



www.elsevier.com/locate/diabres
Diabetes Research and Clinical Practice 76 (2007) 279–289
Thiazolidinediones and the risk of edema: A meta-analysis
Helen D. Berlie, James S. Kalus *, Linda A. Jaber
Eugene Applebaum College of Pharmacy and Health Sciences, Wayne State University, Detroit, MI, United States
Received 26 June 2006; accepted 4 September 2006
Available online 18 October 2006
Abstract
The use of thiazolidinediones (TZDs) in the management of type 2 diabetes mellitus (T2DM) has been associated with an
increased risk of peripheral edema. A meta-analysis was performed to assess the overall risk for developing edema secondary to
TZD. A systematic literature search was conducted using five electronic databases. All prospective, randomized, either placebo-
controlled or comparative studies reporting the incidence of edema with TZD therapy were included. Odds ratios were generated by
pooling estimates across the studies. The analysis included 26 studies consisting of 15,332 patients with T2DM. The pooled odds
ratio for TZD induced edema was 2.26 (95% CI: 2.02–2.53). The results yielded a higher risk for developing edema with
rosiglitazone (3.75 [2.70–5.20]) compared to pioglitazone (2.42 [1.90–3.08]). Concordant results persisted with calculations of the
adjusted indirect estimate. This meta-analysis demonstrates at least a two-fold increase in the risk for developing edema with a TZD
agent. The risk appears to be greater with rosiglitazone than with pioglitazone. Further studies are needed to explore this difference.
# 2006 Elsevier Ireland Ltd. All rights reserved.
Keywords: Thiazolidinediones; Pioglitazone; Rosiglitazone; Edema
1. Introduction
The thiazolidinediones (TZDs), pioglitazone and
rosiglitazone, are insulin sensitizing agents that have
been used in the management of type 2 diabetes
mellitus (T2DM) either as monotherapy or in combina-
tion with other glucose-lowering drugs [1,2]. TZDs are
ligands of the transcription factor peroxisome pro-
liferator activated receptor-gamma (PPAR-g) nuclear
receptors, which are present in high concentrations in
adipocytes [3]. Their insulin sensitizing actions are
mediated largely by the activation of the PPAR-g in the
* Corresponding author at: Department of Pharmacy Practice,
Eugene Applebaum College of Pharmacy and Health Sciences, Wayne
State University, 259 Mack Avenue, Detroit, MI 48201-2417, United
States. Tel.: +1 313 916 7755; fax: +1 313 916 1302.
E-mail address: [email protected] (J.S. Kalus).
0168-8227/$ – see front matter # 2006 Elsevier Ireland Ltd. All rights re
doi:10.1016/j.diabres.2006.09.010
adipose tissues resulting in modulating the genes
responsible for the regulation of glucose and lipid
metabolism [4]. TZDs have been shown to produce
sustained lowering of hyperglycemia with an average
reduction in HbA1c (A1C) levels by 1–1.5% [3]. Aside
from their glucose lowering effects, a preponderance of
evidence indicates that these agents can potentially
modify the metabolic abnormalities commonly asso-
ciated with insulin resistance such as dyslipidemia,
hypertension, abnormal endothelial function, and
procoagulant abnormalities [5–7]. The recently pub-
lished PROactive study has confirmed that pioglitazone
therapy reduces the composite endpoint of all-cause
mortality, non-fatal myocardial infarction, and stroke
[8]. Given that cardiovascular disease (CVD) is
responsible for over 65% of all diabetes related deaths,
the benefits of TZDs apparently extend beyond
achieving glycemic control to the potential reduction
of CVD risks and events [9].
served.
H.D. Berlie et al. / Diabetes Research and Clinical Practice 76 (2007) 279–289280
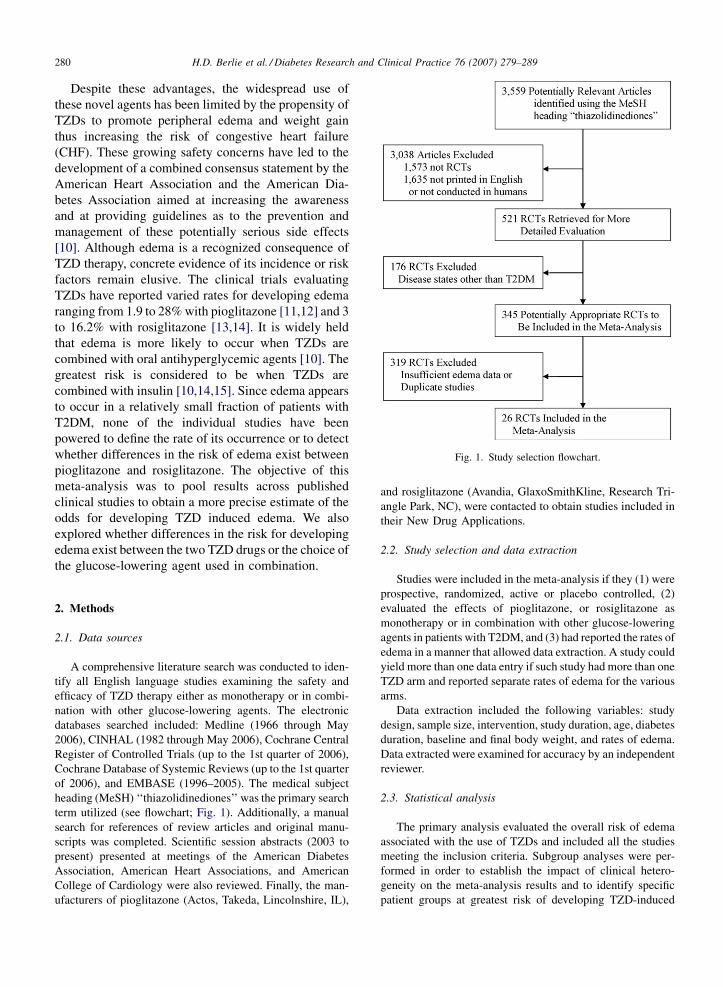
Fig. 1. Study selection flowchart.
Despite these advantages, the widespread use of
these novel agents has been limited by the propensity of
TZDs to promote peripheral edema and weight gain
thus increasing the risk of congestive heart failure
(CHF). These growing safety concerns have led to the
development of a combined consensus statement by the
American Heart Association and the American Dia-
betes Association aimed at increasing the awareness
and at providing guidelines as to the prevention and
management of these potentially serious side effects
[10]. Although edema is a recognized consequence of
TZD therapy, concrete evidence of its incidence or risk
factors remain elusive. The clinical trials evaluating
TZDs have reported varied rates for developing edema
ranging from 1.9 to 28% with pioglitazone [11,12] and 3
to 16.2% with rosiglitazone [13,14]. It is widely held
that edema is more likely to occur when TZDs are
combined with oral antihyperglycemic agents [10]. The
greatest risk is considered to be when TZDs are
combined with insulin [10,14,15]. Since edema appears
to occur in a relatively small fraction of patients with
T2DM, none of the individual studies have been
powered to define the rate of its occurrence or to detect
whether differences in the risk of edema exist between
pioglitazone and rosiglitazone. The objective of this
meta-analysis was to pool results across published
clinical studies to obtain a more precise estimate of the
odds for developing TZD induced edema. We also
explored whether differences in the risk for developing
edema exist between the two TZD drugs or the choice of
the glucose-lowering agent used in combination.
