Thyroid , antithyroid , parathyroid & Calcium metabolism
Suharti K Suherman
Dept. of Pharmacology & Therapeutic
Medical Faculty, Univ. of Indonesia

Thyroid h secreted by thyroid gland → source of 2 different types of hormones :
a. tetraiodothyronine (T4) & triidothyronine (T3) essential
for normal growth &
b. calcitonin secreted by parafollicular cells
Synthesis unique & complex
- synthesized & stored as AA residues
of thyroglobulin = a protein component of
thyroid follicular colloid

Thyroid H the only hormone that contains iodine & need exogenous I – for its synthesize , has 2 important functions :
** in developing phase determinants of normal development espscl
CNS devepl.
** in adult it maintains metabolic homeostasis affecting the functions of all organs


Biosynthesis thyroid hormones
• Uptake of iodide ion (I- )by the gland
• Oxidation of iodide & the iodination of tyrosyl groups of thyroglobulin
• Coupling of iodothyronines residues by ether linkage to generate the iodothyronines
• Resorption of the thyroglobulin colloid from the lumen into the cell
• Proteolysis of thyroglobulin & the release of thyroxine & triiodothyronine into the blood



• Normal daily production of thyroxine is 80 – 100 ug & T3 : 30 – 40 ug
• Under normal condition 40% of T4 is coverted to T3

** thyroid h is bound in TBG major carrier of TH , T4 is also bound
to TB prealbumin & a small
number is bound to albumin or free
** eliminated slowly t½ 6 – 8 dhyperthyroidism shortened to 3 – 4 d
hypothyroidis 9 – 10 d
pregnancy binding to TBG retarded clearence
** metabolism liver

Grugs that alter binding of thyroid to TBG
binding binding
estrogen glucocort
clofibrate androgen
5–fluorouracil salicylates
tamoxifen mefenanic acid
SERM phenytoin, carbarmazepin furosemide
methadon
heroin

Actions of thyroid hormones
• mediated by nuclear TRs• T3 binds to high-affinity TRs then bind
to specific DNA sequences (TREs = thyroid hormone response elements) in the promoter regions of target genes to modulate gene transcrptn protein synthesis
• T4 hasn’t been shown to alter gene transcrpt , it must be converted to T3

• Indications : hormone replacement th/ in hypothyroidism or cretinism;
for TSH suppression th/ in nontoxic goiter or after th/ for thyroid
cancer
Preparations :
* thyroxine Na tab 50–100 ug/d or * levothyroxine Na (L-T4) tab 25 -
50 ug/d or lyophilized powder for inject = drug of choice for replace ment th/ due to its consistent potency &
prolonged duration of action

• Average daily adult replacement dose of levoth is 1.7 ug/kg BW
• The goal of th/ is to normalize the serum TSH ( in primary hypothyroidism) or free T4 ( in secondary hypothyroidism) ; and to relieve symptoms of hypothyroidism

• Liothyronine Na (L-T3) tab & injectable
• form mixture of L-T4 & L-T3 = Liotrix, 0.05 – 0.1 mg/d (tab 100ug)

• L-T4 prefer for thyroid replacement longer duration of action, 50 –
80% of the dose is absorbed
• blood level is easily monitored by FT4 & TSH serum level
• T1/2 7 days once daily
• Side effects : allergic reactions, signs of hyperthyroidis

• Drugs interactions:
# cholestyramin,iron,calcium,Al (OH)3 & soy product interfere L-T4 absorption
# phenytoin, carbamezepin & rifampin biliary excretion of L-T4
often necessary the dose
# pregnant woman/ on OC the dose of levothyroxine need
to be due to serum TBG induced by estrogen

Hyperthyroidism antithyroid
• propylthiouracil ( PTU), methimazole & carbimazol (a carbethoxy derivative of
methimazole it inhibits thyroglobulin to form T4 & T3 within the thyroid gland
• PTU , but not methimazole, block peripheral conversion T4 to T3

PTU Methim
• plasma prot binding ……..75%........nil
• plasma t1/2 ……………….75 min….4 – 6 hrs
• concentrated in thyroid….…yes……yes
• metab in severe
liver disease…………..…normal……. kidney disease………..…normal….normal
dosing frequency……….1- 4 x/d…..1 – 2 x/d transplacental/
breast milk…………………low………..

