https://theses.gla.ac.uk/ Theses Digitisation: https://www.gla.ac.uk/myglasgow/research/enlighten/theses/digitisation/ This is a digitised version of the original print thesis. Copyright and moral rights for this work are retained by the author A copy can be downloaded for personal non-commercial research or study, without prior permission or charge This work cannot be reproduced or quoted extensively from without first obtaining permission in writing from the author The content must not be changed in any way or sold commercially in any format or medium without the formal permission of the author When referring to this work, full bibliographic details including the author, title, awarding institution and date of the thesis must be given Enlighten: Theses https://theses.gla.ac.uk/ [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
https://theses.gla.ac.uk/
Theses Digitisation:
https://www.gla.ac.uk/myglasgow/research/enlighten/theses/digitisation/
This is a digitised version of the original print thesis.
Copyright and moral rights for this work are retained by the author
A copy can be downloaded for personal non-commercial research or study,
without prior permission or charge
This work cannot be reproduced or quoted extensively from without first
obtaining permission in writing from the author
The content must not be changed in any way or sold commercially in any
format or medium without the formal permission of the author
When referring to this work, full bibliographic details including the author,
title, awarding institution and date of the thesis must be given
Enlighten: Theses
https://theses.gla.ac.uk/
SfUBIBS 01 THE m/lTIOHSHI? BETWE# Vmitm B12 and CYIHIBB IN THE AETIOBOBY OF TOBACCO
fAMIiYOPIA AND RELATED GOBBXTIOHS*
■by
im A. CHISHOLM,
Being a Thesis Submitted for The Degree of M.B. of Glasgow University,
September* 1969*
ProQuest Number: 10647294
All rights reserved
INFORMATION TO ALL USERS The quality of this reproduction is dependent upon the quality of the copy submitted.
In the unlikely event that the author did not send a com p le te manuscript and there are missing pages, these will be noted. Also, if material had to be removed,
a note will indicate the deletion.
uesL
ProQuest 10647294
Published by ProQuest LLO (2017). Copyright of the Dissertation is held by the Author.
All rights reserved.This work is protected against unauthorized copying under Title 17, United States C ode
Microform Edition © ProQuest LLO.
ProQuest LLO.789 East Eisenhower Parkway
P.Q. Box 1346 Ann Arbor, Ml 48106- 1346
The association between tobacco smoking and a form of amblyopia has been recognised for over one hundred years» The disease characteristically affects elderly men affects both eyes unequally and does not progress to complete blindness# The patient typicall has poor vision both for near and distance* bentro-caecal scotomas larger for colour than white targets in the field of vision and an acquired colour blindness of each eye. Recent additions to the world literature on the subject have postulated an abnormality of the vitamin B12 cyanide relationship as being the underlying aetiological feature and that tobacco amblyopia is a member of a group of diseases which includes Leber’s hereditary optic atrophy* the optic neuropathy of pernicious anaemia, the optic neuropathy of diabetes and some forms of tropical nutritional amblyopia.
This study reports the findings in 65 patients diagnosed as suffering from tobacco amblyopia which have been collected over a period of three years in the Western Regional Hospital Board area. The patients showed, a marked reduction in visual acuity by the time they have reported for treatment.
It was found that the duration of symptoms did not influence the initial visual acuity but those patients who cam© under treatment early Imd the greatest improvement in visual acuity The Farnsworth Munsell Hundred Hue test was chosen as one of the major parameters evaluating new patients prior to and whilst on therapy* As the Hundred Hue test error scores obtained in the untreated tobacco amblyopes were higher than previously recorded analyses, an investigation to establish the validity of such error scores was carried out. It was found that with error scores above 600 it was better to take the average of several readings rather than the result of one test. In untreated tobacco amblyopia the Farnsworth îtoieell Hundred Hue test result correlated well with visual acuity, and tended to do so with patient ago* #i©re was no aignificant correlation between the Farnsworth Munsell Hundred Hue teat result and duration of symptoms, serum vitamin B12 concentration, or serum folate concentration* The incidence of the disease increases in a positive manner with age, reaching a peak in the ?0*80 years age group. The mean duration of symptoms prior to seeking advice was 6 months and it was found that age played no part in deteriBining when a patient presented for treatment*
Patienta were examined for evidence of avitaminosis B12 by having serological estimations of vitamin B12 and estimations of vitamin B12 absorption carried out, Serum vitamin B12 concentrations were found to be lower in tobacco amblyopia than in the general smoking and non-smoking populations. The serum vitamin BX2 concentration correlated well with tobacco consumption, the Schilling test less well so, and the %lose absorption test poorly so. In the untreated tobacco amblyope the serum folate concentration tended to correlate with tobacco consumption. Patients with tobacco amblyopia in the presence of frank Addisonian Pernicious toaemia exhibited higher aenam folate concentrations than those patients without pernicious anaemia.
As cyanide is Volatile investigations into its metabolism ie to be directed to its detoxication products namely thiooyaWte, Although tobacco amblyopes smoko more tobacco than non-amblyopic subjects, their serum thiocyanate concentrations are lower than those of non-amblyopic smokers and tend to resemble the concentrat3.ons found in non-smokers. These reduced concentrations, on treatment with hydroxocobalamln, tend to revert towards the hi#ier concentrations found in the
non-amblyopic smokers. Associated m t h this rise in the blood there is an increased excretion of thiocyanate in the urine. A si{piifleant negative correlation was found to esixt between the plasma cyanide and the serum vitamin B12 concentrations and between the plasma thiocyanate and the renal clearance of thiocyanate in untreated tobacco amblyopia.
The keystone in therapy up till 10 years ago had been abstinence from the tobacco habit. With the growing awareness of the part played by malnutrition in this disease, preparetiohs of vitamin B12 were used in this analysis* Of the two preparations used, hydroxocobalamin was quickly found to be superior to qyanocobalamin. The mean period that patients remained under observation was nineteen months* The majority (40 in number) had a visual acuity of 6/12 (Snellen) or better. Of the fifteen patients who had a poor restoration of vision, four were undergoing their second attack of the disease* The progress of the disease whilst on. therapy was also observed by following the alteration in colour discrimination. It was found that the Farnsworth Munsell Hundred Hue test results fitted an exponential curve equation.
The rat© of improvement in uncomplicated tobacco amblyopia treated with hydroxocobalamln was as good as that treated by abstinence from tobacco•
Leber’s Hereditary Optic Atrophy is mi inherited disease which primarily attacks the young adult* Abnormalities in cyanide detoxication products, similar to those found in tobacco amblyopia, were found in such patients* These changes underwent similar alteration on treatment with hydroxooobalamin as had been demonstrated in tobacco amblyopia and were associated with Improvement in visual acuity and visual field*
The ocular features of patients suffering from the optic neuropathy of pernicious anaemia who smoked, were identical to those found in patients suffering from tobacco amblyopia* Accordingly, it is Alt that the diagnosis of optic neuropathy of pernicious anaemia be reserved for those non-smoking pernicious anaemia patients, Three case histories are examined which reveal the superiority of hydroxocobalamin therapy over cyanoêobalamln in this condition* In one patient the visual defect commenced after treatment with
cyanooobalamiîi for the haematological disorder had been continued for some time.
It is difficult in the light of present knowledge to explain the rise in thiocyanate concentrations in body fluids following a hydroxocobalamin therapy, unless a hitherto unknoim mechanism sited in the kidney is postulated. It would seem that the principle biochemical defect in tobacco amblyopia would lie in the preparation of a suitable sulphur donor. In the preparation of such a donor coenzyme vitamin B12 is essential.
r
OTînîiBs OH ®iis RmTioMSHip Bsæwmt ,SH <e -*¥,K-— *fh# ë, I. U) W— *W#?.###,#&# l/tff lU**‘HWWWiW
Aim o m m m m ïh e AmiaoeY op îobacco amblyopia~~ - - — — "
AND KSLAf® COHOTl’lOHS,
Being a thosia submlttad for the degree of M*B, to the tlaiveralty of Glasgow
byIA» A. OBISHOLM September, 1369,
* * * # # n. Tnm
ïomcco XHPSHHSaii, 2S’ If M Ul« GOSTOiSÎ ft> œ ORBBIS i
I HfP/S Ksr., a iSS Î rm ÜMÎ 1RB f »ï
BOB! œ
âPPM'ïfS AI# f
#**#*# #
Table of Contenta,
Acknowledgements• .................... Page I.Introduction* Page 4.Chapter Summaries, ..................... Page ,6.Chapter I, Historical Background. Page 15.Chapter II. Ophthalmological Investigation. Page 50,Chapter III. Nutritional Factors. Page 71.Chapter IV. The Toxic Factor in Tobacco. Page 109.Chapter V. Response to Therapy. Page 142.Chapter VI. Leber's Hereditary Optic Atrophy, Page 169.
Optic Neuropathy of PerniciousAnaemia. Page 195.
Chapter VII. Conclusions. Page 207.References• Page 221.Appendix A* Patient Details. Page 258.Appendix B. Publications. Page 269.
The alinloal maWMal for thla survey wae oolleoted and studied at the Tonnent Inetitute of Ophthalmology, University of Glasgow• I wish to record nay thanks to the various ophthalmie apeoialiste of the Western Regional Hospital Board who referred their patients with tohaooo amblyopia and Leber’ s Hereditary Optic âtropî3y, end allowed mo access to their case recordsi*toctora â#H# Wright Thomson, l*d* Smith, H*W* Paterson,B» Ohristison, 0*0. Maolwan, J* Levy and W.à.M* Smith of the Glasgow % e Infirmary* Doctor w. Wilson of the Ophthalmic Institution; Doctor W.W# Boig of the loyal Victoria % e Infirmary, Paisley# Doctor J* Willieioson of the Southern General Hospital, Doctor lU Harrington of Strathclyde Hospital, Mothexwell, and Doctor J*S. Omit of the Western Infirmary, ; Glasgow#
A special debt of gratitute to my associate# In much of the work in this study whose enthusiasm strengthened my faltering steps ## Professor W*S* Foulds, Doctor J, Bronte- ' Stewart and Doctor T* Wilson*
It ia a pleasure to record my thanks to Sisters
MoKiïiïion and Wilaon and the Huroing staff of the % e Department, Western Infizmmry, Glasgow, who midertook the routine specimen collectIona and treatment.
% thanks are due also to Professor A* Goldberg and Doctor J. Morrow of the Gardiner Institute of Glasgow, for help and advice on the haematologioal aspects of the study; Doctor E. Hendry of the biochemistry Departmont, Western Infifmary, for the thiocyanate analysis by the Bowler’s method; Doctor J.F. Adams, Southern General Hospital, Glasgow, for the vitamin B12 essays* Doctor H. lakowski, Psychology Department, University of Edinburgh, who my easily attempts to test colour discrimination*Doctor J# Wilson, M.E.Ü. Genetics Hesearoh Unit, National Hospital for Nervous Diseases, London, who gave of hie time to teach m© the estimation of micro quantities of cyanide and thiocyanate in plasma and urine* lb?ofesaor W.I# Osrd, Professor Medicine in relation to Mathematics and Computing, for help with the statistical treatment of the analyses* te. S.S. Ben Hameid of the computing laboratory for permission to use his exponential curve programme for the KBFG computer.
The illustrations and photoip?apha are the work of
the Medical Illustration Departmmt# Western Infirmary, Glasgow, under the direetlon of Mr# G. Donald#
The later part of this study was eupportod by reeearoh grants frma. Glaxo Lahoratorieo and the Medical Boeearoh Oounoil#
It ia imivamally recognised that tobaooo mblyopie ie a clieoase, almost oxelueively, of the elderly pipe amohlmg œle. It la the impreealoti that, although # m tohaoeo ooneumption has steadily risen ainoe the turn of the century,the reported, number of oaaea of W W o a o amblyopia has fallen* This ia in contrast to the .parallelism accorded to % e alleged cigare tte smoking lung cancer relationsMp*- Assuming th a t
the imcidanoe of tobacco amblyopia line apparently gone down while exposure to its presumed aotiologio agent has risen, other contributory explanations must be sought,
%#%y does only a small proportion of pip© smokers develop the disease? \Ûmt factors cause the disease and how do they alter with treatment? An attempt to answer these questions# using the in-patient and out*patient data of a study into the clinical feature© of the disease, is contained in this thesis, the data been arranged under the following headings!-
1. â historical background,2# Ml analyeis of the means to determine the presence
and severity of the disease, (Ophthalmclogloalinvestigation),
4
5* Kutrltionul faotors*4*, flue tox ic facto r in tobacco*
5* the m&ponm to therapy*
6* Leber’ 8 Hereditary Optio Atrophy* Optic Neuropathy of Pornloioma Anaemia*
7* Oouolueloaa*
5
Chapter I# Hiatorioal Background
Tobacco amblyopia ie a disease of the elderly pipe-smoking male* Females may also contract the diseaseif sufficiently exposed to the toxic agent* Characteristii *Gaily the disease is bilateral, but unequally distributed between the two eyes* The. visual acuity is depressed and a glittering mist obscures objects except when viewed in twilight* A oentro-oaeoal scotoma, larger for colours than white, is present in the field of vision, and is$.acoompanied by an acquired colour blindness*
Tobaooo amblyopia may be associated with a variety of systemic diseases, in particular diabetes, pernicious anaemia and digestive disorders* This has led to the belief tiiat such patients are more liable to tobacco amblyopia because of a deficiency in an essential substance*
The keystone in treatment of tobacco amblyopia has been abstinence from the tobacco habit and has been in vogue from the last century* Over the past thirty years
6
however, the importance of malnutrition has been stressed by various authors, in particular of dafioienoy in vitamin B12*
Within the past eight years much new work has postulated the probable aetiology as being a disturbance in the cyanide - vitamin B12 relationship* This has led to the proposal that tobacco amblyopia is a member of a group of diseases which includes Leber’s Hereditary Optic Atrophy, the Optic Neuropathy of Pernicious Anaemia, the Optic Neuropathy of Diabetes, and some forms of Tropical Nutritional Amblyopia, and in each of which a disturbance of the above relationship is present*
Chapter II* QphthalmologioaX Investigation
In this chapter the ophthalmic methods of investigating the visual loss found to accompany tobacco amblyopia are dealt with*
By the time they report for treatment the patients have a marked reduction in visual acuity, oentro-caeoal scotomas in the field of vision for each eye, and a gross
mpact in oolom? disojriraination feeing present. The teation of ayaptome did not influence the initial visual acuity, but those patiente who came mder treatment early had the greatest improvement in visual acuity#
The Farnsworth îteisell 100 Hue tent u m chosen as one of the major parameters in evaluating individual patients prior to# and whilst on tîierapy. As the 100 Hue test error soores obtained in the untreated tofeaooo amblyopes were higher than previously recorded analyses, mi investigation to establish the validity of suoh error soores was carried out.
In untreated tobaooo amblyopia the Famswortii Munsell 100 Hue test result correlated well with visual acuity and tended to do so with patient age. There was no aignifieant correlation between the Itensworth Mimsell Hundred Hue test result and duration of symptoms, serum vitamin Bl2 oonoentratipn or serum folate oonoentration*
The incidence of the disease inoreaaes in a positive manner with age, reaohing a peak in the 70-80years age group# thereafter declining in frequency. The
0
mean duration of symptoms prior to seeking advice was 6 months and it was found that age played no pari in detersiaining when a patient presented for treatment#
Chanter III* Nutritional Factors»
In this chapter attention has been concentrated on the detection of avitasiinosis B12 and the relationship of the findings to tobacco oonsumption* The patients were examined for coincident disease, serological examinations were carried out for total vitamin B12 and folate concentrations of the blood* Igxamlnation into vitamin il2 absorption were carried out on the patients on an in-patient basis* Liver function tests were performed to screen the patients for defective hepatic storage Of vitamin B12»
Serum v itamin B12 concentrations were found to be lower in tobacco amblyopia than in the general smoking and non-smoking populations. The serum vitamin B12 concentration correlated well with tobacco consumption, the Schilling test less well BO, and the Xylose absorption test poorly so#
The serum folate concentration was also investigated
and a significant proportion of the patients exhibited low concentration© of folate* In the untreated tobacco amblyope the serum folate concentration tended to correlate with tobacco consumption. Patienta with tobacco amblyopia in the presence of frank Addisonian Pernicious Maemia exhibited higher serum folate concentrations than those patients without pernicious anaemia. Age played no part in determining the serum folate concentra tion »
er IV'* The Toxic Factor in Tobacco*
In this chapter the presence of cyanide in tobacco smoke and its metabolic effects are reviewed. As cyanide is volatile investigation of its metabolism has to be directed to its detoxication products* Attention has been concentrated on thiocyanate levels in the blood and urine*
Although tobacco amblyopes smoke more tobacco than non-amblyopio subjects, their serum thiocyanate concentrations are lower than those of non-arablyopic smokers and tend to resemble the concentrations found in non-smokers. These reduced concentrations, on treatment with hydroxocobalamin, tend to revert towards the higher oonoentrations found, in the
10
mon-aia.1>lyopl0 smokers* Associated with this rise in the blood there la am inoroaasd excretion of thlqoyamete 1b the urime and in some patients a diureals oooura* The negative relationship between eerm vitamin BIB oonaentration and urinary thlooyanato exoration, and the positive relationship between plasma cyanide and plasma thiocyanate found by earlier workers in healthy smokers were not confirmed in patients suffering from tobacco amblyopia, Only a tendency towards aucli relationships was observed* A signifloant negative correlation was fomd to exist between the plasma cyanide and the serum vitamin B12 concentrations, and between the plasma thiooyanat© and the renal clearance of thiocyanate in untreated tobacco amblyopia#
The keystone in therapy, up till 10 years ago, for patients with tobacco amblyopia had been abstinence from the tobacco habit; in addition, vasodiXatory drugs and etryehnino had been used with doubtful Buceeee* With the growing ewarenees of the part played by. malnutrition in this disease I preparations of vitamin B12 were used in this analysis. Of the two preparations used, hydroxocobalafin was quickly
11
foimd to be superior to oymoeobulamin and all patients ultimately cam© to be treated with the better droif*
The mean period that patients remained wider observation was nineteen months, with a range from five montha to thirty five months* fhe majority (40 in number) had a visual acuity of 6/l2 or batter after the period cf follmt up. fen patiente became lost from tlie mialyml# by reason of default or death* Of the fifteen patients who had a poor restoration of vialon, four wore undergoing tlioir seoond attaok of the-disease*
The progress of the disease whilst on tliorapy was also observed by following the alteration in colour discrimination# It was found that the remits fitted an exponential ourve equation* By this mems the rate of Impmvemmt in colour discrimination was compared in tobacco amblyopia complicated by pernicious anaemia, pre-perniciouo' anaemia, and diabetes# The rate of improvement in mieoMplloated tcbacoo amblyopia treated by hydroxocofealamin was equally good as that treated by abstinence from tobacco#
12
Leher’ s Hereditary Optic Atmphy is an inherited digeaee which primarily attacks the young adult, both eye# being affaotad and resulting in a aerioue viaual defect# âbnoraalltiaa in cyanide detoxiaation product©, elmllar to thoee found in tohaooo aTaMyopia, were found in auoh patients, These changea undorwmt similar alteration after treatment with hydroxoGobalamln, ae had been demonotrated in tobaoeo amblyopia# The ocular feature© of patiente oufferlng from the optio neuropathy of pernioioiia maemia who emoked, were Identical to those found in patienta suffering from tohaooo amblyopia# âeoordlngly. It la felt that the diagnosis of optlo neuropathy of parnioloua anaemia he reserved for #oae mon-amoklng pernicious anaemia patients who have visual eigne and symptoms# " Three came histories are examined which reveal the superiority of liydroxooohalamln therapy over oyanoQObalamin in this condition# In one patient the visual defect oommenoed after traatjaent with cymoaobalwin for the haematologioal defect had been continued for acme time#An oaeurreno© not previously reported in the literature*
13
Oonoluaicaa
in this chapterf the evidence in favour of a ctletnrhanoe in the vitamin BlB/oygmide relationship, as the hsaio factor in the production of tobacco amblyopia, 1# collected and examined# In the maim sttch a dieturhance leada to a failure of the detoxloation of cyanide to thiocyanate, by its mien with sulphur-* It ie difficult in the light of present toowledgo to explain the rise in thiocyanate eoncentratione in body fluids following on hydroxoooMlamin therapy, unleee a hitherto unWwwn meohaniam cited in the kidney is postulated# Such a mechanism is outlined#
14
o m r œ i.
HxaroiüAii moKORomp
fhe term toxic amblyopia is generally ueed. to designate condition© to which visual losa results from the absorption of exogenous poison or endogenously elaborated toxins* As a group these poisons have features in common# 1?hey involve the ganglion cells or optic nerve fibres of the sub chiasmal portion of the visual pathway# #ie visual disturbance is bilateral and, on the whole, the . defect is not permanent# fhe common group has an affinity for the papillo macular neiva fibre bundle resulting in a central, or centro-»oaeeal scotoma, and may be accompanied by a peripheral neuropathy# In this group are found tobacco, methyl and ethyl alcohol, lead, carbon disulphide and inorganic arsenical compounds* In the less common group, the visual defect takes the fozrm of a peripheral contraction of the visual field while peripheral neuropathy is unusual* fh© quinoline group of drugs act in this way.
Tobacco amblyopia is the most common type of toxic amblyopia met with in Western Burope today. It constitutes a clinical entity which affects mainly the pipe
15
smoking middle-aged male# and ie oharaoteMsed by a bilateral impairment of central vision with the development, in the eentro-eaeoal area of the visual field, of depressed sensitivity to red and green stimuli, without ophthalmosoopio changes* (Buka Bilder 19# )
Ton i*aefe (186$) recognised progressive amblyopia with oontraotad field, and curable amblyopia with full field and central scotoma* He considered that excessive indulgence in alcohol, much smoking of strong cigars, irregular sleep and over use of the eyes might act singly, but m m often acted together in producing amblyopia# leber (I86f) exm*ined the colour sense and found a central defect. He considered that in many cases smoking was a factor in the production of central scotomata. Burster (I069) had found patients with a central scotoma who improved when tobacco moklng was avoided, and in 18?1 he recorded the value of using a rad object on a black background in testing for the never failing central scotoma in amblyopia from abuse of nicotine and spirits*
Although Beer (181?) is credited with the first recorded description of tobacco amblyopia, it is quite possible that Tenner (18§0) ms referring to tMse cases
16
that are novt called tobacco amblyopia# in hi© treatise on tohaooo, l^okengîia (IB50) had repeatedly hinted hie ouepioions that tohaaoo was a cause of amaurosis# and in the 4th edition of "Biseasee of the Bye*' ' (IB54) he mentioned a oaso of amaurosis that improved on giving up tohaoeo without other treatment* He further oonaldered that one of the best proofs of tohaoco being a cause of amaurosis mn in the great Improvement of vision that ensued on givii^ up the use of the poison*
hfmtenhaoh (189#) employed the term "Tobacco Amblyopia" to express retrobulbar neuritis of the optio nerve with a central colour scotoma# followed by optic nerve atrophy m d occurring in those addicted to the exoeceivo use of tobacco* Hhthoff (1886) and Qroenouw (18# ) regarded retrobulbar neuritis and toxic amblyopia as different diseases in spite of the seemingly identical findings* Accordi% to Hhthoff retrobulbar neuritis is distinguished frm toxic amblyopia by the extent of #%e scotoma* Early observers noted that toWccc amblyopia was almost exclusively a male disease (Halson 1880 mid lyle 190$), and was very rare in women (Berry 1884, Bales 1887, Gunn 1887, Oossu 1# 3, %herl # 7e and Traquair 1928)* Hhtoff (Ifll) warned that one should not assume a special predisposition in men, since
17
women wore algo affected when sufficiently exposed to tobacco as was found In female tobaooo workers by legge (1922).
Virtually all authorities are ageeed that tobacco amblyopia ia a disease of the middle-aged male beetween the ages of #-60 years (lelaon 1880, lamaay 1895, %le IgOg,Bar 1906, tîaher 1927a 1 Traquair 1950, Mille 1934* Oreeves 1936, liambreain and Boliopena 194^ m d Heaton et aX 1958), being rare before the age of 30 years (Groenouw 1892) though fraquair (1930) repeated its ooourrenoe in the 20*8 ami Usher (1927a) in the teens* The incidence declines after the age of 60 years (Oromouw 1892) though Traquair (1930) and Seaton et al (1958) reported it» ooourreaco in patients of 60 years and older* Bowling (1908) extensively Investigated legro tobacco workers and conoludad that this race had an immunity to tobacco amblyopia* This work hm not been confirmed or disproved*, hopes (I9OO) stated that tobacco amblyopia was m exceptional disease in -Bpaniards and Oubans but this was eubsequently disproved (finlay 1901)* Van den loeve (1927) stated that he had never seen cases of tobacco amblyopia in Holland and believed that it did not occur there, though he could offer no reason why*
18
Gromouw (I892) stated that all of the usual foma of using tobaooo may load to tohsooo amblyopia | bmutenbaoh (1898) was oonvlmoed that tobaooo must he smoked to produoa the disorder# Boggart (1959) reported a ease f^om the use of snuff and Ohisholm (1S90) itm- chewing tohaoco# Tobaooo amblyopia mm common in patients who smoked tofeaooo as cigars or pipes, usually strong tobacco and pipe smoking was the commonest cause, (Grseves 19)6, Beislman 1951 Boggart 1959) Billie (1934) had never seen the disease from cigarette smoking, hut EVsns (1959) » Oohen (1959)'*Smith (1959) and Heaton et al (1958) had* Beiehman (1951) suggested that a possible explanation of the different incidence rates of tobacco amblyopia in pipe and cigarette smoking may lie in the different routes of absorption of the toxic agent# In pipe smoking the agent was swallowed causing a slow upset of gastric function with resulting metabolic derangement whioh in turn might produce the lesion of tobacco amblyopia#
It ie agreed that prolonged exposure to tobacco is necessary to produce tobacco amblyopia (Galezowski 1683, Mettleship IBS?, Ohieholm 1#90, Bmmsoy 1695$ Heaton et al 1950, Boggart 1959)* Ohioholm (1890) had never seen tobacco amblyopia from tobacco use of less than 10 years and all but
19
om of the patienta of Heaton et al (1958) had emoked for JO yeare or more# Hettleshlp (1887) recorded the dieeaae after one year* $ emoklmg# Gmevee (19J6) and Heaton at al (1956) found that the absolute amount of tobacco was not a determining factor, m there is no demonstrable relationship between thia and the onset of the disease#
In men Berry (IBS?) found that one ounce to half a pound or more weekly was the quantity smoked by ease» of amblyopia, The disease le seen from time to time in those who have smoked surprisingly email qumtities of 'tobacoo# Siioh oases have been recorded by Hales (186?), Berry (IBS?), lîaberahon (ISSS), de Boh'weinitîs (19OO) end others# Chisholm (IBB?) recorded a case that smoked only half a cigar daily# It frequently made hie patient sick and'he had been persevering for years to acquire the habit of smoking#
The onset of tobacco amblyopia has been described as sudden, rapid or abrupt (llartrMge 1886) or slow, gradual or insidious. (Ramsay 1895». Byle 1905» B.owling 1908, Eambresin and Schepene 19#)* The earlier observers tended to emphasise the rapidity and the later observers the slowness of onset# According to some observers failure of eight in tobacco amblyopia progreeaed
20
rapidly for a time .and then remained relatively stationary (lettleship IBS?) or progreaaiva (l»yle 1905$ Bowling IgOS), Most authors are in agreement that tobadoo amblyopia never progressed to complete loam of sight (ïlhthoff 1080, Berry 1S02| Traquair 1930) though Marshall and Seiler (1942) found that tobacco amblyopia accounted for 0#124# of blind registrations#
The prognosis is generally favourable if the patient gives up smoking and comm under early treatment (Hamasy 1895$ ■ Bowling 1908, Traqualr 19J0)# Griffith (1687) from M s study of oases, concluded that there was a tendency for recovery to take place even without complete discontinuance of the toxic agent. Speedy recoveries were marked in those who gave up tobacco completely# Of his 65 examples of tobacco amblyopia, 27 patients- completely recovered their sight (18 complete abstinence emd 9 almost complete), 24 partially recovered their sight (II complete abstinence), II remained stationary (5 complete abstinence), 5 became worse (I complete abstinence), Somewhat similar results were found by Evans (1939) ^ out of 551 23 recovered fully their sight, 27 had partial recovery, 5 no recovery# Oarroll (1937-44) found that patients on adequate diets made partial or complete
21
recovery, in spite of their continued and unabated m e of tobacco and/or alcohol# He claimed hie résulta wero m good a# any previous oeriea Including those in which the patienta abstained from smoking# If the patient with tobacco amblyopia dieaontinned smoking hia vision usually improved but if he oontimied to smoke and take large doeee of vitamin B complex and a well balanced diet there would be improvement over a period of months (Ofarroll 1956).
time for recovery has been variously described as rapid (Euata 1925) or* slow (Oreovea 193^)I not earlier than 2 months (Berry 18$?), J-42 months in 50& of patients (Griffith 1887), 2-10 months (llambreaiE and Hohopens 1946}# Bidden (1936) stated that recovery may take up to 2 years - longer than was usually considered* Berry (1887) noticed that there was a latent period t#ter treatment was commenced before appreciable change occurred mad fraquair (1930) noticed that vision, in some oases, became worse before Improvement set in, after smoking was stopped# Berry (1887) noted that relapses were rare, Gunn (1887) end Bales (188?) had not mmi a recurrence though lîettleahlp (1887) had encountered a relapse#
According to Croenouw (1892) the typical cases
were fotmd in middle-aged men who were heavy smoker# m d eonemmed alcohol. The general condition wa# dietnrbed with, laok of appetite, insomnia, constipation and a feeling of fatigue and dépression# A# daaoribed by Traquair (igJO) the patient wan ueually a man of about 50 years whose eight had been falling for several weeks or months. There was a smell of stale tobaooo about him# ihere may be tremor of the hands# The vision failure was worse for near vision and identity of oolours# The vision was better at dusk than in bright daylight. Oooasionally a silvery mist surrounded any object looked at. The symptoms same on gradually and without any exciting cause* In general, there appeared to be little or no oharaoteristlo ophthalmoscopie findings, (Mettleship and Edmund IBSJ, Traquair 1930» Oarroll 1935» Hambresin and Bchepona 1946), although pallor of the temporal half or quadrant of the optio dies had been observed (Groenouw 1892, Traquair 1930$'8arroll 1935)• Persistent and marked miosis had. been noticed (Osle^owski 1ÛS3) and had been used to differentiate tobaooo amblyopia from alcoholic amblyopia in which the pupils were said to be dilated B.M.d# i»744 (1879)
Diminution of visual acuity was one of the characteristic signs of tobacco amblyopia (QalezowBki 1883). There was conspicuous disproportion between distant vision
which was almost momml im moat oaoea, sad olosa vision which showed pronounced deterioration (fraquair 1930)* Aa long ae the aootoma had not attacked the fixation point, the vision remained good in tohaooo amblyopia# When the fixation point m m affected, the decrease in the visual acuity could he rapid {flamhreein and Hohepens 1946)#
The visual field defect has been variously deeeribed as central (leher 1069, Galeaowoki 1883, Comior 1890, Bedgee 1957) and oentro-oaeeal (fraquair 1930, Oarroll 1935» ieatoii et al 1958) in which the defeot for colour was larger than that far white, m d of the colours that for red and green being larger than that for blue (hyle 1905)#Heaton at si (1958) eryetalliaed the literature in the following criteria#-
(1) The patient muet be a smoker*(2) A oentro-oaeoal eootoma must be preaent#(3) Thia sootoiaa must be horizontally oval and
most readily detected by a reduced-, stimulus#(4) The defect for csolour must be larger than that
for white#(5) The scotoma must be bilateral though not
■ necessarily equal on the two «idee#
Pathological changes in tobacco amblyopia or
24
tobacco-nleohol amblyopia had been thought to involve either the oiroulatory or the neural elements of the sye, or both, although in actual examination, it va» exoeptlonal to find auoh change© (%le 1947)# Hietopathologio findings have been reported in detail (Bameleobn 188Ê, Haoh© 1887*93# Biroh-
IlirsohfeM 1902# Victor and Bryfus 1965)* Wordworth (I863) stated that only one pathologic condition was seen - namely white atrophy of the optic nerve»# Bach© (18Û7) considered that the generally valid anatomic haaie of tobacco amblyopia was the partial degeneration of the optic nerve tract and degeneration of the papillo-macular fasciculus* Hue! (1096) claimed that the central scotoma of tobacco amblyopia was the result of macular disease and not an interstitial neuritis of the optic nerve* Mille (1934) considered the idea that only the maculopapillary bundle of nerves is affected seemed beet established clinically# Grosnouv (1892) favn:a?ed the view that the primary site of tobacco amblyopia vac to be found in the optic nerve and not in the chiasm» or optic tract# byle (IgOg) believed that the amblyopia was centred on a primary degeneration of the ganglion cells of the retina in the neighbourhood of the macula lutes with a secondary degeneration of the neive fibres arising from the cells* Victor and Bryfue (1965) took the opposite view* The interstitial changes noted were considered to be an
25
accompaniment of the degenerative process in the optic nerve itaeif, Sohieok (X9Û3) and Bar (1906) supported the view of Parsons (1901) that the action of nicotine in tobacco amblyopia was in part vascular# causing vasoconstriction of the arterioles, which explained the selection of the macular region with its unique vascular supply, Bohieok (1903) felt that the nerve fibres which maintain the retinal centre were unfavourably situated in the axial part of the optic nerve and therefore were liable to reflect nutritional disturbances# earlier than the fibres located in the periphery of nerve, Thus# tobacco was said to act on the nerve i)y way of a
chronic nutritional disturbance* Several authors had noted that the vision in tobacco amblyopia was improved by vasodilators and had considered that this supported the hypothesis that tobacco amblyopia was due to vascular spasm in the visual pathway (Oordos and Harrington 1935# Duggan 1935*37)• Carroll (1957) challenged this as he had no success with sodium nitrate. It would appear that the lesion in tobacco mablyopia was primarily nervous rather than vascular (Gunn I930) and although the factor of vaso spasm could not be excluded# it is probably not of very great importance (Evans 1939)* Sohepens (1946) suggested that tobacco amblyopia began with an enlargement of normal
26
angioscotomata particularly in the centro-oaecal regions* Heusohueler (1928) summed up the theories proposed to explain tobacco amblyopiaI-
(l) Primary interstitial inflammation of the papillo- macular bundle with predominating localisations in the optic canal and subsequent compression of nerve fibres by the newly formed tissue (ïïhthoff Igll). Primary lesion in the vasal system consisting of inflammation and thickening of the walls# often the phenomenon of endararltis (Sohieok I903).
(3) Primary degeneration of the nerve fibres of the papillo-macular bundle with secondary and simultaneout lesions of the ganglion cells of the macular region (Palen I9O6)#
(4) A primary lesion of the centre of the retina with secondary ascending degeneration of Ihe papille- macular bimdl© (Roenne I910)*He further concluded that none was satisfactory*
parsons (1901) considered that the action of nicotine (or# rather of the unknown cause of tobacco amblyopia) was two-fold; (l) vascular# causing vaso-constriction of the arterioles; (2) paralytic upon the synapsis either of the
2?
eone fibres# of the cone bipolars# or of both, and Fisher(1901) felt that nicotine was directly toxic to the ganglion cells of the retina* Ramsay (1S95) wrote "as far as my own observations go, all oases of tobaooo amblyopia when recovery is Incomplete will sooner or later exhibit peripheral contraction of the visual field» " These observations suggested that parts of the retina m â optic nerve other thm those connected with the papillo**maoular bundle of nerve fibres were involved, though in some cases the nerve fibres even in the papillo#macular bundle were irregularly affected* Doyne (1SS9) auggeeted that tobacco might have a toxic influence on a îjypotîiotioal substance in the retina analogous to the visual pwple, degenerating it m d causing retinal exhaustion, which shows itself in the failure of the more delicate colour sense* The exhaustion naturally takes place at # e point of greatest retinal activity and where the light is proportionately stronger, the rays being more accurately focussed* Sohanz (1920) held the opinion that in toxic mblyopia the retina was damaged by light while the poisonous substances acted as sensitising agents*
Recent experimental and clinical evidence both suggest that there is sme connection between tîie metabolism of Vitamin B12 and that of cyanide, and that smoking, which is
associa tat with a high cyanide Intake (Burgeon General U.S# 1964# Darby and Wiloon 1967) may adversely affect Vitamin B12 metabolism (Boxer and Biokarde 1952# Woke# and Piocard 1955» Braekkan et al 1957» Wbkee 1958# 8ml# I96I» Smith et al IgëJ» Smith 1964$ Smith and Duokett I965# llatthewa et al 1965, Wllaon and Matthew# 1966» hlndatrand et al I966» Smith and Fonilkee 1966)* The hypotheale that intereonneeted diaturhanoea of eyanide/Vitamin BIB metaholim may W concerned in the pathogenesi# of tobacco amblyopia» the retrobulbar neuritis of pemicioue anaemia» Baber’e hereditary optic atropiiy» and certain tropical neurological syndrome# apparently aaeooiatei with a high cyanide intake itm tropical pulses such as cassava» is supported by Smith (1961)» Wilson (196$^)» Montgomery (1965)# Wilson and hangman (1966)» Monekoaso and Wilson (1966)» Freeman (196?)» Chisholm at &1 (l967)»Foulda et al (196s a»b# and a)» M m e l l et al (19#)» and Osimtokim et ml (1969).
29
ES$ÏGâ$M.
Til© material far tliio manusorlpt m m obtained from iAi& out-iiatient and in-patlont investigationa oarritkl out ou 65 patlontw auffer&ng from tobaooo amblyopia, oolleotad o v w a period of J yearn# The patlmte warn referred from Ophtbalmologio&I ol&mlea In tb# area of the woet&BA Regional Hospital Board of SGotlaad, prinolpally from Glasgow and Ita Immediate eurrou&&&&ga,
Being tb# criteria of Heaton at al (1958) &# & guide the diagaoole wae oo&flrmeâ on the finding of bilateral depree&lo# of viaiou, m sotuirei defeot of colour vielom, aad omtro-oaeml defooto in the field of vision, oemrrlmg in a amoklng eubjeot#
The patient ega ranged .from 46*84 yearn, all but m m were male and their tobaaco eoneumptlou lay in the range 0*5*? ozs# per week# The patiente wore informed that it wae not neceoaary to alter #mlr moking habit but five patie&te elected to abetalm from cmw#dhr&4MM& tbie was their
w #
la general, the patlmtc eought medical advice
after itoir visual symptom» had h em present for (> months or so, by which time the visual lose of both eyes was substantial. A number of the patients were ill due to ooinoiient disease and # 1» %m& categorised after investigation. In a few the coincident disease was # e reason for seeking medical advice and they had the visual complaint subseqmntly categorised*
Information about a patient’s direct vision can be obtained by examining his f om sense or visual acuity# his colour sense and his light sense* By examining his field of vision information is gained about his indirect vision* fhe patiente in this analysis of tobacco amblyopia had assessments of tWir visual acuity, colour vision and fields of .vision carried m t to confirm the diagnosis and at intervale whilst on treatment*
As the disease process does not effect the eyes equally# the visual acuity is not equally depressed in tobacco amblyopia. According to #ie majority of observera# vision is poor in sunshine# but improves in the evening or in suMued lighting* (tielson 1880# Groenouw 1892#
31
ïïarman 1904# Traquair 1930# Oarroll 1935). Thia la due to the glimmering mist which cover© all objecta, being removed with twilight mid allowing contours to become aharper, Hirachler (1071) claimed that this was ao only for large objecta and did not apply to reading*
fho distance visual acuity was estimated subjectively by mean» of Snellen’e teat iype at 6 metres (Snellen U62)* In each case the visual acuity recorded was the beet visual acuity with a spectacle correction*,
The near vision was similarly estimated using tlie notation laid, down by the Faculty of Ophthalmologists (baw 1951-52). Examination of the best distance visual acuity obtained from the 65 pairs of eyes, showed that in only 22 was the visual acuity of the right equal to th.at of the left, in 10 the visual acuity of the right was better than that of the left, and in 25 it was worse* Thu© confirming the unequal visual loss in this disease# As four of the left eyes were amblyopic from other causes (5 from long standing squint, 1 from a central retinal artery occlusion) and, as no improvement in vision could be expected in them, the rigîit eye of all patients was selected for all visual compa,risoBs*
32
The viauaX aouity'(Bncllen) was converted to percentage visual acuity (Ridley 1959)*' The visual acuity in untraatecl tobacco amblyopia was found to be within the range 1*5 - 100^ with a mean at 18^ (equivalent to a visual acuity of 6/j6 Snellen)* Of the 65 patients 21 had a Visual acuity of 6/24 or better and 44 ^ visual acuity of 6/36 or worse* The Improvament in vigual acuity with therapy is dealt with In the ©setion on treatment#
The near vision results were similarly transposed into the percentage visual acuity scale* The range for the right eye was 8 - 64^ with a mean at 20*?5# which I0 ■ equivalent to 11$ at a standard reading distance of 15 inches or 3i oms* The disproportion alluded to by classical writers between distance and near vision was not aonfisnaed (t « 0*5?I n ^ 116; p> 0*1)#
The OolQur Sense
The colour sense can be tested by various methods some of which give only a rough estimate, while others are a very sensitive index* The methods are as follows*-
(a) Colour Wamlm?% thia means a subjects ability to name correctly
3)
or incorrectly test colours will reveal gross defects of colour vision. Inability to distinguish one primary colour from another is termed gross colour confusion.
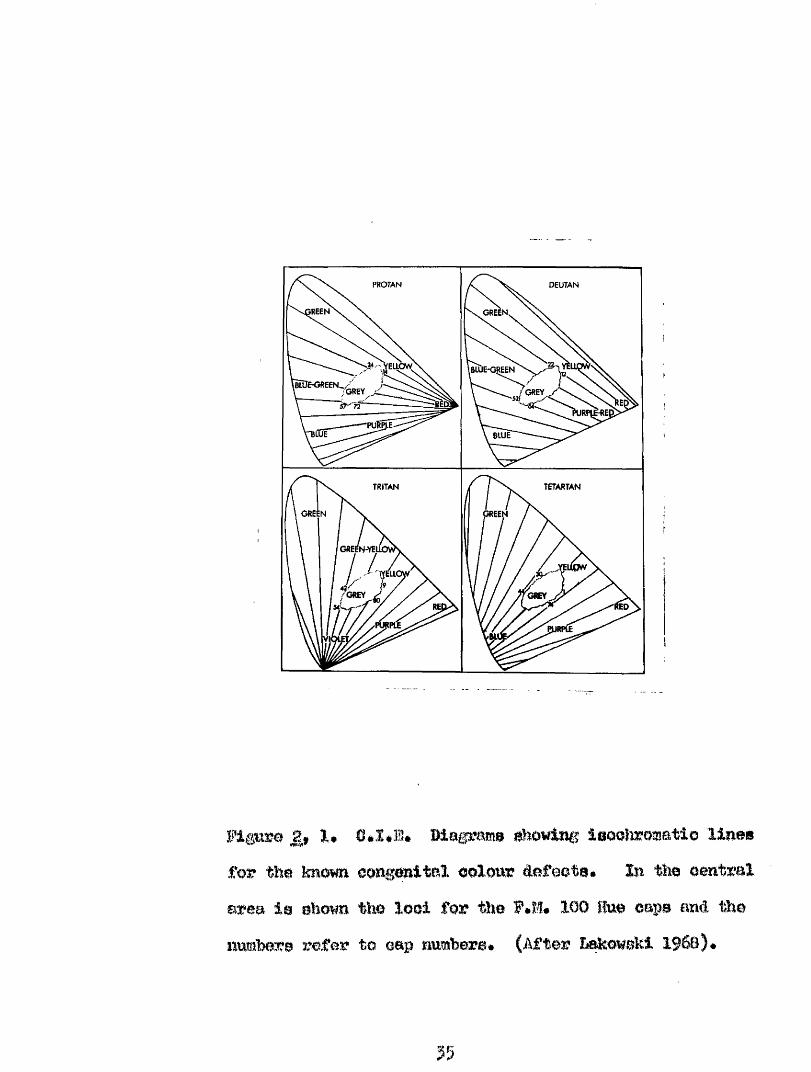
(h) Paéudo-iaoohroroatio Plates or Oonfusion Charts* These plates made up of coloured dots in which
the baokgrotmd colour differs from that of the figure (he it a number or symbol). These plates have been deliberately constructed so that the background and figure coloui's lie at different points m a known confusion asds for one of the congenital dichromats* See Fig 2» By presenting a series of appropriate plates, a patient can be quickly screened for the four congenital colour defioienoies* The plates that are available are after the pattern of Stilling (l88j), Bvorine (1955)$ Hardy- Band-Bittler (1955)$ Ishihara (1959)$ and the Tokyo Medical College (1957) •
(c) Pigment Matching Tests.These test a subject’s ability to discriminate
between colours which differ only by a small amount when viewed under a constant illumination. The Farnsworth- Hansel1 100 Hue test (Farnsworth 1945) i© a refined and Useful member of this group. The test enables a qualitative as well as a quantitative estimation of the colour defect to be carried out (Orone I96I)*
54
PROTAN DEUTAN
ÏREEN GREEN,
TETARTANTRITAN
GREEN ■EN
lED
tPlE
Map?am» iaootoomati© llnmfor %he kmmn. eongonitaX oolow #feote. %n the ©entrai area le ehown tko looi for tîio F.M* 100 Hue caps and the Rumbere refer to cap numbere* (After hekmBkt 196©)#
35
(a) ^
tests a m oarrisd out m an anomaXosoops after the pattern usei W BageX (190?) > or Fiokted and bakowskl (X9#0)# fha subjeot views a halved aperture* one half containing the test speotml oolonr* the other is controlled by the testes* Is is required to moke a colour match by varying the proportions of two other spectral colours which can balance the test colour at \momk proportions* % e Wagel anomaloscope tests for red«*green colour defects (l#e* Frotsn and Deutan)# and the Fiokford*^ ilcolson anomaloscope for red^§rcen.| yellow^hlue - (Sletartan) and green#hlue (fritan) defects* fhis is a delicate method of assesament which requires considorahle experience In its use before the Interpretation of the results are meaningful*
Defective colour vision is acquired hy patients b o m with a potentially normal colour vision syatem which has failed to reach maturity or has deteriorated after reaching maturity» because of local ocular disease» ayatemic disease or the toxic effect of ayateojically aâmiïiictcred drugs* *Bie extent of the acquired colour defect is unequally distributed between the ey#s and each eye must therefore be tested separately* A typical
36
dysohromatopsia develops from normal triohromatio vision though an abnormal triohromatio stage before dlchromatie vision is reaohedi further extension of the process will lead to monoohromatlsm and eventual blindness* Pseudo-- isochromatic plates are of little value in detecting the relatively early triohromatio stage which can be detected by the Famsworth-wMunsell 100 Hue test or by anomaloscope tests*
Disease processes affecting the neuro^sensory or conductive layers of the retina will if severe enough lead to blindness* bees severe disease will degrade visual function In a variety of ways including the development of an acquired dysohromatopsia* #us lesions of the neuro-sensory retina by and large» result in a loss of colour discrimination in the yellow^blue» or violet blue- green» and lesions of the conductive layers in the red-green areas of the spectrum respectively* (Koellner 1912»Cox i960, Verriest I96;)*
The Oolour Sense in fobaoao Amblyopia
One of the dia^iostio criteria of this condition is the finding, in the centro*#caecal area of the field of
37
vision» of depressed Bensitivity to red and green stimuli* Aooompenyiug this is a aubjeotive tiisturhanoe of colour diaarimlnation which traditionally reveals itself by the confusion of gold and silver coins, or today, hetwem copper and cupro-*niohel* Qalejsoweki {IBBJ)' w&s first to draw attention to the subjective colour defect in tobacco amblyopia arid ©roenouw (I0f2) pointed out that this acquired dyacîiromatopsia differed from tlmt of the congenital diohromst* In more recent times Riddell (1936) observed that with treatment the colour sense in tobacco amblyopia took much longer to return to nomal levels, if at all, than did visual acuity* Box (i960), Francois and Terriest (1961) Saraux et al (I966), Bouniq and Cfoaoaa (1966), observed that the dyechrcmatopsia found in tobacco amblyopia had features in common with other toxic amblyopias#
Of the teats available for investigating the colour aenae, the Famstwrth Mmmall 100 Hue Tost was found the most useful in the investigation of the tobacco amblyopia patients* fhe test conaiets of a graded series of 05 coloured caps mmtigéâ in four boxes# The patient la required to arrange the colour caps into a regular colour series between fixed end caps# He is presented with the
38
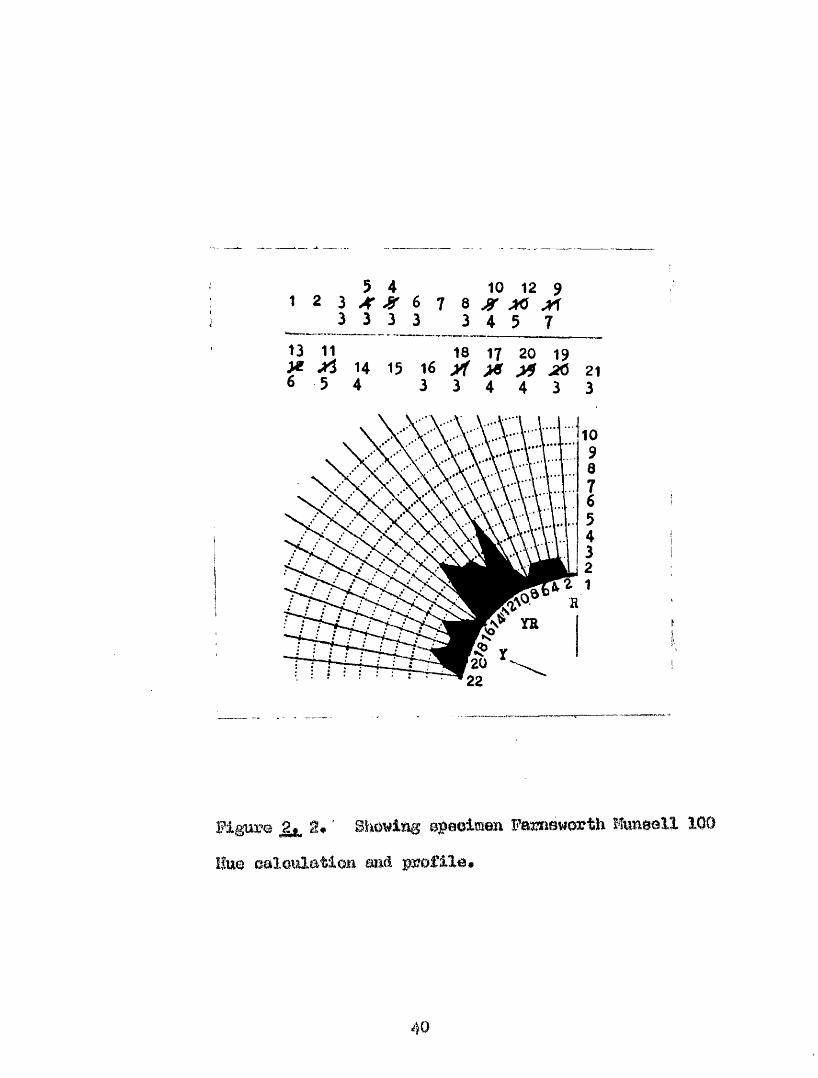
oolourad caps arranged in a etaoclard rmdem fashion*Bach cap Is mimhered on its reverse aide* The patient* 0 arrangement of the caps is recorded on a chart, (fig 2.» 2) » and deviationa from the normal arrangement are soon apparent* As the caps are numbered, the error of m y
particular cap is obtained by summing # w differences between the cap number of the cap in question and the cap mmber x hioh comes before, and the cap which comes after it* If the patient’s arrangement is normal the minimal aiTor score for any cap ia 2# Two is accordingly deducted from Individual cap scores and the sum of these individual error acores gives the total raw score* The individual emror score ■ of the cap# may also be expressed graphically as the patients profile*' (Fig*^, 2)#
fhia teat was originally deaigïied as a binocular test, for the screening of youthful subjects for congenital colour defect, end a time limit of 2 minutes was placed for the completion of each box* This routine required amendment fbr the investigation of the dysclwrnatDpsla of tobacco amblyopia* Booh eye was examined separately, and no time limit wae set for the completion of each box as the patients being tested were elderly# many had defective
5 4 10 12 92 I J( » i, 73 3 3 3 3 4 5 7
13 11 18 17 20 19X ^ 14 15 16 X >«f ^ 216 5 4 3 3 4 4 3 3
Piguw g. ' Showiflg Bpeoimen Farnsworth Hwnsall 100 Hue caloiûation sa& profile»
40
vlelom and had dlffloulty in manipulating the oape# Standard artlfioiai illumination waa provided by a îlubble Verl ?idl oabinet wMoh provided artificial dayli^it illumination with a colour t#%p#):atur# K with anintensity of 1200 *1290 Imc at the teat cape» thus oonforaiing with l#Bè 950 part one (19^7)4
The materials used in thie teat come from all parte of the ootom circle and hue diaorimination near the - centre of the colour epaoe can be tested in all diraotions* O m o f the great merits of the Farnsworth Mtmsell 100 Hue test is that elements suitable for detecting colour confusion om also be used for detesting the variations in colour clisorlmination existing among triohromatio observers, (Hg« ^ %)# to be able to measure these variations tasks presented for discrimination must inelude small oolour differenees ( a B) suoh as are found In this tost* whore A B between suooessive oaps is of the order 2*5 units (ifetion Bureau of Stmdards). The task hero may be considered analogous to visual aouity testing (Wmwaki I9G8)# Subjests with aomto colour discrimination will arrange the % olour series” in each box within the two end lim its oorreotly, tliLOse with lessor discrim ination
41
will accumulate ”error scores" which are a ipcssure of the degree of displacement from the ideal arrangement.
