


ORIGINAL ARTICLE
The effect of TNF-alpha blockers on psychometric measuresin ankylosing spondylitis patients: a preliminary observation
Ozden Arısoy • Cemal Bes • Cigdem Cifci •
Mustafa Sercan • Mehmet Soy
Received: 14 June 2012 / Accepted: 4 January 2013 / Published online: 20 January 2013
� Springer-Verlag Berlin Heidelberg 2013
Abstract There is a high co-morbidity between chronic
inflammatory disorders and depression. Proinflammatory
cytokines like TNF-a seem to play a central role in the
pathogenesis of these disorders, and its neutralization pro-
vides a potent treatment for inflammatory disorders. Few
studies showed that TNF-a blockers also caused an
improvement in depressive symptoms associated with these
chronic inflammatory disorders. To evaluate the effective-
ness of TNF-a blockers on symptoms of ankylosing spon-
dylitis (AS), depression, anxiety and quality of life, 9 AS
patients resistant to classical therapy were enrolled and
followed-up at 2nd and 6th weeks after a TNF-a blocker
was started. Hamilton Depression and Anxiety Scales
(HAM-D, HAM-A), Hospital Depression and Anxiety
Questionnaire (HAD), Quality of Life Scale (SF36) and AS
severity index (BASDAI) were applied to the patients at
weeks 0, 2 and 6. ESR and CRP were evaluated to monitor
biological disease activity. There was a significant reduc-
tion in HAM-D (p = 0.00), HAM-A (p = 0.00), HAD
anxiety scores (p = 0.02) and a significant improvement in
SF36 physical function (p = 0.00), physical role limitations
(p = 0.00), bodily pain (p = 0.05), general health
(p = 0.01), vitality (p = 0.03) and emotional role limita-
tions (p = 0.00) subscales, BASDAI scores (p = 0.00),
ESR (p = 0.00) and CRP (p = 0.00). Change in clinical
disease activity (BASDAI) was not correlated with change
in depression–anxiety scores, while change in biological
disease activity (CRP) was correlated with change in
depression–anxiety scores. TNFa blockers may have a
potential antidepressant effect besides its anti-inflammatory
effect that seems to be independent of its clinical effect.
Keywords Ankylosing spondylitis � TNF-alpha blockers �Depression � Anxiety � Quality of life � Cytokines
Introduction
Ankylosing spondylitis (AS) is a systemic progressive,
chronic inflammatory disease primarily affecting the axial
skeleton causing pain, physical disability, functional
impairment and reduced quality of life (QOL) [1]. It may
also cause psychiatric symptoms since it has a substantial
effect on the mood of patients [2]. Although reduced
physical functioning is well recognized in AS, its impact
on social and mental health has not received that much
attention [1].
Among a few studies performed in the literature, Barlow
et al. [3] showed that psychological disorders frequently
coexist with AS. They found that 1/3 of patients with AS
reported symptoms of depression [3]. A significant reci-
procal association between disease status and anxiety or
depression in AS was reported as well [4, 5].
Generally, medically ill patients are at increased risk for
depression [6]. Depression in those patients is often
O. Arısoy (&) � M. Sercan
Department of Psychiatry, Medical Faculty, Abant Izzet Baysal
University, Bolu, Turkey
e-mail: [email protected]
C. Bes
Department of Rheumatology, Bakırkoy State Hospital, Istanbul,
Turkey
C. Cifci
Department of Psychiatry, Beypazarı State Hospital, Beypazarı,Turkey
M. Soy
Department of Rheumatology, Hisar Intercontinental Hospital,
Istanbul, Turkey
123
Rheumatol Int (2013) 33:1855–1864
DOI 10.1007/s00296-013-2671-x

attributed to the physical impairment that accompanies the
illness, but recent data suggest that other processes like
immune activation may play a role in the pathogenesis of
depressive symptoms [7, 8]. Especially, the actions of
proinflammatory cytokines (PIC), such as interleukin
(IL)-1, tumor necrosis factor-alpha (TNF-a) and interferon-
gamma (IFN-c), may account for various psychopatho-
logical changes associated with major depression [9]. This
view is supported by various findings. Preclinically,
administration of PIC’s in animals induced sickness
behavior characterized by sleepiness, fatigue, loss of
appetite and decreased libido, which are behavioral alter-
ations very similar to the symptoms of depression in
humans [10]. Clinically, administration of PIC’s to cancer
or hepatitis C patients has been found to induce depressive
symptomatology [11]. Also, several medical illnesses,
characterized by chronic inflammatory responses, like
rheumatoid arthritis (RA) and psoriasis, have been reported
to be accompanied by depression [12]. Finally, activated
inflammatory pathways have been shown in clinically
depressed population. Meta-analysis revealed significantly
higher levels of TNF-a, IL-1 and IL-6 in depressed patients
compared to healthy controls [13]. Interestingly, antide-
pressants have been shown to have an anti-inflammatory
activity by reducing TNF-a levels [14, 15]. All these
findings show that immune stimulation induces depression-
like signs and symptoms through the release of PIC’s, and
reducing the effect of PIC’s may reverse depressive
symptoms.
Proinflammatory cytokines are also thought to play a
part in the pathogenesis of several immune-mediated
chronic inflammatory disorders like RA, AS, Crohn’s dis-
ease (CD) and psoriasis [16, 17]. Studies have shown that
TNF-a and IL1b were increased [18–20] and IL-10 was
decreased in AS [20, 21]. This immune activation leads to
synovial inflammation and eventually to the destruction of
cartilage and bone in AS patients [22]. These changes in
cytokines are correlated with disease activity, suggesting
that PIC’s may play an important role during active
inflammation in AS [20]. Especially, TNF-a is the master
cytokine for other inflammatory cytokines, and its neu-
tralization leads to reduced secretion of other PIC’s [23].
This targeted bench-to-bedside research led to the devel-
opment of TNF-a blockers. These agents have been proven
to be a potent treatment for especially patients with AS
who continue to have symptoms of active inflammation
despite medication with nonsteroidal anti-inflammatory
drugs at the maximum possible dose. Insufficient control of
disease activity as indicated by pain, stiffness and decrease
of function is the most common clinical reason for starting
anti-TNF therapy [24].
It is well known that TNF-a blockers are also very
effective in the treatment of other chronic inflammatory
disorders like RA, CD, ulcerative colitis (UC) and psoriasis
[25]. They decrease disease activity and increase QOL in
these patients [1, 26–28]. But, recent evidence has shown
that TNF-a blockers were also effective to decrease
depressive symptoms associated with these disorders. In
one of these trials, Tyring et al. [29] showed that etanercept
caused a 50 % improvement in depressive scores in pso-
riasis patients and the improvement in depression was less
correlated with skin clearance or joint pain. In CD, inflix-
imab also caused a significant decrease in depression
scores, fatigue and a significant increase in QOL [30–32].
