CARBOHYDRATE METABOLISM By :- SANA DANISH SUBAS IMTIAZ NAJAF BATOOL 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CARBOHYDRATE METABOLISM
By :-SANA DANISHSUBAS IMTIAZ NAJAF BATOOL
1
2015/1/3

2015/1/3
UOL PHARMACIST

2015/1/3
UOL

CONTENTS• Introduction
- Nutrition
- Carbohydrates
- Classification of carbohydrates
- Functions of carbohydrates
- What is metabolism?
• Major metabolic pathways of carbohydrates
- Introduction about each pathway
- Step of reactions in every metabolic pathway
- Clinical Aspects 5
• Polysaccharides and clinical aspects
• Role of hormones in carbohydrate metabolism
• Dental aspects of carbohydrate metabolism
• Recent issue related to carbohydrate metabolism
• Summary of carbohydrate metabolism
• Conclusion6

INTRODUCTION
7
NUTRITION
• Nutrition is defined as “ the science of how the
body utilizes food to meet requirements for
development growth, repair and maintenance.”
CARBOHYDRATES
FATS
PROTEINS
VITAMINS
MINERALS
WATER8

Daily Intake
• Nutrient Quantity Per Day
Energy = 8,700 kilojoules
Protein = 50 grams
Fat = 70 grams
Carbohydrates = 310 grams
Sugars = 90 grams
Sodium (salt) = 2.3 grams
Dietary Fibre = 30 grams
Saturated Fatty Acids = 24 grams
9

CARBOHYDRATE:
Most abundant organic molecule on earth.
Carbohydrates are defined as aldehyde or keto derivatives
of polyhydric alcohols.
For example: Glycerol on oxidation is converted to
D-glyceraldehyde, which is a carbohydrate derived from the
trihydric alcohol (glycerol).
All carbohydrates have the general formula CnH2nOn [or it
can be re-written as Cn(H2O)n ] .
10
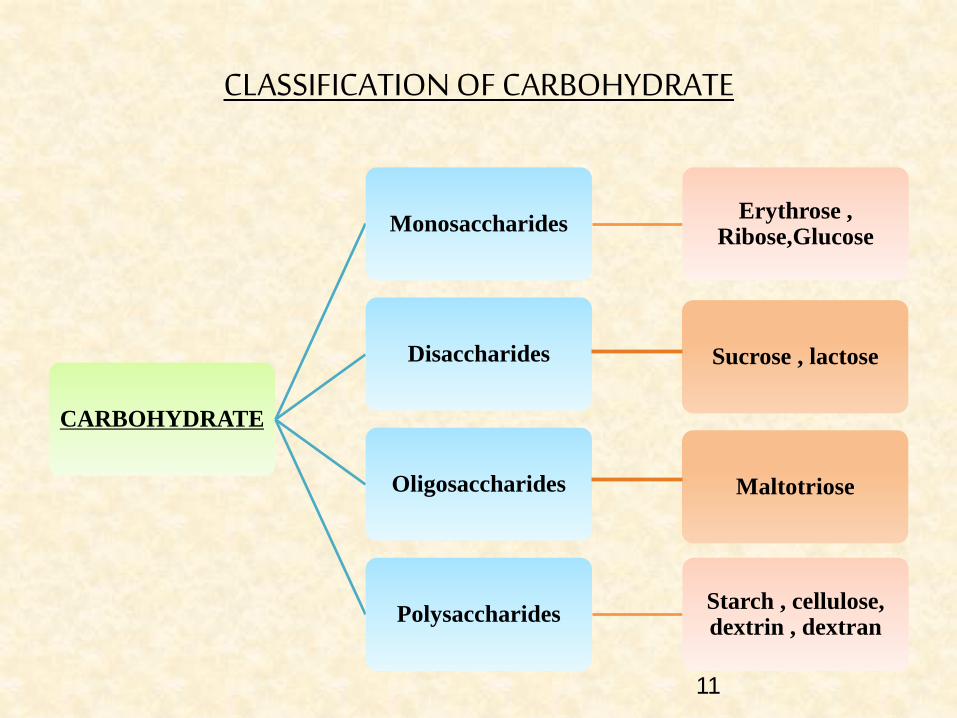
CLASSIFICATION OF CARBOHYDRATE
CARBOHYDRATE
MonosaccharidesErythrose ,
Ribose,Glucose
Disaccharides
Oligosaccharides
Polysaccharides Starch , cellulose, dextrin , dextran
Sucrose , lactose
Maltotriose
11

FUNCTIONS OF CARBOHYDRATES
Main source of energy in the body. Energy
production from carbohydrates will be 4 k
calories/g (16 k Joules/g).
Storage form of energy (starch and glycogen).
Excess carbohydrate is converted to fat.
Glycoproteins and glycolipids are components of
cell membranes and receptors.
Structural basis of many organisms. For example,
cellulose of plants,exoskeleton of insects etc.
12

Biomedical Importance Of Glucose
• Glucose is a major carbohydrate
• It is a major fuel of tissues
• It is converted into other carbohydrates
Glycogen for storage.
Ribose in nucleic acids.
Galactose in lactose of milk.
They form glycoproteins & proteoglycans
They are present in some lipoproteins (LDL) .
Present in plasma membrane:glycocalyx.
Glycophorin is a major intergral membrane glycoprotein
of human erythrocytes.
13

Metabolism
Thousands of chemical reactions are
taking place inside a cell in an
organized, well co-ordinated and
purposeful manner; all these
reactions are called as
METABOLISM.
TYPES OF METABOLIC
PATHWAY:
Catabolic Pathway
Anabolic Pathway
Amphibolic Pathway
STAGES AND PHASES
OF METABOLISM:
Primary
Secondary
Tertiary14
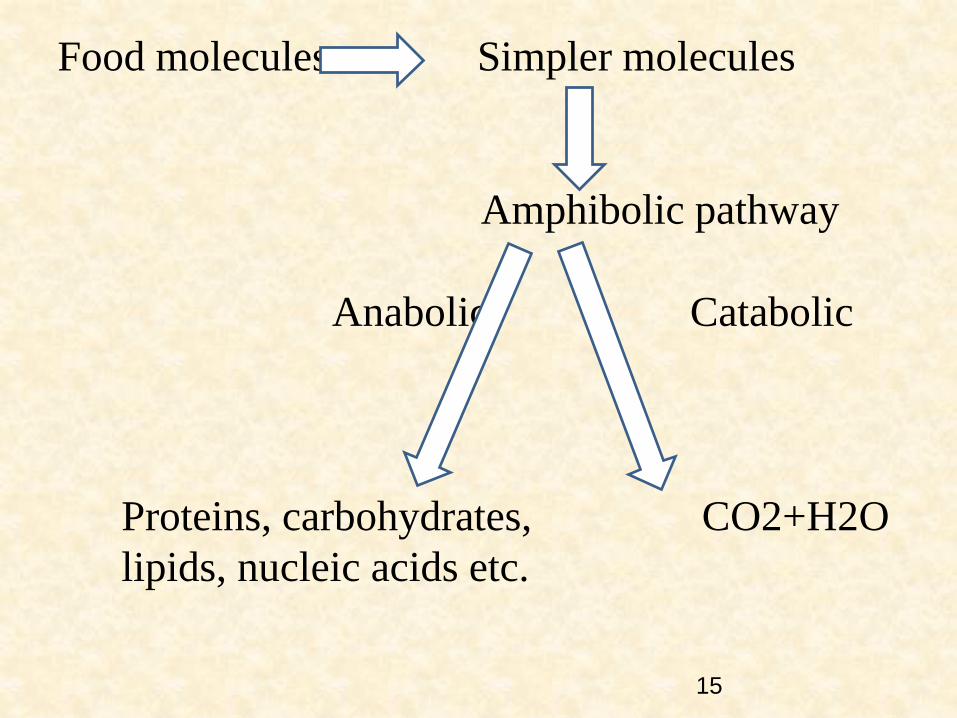
Food molecules Simpler molecules
Amphibolic pathway
Anabolic Catabolic
Proteins, carbohydrates, CO2+H2O
lipids, nucleic acids etc.
15
Major Pathways of
Carbohydrate Metabolism
16

