



9/18/2013
1
Sustainable Compensation Models that Incentivize:Models that Incentivize:Trends and Examples
Jessica A. Johnson, CPABrian M. McCook, CPA
Anders Health Care Webinar SeriesSeptember 18, 2013
Agenda
Introduce and Analyze Trends in PhysicianIntroduce and Analyze Trends in Physician Compensation
Examine Compensation Plan Goalsand Design
Review Basic Models
Identify and Assess Key Benchmark Data

9/18/2013
2
INTRODUCTION AND TRENDS IN PHYSICIAN COMPENSATIONIN PHYSICIAN COMPENSATION
Lessons Learned
Engage physiciansEngage physicians
Invest in the model
Develop clear expectations and goals
Dedicate sufficient management resources

9/18/2013
3
Current Industry Environment
From ToFrom ToFragmented
careCoordinated/Integrated
care
Volume-based
paymentsValue-based payments
Only treating individuals Caring for a population
Payer-driven managed
careProvider-driven
accountable careDGA Partners, Inc. 2012
Compensation Trends
In 2011 the average mix for physician compensationIn 2011, the average mix for physician compensation was 81% guaranteed salary and 19% incentivesWhat to expect going forward?• Physician compensation tied to more complicated
incentives• Technology advancements enable sophisticated data
trackingtracking• Quality plays a greater role for incentive compensation
as over half of physicians have quality metrics included in compensation model
