



therapeutic architecturehousing for people with dementia

by Elizabeth A. Campbell
A design thesis submitted to the Graduate Faculty at VirginiaPolytechnic Institute and State University in partial fulfillment ofthe degree of
Master of Architecture
July 22th, 2005Alexandria Virginia
Defense Date: May 11th, 2005
Paul Emmons, Chair
Susan Piedmont-Palladino
Jaan Holt

introcontentsabstractapproach & idea
developmentcontext / siteprogramprocess
design detailssingle roomreflected ceiling planroom sectiondouble roomwindow detailresidence hallwayliving areaaquatic therapylight well
final designelevationsfloor planssectionsmodel
conclusiondefensebibliography / creditsvita
iiiiii
1-34-78-11
12131415161718
19-2021
22-2526-3435-3637-40
414243
contents
i
intro

abstract
An environment strongly influences the behaviorof individuals with dementia. A well designedphysical environment can maintain and enhancethe ability to function and improve quality of life.My thesis uses a residential environment for peo-ple suffering from dementia as the basis for ther-apeutic intervention. Understanding the physicaland psychological effects of architecture on aperson with dementia is an important tool in slow-ing the progression and effects of the disease.The competence of an individual can effect howhe or she experiences a space and can makethem respond more intensively to the immediateenvironment. Building orientation, color, lighting,and access to nature can affect the psyche of aresident and can help stabilize and reduce theeffects of the disease.
ii
intro
Dementia is a brain dysfunction that leads togradual memory loss and restrictions of dailyactivities. The most common form of dementiais Alzheimer's disease. As our population ages,the number of dementia cases increase, andthe need for long term care settings rises. Theresponse to the growing need of housing hasprimarily been a suburban complex that isremotely located. For most urban residents thetransition to a residential care setting takesthem away from their family and community. Iwanted to create a building in an urban environ-ment that gives people options for choosingcare.
The following thesis presents a design for urbanhousing that focuses on care for people withdementia. My goal was to design spaces thattake greater responsibility for the health of thismentally and physically frail older population ina residential setting rather than an institutionalenvironment. Being both an architecturaldesigner and once a caregiver to a loved onewith dementia has given me a combination ofknowledge and experience that has helped meto understand and take into consideration theimportance of a space in which a person withdementia spends his or her final time. Peoplesuffering from dementia often experience disori-entation, memory lapses, confusion, agitation,and frustration. The environment has a large
impact on this behavior. The competence of anindividual can also effect how he or she experi-ences a space. A dementia patient's visualresponse to light and their perception of spacechanges as the disease progresses. It becomesmore difficult to focus when moving betweenlight levels. Bright light exposure can reduceagitated behavior in some Alzheimer's patients.Institutional environments can be stressful, andstress can increase the effects of dementia aswell as cause changes in immunity that makesthem more susceptible to infection and viruses.These environments can be stressful not only toresidents but also nurses, employees, and visi-tors. Building orientation can reduce confusionand facilitate wayfinding which reduces stressand can improve the quality of life of a resident.The environment should stabilize and build thecompetency of individual residents and helpmaintain their independence. Some designintentions that helped guide the form of the proj-ect include:- clear wayfinding- increase awareness and orientation- provide mental and physical stimulation- allow options for private and social interaction- create a safe environment- respect independence and privacy- be able to adapt to changing needs- provide access to nature- maximize daylight, minimize glare
iii
approach & idea
intro