2. Methods
2.1. Data sources
A comprehensive literature search was conducted to iden-
tify all English language studies examining the safety and
efficacy of TZD therapy either as monotherapy or in combi-
nation with other glucose-lowering agents. The electronic
databases searched included: Medline (1966 through May
2006), CINHAL (1982 through May 2006), Cochrane Central
Register of Controlled Trials (up to the 1st quarter of 2006),
Cochrane Database of Systemic Reviews (up to the 1st quarter
of 2006), and EMBASE (1996–2005). The medical subject
heading (MeSH) ‘‘thiazolidinediones’’ was the primary search
term utilized (see flowchart; Fig. 1). Additionally, a manual
search for references of review articles and original manu-
scripts was completed. Scientific session abstracts (2003 to
present) presented at meetings of the American Diabetes
Association, American Heart Associations, and American
College of Cardiology were also reviewed. Finally, the man-
ufacturers of pioglitazone (Actos, Takeda, Lincolnshire, IL),
and rosiglitazone (Avandia, GlaxoSmithKline, Research Tri-
angle Park, NC), were contacted to obtain studies included in
their New Drug Applications.
2.2. Study selection and data extraction
Studies were included in the meta-analysis if they (1) were
prospective, randomized, active or placebo controlled, (2)
evaluated the effects of pioglitazone, or rosiglitazone as
monotherapy or in combination with other glucose-lowering
agents in patients with T2DM, and (3) had reported the rates of
edema in a manner that allowed data extraction. A study could
yield more than one data entry if such study had more than one
TZD arm and reported separate rates of edema for the various
arms.
Data extraction included the following variables: study
design, sample size, intervention, study duration, age, diabetes
duration, baseline and final body weight, and rates of edema.
Data extracted were examined for accuracy by an independent
reviewer.
2.3. Statistical analysis
The primary analysis evaluated the overall risk of edema
associated with the use of TZDs and included all the studies
meeting the inclusion criteria. Subgroup analyses were per-
formed in order to establish the impact of clinical hetero-
geneity on the meta-analysis results and to identify specific
patient groups at greatest risk of developing TZD-induced
H.D. Berlie et al. / Diabetes Research and Clinical Practice 76 (2007) 279–289 281
edema. These subgroup analyses examined whether differ-
ences in risk for developing edema exist relative to the specific
TZD chosen, the TZD dosages employed, the use of TZDs
alone or in combination, or the specific comparator agent
tested. The comparison of TZD induced edema between
pioglitazone and rosiglitazone was also examined using an
adjusted indirect comparison method [16]. Sensitivity ana-
lyses were conducted to determine the effects of including
open-label studies on the overall outcome and to compare the
fixed versus random effect model results for the primary
analysis.
The incidence of edema was treated as a dichotomous
variable and reported as an odds ratio (OR) with a 95%
confidence interval (CI). For each analysis, the chi-square
test was performed to assess the presence of statistical hetero-
geneity between studies. A p-value <0.1 indicated that sig-
nificant heterogeneity was present. When statistical
heterogeneity was not detected, a fixed-effect model using
Mantel–Haenszel methodology was applied to estimate odds
ratios [17]. When significant heterogeneity was present, a
random-effect model using DerSimonian and Laird metho-
dology was employed [17]. A funnel plot was examined to
assess for bias in the meta-analysis. Review Manager 4.2.8
software was used to calculate a pooled OR for the overall
analysis as well as the subgroup and sensitivity analyses [17].
3. Results
3.1. Studies and patients
Relevant characteristics of the studies included in the
meta-analysis are summarized in Table 1. A total of 26
prospective studies met the inclusion criteria for this
analysis; seven studies had open-label design, five
studies compared TZD monotherapy to placebo, and 20
compared a TZD to other glucose-lowering agents. The
duration of these studies ranged from 16 weeks to 34.5
months. In the TZD monotherapy-placebo trials, the
total daily dosing ranges were 7.5–45 mg for piogli-
tazone, and 4–8 mg for rosiglitazone. In the TZD
combination comparative trials, the daily dosages
ranged from 15 to 30 mg for pioglitazone and from 4
to 8 mg for rosiglitazone. All but seven studies excluded
patients with New York Heart Association (NYHA)
class III or IV heart failure [11,13,18–22]. Additionally,
a recent history of CVD was used as exclusion criteria in
8 of the 26 studies [15,18,23–28]. A recent history was
defined as less than 6 months, and CVD included all or a
combination of the following: unstable angina, myo-
cardial infarction, angioplasty, coronary artery bypass
graft, cerebrovascular accident, and stroke. In these
studies, information as to the proportion of participants
with any cardiac history was not provided. Similarly,
studies not listing any cardiac exclusion criteria did not
report whether any such patients were enrolled.
The 26 studies included a total of 15,332 patients
with T2DM. Of the patients included, 8586 received a
TZD and the remaining 6746 were either in the placebo
or the comparator groups. Individual study population
ranged from 62 to 5238 subjects. Across the included
studies, the average participant age ranged from 53.7 to
61.9 years and the average duration of diabetes ranged
from 5.6 months to 13.6 years. The mean baseline A1C
levels ranged from 7.5 to 10.2% with pioglitazone and
7.9 to 9.1% with rosiglitazone. The mean reduction in
A1C levels ranged from 0.56 to 2.3%. In the three
studies that reported heart failure, the incidence ranged
from 1.9 to 11% [8,14,18]. The range of weight gain
reported by the included studies was �0.59 to +3.86 kg
for pioglitazone (12 studies) and +1.2 to +5.0 kg for
rosiglitazone (six studies). Edema was reported
separately from weight gain. Of the 26 included
studies, only 2 reported the use of an objective scale
for assessing edema [12,31]. Edema was described as
‘‘mild’’ in three studies [15,19,35] and ‘‘moderate’’ in
one study [35]. One study [28] also described edema as
‘‘pitting.’’ Aside from these studies, most simply
reported edema as an adverse effect and described it
as ‘‘peripheral edema’’ or ‘‘edema’’ with no objective
evidence provided. None of the included studies
provided information about concomitant medications
that can precipitate edema, such as calcium channel
blockers or NSAIDs.