There is only one study about the effect of TNF-a blockers
in AS patients up to now, and in that study, Ertenli et al.
[33] showed that infliximab caused a significant decrease in
depression–anxiety scores and disease activity and a sig-
nificant increase in QOL, and this change in disease
activity was not correlated with changes in depression and
anxiety scores.
These observations together with the theoretical back-
ground reported in this article leads to the hypothesis that
TNF-a blockers may reduce the effect of PIC’s and reverse
depressive symptoms associated with chronic inflammatory
disorders both of which are thought to be associated with
increased levels of TNF-a [34]. So, in this study, we aimed
to evaluate the effectiveness of TNF-a blockers on symp-
toms of AS, depression, anxiety and QOL and to see
whether improvement in depression, anxiety and QOL is
correlated with improvement in disease activity or not.
Methods
Ethical approval
In this longitudinal study, 9 patients with AS were asses-
sed. The trial was conducted in accordance with ethical
principles of the Declaration of Helsinki. The study was
approved by the Local Ethics Committee. All patients gave
written informed consent.
Patient recruitment
Patients with AS who were clinically resistant to conven-
tional therapy with disease-modifying antirheumatic drugs
and who were eligible candidates for TNF-a therapy were
invited to participate in the study, and a TNF-a blocker
treatment was started to the eligible patients between
January and April 2009 in the Rheumatology Clinic of
Abant Izzet Baysal University. Diagnosis of AS was based
on American College of Rheumatology criteria. Patients
older than 18 years of age with an active disease of
BASDAI[4 were included in the study. Exclusion criteria
were pregnancy or breast feeding, previous treatment with
1856 Rheumatol Int (2013) 33:1855–1864
123

TNF-a blockers, current treatment with psychotropics and
systemic disorders like chronic obstructive pulmonary
disease, congestive heart failure, stroke, cancer, active
tuberculosis or tuberculosis history in the previous 2 years
or other chronic inflammatory disease like psoriasis and
inflammatory bowel disease. Among 9 patients included in
the study, two of them received adalimumab 40 mg/kg
every other week and seven of them received infliximab
5 mg/kg at 0, 2nd and 6th week.
Rheumatological assessment
Turkish version of BASDAI (Bath Ankylosing Spondylitis
Disease Activity Index) was used to assess clinical disease
activity at 0, 2 and 6 weeks. BASDAI is a visual analog
scale (0–10) for 5 major symptoms of AS over last week
(fatigue, spinal pain, peripheral joint pain, enthesitis,
intensity/duration of morning stiffness). Lower scores
indicate less active disease. Turkish reliability and valida-
tion of BASDAI were made by Akkoc et al. [35]. Biological
disease activity was evaluated with erythrocyte sedimen-
tation rate (ESR) and C-reactive protein (CRP) at 0, 2 and
6 weeks. ESR and CRP were conventionally determined.
Psychiatric assessment
A nonstructured psychiatric clinical interview was per-
formed. According to this clinical interview, seven of the
patients had no history of psychiatric disorder, but one had
an ongoing panic disorder and another had depression.
Depression, anxiety levels and quality of life were assessed
with four questionnaires before treatment and after treat-
ment at 2nd and 6th weeks.
Hospital Anxiety and Depression Scale (HADS)
It is a Likert-type self-evaluation scale used to scan anxiety
and depression in physically ill patients. It consists of two
subscales and 14 items; 7 items investigate depression
symptoms (HAD-D) and 7 items investigate anxiety
symptoms (HAD-A). The items are scored from 0 (no
distress) to 3 (maximum distress). The cut-off point for the
anxiety subscale is 10 and 7 for the depression subscale.
Higher scores reflect higher levels of anxiety and depres-
sion. The validity and reliability of the Turkish version
were performed by Aydemir et al. [36].
Hamilton Depression Rating Scale (HAM-D)
It is a clinician-administered scale widely used for
assessing the severity of depressive symptoms. The present
study used the 17-item version (HAM-D-17). Items are
rated on a Likert scale. The cut-off score is 17 for
depression and higher scores reflect higher depression. Its
reliability and validity for the Turkish population were
assessed by Akdemir et al. [37].
Hamilton Anxiety Rating Scale (HAM-A)
It is a clinician-administered scale designed for assessing
the severity of anxiety. It is composed of 14 items rated on
a Likert scale. Higher scores reflect higher anxiety. Its
validity in the Turkish population was assessed by Yazıcıet al. [38].
Short Form-36 (SF-36)
It is the most preferred instrument in measuring quality of
life (QOL). It is a self-rated instrument consisting of 36
items, which provides assessment in 8 domains in the last
four weeks: physical functioning, social functioning, role
limitations due to emotional problems (role-emotional),
role limitations due to physical problems (role-physical),
bodily pain, vitality, mental health and general health
perception. The score ranges between 0 and 100, and
higher score represents better QOL. The reliability and
validity study of the Turkish version were performed by
Kocyigit et al. [39].
Statistical analysis
SPSS version 13.0 was used for statistical analysis. Data
were expressed as mean (SD) or frequency (%). Normal
distribution was tested by Kolmogorov–Smirnov test.
After Mauchly’s test of sphericity, repeated measures
analysis of variance (ANOVA) was performed on the
normally distributed variables among three consecutive
measurements of depression, anxiety and QOL to explore
the difference between baseline, 2nd week and 6th week.
If sphericity could not be assumed, the Greenhouse–
Geisser adjustment was used for the numerator and
denominator degrees of freedom in the F test. Nonpara-
metric Freidman test was applied for CRP values, since
2nd week CRP value did not distribute normally. When a
significant time effect was demonstrated in the Friedman
test, the Wilcoxon signed-rank test for paired samples was
used as a follow-up procedure to make post hoc pairwise
comparisons. Correlations of baseline scores and corre-
lation of change scores in disease activity, biological
activity and psychopathological status were explored by
using Pearson rank correlation test. Change scores were
determined by taking the difference of means between
week 6 and week 0.
Rheumatol Int (2013) 33:1855–1864 1857
123
Results
Demographic data
There were 8 males and 1 female in the study group. Mean
age was 39.4 ± 10.1 (20–57) and mean disease duration
was 10.6 ± 7.6 years (Table 1).
Comparison of baseline, 2nd and 6th week scores
The mean values of psychiatric questionnaires (HADS,
HAM-D, HAM-A, SF-36) and clinical (BASDAI) and
biological disease activity (ESR, CRP) are given in
Table 1, and changes of these scores are shown in Figs. 1,
2 and 3.