The site is located at 23rd and P Streets in Northwest Washington, D.C. Blocks to the north, east,and south follow the urban fabric of the City. North of the site is a small park. To the west is whereRock Creek Park cuts the grid of the city. The park winds along the creek and under a series of archedbridges. The parkway has long served as both a recreation area for local residents and an attractivecommuter route linking downtown Washington with its northwest suburbs.
1
context / sitearial
N
deve
lopm
ent
2
context / siteplan
deve
lopm
ent
0 40’ 80’ 200’
N
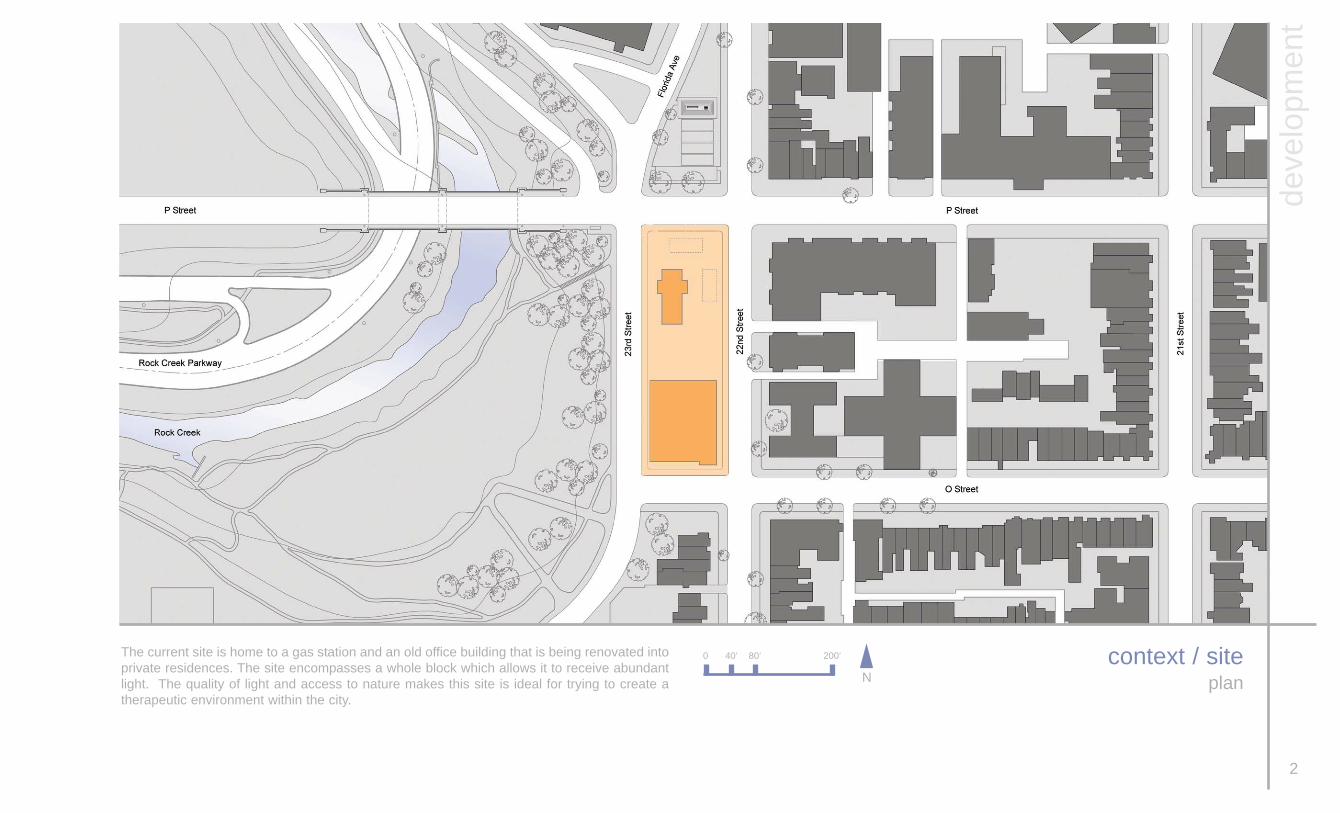
The current site is home to a gas station and an old office building that is being renovated intoprivate residences. The site encompasses a whole block which allows it to receive abundantlight. The quality of light and access to nature makes this site is ideal for trying to create atherapeutic environment within the city.

context / sitephotographs
3
deve
lopm
ent

The site is long and narrow. It runs north to south which makes the majority of the exteriorwalls face either west or east. This east / west divide helped to guide the design and programfor the building. I researched the routines of residents of similar care centers to understandwhich spaces they occupied at different times of day. Morning light can be one of the mostbeneficial qualities in trying to create a therapeutic space. I found that bathing rooms and din-ing rooms received the most use in the morning. So these functions were placed on the eastside of the building to receive the maximum morning light. The private rooms were designedto face west to give each resident views of Rock Creek Park. This access to nature can makea significant difference in the quality of life of a resident.
4
program
deve
lopm
ent
WEST
views of natureevening sun
residents roomsoffices
meeting roomsphysical therapy rooms
adult day carechild day careroof gardens
EAST
views of citymorning sun
resident’s living spacesbathing roomsnurse stations
resident floors outdoor spaceretail spaces
aquatic therapy roomadult day carechild day careroof gardens