DGA Partners, Inc. 2012; Becker’s Hospital Review September 15,2011; Merritt Hawkins, “Trends in Incentive-Based Physician Compensation” 2011
9/18/2013
4
COMPENSATION PLAN GOALSAND DESIGNAND DESIGN
Effective Compensation Model Elements
FlexibleFlexible
Transparent and objective
Economically fair
Comprehensible
Consistent with philosophy and mission statement
Promote provider accountability and responsibility
9/18/2013
5
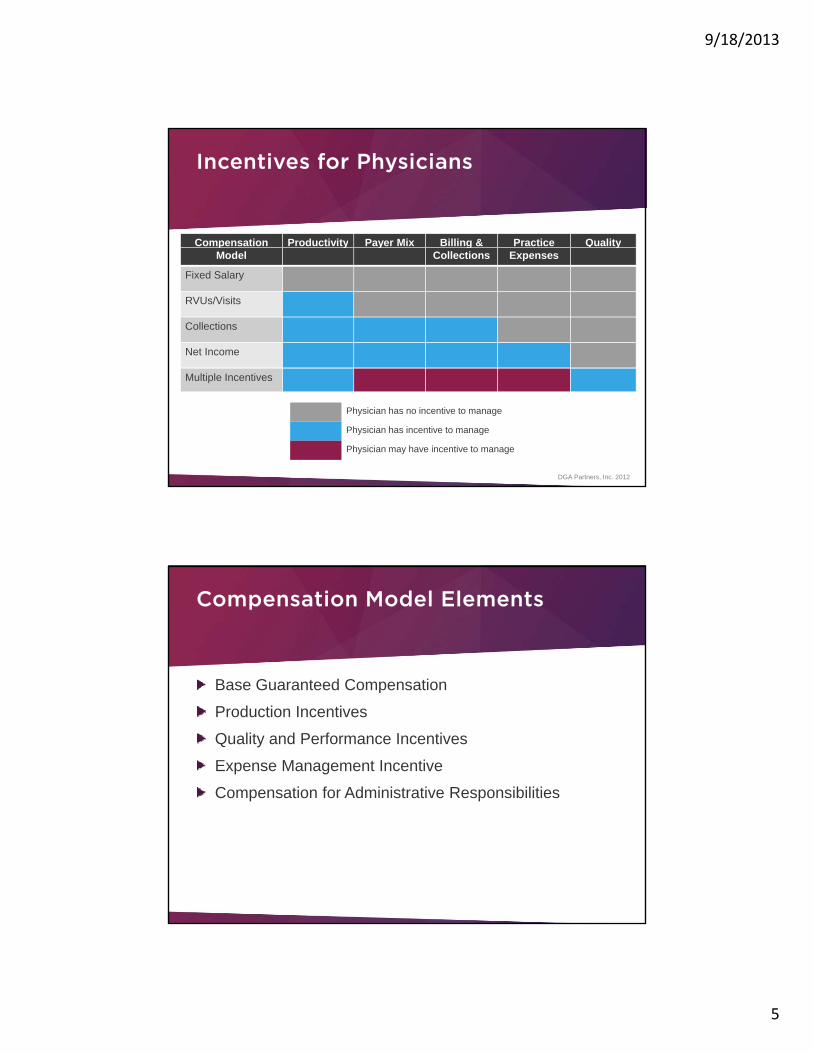
Incentives for Physicians
Compensation Productivity Payer Mix Billing & Practice QualitypModel
y y gCollections Expenses
y
Fixed Salary
RVUs/Visits
Collections
Net Income
Multiple Incentives
Physician has no incentive to manage
Physician has incentive to manage
Physician may have incentive to manage
DGA Partners, Inc. 2012
Compensation Model Elements
Base Guaranteed CompensationBase Guaranteed Compensation
Production Incentives
Quality and Performance Incentives
Expense Management Incentive
Compensation for Administrative Responsibilities
9/18/2013
6
Production Incentives
RVUs (Work and Total)RVUs (Work and Total)
Gross charges
Total collections
Number of new patients
Number of patient encounters
Surgical cases
Procedural volume
Shift in Metrics
Volume
Value

9/18/2013
7
Quality Incentives
Clinical quality measuresClinical quality measures
Patient satisfaction scores