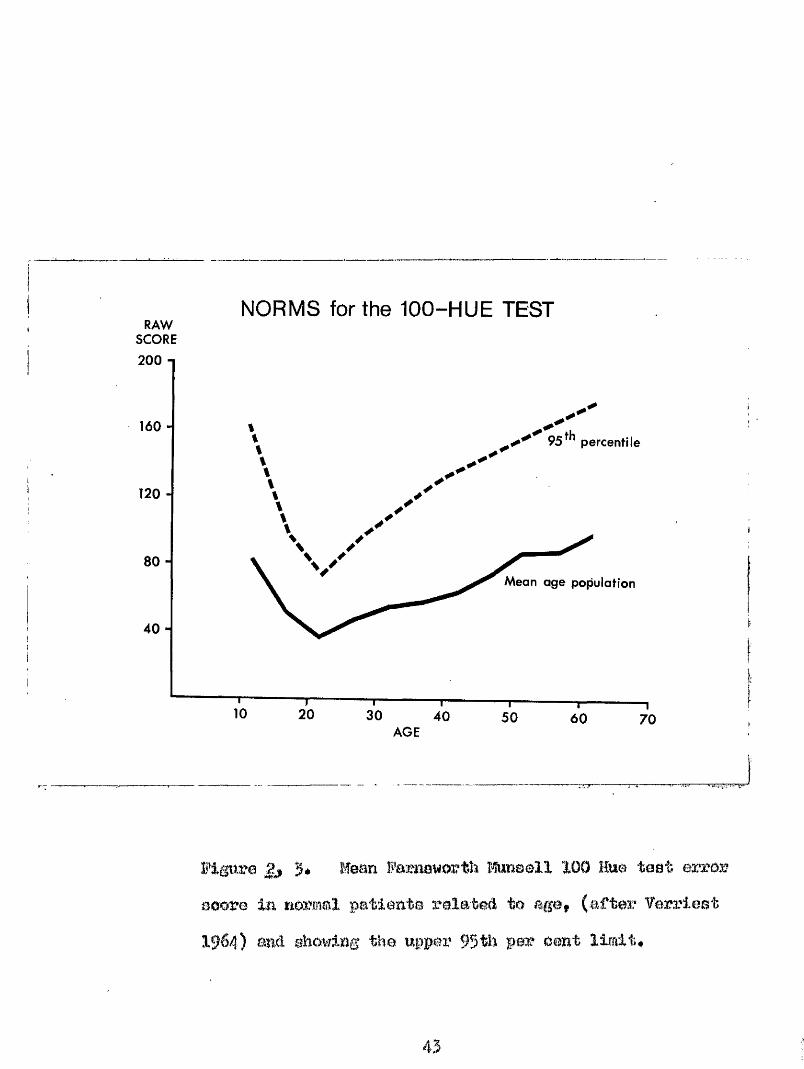
Terriast (196)) demonstrated that in normal healthy subjects the error score of the Farnsworth Himsell 100 Hue test increased in a positive manner with age* after 20 years of age* (Fig# 2# ?)♦ ^his was in agreement with the earlier finding of Imkowski (1958) who described distinct phases in the normal development of colour vision* Colours are perceived and discriminated most accurately between the ages of 16 and )5 years* After 55 years there is a rapid deterioration in ability for fine colour discrimination* Hed*green discrimination is least affected by age* but yellow#b?.ue and violet blne*#green discrimination may deteriorate from as early as the JOth year* lakowski (1962) produced evidence that these observed deteriorations in colour discrimination were due to retinal rather than pre*retinal changes#
Bach patient performed the Farnsworth Munsell 100 Hue test on more than one occasion prior to the commencement of treatment* The error score for the right eye of each patient is presented in this analysis. For the 65 patients* prior to treatment the erxror score lay in
RAWSCORE
NORMS for the 100-HUE TEST
200 1
95^^ percentile
120 -
80 -Mean age population
40 "
20 30 40 50 60 70AGE
Figaro 2 3* Mean B'arnavortîî îteaall 100 Mae taat error aoore in normol patienta rolateA to age, (after Carriest 1964) and showing the upper 95th par oant limit*
43
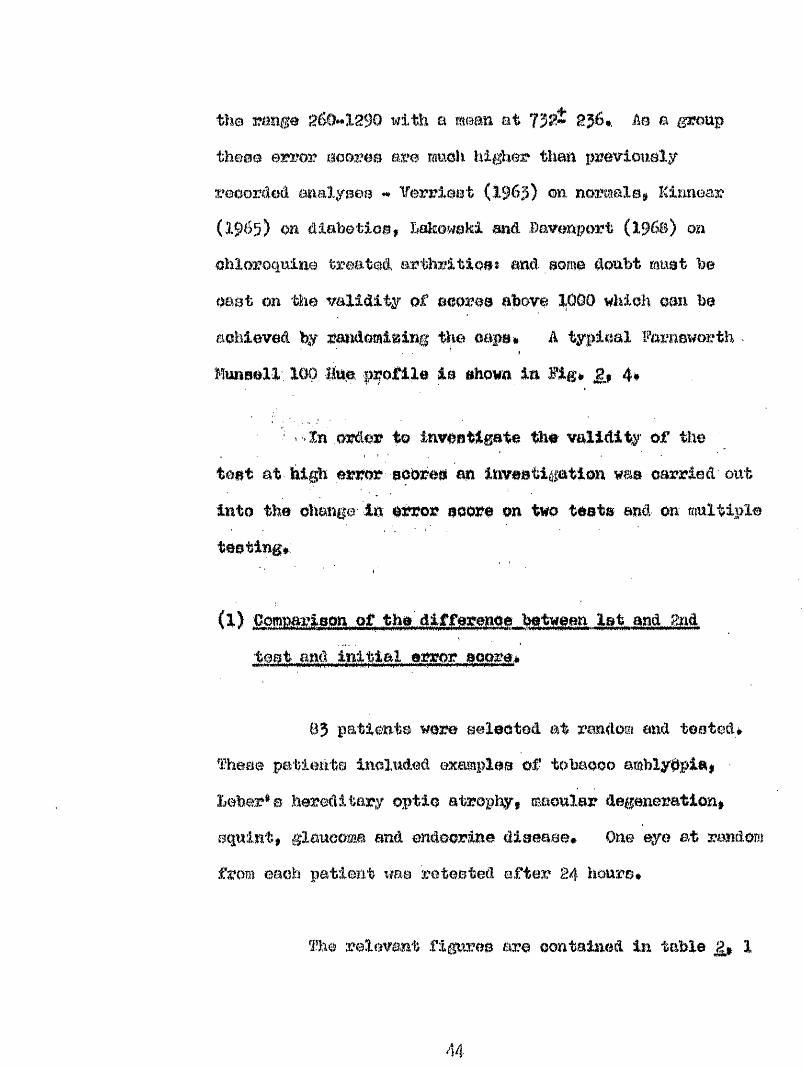
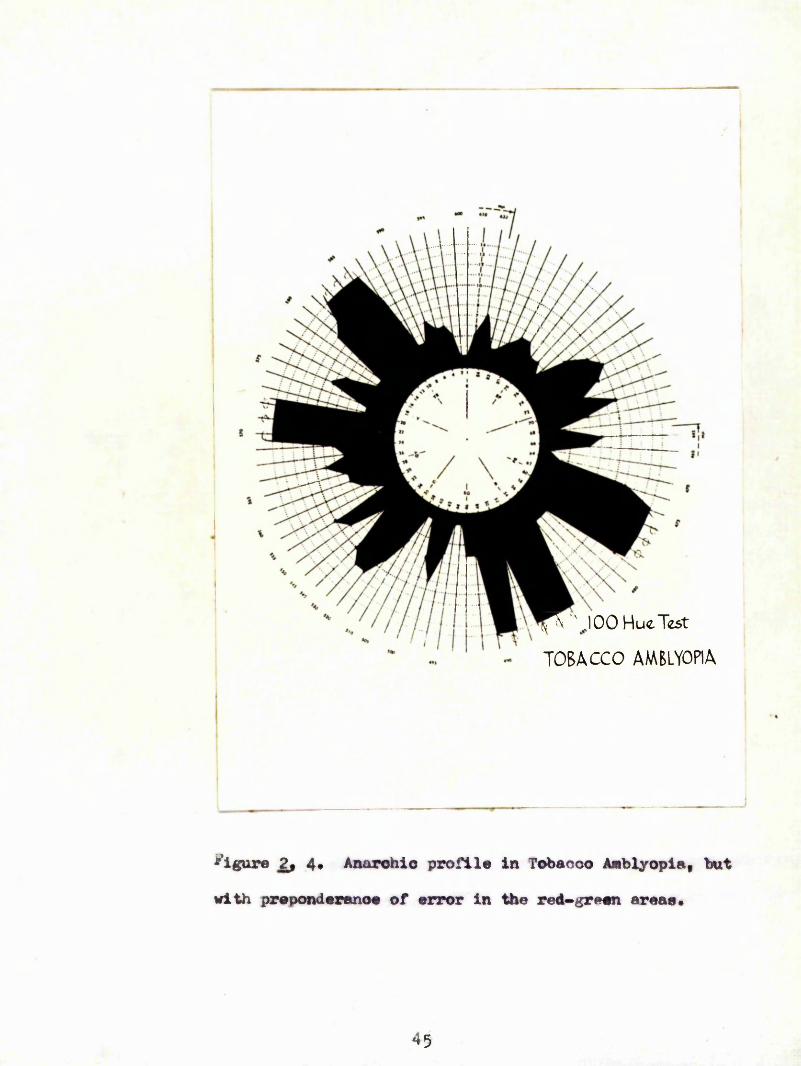
the mmge with a mean et Ab a grouptheme error eooree are mmoh higher them, preirioualy reoorêeâ aumlyaea Verriaet (196 ) mi norfaaXe Kimiear (19^5) on diahetioB, Xakowokl m%à Davenport (i960) on ohlorogulne treated arthrltioa: and aomo doubt meat be oaat on the validity of sooroa above 1OÔ0 which can be achieved %' randomizing the cape# à %plcal Farnaworth . Munaell'. 1#, Hue profile ie «hown in Fig# gj 4#
' ' -In order to invoatigate the validity of the teat at. high error eo&re# m investigation wma carried' out into the change- In error soore on two teats and- on multiple teating#;
(1) CommrWon of t M W W m let and gndteat .and initial error j core#
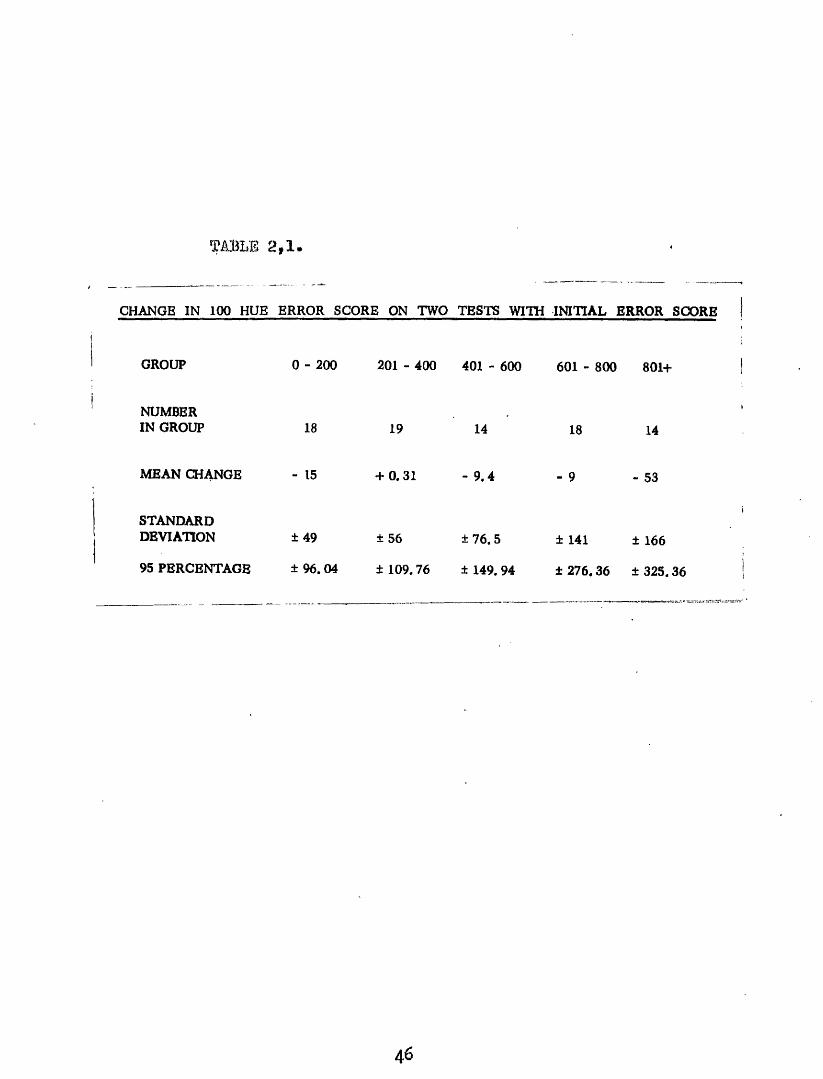
03 patienta were selected at random and tea ted* Theae patients included examples of tobacco amblybpia# ■ heber* e hereditary optic atrophyt macular degeneration^ squint, glaucoma and endocrine diaeaee* One eye at random from each patient use reteated after 24 hourG*
The relevant figures ore contained in table 1
44
* 1»
\,J 0 0 Hue Test
TOBACCO AMBLYOPIA
figure 2j 4* Anarohio profile in Tobaooo Amblyopia, but with preponderance of error in the red-green areae.
45
M L S 2,1.
CHANGE IN 100 HUE ERROR SCORE ON TWO TESTS WITH IN ITIAL ERROR SCORE
GROUP 0 - 200 201 - 400 401 - 600 601 - 800 801+
NUMBERIN GROUP 18 19 14 18 14
MEAN CHANGE - 15 + 0.31 - 9 , 4 - 9 - 53
STANDARDDEVIATION ±49 ±56 ± 76.5 ± 141 ± 166
95 PERCENTAGE ± 96. 04 ± 109.76 ± 149. 94 ± 276. 36 ± 325. 36
46
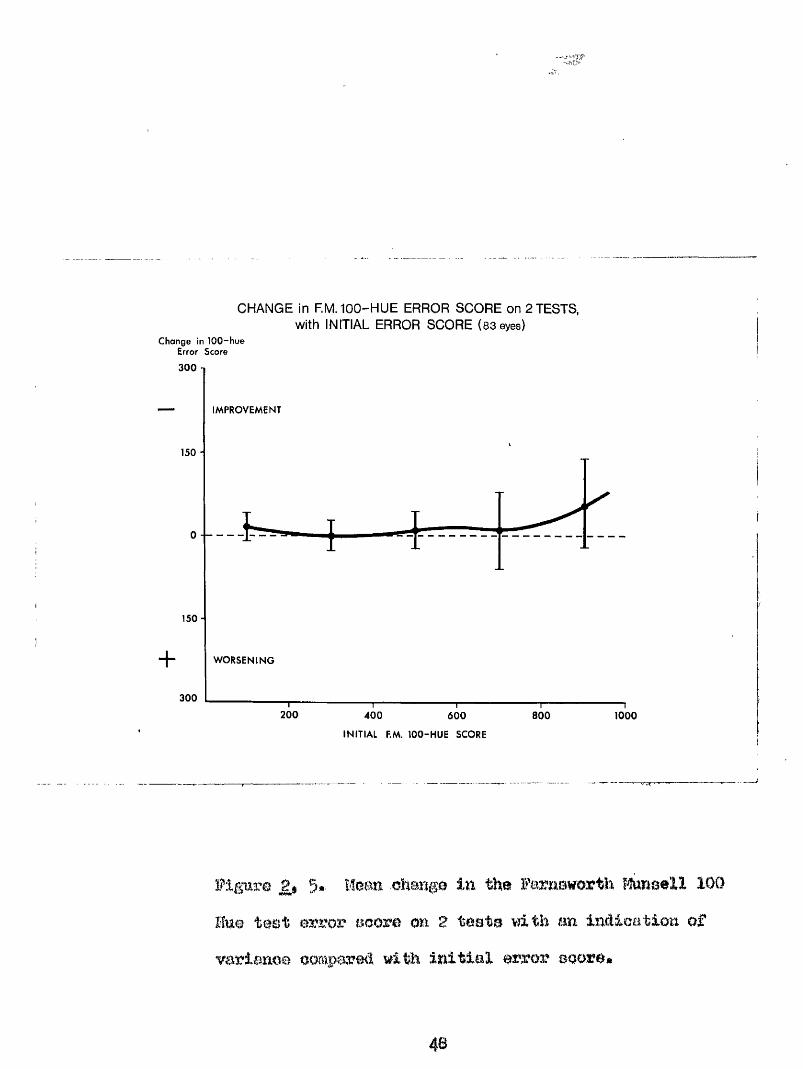
and figure 2 5* As crni be seem lu Figure 5# at error eooree above 601 there appears to be a trend towards spoutaueeme Improvement on retesting* However, the mean change in error score In this group m in each of the other groups is not aIgulflearntly different from the expected value of zero (60I#B00; t «* 0*27, n *» 17# P>0*1î 000+1 t 1*19, u ^ 13, p> 0*1)*.
With increasing initial error score however* there is an imreaeed scatter of remit»* the inoreaee in variance being statistically oignlfioant only for teste at erkOr score» of over 600* (601^a0C% W m 2*B7, p<0*0g; 001+* F « 3*90, p<O,05)* fhero is no. evidmoe to support the premise that repetition of the teat improves performance.
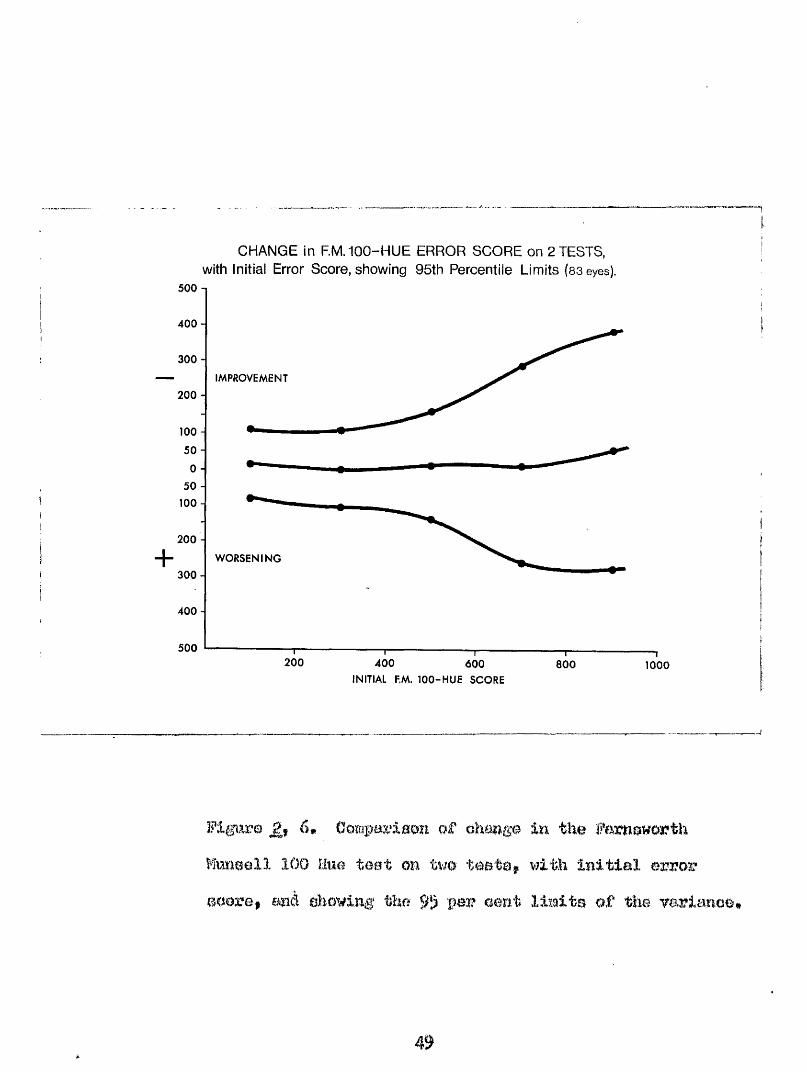
From these figures one can deduce by how much the error score at each particular level must change to beregarded as a aignifioant alteration in the result of the teat* fhi» is illustrated in Figure £, 6* Here the 95# range about the mean is shown* A cimnge In error score lying outside theae limits would Imve m one in twenty probability of arising by chance and would therefore be significant# Fox* example, with mi initial error score of 130, on retest a score of 39 would be a significant
47
CHANGE in RM. 100-HUE ERROR SCORE on 2 TESTS, with INITIAL ERROR SCORE (83 eyes)
Change in 100-hue Error Score300
IMPROVEMENT
150 -
0 - —
150 -
+ WORSENING
300
200 400 800 1000600
INITIAL P.M. 100-HUE SCORE
figure 5.. M e m ehmga in the ftoBell 100Hue te&t error score on 2 teste with tm indication of variance oompored wi# initial error score*
48
CHANGE in RM. 100-HUE ERROR SCORE on 2 TESTS, with initial Error Score, showing 95th Percentile Limits (sseyes).
500 -1
400 -
300 -
IMPROVEMENT
200 -
100 -
50 -
50 -
100 -
200 -+ WORSENING
3 0 0 -
400 -
500200 400 600 800 1000
INITIAL P.M. 1 0 0 -HUE SCORE
Flgtirm 6# Compwiaon o f eh&mge in the
Mmeell 100 Hue teat m U m teeta, v?ith iBitiaX e-x;voweoore, mid ehoving the 95 aent limite qf the varianoe*
improvement ÿ or a aoore of 251» a signifioant deterioration j similarly at an initial error soore of 700, a fall to 415» or an inorease to 967 would be significant*
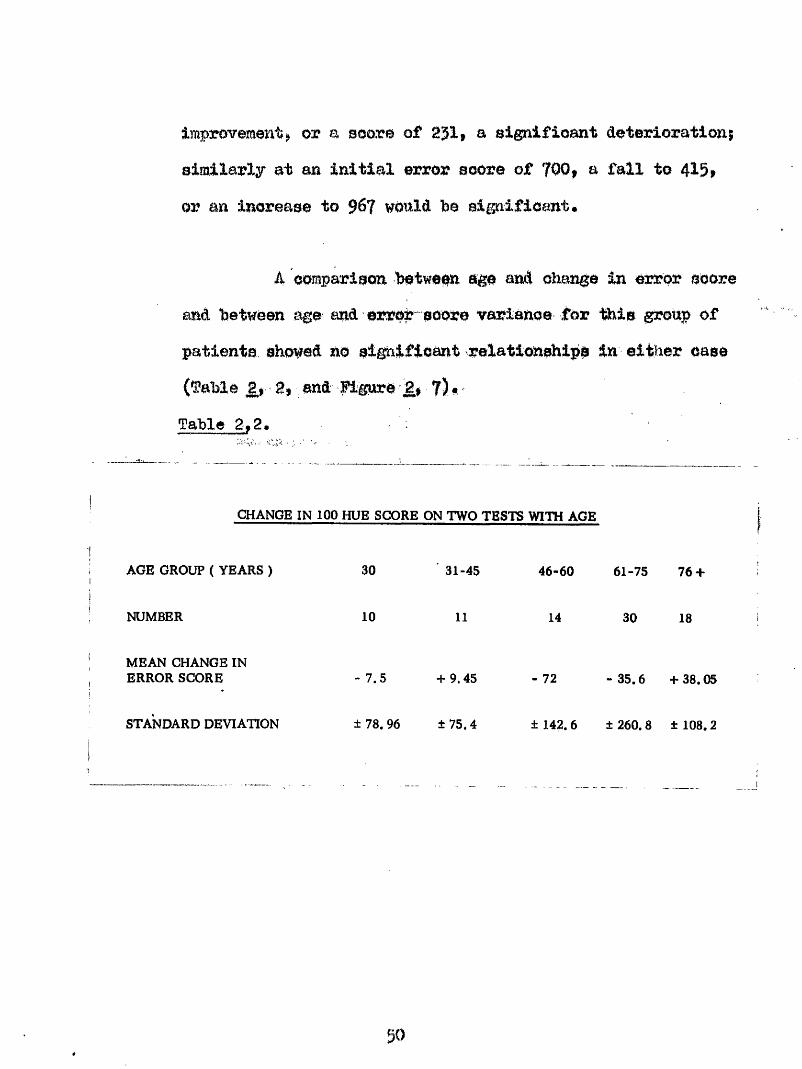
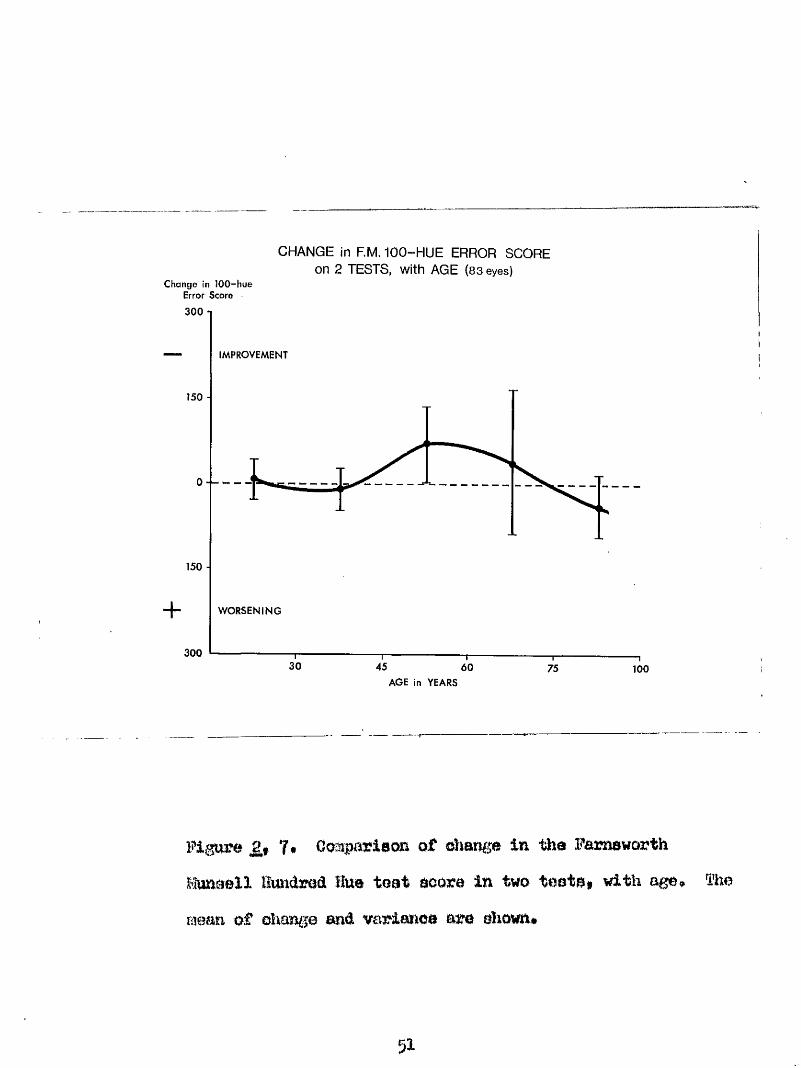
4 comparison between age and change in error score and between age and error soore variance for this group of patients showed no significant relationships in either case (fable 2.1 2, and Hgure 2, 7) *Table 2,2#
CHANGE IN 100 HUE SCORE ON TWO TESTS WITH AGE
AGE GROUP ( YEARS ) 30 31-45 46-60 61-75 76 +
NUMBER 10 11 14 30 18
MEAN CHANGE IN ERROR SCORE - 7.5 + 9.45 - 72 - 35.6 + 38.05
STANDARD DEVIATION ± 78. 96 ± 75.4 ± 142. 6 ± 260. 8 ± 108.2
go
Change in 100-hue Error Score
300
CHANGE in RM. 100-HUE ERROR SCORE on 2 TESTS, with AGE (83 eyes)
150 -
150 ■
+300
IMPROVEMENT
WORSENING
— I—30
—T-45 60 75 100
AGE in YEARS
Figure 7. Coapaïlaon of oliange in the Parneworth Munaell Hundred Hue teat aoora in two teats, with age, îhe mean of ohange and variance are shown*
51
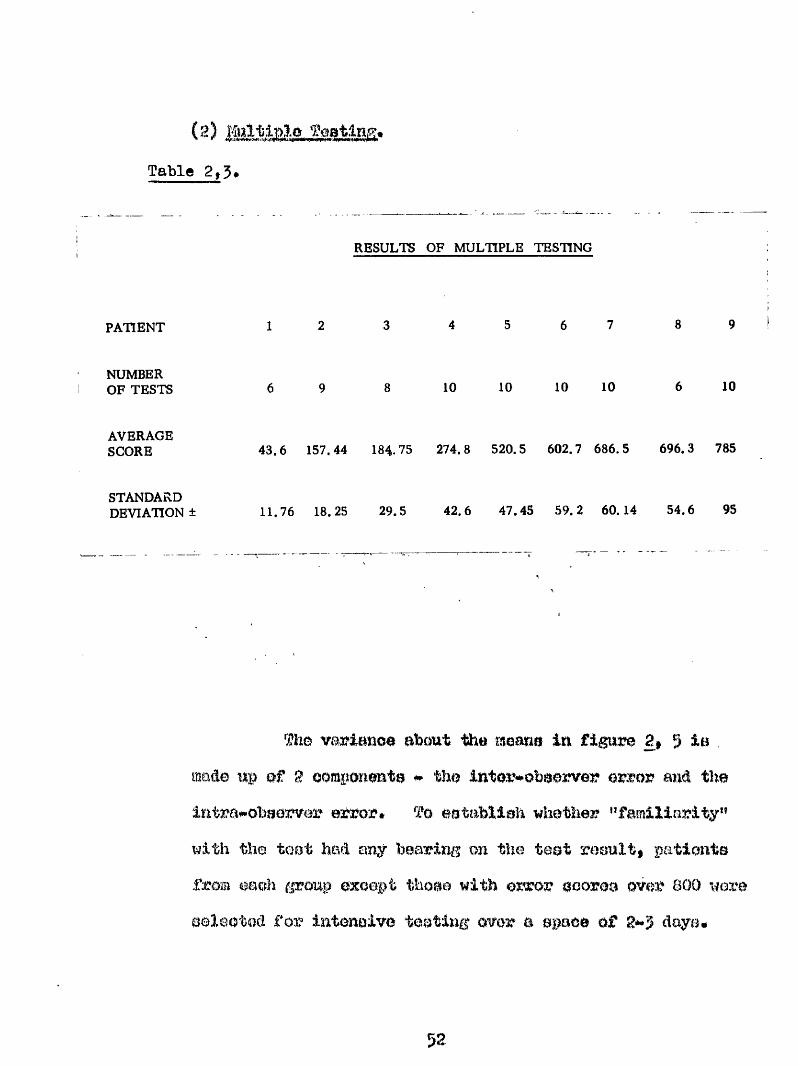
(2) Table 2,5,
RESULTS OF MULTIPLE TESTING
PATIENT 1 2 6 7 8 9
NUMBER OF TESTS 6 9 10 10 10 10 6 10
AVERAGESCORE 43.6 157.44 184.75 274.8 520.5 602.7 686.5 696.3 785
STANDARD DEVIATION ± 11.76 18.25 29.5 42.6 47.45 59.2 60.14 54.6 95
Th© variance about the moane in figure 2, 5 inmade up ef 2 oomponeute * the inter-obeerver error and. the intrawobeerver error» To eetablieh whether "familiarity" with the toot had any bearing on the test result, patients from each éP oup except thoae with error ocorea over 800 wore selected for intonolvo toatiug owr a space of 2**3 doye»
52
INTRA-OBSERVER ERROR Compared with ERROR SCORE (9 patients)
Variance
120
90 -
60 -
30 -
0 200 400 600 800AVERAGE ERROR SCORE
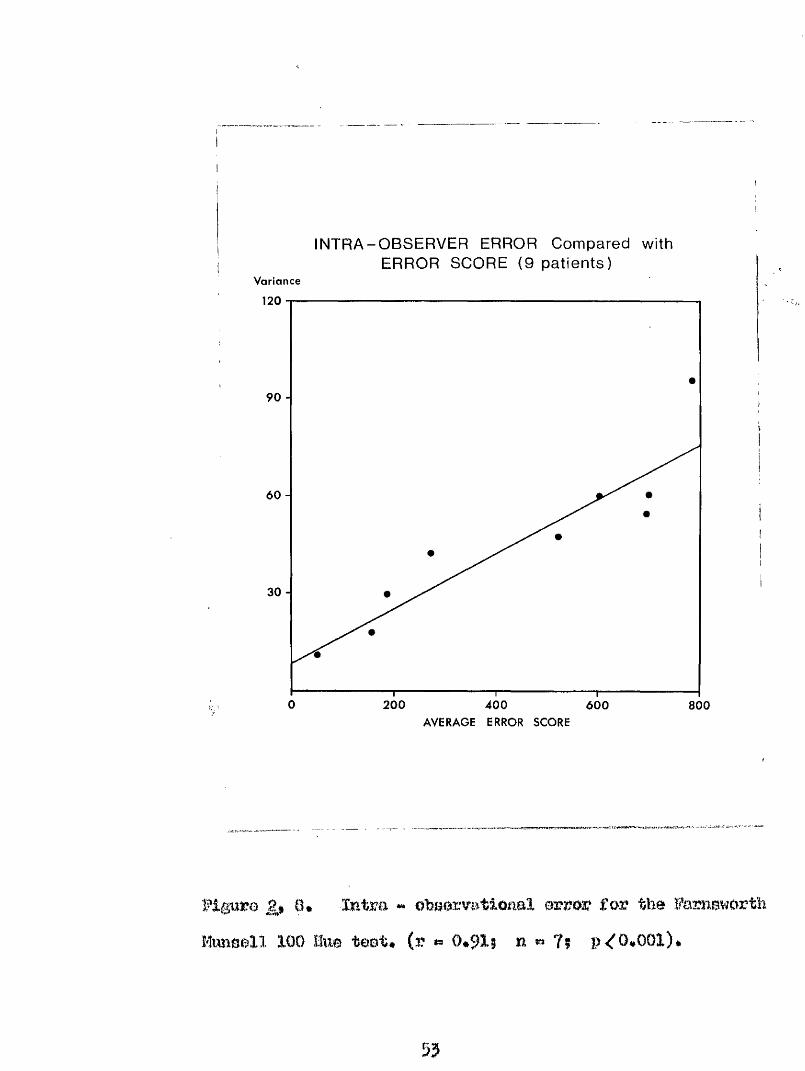
^*0* -Intra ** obriorvatlonaX for the FarnsworthMimaoXl lOD Hue teat# (r 0*915 n » ?? 0*001)*
55
In these teats the same eye was m m i m â ou each oooasiou*For this analysis the aoatter of the results about the mean error soore was useâ* The results are shown In table £t )#In no ease was there any inclieatien that repetition influenoeâ the patient*B performance.
à comparison of the average error score with the error soore varianee for each patient# shows a significant positive relationship (r # ###1, n # 7, p < 0*001)» (Figure 2# S)« As this variance is a measure of the tatra observer error# it can be seen that this quantity increases with error score* The difference between this variance and the variance found on two tests is a meaanre of the inter observer error# 1.0» error inherent in the test. This also inoreaees with error score.
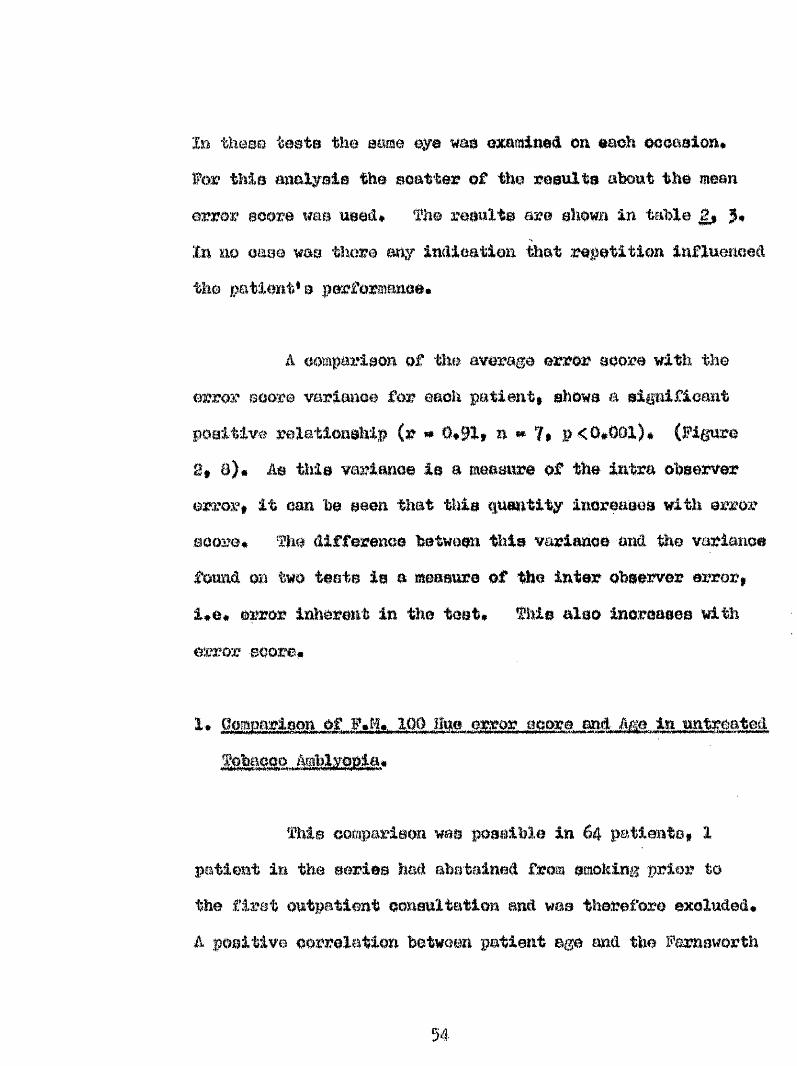
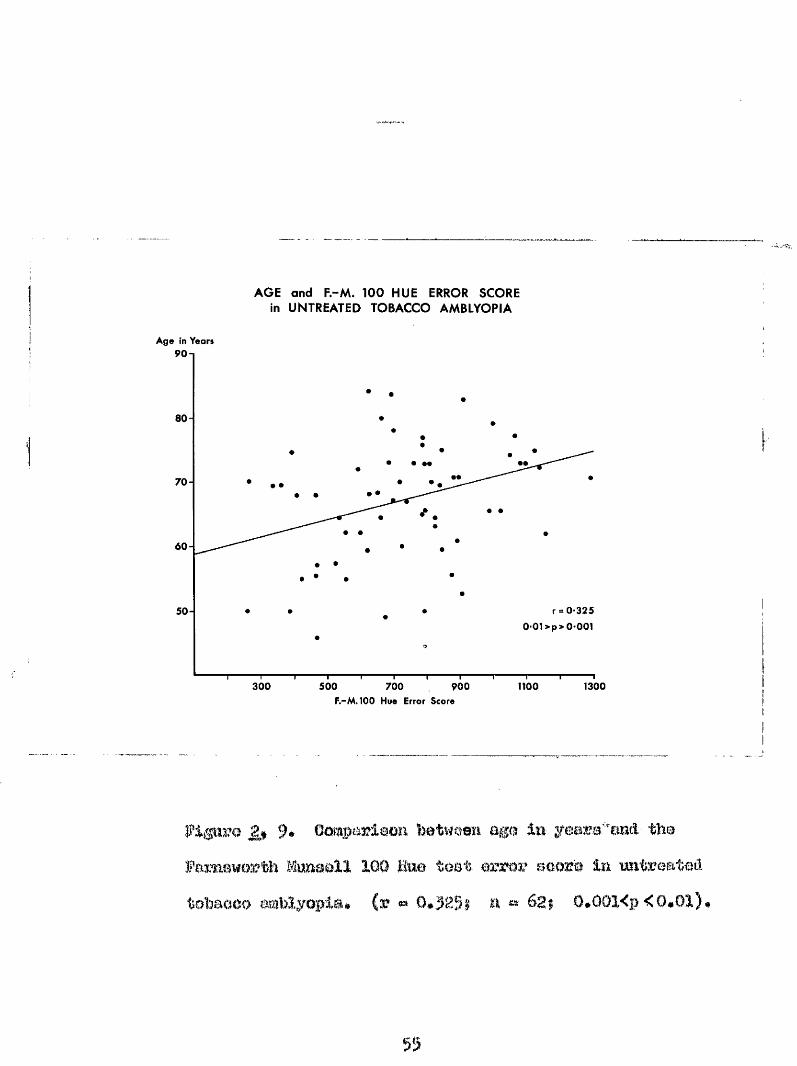
fhie comparison was possible in 64 patients# 1 patient in the saris© had abstained from smoking prior to the first outpatient oonanltatlon and was therefore excluded, à positive correlation between patient age m ü the Farnsworth
54
Ago in Years
AGE and F.-M. 100 HUE ERROR SCOREin UNTREATED TOBACCO AMBLYOPIA
90 n
80 -
7 0 -• #
6 0 -
r = 0-3250-01>p>0'001
50-
300 500 700 900 1100 1300F.-M. 100 Hue Error Score
9* Gomparlaon hetwoen age in yeara/'emâ' the Pamaworth U m B ù ll 100 Mme teat error aoore la mtreated totoaaao amblyopia# (r «» a 68$ O*O01<p <0#01)#
55
ïteisell Hundred Hue teet result was obtained in untreated tobacco amblyopia which was significant (r *» 0*525$ n « 62| p ffi»<0*0l)* (Figure^, 9)#
2• Comparison of ?#M* 100 Hue error soore and visual acuity in untreated tOobaoco Amblyopia*
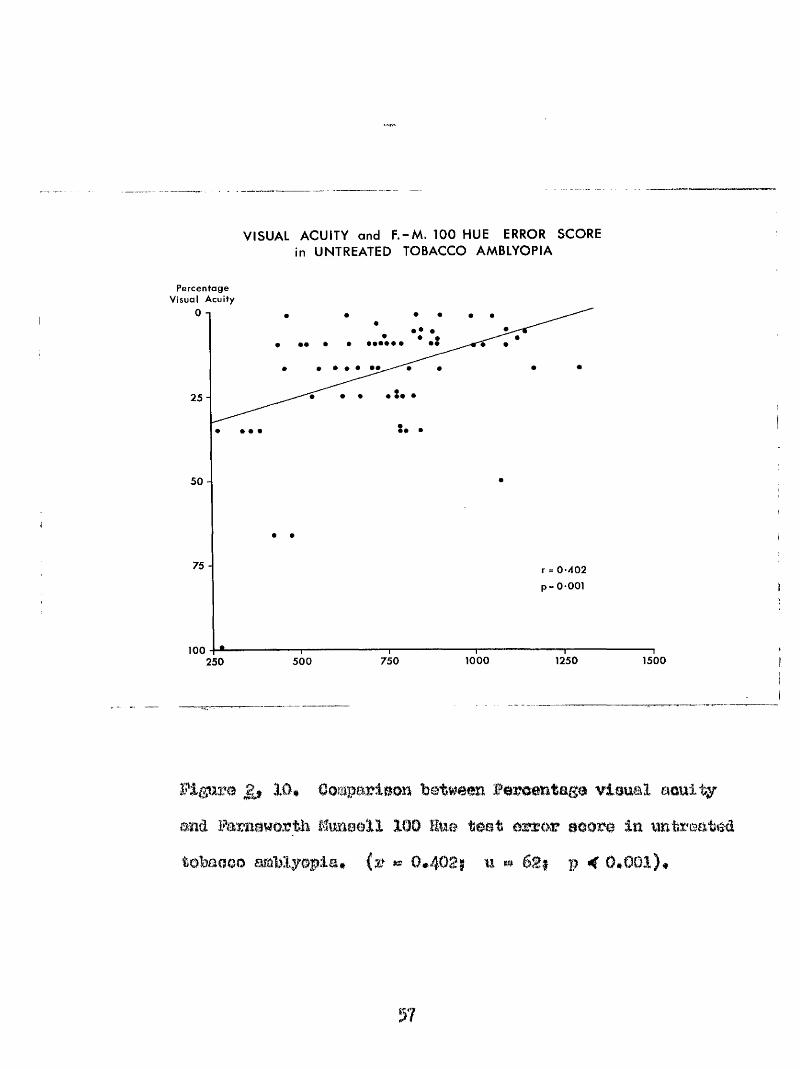
%is comparison was possible in 64 patients* A positive correlation was, obtained which was significant (r ea 0*4^S| n « 625 p ««<O*O0D* fh© visual acuity ^ in this comparison was ©stressed as a percentage taking 6/6 Snellen as lOC^ after Hidley (1959) (Figure 10)*
3 • Comparison of f *M* 100 Hue error soore and duration of symptoms in untreated Tobacco Amblyonia*
The comparison was carried out on 5I patients whose duration of symptoms was definite* A positive correlation between these 2 factors was obtained which was just significant* (r *# 0*242$ ni*» 49; 0*3>p>0*05)* Thuspatient® with a long history of visual disturbance tended to give a poor result on odour vision testing*
56
VISUAL ACUITY and F .-M . 100 HUE ERROR SCOREin UNTREATED TOBACCO AMBLYOPIA
percentage Visual Acuity
25 -
50 -
75 - r = 0 -402p= 0-001
10012501000 1500750250 500
Figure 10* Oompurleon between fereantaga visual acuity and Faraawortb fômaell 100 Hue teat error eoore in untreated tobacco amblyopia# (r «« 0*402; u # p < 0*001),
4* gomcarlBom of 100 Hue error acore and serum vitamin B12 oonoeatration in imtreated tobaoQo mblyepla*
fhia gomparlaoa waa carried out on 60 patients*A positive correlation was obtained but this proved not to besignificant* (r » 0*l6l| n * 58; p > 0*l)*
5* Qomoarison of F%M* 100 Hue error soore and serum folateconcentration in untreated tobaooo amblyonia*
This comparison was carried out on patients*A positive correlation was obtained which proved not to be significant* (r « 0*166; n *« 49; p> 0#l)*
The Field of Vision*
The investigation of a patient*® indirect vision is carried out by examining his field of vision* This can be accomplished by several meansi*
1* Kinetic. Examination of üeld bf Vision*.
(a) The confrontation test is simple and easily applied* In
58
its execution the obsemrer teats the range of the patient*® field of vielOB by that of his mn* The ohaerver and patient ait opposite each other at about one metre apart# a hand or test object Is introduced in the mid plane between opposite eyea# %#en the test object cornea into view the position is noted. The test û m be repeated in as many meridians as neceeeary* It 1# of value in examining the field of vision In. children,
(b) à well established method of delineating the field of vision accurately is by perimetry* The perimeter consists of a half sphere# or rotatable arc revolving around a pivot in order to teat varimîs meridians* fhe arc of the circle is approximately concentric with the retina* The patient with one eye occluded# fixes a stationary central mark at a distance of § of a metre* The test object is moved in from # e periphery until it ie seen* By using teat objects of variable else and colour#but of fixed lumlnmce# and with e oonstont background illumination# the boundaries of those areas of the retina just semitlv# to the given tWeshold a m determined, The linm joining points of equal sensitivity ere called isopters* (Groencuw 1093)*
(o) % using a somewhat similar teclmiqu# the central area
59
of the visual field {2(P aro’uud fixation point) oan be mrMfThirnl m the tangent soreon % oampimetry* The patient site from the soreen at m e metro or two metres distance*Th.0 ooroen over which the toot objecte are moved is flat# and m the mode of projection ie taii iontial# a certEîin arnomit of magnification of the defecta ocmiro which la not 30 in perimetry* The central# oeatr<.>**oaeoal and Mind apot areas can bo itnveatigatod very aoenrately by tills moons*
II* .Po: lT%etry
Quantitative Perlmtry (Bair 1940* %rmo 1952) or light sense perimetry (Sloan 1939) or static |>orim0try ( Fraïikcnhauser and Schmidt 1950) la carried out by moacuringtlio va ria tion o f luminance o f the tos t object to 'produce
recognition at a serloa o f fixed locations in the f ie ld o f
vision* The entire vicua l fie ld oan foe explored from the
contre to periphery in e m m W r of d iffe re n t meridians# and by nsing a mnios o f tost objecte o f d if forent oiiîo ono oan
accurately raeasnra both the density and extent o f a ecotoma,
The apparatus conolots o f a I'iemi-aphoricol bool* Tho
patient*a eye le located 33 oontiiaotroc tmm this sphere* The
60
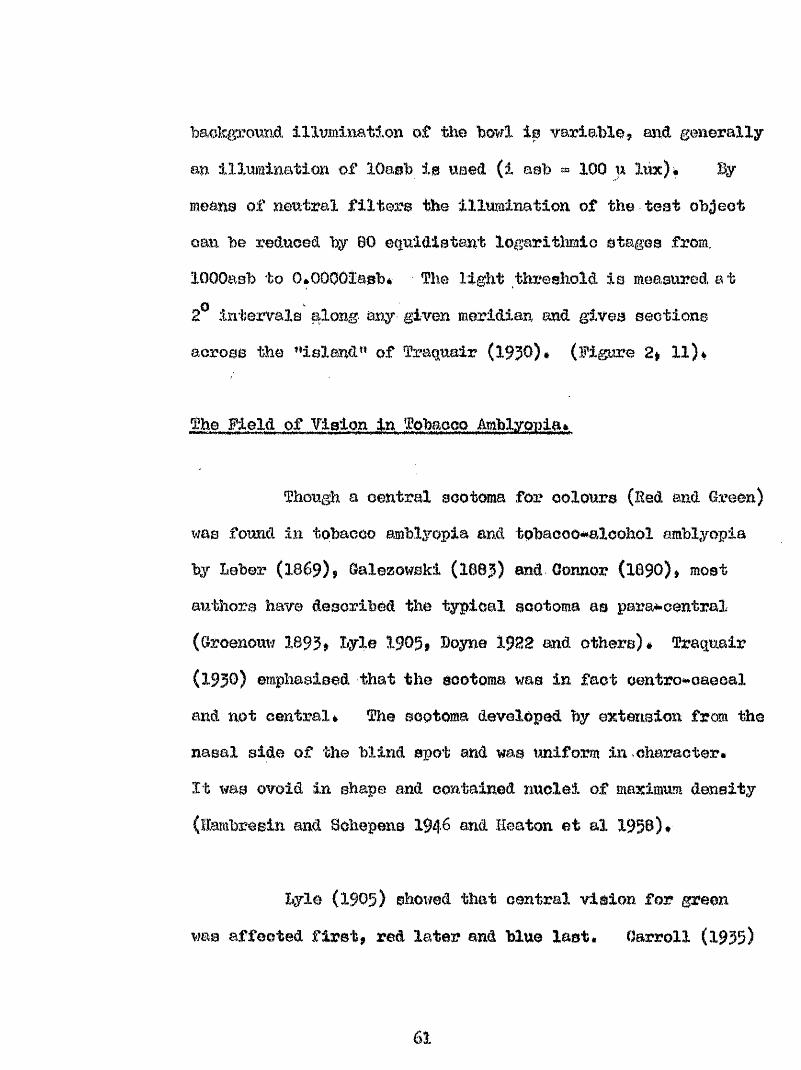
baokgazoimct, Illumination of the howl is variable# and generally an illiminatlon of lOaeh I0 used (l ash « 100 n lux)* By means of neutral filters the illumination of the teat object can be reduced by 80 equidistant logaritiimlo stages from, iOOOasb to 0*00001asb* The light threshold is measured at 2^ intervals along any given meridian and gives sections across the ’ island” of Traquair (1930)* (Figure 2# ll)&
The Field of Vision in Tobacco Amblyouia*
Though a central scotoma for colours (Red and Green) was found in tobacco amblyopia and tpbacco^aloohol amblyopia by beber (1869)# Galezowskl (1683) and Connor (iGgO)* most authors have described the typical scotoma as para**oentral (Oroenouw 1893# Byle I905, Boyne 1922 and others)# Tracxuair (1930) emphasised that the scotoma was in fact centre#caecal and not central# The scotoma developed by extension from the nasal side of the blind spot and was uniform in character.It was ovoid In shape and contained nuclei of maximum density (lambresin and Sohepens 194& end Heaton et al 1958)*
Byle (1903) showed that central vision for green was affected first# red later and blue last. Oarroll (1935)
61
Leuchtdichte: Farbe: Durchm.: asb X ^ m ln IMeridian: —|—Name: Dal.:
a LAPriifp.: VIsus:
FIxlerp.:
Umfeld:
Dlagn.:
Korn:asb
0,32
100IISISOSOD(30
320«0300•to100
1000
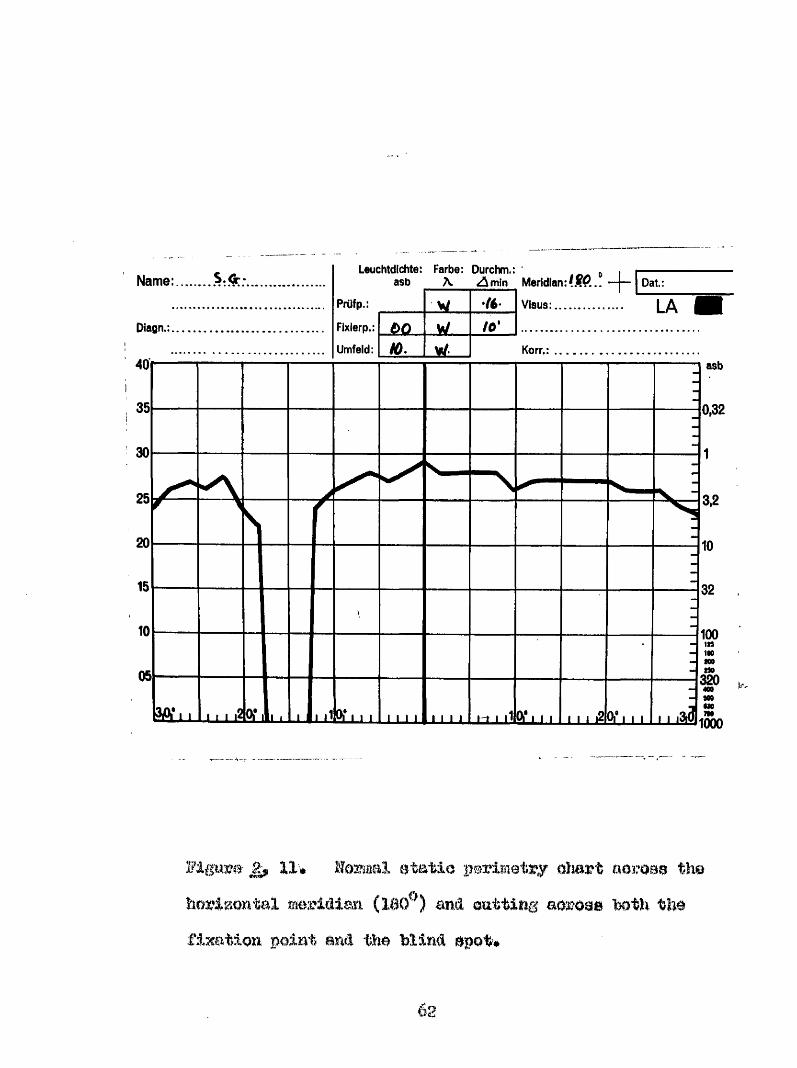
M g u m - II# Ite a a l s ta tio perim etry o M rt aeme# the
horizontal meridian and outtirig aaroais W t h thefixation point and the blind epot#
62
foimd dentro'-'oaeoal eootomae» that for red being larger thaâ that for bine) and Heaton et al (195B) ohowetî that the eoototna was bilateral) larger for oolonr than white# and aocompanled hy a temporal conatrietion for oolour#
ïihrane (1959) found th# following distribution ofscotomata* oonfluent with the blind spot in 71; half way between blind spot and fixation point in 18$ maximum central In 0* Boxmi<x ^nd Coeoae (1966) found almost an equal distribution between central and centrooacioal aootomae* According to Hhthoff (1886) the margin of the scotoma in the most severe cases may enoroaoh into the periphery of the field and de Schweinitz (1922) found tWt the periphery of the field of vision was not always intact and defects could bo found if the tests were carried out under diminished illumination# lîambrosln and Schepene (1949) held the view that the scotoma of tobaooo amblyopia and that of tho hereditary optic atrophy were similar a,îxd they raised the question that the aetiology of both conditions was similar#
The patiente in this analysis had examinations of their field of vision carried out by campimotry «md static perimetry#
#' RA
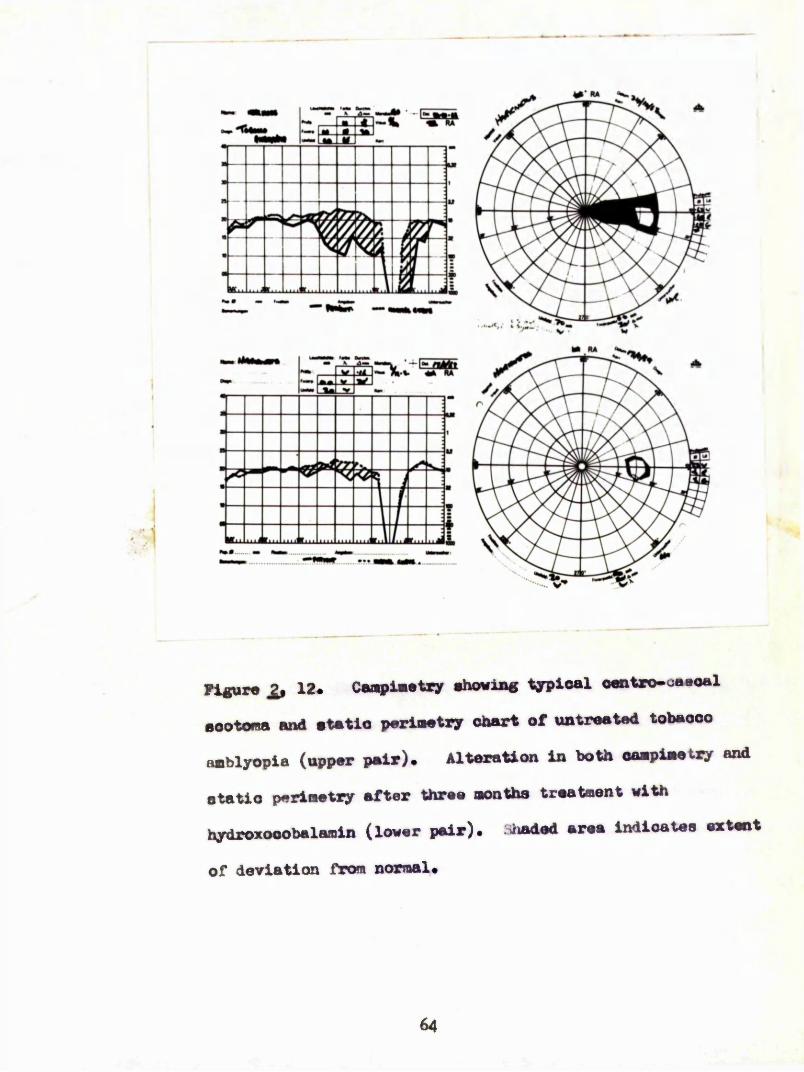
M RA
ytgure 12* Cai^lmetzy abowine typloal oant»o-o«»o«l sootona and atatio parlmatqr chart of uatroatsd tobacco amblyopia (upper pair). Alteration in both oampimetry and
,tatic periaatiy after three months treatment with hydroxooobalamin (lower pair), shaded area indicates extent
of deviation from normal*
64
(a) î5xamination of tho oenWai area of the field of vision revealed topical oentro*saeoal soatomas before eaoh eye in wMoh the defect for colour was larger than that for white*In most patients the scotoma extended some way frm the blind spot towards the fixation point# and in some# included the fixation point* Figure 12 shows a typioal example*
(b) The types of defect detected by static perimetry fell into 2 main categories and were similar to those described by %ingirian and Hivara (1965)* The first type of defect is a relatively uniform slope and was present on examination of 8 eyes# the second is similar but the slope is interupted by a tooth or spike in the juxta caecal area and was present in 52 eyes out of a total of 60 ©yes examined by this method* In all the cases examined the nasal margin of the defect extended beyond the fixation point for a variable distance into the nasal field# even in these oases who retained gsod visual acuity*
The response to therapy can be demonstrated by static perimetry and Mlson (1969) followed patients suffering from tobacco amblyopia, treated with hydroxooobalamin by recording the change in field area* A typical example of
65
the field defect recorded by kimetio and static perimetry before and after several months #erapy with liydroxooobalamin la shown in Figure £#> 12*
f’atient .in fohapeo Mhlyonia* ' '
All the 65 patients were smokers j 5Î pipe onjy# 3 oigarettee only end g$ both* there were 64 male patients and I female* the mean age of this group was &fi 9*1 year©, with a range of 46 * §4 years# 47 of the patients (ahofut §) were of retirai age or older, hut # e greatest ineiienoe lay in the 60^80 years age group* (âs shown in table 2| 4)#This is higher than the previously recorded inoidenoeai maximum incidence in the $0*s recorded by %her (1927a) and Traqpalr (1938)#
However, when the figures are related to the percentage of # e male population in these age ^mups the incidence is fcmd to be maximal in the 70#80 years age group*
*In this analysis the figures for the 1961 census for Glasgow were used* The proportion of males in each age group was compared, aa a ratio Tobacco amblyopia/census* The
66
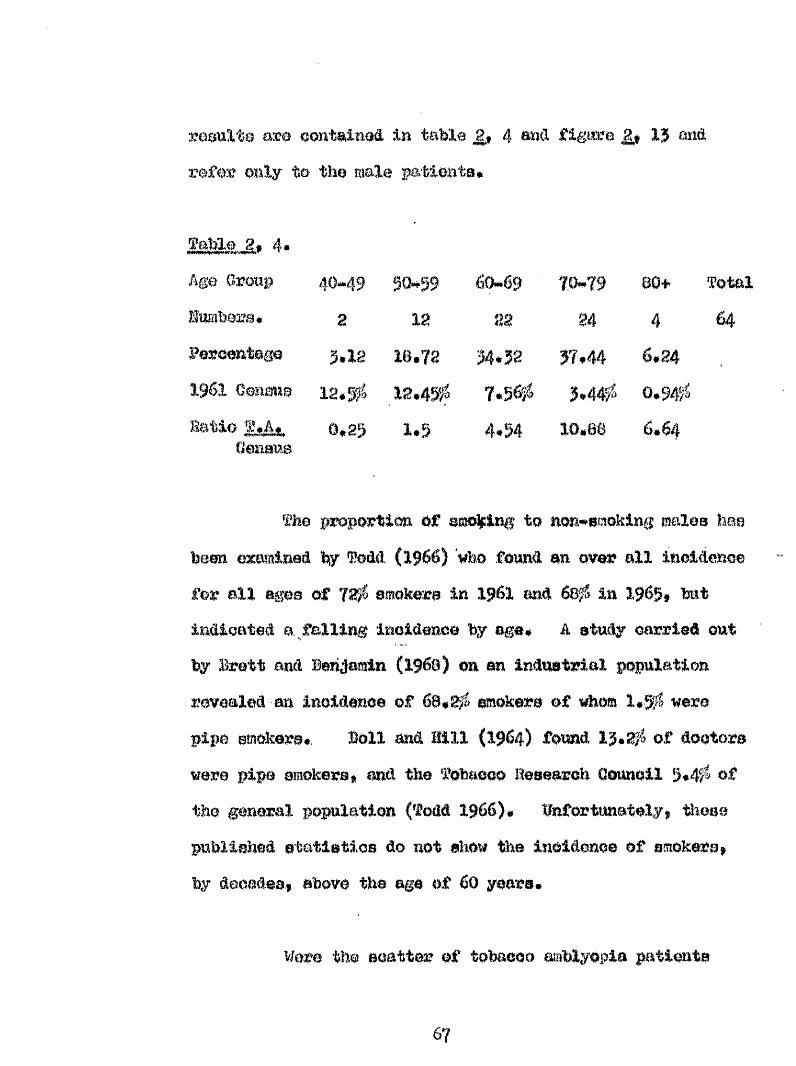
résulta are contaimed in tabla 4 and figure 13 and refer only te the male fatieiits*
Table 2# 4# Age Group 40*49 50*59 60*69 70-79 80+ TotallUBbara# 2 18 28 24 4 64Percentage 3.1s 18.72 34.32 37,44 6,241961 Q m m mHatio M a.