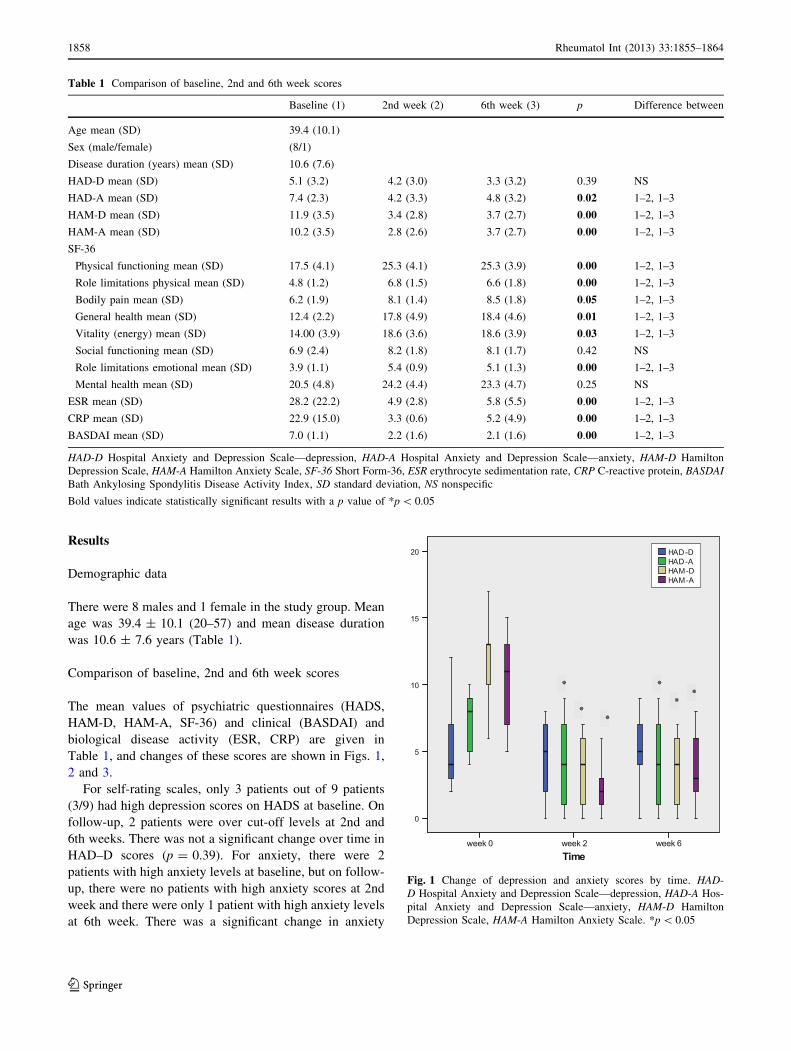
For self-rating scales, only 3 patients out of 9 patients
(3/9) had high depression scores on HADS at baseline. On
follow-up, 2 patients were over cut-off levels at 2nd and
6th weeks. There was not a significant change over time in
HAD–D scores (p = 0.39). For anxiety, there were 2
patients with high anxiety levels at baseline, but on follow-
up, there were no patients with high anxiety scores at 2nd
week and there were only 1 patient with high anxiety levels
at 6th week. There was a significant change in anxiety
Table 1 Comparison of baseline, 2nd and 6th week scores
Baseline (1) 2nd week (2) 6th week (3) p Difference between
Age mean (SD) 39.4 (10.1)
Sex (male/female) (8/1)
Disease duration (years) mean (SD) 10.6 (7.6)
HAD-D mean (SD) 5.1 (3.2) 4.2 (3.0) 3.3 (3.2) 0.39 NS
HAD-A mean (SD) 7.4 (2.3) 4.2 (3.3) 4.8 (3.2) 0.02 1–2, 1–3
HAM-D mean (SD) 11.9 (3.5) 3.4 (2.8) 3.7 (2.7) 0.00 1–2, 1–3
HAM-A mean (SD) 10.2 (3.5) 2.8 (2.6) 3.7 (2.7) 0.00 1–2, 1–3
SF-36
Physical functioning mean (SD) 17.5 (4.1) 25.3 (4.1) 25.3 (3.9) 0.00 1–2, 1–3
Role limitations physical mean (SD) 4.8 (1.2) 6.8 (1.5) 6.6 (1.8) 0.00 1–2, 1–3
Bodily pain mean (SD) 6.2 (1.9) 8.1 (1.4) 8.5 (1.8) 0.05 1–2, 1–3
General health mean (SD) 12.4 (2.2) 17.8 (4.9) 18.4 (4.6) 0.01 1–2, 1–3
Vitality (energy) mean (SD) 14.00 (3.9) 18.6 (3.6) 18.6 (3.9) 0.03 1–2, 1–3
Social functioning mean (SD) 6.9 (2.4) 8.2 (1.8) 8.1 (1.7) 0.42 NS
Role limitations emotional mean (SD) 3.9 (1.1) 5.4 (0.9) 5.1 (1.3) 0.00 1–2, 1–3
Mental health mean (SD) 20.5 (4.8) 24.2 (4.4) 23.3 (4.7) 0.25 NS
ESR mean (SD) 28.2 (22.2) 4.9 (2.8) 5.8 (5.5) 0.00 1–2, 1–3
CRP mean (SD) 22.9 (15.0) 3.3 (0.6) 5.2 (4.9) 0.00 1–2, 1–3
BASDAI mean (SD) 7.0 (1.1) 2.2 (1.6) 2.1 (1.6) 0.00 1–2, 1–3
HAD-D Hospital Anxiety and Depression Scale—depression, HAD-A Hospital Anxiety and Depression Scale—anxiety, HAM-D Hamilton
Depression Scale, HAM-A Hamilton Anxiety Scale, SF-36 Short Form-36, ESR erythrocyte sedimentation rate, CRP C-reactive protein, BASDAI
Bath Ankylosing Spondylitis Disease Activity Index, SD standard deviation, NS nonspecific
Bold values indicate statistically significant results with a p value of *p \ 0.05
Fig. 1 Change of depression and anxiety scores by time. HAD-
D Hospital Anxiety and Depression Scale—depression, HAD-A Hos-
pital Anxiety and Depression Scale—anxiety, HAM-D Hamilton
Depression Scale, HAM-A Hamilton Anxiety Scale. *p \ 0.05
1858 Rheumatol Int (2013) 33:1855–1864
123
scores by time (p = 0.02). The difference was prominent
between baseline and 2nd week and between baseline and
6th week. There was no significant difference in HAD-A
scores between week 2 and week 6.