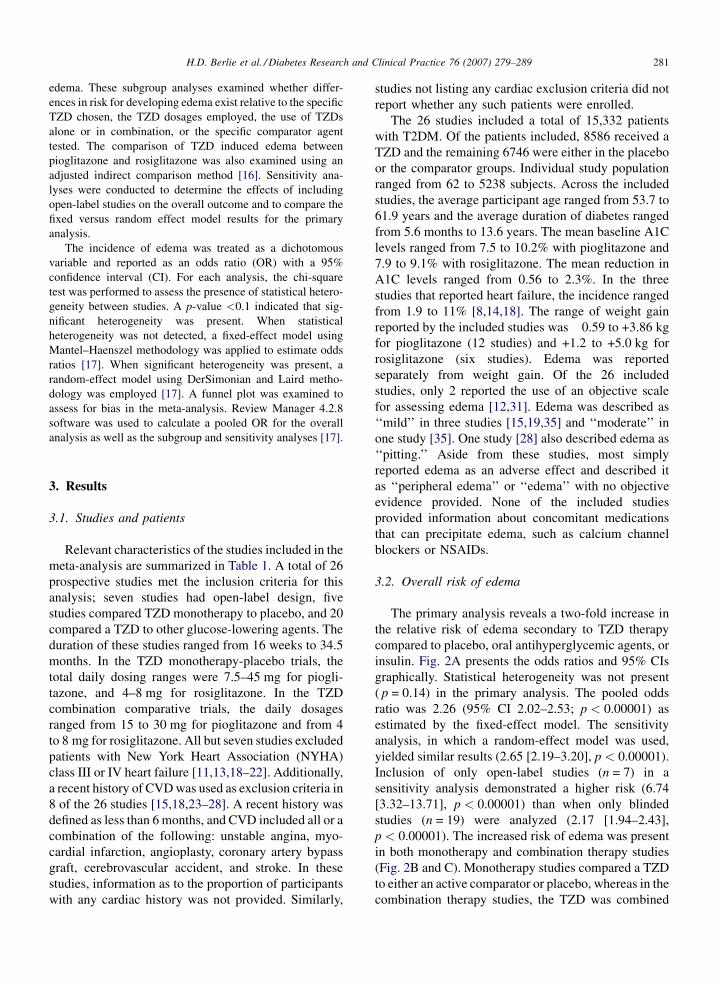
3.2. Overall risk of edema
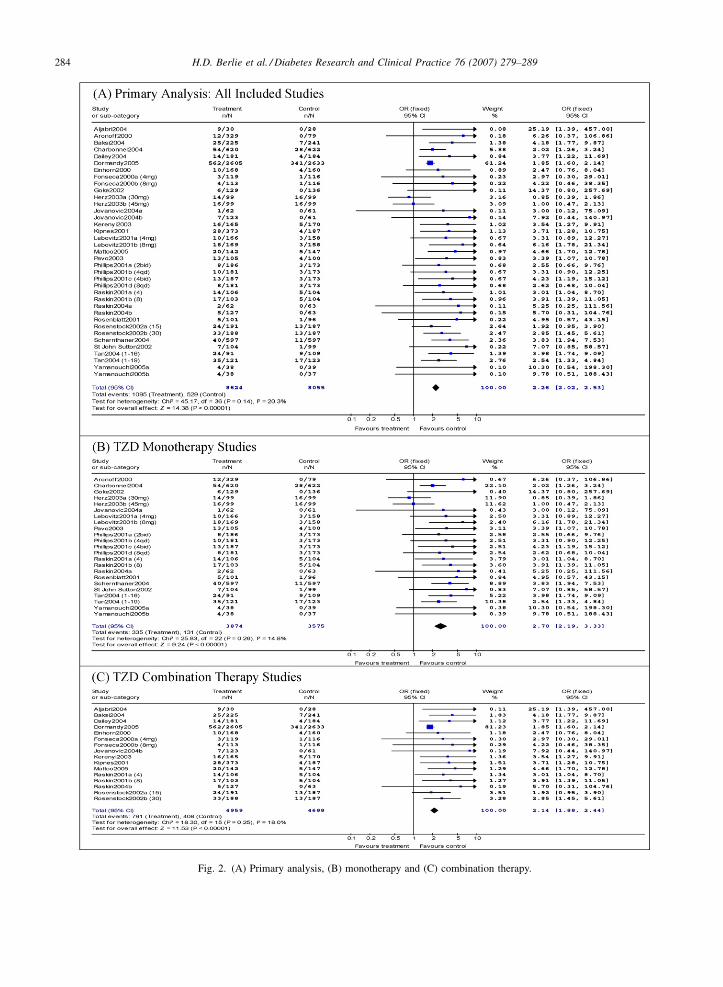
The primary analysis reveals a two-fold increase in
the relative risk of edema secondary to TZD therapy
compared to placebo, oral antihyperglycemic agents, or
insulin. Fig. 2A presents the odds ratios and 95% CIs
graphically. Statistical heterogeneity was not present
( p = 0.14) in the primary analysis. The pooled odds
ratio was 2.26 (95% CI 2.02–2.53; p < 0.00001) as
estimated by the fixed-effect model. The sensitivity
analysis, in which a random-effect model was used,
yielded similar results (2.65 [2.19–3.20], p < 0.00001).
Inclusion of only open-label studies (n = 7) in a
sensitivity analysis demonstrated a higher risk (6.74
[3.32–13.71], p < 0.00001) than when only blinded
studies (n = 19) were analyzed (2.17 [1.94–2.43],
p < 0.00001). The increased risk of edema was present
in both monotherapy and combination therapy studies
(Fig. 2B and C). Monotherapy studies compared a TZD
to either an active comparator or placebo, whereas in the
combination therapy studies, the TZD was combined
H.D. Berlie et al. / Diabetes Research and Clinical Practice 76 (2007) 279–289282
Table 1
Included studies
Study (reference) Study design Comparator Methods Incidence of edema
(cases/no. of treatment arm)
Pioglitazone studies
Aljabri et al. [22] PIO 30 mg titrated to 45 mg.
Combination therapy with
MET + SU
INS (NPH) RCT, open label,
16 weeks, N = 62
PIO: 9/30; INS: 0/28
Aronoff et al. [18] PIO randomized to 7.5, 15,
30 or 45 mg
PLA R, DB, PC, 26
weeks, N = 408
PIO: 12/329; PLA: 0/79
Charbonnel et al. [19] PIO forced titration to 45 mg SU
(gliclazide)
R, PG, DD, DB,
52 weeks, N = 1270
PIO: 54/620; SU: 28/622
Dormandy et al. [8] PIO 15 mg titrated to 45 mg.
Combination therapy with
various pre-study medications
PLA RCT, 150 weeks,
N = 5238
PIO: 562/2605; PLA:
341/2633
Einhorn et al. [23] PIO 30 mg. Combination
(MET + PIO vs. MET + PLA)
MET R, DB, PC, 16
weeks, N = 328
PIO + MET: 10/168;
PLA + MET: 4/160
Goke and German
Pioglitazone Study
Group [24]
PIO 45 mg AGI
(acarbose)
R, PG, MC, open
label, 26 weeks,
N = 265
PIO: 6/129; AGI: 0/136
Herz et al. [28] PIO randomized to 30 or 45 mg PLA R, PG, DB, PC, MC,
16 weeks, N = 297
PIO30: 14/99; PIO45:
16/99; PLA: 16/99
Jovanovic et al. [20] PIO 30 mg fixed dose throughout
study. (a) Monotherapy (PIO vs.
repaglinide); (b) combination
therapy with both agents
(PIO + repaglinide)
Non-SU
(repaglinide)
R, PG, MC, open
label, 24 weeks,
N = 246
PIO: 1/62; PIO + NonSU:
7/123; NonSU: 0/61
Kipnes et al. [25] PIO randomized to 15 or 30 mg.
Combination (SU + PIO15 vs.
SU + PIO30 vs. SU + PLA)
SU R, DB, PC, MC,
16 weeks, N = 560
PIO + SU: 28/373;
PLA + SU: 4/187
Mattoo et al. [29] PIO 30 mg. Combination therapy
(INS + PIO vs. INS + PLA)
INS R, DB, PC, MC,
26 weeks, N = 289
PIO + INS: 20/142;
PLA + INS: 5/147
Pavo et al. [30] PIO 30 mg titrated to 45 mg MET R, DB, MC, 32
weeks, N = 205
PIO: 13/105; MET: 4/100
Rosenblatt et al. [26] PIO 30 mg PLA R, DB, PC, MC,
23 weeks, N = 197
PIO: 5/101; PLA: 1/96
Rosenstock et al. [15] PIO randomized to 15 or 30 mg.