(Zeamœ
12,3#0.85
18.4%&1.5
7.56^ 3.44f4,54 10,88
0.94#6.64
The proportion of emoÿimg to mon#smoking males hae been examined by Todd (1966) who found on over all inoidenoe for all ages of 72# smoker# in 1961 mà 68# in 1963, hat indicated a. falling inoidence by age# A study carried out by Brett and Benjamin (1968) on an industrial population revealed an inoidence of 68## smoker# of #%om l#ÿ# were pipe smoker##, Boll and Hill (1964) found 13#2# of dootora were pipe amokers* and the Tobacco Hesemzch Cornell 3*4# of the general population (Todd 1966)# Hnfortuaately, these published statistics do not show the incidence of smokers, by decades* above the age of 60 years#
Wore the scatter of tobacco m*blyopla patients
10-88
6-64
5-4-54
1-5025
50 60 70Age in Years
90
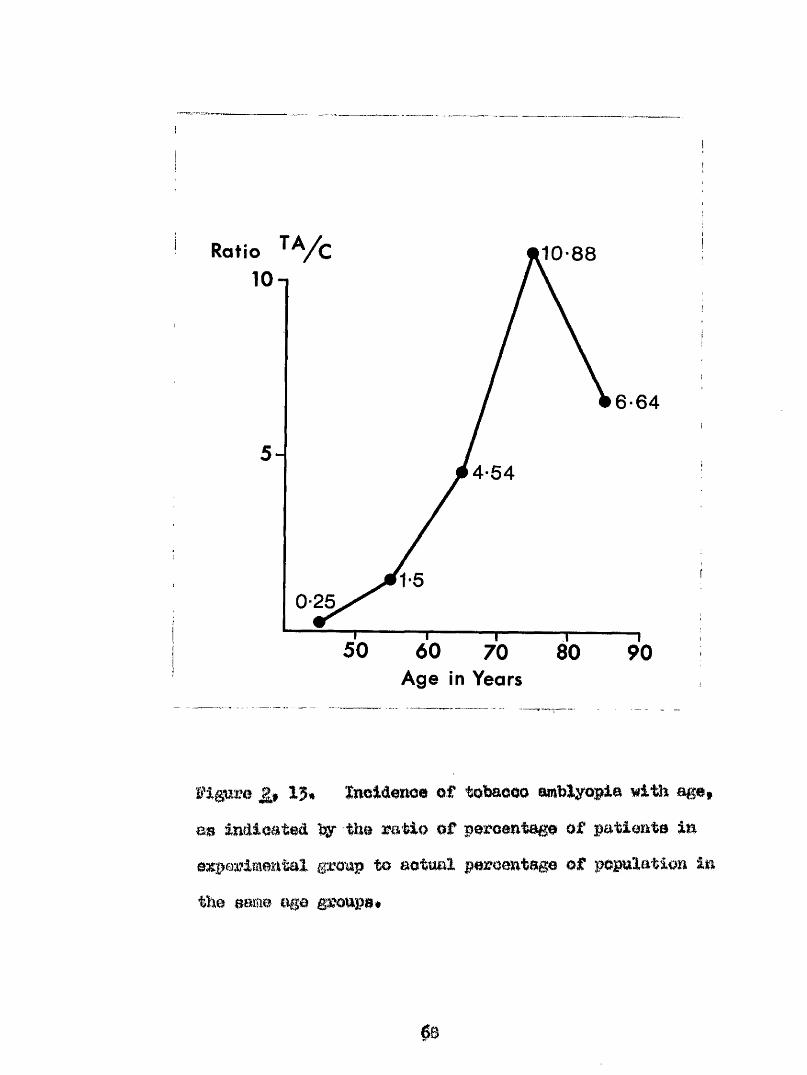
ïi'lgîure 13, Xnoidenoe of tobacco amblyopia with age, as indicated by the ratio of percentage of patients in experimental gronp to actual percentage of population in the same age groups.
08
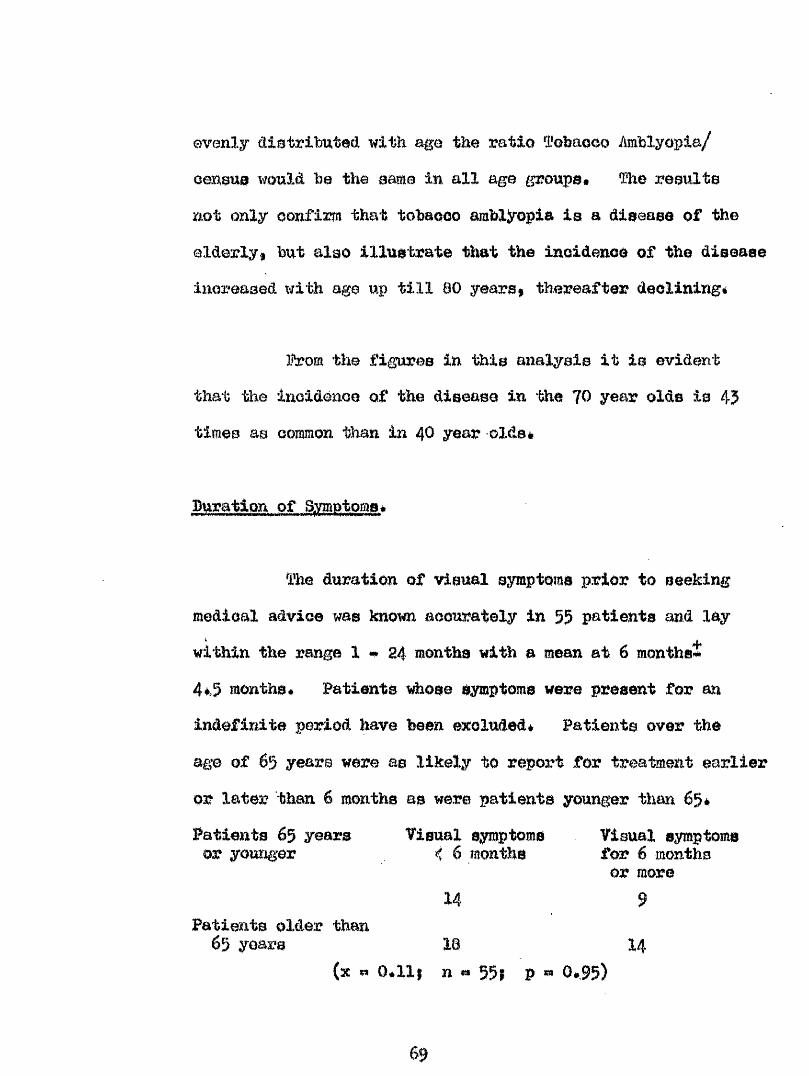
evenly distributed with age the ratio 1'ofeaooo Amblyopia/ censuo would be the same in all age groupe* ïho results not only oonfim that tobaeco mbXjropia is a disease of the elderlyI but also illustrate that the inoidenoe of the disease inoreased xjith age up till 00 years* thereafter declining#
l^om the figures in this analysis it is evident that the inoidènoe of the disease in the 70 year olds is 45 times as common than in 40 year olds*
Duration of Symptoms*
The duration of visual symptoms prior to seekingmedical advio© was known acouratoly in 55 patients and laywithin the rang© 1 • 24 months with a mean at 6 months*4*5 months* Patients whose symptoms were present for anindefinite period have been excluded* Patients over theage of 65 years were as likely to report for treatment earlieror later than 6 months as were patients younger than 65*Patients 65 years Visual symptoms Visual symptoms or younger < 6 months for 6 months
or more14 9
Patients older than65 years 18 I4
(x n 0*111 n «* 55; p 0*95)
69
Thus age played no part in determining when a patient reported for advioe*
Visual Aouity and duration of symntoma in untreated
A comparison between duration of symptoms and the percentage visual acuity yielded a correlation which was not significant (r » 0#085; n * 55; p^ Q.l)* Thus length of illness did not appear to materially affect the extent to which the visual acuity was lost*
Duration of Evmotoms and Visual Outcome*
The effect of duration of symptoms on the visual outcome is dealt with on page 146 where it is demonstrated that the earlier the patient presents for advice the more likely that the outcome will be favourable*
70
c m p T m III,
It ha© been obvloiw to all obaervero that the majority of tobaooo ueere do not develop tobaooo amblyopia ovm when not in perfect health, EutcMnaon (1075*07)»BaXea (1807) n W Tm q w i r (ifJO) postulated an individual inherited ouaoeptihillty to tobaoeo In patients showing tobaooo amblyopia* General ill health (Balae 1007, fraqmair 1930 m â Erlmeky 1934), and psyohio shook (fmqualr 1930* llarnbresim mid Bohepens 1946) have been mentioned m
precipitating oauees. Hutritional dietnrbancee have been blamed for am inoreaaed emeoeptlbility to toxio amblyopia,In particular e vitmmln defioimoy, although Carroll (1935*56), Carroll and ^anklln (1936) did not oonaldei? tobaoGo amblyopia purely the remit of a defloieney state*The aetiologie factor of vitamin Jldefioienoy in the amblyopia of tobacco or alcohol habituée ban been suggested by Duggen (1935), Gottlieb (I941) end Groess (1930)* but olinical trials have not convincingly ehowi that tobacco amblyopia ie oaueed by vitamin B complex deficiency (Heaton at al 1950)#
n
Battler (3,925)® Bach teg; (1920), Baohtes mid Burtsohor (19H0), fraqiiair (1950)# llambresin and Bohepons (1946) m d Grosz (1949), 3mv@ proaaiited atatistioal evidence pointing to an laoreaee in the imiûmo 0 of tobacco amblyopia during wartime, partiomlarly in eoumtriea suffering from food eearoltiee* There appears little doubt that the inoreae© in tehaoco amblyopia during the 1914*1913 and 1959*1945 World Ware w%& due to nutritional faotore rather than by change in the degree or manner of tobacco use*
Carroll (1935) reported that the OSF in ten oases of tobacco amblyopia was essentially normal* Be Bchweinitz and Msall (1903) studied the blood, urine, faeooa and stomach contents and reported evidence of an upset in digestion and metabolism* Lelshm&n (1951) foimd a high Incidence of hypochlorhydrla and achlorhydria in tobacco amblyopia* Heaton et ul (1953) found a ©ignlfioantly low level of B12 in serum In tobacco amblyopia* They further pointed out that mmw workers have noted the Importaniba of nutrition and general state of the patient with tobacco amblyopia*
Carroll (1935) felt tlnat there were other factors
72
in tîie and pmgree» ni tobacco amblyopia other thantobaooo and alcohol# He allowed patiente to oontinue to emoke and oomeme alcohol while rmiintaining them on a high vitamin diet eupplemented by yeast, whe$%t*#rm, ood*liver oil, and liver extract injeotiome. fhe euooesa of M s therapy is reflected in the rate of recovery which is as good as in any previous survey in which the patients had abstained from tobaooo#
Inj^lnenpo of. AlObhol# _
Widely divergent views have b e m expressed cGuoeming the influence of alcohol in the produotion of tobacco mblyopia*. ■ On # e other hand, there are those who deollne to Hntchinson^a view (1876) that total abstainers from stimulants are more liable to suffer than others and that on the whole, alcohol eounteraots tobaooo. Thus# Berry (188?) held that alcohol more probably oounteraots than abets the poisoning which gives rise to the amblyopia, and Gunn (IBB?) believed that total abstainers are probably pemliarly apt to get toxic amblyopia from a oomparatively small amoimt of the poison#
de SOhweinlts (ifOO) stated that alcohol was not
73
antegoEistio to toWooo but# in fact, predisposed to tobaooo amblyopia by producing a chronic dyspepsia* Aooordimg to bhthoff (lB86#lgai) aldohoi alone in excess will cause the oliaioal picture of toxic amblyopia*
The following relationships between tobacco and alcohol in the production of the amblyopia have been suggested#*
(1) Both alcohol m û tobacco are causative agents,(2) Either "agmt alone is capable of causing the
dieeaae, although usually free indulgence in alcohol is associated with heavy smoking# (llamaay 1^9% Parsons I90I# hyle 1905» do Sohweinltz W 7 # lyle 1947 and Maxwell 1953)*
(3) The ' influence of alcohol in the production of tobacco alcohol amblyopia is secondary or doubtful (Traquair IflO) since the amblyopia is observed in non# drinkers# but not in non#smokers# (ieltlaship 10B7, lanibreain and Bchepens 1946). fobaooo*aleohol amblyopia improve# wiien smoking is stopped even though the patient continues to drink (Berry 1##2 and llvans 1939).
(4) Alcohol indirectly forme the toxic effect of tobacco on the eye (Bemy IBi?# Gunn 1887# Mettleship 1887 and Heaton at al 199f)-*' Oarroll (1935^) believed that
increased susoeptiMIity of the patient was a far more important factor than the amount of tohaoco or alcohol oonaumed# Aa a rule, neither tobacco or alcohol directly affect the eye, unless the substances have first attacked the general health (Krimsky 1934), & view which supportsthe bel&af that cîironic retrobulbar neuritis is a true deficiency disee,ee#, -
The alcohol intake of the present group was assessed in 55 of the patients| 16 patients abstained from alcohol, 18 occasionally took alcohol, and 21 had a daily intake of alcohol* The alcohol consumption of 8 patients was considered heavy, but in only 3 of this group did the visual improvement reach 6/9 (Snellen) with treatment*Of the 13 moderate drinkers 5 (38*4^) and of the 16 teetotal patients 10 (62*5^) achieved a visual improvement to 6/9 (Snellen), or better during the period of treatment* It would seem that the alcohol consumption influenced the outcome* However, it was found that those patients who dranic heavily also smoked heavily#*Heavy drinkers mean tobacco consumption 3*68 oae per week* Moderate drinkers mean tobacco consumption 2*6 oz# per week Abstainers from alcohol mean tobacco consumption 2*5 02s•
75
per week*
' It was felt that alcohol ployed little if any part im the aoureo of the illmeee*
Vitamin B12* '
Binoe oyanooohalamin was isolated by Bmith (19#) and the eubaequent elucidation of its etruatura m â that of various analogues, there lim been oonaidorable interest in their biological roaotione* Vitamin B12 is a group of oompounde, each of which ie a complex porphyrin derivative • eontaining-a tervalent cobalt atom lltifced to a nucleotide# 'A nomenclature of the mbmbere of the Vltaniin B12 group# based on the nature of the nucleotide oemposltion has been proposed# in whièh the term Oobalamin i# reserved for those qompounds in which the nucleotide contains # e Imse 5*6, dimethylben&imidasole »
The six qowordinsto valenoiee of the cobalt atom are satisfied by the four nitrogen atoms of the tetrapyrrol, a nitrogen atom of the nucleotide; the sixth'valency is taken up by cyanide in the case of cyanocobalmin (figure* 3,1)
T6
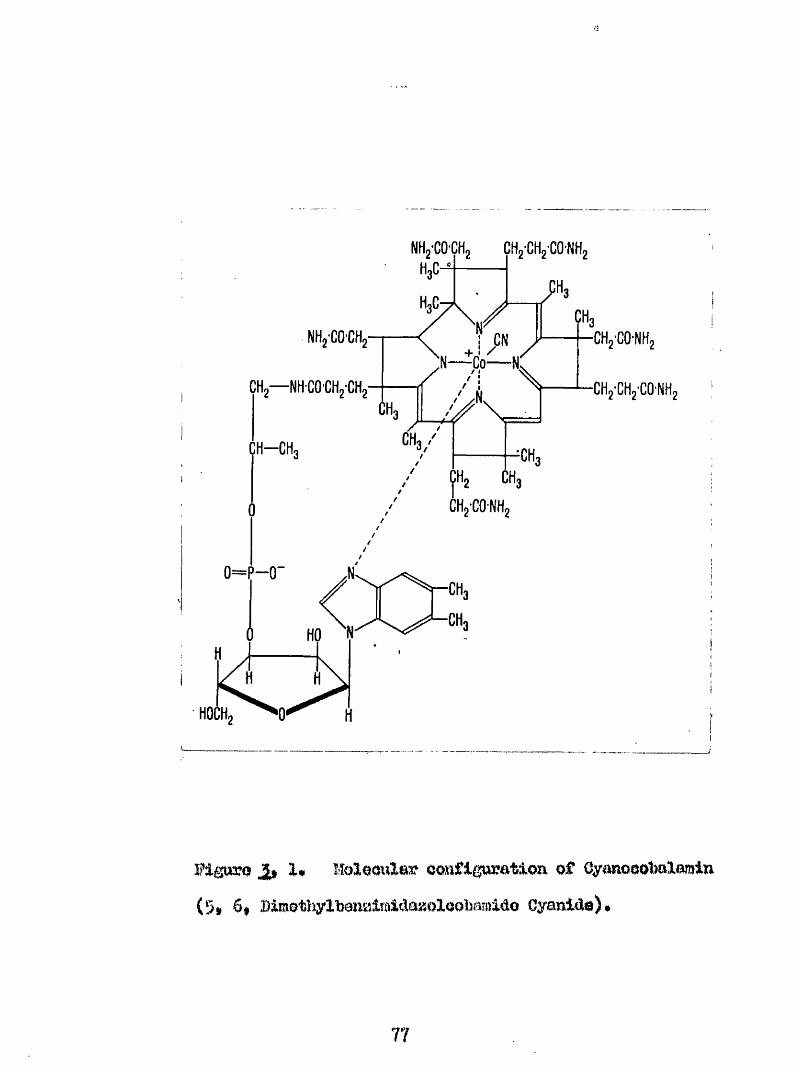
NHg'GO'CH, CHgCHg'CO'NHg
NHo'CO'CH,Co— N
CH — NH'CO'CHg'CHg
CH-CH
CHg-CO-NHg
CHg'GHg'CO'NHg
Figuro 1# lîoleoular configuration of Cyanooot)alamin (5» 6* BimothylfeonsaimMaaoIooljamldo Cyanide)*
77
by a lorn Im and byS#d#oxyadmaayl in co^enssya© B12# the mamfaotnre of vitamin B12 le baaed on its diraot miorobiologioal eyntbeei# by Strmtomyoes oliyaosna. or %oill^a^ me^therinm# It in also obtained m a by^^rodnot of antiMotlo mmfaotnre (Johnson and Todd 195?) ♦
Although oyanooobalamin was isolated from animal liver 60 the anti-^fernloious amimia faotor$ it has been enbseqnently shown that ocMen^yme BX2 is the major analogue in the livor (Toohey and Barker I96I)# aeoounting for 80# of the vitamin B12 analo#es# and is considered to be the active principle of vitamin B12 in the body*
1# J
The oarbm«#to#eobal t bond by mem%s of whioh the 9*demyadenosyl group is attaohed to the cobamide moiety in oo^A^emyme B12, aoeomts for the unique properties of tMs analogue* This bond may be split by the action of visible light, acid or oymide (Weisabaoh et al I960)* ïïndor Bummhin conditimw# light oauaes homely tic cleavage of the carbon^tcmcobalt bond yielding a reduced form of
IB
oymocobalamln*. With the addition of air oxidation to hydroxooobalamin ooouro (Brady and Barker Igêl). The addition of acid aplite not only the oarbOB**to**oobalt bond of ooem^yme B12, but also the nucleotide bond, roloneinif free adenine and a sugar derivative (Brady and Barker 1961)* Cyanide has aomeifhat similar of foots foming not only oyonoeobalamin, but also free adenJrte m û a oyanohydrin* .
Byateme that can oonvart oyanooobala iin or hydroxooobalamin to deoxyadenoeyX BI2 have been deaoribed In baotoria (Weieobaoh et al 1962)# The reaction requires â#T*f* whioli aervoa to transfer the 9#&eoxyadenoeyl moiety#, reduced flavin and a eulphydryl compound; inorgenio phosphate being released an a by*^produat*
A oobmine eompoimd has been shown to be eaaontiaX in name enaymatlo reaetione; # w common active form being teoxyadenoeyl B12*
(1) Icomeri»atien of glutamate to ^ metl^laspartate by the glutamate ieomeraee# (Barker et al 19#)#
(2) In reactions Involving hydrogen transfer under the Influence of the enzyme glycol deliydraee* During this
79
r m o t l m there is deactivation of the deoxyadmoeyl B12#It hm been suggested that this en%yme is deoompoaed to hydroxooobalamin, whioli in turn deactivate# the glyeol delsydraee# thus bringing about the observed slowing of the réaction# (Me and Ahelee 1963)#
(3) Methane fomatim from Co2 Carbon Dioxide,formate, methanol# éerine eto_# by maoroblo bacteria# utilises methyloobelamin m a oofaotor mâ intermediate metabolite*
(4) Diosyntheeie of acetate from 0o2 # CarbonDioxide#
(3) Isomerization of metbylmalonyl OoA to euaoinyl CoA by Methylmalonyl 0oA ieomeraee la m important raaotion in the metabolism of propionate* #%ie reaction involves m intrmoleoular group transfer (Stadtmm et al 1960)*
(6) In Methionine eyntheeis there is a transfer of a methyl group from |*-fethyltetrahydrofolat« to homocysteine yielding methlmine and tetrahydrofolata# thus explaining the relationship between vitamin B12, folio sold and oarbon#ome metabolism* The reaction takes place in three stages, the cobimide ooenzyme is required only for stage 0#
80
«*<**
Borins f tetrahydrofblftte 5» 10, methylinetetrahydrofolate f glycine*
(b) 5» 10# meîAiylinetetrahydrofClate 9, mo thyl tetrahydrofolate
(c) 5, methyltetrabydrofolate « homocysteine tetraî^drofoiate 4 methionine#
Réactions 1 « 4 have been observed in bacteria only (Weiesbach ©t aX 1964)» the ieomerieatlca of metliyl malonyX GoA has been obeerved in mammaXe* and it is felt that methionine eynthesie meydlao occur in maimaXa, though to date this hm only been observed in photoeynthetio bacteria,
2# PhyoiologloaX OonoiderationB#
Vitamin BX2 can bo eyntheeiaed by taicro-organlsme, bacteria, and actinomycetee# It does not occur naturally in yeasts, algae, or plants (Darken 1993); any vitamin B12 content present in th# bei% obtained from syblotie bacteria# Certain lower organisme require vitamin BIS as a growth factor (Ford and Euther 1955)# while others can do without the vitamin (Burton and hoohhead 1951) or replace it with aome other eoBentiaX metabolite# More highly orgariiseti
81
animals depend on ingested vitamin B12 for their supplies of the vitamin and store it in their tissues, especially the liver, kidney, musole, m d In their milk and e^gs*
Man depends on dietary sources for his supplies of vitamin B12# The vitamin is nbJmially synthesised in large amounts by the intestinal flora, hut apart from coprophagy this source is not utilised* The minimal daily requirements are not known with certainty# Although Ganong (l$65) claims a minimal daily requirement of 2.8 ,1 ug. per 24 hours has been shown to he sufficient to prevent pernicious anaemia (Eeisner and West 1949)* Dietary vitamin B12 is absorbed in the terminal ileum after conjugation with the intrinsic factor mucoprotein secreted by the gastric mucosa. In man vitamin B12 is mainly stored in the liver, but large quantities are also found in the kidneys, the Central nervous system and the myocardium# Vitamin B12 is present in serum either "free'* or "bound"* A small amount of vitamin B12 is normally present in serum as the "free" vitamin when it can be utilised by the tissues# The larger portion of the vitamin present in serum is "bound" to plasma protein {Pitney #t al 1954); principally to alpha*globulin (?35 )t albumen (l^), beta*»globulin (7^) and
82
ganima^^globulin (4^) (Heinrich ot nl 1956) # formally the protoine ere not fully aaturated and oan take up additional vitamin B12.#
Hydroxooobalamin la firmly bound to the proteins genorally, whereae oyanooobalamln is bound to apeoiflo globulins only (Miller and Sullivan 1958)*
Bogore et al (1955) otudiod the oerum vitamin B12 aoncon-tration in a large group of normal healtliy eubjeota* They, used a biological method of assay utilising hw Ifqiphmamli as tho test orgw%iem. They discovered a negative correlation betweon aomi vitamin B12 concentration and age# . Analysis of plasma by chromatograpliiy hue em^bled the isolation of four vitamin B12 fractions in tho blood, namely cyanooobalamin, hydroxooobalamin, dooxyadenosyl Big, and îîietîiylcobalafâin (Bindstrend and Btahlberg 1963, Bindotmnd 1964)* Of these me#:tylGObalamln m n present in the largest proportion and Smith (196S) believes that this is the form in which vitamin B12 usually is transported within the body fluids*
3# Pa tho Physiological. Qoneiderations*
B3
Bifiistraiiâ ©t al (1966) examined the plasma of a group of healtî^ emoklng euhjeota* fhey did not find a algaifioant ri.ee in the level of the oyanooohalarsin fraction, and felt that their résulta did not support the liyfotheoie proposed by Smith# Smith (I96I) had found that the difference In eaeay levels, by h# Miehmanil# of serum vitamin Bia oonoentratioh with ant without added oranlde, was lees in smokers than non^-amokers# He proposed that thin was brought about by the presence of a higher concentration of oyanooobalamin In the plasma of smokers# This he claimed was part of the derangement in cyanide metabolism underlying tobacco amblyopia and related conditions, Bimell et al (196b) found that the urinary excretion of vitamin B12 and thlocyanate was raised In smokers and that the concentrations of these substances bore a positive relationship to eaoh other, and further, the urinary thloeyanato concentration bora a negative relationship to serma vitamin B12 oonoentratlon* avery high thiocyanatc excretion may be associated with subnormal semm vitamin BI2 concentration*
In hepatic cirrhosis Bwemdseid et al (1957) found that there was a greatly reduced concentration of
84
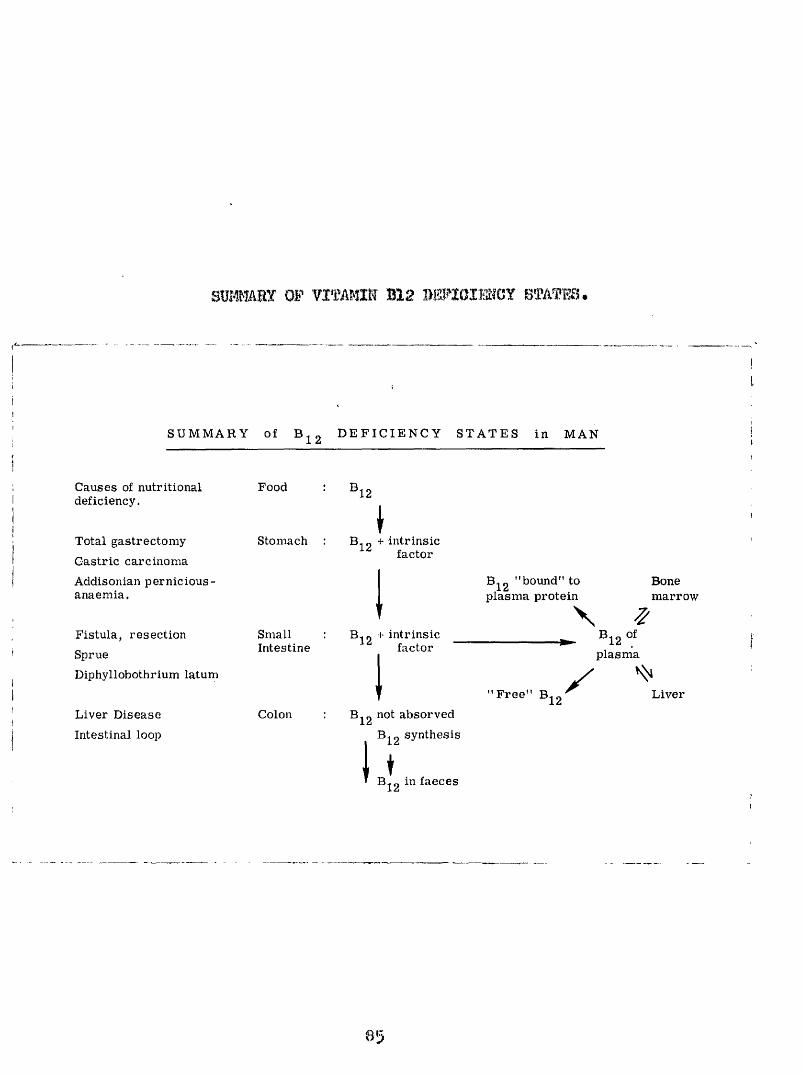
OF V ITAM IN B12 W IO im O Y BTATO -
S U M M A R Y of D E F I C I E N C Y S T A T E S i n M A N
Causes of nutritional deficiency.
Food B 12
Total gastrectomy
Gastric carcinoma
Addisonian pernicious- anaemia.
Fistula, resection
Sprue
Diphyllobothrium latum
Liver Disease
Intestinal loop
Stomach
SmallIntestine
Colon
B- „ + intrinsic factor
B-n + intrinsic factor
Bj 2 not absorved
Bj^g synthesis
♦B jg in faeces
"bound" to plasma protein
Bonemarrow\
Bi2plasma
"F re e " B X12 L iver
vitamin ÎE2 in the liver, ami M m et al (.1954) and llaokay at al (1957) that there waa oa laoroaao la the "bound" vitamin B12 and often a fall of the "free" vitamin B12 In plaama*
It la well reeogmiaed that the eerim vitamin B12 ooAoeAtratione may he very low after partial or total gaatreotomy and in aaaoalation with the "blind" loop, (ladenooh et al 1955) m d malabsorption syMromee, (O'Brien and %gland 1964)# divertiouXoale of the email inteetime, - treatment with mtioonvulemte# (Bpmy m à Witte IggB) and in the preeomoe of helminthic iîifeetation» (BjorWnh.eim 196#)# Administration'of intrineto faetor does not improve vitamin BIB absorption in patients with intestinal lésions * However# there may bo #i improvemmt in absorption after ■ apeoifie treatment# suoli m gluten free diet in adult ooeliao disease (Mollin ©t al W31)$ which may be o f
dlagnoatlo value*
Beoker e t a l (1954) have Bltmm tha t diabetics
have a tmdenoy to vitamin 112 dofioienoy and th is may
explain the inoressed inoidenoe of tobaooo amblyopia in diabetics* low aerum vitam in BIB oonoentmtiona have bem
reported in "vegans" (Smith 1962) whose dietary intake is low in foods containing vitamin Bl2* A dietary defioienoy may fee present in some elderly men, especially if they live alone (Bead et al 1965) and this deficiency might fee expected to predispose towards the development of tofeaooo amblyopia in such patients#
One of the effects of vitamin B12 deficiency is defective synthesis of nucleo'^protsln (Oirdwood 1950)# desoxyrifeonucleic acid in particular (Book 1961),consequently many cells of thé body are unable to form new cells at the normal rate, large cells feeing produced at a slower rate (Gastie 1955)♦ This is most apparent in tissues with aWpid turn^over of ziew cells# such as bone marrow* In pernicious anaemia the marrow cells show abnormalities in nucleic acid content which revert to normal on therapy with vitamin B12 (Glaaer et al 1954)* The deficiency of ribonucleic acid is particularly injurious to the axon cylinders of the spinal neurones which show progressive degeneration (Gastie 195))* Mental disturbances in pernicious anaemia are common and vary from minor defects of memory to major psychoses (Smith I960, Shuliian 196?) and show benefit from treatment with liver or vitamin B12
87
(ïJng'loy 1949); the improvement being rapid and coincident with belief of the anaemia (Walton et al 1954)* Smith (1964) reported the ooourrmoe of metabolle moephalopathy in a patient suffering pemioloue anaemia who whilst on treatment with qyanooobalamin developed a lung afeaeeea* Tho improvement of the encephalopathy after gOO ug of hydroxooobalamin was taken by Smith to indicate the toxic effect of cyanide aa the muee of the encephalopathy# A somewhat aimilar cane of tobaoco amblyopia oomplieated by lung abecame and ooma# was reported by Bronte«*'Stewart et al (1968# appendix B4)i which responded to oyanooobalamin thus indicating a deficiency of vitamin B12 rather #mn a toxic effect of cyanide at the dominent factor in the encephalopathy*^
Methods of Examination and .Eet)ult. A
The patients in this' analysis w#r# investigated for avitaminosis Bia md# when possible# theywmre admitted to hospital for the testa 'to be performed* Estimations of the total serum concentration of vitamin 112# studies of theintestinal absorption of vitamin B12 by the Schilling tost# and a general test for intestinal malabsorption by the
88
Xylose absorption test were carried out# In addition the serum concentration of folate was estimated, and the patients examined for evidence of coincident disease# An assessment of the dietary intake was carried out in some of the patients# In this section the results of these investigations are presented and their significance in relation to other factors is discussed# %amination of Hie peripheral blood and bone marrow were also carried out and their discussion will be found in the section on the Optic leuropathy of Pernicious Anaemia#
A* Serum Concentration
The serum concentration is believed to reflect the state of the body stores of vitamin B12# This concentration may be assayed by biological (Cirdwood i960), or radlo-isotopio means (Matthews et al 196?)* At present the biological assay is universally used and was the method used in the present group# The organisms that have been utilised for this type of estimation are Hia flagellate JSiââSa-œSSiUâJ tootobaolllua lej-ohmanll a nutant of Mcherichia ooli and the protozoan .OohromonaB mBlhemenalg.» Englena graoille posaeoses the greatest sensitivity for
89
vitamin B12# Ochromonaa malhamenaia the greatest epeoifioitÿ'*
Ü?he estimation© of the ©eram vitamin B12 oonoentration were carried out hy the Eju^jena gracilis method of assay after the method of lose (1952)» Thie organism was first used by Hutner et al (1949) and applied to body fluids by Mollin and Bose (1992)# The present assays were carried out by Doctor J#F. Adams, Southern General Hospital^ Glasgow*
Serum Vitamin B12 concentrations in Tbbacoo Amblyonia*
This was determined in 62 of the 6g patients*The serum #12 concentrations lay within the range 15 PS 572 pg/^1# with a mean at I96# 150*27 pg/ml* The serum B12 concentration was below 100 pg/ml* In 9 patient© and below 150 pg/ml* in 25 patients* Taking values of 150 pg/ml and below as abnormal 26 of the amblyopes (40^) had reduced concentrations of vitamin B12 in the serum*
A comparison was made between the mean serum B12 concentration of a control group of 71 non#amblyopio sub jects
90
and the amblyopes* The subjacts of the control group were drawn from the hospital population attending with conditions other than amblyopia and who were over the age of 45 years# In age composition the groups matched (t « 0*07, n K» IMV P «* >0#l) but the control group contained smokers and non»smokers*
Numbers
Amblyopic Group 6?** 9*1 years Ibg#* 150#27 pg/ml* 65Hon^amblyopic ' '
group 67*5* 11*0 years 2^7^ 119 pg/ml# 71
The mean serum vitamin #12 concentration in the amblyopic ^?oup was significantly lower than in the non# amblyopic group (t 2*90, n «» I54* p < O&01) thus confirming the findings of Heaton et al (iggS)*
In an attempt to determine whether the low concentration of serum vitamin #12 found in 4^0 of the tobacco amblyopes was the result of tobacco smoking or an independently determined factor, the tobacco consumption in these patients was plotted against the serum vitamin #12 concentration (Fig# J., 2)* A significant but not very
91
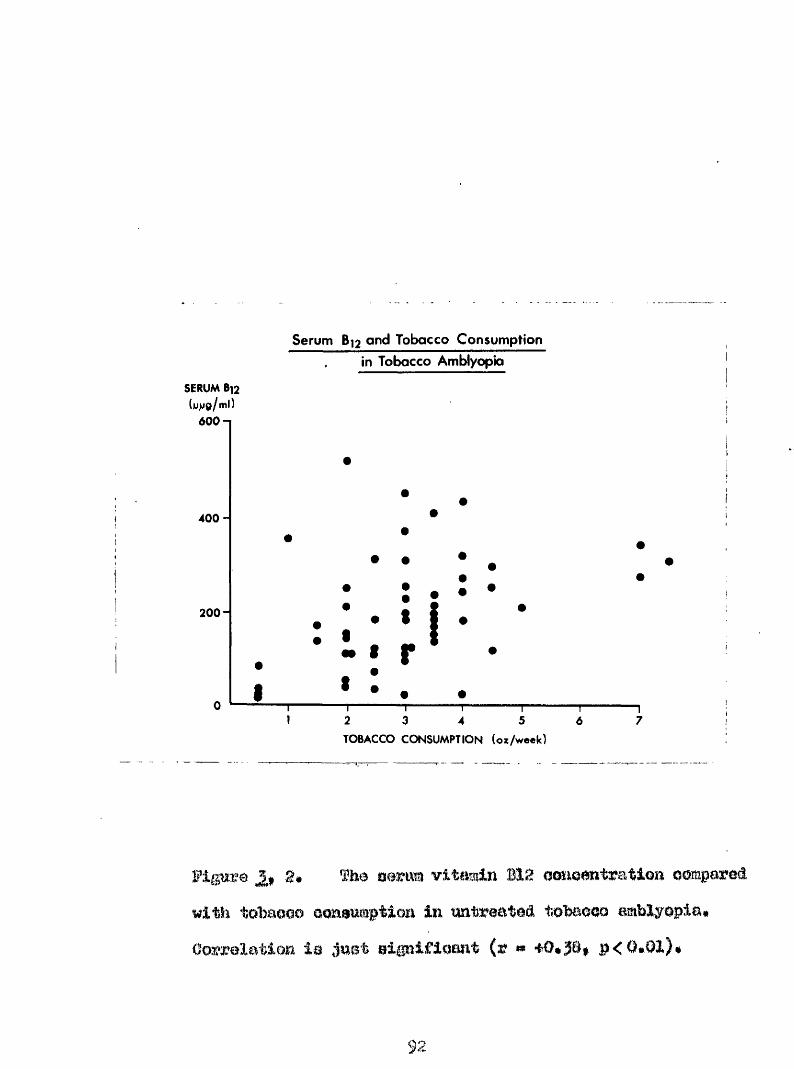
SERUM(yva/ml)
Sérum B]2 and Tobacco Consumption In Tobacco Amblyopia
400
200-
2 3 5 764TOBACCO CONSUMPTION (oz/w eek)
vitamin Bie oonaetitratlon oompared with totaoao oonamm^ption Im tmtreateâ tobaooo amblyopia# Oo^reXatioa la jaet elgalflqaat (r # •fO#3S| p<0«0l)#
9
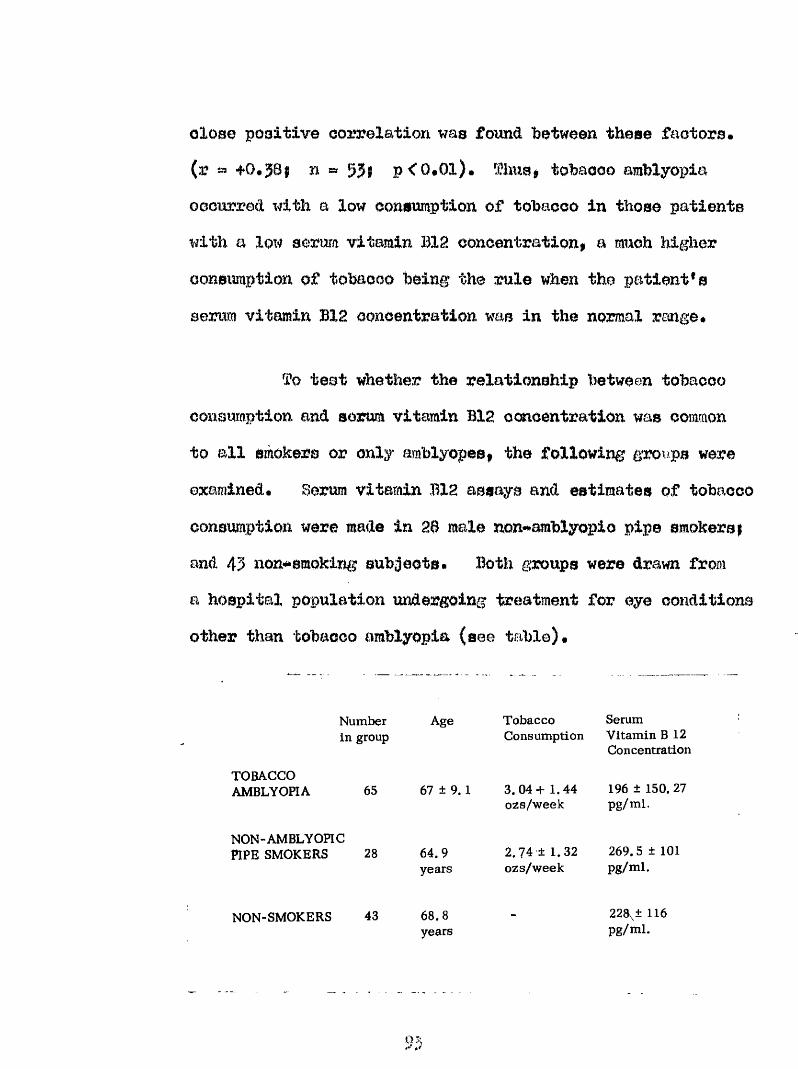
clos© positive correlation was foimd between these factors.(r a fO#38; n = 53; p<0*0l). fhns> tobacco amblyopiaoccurred with a low consumption of tobacco in those patients with a low sorura vitamin BIS concentration, a much higher consumption of tobacco being the rule when the patient's serum vitamin B12 concentration was in the normal range#
Tq teot whether the relationship between tobacco consumption and serum vitamin BIS concentration was common to all smokers or only amblyopes, the following groiips were examined. Serum vitamin B12 assays and estimates of tobacco consumption were made In 26 male non**amblyopio pipe smokers | and 43 non*<*emoking subjects. Both groups were drawn from a hospital population undergoing treatment for eye conditions other than tobacco amblyopia (see table).
TOBACCOAMBLYOPIA
Number in group
65
Age
67 ± 9.1
Tobacco SerumConsumption Vitamin B 12
Concentration
3 .04+ 1.44 ozs/week
196 ± 150. 27 pg/ml.
NON-AMBLYOHC PIPE SMOKERS 28 64.9
years2.74 ± 1.32 ozs/week
269. 5 ± 101 pg/ml.
NON-SMOKERS 43 68.8years
228\± 116 pg/ml.
0;,r
(s)o]bbà0èo consumption mâ m x m vitamin B12 eonoontratlon for 20 mlm ncm-amblyopio pipe omokere of elmllnr age composition to the amblyopic patients vas plotted# fhe result is shown in Fig# 3* î o significant statistical correlation was found between these two factors (r * ##0.001) The mean tobacco consumption of this group was not significantly differmt i ?om that of the amblyopic group of patients.
2.57Î 1.3 oss/wk in non^amblyopio groupi3.04* 1.44 OKs/wk in the amblyopic group (t « 0.30* n # 91# p 0.1)
(b) The mean serum vitamin B12 concentration in a group of non##smoking subjects was compared with that of the pipe^smoking non#amblycpic subjects. In the former group the assay was 228pgî 116 pg/ml. and in the latter 269.§«101 pg/ml# There is no significant statistical difference between the two groups, (t # 1*55# n * 69» p>0.1). The mean serum vitamin BIS concentration in the %%on*mblyopic smokers is significantly greater than that of the amblyopic group (t w 2*79# n # 91# p< 0.01).
94
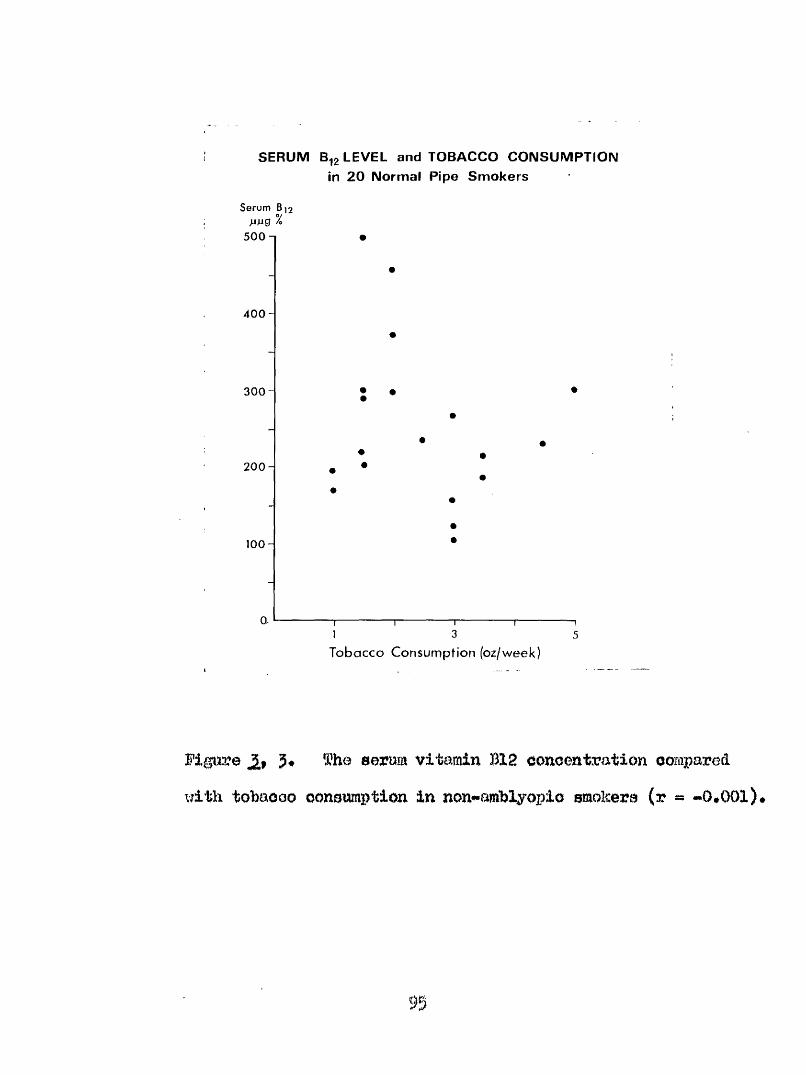
SERUM B,2 LEVEL and TOBACCO CONSUMPTION in 20 Normal Pipe Smokers
Serum 8,2 pjug % 5 0 0 n
4 0 0 -
3 0 0
200 -
1 0 0 -
Or
• •
1 3 5Tobacco Consumption (oz/week)
Figure 3* The serum vitamin B12 concentration compared with tobacco consumption In non#«amhlyopio smokers (r - -O.OOl)*
B* Absorption étudies»
1# fitgffiiiT BX2 Âbsôriation Teat'.
HaXabsorption of vltaiain B12 may W due to gastrio t m t o m whloh impair the eeoretion of intrineio factor# or to lésions of the email inteetlne which interfere with the absorption of the vitamin BlS/intrinsio factor complex, tests of vitamin B12 absorption using radioactive 312 have their most useful application in the diagnosis of pernicious anaemia# but arc also useful for demonstrating intestinal malabsorption of vitamin 112# even when there is m other evidence of intestinal malabsorption*
The measurement of vitamin 112 absorption is essentially a twc#atage procedure, the teat is first carried out by giving # @ patient a small oral dose of radioactive vitamin 112# If the patient fails to absorb this orally the test is repeated with the addition of intrinsic factor* The absorption is assessed by one of the following methods**
%
(#) Urinary excretion method 1955) •(b) Faeoal excretion method (Eelnle ot el 1992)•(e) Hepatic uptake method#.., (Glass et al 1994)*(d) #01# body radioactivity method (Hei^eneteln
ot al 1961).(e) Plasma radioactivity (Booth and Mollin 1996).
In olinioal practice # e urinary excretion method in the moat widely wed; however the whole body radioactivity method or plasma radioactivity method ia .probably the more accurate#
Schilling teata were performed on 46 of the 65 tobacco amblyopia patient# a# follow# 1*
1# Patient faated overnight#0# Bladder emptied and urine discarded 3# Drank dose of radioactive Vitamin B10
labelled with Cobalt SB#-4# After Ë houre I mg# hydroxocobalorain waa
given imtramuBcularly#5# All urine was collected for 24 hours mâ the
radioactivity present measured#
97
TaXues of less than recovery were found in 21 taeta (45*7^) and of Xoas than 9^ in 6 teata (ij^)*The Schilling teat results were plotted against tobacco consumption.. à similar trend to that found on comparing serum vitamin B12 concentration and tobacco consumption was revealed though the relationship was not so statistically significant (r *» n» 40$ P< O.O5)* The Schillingtest results showed that in tobaooo mablyopla, -poor absorption of vitamin 1X2 tended to be associated with low levels of tobacco consumption and with test results within the normal range, tobacco consumption was high (Fig. 4)>
2* . Xylose Absorption Test of Helmer and Fo^ts (1937). -
This test was used as a general indicator of intestinal malabsorption* Xylose is a metabolioally inert sugar and its rate of appearance in the urine is an indicator of its rate of absorption*
This test was carried out on 53 of the tobacco æiblyopia patients as followsi*
1. Patient fasted overnight.2* Bladder emptied and urine discarded*
98
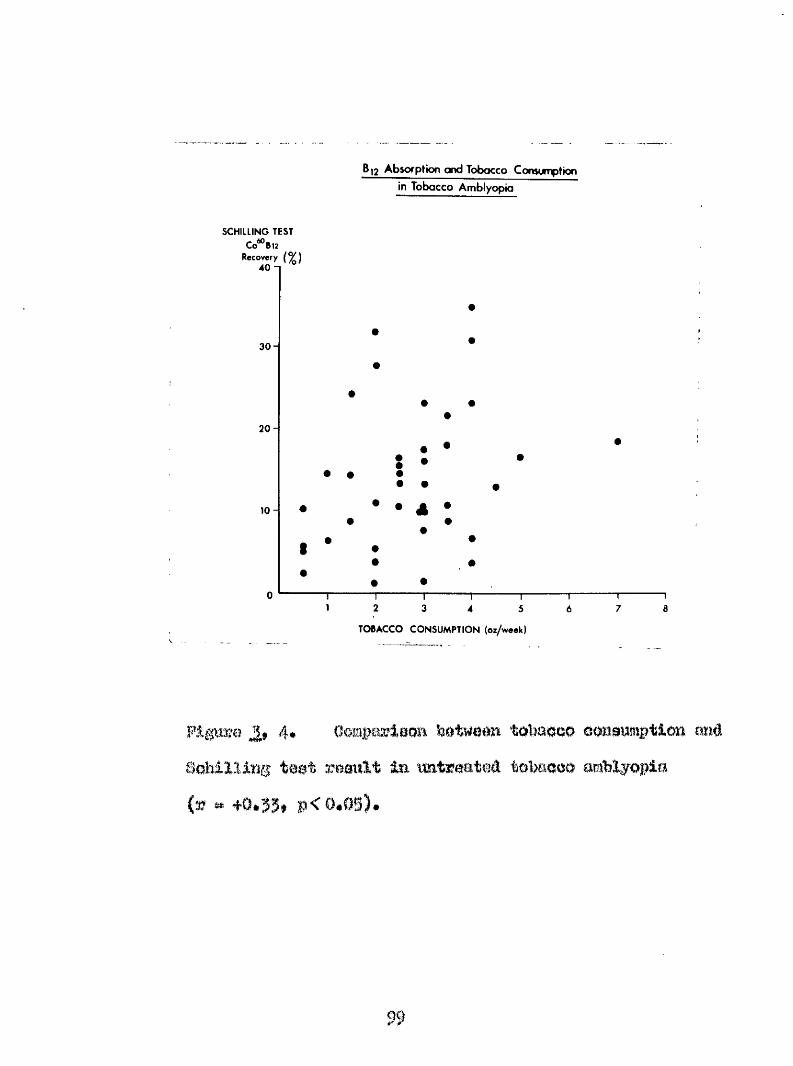
SCHILLING TEST 60CoBiï
Recovery (% ) 40 - 1
3 0 -
20
10
B,2 Absorption ond Tobacco Consumption
in Tobacco Amblyopia
A#
4
TOBACCO CONSUMPTION (oz/week)
^9 4* OomparlBOR tôbacao oonaumption ma#SolîiXIlng test mmxlt in untreated tobacco cmiblyopia (æ » +0.53* »<0.0§).
99
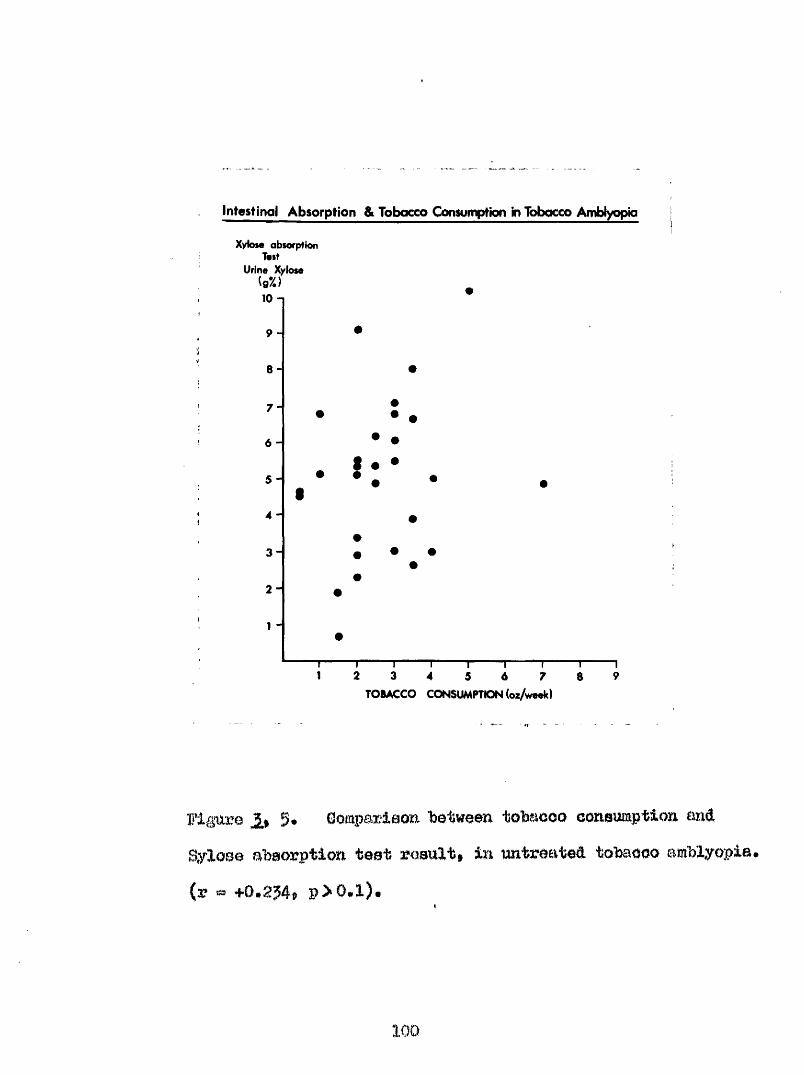
Intestinal Absorption & Tobacco Consumption in Tobacco Amblyopia
Xykwe absorption Test
Urine Xylose
6 -
4 -
3 -
1 2 3 4 95 6 7 8TOBACCO CONSUMPTION (oz/week)
1‘lgure il 5* Gomparlaom betweem tobaooo consmptlo» aad 8ylo$e a’baojyption teat m m l % tn mtreated tobaeoo amblyopia,
(3? 4-0» 254® P 0*1) e
100
3» 3 ### Xyloee taken omily in BgO mla* of water* Thla m e then followed by a oooond 250 mln# of water*
4* Patient waa kept at roat and had nothing to eat or drink till emi of teat#
9» Blood aample was t^mn at t h m m after oralXylose,
6# Bladder emptied at 5 hoars after oral 3*ylos@*
When the Xylose absorption test reault was plotted against tobacao oonaitmption a eimilm? trend to that found on oomparing tobaooo ooneumption with serum vitamin M2 Gonoentmtion# or the Schilling teat was obtained# The statistical correlation however, fails to bo si#iifioant,{%f f0,234$ n «» 29f #0*1)# (Pigure g)*
The Xylose absorption test probably gives a measure of intestinal absorption, partioulairly in these patienta whose faulty vitamin B12 absorption is not due to a specific defeat euoh as Addisonian Pemiciou.a Anaemia#-
Û#, Serum Folate Ocaucentmtion*
In contrast to the well recognised neurological abnormalities produced by a low oonoentration of vitamin B18 In the serum the effects of a lack of folio acid on the nervous system are relatively unknown* Reynolds (196B) suggested that folate deficiency was the cause of some of the mental changes seen in old age and that apathy led to a deficient intake of dietary folate. Girdwood et al (1967) were unable to confirm low folate concentrations in an elderly Scottish population,
Though dietary deficiency alone can produce megaloblastic anaemia (Jackson 1965), in Great Britain this type of anaemia is often associated with conditions which increase the requirement for folate, such as pregnancy (Gough et al 1965), psychiatric problems (Oaimoy I967), Ingestion of drugs (îîalpas et al I966), alcoholism and alcoholic cirrhosis, (McGurdy et al I962, and Waters et al 1966), chronic renal disease (Sevitt and loffbrand 19&9), Orohn*8 disease (Hoffbrand et al 1968), and rheumatoid arthritis (Gough et al 1964)* The serum folate concentration is the earliest and most sensitive index of folate deficiency (^rit. Med. J*, (i960), 2,570^ , and on this basis Head et
al (1965) and Bundle and Piéton Williams (19É6) found defioieaey common in elderly patlarite in imetitntions#
.Serum Folate Cloneefitrations in Untreated ToWeeo Amblyopia.
fhe serum folate ooneantrations were eetimated by a bioiogieal method of aessy after Maters and Mollin C196I) utilising laotobaoillna easel. One patient in this series was receiving thorapeutlo folate for a macros soy tie anaemia due to alcoholic airrhoeis, m û le excluded from the analysis, Serum folate oonoentratlons wereobtained in @1 patientsi**
Of 9 patients with pemioiom anaemia the moan folate was S.28 ng/ml Î 2*89 ng/ml.
Of 42 patients without anaemiathe mean folate was 6*17 ng/ml t 5.06 ng/ml
Of all patient# the mean folate was 6*43 ng/ml t ng/ml*
1 0?
