle. This ventriclehad a large communication with the right ventricle.The latter supported both great arteries (double out-let right ventricle). The outflow to the aorta wasobstructed by a muscle band. The aortic arch wasleft-sided with a left-sided arterial duct and a para-ductal coarctation.
S ET1 2The hearts, which were studied in isolation, werejoined at atrial and ventricular levels in book-leaffashion. There were four atrial appendages. Eachtwin showed the usual atrial arrangement (fig 4).There were bilateral superior and inferior cavalveins. The anterior morphologically right atrium oftwin A received all the pulmonary venous drainagefrom this twin through a common pulmonary vein.The pulmonary veins of twin B were connected tothe appropriate anterior morphologically leftatrium, again through a common channel.The anterior morphologically right atrium of twin
519
copyright. on N
ovember 27, 2020 by guest. P
rotected byhttp://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.58.5.518 on 1 Novem
ber 1987. Dow
nloaded from

Table Summary of the cardiac an'omaliesfound in three sets of conjoined twins
Twin B Twin A
Set 1:Right atrial isomerismAmbiguous atrioventricular connectionRight-hand topologyDouble outlet right ventricleTotally anomalous pulmonary venous connection
Set 2:Usual atrial arrangementConcordant atrioventricular connectionConcordant ventriculoarterial connectionAtrioventricular septal defect
Set 3:Usual atrial arrangementConcordant atrioventricular connectionConcordant ventriculoarterial connectionTotally anomalous pulmonary venous connection
Set 1:Usual atrial arrangementDouble inlet left ventricleDouble outlet right ventricle
Set 2:Usual atrial arrangementAbsent left atrioventricular connectionAnterior left-sided rudimentary right ventricleDiscordant ventriculoarterial connectionTotally anomalous pulmonary venous connection
Set 3:Usual atrial arrangementAbsent right atrioventricular connectionAnterior right-sided rudimentary right ventricleDiscordant ventriculoarterial connectionTotally anomalous pulmonary venous connection
A was connected to a morphologically left ventricle(fig 5) through a slightly dysplastic atrioventricularvalve. This left ventricle supported the pulmonarytrunk (discordant ventriculoarterial connection).The posterior morphologically left atrium was smallwith a complete muscular floor (absent leftatrioventricular connection) and communicatedwith the right atrium through an oval fossa defect.An anterosuperior and left-sided rudimentary rightventricle supported the aorta which was left-sidedand posterior. There was a left aortic arch with apatent left arterial duct and a retro-oesophageal
Left-sided morph.left atriumof twin B......
N.,. :;
Right-sided morph.right atriumnof twin A
/
%r gra.tMorph. leftatrium oftwin A ..:i
\; l....
ally related Posterior aortaarteries of twin B of twin1
Morph. right Openingatrium the morph.
/I2. peft atriumPV:) e- <PV,Right s6 Right Left 'atrium attrium aitriumn
Fig 3 Diagram showing the conjoined atrioventricularjunction of set 1. LV, left ventricle; RV, right ventricle.
Fig 4 (a) Anterosuperior view of the hearts of set 2showing the morphologically left atrium of twin B,morphologically right atrium of twin A, and the greatarteries of both twins. (b) Internal view of atria from behind.
Twin B Twin A
520 Rossi, Burn, Ho, Thiene, Devine, Anderson
copyright. on N
ovember 27, 2020 by guest. P
rotected byhttp://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.58.5.518 on 1 Novem
ber 1987. Dow
nloaded from

Conjoined twins, right atrial isomerism, and sequential segmental analysis
Twin B Twin Aa j
I- I I -1~~~.
Twin A
Fig 5 Diagrammatic representation of the hearts of set 2.ICV, inferior caval vein; LV, left ventricle; OF, ovalfossa;PV, pulmonary vein; RV, right ventricle; SCV, superiorcaval vein.
right subclavian artery. The proximal part of the leftpulmonary artery was hypoplastic.Twin B had a concordant atrioventricular con-
nection with right-hand topology of its ventricularmass. Its atrioventricular junction was guarded by acommon valve and there was an atrioventricular sep-tal defect. There was minimal bridging of the supe-rior bridging leaflet (Rastelli type A) and the barecrest of the ventricular septum was visible betweenthe superior and inferior bridging leaflets. The mor-phologically right ventricle supported the pul-monary trunk and the morphologically left ventriclesupported the aorta (concordant ventriculoarterialconnection). The aorta was posterior and to the rightin relation to the pulmonary trunk, which wasdilated- (normal relations). Twin A, therefore, hadabsence of the left-sided atrioventricular connectionwith the right atrium connected to a dominant leftventricle and a discordant ventriculoarterial con-nection. Twin B had normal chamber conmectionsbut showed an atrioventricular septal defect. Theventricles of both hearts were contained within thematrix of a common ventricular mass.
SET 3These twins were positioned face to face and joinedacross the chest and abdomen (fig 6). The chest wallswere contiguous laterally, each side being made upby a common sternum articulating with the ribs ofeach twin. The lungs of both twins showed the usual
Fig 6 Set offemale conjoined twins (set 3) joined acrossthe chest.
lobulation and both twins had a spleen. The liverwas common to both, and they also shared a smallbowel.The hearts were joined at atrial and ventricular
levels. There were four atrial appendages. Each twinshowed the usual atrial arrangement (fig7). Therewere bilateral superior caval veins. The left-sidedvein received the entire pulmonary venous drainageof twin A and was then connected to the posteriormorphologically right atrium of this twin, whichalso received the entire pulmonary venous return oftwin B through the coronary sinus. This mor-phologically right atrium was small and had a dim-pIe in its muscular floor. There was a defect acrossthe oval fossa which connected to the anterior mor-phologically left atrium of twin A. The left atriumwas connected, through a normal mitral valve, to amorphologically left ventricle which supported thepulmonary trunk. An anterosuperior and right-sided rudimentary right ventricle was carried on theshoulder of the dominant left ventricle and sup-ported an aorta which was anterior and right-sided.The aortic arch then coursed to the left side of twinA. There was a patent left-sided arterial duct.The anterior morphologically right atrium of twin
521
copyright. on N
ovember 27, 2020 by guest. P
rotected byhttp://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.58.5.518 on 1 Novem
ber 1987. Dow
nloaded from

