
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
2
Aims and objectives
• Why is haematology so difficult?
• Classification of anaemias
• Duration: 70 mins
• Slides and recordings: app.bitemedicine.com

History and examination
A 20-year-old lady presents to the GP with lethargy.
She is a medical student and complains of intense
fatigue, struggling to stay awake during lectures. As
soon as she gets home, she goes straight to bed.
She reveals that she often has heavy periods.
Observations
HR 80, BP 118/77, RR 18, SpO2 98%, Temp 37.0
3
Case-based discussion: 1

4
A 20-year-old lady presents to the GP with lethargy. She is a medical student and
complains of intense fatigue, struggling to stay awake during lectures. As soon
as she gets home, she goes straight to bed.
She reveals that she often has heavy periods.
Observations: HR 80, BP 118/77, RR 18, SpO2 98%, Temp 37.0
Which of the following is the most likely type of anaemia?
Question 1
Microcytic
Normocytic
Macrocytic
Megaloblastic
Aplastic
app.bitemedicine.com
Q3 Q4 Q5Q1 Q2

5
Explanations
app.bitemedicine.com
Which of the following is the most likely type of anaemia?
Microcytic
Chronic blood loss, e.g. menstrual bleeding, leads to iron deficiency and is the commonest cause
of anaemia worldwide
Normocytic
Iron deficiency is microcytic
Macrocytic
Iron deficiency is microcytic
Megaloblastic
This is a subtype of macrocytic anaemia
Aplastic
This is a cause of a normocytic anaemia and may occur secondary to infection e.g. parvovirus B19
Q3 Q4 Q5Q1 Q2
6
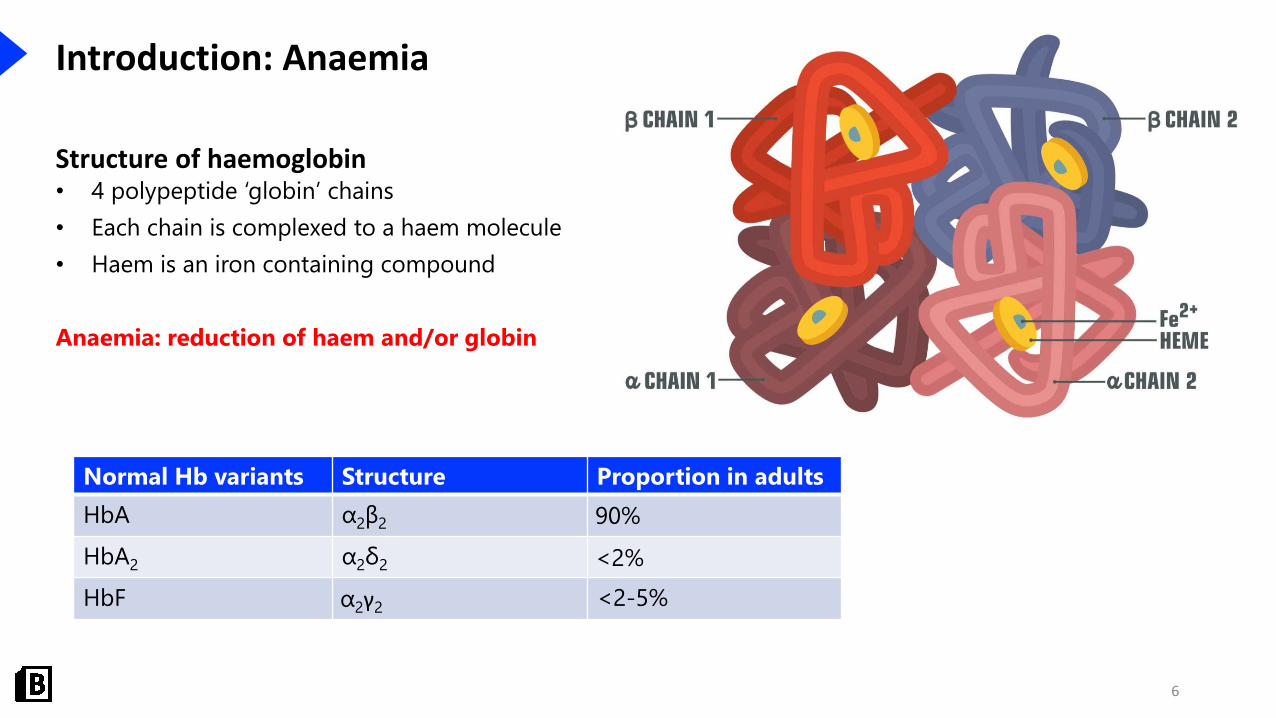
Introduction: Anaemia
Structure of haemoglobin• 4 polypeptide ‘globin’ chains
• Each chain is complexed to a haem molecule
• Haem is an iron containing compound
Anaemia: reduction of haem and/or globin
Normal Hb variants Structure Proportion in adults
HbA α2β2 90%
HbA2 α2δ2 <2%
HbF α2γ2 <2-5%

7
Introduction: Anaemia
Anaemia• Men: Hb <130g/L
• Women: Hb <120g/L
• Classified based on mean corpuscular volume (MCV)
Microcytic (MCV < 80fL) Normocytic (MCV 80-95fL) Macrocytic (MCV >95fL)
Iron deficiency Acute blood loss B12 deficiency
Thalassaemia Haemolytic anaemia Folate deficiency
Anaemia of chronic disease Anaemia of chronic disease Alcohol
Sideroblastic anaemia Chronic kidney disease Liver disease
Aplastic anaemia Hypothyroidism

8
Clinical features: General principles
Symptoms Signs
Fatigue Tachycardia
SOB on exertion Tachypnoea
Chest pain Hypotension
Palpitations Pallor

9
History taking: General principles
History of presenting complaint
• Symptoms of anaemia e.g. SOB
• Screen for areas of blood loss: GI, resp, urinary tract, menstrual
• Alarm symptoms: weight loss, loss of appetite, night sweats, lymphadenopathy
• Dietary habit
Past medical history
• Chronic disease
• Trauma
Family history
• Inherited disorders e.g. haemoglobinopathies
Drug history, social history

