




Society of Cardiovascular Anesthesiologists
Cardiovascular Anesthesiology Section Editor: Charles W. Hogue, Jr.
Perioperative Echocardiography and Cardiovascular Education Section Editor: Martin J. London
Hemostasis and Transfusion Medicine Section Editor: Jerrold H. Levy
REVIEW ARTICLE
CME
Fibrinogen and Hemostasis: A Primary HemostaticTarget for the Management of Acquired BleedingJerrold H. Levy, MD, FAHA, Fania Szlam, MMSc, Kenichi A. Tanaka, MD, and Roman M. Sniecienski, MD
Fibrinogen plays several key roles in the maintenance of hemostasis. Its cleavage by thrombinand subsequent polymerization to form fibrin strands provides the structural networkrequired for effective clot formation. During cases of acute blood loss, attempts to maintaincirculating volume and tissue perfusion often involve the infusion of crystalloids, colloids, andred blood cells. Intravascular volume resuscitation, although vital, frequently results indilution of the remaining clotting factors and onset of dilutional coagulopathy. In such cases,fibrinogen is the first coagulation factor to decrease to critically low levels. There currently isa lack of awareness among physicians regarding the significance of fibrinogen during acutebleeding and, at many centers, fibrinogen is not monitored routinely during treatment. Wereviewed current studies that demonstrate the importance of considering fibrinogen replace-ment during the treatment of acquired bleeding across clinical settings. If depleted, thesupplementation of fibrinogen is key for the rescue and maintenance of hemostatic function;however, the threshold at which such intervention should be triggered is currently poorlydefined. Although traditionally performed via administration of fresh frozen plasma orcryoprecipitate, the use of lyophilized fibrinogen (concentrate) is becoming more prevalent insome countries. Recent reports relating to the efficacy of fibrinogen concentrate suggest that itis a viable alternative to traditional hemostatic approaches, which should be considered. Theprospective study of fibrinogen supplementation in acquired bleeding is needed to accuratelyassess the range of clinical settings in which this management strategy is appropriate, the mosteffective method of supplementation and a comprehensive safety profile of fibrinogenconcentrate used for such an approach. (Anesth Analg 2012;114:261–74)
Fibrinogen is a plasma protein critical to hemostasisand clot formation.1 The blood plasma concentrationof fibrinogen ranges between 1.5 and 4.0 g/L but it
can be higher, particularly in certain conditions such aspregnancy.2 Structurally, human fibrinogen comprises 2outer D domains, which are both linked by a central Edomain.3 Each D domain is made up of 3 polypeptidechains (�, �, and �), which together form a coiled-coilconfiguration. These domains are linked at the N-terminusto the central E domain via a series of disulfide bonds.4
Thrombin cleavage occurs at specific amino-acid sequencespresent on the � and � polypeptide chains, removing the
N-terminal peptides (fibrinopeptides) and exposing the po-lymerization sites (Fig. 1).3 Fibrin polymerization then occursvia noncovalent interaction of the exposed polypeptide chainwith complementary binding sites present on the D domain ofa neighboring molecule.3 Furthermore, recent preliminarydata have suggested that fibrinogen may be heme associatedand could play a role in carbon monoxide sensing.5
Studies from our laboratory and others have demonstratedthe importance of thrombin generation and hemostatic acti-vation for clot formation.6–11 Functionally, fibrinogen mol-ecules act during both cellular and fluid phases of coagula-tion. In the cellular phase, it facilitates the aggregation ofplatelets via binding of glycoprotein IIb/IIIa receptors onplatelet surfaces. In the fluid phase, it is cleaved by throm-bin to produce fibrin monomers, which polymerize to formthe basis of the clot (Fig. 2).4,12–14 Fibrinogen also playsother important roles, functioning in vivo as an acute phasereactant, helping modulate inflammatory cellular reactionsand also increasing in plasma concentration after injury.
When acute hemorrhage occurs, the resulting blood lossand consumption of procoagulants combine to reduce thecirculating concentration of multiple clotting factors. De-rangement in common measures of coagulation (prothrom-bin time and activated partial thromboplastin time) candevelop in cases of acute trauma, before administration offluid therapy.15 Such derangements are associated with
From the Department of Anesthesiology, Emory University School ofMedicine, Cardiothoracic Anesthesiology and Critical Care, Emory Health-care, Atlanta, Georgia.
Accepted for publication July 11, 2011.
Funding: Funded by Department of Anesthesiology at the Emory UniversitySchool of Medicine.
Conflict of Interest: See Disclosures at the end of the article.
Reprints will not be available from the authors.
Address correspondence to Jerrold H. Levy, MD, FAHA, Department ofAnesthesiology, Emory University School of Medicine, Cardiothoracic An-esthesiology and Critical Care, Emory Healthcare, Atlanta, GA. Addresse-mail [email protected].
Copyright © 2012 International Anesthesia Research SocietyDOI: 10.1213/ANE.0b013e31822e1853
February 2012 • Volume 114 • Number 2 www.anesthesia-analgesia.org 261

