



Teachers as Partners in Teachers as Partners in Effective School-Based Mental Effective School-Based Mental
Health ProgramsHealth Programs
Teachers as Partners in Teachers as Partners in Effective School-Based Mental Effective School-Based Mental
Health ProgramsHealth ProgramsTherese C. Johnston, Ph.D.Therese C. Johnston, Ph.D.
Carl E. Paternite, Ph.D.Carl E. Paternite, Ph.D.Ohio Mental Health Network for School SuccessOhio Mental Health Network for School Success

Johnston & Paternite, OMHNSS 2
IntroductionsCarl Paternite, Ph.D.
Department of Psychology
Miami University
Oxford, Ohio 45056
Johnston & Paternite, OMHNSS 3
Introductions
Terri Johnston, Ph.D.Educator Consultant
Behavior Consultant

Johnston & Paternite, OMHNSS 4
Background and Context• Most youth in need of MH intervention
don’t receive it
• Of the small percentage that do the majority receive treatment within a school setting
(Rones & Hoagwood, 2000)

Johnston & Paternite, OMHNSS 5
Background and Context• Service realities
– Reliance on primary care medical settings
– Community mental health clinics
– Private practitioners

Johnston & Paternite, OMHNSS 6
Background and Context• Historically, school
services focused on special education population
• Emphasized individual assessment and intervention
Johnston & Paternite, OMHNSS 7
Historical Relationship• Teachers seen as
information source• Teachers often
perceived as untrained and unreceptive to consultation from MH provider

Johnston & Paternite, OMHNSS 8
Educators vs. Therapists• Sedlak (1997) discussed the uneasy
alliance between service providers and schools
• Mental health staff (e.g., social workers, psychologists, counselors, etc.) seen as “frills” not essential to the academic mission of schools
Johnston & Paternite, OMHNSS 9
Educators vs. Therapists• MH Provider Goals
– Focused on the individual– Social/emotional goals considered to be
not related to academic success– Therapeutic interventions occur in private
“pull-out” sessions– Confidentiality sited as reasons not to
inform teachers of progress
Johnston & Paternite, OMHNSS 10
Educators vs. Therapists• Teacher Goals
– Focused on the group rather than the individual
– Academic achievement mandated as primary concern
– Feel unprepared to face the emotional demands of ever-changing population
Johnston & Paternite, OMHNSS 11
Cooperation vs. Integration
• Many so called school-based programs co-exist in the buildings
• Rarely are mental health staff and educators actually working together identifying and sharing– Values– Goals– Strategies

Johnston & Paternite, OMHNSS 12
The Role of Schools• Can’t be responsible for meeting the all
the needs• Must meet then challenges when needs
directly affect learning and school success (Carnegie Council Task Force on Education of Young Adolescents, 1989; Elias, Zins, Graczyk, & Weissberg, 2003)
Johnston & Paternite, OMHNSS 13
The Role of Schools• Compelling evidence
– Positive associations between mental health and academic success
– Emotional, social, and behavioral health problems are significant barriers to learning (Adelman & Taylor, 1999; Atkins, Frazzier, Adil & Talbott, 2003)
Johnston & Paternite, OMHNSS 14
Partnership is Critical• Public schools’ mission is to educate all students• Students with challenges of SED have the highest rates
of school failure– 50% drop out compared to 30% for students with other
disabilities
• Mental health is essential to learning as well as social and emotional development
• The interplay between emotional health and school success indicates schools must be partnersPresident’s New Freedom Commission on Mental Health Achieving
the Promise: Transforming Mental Health Care in America (2003)

Johnston & Paternite, OMHNSS 15
Essential Attitudes for Collaboration
• Providers should view educators as valued customers
• Focus should explicitly be on MH barriers to schools success

Johnston & Paternite, OMHNSS 16
Essential Attitudes for Collaboration
• Educators should be viewed as…– valued colleagues– Essential members
of the mental health team
Johnston & Paternite, OMHNSS 17
Cognitive Dissonance• “Equal standing”??????• Mental health hierarchies
– Expert vs. consultee
Johnston & Paternite, OMHNSS 18
Teachers Lack Confidence• Feel ill prepared to
design or support interventions for students with psychiatric disorders even when primary disability is attributed to emotional or behavior problems (Maag, 2002)