10
Investigations: General principles
Bedside• Full set of observations
Bloods• FBC: reduced Hb. Assess MCV
• Blood film
• Iron studies
• B12 and folate levels
• Haemolysis screen: bilirubin, haptoglobin, Coombs test
• U&Es: CKD
• TFTs: hypothyroidism
• LFTs: chronic liver disease
Imaging• Assess for site of blood loss
Special tests• Bone marrow biopsy
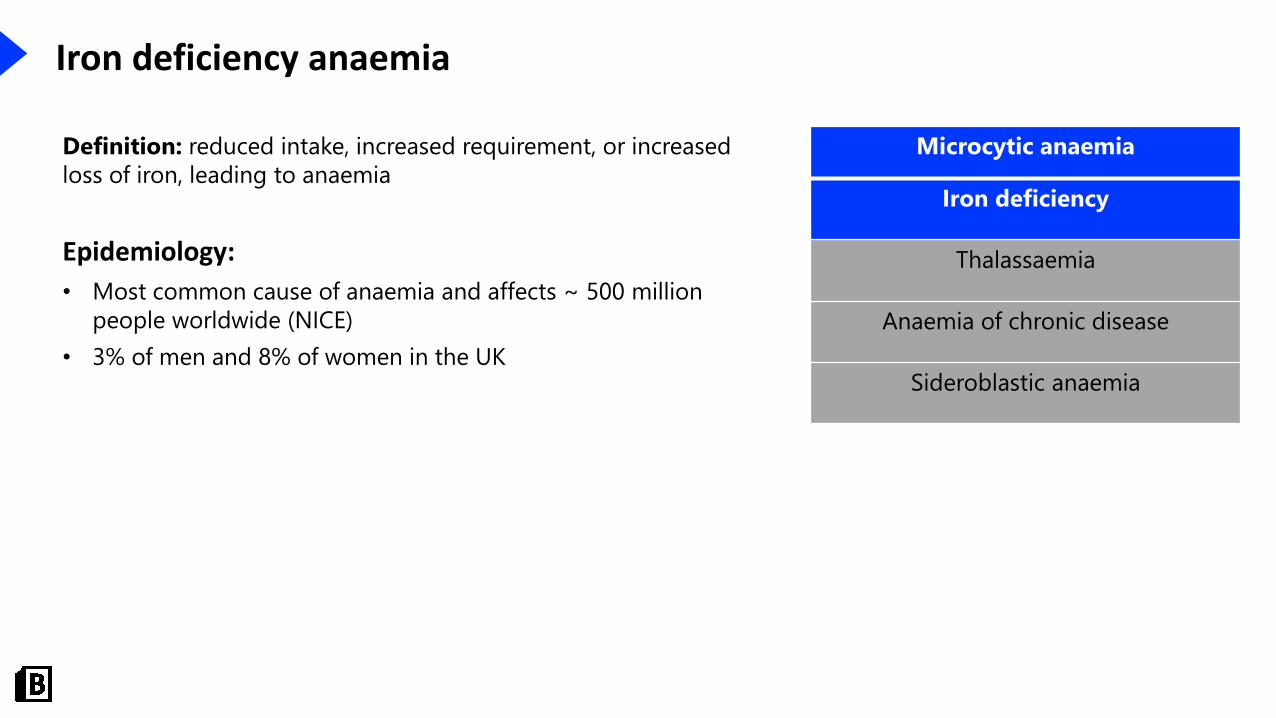
Iron deficiency anaemia
Microcytic anaemia
Iron deficiency
Thalassaemia
Anaemia of chronic disease
Sideroblastic anaemia
Definition: reduced intake, increased requirement, or increased
loss of iron, leading to anaemia
Epidemiology:
• Most common cause of anaemia and affects ~ 500 million
people worldwide (NICE)
• 3% of men and 8% of women in the UK
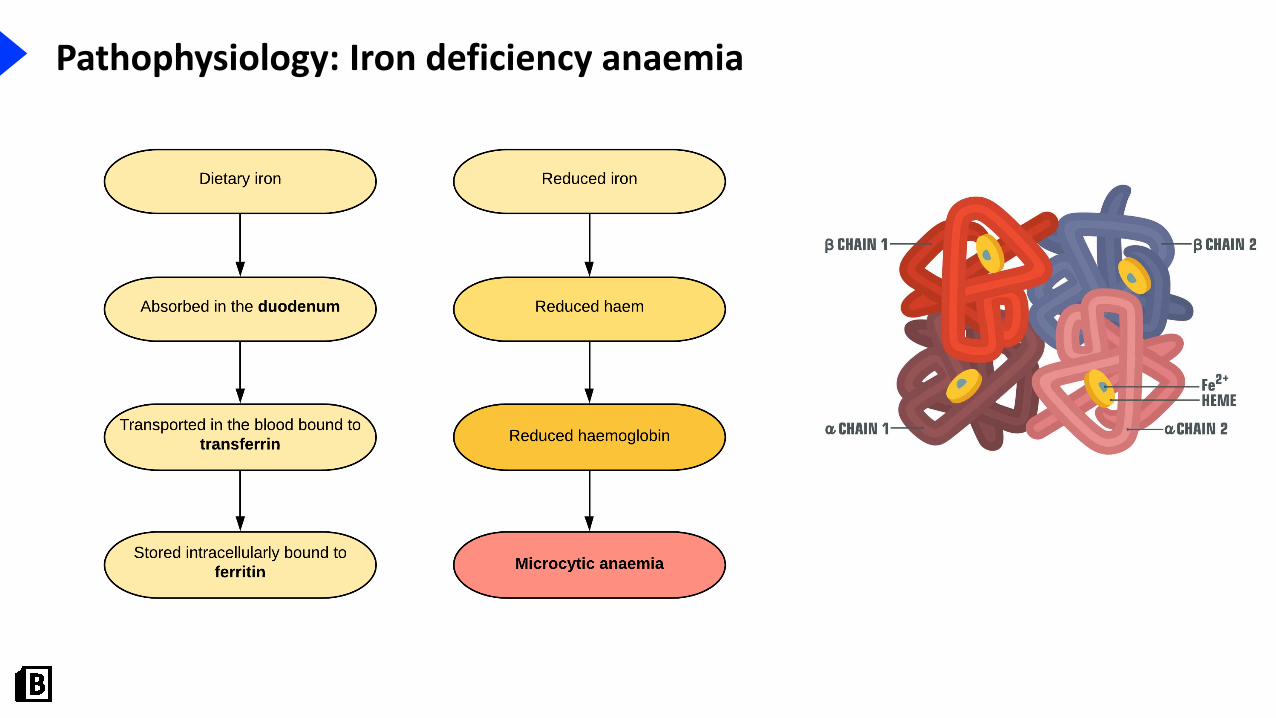
Pathophysiology: Iron deficiency anaemia
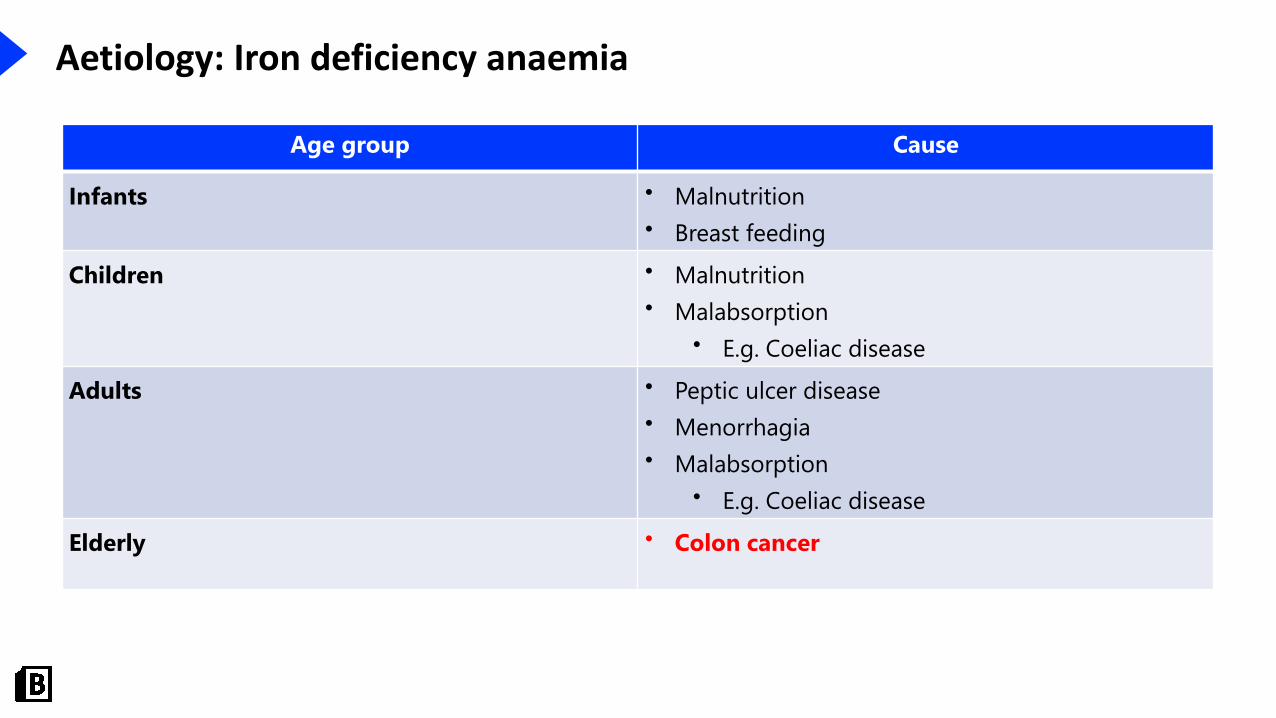
Aetiology: Iron deficiency anaemia
Age group Cause
Infants • Malnutrition
• Breast feeding
Children • Malnutrition
• Malabsorption
• E.g. Coeliac disease
Adults • Peptic ulcer disease
• Menorrhagia
• Malabsorption