1) Glycolysis
2) Citric Acid Cycle
3) Gluconeogenesis
4) Glycogenesis
5) Glycogenolysis
6) Hexose monophosphate shunt
7) Uronic Acid Pathway
8) Galactose Metabolism
9) Fructose Metabolism
10) Amino sugar metabolism17
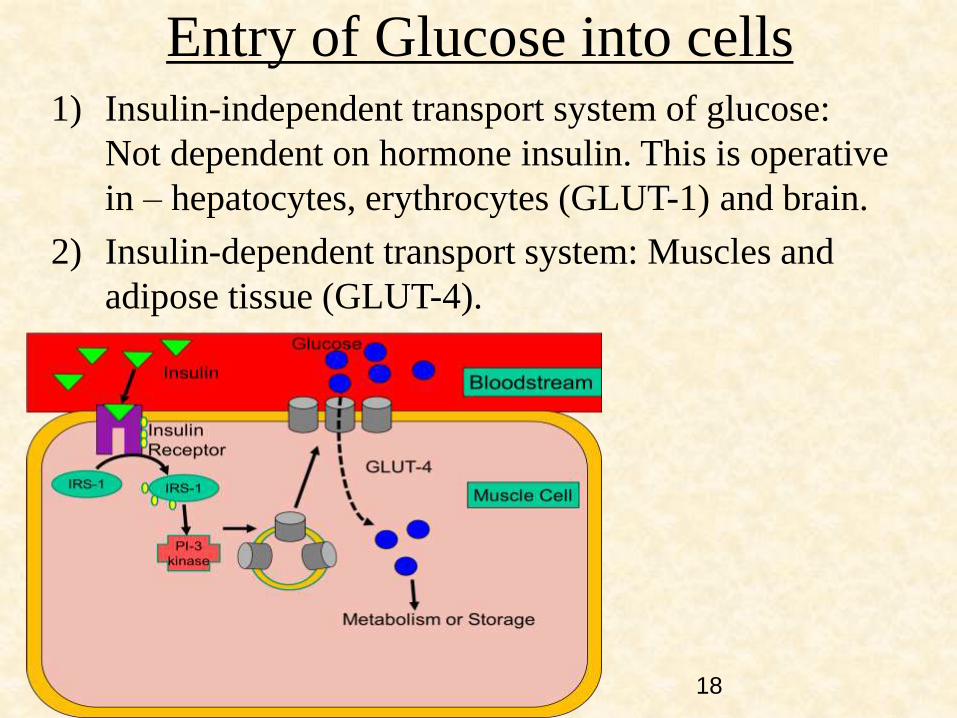
Entry of Glucose into cells1) Insulin-independent transport system of glucose:
Not dependent on hormone insulin. This is operative
in – hepatocytes, erythrocytes (GLUT-1) and brain.
2) Insulin-dependent transport system: Muscles and
adipose tissue (GLUT-4).
18

GlycolysisEmbden-Meyerhof pathway
(or)
E.M.Pathway
Definition:
Glycolysis is defined as the sequence of
reactions converting glucose (or glycogen) to
pyruvate or lactate, with the production of ATP
19

Salient features:
1) Takes place in all cells of the body.
2) Enzymes present in “cytosomal fraction” of the
cell.
3) Lactate – end product – anaerobic condition.
4) Pyruvate(finally oxidized to CO2 & H2O) – end
product of aerobic condition.
5) Tissues lacking mitochondria – major pathway –
ATP synthesis.
6) Very essential for brain – dependent on glucose for
energy.
7) Central metabolic pathway
8) Reversal of glycolysis – results in gluconeogenesis.20
Reactions of Glycolysis
1) Energy Investment phase (or) priming phase
2) Splitting phase
3) Energy generation phase
21

Energy Investment
Phase
• Glucose is phosphorylated to glucose-6-phosphate by hexokinase (or) glucokinase.
• Glucose-6-phosphate undergoes isomerization to give fructose -6- phosphate in the presense of phospho-hexose isomerase and Mg2+
• Fructose-6-phosphate is phoshorylated to fructose 1,6-bisphosphate by phosphofructokinase.
Splitting Phase
• Fructose 1,6-bisphosphate glyceraldehyde 3-phosphate + dihydroxyacetone phosphate.(aldolase enzyme)
• 2 molecules of glyceraldehyde 3-phosphate are obtained from 1 molecule of glucose
Energy Generation
Phase
• Glyceraldehyde 3-phosphate 1,3-bisphosphoglycerate(glyceraldehyde 3-phosphate hydrogenase )
• 1,3-bisphosphoglycerate 3-phosphoglycerate (phosphoglycerate kinase)
• 3-phosphoglycerate 2-phosphoglycerate (phosphoglycerate mutase)
• 2-phosphoglycerate phosphoenol pyruvate (enolase + Mg2+ & Mn2+)
• Phosphoenol pyruvate pyruvate [enol] (pyruvate kinase ) pyruvate [keto] L-Lactate (lactate dehydrogenase)
22

23

24

Energy production of glycolysis:
Net energy ATP utilized ATP produced
2 ATP 2ATP
From glucose to glucose -
6-p.
From fructose -6-p to
fructose 1,6 p.
4 ATP
(Substrate level
phosphorylation)
2ATP from 1,3 DPG.
2ATP from phosphoenol
pyruvate
In absence of oxygen
(anaerobic glycolysis)
8 ATP /
6 ATP (Pyruvate
dehydrogenase
2NADH,ETC,
Oxidative
phosphorylation)
2ATP
-From glucose to glucose -
6-p.
From fructose -6-p to
fructose 1,6 p.
4 ATP
(substrate level
phosphorylation)
2ATP from 1,3 BPG.
2ATP from phosphoenol
pyruvate.
+ 4ATP or 6ATP
(from oxidation of 2
NADH + H in
mitochondria).
In presence of oxygen
(aerobic glycolysis)
ATP production = ATP produced - ATP utilized
25
CLINICAL ASPECT
1) Lactic acidosis
- Normal value – 4 to 15 mg/dl.
- Mild forms – strenous exercise, shock,
respiratory diseases, cancers
- Severe forms – Impairment/collapse of
circulatory system – myocardial infarction,
pulmonary embolism, uncontrolled
hemmorrhage and severe shock.
26
2) Cancer and glycolysis :
- Cancer cells – increased uptake of glucose and glycolysis.
- Blood vessels unable to supply adequate oxygen – HYPOXIC condition – Anaerobic glycolysis / hypoxic glycolysis – Involvement of Hypoxic inducible transcription factor (HIF).
- Treatment : Use drugs that inhibit vascularization of tumours
27
Pasteur effect : Inhibition of glycolysis by
oxygen (Phosphofructokinase) .
Crabtree effect : The phenomenon of
inhibition of oxygen consumption by the
addition of glucose to tissues having high
aerobic glycolysis.
28