Side effects
• Skin rash ( 3% & 7%)
• Agranulocytosis ( 0.44 & 0.12% )
• Tremor, tachycardia, palpitation, flushing, headache
Interactions
Anticoagulants, digitalis, amiodarone, cholestyramine

Parathyroid H & vit D
• importance role in calcium metabolism
• secreted by parathyroid gland Ca++ plasma = the most powerful regulator for its secretion
• Ca++ plasma is low PTH secretion , if the hypocalcemia is sustained
hypertrophy & hyperplasia of the gland

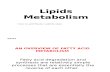
Whole body daily turnover of calcium

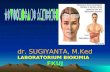
Calcium homeostasis & its regulation by PTH & 1.25- dihydroxyvitamin D.

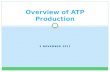
Bone remodeling sequence in healthy subjects
Other factor to bone strength : bone turn over


Faaltirotoksikosis --------hipotiroidism
*Kulit: panas,lembab -------------pucat,dingin,kering *mata: retraksi kelopak-----------kelopak terjatuh
periorbital edema-------------( lidah besar )
exopthalmus
*jantung : freq & CO ------------ freq jatng,nadi,CO*resp : dyspnoe -------------------- hipoventilasi
* GI : nafsu makan ------------------ peristaltik
*otot: lemah, lelah ---------------------kaku , lelah

• Primary target cell PTH is osteoblast , although some PTH receptors
has been found in osteocytes
• PTH also recruits osteoclast precursor cells to form new bone remodeling units
• Sustained increases in circulating PTH increase in the prevalence of osteoclasts resorption sites
• PTH increase total number of osteoblast initiation of bone remodeling

• PTH stimulates cyclic AMP production in osteoblast
• Teriparatide for severe osteoporosis
• 20 ug SQ/daily serum PTH increase to peak concen within 30 min after the inj & decline within 3 hrs, serum Ca increase to peak concent at 4 – 6 hrs

• Preparat: l-tiroksin (T4) 75-100ug atau 1-1.5ug/kg/h, Liotironon (T3) --25-50ug Liotrix (T3 : T4=4:1) 60-80ug

Biosintesis H tiroid
• Iodide trapping = transport iodida ke kel tiroid
• di oksidasi - thyroidal peroxidase iodium iodinasi residu tirosin di molekul tiroglobulin monoiodoti rosin (MIT) & diiodotirosin (DIT)
• 2 mol DIT bergab diantara mol tiroglo bulin L-tiroksin (T4)
• 1 mol MIT+1mol DIT T3

• Stimulasi TSH T3 ,T4 darah , Proses ini tehambat bila iodium berlebihan.
• T4 > T3 , potensi ikatannya dg reseptor T3 10 x > T4 .
• Dlm darah , hepar & organ lain T4 diubah T3 , dihambat oleh obat anti- tiroid
• T3 & T4 terikat : TBG , album , prealbum
• TBG dibentuk hepar dibawah pengaruh : estrog , androg, glukokort

ANTI-TIROID
• Gol.tioamida , iodida, radioactive Iodium.
• Indikasi : hipertiroidism
• Sering: propiltiourasil , metimazol, karbimasol , atau iodium radioaktiv
• Kerja: menghambat sintesis tiroksin peroksidase
• oral

Calcitonin
• hormone produced by parafollicular C cells
• A single chain peptide hormone IM / nasal spray
• Postmenopausal oeteoporosis calcitonin inhibit osteoclast activity in bone
resorption osteoklast
BMD = Bone Mineral Density)

enough intake Calcium & vit D• Preparations : synthetic salmon
calcitonin nasal spray 50 IU 2x/ day or injection ampul 50 IU 1 x / 2 days
• Adverse reactions : nausea, flushing, dose-dependent

Calcitriol
• Metabolit aktif vit. D3• Normal dibentuk ginjal dari
prekursornya 25-OH cholecalciferol (25-HCl)
• Produksi sehari : 0,5---1,0 gme pada masa pembentukan tulang (masa kehamilan)
• Normal : peran me absorpsi Ca++ di usus & meregulasi mineralisasi tulang

• Postmenopausal osteoporosis • calcitriol resorpsi tulang prevention
of lost bone mass
• Dosage : 0,25 ug 1 x / 2 x / d risk of & hyper - calemia / siuria

OK dosis awal dimulai 0.25mg/h --
setelah itu dapat di 0.5 mg/h
monitor kadar Ca++
• Adverse reactions : hypersens, hypercalcemia

• Preparat Iodida u/ hipertiroidism kurang memuaskan, krn setelah th/ sering terjd hipertiroidism yg > hebat