For clinician-administered scales, there was only 1
patient who was above cut-off level in HAM-D scale. On
follow-up, there were no patients with high depression
scores. There was a significant change over time in HAM-D
scores (p = 0.00). The difference was significant between
baseline and week 2 and between baseline and week 6
assessments. Similarly, anxiety scores dropped significantly
with time (p = 0.00). The change in HAM-A scores was
significant between baseline and week 2 and between
baseline and week 6. There were no significant differences
in HAM-D and HAM-A scores between 2nd and 6th week.
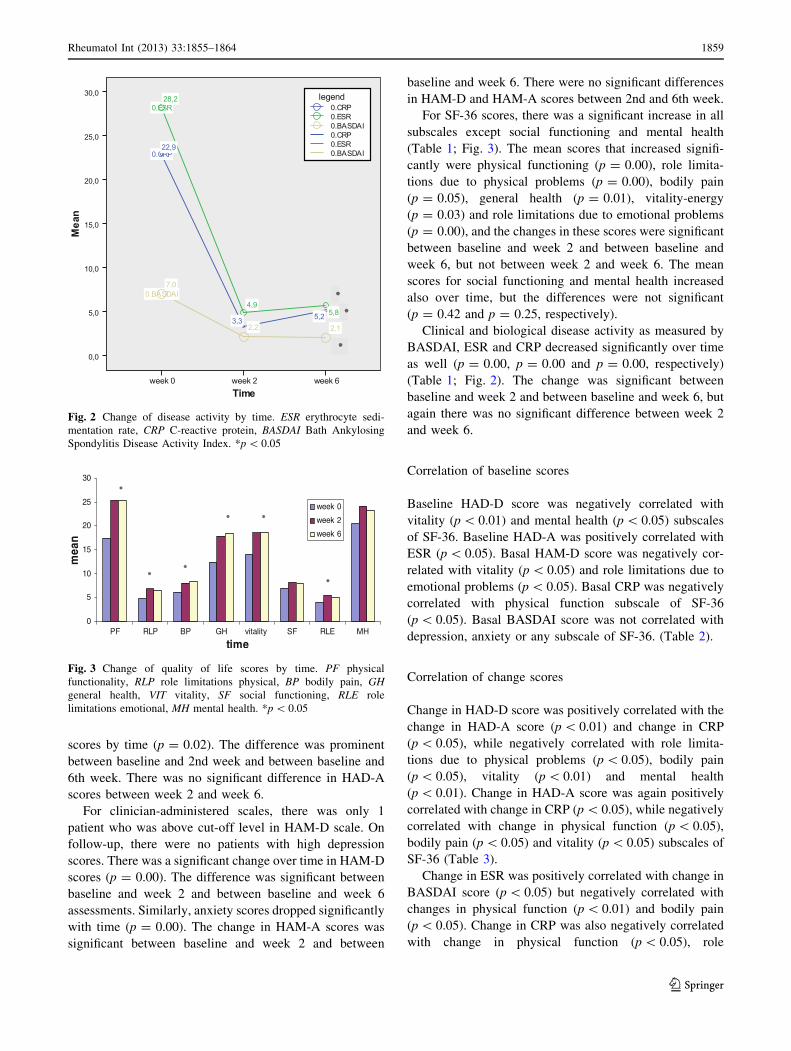
For SF-36 scores, there was a significant increase in all
subscales except social functioning and mental health
(Table 1; Fig. 3). The mean scores that increased signifi-
cantly were physical functioning (p = 0.00), role limita-
tions due to physical problems (p = 0.00), bodily pain
(p = 0.05), general health (p = 0.01), vitality-energy
(p = 0.03) and role limitations due to emotional problems
(p = 0.00), and the changes in these scores were significant
between baseline and week 2 and between baseline and
week 6, but not between week 2 and week 6. The mean
scores for social functioning and mental health increased
also over time, but the differences were not significant
(p = 0.42 and p = 0.25, respectively).
Clinical and biological disease activity as measured by
BASDAI, ESR and CRP decreased significantly over time
as well (p = 0.00, p = 0.00 and p = 0.00, respectively)
(Table 1; Fig. 2). The change was significant between
baseline and week 2 and between baseline and week 6, but
again there was no significant difference between week 2
and week 6.
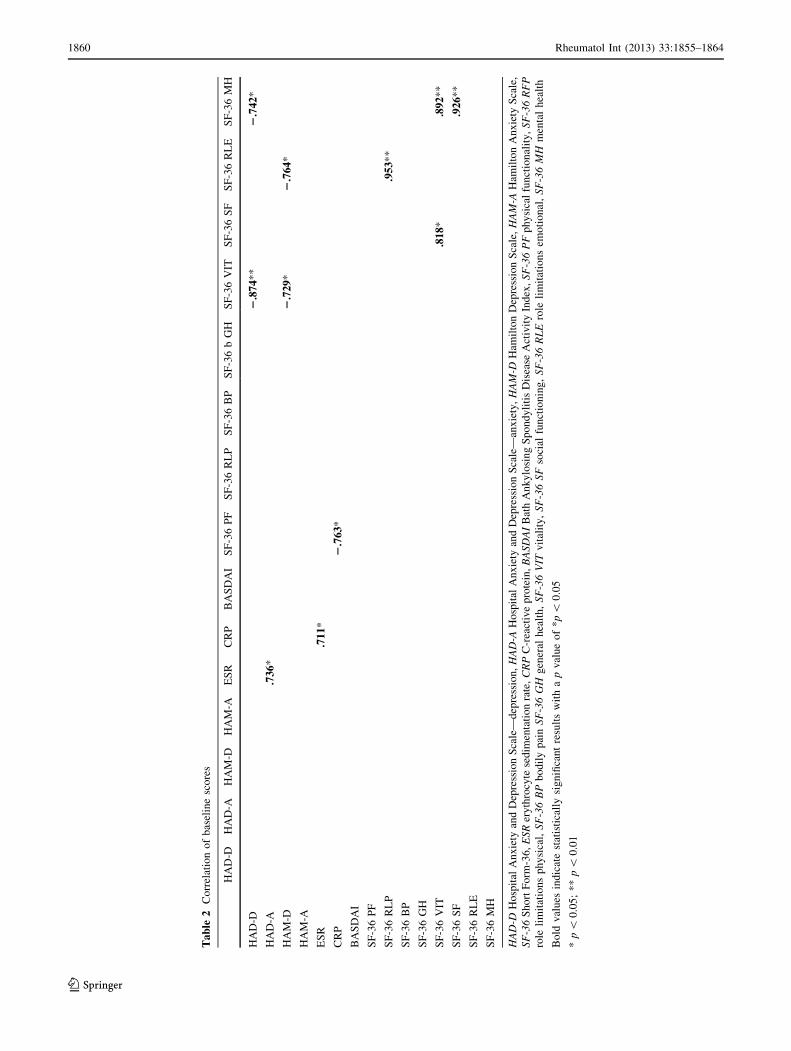
Correlation of baseline scores
Baseline HAD-D score was negatively correlated with
vitality (p \ 0.01) and mental health (p \ 0.05) subscales
of SF-36. Baseline HAD-A was positively correlated with
ESR (p \ 0.05). Basal HAM-D score was negatively cor-
related with vitality (p \ 0.05) and role limitations due to
emotional problems (p \ 0.05). Basal CRP was negatively
correlated with physical function subscale of SF-36
(p \ 0.05). Basal BASDAI score was not correlated with
depression, anxiety or any subscale of SF-36. (Table 2).