RAPARPORT – LEUBERING CYCLE
• Supplementary pathway/ Shunt pathway to glycolysis .
• Erythrocytes
• Synthesis of 2,3-bisphosphoglycerate (2,3-BPG).
• Without the synthesis of ATP.
• Help to dissipate or waste the energy not needed by RBCs.
• Supply more oxygen to the tissues.
29
CITRIC ACID CYCLEKREBS CYCLE / TRICARBOXYLIC ACID/
TCA CYCLE
Essentially involves the oxidation of acetyl CoA
to CO2 and H2O.
This Cycle utilizes about two-third of total
oxygen consumed by the body.
30

Brief History:
• Hans Adolf Krebs
• 1937
• Studies of oxygen consumptiom in pigeon breast muscle.
Location of TCA
• Mitochondrial matrix
• In close proximity to the electronic transport chain.
Overview
• 65-70% of the ATP is synthesized
• Name : TCA used because at the ouset of the cycle tricarboxylic acids participate.
31

Reactions of citric acid cycle
1) Formation of citrate : Condensation of acetyl CoA and
oxaloacetate catalysed by citrate synthase.
2) & 3) Citrate is isomerized to isocitrate aconitase (two
steps).
4) & 5) Formation of ᾀ-ketoglutarate : enzyme isocitrate
dehydrogenase.
6) Conversion of ᾀ-ketoglutarate to succinyl CoA :
through oxidative decarboxylation, catalysed by ᾀ-
ketoglutarate dehydrogenase complex.32

33
7)Formation of succinate : enzyme succinate thiokinase
GTP + ADP ATP + GDP (nucleoside diphosphate kinase)
8)Conversion of succinate to fumarase : enzyme succinate dehydrogenase
9)Formation of malate : enzyme fumarase
10)Conversion of malate to oxaloacetate : enzyme malate dehydrogenase.
33

34
• TCA cycle is strictly aerobic in contrast to glycolysis.
• Total of 12 ATP are produced from one acetyl CoA :-
During the process of oxidation of acetyl CoA via
citric acid cycle 3 NADH & 1 FADH2.
Oxidation of 3 NADH by electron transport chain
coupled with oxidative phosphorylation results in 9
ATP, FADH2 2 ATP.
One substrate level phosphorylation.35
Mitochondrial encephalopathy occurs due to fumarase deficiency .
It is a mitochondrial myopathy affecting both the skeletal muscles and brain .
APPLIED ASPECTS OF
TCA CYCLE
36