• E.g. Coeliac disease
Elderly • Colon cancer
14
You confirm a microcytic anaemia. Which of the following tests should be conducted next if you
suspect iron deficiency?
Question 2
Serum iron
Transferrin
Ferritin
Total iron binding capacity
Urinary iron
app.bitemedicine.com
Q3 Q4 Q5Q2Q1
A 20-year-old lady presents to the GP with lethargy. She is a medical student and
complains of intense fatigue, struggling to stay awake during lectures. As soon
as she gets home, she goes straight to bed.
She reveals that she often has heavy periods.
Observations: HR 80, BP 118/77, RR 18, SpO2 98%, Temp 37.0
15
Explanations
app.bitemedicine.com
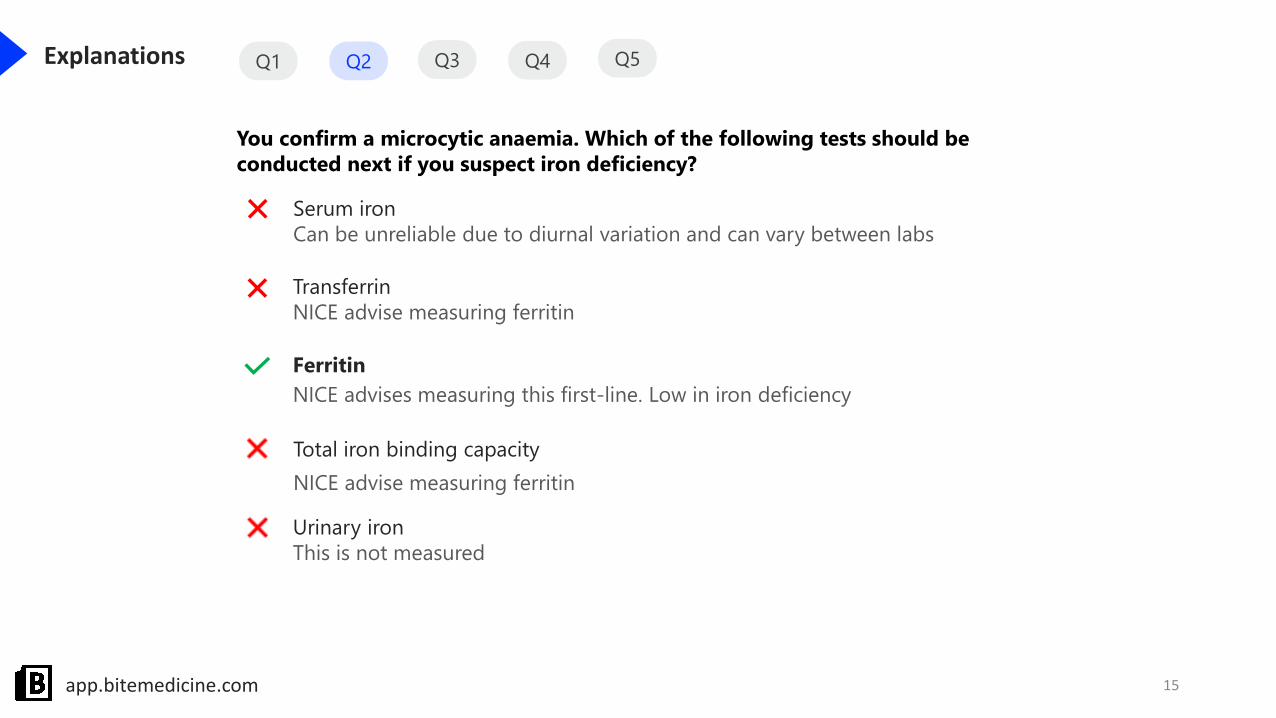
You confirm a microcytic anaemia. Which of the following tests should be
conducted next if you suspect iron deficiency?
Serum iron
Can be unreliable due to diurnal variation and can vary between labs
Transferrin
NICE advise measuring ferritin
Ferritin
NICE advises measuring this first-line. Low in iron deficiency
Total iron binding capacity
NICE advise measuring ferritin
Urinary iron
This is not measured
Q3 Q4 Q5Q2Q1

