The Shoulder andShoulder Girdle
PAINFUL SHOULDER SYNDROMES, IMPINGEMENT SYNDROMES: NONOPERATIVE
MANAGEMENT
Ghurki Trust Teaching Hospital
Categories of Painful ShoulderSyndromes

Neer’s Classification of Rotator Cuff Disease

• Stage I. Edema, hemorrhage (patient usually <25 years of age)
• Stage II. Tendonitis/bursitis and fibrosis (patient usually 25 to 40 years of age)
• Stage III. Bone spurs and tendon rupture (patient usually >40 years of age)
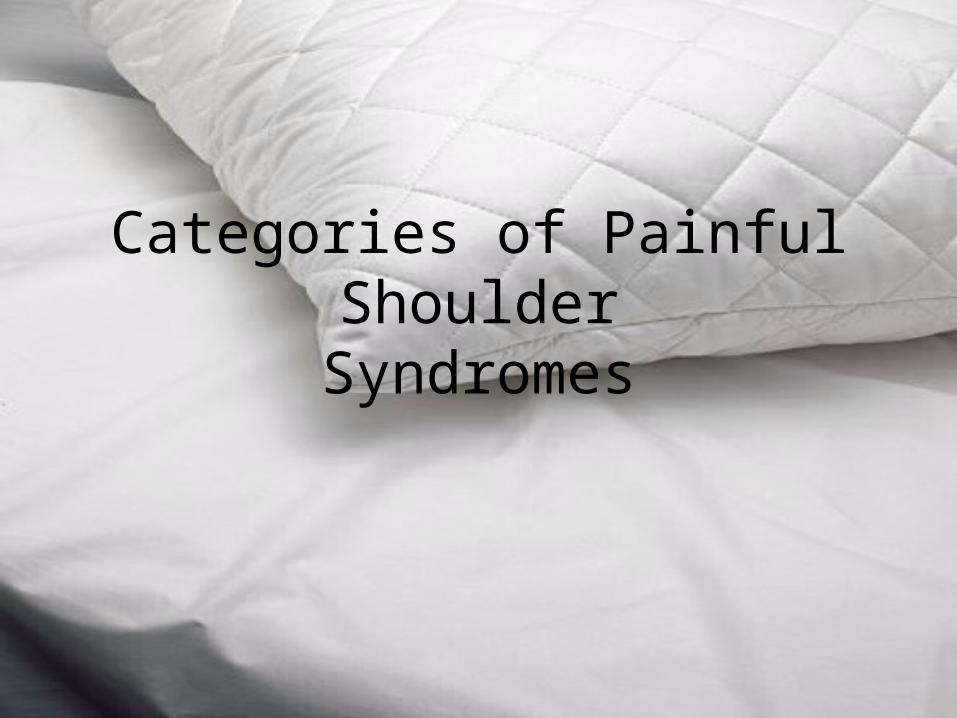
Jobe’s classification of impingement

