



Vancomycin plus Piperacillin/Tazobactam….Bad
for the Beans?
Emmanuel U. Aniemeke, Pharm.D. PGY1 Pharmacy Resident
University Health System, San Antonio, Texas Division of Pharmacotherapy, The University of Texas Health Science College of Pharmacy
Pharmacotherapy Education and Research Center The University of Texas Health Science Center San Antonio
Pharmacotherapy Rounds February 27th, 2015
LEARNING OBJECTIVES
1. Describe the pathophysiology, clinical presentation, and causes of acute kidney injury
2. Summarize the proposed mechanism of acute kidney injury associated with vancomycin and
piperacillin/tazobactam
3. Evaluate the current literature regarding the risk of acute kidney injury while on combination vancomycin and
piperacillin/tazobactam therapy
4. Provide practical recommendations regarding the combined use of vancomycin and piperacillin/tazobactam
based on recently published literature
Aniemeke 2
ACUTE KIDNEY INJURY (AKI)
I. BACKGROUND 1, 2, 3
A. Sudden (hours to days) decline in excretory function of the kidney
B. Characterized by
i. Dysregulation of fluids, electrolytes and acid-base balance
ii. Decreased glomerular filtration rate (GFR)
iii. Increase in serum creatinine (Scr)
II. EPIDEMIOLOGY/INCIDENCE 1, 2, 4
A. Associated with significantly high mortality and morbidity rates
B. Incidence
i. Community-acquired : <1%
ii. Hospital-acquired: ~9%
iii. ICU-acquired: 30-67%
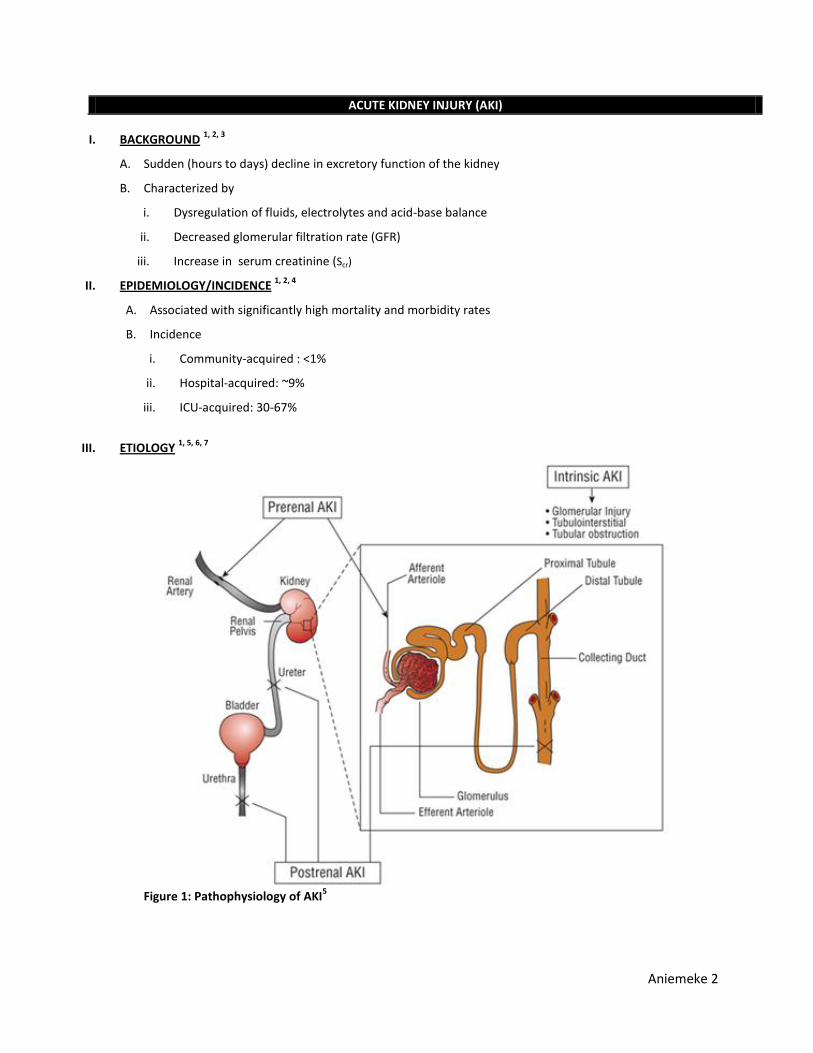
III. ETIOLOGY
1, 5, 6, 7
Figure 1: Pathophysiology of AKI
5
Aniemeke 3
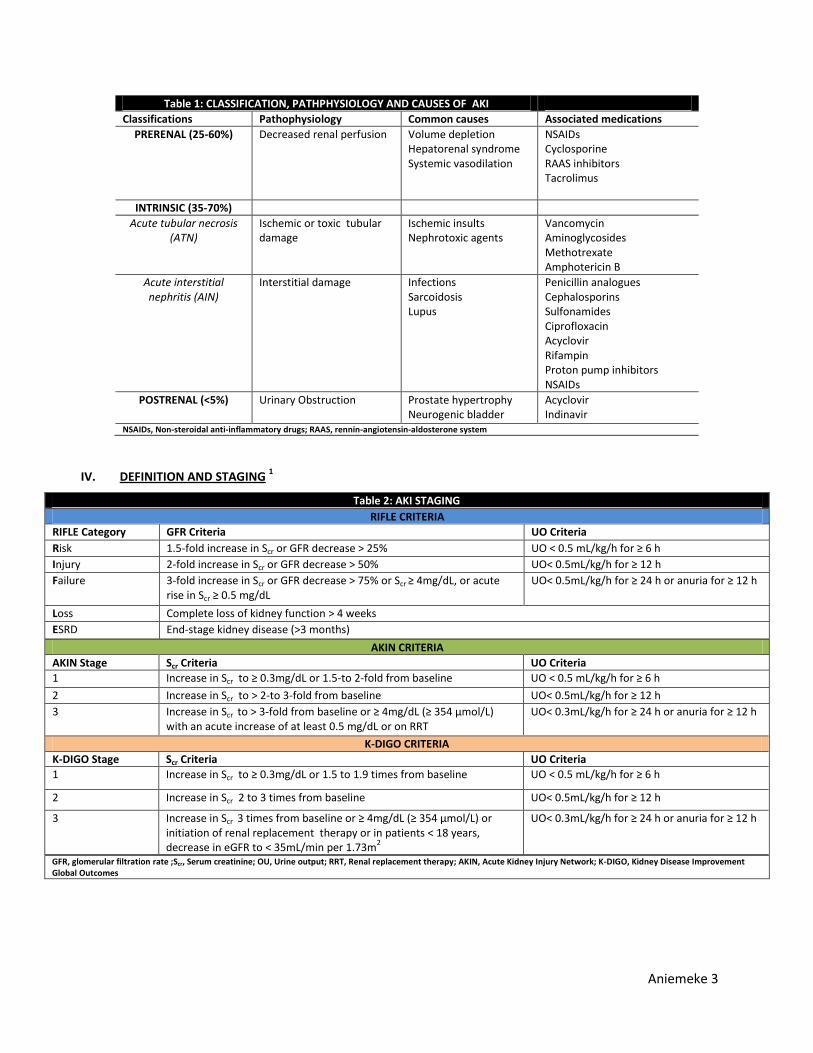
Table 1: CLASSIFICATION, PATHPHYSIOLOGY AND CAUSES OF AKI
Classifications Pathophysiology Common causes Associated medications
PRERENAL (25-60%) Decreased renal perfusion Volume depletion Hepatorenal syndrome Systemic vasodilation
NSAIDs Cyclosporine RAAS inhibitors Tacrolimus
INTRINSIC (35-70%)
Acute tubular necrosis (ATN)
Ischemic or toxic tubular damage
Ischemic insults Nephrotoxic agents
Vancomycin Aminoglycosides Methotrexate Amphotericin B
Acute interstitial nephritis (AIN)
Interstitial damage Infections Sarcoidosis Lupus
Penicillin analogues Cephalosporins Sulfonamides Ciprofloxacin Acyclovir Rifampin Proton pump inhibitors NSAIDs
POSTRENAL (<5%) Urinary Obstruction Prostate hypertrophy Neurogenic bladder
Acyclovir Indinavir
NSAIDs, Non-steroidal anti-inflammatory drugs; RAAS, rennin-angiotensin-aldosterone system
IV. DEFINITION AND STAGING 1
Table 2: AKI STAGING
RIFLE CRITERIA
RIFLE Category GFR Criteria UO Criteria
Risk 1.5-fold increase in Scr or GFR decrease > 25% UO < 0.5 mL/kg/h for ≥ 6 h
Injury 2-fold increase in Scr or GFR decrease > 50% UO< 0.5mL/kg/h for ≥ 12 h
Failure 3-fold increase in Scr or GFR decrease > 75% or Scr ≥ 4mg/dL, or acute rise in Scr ≥ 0.5 mg/dL
UO< 0.5mL/kg/h for ≥ 24 h or anuria for ≥ 12 h
Loss Complete loss of kidney function > 4 weeks
ESRD End-stage kidney disease (>3 months)
AKIN CRITERIA
AKIN Stage Scr Criteria UO Criteria
1 Increase in Scr to ≥ 0.3mg/dL or 1.5-to 2-fold from baseline UO < 0.5 mL/kg/h for ≥ 6 h
2 Increase in Scr to > 2-to 3-fold from baseline UO< 0.5mL/kg/h for ≥ 12 h
3 Increase in Scr to > 3-fold from baseline or ≥ 4mg/dL (≥ 354 μmol/L) with an acute increase of at least 0.5 mg/dL or on RRT
UO< 0.3mL/kg/h for ≥ 24 h or anuria for ≥ 12 h
K-DIGO CRITERIA
K-DIGO Stage Scr Criteria UO Criteria
1 Increase in Scr to ≥ 0.3mg/dL or 1.5 to 1.9 times from baseline UO < 0.5 mL/kg/h for ≥ 6 h
2 Increase in Scr 2 to 3 times from baseline UO< 0.5mL/kg/h for ≥ 12 h
3 Increase in Scr 3 times from baseline or ≥ 4mg/dL (≥ 354 μmol/L) or initiation of renal replacement therapy or in patients < 18 years, decrease in eGFR to < 35mL/min per 1.73m