Aetiology: Iron deficiency anaemia
Cause
Reduced intake • Malnutrition
• Breastfeeding
• Malabsorption
• Coeliac disease
Increased requirement • Pregnancy
Increased loss • Chronic bleeding
• Colon cancer
• Menorrhagia
• Peptic ulcer disease

Clinical features: Iron deficiency anaemia
Features
Glossitis
Angular stomatitis/chelitis
Koilonychia
Pica
(1)
(2)

18
Q2
Which of the following is true for a patient with iron deficiency anaemia?
Question 3
Treat with blood transfusion
Treat with intravenous iron
Arrange urgent upper GI endoscopy if ≥50
Arrange urgent colonoscopy if ≥60
Arrange urgent colonoscopy if ≥65
app.bitemedicine.com
Q3Q1 Q4 Q5
A 20-year-old lady presents to the GP with lethargy. She is a medical student and
complains of intense fatigue, struggling to stay awake during lectures. As soon
as she gets home, she goes straight to bed.
She reveals that she often has heavy periods.
Observations: HR 80, BP 118/77, RR 18, SpO2 98%, Temp 37.0

19
Explanations
app.bitemedicine.com
Which of the following is true for a patient with iron deficiency anaemia?
Treat with blood transfusion
Oral iron is first line
Treat with intravenous iron
Oral iron is first line. IV iron can be used if oral therapy not tolerated
Arrange urgent upper GI endoscopy if ≥50
Not indicated unless suspecting an upper GI bleed in any age group
Arrange urgent colonoscopy if ≥60
As per NICE guidelines
Arrange urgent colonoscopy if ≥65
NICE suggest ≥60
Q2 Q3Q1 Q4 Q5

20
Investigations: Iron deficiency anaemia
Bloods• FBC: microcytic anaemia (MCV <80fL)
• Blood film: hypochromic red cells, target cells
• Iron studies
• Ferritin: reduced
• Serum iron: reduced
• TIBC: increased
• Transferrin saturation: decreased
Imaging • Endoscopy
• Suspecting upper GI bleed
• ≥60 years old with iron deficiency anaemia
Special tests• Coeliac serology

21
Management: Iron deficiency anaemia
Address the underlying cause
Oral iron replacement
• Ferrous sulphate or ferrous fumarate
• Monitor Hb 2-4 weeks after starting and then at 2-4 months
• Treatment should continue for 3 months after anaemia corrected
Intravenous iron replacement
• Not responding or intolerant to oral therapy
• Malabsorption
• Renal failure
Blood transfusion
• Hb <70g/L or
• Hb <80g/L and cardiac co-morbidity

History and examination
A 1-year-old child is brought to the GP as his mother
is concerned he is not gaining weight. He is dropping
off the centiles on his growth chart.
On examination he appears pale and has evidence of
hepatosplenomegaly. His forehead looks prominent.
Further investigations reveal a diagnosis of beta
thalassaemia major.
22
Case-based discussion: 2
(3)

23
Which of the following would you expect to see on haemoglobin electrophoresis in this
patient?
Question 1
Raised HbH
Raised HbA
Raised HbA2
Reduced HbF
HbS
app.bitemedicine.com
A 1-year-old child is brought to the GP as his mother is concerned he is not
gaining weight. He is dropping off the centiles on his growth chart.
On examination he appears pale and has evidence of hepatosplenomegaly. His
forehead looks prominent.
Further investigations reveal a diagnosis of beta Thalassaemia major.
Q1 Q2

