Toxicity and Outcome of a Phase II Trial ofTaxane-Based Neoadjuvant Chemotherapy and3-Dimensional, Conformal, Accelerated Radiotherapyin Locally Advanced Nonsmall Cell Lung Cancer
Ana M. Rojas, MD, PhDBasil E. Lyn, BAElena M. Wilson, MDFrances J. Williams, MScNihal Shah, MDJeanette Dickson, MBMichele I. Saunders, MD
Marie Curie Research Wing, Mount Vernon Hos-pital, Northwood, Middlesex, United Kingdom.
BACKGROUND. The objective of this study was to evaluate prospectively the acute
and late adverse effects of taxane/carboplatin neoadjuvant chemotherapy and 3-
dimensional, conformal radiotherapy in patients with locally advanced nonsmall
cell lung cancer (NSCLC).
METHODS. Forty-two patients were entered into a nonrandomized Phase II study of
continuous, hyperfractionated, accelerated radiotherapy (CHART) week-end less
(CHARTWEL) to a dose of 60 grays (Gy). Three cycles of chemotherapy were given
over 9 weeks before radiotherapy. Dose escalation with paclitaxel was from 150 mg/
m2 to 225 mg/m2. Systemic toxicity to chemotherapy was monitored throughout.
Radiation-induced, early, adverse effects were assessed during the first 9 weeks from
the start of radiotherapy, and late effects were assessed from 3 months onward.
Overall survival, disease-free survival, and locoregional tumor control also were
monitored.
RESULTS. Twenty percent of patients failed to receive chemotherapy as planned, pri-
marily because of neutropenia. The incidence of Dische Dictionary Grade �2 and
Grade �3 dysphagia was 57.5% and 10%, respectively, with an average duration of
1.2 weeks and 1.5 days, respectively. By 9 weeks, <3% of patients were symptomatic;
and, eventually, all acute reactions were healed, and there has been no evidence of
consequential damage. At 6 months, the actuarial incidence of moderate-to-severe
pneumonitis was 10%. During this time, all patients were free of severe pulmonary
complications. Actuarial estimates of Grade �2 late lung dysfunction were 3% at
1 year, 10% at 2 years, and remained at this level thereafter. The actuarial 3-year
locoregional control and overall survival rates were 54% and 45%, respectively.
CONCLUSIONS. Neoadjuvant chemotherapy followed by 3-dimensional, conformal
CHARTWEL 60-Gy radiotherapy in patients with advanced NSCLC was feasible and
was tolerated well. Historic comparisons indicated that locoregional tumor control
is not compromised by the use of conformal techniques. Cancer 2006;107:1321–30.
� 2006 American Cancer Society.
KEYWORDS: continuous, hyperfractionated, accelerated radiotherapy week-endless, early morbidity, late morbidity, neoadjuvant chemotherapy, nonsmall-cell lungcancer, 3-dimensional conformal radiotherapy.
A nalyses of patterns of treatment failure indicate that local recur-
rence is a major cause of death in patients with advanced non-
small cell lung cancer (NSCLC) and underpins the belief that local
control is a prerequisite for improved survival.1–3 Bronchoscopic and
radiographic assessment of 353 randomized patients showed a 17%
rate of complete response at the primary site and, at best, a 20% 1-year
Supported by the Cancer Research Campaign UKand by the Mount Vernon Marie Curie ResearchTrust.
Address for reprints: Ana M. Rojas, MD, PhD, MarieCurie Research Wing, Mount Vernon Hospital, North-wood, Middlesex, HA6 2RN United Kingdom; Fax:(011) 44 1923844167; E-mail: [email protected]
Received April 28, 2006; revision received May31, 2006; accepted June 7, 2006.
ª 2006 American Cancer SocietyDOI 10.1002/cncr.22123Published online 10 August 2006 in Wiley InterScience (www.interscience.wiley.com).
1321

locoregional control rate after radical radiotherapy and
radiochemotherapy.4 The demonstration of a radiation
dose-response relation for NSCLC,5 together with the
realization that dose escalation with conventional ra-
diotherapy dose planning and delivery6 has a serious
risk of severe morbidity, has led to the design and eva-
luation of other approaches. Dose intensification to the
primary site has been attempted, for example, with the
use of accelerated, hyperfractionated radiotherapy and
a variety of radiochemotherapy protocols, with varying
degrees of success. More recently, the development of
3-dimensional conformal radiotherapy (3D-CRT) holds
considerable promise for improved locoregional con-
trol from dose escalation while maintaining acceptable
normal tissue effects.7,8
Both treatment acceleration and radiochemother-
apy, in particular concurrent, platinum-based regimens,
can improve treatment outcomes for patients with
NSCLC. For example, the continuous, hyperfractio-
nated, accelerated radiotherapy (CHART) regimen
produced a survival advantage of 9% at 2 years (eq-
uivalent to a 22% reduction in the risk of death) over
conventional 6-week radiotherapy,9 whereas a meta-
analysis of randomized trials of radiochemotherapy
showed a 13% reduction in the risk of death.10 Because
it is possible that an additional survival benefit may be
obtained by combining CHART or CHART-like regi-
mens with chemotherapy, a series of Phase I and II
nonrandomized studies of neoadjuvant chemotherapy
with the CHART week-end less (CHARTWEL) regimen
were undertaken at our center from 1997. The studies
showed that the addition of neoadjuvant chemother-
apy to CHARTWEL heightened acute dysphagia, but
the increase was transient, and there was no evidence
of long-term esophageal complications. Nearly 25% of
patients who received chemoradiotherapy had clinical
evidence of moderate pneumonitis, which was higher
than that observed among patients who received ra-
diation alone, but no signs of severe, late, clinical pul-
monary fibrosis were observed. Relative to late adverse
effects, the higher locoregional control rates observed
with CHARTWEL plus neoadjuvant chemotherapy sug-
gested the possibility of a therapeutic gain.11
More recently, the feasibility of delivering 3D-CRT
with the CHARTWEL regimen, which requires the use
of 3 treatments per day, was evaluated. In addition, the
incidence and severity of adverse effects when 3D-CRT
was combined with neoadjuvant chemotherapy was
monitored. Comparisons with the previous series should
provide a basis for determining whether further radia-
tion dose escalation and/or the introduction of con-
current radiochemotherapy protocols are feasible with
CHARTWEL. This article reports on normal tissue
responses and, as secondary endpoints, locoregional
tumor control and survival in patients with locally ad-
vanced, UICC Stage III or inoperable Stage I/II NSCLC.