2
UO< 0.3mL/kg/h for ≥ 24 h or anuria for ≥ 12 h
GFR, glomerular filtration rate ;Scr, Serum creatinine; OU, Urine output; RRT, Renal replacement therapy; AKIN, Acute Kidney Injury Network; K-DIGO, Kidney Disease Improvement Global Outcomes
Aniemeke 4
VANCOMYCIN ASSOCIATED NEPHROTOXICITY (VAN)
I. BACKGROUND 8, 9, 10
A. Vancomycin
i. Glycopeptide antibiotic
ii. Early formulation of vancomycin contained significant impurities, nicknamed “Mississippi mud”
iii. Subsequent formulations increased the purity, reducing the severities of toxicity
iv. Cornerstone antibiotic for management of severe gram-positive infections
1. Methicillin-resistant Staphylococcus aureus (MRSA)
2. Methicillin-resistant coagulase-negative staphylococci
3. Non-vancomycin-resistant entercocci
B. Primary renal excretion
i. Glomerular filtration and active tubular secretion (90%)
ii. Hepatic conjugation (~10%)
II. MECHANISM OF ACTION 8
A. Inhibits cell wall synthesis of gram-positive bacteria
B. Inhibition of peptidoglycan elongation and cross-linking
C. Slowly bactericidal
V. ADVERSE EFFECTS 8, 11, 12
A. Nephrotoxicity (5-43%)
B. Infusion reactions: “Redman syndrome”
C. Drug fever
D. IgA bollous dermatosis
VI. POSTULATED MECHANISM OF VAN 9, 13, 14, 15, 16, 17
A. Drug-induced oxidative stress
B. Mitochondrial damage in the proximal renal tubular cell
C. Proximal renal tubular cell necrosis
D. Contribution to complement pathway and inflammation
E. Believed to be mostly reversible
Aniemeke 5
VII. INCIDENCE OF VAN 9, 13, 14,15, 16, 17
A. Incidence ranges from 5 - 43 %
B. Associated with
i. Prolonged hospitalization
ii. Increased mortality
iii. Need for renal replacement therapy
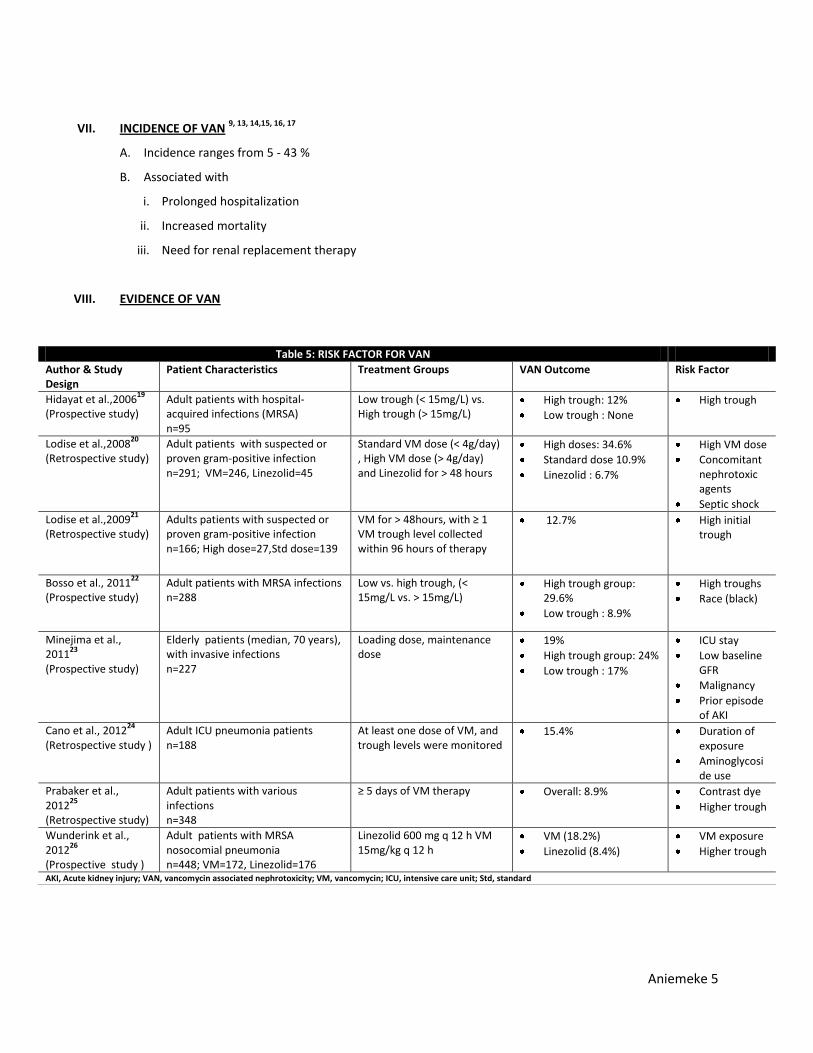
VIII. EVIDENCE OF VAN
Table 5: RISK FACTOR FOR VAN
Author & Study Design
Patient Characteristics Treatment Groups VAN Outcome Risk Factor
Hidayat et al.,200619
(Prospective study) Adult patients with hospital-acquired infections (MRSA) n=95
Low trough (< 15mg/L) vs. High trough (> 15mg/L)
High trough: 12%
Low trough : None
High trough
Lodise et al.,200820
(Retrospective study)
Adult patients with suspected or proven gram-positive infection n=291; VM=246, Linezolid=45
Standard VM dose (< 4g/day) , High VM dose (> 4g/day) and Linezolid for > 48 hours
High doses: 34.6%
Standard dose 10.9%
Linezolid : 6.7%
High VM dose
Concomitant nephrotoxic agents
Septic shock
Lodise et al.,200921
(Retrospective study)
Adults patients with suspected or proven gram-positive infection n=166; High dose=27,Std dose=139
VM for > 48hours, with ≥ 1 VM trough level collected within 96 hours of therapy
12.7% High initial trough
Bosso et al., 201122
(Prospective study)
Adult patients with MRSA infections n=288
Low vs. high trough, (< 15mg/L vs. > 15mg/L)
High trough group: 29.6%
Low trough : 8.9%
High troughs
Race (black)
Minejima et al., 2011
23
(Prospective study)
Elderly patients (median, 70 years), with invasive infections n=227
Loading dose, maintenance dose
19%
High trough group: 24%
Low trough : 17%
ICU stay
Low baseline GFR
Malignancy
Prior episode of AKI
Cano et al., 201224
(Retrospective study )
Adult ICU pneumonia patients n=188
At least one dose of VM, and trough levels were monitored
15.4% Duration of exposure
Aminoglycoside use
Prabaker et al., 2012
25
(Retrospective study)
Adult patients with various infections n=348
≥ 5 days of VM therapy Overall: 8.9% Contrast dye
Higher trough
Wunderink et al., 2012
26
(Prospective study )
Adult patients with MRSA nosocomial pneumonia n=448; VM=172, Linezolid=176
Linezolid 600 mg q 12 h VM 15mg/kg q 12 h
VM (18.2%)
Linezolid (8.4%)
VM exposure
Higher trough