Pathologically low folate omomtmtlon#( 4 ng/mX*) wsro found in 10 patianto (l0fS) of whom 1 hed pamioioiia aaeomia and g did mot* A comporiaom between # e moan folate ooBoomtratidmo im tobaooo amblyopia complicated by pemiolow anaemia and mot complicated by permlelomn anaemia ahmed little etatietieai difference#(t *»f i.757, n m 49, O.05<9<O*l)-#
Although a comparison he Worn, age m â aemm folate oonoentration yielded a positive oorralatlom %#ich proved not to be eignifiaamt (r # 0#?f n # ## p>0,l), a significant mnmber of patiente m m - the age of 6g yeam had emmm folate ommntmtiom in the subnormal range (Wlo%f 6 tkl/ml)#(% * 4,774# m * 49* 0»&%<p<0t05)t
In untreated tobaooo amblyopia the mm\m folate concentration was compared with tobacco eonawmptien in 51 patiente, a positive correlation was obtained but thin proved mot to be (r ## 0,074# n 49ip>0*l)# Vlhmi the pernloimne anaemia patiente m m excluded the correlation became more positive* (r # 0##6# n ## p * 0.1) Ficpre 6*
04
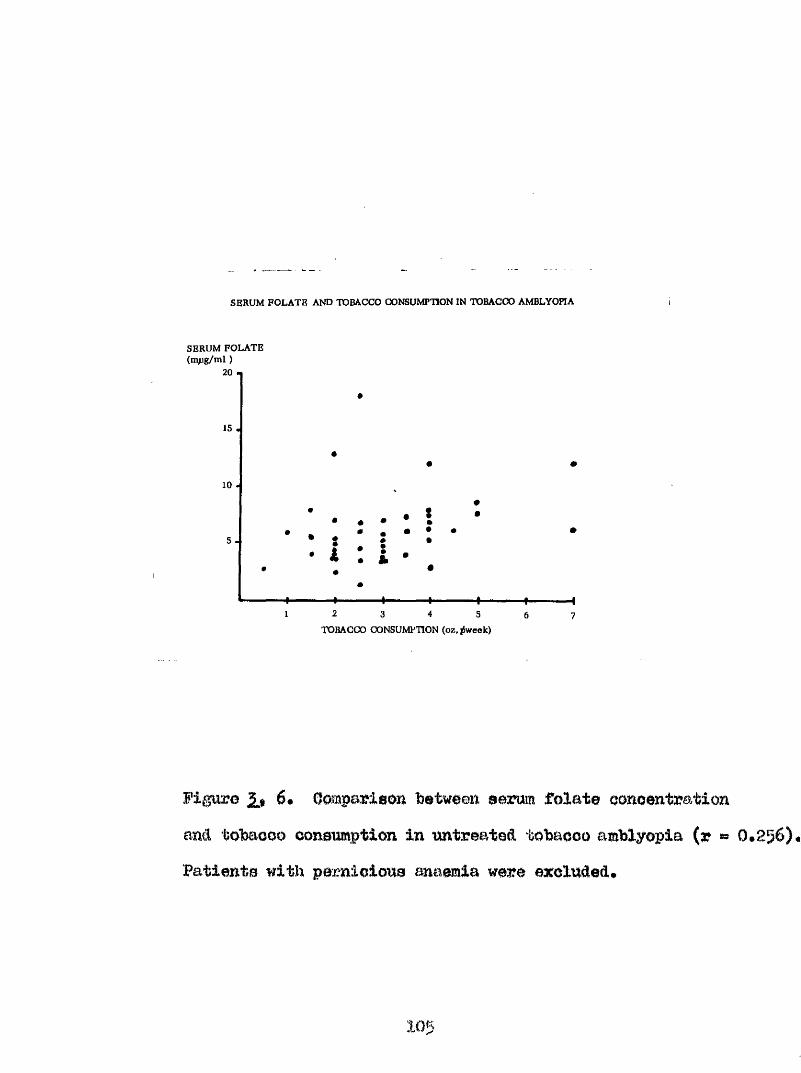
SERUM FOLATE AND TOBACCO CONSUMPTION IN TOBACCO AMBLYOPIA
SERUM FOLATE (mpg/m l )
20
15
10 .
5 .
4-
• •• #: i # f- 4- 4-
1 2 3 4 5
TOBACCO CONSUMPTION (oz.,w eek )
Figure 2* 6# Oemparison between serum folate oonoentrationmil tobaooo ooneumption in untreated tobaooo amblyopia (r » 0*256) •Patiente with pernioioue anaemia were excluded#
105
B12.
Ganong (1965) claim# that the minimum daily dietary requirement of vitamin B12 is 2»B Heinrich (I968) has shown that the tmmover rate of vitamin B12 in the body metabolic pool is O.Og^ (approximately 2*55 U® per day).This daily faecal and urinary excretion represents the optimal nutritional requirements. The minimum vitamin B12 requirement of 0*5 •“ 1#0 pB P®^ day is just sufficient to satisfy the needs for normal erythrooytopoiesis end central nervous system function, but does not normalise vitamin B12 levels in the serum and tissues* If the daily metabolic turnover is not compensated for only the vitamin B12 pools in the storage organs and tissues can bo used as a source for the metabolic vitamin B12 requirement* Thus, in face of reduced intestinal absorption of v it#ln B12, there is progressive depletion of ooenzym© 312 stores and a reduction in the senm concentration of vitamin B12*
With the aid of the hospital dietician the diets of 13 patients ware analysed for vitamin B12 content* W i m
the vitamin B12 content of uncooked food was estimated, the mean daily intake was 4*04 ug per day; 7 patients having
106
intake of 2*5 ug per day or Imm* Aosmin# a g # loan through cooking, the mmher of pationta whoa© diet oontained 2*5 u|| per day vitamin B12 or lose, roaa to $ (6%'G), Of thoae patients 5* (30,5#) were helo# the minimal dally requirment of 1,0 %-# outlined by IMnrioh (1960), Tlieaa figures oonfim that the majority of tobaooo amblyopes diet in low in foods containing vitamin B12,
m,
do prediapooin® to tobaooo amblyopia the ioltmims diaeaaea have been olted ##- digestive cliaorâera (de Boîiweinitss
aad Msall IgOg), diahateo (llattiaehip and iWmonda 1883* OazToIl 19561 Mggmt 1959)# syphilis (B'ttaay 1926), and m alm tritim (Barry 1804* ialati 1687# %1$ 190$, îta te a iii
and Sohepcme Ig#, #roa% 1949? Boggart 1959), Wiahmm (15)51) found that tobaeao mblyopia and the opt'Ie nmropathy of pemioioue anaemia could eo exiot,
Examination of the patients investigated revealed the following eyatemio dleeaee##*
(a) àMimnisu Pemioiow Anaemia 11 (16*94#)
(b) Fra Pmmlolouu Amamla 11 (16,94#)(c) Dlmbetos 6 (9.24#)(&) Hepatlo d&ea&s# 2 (5,08#)(#) Skeletal system âisoase
Badge0 flisaaaa of home 1 (1.54#)Hhemimtolé arteiti# I (1,54#)Ûhroïii a omteomyoll ti o I (1.54#)
(f) 8quamow& oaroi&om& of skin % (1.54#)
Bo e^Menco of other oofijplioatiue fliseasa isi 3S1 (47«?4f0*
lOf
m m TOKia i m m n m Tomooo
All olaseio writers attributed to tobaooo its full share of causation as a source of amblyopia (Wordsworth 1065)* fho opinions of later writers (Mottleshlp ISBTt bautenbaoh 1890$ Gottlieb 1941$ and Boggart 1959) that tobaooo as a cause of toxic amblyopia (but not necessarily the only agent capgible of producing this condition) were not synonymous with proof* The observation that recovery from tobacco amblyopia could lie in abstinence from tobacco would seem to implicate tobacco in some way (HoKenssie 1854) * heishman (l95l) was of the opinion that some noxious agent associated with tobacco, other than nicotine, would appear to be the ultimate source of tobacco amblyopia, and Hambresin and Bohepens (1946) considered that tobacco amblyopia was only one symptom of chronic tobacooism* bautenbaeh (189S) comsidered tobacco amblyopia occurring in smokers to be induced not by the direct absorption of nicotine, but by the volatile products of combusion; but this could not explain tobacco amblyopia observed in tobacco ohewers and
109
muff tekera* f m p a l r (I930) olaimed that # # excltl% m m m of tobaooo amblyopia woo tobaooo# but the dlaeago was determined by a in the patient* 0 health# ora nmtritionel defieienoy oepeoielly of vltmmim## Thus# in peraono with worn mild vitamin B12 âofioimoy the retina or optio nerve Mmtû hmorm unduly eemeitlvo to the offoots of tobaooo (Heaton #t al 1958) • liana (1908) after e^iMorating various aubetanoea found in tobaooo smoke, stated that mm&t Investigation# pointed to nicotine m the sole effective p M m m m conetituent and referred to Habemann and Eheenf&eld who had statecl that in tobacco moke nicotine mm by far the mo*t important component, the others Including i>yrMine m m of no importance*%hor (1927a) examined mrlome tobaccos % estimating the nicotine content; of the brand of tobacco smoked by 92*9|S of hie amblyopia oa*e# the nicotine content mu 3 3*07##
Bontly and Bomy (1959) in their review atate that early reecarchee on cigar moke reported the Isolation of pyridine (05II9i) end its analogue#* Arsenic appear# to have engaged the ettentioa of many early worker# but
and (hmdemaon (I9I2) were firat to diacua# cysnMo* They found hydi ogcn cyanide and hydrogen thiocyanido in both
110
the gaseous amé partlqulete phase of tobaooo make from acid mid alkallae tabaooosf oigsr mok# coiitaining more apmide tMm cigarette moke (Boholler 1935)» Oebome et al (1956) mail Jotoatoue mû flismaer (&9S@) examined the ganmm phase of cigarette amok# by infra-red methods# and fomd oyanide present in the oondenoable fraction to the amount % 3 ^ 31 #0x1#''2 mole## ' the h#B# Bmrgeon General (1964) reported a tobaooo moke oyimlde ooutmt of up to 1*600 p#p.m# These are high values Indeed in the light of aialeter* e (1953) etatmmt that- 011 etmoephero' containing 3*000 p,p#m# of oymide mn letlml to homo aaplem# à reofiat report (Darby ami Wileon 107) indioat-ed that them m m little variation in the smoke cyanide content of various temde of pipe tobaooo# fhesa author# further eonolude that the meooiatlon between certain brand #■ of tobaooo and tobaooo amblyopia was dependent m t on differenoe in meumto%iol%^ but mi popularity and eheapnem#
llohor (1927a) from hie analyeia of 1100 oaeoa oftobaooo amblyopia eolleoted in Aberdeen* oonoluded that the majority of tobaooo amblyopes moke rather lean tobaooo then
111
mokers# III# figures m m 8+8$ om§
per m m k for the amblyopes me against 2*72 oza# per week for the mom#amblyoplo mokers ^d\m the total mmlmra were ooîîeidereâf W t when only subjects over the age of 50 year# were oonoidtred.| the average- oomemptio# for the amblyopia group fell to 2*56 mu* p m weak, and the mouwamhlyoplo group to 2#6o 0%## per week*
The mean tobaooo oonemptlom of the present group of patients suffering from tobaooo amblyopia is 3*04 1*44 o^s* per week with a range o f 0*5 oaa* to
7 08S* per week# th is -group comprises both pipe miâ
olgarette smokers, 57 pipe only, 3 cigarettes only and 5 hath. The tobaooo omeumptlm In the amblyopic group is s is n ifio im tly higher them tha t of a comparable grouf
o f 37 uoE**anMyopio smoking subjects dram from a
hospital population, in which I t ie l#0ÿ£ 1.19 oas* per week f t # 14*39$ u # 75$ p 4 0*001)#
The following schem# was used to convert cigarettes smoked per day Into m m m $ of tobacco perweek# The average weight of tobacco contained in 28- tlifforant brands o f c igare ttes, plain o r tipped, was
1 12
fom d to bo 0*7665 gm# (im idoy Times# 8th June# 1969)#
5 Qigamttm per day # 1 o%# tobaooo per week 10 *' " (* o&* " " w15 " # 3 0%.80 " " % * 4 08* " " "25 '* " " * 5 00* » '* ''
Beoeuee o f its reactive nature# and
difficulty in its detection in body fluide# 'Vlileon (1965a) concluded #at m investigation of cyanide metabolism must ooneentrate on the products of that metabolism# Although cyanide ia mainly converted to thiooyanate#. the estimation of thiocyanate in body fluids is not an accurate index of cyanide exposure# because of alimentary absorption of dietary thiooyanato and variable concentration in body fluids* lïmoxi ut the factors which effect the concentration of thiooyanate the following ate recognised#*
(1) Dietary intake of preformed thiooyaimte contained in green vagctablee and milk# is aubjootcd to
113
seasonal variations (Stoa 1957)•(2) Deficient intake, as in anorexia nervosa
and prolonged vomiting, I0 associated with low concentrations of thiooyanate in plasma (stoa 195?)•
(3) Defective absorption of oral thiocyanate has been observed in patients suffering from gastric carcinoma (ïiaïigman et al 1966),
(4) The ïïrinary excretion of thlocyanate tends to vary directly with urine volume and with chloride excretion (Btoa 1957).
(5) Cyclical changes in thiooyanate concentration of plasma have been found to coincide with the menstrual cycle (stoa 1957)* These alterations are probably related to the state of hydration*
Naturally oocUrrlng cyanide and thiooyanate are found in foodstuffs such as cabbage and spinach (Btoa 1957)$ . in dairy produce and milk (Wokes et al 1952), in alcoholic beverages such as beer and stout (Stoa 1957), and in tobacco leaf and smoke (Lehmann and Gundormann 1912)* Cyanide is produced endogenously from thiooyanate by enaymio action end is a by-product of bacterial growth in closed cavities*
1 1 4
that the major portion of mcogenone or ©Mogenoue oyanid# is eæoreteâ in the wine ae thiooyanate was first deeorifeed % lang, S# (2.S94) and later by Smith ant Maleolm (l93û)«- The idontifloation of the meyme ays tom was eetabliaiied by lang» E* (1935.)* The enoyme was sailed Ihiodfinee© and it has been fonnd to be speoifio i m free cyanide withont action on organically bound cyanc^ groupe* In tlds context it competes with hydroxoooljalamin which takes up cyanide avidly to form the harmless cyanooobalamin {Smith 19#)* Eecent studies on the distribution of rhodanese in the tissues* show it to be widely distributed in the body* activity being greatest in the liver (Himwioh and Saunders Ig# mid Eaunders mid llimwioh 1950)*
As well as a mechanism for converting cyanide to thiocyamte* there exists a reverse pathway which mediated through fhiocyanate Oxidase (Goldstein and Hiedera 1953)-* This en%me is found in red blood corpuscles. The presence of thiooyamte osdldaso* which ensuroa a persistent trace of cyanide in the blood* is confirmatory evidence that the latter in minute amounts is an essential metabolite (Smith
115
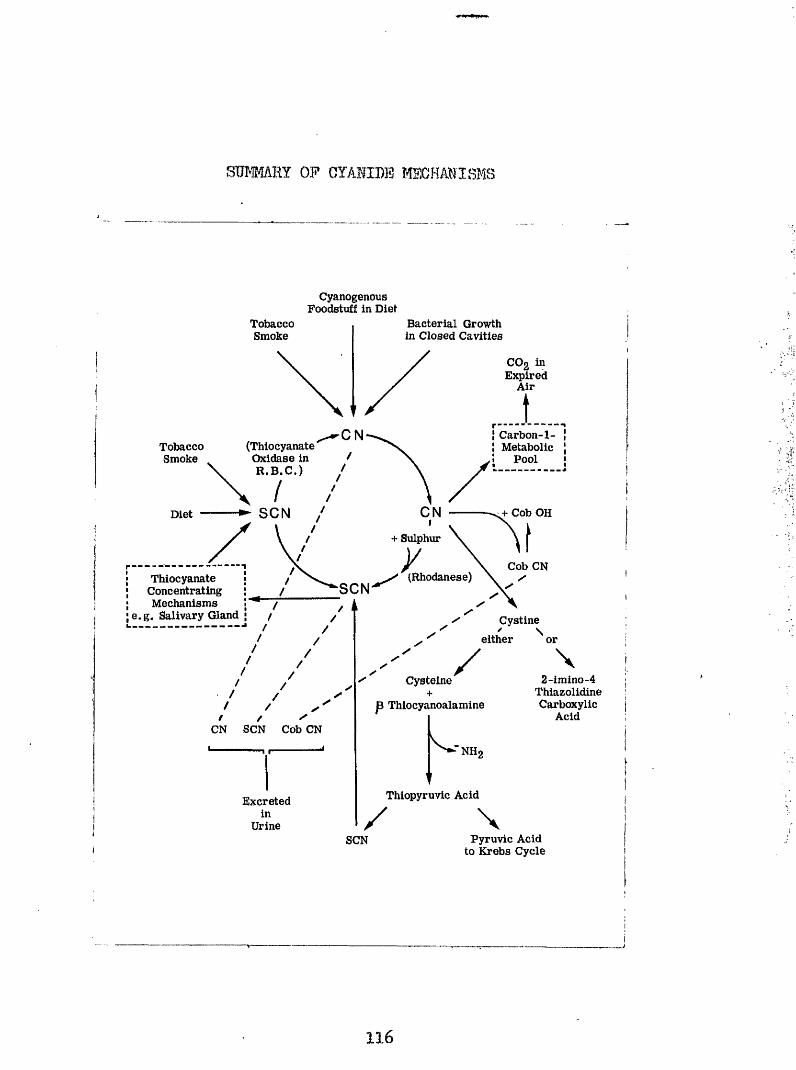
STOMAHY OP CYAMDB I4SCHANISMS
Cyanogenous Foodstuff In Diet
Bacterial Growth in Closed Cavities
TobaccoSmoke
COg in Expired
Air
N Carbon-1- Metabolic
Pool(Thiocyanate Oxidase in R .B .C .)
TobaccoSmoke
CNSCN Cob OHDiet
+ Sulphur
Cob CN(Rhodanese)Thiocyanate
Concentrating Mechanisms
e.g. Salivary Gland
SCN
Cystineeither or
2-imino-4ThiazolidineCarboxylic
Acid
Cysteine+
jB Thiocyanoalamine
^ “NHgCN SCN Cob CN
Thiopyruvic AcidExcreted
UrinePyruvic AcidSCN
to Krebs Cycle
1 1 6
et al 1963)1 1$ reeponsibl© for the positiverelationship between plasma cyanide and thiocyanate concentrations found in non#9mokers and healthy smokers by Wilson and Matthews (1966)*
Patty (1921) observed that organisms grown on stagnant protein produced cyanide in quantity. %is was especially true of the pyocyaneus and coliform organismsi ‘l?hus oyanide may be produced as a by-product in abscess formation» in urinary diverticula» or in the blind**loopintestinal syndrome (üngley 19551 Smith et al I963)*
'
Boxer and Pickards (1952) concluded from their studies On the metabolism of the carbon of oyanide and thiocyanate that cyanide carbon enters the carbon-one metabolic pool# Their studies made use of radio-active carbon as a tracer* Cyanide injected into the experimental animal appeared in the urine as free cyanide» thiocyanate» and vitamin B12 bound cyanide (oyanooobalamin). Cyanide and thiocyanate were found to be in dynamic equilibrium as demonstrated by the activity of hydrogen oyanide in expired air following the administration of labelled cyanide and thiocyanate* Activity was also demonstrated in choline
and methionine» and In the intermediate formatej aotivity waa also observed in liver proteins* These authors further state that the oxidation of cyanide to carbon dioxide occurs to a large extent*
Baumann and associates (1933) concluded that the thyroid gland had no part to play in the conversion of cyanide to thiocyanate but it had in the de-methylation of aoetonitrils, thus accounting for the increased excretion of thiocyanate on its administration# The tliyroid gland along with the salivary glands form part of a concentrating mechanism for thiooyshate* Olemedson et al (i960) demonstrated active secretion of thiocyanate into the gastric juice# and deposits of thiocyanate in the walls of the major blood vessels by means of auto-radiographio studies#
Oyanide Semyellnation*
Wilson and Matthews (I966) thought it possible that relatively low (though physiological) vitamin B12 conoentrations may reduce the body*s ability to detoxicate oyanide and result in relatively high blood concentration
118
QÎ this radicle* Suoh ooncontratioB© may contribute to the potbogeneaie of the neurological oomplioatioua of vltemlu B12 deficsienoy aa well m reported ahnormalitiee of pyruvate tolerance (Homabrook and larke 1#60)# Over the past 80 years much research effort Ime been put into solving the mechanism of oyanide dei;^ellmtlon without ‘ concrete auooeea* . The earlier workera used relatively large û m m of oymlde and the neurological leaiona were diverse and inoonatant» m d could not be separated from the effect of anoxia# . (Golllma end Itetland 19OB» Buret 1942# moke 1950, humaden 1950» Boee et al 1954» and Bovine and Biypulkowaki 1959)* That cyanide in small 'dcmea was capable of producing fool of -dcmyelination in a conatant and reproduceable manner was shown by Smith et al (1963) and Smith and Duckett (1965). . It has further been demonatrated that the liver atorea of vitamin B12 in ' the experimental animal were depleted on chronic oyanide administration (Braokkan et al 195?)» and that over a long period the ability to excrete the bulk of the administered oyanide se- thiocyanate was lost (Smith mid Duckett 1965)* Huohett et al (1952) have shown that hydroKOOObalamin protects the laboratory animal against lethal doses of
119
oyanide» a property confirmed by the studies of Smith et al (1963) and found not to be shared by oyanooobalamin (Smith and Duckett I965)# The latter researchers felt that hydroxocobalamin in some way preserved the integrity of myelin# as there was no evidence of demyelination in a group of animals subjected to chronic oyanide administration covered by hydroxocobalamin such as there was in a comparable group of rats in whom the oyanide was covered with oyanooobalamin*
Gystine# a highly insoluble amino acid# is capable of passing freely through the blood-brain barrier and becomes incorporated into the neural proteins (Ford et al 1961)* Oyanide combines with cystine to yield 2-imino#'4*‘thia^olidineoarboxylic acid both invivo and in vitroo(wood and Cooley 1956)# These authors further found that the expected reaction on combining cyanide with cystine to yield cysteine (Toegtlin et al 1926), and B-thiocyanoalanine did not occur under normal physiological conditions in the experimental animal* The thlooyano- alanine would yield thiocyanate after deamination to thiocyanopyruvio acid and subsequent decomposition. This
1 2 0
aomvoreion may Indicate m alterna tlv# pathway of cyanide dotoxication* The imiwrtance of thiaaolidlnaoax/boxyllo acid in relation to denyelinaticin is as yet mtoown*
Methods. Itsed in the api^lysls of pvanlde end thiocyanate
In a critique of the methods for thiocyanate determination Stoa (195?) observed that the Pyridine- Benzidine reaction was the method meet m l table for the determination of thiocyanate in blood aerum# Aa a routine method of aorum analyais tlio pyridine^bonaiidine method cannot be rivalled# as the reaulta obtained at low conoentrationo of thiocyanate were as reliable as those at high oonoentratiens. This property was not shared by theFerric nitrate method which is not accurate at low Gonoentrations $
In the earlier part of this analysis the Ferric nitrate method of Bowler (1944) was used as this was the only method available* later when in reoept of a Medical
1 2 1
Researoh Gommll grant# determlaatloma were carried out after pyrldi%ie#*ben%ldine meMiad of Aldridge (1945)* iu thie subsequent portion of the oaalyaio# the amendment® of Wilson (1963*65) to the Aldridge method# and the aeration technique of Boxer and Biokarda (1952)# were followed*
(a) 0plp3t?ifflptria yalyale of Ferric fhioovanate (Bowler 1944)
To 1ml* of serum in a test tube# 6*5 ml* of water and 2*5 ml* 2(# friohloraoetio Aoid are added* Mix and stand for 10*15 minutes* filter* To 5 ml# filtrate add 5 ml# ferric nitrate aoid reagent* Bead in photo-, electric colorimeter using transmission of wavelength 470 m u* from a standard curve the optical density readings are converted to milligrams thlooymate*
ferrie Hitrato - litrio acid reagent is prepared by dissolving B'errle Witrata in 2 I nitric acid* Standard curve is prepared by measuring the optical density of known concentration of potassium thiocyanate solutions*
(b) qp^oyimetgie amlyBis of 194S>
12s
I# X ml* sample (depreteimieed plasma,# or urine).IIfO#5 ml. Ÿ Hydroehloric Acid*
2. 0*1 ml* (â drops) solution of Bromine water# Thiscouverte oyanide and thiocyanate to cyanogen bromide*
3# 0*1 ml* ^ araonious aoid - removea exoeee Bromine* Shake well*
4* Draw air off surface of liquid with water pump to remove any %»omlne vapour preemt#
5* Add 1*8 ml* of fro# Beuisidiiie-pyrldine mixture*6* heave lg*20 minutes.7# Head in epeotro-photometer at a transmiesion wavelength
of 532 m yU, The optical density reading is oonverted to micro moles (xm) per 100 ml#.' from a standard curve prepared from known ooncentratione of potassium thiooyanato.
2^ araeniôus aoid ia prepared by dissolving sraoirioue oxide in sodium %<£lroxid#' solution* The solution is then rendered aoidio by back titrating with aoid using phenophthalein as indicator till jh ? Is reached#
The Beai^ldim-pyridine solution is freshly prepared by mixing a solution of pyridine with a benzidine
123
©olution in proportions 5 * 1*(a) pyridine solution in Hydroohlorio aoid is prepared
in the following proportione - Pyridine s Gone* llydroohlorio aoid * water - 6 « 1 s 4»
(b) Bensidine solution is prepared m a 8 5 w/v oolii* in Sydroohlorio aoid*
Analysis of urine for thiocyanate ia carried out S0 followas- .
t* A 20 ml* aliquot of.urine is diluted in 200 ml* with distilled water* 1 ml* aamples arc taken for thiocyanate estimations after the method of Aldridge*
2« lo farther preparation of the urine is required unlessprotein is present• The protein must he removed byprecipitation, with friehloroaoetlc acid before dilution la carried out*
(o) Sanroteiniaatipn o^.olaamai
1* 10 ml* blood placed in a heparinlsed tube*2m Centrifuge at 3,000 r#p*m* for gO minutes*3* 5 ml* of supernatant plasma are then mixed thoroughly
with 10 mis, 10^ Trichloracetic acid# allowed to stand
124
for 10 minutes emd then centrifuged for 30 minutes*4* Supernatant is then decanted into a $0 ml# volumetric
flack, or an aeratiom-tube*5* 5 ml* lO o frioliloracotic acid arc then mixed with the
residual protein coagulation and c0nt3Èi.fùged for a further 10-15 minutes*
6* fhe empematant is decanted m before*7» Steps 5 and 6 are now repeated two farther times.8* the volume of eupejmatant fluid la now 30 mis# This . ia either diluted in'the voitusetric flask to 50 mla. by the addition of diatilled water, 1 ml, aample# being used for thiocyanate estimations after the method of ■- Aldridge, or the 30 mla# are used for the estimation of plasma cyanide* ^
The method of Aldridge makes no distinction ‘ between thiocyanate and cyanide* The cyanide being volatile ia removed by the aeration technique of Boxer and Rickard© (1952), as ■follov>/et-■1, The ample before dilution, 30 mla* of deprotelïâaeâ
plasma, is placed in an aeration tube*
125
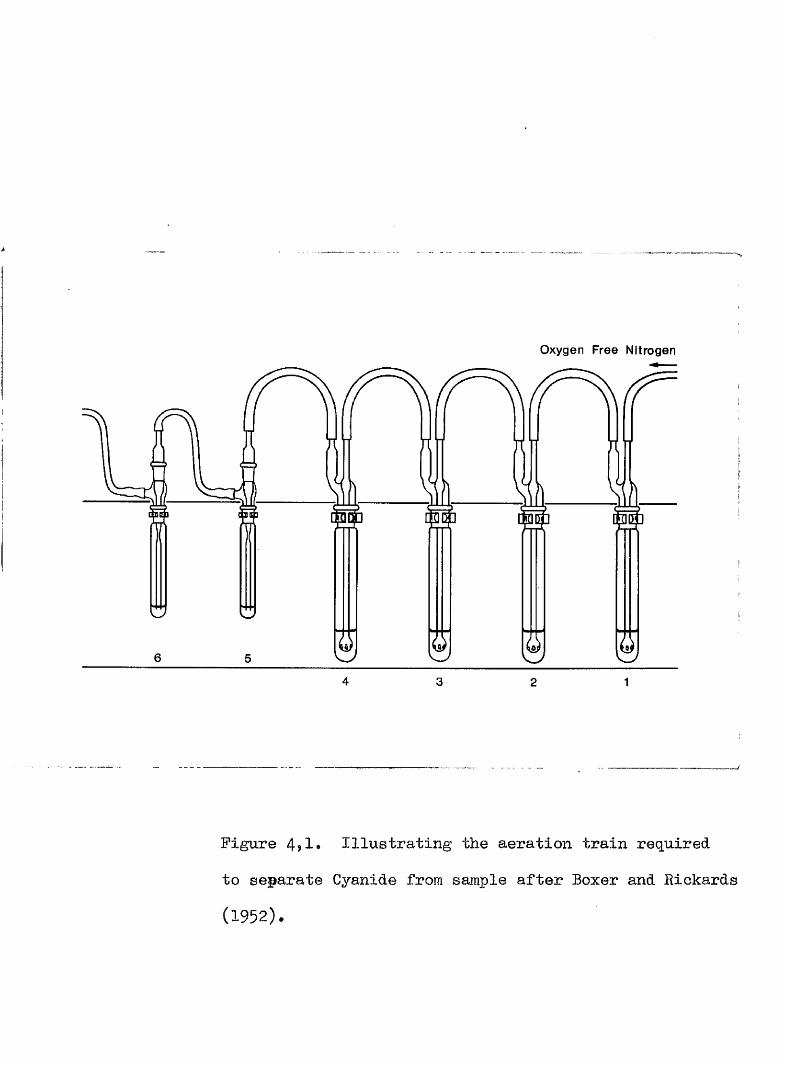
Oxygen Free Nitrogen
W
4 3 12
Figure 4?1« Illustrating the aeration train required
to separate Cyanide from sample after Boxer and Rickards
(1952).
2#' fnia tube le p M m à in àm aemtlon train ae f#Iawe# lie* I 20 ml & mvi0 Bulphate in sulphuric aoM*Be. 2 20 ml 20# w/v Silver sulphate in y sulphuric aoid.He» 5 20 ml$^ Sodium iydroxid© oolutlon*.
No* 4 Sample#lo* 5 1 ml* § #diu# hydroxide aolutlon#No* 6 1 ml* V sodiua, hydroxide eolution*
3* Oxygen free nitrogen is bubbled tîirough the train .at a flow of 790 mle/mirnte for one hour*
' ■. ■'■ -4# êfter this'time the sample ia diluted to gO mle*
before and 1 ml* aamplea used to measure the thiooyabate concentration*
5* # 0 & ml* eamplcs of sodium hydroxide not as an alkali trap for oyanide and the measurement» are carried out on them directly by the method of Aldridge* fhe mm of their omcentmtlome gives the cyanide ooncentration
) i I
in the original sample of plasma^ l*e* in 5 mis* plasma#
The cyanide estlmatioii in urine requires a alight modification of the aeration technique, as follows**#
Tube Bos* l-»3 as before*Bo* 4 20 ml* aliquot with addition of 4 ml*
4H sulphuric acid*Bo*. 5 repeat of eerie sulphate solution*
1:6
Ifo# 6 repeat of silver sulphate solution <Mlo* 7 80 mlsgwx sulpWrio aoid#
Bos# 8 end 9 alkali trap®
The aeration time ia B homm# The a lk a li trap
is ©hanged after 1 hour, m d the oyanide oontent in êietriWteâ in 4 eampl## ef I ml# sodium liyaroxido#
After aeration dilution of the 80 ml# aliquot to BOO m%B$ ie carried out as before and 1 ml# eemplea are taken for thiooyanute amlyeim,
,ln. .Tqîmooo âfjiblyopia#
8emm thiocyanate determinatione by Bowler’smethod (1944) were made m three |p;mipa of mbjeete# GroupI eoneinted of 40 patiwte suffering from tohacoo amblyopie, dia^oeod aoooz'ding to t*)© criteria of B m t m et al (iggO)#In group %I were 37 non#mblyopio emoking auhjeeta dmum from a hoBpita& population# Group III contained # non- smoking Wepital patients# Thoee In group II and III were elderly patiente attending lioepital with ooMitlme imrelated
187
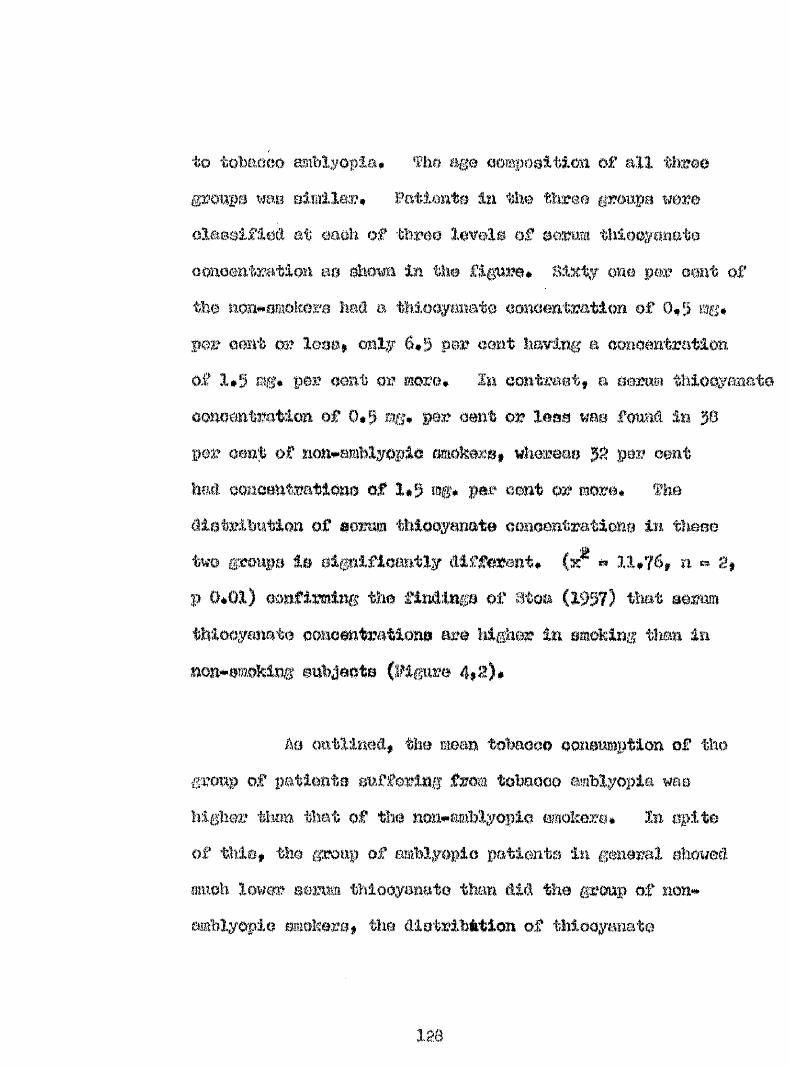
to tobaaoo miblyopia# oomposltioxi of all threegroupa was olmllm?* Patimte i*i the three groups were olaeelfled at eaoh of three levels of aemm thloaymatao<moentratlo%% as show In the figure# Sixty one per omt of the non omokere had a thlooyanato eomentratlon of 0*5 mg*per eemt m leoe# only 6*5 per cent having a aonoantration of 1*5 % * per omt or more* In oontmot, a oezm* thioqyaaate ooaoôtt'teitioa o f 0*5 mg# per cent o r less mm foiraû Im gO
per Qm0 of aoa#emblyopio mokera, whereas g: per cent had oomoehtmtlome of 1*5 mg* par omt or more* the cliateihiitioa o f aomm thloa anate oonoentratlohe ia these two groups ta el#lfioamtly different* ^ 11*76, ri 2$ p 0*01) eomfimih# the findings o f Btoa (1957) that aerm thlooygmate oonoantrationa are higher in amoking tlian in mon^emokim# euhjaota (figiire 4,t)#
Â0 outlined, the mean tohaoeo acmaimption of the grmp of patieiite suffering from tohaooo amblyopia warn hi#ier thm that of the no%i#amhlyopio mokere* In spite of tills, the group of amblyoplo patients in gmeral showed mmoh lower &mmm thiooyaaato than tlM the group of non# emblyoplo mokere, the âietrihàtion of thiooyanate
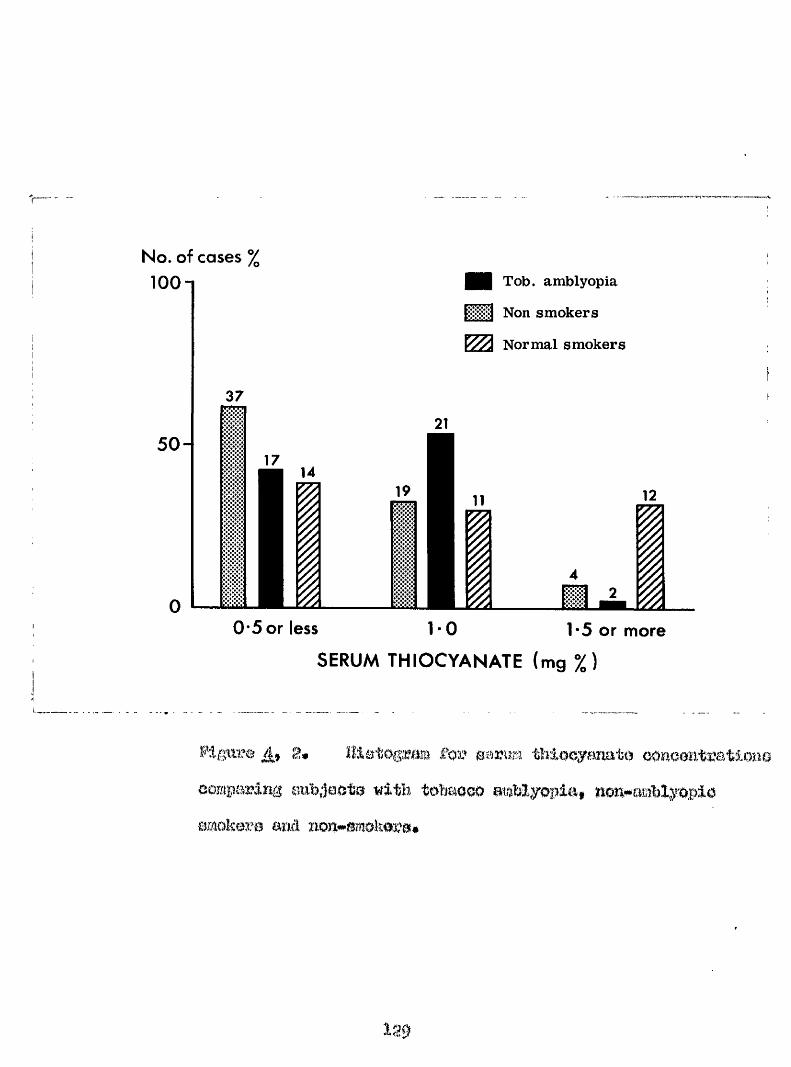
No. of cases %
lOOn
50-
37
14
I
i m Tob. amblyopia
Non smokers
Norm al smokers
12I0 5 or less 1 0 1 5 or more
SERUM THIOCYANATE (mg %)
SUgiir® 8» t’ot' Btmm thiocyanate oOHoanteationoecmparlng snh.iooto with toMoco atamyopla, non-aablyopio smok®3.’0 and non-smokosa.
139
concentrations being significantly différent In the tvo9:;*oups (%*' Î* 10*47$ ^ 2» f 4 0*01)*
Somewhat fôtirprieingly, in apit© of thoir heav; ooîieuî iption of tobacco, the distribution of thlo%mnato concontratlono In thio group of mmhlyopic patient© rGoemhlod that of the noii amokora end in fact the distribution of th.ioQyanato concentrations in thooe two groups waa not oigrjlfioautly different «» 3,9% n # 1, p> 0*05)•(Soo appendix B0)*
These relatively reduced oonoentratiouB of serum thiooyaiiato in tobacco amblyopae m compared with healthy cmokora, cuggost that if cyanide derived from toWcoo smoke is indeed a factor of aotlological importance in the development of tobaooo amblyopia, the biochemical defect in theao oaeoa may be a failure of conversion of oyanide to thiocyanate, its main detoxification product, as cuggoatod by Smith and Duckett (1965)#
B* During frea’tnemt wit!
Sorum thlocyanato eist.imatlona we»o sopoatotil aftor
1 3 0
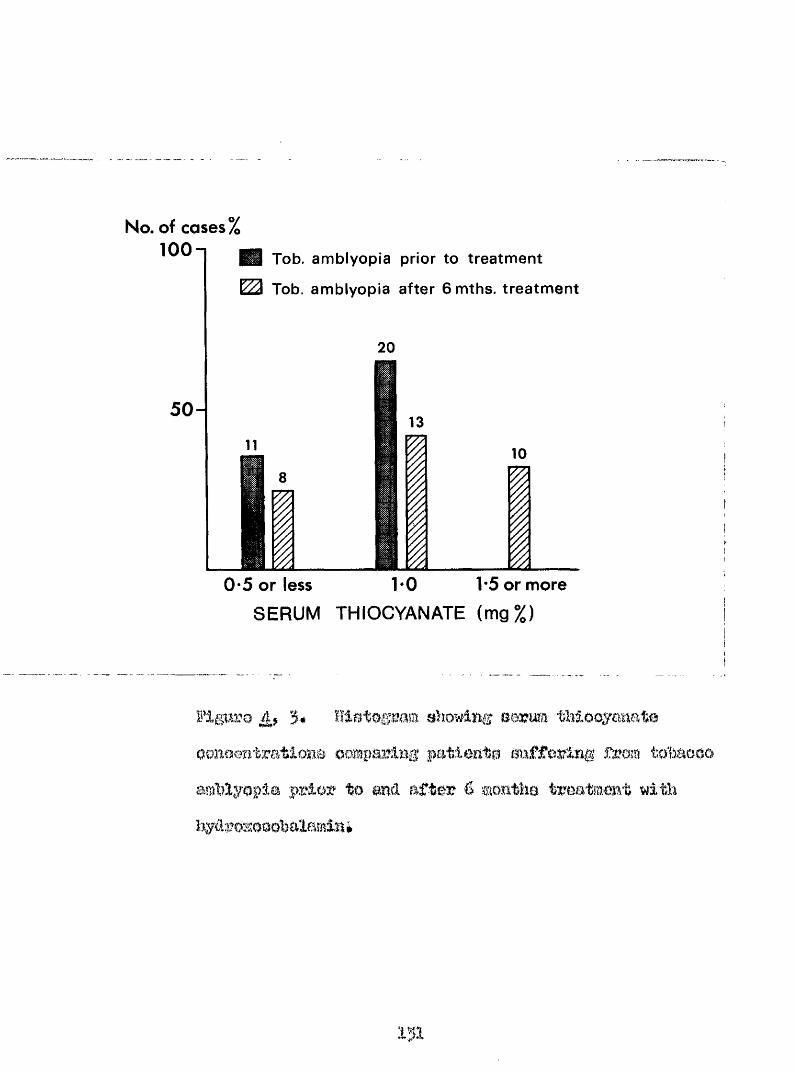
No. of cases % 100
5 0
Tob. amblyopia prior to treatment
Tob. amblyopia after 6 mths. treatment
20
13
I10
0*5 or less 1-0 1*5 or more
SERUM THIOCYANATE (mg%)
3* nistogram showing serum tMooymate oonoentratlone oomparlng patients Buffering from totaooo amblyopia prior to and after 6 months treatmmt with hydrozooohalamln*
131
aix month© treatment with hydroxocohalamin in the group of patients with tobaoco amblyopia* Of the 40 patient» with tobacco amblyopia who had serum thiocyanate estimatione carried out by Bowler*» method described above, only J1 were availsble for repeat analyaie after 6 monthe* The reasone for tbia included replacement by Aldridge’s method for Bowler’s method, default, and death of a patient* Detailsof the treatment are given in the appropriate section*
Mhcreas 11 of the amblyope» had a serum thiocyanatelevel of 0*5 or less, 20 had a level of 1*0 andnone a level of 1*5 or greater^ after 6 months treatment 8 aubjeots had a level of 0*5 or less, IJ alevel of 1,0 mgm^ and 10 a level of 1*5 mgn^ or greater^There Is a significant alteration in the distribution of
pthiocyanate levels in the treated group (% - 10,02, n ^ 2, p 0.01), 80 significant difference in distribution iadetected when the treated group Is compared with the non- amblyopic smoking group of the previous section {x^ ^ 1*57# n w 2, p S3 0*5)*
Plasma Oyanide and ThlcoyaBOte Gonoentrations in
Wilson and l latthowa (l$ô6) showed that a negative relationship existed between the plasma oyanide and aerum vitamin, B12 oonoontratione in healthy ©mokere and non-smokera* Plasma cymid© ooncentrationa were estimated in il patients suffering from tobaooo amblyopia by the method described above and the serum vitamin B12 concentration was estimated after the method of Boss (1952)* Bee Table 4# 1 for results*
Of these patients the mean cyanide concentration was 0*065 Ï 0$0:4 mioro moles/lOO mis* This value is considerably higher than the value of 0*022 micro moles/100 mis# found by Wilson and Matthews (1966) in non- amblyopic smokers by a similar method of analysis* When the plasma cyanide and serum vitamin B12 were compared a negative correlation was obtained, and this proved to fall just within the significant level (r « #0*555» n « 9»0*05 <p <0»l)# Although not a very significant correlation, possibly due to the small number in the sample, the general
153
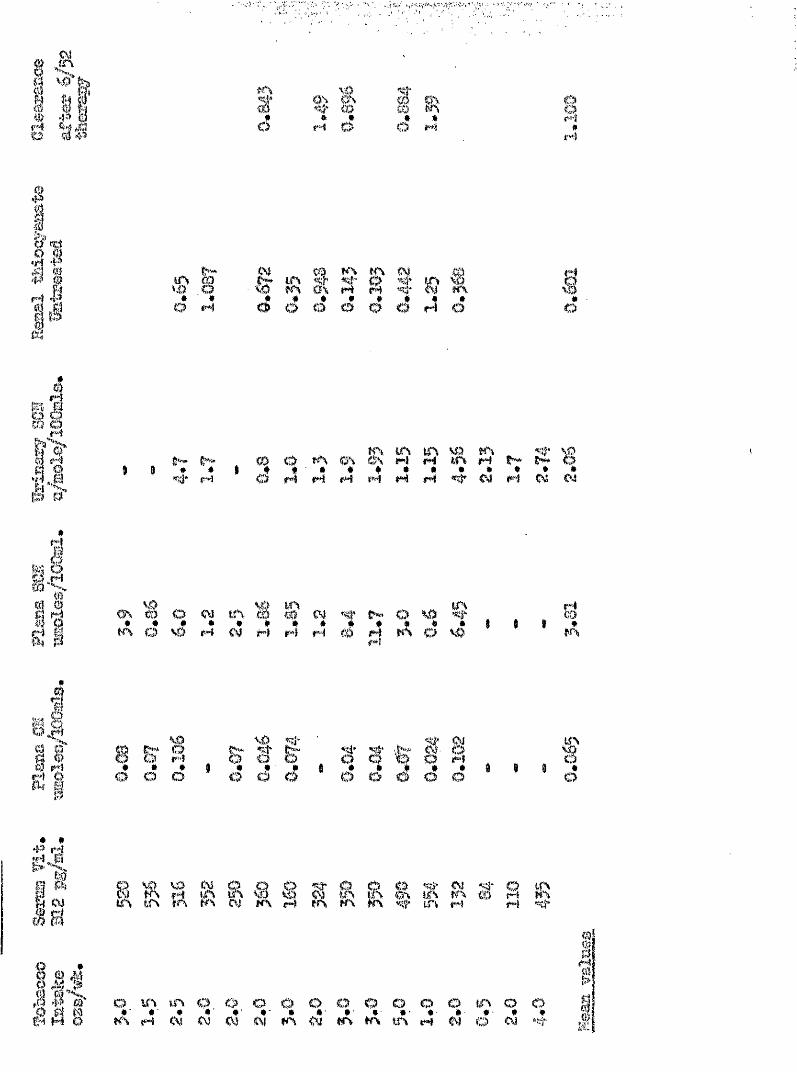
iar4 W 4jd c?OS* #M O
m*O M I#
m)
1 1 I s
Hf*4 <r?@ g
_ ^ N CÛ KS K\ (M _ 0® § 15* ^ s( ^ s ^ t« ' * « # # * # # « • O M O O O O O O H O
Io
I
r4i?>d MII K\ W\ tn \0 KS ^Ê* 0) O 0\ &S M kfS M I** O* * $ * # ' # * * # # # # # * #««xj* M # N M N M N M C4 ml 04
#
ifm ë< A % 0* * * # # # * *t r \ O \ D M N ml ml H
'-W SSVmiml
trsO V) <f‘ « « • K\ O V) I 9c3m
B.#■'*1aa «
é
\Ù g!" O». * to o b# # ' #o o o
3* f % I’ IÔ o o <5 o
fc?
lil
8 i R % % & a @ g & A & X % 3 5 l Rit% t n in o i K% ml ers fn #A %f m M M
o v s t n o o o o o o o o o o t n o o#' *■ • •’ #' •' ê *• #■ •■ •• ♦■ #' #' * *K \ M 0 4 ( \ i O ( V K \ < V K S W \ W \ M W O OI
41I
trend does support the view that high plasma oymlde oonomtratlom In # 0 preoenee of redueed serum vltmlnII a eonoaatratione ooald Ise ussooiateci with neurological lO0lOA8,
On comparing the plasma oyanide ooaoontmtlon with the omonmptlon of tobaooo (tho prommed eouroo of ©yaaidt) ii% these patlonto a poaitivo correlation waa obtained which failed to be olgnlfloant (r # 0*344$ n M* 7# p>0#l)#
flia mean plaasa thiooyanato oonoentratiom of Ig imtrmted tobaooo mblyopoa was found to bo g#8lt 3# 386 mloro molea/lOO mie* This value le lower than #iat Qbtalnod, by a olmllar method of amlyalo# by Wilson m d Matthews (1966) who found a mean oonoontmtlon of 11*5 mloro molee/lOG mle# In 18 non-eWblyoplo emokere* Them autWra fhrtWr deaorlhod a 8l#lflomt poeltlvo eormlatlm hetwemx the plama oyanide end plaama thiocyanate oonomtmtlono# On oomporlng thoee two faotoro In the present group# the oorrolatlon obtained# although positive was m t eignlflemt (r $0#351$ n 7; p>0*l)#
Ae desorlbeâ above# a rise ia the aorum thiocyaiiate concentration oocura on trea#mmt with l^âroxooohalamiïi for tobaooo amblybpia# If # m renal olomranoe of thiooyaaate rmtilmd at the value of 1*33 ^l* per ailmte# found by Btoa (1957)# t h m the rioe in blood tnioofBnato may bo mfimtml by a rime in iirinaiy exoretion# Thmoon (igO:) foimd #at the toxicity of the wine in tobaooo mblyopea# treated by abatimenoo from tobaooo# readied a podc 7#14 df yo after # o oommenoement of troatmmt and was aooompaniml by a diwoala, This Inomaoo in toxicity wao taken by him to indicate the body getting rid of poieonoaa aubatmoes# The renal clearance of thiooymate wae foimd by Thomas (1949) and $toa (1997) to depend on wine volume m d renal excretion of chloride# as the thiocyanate ion Wiavee ne a pemdo halogm# Wokoe m d Bllia (1966) found that the diwnal rhy#m of reml thiocyanate olearanco paralleled that of the total nitrogen clearance#
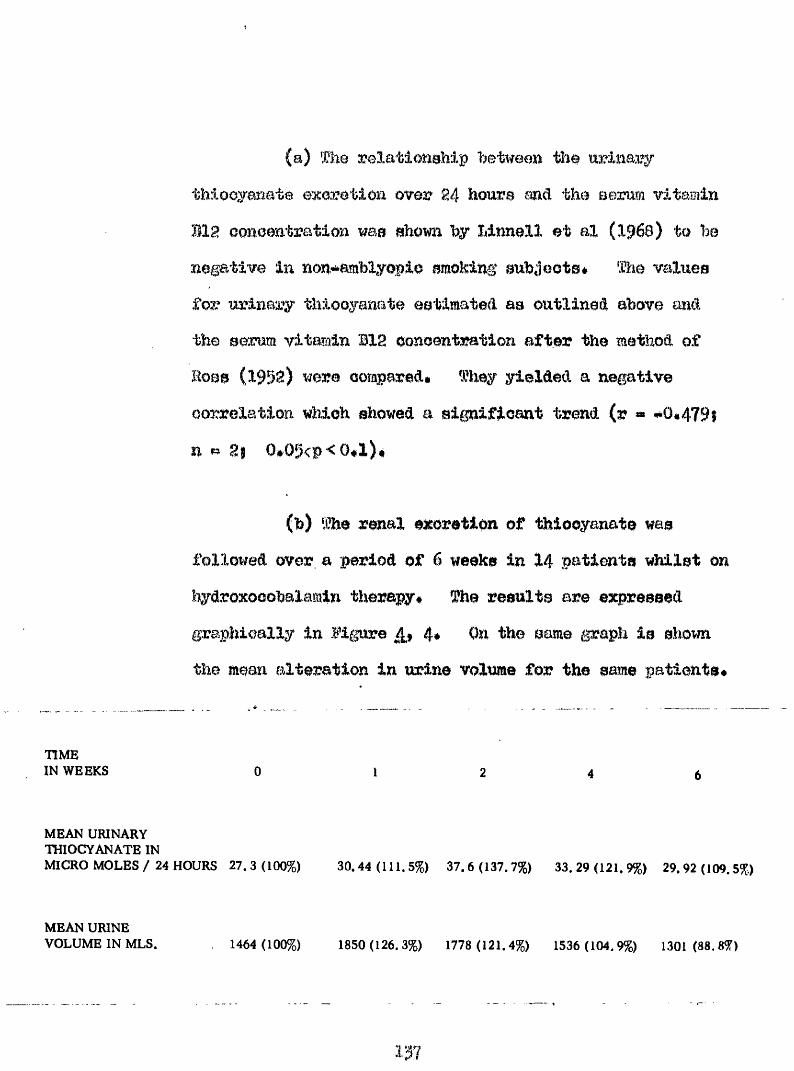
(a) The relatioBahip between the urinary thiooyanate excretion over 24 hours and the serum vitamin B12 oonoentration was shown hy Mnnell et al (1968) ta he negative in non**amblyofio smoking anhjeots* The values for urinary thiooyanate estimated as outlined above and the serum vitamin B12 oonoentration after the method of Robs (1952) were ooapared* They yielded a negative oorrelation which showed a significant trend (r « #0*479$ n ^ 2i 0#05<p<0*l)$
(b) The renal excretion of thiocyanate was followed over a period of 6 weeks in 14 patients whilst on iiydroxooobalamln therapy* The results are expressed graphically in figure 4* On the same graph is sWwn the mean alteration in urine volume for the same patients*
TIME IN WEEKS
MEAN URINARY THIOCYANATE INMICRO MOLES / 24 HOURS 27.3 (100%) 30.44 (111.5%) 37.6 (137.7%) 33.29 (121.9%) 29.92 (109.5%)
MEAN URINE VOLUME IN MLS. 1464 (100%) 1850(126.3%) 1778 (121.4%) 1536 (104.9%) 1301 (88.8%)
137
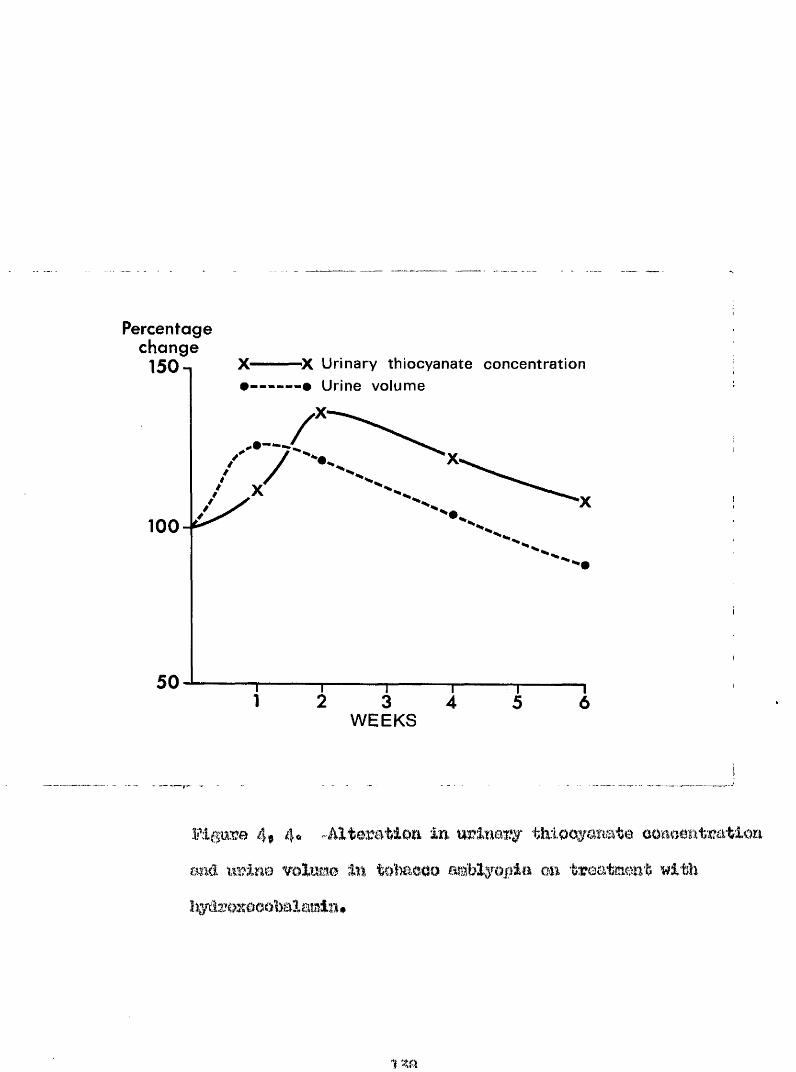
Percentage change
X Urinary thiocyanate concentration '# Urine volume
150-1
100
50
WEEKS
4f 4o Altération in urinary tlnloc^anate conacmtratlori ailé urine volume 1% toîmcoo cm treatment with
1 m
There van a r tm in the u riîia ry exeretlon o f
tMooyaaat© on treatment w ith liydroxoeobalamin* which
reached a peak a t 2 weekc* ehowliMI a inoreaee* before
alowly declin ing* â s im ila r ric e was noted in the nrinary
volume*
(c) Stoa (1957) examined the renal thioeyanate clearance in healthy amokera and non#*am.Dkera* He foundJ' : an average clearance of .1*33 ml* per minute, with a rahge'v> of 0*14 - 3.* 53 ml#* per minute* There wa# no correlation hetween the thiocyanate concentration in the blood and the renal clearance for thiocyanate* In the preeent group %, of patients a significant negative correlation was found between those two factors (r « n # 0#001<pc0*0l)(B’igura 4»5)* After six weeks therapy with hydrozocobalaminthe correlation showed a trend to becoming positive (r w f0*770; n m 3§ p> 0*1)# The average clearance of thiocyahste rose from 0*601 to 1*1 mis# pei* minute on this therapy after six weeks*
139
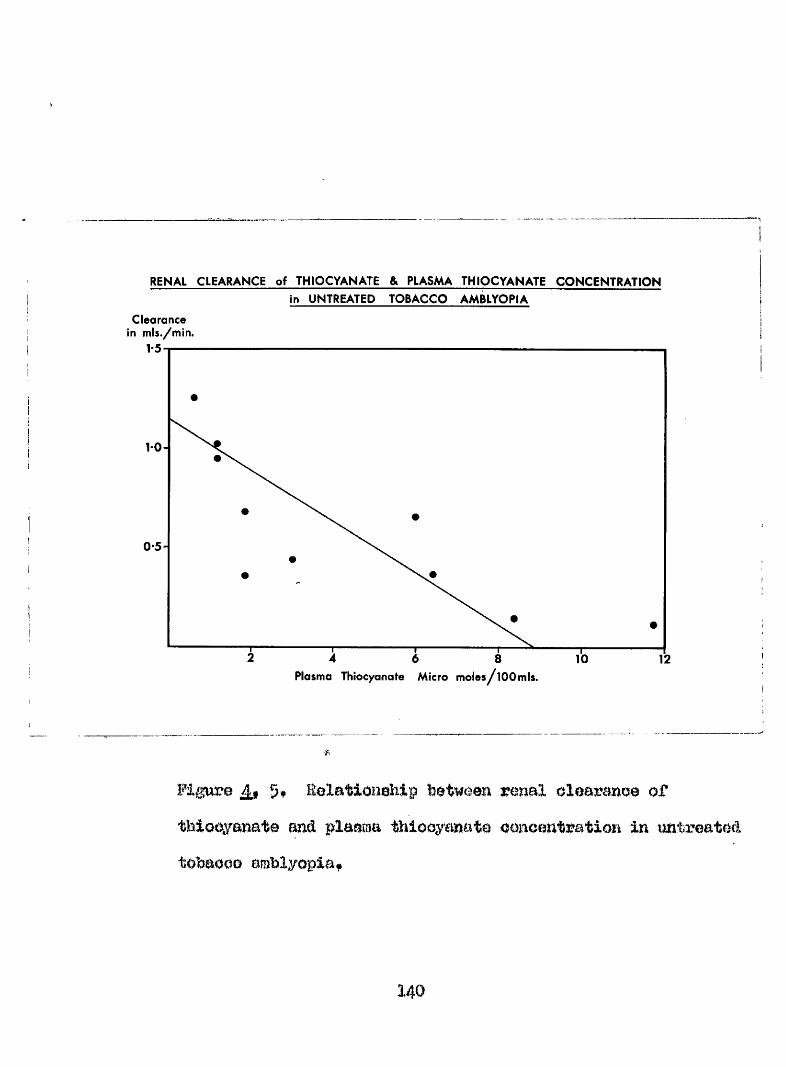
RENAL CLEARANCE of THIOCYANATE & PLASMA THIOCYANATE CONCENTRATION
Clearance in m is./m in.
in UNTREATED TOBACCO AMBLYOPIA
1*5
Plasma Thiocyanate Micro moies^lOOmls.