Acute morbidity was assessed by scoring the incidence
and severity of dysphagia and the degree of analgesia
required by each patient during and after radiotherapy
for up to 9 weeks. Early and late pulmonary morbidity,
spinal cord morbidity, and esophageal morbidity were
assessed by using clinical and/or radiologic criteria.
Hematologic and gastrointestinal acute toxicity also was
monitored in patients who received chemotherapy.
MATERIALS AND METHODSFrom October 1999 to December 2003, 42 patients
were entered into a nonrandomized prospective study
of 3D-CRT CHARTWEL and neoadjuvant chemother-
apy. Patients who were not suitable for treatment with
chemotherapy because of comorbidity or who de-
clined chemotherapy received 3D-CRT CHARTWEL
alone to 60 grays (Gy). The local ethics committee
granted approval, and written informed consent was
obtained from each patient. Only patients age >18
years with histologically proven, inoperable NSCLC
confined to the thorax who were eligible for radical
radiotherapy and who had a World Health Organiza-
tion performance status of 0 or 1 were selected. Pre-
treatment lung function was assessed by measuring
the forced expiratory volume (FEV). In general, the
FEV in 1 second (FEV1) was >1.5 liters, but patients
who had an FEV1 of 1 to 1.5 liters were included in
the study at the physicians’ discretion. Prior to treat-
ment, patients also had a chest X-ray, bronchoscopy,
computed tomography (CT) scan of the chest, and his-
tology or brush cytology. Serum urea and electrolyte
levels, liver function tests, and ethylenediamine tetraa-
cetic acid (EDTA) clearance were obtained prior to the
first course of chemotherapy and subsequently if indi-
cated. Full blood counts were obtained before each
TABLE 1Patient Demographics and Tumor Staging
Parameter Value
No. of patients 42
Male:female ratio 32:10
Age, y
Range 48–88
Mean 66.8
Median 68.1
Stage
Stage IA 3
Stage IB 10
Stage IIB 6
Stage IIIA 6
Stage IIIB 16
Not known 1
1322 CANCER September 15, 2006 / Volume 107 / Number 6

course of chemotherapy. The presence of liver metasta-
ses was assessed biochemically and by CTor ultrasound
scans. Further investigations to exclude metastases in
other sites were carried out only if they were indicated
clinically.
CHARTWEL to 60 Gy was given in 40 fractions, at
1.5 Gy per fraction, 3 times per day (with a minimum
6-hour interfraction interval), in 15 fractions per week
over 18 to 19 days. Forty-two patients were planned
and treated with 3D-conformal radiotherapy either
alone (n ¼ 12 patients) or combined with chemother-
apy (n ¼ 30 patients). Demographic details and tumor
staging are shown in Table 1. In all, 28 squamous cell
carcinomas, 5 adenocarcinomas, 1 large cell carcinoma,
and 5 tumors characterized as NSCLC were identified
either by histologic and/or cytologic examination. In 3
patients, the histologic classification was not known.
A diagnostic CT scan of the chest and upper ab-
domen was obtained to aid interpretation of the plan-
ning CT scan. The patient was positioned supine with
shoulders and elbows held in flexion by using a metal
external immobilization frame, which was designed
and built in-house. A planning CT scan of the chest
that encompassed the whole of both lungs was then
obtained by using 5-mm contiguous and sequential
slices in quiet respiration. The scan was transferred to
the treatment-planning computer by Dicom link.12
3D-CRT treatment planning was then performed by
using PinnacleTM software (version 4.2f). Skin, lung,
and spinal cord were outlined on each slice through
the chest. Target volumes were defined according to
International Commission on Radiation Units and
Measurements Report 50.13 On each relevant slice, the
gross tumor volume (primary tumor and lymph node
disease; lymph nodes measuring >1 cm short axis) was
marked. Areas for elective lymph node irradiation, a
subset of the clinical target volume, also were marked.
The clinical target volume was determined by expand-
ing of the gross tumor volume by 5 mm to allow for mi-
croscopic invasion, as described in detail elsewhere12;
and the planning treatment volume was determined by
a further expansion of 5 mm to allow for set-up errors
and organ motion. Treatment was then delivered by
using 6-megavolt photons. The primary tumor and
known lymph node disease received a total dose of 60 Gy.
The Phase-1 volume encompassed the primary tu-
mor, the involved hilar and mediastinal lymph nodes,
and suspicious mediastinal lymph nodes (which
received elective lymph node irradiation). Lymph
nodes with a shortest axis >1 cm were considered to
contain metastatic disease. The Phase-2 volume com-
prised a boost dose to the primary tumor and to
known lymph node disease only. Some patients with
small peripheral tumors, in whom the involvement of
mediastinal lymph nodes was unlikely, and patients
who had relatively poor respiratory function were trea-
ted in a single Phase-2 technique. The esophagus gen-
erally was included in the Phase-1 volume and, if it
TABLE 2Scoring Criteria for Early and Late Morbidity *
Morbidity scores 0 1 2 3 4
Acute
Dysphagia None Discomfort on swallowing Soft diet Fluids only Severe difficulty
with fluids
Analgesia None Surface medicine Nonnarcotic medicines Narcotic medicines
Chronic
Dysphagia (stricture) None Caused by tumor Caused by radiotherapy Not known
Lung (clinical) None Symptoms not interfering
with lifestyle
Symptoms requiring treatment Hospitalized/house bound
Spinal cord None L’Hermittes Incomplete paraplegia Complete paraplegia
* Assessment according to the Dische Dictionary scoring system.