• Group 1. Pure impingement (usually in an older recreational athlete with partial undersurface rotator cuff tear and subacromial bursitis)
• Group 2. Impingement associated with labral and/or capsular injury, instability, and secondary impingement
• Group 3. Hyperelastic soft tissues resulting in anterior or multidirectional instability and impingement (usually attenuated but intact labrum, undersurface rotator cuff tear)
• Group 4. Anterior instability without associated impingement (result of trauma; results in partial or complete dislocation)
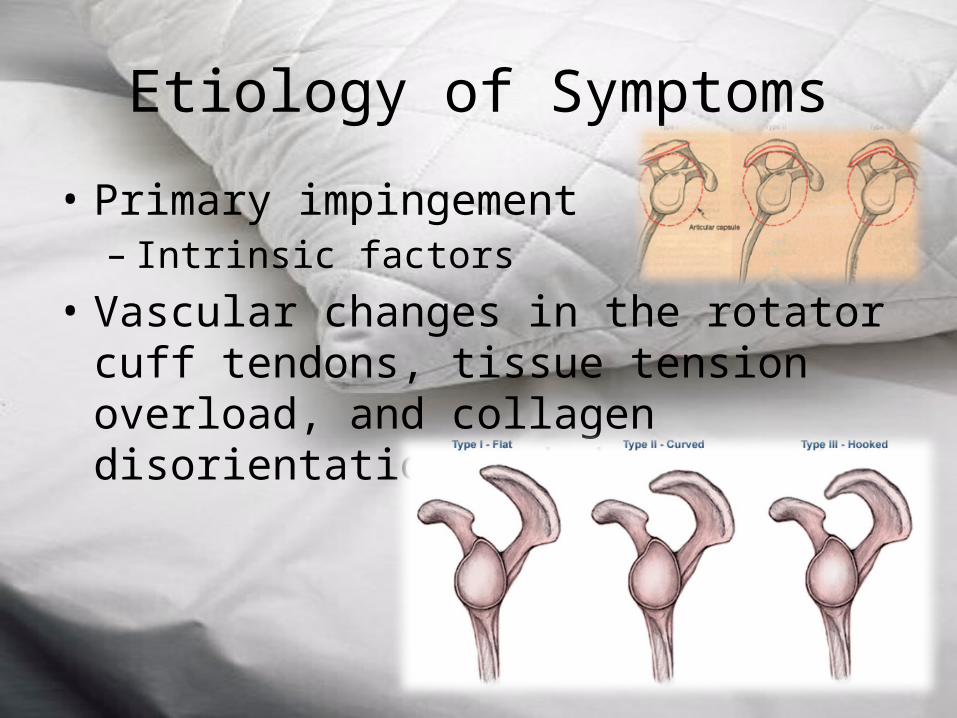
Etiology of Symptoms
• Primary impingement– Intrinsic factors
• Vascular changes in the rotator cuff tendons, tissue tension overload, and collagen disorientation and degeneration
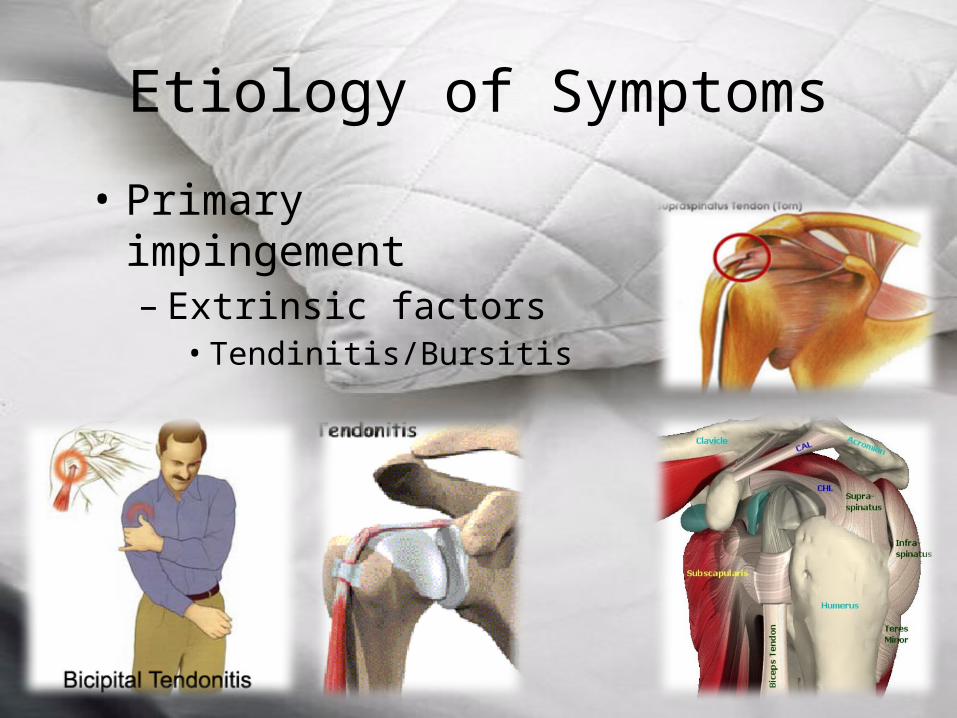
Etiology of Symptoms
• Primary impingement– Extrinsic factors• Tendinitis/Bursitis
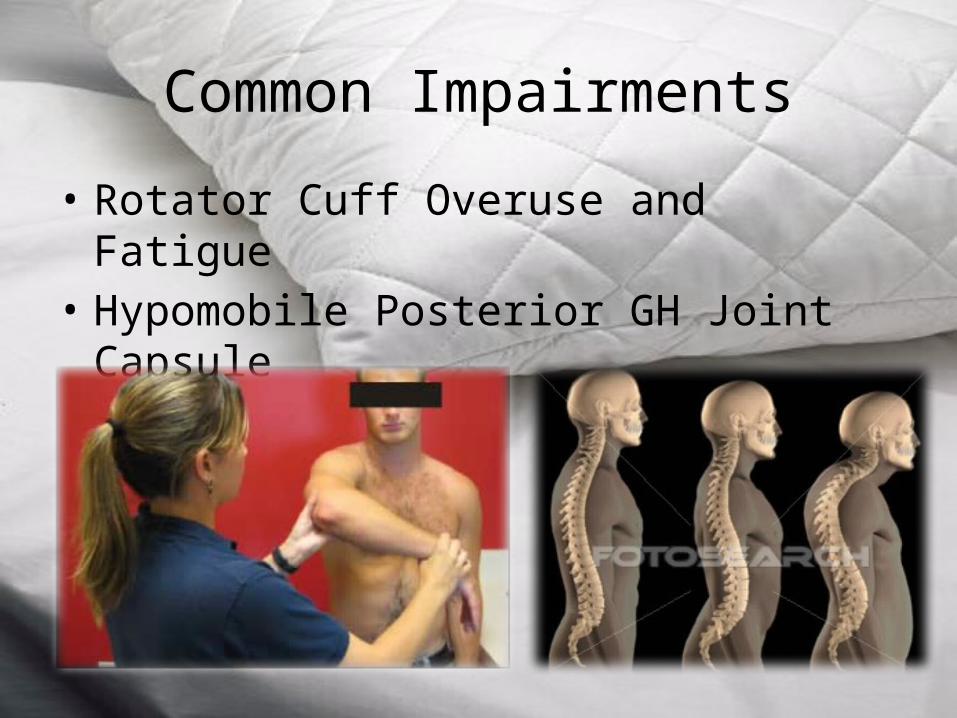
Common Impairments
• Rotator Cuff Overuse and Fatigue• Hypomobile Posterior GH Joint Capsule

