



Transesophageal
Echocardiography
Dhaval Patel
History • In 1976, Dr. Leon Frazin published the
results of studies using an esophageal M-mode transducer
• Matsumoto and associates used M-mode TEE to study left ventricular (LV) function
• In the early 1980s, investigators led by Hanrath introduced a two-dimensional (2D), phased-array transducer mounted on the tip of a flexible gastroscope

Reasons for success of TEE
1. Close proximity of esophagus to post wall of heart – no intervening structure like bone or lung
2. Monitor the heart over time, such as during cardiac surgeries
3. Extremely safe & well tolerated so that it can be performed in critically ill patients & very small infants
Unique data from TEE • Atrial thrombi/mass
left atrial appendage clot
clot in LA
thrombus in RA
• Mitral valve
MR (very precisely)
function of prosthetic valves
refined suitability for valvotomy in severe MS
Cont.
• Aorta
Detection of dissection
Detection of atheroma
• Chambers
Patent foramen ovale
• Online monitoring
Monitoring interventional procedures
o atrial septostomy
o baloon valvotomy
o pulmonary vein interventions
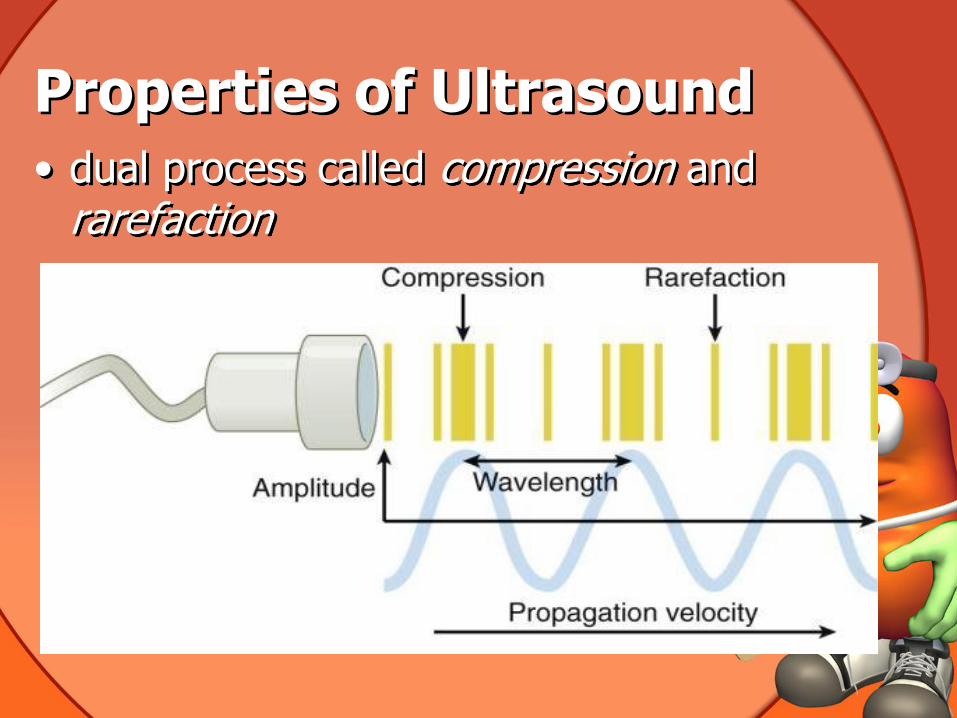
Properties of Ultrasound • dual process called compression and
rarefaction