TABLE 3Hematologic Toxicity for Each of the 3 Cycles ofNeoadjuvant Chemotherapy
Schedule
(No. of patients)
Mean 6 SEM
Hb concentration
(g/dL)
Mean 6 SEM
WBC count
(3 109/L)
Mean 6 SEM
platelet count
(3 109/L)
MIC (n ¼ 8)
Cycle 1 13.7 6 0.8 7.9 6 0.7 356 6 25
Cycle 2 12.1 6 0.4 5.1 6 0.9 278 6 20
Cycle 3 11.9 6 0.6 4.5 6 0.3 235 6 27
P .06 .002 .002
Tax/Cb (n ¼ 16)
Cycle 1 13.8 6 0.4 9.6 6 0.8 335 6 23
Cycle 2 13.0 6 0.4 9.1 60.8 312 6 23
Cycle 2 12.1 6 0.4 6.9 6 0.5 232 6 25
P .01 .01 .003
SEM indicates standard error of the mean; Hb, hemoglobin; WBC, white blood cell; MIC, mitomycin
C, cisplatin, and ifosfamide; Tax/Cb, taxol plus carboplatin.
3-D Conformal Radiochemotherapy in NSCLC/Rojas et al. 1323
was located close to disease, in the Phase-2 volume,
particularly if there was aortal-pulmonary and subcar-
inal disease. Therefore, the esophagus received a dose
intermediate between that given in Phase 1 (37.5 Gy)
and the full tumor dose (60 Gy). No attempt was made
to avoid the esophagus. The organ was not outlined as
part of the 3D treatment-planning process, and esoph-
ageal dose-volume histograms were not constructed.
Neoadjuvant chemotherapy, which consisted of 3
cycles of paclitaxel plus carboplatin (area under the
concentration-time curve [AUC] � 6; note that the
AUC for EDTA clearance is AUC ¼ [glomerular filtra-
tion rate þ 25] mg/min), was given over 6 weeks be-
fore the start of 3D-CRT. Dose escalation with
paclitaxel was from 150 mg/m2 (n ¼ 5 patients), 175
mg/m2 (n ¼ 5 patients), 200 mg/m2 (n ¼ 6 patients),
and 225 mg/m2 (n ¼ 1 patient). Patients who had a
history of previous malignancy, poor respiratory func-
tion, and/or were to be treated with a single-phase
CRT technique were excluded a priori from the dose-
escalation study. Twelve patients fell into this category
and received mitomycin C (6 mg/m2) plus cisplatin
(50 mg/m2) combined with either ifosfamide (3 mg/
m2) or vinblastine (6 mg/m2). One patient who was
treated off-site was given gemcitabine together with
carboplatin (dose levels unknown). All but 1 patient (who
received 4 chemotherapy cycles) were given 3 cycles of
chemotherapy spaced at 3-weekly intervals and CRT,
which started 3 weeks after the 3rd cycle.
All patients received radiotherapy as planned. Af-
ter the start of radiotherapy, patients were seen weekly
for up to 9 weeks, subsequently at 3 months, every
3 months up to 2 years, twice yearly for up to 5 years,
and annually thereafter. During treatment and until
the acute reactions had settled, the severity of dyspha-
gia and the type of medication used were assessed by
using the Dische Dictionary scoring system, which is
summarized in Table 2.14 Two patients who had a pe-
ripheral presentation of the primary tumor were elimi-
nated from the analysis of esophageal damage and
analgesia, because the irradiation fields excluded the
mediastinum (both patients were in the radiation-
alone arm). The prevalence, incidence, and duration of
early adverse events at different levels of severity were
calculated for both dysphagia and analgesia.
Late radiation-induced adverse effects were as-
sessed initially every 3 months for up to 2 years, bi-
annually up to 5 years, and annually thereafter. At each
follow-up, a chest X-ray and/or CT scans were ob-
tained. Time-incidence curves and statistical compari-
sons were calculated by computing actuarial disease-
free intervals by using the product-limit (Kaplan–
Meier) method. Lung dysfunction was diagnosed by
both clinical and radiologic examination. Pneumonitis
was considered the transient, intermediate syndrome
that occurred during the first 6 months after the first
radiotherapy treatment, and late pulmonary toxicity
(lung fibrosis) as the syndrome evolving thereafter.
Locoregional control was attained if there was ei-
ther complete disappearance of all radiologic abnorm-
alities in the lung or when any residual abnormality
observed at 6 months remained stable for another 6
months or more. Patients who did not achieve this
were categorized as ‘‘never disease-free.’’ Overall sur-
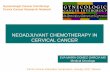
FIGURE 1. These graphs illustrateacute dysphagia and the degree of
analgesia required. Top. The preva-
lence of Grade �2 (circles), Grade�3 (triangles), and Grade 4 (squares)dysphagia is illustrated on the left,
and the prevalence of Grade �1 (cir-cles), Grade �2 (triangles), and Grade3 (squares) analgesia is illustrated on
the right. Error bars 6 1 standard
deviation (SD). Bottom: The incidence
of Grade �2 (solid bars) and Grade�3 (open bars) dysphagia and anal-gesia are illustrated on the left, and
the duration of dysphagia and analge-
sia are illustrated on the right. SEM
indicates standard error of the mean.
1324 CANCER September 15, 2006 / Volume 107 / Number 6

vival was calculated as the time from the first radio-
therapy treatment to death; patients who remained
alive were censored at the last date they were seen. Dis-
ease-free survival was calculated as the time between
the commencement of CHARTWEL and the first evi-
dence of locoregional recurrence or distant metastases
or the date of death from any other cause. Survival fits
were obtained by using the product-limit (Kaplan–
Meier) method.