Fipœe % Eolation^hip renal olearanoe oftbiooyanate and pl&ama thiocyanate ooneentration in untreated tohaooD amblyopiaf
140
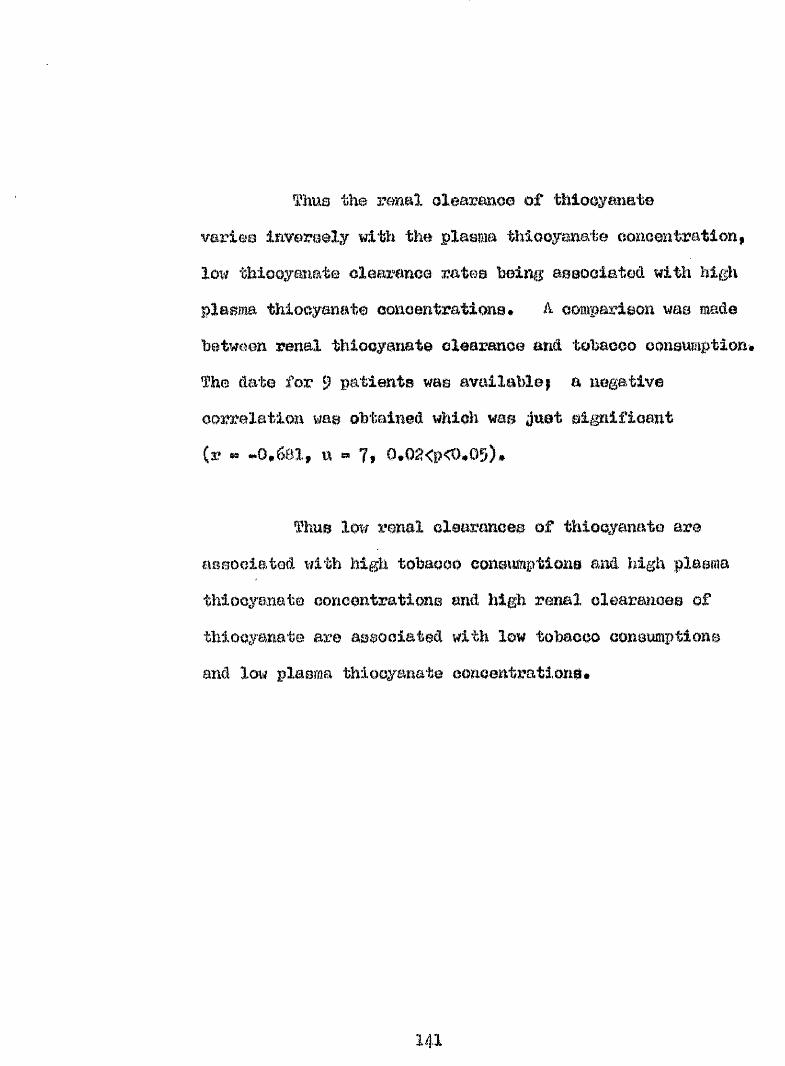
ThUG the renal olearanoo of thiocyanate varies inversely with the plasma thiooyanate coïioen trail on low thicoyaiiat© clearance mtea being associated with high plasma thiocyanate concentrations * A comparison wae madebetween renal thiocyanate clearance and toWcco ccnsmaption# The date for 9 patients was available; a negative correlation was obtained %Aioh was Just significant (r -0*681f u » 7# 0,02<p<0#05)#
% n s low renal clearances of thiocyanate are associated with high tobacco coneimptlons and high plasma thiocyanate concentrations and high renal clearances of thiocyanate are associated with low tobacco consumptions and low plasma thiocyanate concentrations.
141
âlistlnenofâ from tobacco has boon considered neoeeeary# important> or desirable in the eiiccessfal treatment of tobacco amblyopia (Hutehlnson 187)# Webster 1880* Hartriilgo 1886* Ohieholm 1890# Fairley 1901, Dyle 1905, Oarroll 1935» ^ambrasin and Bohepene I946, Hedges 1957, Boggart 1959)# For many years this belief was thekeystone of treatment, till Oarroll (193?) showed that_abstinenoe was not necessary# 9?he effect of pharmacological preparations has been investigated by authors to ascertain which, if any, accelerated return.of visual finiotion*
The earliest and most popular drug used was strychnine# Injections of this drag were considered to hasten recovery by Chisholm (1878); combined therapy with strychnine end potassium iodide was used by hautenbaoh (1898) and Findlay (igOl), Hartridge (1886) in a controlled series, discontinued smoÿlng in all patients, administered strychnine to half, and a placebo to the other
14^
(3d* agsxpgip iwN&#agi%Gdl3.;y igSKKl,
Tüdltdb llim
m
I nitrites were used by Powers (1886] g%%k) (wuGoewse t&iibh t#t& tiee <)f
m d lfa»ington (19)5) was
that vlemlI m p m v m m t was hastened by m d that tMe d m # was superior to nmâ%m
*1
diet# I te;e (m (a&OQuadx)
> a partial or complete reoovery# in ei twae of tw)%H&oeo üwloo&woüL* Ils* (%&$
il/tBi tfGwe aw) 4gcM&d ate awa&r %%&(&vdLowei (sawejLee* jku wiiidsti idbe
rhBimû. from tobaooo. Oarroll further eWwed i#w&t lcw%#e dooGB of TfitaBdhi B c%mg&le% &%%& 8 iwall diet were eeaentiml for m rapid return of vision# GomeewKwxaoiBe iweae <)%ytw%&JOWSGl Tbgr tfsüüasaHoat (31S>30) Tbar &&&G) atd%BjU&:ltrtKK%&tdl(%KL
of vitamin B1 fThta^s
leatou et #% finding reduced
concentrations of vitamin B12 in the blood pi patients suffering from tobacco amblyopia, treated their patients successfully with parenteral oyanocobalamin whilst allowing continued smoking# Their patiente recovered vision more quickly than would have been expected on treatment with vitamin B complex* the dose schedule was lOGpg twice weekly, where amemia was absent, 1 0 0 daily for fourteen days followed by 100 twice weekly, where anaemia was present • Treatment was discontinued after six months if there was ■ no evidence of pernicious anaemia* Quatermas» (1950) achieved some success with parenteral oyanooobalasdn in the amblyopia found in a smoking alcoholic#
It had been shown that commercial preparations of oyanpcobalamin contained traces of other vitamin B12 analogues (Baxter et al 1955)» notably of hydroxooobalemln* This, reasoned Smith (196I) had brought about the cure in the patients reported by Heaton et al (1958)# As the result of a personal comnmnication this author is assured that the commercial preparations of cyanocobalamin and liydroxocobalamin available in Great Britain today do not now contain other vitamin Big analogues as impurities* (Snell 1967).
144
T re a tm e n t o f Tobaooa
The patiente la the proaeat study woro treated prenarationo of vitamin Dig maimfaotwod by Glaxoim VÆ V.L mxAi*
Itsboratorioo Btd* They were roquoatod not to el tor their oBXoMng habit# la gmoral» the patimte moolvod their first fourteen d%o troa#mt as in-patients in hoopltal# They worn reviewed, ae mar am poooihle# at monthly intervale# Adjuetmonto to Mxorapy wore made from time
%follow up period varied five months to thirty five monthe % ith a mean at ninetom month#*
The progroso of each patient at the end of tho follow up period was amoemood visually end graded by a oorloo of oymhale*#*
0 $» no ohango- % Woreonim
H Improvement in visual acuity to
0)7 35^ on the perotmtago acuity eoale#4^ A» Improvement In vlou#l amity to 6
on the poroenta# wulty eealo#
miell
145
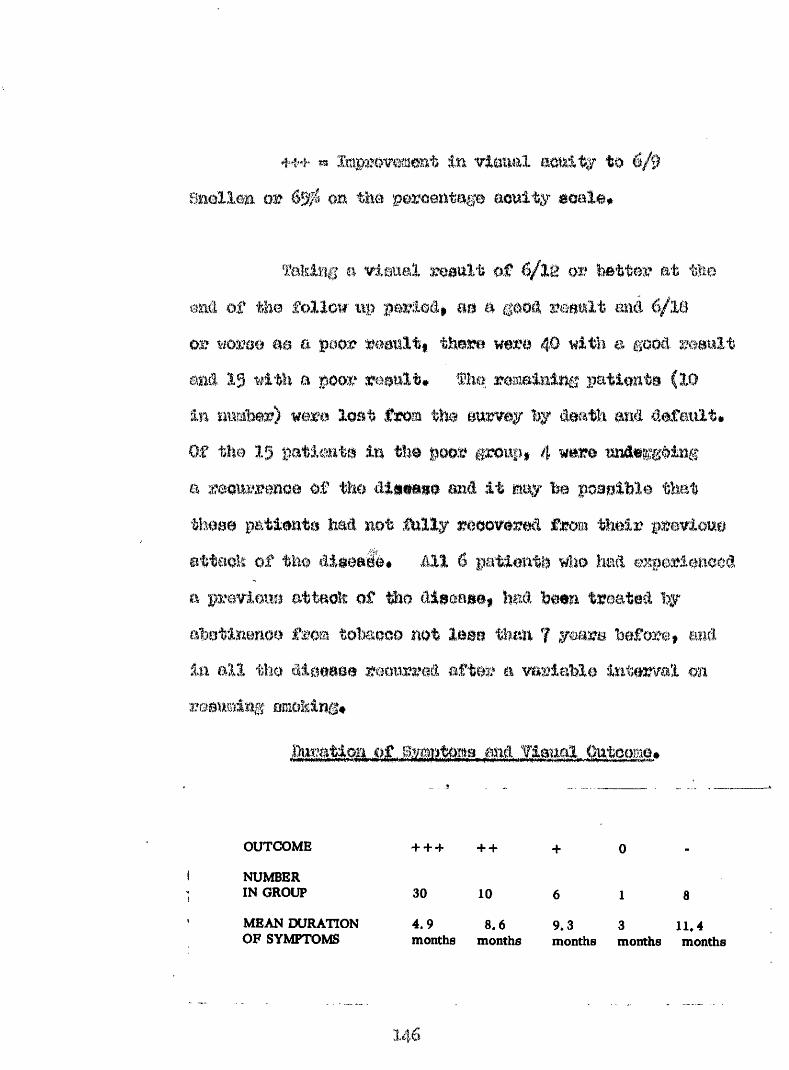
m or ony to
faking # visual reault o f 6/12 or Wttor at #e smci of #e follow' up period, m a good result and 6/lê or wome #a a poor roault# there were # witli a good and 19 with a poor result# The remaining patient#In n £S M
Of the 15 patlaite In t%)0 a roomTenoe of # 0
a p%*eviouo attack of #0
roup, 4 w#m undergoingi t may be poaslMe tha t
recovered fmm th e ir pi
6 patient# wlio had expo , had been treated by
&88B than 7 yearn before, am after a variable Interval on
OUTCOME
NUMBER IN GROUP
MEAN DURATION OF SYMPTOMS
+ + + + +
30
4.9months
10
8.6months
89.3 3 11.4months months months
Thus 40 patients (72.^) whose mean testation of symptoms, before seeking adTice, was 3*45 months, had their vision restored to 6/12 (Snellen) or better during the mean follow up period of 19 months and the. remaining 15 (27*8?l) (mean duration of symptoms 9.6 months) showed little or no Improvement, There is a significant difference between these ^oups (t *« 2*07; u 53? p<0*05)# Thus it would appear that the duration of symptoms influenced the outcome*
The 30 patients who had a visual improvement to 6/9 (Snellen) or better were examined for the rate of visual improvement* This group consisted of 26 patients who received hydroxocobalamin while contiîiuing to smoke,3 patients who were treated by abstinence from tobacco, and one patient who failed to respond to hydroxooobalamin and in whom visual improvement only occurred when smoking was stopped in addition to receiving hydroxooobalamin (Patient Ho* 52)* This patient is excluded from this analysis*
Of the 26 patients treated with liydroxocohalamiii only, the mean period of treatment over which the visual improvement oociirred was 6,82 i 4*49 months, The improvement in vision waa calculated from the ratio
initial visual aouityÿü The mean improvement in visual acuity per month of the right eye of the 26 patients was 1*75 ^ 2*)8 units.
Of the 3 patients treated by abstinence from smoking the mean period required to produce a visual improvement to the same standard was 3*0 months, and the mean improvement in visual acuity per month of the right eye was 1,58 t 0,54 units, The rate of visual improvement was thus equally good by either method of treatment (t c 0,264; u « 27; p>0,l).
Initially patients were placed on therapy alternately with cymocobalamin and hydroxocobalamin,
By analysing the first thirteen patients M whom seven
148
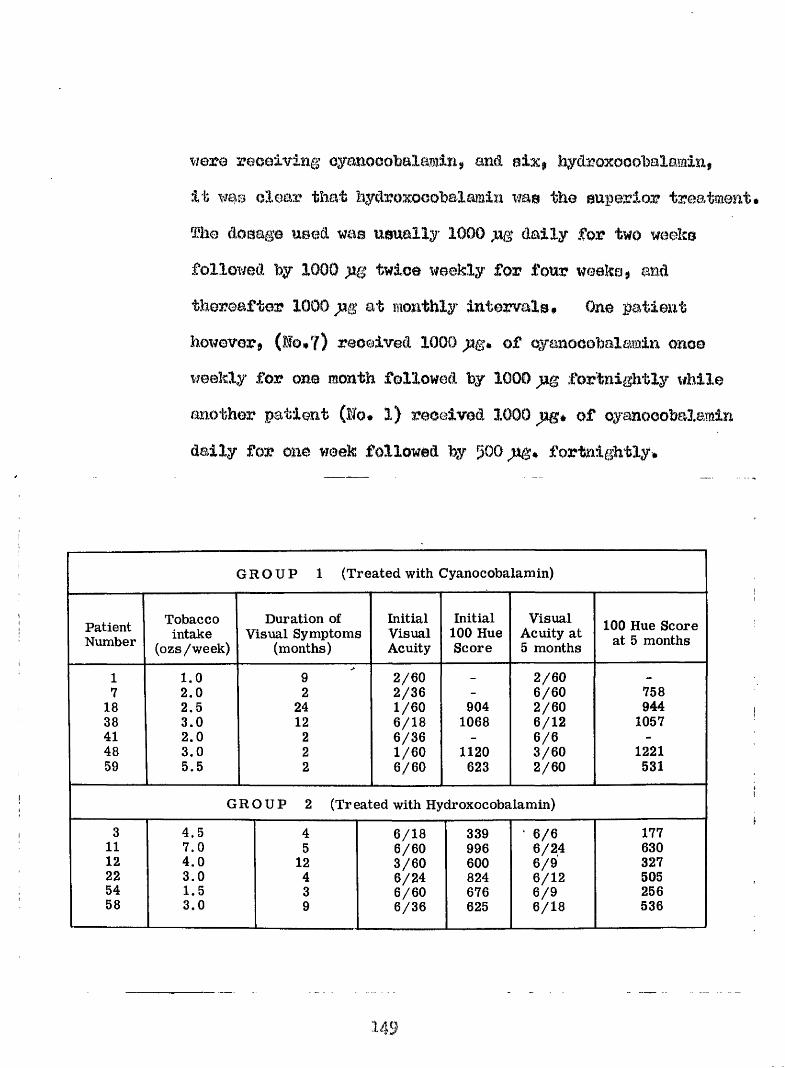
were receiving cyanocebalamin, and six, hydroxooobalamin.It was clear that hyclroxocohalamin was the superior treatment* The dosage used was usually 1000 daily for two weeks followed by 1000 jug twice weekly for four weeks, and thereafter 1000 at monthly Intervals* One patient however, (lo*?) received 1000 ag* of oyanocobalamin once weekly for one month followed by 1000 fortnightly while another patient (Ho. 1) received 1000 )%* of oyaaooobalamin daily for one week followed by gOO 3%* fortnightly.
G R O U P 1 (Treated with Cyanocobalamin)
PatientNumber
Tobaccointake
(ozs/week)
Duration of Visual Symptoms
(months)
InitialVisualAcuity
Initial 100 Hue Score
Visual Acuity at 5 months
100 Hue Score at 5 months
1 1.0 9 2/60 - 2 /607 2.0 2 2/36 - 6/60 758
18 2.5 24 1/60 904 2/60 94438 3.0 12 6 /18 1068 6/12 105741 2.0 2 6/36 - 6 /6 -
48 3,0 2 1/60 1120 3/60 122159 5.5 2 6 /60 623 2/60 531
G R O U P 2 (Treated with Hydroxocobalamin)
3 4.5 4 6/18 339 ■ 6 /6 17711 7.0 5 6/60 996 6/2.4 63012 4.0 12 3/60 600 6 /9 32722 3.0 4 6/24 824 6/12 50554 1.5 3 6/60 676 6 /9 25658 3.0 9 6/36 625 6/18 536
149
Details of the patients treated are met out In Table 1# All hut o w were pipe smoking elderly males* the exoeption was one who smoked only eigarettoe* All had impairiaent of oentral vision and of oolomz vision at the etart of the trial# The memi ago of the patients in eaoh group wae oimilar (Group 1 69#? years; group 61*5 years) alüiou^i group 1 ooatalwd eome patiente who were older than any in group 8# m e m tolmooo oononmption in group 2 woehigher than in group 1 (5*0 osa* per week ae compared with 2*7 0S8# per week)# The mean length of visual history was 0imilf3a7 In each group (group 1$ 7*6 months; grou%? 26*2 mmthe)* The slightly hi^ier figure for group 1 was
W proaenee in this group of one patimit with a history of vlmml failure (two yearn) *
To esBoae the reeulte of treatf^ent* the vieiml acuity on the Baollen teat type at 6 metres wder standard Qonditione of Illumination was expraeeed as a peromtagetakiïig ê/ê tm 100^ (Blclloy 1959)* %o improvement in
per month wa@ oaleulated as eliown on page
mean 3j%provement vieua
of the poorer eye of each caee Im the two groups Is shorn in figure 1, xAera it can he seen that both the rate and magnitude of the improvemait in vision of those 08888 treated with hydroxooohaXamin is greater than of those treated with oyanooohale^in, The recovery of
vision in the two groups is equivalent to an improvement from 6/60 to 6/9 in the case of those treated with hydrOKOOOfoaiumin and from 6/60 to 6/36 partly in those treated with cyanocobalamin#
There is a ai^^iifioant statistical difference between the two therapies# (The mean improvement in vision over five months for those oases treated with hydroxoooi tbalamin è» 5*54 4*4 %%nits# Mean improvement in vision over five months for the oases treated with cyanocobalamin« 1.91 * 1.64 HMi-iiS. (t » 0*39? a = 2; p » <0.05)]
Measurements of colour discrimination were also used to assess the progress of the condition in the .patients described above# The initial and final error scores with this test for each patient are shown in fable 5,1 where it can be seen that prior to the start of treatment, the error score was g#ossly abnomal in all
151
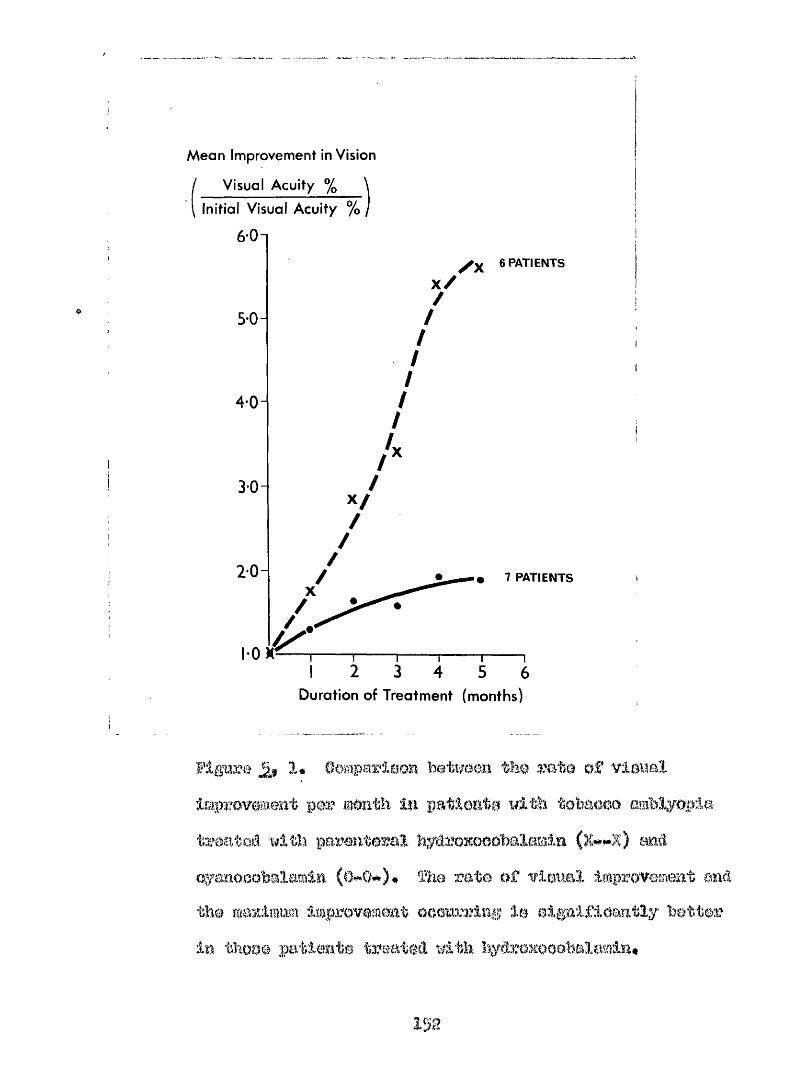
Mean Improvement in Vision
/ Visual Acuity % \
\ Initial Visual Acuity % /
601/ X 6 PATIENTS
X /
50-
3*0"
7 PATIENTS
2 3 4 5 6Duration of Treatment (months)
Figure 1# Oomparlùom betimm the rate of vlaual ImpTOveamt per moath la patlmte i&th tobaoae amblyopia
%flth pareateral hylroxooobalomla mtioyaaooobalamla 9)he ra te o f viaim l Improvemmt oaâ
tim maximum improvemmt ooomzizlag le elgalflomtly better In tïïooe patiente treataû with liyârexeoebala^lm#
ig e
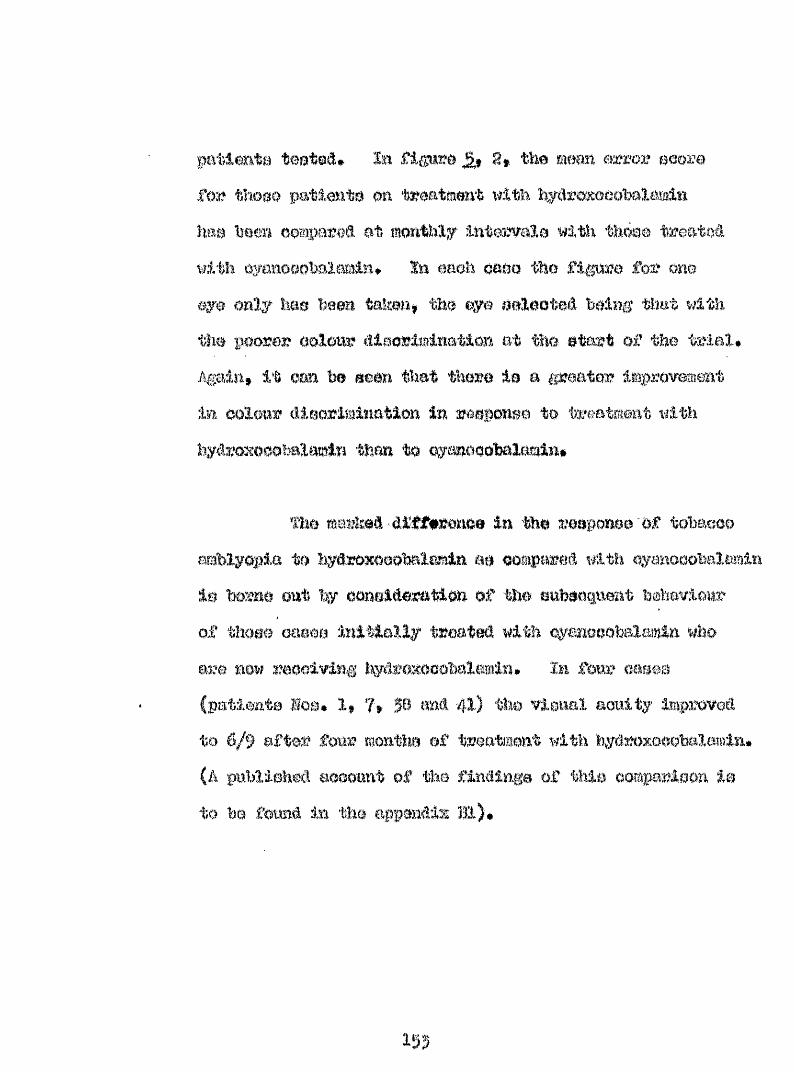
toot®A# la flgum the memi error ecorefor thoee patim^ta on treatment iflth l%yt%raKooobalmln hem been oompamâ at monthly Intervale with thème troatoâ with oyanooohalomln* In oaoh oaoo the figure for one eye only W e been taimn# the eye oelooteâ being that with the poorer oolow diaorimination at the etwt of the trial* Again# it earn be m m that there ie a greater improvement in oolow dieoriminatlon in reeponeo to treatment with ïiydroxooobalamin than to oymooobalamin#
mam' in the reeponee Of tobaoooamblyopia to hydroxoeobalamin e# ooisiparoi wi*» is borne out by oonei&eration of the ehbecqnent bmhaviow of t W m oaeoe initially treated with oyanoeobalamin who are mow moelving hydroxooobalmin* In f e w oaeee (patiente Moo# 1# 7# 50 m i 41) tlw vional aonity improved
W ft* of treatment wit(A published aoeonnt of the findlnge of thie
Bi)#Dameon 3
Mean 100-hue Error Score
1200-1
8 0 0 -
4 0 0 -
53 42Start
Duration of Treatment (months)
2# Heea Iti oolom? (tleorimlnatlonIm with tobaoGO amblyopia tyaatedk t lthliydmxoooWlamln aa oomparoâ with oymooobalmln(0«"#0). Improvement 1% oolour vieion (a reâaotlon in 100line error score) oooiira mtmig patlmto treatei withl)ydro3cooobalamln W t not maong those treated with oymo# (oobalamln, Vbrtloal bare indicate the range of eoores,*
Following on oomparloon of rato of Improvement following thempy with oyanooobalmiln and%'êr03iowbmlamlm$ anû # # fovowmble outcome for hyêromaobalmm#) # a ll patiente have boon plaoed
OB. therapy with h^^oxooobalamln#
rate o: , ylffital xv ODVai y, a M oolour
Fig* 5# g lo a gmphlo representation of the Imprevemmt In vlmal aonlty anti Farnsworth 100 Hue error aeoro on treatment with hy roxoeohalamlni* fli© patimt is a pipe*emoId.ng male ageâ 6g yoaro who haa been amoking 4"*5 of pipe tobaeoo weekly miâ haâ a daily intake of alcohol* Hie vlenal aym%)tome tfore for five mwithe only* Gorreoted vlonel aonity In the right eye was 6/18 and in the loft eye 6/1: # Oontm#*oaeoBl defeote to oolonr woro found both vimal fielde end tho Pomeworth Mmieell 100 Hue toot error wore in the right eye wae 5)9 and In the left 4)4$ eemm vitamin Bia woe 110 pg/ml# He %me placed on treatment with IiydroxoaoMlamln and oontlimed to emoke* After few monthe treatment the vieiml aonity had Moon
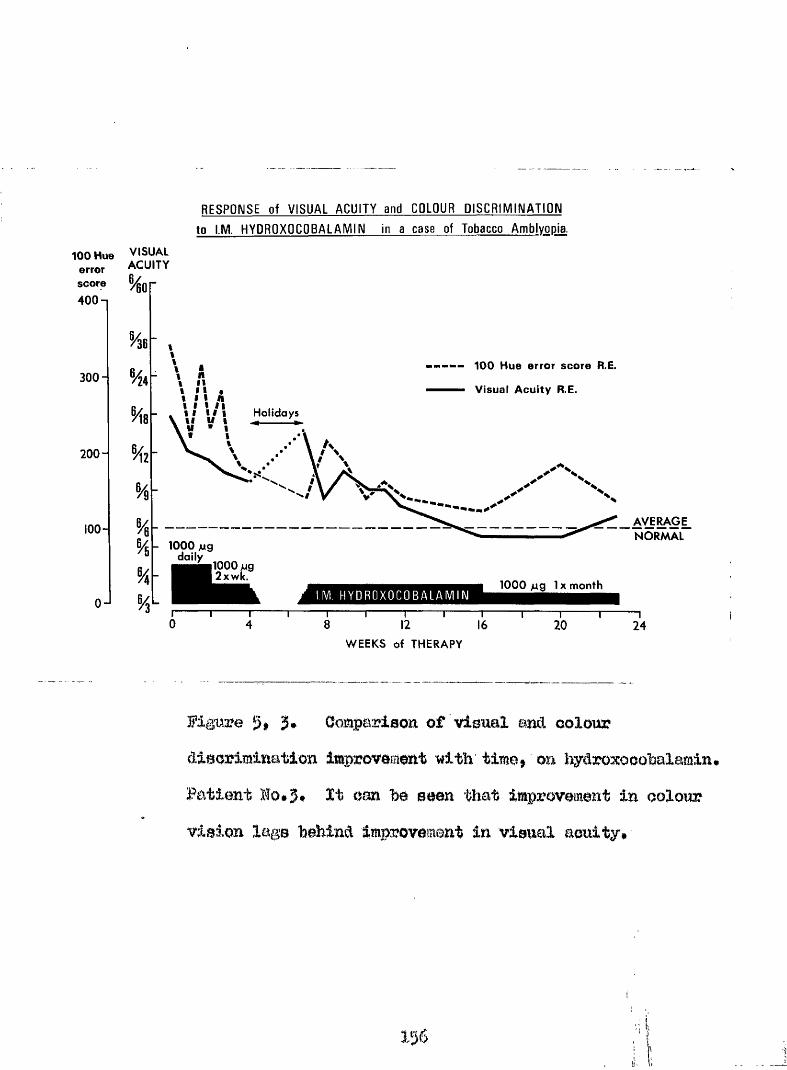
RESPONSE of V ISU A L A C U IT Y and COLOUR D I S C R IM IN A T IO N to I.M. H Y DRO XOC O BALAIV IIN in a case of Tobacco Amblyopia.
100 Hue VISUAL error ACUITY score
400-1
300-
200-
100-
0-J
100 Hue error score R E.
Visual A cuity R E.
% Holidays
%AVERAGENORMAL
- 1000 jug doily
1000 jug 2xwk.
1000 ug 1X monthH Y D R O X O C O B A L A M I N
WEEKS of THERAPY
Figure Oomparison of visual and colourdiscrimination improvement with time» on hydroxocobalamin» Patient Ho*3* It can he seen that improvement in colour vision lags behind improvement in visual acuity# ■
156
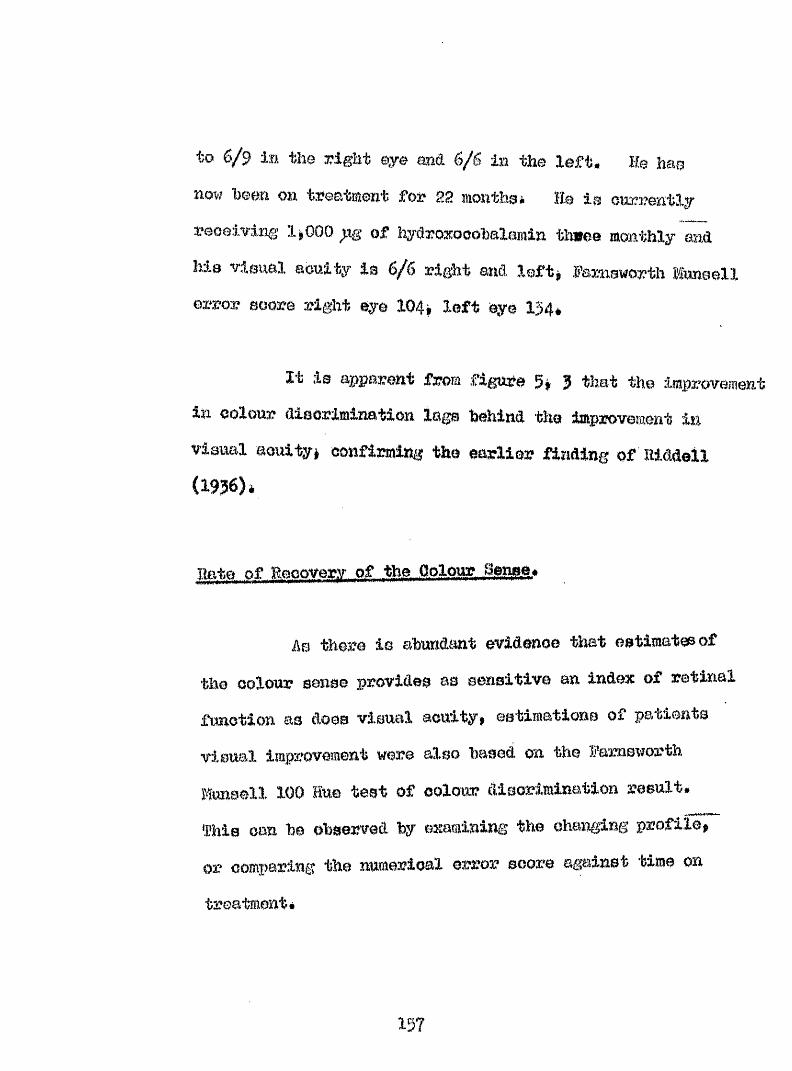
to 6/9 in the right eye and 6/6 ia the left. He has now heen on treatment for 22 monthsi ÏI® ia oncrently reoeiving 1*000 p.g of hydroxoaohalamin th»ee monthly and hia visual acuity is 6/6 right and left* Paimsworth Mtmaell error soore right eye 104* left eye 134*
It ie apparent from figure 5* 3 that the improvement in colour disorimination Inga behind the improvement in visual acuity* confirming the earlier finding of Riddell (1956)*
Rate of Reooverv of the Oolour 8en$e,
As there is abundant evidence that eetimateeof the oolour sense provides as sensitive an index of retinal function as does visual acuity* estimations of patients visual improvement were also based on the Ramsworth Huneell 100 Hue test of oolour disorimination result.This can be observed by examining the changing profile, or comparing the numerical error score against time on
treatment*
157
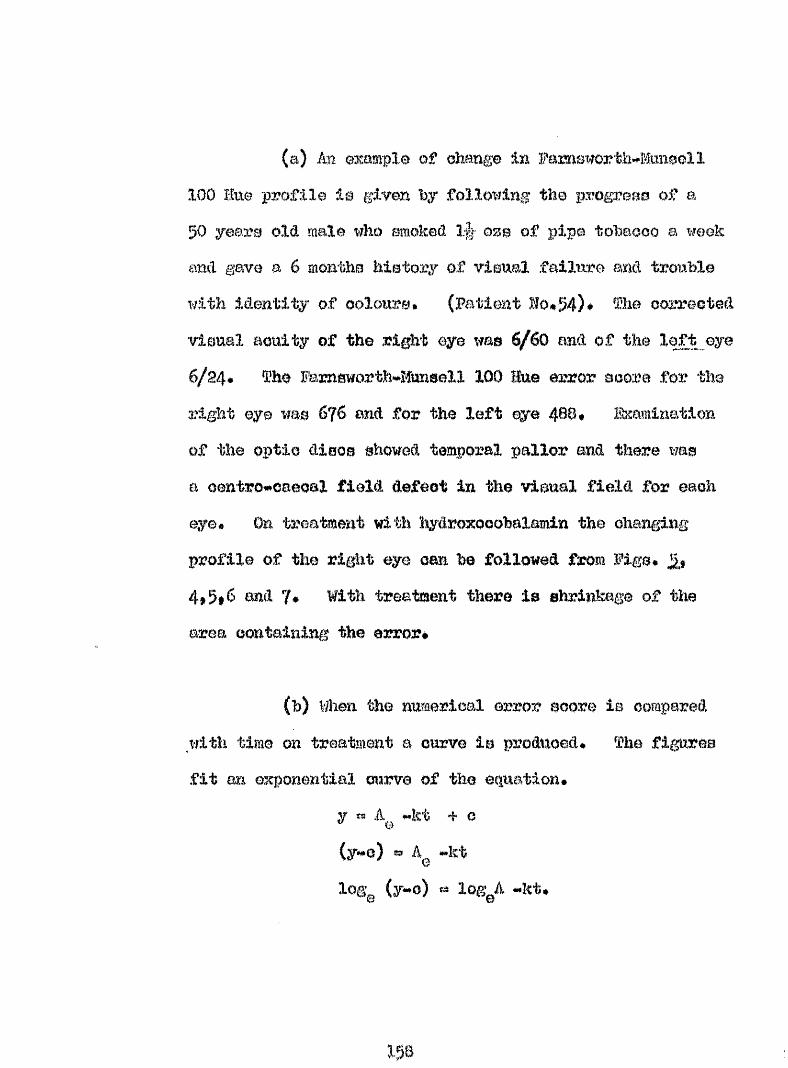
(a) îm example of change in Fameworth^îtoeell 100 Hu© profile ie given by following the progreae of a 50 year© old male who amoked ozb of pipe tobacco a week and gave a 6 moniîha hie tory of vlaual fallwe and trouble with identity of oolour©# (Patient Bo#54)* ^ha corraoted vieual acuity of the right eye was 6/6O and of the lefjfc ©ye 6/24# Who Famsworth'*îtosell 100 Hue error score for the right eye was 676 and for the left ©ye 4B0# Bxamination of the optic discs showed temporal pallor and there was a o@ntro*»oaecal field defect in the visual field for each eye# On treatmexit with 'hydroxocobalamin the changing profile of the right eye can he followed from Figs.4,5i6 and 7* With treatment there is shrinkage of the area containing the error*
(h) When the nwflerical error score ie compared with time on treatment a curve is produced* The figures fit an O3cponeritiai curve of the equation*
y « A wkt + c(y*#o) es à *.kt
G
log: (y-c) « log A ~kt*Ç3 w
1 5 8
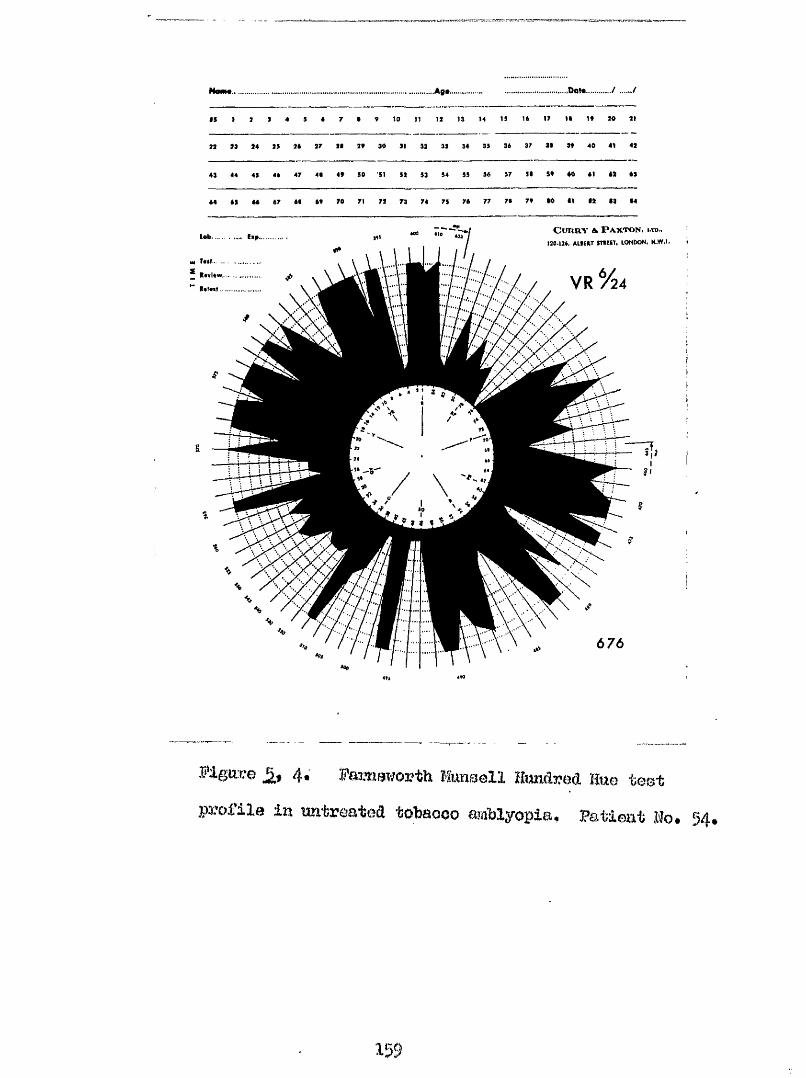
.............................................. Ag*.... .....Dot*........./ ....../
IS I 1 1 4 5 « 7 t V to 11 11 1) M 19 16 W II It M 11
11 M 14 19 16 17 II It 30 11 11 11 14 19 36 37 31 It 40 41 41
41 44 49 44 47 41 4t SO SI 51 91 94 95 96 97 91 St 60 61 61 61
64 69 66 67 61 6t 70 71 71 73 74 75 76 77 71 7* 10 II II II 14
7iJ— Cui m- v H P a x to n , i.td..lob........ lap......... «J / ;I 130-134, AllEIT sntrr, iontx>N. h.w.i. t\ \ \ I I I / //H| ... . . ...t.t . .
: IZ :::z / / v r /44
\
Figiiue 4« PanwTiorth Kmsell Hundred Hue test profile in untreated tobacco amblyopia. Patient Ho. 54.
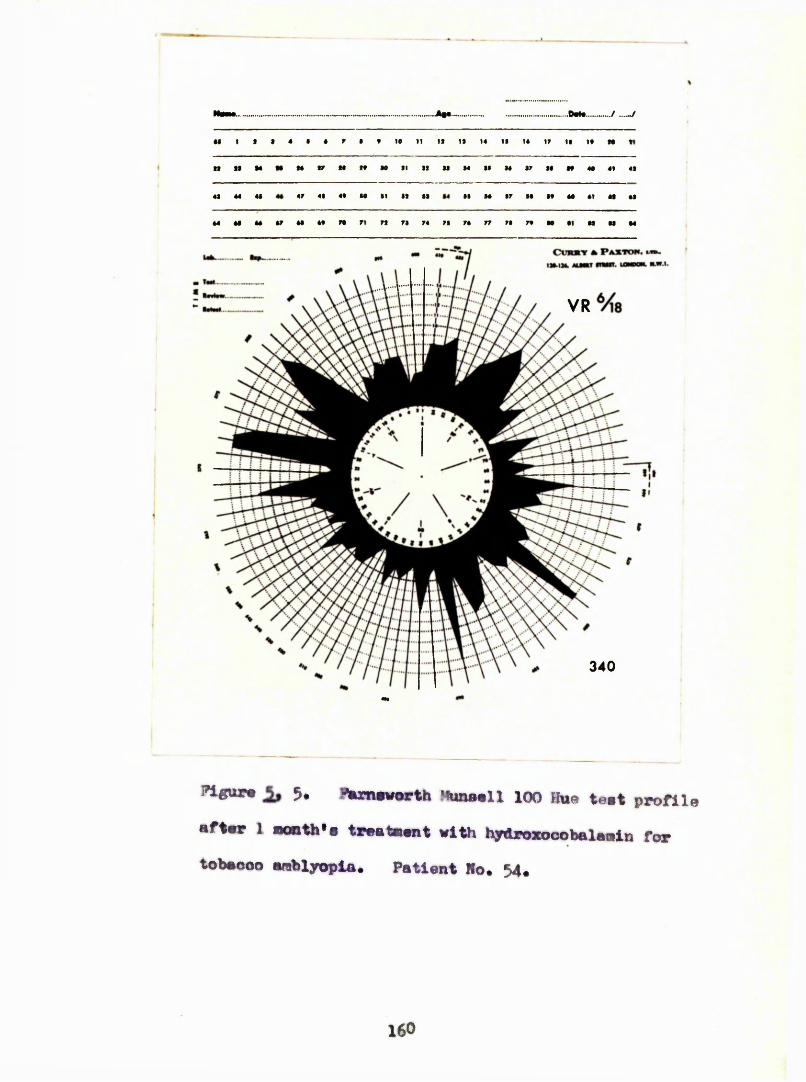
M J7 *1 W «• 41 «1
*1 44 41 «4
47 M 4* 7* 71 7141 M 41
Cvwmrr * P a x t o h .I14.IJ4. 44JHT 44*441. U — «»»■ '
Plgur* i 5. 7#xnaworth Munamll 100 Hua teat profile aftar 1 month'# treatment with hydroxocobalamin for tobaooo amblyopia. Patient Ho. 54.
1 6 0
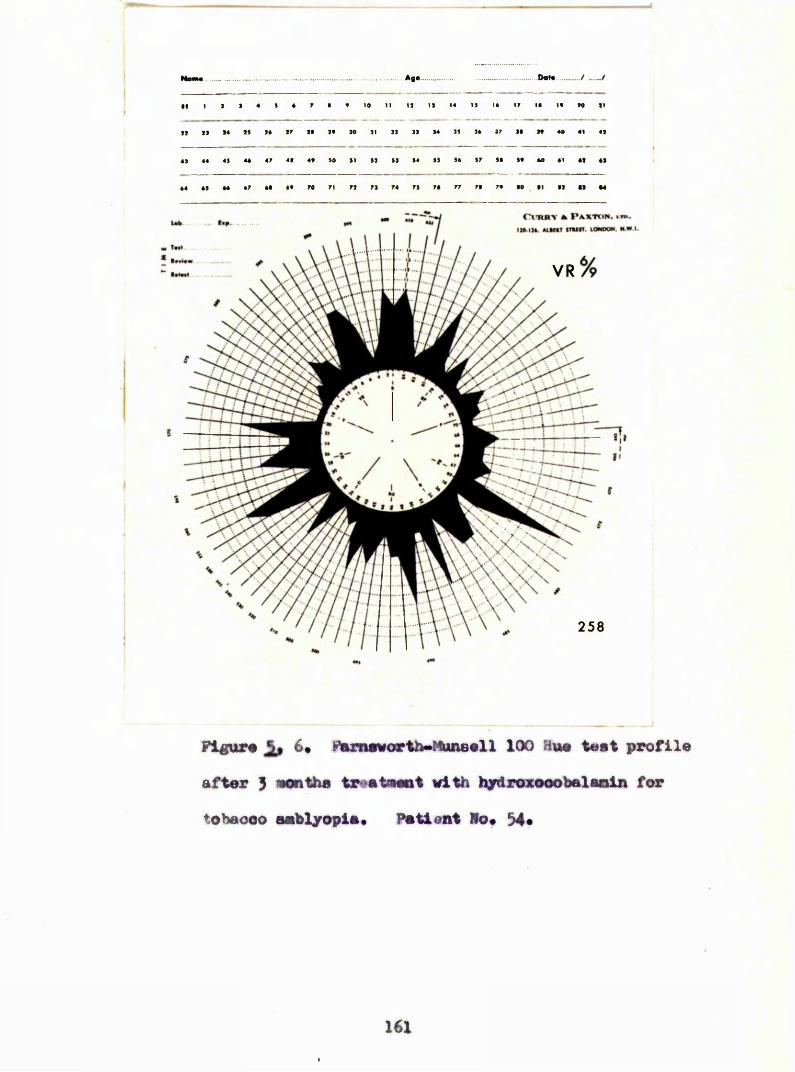
..Aga.. .Dota / .. /
Il I J I « s 4 7 • « 10 11 11 IS 14 IS 14 17 II If N II
11 11 14 IS 14 17 II If SO SI SI IS S4 IS 14 17 Si If 40 41 41
47 41 4f SO SI SI SS S4 SS S4 S7 Si if 40
44 41 44
V R %
258
Pigur# 6# Pam#vorihmMun8ell 100 Hu« t«at profile after 3 eon the treatMnt with t^roxooobalaoin for tohaoeo amblyopia. Patient Ho. 34#
161
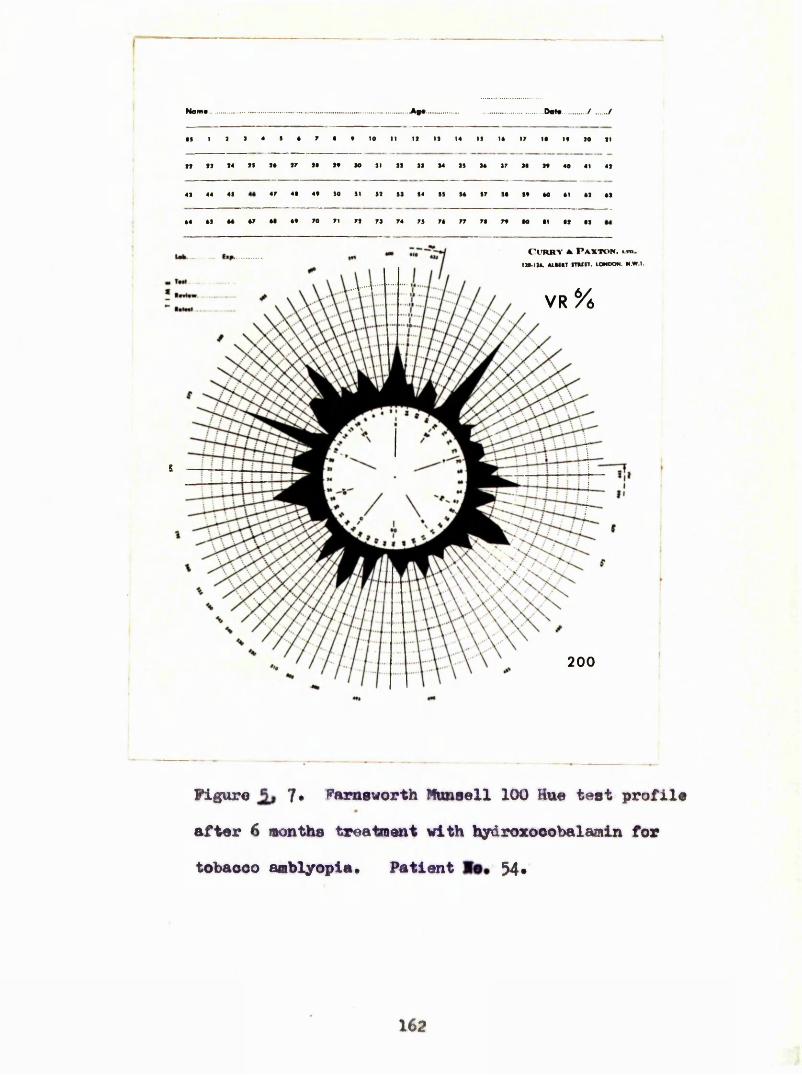
-A|«. Do M / ......./
If I 1 I 4 S é 7 • t 10 n II II M IS 14 17 II If 10 II
M II II II 14 IS 14 17 14 If
44 41 4440 41 41 41
77 74 7f M tl 41 41
s
S
200
Figure 7 * Farnsworth Nonaell 100 Hue test profile after 6 months treatment with hydroxooobalaoiin for tobacco amblyopia* Patient Be# 54#
1 6 2
y ** Î W 100 Bue eooreo # Oometmt #ilob la ea individual
d h a m o t e ^ e t l o o f o a o h p a t l m t * I t . i o t h o 0 3 ? r o : ?
o o o r a a t w M o h t h e e x p m o a t l a l o u r v a w o t % l d b e o o m o
h e a ? i m o a t a l * ' I h i o v a l u e le d e p o M e a t o a p a t i e n t
o e u l a r d l e e m e e m â e o m e e y o t m l o d l e e a e e e
which # œ toown to mmB m upect tu the oolom? emee» : | [ ( # % m e a r 1066) » Pemlolow m a m l a ( A d m e e t e l 1 9 6 ? ) {
k # B l q p e o f ( y « " o ) O j ^ l a e t t i m e # m % d l e m l M e %
of the mte of Improvommt Im colow dleozdmiaatlm, t # fImst
#elmg the fomule the ouwe um tmnmm linear -*1lo0 of the MW9 computer at Olaogow IMlverelty wao made to fini the moat suitable v#Im# for CJ which #vo the ^*bmt fit** to the reeulte over the flrat 18 mouthe of tmatment#
An llluetmtlve oxaaple la that of a 68 yeore old male (patient Wo#ÿ?) oolour niatoher of a cotton xxdll# who smoked 2^000* of pipe tobacco weekly and a vlwaldletm?hanoe mtoMlng over two mmthe# left eye waeImom to have poorer violon #@â the % o oorreoted
163
of left|%&nH&ï3L(W&)# l8%N&1k%K>*f38W&CN&3L a%(N)tH3K&GW& lWe%%& %f%NS2w3%
(&f 488H0&& (%yx&* g!]ba !&BKR%w&%f03;t%& &%%&%& &0# IÎW8 tioat» a&8Mf(% i&Bk <3G2KM3W iDdT ,$08 tfl't&i t&%0 ar3.0$*1) (sgfe %w&&
{ïoveâ03? with the left» After 10 mmÆm of treatment with h^armsoùolmiamiü the viemal aoititf of moh
to Û/9 pt# (Bmellen) a M the Fameworth Hmi error hoâ falim to 180 with the ri^t oaro ana 860 with the
h Z&mw*.
error e m m with time la ohown In fig*. 5, 8,
With a o valno of iO and plott:
n » %. p<0.00l)., ®te $)lonIlm le mi* a
la ehow on 9*.
% msaiie of *IMo teoMiqne, It le poaeihl# to
oomparo the ratw of Improvement In oolow Oloorlmlnatlonwith Weatmmt In m m y patienta» % e following gronpe of oatiaiite were aval labia for oomparieon##
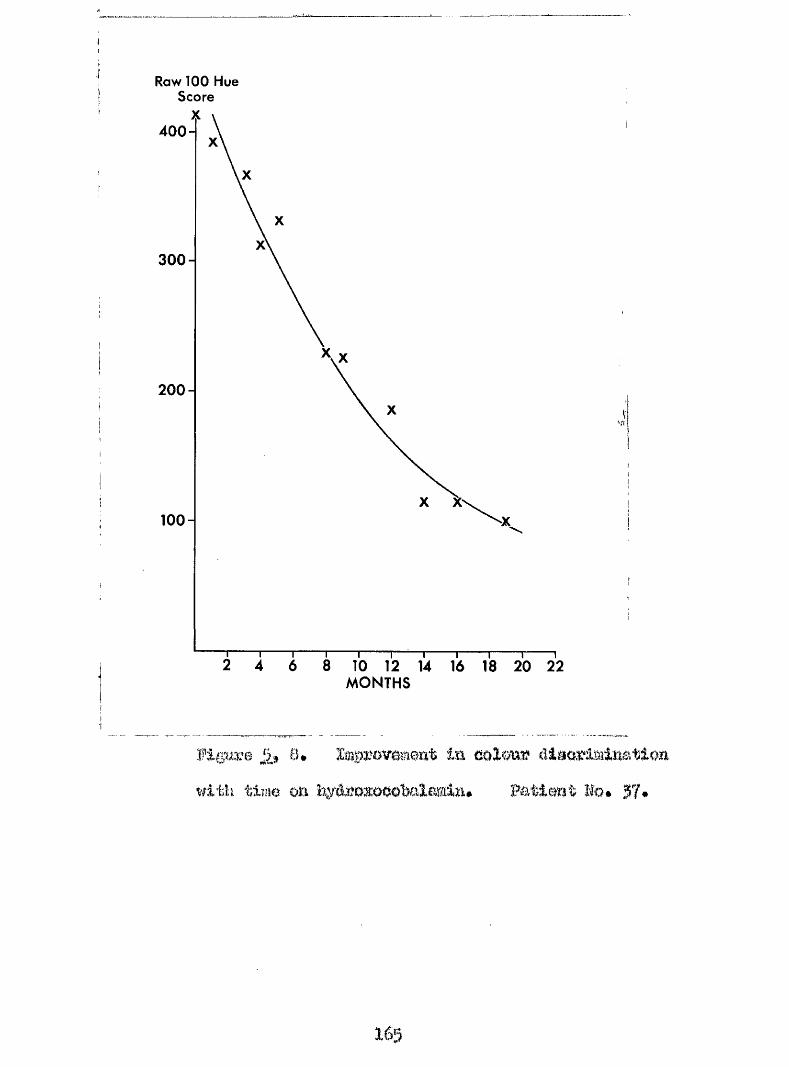
Raw 100 Hue Score
400 ”
3 0 0 -
200-
100-
MONTHS
with tiîiie Oïl h^é^B%owhaIamim# Pa tie# Mo<
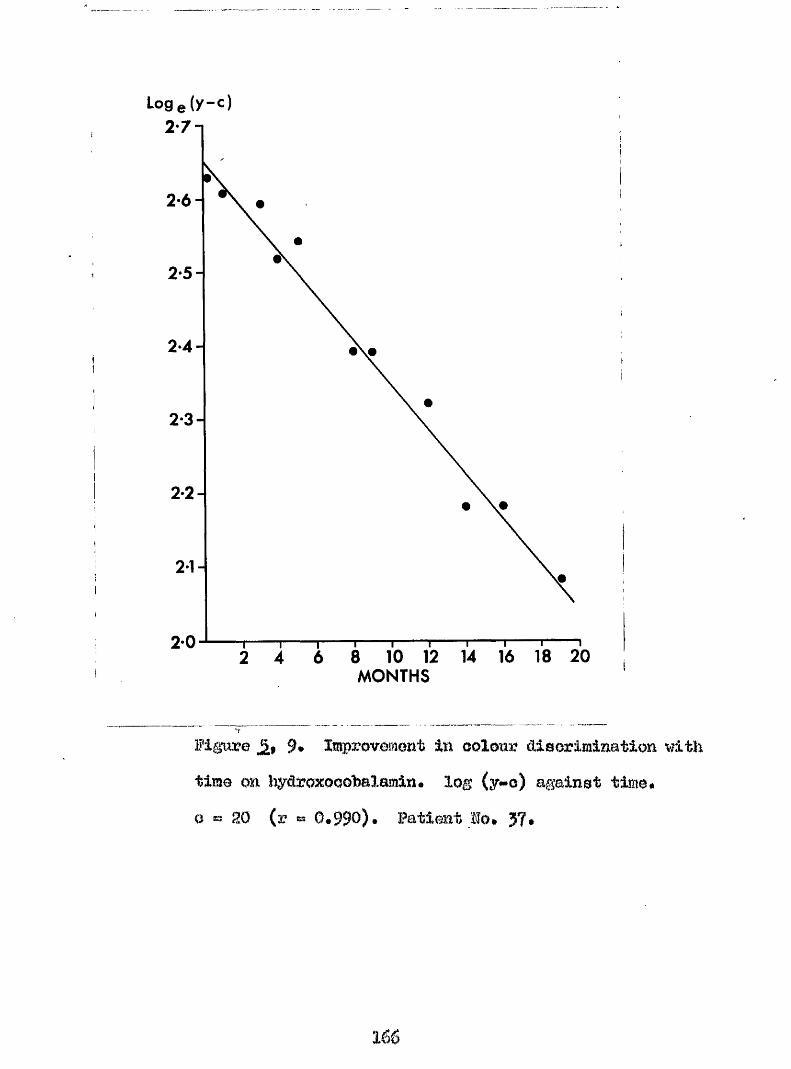
Loge(y-c)2 7-1
2 6 -
2-5-
2*4 -
2-3-
2 2 -
2-0MONTHS
Wigiivù 9* Improvement in colour ctisorimination with time on hyaroxooolsalamin. log (y»o) against time, o ■=> 20 (r = G.990). Patient Mo. JT.