Combination (INS + PIO15 vs.
INS + PIO30 vs. INS + PLA)
INS R, DB, PC, MC,
16 week, N = 566
PIO15 + INS: 24/191;
PIO30 + INS: 33/188;
PLA + INS: 13/187
Schernthaner et al. [11] PIO titrated up to 45 mg MET R, PG, DB, MC,
52 weeks, N = 1199
PIO: 40/597; MET: 11/597
Tan et al. [31] PIO 30 mg increased to 45 mg SU
(glibenclamide)
R, MC, 52 weeks,
N = 200
PIO: 24/91; SU: 9/109
Tan et al. [12] PIO 15 mg increase to 45 mg SU
(glimepiride)
R, PG, DB, MC,
52 weeks, N = 244
PIO: 35/121; SU: 17/123
Yamanouchi et al. [27] PIO started on 30–45 mg/d.
Monotherapy (MET vs. SU
vs. PIO)
MET SU RCT, open label,
52 weeks, N = 114
PIO: 4/38, MET: 0/39;
SU: 0/37
Rosiglitazone studies
Baksi [32] ROSI 4 mg bid. Combination
(SU + ROSI vs. SU + placebo)
SU
(gliclazide)
R, PG, DB, PC, MC,
26 weeks, N = 473
ROSI + SU: 25/225;
SU: 7/241
Dailey et al. [21] ROSI 4 mg/d titrated to 4 mg bid.
Combination (MET + SU + ROSI
vs. MET + SU + PLA)
MET SU
(glyburide)
R, PC, open label,
24 weeks, N = 365
ROSI + MET + SU:
14/181; PLA + MET +
SU: 4/184
Fonseca et al. [33] ROSI randomized to 4 or 8 mg/d.
Combination (MET + ROSI4 vs.
MET + ROSI8 vs. MET + PLA)
MET R, DB, PC, MC,
26 weeks, N = 348
ROSI4 + MET: 3/119;
ROSI8 + MET: 4/113;
PLA + MET: 1/116
Kerenyi et al. [34] ROSI 4 mg bid. Combination
(SU + ROSI vs. SU + PLA)
SU
(glibenclamide)
R, PG, DB, PC, MC,
26 weeks, N = 340
ROSI + SU: 16/165;
PLA + SU: 5/170
H.D. Berlie et al. / Diabetes Research and Clinical Practice 76 (2007) 279–289 283
Table 1 (Continued )
Study (reference) Study design Comparator Methods Incidence of edema
(cases/no. of treatment arm)
Lebovitz et al. [35] ROSI randomized to 2 or 4 mg
bid
PLA R, PC, DB, MC,
26 weeks, N = 493
ROSI2bid: 10/166;
ROSI4bid: 18/169;
PLA: 3/158
Phillips et al. [36] ROSI randomized to 2 mg bid,
4 mg qd, 4 mg bid, or 8 mg qd
PLA R, DB, PC, MC,
26 weeks, N = 959
ROSI2bid: 8/186 R4:
10/181; R4bid: 13/187
R8: 8/181; PLA: 3/173
Raskin et al. [14] ROSI randomized to 2 mg bid
or 4 mg bid. Combination therapy
(INS + ROSI2 vs. INS + ROSI4
vs. INS + PLA)
INS R, DB, PC, MC,
26 weeks, N = 319
ROSI4 + INS: 14/106;
ROSI8 + INS: 17/103;
PLA + INS: 5/104
Raskin et al. [13] ROSI 2 mg bid, option to double to
4 mg bid. (a) Monotherpay (ROSI
vs. repaglinide); (b) combination
therapy (ROSI + repaglinide)
Non-SU
(repaglinide)
R, PG, MC, open
label, 24 weeks,
N = 252
ROSI: 2/62; ROSI +
NonSU: 5/127;
NonSU: 0/63
St John Sutton
et al. [37]
ROSI 4 mg bid SU
(glyburide)
RCT, open label,
52 weeks, N = 203
ROSI: 7/104; SU: 1/99
PIO: pioglitazone; ROSI: rosiglitazone; PLA: placebo; MET: metfromin; SU: sulfonylurea; NonSU: non-sulfonylurea secretagogue; AGI: alpha-
glucosidase inhibitor; INS: insulin; R: randomised; PC: placebo controlled; CT: controlled trial; DB: double blind; MC: multi-centre.
with the active comparator versus the active comparator