GLUCONEOGENESIS
The synthesis of glucose from non-carbohydrate compounds is known as gluconeogenesis.
Major substrate/precursors : lactate, pyruvate, glycogenic amino acids, propionate & glycerol.
-Takes place in liver (1kg glucose) ; kidney matrix( 1/3rd).
- Occurs in cytosol and some produced in mitochondria.
37
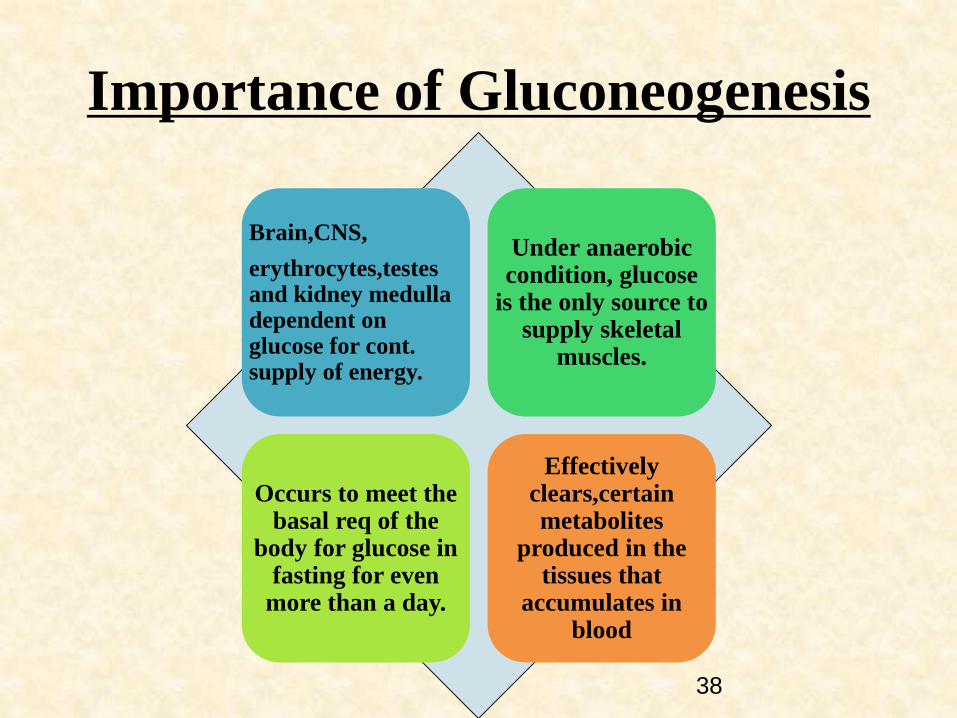
Importance of Gluconeogenesis
Brain,CNS,
erythrocytes,testes and kidney medulla dependent on glucose for cont. supply of energy.
Under anaerobic condition, glucose
is the only source to supply skeletal
muscles.
Occurs to meet the basal req of the
body for glucose in fasting for even
more than a day.
Effectively clears,certain metabolites
produced in the tissues that
accumulates in blood
38
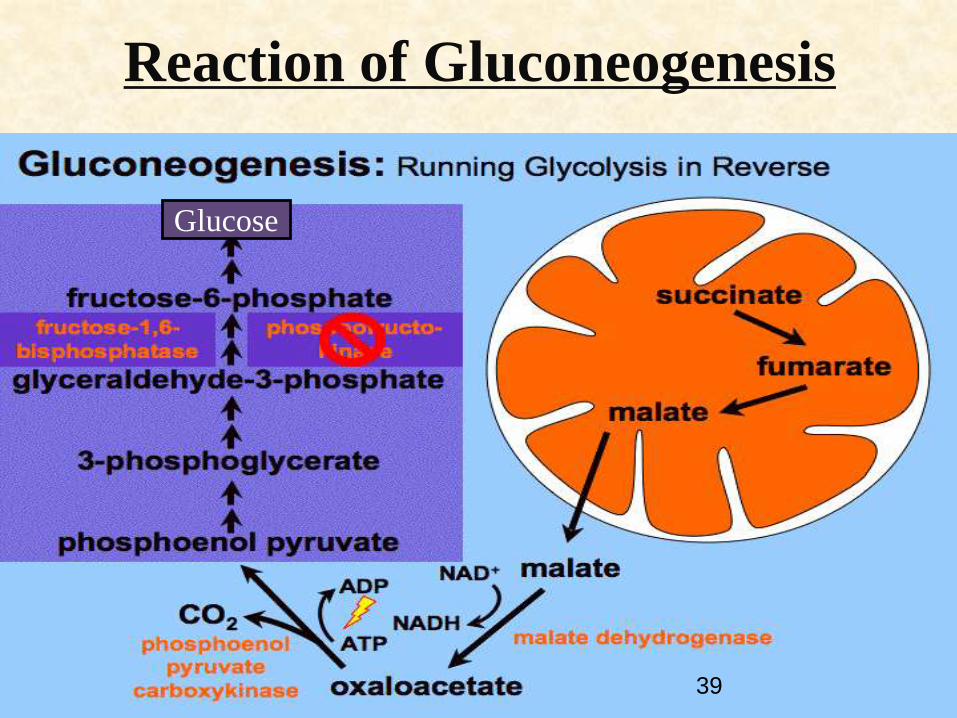
Reaction of Gluconeogenesis
Glucose
39
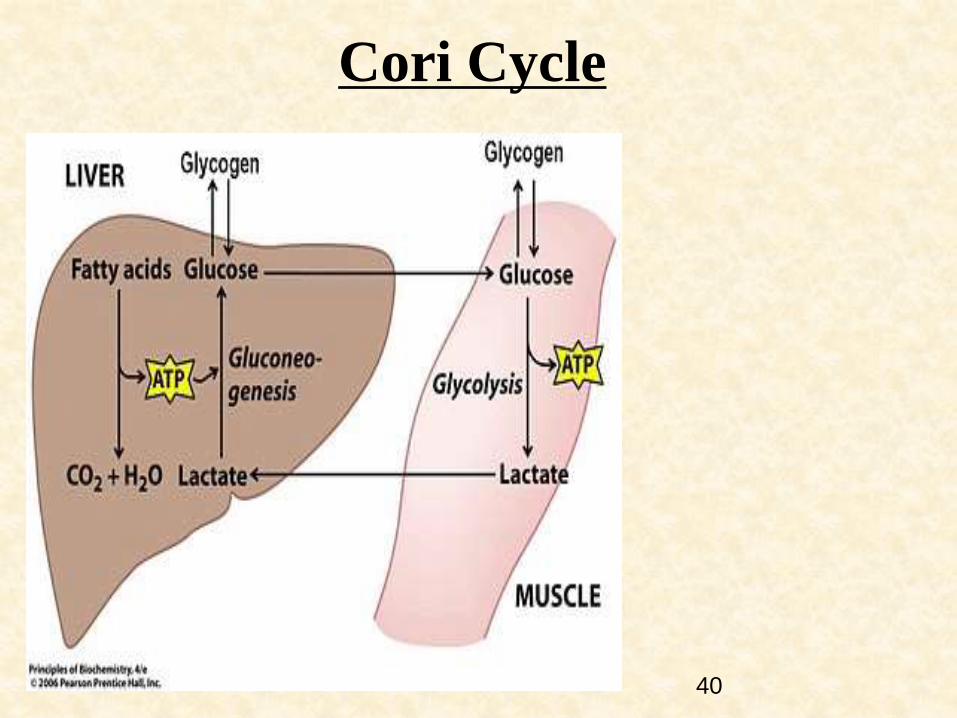
Cori Cycle
40
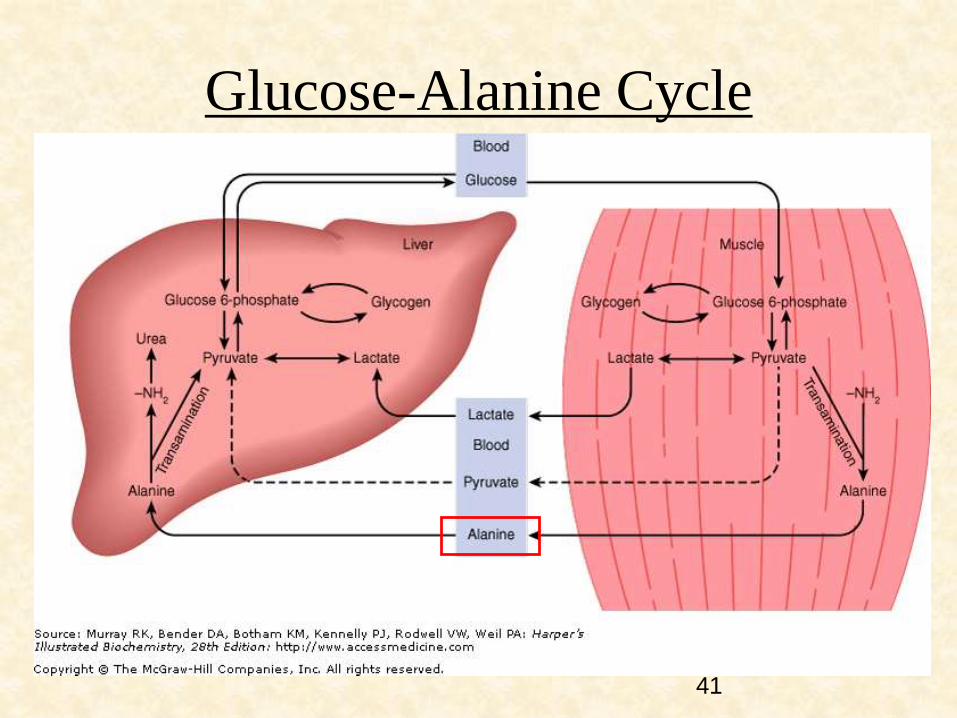
Glucose-Alanine Cycle
41

Clinical Aspects
* Glucagon stimulates gluconeogenesis:
1)Active pyruvate kinase converted to inactive form
2)Reduces the concentration of fructose 2,6-bisphosphate.
* Glycogenic amino acids have stimulating influence on gluconeogenesis.
* Diabetes mellitus where amino acids are mobilized from muscle protein for the purpose of gluconeogenesis.
Acetyl CoA promotes gluconeogenesis:
* During starvation – due to excessive lipolysis in adipose tissue –acetyl CoA accumulates in the liver.
* Acetyl CoA allosterically activates pyruvate carboxylase resulting in enhanced glucose production
* Alcohol inhibits gluconeogenesis
42
GLYCOGEN METABOLISM
Glycogen is a storage form of glucose in animals.
Stored mostly in liver (6-8%) and muscle (1-2%)
Due to muscle mass the quantity of glycogen in muscle = 250g
and liver =75g
Stored as granules in the cytosol.
Functions : Liver glycogen – maintain the blood glucose level
Muscle glycogen – serves as fuel reserve
43
GLYCOGENESIS
Synthesis of glycogen from glucose.
Takes place in cytosol.
Requires UTP and ATP besides glucose.
Steps in synthesis :
1) Synthesis of UDP- glucose
2) Requirement of primer to initiate glycogenesis
3) Glycogen synthesis by glycogen synthase
4) Formation of branches in glycogen
44