Properties of Ultrasound cont. • sequence of compression and rarefaction is
described by sine waves
• characterized in terms of
Wavelength distance between two peaks of the sine wave
Frequency number of cycles that occur in 1 second
Amplitude measure of tissue compression
Propagation velocity speed of an ultrasound wave
traveling through tissue
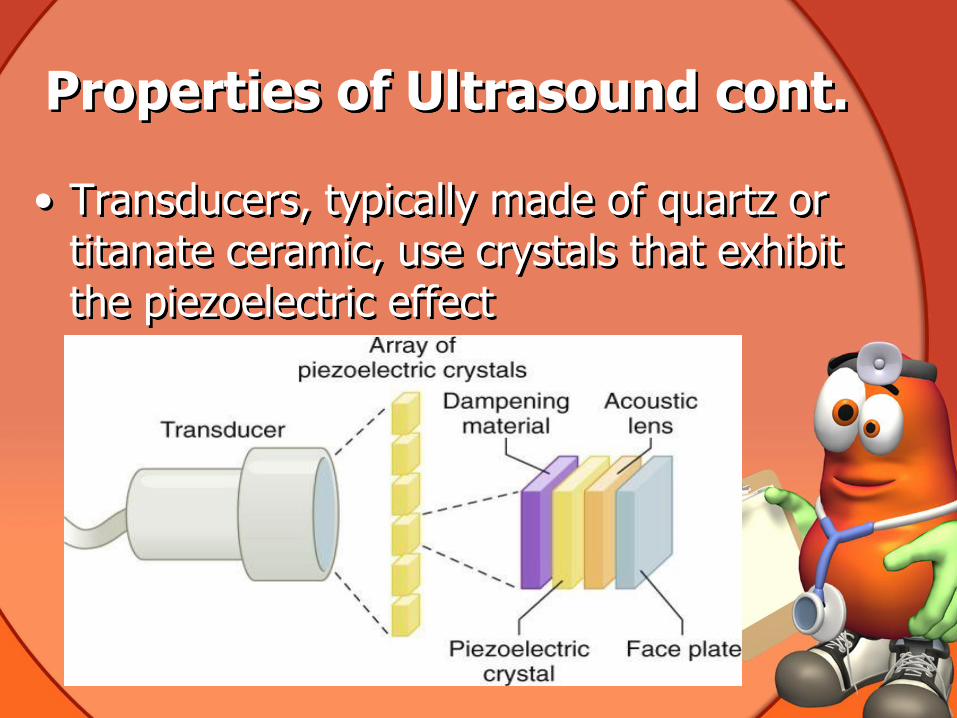
Properties of Ultrasound cont.
• Transducers, typically made of quartz or titanate ceramic, use crystals that exhibit the piezoelectric effect
Transducer Frequency, Image Resolution, and Depth of
Penetration • Echocardiography uses frequencies of 2.5 to
7.5 million cycles/sec (MHz)
• Important relationships between transducer frequency, depth, and resolution include
(1) the slower the frequency, the greater the depth of penetration at the expense of resolution, and
(2) the faster the frequency, the greater the resolution at the expense of depth of penetration
Cont. • Image resolution is characterized in terms
of
Axial resolution
Elevational resolution
Lateral resolution
Temporal resolution

Cont.
• Axial resolution is resolution along the length of an ultrasound beam
A function of transducer frequency and pulse width
• Elevational resolution refers to the thickness of the ultrasound image: typically 8 to 10 mm
Cont. • Lateral resolution is a function of
ultrasound beam formation
The initial segment (near field) of an ultrasound beam is columnar
Beyond the near field, the beam diverges (far field)
Divergence is also a function of transducer frequency. As the frequency rises, the near field gets longer and the divergence angle decreases.

Cont.

Cont.
• Temporal resolution is the ability to accurately locate moving structures at a particular instant in time

• Attenuation :- a function of tissue absorption , divergence of ultrasound energy as it moves away from the transducer, reflection, and scattering