Rossi, Burn, Ho, Thiene, Devine, AndersonTwin B
I-
Twin A
Fig 8 Diagram showing the cardiac anomaliesfound in thehearts of set 3. Abbreviations as in fig5.
Fig 7 External morphology of the atriums of both twinsof set 3.
B received the right-sided superior caval vein and aninferior caval vein common to both twins. This rightatrium connected through an oval fossa defect to theleft atrium and through a stenotic tricuspid valve toa morphologically right ventricle. The right ventri-cle supported the pulmonary trunk. The posteriormorphologically left atrium of twin B was connectedto a heavily trabeculated morphologically left ventri-cle which supported the aorta. The aorta was poste-rior and right-sided. The aortic arch was to the leftand there was patency of the arterial duct. The greatarteries of twin B were normally related.Thus there was considerably admixture of the
venous connections of both twins, there being totallyanomalous pulmonary connections of both to themorphologically right atrium of twin A. In terms ofcardiac morphology, twin A had tricuspid atresia(absent right atrioventricular connection) with theleft atrium connected to a dominant left ventricleand a discordant ventriculoarterial connection.Twin B had normal chamber connections but a ste-
notic tricuspid valve, The ventricles of both heartswere contained, as in set 2, within the matrix of acommon ventricular mass (fig 8).
Discussion
The general belief is that conjoined malformationsresult from incomplete fission of the developingzygote. Conjunction represents the extreme of atime spectrum at the other end of which are "identi-cal" twins with separate placentas (dichorionicmonozygotic twins). The developmental separationin the setting of discrete placentas predates theblastocyst stage. The chorion is committed beforedivision in monochorionic monozygotic twins.Monoamniotc twins share an amnion while con-joined twins share some body part, most often in thethoracic region. When joined, the hearts are usuallyconnected at atrial level and may additionally bejoined at ventricular level. Usually the venous andarterial connections are distinct.
Isomerism in one of a conjoined twin pair -isimportant in the precise diagnosis of cardiac mal-formation. It is also pertinent to our understandingof cardiac embryology and to the determination oflaterality itself. The important relation betweentwinning, laterality, and development of the heartand other organs has become clear only recently.Noonan commented on the similarity between thepattern of cardiac malformation in conjoined twinsand that seen in isomerism.2 Ursell and Wigger sub-sequently reported right isomerism in one of a set ofconjoined twins and drew attention to two othersets.3 In their interpretation, they did not discuss
522
copyright. on N
ovember 27, 2020 by guest. P
rotected byhttp://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.58.5.518 on 1 Novem
ber 1987. Dow
nloaded from