AKI, Acute kidney injury; VAN, vancomycin associated nephrotoxicity; VM, vancomycin; ICU, intensive care unit; Std, standard
Aniemeke 6
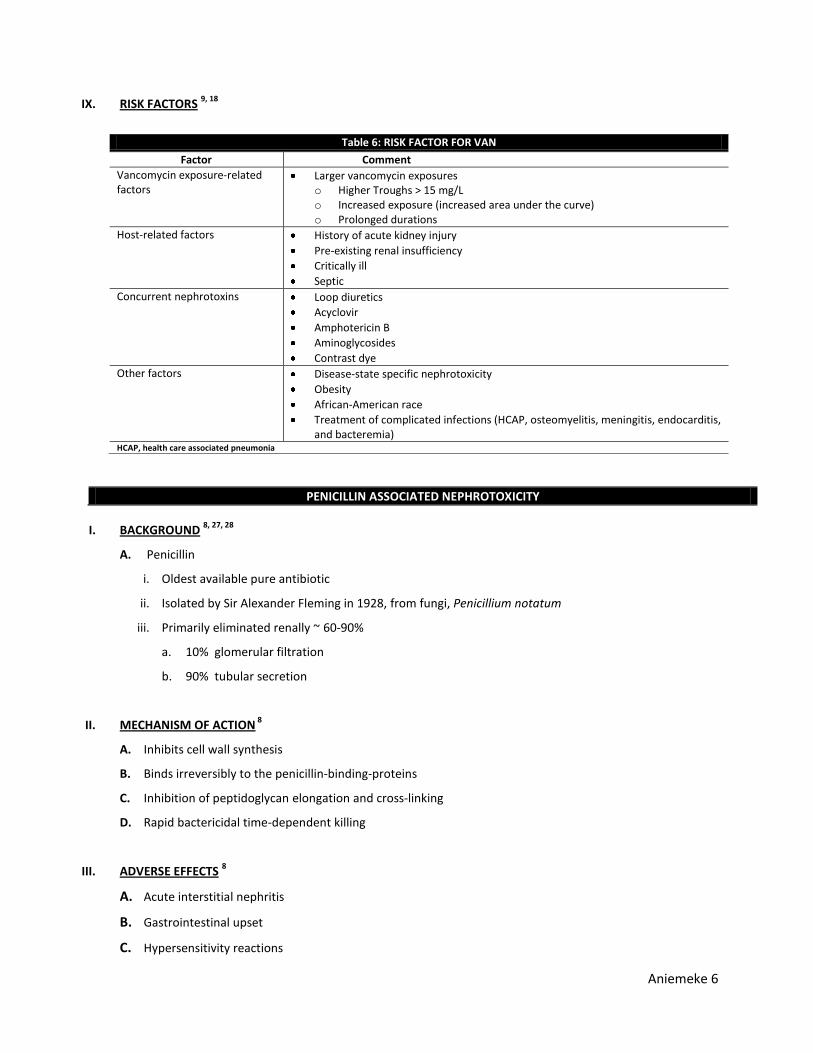
IX. RISK FACTORS 9, 18
PENICILLIN ASSOCIATED NEPHROTOXICITY
I. BACKGROUND
8, 27, 28
A. Penicillin
i. Oldest available pure antibiotic
ii. Isolated by Sir Alexander Fleming in 1928, from fungi, Penicillium notatum
iii. Primarily eliminated renally ~ 60-90%
a. 10% glomerular filtration
b. 90% tubular secretion
II. MECHANISM OF ACTION 8
A. Inhibits cell wall synthesis
B. Binds irreversibly to the penicillin-binding-proteins
C. Inhibition of peptidoglycan elongation and cross-linking
D. Rapid bactericidal time-dependent killing
III. ADVERSE EFFECTS 8
A. Acute interstitial nephritis
B. Gastrointestinal upset
C. Hypersensitivity reactions
Table 6: RISK FACTOR FOR VAN
Factor Comment
Vancomycin exposure-related factors
Larger vancomycin exposures o Higher Troughs > 15 mg/L o Increased exposure (increased area under the curve) o Prolonged durations
Host-related factors History of acute kidney injury
Pre-existing renal insufficiency
Critically ill
Septic
Concurrent nephrotoxins Loop diuretics
Acyclovir
Amphotericin B
Aminoglycosides
Contrast dye
Other factors Disease-state specific nephrotoxicity
Obesity
African-American race
Treatment of complicated infections (HCAP, osteomyelitis, meningitis, endocarditis, and bacteremia)
HCAP, health care associated pneumonia
Aniemeke 7
IV. POSTULATED MECHANISM OF NEPHROTOXICITY 29, 30, 31, 32
A. Dimethoxyphenylpenicilloyl (DPO) binding to host renal structural protein
B. Formation an antigen-protein complex (hapten) along the tubular basement membrane
C. Mounting an immunogenic response developing into interstitial nephritis
V. PIPERACILLIN-TAZOBACTAM (PT) 33, 34, 35
A. Extended-spectrum semisynthetic penicillin combined with β-lactamase inhibitor
B. Approved by the FDA in 1993
C. Composed at an 8:1 ratio of piperacillin and tazobactam
D. FDA Indications
i. Nosocomial pneumonia
ii. Intra-abdominal infections
iii. Skin and soft tissue infections
iv. Pelvic inflammatory disease
v. Septicemia
vi. Neutropenic fever
vii. Osteomyelitis
viii. Septic arthritis
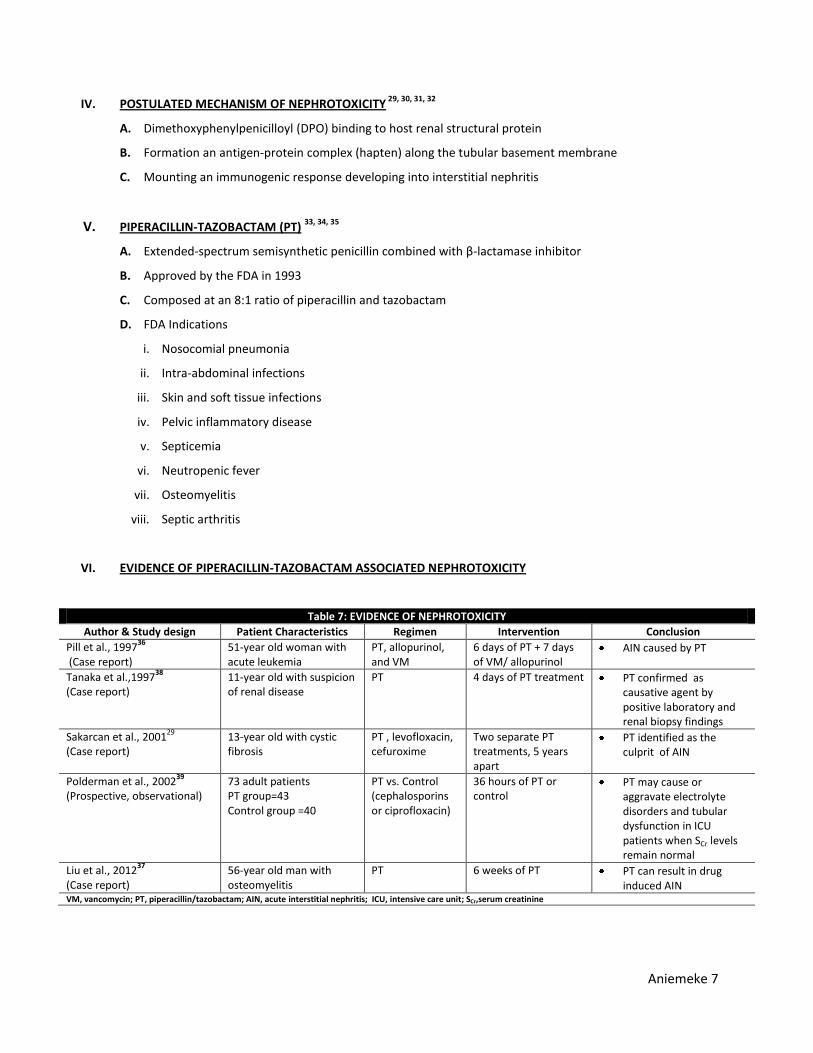
VI. EVIDENCE OF PIPERACILLIN-TAZOBACTAM ASSOCIATED NEPHROTOXICITY
Table 7: EVIDENCE OF NEPHROTOXICITY
Author & Study design Patient Characteristics Regimen Intervention Conclusion
Pill et al., 199736
(Case report) 51-year old woman with acute leukemia
PT, allopurinol, and VM
6 days of PT + 7 days of VM/ allopurinol
AIN caused by PT
Tanaka et al.,199738
(Case report)
11-year old with suspicion of renal disease
PT 4 days of PT treatment PT confirmed as causative agent by positive laboratory and renal biopsy findings
Sakarcan et al., 200129
(Case report)
13-year old with cystic fibrosis
PT , levofloxacin, cefuroxime
Two separate PT treatments, 5 years apart
PT identified as the culprit of AIN
Polderman et al., 200239
(Prospective, observational)
73 adult patients PT group=43 Control group =40
PT vs. Control (cephalosporins or ciprofloxacin)
36 hours of PT or control
PT may cause or aggravate electrolyte disorders and tubular dysfunction in ICU patients when SCr levels remain normal
Liu et al., 201237
(Case report)
56-year old man with osteomyelitis
PT 6 weeks of PT PT can result in drug induced AIN
VM, vancomycin; PT, piperacillin/tazobactam; AIN, acute interstitial nephritis; ICU, intensive care unit; SCr,serum creatinine
Aniemeke 8
VANCOMYCIN PLUS PIPERACILLIN/TAZOBACTAM ASSOCIATED NEPHROTOXICITY
I. CLINICAL QUESTION
A. Does the combination therapy of vancomycin and piperacillin/tazobactam (VPT) increase the risk
incidence of nephrotoxicity?
