2/19/06 Case

2/19/06 Case. Chief Complaint Pt is a 33 y/o aa male who presents with new onset dyspnea.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
2/19/06 Case
Chief Complaint
• Pt is a 33 y/o aa male who presents with new onset dyspnea
• What questions do we want to ask this patient?
• CC• HPI• PMHx• MEDS• Allergies• SocHx• FMHx• ROS• Physical Exam• Differential• LABS• Radiological• Diagnosis• Treatment
History of Present Illness
Pt is a 33 y/o aa male w/ hx of a murmur in childhood who presents w new onset dyspnea. Pt noticed that he became short of breath while driving today. This is the first time that he has felt this way and it lasted for about twenty minutes. It became better with time and was self limiting. The patient denies having any chest pain, palpitations, light headedness or recent URI. He also denies any recent trauma, calf tenderness, immobility, or history of clotting. He does however admit to being an anxious person and noticed some tingling down his left arm and right side of his body. He also noticed having a muscle cramp in his right arm and diffuse pain across his abdomen.
• CC• HPI• PMHx• MEDS• Allergies• SocHx• FMHx• ROS• Physical Exam• Differential• LABS• Radiological• Diagnosis• Treatment
Past Medical History
Anxiety
Hx of heart murmur
No surgical history
• CC• HPI• PMHx• MEDS• Allergies• SocHx• FMHx• ROS• Physical Exam• Differential• LABS• Radiological• Diagnosis• Treatment
Medications
None
• CC• HPI• PMHx• MEDS• Allergies• SocHx• FMHx• ROS• Physical Exam• Differential• LABS• Radiological• Diagnosis• Treatment
AllergiesNKDA
• CC• HPI• PMHx• MEDS• Allergies• SocHx• FMHx• ROS• Physical Exam• Differential• LABS• Radiological• Diagnosis• Treatment
Social History
Smokes 3 cigars a day
Drinks 24 oz beer / day
• CC• HPI• PMHx• MEDS• Allergies• SocHx• FMHx• ROS• Physical Exam• Differential• LABS• Radiological• Diagnosis• Treatment
Family Medical HistoryMother- SarcoidosisFather-
• CC• HPI• PMHx• MEDS• Allergies• SocHx• FMHx• ROS• Physical Exam• Differential• LABS• Radiological• Diagnosis• Treatment
Review of systems
General: weight change, fever, chills, weakHead: headache, nasuea, vomittingRespiratory: SOB, wheeze, no cough or URICardiac: HTN, murmurs, angina, palpitationsGI: appetite, n/v, incont., const/diarrhea,
mild abdomen painGU: frequency, hesitancy, urgency, dysuria
hematuria, incont., stones, no dyspareunia, no discharge
MSK: muscle weakness, flank pain, muscle cramps
Neuro: parasthesias, loss of sensationPsychiatric- Pt is not depressed
• CC• HPI• PMHx• MEDS• Allergies• SocHx• FMHx• ROS• Physical Exam• Differential• LABS• Radiological
• Diagnosis• Treatment
Physical ExamVS- BP- 146/80 T-98.8 R-15 P-120General- Pt is well nourished and AxOx3Heent- EOMI, PERRLA, no vision changesCV- RRR w/o murmurs or rubs, clicks or gallopsRESP- Clear to auscultation bilaterally, no wheezes,
rales or cracklesAbdomen- Soft, NT, ND, no masses, BS, no bruitsGU- No discharge, bleeding, nodules or masses
Positive lloyd’s testMSK- No weakness, mild tenderness in R flank
TTA T11-L-1 EXT- No edema, negative homans, pulses b/l,
negative troussau signNeuro- No neurodeficits, CN II-XII intact
• CC• HPI• PMHx• MEDS• Allergies• SocHx• FMHx• ROS• Physical Exam• Differential• LABS• Radiological• Diagnosis• Treatment
Differential