alone. The funnel plot for studies included in the
primary analysis was asymmetrical (figure not shown),
indicating that the presence of bias cannot be ruled out.
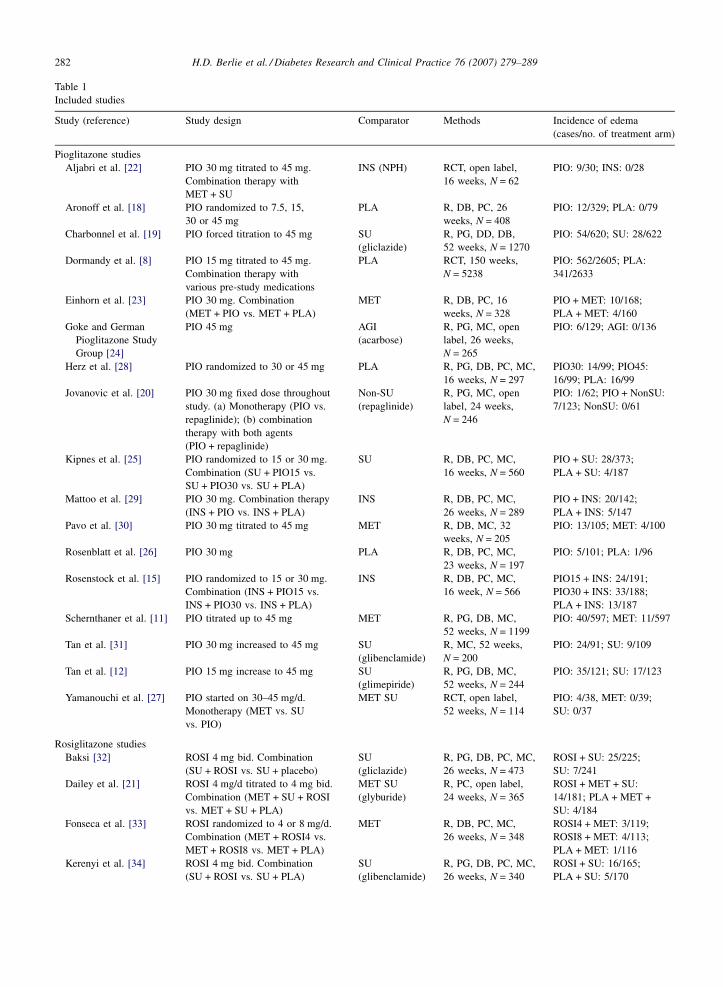
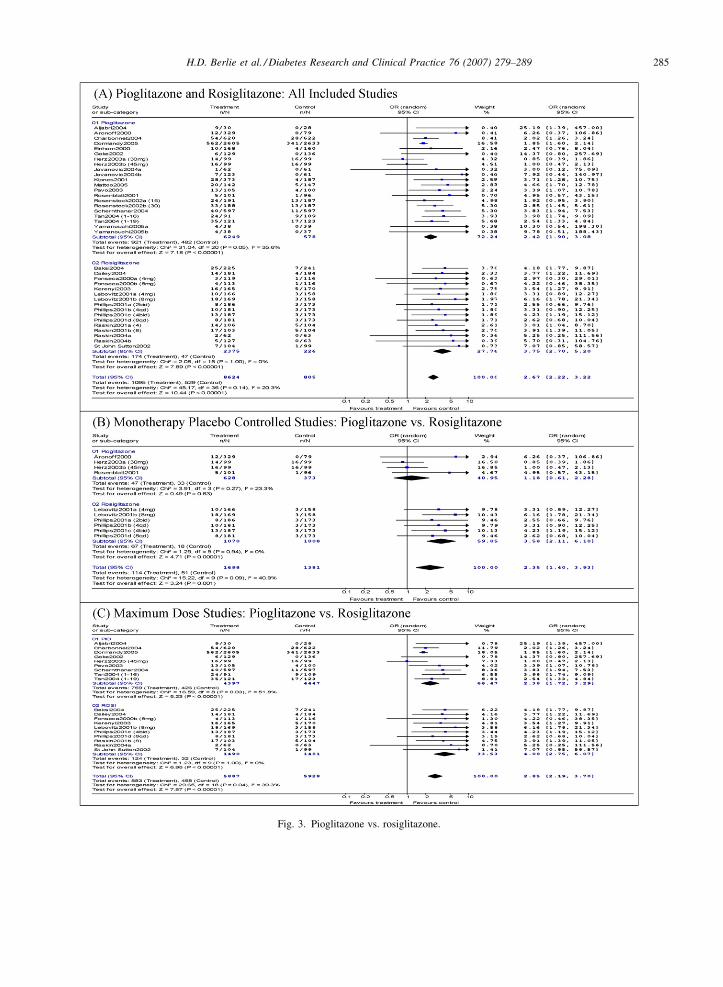
3.3. Pioglitazone and rosiglitazone
To explore the differences in the risk for developing
edema between the two TZD agents, 17 pioglitazone
studies with 21 data entries were compared to 9
rosiglitazone studies with 16 data entries (Fig. 3A). In
this secondary analysis, rosiglitazone was associated
with a more pronounced risk for edema than
pioglitazone. The calculated adjusted indirect compar-
ison of rosiglitazone to pioglitazone based on all
included studies, yielded an approximate three fold
higher risk of edema with rosiglitazone (2.74 [2.33–
3.14]).
When only placebo controlled studies of pioglita-
zone (1.18 [0.61–2.28], p < 0.063) and rosiglitazone
(3.58 [2.11–6.10], p < 0.00001) were considered
(Fig. 3B), the risk was still greater with rosiglitazone.
The calculated adjusted indirect comparison of rosigli-
tazone to pioglitazone using only placebo controlled
trials was 3.03 (2.15–3.91). The omission of all open
label trials also pointed towards an increased risk with
rosiglitazone (3.64 [2.56–5.17], p < 0.00001) over
piogltiazone (2.18 [1.72–2.75], p < 0.00001). Further
analyses were performed to examine whether the
increase in risk for edema with rosiglitazone is related
to differences in total daily dosages used. For this ana-
lysis, only studies with titrations to the recommended
maximum daily dosages of either agent (8 mg/day for
rosiglitazone and 45 mg/day for pioglitazone) were
included. Here too, there was a trend for higher risk of
edema with rosiglitazone (Fig. 3C). The analysis was
repeated with the removal of those studies indicating
less than 90% of subjects were maintained on maximal
doses by the end of the study period. This analysis
yielded similar trends in edema risk for pioglitazone
(2.02 [0.91–4.47], p = 0.08) and rosiglitazone (4.13
[2.70–6.30], p < 0.00001).
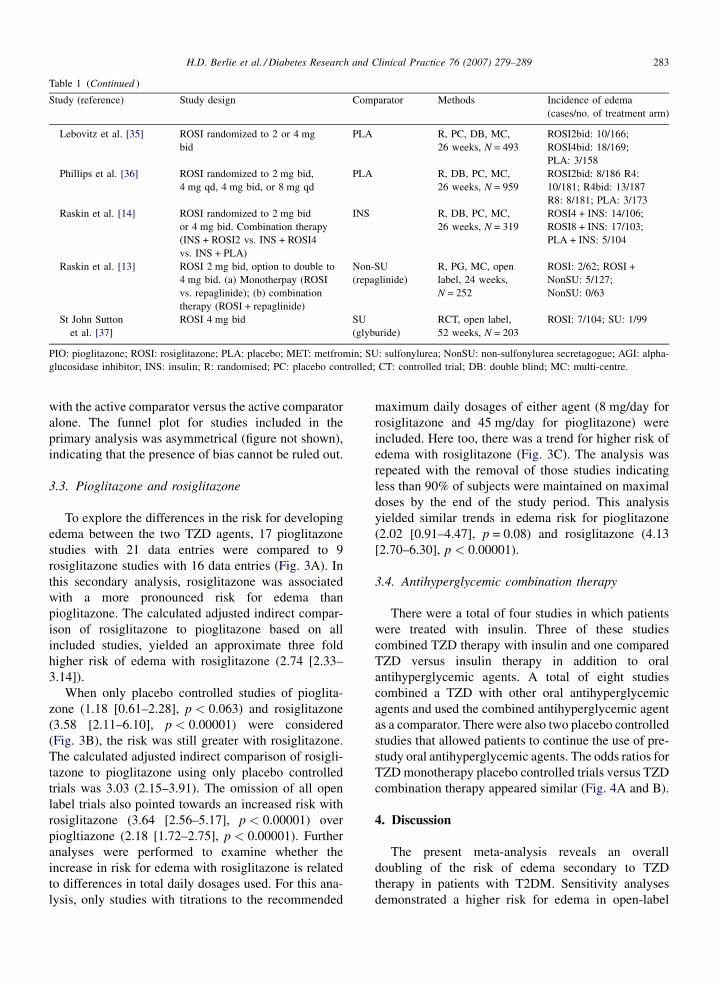
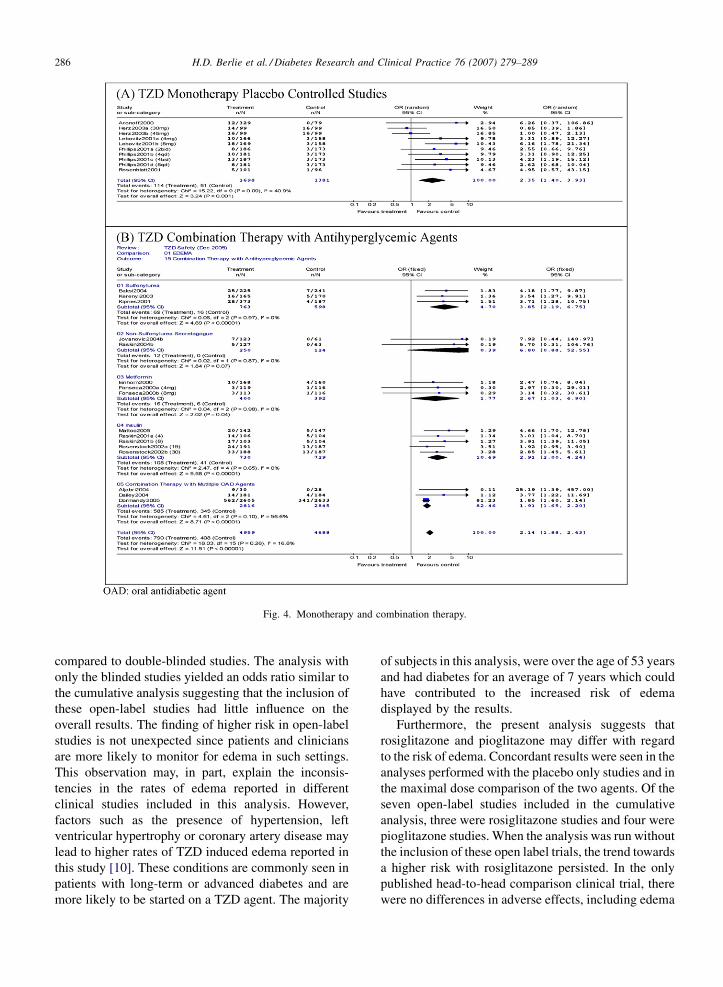
3.4. Antihyperglycemic combination therapy
There were a total of four studies in which patients
were treated with insulin. Three of these studies
combined TZD therapy with insulin and one compared
TZD versus insulin therapy in addition to oral
antihyperglycemic agents. A total of eight studies
combined a TZD with other oral antihyperglycemic
agents and used the combined antihyperglycemic agent
as a comparator. There were also two placebo controlled
studies that allowed patients to continue the use of pre-
study oral antihyperglycemic agents. The odds ratios for
TZD monotherapy placebo controlled trials versus TZD
combination therapy appeared similar (Fig. 4A and B).