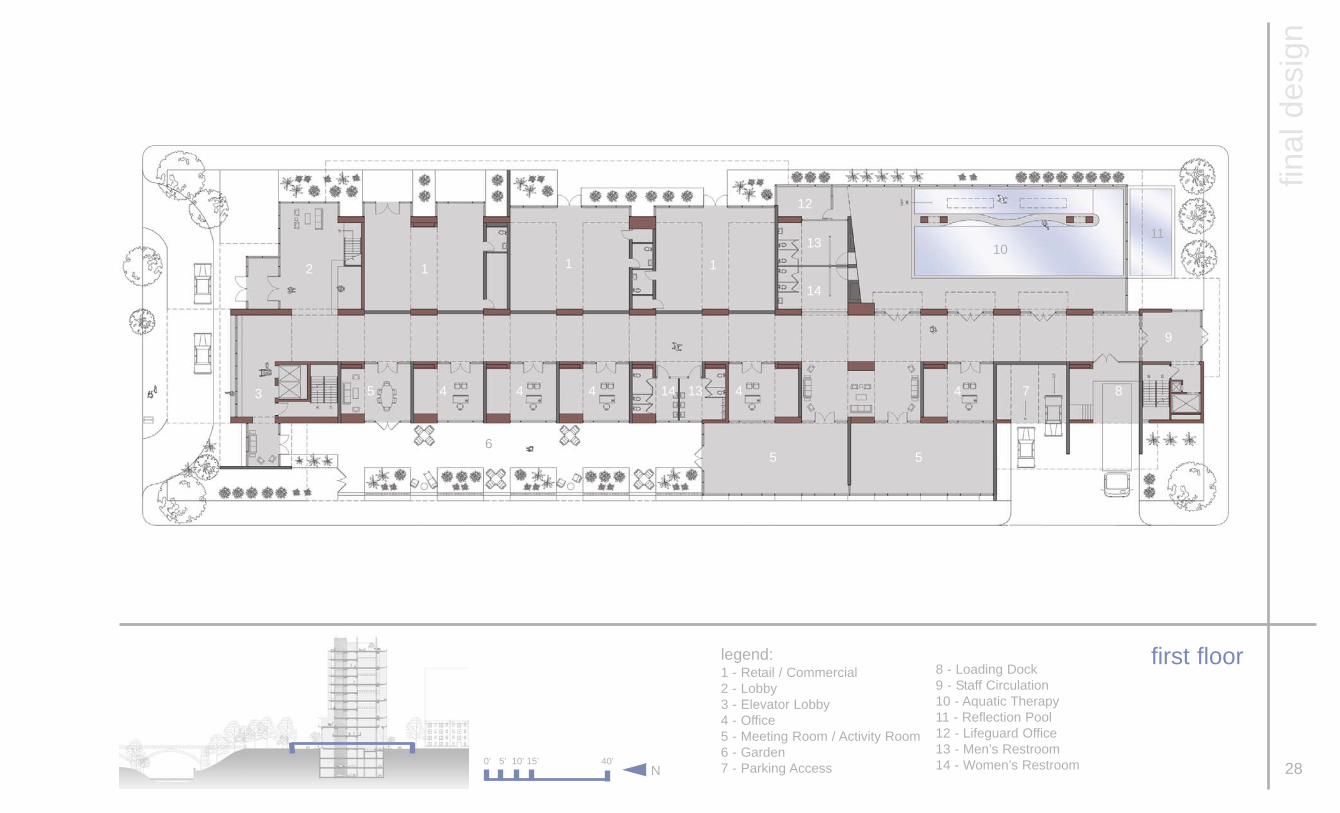
Throughout the design process the program and organizations of the building didnot change significantly. Once I determined the site I developed the program forthe building. The main focus of this building is a therapeutic residential environ-ment for people with dementia or Alzhiemer’s disease. The residence floors takeup the upper 7 floors of the building. The other floors service the residents andthe community as well. The first floor has retail spaces for shops, restaurants, cof-fee shops, and similar functions. These spaces provide places for residents andfamily members to get away to, but remain close at the same time. The first flooralso has offices, meeting / activity rooms and the aquatic therapy pool.
5
programp street
deve
lopm
ent
retailoffices
multipurpose rooms
staff / nurse area
recreation / therapy
child day care
adult day care
residents rooms
living spaces
parking
circulation
kitchen / laundry
6
program
deve
lopm
ent
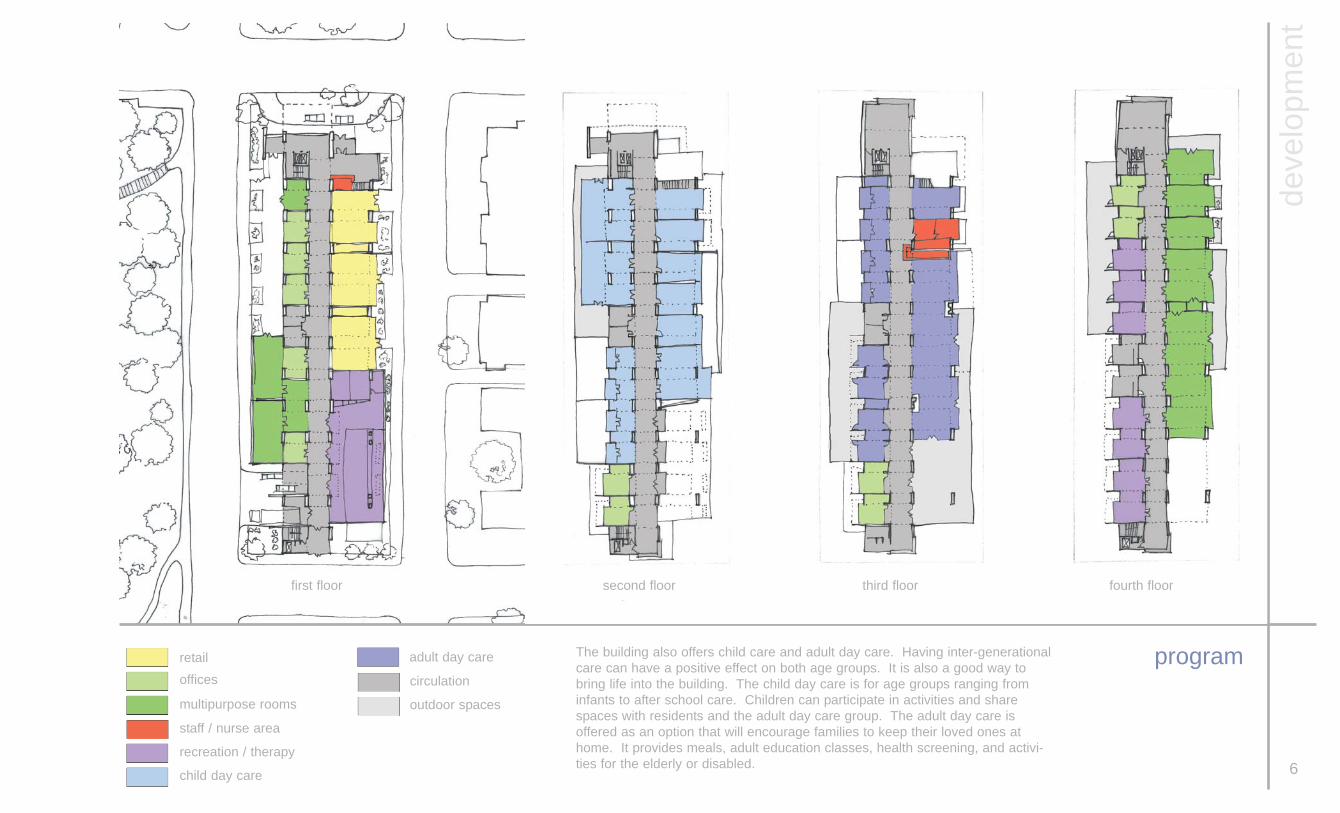
The building also offers child care and adult day care. Having inter-generationalcare can have a positive effect on both age groups. It is also a good way tobring life into the building. The child day care is for age groups ranging frominfants to after school care. Children can participate in activities and sharespaces with residents and the adult day care group. The adult day care isoffered as an option that will encourage families to keep their loved ones athome. It provides meals, adult education classes, health screening, and activi-ties for the elderly or disabled.
retailoffices
multipurpose rooms
staff / nurse area
recreation / therapy
child day care
adult day care
circulation
outdoor spaces
first floor second floor third floor fourth floor