On-time starts
Turn-around time
EHR utilization
Strategic and goal achievement
Coding and charting
Management of the Bottom Line
Staff managementStaff managementOperational managementFinancial management
Practice management• +/- 10% of practice operating budgetp p g g• Sharing of net profit of practice profit/loss
9/18/2013
8
Is the model too complicated?
Design Process
Assess current compensation modelAssess current compensation model• Do you understand current methodology?
• Review compensation and production levels
9/18/2013
9
Design Process
Design modelDesign model• Involve physicians
• Understand priorities
• Develop options
• Identify special situations
• Request feedback
Design Process
Transition to new modelTransition to new model• Develop timeline
• Explain new model and provide case scenarios

9/18/2013
10
REVIEW BASIC MODELS
Types of Compensation Models
Equal sharingEqual sharing
Fixed salary
Base salary plus bonus
Productivity and quality models
9/18/2013
11
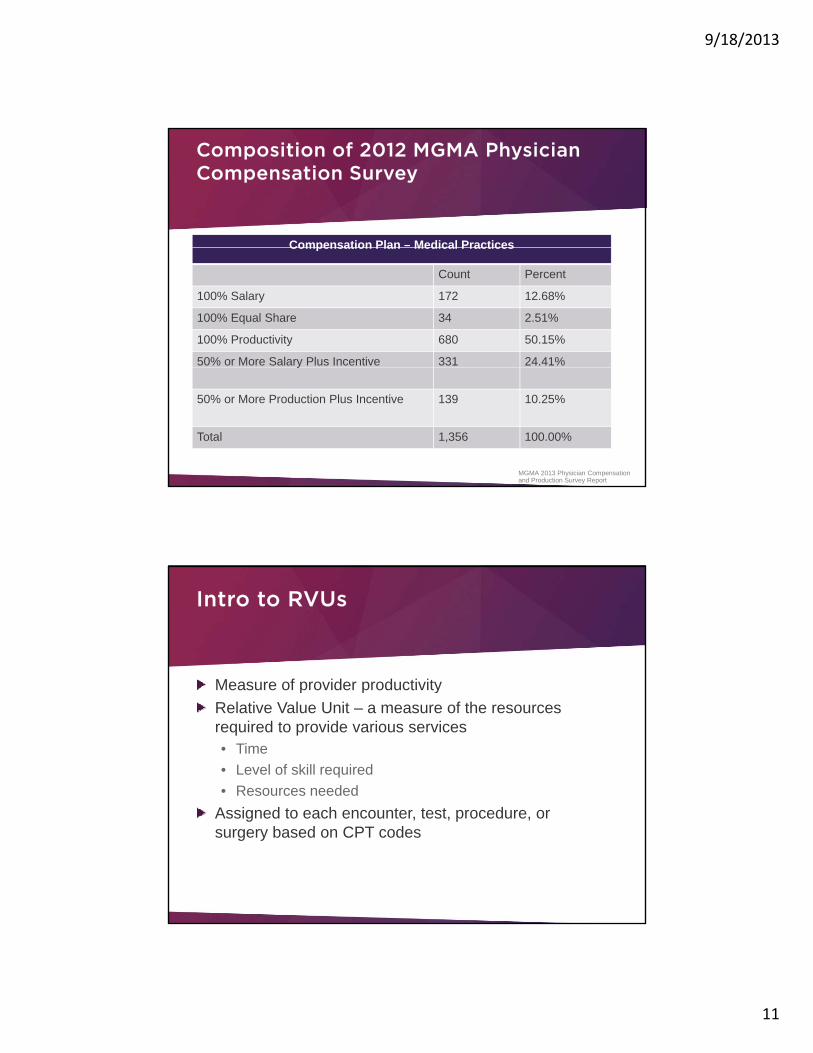
Composition of 2012 MGMA Physician Compensation Survey
Compensation Plan – Medical PracticesCompensation Plan Medical Practices
Count Percent
100% Salary 172 12.68%
100% Equal Share 34 2.51%
100% Productivity 680 50.15%
50% or More Salary Plus Incentive 331 24.41%y
50% or More Production Plus Incentive 139 10.25%
Total 1,356 100.00%