II. ABSTRACT EVALUATION
A. Hellwig et al. 40
i. Retrospective evaluation of 735 adult patients over a 6 month period
ii. Compared patients who received VM alone versus PT alone versus combination therapy of VPT for
more than 48 hours
iii. AKI defined as increase of serum creatinine greater than 0.5 mg/dL or a 50% increase from
baseline
iv. Result
B. Min et al. 41
i. Evaluation of 140 surgical ICU patients over one year
ii. Compared patients on the combination therapy of VPT versus monotherapy of VM alone for at
least 48 hours
iii. AKI defined as increase of serum creatinine more than 1.5 times baseline during antibiotic therapy
iv. Result
Incidence of AKI
VPT group (40.5%)
VM group (9.0%)
p<0.001
III. LITERATURE REVIEW
A. Meaney et al. Pharmacotherapy 2014
B. Burgess et al. Pharmacotherapy 2014
C. Moenseter et al. Clin Micro Biol Infect 2014
D. Gomes et al. Pharmacotherapy 2014
Table 8: INCIDENCE OF AKI
Patient population VM (%) PT (%) VPT (%) p value
General medicine 4.9 11.1 18.6 0.005
ICU 6.0 12.2 21.2 0.279 VM, vancomycin; PT, piperacillin/tazobactam; VPT, vancomycin and piperacillin/tazobactam
Aniemeke 9
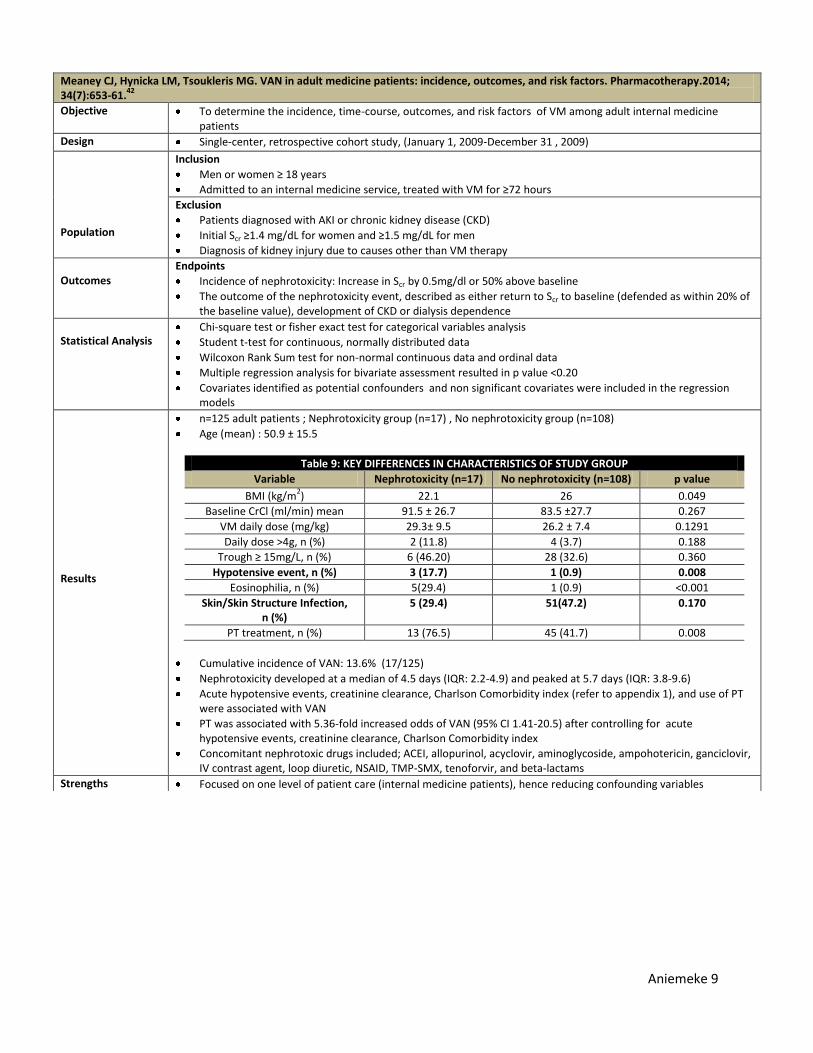
Meaney CJ, Hynicka LM, Tsoukleris MG. VAN in adult medicine patients: incidence, outcomes, and risk factors. Pharmacotherapy.2014; 34(7):653-61.
42
Objective To determine the incidence, time-course, outcomes, and risk factors of VM among adult internal medicine patients
Design Single-center, retrospective cohort study, (January 1, 2009-December 31 , 2009)
Population
Inclusion
Men or women ≥ 18 years
Admitted to an internal medicine service, treated with VM for ≥72 hours
Exclusion
Patients diagnosed with AKI or chronic kidney disease (CKD)
Initial Scr ≥1.4 mg/dL for women and ≥1.5 mg/dL for men
Diagnosis of kidney injury due to causes other than VM therapy
Outcomes
Endpoints
Incidence of nephrotoxicity: Increase in Scr by 0.5mg/dl or 50% above baseline
The outcome of the nephrotoxicity event, described as either return to Scr to baseline (defended as within 20% of the baseline value), development of CKD or dialysis dependence
Statistical Analysis
Chi-square test or fisher exact test for categorical variables analysis
Student t-test for continuous, normally distributed data
Wilcoxon Rank Sum test for non-normal continuous data and ordinal data
Multiple regression analysis for bivariate assessment resulted in p value <0.20
Covariates identified as potential confounders and non significant covariates were included in the regression models
Results
n=125 adult patients ; Nephrotoxicity group (n=17) , No nephrotoxicity group (n=108)
Age (mean) : 50.9 ± 15.5
Table 9: KEY DIFFERENCES IN CHARACTERISTICS OF STUDY GROUP
Variable Nephrotoxicity (n=17) No nephrotoxicity (n=108) p value
BMI (kg/m2) 22.1 26 0.049
Baseline CrCl (ml/min) mean 91.5 ± 26.7 83.5 ±27.7 0.267
VM daily dose (mg/kg) 29.3± 9.5 26.2 ± 7.4 0.1291
Daily dose >4g, n (%) 2 (11.8) 4 (3.7) 0.188
Trough ≥ 15mg/L, n (%) 6 (46.20) 28 (32.6) 0.360
Hypotensive event, n (%) 3 (17.7) 1 (0.9) 0.008
Eosinophilia, n (%) 5(29.4) 1 (0.9) <0.001
Skin/Skin Structure Infection, n (%)
5 (29.4) 51(47.2) 0.170
PT treatment, n (%) 13 (76.5) 45 (41.7) 0.008
Cumulative incidence of VAN: 13.6% (17/125)
Nephrotoxicity developed at a median of 4.5 days (IQR: 2.2-4.9) and peaked at 5.7 days (IQR: 3.8-9.6)
Acute hypotensive events, creatinine clearance, Charlson Comorbidity index (refer to appendix 1), and use of PT were associated with VAN
PT was associated with 5.36-fold increased odds of VAN (95% CI 1.41-20.5) after controlling for acute hypotensive events, creatinine clearance, Charlson Comorbidity index
Concomitant nephrotoxic drugs included; ACEI, allopurinol, acyclovir, aminoglycoside, ampohotericin, ganciclovir, IV contrast agent, loop diuretic, NSAID, TMP-SMX, tenoforvir, and beta-lactams
Strengths Focused on one level of patient care (internal medicine patients), hence reducing confounding variables
Aniemeke 10
Limitations Retrospective, unblinded
Small sample size within the nephrotoxic group, hence limited data on significant differences in occurrence of the risk factors between groups
Large type II error on variable analysis
Stability of Scr was not assessed before the patient were entered into the study
Wide confidence intervals, low precision
Exclusion of treatment related variables, such as dose, trough concentrations, patient weight ≥ 101.4kg or 2 or more concomitant nephrotoxic agents in the regression model
Authors Conclusion Use of concomitant piperacillin-tazobactam is significantly associated with development of nephrotoxicity
Take Home Points Higher acuity patients are at risk for VAN
Nephrotoxicity was seen after 4 days of therapy
AKI developed from VPT is reversible
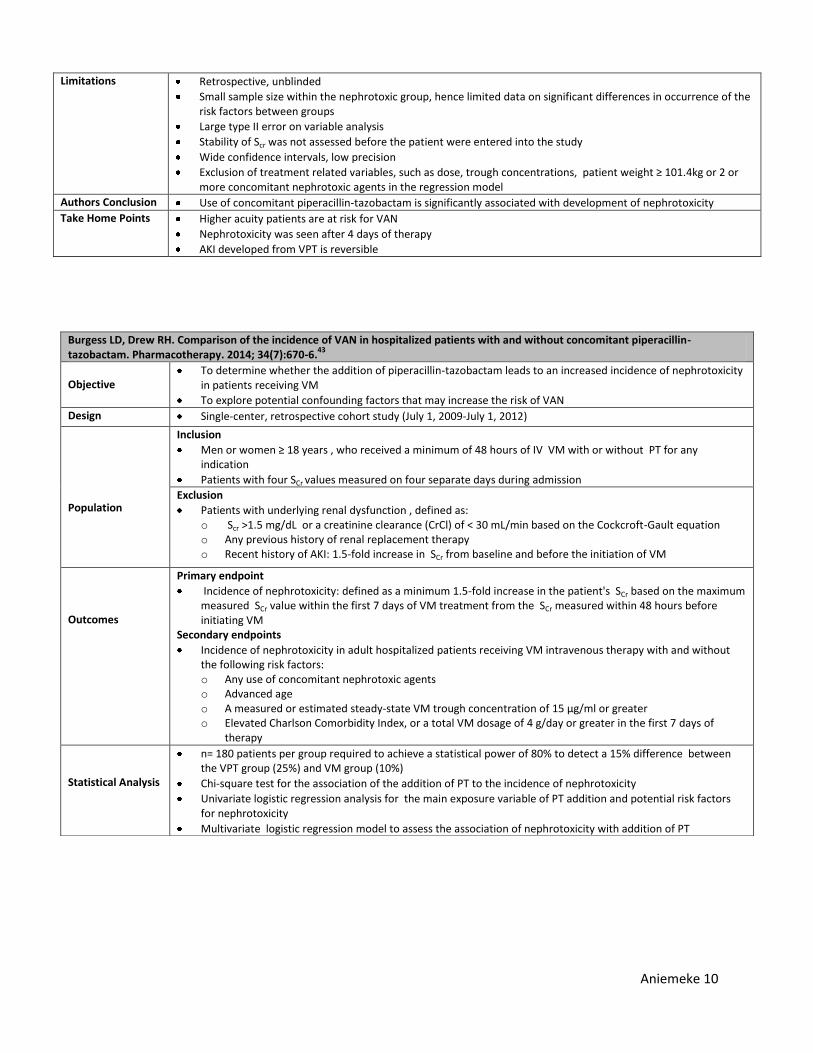
Burgess LD, Drew RH. Comparison of the incidence of VAN in hospitalized patients with and without concomitant piperacillin-tazobactam. Pharmacotherapy. 2014; 34(7):670-6.