7
program
deve
lopm
ent
The residence floors occupy most of the building. There are single and doublerooms for elderly residents. Spaces can accommodate residents from inde-pendent living, to those in severe stages of dementia and Alzheimer’s disease.Each resident floor groups 11-15 residents. The nursing staff can be shifted asthe needs of each living cluster change.
staff / nurse areabathing room
residents rooms
living spaces
circulation
outdoor spaces
5th, 7th, 9th, 11th floor 6th, 8th, 10th floor roof garden

8
processsingle room
deve
lopm
ent
The design process began with the individual room. This is the place where a resident spends mostof his or her time. I wanted to create a therapeutic environment that is designed specifically for a per-son with dementia or Alzheimer’s disease. Throughout my thesis the room has evolved significantlybut still maintained some of my earlier design intentions. The front porch idea was something that Iwanted to include when I began to research this topic. The ability to control the natural light and stillmaintain the view of nature was also an important aspect to the room design.

9
processresidence floors
deve
lopm
ent
The early program and room design are evident in most of the schemes for the building design. I triedto accomplish all my original desires to have the rooms face west, the living areas face east. I want-ed the circulation to run along the center of the building but to still allow it to have access to naturallight and to create an open feel.

10
processresidence floors
deve
lopm
ent

11
process
deve
lopm
ent

The residence room is designed to be an environment that can accommodate a resident at any stageof dementia. The main living space is an open flexible studio that allows furniture placement to changewith each resident. The bathroom / changing area is sperate by sliding panels that can be closed com-pletely or pushed away so that all the functions of the space are visible to the resident. This can bevery important to a person with dementia. They may not remember or realize that there is somethingbehind the closed doors. So having the toilet and sink be visible it can help prevent incontinence andpromote self care.
12
single roomplan
desi
gn d
etai
ls

Residents in the later stages of dementia and Alzheimer’s disease will begin to spend more time intheir beds as their mobility decreases. I wanted to do something more to the ceiling than just sus-pended tiles and florescent lighting. There are a series of floating panels that are stretched canvas,acrylic, and painted drywall. They give depth the the ceiling plane as well as diffusing the artificial light-ing to prevent unwanted glare. As we age our sensitivity to glare changes and it makes it more diffi-cult to focus in changing light levels.
13
single roomreflected ceiling plan
desi
gn d
etai
ls

14
single roomsection
desi
gn d
etai
ls

15
double room / suiteplan
desi
gn d
etai
ls
Each floor has a double room or suite that can be used for a person in early stages of dementia or forrelated patients who want to share a room. The space is similar the single room but provides a littlemore privacy to the residents. It is similar to an apartment that has its own kitchen and full bathroomand private bedroom. It is a good transition space for a resident who may need assistance from anurse but is still very independent.