MGMA 2013 Physician Compensation and Production Survey Report
Intro to RVUs
Measure of provider productivityMeasure of provider productivityRelative Value Unit – a measure of the resources required to provide various services• Time• Level of skill required• Resources needed
Assigned to each encounter, test, procedure, or surgery based on CPT codes
9/18/2013
12
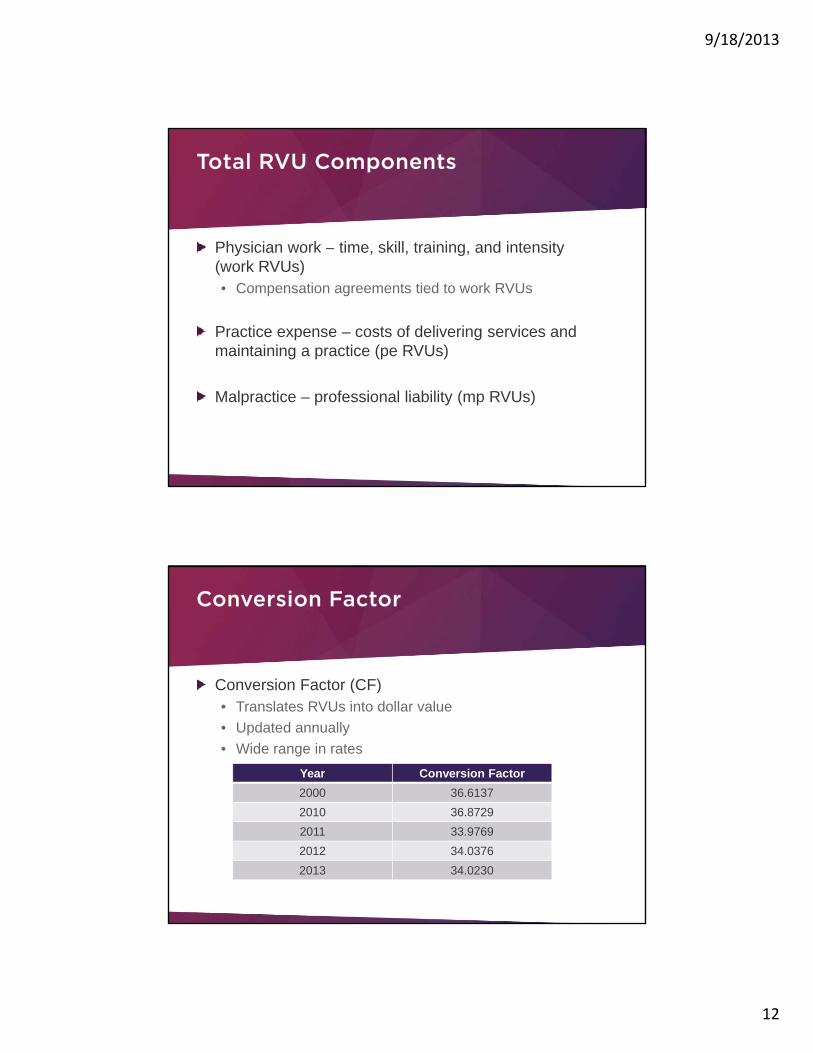
Total RVU Components
Physician work time skill training and intensityPhysician work – time, skill, training, and intensity (work RVUs)• Compensation agreements tied to work RVUs
Practice expense – costs of delivering services and maintaining a practice (pe RVUs)
Malpractice – professional liability (mp RVUs)
Conversion Factor
Conversion Factor (CF)Conversion Factor (CF)• Translates RVUs into dollar value• Updated annually• Wide range in rates
Year Conversion Factor2000 36.61372010 36.87292011 33.97692012 34.03762013 34.0230
9/18/2013
13
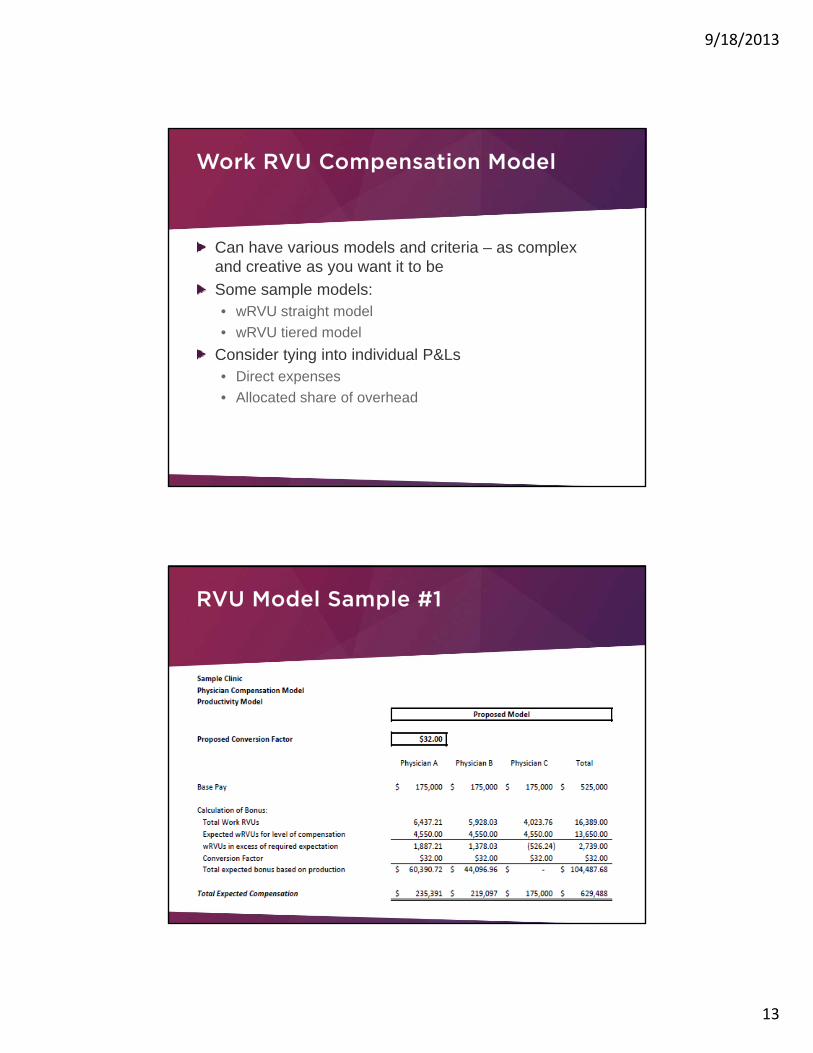
Work RVU Compensation Model
Can have various models and criteria as complexCan have various models and criteria – as complex and creative as you want it to beSome sample models:• wRVU straight model• wRVU tiered model
Consider tying into individual P&Ls • Direct expenses• Allocated share of overhead
RVU Model Sample #1
9/18/2013
14
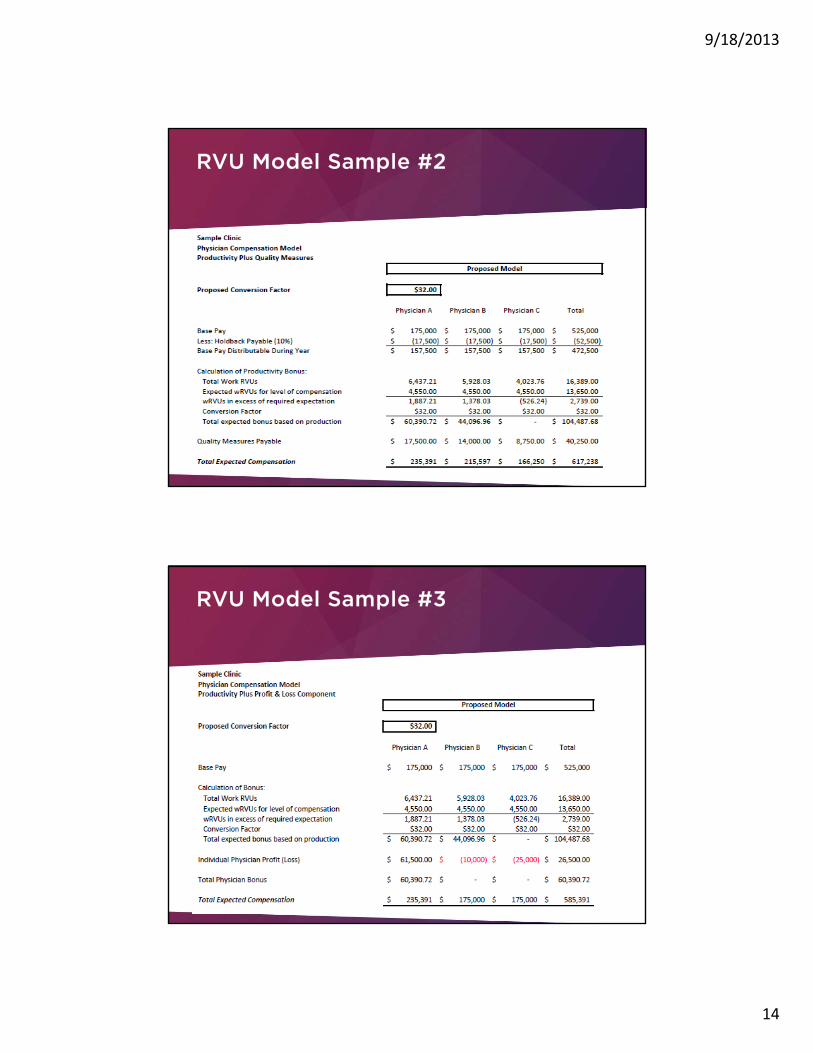
RVU Model Sample #2