45

GLYCOGENOLYSIS
Degradation of stored glycogen in liver and muscle constitutes
glycogenolysis.
Irreversible pathway takes place in cytosol.
Hormonal effect on glycogen metabolism :
1) Elevated glucagon – increases glycogen degradation
2) Elevated insulin – increases glycogen synthesis
Degraded by breaking majorly α-1,4- and α-1,6-glycosidic bonds.
Steps in glycogenolysis:
1) Action of glycogen phosphorylase
2) Action of debranching enzyme
3) Formation of glucose-6-phosphate and glucose
46

47
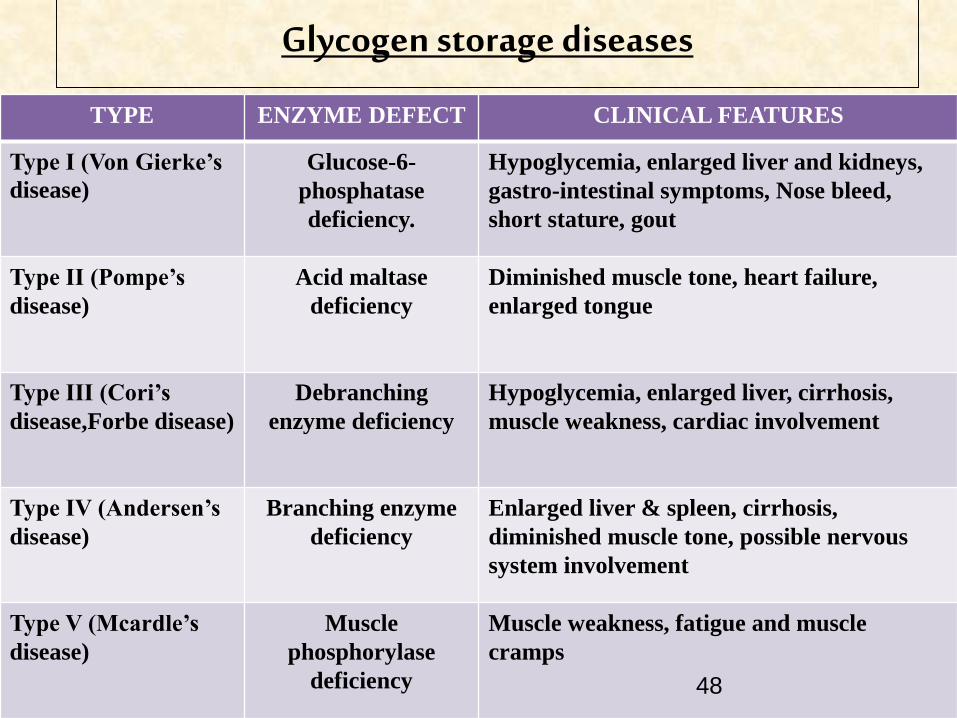
TYPE ENZYME DEFECT CLINICAL FEATURES
Type I (Von Gierke’s
disease)
Glucose-6-
phosphatase
deficiency.
Hypoglycemia, enlarged liver and kidneys,
gastro-intestinal symptoms, Nose bleed,
short stature, gout
Type II (Pompe’s
disease)
Acid maltase
deficiency
Diminished muscle tone, heart failure,
enlarged tongue
Type III (Cori’s
disease,Forbe disease)
Debranching
enzyme deficiency
Hypoglycemia, enlarged liver, cirrhosis,
muscle weakness, cardiac involvement
Type IV (Andersen’s
disease)
Branching enzyme
deficiency
Enlarged liver & spleen, cirrhosis,
diminished muscle tone, possible nervous
system involvement
Type V (Mcardle’s
disease)
Muscle
phosphorylase
deficiency
Muscle weakness, fatigue and muscle
cramps
Glycogen storage diseases
48
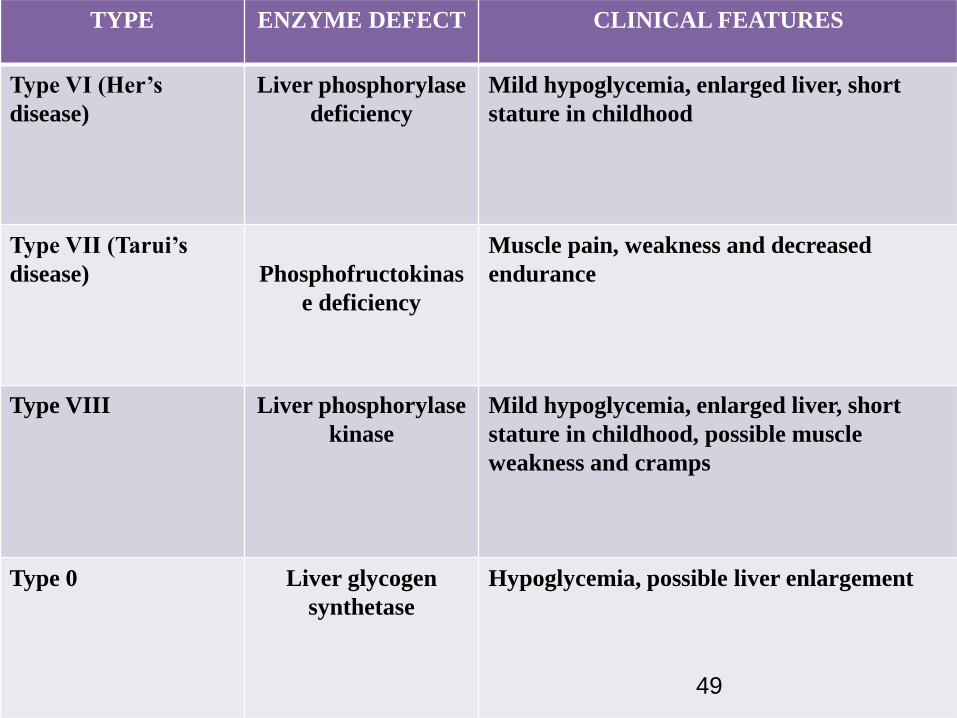
TYPE ENZYME DEFECT CLINICAL FEATURES
Type VI (Her’s
disease)
Liver phosphorylase
deficiency
Mild hypoglycemia, enlarged liver, short
stature in childhood
Type VII (Tarui’s
disease) Phosphofructokinas
e deficiency
Muscle pain, weakness and decreased
endurance
Type VIII Liver phosphorylase
kinase
Mild hypoglycemia, enlarged liver, short
stature in childhood, possible muscle
weakness and cramps
Type 0 Liver glycogen
synthetase
Hypoglycemia, possible liver enlargement
49
Von Gierke’s disease)
Pompe’s disease
50

Cori’s disease, Forbe
disease
51
HEXOSE MONOPHOSPHATE SHUNT
HMP Shunt/ Pentose Phosphate Pathway/
Phosphogluconate Pathway
52