43
Objective
To determine whether the addition of piperacillin-tazobactam leads to an increased incidence of nephrotoxicity in patients receiving VM
To explore potential confounding factors that may increase the risk of VAN
Design Single-center, retrospective cohort study (July 1, 2009-July 1, 2012)
Population
Inclusion
Men or women ≥ 18 years , who received a minimum of 48 hours of IV VM with or without PT for any indication
Patients with four SCr values measured on four separate days during admission
Exclusion
Patients with underlying renal dysfunction , defined as: o Scr >1.5 mg/dL or a creatinine clearance (CrCl) of < 30 mL/min based on the Cockcroft-Gault equation o Any previous history of renal replacement therapy o Recent history of AKI: 1.5-fold increase in SCr from baseline and before the initiation of VM
Outcomes
Primary endpoint
Incidence of nephrotoxicity: defined as a minimum 1.5-fold increase in the patient's SCr based on the maximum measured SCr value within the first 7 days of VM treatment from the SCr measured within 48 hours before initiating VM
Secondary endpoints
Incidence of nephrotoxicity in adult hospitalized patients receiving VM intravenous therapy with and without the following risk factors: o Any use of concomitant nephrotoxic agents o Advanced age o A measured or estimated steady-state VM trough concentration of 15 μg/ml or greater o Elevated Charlson Comorbidity Index, or a total VM dosage of 4 g/day or greater in the first 7 days of
therapy
Statistical Analysis
n= 180 patients per group required to achieve a statistical power of 80% to detect a 15% difference between the VPT group (25%) and VM group (10%)
Chi-square test for the association of the addition of PT to the incidence of nephrotoxicity
Univariate logistic regression analysis for the main exposure variable of PT addition and potential risk factors for nephrotoxicity
Multivariate logistic regression model to assess the association of nephrotoxicity with addition of PT
Aniemeke 11
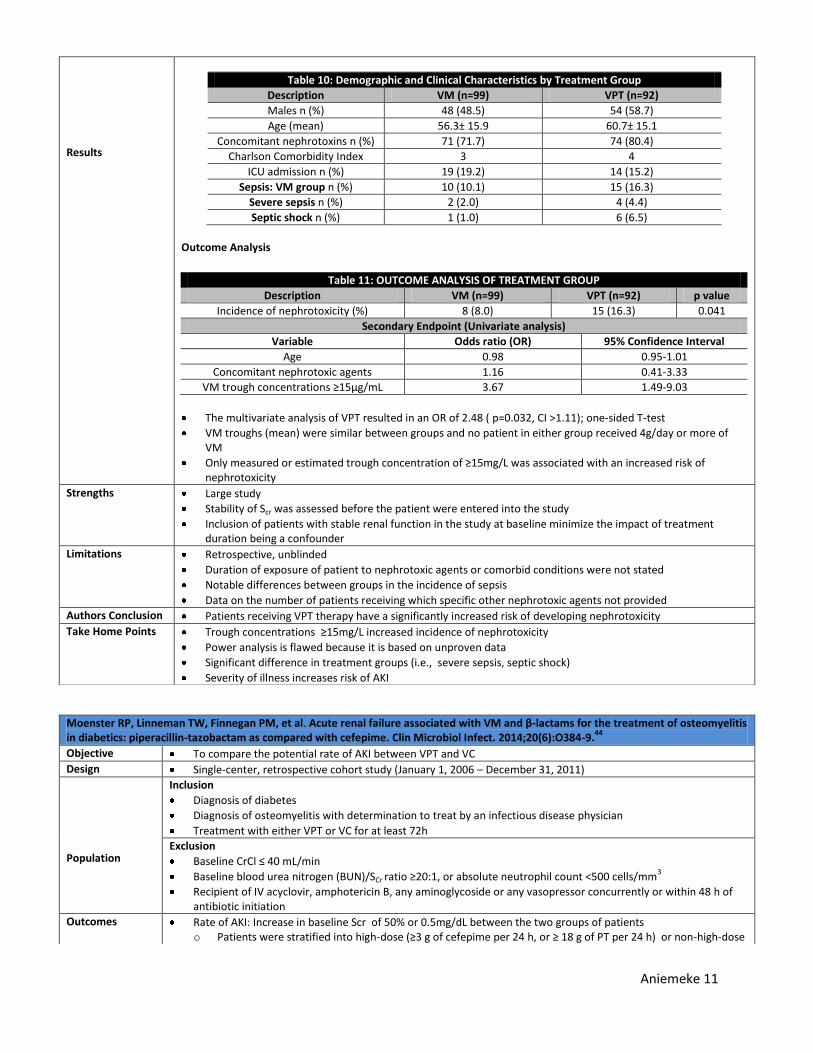
Results
Table 10: Demographic and Clinical Characteristics by Treatment Group
Description VM (n=99) VPT (n=92)
Males n (%) 48 (48.5) 54 (58.7)
Age (mean) 56.3± 15.9 60.7± 15.1
Concomitant nephrotoxins n (%) 71 (71.7) 74 (80.4)
Charlson Comorbidity Index 3 4
ICU admission n (%) 19 (19.2) 14 (15.2)
Sepsis: VM group n (%) 10 (10.1) 15 (16.3)
Severe sepsis n (%) 2 (2.0) 4 (4.4)
Septic shock n (%) 1 (1.0) 6 (6.5)
Outcome Analysis
Table 11: OUTCOME ANALYSIS OF TREATMENT GROUP
Description VM (n=99) VPT (n=92) p value
Incidence of nephrotoxicity (%) 8 (8.0) 15 (16.3) 0.041
Secondary Endpoint (Univariate analysis)
Variable Odds ratio (OR) 95% Confidence Interval
Age 0.98 0.95-1.01
Concomitant nephrotoxic agents 1.16 0.41-3.33
VM trough concentrations ≥15μg/mL 3.67 1.49-9.03
The multivariate analysis of VPT resulted in an OR of 2.48 ( p=0.032, CI >1.11); one-sided T-test
VM troughs (mean) were similar between groups and no patient in either group received 4g/day or more of VM
Only measured or estimated trough concentration of ≥15mg/L was associated with an increased risk of nephrotoxicity
Strengths Large study
Stability of Scr was assessed before the patient were entered into the study
Inclusion of patients with stable renal function in the study at baseline minimize the impact of treatment duration being a confounder
Limitations Retrospective, unblinded
Duration of exposure of patient to nephrotoxic agents or comorbid conditions were not stated
Notable differences between groups in the incidence of sepsis
Data on the number of patients receiving which specific other nephrotoxic agents not provided
Authors Conclusion Patients receiving VPT therapy have a significantly increased risk of developing nephrotoxicity
Take Home Points Trough concentrations ≥15mg/L increased incidence of nephrotoxicity
Power analysis is flawed because it is based on unproven data
Significant difference in treatment groups (i.e., severe sepsis, septic shock)
Severity of illness increases risk of AKI
Moenster RP, Linneman TW, Finnegan PM, et al. Acute renal failure associated with VM and β-lactams for the treatment of osteomyelitis in diabetics: piperacillin-tazobactam as compared with cefepime. Clin Microbiol Infect. 2014;20(6):O384-9.