Impaired posture
• Increased thoracic kyphosis, forward head, and protracted and forward-tilted scapula are often identified as related to impingement syndrome.
• Faulty scapular alignment may be one factor in decreasing the suprahumeral space and therefore leading to irritation of the rotator cuff tendons with overhead activities
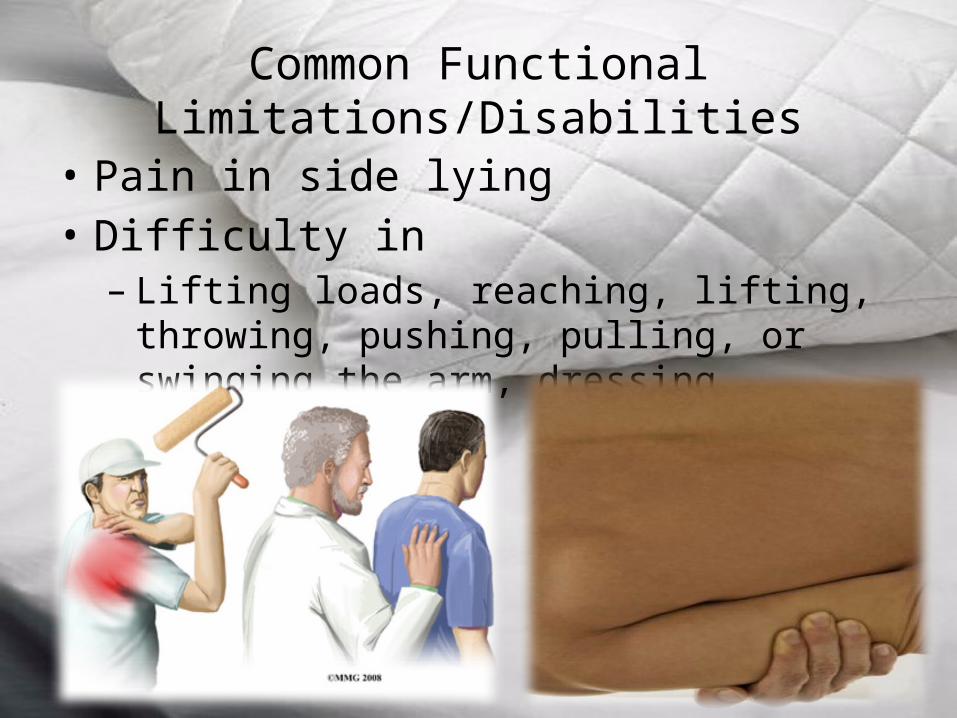
Common Functional Limitations/Disabilities
• Pain in side lying• Difficulty in– Lifting loads, reaching, lifting, throwing, pushing,
pulling, or swinging the arm, dressing
Management: Painful ShoulderSyndromes (Without Dislocation)