* This is an alternative pathway to glycolysis and TCA cycle for the oxidation of glucose.
* Anabolic in nature, since it is concerned with the biosynthesis of NADPH and pentoses.
* Unique multifunctional pathway
* Enzymes located – cytosol
* Tissues active – liver, adipose tissue, adrenal gland, erythrocytes, testes and lactating mammary gland.53

Reactions of the HMP Shunt Pathway
54
• Pentose or its derivatives are useful for the synthesis of nucleic acids and nucleotides.
• NADPH is required :
- For reductive biosynthesis of fatty acids and steroids.
- For the synthesis of certain amino acids.
- Anti-oxidant reaction
- Hydroxylation reaction– detoxification of drugs.
- Phagocytosis
- Preserve the integrity of RBC membrane.
Significance of HMP Shunt
55

• Glucose-6-Phosphate dehydrogenase
deficiency :
- Inherited sex-linked trait
- Red blood cells
- Impaired synthesis of NADPH
- hemolysis , developing hemolytic anemia
Resistance towards malaria [Africans]
Clinical Aspects
56
Clinical Aspects
• Wernicke-Korsakoff syndrome :
- Genetic disorder
- Alteration in transketolase activity
- Symptoms : mental disorder, loss of memory,
partial paralysis
• Pernicious anemia : transketolase activity
increases.
57
URONIC ACID PATHWAY
(Or)
Glucoronic acis pathway
58

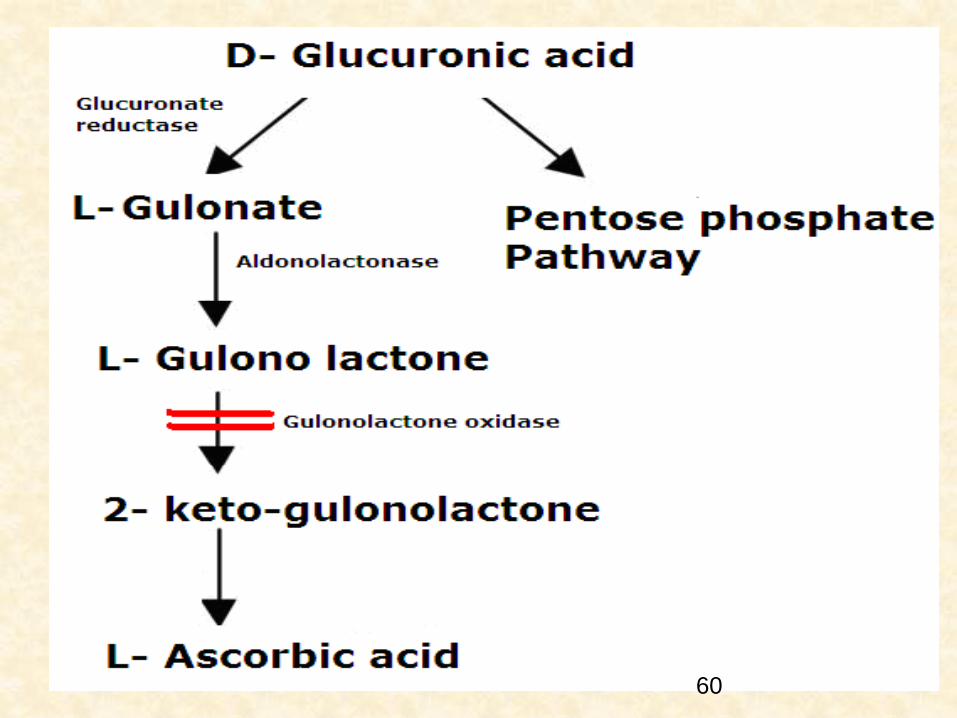
Alternative oxidative pathway for glucose.
synthesis of glucorinc acid,pentoses and vitamin (ascorbic acid).
Normal carbohydrate metabolism ,phosphate esters are involved – but in uronic acid pathway free sugars and sugar acids are involved.
Steps of reactions :
1) Formation of UDP-glucoronate
2) Conversion of UDP- glucoronate to L-gulonate
3) Synthesis of ascorbic acid in some animals
4) Oxidation of L-gulonate59
60

Clinical Aspects
• Effects of drugs : increases the pathway to achieve more synthesis of glucaronate from glucose .
- barbital,chloro-butanol etc.
• Essential pentosuria : deficiency of xylitol-dehydrogenase
- Rare genetic disorder
- Asymptomatic
- Excrete large amount of L-xylulose in urine
- No ill-effects61
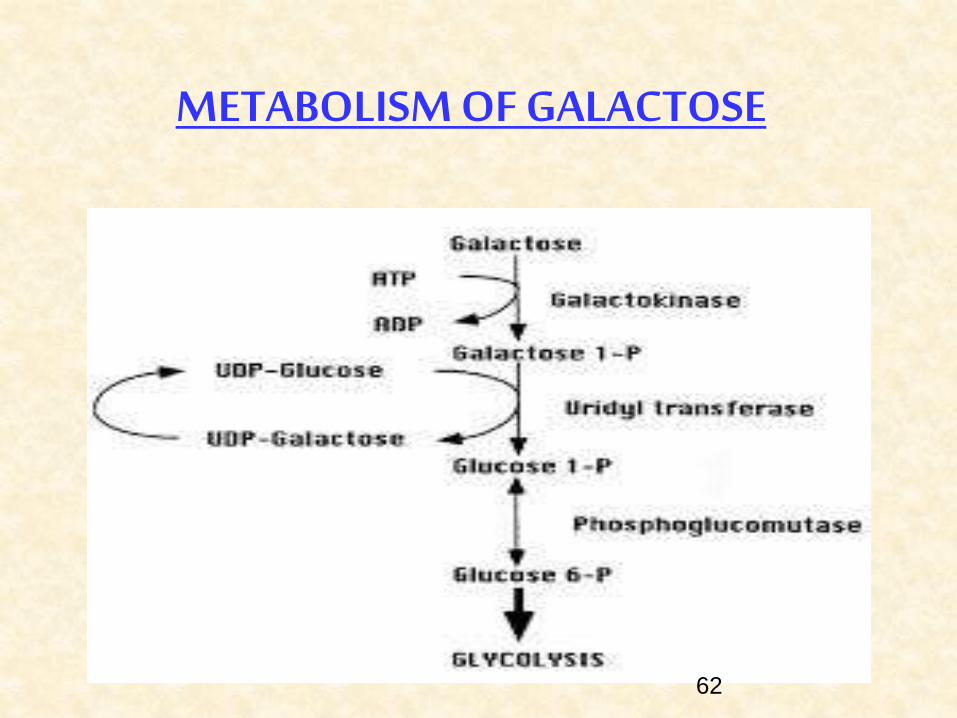
METABOLISM OF GALACTOSE
62