• Absorption is dependent on tissue type. For example, air absorbs more ultrasound energy than bone does, but bone absorbs more than blood or water does.
• Acoustic impedance :- refers to the resistance that an ultrasound wave meets when traveling though tissue
• The greater the tissue density, the faster the ultrasound beam moves through the tissue.
• Extent of ultrasound beam reflection is a function of the difference in acoustic impedance between two adjacent tissues larger the difference - the more ultrasound energy will be reflected
• Mismatches in acoustic impedance and attenuation are important to consider in imaging the heart
• For example, the upper aortic arch is difficult to visualize from the esophagus because
of interposition of the air-filled trachea. Most of the ultrasound energy that does make it to the trachea-tissue interface is reflected as a result of the large difference in acoustic impedance between air and tissue.
Integration of Flow and Structure
• Christian Doppler, a physicist, studied a band playing a specific pitch on a moving train – Doppler Shift
• Ultrasound that bounces off moving red blood cells is reflected back to the transducer at a slightly different frequency
• Shift in frequency allows the ultrasound machine to estimate blood flow velocity and direction of flow.
Cont.
• Doppler shifts are presented in three ways:
1. Pulsed Wave Doppler (PWD),
2. Continuous Wave Doppler (CWD), and
3. Color Flow Doppler (CFD).
• One limitation of PWD is that it may be too slow to capture the velocity of fast-moving blood cells. This phenomenon is known as aliasing.
• The limit at which the sampling rate fails to accurately capture the true velocity is called the Nyquist limit
• Aliasing of PWD occurs at blood flow velocities greater than 0.8 to 1.0 m/sec. Normal flow within the heart may reach 1.4 m/sec and pathologic flow up to 6 m/sec.

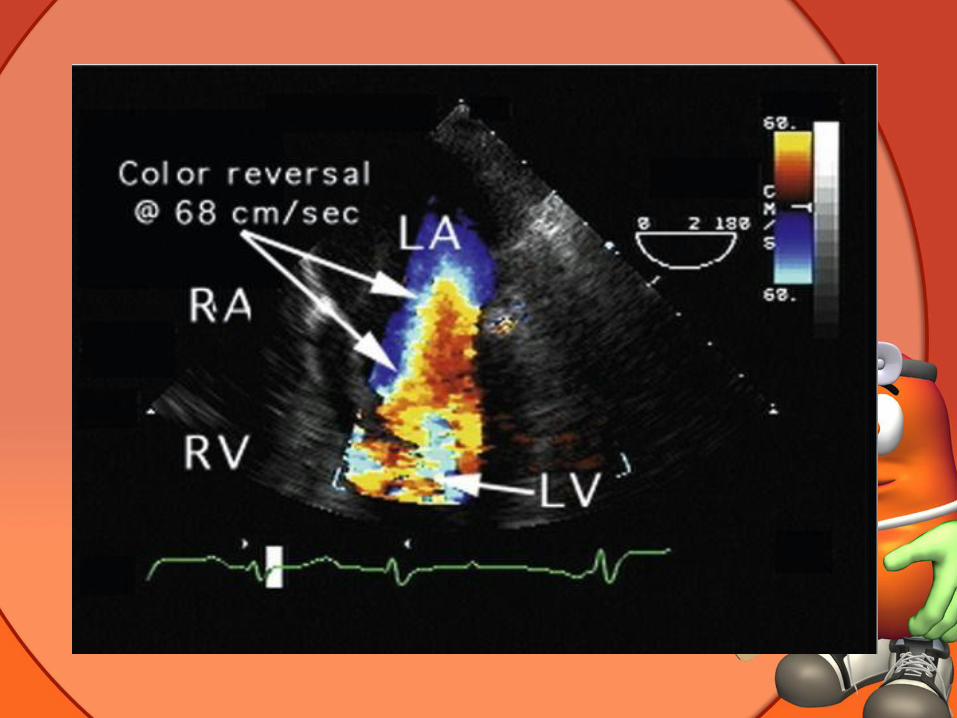
• CFD is based on PWD and uses multiple sample volumes along a scan line
• A color code is used to depict flow toward (red) and away (blue) from the transducer