Management: Protection Phase
• Massage• Support
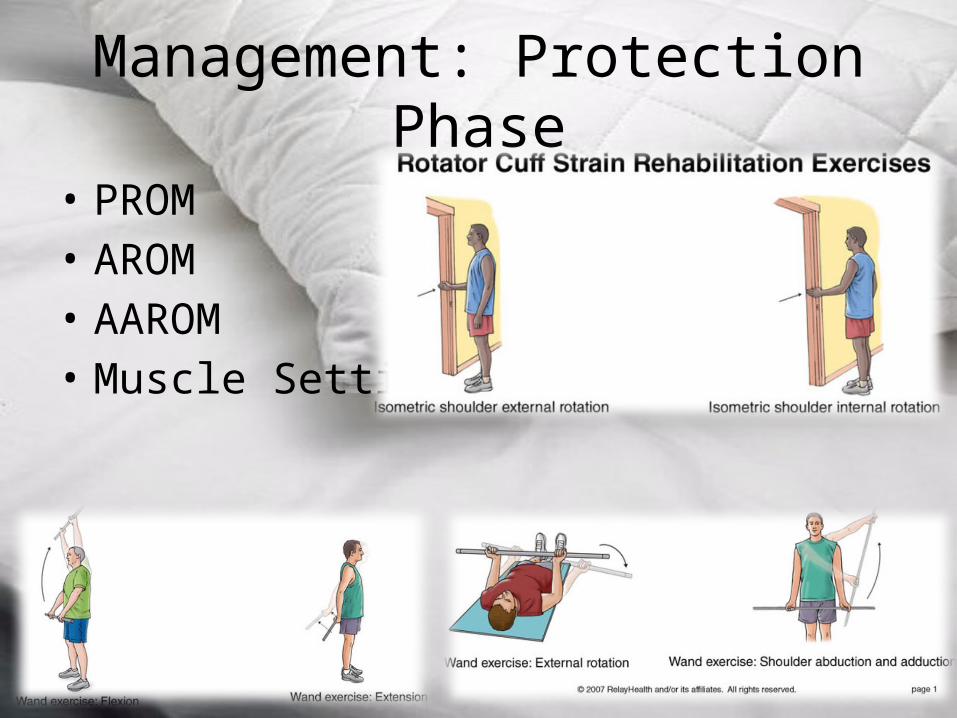
Management: Protection Phase
• PROM• AROM• AAROM• Muscle Setting
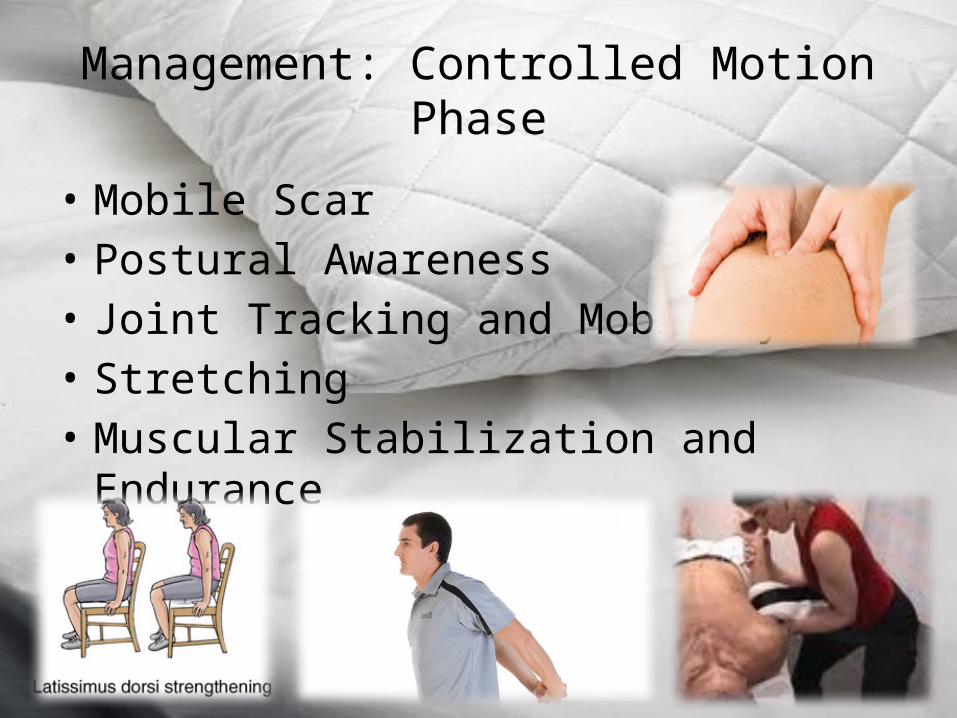
Management: Controlled Motion Phase
• Mobile Scar• Postural Awareness• Joint Tracking and Mobility• Stretching• Muscular Stabilization and Endurance