24
Question 1
app.bitemedicine.com
Which of the following would you expect to see on haemoglobin electrophoresis?
Raised HbH
Associated with alpha thalassaemia
Raised HbA
Reduced in beta thalassaemia
Raised HbA2
Raised along with HbF
Reduced HbF
Should be raised
HbS
Associated with sickle cell disease
Q1 Q2

Introduction: Thalassaemia
Microcytic anaemia
Iron deficiency
Thalassaemia
Anaemia of chronic disease
Sideroblastic anaemia
Definition: autosomal recessive haemoglobinopathy
• Impaired globin chain synthesis
Epidemiology:
• Prevalent in areas of malaria
• Alpha thalassaemia: Asian and African
• Beta thalassaemia: Asian, Mediterranean and Middle Eastern
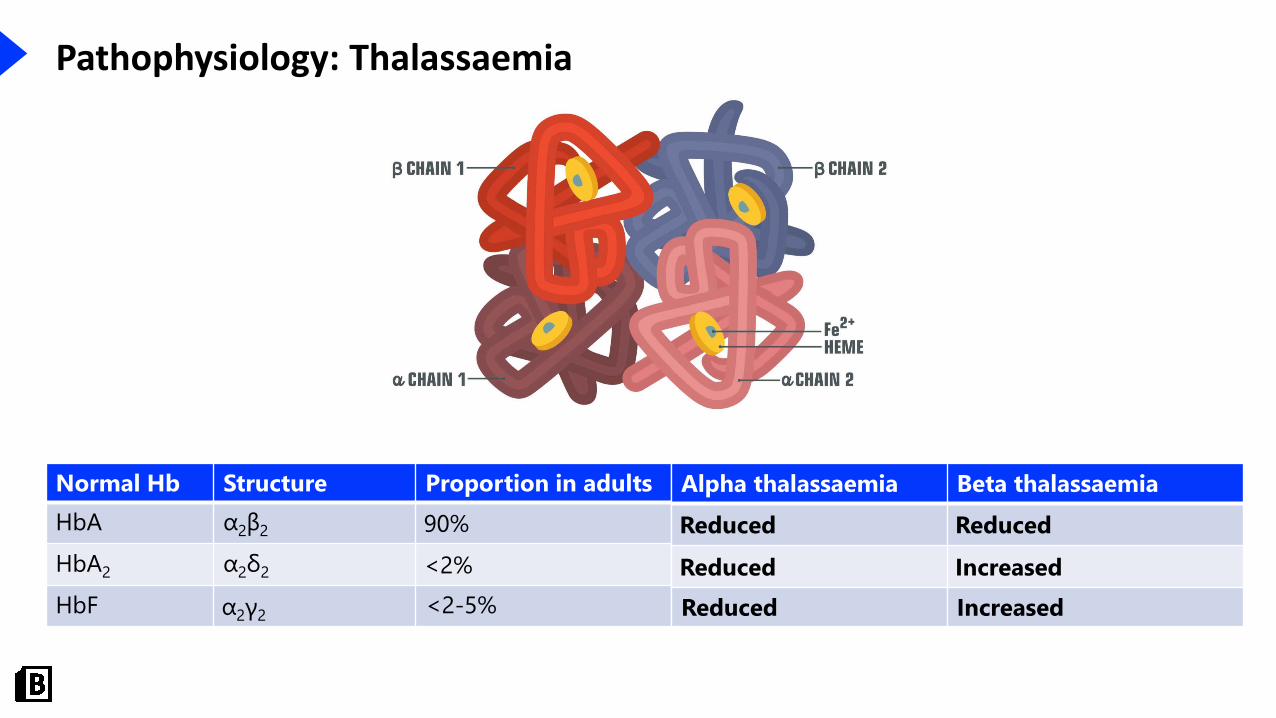
Pathophysiology: Thalassaemia
Normal Hb Structure Proportion in adults
HbA α2β2 90%
HbA2 α2δ2 <2%
HbF α2γ2<2-5%
Alpha thalassaemia Beta thalassaemia
Reduced Reduced
Reduced Increased
Reduced Increased

Pathophysiology: Alpha Thalassaemia
Impaired synthesis of alpha globin
• 4 alleles on chromosome 16 are responsible for alpha globin production
• Gene deletions
Disease No. of
deletions
HbA
(α2β2)
HbA2
(α2δ2)
HbF
(α2γ2)
Features
Silent
carrier
1 N N N Asymptomatic
Trait 2 ↓ ↓ ↓ Mild anaemia
HbH 3↓↓ ↓↓ ↓↓
Beta chains form tetramers
Marked anaemia
Hb Barts 4
Absent Absent Absent
Gamma chains form tetramers
Hydrops fetalis
Death in utero

Pathophysiology: Beta Thalassaemia
Impaired synthesis of beta globin
• 2 alleles on chromosome 11 are responsible for beta globin production
• Gene mutations
• Reduced production (β+)
• Absent production (β0)
Disease Genetics HbA
(α2β2)
HbA2
(α2δ2)
HbF
(α2γ2)
Features
Trait β/β+ ↓ ↑ ↑Asymptomatic or mild symptoms
Intermedia β+/β+
β+/β0
Variable Variable Variable
Variable
Major β0/β0 Absent ↑↑ ↑↑Marked anaemia

29
Which of the following is the cause of his prominent forehead?
Question 2
Trauma
Cortical thickening
Normal variant
Bone marrow expansion
Osteomyelitis
app.bitemedicine.com
A 1-year-old child is brought to the GP as his mother is concerned he is not
gaining weight. He is dropping off the centiles on his growth chart.
On examination he appears pale and has evidence of hepatosplenomegaly. His
forehead looks prominent.
Further investigations reveal a diagnosis of beta Thalassaemia major.
Q2Q1