Equipment Design and Operation
• A miniaturized echocardiographic transducer (about 40 mm long, 13 mm wide, and 11 mm thick) mounted on the tip of a gastroscope.
• Transducer is with 64 piezoelectric elements operating at 3.7 to 7.5 MHz

• Like standard
gastroscopes two
rotary knobs control
the movements

Contraindications
• Absolute
1. Previous esophagectomy,
2. Severe esophageal obstruction,
3. Esophageal perforation, and
4. Ongoing esophageal hemorrhage
Cont.
• Relative
1. Esophageal diverticulum,
2. Varices,
3. Fistula, and
4. Previous esophageal surgery, as well as a history of gastric surgery, mediastinal irradiation, unexplained swallowing difficulties
Patient preparation
• Informed consent
• Pt. should fast for at least 4 – 6 hrs
• Thorough history should be taken – any dysphagia
• i.v. access
• Pre oxygenation
• Suction should be available

Basic Transesophageal Examination
• Patient is anesthetized (topically)
• The contents of the stomach are suctioned
• Patient's neck is then extended and the well-lubricated TEE probe is introduced
• If the probe does not pass blindly, a laryngoscope can be used
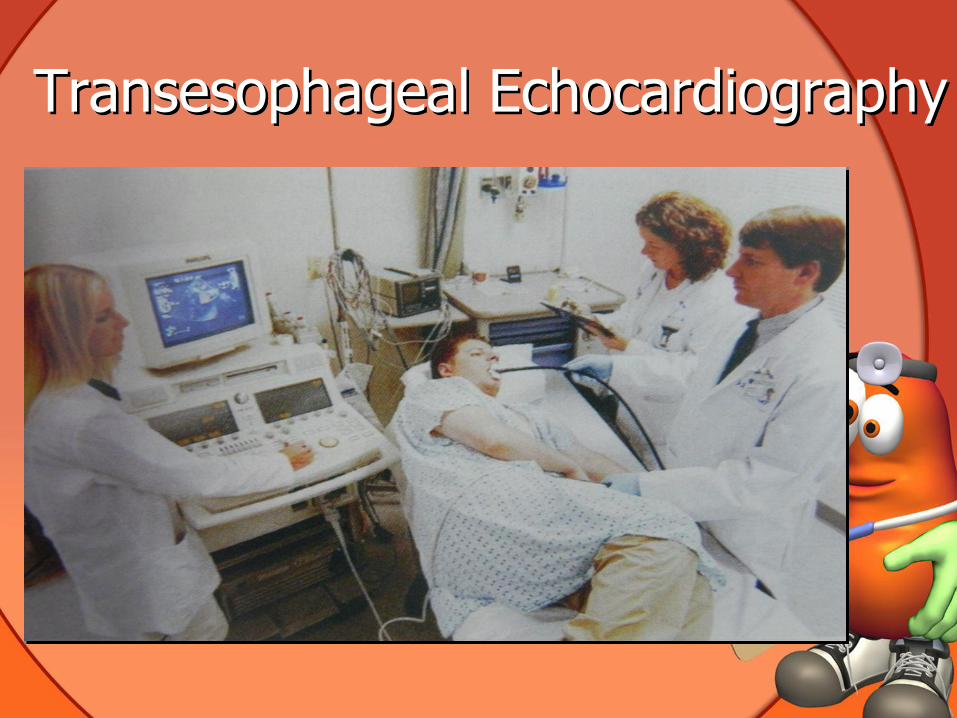
Transesophageal Echocardiography

Risks of TEE
• Topical anesthesia
Allergic reactions
Toxic methemoglobinemia
• Conscious sedation
Hypoxia
Hypotention
Agitation
Idiosyncratic reactions