44
Objective To compare the potential rate of AKI between VPT and VC
Design Single-center, retrospective cohort study (January 1, 2006 – December 31, 2011)
Population
Inclusion
Diagnosis of diabetes
Diagnosis of osteomyelitis with determination to treat by an infectious disease physician
Treatment with either VPT or VC for at least 72h
Exclusion
Baseline CrCl ≤ 40 mL/min
Baseline blood urea nitrogen (BUN)/SCr ratio ≥20:1, or absolute neutrophil count <500 cells/mm3
Recipient of IV acyclovir, amphotericin B, any aminoglycoside or any vasopressor concurrently or within 48 h of antibiotic initiation
Outcomes Rate of AKI: Increase in baseline Scr of 50% or 0.5mg/dL between the two groups of patients o Patients were stratified into high-dose (≥3 g of cefepime per 24 h, or ≥ 18 g of PT per 24 h) or non-high-dose
Aniemeke 12
therapy
Statistical Analysis
n= 200 patients per group was required to achieve a statistical power of 80%, to detect a 19% difference between groups
Chi-square test or Fisher’s extract test to compare non-parametric data
Student’s t-test to evaluate parametric data, an alpha of <0.05was considered significant
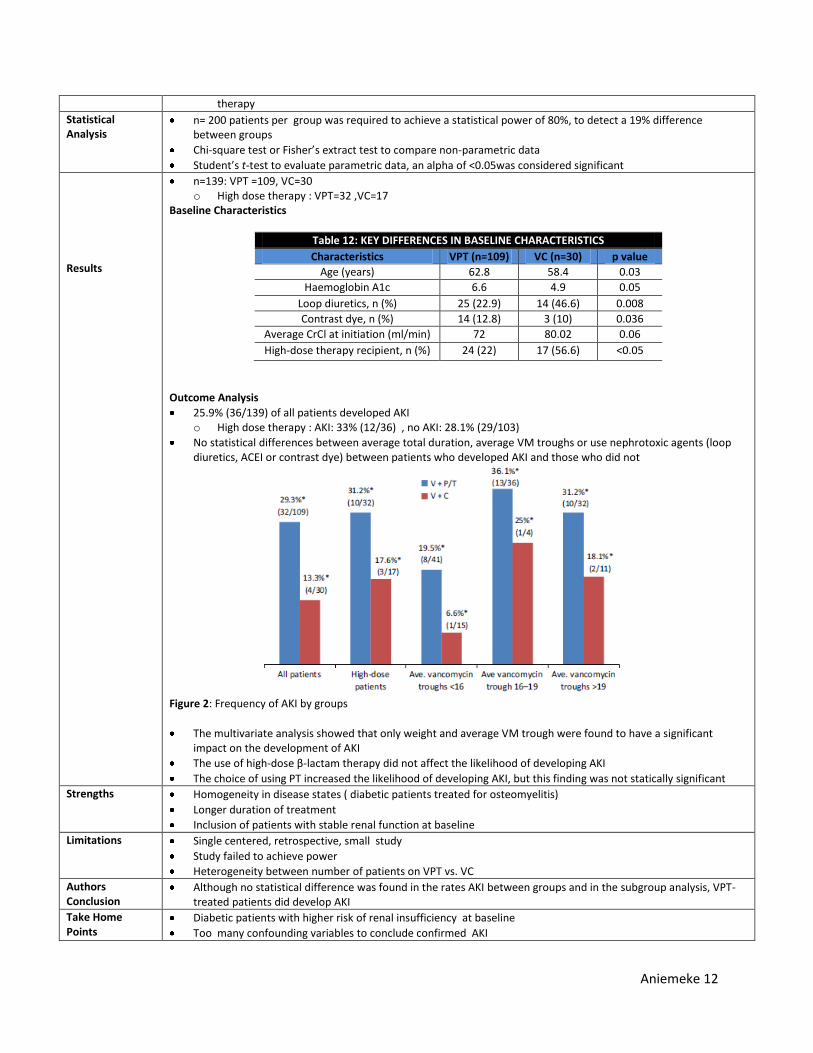
Results
n=139: VPT =109, VC=30 o High dose therapy : VPT=32 ,VC=17
Baseline Characteristics
Table 12: KEY DIFFERENCES IN BASELINE CHARACTERISTICS
Characteristics VPT (n=109) VC (n=30) p value
Age (years) 62.8 58.4 0.03
Haemoglobin A1c 6.6 4.9 0.05
Loop diuretics, n (%) 25 (22.9) 14 (46.6) 0.008
Contrast dye, n (%) 14 (12.8) 3 (10) 0.036
Average CrCl at initiation (ml/min) 72 80.02 0.06
High-dose therapy recipient, n (%) 24 (22) 17 (56.6) <0.05
Outcome Analysis
25.9% (36/139) of all patients developed AKI o High dose therapy : AKI: 33% (12/36) , no AKI: 28.1% (29/103)
No statistical differences between average total duration, average VM troughs or use nephrotoxic agents (loop diuretics, ACEI or contrast dye) between patients who developed AKI and those who did not
Figure 2: Frequency of AKI by groups
The multivariate analysis showed that only weight and average VM trough were found to have a significant impact on the development of AKI
The use of high-dose β-lactam therapy did not affect the likelihood of developing AKI
The choice of using PT increased the likelihood of developing AKI, but this finding was not statically significant
Strengths Homogeneity in disease states ( diabetic patients treated for osteomyelitis)
Longer duration of treatment
Inclusion of patients with stable renal function at baseline
Limitations Single centered, retrospective, small study
Study failed to achieve power
Heterogeneity between number of patients on VPT vs. VC
Authors Conclusion
Although no statistical difference was found in the rates AKI between groups and in the subgroup analysis, VPT-treated patients did develop AKI
Take Home Points
Diabetic patients with higher risk of renal insufficiency at baseline
Too many confounding variables to conclude confirmed AKI
Aniemeke 13
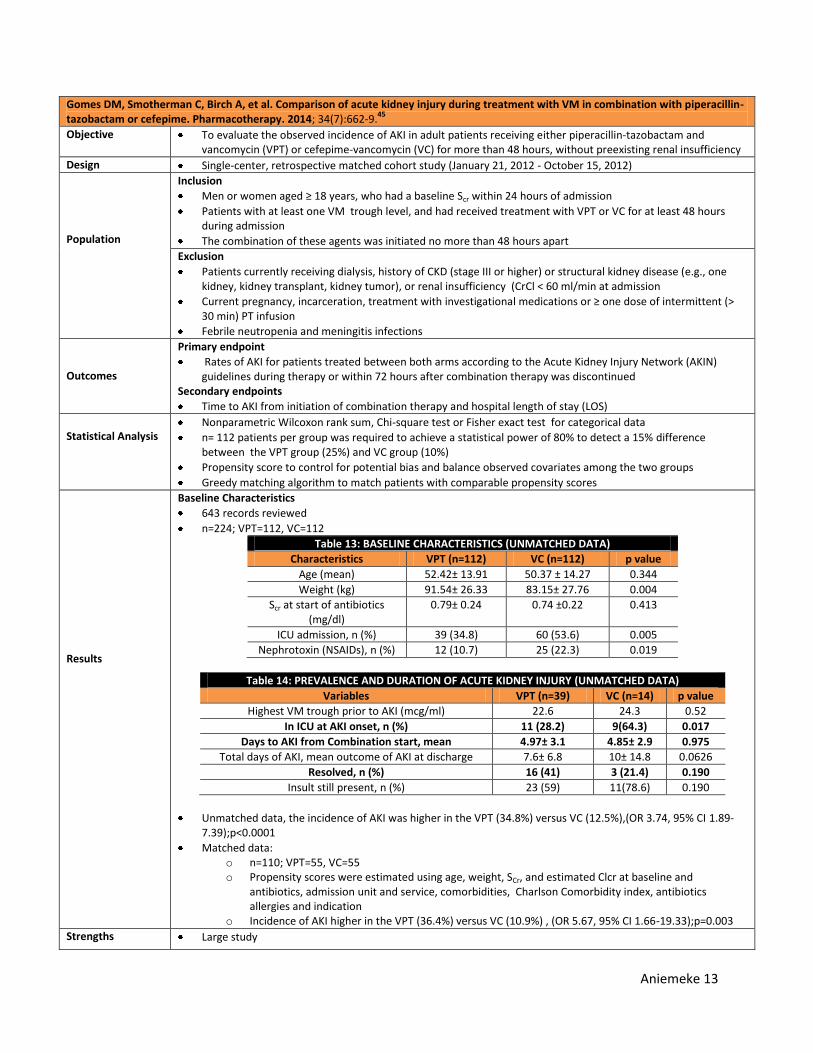
Gomes DM, Smotherman C, Birch A, et al. Comparison of acute kidney injury during treatment with VM in combination with piperacillin-tazobactam or cefepime. Pharmacotherapy. 2014; 34(7):662-9.