Johnston & Paternite, OMHNSS 19
Student Support• Educators rarely know anything about mental
health services students are receiving nor the nature or intensity of the services
• Teachers who are engaged with students day after day play central roles in facilitating social and emotional learning

Johnston & Paternite, OMHNSS 20
Student Support• Important collaboration could include
– Assistance and consultation with social skill instruction IN THE CLASSROOM
– Development and monitoring of behavior intervention plans
– Consultation with parents to encourage consistent strategies and promotion of practice and reinforcement of alternative behaviors across contexts
Johnston & Paternite, OMHNSS 21
Models Fully Engaging Educators
• Positive Behavior Support• Re-Education
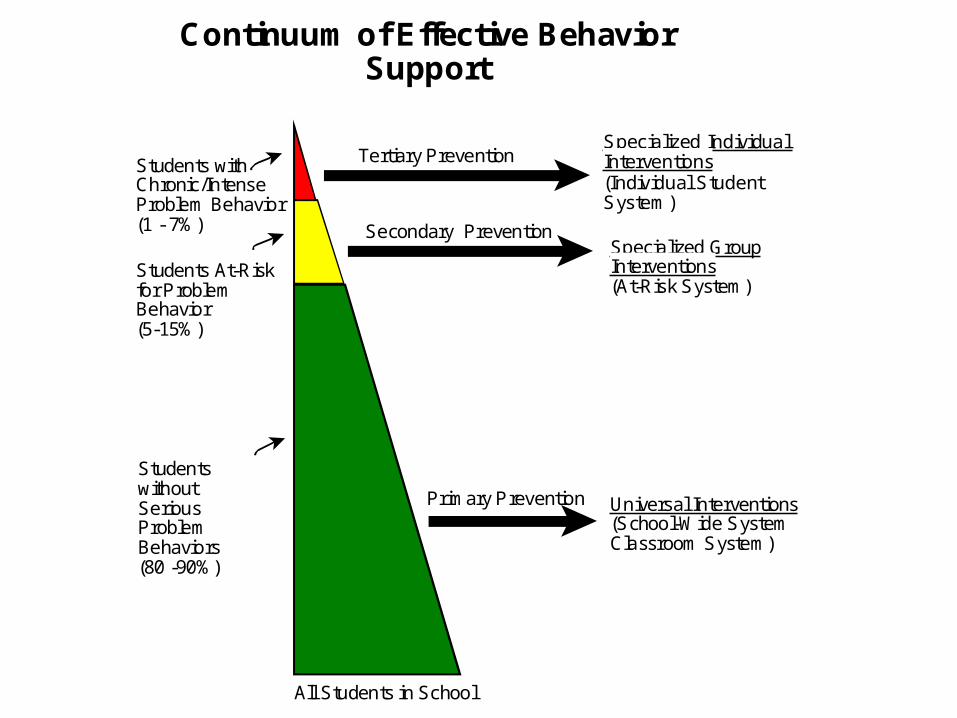
Specialized Individual Interventions(Individual StudentSystem)
Continuum of Effective BehaviorSupport
Specialized GroupInterventions(At-Risk System)
Universal Interventions (School-Wide SystemClassroom System)
Studentswithout SeriousProblemBehaviors (80 -90%)
Students At-Risk for Problem Behavior(5-15%)
Students withChronic/IntenseProblem Behavior(1 - 7%)
Primary Prevention
Secondary Prevention
Tertiary Prevention
All Students in School
Johnston & Paternite, OMHNSS 23
School-Wide PBS• Continuum of integrated activities
– Health promotion through intensive intervention– Dependent on effective multi-disciplinary teamwork and
engagement of families
• “Positive behavior” refers to all skills that increase a student’s success in the home, school and community setting
• “Support” refers to the methods used to teach, strengthen and expand positive behaviors
(Sugai et al., 2000)

Johnston & Paternite, OMHNSS 24
PBS• Shows promise as an
effective preventative strategy
• Decreases antisocial and other behavior difficulties amongst a growing population of children and youth

Specialized Individual Interventions(Individual StudentSystem)
Continuum of Effective BehaviorSupport
Specialized GroupInterventions(At-Risk System)
Universal Interventions (School-Wide SystemClassroom System)
Studentswithout SeriousProblemBehaviors (80 -90%)
Students At-Risk for Problem Behavior(5-15%)
Students withChronic/IntenseProblem Behavior(1 - 7%)
Primary Prevention
Secondary Prevention
Tertiary Prevention
All Students in School