RVU Model Sample #3

9/18/2013
15
New Provider – First Year Model
IDENTIFY AND ASSESS KEY BENCHMARK DATABENCHMARK DATA
9/18/2013
16
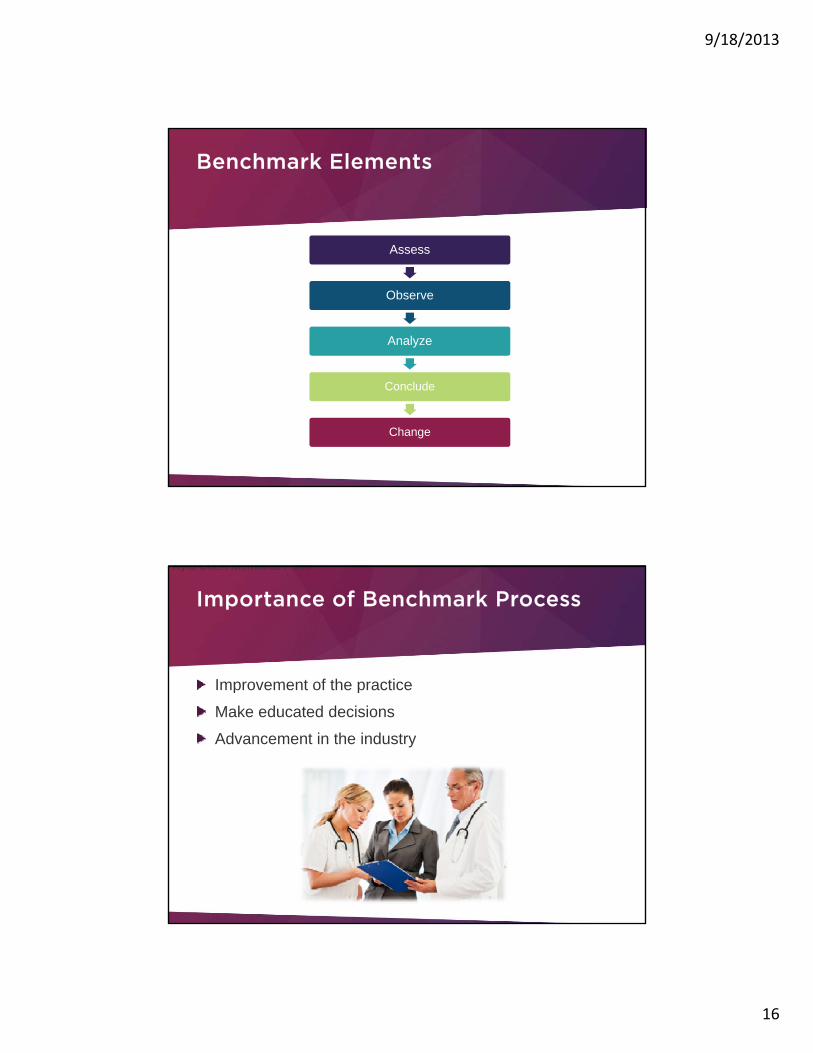
Benchmark Elements
AssessAssess
Observe
Analyze
Conclude
Change
Importance of Benchmark Process
Improvement of the practice
Kyla Coen Memorial Fund
Improvement of the practice
Make educated decisions
Advancement in the industry

9/18/2013
17
Benchmark Data Sources
InternalInternalExternal• Several national surveys are conducted annually
MGMASullivan, Cotter and AssociatesRegional and specialty-specific surveys
Using Benchmark Data
Understand how the data was derivedUnderstand how the data was derived• Type of respondents
• Number of respondents
May consider blending multiple sources of data
Be aware of potential inconsistencies that exist in data• RVU data using different fee schedules
9/18/2013
18
Components of a Sustainable Model
Expectations that must be established for a long termExpectations that must be established for a long-term sustainable model• Financial viability
• Allow for reinvestment
• Must be a win-win for parties involved
Questions

9/18/2013
19
What does all this mean?
Develop a compensation plan that balances effort andDevelop a compensation plan that balances effort and quality.
Identify the metrics that are important to your practice and build around them.