Management: Return to Function Phase

PAINFUL SHOULDER SYNDROMES:SURGERY

Rotator Cuff Repair

Indications for Surgery
• Partial-thickness with irreversible degenerative changes
• Neer stage II lesions• Neer stage III lesions• Acute full-thickness tear
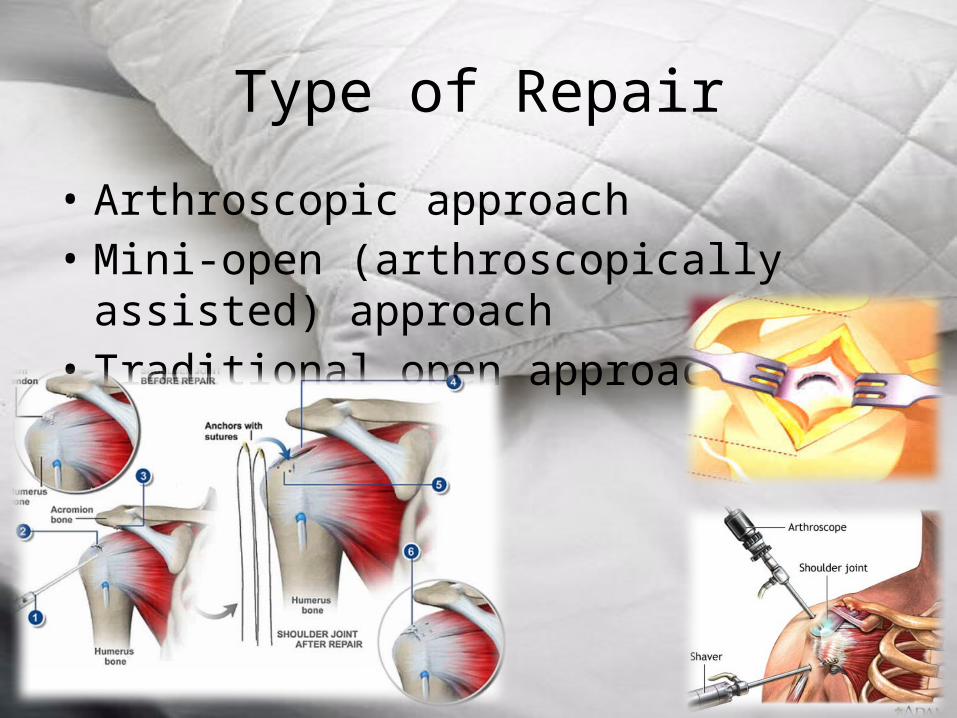
Type of Repair
• Arthroscopic approach• Mini-open (arthroscopically assisted) approach• Traditional open approach
Postoperative Management