4. Discussion
The present meta-analysis reveals an overall
doubling of the risk of edema secondary to TZD
therapy in patients with T2DM. Sensitivity analyses
demonstrated a higher risk for edema in open-label
H.D. Berlie et al. / Diabetes Research and Clinical Practice 76 (2007) 279–289284
Fig. 2. (A) Primary analysis, (B) monotherapy and (C) combination therapy.
H.D. Berlie et al. / Diabetes Research and Clinical Practice 76 (2007) 279–289 285
Fig. 3. Pioglitazone vs. rosiglitazone.
H.D. Berlie et al. / Diabetes Research and Clinical Practice 76 (2007) 279–289286
Fig. 4. Monotherapy and combination therapy.
compared to double-blinded studies. The analysis with
only the blinded studies yielded an odds ratio similar to
the cumulative analysis suggesting that the inclusion of
these open-label studies had little influence on the
overall results. The finding of higher risk in open-label
studies is not unexpected since patients and clinicians
are more likely to monitor for edema in such settings.
This observation may, in part, explain the inconsis-
tencies in the rates of edema reported in different
clinical studies included in this analysis. However,
factors such as the presence of hypertension, left
ventricular hypertrophy or coronary artery disease may
lead to higher rates of TZD induced edema reported in
this study [10]. These conditions are commonly seen in
patients with long-term or advanced diabetes and are
more likely to be started on a TZD agent. The majority
of subjects in this analysis, were over the age of 53 years
and had diabetes for an average of 7 years which could
have contributed to the increased risk of edema
displayed by the results.
Furthermore, the present analysis suggests that
rosiglitazone and pioglitazone may differ with regard
to the risk of edema. Concordant results were seen in the
analyses performed with the placebo only studies and in
the maximal dose comparison of the two agents. Of the
seven open-label studies included in the cumulative
analysis, three were rosiglitazone studies and four were
pioglitazone studies. When the analysis was run without
the inclusion of these open label trials, the trend towards
a higher risk with rosiglitazone persisted. In the only
published head-to-head comparison clinical trial, there
were no differences in adverse effects, including edema

H.D. Berlie et al. / Diabetes Research and Clinical Practice 76 (2007) 279–289 287
[5]. However, the actual rates of edema were not
reported and the study was not designed to detect
differences in the incidence of edema between these two
agents.
The finding of increased risk for developing edema
with rosiglitazone is intriguing. Although the exact
mechanism for TZD induced-edema is not fully
understood, several mechanisms including increased
plasma volume, reflex sympathetic activation, altered
intestinal ion transport, and increased production of
vascular endothelial growth factor have been postulated
[38]. Additionally, an association between the activa-
tion of the PPARg receptors, which are present in the
nephron, and the risk of edema secondary to TZD has
been demonstrated in rodents [39,40]. The activation of
these receptors in the collecting duct leads to the
upregulation of sodium transporters, increased sodium
retention and in turn edema. Consequently, a plausible
explanation for greater tendency for edema with
rosiglitazone is the drug’s higher affinity for these
receptors in the nephron [41].
This analysis is not in agreement with the previous
observation of higher frequency of edema when TZDs
are used in combination with other glucose-lowering
agents compared to TZD monotherapy. It is likely that
there may be a varying risk of edema depending on the
glucose-lowering agent used, some agents having
additive effects and others having protective effects.
However, this meta-analysis is not the ideal study
design to address this issue.
The weight gain associated with the use of TZDs
noted in the included studies is consistent with the
adverse effect profiles of these agents [1,2]. It has been
demonstrated that improved glycemic control is often
accompanied by weight gain, which may be linked
with edema [10]. Improved glycemic control was
achieved in the studies which reported weight gain,
which is evident by the reported decreases in A1C. It is
also important to note that the weight gain associated
with the use of TZDs is a cosmetic concern rather than
a cardiovascular risk factor. The reason that increased
weight is not associated with increased cardiovascular
risks with these agents is because they result in a
decrease in visceral fat and a subsequent increase in
subcutaneous adipose tissue, which is partly respon-
sible for the improvement in insulin resistance seen in
TZD treated patients. Furthermore, few studies
reported the incidence of heart failure occurring as
an adverse effect secondary to TZD therapy. Con-
sistent with previous findings, although the risk of
heart failure is of concern, it is not a common side
effect of these agents [10]. It should be noted,
however, that NYHA Class III and IV heart failure was
used as exclusion criteria in the majority of studies,
and some studies also excluded patients with coronary
artery disease, therefore excluding patients who would
be at increased risk for developing heart failure. There
are a number of risk factors which may contribute to
the risk of developing heart failure while being treated
with a TZD. Some of these risk factors include age
greater than 70 years, duration of diabetes for greater
than 10 years, and history of heart failure [10]. The
majority of subjects from the included studies were
less than 70 years of age and had diabetes for less than
10 years.
Several important limitations of this analysis should
be considered. First, our search was confined to
English-language published studies. Also, this meta-
analysis compared multiple intervention groups from a
given study (when data was present). According to the
Cochrane Handbook, data from trials containing
multiple intervention groups should be treated with
care [42]. However, other meta-analyses have used the
same methodology employed in this paper [43].