Each residence floor has one large open outdoor space off of the main living area for residents to use.The outdoor area is easily observed by the nursing staff. I wanted to have some kind of outdoor con-nection with each private room as well. But the private rooms need to be a place where the residentcan be alone and be safe at the same time. An accessible balcony was not an option for the privaterooms. Instead a planting area was provided to allow the residents and family a place to garden. Theplanters are accessible from two swinging windows that open to allow a person to reach the plantersstanding as well as sitting. It allows each resident and visitors to personalize each space. The con-crete planting area also functions as a shading device for the floor below. It controls the light but stillallows full views of the park below.
16
window detail
desi
gn d
etai
ls

Double loaded corridors can be disorienting to a person with dementia. Clear wayfinding is an impor-tant way to reduce stress among residents. The main hall in the residence floor has private rooms lin-ing one side while the other is open to the living space. Corridors are designed to simulate a street.Each room has a small seating area that acts as a front porch for the residents. There is a displaycase to emphasize each person’s separate space and individuality. This area acts as a transitionspace which allows residents to gradually enter social situations in the main living areas. A “dutch”-door is used to allow the staff to constantly supervise without hovering. It also allows the resident asense of privacy and to keep unwanted residents from wandering into their room. 17
residence hallway
desi
gn d
etai
ls