Maximum Protection Phase
• Control pain and inflammation• Prevent loss of mobility of peripheral joints• Restore shoulder mobility• Correct postural deviations• Develop control of scapulothoracic stabilizers• Prevent inhibition and atrophy

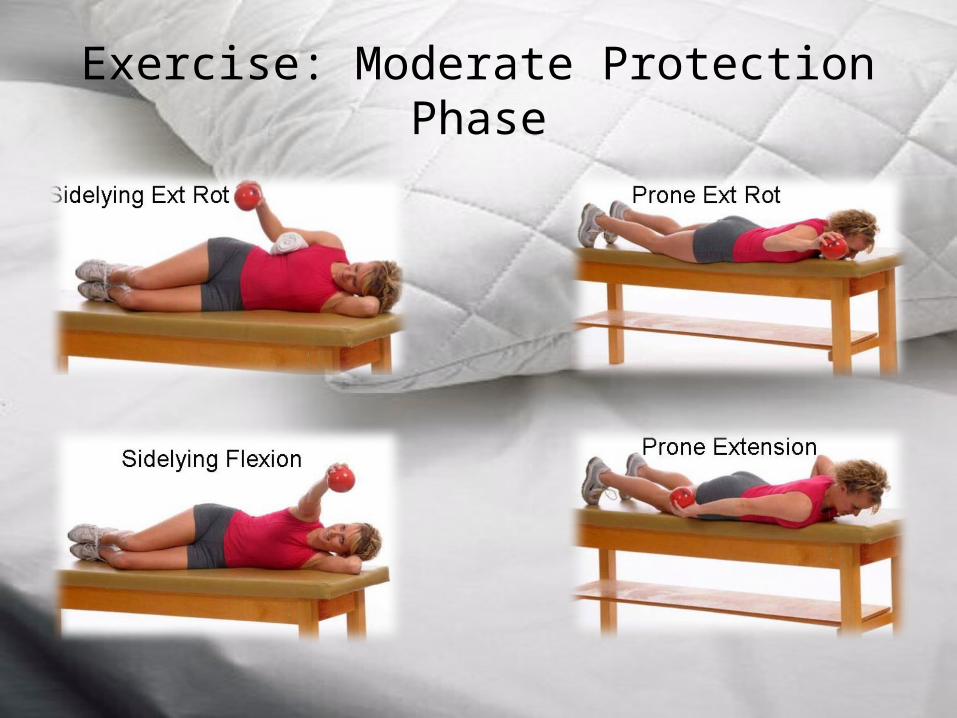
Exercise: Moderate Protection Phase

Exercise: Minimum Protection/Return to Function Phase
Shoulder Instabilities:Nonoperative Management
• Atraumatic Hypermobility• It may be the result of physiological laxity of the connective tissues
or repetitive non uniform loading of the joint.• Anterior instability usually occurs with forces against the arm when
it is in an abducted and externally rotated position, resulting in anterior humeral head translations.
• Posterior instability is much less common but can occur from repetitive forces against a forward-flexed humerus, translating the humeral head posteriorly
• Inferior instability is typically the result of rotator cuff weakness/paralysis and is frequently seen in patients with hemiplegia. It is also prevalent in patients who repetitively reach overhead (workers or swimmers, for example)