Correlation of change scores
Change in HAD-D score was positively correlated with the
change in HAD-A score (p \ 0.01) and change in CRP
(p \ 0.05), while negatively correlated with role limita-
tions due to physical problems (p \ 0.05), bodily pain
(p \ 0.05), vitality (p \ 0.01) and mental health
(p \ 0.01). Change in HAD-A score was again positively
correlated with change in CRP (p \ 0.05), while negatively
correlated with change in physical function (p \ 0.05),
bodily pain (p \ 0.05) and vitality (p \ 0.05) subscales of
SF-36 (Table 3).
Change in ESR was positively correlated with change in
BASDAI score (p \ 0.05) but negatively correlated with
changes in physical function (p \ 0.01) and bodily pain
(p \ 0.05). Change in CRP was also negatively correlated
with change in physical function (p \ 0.05), role
Fig. 2 Change of disease activity by time. ESR erythrocyte sedi-
mentation rate, CRP C-reactive protein, BASDAI Bath Ankylosing
Spondylitis Disease Activity Index. *p \ 0.05
Fig. 3 Change of quality of life scores by time. PF physical
functionality, RLP role limitations physical, BP bodily pain, GH
general health, VIT vitality, SF social functioning, RLE role
limitations emotional, MH mental health. *p \ 0.05
Rheumatol Int (2013) 33:1855–1864 1859
123
Ta
ble
2C
orr
elat
ion
of
bas
elin
esc
ore
s
HA
D-D
HA
D-A
HA
M-D
HA
M-A
ES
RC
RP
BA
SD
AI
SF
-36
PF
SF
-36
RL
PS
F-3
6B
PS
F-3
6b
GH
SF
-36
VIT
SF
-36
SF
SF
-36
RL
ES
F-3
6M
H
HA
D-D
2.8
74
**
2.7
42*
HA
D-A
.73
6*
HA
M-D
2.7
29
*2
.76
4*
HA
M-A
ES
R.7
11*
CR
P2
.76
3*
BA
SD
AI
SF
-36
PF
SF
-36
RL
P.9
53*
*
SF
-36
BP
SF
-36
GH
SF
-36
VIT
.81
8*
.89
2*
*
SF
-36
SF
.92
6*
*
SF
-36
RL
E
SF
-36
MH
HA
D-D
Ho
spit
alA
nx
iety
and
Dep
ress
ion
Sca
le—
dep
ress
ion
,H
AD
-AH
osp
ital
An
xie
tyan
dD
epre
ssio
nS
cale
—an
xie
ty,
HA
M-D
Ham
ilto
nD
epre
ssio
nS
cale
,H
AM
-AH
amil
ton
An
xie
tyS
cale
,
SF
-36
Sh
ort
Fo
rm-3
6,
ES
Rer
yth
rocy
tese
dim
enta
tio
nra
te,
CR
PC
-rea
ctiv
ep
rote
in,
BA
SD
AI
Bat
hA
nk
ylo
sin
gS
po
nd
yli
tis
Dis
ease
Act
ivit
yIn
dex
,S
F-3
6P
Fp
hy
sica
lfu
nct
ion
alit
y,
SF
-36
RF
P
role
lim
itat
ion
sp
hy
sica
l,S
F-3
6B
Pb
od
ily
pai
nS
F-3
6G
Hg
ener
alh
ealt
h,
SF
-36
VIT
vit
alit
y,
SF
-36
SF
soci
alfu
nct
ion
ing
,S
F-3
6R
LE
role
lim
itat
ion
sem
oti
on
al,
SF
-36
MH
men
tal
hea
lth
Bo
ldv
alu
esin
dic
ate
stat
isti
call
ysi
gn
ifica
nt
resu
lts
wit
ha
pv
alu
eo
f*
p\
0.0
5
*p
\0
.05
;*
*p\
0.0
1
1860 Rheumatol Int (2013) 33:1855–1864
123
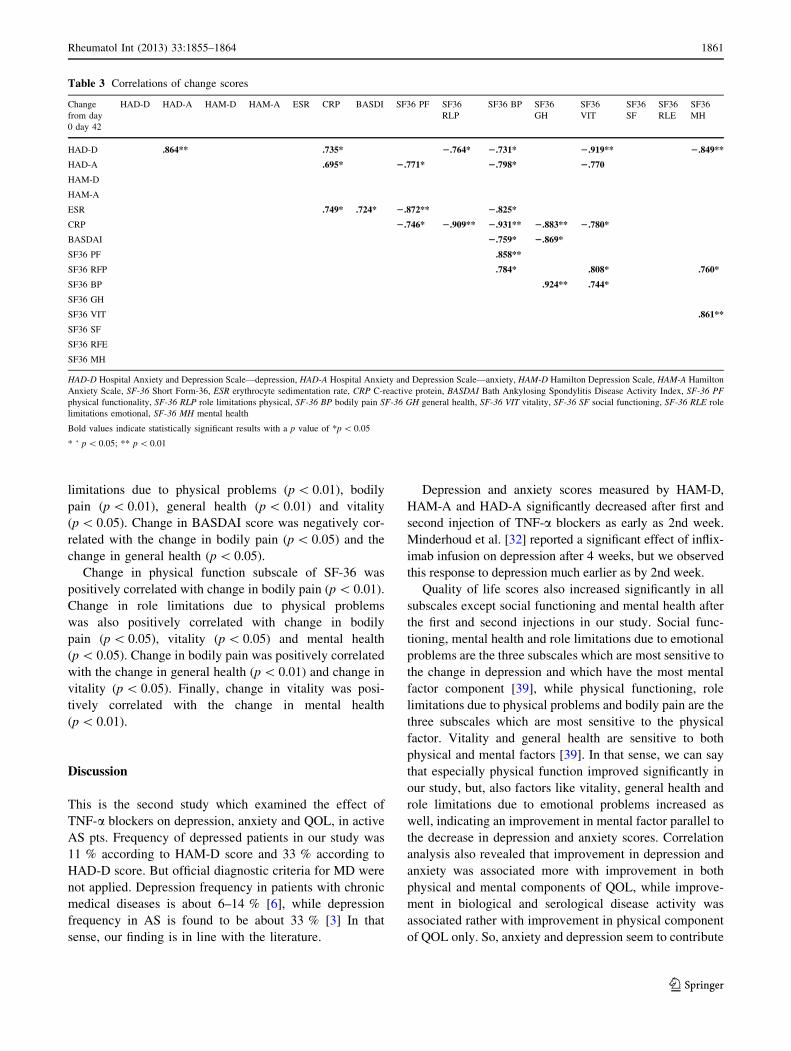
limitations due to physical problems (p \ 0.01), bodily
pain (p \ 0.01), general health (p \ 0.01) and vitality
(p \ 0.05). Change in BASDAI score was negatively cor-
related with the change in bodily pain (p \ 0.05) and the
change in general health (p \ 0.05).