Johnston & Paternite, OMHNSS 26
Project Re-ED• Re-ED
– Re-Education of Emotionally Disturbed Children– Based on the work of Dr. Nicholas Hobbs more than 40
years ago
• Observation of residential treatment programs in Western European countries
• Noted that programs dominated by an elaborate professional hierarchy were less effective than those relying on and valued the interpersonal rapport of “natural child care workers”
Johnston & Paternite, OMHNSS 27
The Heart of Re-ED• Problems do not
reside within a child• Instead, the
interaction of contextual variables in the natural setting contributes to the discord

Johnston & Paternite, OMHNSS 28
12 Principles of Re-ED• Life is to be lived now
• The group is important
• Trust is essential
• Competence makes a different
• Time is an ally
• Intelligence can be taught
Johnston & Paternite, OMHNSS 29
12 Principles of Re-ED• The body is the armature of the self (i.e., the
physical self around which the psychological self is constructed
• Communities are important• Feelings should be nurtured• Self-control can be taught• Ceremony and ritual give order• A child should know some joy in each day
Johnston & Paternite, OMHNSS 30
The Heart of Re-ED• Therapeutic focus is competence
enhancement rather than deficit reduction• Academic achievement is of particular
importance• School and school work is the business of
children, and successful living is healing (Valore, 2002)

Johnston & Paternite, OMHNSS 31
Educators Supporting Mental Health
• Most children fail in school because the feel detached, alienated and isolated from the process, not due to the lack of cognitive skills
• “…the bond between the teacher and student creates the foundation upon which a sense of belonging can develop”
(Beck & Malley, 1998)

Johnston & Paternite, OMHNSS 32
Resilient Youth• Several studies suggest factors present in
resilient youth include– Successful school experiences– Development of reading skills above the 3rd
grade– Associations with caring adults outside the family– Ability to maintain hope
(Gilliam & Scoot, 1998; McEvoy & Welker, 2000)
Johnston & Paternite, OMHNSS 33
Conclusion• It is essential to
engage educators in collaborative partnerships in order to promote both mental health and school success for children and adolescents

Johnston & Paternite, OMHNSS 34
Adopt Inclusive definition of the term “educator”• Policy makers, central office administrators,
building-level administrators, classroom and non-classroom staff (e.g., guidance counselors, school psychologists, nurses, etc.)
• Recognize the diversity of roles and the diversity of strategies these folks can support

Johnston & Paternite, OMHNSS 35
Establish formal relationships with key opinion leaders among the educational staff
• Teacher-consultants model– Serve as program advisors and champions
for initiatives within school related mental health promotion
– Can become peer mentors and advocates for demystifying the concept of “mental health”
Johnston & Paternite, OMHNSS 36
Become immersed in the school community• Be reliable about attendance and flexible in
program delivery• Attend school events, e.g., sports, concerts
award ceremonies, etc.• Don’t unwittingly transfer the tendency to
view what happens behind closed doors with a client as the essence of the providers work

Johnston & Paternite, OMHNSS 37
Conduct detailed, local needs assessments • Survey the perspective of educators,
students and parents
• Include school climate assessments
• Understand the unique characteristics of school cultures
Johnston & Paternite, OMHNSS 38
Prioritize mental health promotion and problem prevention initiatives• Recognize the difficulty in delivering a
full spectrum of services• Refuse to allow “drift” toward primarily
individual services for students with severe/chronic problems
• Focus on adapting programs to the needs and competencies of teachers
Johnston & Paternite, OMHNSS 39
Promote EFFECTIVE practices• This involves more than selecting
“evidence-based” practice– Most have not bee examined for
effectiveness, palatability, durability, affordability, and sustainability in real-world school settings
– Remember to include academic and school success outcomes

Johnston & Paternite, OMHNSS 40
“Heart Test”The story of Teddy.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.









![Evidence-Based Practice in Child and Adolescent ~R ......Evidence-Based Practice in Child and Adolescent Mental Health Services Kimberly Hoagwood, Ph.D. Barbara]. Bums, Ph.D. Laurel~er,Ph.D.](https://static.cupdf.com/doc/110x72/6032bcddf5835d70ad7b47d6/evidence-based-practice-in-child-and-adolescent-r-evidence-based-practice.jpg)



















