Features
Sample
Community
JOIN FREE
X
YOU ARE DOWNLOADING DOCUMENT
·
[email protected]
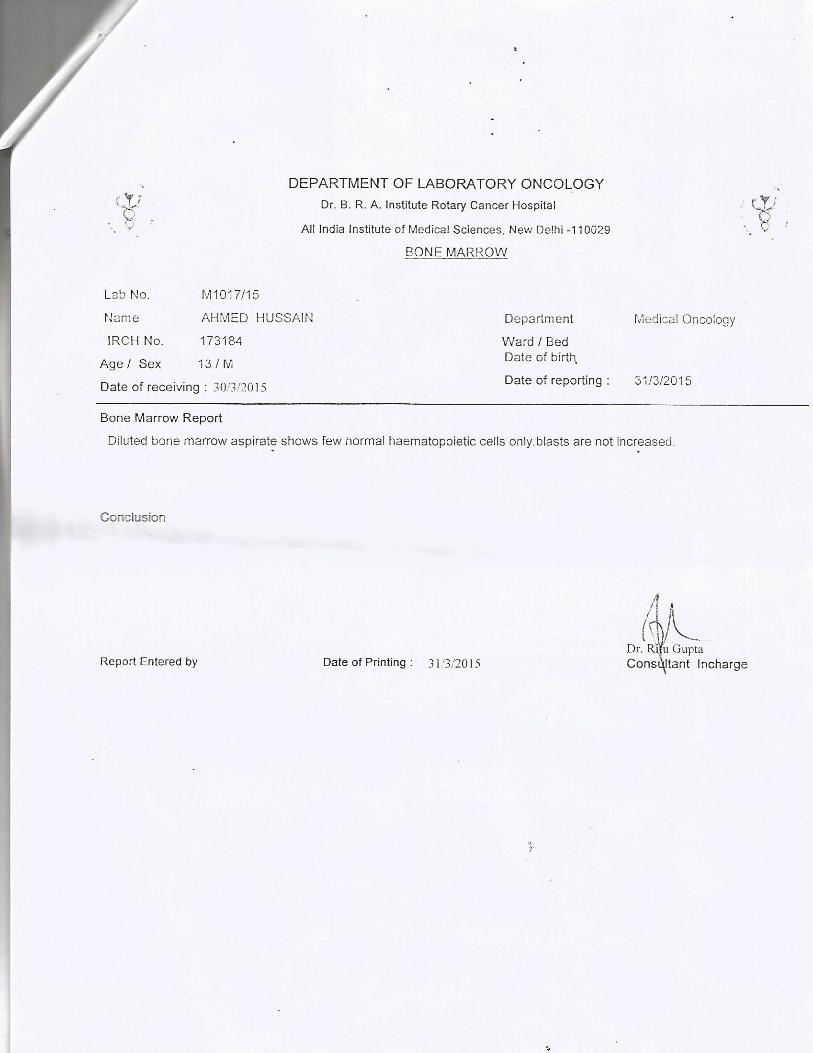
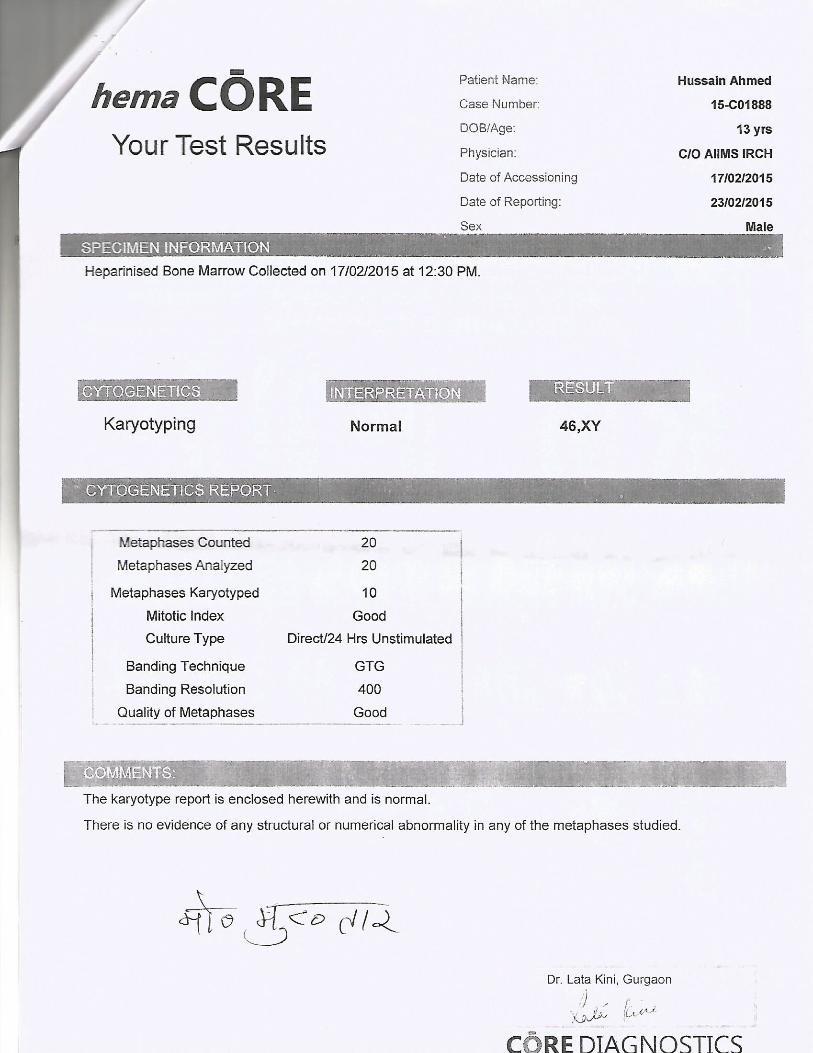
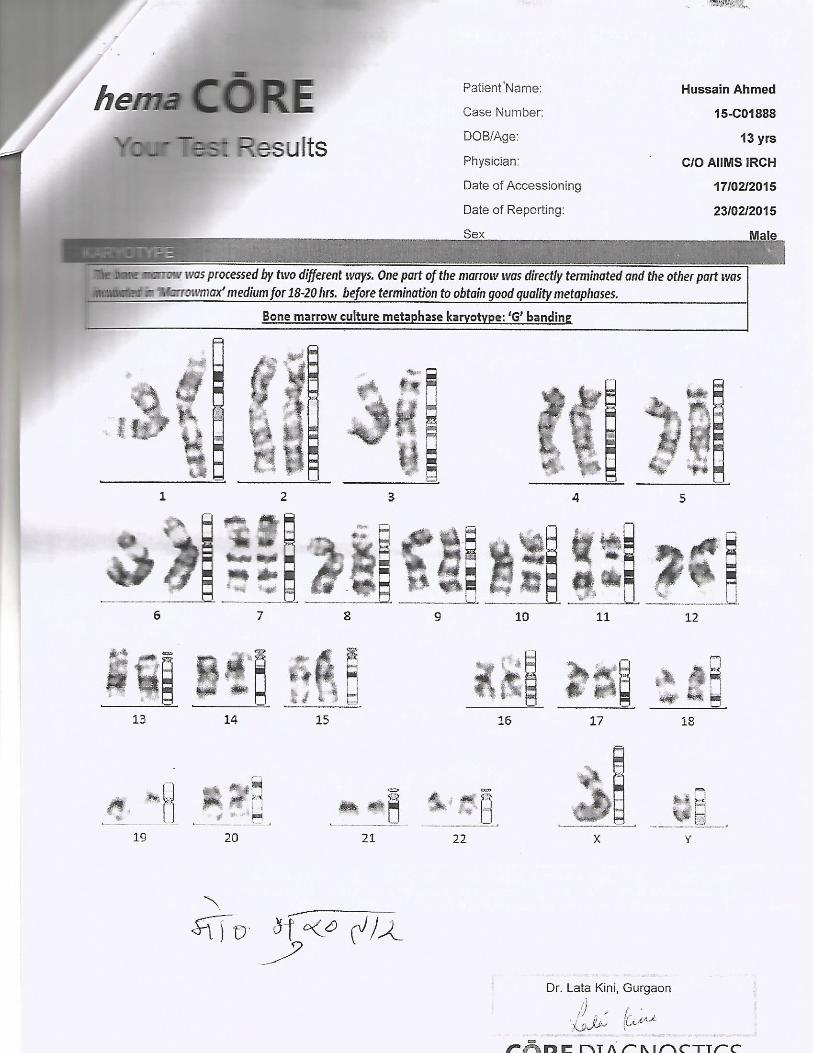
1947 1800 300 1947 . hema CÖRE Your Test Results SPECIMEN INFORMATION Patient Name: Case Number: DOB/Age. Physician:
Category:
Documents
·
[email protected]
1947 1800 300 1947 . hema CÖRE Your Test Results SPECIMEN INFORMATION Patient Name: Case Number: DOB/Age. Physician:
Please tick the box to continue:
DOWNLOAD NOW
Transcript
Page 1
Page 2
Page 3
Page 4
Page 5
Page 6
Page 7
Page 8
Page 9
LOAD MORE
Related Documents
Hema Science
Category:
Documents
April 2020 - UIDAI1. By visiting UIDAI official website...
Category:
Documents
Hema Diseases
Category:
Documents
Brochure Hema
Category:
Documents
· wv,w.uidai.gov.in 1947 1947 #4107 6966 3910 8084...
Category:
Documents
barnala.gov.inbarnala.gov.in/pdf/Aadhaar Info.pdfà...
Category:
Documents
journal hema
Category:
Documents
Scanned by CamScanner -...
Category:
Documents