Each residence floor has an open living and dining space off of the main corridor. These spaces faceeast to get maximum morning light. There are double height spaces that alternate up through thebuilding to allow the interaction between the floor above and below. Open spaces alternate locationsevery floor so that there is not one large open space the entire height of the building. A large openarea can be overwhelming to a person with dementia.
18
living areaperspectives
desi
gn d
etai
ls
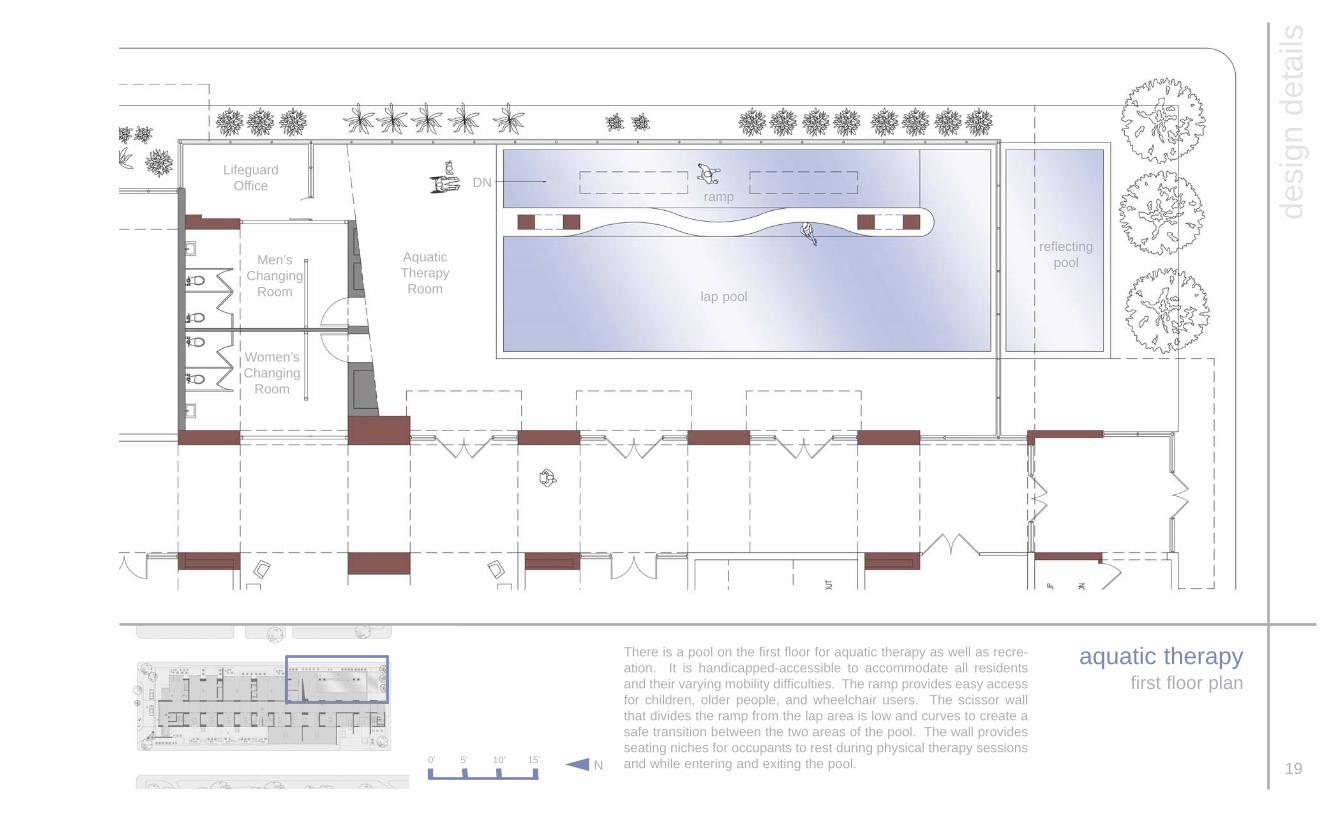
There is a pool on the first floor for aquatic therapy as well as recre-ation. It is handicapped-accessible to accommodate all residentsand their varying mobility difficulties. The ramp provides easy accessfor children, older people, and wheelchair users. The scissor wallthat divides the ramp from the lap area is low and curves to create asafe transition between the two areas of the pool. The wall providesseating niches for occupants to rest during physical therapy sessionsand while entering and exiting the pool. 19
aquatic therapyfirst floor plan
desi
gn d
etai
ls
0’ 5’ 10’ 15’ N
DNLifeguard
Office
Men’sChanging
Room
Women’sChanging
Room
Aquatic Therapy Room
reflectingpool
lap pool
ramp
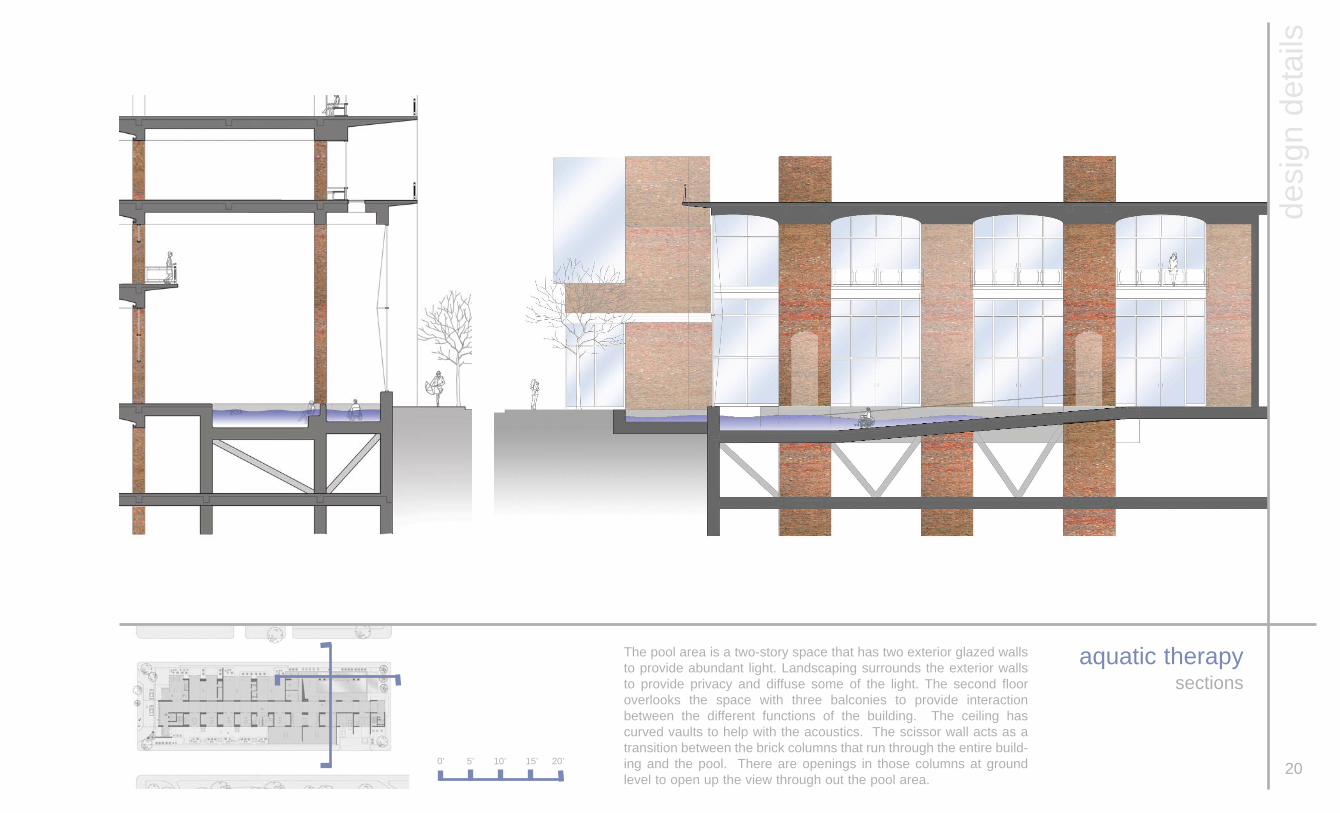
The pool area is a two-story space that has two exterior glazed wallsto provide abundant light. Landscaping surrounds the exterior wallsto provide privacy and diffuse some of the light. The second flooroverlooks the space with three balconies to provide interactionbetween the different functions of the building. The ceiling hascurved vaults to help with the acoustics. The scissor wall acts as atransition between the brick columns that run through the entire build-ing and the pool. There are openings in those columns at groundlevel to open up the view through out the pool area.
20
aquatic therapysections
0’ 5’ 10’ 15’ 20’
desi
gn d
etai
ls

21
light wellkitchen / laundry rooms
desi
gn d
etai
ls
In the kitchen and laundry areas on the lower level there are lightwells that run along the exterior of the building. They wash naturallight down the interior wall creating a soft indirect light.

