Burn 5 th Lecture EFFECT OF PRESSURE ON HYPERTROPHIC SCARS AND KELOID

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Burn 5th Lecture
EFFECT OF PRESSURE ON
HYPERTROPHIC SCARS AND KELOID
EFFECT OF PRESSURE ON
HYPERTROPHIC SCARS AND KELOID
EFFECT OF PRESSURE ON HYPERTROPHIC SCARS AND KELOID• Keloid remains a problem for surgeons, topical and
intralesional corticosteroids positive pressure dressings, and laser therapy are helpful but not uniformly successful.
• Hypertrophic scars (HS) commonly attend burns.• It may also develop after surgical incision or other trauma
that extend into the reticular dermis.• Hypertrophic scar may be partial or complete resolution or
may be remain permanently.• This complication is severe and causes much functional,
cosmetic and psychological morbidity.• Hypertrophic scar is an over growth of dermal constituents
that remains within the boundaries of the wound. Or it is raised car that stays within the boundaries of the burn wound & it is characterized by being red, raised and rigid .
• Keloid is a scar that extends beyond the boundaries of the original wound or raised scar that extend the boundaries of the original burn wound.
• Trauma of various origins can induce a connective tissue disorder that leads to Keloids. This condition has yet not been clearly distinguished from scars and hypertrophic scars.
Only electromicroscopic and biochemical data can help to do this.
• The use of silicon (Polydime - Thylsiloxan) Plates as mechanical pressure, wrapped on the keloid surface, has been reported effective by some authors.
Keloid compared with hypertrophic scarsHypertrophic scars are often mistakenly
referred to as Keloid(s). However, they have several characteristics which differentiate them. Keloid scars are described as thick scar tissue of the human skin that are produced by excessive amounts of collagen deposited over prolonged periods. They develop gradually following even small skin wounds and are accompanied by itchiness or pruritus.
Keloid scars also differ significantly from hyper-trophied scars in that the latter will spontaneously soften and flatten with time, whereas keloid scars can remain elevated indefinitely (Tortura, 1993).
Characteristics of scarIn normal epidermal healing:
• The skin is replaced with minimal discrepancies (change) in the original texture, color surface, and height.
• The epidermis does not thicken and therefore does not contribute to the height of scar.
• If a burn injury extends into the dermis the skin repair through the scar formation. Keloid represents the most severe degree of U.S.
H.S. development
(1) If an injury extends into the deep reticular layer of the dermis as in the case of deep partial thickness burn.
(2) Or if there is delayed wound healing of greater than 3 week.
(3) When full thickness burns have healed by re -epithilization, granulation tissue formation.
(4) When donor sites have been re-harvest (cut) too deeply, rehavest several time donor site
(5) Delayed healing due to infection or trauma.N.B.: Hypertrophic scar usually don't occur in burned
areas that have been repaired with split thickness or full thickness skin grafts.
Causes of hypertrophic scar1. Prolonged healing time.2. Granulation tissue.3. Increase blood flow.4. Chronic inflammatory process.5. Trapped foreign material.6. Infection.7. Increase serum protein.8. Increase proline hydroxylase.9. Mast cell degranulation.10.Myofibroblast.11.Mechanical tissue deformity.12.Repeated harvesting of donor sites.13.Immunologic factor
Factor affecting scar formation:1. Age
Studies revealed that age was not a predictor of hypertrophic scarring. But clinical studies show that younger people scare more than older people. This may be due to the fact that younger people are more susceptible trauma, have greater skin tension and the rate of collagen synthesis is greater in this group.
2. LocationCertain areas of the body appear more predisposed to the
formation of hypertrophic scars. These are mostly involved are the sternum, upper back and shoulder, buttocks and dorsal aspect of the foot.
3. DepthDeeper bums, which involve the reticular dermis, scar
more than superficial burns that involve only the epidermis or the
papillary dermis, due to the formation of granulation tissue and prolonged healing time.
4.Gender It got no relation with scarring. Other predisposing factors.
5.Areas6.Excessive motion of the skin grafts edges during
healing.7. Persistent presence of necrotic tissue.
Pressure therapy• The application of mechanical pressure is the
standard treatment used to minimize the effect of hypertrophic scarring.
• Many researchers have stated that approximately 25 mmHg capillary pressure is necessary to produce change in scar tissue, but this value has not been proven absolute.
• Scars treated with pressure greater than 15 mmHg have been noted to be flatter, smoother and less erythematous than scars treated with lower pressure. However accelerated remodeling may occur with pressures less than 10 mmHg.
• At pressures greater than 40 mmHg. maceration and paraesthesia may occur.
N.B.1. Special air flow measuring manometer to measure
garment scar interface pressure on patients.2. Pressure garments can be applied as soon as a wound
has healed.3. Reported benefits of silicone gel pressure pads
including Increase of range of motion.Minimizing pain.Preventing shrinkage of skin grafts.Minimizing hypertrophic scarring.Assisting with softening and smoothing of scars. Increase of pressure over movable areas where
pressure is difficult to maintain.So, silicon gel pressure is effective in the
reduction of evolving keloid.