166
(a ) Tobaooo amblyopia oompIloateA by fon iio icae
(o) foteooo amblyopia ooapliüsteâ by âiabotos#(<l) fobacoo amblyopia treated witli hydmxooobalamln#(e) % W o o o omblyopla treated by aWti$ionoe from tob&Qoo^
mean valum for k (rate of lmprovemmt)wer0for all #ea$ groi%p$ m d are contained of k do the tangent of the elope
Tobaooo omblyopla In proeenoe of pro pomloloim anaemia fobaooo amblyopia in preaenoe of dlabetea
r w value
0,195 2*1'
0.?
o.s
S0®42‘
IB*
Theae three 0 ^ p B all reeelvod the eame therapy )ln 1000 dally for 14 doya followed
by 1000 jag thrlee weekly, % m the rate of Improvement In eolow emae %me pooreet In the group oomplleated by pernloloue anaemia# %ere la Inenfflelent data to observe whether thle could be Improved on; by giving a larger doae
Oyt rt f
of hydroxooobslamin, g. An l©ïïïioomplioatecl tobacco amblyopia treated with hydroxooohalamin 0*284 15ÏÏncomplioated tohacoo amblyopia treated by abstinence from tob£?.oqo 0*302 15 43*
%here is little difference in theeo two groups| the rate of improvement in the colour sense being equally good by either method of therapy*
1 6 8
OMFi'SÏI VI.
l*0bor*s hereditary optio atrophy la a relatlvoly rare condition obaroetorisod hy ooute or euhaoute failure of oentml vieion preomting a» a rotroWlWr nowltie or optlo atrophy, typically in yomng males in their late teono, or early twantiea* It ie moommon for mly cmo eye to he affeoted and equally imoomon for the condition to resolve completely, thou# <imamplee of complete or marly omplete recovery have hem dooorihed, Many patiente with Wher*8 hereditary optlo atrophy ore registered ae hllnd pereom ae the central aootoma is large and demae in eaoh eye and aoQonnt for 0*g^ of blind regietrationa (î&reholl and Beilw 194: )$
labor (1071) ommidered that the ago of meet %me moot common between 13 and Ê6 years# àmeman (1936) found that the dieeaoe hegm hetwem 20 mi 30 yearn in 47#0 of hie eeriee# Boveml antliom have stated that the age of onaet in mmoeedlng generations beemeo progreealvely
169
younger ao called mtlolpatlon 1909$MaaMenfeurg I9B3)#
Aoeman (1950) fomd that the dlemee invariably begm %flth m acute reduotlm of violon, i hloh was followed by a period of alow progreoolon which oould last for several menthe# % e dloeaee nearly alwaye attacked both eyoa$ eoDaotlmee elmultmeomly# eometlmae with an lnte%*val which varied from weeke to mmtho before the second eye was ai ffeoted# The acute diminution of vision may lead to oomplete bllndneee or aufflelent Impalmmt to warrant blind oertifloatlon# In a minority# the oonditlen Impmvee apontanoouely after a variable Interval, with clearing of the centre of the eootoma leaving a ring sootoma.Generally# ho%mver$ the patlmt la loft with a deizee permanent aootoma affootlng tho fimtlm point in oaoh eye# In a study of #o dyaohmmatopaia which aooompanloe this mnditlon# Pranooio at el (I96I) oonolWed that the oolom? defeot was ohamotèristioally to be found in the red 'g oen arm# of the opeotrm %Aloh served to differentiate hober*0 hereditary optio atrophy from the dominantly
1?0
inherited optlo atrophy in which wore affected#
*hlim 3?qgifMs
OphthalmooQOpy in the amte phsae may mve&l a normal optio disc or a disc ehot ing the oedema gmd hyperamla of papillitis# Amduo plotwo es deeorihedby leher (1871) %me of a pE%plllitis# %her (1927h)oommmtad on the preemoe of haemorrhagoa at the diao in the amte phase# àtrophy of the optic dieo met in after an interval of 2 montW or no, hut the dogroo of atro#iy gave no indication of the final vional aouii! (Battm 1909# tieher 1927h, IWiAsgaoi# 1944)» Bmigioal exploration of the ohiaemal area revoalad araohnoidltio and a oeroue moningitia in a nnmhor of
Autopay reports have been publlehed on imquwtioned oamea# In Rehetoinor*e (1930) the eyes and the optio nervoe were e$samined; IWittken m d Bareat (I93h) claim to have carried out t W first oomplete exaisination# Further oo^o^lete pathologiesl e^Eomi^mtiono Imvo h e m reported by %;ilaon (1963)# and Adame ot al (1966] In all reports there were atrophic oMngee in the retina
miâ the optlo nerves were exteaoivoly dcFKyelinatsd, the papillo#maoular bundles being completely atrophied*IWlttkon and Barest (1930) noted that there appeared to W a primary trmtomwoml degmiomtlm la # o whole optle traot exoept for the oalornrlm cortex# These authora f\%r#er deaorlbed aplml oord eymptoms and for w%üohoorreopmdlag newo»patholo#loal changes couM he demoaetrated, %eee oha%aa In tha spinal cord thoee authore attributed to malnutrltlcm# Rehotoluor (1930) oonolWod that the pathological evldawo w m iâoutloal with that found following the toxlo etrophy of the optlo norvo in diahotoa or tohaooo gai#lyopla, and did not roaemblo the atrophy resulting from retrobulbar wurltlo* The majority of # o oaaee dooorlbod hy.Wllam (I963) showed manlfeatatlone of a diffuse nourologlool disorder, Long tract el^o were preomt In moot m d luoluded lower or upper llm%) paraootheelao, defective vibration seme, œteneor planter reepowaa, epaetlolty and hyperreflexla#An eighth nerve dyeibnotlon of varying degree was demonetrable In half the eaees, There %me no oonvinolng huematologloal abnormality; but all the oaeea for whom relevant Information was available wore amokere#
17g
Additional infozimation of a like nature was presented by Adams et al (1966)*
Leber (1871) himself wrote that even unaffected members of a family may suffer from px otean neurological disordera such as migraine# giddiness# wealmess, or were easily fatigued* This has been amplified by the frUiding of associated neurological conditions# such as epilepsy# mental retardation# spastic quadrlpesis# ataxia of cerebellar origin, posterior colmm loss# various aches and pains, and paranoid schizophrenia. (Taylor 1892, Ne#tleship 1909t Taylor and Holmes 1913# Ferguson and Oritohlay 1926, Golenbrander 1962, Walsh 1957, Kwittken and Barest 1998). In moat of the reported cases the neurological disorders have developed in the presence of advanced optic atropliy or severe retrobulbar neuritis and usually some time after the initial visual disturbance# however, this was not so in oases described by Bruyn and Went (1964) and Adams et al (1966)*
Manifestations of the malady are not confined to the central nervous system diverse skeletal
173
abnormalities, a tendency to fracture, arachnodactyly and atypical ankylosing spondylitis have been described (wilaon 1965b)♦
I'he pattewx of inheritanoe is p wssling. Shereported pedigrees variously show features suggestive of a S0X#linked Inheritance, autosomal inheritance, or oytoplasmio trmsmission* Oolenbrander (I962) postulated the presence of a ^%ebervirus^* in the cytoplasm whioh produced a cellular mutation* Van Benue {1963) felt that an autosomal modifier gene was required for the full expression of a sex linked inheritance# Wilson (1963, 1965a) and Adams et al (1966) feel that the basic condition is an inborn metabolic error, for whose oxpression exogenous factors are pre*#eminent, and that there are relatives of affected persons at risk who are predisposed . to the malady but have not encountered the exogenous factor, These authors further postulate cyanide to be the toxic factor#
Wilson (1965a) examined patients suffering from Lobar* s hereditary optic atropîiy for products of cyanide
metabolism, and found aignifiosntly reduced oonoentratlons of thiooyanate in the plasma and in the urine, the dlfforenoea being more marked in those patiente who smoked* In this respect the disease resmahles tobacco amblyopia* Because of the reported success in treating tobacco amblyopia with hydroxocobalamin (Ohisholm, Foulds and Bronte^Btewart, I967), the following patient suffering from Leber*a hereditary optic atrophy was given similar treatment*
This man, aged was aeon with a year* s history of numbness and paraasthesiae affecting the right side of the body and coincident blurring of vision of the right eye* Similar bltuxring of vision of the left eye had been present for one month* He sriioked # cigarettes daily and drank several pints of stout per day* On examination the visual acuity of the right eye was 2/60 ( Snellen) and that of the left eye 6/12 (Snellen) with a dense central scotoma in the right field of vision and a smaller oentro«*oaeoal scotoma, more striking to a red target, in the left* The right optic disc was pale and the left oedema tous* The rightplantar response was extensor but there were no other
#5
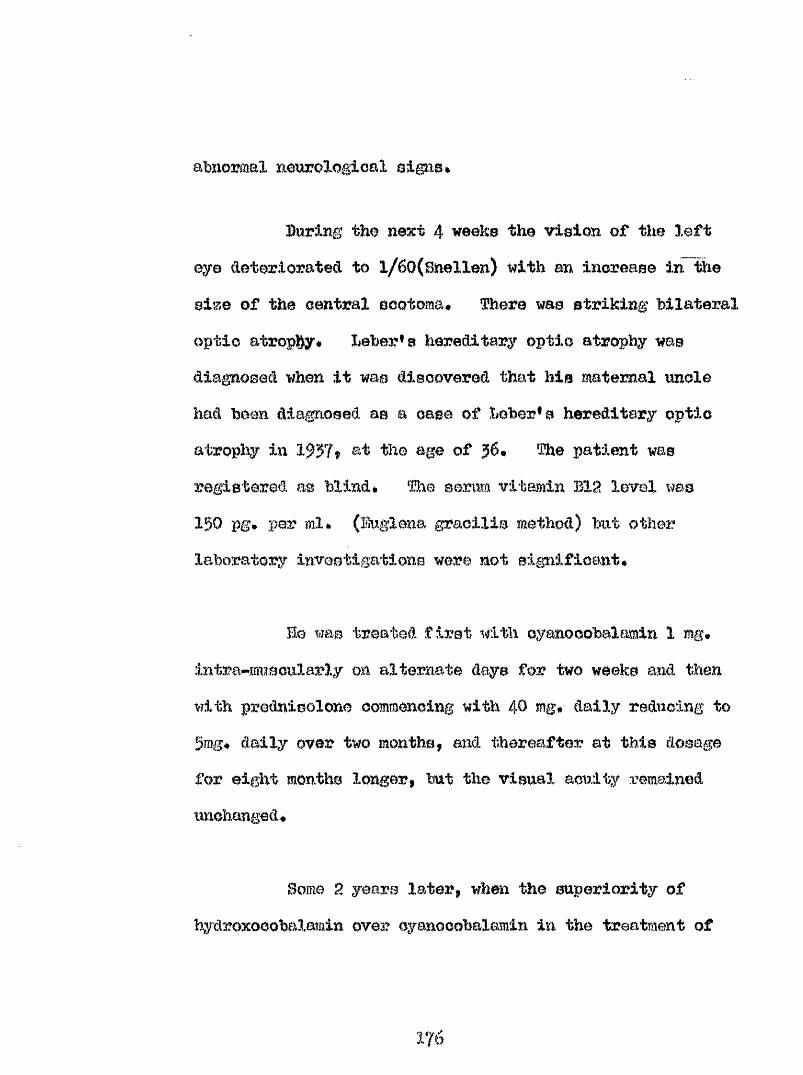
abnormal meurolo#oal signs*
During the next 4 weeks the vision of the left eye deteriorated to l/60(BneXlen) with an increase in # e size of the central scotoma# There was striking bilateral optic atrophy# Leber* s hereditary optic atrophy was diagnosed when it was discovered that his maternal uncle had been diagnosed as a case of Leber* s hereditary optic atrophy in 1957» &t the age of 36# The patient was registered m blind* % e sorm vitamin BX2 level was 150 pg* per ml* (Biglona gracilis method) but other laboratory inveetigations were not signifioant#
Bo was treated first with oyanooobalamin 1 mg# intra**muBoularly on alternate days for two weeks and then with prednieoXone commencing with # mg# daily reducing to 5mg# daily over two months, and thereafter at this dosage for eight months longer, but the visual acuity remained unchanged#
Borne 2 years later, when the superiority of hydroxooobalamin ovea? cyanocobalamin in the treatment of
176
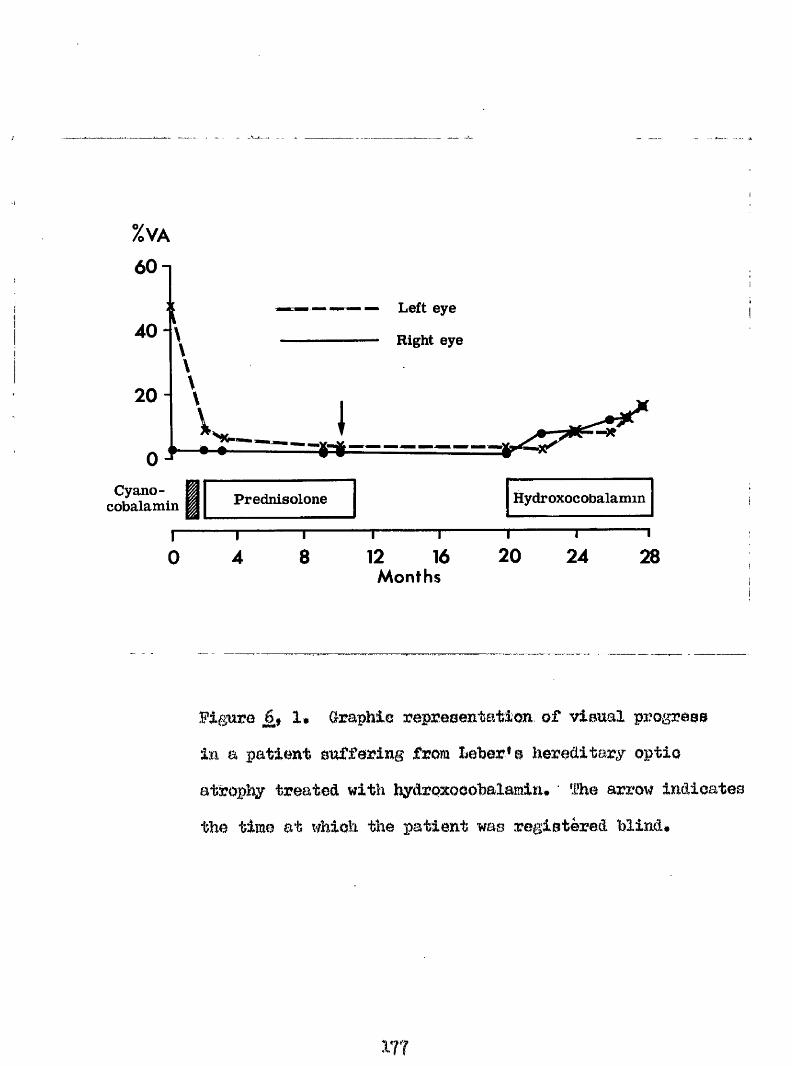
%VA
60-1
Left eye
4 0 - Right eye
20 -
0 ^Cya.no-
cobalamin Prednisolone
"T4
"T8
"I------ r-12 16
Months
Hydroxocobalamin
“T“20
I24
—I 28
Hguro I. Graphie repreaentatloR of vlmal px^ogross im a patient oufforing from Leher* o hereditary optio atrophy treated with hydroxooohalamin* The arrow indioatee the time at which the patient was registered blind*
tobaoGO amblyopia mbb realised^ the patient wae treated with patenterai hydroxooobalamin 1 mg. daily for 2 weeks and thereafter twice weekly# 33efore starting this treatment the acuity of the right eye was 2/60 and of the left l/60 (Snellen)*
After 3 months the visual acuity had improved to 5/60 in each eye and after 6 months it was 6/60 in the right eye and 6/36 in the left* The patient could now read large print and was no longer ooneidered regiatrablo as blind*The progress of the visual defect is shown graphically in Figure 6# 1* (A published account of this case is fcoated in Appendix 1% 2).
Members of the following Spanish family have been examined m d treated with hydroxocobalamin* Three of the patients have been followed for five months* All the members examined belong to the tliird generation (See Fig.6,2)*
III. I* A male aged 34 yoars was examined in October*I96B* There was a history of sudden bilateral loss of vision whilst on a business trip 6 years previously* The
1 7 8
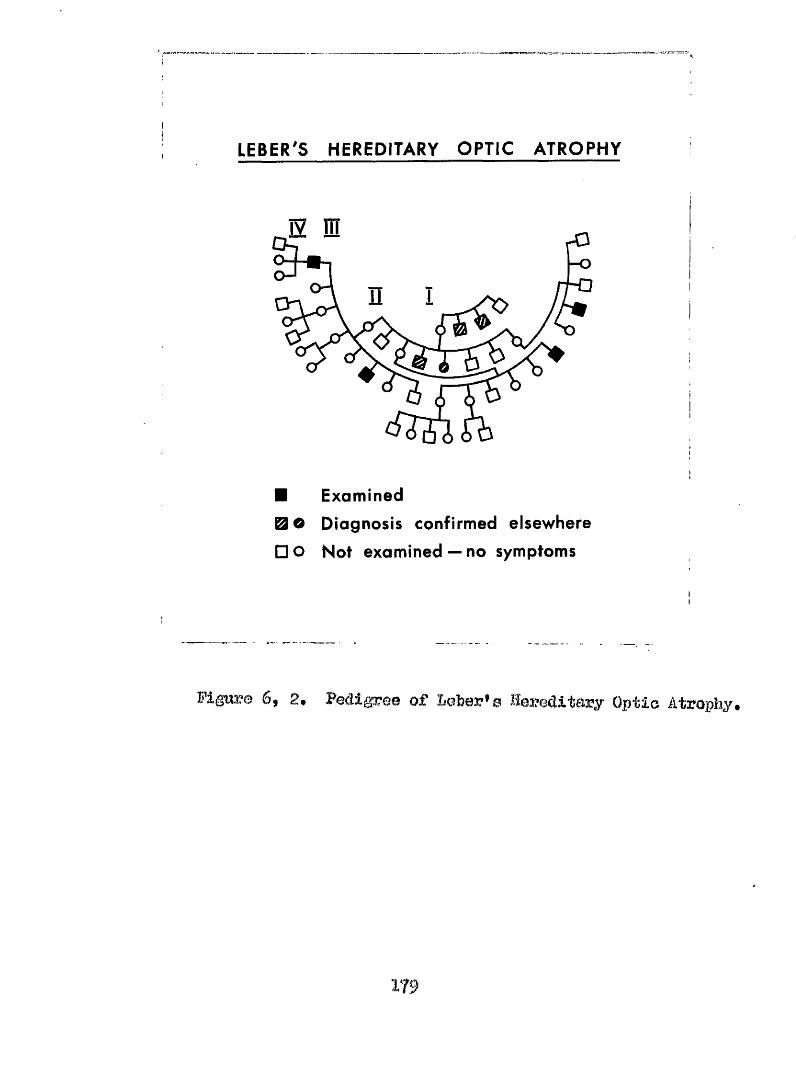
LEBER'S HEREDITARY OPTIC ATROPHY
rO-o
■ Examined0 0 Diagnosis confirmed elsewhere
□ O Not examined — no symptoms
Figure 6j 2# of I»e’ber*3 Bereditsry Optio Atrophy#
ifiewBl loem Mû horn preoaedod hy mi inîlmmiimliMi illîiaaa of ono#two daya duration* Ha amokat 20 or- more oigarattea i)m day» fha year following the vleaal loaa
ho had imdergone omnlotomy for ohiaamaX oraelmoidâtia»The Visual loao waa Bavera and had remained no»
ËKemlnatlon revealed a oorreotod vienai aontty inthe rig h t end leff eyee o f j/iO (S nellan)i with a x4 low
vleaal, aid Mb ne#r v is ion wet Ophtlmlmoaoopio ’’
e^samlnation revealed marked p a llo r o f the optio diooa, w ith
ehosthing o f the re tin a l vweele a t the iio o in each eye»
The oeular media were oloar end the rnaoulaa normal# Ikamlnatim of the aentral field of violon revealed a central aoetomata# extending to 10 around fixation in the right eye and 3^ in the left eye# (Figmre 6$g)# The eootoimta wore confirmed hy eta tie perimetry# The Fmmeworth#ffmeell 100 Mne teet reenlt gave an error of 560 for right eye# 580 for left eye»
General examination mvealed m Byctemio or neurologloal abnormality# ïj!lootro#'miqephalograpbie "ommination revealed a normal tracing» The haemoglobin
180
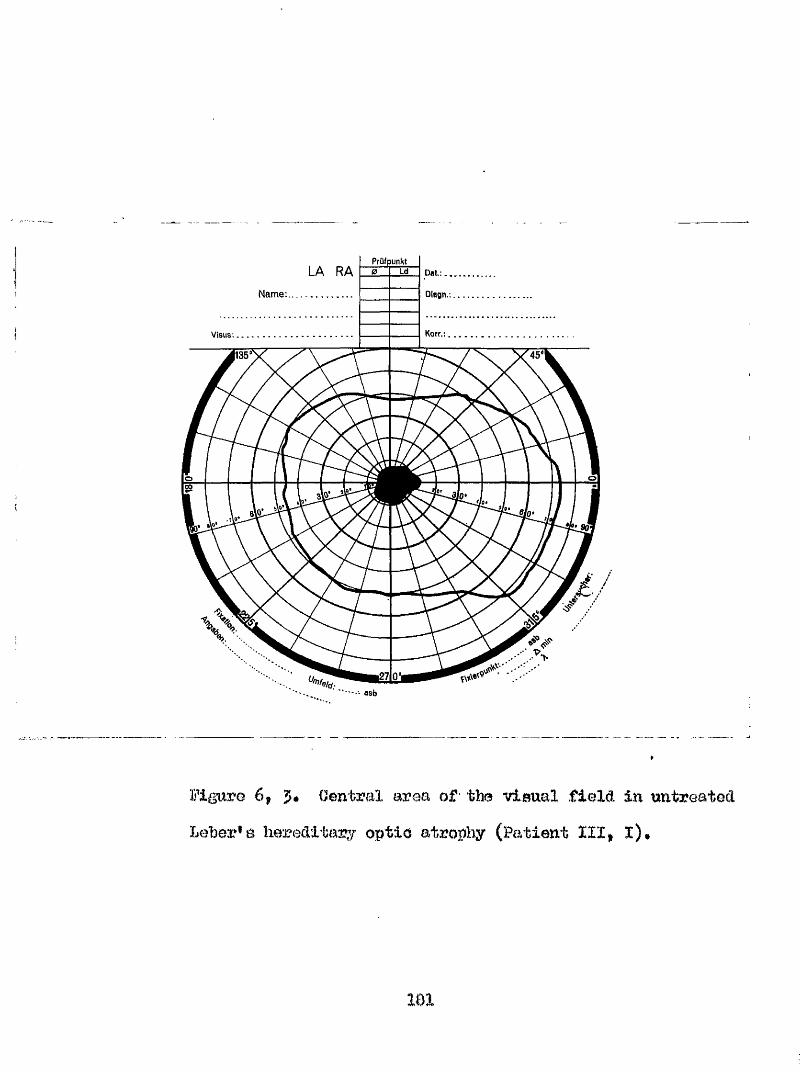
PrüfpunhtLA RA
Name
-■ asb
Figura 6# J* Oentral area of the visual field in untreated heher^B hereditary optic atropî:iy (Patient III# l)#
181
concentration was oeruia vitamin B12 306 pg/mljserum folate 4*4ng/Bilf a week 4ve result on testing for gaatrio parietal cell antibodyç and a «•ve result on testing for antibody to intrinsic factor*; the Schilling test showed recovery.
%eatment with hydroxocobalamin was comienced with 5 daily for I4 days and then reduced to 1 mgm» thrice weekly thereafter* After 5 months on this treatment there was eubjoctive improvement in visual acuity# not confimed on the Bnellen chart# hut confirmed by static perimetry which showed a reduction in the sise of the scotoma*
III# 6# A male aged 24 years was examined In October# 196s* There was a history of sudden bilateral loss of vision 4 years previously while studying for examinations* There was no precipitating illness* He smoked upt ards of 20 cigarettes per day*
Examination revealed a corrected visual acuity right eye 8/60# left eye I/60 (Snellen) with x4 low visual
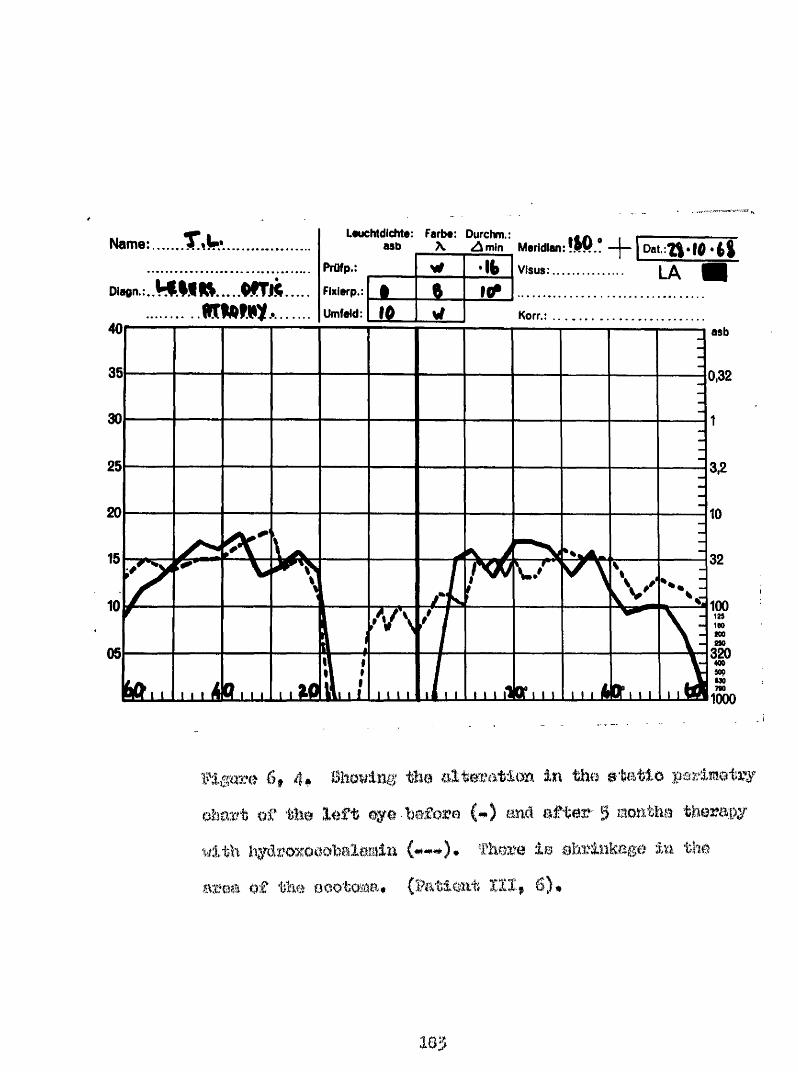
Name r.u. L«uchtdlchte; Fait#: Durchm.: , .M b \ Z im in M erid ian :fjW f.. —I— I Pat.
Diagn, :. . V W l U . . . . . W T j l t
t i m m -40
FIxierp.:
Umfeld:
111
6» 4^ Ühowln^ thei in tho etatioof the left eye before m<l e f t w 5 monthe therapy
th iiydmxOQobalemin (#^#). There le ahrlnkege In the area o f the eootoma* (Patient I I I , 6)#
aid he vms able to read 15 with either eye# Ophthalmoseopj revealed bilateral pallor and atrophy of the optic disco with sheathing of the retinal vessels at diso* The ocalar media were clear end the maculae normal# Examination of the central field of vision revealed a central scotoma extending to 3^ from fixation in the right eye and 10^ in the left eye# The scotomata were confirmed by static perimetry* The Farnsworth Munsell Hundred Hue test result gavo an error of 244 for right eye and 5S9 for left eye (Fig, 6,5),
General examination revealed no systemic neurological abnormality* lleotro*#enoephslographio examination revealed a normal tracing* The haemoglobin concentration was 1135 # serum vitamin B12 446 pg/ml* serum folate 3*7 ug/ml, a negative result on testing for antibody to gastric parietal cells and intrinsic factor* the Bohilling test result showed wf& recovery#
Treatment with hydroxocobalamin was commenced with 5 mgm# daily for 14 days and followed with 1 mgm# three v/eehly# After 5 months on this treatment there was a
164
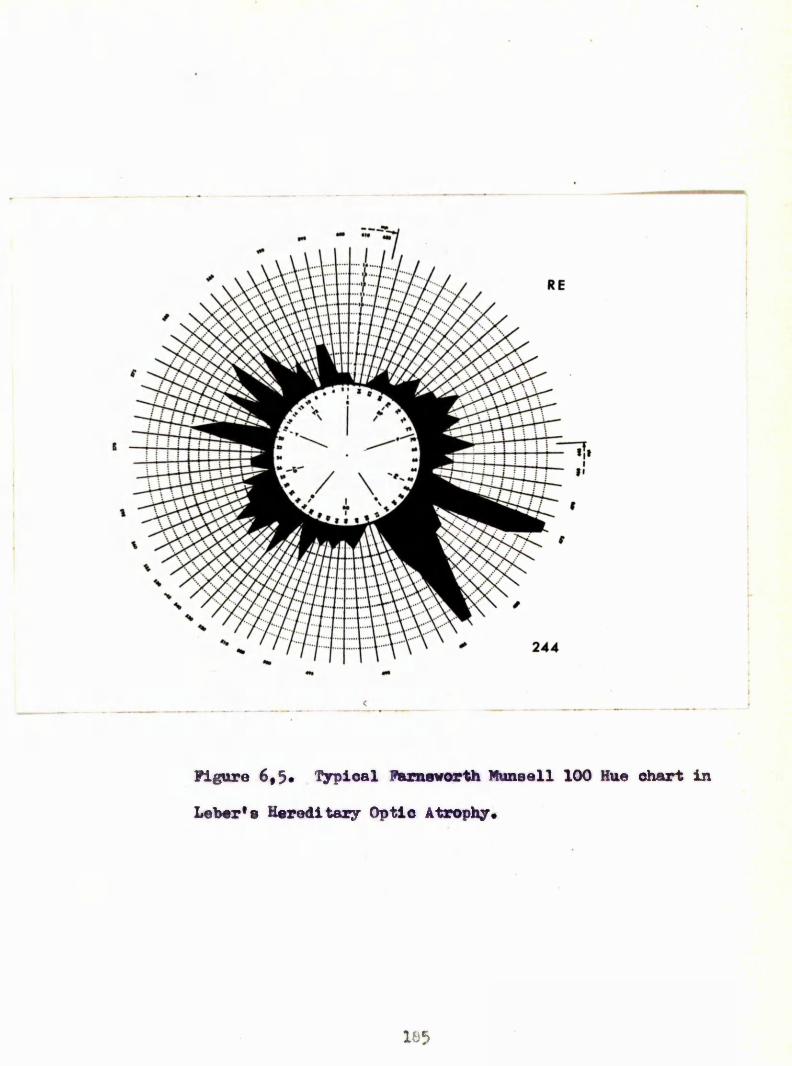
Figure 6,5. '^rpioal Farnsworth Muneall 100 Hue chart in
Leber's Hereditary Optic Atrophy.
1 8 5
, The oorreoted vlswl acuity had In the right eye to 3/60 and left oyo to 2/60 * There Ime boon Improvmmat on otatio porlme^
$4)*
HI# 14# A male ogod 16 yoara wae oxmlned jn #rch, 1969# Them wao a &%latory extending over the previous 6 monthm# The visual acuity of the rl#kt eye failed first vfithout any dieoovorable ophthmMlo oauae# the vieion in the left eye deteriorated eoee 3 weeke before exeminatim* An ophthalmologist at the patient^ e home town had eoRmenoed therapy with eyetemio etoroid (Prodnieolono) &md a mu vitamin %>r#a%*ation # which include#
10 olgerettea per day*
al acuity of the right eye was 1/60 and that of the left eye 6/I8, (Partly) ( % 0llen)# Ophthalmoeeopy revealed hyperamia of both optid diaee with vaequlor engagement of the upper halves of each dlao# Ho vaumlar ehmthing wae observed in either eye# Fluoresomeo an^^ograpby confirmed the preemoe of mall voooel dilatation of the upper halvee of eaoh optio dioo# iYom whioh no leakage of dye ooourred dwing the dye
186
The examination of the central fields showed a ohsraoterietic central aeotoma in the right eye and a oentro«#oaecal scotoma in the left eye* whioh were confirmed by static perimetry#The Farnsworth Mansell 100 Hue test gave an error score of 550 with the right eye and $16 with the left eye.
General examination revealed no systemic or neurological abnormality* Blectro**enoophalographio examination gave a normal tracing* The haemoglobin concentration was 182 6, serum vitamin concentration was nonml* serum folate 5*9 u| /ml* a negative result in testing for gastric parietal cell antibody, the Schilling test result showed 6*9^ recovery*
The patient was treated with the following intensiverégimes*
Day 1* 10 mgm* liydroxooobalamin given as an intravenous infusion in 500 ml* saline*
Day 8# 5 mgm. îiydroxoeobalamin given by intramuscular Injection*
Day 3* Repeat of the intravenous infusion with lOmgm* hydr oxocobalaïîin •
107
patientas previous therapy with eyatmlc steroid was continue# tlirmghout at the same doee# %# y 4 the visual aouity of the loft had rlem to 6/9 (partly) Saollon# an# the therapy was continued with hydroxooohalamin 5 mgm# thrloo weekly W t in opite of ü%io the visual aoidLty fell to 6/g6 (6nollm) over the m x tmeké âoso of %#mxooohalmim woe imnnmûâ to 5 :%## dally without any additional improvement in violon. Although the visual aoWLty fell after the initial improvemont, the oboerve# improvement in the visual field has been maintained.
Thla patimt has been etudled in the aoute early phase of lober*a hereditary optio atrophy# Hie preemt therapy ooneiete of hydroxooobalemin 5 e## daily# Frednieolone 5 mgm. thrice dally# He M e been advised to stop smoking#
III# l6* A male aged 14 years was mcamined in October,19# # There was a hiotcccy of abmpt lose of vlaion in both eyes whmi aged 10 yeara, He had imdorgono wrgery for 0 mastoMitia at 7 yeara of age# He wan a non#moker# Profoeeor l^auelachettl had prescribed male hormone injeotione T*:dth no benefit#
1 6 8
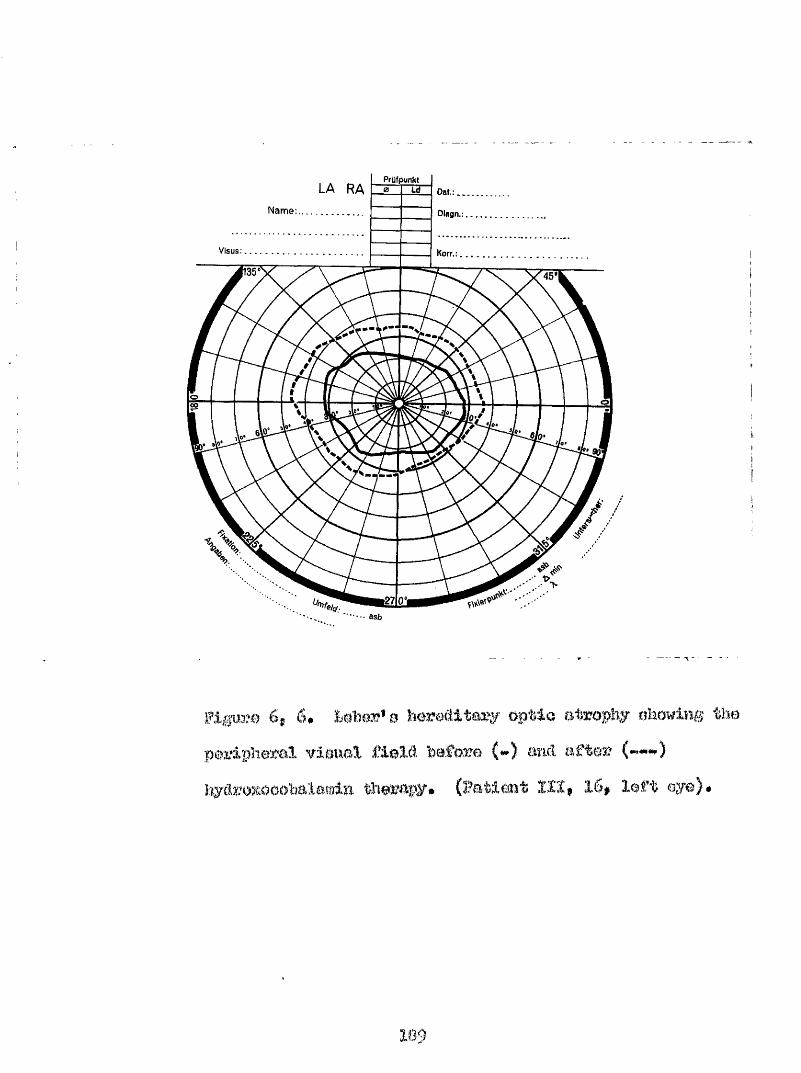
PrÜfpunMLA RA
Nam e:..............
VISUS
...
6, 6# &e%Gr*8 awMceaitoay (%p%&o ohowdü%& thepmrlphe^eal vlaiml field befozre (*►) miel aftei?
42cwc3%B#tü*dL ifieauual E&o&tilbjr im # 0 right # e smé Xaft eye of l/êO (Bnellm) aaâ wi th &%&#]&)% Tfietwal a&l<& ï%& G%at%a%0GHl !R%)# <3%&brt&Hs3kiK)CHDc%p:lo CKKaiüdLncttdLcMü :e<yy&a]Leil iaGKK&&eft g allor <)f (>prblo illeats swact eWmthlng of the retinal mimolB on the disc in each eye#
of the visual fields reveàled perlphoml ooaetMotim to both colour and white targets and a donee absolute scotoma extending to about the fixation point. Who Fmmoworth llmeoll 100 Itia teat gave an armr of 1195 for the right eye and 15# i m the left eye#
General examination revealed no eyotemio or neurological abnomalityi Bleotro encéphalographie examination revealed a normal traoin#. %he haemoglobin oonocntr&tion wao 1100, eerum vitamin #18 5Ô0 pg/ml, serum folate 5#5 ng/ml*, a negative result on testing for gaatriô parietal cell antibody #n& antibody to intrinolo f&otor; the Schilling tomt reoult Showed 7*9# rooovery.
%eeatment 'With lnydroxocoWlamin waa commenced with a dooe of 5 i%m* daily for 14 dsyo and thm oontlnued
1 9 0
with 1 nigtn* thrice weekly thereafter* At the end of 5 months there was mhjeotlve visual Improveraeat in visual aouity which was not confirmed on the Snellen chart, hut was m static perimetry and there was less oonstxiotion of the periphery of his visual field (Fig# 6,6).
Bkaminatlon of these patients for defects in vitamin Bis/oyanide relationships was carried out. fha relative data are contained in fable 6, 1 and 6* 2* As previously reported (Foulds et al 1968c) no significant abnormalities were detected in serum vitamin B12 assay, or Schilling test results in hober* s hereditary optic atropîiy# fhe mean plasma cyanide concentration was 0i054 micro moles# When only the smokers were considered the mean cyanide concentration was 0*045 micro moles#A similar higher level was found in the smokers, when the plasma thiocyanat# concentrations were examined « mean 2*88 micro moles per 100 mis, 5#18 micro moles per 100 mis* for smokers only, and in the urine where the thiocyanate concentrations were 5*97 micro molea/lOO mis* urine and, 3*75 micro molos/lOO mis* urine for the smokers*
191
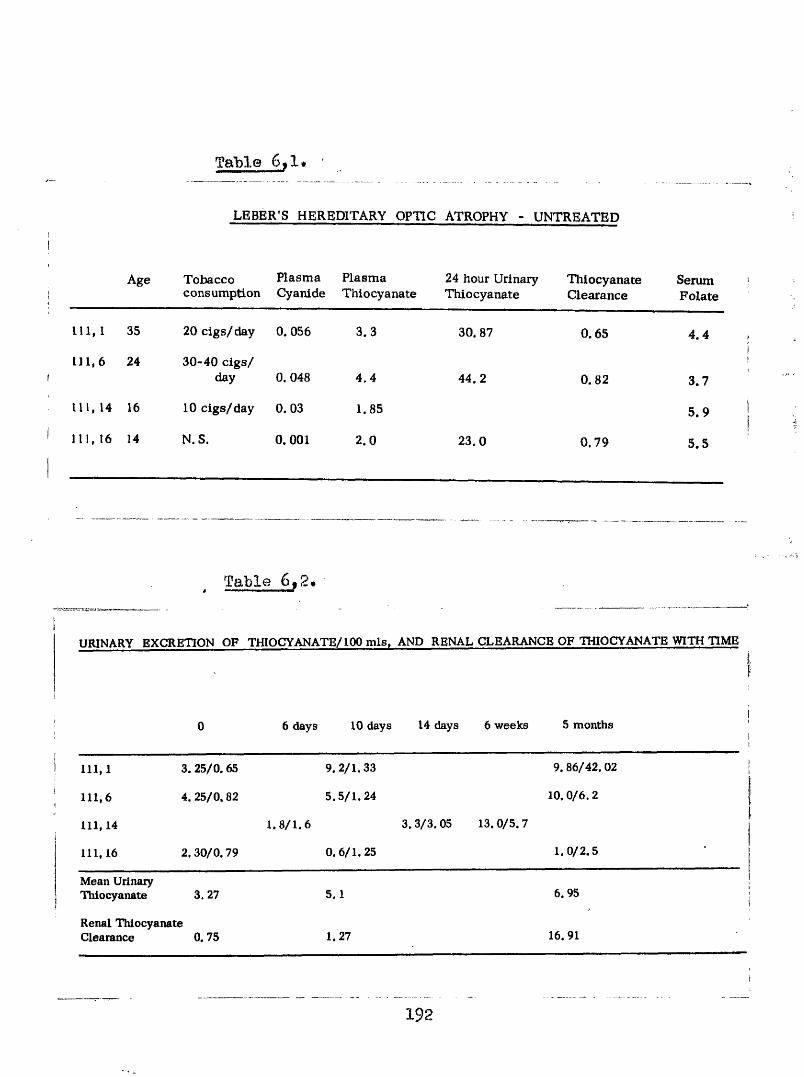
Table 6,1*
LEBER’S HEREDITARY OPTIC ATROPHY - UNTREATED
Age Tobaccoconsumption
PlasmaCyanide
PlasmaThiocyanate
24 hour Urinary Thiocyanate
ThiocyanateClearance
SerumFolate
111, I 35 20 clgs/day 0. 056 3.3 30. 87 0.65 4.4
i n , 6 24 30-40 cigs/ day 0. 048 4.4 44.2 0.82 3.7
111, 14 16 10 clgs/day 0. 03 1.85 5.9
111, 16 14 N.S. 0. 001 2.0 23.0 0.79 5.5
Table 6,2,
URINARY EXCRETION OF THIOCYANATE/100 mis. AND RENAL CLEARANCE OF THIOCYANATE WITH TIME
0 6 days 10 days 14 days 6 weeks 5 months1
111,1 3. 25/0.65 9 .2 /1 .33 9.86/42. 02
111,6 4.25/0 .82 5 .5 /1 .24 10.0 /6 .2
111,14 1 .8 /1 .6 3. 3/3. 05 13. 0/5. 7
111,16 2. 30/0.79 0 .6 /1 ,25 1 .0 /2 .5
Mean Urinary Thiocyanate 3. 27 5.1 6. 95
Renal Thiocyanate Clearance 0.75 1.27 16.91
- - - - ~-------192
---— ■ ------------ - ■ ■
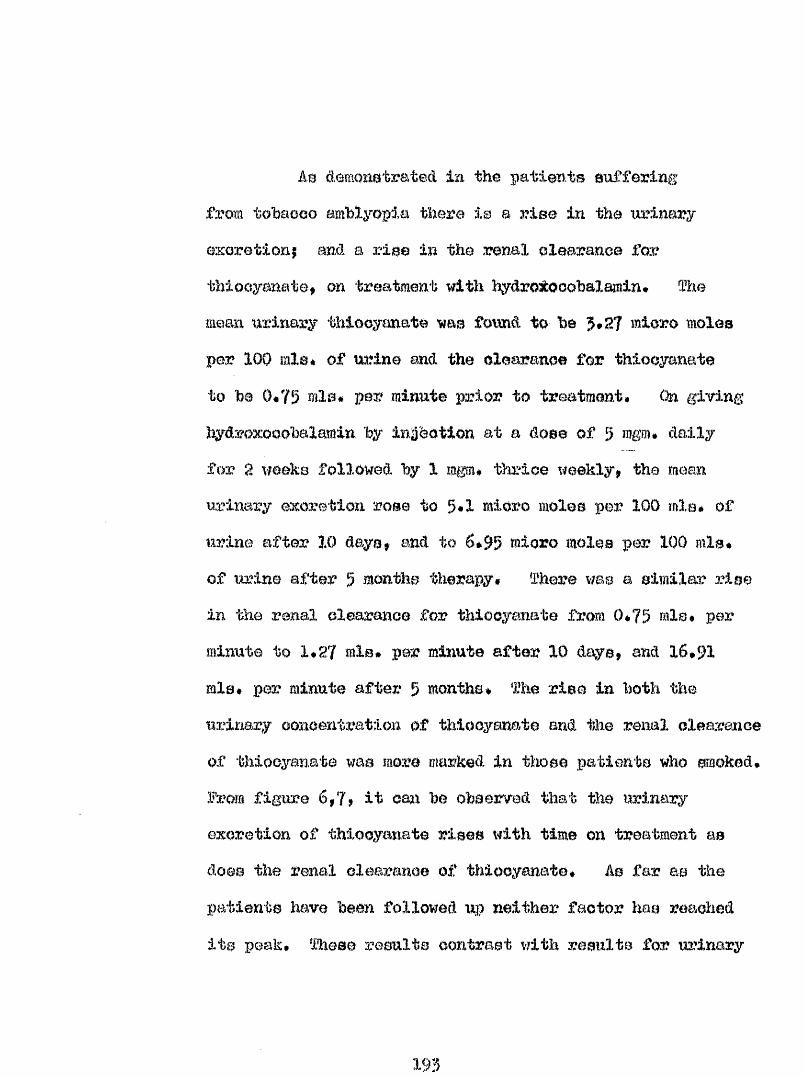
Am demonstrated in the patients suffering from tobacco amblyopia there is a rise in the urinary excretionj and a rise in the renal clearance for thiocyanate, on treatment with hydro:^ooabalamin* The mean urinary thiocyanate was found to be 5*27 micro moles per 100 mle# of urine and the clearance for thiocyanate to be 0*75 mis* per minute prior to treatment# On giving hydroxooobalamin by injection at a dose of 5 mgm# daily for 2 weeks fallowed by 1 mgm* thrice weekly, the mean urinary excretion rose to 5*1 micro moles per 100 mis# of urine after 10 days, end to 6*95 micro moles per 100 mis* of urine after 5 months therapy* There was a similar rise in the renal clearance for thiocyanate from 0*75 mis* per minute to 1*27 mis# per minute after 10 days, and 16*91 mis* per ailnute after 5 months* The rise in both the urinary concentration of thiocyanate and the renal clearance of thiocyanate was more marked In those patients who smoked, from figure 6,7, It om% be observed that the urinary excretion of thiocyanate rises with time on treatment as does the renal clearance of thiocyanate* As far as the patients have been followed up neither factor has reached its peak* These results contrast with results for urinary
193
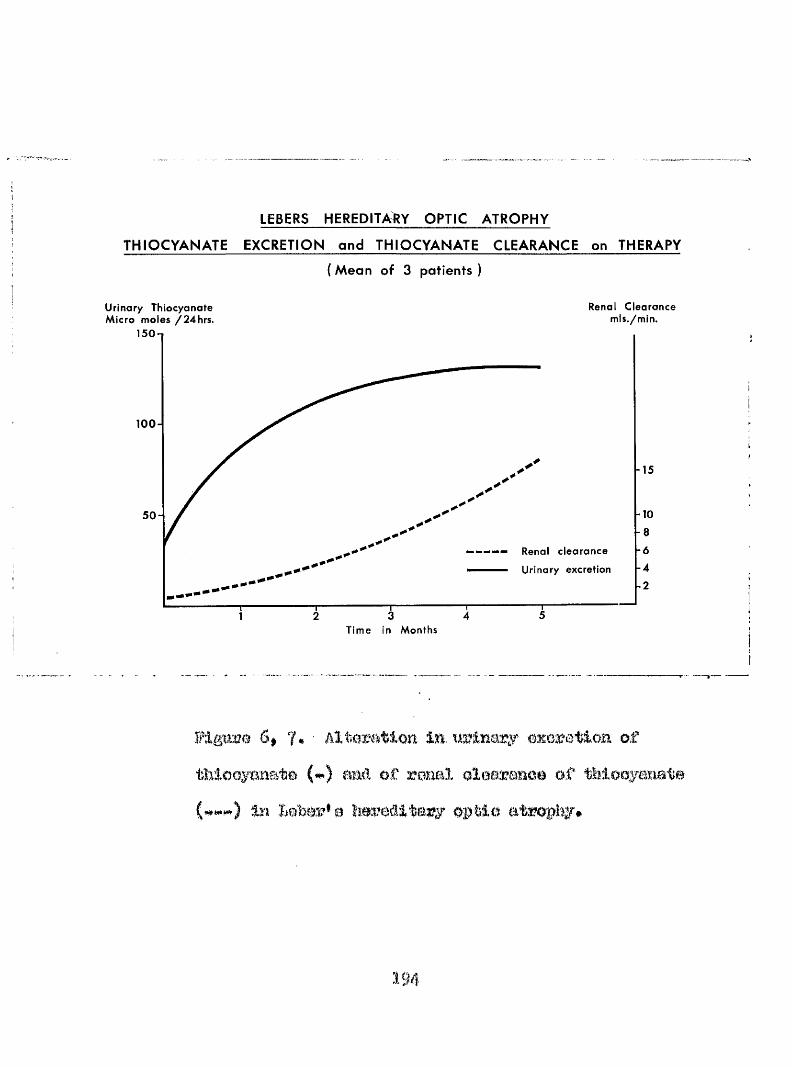
LEBERS HEREDITARY OPTIC ATROPHY
THIO C YA N A TE EXCRETION and THIOCYANATE CLEARANCE on THERAPY
(M e a n of 3 patients)
U r i n a r y T h i o c y a n a t e M i c r o m o l e s / 2 4 h r s .
R e n a l C l e a r a n c e mis./min.
100-
5 0 “
R e n a l c l e a r a n c e Uri nary excretion
T i m e In M o n t h s
15
-10
- 8 -6 - 4
-2
Plgmme 6» 7* ■ AlWmtloa la uaylnary eaceration of thlooyaaate (#) aad of rmal olomzaaoo of thlooyaimte
In optlo atmpi##
194
obtained in # m tobaaao aablyopia patienta
whoae thiooyanato «Korotlon raaohed a peak aome tvro mokB after the emmenoemeat of therapy#
II. &8E
Th0 0stmolBM.on haWean theae two oomlttionw hao Wen reoo0niee& for eome time* flms Leiehmsn (19S5H) found 10 mamplea of a#leonlm% pmmloiomB maemla in hi# review of 75 patienta eufforing from tohaooo amhlyopia and Heaton et a% (1958) 2 e%amplea in their analpiie of 13 tohaoeo m%blyopia patiente* fhe latter authors further felt that patiente with the retrohulhar neurltie of pemloione anaemia who emoked ooiiM equally be deaorlbed ae suffering from tobaooo amblyopia, fhie theme was farther amplified end confirmed by WmmBu mû Heaton (1961)# Heiahman (1951) was of the opinion that tobedoo amblyopia and the retrobulbar neuritle of pemloloue anaemia oouM oo-exiat and Oohen (1936) end Moàlpine and Goldsmith (if51) fmnd optio atrophy ae the prwentimg elgn of perniolowe anaemia#
195
dallemêer Dmborough (1957) produced miâm00 that there is a **pra*pWAicioue anaemia* etato in which there ie laboratory evidonoo of pomioiouo m & m i a (&#e, 8ohlorhydria$ poor absorption of vitamin low or low mmuX serum vitamin B18 oonoeatration) without anaemia# mû wldoh prooedea the anaemia by an interval of years (fewt I92&)* Patients fitting this pre"*pemioiom anaemia at&ta were ifoimi both by hoiiilman (1$%) and Heaton et al
(195®) iu their studies#
Turner (1940) noted #mt the development of amblyopia in pernioiow anaemia was not related to the degree of amemia# but was pmalbly related to the smoking habit of the patient# Adame at al (1967) and fonlcls et al (1968e) reported exmploa of amblyopia in non^emohore. Of the 5 patients reported by IRmldn et al (19680) all m m
female#
In this p%*eomt analysis of 65 patients Buffering from tobacco amblyopia 11 patiente m m found to anffer
from Addisonian pemleioua ammla# dlognoeim Wing baaed on anaemia (haemoglobin leas then lOQm^)# megaloblastic
196
arythopoaala Im marrow examination eerum vitam in BIB
oowentration 110 pg/ml oirouXatiBg antibody to gaeirio parietal celle# aohlorhydria# end a Schilling toat result of <6 recovery# In a further 11 patients evldenoe of the ‘■ pre' parnloicme anmemin" atato without anaemia was found#Of tho80 patienta 1 subsequently proved to have a gaotrio oaz'oinomm and 4 had undergone previous gaetrlo or Intestinal
ourgory# %u# slightly more than tl of the patienta in tliia analyela eWwod evl&enqe o f overt o r weult pernloloum
fhe patienta mfferlng f m m Addieonian powJloioue anaemia were Hon# 1#Y,8*13#17*27#B9,33#36#90 md 57# and
included the only female patient in the analyala who smoked oigarottea (those In #e**pre^pornlolouo anamia"* otato were
Moa# 6,18#80*%3#85,44#46,48,56,98,65*
Hone showed the retinopathy of pomlolous anaemia and ofhthalmoeaopy revealed p a llo r of the optlo diaoe.lEaminatioE of the visual field# revealed the oentro-oaeoal sootom of tobacco amblyopia and the emmlnatlon of the colour aenao showed a grooa distwhanoe* Several patienta
1 9 7
Mil bem diagaosed m suffering from pomiolouo ememla initially end h M the visual defect oatogorieod subseqiimtly*
fho olinloal details of three of the oaeee merit mention IndivitioBily# ftieae m:# two obbbb of tobaooo
amblyopia ocowwihg In patienta # m m to have pernloious mmmia and whose vision failed to Improve on traatraant with oyanoooMlamln in apite of a mtimi to normality of the blood pioture# In each oaae there was a prompt Improvement in vision wtoi tmatmemt m m ehmmgeë to %#ifoxoooh$lamlm* The third patient aatuaXly developed tohaooo amblyopia while on
with oymiocobalamin for permloioua anaemia ant who only vision when the treatment was changed tohydimooohalamin.