45
Objective To evaluate the observed incidence of AKI in adult patients receiving either piperacillin-tazobactam and vancomycin (VPT) or cefepime-vancomycin (VC) for more than 48 hours, without preexisting renal insufficiency
Design Single-center, retrospective matched cohort study (January 21, 2012 - October 15, 2012)
Population
Inclusion
Men or women aged ≥ 18 years, who had a baseline Scr within 24 hours of admission
Patients with at least one VM trough level, and had received treatment with VPT or VC for at least 48 hours during admission
The combination of these agents was initiated no more than 48 hours apart
Exclusion
Patients currently receiving dialysis, history of CKD (stage III or higher) or structural kidney disease (e.g., one kidney, kidney transplant, kidney tumor), or renal insufficiency (CrCl < 60 ml/min at admission
Current pregnancy, incarceration, treatment with investigational medications or ≥ one dose of intermittent (> 30 min) PT infusion
Febrile neutropenia and meningitis infections
Outcomes
Primary endpoint
Rates of AKI for patients treated between both arms according to the Acute Kidney Injury Network (AKIN) guidelines during therapy or within 72 hours after combination therapy was discontinued
Secondary endpoints
Time to AKI from initiation of combination therapy and hospital length of stay (LOS)
Statistical Analysis
Nonparametric Wilcoxon rank sum, Chi-square test or Fisher exact test for categorical data
n= 112 patients per group was required to achieve a statistical power of 80% to detect a 15% difference between the VPT group (25%) and VC group (10%)
Propensity score to control for potential bias and balance observed covariates among the two groups
Greedy matching algorithm to match patients with comparable propensity scores
Results
Baseline Characteristics
643 records reviewed
n=224; VPT=112, VC=112
Table 13: BASELINE CHARACTERISTICS (UNMATCHED DATA)
Characteristics VPT (n=112) VC (n=112) p value
Age (mean) 52.42± 13.91 50.37 ± 14.27 0.344
Weight (kg) 91.54± 26.33 83.15± 27.76 0.004
Scr at start of antibiotics (mg/dl)
0.79± 0.24 0.74 ±0.22 0.413
ICU admission, n (%) 39 (34.8) 60 (53.6) 0.005
Nephrotoxin (NSAIDs), n (%) 12 (10.7) 25 (22.3) 0.019
Table 14: PREVALENCE AND DURATION OF ACUTE KIDNEY INJURY (UNMATCHED DATA)
Variables VPT (n=39) VC (n=14) p value
Highest VM trough prior to AKI (mcg/ml) 22.6 24.3 0.52
In ICU at AKI onset, n (%) 11 (28.2) 9(64.3) 0.017
Days to AKI from Combination start, mean 4.97± 3.1 4.85± 2.9 0.975
Total days of AKI, mean outcome of AKI at discharge 7.6± 6.8 10± 14.8 0.0626
Resolved, n (%) 16 (41) 3 (21.4) 0.190
Insult still present, n (%) 23 (59) 11(78.6) 0.190
Unmatched data, the incidence of AKI was higher in the VPT (34.8%) versus VC (12.5%),(OR 3.74, 95% CI 1.89-7.39);p<0.0001
Matched data: o n=110; VPT=55, VC=55 o Propensity scores were estimated using age, weight, SCr, and estimated Clcr at baseline and
antibiotics, admission unit and service, comorbidities, Charlson Comorbidity index, antibiotics allergies and indication
o Incidence of AKI higher in the VPT (36.4%) versus VC (10.9%) , (OR 5.67, 95% CI 1.66-19.33);p=0.003
Strengths Large study
Aniemeke 14
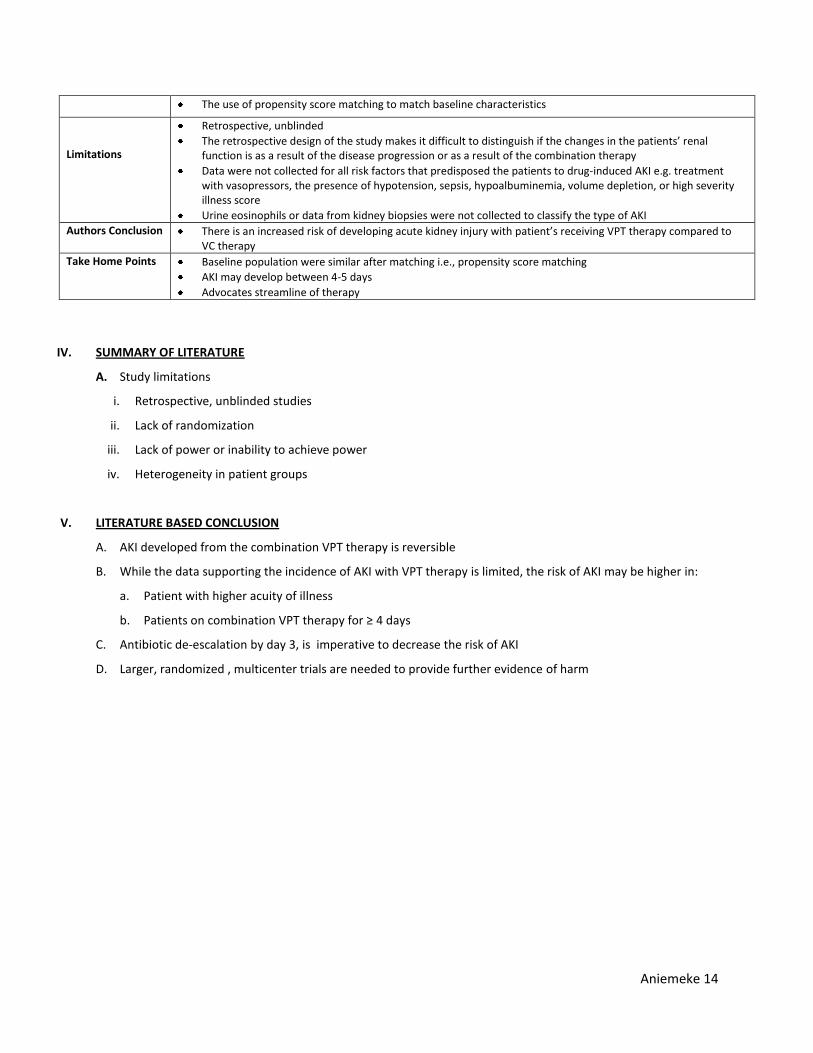
IV. SUMMARY OF LITERATURE
A. Study limitations
i. Retrospective, unblinded studies
ii. Lack of randomization
iii. Lack of power or inability to achieve power
iv. Heterogeneity in patient groups
V. LITERATURE BASED CONCLUSION
A. AKI developed from the combination VPT therapy is reversible
B. While the data supporting the incidence of AKI with VPT therapy is limited, the risk of AKI may be higher in:
a. Patient with higher acuity of illness
b. Patients on combination VPT therapy for ≥ 4 days
C. Antibiotic de-escalation by day 3, is imperative to decrease the risk of AKI
D. Larger, randomized , multicenter trials are needed to provide further evidence of harm
The use of propensity score matching to match baseline characteristics
Limitations
Retrospective, unblinded
The retrospective design of the study makes it difficult to distinguish if the changes in the patients’ renal function is as a result of the disease progression or as a result of the combination therapy
Data were not collected for all risk factors that predisposed the patients to drug-induced AKI e.g. treatment with vasopressors, the presence of hypotension, sepsis, hypoalbuminemia, volume depletion, or high severity illness score
Urine eosinophils or data from kidney biopsies were not collected to classify the type of AKI
Authors Conclusion There is an increased risk of developing acute kidney injury with patient’s receiving VPT therapy compared to VC therapy
Take Home Points Baseline population were similar after matching i.e., propensity score matching
AKI may develop between 4-5 days
Advocates streamline of therapy
Aniemeke 15
REFERENCES
1. The Kidney Disease Improving Global Outcomes (KDIGO). Acute Kidney Injury Working Group. KDIGO Clinical
Practice Guidelines for Acute Kidney Injury. Kidney Inter,.Suppl. 2012; 1–138. 2. Dennen P, Douglas IS, Anderson R. Acute kidney injury in the intensive care unit: an update and primer for the
intensivist. Crit Care Med. 2010;38(1):261-75. 3. Bellomo R, Kellum JA, Ronco C. Acute kidney injury. Lancet.2012;14(9843):756-766. 4. Singri N, Ahya SN, Levin ML. Acute Renal Failure.JAMA. 2003;289(6):747-751. 5. Dager W, Halilovic J. Acute Kidney Injury. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM, editors.
Pharmacotherapy: A Pathophysiologic Approach. 9th
ed. New York (NY): McGraw-Hill; 2014. P.611-32. 6. Rahman M, Shad F, Smith MC. Acute kidney injury: a guide to diagnosis and management. Am Fam Physician.
2012;86(7):631-9. 7. Basile DP, Anderson MD, Sutton TA. Pathophysiology of acute kidney injury. Compr Physiol. 2012;2(2):1303-53. 8. Mandell GL, Bennett JE, Dolin R. Mandell, Douglas and Bennett’s Principles and Practice of Infectious Diseases. 7th
ed. Philadelphia: Churchill Livingstone; c2009. 9. Gupta A, Biyani M, Khaira A. Vancomycin nephrotoxicity: myths and facts. Neth J Med. 2011;69(9):379-83. 10. Moh'd H, Kheir F, Kong L, et al. Incidence and predictors of vancomycin-associated nephrotoxicity. South Med J.
2014;107(6):383-8. 11. Vancomycin. In: DRUGDEX
® System (electronic version). Thomson Reuters, Greenwood Village, Colorado, USA.
Available at: http://www.micromedexsolutions.com.ezproxy.lib.utexas.edu. Accessed January 4, 2015. 12. Vancomycin. Lexi-Drugs Online.Lexi-Comp, Hudson, Ohio, USA. Available at:
http://www.micromedexsolutions.com.ezproxy.lib.utexas.edu. Accessed January 4, 2015. 13. Toyoguchi T, Takahashi S, Hosoya J, et al. Nephrotoxicity of vancomycin and drug interaction study with cilastatin
in rabbits. Antimicrobial Agents Chemother. 1997;41(9):1985-1990. 14. Oktem F, Arslan MK, Ozguner F, et al. In vivo evidences suggesting the role of oxidative stress in pathogenesis of
vancomycin induced nephrotoxicity: protection by erdosteine. Toxicology. 2005; 215(3):227-233. 15. King DW, Smith MA. Proliferative responses observed following vancomycin treatment in renal proximal tubule
epithelial cells.Toxicol In Vitro. 2004; 18(6):797-803. 16. Mergenhagen KA, Borton AR. Vancomycin nephrotoxicity: a review. J. Pharm Pract. 2014;27(6):545-53. 17. Elyasi S, Khalili H, Dashti-khavidaki S, et al. Vancomycin-induced nephrotoxicity: mechanism, incidence, risk factors
and special populations. A literature review. Eur J Clin Pharmacol. 2012;68(9):1243-55. 18. Carreno JJ, Kenney RM, Lomaestro B. Vancomycin-associated renal dysfunction: where are we now?.
Pharmacotherapy. 2014;34(12):1259-68. 19. Hidayat LK, Hsu DI, Quist R, et al. High-dose vancomycin therapy for methicillin-resistant Staphylococcus aureus
infections: efficacy and toxicity. Arch Intern Med. 2006;166(19):2138-44. 20. Lodise TP, Lomaestro B, Graves J, et al.Larger vancomycin doses (at least four grams per day) are associated with
an increased incidence of nephrotoxicity. Antimicrob Agents Chemother. 2008;52(4):1330-6. 21. Lodise TP, Patel N, Lomaestro BM, et al. Relationship between initial vancomycin concentration-time profile and
nephrotoxicity among hospitalized patients. Clin Infect Dis. 2009;49(4):507-14. 22. Bosso JA, Nappi J, Rudisill C, et al. Relationship between vancomycin trough concentrations and nephrotoxicity: a
prospective multicenter trial. Antimicrob Agents Chemother. 2011;55(12):5475-9. 23. Minejima E, Choi J, Beringer P, et al. Applying new diagnostic criteria for acute kidney injury to facilitate early
identification of nephrotoxicity in vancomycin-treated patients. Antimicrob Agents Chemother. 2011;55(7):3278-83.