Edema itself is a subjective finding, and there was
no consistent definition of edema among the included
studies. Only two studies used objective methods for
evaluating for the presence of edema and the severity
of edema was only noted in three studies. Addition-
ally, little is known regarding the use of concomitant
medications that can contribute to the occurrence of
edema in the included studies. This meta-analysis
excluded studies examining the use of TZDs in other
insulin-resistant conditions such as polycystic ovary
syndrome, pre-diabetes, and lipodystrophies. Patients
with T2DM, commonly have co-morbidities which
put them at an increased risk for developing fluid
retention and edema. However, the inclusion of
studies in non-diabetic populations would have
increased clinical heterogeneity and detracted from
the clinical relevance of this analysis. Publication bias
may have been present. However, the impact of
publication bias on the overall results of a meta-
analysis has been questioned [44]. Finally, a meta-
analysis is not a substitute for a randomized controlled
trial and should instead be regarded as hypothesis
generating.
This meta-analysis provides evidence that TZD
therapy is associated with at least a two-fold increase
in the risk of peripheral edema in patients with
T2DM. The increased risk of edema appears to be
greater with rosiglitazone. Future research is needed
to identify those at the greatest risk for developing
TZD induced-edema.
H.D. Berlie et al. / Diabetes Research and Clinical Practice 76 (2007) 279–289288
References
[1] Actos [package insert], Takeda Pharmaceuticals America Inc.,
Lincolnshire, IL, 2004.
[2] Avandia [package insert]. Research Triangle Park, NC, Glax-
oSmithKline, 2005.
[3] H. Yki-Jarvinen, Thiazolidinediones, N. Engl. J. Med. 351
(2004) 1106–1118.
[4] S.M. Rangwala, M.A. Laza, Peroxisome prolliferator-activiated
receptor gamma in diabetes and metabolism, Trends Pharmacol.
Sci. 25 (2004) 331–336.
[5] R.B. Goldberg, D.M. Kendall, M.A. Deeg, J.B. Buse, A.J. Zagar,
J.A. Pinaire, et al., A comparison of lipid and glycemic effects of
pioglitazone and rosiglitazone in patients with type 2 diabetes
and dyslipidemia, Diabetes Care 28 (2005) 1547–1554.
[6] B.H. Sung, J.L. Izzo Jr., P. Dandona, M.F. Wilson, Vasodilatory
effects of troglitazone improve blood pressure at rest and during
mental stress in type 2 diabetes mellitus, Hypertension 34 (1999)
83–88.
[7] A.E. Caballero, R. Saouaf, S.C. Lim, O. Hamdy, K. Abou-
Elenin, C. O’Connor, et al., The effects of troglitazone, an
insulin-sensitizing agent, on the endothelial function in early
and late type 2 diabetes: a placebo-controlled randomized
clinical trial, Metabolism 52 (2003) 173–180.
[8] J.A. Dormandy, B. Charbonnel, D.J.A. Eckland, E. Erdmann, M.
Massi-Benedetti, I.K. Moules, et al., Secondary prevention of
macrovascular events in patients with type 2 diabetes in the
PROactive Study (PROspective pioglitAzone Clinical Trial In
macroVascular Events): a randomised controlled trial, Lancet 66
(2005) 1279–1289.
[9] American Diabetes Association (2005) All About Diabetes:
Diabetes Statistics. Available from http://diabetes.org/diabetes-
statistics.jsp, accessed December 3, 2005.
[10] R.W. Nesto, D. Bell, R.O. Bonow, V. Fonseca, S.M. Grundy, E.S.
Horton, et al., Thiazolidinedione use, fluid retention, and con-
gestive heart failure: a consensus statement from the American
Heart Association and American Diabetes Association, Diabetes
Care 27 (2004) 256–263.
[11] G. Schernthaner, D.R. Matthews, B. Charbonnel, M. Hanefeld,
P. Brunetti, Efficacy and safety of pioglitazone versus met-
formin in patients with type 2 diabetes mellitus: a double-
blind, randomized trial, J. Clin. Endocrinol. Metab. 89 (2004)
6068–6076.
[12] M. Tan, D. Johns, G. Gonzalez Galvez, O. Antunez, G. Fabian, F.
Flores-Lozano, et al., Effects of pioglitazone and glimepiride on
glycemic control and insulin sensitivity in Mexican patients with
type 2 diabetes mellitus: A multicenter, randomized, double-
blind, parallel-group trial, Clin Ther 26 (2004) 680–693.
[13] P. Raskin, J. McGill, M.F. Saad, J.M. Cappleman, W. Kaye, N.
Khutoryansky, et al., Combination therapy for type 2 diabetes:
repaglinide plus rosiglitazone, Diabet Med 21 (2004) 329–335.
[14] P. Raskin, M. Rendell, M.C. Riddle, J.F. Dole, M.I. Freed, J.
Rosenstock, et al., A randomized trial of rosiglitazone therapy in
patients with inadequately controlled insulin-treated type 2
diabetes, Diabetes Care 24 (2001) 1226–1232.
[15] J. Rosenstock, D. Einhorn, K. Hershon, N.B. Glazer, S. Yu,
Pioglitazone 014 Study Group, Efficacy and safety of pioglita-
zone in type 2 diabetes: a randomised, placebo-controlled study
in patients receiving stable insulin therapy, Int. J. Clin. Pract. 56
(2002) 251–257.
[16] British Medical Journal (2003) Adjusted indirect comparison
of competing interventions: method and worked example.
Available from http://bmj.bmjjournals.com/cgi/content/full//
326/7387/472/DCI, accessed May 4, 2006.
[17] The Cochrane Collaboration’s Information Management System
(2005) RevMan 4.2.8 Available from http://www.cc-ims.net/
RevMan, accessed November 1, 2005.
[18] S. Aronoff, S. Rosenblatt, S. Braithwaite, J.W. Egan, A.L.
Mathisen, R.L. Schneider, et al.,The Pioglitazone 001 Study
Group, Pioglitazone hydrochloride monotherapy improves gly-
cemic control in the treatment of patients with type 2 diabetes: a
6-month randomized placebo-controlled dose-response study,
Diabetes Care 23 (2000) 1605–1611.
[19] B.H. Charbonnel, D.R. Matthews, G. Schernthaner, M. Hane-
feld, P. Brunetti, A long-term comparison of pioglitazone and
gliclazide in patients with Type 2 diabetes mellitus: a rando-
mized, double-blind, parallel-group comparison trial, Diabet.
Med. 22 (2005) 399–405.
[20] L. Jovanovic, D.R. Hassman, B. Gooch, R. Jain, S. Greco, N.
Khutoryansky, et al., Treatment of type 2 diabetes with a
combination regimen of repaglinide plus pioglitazone, Diabetes
Res Clin Prac 63 (2004) 127–134.
[21] G.E. Dailey, 3rd, M.A. Noor, J.S. Park, S. Bruce, F.T. Fie-
dorek, Glycemic control with glyburide/metformin tablets in
combination with rosiglitazone in patients with type 2 dia-
betes: a randomized, double-blind trial, Am. J. Med. 116
(2004) 223–229.
[22] K. Aljabri, S.E. Kozak, D.M. Thompson, Addition of piogli-
tazone or bedtime insulin to maximal doses of sulfonylurea
and metformin in type 2 diabetes patients with poor glucose
control: a prospective, randomized trial, Am. J. Med. 116
(2004) 230–235.