Cont.
• Probe insertion : immediate
Oral trauma
Dental trauma
Esophageal trauma
Vagal reaction
• Probe insertion : delayed
Aspiration
Tachycardia – PSVT and VT
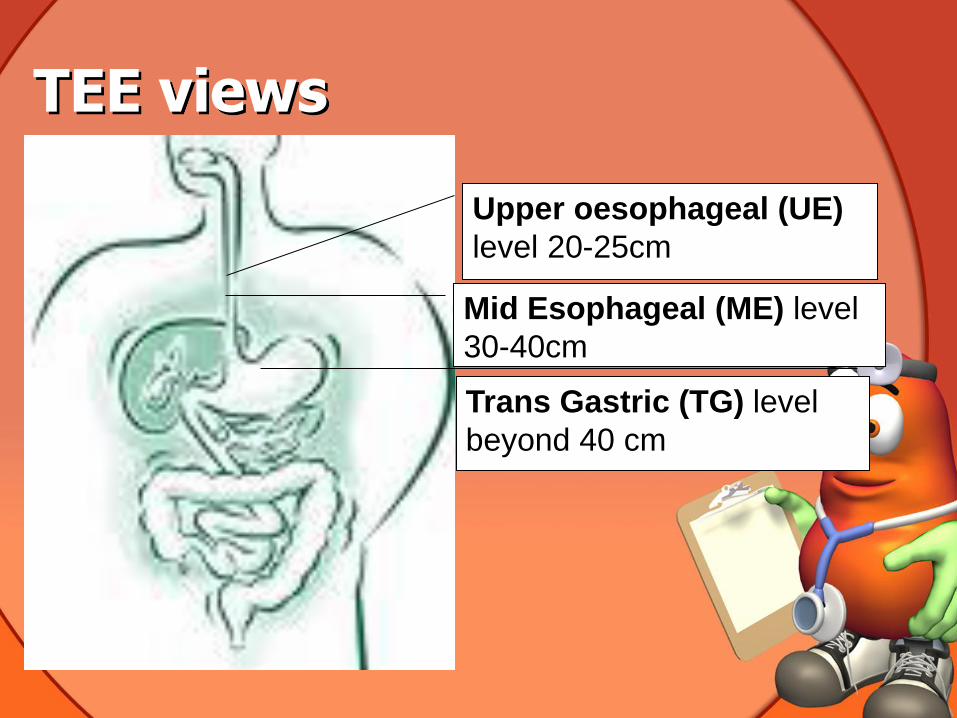
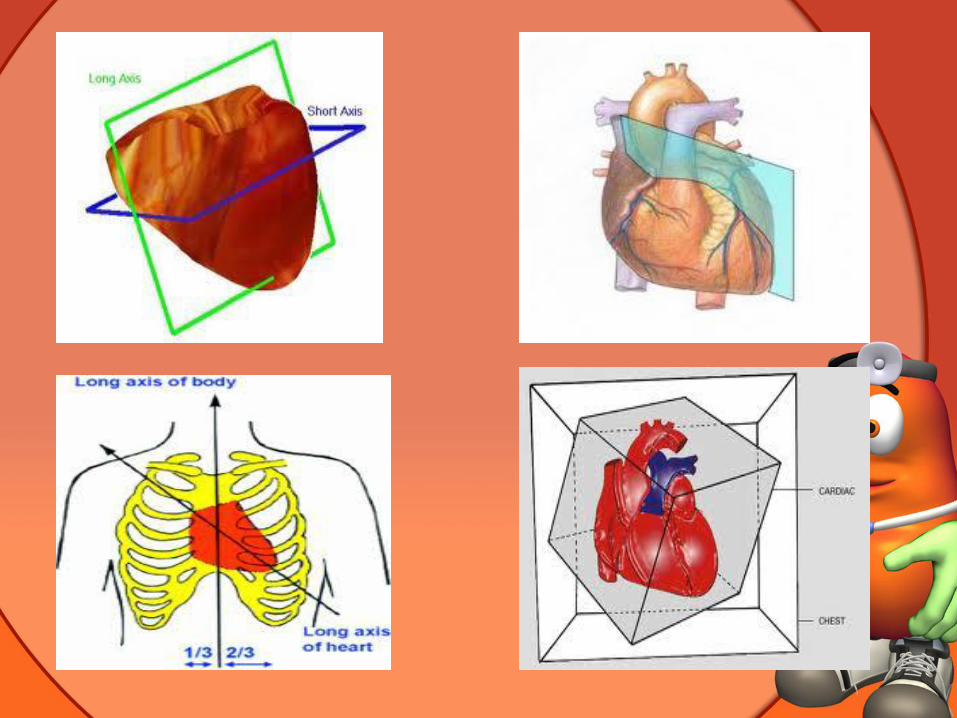
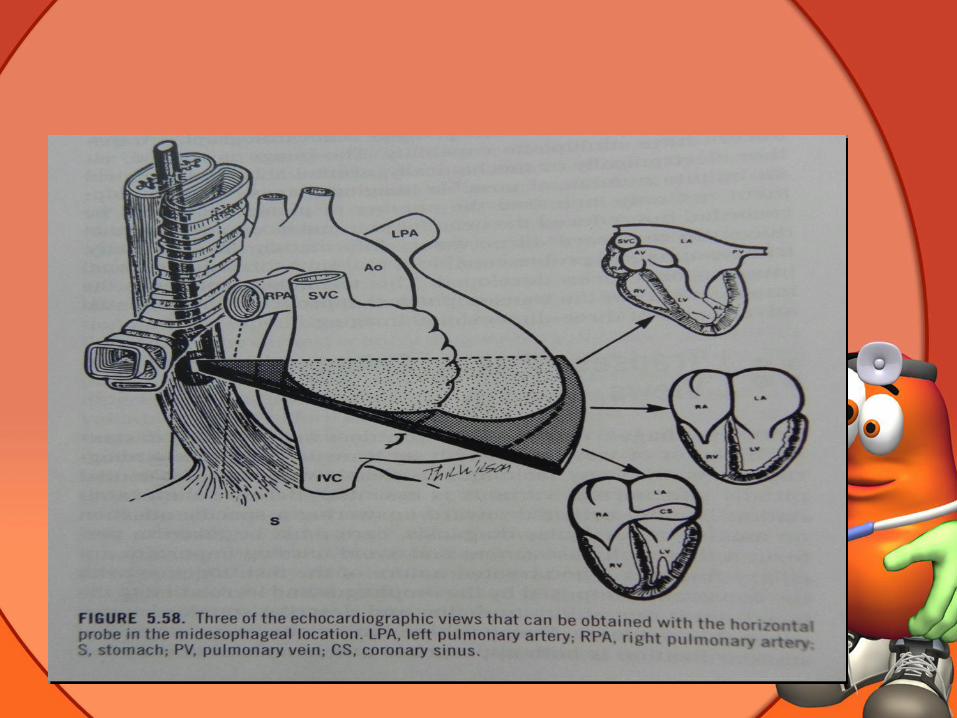
TEE views
Upper oesophageal (UE)
level 20-25cm
Mid Esophageal (ME) level
30-40cm
Trans Gastric (TG) level
beyond 40 cm