24. Cano EL, Haque NZ, Welch VL, et al. Incidence of nephrotoxicity and association with vancomycin use in intensive care unit patients with pneumonia: retrospective analysis of the IMPACT-HAP Database. Clin Ther. 2012;34(1):149-57.
25. Prabaker KK, Tran TP, Pratummas T, et al. Elevated vancomycin trough is not associated with nephrotoxicity among inpatient veterans. J Hosp Med. 2012;7(2):91-7.
26. Wunderink RG, Niederman MS, Kollef MH, et al. Linezolid in methicillin-resistant Staphylococcus aureus nosocomial pneumonia: a randomized, controlled study. Clin Infect Dis. 2012;54(5):621-9.
27. Miller EL. The penicillins: a review and update. J Midwifery Womens Health. 2002;47(6):426-34 28. Brunton LB, Lazo JS, Parker KL, eds. Goodman & Gilman's The Pharmacological Basis of Therapeutics. 12th ed. New
Aniemeke 16
York: McGraw-Hill; 2011 29. Sakarcan A, Marcille R, Stallworth J. Antibiotic-induced recurring interstitial nephritis. Pediatr Nephrol.
2002;17(1):50-1. 30. Border WA, Lehman DH, Egan JD. Anti-tubular basement membrane antibodies and methicillin associated
interstitial nephritis. N Engl J Med.1974;291:381–384 31. Ditlove J, Weidmann P, Bernstein M, et al. Methicillin nephritis. Medicine.1977;56:483-91 32. Liu P, Tepperman BS, Logan AG. Acute renal failure induced by semi-synthetic penicillins. Can Fam Physician.
1981;27:507-12. 33. Piperacillin and Tazobactam (Zosyn ®) package insert.Wyeth Pharmaceuticals Inc.,January, 2015 34. Kim MK, Xuan D, Quintiliani R, et al. Pharmacokinetic and pharmacodynamic profile of high dose extended interval
piperacillin-tazobactam. J Antimicrob Chemother. 2001;48(2):259-67. 35. Desai NR, Shah SM, Cohen J, et al. Zosyn (piperacillin/tazobactam) reformulation: Expanded compatibility and
coadministration with lactated Ringer's solutions and selected aminoglycosides. Ther Clin Risk Manag. 2008;4(2):303-14.
36. Pill MW, O'neill CV, Chapman MM, et al. Suspected acute interstitial nephritis induced by piperacillin-tazobactam. Pharmacotherapy. 1997;17(1):166-9.
37. Liu TJ, Lam JP. Piperacillin-tazobactam-induced acute interstitial nephritis with possible meropenem cross-sensitivity in a patient with osteomyelitis. Am J Health Syst Pharm. 2012;69(13):1109.
38. Tanaka H, Waga S, Kakizaki Y, et al. Acute tubulointerstitial nephritis associated with piperacillin therapy in a boy with glomerulonephritis. Acta Paediatr Jpn. 1997;39(6):698-700.
39. Polderman KH, Girbes AR. Piperacillin-induced magnesium and potassium loss in intensive care unit patients. Intensive Care Med. 2002;28(4):520-2.
40. Hellwig T, Hammerquist R, Loecker B, et al. Retrospective Evaluation of the Incidence of Vancomycin and/or Piperacillin-Tazobactam Induced Acute Renal Failure. Crit Care Med. December 2011. 39(12); p 79
41. Min E, Box K, Lane J, et al. Acute Kidney Injury in Patients Receiving Concomitant Vancomycin and Piperacillin/Tazobactam. Crit. Care Med. December 2011. 39(12); p 200.
42. Meaney CJ, Hynicka LM, Tsoukleris MG. Vancomycin-associated nephrotoxicity in adult medicine patients: incidence, outcomes, and risk factors. Pharmacotherapy. 2014;34(7):653-61.
43. Burgess LD, Drew RH. Comparison of the incidence of vancomycin-induced nephrotoxicity in hospitalized patients with and without concomitant piperacillin-tazobactam. Pharmacotherapy. 2014;34(7):670-6.
44. Moenster RP, Linneman TW, Finnegan PM, et al. Acute renal failure associated with vancomycin and β-lactams for the treatment of osteomyelitis in diabetics: piperacillin-tazobactam as compared with cefepime. Clin Microbiol Infect. 2014;20(6):O384-9.
45. Gomes DM, Smotherman C, Birch A, et al. Comparison of acute kidney injury during treatment with vancomycin in combination with piperacillin-tazobactam or cefepime. Pharmacotherapy. 2014;34(7):662-9.
46. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245-51.
Aniemeke 17
APPENDIXES
Appendix A:
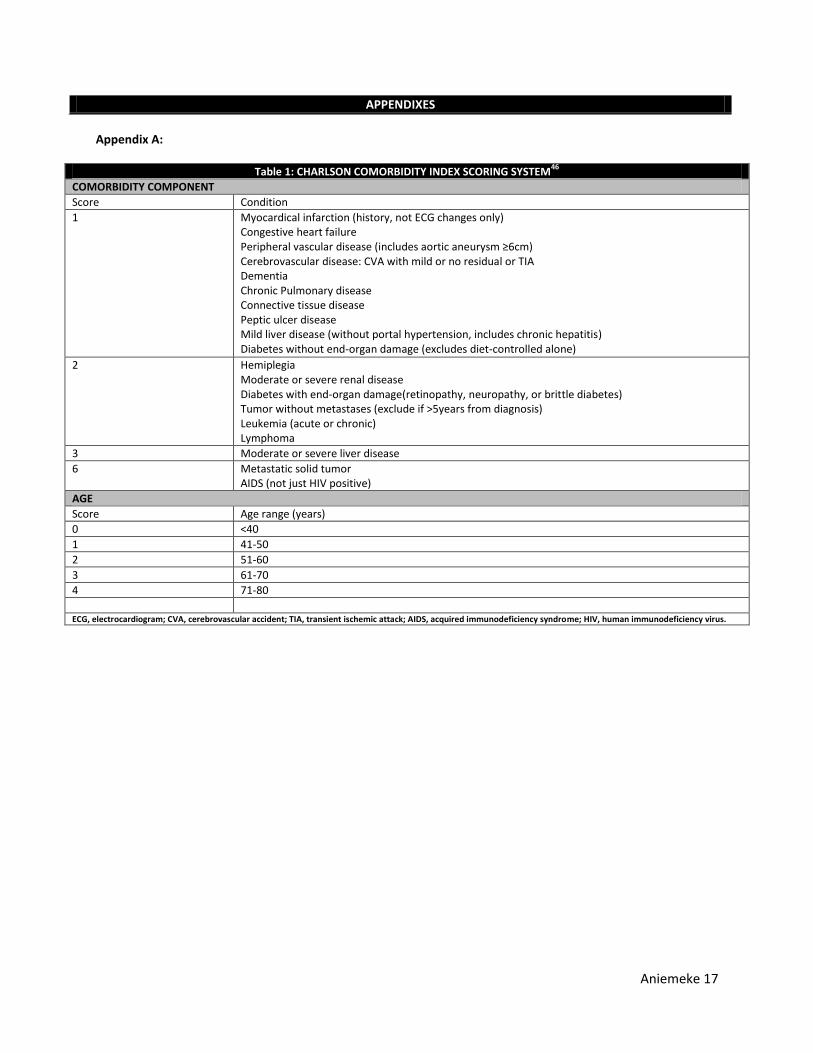
Table 1: CHARLSON COMORBIDITY INDEX SCORING SYSTEM46
COMORBIDITY COMPONENT
Score Condition
1 Myocardical infarction (history, not ECG changes only) Congestive heart failure Peripheral vascular disease (includes aortic aneurysm ≥6cm) Cerebrovascular disease: CVA with mild or no residual or TIA Dementia Chronic Pulmonary disease Connective tissue disease Peptic ulcer disease Mild liver disease (without portal hypertension, includes chronic hepatitis) Diabetes without end-organ damage (excludes diet-controlled alone)
2 Hemiplegia Moderate or severe renal disease Diabetes with end-organ damage(retinopathy, neuropathy, or brittle diabetes) Tumor without metastases (exclude if >5years from diagnosis) Leukemia (acute or chronic) Lymphoma
3 Moderate or severe liver disease
6 Metastatic solid tumor AIDS (not just HIV positive)
AGE
Score Age range (years)
0 <40
1 41-50
2 51-60
3 61-70
4 71-80
ECG, electrocardiogram; CVA, cerebrovascular accident; TIA, transient ischemic attack; AIDS, acquired immunodeficiency syndrome; HIV, human immunodeficiency virus.

















![[Product Monograph Template - Standard] - Pfizer · PDF filePRODUCT MONOGRAPH . PrTAZOCIN® Piperacillin and Tazobactam powder for injection . 2.0g/0.25g, 3g/0.375g, 4.0g/0.5g per](https://static.cupdf.com/doc/110x72/5aa7236e7f8b9ab8228bd94a/product-monograph-template-standard-pfizer-monograph-prtazocin-piperacillin.jpg)