Change in physical function subscale of SF-36 was
positively correlated with change in bodily pain (p \ 0.01).
Change in role limitations due to physical problems
was also positively correlated with change in bodily
pain (p \ 0.05), vitality (p \ 0.05) and mental health
(p \ 0.05). Change in bodily pain was positively correlated
with the change in general health (p \ 0.01) and change in
vitality (p \ 0.05). Finally, change in vitality was posi-
tively correlated with the change in mental health
(p \ 0.01).
Discussion
This is the second study which examined the effect of
TNF-a blockers on depression, anxiety and QOL, in active
AS pts. Frequency of depressed patients in our study was
11 % according to HAM-D score and 33 % according to
HAD-D score. But official diagnostic criteria for MD were
not applied. Depression frequency in patients with chronic
medical diseases is about 6–14 % [6], while depression
frequency in AS is found to be about 33 % [3] In that
sense, our finding is in line with the literature.
Depression and anxiety scores measured by HAM-D,
HAM-A and HAD-A significantly decreased after first and
second injection of TNF-a blockers as early as 2nd week.
Minderhoud et al. [32] reported a significant effect of inflix-
imab infusion on depression after 4 weeks, but we observed
this response to depression much earlier as by 2nd week.
Quality of life scores also increased significantly in all
subscales except social functioning and mental health after
the first and second injections in our study. Social func-
tioning, mental health and role limitations due to emotional
problems are the three subscales which are most sensitive to
the change in depression and which have the most mental
factor component [39], while physical functioning, role
limitations due to physical problems and bodily pain are the
three subscales which are most sensitive to the physical
factor. Vitality and general health are sensitive to both
physical and mental factors [39]. In that sense, we can say
that especially physical function improved significantly in
our study, but, also factors like vitality, general health and
role limitations due to emotional problems increased as
well, indicating an improvement in mental factor parallel to
the decrease in depression and anxiety scores. Correlation
analysis also revealed that improvement in depression and
anxiety was associated more with improvement in both
physical and mental components of QOL, while improve-
ment in biological and serological disease activity was
associated rather with improvement in physical component
of QOL only. So, anxiety and depression seem to contribute
Table 3 Correlations of change scores
Change
from day
0 day 42
HAD-D HAD-A HAM-D HAM-A ESR CRP BASDI SF36 PF SF36
RLP
SF36 BP SF36
GH
SF36
VIT
SF36
SF
SF36
RLE
SF36
MH
HAD-D .864** .735* 2.764* 2.731* 2.919** 2.849**
HAD-A .695* 2.771* 2.798* 2.770
HAM-D
HAM-A
ESR .749* .724* 2.872** 2.825*
CRP 2.746* 2.909** 2.931** 2.883** 2.780*
BASDAI 2.759* 2.869*
SF36 PF .858**
SF36 RFP .784* .808* .760*
SF36 BP .924** .744*
SF36 GH
SF36 VIT .861**
SF36 SF
SF36 RFE
SF36 MH
HAD-D Hospital Anxiety and Depression Scale—depression, HAD-A Hospital Anxiety and Depression Scale—anxiety, HAM-D Hamilton Depression Scale, HAM-A Hamilton
Anxiety Scale, SF-36 Short Form-36, ESR erythrocyte sedimentation rate, CRP C-reactive protein, BASDAI Bath Ankylosing Spondylitis Disease Activity Index, SF-36 PF
physical functionality, SF-36 RLP role limitations physical, SF-36 BP bodily pain SF-36 GH general health, SF-36 VIT vitality, SF-36 SF social functioning, SF-36 RLE role
limitations emotional, SF-36 MH mental health
Bold values indicate statistically significant results with a p value of *p \ 0.05
* ‘ p \ 0.05; ** p \ 0.01
Rheumatol Int (2013) 33:1855–1864 1861
123

to decreased QOL caused by the disease itself [40], and
improvement in psychological status seems to be associated
with a more global improvement in QOL.
Correlation analysis also revealed that baseline clinical
disease activity (BASDAI) was not associated with base-
line depression and anxiety, but baseline serological dis-
ease activity (ESR) was associated with baseline anxiety
scores (HAD-A). Previous studies showed that clinical or
serological disease activity was associated with the severity
of depression and anxiety in AS [4, 5, 41]. But Persoons
et al. [30] found no correlation between clinical disease
activity and depression scores neither at baseline nor after
infliximab infusion in CD similar to our study. Likewise,
Ertenli et al. [33] found no correlation between baseline
clinical disease activity and baseline depression–anxiety
scores as well, but they found a positive correlation of
baseline ESR with basal HAD-D scores. So, it seems that
increase in ESR is probably associated with an increase in
depression and anxiety scores, suggesting a role of
inflammation in depression and anxiety.
As for correlation of change scores, we could not find an
association between change in clinical disease activity
(BASDAI) and change in depression–anxiety scores, which
was similar to Ertenli et al.’s [33] finding. But apart from
their studies, we found that change in serological disease
activity (CRP) was correlated with change in depression
and anxiety scores, again suggesting a role of inflammation
in depression and anxiety.
In view of all these findings, it seems reasonable to
suggest that improvement in depression is not associated
with clinical improvement in our study. Similar to our
findings, it was shown that infliximab in CD caused a rapid
and significant decrease in depression scores, prior to any
improvement in the intestinal pathology [30, 32]. These
data were consistent with our findings in AS patients,
because change in the activity of clinical disease was not
associated with the change in depression scores. If
improvement of depression is not related to improvement
of clinical disease activity, then this may suggest
involvement of other mechanisms in improvement of
depression associated with AS.