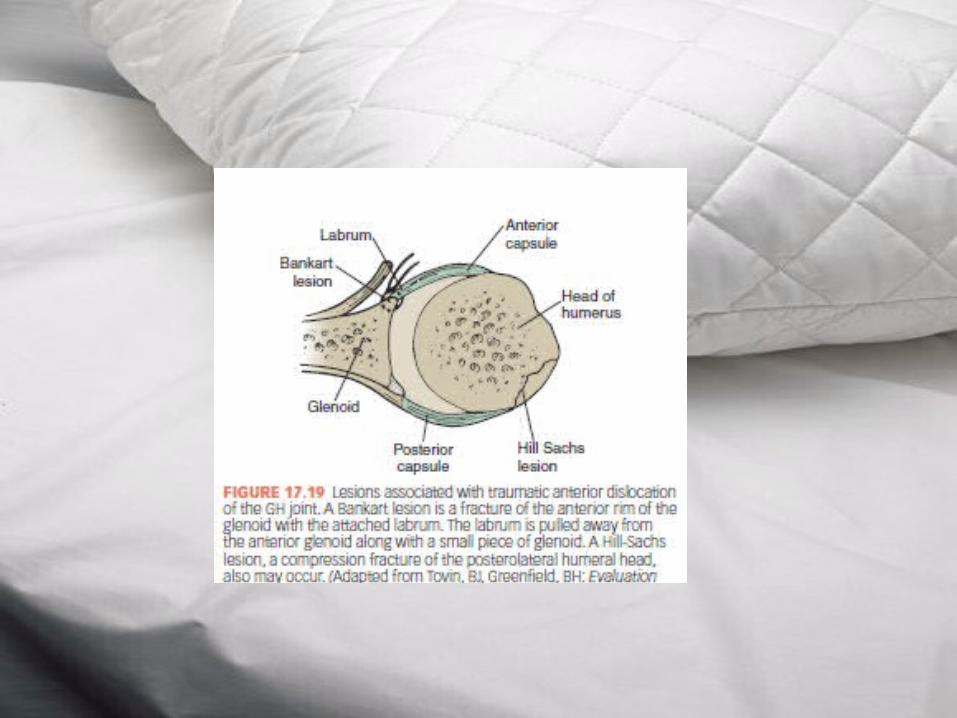
• Traumatic Hypermobility• Traumatic anterior shoulder dislocation• In shoulder abducted and externally rotated
position stability is provided by the subscapularis, GH ligaments (particularly the anterior band of the inferior ligament), and long head of the biceps. A significant force to the arm may damage these structures, along with the attachment of the anterior capsule and glenoid labrum (Bankart lesion)

• Traumatic posterior shoulder dislocation. Traumatic posterior shoulder dislocation is less common. The mechanism of injury is usually a force applied to the arm when the humerus is positioned in flexion, adduction, and internal rotation, such as falling on an outstretched arm

Closed Reduction of AnteriorDislocation
• Management: Protection Phase• Protect the Healing Tissue• Activity restriction is recommended for 6 to 8 weeks
in a young patient. If a sling is used, the arm is removed from the sling only for controlled exercise
• Promote Tissue Health• Protected ROM, intermittent muscle setting of the
rotator cuff, deltoid, and biceps brachii muscles, and grade II joint mobilization techniques