[23] D. Einhorn, M. Rendell, J. Rosenzweig, J.W. Egan, A.L. Mathi-
sen Mathisen, R.L. Schneider, The Pioglitazone 027 Study
Group, Pioglitazone hydrochloride in combination with metfor-
min in the treatment of type 2 diabetes mellitus: a randomized,
placebo-controlled study, Clin Ther 22 (2000) 1395–1409.
[24] B. Goke, German Pioglitazone Study Group, Improved glycemic
control and lipid profile in a randomized study of pioglitazone
compared with acarbose in patients with type 2 diabetes mellitus,
Treat. Endocrinol. 1 (2002) 329–336.
[25] M.S. Kipnes, A. Krosnick, M.S. Rendell, J.W. Egan, A.L.
Mathisen, R.L. Schneider, et al., Pioglitazone hydrochloride
in combination with sulfonylurea therapy improves glycemic
control in patients with type 2 diabetes mellitus: a randomized,
placebo-controlled study, Am J Med 111 (2001) 10–17.
[26] S. Rosenblatt, B. Miskin, N.B. Glazer, M.J. Prince, K.E.
Robertson, Pioglitazone 026 Study Group, The impact of
pioglitazone on glycemic control and atherogenic dyslipidemia
in patients with type 2 diabetes mellitus, Coron Artery Dis. 12
(2001) 413–423.
[27] T. Yamanouchi, T. Sakai, K. Igarashi, K. Ichiyanagi, H. Wata-
nabe, T. Kawasaki, Comparison of metabolic effects of piogli-
tazone, metformin, and glimepiride over 1 year in Japanese
patients with newly diagnosed Type 2 diabetes, Diabet Med
22 (2005) 980–985.
[28] M. Herz, D. Johns, J. Reviriego, L.D. Grossman, C. Godin, S.
Duran, et al., A randomized, double-blind, placebo-controlled,
clinical trial of the effects of pioglitazone on glycemic control
and dyslipidemia in oral antihyperglycemic medication-naive
patients with type 2 diabetes mellitus, Clin Ther 25 (2003)
1074–1095.
[29] V. Mattoo, D. Eckland, M. Widel, S. Duran, C. Fajardo, J. Strand,
et al., Metabolic effects of pioglitazone in combination with
H.D. Berlie et al. / Diabetes Research and Clinical Practice 76 (2007) 279–289 289
insulin in patients with type 2 diabetes mellitus whose disease is
not adequately controlled with insulin therapy: results of a six-
month, randomized, double-blind, prospective, multicenter, par-
allel-group study, Clin Ther 27 (2005) 554–567.
[30] I. Pavo, G. Jermendy, T.T. Varkonyi, Z. Kerenyi, A. Gyimesi, S.
Shoustov, et al., Effect of pioglitazone compared with metformin
on glycemic control and indicators of insulin sensitivity in
recently diagnosed patients with type 2 diabetes, J Clin Endo-
crinol Metab 88 (2003) 1637–1645.
[31] M.H. Tan, D. Johns, J. Strand, J. Halset, S. Madsbad, J.W.
Eriksson, et al., Sustained effects of pioglitazone vs. glibencla-
mide on insulin sensitivity, glycaemic control, and lipid profiles
in patients with Type 2 diabetes, Diabet Med 21 (2004) 859–866.
[32] A. Baksi, R.E. James, B. Zhou, J.J. Nolan, Comparison of
uptitration of gliclazide with the addition of rosiglitazone to
gliclazide in patients with type 2 diabetes inadequately con-
trolled on half-maximal doses of a sulphonylurea, Acta Diabetol.
41 (2004) 63–69.
[33] V. Fonseca, J. Rosenstock, R. Patwardhan, A. Salzman, Effect of
metformin and rosiglitazone combination therapy in patients
with type 2 diabetes mellitus: a randomized controlled trial,
JAMA 283 (2000) 1695–1702.
[34] Z. Kerenyi, H. Samer, R. James, Y. Yan, M. Stewart, Combina-
tion therapy with rosiglitazone and glibenclamide compared
with upward titration of glibenclamide alone in patients with
type 2 diabetes mellitus, Diabetes Res. Clin. Pract. 63 (2004)
213–223.
[35] H.E. Lebovitz, J.F. Dole, R. Patwardhan, E.B. Rappaport, M.I.
Freed, Rosiglitazone Clinical Trials Study Group, Rosiglitazone
monotherapy is effective in patients with type 2 diabetes, J. Clin.
Endocrinol. Metab. 86 (2001) 280–288.
[36] L.S. Phillips, G. Grunberger, E. Miller, R. Patwardhan, E.B.
Rappaport, A. Salzman, Once- and twice-daily dosing with
rosiglitazone improves glycemic control in patients with type
2 diabetes, Diabetes Care 24 (2001) 308–315.
[37] M. St John Sutton, M. Rendell, P. Dandona, J.F. Dole, K.
Murphy, R. Patwardhan, et al., A comparison of the effects of
rosiglitazone and glyburide on cardiovascular function and
glycemic control in patients with type 2 diabetes, Diabetes Care
25 (2002) 2058–2064.
[38] S. Mudaliar, A.R. Chang, R.R. Henry, Thiazolidinediones, per-
ipheral edema, and Type 2 diabetes: incidence, pathophysiology,
and clinical implications, Endocr. Prac. 9 (2003) 406–416.
[39] H. Zhang, A. Zhang, D.E. Kohan, R.D. Nelson, F.J. Gonzalez, T.
Yang, Collecting duct-specific deletion of peroxisome prolif-
erator-activated receptor gamma blocks thiazolidinedione-
induced fluid retention, Proc Natl Acad Sci U S A 102 (2005)
9406–9411.
[40] Y. Guan, C. Hao, D.R. Cha, R. Rao, W. Lu, D.E. Kohan, et al.,
Thiazolidinediones expand body fluid volume through PPAR-
gamma stimulation of ENaC-mediated renal salt absorption, Nat
Med 11 (2005) 861–866.
[41] J. Sakamoto, H. Kimura, S. Moriyama, H. Odaka, Y. Momose, Y.
Sugiyama, et al., Activation of human peroxisome proliferator-
activated receptor (PPAR) subtypes by pioglitazone, Biochem
Biophys Res Commun 278 (2000) 704–711.
[42] J.P.T. Higgins, S. Green (Eds.), Cochrane Handbook for Sys-
tematic Reviews of Interventions 4.2.5 (2005). Available from
http://www.cochrane.dk/cochrane/handbook/hbook.htm,
accessed May 4, 2006.
[43] E. Chiquette, G. Ramirez, R. DeFronzo, A meta-analysis com-
paring the effect of thiazolidinediones on cardiovascular risk
factors, Arch. Intern. Med. 164 (2004) 2097–2104.
[44] A.J. Sutton, S.J. Duval, R.L. Tweedie, K.R. Abrams, D.R. Jones,
Empirical assessment of effect of publication bias on meta-
analyses, BMJ 320 (2000) 1574–1577.



























![Uveitic macular edema: a stepladder treatment paradigm€¦ · of macular edema [1,3–4], this review will focus on uveitic macular edema specifically. Uveitic macular edema Macular](https://static.cupdf.com/doc/110x72/5ed770e44d676a3f4a7efe51/uveitic-macular-edema-a-stepladder-treatment-paradigm-of-macular-edema-13a4.jpg)