Different Views
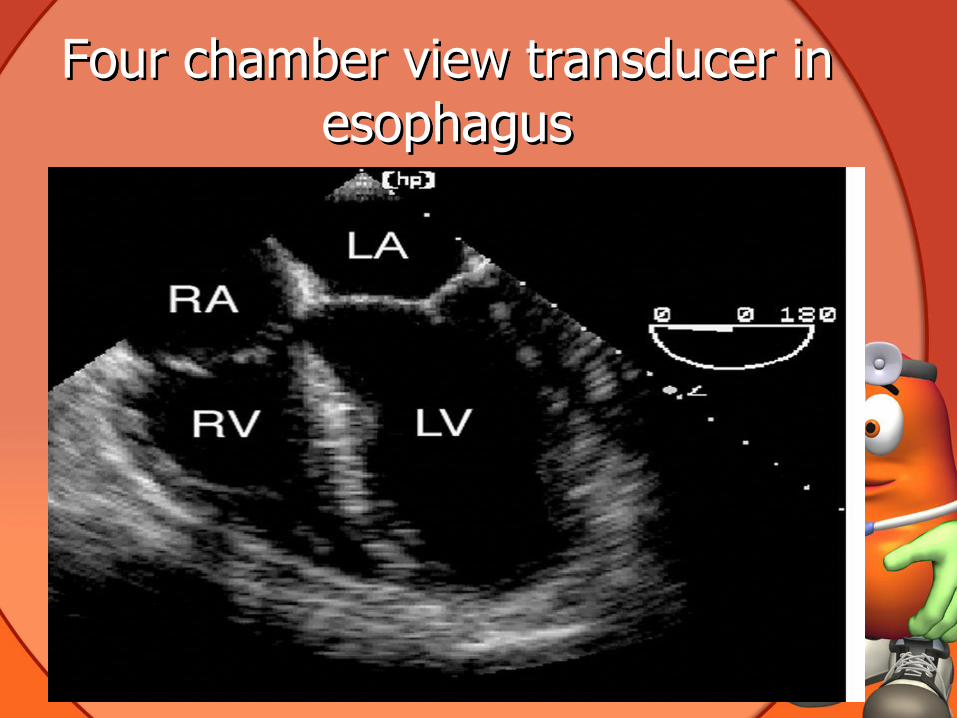
Four chamber view transducer in esophagus