22
view from p street
final
des
ign

23
view from 23rd street
final
des
ign

24
view from o street
final
des
ign

25
view from 22nd street
final
des
ign

26
site plan
0’ 40’ 80’ 200’N
final
des
ign

27
lower level 1lower level 2 & 3
0’ 10’ 20’ 50’N
final
des
ign
legend:1 - Mechanical / Storage2 - Kitchen3 - Laundry4 - Elevator Lobby5 - Men’s Restroom6 - Women’s Restroom7 - Parking Ramp
1 1 1 1 1 1
3 2
1 1 1 1 6 5 1 1 1
4 4
4
4
1
1
7
7
28
first floor
0’ 5’ 10’ 15’ 40’N
final
des
ign
1 112
3 5 4 4 4 14 13 4 4 7 8
5 5
9
10
12
13
14
11
legend:1 - Retail / Commercial2 - Lobby3 - Elevator Lobby4 - Office5 - Meeting Room / Activity Room6 - Garden7 - Parking Access
8 - Loading Dock9 - Staff Circulation10 - Aquatic Therapy11 - Reflection Pool12 - Lifeguard Office13 - Men’s Restroom14 - Women’s Restroom
6

29
secondfloor
N
final
des
ign
legend:1 - Elevator Lobby2 - Library3 - Classroom4 - After-school Room5 - Study Room6 - Art / Music Room7 - Computer Room8 - Office
9 - Staff Circulation10 - Boy’s Restroom11 - Girls’s Restroom12 - Balcony13 - Outdoor SpaceOTB - Open to BelowOTA - Open to Above
OTB 2 3 3 3 3 4 OTB
6 7 13
11 10 5 5 5 5 8 8
12 12 12
12 12 12 12
OTB OTB
19
OTA OTA
0’ 5’ 10’ 15’ 40’

30N
final
des
ign
2 3 3 4 4 12
1 5 5 5 5 6 7 8 8 9 9 10 10 11
12
13 13 13 13
OTB
third floorlegend:1 - Elevator Lobby2 - Library3 - Nurse / Staff Area4 - Living / Dining Area5 - Lounge6 - Women’s Restroom7 - Men’s Restroom
8 - Women’s Resting Area9 - Men’s Resting Area10 - Office11 - Staff Circulation12 - Outdoor Space13 - BalconyOTB - Open to Below0’ 5’ 10’ 15’ 40’

31
fourth floor
N
final
des
ign
legend:1 - Elevator Lobby2 - Activity Room3 - Office4 - Lounge5 - Women’s Restroom
6 -Men’s Restroom7 - Physical Therapy Room8 - Staff Circulation9 - Outdoor Space
9 2 2 2 2 2 2
1 3 3 4 4 4 5 6 7 7
9
9
8
0’ 5’ 10’ 15’ 40’

32N
final
des
ign
legend:1 - Elevator Lobby2 - Family Room3 - Bathing Room4 - Nurse / Staff Area5 - Dining / Living Area
6 - Double Room7 - Single Room8 - Staff Circulation9 - Outdoor Space
5th, 7th, 9th, 11th floor
9 2 3 4 4 OTB 5 5 9
1 6 6 7 7 7 7 7 7 7 7 7 8
OTA
0’ 5’ 10’ 15’ 40’

33N
final
des
ign
legend:1 - Elevator Lobby2 - Family Room3 - Bathing Room4 - Nurse / Staff Area5 - Dining / Living Area
6 - Double Room7 - Single Room8 - Staff Circulation9 - Outdoor Space
9 2 3 4 4 5 5 OTB
1 6 6 7 7 7 7 7 7 7 7 7 8
OTA
6th, 8th, 10th floor
9
0’ 5’ 10’ 15’ 40’
34
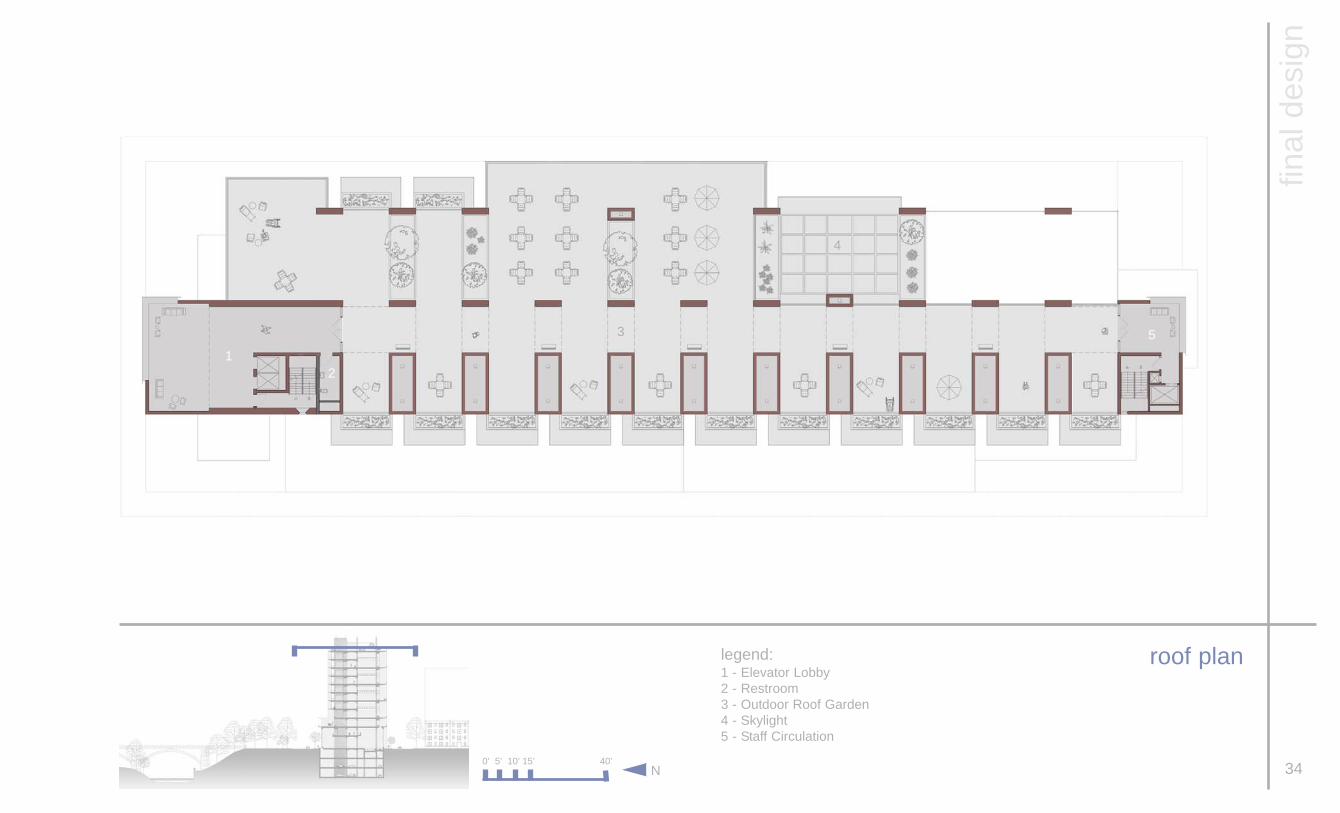
roof plan
N
final
des
ign
legend:1 - Elevator Lobby2 - Restroom3 - Outdoor Roof Garden4 - Skylight5 - Staff Circulation
15
2
3
4
0’ 5’ 10’ 15’ 40’