Be transparent.
Try to keep it as simple as possibleTry to keep it as simple as possible.
Make the physician compensation model a recruiting tool for your practice.
www.anderscpa.com/webinar-series
November 6 Operational Effectiveness and Profitability: Identifying and Prioritizing Opportunities
December 4Keeping the Financial Pulse of Your Practice Healthy: Benchmarking and Trends

9/18/2013
20
Anders Health Care Services
Anders Health Care Services optimizes staff, resources and revenue for hospitals and
physicians by offering solutions and direction to complex practice management issues.
We provide an integrated approach from the financial, operational, compliance and strategic
perspectives.
Anders Health Care Services
Jessica A. Johnson, CPA314-655-5556
Brian M. McCook, CPABrian M. McCook, CPA314-655-5564
9/18/2013
21
Anders Health Care Services
John McGuire [email protected] Meyers [email protected] Weith [email protected] Werner [email protected]
314-655-5500www.andershealthcare.com




















![The Longshore and Harbor Workers’ Compensation Act (LHWCA ... · Compensation Act [5 U.S.C. §§8101 et seq.] and also provides limited workers’ compensation programs that cover](https://static.cupdf.com/doc/110x72/5f44a37019207a29571d6b84/the-longshore-and-harbor-workersa-compensation-act-lhwca-compensation-act.jpg)