63
METABOLISM OF FRUCTOSE
64

METABOLISM OF AMINO SUGARS
65
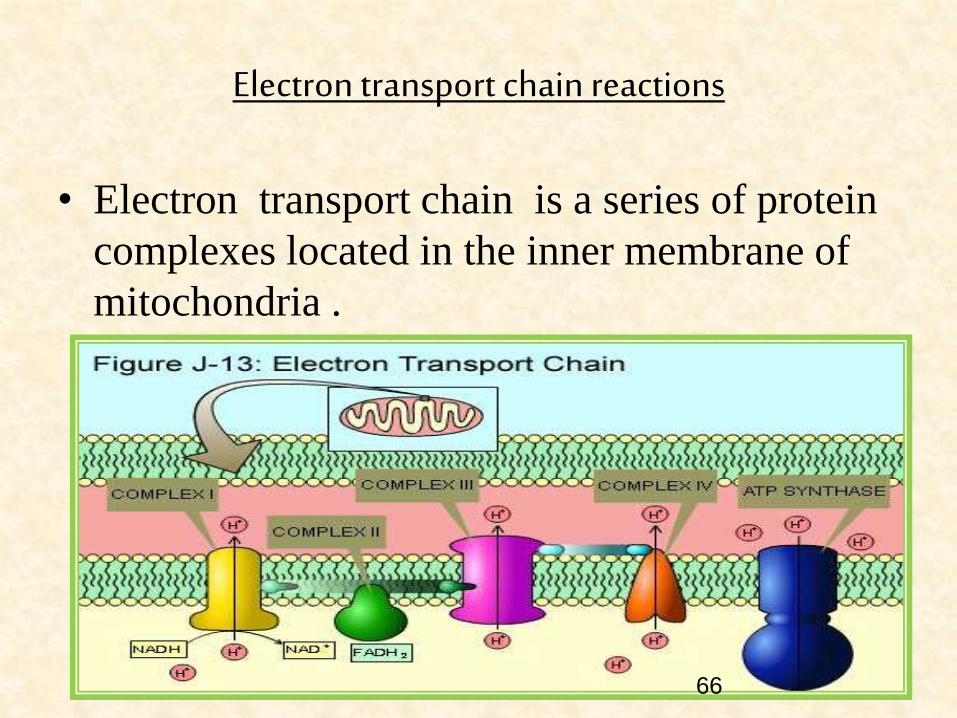
Electron transport chain reactions
• Electron transport chain is a series of protein
complexes located in the inner membrane of
mitochondria .
66

POLYSACCHARIDES&
CLINICAL ASPECTS
67

Proteoglycans & Glycosaminoglycans
Seven glycosaminoglycans :
1 ) Hyaluronic acid
2 ) Chondriotin sulfate
3 ) Keratan sulfate I
4 ) Keratan sulfate II
5 ) Heparin
6 ) Heparan sulfate
7 ) Dermatan sulfate
68

• Structural components of extracellular matrix.
• Act as sieves in extracellular matrix.
• Facilitate cell migration.
• Corneal transparency.
• Anticoagulant (Heparin).
• Components of synaptic & other vesicles.
Functions of glycoaminoglycans
69

MPS Defect Symptoms
MPS I (Hurler
syndrome)
Alpha-L-Iduronidase Mental retardation, micrognathia, coarse
facial features, macroglossia, retinal
degeneration,
corneal clouding, cardiomyopathy,
hepatosplenomegaly
MPS II (Hunter
syndrome)
Iduronate sulfatase Mental retardation (similar, but milder,
symptoms to MPS I). This type
exceptionally has X-linked
recessive inheritance
MPS IIIA
(Sanfilippo A)
Heparan sulfate N
sulfatase
Developmental delay, severe hyperactivity,
spasticity, motor dysfunction, death by the
second decade
MPS IIIB
(Sanfilippo B)
Alpha-
Acetylglucosaminidase
MPS IIIC
(Sanfilippo C)
Acetyl transferase
Mucopolysaccharidoses
70
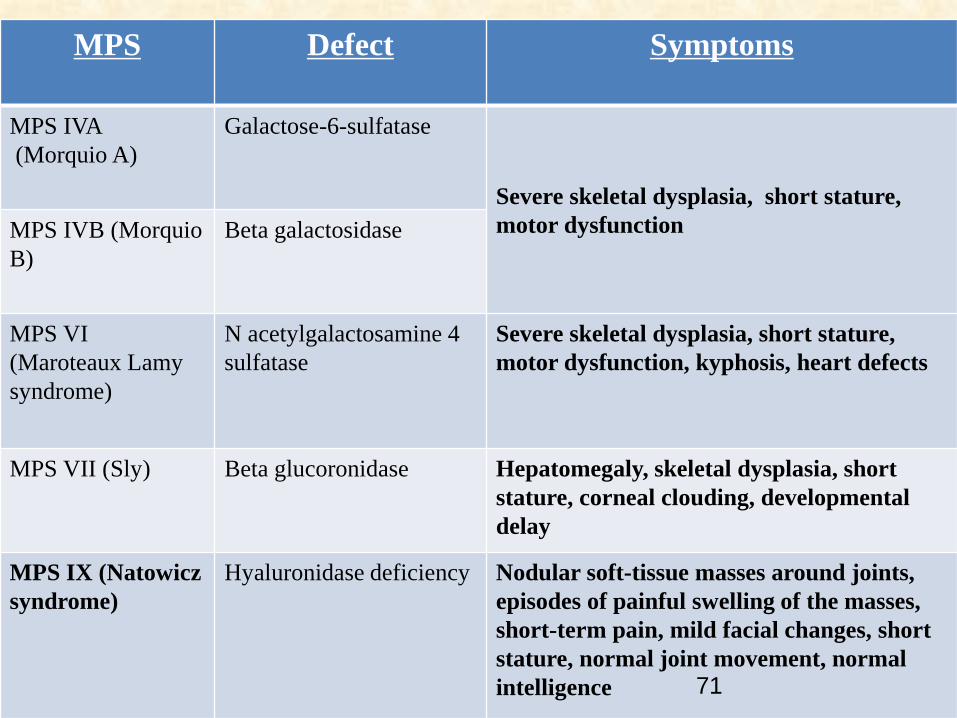
MPS Defect Symptoms
MPS IVA
(Morquio A)
Galactose-6-sulfatase
Severe skeletal dysplasia, short stature,
motor dysfunctionMPS IVB (Morquio
B)
Beta galactosidase
MPS VI
(Maroteaux Lamy
syndrome)
N acetylgalactosamine 4
sulfatase
Severe skeletal dysplasia, short stature,
motor dysfunction, kyphosis, heart defects
MPS VII (Sly) Beta glucoronidase Hepatomegaly, skeletal dysplasia, short
stature, corneal clouding, developmental
delay
MPS IX (Natowicz
syndrome)
Hyaluronidase deficiency Nodular soft-tissue masses around joints,
episodes of painful swelling of the masses,
short-term pain, mild facial changes, short
stature, normal joint movement, normal
intelligence 71

Hunter’s syndrome
72

ROLE OF HORMONES IN CARBOHYDRATE METABOLISM
73

• Postabsorptive state: Blood glucose is 4.5-
5.5mmol/L.
• After carbohydrate meal: 6.5-7.2mmol/L
• During fasting : 3.3-3.9mmol/L
Regulation of Blood glucose
74