Q flTBt.i patient (Claeo Ho#X) was a man of 56 years of age who smoked 1 os# of tobacco per week as oigarettss# He was a vegetarian# When first seen he had a visual soulty of 5/60 with the right eye and 5/6O with the left eye# Examination of the visual fields revealed the oharaat'èrietio ohanges of tobaoeo amblyopia* Jle was not anaemia (haemoglobin 14 g/lOO ml# PGV 45) hut the serum SI a
198
level warn lose than 8$ the folate being normal(11 Bmg/ml)# of the eternal marrow rmroaledmegalohleetlo oryt&nropooolm# There warn a hletamlne imt aohloTl'jydrla# an aWomal Qohllllng toot snd eerolo^
showed the preeowe of antlhodiee to gaetrlo parietal oeXXs* ^amlnatlm of #e fünûl ehotmd aom # degree of optlo atrophy and the patient admitted thot Me vlalom had bom poor for at least ntm mom### #rea$mmt with oyanooohalemln 1000 uga# dally for one week wee etarted mâ thle was followed 1:y §00 ug# fortnightly for six months# Bomohlmtlo orythropooBia was reetoreâ imt tlM viaml acuity mmalmd unaltered sM the patient* a treatment mm therefore changed to hydroxooobalamln 1000 ttgt Again there was a rapid Improvementin vla&on# particularly of the right eye# which within a month hai improved to 6/M mal has continue# to improve reaoMng 6/6 in six months# fhe vicioa In the left eye
liarj boon slower to respond# improving from B/6Ü to 6/18 over the course of six months# fhc pmgreae of the visual clef set
la each of these oasw 1# mcorded in figure 6,0*
file G'orid patient (Claae io#T) a male agcâ fl years#
smoked 2 o%# of pipe tohaooo per week# Hie visual aoulty when first seen was lees thai% 6/60 with either eye nnd there
i#
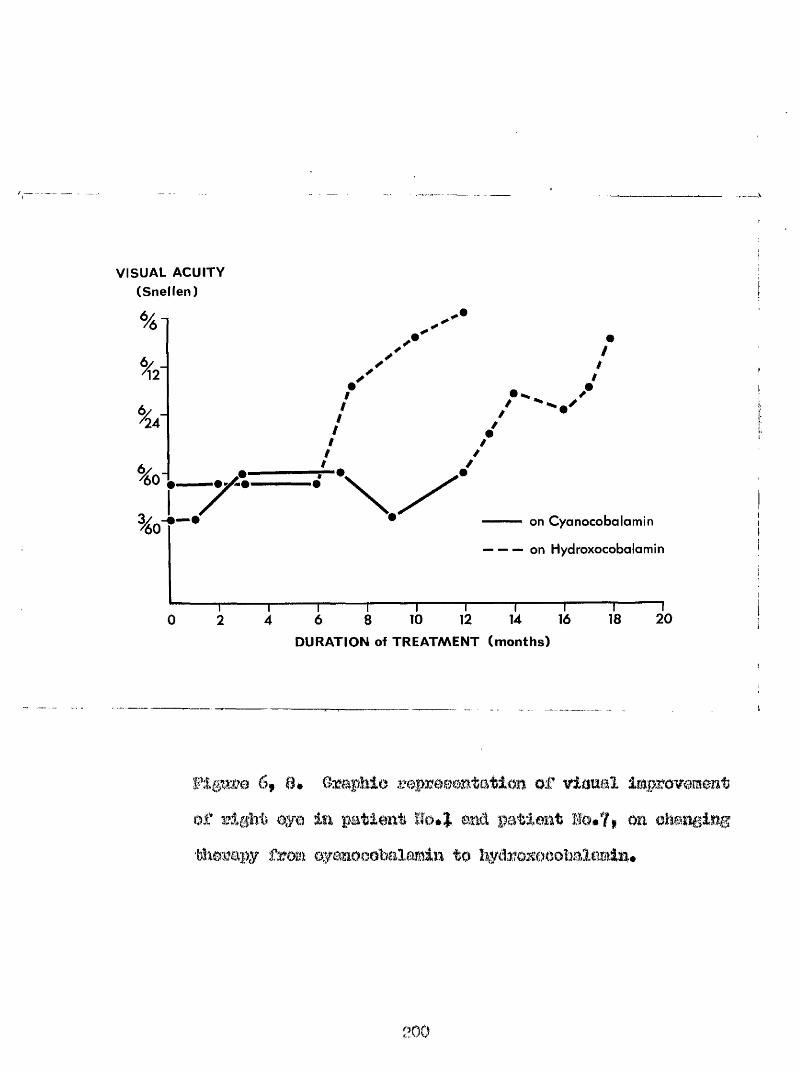
VISUAL ACUITY (Snellen)
t
on Cyanocobalamin
on Hydroxocobalamin
12 14 16 184 6 8 10DURATION of TREATMENT (months)
20
6f ##of qyo
m of viamal Improvement
wao a éofeot of tobawo amblyopia% 0 patient wao POV Ê4#5) O M was
/.Vi gf*uifmm to be ÿ wv^«wkwu*aotlo memfow,
positive aerology for gaaWlo pmzletal oe&l oatlbodles# 6ohllllmg^ toot 3#7^0# '^aatmmt witb parenteml0ytiK)0Obalai«lm 1000 %a* once weekly for one month was iBitituted am# was followed by 1000 %a* onoù par fortml#t for eemm momth# when the doae wa# redneed to 500 mg@* at Intervale of three weeka# On this treatment the blood ploture ret%#%ed rapidly to normal# Imt the vieiml amrity whioh initially improved over a period of tm months# from leas than 6/60 to 6/60 in eaoh eye# did not improve farther* After one year on oyanooobalamin treatment was ohmged to hydro%:oeObal8min (1000 mge# twlee per week), There was am almost immediate improvement in viaual amity, Within two weeks the vision had impmvmd to é/$6 with the right #e m 6/24 partly with the left# and the vision has contlnned to Improve eimoo then reaching 6/gf with the right eye ©mtl 6/l
eye in #1% montho.
m&0 Iw* a male
.!01
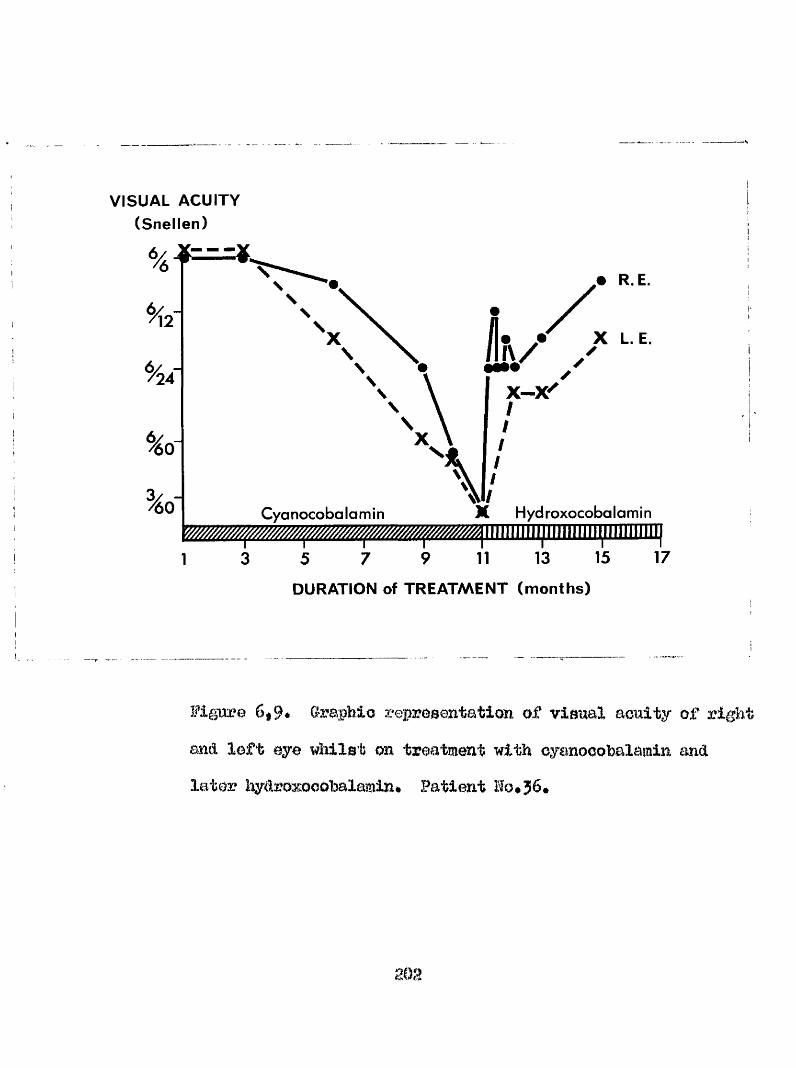
VISUAL ACUITY (Snellen)
% i
V
e R E.
X L. E.
Cyanocobalamin Hyd roxocoba lamin
1 5 7 9 11 13 15DURATION of TREATMENT (months)
17
Figure 6#9* Oraphio representation of visual acuity of right and loft eye whilst on treatment with eygmooohalamin and later hydroxooohalamin* Patient Ho, 56.
pipe smoker# of 51 years of age, smoked one half to three quarters of an otmoe of tohacoo per week. In May, 1966, hesustained a contusion injury to the hack of his head andfollowing this noted a proptosis of the left eye without eechymosls# He was admitted to hospital where h# was found to have pernicious anaemia and treatment with oyanooohalamin was started (lOOO ug* daily for one week followed by 250 ugo# weekly for one month, when the dosewas reduced to 250 ug* fortnightly. Four weeks later thedose was further reduced to 250 ug# monthly). On this treatment the blood pictwe returned rapidly to normal.His proptosis however increased and he developed diplopia.In July 1966 he was admitted to the Glasgow Institute of Neurological Sciences where he was found to have 6 mm. of left proptosis, slight blurring of the optic disc in the left eye and a bilateral depression of the centro-*oaeoal area of the visual fields to a small red target, suggestive of early tobacco amblyopia. At that time the viemal acuity was normal in eaoh eye* In August I966 an exploration of the left orbit was carried out, a biopsy showing a non* specific orbital granuloma* Following this procedure the proptosis disappeared and has not recurred. In October 1966
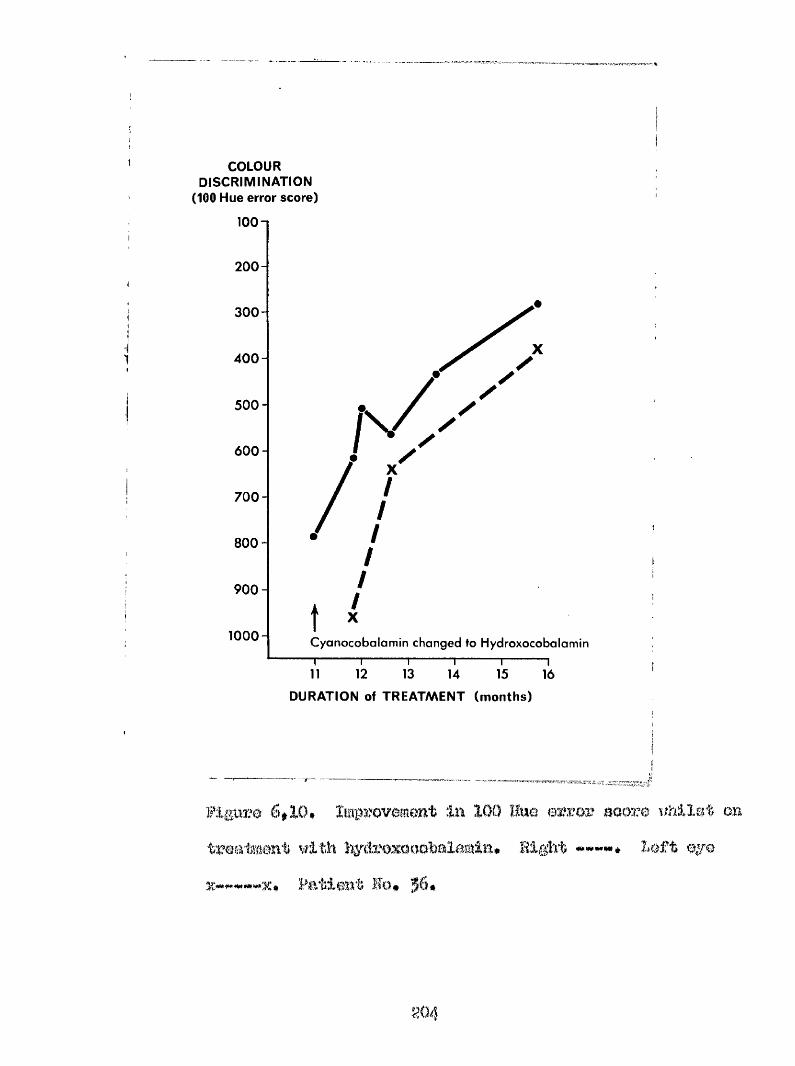
COLOUR DISCRIMINATION
(100 Hue error score)
100 n
200-
300 -
4 0 0 -
500 -
600 -
700 -
8 00 -
9 0 0 -
1000- Cyanocobalamin changed to Hydroxocobalomi
12 13 1514 16DURATION of TREATMENT (months)
6*10# Improvement in 100 I; treatment with
Patient Bo* 56*
3 error aaore nhilet on it lOift
the vimml aooity v;ae noted au 6/9 p a rtly w ith the r l^ h t
eye tmd 6/18 with the le f t . Four mcmtho la te r he was
OGoa aipAn and the vleual aoaity in Um rig h t ey© wso
recorded ao 6/24 pa rtly while the vi.3ioa in the lo f t eye had
falXon to 6/60# Bie reading vio lon wao groooly impaired
and the visual fie ld s ohowed groB$ contro^oaeoal Xoeo with
dense ielando o f oootoma typ ica l o f tobacco aabl 'Opia#
There wao no peripheral IOO0 of visual field; the right optic fliao appeared normal but the left was cllghtly pale# The patient was transferred to our care for further iv:).vo0tlgation xému It was fou.nd that # m visual acuity !iad fallen to g/60 (coxwctod) with either eye, the reading acuity in the right eye being M24 and in the loft B48#There visa a groao defect of colour discrimination* the l%3mev;orth Huneell 100 Hue score for tho right eye being 7969 a partial taiviorrhai hy oa the left aide raeking colour vision tooting ia this eye difficult. Boring all the time that the patients vi,Bion had been d.ettml ora ting* trcatïsïont with parentorml oymiooobalamiu had been maintained and the patioat continued to smoke#
Treatment with Ip/droxocobalemin lOQD ug. daily was Otar tod and jithin throe days tlio visual acuity in the right
eye which had hmn 2/60 improved to 6/24 p a r t l y One week after the oomwmoement of treatment the visuel acuity in the right eye had Improved to 6/12* euhaetpentXy fluctuating during the eucoeedlng week between 6/l0 and 6/24# fwo weeks after the oommenoement of therapy the left tarsorrhaphy was divided. fhe eourao of the visual acuity for each eye in shown in Flg»6*9 where it will bo B m n that over a period of four moBtha the visual acuity in the right eye improved to 6/9 and in the left to 6/18 partly* There waa a ooinoident improvement in colour diaorlmination which is shown graphically in Fig*6,10*These patients illustrate the incffaotlve value of cyanocobalamin in the tremtmont of pernicious anaemia accompanied by visual disturbance# They further eupport the view that Îîydroxooobalamiîi should replace cyanocobalamin in the treatment of pernloioue anaemia* particularly If the patient is a smoker*
206
fh© hypotheale that inter connected dleturbsnoeeof oyanide/vitamin 112 metabolism may be oonoerned in the pathogenesis of tohaoeo amllyo%)la* - the retrobulbar wtLeltla of peamioieao anaemia*^ Maar’e hereditary optic atrophy and certain tropical neurologloal syndromes apparently associated with a high oyanlcie intake# is si^pported by the investigations of Smith (I96I) Wilson (I95^a)#. Montgomery(1965) Wilson and hangman (I966)# Monekoseo and Wilson '(1966)# freeman (196?)#-Ohlaholia et al (196?) and Osnntokim et al (1969).
Observations apparently provi.dlng # direct link between smoking and vitmaln B12 metabolism are few, They inoludei-**
I, Thera may be a slight or moderate inoreas# in eyanooobalamin In the plasma of some heavy smokers,(Lindstrand et al 1966),
2* The finding that a larger proportion of norm
ao?
vitamin B12 is extraotable in the absence of added cyanide in smokers than in non-smokers# (Smith 1961)*
5* The finding of a negative correlation between plasma cyanide and total serum B12 concentrations#(Matthews et al 1969* Wilson and Matthews I966)*
4. The urinary excretion of vitamin B12 is increased in smokers# and is assooiated with an increase in vitamin B12 excretion and a relatively low serum vitamin B12 concentration (Wilson and Matthews 1966) #
The findings contained in this thesis are presented to amplify and strengthen the theory underlying the aetiology of tobacco amblyopia and related conditions - namely a disturbance in the cyanide / vitamin Bl2 relationship and the following new facts may be emphasised#
(a) The concentrations of serum vitamin BX2 in tobacco amblyopia are reduced when compared with the concentrations in non-amblyopio smokers and non-smokers#
(b) There is a positive correlation between tobacco intake# on the one hand and serum vitamin B12 concentrations# and vitamin B12 absorption on the other# in subjects suffering from tobacco amblyopia#
2 0 8
(o) There are reduced concentrations of thiocyanate in the blood of tobacco amblyopes which undergo elevation in response to therapy with hydroxocobalamin.
(d) A rise in the renal excretion of thiocyanate in tobacco amblyopia occurs in response to therapy with hydroxocobalamin •
(e) The elevation of the thiocyanate concentration in the blood and urine is also found in patients suffering from Leber’s hereditary optic atrophy who are treated by hydroxocobalamin..
(f) Changes in the renal clearance of thiocyanate observed in tobacco amblyopia, Leber’s hereditary optic atrophy and non-amblyopic smoking subjects, receiving hydroxocobalamin can only be explained by the renal tubular epithelium being a site of production of thiocyanate*
If the intestinal absorption of vitamin 112 is reduced to such a degree that the daily metabolic turnover rate or lose of vitamin B12 (approximately 2.55 ug per day, Heinrich I968) is no longer compensated for, only the vitamin B12 pools in the storage organs and tissues can be
as ô source for the matsbollo vitamin 'B12 roquirommt. Tille situation results in a progressive depletion of the vitamin B12 ooenayme body stores * which ia refleoted in a
réduction of the vitamin #12 oonomtrationa in the eerm rniâ urine and am inoreased methyl melomato urinary exoretlon#
Following manifestation of the biochemical vitamin Bit defioienoy aymptoms# the morphological and olimioal
eymptoms of Bit avitamlnoeio oam become menifeot (#$#2*1)
There is ample evidmoa by other authors miâ in this thesis that, in general, tobaooo amblyopia patienta have a lower m m m vitcmia B12 concentration than do noit-aablyopio amokera, though in only 18^ was the cmmm concentration found to be pathologically low* â aignificant proportion of the tobaeoc amblyopes showed, in addition a defective absorption of radioactive labelled vitamin Big,
It Ima boom shown that cases of tobacco aort)lyopia, whether overtly vitamin Big deficient or not, recover vision on treatment with îaydroxooobGlamln, even if smoking is oontinuod (Ohioholm et al Igë?)* From this alone it ie
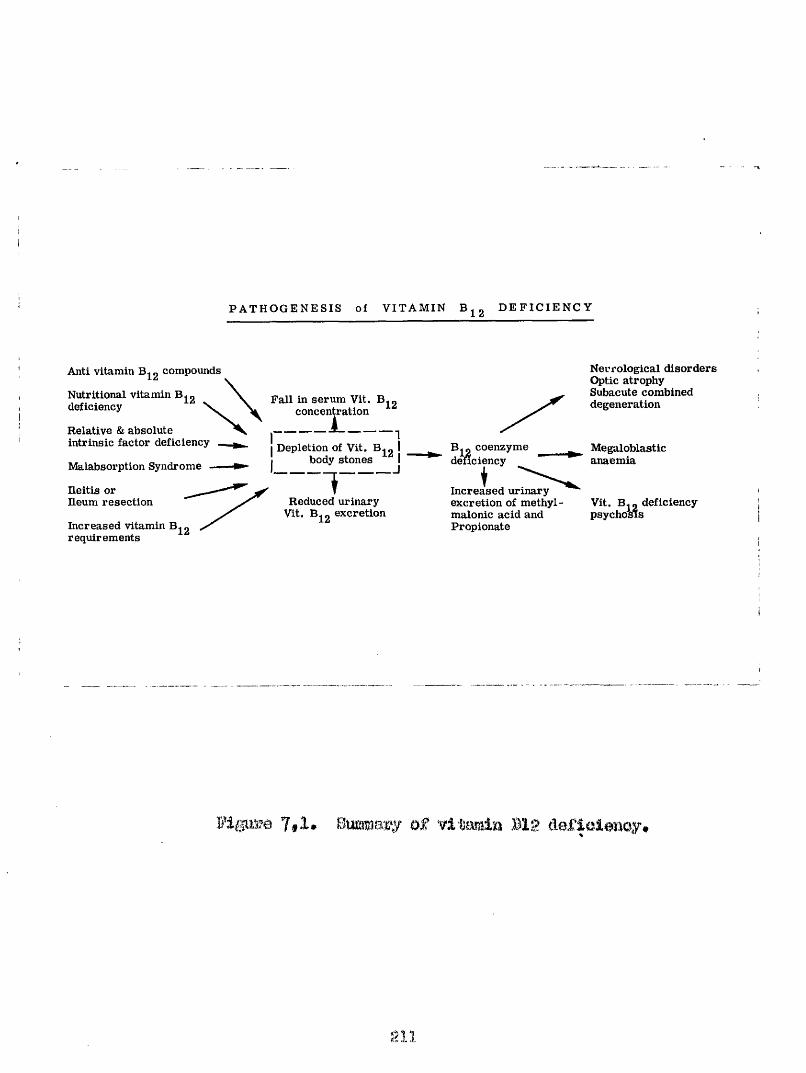
P A T H O G E N E S I S of V I T A M I N D E F I C I E N C Y
Anti vitamin compounds
Nutritional vitamin B deficiency
Relative & absolute intrinsic factor deficiency
Malabsorption Syndrome ■
Ileitis or Ileum resection
Increased vitamin B
Fall in serum Vit. B^g concentration
I Depletion of Vit. B. g I I body stones J
requirements
TReduced urinary
Vit. Bj g excretion
B. 2 coenzyme denciency
+Increased urinary excretion of methylmalonic acid and Propionate
Necrological disorders Optic atrophy Subacute combined degeneration
Megaloblasticanaemia
Vit. B^g deficiency psychosis
Fi||UM 7,1, Summary of vitamin Big dofioleuoy#
evident that in these patients, although there may he no apparent vitamin B12 defioienoy, there must he a relative deficiency of vitamin B12 itself or some active vitamin B12 analogue*
The development of tohacoo amblyopia, however, cannot be merely the consequence of a high cyanide intake in the presence of vitamin B12 depletion, for the correlation between tobacco consumption and serum vitamin B12 concentration is not very close* In addition, examination of a number of patients with Addisonian pernicious anaemia who were also heavy smokers, has shown no discoverable disturbance of visual function. If vitamin B12 deficiency and heavy tobacco consumption were the sole factors in the production of the amblyopia# such patients would inevitably develop the condition*
The results do not reflect the view that tobacco consumption may depress vitamin B12 absorption* There is no statistical difference in the serum vitamin B12 concentration of smoking and non-smoking subjects and there is- no correlation between tobacco intake and serum vitamin
212
B12 concentration in healthy pipe amokera* (Only in the amblyopic patient do the intestinal absorption and serum concentrations of vitamin 312 vary directly with tobacco intake). It would seem from the results that depressed absorption of vitamin 312 as shown by the Schilling test or low serum concentrations of vitamin 312, is an Independently determined factor of aetiologioal significance in relation to the development of tobacco amblyopia,*
It is well recognised that patients suffering from tobacco amblyopia show a high incidence of systemic disease, especially of those diseases known to be associated with abnormalities of vitamin 312 metabolism* Even in patients with a normal capacity for absorbing vitamin 312, the serum vitamin 312 iéf often low, and the results suggest that there is often a dietary insufficiency, which is further reflected by the finding of low serum concentrations of other factors such as folic acid.
The therapeutic effect of hydroxocobalamin in these diseases is difficult to explain and requires examination of the known detoxication mechanisms for cyanide.
2 1 9
1* O^aniâe is oom’bined with inorganlo sulphur iu the liver to form thiooyanate. This reaction is cateljsed by the enzyme thiocyanate*^oyanide sulphur transferase* (Hhodanese, EC* 2*8.1,!,)
2. Cyanide may react directly with 3 mereapto - pyruvate to yield thiooyanate and pyruvate* This reaction is catalysed by the enzyme 3 mereapto pyruvate ^ cyanide sulphur transferase* The 3 mereapto pyruvate is obtained by transamination of l*-oysteine,
3* Cyanide is known to react spontaneously with cystine to yield cysteine and either 2 •<- imino 4 - thiazolidine carboxylio acid, or B^thiocyanoalanine* little is known of the further reactions of 2-imino, 4 thlazolidine carboxylic acid, but B - thiocyanoalanine after deamination will yield thiooyanate and pyruvate*
4* Incorporation into the carbon « one metabolic pool and subset^uent excretion as carbon dioxide or synthesis into formate, allantoin, choline etc*
3* Direct union with hydroxocobalamin to yield cyanocobalamin *
The therapeutic effect of hydroxocobalamin has been shown to bring about a rise in the thiooyanate
214
ooaoontration In the blood and urine, Somewhat elmllar changes have been shown to occur-also In patienta suffering from the optic neuropathy of pernloioua anaemia, and Leber*s hereditary optic atroplsy on the came treatment* It would be naive to ' aasume that the therepeutio effect of hydroxocobalamin is merely its union to form eyanocobalamin,88 £!mlth (196§) has shown that the amount of cyanide removable by each moans is very small* It would eeem unlikely also, that hydroxocobalamin was acting m a '*carrier" for oysnidei as the cyanide cobald bond Is stable, and cyanocobalamin is metsbolically inactive and is excreted unchanged in the m: lne* (Smith I960)* * â more ratioïial consideration would be that therapeutic hydroxocobalamin replenishes the depleted adenosyi coenzymo vitamin B12 stores necessary for the preparation of a suitable sulphur donox’ for the conversion to thiooyanate of cyanide*
Dietary sulphur is ingested aa protein containing the sulphur amino acids, cystine, cyatein© and methionine*Such sulphur containing amino acids are utilised in the syntheeis of tissue protein such as hair, insulin, glutathione, B mercapto^ethanolmnine and taurine and some
215
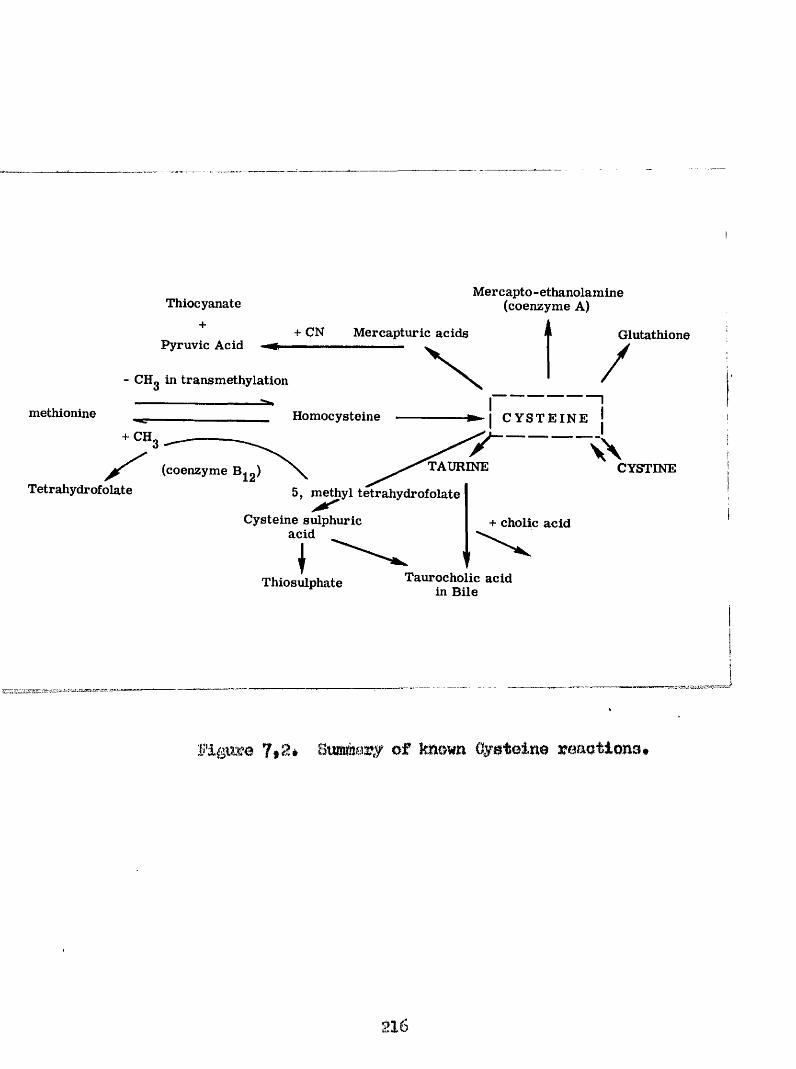
Thiocyanate+
Pyruvic Acid
Mercapto-ethanolamine (coenzyme A)
+ CN Mercapturic acids A- CHg in transmethylation
Glutathione/methionine Homocysteine
+ CH,
(coenzyme B^g)Tetrahydrofolate 5, methyl tetrahydrofolate
- j C Y S T E I N E
TAURINE CYSTINE
Cysteine sulphuric acid
Thiosulphate
+ cholic acid
Taurocholic acid in Bile
ï'igïœe 7,2* Bummary of known Oyatoine jroaotiona,
8 1 6
are degraded to urea and sulphate# The ooheme is outlined in Figure 7, 3 from v/hloh it can be seen that neoeaaary aubatratea for the oonvex'alon of cyanide to thiocyanate are made available# Both ooenzymo vitamin :B12 and .folate are nadeaaary for the aucceaaful preparation#
Failure to detoxify cyanide may ooour in aavoral ways. Loea of liver parenchymal cells will interfere with the conversion of cyanide to thiooyanate due to diminished available rhodaneee, time 'explaining toxic amblyopia in patients with oimzhoBlB in whom the serum vitamin Big concentration is often high#
hack of ooensyma Big will interfere with the conversion of methionine to cysteine rnià this may be a factor in cases of optic neiïropatîiy of pernicious anaemia# Such patients would b# expected to show a high concentration of folio acid in the serum., as has been • ahomu*
Malnutrition will interfere with the preparation of a sulphur donor by dietary deficiency of vitamin B12, folic acid and the necessary proteina# Such patients will
2 1 7
show low ooncontrationa of vitamin Big and folio aoid in their serum. Oeuntohim et al (1969) have ouggested that dietary defiolanoy of cyotlno is oritioal in tropical nut3?itional neuropathy#
Vllleon (1963) has suggested that in Leherfs hereditary optio atx'ophy there is an enzymic dafiplenoy which prevents the conversion of oymiide to thiooyanate#If this is 00, it is difficult to explain the rise in thiooyanate found in the body fluids of patients suffering from this condition on treatment with hydroxoeobalamis^# Although in general patients suffering from Leber*e herciditary optic atrophy show normal serum concentrations of vitamin B12 and normal vitamin B12 absorption (FouMo at al 19680), there may be a defect in the preparation of the suitable sulphur donor either before or after the point at which ooenzyme B12 is utilised#
Direct combination with cyanide or replenishing coenzyme B12 stores may be functions of hydroxocobalamin, but neither explain the observed alteration in renal clearance of thiooyanate found in patients whilst on
aia
treatment with hydroxocobalamin*
It is proposed that therapeutic hyd'rozooobalûKin may affect the tubular resorption of thiooyanate, or altemmtlvely the tubular* epithelium may be the site of extra hepsvtie couverelon of cyanide to thiooyanate* Such renal tubular mechaniame concerned in the active x»eabeorption of thiooyanate i'rom the glomerular filtrate, or active accretion of thiooyanate Into the renal tubulec, may have been "poisoned" by the abnormally high concentrations of cyanide and became corrected by the removal of cyanide on therapy with hydroxocobalamin* However, the renal clearance values for thiocyanate in untreated tobacco amblyopia and Leber*8 hereditary optic atrophy were not abnormal when compared with the values found by Btoa (1957) in healtîay emokera*
It eeema more probable that the tubular epithelium of the kidney la in fact a site for the conversion of cyanide to thiocyanate* This thiooyanate partly diffuses into the blood stream and partly la secreted into the renal tubulaa* Such a meohaniam votxld require not to be dependent
219
on rhodaneae aa it has been demonstrated that on chronic cyanide exposure, rhodanese activity becomes lost, (Sorbo 1951» Schlevelbein et al I969) but would be an alternative and little used pathway, present in both healthy smokers and tobacco amblyopes*
The possible source of the thiooyanate would be from the imlon of mercaptopyruvio acids with cyanide or the degradation of thiocyanopyruvic acid following on the oxidative deamination of B thiocyanoalanine in the kidney*
An alternative reasoning would be contained in the proposal that cyanide combines with a body constituent to form a vitamin B12 antagonist* Smith (l9&3) shows evidence that monocarboxylic acids act as antagonists to vitamin Bl2 action* The union of cyanide with cystine has been shown to produce 2-imino^4*^thiazolidinecarboxylio acid, a monocarboxylic acid* This aoid then blocks the coenzyme action of vitamin B12 in the formation of thiooyanate*By simply raising the amount of available coenzyme B12 this competitive Inhibition is overcome*

E E F F H E I 0 B E
2 2 1
Adams, J.H*, Blackwood, W#, and Wilson, J* (1966). "Further clinical and Pathological Observations on Leber*s Optic Atrophy#'* Brain, 82., I5.
Adams, P., Chalmers, , Fonlds, W.8., and Withey, J*L#(1967)* "Megaloblastic anaemia and vision"# Lancet London, %, 299*
Aldridge, W*H. (194b)* "The estimation of micro quantities of cyanide and thiooyanate#" Analyst, 70*474.
Asaeman, E* (195B)# "La Maladie de Leber, Etude clinique et genetique a propos de 86 cas examines". M.D. Thesis, Lille University#
Bachstez, E# (1920)* "Bericht uber die Haufung von Fallen retrobulborer Neuritis toxischer Amblyopie"# Klin# Monats# f# Augenh., 593
— f and Purtscher, 0# (1920)# "Uber die Hanfung retrobulbarer Neuritiéen ein sohli^lich toxischer Amblyoplen gegenuber der %eit vor dem Kriege"# Zl8chr.f.Augenheilk,44,38.
Badenooh, J#, Bedford, P.D., and ISvans, J#H# (1955)."Massive divartidularis of the small intestine with steatorrhoea and megaloblastic anaemia"# Quart.J# Med., 21,521#
2 2 2
Bair, H*L. (194O). "Some Fundamental PhysiologicalPrinciples in the Study of the Visual Fields"* A*M*A. Arch* Ophth*, 94#10» ^
Bar, J. (1906)* "Untersuohungen hei Tahak Alkohol amhlyopie"* Arch* f* augenhellk#, 391*
Barker, B*At, Weissfeaoh, H* and Smyth, EèD* (1950)* "A coenzyme containing pseudo^vitamin B12"* Proo* Nat* Acad* Soi* U*3*, iif3*093
Batten, E* (1909)* "Two oases of hereditary optic atropiiy in a family with recovery in one case "* Trans* Ophthal*, SCO* U*K*, J£,144*
Baumann, E*d*, Sprinson, B*B*, Metzger, N* (1953)* "The relation of Thyroid to the conversion of cyanide to Thiooyanate"* J. Biol* Chem*, 102, 773*
Baxter, H*, Worsford, J*, Wokes, F*, Norris, F*¥* andFernandes, S.J.O* "Oyanooohalamin and Ifydroxocobalarain in Vitamin B12 injections". J* Pharm* Pharmacol*, 10#723,
Beck, W*0* (1961)* "Metabolic Functions of vitamin B12*The Possible Relationship of Megaloblast formation to Unbalanced Growth in Bacteria requiring vit.BlS"#.J. Olin* Invest*, 1024*
223
Becker, B* R*, Winter, Maaîigwyn-'Davics, G*.,and FriedenwaXd, JgB# (X954)* "The role of the Adrenal Oortex and Vitamin B12 in diabetic retinopetiliy". Amor, d* Ophthal*,
Baer, d#G. Lehre der Au^jenkrankheiten#, ^$499*Tlema#
Bentley, E*E#, and'Berry, (1959)# ^The constituentsof Toîsacoo Smoke; An annotated Bibliography".* Tobacco Manufacturers'Standing Committee, Research Paper No*3*, London*
Berry, G* (1882)* "On central amblyopia"* Royal London Ophtlial* Sosp* Rep., 10*44*
Berry, O.A* (I6B4)# "Motes 6n Tobacco Amblyopia in women, with remarks". Ophthalmic Review, 101. — 1 (iBi?) Discussion on Toxic Amblyopia, Trans*Ophthàl. 800. U.K. 2,91.
Birch-*Hir0chfèld, A* (1902). "%ur Pmthogeneee de cteoniaohen Bicotin amblyopia", v* Oraefe’s Arch. f. Ophthal*, 55*79
Bjorkenheim, B. (%956). "Optic neuropathy caused by vitamin #12 deficiency in carriers of the fish tape#*woa?m Diphyllobothrium latmf * Lancet %, 680»
224
Boger, W,P#, Wright, L.D*, Strickland, 8,0,, Oylfe, J,S, and Gimlnera, J,I»# (1955)* "Vitamin B12* correlation of serum concentrations and age"# Proc# Soo. Exp. Biol#(K.Y.), 82, 3T5i
Bonnefon, (l95l)* "3he value of aoetyloholine in the treatment of toxic amblyopia". Prat# Med# Franc., 12,65#
Booth, 0.0#, and Mollin, B.L. (1956)* "Plasma, Tissue and Urinary Radioactivity after Oral Administration of ^^Go*lah0lled vitamin B12"* Brit# J. Haemat#, 2*^^?
Bouniq, 0. and Cosoas, G# (1966). "Etude statistique etanalytique de I64 oas de negrite optique alcoolo-#-tabaguique", Ann* B^oeulist#, 199*955»
Bowler, 11,0. (1944)* "The Determination of Thiooyanate in Blood serum"# Biochem* J* 30#385*
Boxer, G.E., and Rickards, J#C. (1952)* "Studies in the Metabolism of thé Carbon of Cyanide and Thiooyanate".Arch# Biochem., 39*7
Brady, E.G. and Barker, H.A. (196I). "Influence of dxygen on the photolysis of coenzyme B12"* Bioohem* Biophya#Res.Commun., 4.»373
Braekkan, O.R., NJaa, L.E., and Utne, F. (1957)* "The effect of cyanide on Liver reserves of vitamin B12". Acta
225
phammool* et toxlool#, 1^,228.Brett, O.S* m à Benjamin, B. (1968)* "Smoking habits of
men employed in induatry and mortality"* Brlt.MecUU*, ,82 Britiah Standard 950, Pt.I, (196?)• "ârtifioial Daylight
for the aaseasment of colour"* British Standards Institution, London*
Bronte*Stewart, %T*, Ohisholm, I#A*, and Lewis, B*E*n* (1968)* "Response of metabolic enoephalopatby to treatment with Oyanooohalamin" Soot.Hed* J*, 3.5*274*
Bniyn, G.W*, and Wont, L*H* (1964)+ "A sex#.linked Heredo- degenerative ieurological Disorder associated with Leber* s Optic atropiiy"* J .Neurol# Soi*, X.,59
Burton, H*0*, and LooWiead, A*d* (1951)* "Studies on the production of Vitamin - B12 active substances hy microorganisms"» Oanad* J* ■Botany, 2^*352*
Bussy, tim (1926) * Quoted in Lancet, £#818 Oairnoy, M*M.P* (1967)* "Senam folate Values in 423
Psychiatric Patients"* Brit* Med# J., 512*OalXeiider, S#T*, and Benborough, M*A* (1957)* "A family
study of î?Perhâoi©Uô Anaemia"* Brit*J* Haemat., i,BB* Oarrol, F.B* (1935&)# "Analysis of Fifty five cases of
tobacco alcohol amblyopia"* A.M.A* Arch. Ophthal*, 14*421*
226
— } (1935b)• "Oerebro spinal fluid studies in ten oases of tobaooo alcohol amblyopia"* Amer. J* Ophthal., 18.720*
— ; (1936). "Alcohol amblyopia, Pellagra, Polyneuritis;report on ten cases". A.M.A. Arch* Ophthal., 16.919
— ; (1957)• "Importance of diet in the aetiology andtreatment of tobaoco alcohol amblyopia." A.H.A. Arch* Ophthal., 18.948.
— > (1944) "The aetiology and treatment of Tobaoco alcohol amblyopia". Amer. J. Ophthal., 27*847
— } (1945)* "Recurrence of Tobacco alcohol amblyopia".Amer. J* Ophthal*, 28,656
— (1956)* "Toxic Amblyopia". Trans* Amer. Acad. Ophth.,
68» 74*— f and Franklin, G*E* (1936)* "Tobacco amblyopia: Alcohol
amblyopia". Amer. J. Ophthal., 19*1070 Castle, W.B. (1955) "Development of knowledge concerning the
gastric intrinsic factor and its relation to Pernicious Anaemia". New Engl. J. Med*, 249* 603.
Chisholm, I.A,, Bronte*»3tewart, J., Foulds, W.S* (1967)* "Hydroxocobalamin versus cyanocobalamin in the treatment of Tobacco Amblyopia". Lancet, Lond., 2,450*
227
CMaholîîî, (iSa?).- "An intareatiïig osse of tobaocoamblyopia in a lady". Amer, J, Ophthl., (Refr. -Qraefe Sâèmieoh XI,2*30),
Ohiobolm, J#J, (1890), **Tobaooc Amblyopia", d,A,M,A, 14,224 Olemedooa, C,J*, Sorbo, B,, and ÏÏllborg, S, (196O)#
"Autoradiographic Observations on Injected 33B-.fhiooyanato and I40#,cyamide in mice", Acta pl'ïysiôl, Soand,, 48,302»
Gohen, 0,3, (1959), "iobdcoo-amblyopia", Brit,Med,J,,£$T2 Oohen* H, (1936), "Optic atrophy aa the presenting sign in
Pamioiotis Anaemia", Imoet, Lond#., £#1202,Oolenbrander, M,C, (I962), "Observatione on the Heredity:'-,y
of Leber*B Dlaeaae", Ophthalmologies, 144*446 Oolline, J,, and Martlmd, 1,0, (I9O8). "Disease of the
Primary Motor leuronoa causing the clinical picture of acute anterior poliomyelitis; The result of poisoning by cyanide of potassium", J, 1er, Mental Bis*, J$£»417
Oonnor, 1, (1690), "Tobacco Amblyopia", 4*A,M,A,, 14,217 Cordes, F,C, and Harrington, D,D, (1935), "toxic amblyopia
due to tobacco and alcohol, treatment with vasodilators; a report of eight cases"* A,M.a , Arch, Ophth,, 13,455
CosBU, A. (1923), "AmbXiopia alcoolioo-nicotlnica", Boll d*ooullst,, £,297 (Ref# Eentralbl. f,d, gee, Ophthal,,1Î.295).
2 2 8
GoX| J, (i960). "ColoTB? vision defootb acquired in diseases of the eye". Brit. J. Physiol* Optics, 1%, 195*
Gragg, B.H. (1936). "The treatment of Tobacco Amhlyopla by Acetyldholino". Bristol Med. Ohir. J., 51,23?.
Orone, B.A. (196I) "Quantitative diagmoeis of Defective Color Vieion. A comparative evaluation of the Ishehara test, the Farnsworth Biohotomous test and the Ilardy-Hand Bittler polycliromatlo plates". Amer# J. Ophthal., gl»g96
Dalon (1906) "Ueher die anatomisohe Grandloge de Alkohol fahak amhlyopio". Augenkl. d. Cax*ol. mod. ohir, Inst. Stockholm. (Ref. Jatmeehr. f. ophthal., 1%,220).
Darby, D.¥. and Wilson, J. (196?). "Cyanide smoking and tobacco amblyopia. Observations on the cyanide content of tobacco smoke". Brit. J. Ophthal., gj.,356.
Darken, M.A, (1953) "Production of Vitamin B12 by micro- organisms m à its occurrence in plant tissues". Dot. Rev., j£,99
Doggert, J.H. (1959). "Smoking as a factor in visual disturbance". Practitioner, 182. 204.
Doll, 1., and Hill, A.B. (1964). "Mortality in Relation tn Smoking; Ten year’s Observations of British Doctors". Brit. Med. J., I,
229
Dowling, F* (1908). "Tobacco and the eyes". lancet- Glim. £2,699
Boyjtxe, F.G. (1922). "The scotomata of tobacco amblyopia".Brit. J. Ophthal*, £,X.
Boyne, É.W. (1889). "Obeervatlone on tobacco amblyopia".HoyaX London Ophth. loop. Rep., 12.51
Duggan, V.F. {1935) ^Vascular basis of Tobacco Amblyopia;Treatment with Mtroseleran" * A.M.A* Arch* Ophthal. i l£il059
— / (1937a). "Acetylcholine in the treatment of acute retrobulbar neuritis" • A.M.A. Arch. Ophthal*. 17*579
— > (1937b). "Treatment of Tobacco Amblyopia with vasodilators".J.A.M.A., 1354.
Duke-Elder, 8* (194^)* Testbook of Ophthalmology# III* 3GG9 Kimpton, London*
Bvorihe, X. (1953)* Fseudo-isoohromatic Plates. 2nd M * , Boientifio Publishing Go*, Baltimore, U.S.A*
Sales, 1* (1887)* Discussion on Toxic Amblyopia* Trans* Ophthal* Boo* U.K., X,54
Evans, A.f.G. (1959) *»Tobacco iimblyopia". Brit. Med* J*, £,72 Evans, F.J. (1939) "Tobacco Amblyopia". Trans. Ophthal* Soo.
U.K., 22j 241.
230
Farnsworth# D* (1945) • "Tho Ifarnawox’tk-ltaaèll 100 Hue amê dlohotonou® teats for colour vision"# J# Opt# Soo,Amer#
PergusoA# f *E# and'Oritohlej# #. (1920)# "Labor* 0 Optic atroplij'ancl Its relation to tlm Umeào Familial âtaxléa"#J# Neurol# Psychopath## £#120' '
fiïïlay# (19OI)* ."âlcbihol m â Tobaoco Amblyopia in Ouba."* A#M#A# Arch# Ophth## J^#%1
Fisher# J#M* (1901) influence of licotin on ganglion ' . .■ cells; its hearing cm iAm pathology of tohsCco amblyopia-"# OphthaMio Ileviev, 20*151
Ford# B.H## Eirsohman# 'A.# EMnas# E*# unà 01mborg# S. (Ig6l)& "The rate of uptake and Eadioauto^aphlo looalizatlon of 35s labelled eyctlno"# B%p. Neurol.# £#444
?0x€f J.ll* end Bather# H. (1955). "Bole of Titamin 112 in the metabolism of #loro-or#hlama". Ifltmiu mmâ Morm. #
forotor# (1869). "%er à m schadlicben Mmflws des Tabakrauohaas axif dee "Mmemiogen". Graefe*e /irolufT Ophth.# J£#f3* (Referred to in Jateeshr. cl. Bohlee.
B&stor# (1071). "LWitsiim bel ErWthelten der OhoxiMea uiKl Retime". Klim. Itoate bl.f. Augem## £#344
231
BmMa, Oant# J.B. (OMshoM, I.A., Bronte-Btewart#J#, Wllsmi, T. and Wilsoa, J* (1968a). "Hyâraxoeobalamim in Mm traatmmt of Leber*a Herodltmey Optio Atrophy", lanoet, Lmd.# £#096
fauMst M.S., Ghlsholm# !*&.# m à Bromte-Stowart, J. (1966b) "Serum Thiooyanate eomoentrationa in tob&oco amblyopia", Nature# Lomé», 218,586
Foulde* W.3.# Ghleholm, I.A., Iromte-Stewart# J. mà ¥ilaon# f. (196B&). "Gyanide iMuoed Optio leuropatliy". Fraoesdings of Third Bumpeam OphtWlmologioal Gongreee. (In press),
François* J#, a M Werrieet# 8. (igël). "On acquired deficteioy of colour vlelonlU- ?icion Eos.# £#20i,Franooie* $. and àm m m t^ H# (3$6l). "Etude comparative des Dysohromatopeioa acquises associées m % différants types IFatrophia optique hereclo-faiBiliale". -Aiiruoomliat*,
fTBnU\iBmw$ F,#. mi# Schmidt# T. (%95S) "Bio Untersuoliung der ianmliohor Summation mit itaîiender m d Bewazter, Beismarke naoh dor Methods der Quantitative^ Mohtsinnt sferimotrlo", Ophthslmologica.- 135.6#
froomaii# A.G, (ig#?). "Magaloblaatle anaemia and vision", lancet# Load., 2#422.
2 3 2
— , îîeatüii, "The aetiology of retrobulbar,
B ou rltia in AMtBOiitm peraioloue. anaemia"* Lanoet#
LOM. £#968©alozGWBki (1683') "Dos tromMea vlamela oonsemitita à ï*abua
én tabac". Bec* <|*opht*, £#6??Ganong# ¥*F. (19&5) "Médical Phyaiology". tnd M*# Lange
Médical Fablioationo# Calif-omia# #*$*&.
Clirtlwood# H*ll* (1950} "Vitamin BI2 and re lated faotoras
à o lin io a l and experimental review"* Bdiab* Mai*# J*
— ) (i960) "lîiex oblologieal .methods of assay in oXiaicalmedicine with particular reformxoe to the Investigation of deficiency of vitamin Big and Folia aoid"* Scot*Med*# £#10
— ) fhomeop.#: â*l)*# and Williamson# J# (1967)* "folate Statue
in the Elderly*. Brit. %d. J.# £#670.Glalater# J* (1953) "IW ic a l Jnreapmdemoe ami Toxlcoioiiy"
9 # IM*t -It & S* Llvlngetone Ltd. Edinburgh anil London.
01888, CI*l.J*t Boyd# L.J.# Oellln# #*&*# and Stephaneon, L*(1954)# "Uptake of Badioaetiire Vitamin B12 by the ' Mirer In Iteaaai Tmt fm moaemrement of Intestinal Absorption' of Vitamin Big and Intrinoio factor activity''** Arch# Biochem. Blopbyo.# 51,251
233
Glazer, H*B*, Mueller, J.F*, Jarrold, T., Sakurai, K«,Will, J.J., fmd Vilter, H.W, (1954)* "%e effect of vitamin Big and Folie Acid on Nucleic Aoid composition of the bone marrow of patients with megaloblastic anaemia" *
Lab#' Olin# Med#, £2^,905 . Goldstein# f# and Eledéra# F# (l955)v "Conversion of
Thiocyanate to Cyanide by an Bt^throcytio Enzymè"#Amer# Jv: Phyeiol.# 173*207
Gottlieb, B* (1941) "Vitamin B complex deficiency as a Cause of retrobulbar neuritis and peripheral neuritis in a chronic alcoholic and pipe moker"v Iriti;Ophthal#,-
Gough# K^E* # McOarthy,; 0 . Head# A#$k# Mollin,? andWater#,;' A*ll*= (1964) "Folic aoid Deficiency in Hheumatoid Arth0tiW"#r Brit.^ Med.' J#> 1^212.'
— ) Read, A*l#> McCarthy,> CvF*, and Waters# A#H# (l)^))#"Megaloblastic anaemia due to Nutritional Deficiency Of Fdllc'-Acid"*' Q uartJ *" % d #-# 32 # 24 3
v.Graefe, A* (IB65)# Klin* Monatsbl.f* Augen*, £,192 (Ref* Graefe-Baemiach XI,2,30)
Greaves, H.A. (1936) "Ophthalmology" Practitioner, 137*593*
254
Griffith, A,H# (188?) "Toxic Amblyopia: Analysis of mmufrom the cliniques of IW# Little -and Glasoott".Tràtm. Ophthal. 8oo.U#K., %,81.
Groenouw,- A# (1892) "Dehor die XntoxioatioBa amblyople".Arch,f,Ophth., £8,1.(1893) "Ueher die Sehsoharfe tier NeWmutporlpherle and eine nemo UmtersuoWmgamethode deraeiban". Aroh.f*Auganh., £6,8$.
GroBB, 8. ,(1938) "Bedemtuiig der S-vitamin© in der Angenheil: skundah. v. Graefe* e Aroh. O p W M # 140.149
’— :> (1949) "Retrobulbar neuritis due to malnutritltm".Ophthalmologioa, llS.tlS4
(Mam, J » A. (1930) "Toxlo- Amblyopia". Trans. Ophthal. See. J^390.
#mm, M. (1067) Biecneaion on Toxic Amblyopia* Trans; Ophthal* 800. U.K. %,67.
Baberahon, B.B. (1888) "Case of Juvenile fobaeeo Amblyopia".Traw. Ophthal. Soo*. f.lC-., £,229
Ihmhraein, &*, end Sohepehe, 0*L# (1946) "l/âmhlyopio fahagiqme"* Ann. S-*oemli0t„ 179*191.
— ) (1949) "Amblyopia tabnglquo et Atrophie Optique herMo- familialeOph#almelo#ea, 118*749
235
Hardy, L#H«, Band, G», and Bittler, K#G# (1955)* Fseudo- ' isochromatio plates for Betecting, Classifying and Bstimating the Begi'eo of Defective Colour Vision* âraerical Optical Co*, Sonthbridge, U»S*A.
Harman, N*B* (1904) "The visual fields in tobacco amblyopia" Lancet, Lond., £,821
Harms, 1. (1952) "Die Draktisohe Bedeutmig Quantitatives Perimetrie"* Klin, Monats bl, Augenh*, 121*603*
Hartrldgo, C, (1886) "Tobacco Amblyopia" Brit* Med, J*, £,200 Heaton, J.M*, McCormick, A*J*A,, and :Freeman, A*0, (1958)
"Tobacco Amblyopia# Â clinical manifestation of vitamin B12 deficiency"* Lancet, Lond*, £,286
Hedges, lUB* (195T) "Tobacco amblyopia"* Med. Times, 85,1151 Heinle, K*¥*, Welch, Â.D*, Boharf, J*, Meaoham, G*C*, and
Prusoff, ¥*H. (1952)* "Studies of excretion (and absorption) of Co 68 labelled vitamin B12 in Pernicious Anaemia"* Trans* Ass* Amor* Physics#, 65*214
Heinrich, 1*0* (1968) "Biochemical basis of vitamin B12 - action in therapy"* Proc.XlI Internat* Soc. Haemat* pll2*
— , IMmann-Oehleoker, S*, Sommer, L., and Eadel, G* (1956) "Der vitamin B12 - Stoffweohsel bel Hamoblastosen"*Clin, chim* Acta, £,311*
236
Eelmer,. and Pouts, (1937) "Gastro intestinal *Btudies*.fïX fha excretion of xylaae in Pemloioue Amaemlm"# J# Olin* Invest*, 16» 343
llioko, 8*P. (1950) "teiin metmWllem in vivo I* The distribution of Lésions oatiaeâ by cyanide poisoning. Insulin %poglyoaemla, asphyxia in B'itmgm and fluoroacetate poloenlng in rata*" Arch# Path., £2,11%
Ilmwieïi, W*A$, m à apundere# J*f* (1940)# "Basymatiooonveroion of Cyanide to Thiooyanate % Amer. J. Physiol# #
m , M8#lirechler,- I* "Ueher dem lieehraucdi von Spirituosen
xmû. ale teaache von Amhlyople". Arch.f. Ophth.,
Eofftemd., â#V,, $tewart, J##*, Booth, 0*0., and tfollin, B.h (1968). "Folate deflolenoy In C-rohn’a Blsease; Incidence Fathogenesie and treatment". Brit.Mcii. %#., 2,71.
Hornabrcck, E.W., and Ifarlw, V. (i960). "Bffeot of vitamin Big therapy on blood pyruvate- levels- In subacnte combined degeneration of the cord". lancet, Lond#, £,095*
Hmdle, A.D.P., and Ploton millarne, T.0. (1966) "Folic acid Deficiency in Elderly patients admitted to hospital" Brit.md. .J*, 2,202 #
237
lurst, A#F.’ (1922)♦ ^'Fèmlcious Anaemia", Brit# Med.
J., £,970H'orst, B,¥, ■ (1942) "ï 3cperxmental defi^èlânàtion of the
Central Nervous System", Aust, J* Hxp* Biol# Med.Scl#,
20.^97*lutohinsoïi, J, (lBT3) "Statistical details of Four Years
ISxperienoe in Respect to the form of Amaurosis Supposed to be duo to Tobacco"* Royal London Ophth# Hosp, Rep#,
1 , 169— (I876) "Report on the prognosis in tobacco amaurosis"*
Royal London Ophth* Hosp# Reports, £,456*— (188?) Bisoussion on Toxic Amblyopia. Trans* Ophthal*
Bog* b*IC., 2 ,61*
Htttner, S*H#, Provosoli, L., Btokstad, B#L#H*, Hoffman, 'C*B# Belt, K*, I»T'anklin, A.L*, and Jukes, T*H# (l949) "Assay of antl-pernicious anaemia factor with Buglena", jProe* Soe* exp.Biol* (H.Ï.) JO^lla#
Ishihara, S* (1939) Tests for cUlour Blindness* 14th M*, Tokyo, Japan*
Jackson, l.M.D* (1965) "Nutritional Megaloblastic Anaemia"* Scot.Med, J., 10,309*
238
Johnaon, ⻥#^ A*. (195?) vltaailA1&2». TMLtaKk (B%& 2&x#%,,
Jolmeon* 1#.V# (1959) ^*Meoht#l*toWGoo (toEio) amblyopia treated with fhlamltie ühlorlde *». A.#*à# Arob. Ophthal#, Zh-SOS
J'ùlïïiBtonB.f iUAA^Ut Pllmter, J*R* (1959) chamieal ooBOtltiieîita of fobaabo md %baooo Bmoko^, Ohem* Bev#^ 885
Eiimoar, P*B, (1966) Oolour Bleorlmlimtlom of Mabetloo^. fhaoia* Ibiivorolty of Mlnhtïrgh»
Koellner, I« * (1912) "'Dio Storuïigm d m Farbenoiam, Ihre kllmlmclie heâBUttmg mid ibra dlagaooo^f* Earger» Berlin.
Krimoky^ E# (1954)* "%mmetrio ineamplete ammler oootoma of fobacQD origin wltbont mlargement of the blind spot.Amer# 1# Opbthal.,
Ewlttheîijr d*f and .Barest B.B. (1958) amrqpathology of Hereditary Optio .4trophy (baber^s Dieease); #he firat oomplete anatoaio stady*.?# Amer# d. Pa#.»
Ijimgs 1C. (1935) Die ËhadanbiMimg im fiarkorper. Bioohem.%taohr., igg&,245
liang., S. (3.B94) ^eber die Wmwandlrng des âoetonitriis wicl oelmer Momolo#m im TMorkmrper^*. Ardh. 0%p. Bath, u Pharmakol., 247*
259
WmgrnaB, J. (1966)# **Plawmand aaîlTœ y 'Eiloayamate in gsatrie ornioer^*. Btit, X»549
Imntenbaeh) & .J. (I#g8) reen lta in oaee-s o f Tobacco
h aw fe ll*. (1951) **StantlariiS!Stion o f Beading %pe8^« to it .