Several factors have to be born in mind when selecting which type of garment you will make.
1. In order to exert adequate pressure over a scar site, garments should extend 5 cm above and below the scar site(s).
2. Garments should not cause or contribute to oedema. Where oedema is or could become a problem garments should be extended to the distal end of limbs.
3. Pressure garments because they are close fitting are susceptible to rolling when the patient moves.
4. The amount of pressure exerted by garments is related to the degree of curvature of the underlying body parts.
5. When scars are very lumpy or have thick ridges on them. The pressure exerted by a garment will not reach the dips or troughs between these ridges.
• How pressure is applied (Procedure)
1.Custom made pressure garment were approximately 60% porous, therefore sunscreen was used in conjunction with them if patient would be out in the sun for any period of time.
2.The pressure garments used were a combination of nylon and spanned material that is compatible with all moisturizing creams.
3.Change of garments was done every 12 hours and careful cleaning of the garments to prolong the life of the garments.
Tips for proper use of pressure garmentts Wearing1. Rub moisturizing cream completely into the skin to
minimize build-up in garment.2. Do not over stretch garment when applying or
removing.3. Wear socks over the garment when garment cover
feet.Washing1. Wash garment daily to avoid build up of bodily oil &
moisturizing cream. 2. Soak the garment one hour before washing. Drying• Do not use heat.
Complications of pressure therapyPressure therapy is not without its
complications. Those known include swelling blistering and an adverse effect on growing children. As human tissue is viscoelastic it will become deformed after sustained pressure. Biomechanical principles need to be considered when playing pressure to preserve the body's natural contours, i.e. convexities and concavities like the metacarpal arch and the transverse diameter of the thoracic cage. Padding can be used under garments to fill concavities so that the surface diameter is decreased, and a more even distribution of pressure is encouraged (Leung et al., 1984).
Table (6): Hypothetical Effects of Compression Therapy on Burn Scar.
1. Accelerates the scar maturation process2. Superficial blanching3. Flattening of the scar4. Increased pliability5. Decreased blood flow6. Decreased edema7. Decreased rate of collagen synthesis8. Collagen bundles realign parallel to epidermal surface9. Absent or less prominent nodules10.Decreased cohesiveness of intercollagen fibers11.Increased collagenase-mediated collagen breakdown12.Gradual decrease in myofibroblasts13.Stabilization and gradual decrease in mast cells14.Decreased deposition and change in ground substance15.Thinning of dermis
Pressure Therapy: The tensile strength of a wound depends on
collagen synthesis and remodeling within the wound area (Ahn et al, 1989 and Baum & Busuito, 1998). Hypertrophic scar is a term used to describe an overabundance of collagen and other extracellular matrix components within the margins of the original wound. The physical properties of scar give the therapist an indication of the biologic activity of the wound and are responsible for the functional and cosmetic problems a therapist must treat. According to Leung (1989) hypertrophic scars can be graded on vascularity, rigidity, elasticity, and height
The undesirable features of hypertrophic scars may not become noticeable until weeks or months following wound closure. Skin tightness from wound contracture and hypertrophic scar ring peaks between 3 and 6 months post injury (Schwanholt et al, 1994). The volume of the scar may continue to increase in size before undergoing spontaneous remodelling, in which the scar flattens and softens, but usually to an incomplete extent. The length of time to wound closure is generally considered to be the best predictor in determining the potential for and severity of scarring.
Ahn et al, (1989) noticed that wounds spontaneously closed within 2 weeks have reduced potential for hypertrophic scar formation. For wounds taking between 2 and 3 weeks to heal, it becomes more the discretion of the physician and therapist whether to begin treatment for potential hypertrophic scar formation. Factors such as age, race, and location of scar may affect the decision (Baum & Busuito, 1998).
Johnson et al, (1994) stated that pressure therapy for a grafted area of hand may be initiated 5 to 6 days postoperatively. Hand tracings may be transferred onto tubular compression bandage material used as a glove or a prefabricated, commercially available glove may be provided. Tenuous skin grafts with open areas may be left longer but gentle compression may be initiated over wound dressings, applied using compressive wraps that avoid shear forces with application and removal (Kealey, 1990, Chick et al, 1992 and Mann et al, 1997).
In addition to treating scars of hand, pressure garments can also used for treating scars, pressure garments can also decrease itching; protect the newly healed, fragile skin; and aid in circulation by preventing venous congestion (Kealey, 1990 and Ward, 1991).
Bielcy & Berman, (1996) and Wendy et al., (2000) noticed that gel sheets are used effectively for hand burn as adjuncts to pressure therapy in scar management. They are useful in treating small burn areas or to fill spaces where pressure garments cannot reach. Gel sheeting can be used with and without pressure to soften and flatten scars. Many types of gel sheeting are available, with various levels of durability thickness, size, and adhesiveness.