4 of SAX views – Upper Esophagus

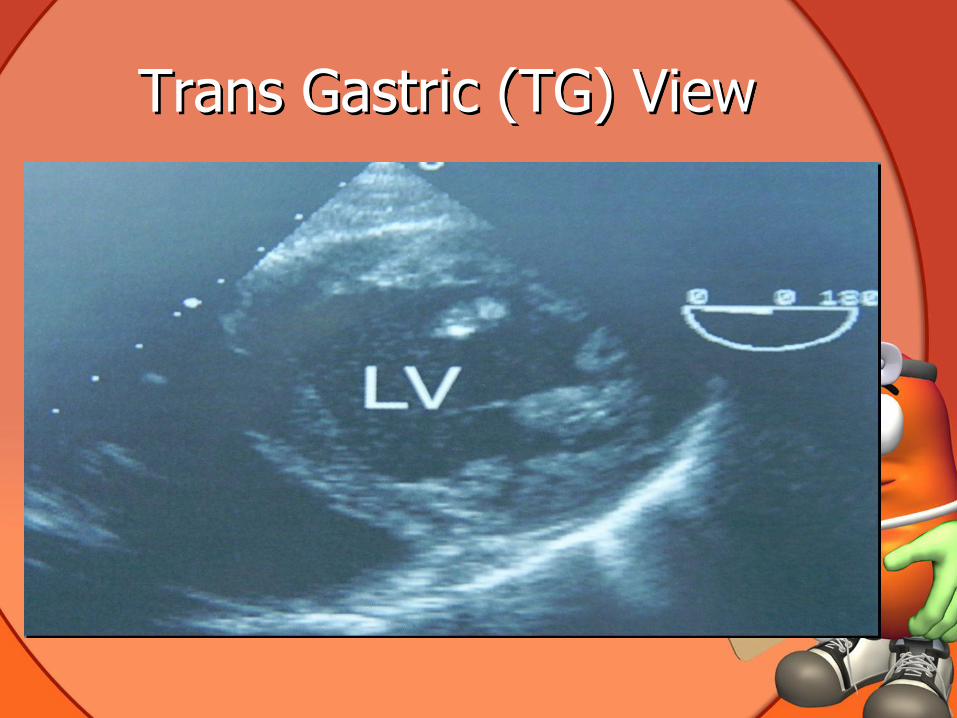
Trans Gastric (TG) View

Assessment of Hemodynamics
• Evaluation of Ventricular Filling
o TEE reveals changes in LV preload more
reliably than filling pressure
o TEE demonstrates a significant decrease in cross-sectional area at end diastole (EDA)
o An EDA of less than 12 cm2 indicates
hypovolemia
Cont.
• Estimation of Cardiac Output
o TEE can quantify cardiac output more
precisely
o By measuring both the velocity and the
cross-sectional area of blood flow at
appropriate locations in the heart or great
vessels