Conjoined twins, right atrial isomerism, and sequential segmental analysis 523
the relation with laterality. In his classic evaluationof the biases involved in the use of twins as aresearch tool, Price reviewed the extensive early lite-rature on mirror imagery and lateral inversions.4 Heconcluded that such disturbance was unlikely to be amajor cause of abnormality. Ivemark, in his reviewof the asplenia syndrome, commented on the abnor-mal symmetry of the body.5 The importance of thisfeature was brought to the fore by Van Mierop et al.6In particular, Van Mierop et al noted the value of theatrial appendages in the recognition of isomerism. Itcan be argued that this abnormal symmetry leads toa disturbance of the expected rightward bend of theheart tube (or dextral heart loop) with consequentmalformation. This deduction is supported by stud-ies in a particular strain of mouse where disturbanceof laterality has an autosomal recessive geneticbasis.7
Biologists have noted disturbance of organarrangement in conjoined twins in other species. Agood example is the right-sided heart seen in the onehalf of conjoined trout.8 This observation providedpart of the evidence in favour of a left/right gradientunderlying the determination of laterality in theembryo.9 Bringing together these strands of evi-dence, it may be concluded that the late twinningthat produces conjoined individuals is liable to inter-rupt the "left/right gradient". The result is that the"right" half loses its point of reference and is liableto suffer a disturbance of laterality. This results, inthe extreme case, in a twin with two morphologicallyright sides. A similar explanation may be offered forthe right isomerism reported in one of monozygotictwins.10 ii It is in keeping with the suggestion thatthe excess of heart defects in monozygotic twin setsis due in part to disturbance of laterality in one set.12In theory, two left sides (left isomerism) could alsoexist in conjoined twins though this seems not tooccur often. One possible example was the conjoinedset described by Marin-Padilla et al in which onetwin was noted to have two bilobed or "left"lungs.13Our study exemplifies the need for precise
identification of atrial morphology. The initial diag-nosis of isomerism in one of the twins in set 1 wasmade by studying the atrial morphology. Sub-sequent inquiry revealed the absence of spleen in theappropriate twin, the organs being usually arrangedin the complementary twin. Atrial morphology wasascertained from constant features, namely the pres-ence (morphologically right atrium) or absence(morphologically left atrium) of the terminal cresttogether with shape of the appendages. Other crite-ria such as septal morphology and systemic or pul-monary venous connections are less reliable.Common atrial chambers were present in two of our
three cases. There were totally anomalous pul-monary venous connections in four cases within thethree sets. Although draining via a common vein,the pulmonary veins were connected to the mor-phologically left atrium in the remaining two cases.These malformations did not invalidate recognitionaccording to the morphology of the appendages andtheir junctions with the venous components of theatrial chambers. Accurate diagnosis of the atrialarrangement sets the scene in all instances for suc-cessful sequential analysis of the complex cardiacarrangements. Sharing of ventricular chambers hasnot precluded the use of sequential analysis sinceeach heart can be studied fully in terms of segments.Our study demonstrates the ease of investigating"complex" heart malformations by the use of a sys-tematic approach. Although from a clinical stand-point the shared atrioventricular junctions and/orventricular musculature in all our sets would havemade surgical separation impractical, the sameapproach would identify those sets which might, infuture, be amenable to corrective surgical pro-cedures.
We are grateful to Mr P Silverstone, consultantobstetrician in Gateshead, who referred set 3.MBR was research fellow at the Department of
Paediatrics, Cardiothoracic Institute from "Funda-cao Federal de Ciencias Medicas de Porto Alegre"supported by "Coordenacao de Aperfeicoamento doPessoal de Nivel Superior", Education and CultureMinistry of Brazil. SYH is supported by the BritishHeart Foundation. RHA is supported by the BritishHeart Foundation together with the Joseph LevyFoundation.
References
1 Benirschke K, Temple WW, Bloor CM. Conjoinedtwins: nosology and congenital malformations. In:Birth defects: original series, volume XIV, number 6A.New York: Alan R Liss for The National Founda-tion, 1978:170-92.
2 Noonan JA. Twins, conjoined twins and cardiacdefects. Am J Dis Child 1978;132:17-8.
3 Ursell PC, Wigger HJ. Asplenia syndrome in conjoinedtwins: a case report. Teratology 1983;27:301-4.
4 Price B. Primary biases in twin studies. A review ofprenatal and natal difference-producing factors inmonozygotic pairs. Am J Hum Genet 1950;2:293-352.
5 Ivemark BI. Implications of agenesis of the spleen onthe pathogenesis of conotruncus anomalies in child-hood. An analysis of the heart; malformations in thesplenic agenesis syndrome, with 14 new cases. ActaPaediatr Scand 1955;44(suppl 104):1-110.
copyright. on N
ovember 27, 2020 by guest. P
rotected byhttp://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.58.5.518 on 1 Novem
ber 1987. Dow
nloaded from

524 Rossi, Burn, Ho, Thiene, Devine, Anderson
6 Van Mierop LHS, Gessner IH, Schiebler GL.Asplenia and polysplenia syndromes. In: Birthdefects: original article series volume VIII, number 5.Baltimore: Williams and Wilkins for the NationalFoundation, 1972:36-44.
7 Layton WM, Manasek FJ. Cardiac looping in early ivembryos. In: Van Praagh R, Takao A, eds. Etiologyand morphogenesis of congenital heart disease. MountKisco, New York: Futura Publishing Company,1980:109-26.
8 Neville AC. Animal asymmetry. In: Studies in biology.London: Edward Arnold, 1976:67.
9 Corballis MC, Morgan MJ. On the biological basis of
human laterality. Evidence of a maturational left toright gradient. Behavioural and Brain Sciences1978;2:261-3.
10 Schinzel A, Smith D, Miller J. Monozygotic twinningand structural defects. J Pediatr 1979;95:921-30.
11 Wilkinson JL, Holt PA, Dickinson DF, Jivani SK.Asplenia syndrome in one of monozygotic twins. EurJ Cardiol 1979;10:301-4.
12 Burn J, Corney G. Congenital heart defects andtwinning. Acta Genet Med Gemellol 1984;33:61-9.
13 Marin-Padilla M, Chin AJ, Marin-Padilla TM.Cardiovascular abnormalities in thoracopagus twins.Teratology 1981;23:101-13.
copyright. on N
ovember 27, 2020 by guest. P
rotected byhttp://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.58.5.518 on 1 Novem
ber 1987. Dow
nloaded from
Related Documents