One of these mechanisms might be the correction of
inflammation. Because, PIC release in inflammation might
be involved in the pathogenesis of depression by causing
disturbances in neurotransmitter metabolism, by increasing
hypothalomopituitary axis (HPA) activity and decreasing
production of relevant central nervous system growth fac-
tors. PIC’s may cause reduction in tryptophan availability
for serotonin synthesis by activating indoleamine-2,3-
dioxygenase (IDO) enzyme [42]. IDO switches the syn-
thesis of serotonin from tryptophan to kynurenine and
quinolinic acid instead of serotonin and by this way
decrease serotonin synthesis [43]. IL-1 and TNF-a are
potent inducers of IDO (43). IL-1 and TNF-a increase the
activity of the serotonin transporter as well. [44]. Espe-
cially, TNF-a contributes to a decrease in synaptic avail-
ability of serotonin. This decrease in serotonin levels
eventually leads to depressive symptoms. All the above
changes are frequently observed in depressive disorders.
Thus, TNF-a blockers, by causing a decrease in TNF-alevels, might increase serotonin levels and therefore correct
depression via this mechanism. In our study, although we
have not studied PIC levels like TNF-a, a decrease in CRP
levels—which is also considered as a PIC—was associated
with improvement in both depression and anxiety. Tuglu
et al. [15] also showed a decrease in CRP levels in depressed
patients with antidepressant treatment. So, as our results also
suggest, TNF-a blockers might be effective in treatment of
depressive symptoms accompanying AS. This may mean
that TNF-a blockers may be promising targets for the
treatment of MD associated with chronic inflammatory
disorders or in otherwise healthy MD patients who have
increased levels of PIC’s. Accordingly, a randomized, dou-
ble-blind, placebo-controlled phase IV trial of infliximab in
treatment-resistant MD patients has been recently completed
by Raison et al. [45] to test the potential antidepressive effect
of TNF-a blockers in a psychiatric population.
Limitations
The major limitations of our study was its small sample
size, absence of a control group, short follow-up interval,
nonstructured psychiatric interview, scarcity of depressed
patients and absence of biochemical measurements of
cytokines. If the number of depressed or anxious AS
patients would have been higher, the findings might have
been more precious. Also, though we showed a decrease in
depression and anxiety scores irrespective of BASDAI
scores, improvement in mental state can still be due to
improvement in pain and stiffness, so it would be much
better to test the potential antidepressant effects of TNF-
alpha blockers in resistant depressive patients without a
chronic inflammatory disorder like AS.
Conclusion
Despite these limitations, our results show that TNF-ablockers may be effective in the treatment of depressive
symptoms accompanying AS. But to clarify the underlying
mechanism of this potential antidepressive effect of TNF-ablockers, change in cytokine levels should also be analyzed
in these patients. This may help to better understand the
role of cytokines in the pathogenesis of depression in active
AS. Also, future studies should be designed to further
1862 Rheumatol Int (2013) 33:1855–1864
123
clarify the role of antiinflammatory drugs as potential new
therapeutic agents for the treatment of MD.
Conflict of interest The authors declare that they have no conflict
of interest.
References
1. Braun J, Sieper J (2007) Ankylosing spondylitis. Lancet 369:
1379–1390
2. Ortancil O, Konuk N, May H, Sanli A, Ozturk D, Ankarali H
(2010) Psychological status and patient-assessed health instru-
ments in ankylosing spondylitis. J Clin Rheumatol 16:313–316
3. Barlow JH, Macey SJ, Struthers GR (1993) Gender, depression
and ankylosing spondylitis. Arthritis Care Res 6:45–51
4. Zink A, Braun J, Listing J, Wollenhaupt J (2000) Disability and
handicap in rheumatoid arthritis and ankylosing spondylitis-
results from the German rheumatological database. J Rheumatol
27:613–622
5. Martindale J, Smith J, Sutton CJ, Grennan D, Goodacre L,
Goodacre JA (2006) Disease and psychological status in anky-
losing spondylitis. Rheumatology 45:1288–1293
6. Evans DL, Charney DS, Lewis L et al (2005) Mood disorders in
the medically ill: scientific review and recommendations. Biol
Psychiatry 58:175–189
7. Raison CL, Capuron L, Miller AH (2006) Cytokines sing the
blues: inflammation and the pathogenesis of depression. Trends
Immunol 27:24–31
8. Leonard BE (2010) The concept of depression as a dysfunction of
the immune system. Curr Immunol Rev 6:205–212
9. Schiepers OJ, Wichers MC, Maes M (2005) Cytokines and major
depression. Prog Neuropsychopharmacol Biol Psychiatry
29:201–217
10. Dantzer R (2001) Cytokine-induced sickness behavior: mecha-
nisms and implications. Ann N Y Acad Sci 933:222–234
11. Patten SB (2006) Psychiatric side effects of interferon treatment.
Curr Drug Saf 1:143–150
12. Dantzer R, Capuron L, Irwin MR et al (2008) Identification and
treatment of symptoms associated with ınflammation in medically
ıll patients. Psychoneuroendocrinology 33:18–29
13. Dowlati Y, Herrmann N, Swardfager W et al (2010) A meta-
analysis of cytokines in major depression. Biol Psychiatry
67:446–457
14. Reynolds JL, Ignatowski TA, Sud R, Spengler RN (2005) An
antidepressant mechanism of desipramine is to decrease tumor
necrosis factor-alpha production culminating in increases in
noradrenergic neurotransmission. Neuroscience 133:519–531
15. Tuglu C, Kara SH, Caliyurt O, Vardar E, Abay E (2003)
Increased serum tumor necrosis factor-alpha levels and treatment
response in major depressive disorder. Psychopharmacology 170:
429–433
16. Bradley JR (2008) TNF-mediated inflammatory disease. J Pathol
214:149–160
17. Braun J, Sieper J (2003) Overview of the use of the anti-TNF
agent infliximab in chronic inflammatory diseases. Expert Opin
Biol Ther 3:141–168
18. Lange U, Teichmann J, Stracke H (2000) Correlation between
plasma TNF-alpha, IGF-1, biochemical markers of bone metab-
olism, markers of inflammation/disease activity, and clinical
manifestations in ankylosing spondylitis. Eur J Med Res
29:507–511
19. Sonel B, Tutkak H, Duzgun N (2002) Serum levels of IL-1 beta,
TNF-alpha, IL-8, and acute phase proteins in seronegative
spondyloarthropathies. Joint Bone Spine 69:463e467
20. Chou CT, Huo AP, Chang HN, Tsai CY, Chen WS, Wang HP
(2007) Cytokine production from peripheral blood mononuclear
cells in patients with ankylosing spondylitis and their first-degree
relatives. Arch Med Res 38:190–195
21. Kozaci LD, Sari I, Alacacioglu A, Akar S, Akkoc N (2010)
Evaluation of inflammation and oxidative stress in ankylosing
spondylitis: a role for macrophage migration inhibitory factor.