RESULTSChemotherapy, as planned, was received by 80% of
patients. Dose reductions and/or delays between
chemotherapy cycles and/or the start of radiotherapy
were caused primarily by neutropenia. Three patients
had severe neutropenia after the first or second cycle
of mitomycin C, ifosfamide, and cisplatin (MIC),
whereas another patient presented with severe to
life-threatening neutropenia after the first cycle of
paclitaxel/carboplatin therapy and was hospitalized
because of neutropenic sepsis. All these events were
managed and resolved with standard medical proce-
dures. The median time from the last chemotherapy
cycle and the start of radiotherapy was 33 days. Table 3
summarizes the mean values for hemoglobin concen-
trations, white blood cell counts, and platelet counts
throughout chemotherapy for 24 patients who received
either MIC (n ¼ 8 patients) or paclitaxel/carboplatin
(n ¼ 16 patients). There was a progressive reduction in
all 3 parameters that was significant for all compari-
sons except for hemoglobin in patients who received
MIC. Six patients were treated elsewhere and had no
toxicity data available. Severe nonhematologic morbid-
ity was not encountered in this series. There were 2
events of mild peripheral neuropathy (Patients 169
and 173), and there was 1 event of moderate neuropa-
thy (Patient 173): Both patients were receiving pacli-
taxel/carboplatin chemotherapy.
Figure 1 shows the prevalence of acute esophageal
reactions for 3 levels of severity (Grades �2, �3, and 4)
and of the type of medication (i.e., topical, nonnarco-
tic, narcotic) that was used to ameliorate the symp-
toms during the first 9 weeks after the start of 60-Gy
CHARTWEL in 40 patients who were treated with or
without adjuvant chemotherapy (2 patients were
excluded from the analysis). For moderate or worse
levels of dysphagia (i.e., Grade �2), the peak preva-
lence was observed at approximately 3 to 4 weeks after
the start of radiotherapy and was followed by a rapid
decline in the proportion of symptomatic patients, so
that, by 9 weeks, the prevalence of acute esophageal
reactions was <3%. For more severe levels of morbidity
(i.e., Grades �3 and 4), the response was shallower and
less time-dependent. Similar conclusions can be drawn
from the analysis of analgesia. The incidence and dura-
tion of Grade 2 or worse and Grade 3 or worse dyspha-
gia and the incidence and duration of Grade 2
analgesia (i.e., the use of nonnarcotic or worse analge-
sia) and Grade 3 analgesia (i.e., narcotic analgesia) also
are shown. Virtually 60% of patients had moderate-to-
severe dysphagia, but severe or worse dysphagia was
present in only 10% of patients during this 9-week ob-
servation period: All of these patients received narcotic
medication. On average, Grade 2 or worse reactions
lasted for 1.2 6 0.2 weeks (6 1 standard error of the
mean), whereas Grade 3 or worse reactions lasted for
1.4 6 0.1 days. At all times during follow-up, the preva-
lence, incidence, and duration of reactions in the
12 patients who received radiation alone were consid-
erably lower compared with those among the patients
who received chemotherapy, however, the differences
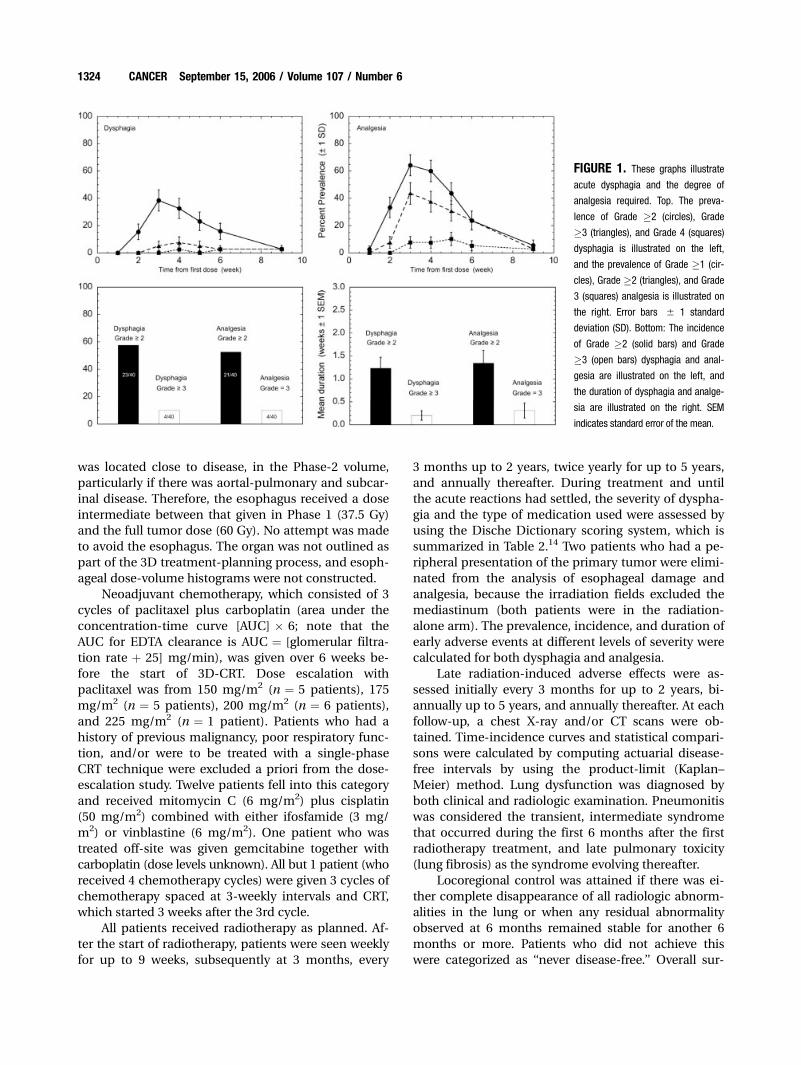
FIGURE 2. These charts illustrate the actuarial incidence of Grade �2(dashed lines) and Grade 3 (solid lines) early pneumonitis (top) and late lung
dysfunction (bottom).
3-D Conformal Radiochemotherapy in NSCLC/Rojas et al. 1325

were not significant, probably because of the small
number of patients in the radiation-alone arm (data
not shown).