30
Explanations
app.bitemedicine.com
Which of the following is the cause of his prominent forehead?
Trauma
No evidence of trauma
Cortical thickening
It’s an issue with the marrow, not the cortex
Normal variant
Not normal as the patient has thalassaemia
Bone marrow expansion
Compensatory bone marrow expansion in sites away from the long bones occurs, causing
frontal bossing and prominent zygomatic bones
Osteomyelitis
We would not expect this in thalassaemia, nor would we expect it to occur in the frontal bone
Q2Q1

31
Clinical features: Thalassaemia
Signs
Neonatal jaundice
Hepatosplenomegaly
Failure to thrive
Chipmunk facies
(3)
32
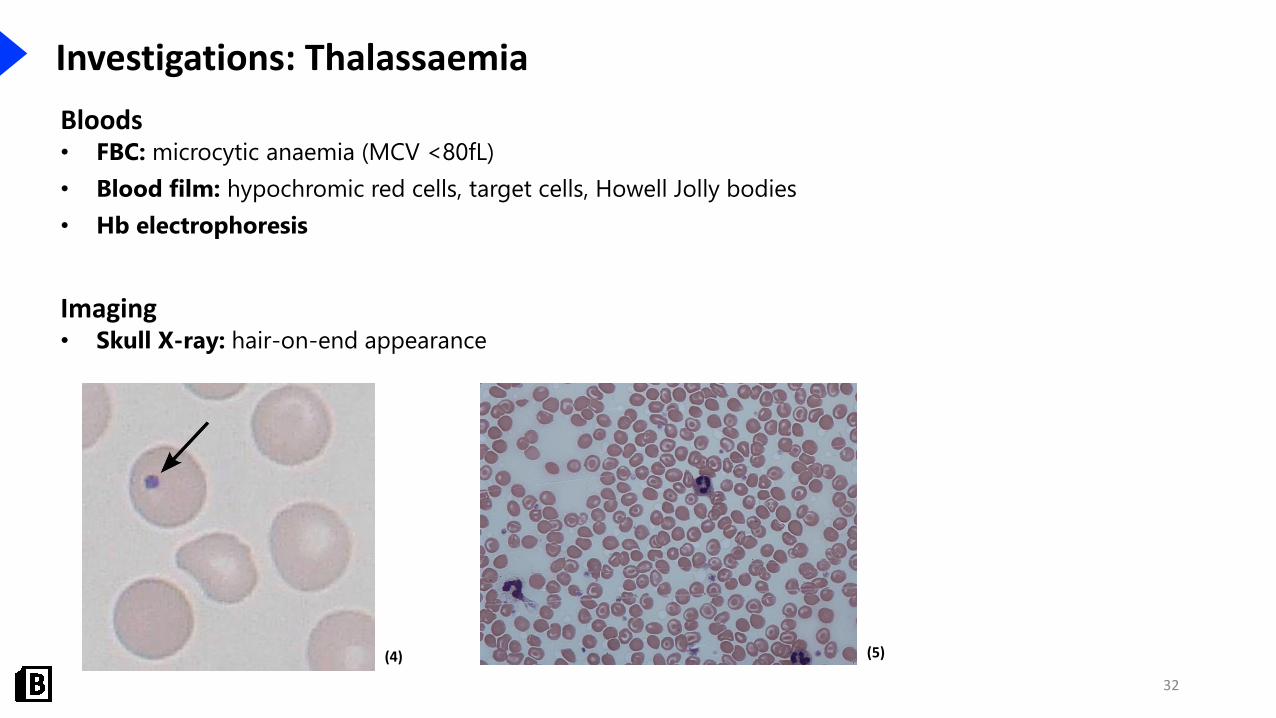
Investigations: Thalassaemia
Bloods• FBC: microcytic anaemia (MCV <80fL)
• Blood film: hypochromic red cells, target cells, Howell Jolly bodies
• Hb electrophoresis
Imaging • Skull X-ray: hair-on-end appearance
(4) (5)
33
Management: Thalassaemia
Alpha and Beta thalassaemia trait
• No intervention required
HbH and beta thalassaemia major
• Regular blood transfusions
• Folate supplementation: haemolysis leads to folate deficiency
• Iron chelation: desferrioxamine reduces the risk of iron overload
• Splenectomy
• Patients develop splenomegaly due to extramedullary haematopoiesis
• Leads to hypersplenism and increased haemolysis
• Stem cell transplant: only curative option

Introduction: Anaemia of chronic disease
Microcytic anaemia
Iron deficiency
Thalassaemia
Anaemia of chronic disease
Sideroblastic anaemia
Definition: anaemia due to inflammation mediated reduction in
RBC production
• Microcytic or normocytic anaemia
Epidemiology:
• Second most common anaemia worldwide
• Multiple causes
• E.g. prevalence of ACD in rheumatoid arthritis ~ 30-40%