PsychiatricAnxietyPanic attack
PulmonaryMost probably acute PEPneumothorax
Less likely chronic etiologyCOPD
CardiacArrhythmiaMIUSA
• CC• HPI• PMHx• MEDS• Allergies• SocHx• FMHx• ROS• Physical Exam• Differential• LABS• Radiological• Diagnosis• Treatment
What do we want to order?
• CC• HPI• PMHx• MEDS• Allergies• SocHx• FMHx• ROS• Physical Exam• Differential• LABS• Radiological• Diagnosis• Treatment
Labs
ChemistryCBCD-dimerEKGChest X-rayCardiac enzymes
• CC• HPI• PMHx• MEDS• Allergies• SocHx• FMHx• ROS• Physical Exam• Differential• LABS• Radiological• Diagnosis• Treatment
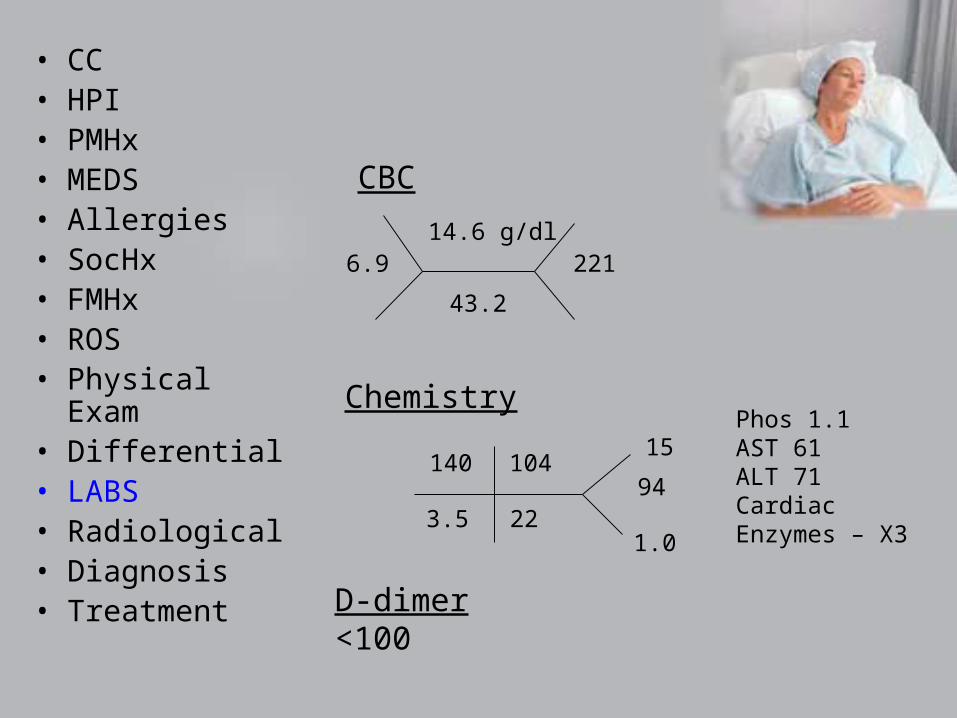
CBC
6.914.6 g/dl
43.2
221
Chemistry
140
3.5
104
22
15
1.0
94
D-dimer<100
Phos 1.1AST 61ALT 71Cardiac Enzymes – X3
• CC• HPI• PMHx• MEDS• Allergies• SocHx• FMHx• ROS• Physical Exam• Differential• LABS• Radiological• Diagnosis• Treatment
Chest X-rayRight hilar vascularityNo flattening of diaghram
EKGNSR
• CC• HPI• PMHx• MEDS• Allergies• SocHx• FMHx• ROS• Physical Exam• Differential• LABS• Radiological• Diagnosis• Treatment
Diagnosis
1. 33 y/o aa male presenting with hyperventilation and dyspnea with left arm tinglingMost likely panic attack; must rule out pulmonary (PE) and cardiac process (MI)
Cardiac enzymes, monitor patient for new episodes, D-dimer, out patient echo
2. HypophosphatemiaMost likely secondary to above and secondary to alcohol history0.1 mmol/ kg IBW potassium phosphate
3. Hx of sarcoid; aa raceSerum angiotensin converting enzyme
Hyperventilation
• Acid base balance maintained by kidney and lungs– Carbon dioxide is removed via lungs
• Hyperventilation can cause respiratory alkalosis
– Acid removed via kidney• Hydrogen and volatile acids like phosphate
Hyperventilation
• Respiratory alkalosis– Acute respiratory alkalosis
• Fall in partial pressure of carbon dioxide – Similar change in the cells
– Carbon dioxide readily diffuses across cell membranes.
– Rise in intracellular pH
» Stimulates phosphofructokinase
» Stimulates glycolysis
– Extreme hyperventilation
– Can lower serum phosphate concentrations to below 1.0 mg/dL
– Most common cause of marked hypophosphatemia in hospitalized patients
Hyperventilation
• Hypophosphatemia– Other causes
• Poor intake (rare)– Kidney usually will reabsorb phosphate
• Antacids• Hyperparathyrdoidism• Vitamin D deficiency• Renal wasting• Alcoholism• Hypersecretion• Hungry bone syndrome• During treatment of DKA
HyperventilationHypophosphatemia
• Signs and symptoms– CNS –
• Irritability • Paresthesias• Confusion• Seizures• Delirium• Coma
– MSK• Proximal myopathy leading to
rhabdomyolysis– May mask low phosphate
– Hematological• Hemolysis• Poor phagocytosis• Defective clotting
• Cardiopulmonary– Impaired Myocardial
contractility• ATP depletion
– Respiratory failure • Weakness of the diaphragm
– Reduction in cardiac output• Congestive heart failure• If plasma phosphate
concentration falls to 1.0 mg/dL

Thank you!
• Questions, comments, concerns?
Related Documents




![IRESSA- gefitinib tablet, coated AstraZeneca ...Acute onset or worsening of pulmonary symptoms (dyspnea, cough, fever) [see Warnings and Precautions (5.1)] NCI CTCAE Grade 2 or higher](https://static.cupdf.com/doc/110x72/60909b7f2bb95331300e699d/iressa-gefitinib-tablet-coated-astrazeneca-acute-onset-or-worsening-of-pulmonary.jpg)