The proportion of patients who were free of clini-
cal symptoms of pneumonitis and late lung dysfunc-
tion is shown in Figure 2. At 6 months, 29% of
patients had some sign and/or symptom of clinical
pneumonitis (i.e., Grade 1 or worse; curve not shown),
whereas moderate-to-severe pneumonitis was ob-
served in 10% of patients. Moreover, all patients were
free of severe complications (Grade 3) throughout this
time. The actuarial incidence of Grade 2 or worse late
lung morbidity was 3% at 1 year, rose to 10% at
2 years, and remained at that level for the remaining
time. Only 1 patient in this series presented with
severe pulmonary symptoms, which occurred 3 years
after treatment, yielding an actuarial Grade 3 morbid-
ity estimate of 7%.
The correlation between the percent volume of the
lung that receives �20 Gy (V20) or mean radiation dose
to the lung (MLD) and the severity of pneumonitis or
late lung dysfunction is shown in Figure 3. Within the
relatively narrow range of V20 (11–40%) and MLD (6.8–
21.7 Gy), the data show little indication of an increase
in the severity of damage with increasing parameter
values, particularly for pneumonitis. There was a good
correlation between V20 and MLD (r ¼ 0.75; P< .0001).
Treatment outcomes were assessed by means of
locoregional tumor control, disease-free survival, and
overall survival and are illustrated in Figure 4. The ac-
tuarial rates at 1 year, 2 years, and 3 years for locore-
gional tumor control, disease-free survival, and overall
survival were 76%, 61%, and 54% (locoregional con-
trol);, 74%, 48%, and 39% (disease-free survival), and
81%, 57%, and 45% (overall survival), respectively. To
date, no deaths have been attributable directly to
radiation-induced damage. Actuarial analyses of over-
all survival and metastases-free survival in patients
who did and did not attain control of their primary tu-
mor was carried out and also are shown in Figure 4.
Control of local disease had a significant impact on
survival: At 2 years, the overall survival rate was 67%
compared with 47% (P ¼ .05; log-rank test), and the
metastases-free survival rate was 67% compared with
43% (P ¼ .03; log-rank test) for patients who achieved
and did not achieve control of their primary tumor
site, respectively.
DISCUSSIONThe current data indicate that the dose-escalation sched-
ule of neoadjuvant chemotherapy with CHARTWEL to
60 Gy planned and delivered by using 3D-conformal
techniques is feasible and well tolerated. Compliance to
3 cycles of neoadjuvant chemotherapy (80%) was in the
lower range of that reported in other nonrandomized
trials of chemotherapy combined with 3D-CRT.15–17
Severe, radiation-induced, acute toxicity was mini-
mal and of short duration. The extent and duration
of all levels of early dysphagia was considerably less
FIGURE 3. The percent of lung vol-ume that received a radiation dose �20grays (Gy) (left graphs) and the mean
dose to the lung (right graphs) were
plotted against pneumonitis by grade
(top) or by late lung dysfunction (bottom).
Correlation coefficients (r) obtained from
the linear regression fits varied from
r ¼ 0.17 to r ¼ 0.43.
1326 CANCER September 15, 2006 / Volume 107 / Number 6

than that observed previously in patients who received
treatment in this center using nonconformal CHARTWEL
radiotherapy. Although there was no a priori intention
to spare the esophagus, the ability to delineate signifi-
cantly shorter superior-inferior lengths with conformal
techniques, relative to nonconformal delivery, for both
large and small volumes (P � .03) may explain the re-
duced mucositis. To date, there is no evidence of radia-
tion-induced, late damage to the esophagus. Likewise,
pulmonary morbidity was low. Moderate pneumonitis
(assessed during the first 6 months) developed in 10%
of patients, and severe pneumonitis developed in none
of the patients. The actuarial incidence of patients with
moderate or worse late lung dysfunction was 3% at 1
year and rose to 10% at 2 years. No events of severe
late symptoms were observed during that time. To
date, randomized comparisons of therapeutic gains
with CRT are not available. Bearing in mind all the
caveats associated with comparisons made using his-
toric controls from nonrandomized studies, our 3D-
CRT data relative to nonconformal techniques11 show
reduced incidence of adverse effects, particularly com-
pared with nonconformal CHARTWEL plus chemo-
therapy. These observations, namely, the reduced adverse
effects with CRT and their exacerbation by neoadjuvant
or concurrent chemotherapy, are well documented.8,18–20
Feasibility trials of 3D-CRT therapy that, like the
current trial, had the primary objective of evaluating
radiation adverse effects, are summarized in Table 4.
Because of differences in the scoring systems, methods
of analyses, variability in timing, and frequency of fol-
low-up, it is difficult to make valid cross-comparisons
between series. Comparing incidence rates of acute
morbidity may be straight forward enough. However,
such a comparison assumes that patients are scored at
the time during which peak reactions occur. Generally,
patients are seen once per week during radiotherapy, a
gap long enough for peak reactions to occur and even
resolve. Furthermore, this approach does not consider
the time spent at a particular reaction level. Determin-
ing this parameter or, equally, determining prevalence
over an appropriate observation period is akin to
defining an area under the curve; from it, the time of
onset of the reaction and, most important, the kinetics
of the recovery phase can be obtained and should be a
more reliable estimate of toxicity. In addition, it
enables the clinician to identify the patients who are at
risk of sustaining consequential damage. Two relatively
recent reviews discussed in detail the complexities
associated with normal tissue analyses and report-
ing.21,22 Because of the continually evolving nature of
radiation damage, late effects are far more difficult to
record and report, and many series suffer from paucity
of data and from suboptimal analytic methodology
FIGURE 4. Actuarial survival curves. Top: Locoregional (LRC) tumor control(solid line), disease-free survival (DFS) (dotted line), and overall survival
(dashed line) are illustrated. Middle: Overall survival is illustrated in patients
who maintained permanent tumor control (solid line) and in patients who
never attained or lost control of the primary tumor (dashed line) (log-rank
P ¼ .05). Bottom: Metastases-free survival is illustrated in patients whoattained permanent tumor control (solid line) and in patients who never
attained or lost control of the primary tumor (dashed line) (log-rank P ¼ .03).