Metabolic & hormonal mechanisms
regulate blood glucose level
Maintenance of stable levels of glucose in blood is by
Liver.
Extrahepatic tissues.
Hormones .
75
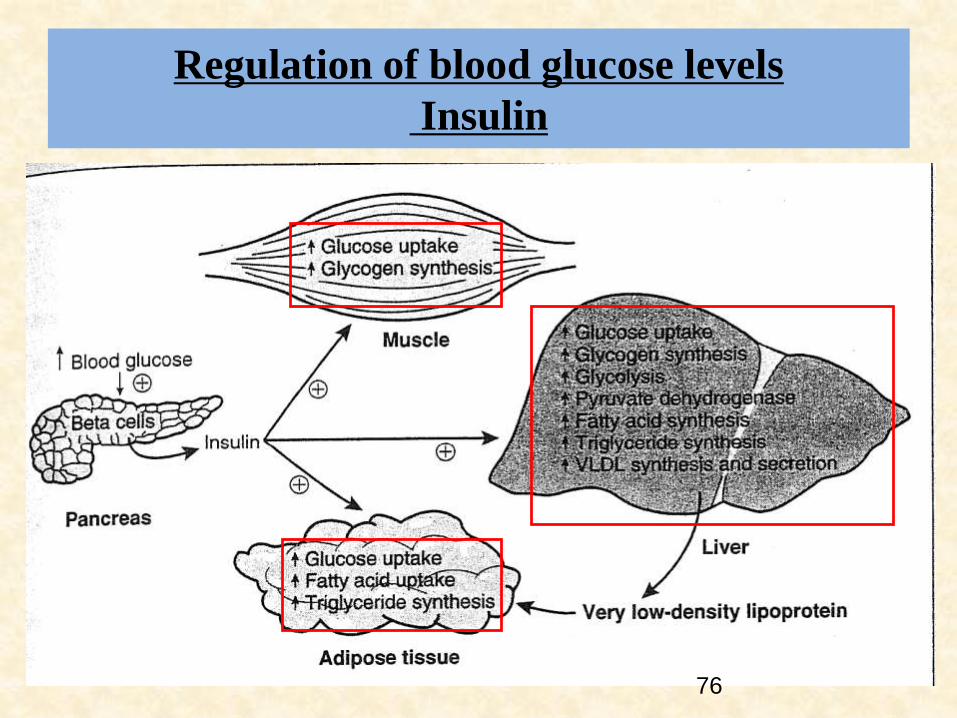
Regulation of blood glucose levels
Insulin
76

Role of glucagon
77

Role of thyroid hormone
It stimulates glycogenolysis & gluconeogenesis.
Hypothyroid
Fasting blood glucose
is lowered.
Patients have
decreased ability to
utilise glucose.
Patients are less
sensitive to insulin
than normal or
hyperthyroid
patients.
Hyperthyroid
Fasting blood
glucose is elevated
Patients utilise
glucose at normal
or increased rate
78

Glucocorticoids
Glucocorticoids are antagonistic to insulin.
Inhibit the utilisation of glucose in extrahepatic tissues.
Increased gluconeogenesis .
79
Epinephrine
Secreted by adrenal medulla.
It stimulates glycogenolysis in liver & muscle.
It diminishes the release of insulin from pancreas.
80

Other Hormones
Anterior pituitary hormones
Growth hormone:
Elevates blood glucose level & antagonizes action of insulin.
Growth hormone is stimulated by hypoglycemia (decreases
glucose uptake in tissues)
Chronic administration of growth hormone leads to diabetes
due to B cell exhaustion.
81

SEX HORMONES
Estrogens cause increased liberation of
insulin.
Testosterone decrease blood sugar level.
82
Hyperglycemia
Thirst, dry mouth
Polyuria
Tiredness, fatigue
Blurring of vision.
Nausea, headache,
Hyperphagia
Mood change
Hypoglycemia
Sweating
Trembling,pounding heart
Anxiety, hunger
Confusion, drowsiness
Speech difficulty
Incoordination.
Inability to concentrate
83

Clinical aspects
Glycosuria: occurs when venous blood
glucose concentration exceeds
9.5-10.0mmol/L
Fructose-1,6-Biphosphatase deficiency causes
lactic acidosis & hypoglycemia..
84

Diabetes Mellitus
A multi-organ catabolic response caused by insulin insufficiency
Muscle
– Protein catabolism for gluconeogenesis
Adipose tissue
– Lipolysis for fatty acid release
Liver
– Ketogenesis from fatty acid oxidation
– Gluconeogenesis from amino acids and glycerol
Kidney
– Ketonuria and cation excretion
– Renal ammoniagenesis.
85

DENTAL ASPECTS OF CARBOHYDRATES METABOLISM
86

Role of carbohydrates in dental caries
• Fermentable carbohydrates causes loss of
caries resistance.
• Caries process is an interplay between oral
bacteria, local carbohydrates & tooth surface
Bacteria + Sugars+ Teeth Organic acids
Caries
87

Role of carbohydrates in periodontal
disease
Abnormal
glucose metabolism
Diabetes Mellitus
Periodontal disease
Excessive carbohydrate
intake
Obesity
Periodontal disease
88

RECENT CLINICAL ISSUES RELATED TO CARBOHYDRATES METABOLISM
89

Cystic Fibrosis
• CMD in Cystic Fibrosis is characterized by its high rates and
latent course.
• The patients with CMD have retarded physical development,
more pronounced morphofunctional disorders in the
bronchopulmonary system, lower lung functional parameters,
and more aggressive sputum microbial composition.
(Samoĭlenko VA et al.)
90

CMD in Gout
• OGTT causes a 34% increase in the detection rate of T2D in
patients with gout.
• Carbohydrate metabolic disturbances are revealed in the
majority of patients with gout and associated with obesity,
hypertriglyceridemia, high serum UA levels, chronic disease
forms, the high incidence of CHD and arterial
hypertension.(Eliseev MS et al.)
91

SUMMARY OF CARBOHYDRATE METABOLISM
92

PER DAY INTAKE OF CARBOHYDRATE
• Carbohydrate Calculator
http://www.calculator.net/carbohydrate-
calculator.html?ctype=metric&cage=25&csex
=f&cheightfeet=5&cheightinch=10&cpound=
160&cheightmeter=163&ckg=74&cactivity=1.
375&x=85&y=10#
93
CONCLUSION
• Carbohydrate are the measure source of energy
for the living cells. Glucose is the central
molecule in carbohydrate metabolism, actively
participating in a number of metabolic pathway.
• One component of etiology of dental caries is
carbohydrate which act as substrate for
bacteria. Every effort should be made to
reduce sugar intake for healthy tooth.
94

REFERENCES
1) Biochemistry – U.Satyanarayana-3rd Ed.
2) Textbook of Biochemistry- D.M.Vasudevan -14th Ed.
3) Textbook of Medical Biochemistry – M.N.Chattergy
– 17th Ed.
4) Text book of Physiology –Ganong – 24th Ed.
5) Text book of Oral Pathology – Shafers- 7th Ed.
6) Principles & practice of Medicine-Davidson – 21st
Ed.
95

2015/1/3
• Submitted TO SIR JAVED
• Submitted by SANA DANISH
SUBAS IMTIAZ NAJAF BATOOL
Related Documents