Cont.
• Assessment of Ventricular Systolic Function
Fractional area change (FAC) during systole
is a commonly used measure of global LV
function.
FAC = (EDA - ESA)/EDA
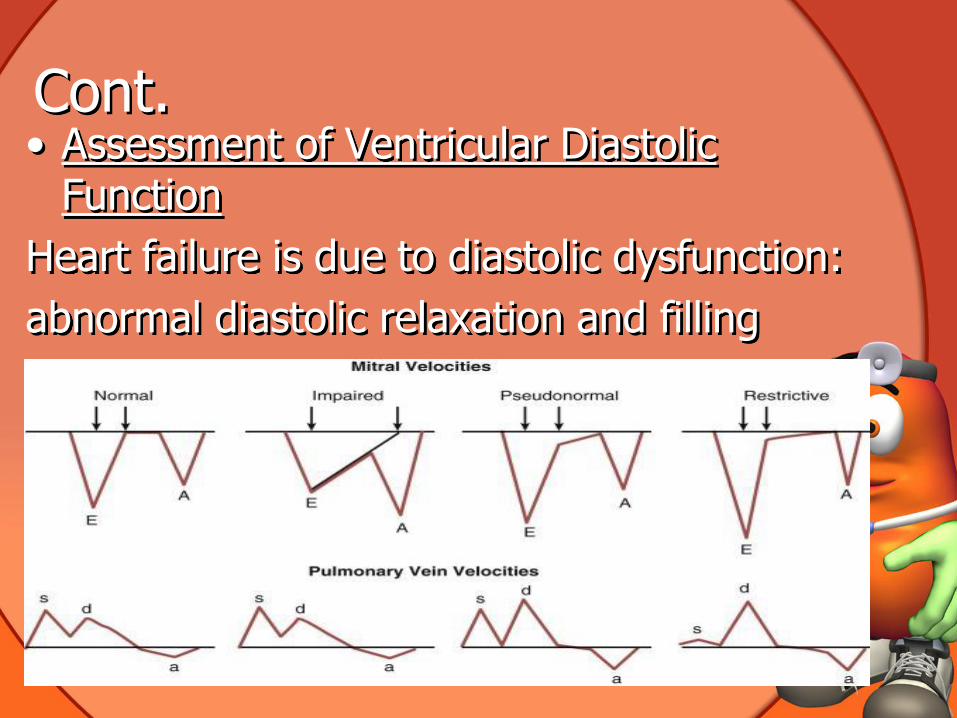
Cont. • Assessment of Ventricular Diastolic
Function
Heart failure is due to diastolic dysfunction:
abnormal diastolic relaxation and filling
Cont. • TEE During Life-Threatening Hypotension
Hypotension has only two possible causes:
inadequate cardiac output or
inappropriately low systemic vascular
resistance
Qualitative TEE estimates of ventricular
filling and function serve as practical guides for
the administration of fluids, inotropes, and
vasopressors
Detection of Myocardial Ischemia
• Within seconds after the onset of myocardial ischemia, affected segments of the heart cease contracting normally
• New intraoperative segmental wall motion abnormalities (SWMAs) diagnostic of myocardial ischemia
• Not all SWMAs are indicative of myocardial ischemia.

Cont.
• Myocarditis, myocardial infarction, and myocardial stunning also cause SWMAs.
• However,a sudden, severe decrease in segmental contraction is almost certainly due to myocardial ischemia.

Thank You…





