• Management: Controlled Motion Phase• Provide Protection• The patient continues to protect the joint and delay full return to
unrestricted activity. If a sling is being used, the patient increases the time the sling is off. The sling is used when the shoulder is tired or if protection is needed.
• Increase Shoulder Mobility• Mobilization techniques are initiated using all appropriate glides except
the anterior glide• Increase Stability and Strength of Rotator Cuff and Scapular Muscles• Both the internal and external rotators need to be strengthened as healing
occurs• Dynamic resistance, limiting external rotation to 50° and avoiding the
position of dislocation.
• Management: Return to Function Phase• Restore Functional Control• The following are emphasized.• A balance in strength of all shoulder and scapular muscles• Coordinated scapulothoracic and arm motions• Endurance for each previously described shoulder instability
exercise• As stability improves, progress to:• Eccentric training to maximum load.• Increasing speed and control of combined motions.• Simulating desired functional patterns for activity
Shoulder Instabilities:Surgery and Postoperative
Management
• Bankart repair. A Bankart repair involves an open or arthroscopic repair of a Bankart lesion (detachment of the capsulolabral complex from the anterior rim of the glenoid) which commonly accompanies a traumatic anterior dislocation. During the repair an anterior capsulolabral reconstruction is performed to reattach the labrum to the surface of the glenoid lip
Exercise: Maximum Protection Phase
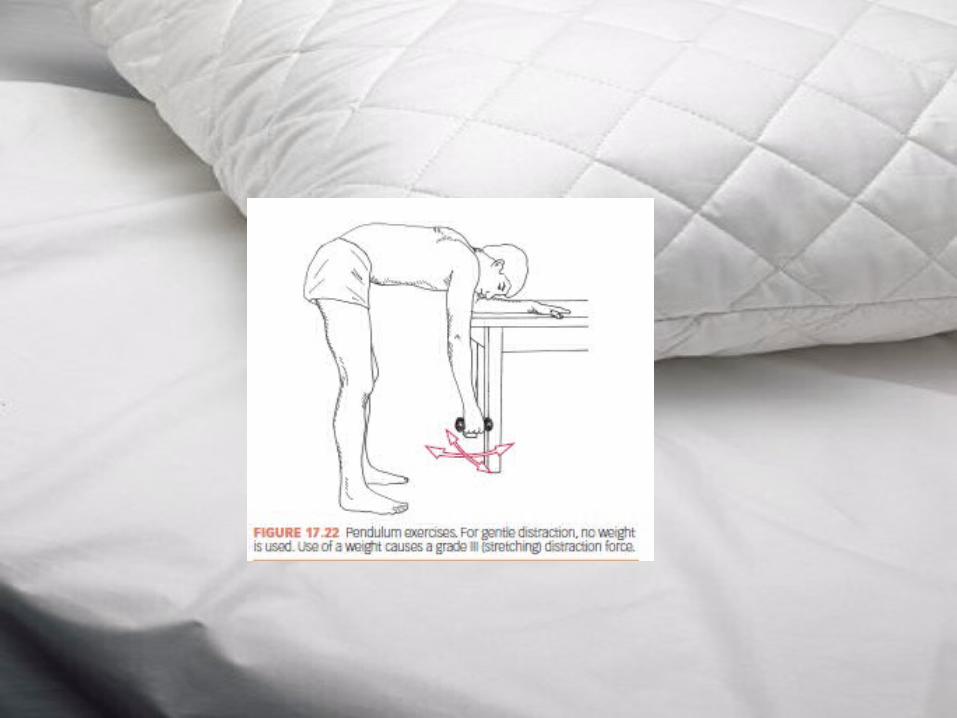
The initial phase of rehabilitation extends for about 6 weeks after surgery.• Control pain and inflammation.• A sling for comfort when the arm is dependent. • Cryotherapy and prescribed anti-inflammatory medication• Shoulder relaxation exercises• Prevent or correct posture impairments.• Emphasis on spinal extension and scapular retraction; avoid excessive thoracic kyphosis• Restore shoulder mobility while protecting tightened or• repaired tissues.• Pendulum exercises for the first 2 weeks postoperatively.• Self-assisted ROM and wand exercises for the GH joint within protected ranges as early
as 2 weeks or as late as 6 weeks postoperatively.• Prevent reflex inhibition and atrophy of GH musculature.• Multiple-angle, low-intensity isometric exercises of GH musculature as early as the first
week or by 3 to 4 weeks postoperatively
Exercise: Moderate Protection Phase
• Regain nearly full, pain-free, active ROM of the shoulder.
• Continue active ROM with the goal of achieving nearly full ROM by 12 weeks
• Continue to increase strength and endurance of shoulder musculature.
• Alternating isometrics against increasing resistance with emphasis on the scapula and rotator cuff musculature.
Exercise: Minimum Protection/Return to Function Phase
• This phase usually begins around 12 weeks postoperatively or as late as 16 weeks, depending on individual characteristics of the patient and the surgical stabilization procedure.
• Stretching should continue until ROM consistent with functional needs has been attained

Exercise interventions for the shoulder
• Girdle Exercise Techniques During Acute And Early Subacute Stages of tissue healing
• Exercise techniques to increase flexibility and range of motion
• Exercises to develop and improve muscle performance and functional control.