J* Opbtbal,, a&,?65
( 1952) "Boaain# Typea" B rit* J* O phthal., ,36,689
Bako#aki# 1* (195®) * "Ago and colour vision.'’'** Mvancomont
of Scionoo, I%$2 %— y (1962) *'*îa the deterioration of Colour Discrim ination
with age -due to 1mm or retinal' ehangos"* Die farbe, 11.69 — V (196®):#. Farneuortb. #m@all IÛQ Hue %ct". . Ophthalmic
Optician, 8,B62 —; cmt Davenport, M. ( I 96S) E ffect o f GbloroQuine
therapy on 100 Hue. toat result'** 2nd Scottish Oolour
Symposium, Itlintargh* hear. A,A., Barrie, Oactle,. W,R., mià flealng, #.#*
(1954) scrum Vitamin B12 coneentratiom in Famiclou®J, Lab# Cllirt#. NCd#, ââ.»?^5
heW r, Til* ( I 869) *% her dec vorkoamen von anomalicn dee
WetT'bmmttmm hei Iranldm lten dec Augee, nebot Icmcrfemigm
uber elnlge Forman von Amblyople*** Aroh. f# Ophth*, lg *5#26
240
— ^ (I871) heredltsre imd oongenitalengelegteSchmervenleiden"*V. iraaf0»s Arch* OphtMl*, 17,249
&ee, H*A*, amâ Abeles, 1*E* C1963) "Purification and proportion of DloMehydraoo, an ei^yme requiring a Gotadfio Ooonaymo"» J* Biol* Ghem., JJB, 23^7
Beggc, T.IÎ. C1923) "Dloounalon on Industriel dieeaoe of the oyo * fraim* Opiitli. 800, II.IC*, 4⻑î
hehmamm, and Gimdermann, E* (1912) "Beim iJatorauohmgonuber die Bedontung dor Blameaime for die Olftl^eit das TobakrauoW"* Areh* %g*, 76*90
heiehmmi, S* (l9gl) "#ao$rlo fonotion In tobaoco amblyopia"t %h#al*, 800. B*K*, 11,319
hovinOj S*, and 8typnlkoweki, W. (1959)" "Eacporlmontal oyaaido enooplialopatliy"* ârolu Path#, 67*306
Mille, M*I* (1934) ^The olinioal oignifloanoe of ratrolmlbar aat optic neurltlo*?# Amer* d* Ophthel*, 3%, 110*
Mnclotrandf E. (1964) '^leoIatioB of methylodbalmnin from imtmral nouroe »torialH* Mature (bond*.) 204,11®
— > and Btmhlberg, K*0* (1963) Vitamin B12 Womm In îtean W M m m % Acta %d* Itoahd#, 174*665
241
— ) Wilson, J* end Matthews, D#M. (1966), "Ghromatography and MicroblologieaX Assay of Vitamin B12 in Smokers"*Brit* Med* J*, X,9B8
hinnell, d#G*, Smith,. A*D*M., Smith, G.h,, Wilson, J*, and Matthews, D*H* (196B). "Bffeats of Smoking on metabolism and excretion of vitamin B12**# Brit. Med.J., 2,215
hopeg, ®. (I9OD). "Ainhiiopia par malnutrition". Arch.poliolin.. Havana. (Ref. Jahreshr. f. ophthal., 31»386)»
lumsden, G.l. (1950). "Cyanide leucoencephalopathy in rats and observations on the vascular and ferment hypothesis of demyelinating diseases". J. Beurol. Heurasurg. Dsychiat., 13*1#
hundsgaard, H. (l944) "heber^e disease. A généalogie, genetic and clinical study". Acta ophthal., Suppl.21.
Lyle, D.J. (l94?) "Changes in the visual fields confirmed by pathological diagnosis• J.A.M.A., 135.51?
Lyle, H.W. (1905) "The ÏSffact of Tobacco in Health and Disease". Practitioner. 75.6b
MoAlpine, D., and Goldsmith, A.J.B* (1951) " Optic atrophy and Pernicious Anaemia". Arch, of the. Middlesex Eosp.%, 110.
242
îMurdy* P.R*, Pierce, Math, O.B. (l96s)."Abnemal Boue Harrow Morphology tn Amste Aloohollsa"*Mes migl* d* Med. 2&6.505
MaoWy, I*R., üowliBg, 3)*G., mal Gray, A# (1957).raioeâ vitamin S12 levels Im obstraotive hepaticnearosia". toit# Moâ*
Maokenaie#. 0. (18)0) "Dleeneee of the I%re". 1st Mitioa, Longman, Brown, üreem m # Longmans. London* ’
(1854) 4th mitidn.Ilalpaa, 8.ÏÏ. and Witts, L.d, (l$66) "Bemm
Folia Agid emâ Vltmla B12 Levels in Antioonvuloant Therapy", toit* Med. J*, %,#55
Marna, J*#* (1908) "Some of t W Bffeota of Iteeseivo Smoking".Brit. Mod. J., ^,16?3*
Marshall, J,, amê Seilor, B.l*'(1942)* "A .Statiotioal Analysis of 3*219 poraons certified Mind at the Regional Glinio for Gertifioatioa of the Blind,, Glasgow and Bomtîi West
Bootlomd 1929 1935". Brit. J. Ophthal., 3 3 7 Matthews, B.M., Ctoasegaram, S., and Mnnell, J.O. (1967).
"heemlts with radioisotopih assay of serum Bis using ssmm felmliBg agent", d. Glih. Path., 20*685
243
Ifetltows, B.M*, llileon, J*, aad %%kha, E*d* (1965),"Gyanid© metahall am and vitamin B12 in ISnltiplo Saleroelg". J. ll®urosm?g. Feyobiat,, Xi,*426*
Maxwell, E,W, (1953) "Tobacao alcohol (toxlo) amblyopia".faxaa State d. I%â», 49.137
Miller, &#, and Sullivan, d,F. (1958) "Increased binding of vitamin .BÎ2 by cemm rauooprototns in OEirmlo B%relogewne Leukemia"# d*. Glim* Invest*, ,91?
Mollin, toL*. Booth, a.ü*# md Baker, a,J* (1957) "The absorption of vitamin B12 in Gontrol mAjeote,- in ââdiaonian Pomioiome Anaemia, and in the fflaiabaorptlon Syndrome"# toit# J* laomat*, ,412
— , -and Boas,- G,ï#H, (1952)* "The Vitomin 112 ooaoœtrationa ■ of oorum and urine of normale, and of patiente with megalobleetlo gmmemlae and other dioeaeee"*' J.- Ulln* Path# 1*129
IfOEekoaaot ##&#., and Wilaon, J* (1966)* "Plaoma thioqyanate and vltmln B12 In l lgerien patlmta with degonerative neurologioBl disease"* Lancet,
Montgomery (1965) "The medical eiipxlfioaneo of Cyanogen in Plant foodstuffs"#. ■ Aner*= J* (llin* ■ lutr*, 17*103
244
Vlmhmttf Kelley I K.L., Boxer, 0*I1* onâ'ElükarclOfa.q. (1952) "Antidotal Bffioeoy of Vitamin B12 (%dro%oeabelamln) in exporlmezitnl oyanlâe polgonlng".Proo.Soo, exper. Mol. •(11*7*), ,§|,*234
Bagel, W. (1907) apparats fur die amgeimrmtliehoFonktioB aprafang, Maptometer vmà kloinea Bpoktral photometer (ânemalakop). Beitschr* âugmdmilk., g .201
y’’
iel0OBi J. (1800) "On fotoooo Amblyopia", Brit# M e d , 774 lettlaoMf, (1087) Moouaaion mi Toxlo amblyopia, frans#
Ophthal, 000, W # ,
lottleahip, B, (1909) "On some hereditary diseases of the eye", Trane, Ophthal., SOo, gg^LVII,
— , end Sdmuftclet W*'(1803) "On central miblyopia in diabetes* eapaoially as to its dopandence on* or indep£mâoï^f|gf* tobaoeo smoking". Trane. Ophthal. Boa. W.IC,*
l0ns<dmelor* I, (igBB). "Ambllopl# nicotiniolis". Lett, oftal. 3 9 9
fcel* (ÏB96) "Alterations de 1# macula lutea". Arch, dmphtbel.* 1&479,
O^Brien* M.$ miü Ihflmd* (1964) "Folate defiolenoyin Acute fropieal Bprue". Brit, ffeâ. 4** &*1573#
#rr, E.O. (1936) "âofôtiflotelina in tobaoco Amblyopia". Brit,ÎW. d.* 2*69.
245
Osbome, J.6., Adamek, S** and Eobbs, M.B# (1956) "Borne components of Gas Phase of cigarettes smoke", ilnalyt,
OsiHitokun* B*0.* Monekosso* and Wilson, J# (1969)"Relationship of a Degenerative Tropical Heuropathy to Diet - Report of a B ield Survey". Brit* Med, J,, 1,547
Parsons, d,H* (19DI) "B'urther note on the pathology of toxic amblyopia". Ophthalmic Review 20*181
Patty, F.Ai (1921) "The production of Hydrocyanic acid by Baeillus Fyooyameus", J. Infect, Dis», 22*73»
Pickford, E*W, and î akowski, B# (i960) "The Piokford-Eioolson Anomaloscope", Brit, d, 3?lTysiol, Opt;, 17.151
Pitaey, W,l,, Beard, M,BV, and Tan Loon (1954) ■‘Observations on the Bound form of Titamin 112 in human serum", J, Biol. Ohem,, 207,145
Powers, (r.H> (1806) "Diagnosis and Treatment of Tobacco Amblyopia" Med, lews, 49» 642,
Quatermass, H, (1958) "Amblyopia due to ethyl elcohol". Brit.J, Ophthal., ^ , 6 # .
Hamsay, â.îî. (1895) "Tobacco Amblyopia" Lancet Lend., ^^1174 Head, I.B., Gough, E.R., Fardoe, J.L., and Hicholas, A.(l965).
2 4 6
"nutritional Studies on the lîhitrants to an Old Peoples Home* with particular reference to Polie acid Deficiency" Brit. Med. J,, 2fH3
Hehsteiiier* K. (l930) "Die era te anatoraisohe ïïntersuohung eines falles von gesohleohts gehimden hereditarer Sohnervenatraphie (Lehersohor KranMieit)". Orafea Arch, f* Ophth.* 125.14.
Beisner, B .E** and West, H., (1949) "Effect of Thymine Desossyrihoaide (9%y*idine) in human Pernicious Maaaia" Proc.Boc.Bbcper.Biol., 21^651
Heisenetein, P.O., Oronkite, E.P., and Oolm, B.IU (1961) "Measurement of absorption, of Vitamin B12 by whole body Gamma Spectromets^". Blood, 18.95.
Seynolds, B.É. (1968) "Mental effects of Anti-convuleants and Folic acid metahplism". Brain, 9I.197
Hidden, , (193&) "The early stages of Tobacco Amblyopia"Glas.Med.J., 125.268.
Ridley, P. (1959) "The Contact Lens in Investigation and Treatment". Trane. Ophthal. Boc* E.K., 79*535.
Rmme, H. (I910) "Pathoïogische^-anatoBiisoha üntersuoîiuïïgen uber Aleoholisehe Intoxikationsarablyople^' Arch.f.Ophthal*,
11,1.
247
losa, C.t., marris. P.m., a»d eiioH, K.K. (1554) "Effect of%amlêe polsoning on the oentrsl nervous systeia of rate and dogs". Pros, Boo* Biol* (M.Y.) 8%,6)2.
loss, (1952) "Fitevain B12 aasey In ho# fluids melmgIkiglmm gmollls"# J* CI3.iB* Path.,
llueta, f* (1925} "OtmsMeratlons mw le nlootlnlsmo,l*0iiîMyopie siieotlnique at Imr traitement". 011%. Optai.,
Baeha, (l#7) '*^tudlen zim Pathologie des iérvottaOptleus. I. Ammtemleehe kllmleeher heitrag m r kemmWlem dee Üeîîferaleeototifi bel Be BWmervenlelden!^. ârch. f# Augenh., %B*21
— f CIC193) - Stmlien m r Pathologie dea %rvous Optleue.2* Welter aîiatoïlaelie kliniseher beitrag m m keimtnlas dee Clentral see tome bel Selmervemleldem'' . IhM *.g7»154.
Bmùlmhn^ J* (1082) "Ite Anatomie imd foaologie der , ratroMlWrem newltle (Amblyopia Oeatralla)". âreîï* f.Ophth** # . 1.1.
Baraim, 1.* IP abat, IL* Biais * B. (1966) "Aapeets aotuale ÛÛ la mmit^ optique de l^etbyllque". Ama. B'eoul.#
Battler, O.ll* (1925) "Ifeher die tosaehen der Smmkme der TaWsmAlkohoI Amhlyoplem nooh dem Eriege". Ilin. Ilonatahl* f.Augamh* * ^0^ 310 •
248
S a i i ï M l e r a , Ë W w i o h , ILâ*- (I9 § 0 ) *%op@rtles o f tte
%8%e#»ou%&mram reapom iblo îm miwmmi.mk o f GyamMe
to fhiooyam ta'". Amem fhaioli* %63##4 Bol-mm*. F* (%§20) "Wortoitgoii des Itokto- bel é m %oxl#oh#m
mmblyoptom"-* BoitoohM ft f i AugemlL* 43.75.
WiepmB* #*L* (1940 "lë tobéooo amblyopia a deftoim oy
àloeas#"?* Traw * 6 é .309
$ o M # , (190)') ‘ #)or ^oamoGhang gowloaer fomea der
wtm&ial&awa mouritiii mit ortoatteiigon do# gofaomyotw#
ièmMîmà ##éh.f * §§.1M .:
BoMevelWlo#,' E#$ Worle, 1.* Bëhula, B.K.# end lanaeiotto*Tim fifi?) *fho tnSkmum of ToWooo feoko m # llaotimo- m %loagmm&to % toW ilem ", Aroh. Pharmak. ■ .
Ë & 3##'@#%llllng# Ë .f* ClfS5) î*& tolB »io facto r o M iio s . I I . thé ■■
e ffë o t o f 'fas te io Juloo m #m w lœ fr exorotioa o f
raâioaottvi# after #e mml aimlmlotoatlm of iaâloéot##-
011:1# iw#, jg,a6a# -Wmllor* "1# CW30 Fwhlâoh# Ifiit. m tm t Tahatoegle So#3*7 '
%%oteê 1# Jolmetomo, ant, PlÉmme% (l#§9) Ghém.Bav*,, âo ic to o iiiâ to , ##@. f l f 00) toxlo am%ly#lme". Byatm
of lloeasé# of too %o. Boml# m d Ollvw# #1#B# - ^Mpplnoo# 00#* londm oaû Fhllodolphlo# \
249
— > (1922) Toxic Amblyopia with oases III* Tobacco alcohol amblyopia relation of intestinal stasis* Amer. J*Ophthal., 5,t38T
— > (1927) "Tobacco amblyopia" Lancet Lond*, Xt604 — > and Edsall, I. (1903) "Concerning a possible etiological
factor in tobacco alcohol amblyopia revealed by an analysis of the urine of cases of this character"..Amer# J. Med. Soi* 126,216
van Senus, A.H#C# (1965) "Leber*a disease in the Motherlands" Booum. ophthal. 17*1.
Sovitt, L.H* and Iloffbrand, A.V# (1969) "Berom Folate and Vitamin B12 levels in acute and chronic renal disease.Effect of Peritoneal Dialysis". Brit. Med. J.,
Shulman, H. (1967) "Psychiatric aspects of PerniciousAnaemiaÎ A prospective controlled investigation". Brit*Med. J., 1 ,266.
Sloan, L.L. (1939) "Instruments and Techniques for the Clinical Testing of Light Bense. III". A.M.A* Arch*'Ophth., 21,235.
Smith, A.B.M. (I96O) "Megaloblastic madness". Brit.Med* J*, 2,1840.
— ) (1961) "Retrobulbar neuritiss Addisonian Pernicious Anaemia". Lancet Lond., 1,1001*
250
— > ( 1962)"Veganiem: A clinical suwey with oheervationson vitamin B12 metabolism"# Brit.Med. J., %,1655.
> (1964) "Cyanide encephalopathy in man". Lancet Lond., 2,668. — ; and Duckett, S* (1965) "Cyanide, Vitamin B12, experimental
demyelination and Tobacco iimhlyopia". Brit.J. libcper. Path* 18.615.
— ; Duckett, 8., and Waters, A.H. (1963) "Heuropathologioal changes in ohx'onic cyanide Intoxication". Mature Lond. 200.179.and foulkes, H. (I966) "Cyanide excretion in the Eat"Nature Lond*, 209.919.
Smith, E.L. (1948) "Purification of Antl«*pemicious Anaemia Factors from Liver". Mature Lond., 161,636.
— > (1965) ‘Vitamin Big" Jrd Ed* Hethuen^a Monographs. Methuen & Co* Ltd., London*
— > (1968) "Trapped Vitamdn Big" Plant Foods, Hum.Mutr., 1^7 Smith, F.P.E* (1959) "Tobacco Amblyopia" Brit.Med* J#, g,,123* Smith, B.C. and Malcolm, H.L. (I930) "Brinary sulphur and
Thiocymiate excretion in Cyanide poisoning". J* Pharmacol. Exper. Therap*, 40*457*
Snell, B. (1967) Personal Communication*Snellen, H. (l86g) "Optotypi ad visum determinandum"* ïïtreoht,
Holland.Sorbo, B.H* (195I) "On the properties of Hhodanese. Partial
251
purification# Inhibitor# and Intraoellular âlstoibwtion". Âota# Ohem* Scand»,
Spray, G*E* and Witts, L.J# (195S) "Itaaulta of Three Veare experlenoe with miorobiologioal assay of vitamin 'B%2 in eemm"» ■ Brit. Med. J.$ %,895#
Stadtoan, B#R* Overath, P., Sggerer, H., and lynon, P. (i960) "The role of Biotin and Vitamin Big comm^m In Propionate Metabolism". Biochem. Biophye# Ban. Oommim. ^,1.
Stilling, (1685) "Beendo#leoohro*:mtiaohe fafelm f.d.timifimg d. farbonoinnoo". Kamael, Oersany.
itoa, E.F. (1957) ‘‘Btndlea on Tbiooymato in Bnivoaitetet I Bergm# Mediolnek, lokke lo.S*
Biirgeon«Oaue*ral., E.i.. (I964) Report on smoking end health.* B#.* Department of .Health, Education and Welfare Publia Health Service Fublioatioà Ho.llGJ*
Swendoeifl,.. Méîi* Ifvolboll# I#-, Bohiok, Cl., and Haleted, J.A* (1957) "The Vitamin B12 oontez&t of Human Liver tiosuo and ita nutritional signifioanoe";. Blood, 12,24*
Taylor, i.d# (1892) "Hereditary optic atrop#". Trane# ophthal.* Sdo*!I*E*, 11,146.
fay:ior, J*. mid Bolmee, Cl. (1913) "llervouo eymptome asaoaiated with optic atrophy of the familial type"* franc* ophthal. 800,, U.K. il, 116*
2 5 2
Thomas, J# (1949) "Thlocyama# ISxorotion" J. Pharmacol#
E%p@r#%ermp#, ##337*- Tqdd, G*F» (l#66} "Statiatloa of Smoking In the ¥nited
Eiagdom",# fobaoeo liesoaroh Gomoll ïimam^Qh paper lo,.I##h # # London# . ■
%Kyo %dloRl Oollege (1957 )* ' W w Vleloa Test"#Murakami Golor lleaearoh laboratory# Tokyo# Japan#
Tooîiey# Jif*# m û farter# lï#â* (.1961) ^Isolation of o@en%ymo B12 f m M Livar"*. J#, .Biol*.. Otem*-# .236#360#. ■ -
Traqimir# ll*lî# (1928) "lobaooo amblyopia" Lancet fond## 2j|lIÎ3# — ; (1930) Amblyopia, including Retrobulbar lenrltia"#
franco, ophthal* SoûéîîèE*# # 331*. - *Turner# J*W#A# (194O) "Optic atrophy aaaoeiatcd with
Fen&ieion$ Anaemia"*, Brain#, 225 * >flithoff#., ¥# (10BO)*-. "Beitrag %mr B'ahnervenatrophic"* ■, Arch*
f#, Ophth# 1*244(1886) "fhteranchnngen uber dor Mnfinac é m cbronlsehen âlkoholisoms amf das menoohliohe Sehergan"# Arcb*f# ■ Ophth* ^ 9 5 *
— > (1901) "tesîiahmîgen ê.âllglmeinleiclea un Vorandemmgen d# Seborgenea 2.. l î i k o t i n v e r g e f , Graefe-Btmmlach. Itodb* g08 Angen#II#2,25.
2 5 3
— (1911} Ibia* 2nd m*ïlaglej# OëO*. (1949) "Oubacute combined degeneration of the
aord -*■ Recpmae to liver extraota #» friala with vitamin me", toaln 22,382#
Dhgiey# '0»{|# (1955) "The ohmotherapontlo action of Vitamin B12% VI tarn# andHorm#,
%her# 0*H# (1927a) "An analyeie of the omeomptloa oftobacco m d alcohol in aases of Tobacco amblyopia"# Aim ... %gonlo^# 243# . .
— p (1927b) "Two pedigrees. of. Hemdltery Optic Atrophy"#-■Init*J » Ophthal*, II#417*
van dm Hoeve (1927) "Tobacco amblyopia" Lancet J,t604 W m m m y f#. (I650) ¥ia.-Beota atl Titam Longm#^ Hoad.
London*Forrieatt 0* (1965) "Farther studiea on acquired âefioioney
of colour dloerimination"» J* %t# Soo# Amor##— 3 (1964) "Lea. defiolencea acquires da la iisorimination
Chromatique"* Mhmolree de 1* Académie loyale de Medocine- de :Wgl#e"* ,57#\ . .
Viator,, M. and Dreyfue, f*H* (1965) *' l©baoco’**Alcohol Amblyopia' â*|l*A*. Arch, ophth*, 21,649*
Véogtlin, Jolmoon, J##*, and %ar, ll*â* (1926) "Biological
% 4
significance of üystine and Glutathione**. J* Pharmacol# Exper* Therap#, 27#467.
Waardenhurg, P.J. (1923) "Beitrag uur Vererbung dor familiaren Eehnervanatrophie (Lebersehen Krankheit)*** Klin# Monats. f* Augoii., 73.619.
Walsh, FiB. (1957) "Glinlcal Meuro-^Ophthalmology** 2nd Bdition$ Williams & Wilkins, Baltimore, ÏÏ.S.A*
Walton, J.N., Kiloh, L.0. , Oeselton, J.W. and Farrall, J#(1954) "The electroencephalogram in Periilcioue Anaemia and Subaoute Oombinad Degeneration of the Cord**. 33.E+Q# olin# neurophysiol., ^»45*
Waters, A.H#, and Mollin, B.I». (196I) "Studies on the Folio acid activity of Human eenm". J. Glin* Path* 14,335.
— ; Morley, A.A*, and Rankin, J.G# (1966) "Effect of Alcohol on Haemopoiesis". Brit. Med. J., ^,1565*
1 /ebster, D. (1880) "Amblyopia from the abuse of Tobacco andAlcohol". Med. Heo., 18,649. (Ref. Ora#fB$8acnl80h m#2»30).
Weissbaoh, H., Ladd, îf.N., Tolcani, B.E., Smyth, H.B. and Barker, H.â. (i960). **Btruoture of the Adenyleobamine Goen%yme; Degradation by Cyanide, Acid and Light".J. Biol. Ghem., 235,:
255
— # Eedfield, B.G., and Peterkofaky» A* (I962) '’Biosynthesis of the B12 Coensyme* Requirements for release of Cyanide and Spectral changes". J. Biol* Ohem*, 237,3217# and Diokerman, H# (I964) "Effect of Vitamin B12 analogues on Methionine formation from B5-Methyl tetra hydrofolic acid". Ibid 239#146#
Wilson, J. (1963) "Leber*8 Hereditary Optic atropliy, some clinical and aetiological observations". Brain 86#347#
— > (1963a) "Leber* 8 Hereditary Optic Atrophy: A possibledefect of cyanide metabolism". Clin. Soi# .22*505#
— } (1965b) "Skeletal manifestations in Leber*s hereditary Optic Atrophy". Ann# Fhye. Med#, 8*91#
— and Longman, M#J*S# (1966) "Relation of Subaoute IJombined Degeneration of the Cord to Vitamin B12 Deficiency". Nature, Lond., 212«787.
.— I and Matthews, A#D#M# (1966) "Metabolic inter-relationship between cyanide, thiooyanate, and vitamin B12 in smokers and non-smokers. Clin, Soi#, ^1,1#
Vfilcon, T#M* (1969) "Quantitative Perimetry in the Assessment of Optic Nerve Conduction Defects". Trane. Ophthal* Sac. ÏÏ.K. (in press).
2 5 6
Wekee, f. (1958) "Tobacoo amblyopia" Wioet, Load., 2,#526 miû Vimæ ûf CI.M. (1955) "The m lù of fitomto B12 iu Summ nutrition" Amor. J. cliti. lutr., J,f383.
Wok©0, f. anâ Bllia, F.B. (1966) "Plaam Thiooyanate and Fit# 1112 in M m m lügtQ B l Bisoaao". lamoet Load#, J.,49*
Mokoa, P., Wodgowood, P., and %all# J# (1952) *^hiooyanato in mIM mà other biological flulda**# Bioehem* J.* jfXïJC#
Wood, J.Î**, -mû Cooley, S.L. (iggë) "Botoxioatioa of cyanide W oyotino". J. Bi-ol. #mm*, J|B,449*
WdMs^ortkf J.0. (1865) "Report of three oases of amaurosis produaed % tobnooo". totoet Load., .£,99
toigbwrhomeon* 1. "A olinloal study of tabaaeo hltuâtxmu with an iaveatigation- into its relation to oertaln aympteia other tlmn ooular". M.B. fhesis Glasgow Bniveraitÿ^ (1902)*
iMagiriam, M* and liTOra, â. (I965) "âloohol-fdbaoeo Optio. Neuropathy - ikmlysis of Oomplmetrio lafoate by the Btatlo Method". Ophthalmologioa 1^,185 •
297
APPsroiX A. DETAILS of PATIENTS.
2 5 8
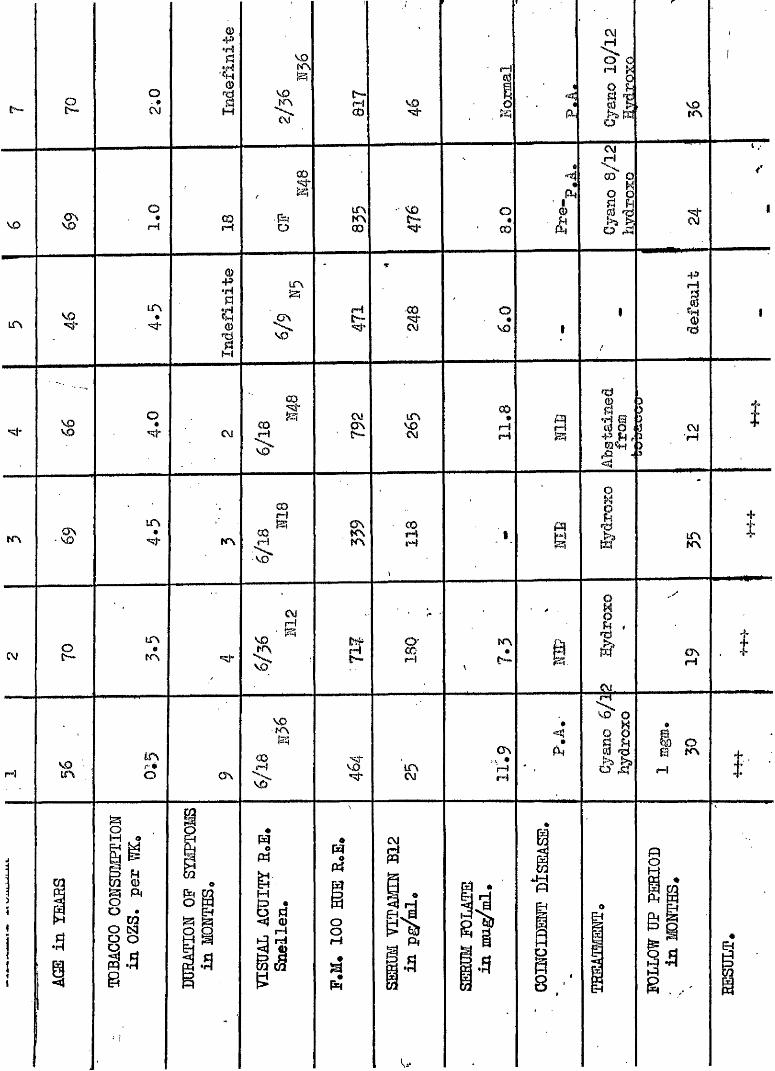
h - & O - •C\J
ü)
•H
S•ÎSIa
VD
KOtr\C\)
C ^i"—I 00
fH
P
a
voo
#rH
LfNLf\*
gq% P4
GOiH .Jj*)O
tnK>00 5 -
O
00
est
S o g s1*43
tr\
S r4q r•e^
coCM
O*KO
4»I1
O
s i-
§ •
CM § CM IT S« CO•rHfH
3 • S i■ ë ü
CM■|H
K \m
#
CM
LTS«
m
r™!KOm
i nr *O
S
K \00fH
8^K \
3iH
KO
§CMg
N »
î i gVOK \M
CT\ § '< î'
'ï§ *imCM
IK >
Irdr H
a\H *rH
i04kO
I
K \t
o\
mfH
g
«P4om
M
. 3 .3
§ grH
i l«
a
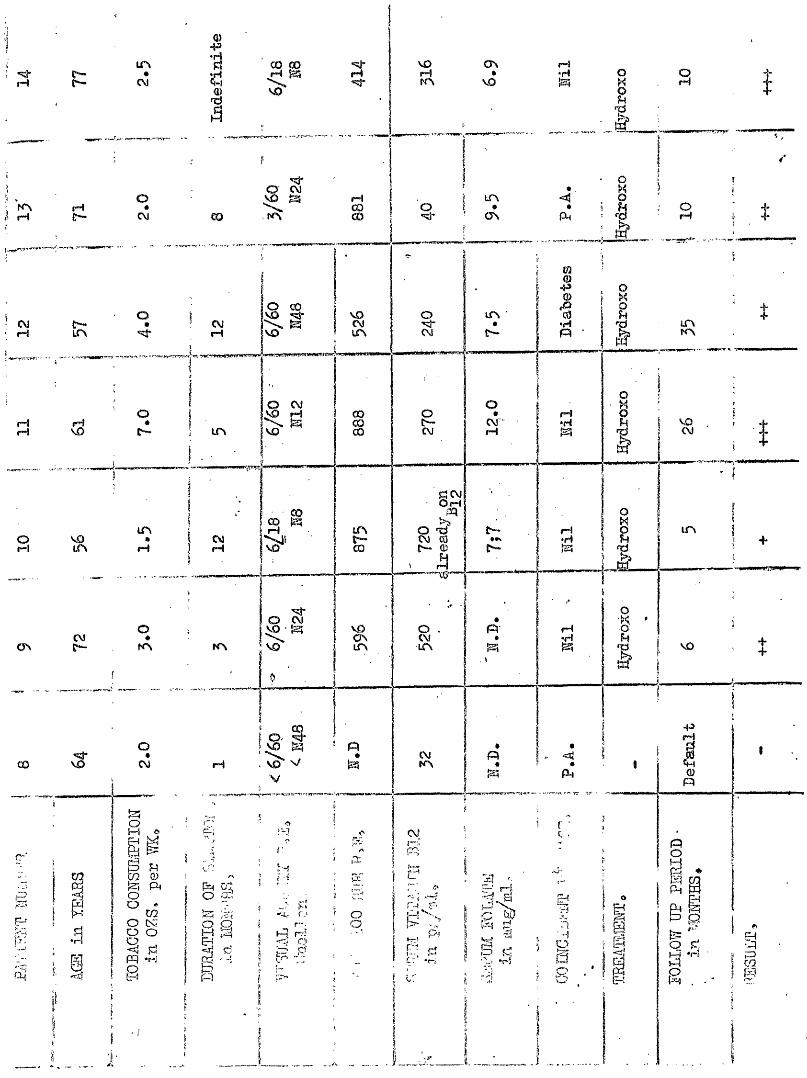
ON00 CO
NO iHCM
rH00rHCM
INOCMlf\ ur\K\CM
rHNOCM
rHrH
(D atnCM t—II—I
NOOSIT\
CMC KN LCN
CMfCNCM rHCO
O
pq yOO
S-So
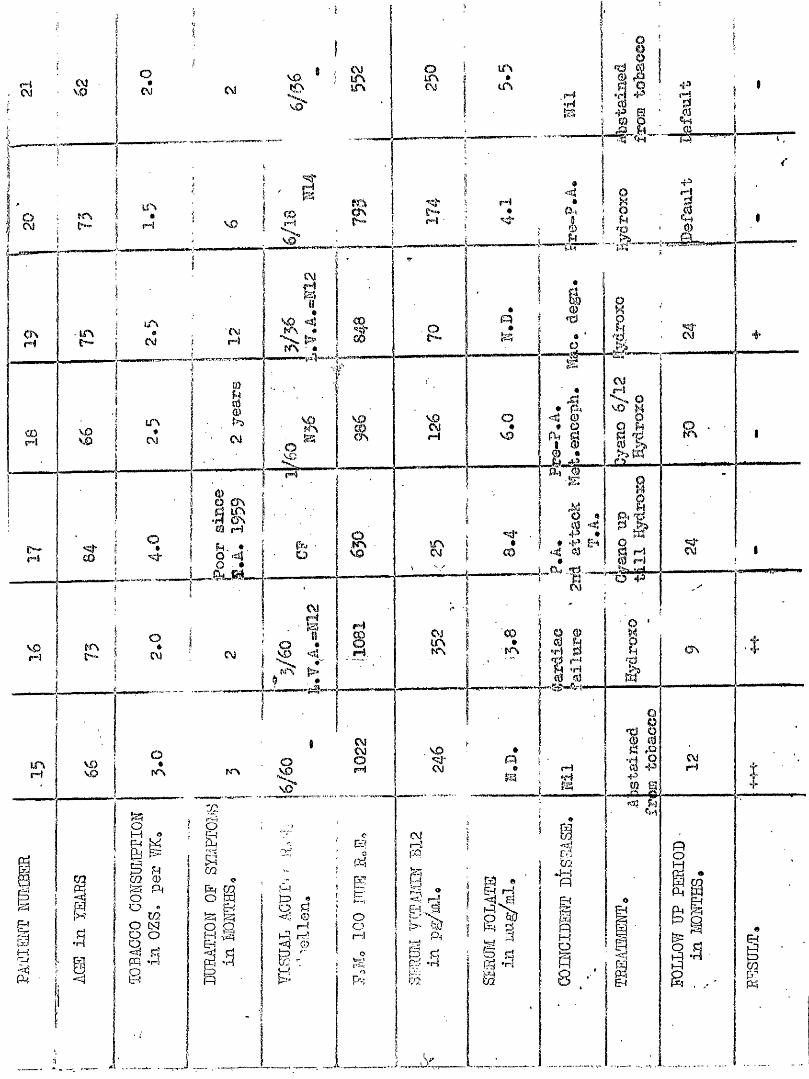
V.0VO
CM
# CM
V 0VO V 0CM
O ÜS £Q rH
in
j . , a -' R
ON
CM . \D CMVD
VO
—
§ s CM
iloow. oo
§I—rP
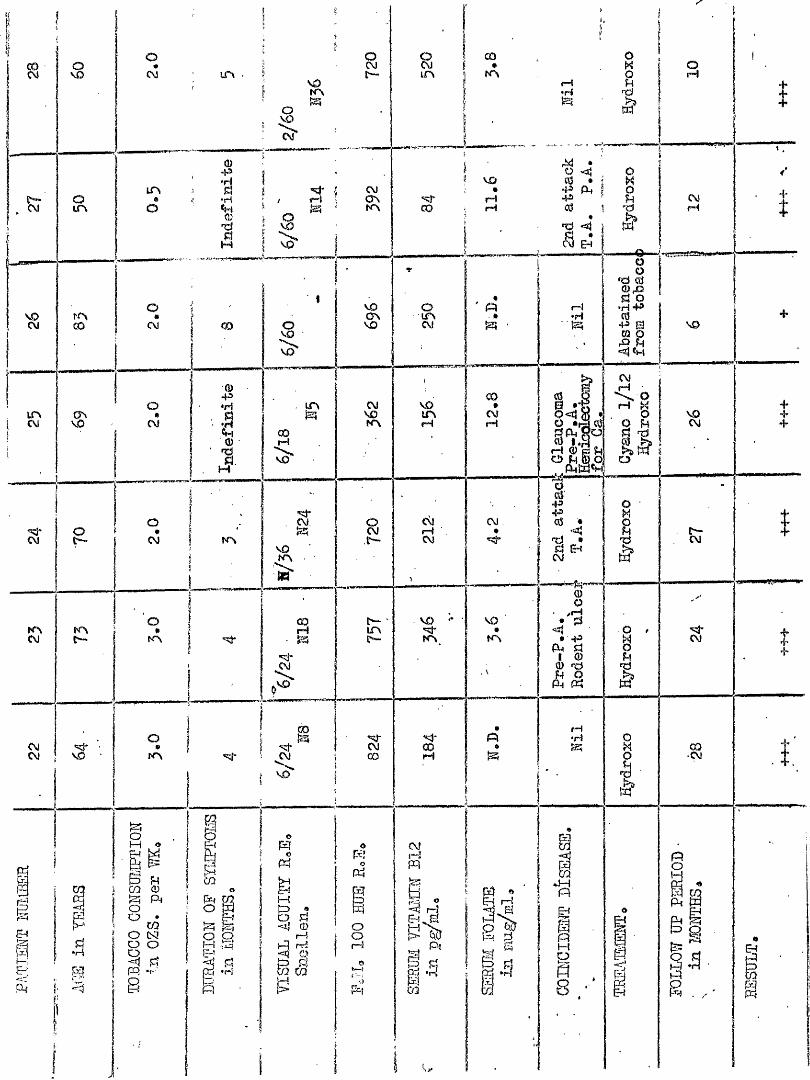
COCM
«»
O
CM IT%
QJP'HLCN PÎ0 < 'Ho *Mflj0M
CO
CM
KNCM
K \
i54(-:
Bd{
O
CM
O
CM
O
CM
O#
K \
eCO 0) Î2h P4 o^ CO O tS3s°fzq .r-' 8
GO
K \
OCM «îd* ■CM V O K N
O1— 1 *
R W
sE—
3CM
3 CM
MO
VO>»m3i.nr"»inr5
0)P*gLi COQ) rHd. VOtL__
3VOC3VVO
\Ù
sVO_KVÎW
8,sr—
I LTVi>“
,VD
VO
gCM00
8ir\
CD
VO•
(H(H
O
Sf« ■ #
COCM VO £ #VO IfN CMKN rH 1 rH
omo
1—Ît=y •Ü ^ -=îj CD
il
CM
VO#KN
o9 MKN O
rH•H ref
W
OiH
■o JΫ3 •
•P03
«ajPÎ • CM (M
I C\3fH t
rH•H
O O
•xi GjIIl iA
VO
L* ^0 csjS'v.ra Sis,
1
CM< orH ^Q Ait! 8 I!•I Rr $
Q)O
-4
ACDP4 O PM M§rH'f4!33
:4
* AI88
I CM
§ .8 t
EHCO
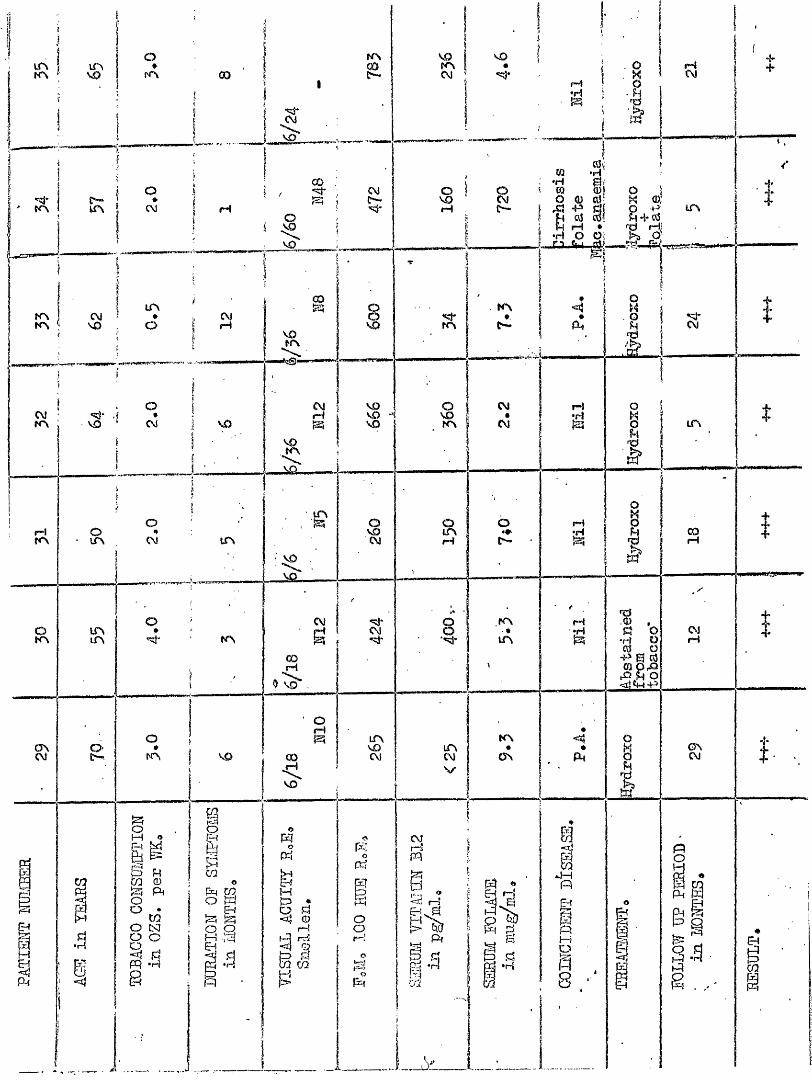
mKN NO OD
OJCM s+s^ H3
MNO
grHNO
r~*lrH
NOCMNO
COI—ICM
fc I II
CM KN rH•Hmm UN
COrH
rHKNUN
NOCMK CO
rH N /
O
gMO m
or-’ MOQCQ en
>:a
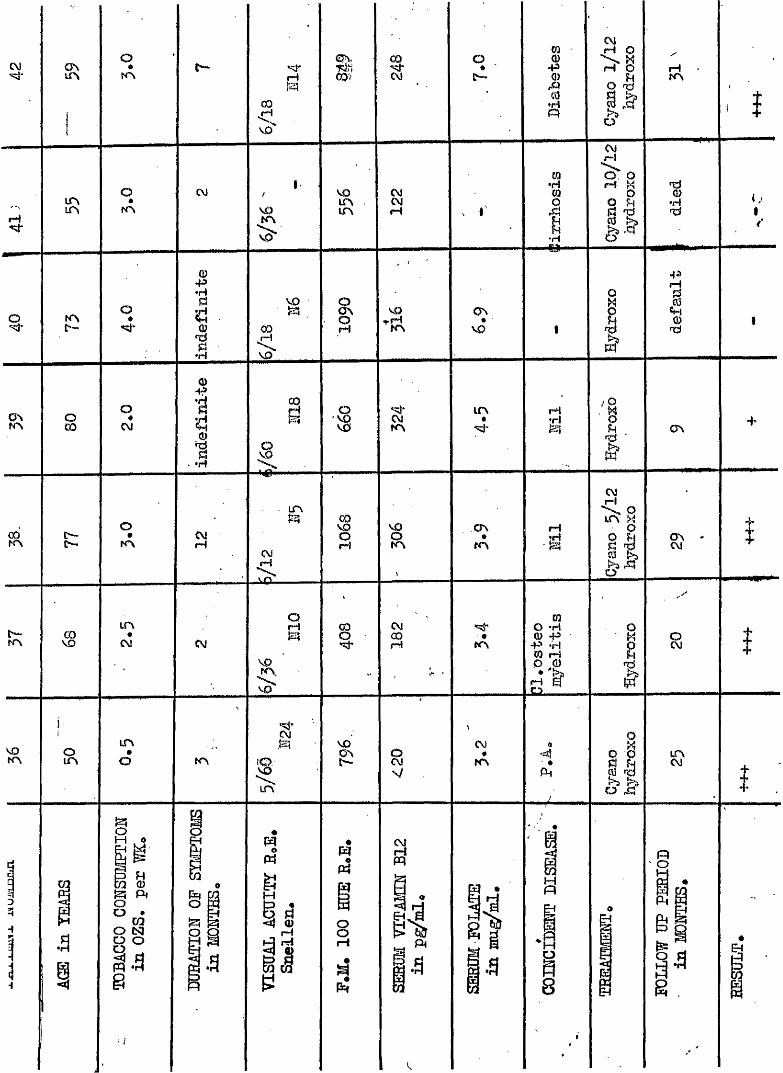
C\J o
COSI o# I
MCO
Q
H O> gO " §
&iHKN
IR
q•=5j* tC\
O
r r \
O*Kt
CVJK \
VO
VOmLPi %
M
CQ
t•H
Cvj( H
S 8o
o up) ndè S ’
0tj-jfXS
i*mQ)45:I §
as 'A ON#
VO I4 3IttS
§
fa c—
s
V D a
oCM
O *K \
L T \
CM
L T \*o
0 a i %r r \
l f \ r * l
'01s I O N
LTN
CMCMM
I ON*K N ■S
CMi H
^ O LfN yQ H|i a?
CMQc Hm I CM
' #
' i a .
V O
mo -H0 43 4» * Hra (H 11 I
g. t ^
KN
i r \
a 8V /
CM#
NNa
' *Ph il
o ^LTNCM
a a
om
i s
II «E4
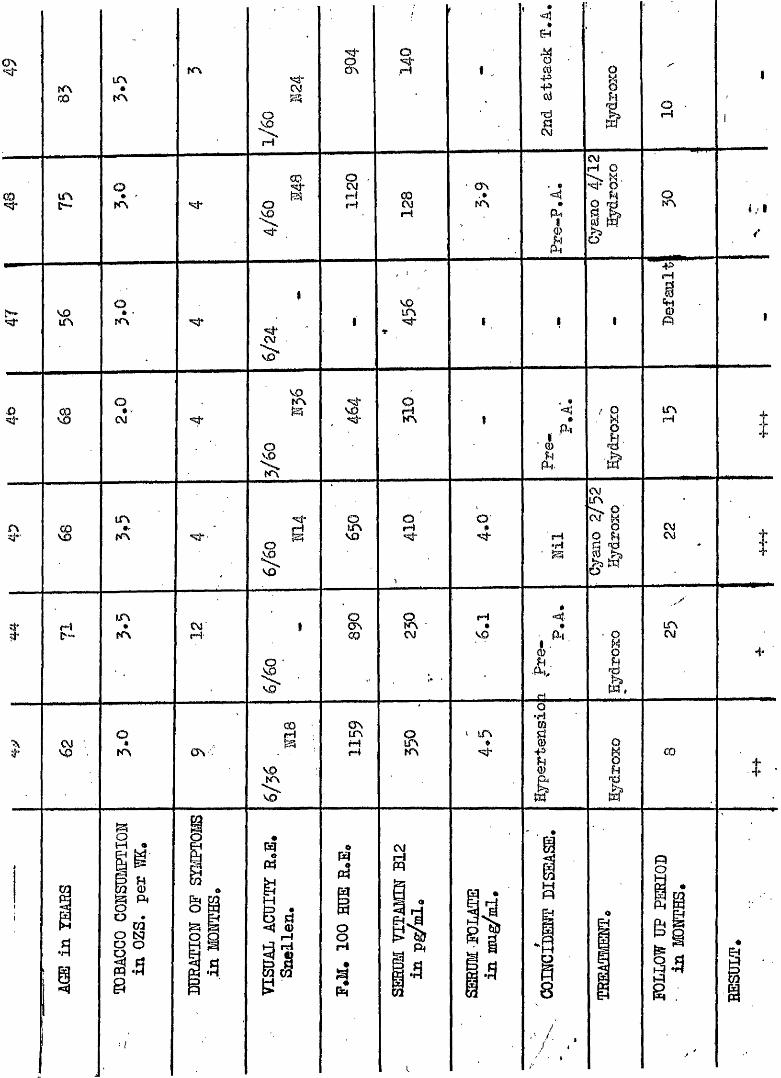
CO
m
VOm
O*KN
OKN
KN
s
s
VO
a
§M COOJH
VOLfN
ON . #KN
<!tr*
'SI
p.-tI o
or 4
a4&M
IO • ^cvj
aH I a
3KN
I
#Pi !UN(H
Fi
UNKN
UN*KN CMr4
aSVO
aVO orH<«j- M
iS
CVI
o(M X|i
ot (j\
CO
O •
VO
§ O nUN
fei ' rHr4
VO
\VO
aCM tHVO
IA
fAl IRl
'S)O«KN ON
arn ' UN «oa
Im I CO
I.,
i sg p.O NIP
O
.3
«P£|O
aII
mp5
Sg i
Pl,
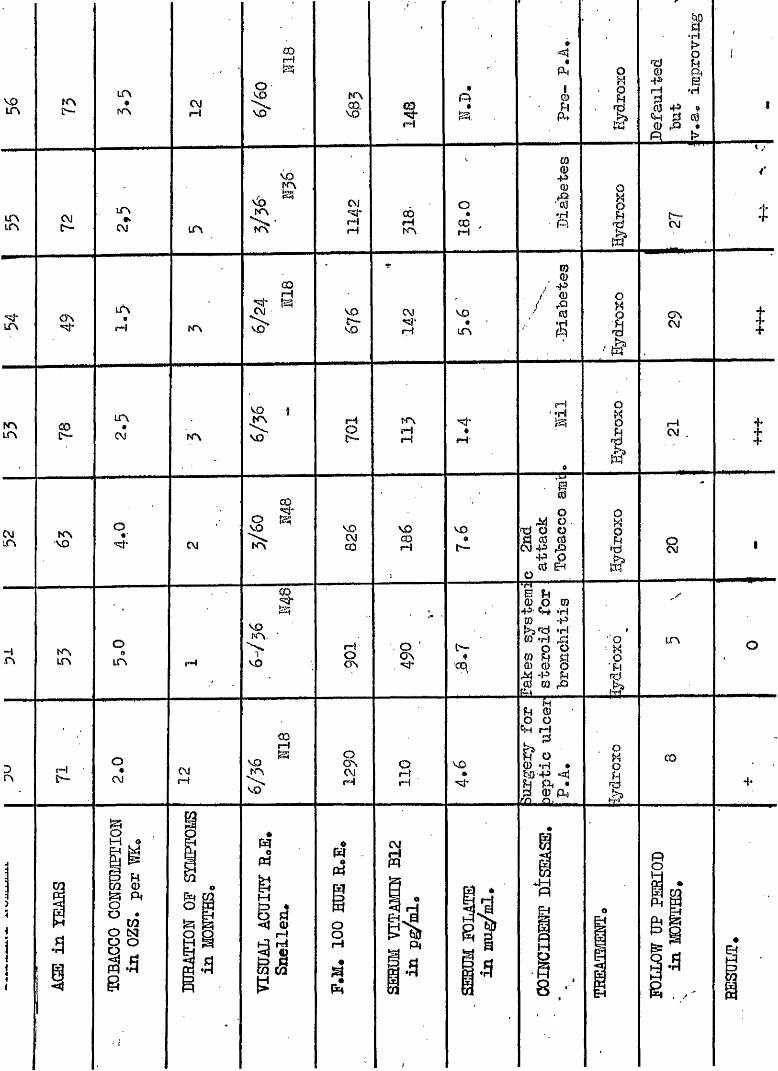
VOLT\
KN£>,
03r-4
UN*
NN CMpH VO
NN
a iHm
< î«Çk
è I
%0
*fHî>
rd0u
0 P 443 erH •H00 43 *
0 CÏÎm •
tR CMC-~
UNON
UN
CM
VOKN
UN KN
C\i*54-rHfH S
KN
O
COrH
03
I I CM
lArH KN
<0 . fH
VO
&CM<#'rH
VO
UN
•I1 4 3 / 0 / rO
0
g I ONCM
KNUN
a KNVO
KNUN
UN
CM K \
VO
s I^fNrH(H
O
CM
3KN UD
O
UN rH
VOKN.
>VO a
VOCO
I
rH
(HjH
VO
0
B000
^ P 0d 03 0c3 43 fO-P 00 fHÜ
I rHCM
I.h )
à
0-4-<x\
§ § m"S'*' Chf *Hp 43
’HCQ .*tHisg
0 *EQ ^ __I1
UN
fHO -
o#
CM
aCvJr4 a
VO§(H
srH
VO#
UH00 00
b " 00 •H •w 43 <Ej
Ck #Q) CL
UL,Mi.IM. CO
a a
gi si
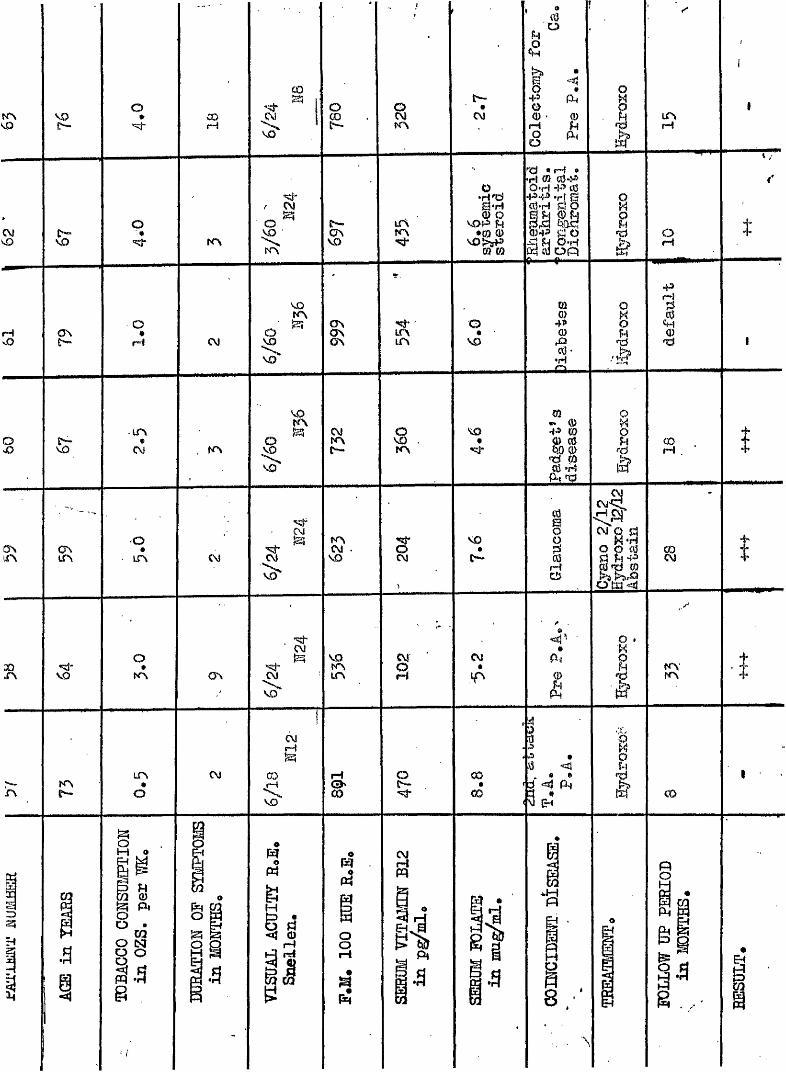
KNVO VO
£ > •
O» 00rHGO
V O
o a CM
£
Îo 0 '
rH
3
CÛo
#
#fXiI
§
i f f
U NM
CMvO & o
KN I AKN
goVOP N *0 0 vO>a 0 0
rd * rH * iH 0 0'PO 'H H'3 0 •PH-3 *rî B 0‘H glp043 0 o .q M O'Hodffl o p - — ^—
I orH tg A
O
rH CM 3VO
AU N
O *V O
0
30
■§• H
n a .
I43I
s &UNt
CM KN ss CM
K NC—
3KN
V O*ȍj*
V O
m ^ * • 0 43 0
JpSpui <tJ
AliN a oUN CM CM
A
3 I V O
C—
VO
IIo
#0*d 0 8
si*VO
O
A
CM
A CM
V OAA s
CM‘A PtI I A
A
CM
g
nA
Ae
O
CM CfJ
< 3 I CO
CO
. 3.\5
6d <# pH IIzf CO
Z )Si
Pi
H
. a
§ g
f a
APPENDIX Bo Publications;
1* Cyanocobalamin versus Hydroxooobalamin in the treatment of Tohaooo ihablyopia, Lancetj 196? 2)490#
2. Hydroxooohalarain in the treatment of Leber*e hereditary optic atropî^, Lancet 1968, 1, 696*
3* Serum Thlocyanate Concentrations in Tobacco Amblyopia, Nature, 1968, 216* 386.
4# Response of Metabolic encephalopathy to treatment with Gyanooobalamin, Scot. Med.J*, 1968, 22,274
9« Vitamin B12 absorption in Tobacco Amblyopia, Brit* J. Ophthal., 21)393
269
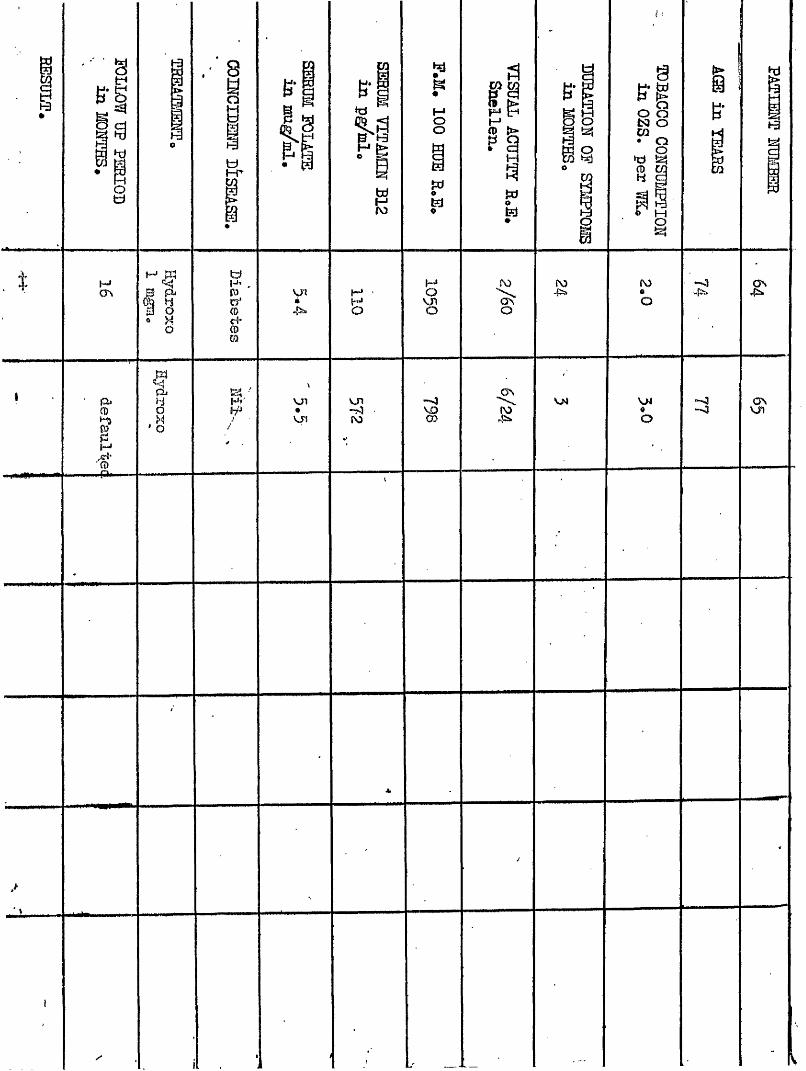
H3;
§
01&
;ëo
p
s
pp I Nwow
9 w
“ 8*d M8 B îd
‘ §
HJON
p»
I'ffl'
- fk .
M M tdt -^ ,
B pü 0% H etm Q ®Q X c4
o (Dm
}
VJ1é I—'O
Oo
HfM ' VJ1#vjn
VJ1
ro- 4œ
ro
o
A
P O-p5>
VJH
PO»O
VK«o
"-Owjïs»
Related Documents






![Welcome to Enlighten: Theses - Enlighten: Thesestheses.gla.ac.uk/71878/1/10394171.pdf · 2019. 5. 10. · [Chronicle of the EOKA struggle 1955-1959] (Athens: [n. pub.], 1971); Georgios](https://static.cupdf.com/doc/110x72/612d4a4a1ecc5158694218df/welcome-to-enlighten-theses-enlighten-2019-5-10-chronicle-of-the-eoka.jpg)