Tutor hema hotim
Category:
Technology
makalah hema
Category:
Documents
hema screen
Category:
Documents
Biometric Data Capture - uidai.gov.in
Category:
Documents
Hema Upasani
Category:
Documents
uidai.gov.in...Created Date 2/7/2019 12:57:56 PM
Category:
Documents
hema chakraborty
Category:
Documents
Module 3B Installation & Configuration of Aadhaar ... · PDF...
Category:
Documents
MergedFile - kilkaricarefoundation.org · 1947 1800 300...
Category:
Documents
Hema Brochure
Category:
Documents
Hema Research
Category:
Documents
Atherosclerosis- Hema Negi
Category:
Documents
HEMA gaat Bric Brac -...
Category:
Documents
Titas Presentation Hema
Category:
Documents
HATTAT HOLDING€¦ · HATTAT HOLDING Hattat Tarım Hema...
Category:
Documents
CATALOGO ¡HEMA!
Category:
Documents
Hema launch release
Category:
Documents
HEMA Dasar Hema
Category:
Documents
Hema Hema Hema Ra Ki Rangarajan
Category:
Documents
Hema intro anemia
Category:
Documents
bloominglivesfoundation.combloominglivesfoundation.com/wp-co...
Category:
Documents
Atlas Hema
Category:
Documents