Mod Rheumatol 20:34–39
22. Frech T (2007) Treatment of ankylosing spondylitis: focus on
etanercept. Biologics 1:45–51
23. Lin J, Ziring D, Desai S et al (2008) TNFalpha blockade in
human diseases: an overview of efficacy and safety. Clin
Immunol 126:13–30
24. Braun J, Pham T, Sieper J, Davis J, van der Linden S, Dougados
M, van der Heijde D; ASAS Working Group (2003) International
ASAS consensus statement for the use of anti-tumour necrosis
factor agents in patients with ankylosing spondylitis. Ann Rheum
Dis 62:817–824
25. Silva LC, Ortigosa LC, Benard G (2010) Anti-TNF-a agents in
the treatment of immune-mediated inflammatory diseases:
mechanisms of action and pitfalls. Immunotherapy 2:817–833
26. Loftus EV, Feagan BG, Colombel JF et al (2008) Effects of
adalimumab maintenance therapy on health-related quality of life
of patients with Crohn’s disease: patient-reported outcomes of the
CHARM trial. Am J Gastroenterol 103:3132–3141
27. Fernandez Lison LC, Vazquez Domınguez B, Luis Fernandez J,
Moreno Alvarez P, Fruns Gimenez I, Liso Rubio J (2008) Quality
of life of patients with rheumatoid arthritis undergoing out-
patient treatment with TNF inhibitors. Farm Hosp 32:178–181
28. Abalos-Medina GM, Ruiz-Villaverde G, Sanchez-Cano D, Ruiz-
Villaverde R, Ocana-Peinado F, Villaverde-Gutierrez C (2010)
Functional level and quality of life in ankylosing spondylitis,
pilot study after 16 weeks TNF blocker treatment. Rev Esp Ge-
riatr Gerontol 45:331–334
29. Tyring S, Gottlieb A, Papp K et al (2006) Etanercept and clinical
outcomes, fatigue, and depression in psoriasis: double-blind
placebo-controlled randomized phase III trial. Lancet 367:29–35
30. Persoons P, Vermeire S, Demyttenaere K et al (2005) The impactof major depressive disorder on the short- and long-term outcome
of Crohn’s disease treatment with infliximab. Aliment Pharmacol
Ther 22:101–110
31. Lichtenstein GR, Bala M, Han C, DeWoody K, Schaible T (2002)
Infliximab improves quality of life in patients with Crohn’s dis-
ease. Inflamm Bowel Dis 8:237–243
32. Minderhoud IM, Samsom M, Oldenburg B (2007) Crohn’s dis-
ease, fatigue, and infliximab: is there a role for cytokines in the
pathogenesis of fatigue? World J Gastroenterol 13:2089–2093
33. Ertenli I, Ozer S, Kiraz S et al (2010) Infliximab, a TNF-alpha
antagonist treatment in patients with ankylosing spondylitis: the
impact on depression, anxiety and quality of life level. Rheumatol
Int. doi:10.1007/s00296-010-1616-x
34. Berthold-Losleben M, Heitmann S, Himmerich H (2009) Anti-
inflammatory drugs in psychiatry. Inflamm Allergy Drug Targets
8:266–276
35. Akkoc Y, Karatepe AG, Akar S, Kirazli Y, Akkoc N (2005) A
Turkish version of the Bath Ankylosing Spondylitis Disease
Activity Index: reliability and validity. Rheumatol Int 25:280–284
36. Aydemir O, Guvenir T, Kuey L et al (1997). Reliability and
validity of Turkish version of Hospital Depression and Anxiety
Questionnaire. Turk Psik Derg 8:280–287 (Turkish)
37. Akdemir A, Orsel S, Dag I et al (1996) Reliability and validity of
Turkish version of Hamilton Depression Scale. Psikiyatri Psiko-
loji Psikofarmakoloji Dergisi 4:251–259 [Turkish]
38. Yazıcı MK, Demir B, Tanrıverdi N et al (1998) Interrater reli-
ability and validity of Turkish version of Hamilton Anxiety Scale.
Turk Psikiyatri Dergisi 9:114–117 [Turkish]
Rheumatol Int (2013) 33:1855–1864 1863
123

39. Kocyigit H, Aydemir O, Olmez N et al (1992) Reliability and
validity of Turkish version of Short Form 36 (SF-36). Ilac ve
Tedavi Dergisi 12:102–106 [Turkish]
40. Baysal O, Durmus B, Ersoy Y et al (2011) Relationship between
psychological status and disease activity and quality of life in
ankylosing spondylitis. Rheumatol Int 31:795–800
41. Eren I, Sahin M, Cure E et al (2007) Interactions between psy-
chiatric symptoms and disability and quality of life in ankylosing
spondylitis patients. Arch Neuropsychiatry 44:1–9
42. Wichers M, Maes M (2002) The psychoneuroimmuno-patho-
physiology of cytokine-induced depression in humans. Int J
Neuropsychopharmacol 5:375–388
43. Myint AM, Kim YK (2003) Cytokine-serotonin interaction
through IDO: a neurodegeneration hypothesis of depression. Med
Hypothesis 61:519–525
44. Zhu CB, Blakely RD, Hewlett WA (2006) The proinflammatory
cytokines interleukin-1beta and tumor necrosis factor-alpha acti-
vate serotonin transporters. Neuropsychopharmacol 31:2121–2131
45. Raison CL, Rutherford RE, Woolwine BJ, Shuo C, Schettler P,
Drake DF, Haroon E, Miller AH (2012) A randomized controlled
trial of the tumor necrosis factor antagonist infliximab for treat-
ment-resistant depression: the role of baseline inflammatory
biomarkers. Arch Gen Psychiatry 3:1–11. doi:10.1001/2013
1864 Rheumatol Int (2013) 33:1855–1864
123
Copyright of Rheumatology International is the property of Springer Science & BusinessMedia B.V. and its content may not be copied or emailed to multiple sites or posted to alistserv without the copyright holder's express written permission. However, users may print,download, or email articles for individual use.

















![Ankylosing spondylitis and related conditions - NHS Wales1].pdf · Condition Ankylosing spondylitis Ankylosing spondylitis and related conditions This booklet provides information](https://static.cupdf.com/doc/110x72/5d53eb2788c993a4728b841d/ankylosing-spondylitis-and-related-conditions-nhs-1pdf-condition-ankylosing.jpg)