3-D Conformal Radiochemotherapy in NSCLC/Rojas et al. 1327

and reporting.21,23 It is disconcerting that crude inci-
dence rates still are in use in an appreciable number of
reports. This can underestimate the real incidence sig-
nificantly, because it considers all patients included in
the study and not just those at risk from suffering the
event. Cumulative incidence is an improved method;
however, the actuarial analysis is considered the me-
thod of choice. Albeit and as shown in Table 4, our
results for early incidence of esophagitis and actuarial
estimates for late effects compare favorably with those
reported by others. Bearing in mind the extremely
accelerated nature of the CHARTWEL regimen, it is
noteworthy that a relatively low incidence of severe
esophageal toxicity was encountered, and late esopha-
geal complications were completely absent. Likewise,
there is no evidence of spinal cord or late normal tis-
sue complications in other organs at risk.
Both V20 and MLD have been proven to be useful
predictors of radiation-induced pneumonitis. In the
current study, no correlation was observed between the
severity of lung complications and either V20 or MLD.
However, the volumes of lung irradiated to �20 Gy var-
ied from 11% to 40%, and MLD did not exceed 22 Gy.
The upper limits for both parameters were lower than
those reported in other published series,.6,24,25 which
demonstrated that a threshold must be exceeded be-
fore the predictive value becomes apparent.
Because of the nonrandomized nature of the stu-
dies conducted to date and the small number of pa-
tients treated by most centers, estimates of treatment
outcome with 3D-CRTare not robust and, thus, should
be interpreted with caution. Tables 5 and 6 illustrate that
the 1-year, 2-year, and 3-year actuarial estimates of local
tumor control and overall survival for neoadjuvant
CHARTWEL are in good agreement with outcome esti-
mates from other studies. Although CHARTWEL delivers
a relatively low total radiation dose, it still achieves good
control of disease and survival. The precursor of
CHARTWEL (i.e., CHART, an even more accelerated
regimen up to 54 Gy in 12 days), in a randomized set-
ting, produced an absolute survival advantage of 9% at
TABLE 4Incidence of Severe Early and Late Esophageal and Pulmonary Complications in Trials of Conformal RadiotherapyAlone or Combined with Chemotherapy
No. of patients Dose, Gy Time, Weeks
Complications (% of patients)
Reference
Esophagus Lung
Early Late Early Late
45 52.2–72 6–8 2 0 9* Armstrong et al., 19977
55 60.8–87.8 6 0 0 6* Belderbos et al., 200328
177 70.9–90.3 7–8 0 �8 �9 �16 Bradley et al., 200530
91 73.6–80 11 3 Maguire et al., 199929
44 73.6–86.4 4–5 8–14 0–8 0 0–25 Marks et al., 200431
62 60–74 6–7.5 10 0 Rosennman et al., 200216
104 70.2–90 8–9 0–10 0 5–43 10–34 Rosenzweig et al., 200532
152 50–81 6–8 3 15* Sim et al., 200117
207 60–74 6–7 5 6 Singh et al., 200333
25 78–90 8–9 16 12 0 4 Socinski et al., 200434
62 60–74 6–8 8 0 0 0 Socinski et al., 200235
38 60 6 15 3 27 0 Willner et al., 200136
68 31–80 0–19 0–11 0–4 4 Wolski et al., 200537
Gy indicates grays.
* The report did not make it clear whether this was early or late lung morbidity.
TABLE 5Locoregional Control Rates in Trials of Conformal Radiotherapy Aloneor Combined with Neoadjuvant and/or Concurrent Chemotherapy
No. of
patients
CT (No. of
patients)
LCR (%)
Reference1 year 2 years 3 years
177 25 61–92 50–78 Bradley et al.,
200530
106 20 58 40 31 Kong et al., 200538
146 146 65 42 �39* Lee et al., 200315
104 16 27–84 Rosenzweig
et al., 200532
37 NS 62 23 23 Sibley et al., 199539
82 82 �77* 43 �38* Sim et al., 200117
70 0 �59* 35 �32* Sim et al., 200117
58y 41 77 41 26 Wolski et al., 200537
42 30 76 61 54 Current study
LCR indicates locoregional control; CT, chemotherapy; NS, not specified.
* Read off from graph.y Included only patients with Stage III disease.
1328 CANCER September 15, 2006 / Volume 107 / Number 6

2 years compared with 6 weeks of conventional radio-
therapy. The contention that a ‘‘tumorocidal effect’’ is
obtained by shortening the overall treatment time
(and, thus, minimizing compensatory proliferation) is
underpinned by the findings of Fowler and Chappell,
who showed that NSCLC tumors can repopulate dur-
ing treatment with a potential doubling time of ap-
proximately 3 days.26 A recent retrospective analysis of
3 prospective Radiation Therapy Oncology Group trials
showed that prolonged treatment time was associated
with poorer survival (P ¼ .02): Those authors reported
a 2% increase in the risk of death for each day that
treatment was prolonged.27
Despite advances in the treatment of locally ad-
vanced NSCLC, outcomes remain disappointing, and
local recurrence and distant metastases remain the
major causes of death. Previous studies have demon-
strated that patients with locally controlled disease
have a significant advantage in terms of overall survival
and metastases-free survival compared with patients
who either lost or never achieved control of the pri-
mary tumor.3,5 Perhaps the widely held view that con-
trol of primary disease is the prerequisite to improving
survival may be achieved with the use of CRT based on
the unproven assumption that dose escalation would
achieve improved locoregional control while maintain-
ing acceptable morbidity.
In general, concurrent radiochemotherapy appears
to achieve higher tumor control and survival rates than
neoadjuvant treatments10; therefore, future investiga-
tions at our center will combine neoadjuvant and
concomitant chemotherapy. Unfortunately, the clini-
cal results indicate that it is unlikely that any combina-
tion of radiotherapy with the drugs currently available
will lead to dramatic improvements in treatment out-
come. Furthermore, most studies have shown that
normal tissue affects are more severe with radioche-
motherapy schedules20 and reduce the therapeutic
benefit. The very low level of both early and late mor-
bidity encountered with CHARTWEL using conformal
delivery and the high regional control and survival
observed in these patients indicate that dose-escala-
tion protocols of conformal CHARTWEL radiotherapy
alone and combined with chemotherapy, coupled with
stratification of patients by known risk factors,24,28,29
warrant evaluation.