Introduction: Anaemia of chronic disease
Aetiology
• Autoimmune disorders e.g. rheumatoid arthritis
• Chronic infection
• Chronic disease e.g. CKD, heart failure
• Malignancy
• Major trauma
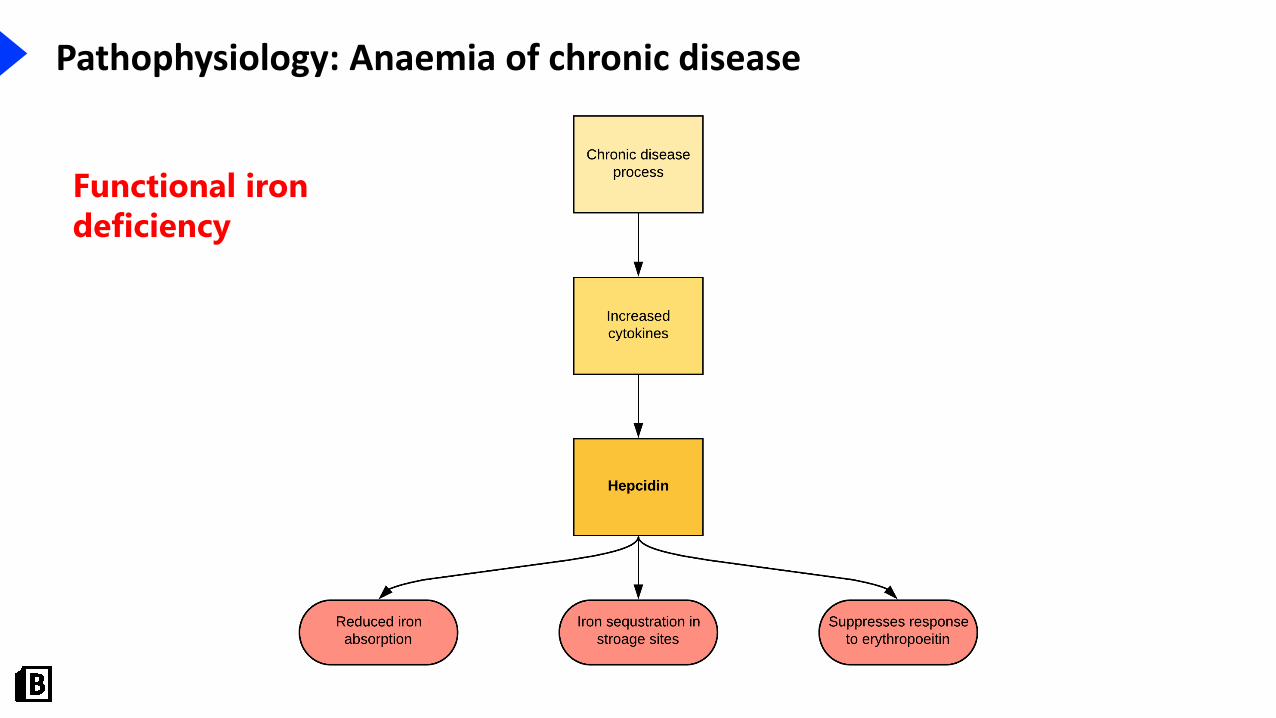
Pathophysiology: Anaemia of chronic disease
Functional iron
deficiency

Investigations: Anaemia of chronic disease
Bloods
• Iron studies
• Ferritin: raised
• Serum iron: reduced
• Transferrin saturation: reduced
• TIBC: reduced
• Inflammatory markers: raised
Chronic disease Iron deficiency
Hb Reduced Reduced
Serum Fe Reduced Reduced
Ferritin Raised Reduced
Transferrin saturation Reduced Reduced
TIBC Reduced Raised
Inflammatory markers Raised Reduced