The mechanisms by which pressure and gel sheeting work to control hypertrophic scars are not completely understood. Pressure decreases blood flow to the scar, which may reduce fibroblast and collagen synthesis. Pressure may also help collagen bundles, realign parallel to the epidermal surface. Increases in skin temperature that garments and inserts, may facilitate increased collagenase activity (Kealey, 1990, Ward, 1991, Bieley & Berman, 1996 and Wendy et al, 2000).
Assessment of scar
Researchers are using several methods to determine the state of scar maturation, although some techniques lend themselves better to the research environment than to the clinical setting. Esposito (1990) has used a (1) Modified tonometer to measure skin tone, which correlates to skin pliability and tension. Results from this work produced a firmness index (Fl), which is zero in normal skin and increases with the firmness of scar. This study compared a subjective clinical rating to the Fl, which may assist the investigators in design of an (2) Electronic tonometer to quickly and accurately calculate average scar tension values (Katz, 1985).
Katz (1985) appeared to have greater success when he compared scar thickness, determined by (3) High-resolution ultrasonic scanning, with firmness and flexibility of a scar, as measured by a tonometer. Decreased skin thickness correlated with decreased tension within the scar change over time, but he was unable to compare cue site to another or different individuals to each other. Also,Katz felt the ultrasonic scanning method was better suited for research, while the tonometer was more useful in the clinic.
(4)The elastometer, a hand-held non-invasive device that quantifies the elastic properties of normal skin or hypertrophic scar, has been used by Bartell and colleagues (1988). The device detects differences in elasticity between normal skin and hypertrophic scars and yields reproducible results. As scars matured, their elasticity increased. By measuring the elasticity of scars overtime, the effectiveness of a scar management program could be monitored. This study also showed that some scars improved over time even if left untreated.
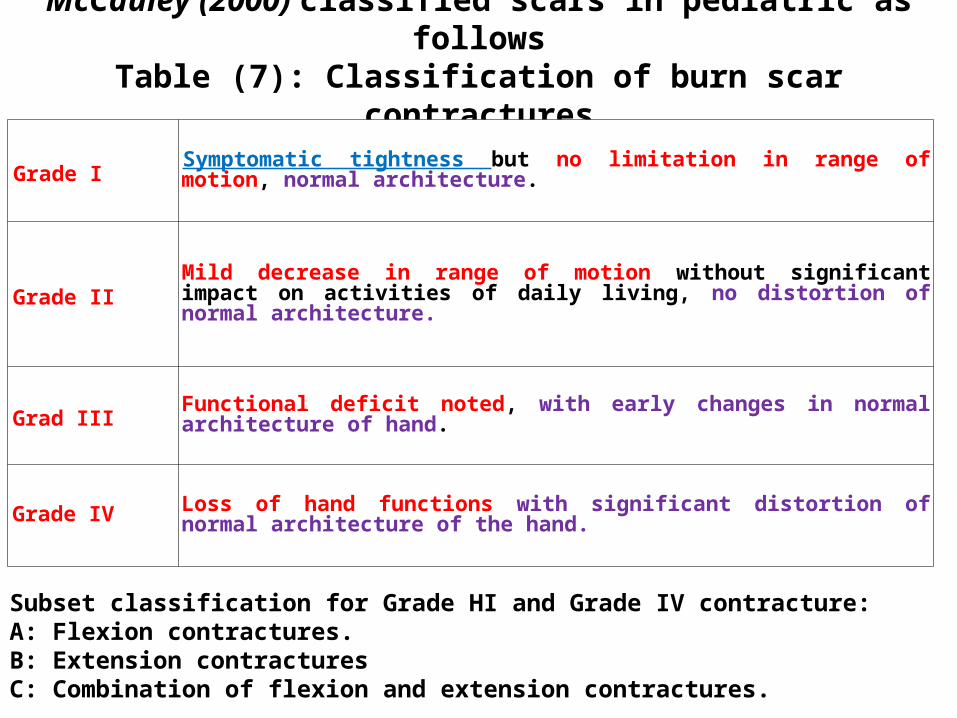
McCauley (2000) classified scars in pediatric as followsTable (7): Classification of burn scar contractures
Grade I Symptomatic tightness but no limitation in range of motion, normal architecture.
Grade IIMild decrease in range of motion without significant impact on activities of daily living, no distortion of normal architecture.
Grad III Functional deficit noted, with early changes in normal architecture of hand.
Grade IV Loss of hand functions with significant distortion of normal architecture of the hand.
Subset classification for Grade HI and Grade IV contracture:A: Flexion contractures.B: Extension contracturesC: Combination of flexion and extension contractures.
(5) A rating scale for assessing scar maturation was developed by Sullivan (1990). The scale consists of rating four burn scar characteristics: pigmentation, vascularity, pliability, and height. In general, the higher the total score the more immature or active the scar. As a scar becomes more mature or inactive, the scores return to zero. The rating scale is a rather subjective means of evaluating burn scar, but can be a useful clinical tool, especially for monitoring outpatient progress toward scar maturity. Hosoda et al, (1986) reported that early detection of hypertrophic burn scar could be done using (6) Laser Doppler fiowmetry.
Related Documents