REFERENCES1. Arriagada R, Le Chevalier T, Quoix E, et al. ASTRO (American
Society for Therapeutic Radiology and Oncology) plenary:
effect of chemotherapy on locally advanced non-small cell
lung carcinoma: a randomized study of 353 patients. GETCB
(Groupe d’Etude et Traitement des Cancers Bronchiques),
FNCLCC (Federation Nationale des Centres de Lutte Contre
le Cancer) and the CEBI trialists. Int J Radiat Oncol Biol Phys.
1991;20:1183–1190.
2. Cox JD, Yesner RA. Causes of treatment failure and death in
carcinoma of the lung. Yale J Biol Med. 1981;54:201–207.
3. Saunders M, Dische S, Barrett A, et al. Continuous hyper-
fractionated accelerated radiotherapy (CHART) versus con-
ventional radiotherapy in non-small-cell lung cancer: a
randomised multicentre trial. CHART Steering Committee.
Lancet 1997;350:161–165.
4. Le Chevalier T, Arriagada R, Quoix E, et al. Radiotherapy alone
versus combined chemotherapy and radiotherapy in nonre-
sectable non-small-cell lung cancer: first analysis of a rando-
mized trial in 353 patients. J Natl Cancer Inst. 1991;83:417–423.
5. Perez CA, Bauer M, Edelstein S, et al. Impact of tumor control
on survival in carcinoma of the lung treated with irradiation.
Int J Radiat Oncol Biol Phys. 1986;12:539–547.
6. Kwa SL, Lebesque JV, Theuws JC, et al. Radiation pneumonitis
as a function of mean lung dose: an analysis of pooled data
of 540 patients. Int J Radiat Oncol Biol Phys. 1998;42:1–9.
7. Armstrong J, Raben A, Zelefsky M, et al. Promising survival
with three-dimensional conformal radiation therapy for
non-small cell lung cancer. Radiother Oncol. 1997;44:17–22.
8. Patel RR, Mehta M. Three-dimensional conformal radio-
therapy for lung cancer: promises and pitfalls. Curr Oncol
Rep. 2002;4:347–353.
9. Saunders M, Dische S, Barrett A, et al. Continuous, hyper-
fractionated, accelerated radiotherapy (CHART) versus con-
ventional radiotherapy in non-small cell lung cancer: mature
data from the randomised multicentre trial. CHART Steering
Committee. Radiother Oncol. 1999;52:137–148.
TABLE 6Overall Survival Rates in Nonrandomized Trials of ConformalRadiotherapy Alone or Combined with Neoadjuvant and/orConcurrent Chemotherapy
No. of
patients
CT (No. of
patients)
OS rate (%)
Reference1 year 2 years 3 years
45 0 32 Armstrong et al.,
19977
177 25 59–75 20–50 Bradley et al., 200530
207 95 59 41 Bradley et al., 200240
106 20 61 37 23 Kong et al., 200538
146 146 51 25 �18* Lee et al., 200315
44 44 47 Marks et al., 200431
62 62 71 50 38 Rosennman
et al., 200216
104 16 21–71 Rosenzweig
et al., 200532
37 NS 75 37 �28* Sibley et al., 199539
82 82 �75* �31* �25* Sim et al., 200117
70 0 �50* �23* �16* Sim et al., 200117
25 25 69 46 Socinski et al.,
200434
62 62 71 52 40 Socinski et al.,
200135
34 34 73 34 Willner et al., 200136
58y 41 44 27 12 Wolski et al., 200537
42 30 81 57 45 Current study
OS indicates overall survival; CT, chemotherapy; NS, not specified.
* Read off from graph.y Included only patients with Stage III disease.
3-D Conformal Radiochemotherapy in NSCLC/Rojas et al. 1329

10. Non-Small Cell Lung Cancer Collaborative Group. Chemo-
therapy in non-small cell lung cancer: a meta-analysis using
updated data on individual patients from 52 randomised
clinical trials. BMJ. 1995;311:899–909.
11. Saunders MI, Rojas A, Lyn BE, et al. Dose-escalation with
CHARTWEL (continuous hyperfractionated accelerated radio-
therapy week-end less) combined with neo-adjuvant chemo-
therapy in the treatment of locally advanced non-small cell
lung cancer. J Clin Oncol. 2002;14:352–360.
12. Wilson EM, Williams FJ, Lyn BE, et al. Validation of active
breathing control in patients with non-small-cell lung can-
cer to be treated with CHARTWEL. Int J Radiat Oncol Biol
Phys. 2003;57:864–874.
13. International Commission on Radiation Units and Measure-
ments. Prescribing, recording, and reporting photon beam
therapy (ICRU Report 50). Bethesda, MD: International
Commission on Radiation Units and Measurements; 1993.
14. Dische S, Warburton MF, Jones D, et al. The recording of
morbidity related to radiotherapy. Radiother Oncol. 1989;16:
103–108.
15. Lee SW, Choi EK, Lee JS, et al. Phase II study of three-
dimensional conformal radiotherapy and concurrent mito-
mycin-C, vinblastine, and cisplatin chemotherapy for Stage
III locally advanced, unresectable, non-small-cell lung can-
cer. Int J Radiat Oncol Biol Phys. 2003;56:996–1004.
16. Rosenman JG, Halle JS, Socinski MA, et al. High-dose confor-
mal radiotherapy for treatment of Stage IIIA/IIIB non-small-
cell lung cancer: technical issues and results of a Phase I/II
trial. Int J Radiat Oncol Biol Phys. 2002;54:348–356.
17. Sim S, Rosenzweig KE, Schindelheim R, et al. Induction
chemotherapy plus three-dimensional conformal radiation
therapy in the definitive treatment of locally advanced non-
small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2001;51:
660–665.