35
section
0 10’ 20’ 30’ 70’
final
des
ign

36
section
final
des
ign
0 10’ 20’ 30’ 70’

37
exterior views
final
des
ign

38
view looking east
final
des
ign

39
view looking south
final
des
ign

40
view looking east
final
des
ign

41
defense

References:
Amducci,L., ed. Aging of the Brain andDementia: Raven Press. New York: 1980
Brawley, Elizabeth C. Designing forAlzheimer’s Disease: Strategies for CreatingBetter Care. John Wiley & Sons, Inc. NewYork: 1997
Corkin, Suzanne, ed. Alzheimer's Disease : AReport of Progress in Research: RavenPress. New York:1982.
Fraser, Morris. Dementia : Its Nature andManagement: Wiley Chichester, New York :1987
Kitwood, Tom. Dementia Reconsidered: ThePerson Comes First: Open University Press:Buckingham, England & Philadelphia :
Landau, Elaine. Alzheimer's Disease: FranklinWatts: New York: 1996.
Leibrock, Cynthia. Design Details for Health:Making the Most of Interior Design’s HealingPotential. John Wiley & Sons, Inc. New York:2000
Miller, Nancy, ed./ Cohen, Gene, ed. ClinicalAspects of Alzheimer's Disease and SenileDementia: Raven Press. New York: 1981
Reisberg, Barry, ed.. Alzheimer's Disease:Free Press. New York: 1983
Samuel, David, ed. Aging of the Brain: RavenPress. New York: 1983.
Shamoian, Charles, ed. Biology and Treatmentof Dementia in the Elderly: AmericanPsychiatric Press: Washington, D.C.:1984.
Slaby, Andrew Edmund. Dementia in the pre-senium: Thomas.Springfield, Illinois: 1974
Turkington, Carol. The Encyclopedia ofAlzheimer's Disease: Facts on File. New York :2003
Weston, Richard. Alvar Alto: Phaidon PressLimited. London: 1995
Wells, Nicholas E. Dementia in Old Age:Office of Health Economics. London: 1979
Zarit, Steven/ Zarit, Judy/ Orr, Nancy. WorkingWith Families of Dementia Victims: Volume IV:A Treatment Manual: U.S. Dept. of Health andHuman Services, Office: Washington, D.C.:
bibliography
42
Note:
all text and images are by author unlessotherwise noted
Case Studies:
Drake Center151 West Galbraith RoadCincinnati, Ohio 45216
Meadowbrook Care Center 8211 Weller RoadCincinnati, Ohio 45242

Elizabeth A. Campbell
February 8th, 1981Rochester, New York
education:
Master of ArchitectureVirginia Polytechnic Institute and State UniversityWashington - Alexandria Campus2005
Bachelor of Arts in ArchitectureMiami UniversityOxford, Ohio2003
experience:
Lewis & AssociatesAlexandria, Virginia2004 - 2005
BHDP ArchitectureCincinnati, Ohio2004
John Milner AssociatesAlexandria, Virginia2003 - 2004
FRCH Design WorldwideCincinnati, Ohio2003
vita
43





