Management: Anaemia of chronic disease
Treat the underlying cause• Anaemia is frequently mild and the below is may not be required
Iron supplementation• Oral or intravenous
Erythropoietin
Blood transfusion• Not usually required
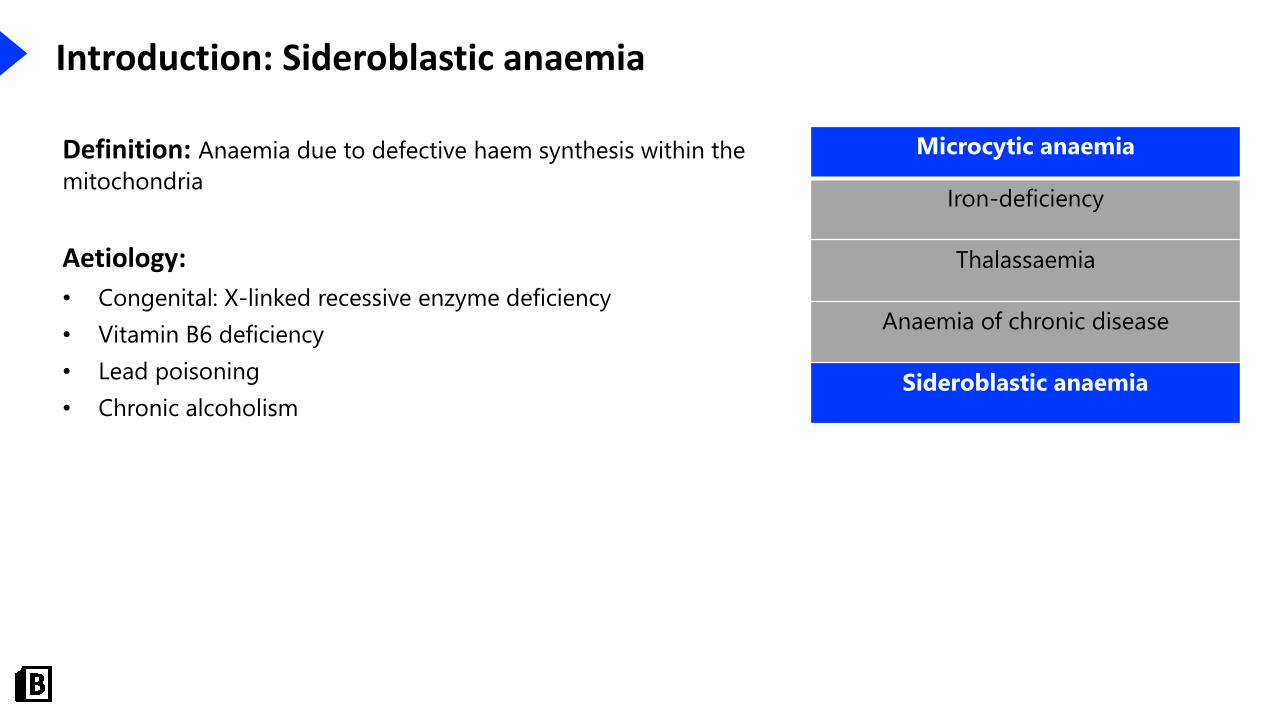
Introduction: Sideroblastic anaemia
Microcytic anaemia
Iron-deficiency
Thalassaemia
Anaemia of chronic disease
Sideroblastic anaemia
Definition: Anaemia due to defective haem synthesis within the
mitochondria
Aetiology:
• Congenital: X-linked recessive enzyme deficiency
• Vitamin B6 deficiency
• Lead poisoning
• Chronic alcoholism
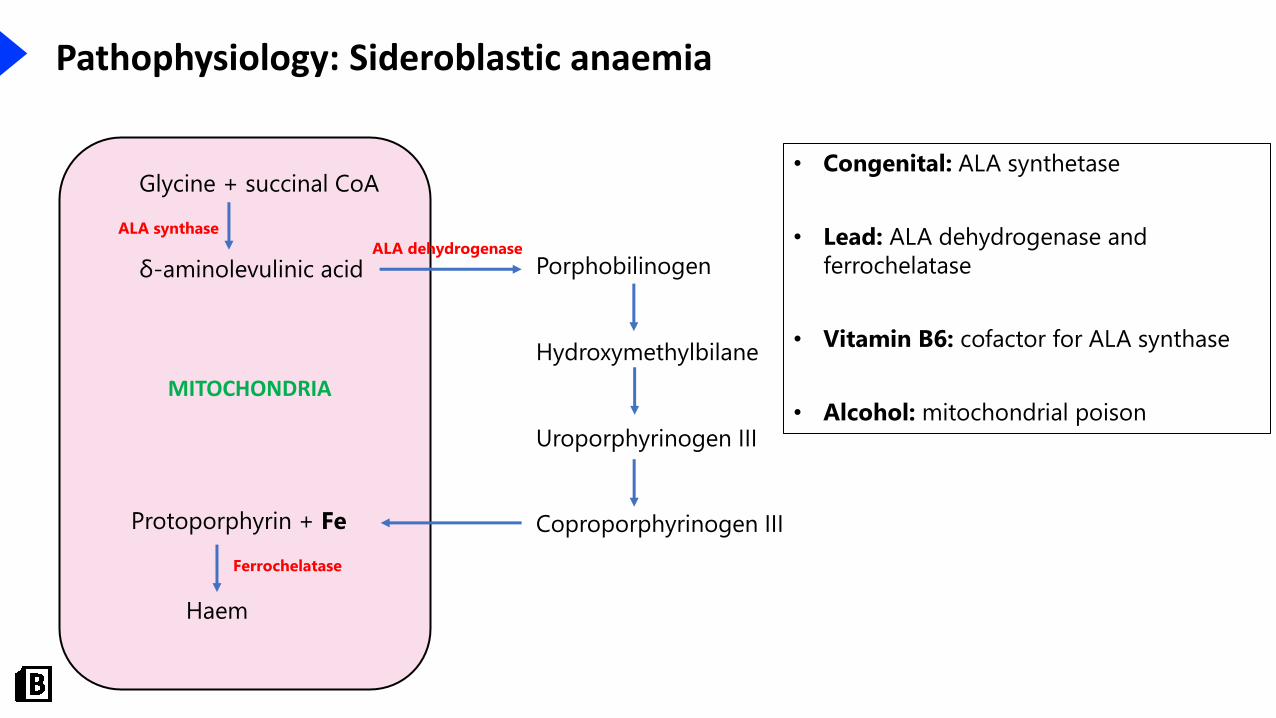
Pathophysiology: Sideroblastic anaemia
Glycine + succinal CoA
δ-aminolevulinic acid Porphobilinogen
Hydroxymethylbilane
Uroporphyrinogen III
Coproporphyrinogen IIIProtoporphyrin + Fe
Haem
ALA synthase
ALA dehydrogenase
Ferrochelatase
• Congenital: ALA synthetase
• Lead: ALA dehydrogenase and
ferrochelatase
• Vitamin B6: cofactor for ALA synthase
• Alcohol: mitochondrial poison MITOCHONDRIA

Pathophysiology: Sideroblastic anaemia
• Iron becomes trapped in the mitochondria and forms a ring around the nucleus of the
erythroblast
• Ringed sideroblast
(6)

Investigations: Sideroblastic anaemia
Bloods
• FBC: microcytic anaemia (MCV <80fL)
• Blood film: ringed sideroblasts
• Iron studies
• Ferrtin: increased
• Serum iron: increased
• Transferrin saturation: increased
• TIBC: reduced

43
Top-decile question

44
Explanations
app.bitemedicine.com
Which of the following is most associated with choriocarcinoma?
Iron deficiency
Not associated
Anaemia of chronic disease
Not associated
Sideroblastic anaemia
Not associated
Alpha thalassaemia
Increased spontaneous abortion in Hb Barts disease
Beta thalassaemia
Not associated

45
Recap
• Microcytic
• Iron deficiency: most common
• Chronic disease: second most common
• Thalassaemia
• Sideroblastic anaemia
Microcytic (MCV < 80fL) Normocytic (MCV 80-95fL) Macrocytic (MCV >95fL)
Iron deficiency Acute blood loss B12 deficiency
Thalassaemia Haemolytic anaemia Folate deficiency
Anaemia of chronic disease Anaemia of chronic disease Alcohol
Sideroblastic anaemia Chronic kidney disease Liver disease
Aplastic anaemia Hypothyroidism


48
References
1. Matthew Ferguson 57 / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0)
2. CHeitz / CC BY (https://creativecommons.org/licenses/by/2.0)3. US Federal Government / Public domain4. Paulo Henrique Orlandi Mourao and Mikael Häggström / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0)5. Dr Graham Beards / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0)6. Paulo Henrique Orlandi Mourao / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0)
All other images were made by BiteMedicine or under basic license from Shutterstock and not suitable for
redistribution.

49
Further information
You will now receive a Certificate of Attendance for attendance at each webinar! Simply fill out thefeedback form.
Stay up-to-date!
• Website: www.bitemedicine.com
• Facebook: ‘BiteMedicine for Students’ for all our updates
• Instagram: @bitemedicine
• Email: [email protected]
Related Documents