18. Bradley J, Movsas B. Radiation esophagitis: predictive fac-
tors and preventive strategies. Semin Radiat Oncol. 2004;14:
280–286.
19. Byhardt RW. The evolution of Radiation Therapy Oncology
Group (RTOG) protocols for nonsmall cell lung cancer. Int J
Radiat Oncol Biol Phys. 1995;32:1513–1525.
20. Byhardt RW, Scott C, Sause WT, et al. Response, toxicity, fail-
ure patterns, and survival in five Radiation Therapy Oncol-
ogy Group (RTOG) trials of sequential and/or concurrent
chemotherapy and radiotherapy for locally advanced non-
small-cell carcinoma of the lung. Int J Radiat Oncol Biol
Phys. 1998;42:469–478.
21. Bentzen SM, Dorr W, Anscher MS, et al. Normal tissue
effects: reporting and analysis. Semin Radiat Oncol. 2003;13:
189–202.
22. Trotti A. Toxicity in head and neck cancer: a review of trends
and issues. Int J Radiat Oncol Biol Phys. 2000;47:1–12.
23. Trotti A, Bentzen SM. The need for adverse effects reporting
standards in oncology clinical trials. J Clin Oncol. 2004;22:
19–22.
24. Graham MV, Purdy JA, Emami B, et al. Clinical dose-volume
histogram analysis for pneumonitis after 3D treatment for
non-small cell lung cancer (NSCLC). Int J Radiat Oncol Biol
Phys. 1999;45:323–329.
25. Graham MV, Purdy JA, Emami B, et al. Preliminary results of
a prospective trial using three dimensional radiotherapy for
lung cancer. Int J Radiat Oncol Biol Phys. 1995;33:993–1000.
26. Fowler JF, Chappell R. Non-small cell lung tumors repopu-
late rapidly during radiation therapy. Int J Radiat Oncol Biol
Phys. 2000;46:516–517.
27. Machtay M, Hsu C, Komaki R, et al. Effect of overall treat-
ment time on outcomes after concurrent chemoradiation
for locally advanced non-small-cell lung carcinoma: analy-
sis of the Radiation Therapy Oncology Group (RTOG) expe-
rience. Int J Radiat Oncol Biol Phys. 2005;63:667–671.
28. Belderbos JS, De Jaeger K, Heemsbergen WD, et al. First
results of a Phase I/II dose escalation trial in non-small cell
lung cancer using three-dimensional conformal radiother-
apy. Radiother Oncol. 2003;66:119–126.
29. Maguire PD, Sibley GS, Zhou SM, et al. Clinical and dosi-
metric predictors of radiation-induced esophageal toxicity.
Int J Radiat Oncol Biol Phys. 1999;45:97–103.
30. Bradley J, Graham MV, Winter K, et al. Toxicity and outcome
results of RTOG 9311: a Phase I-II dose-escalation study
using three-dimensional conformal radiotherapy in patients
with inoperable non-small-cell lung carcinoma. Int J Radiat
Oncol Biol Phys. 2005;61:318–328.
31. Marks LB, Garst J, Socinski MA, et al. Carboplatin/paclitaxel
or carboplatin/vinorelbine followed by accelerated hyperfrac-
tionated conformal radiation therapy: report of a prospective
Phase I dose escalation trial from the Carolina ConformalTherapy Consortium. J Clin Oncol. 2004;22:4329–4340.
32. Rosenzweig KE, Fox JL, Yorke E, et al. Results of a Phase I
dose-escalation study using three-dimensional conformal
radiotherapy in the treatment of inoperable nonsmall cell
lung carcinoma. Cancer. 2005;103:2118–2127.
33. Singh AK, Lockett MA, Bradley JD. Predictors of radiation-
induced esophageal toxicity in patients with non-small-cell
lung cancer treated with three-dimensional conformal
radiotherapy. Int J Radiat Oncol Biol Phys. 2003;55:337–341.
34. Socinski MA, Morris DE, Halle JS, et al. Induction and con-
current chemotherapy with high-dose thoracic conformal
radiation therapy in unresectable Stage IIIA and IIIB non-
small-cell lung cancer: a dose-escalation Phase I trial. J Clin
Oncol. 2004;22:4341–4350.
35. Socinski MA, Rosenman JG, Halle J, et al. Dose-escalating
conformal thoracic radiation therapy with induction and
concurrent carboplatin/paclitaxel in unresectable Stage
IIIA/B nonsmall cell lung carcinoma: a modified Phase I/II
trial. Cancer. 2001;92:1213–1223.
36. Willner J, Schmidt M, Kirschner J, et al. Sequential chemo-
and radiochemotherapy with weekly paclitaxel (Taxol) and
3D-conformal radiotherapy of Stage III inoperable non-
small cell lung cancer. Results of a dose escalation study.
Lung Cancer. 2001;32:163–171.
37. Wolski MJ, Bhatnagar A, Flickinger JC, et al. Multivariate
analysis of survival, local control, and time to distant metas-
tases in patients with unresectable non-small-cell lung car-
cinoma treated with 3-dimensional conformal radiation
therapy with or without concurrent chemotherapy. Clin
Lung Cancer. 2005;7:100–106.
38. Kong FM, Ten Haken RK, Schipper MJ, et al. High-dose
radiation improved local tumor control and overall survival
in patients with inoperable/unresectable non-small-cell
lung cancer: long-term results of a radiation dose escalation
study. Int J Radiat Oncol Biol Phys. 2005;63:324–333.
39. Sibley GS, Mundt AJ, Shapiro C, et al. The treatment of Stage
III nonsmall cell lung cancer using high dose conformal
radiotherapy. Int J Radiat Oncol Biol Phys. 1995;33:1001–
1007.
40. Bradley JD, Ieumwananonthachai N, Purdy JA, et al. Gross
tumor volume, critical prognostic factor in patients treated
with three-dimensional conformal radiation therapy for
non-small-cell lung carcinoma. Int J Radiat Oncol Biol Phys.
2002;52:49–57.
1330 CANCER September 15, 2006 / Volume 107 / Number 6