significantly increased mortality rates in trauma patients.15
The dilution of clotting factors during intravascular volumereplacement can result in further coagulopathy; however,such hemostatic intervention is essential for the restorationof circulating volume and tissue perfusion. A prospectiveobservation of plasma concentrations of clotting factors inpatients undergoing major urologic or abdominal surgery(n � 60) showed that levels of prothrombin, factor V, factorVII and fibrinogen were all significantly reduced afterblood loss and subsequent fluid replacement (red bloodcells [RBCs] and colloids).16 Because of its relatively highinitial plasma concentration, fibrinogen was the first clot-ting factor to decrease to critically low levels.16 In noncar-diac major surgery, it has been shown that fibrinogenreaches plasma concentrations of 1 g/L when 142% (95%confidence interval [CI], 117 to 169%) of the circulatingblood volume has been lost.16
The maintenance of hemostasis relies on a series ofcomplex interactions between both the cellular and proteincomponents of coagulation.17 Importantly, platelets play akey role in many of these interactions; the platelet surface isthe primary site for thrombin generation,17 and plateletsaggregate to form the primary hemostatic plug,18 as well asstabilizing clot formation.1 Circulating platelet concentra-tions reduce in a similar manner to the observed depletionof clotting factors during major surgery.16 As such, thedevelopment of thrombocytopenia in critically bleedingpatients is a significant challenge to hemostasis. In vitroanalysis of platelet-poor plasma showed a positive correla-tion of viscoelastic measurements of clot strength withincreasing fibrinogen concentration,1 a result that wascorroborated by a retrospective analysis of 904 thrombocy-topenic patients. As such, the maintenance of fibrinogenconcentrations is crucial in cases of thrombocytopenia.1
The clinical relevance of plasma fibrinogen concentrationsin bleeding patients is not widely recognized and, as a result,physicians may not routinely measure fibrinogen levels orconsider supplementation options when treating major bleed-ing. In this review we will discuss the importance of fibrino-gen in clot formation and the therapeutic approaches forreplacing fibrinogen in acquired bleeding states.
ACUTE BLOOD LOSS AND MASSIVETRANSFUSION COAGULOPATHYIn cases of acute blood loss, restoring circulatory volume isa primary objective often addressed with volume expand-ers such as crystalloids, colloids, or a combination ofboth.19,20 The ideal volume expander has been the subjectof significant debate; however, the administration of anyvolume expander will result in the reduction of plateletsand plasma clotting factor concentrations.21 In such cases,the commonly observed change is dilutional thrombocyto-penia, but continuing blood loss can lead to a morecomplex coagulopathy. Neither concentrates of RBCs orplatelets contain enough plasma to supplement the de-pleted factors sufficiently to maintain hemostatic balance.16
Thus, continued consumption of clotting factors coupledwith their dilution with volume expanders can lead to thedevelopment of dilutional coagulopathy.
The critical role of fibrinogen deficiency and fibrinolysis incases of major bleeding is increasingly described.1,22,23 Thepreoperative measurement of plasma fibrinogen concentra-tion was found to be predictive of postoperative bleedingvolume and transfusion requirements in a prospectiveobservation of coronary bypass grafting surgical patients(n � 170).24 In another example, a multivariate analysis ofpostpartum hemorrhage (n � 128) reported that fibrinogenconcentration was the only hemostatic marker consistentlyassociated with the occurrence of severe postpartum hemor-rhage. It was concluded that the early measurement of fibrino-gen was able to detect reductions in plasma fibrinogenconcentration, allowing the risk of severe bleeding to bepredicted. As such, monitoring of this kind is recommendedduring the management of obstetric-related bleeding events.25
A greater understanding of the predictive value ofplasma fibrinogen concentrations has led to the potentialfor laboratory-guided, prophylactic supplementation ofcoagulation factors in cases of elective procedures. Thus, in
Figure 1. The thrombin cleavage of fibrinogen and polymerization offibrin monomers to fibrin. A schematic representation of the throm-bin cleavage of fibrinogen, followed by the polymerization of fibrinmonomers to form fibrin strands is illustrated.
Figure 2. A fibrin blood clot: the constituent parts of a blood clot are shown(red blood cells, red; fibrin fibers, blue; platelet aggregates, purple). FromJohn W. Weisel, PhD, University of Pennsylvania, with permission.
REVIEW ARTICLE
262 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA

events when hemorrhage is likely, the onset of coagulopa-thy can be delayed and the extent of bleeding reduced. Arecent prospective randomized controlled pilot study (n �20) investigating prophylactic fibrinogen supplementationbefore coronary artery bypass grafting showed thatpostoperative bleeding was reduced by 32% in patientsreceiving 2 g fibrinogen concentrate preoperatively in com-parison with the control group (565 � 150 vs 830 � 268 mL;P � 0.010), without any evidence of hypercoagulability.26
Recognizing the emerging evidence, which highlights theimportance of maintaining adequate plasma fibrinogenconcentrations, European guidelines now include theadministration of fibrinogen concentrate among their rec-ommendations for the treatment of trauma-related, life-threatening hemorrhage; however, it should be noted thatthis recommendation is based upon the lowest level ofevidence available to the guideline authors.19,27
FIBRINOGEN REPLACEMENTThere are 3 main approaches to fibrinogen supplementa-tion, which involve the infusion of fresh frozen plasma(FFP), cryoprecipitate, or fibrinogen concentrate.
Fresh Frozen PlasmaFFP contains all proteins present in human plasma, includingalbumin, immunoglobulins, and coagulation and fibrinolyticelements, which are at or below physiological concentrations(Table 1).28 It is commonly transfused for the reversal of oralanticoagulation therapy,29 but is also used for coagulationfactor supplementation during acute bleeding.30 Althoughextensively used during massive transfusion protocols, FFPpreparations have been associated with the potential risk of
pathogen transmission.31,32 Commercially available plasmacan be virally inactivated using 1 of 4 major treatmentprocesses to minimize the risk of pathogen contamination:solvent-detergent (SD), methylene blue, amotosalen, or ribo-flavin. All 4 methods demonstrate effectiveness against com-mon pathogens, including human immunodeficiency virus.33
With the exception of SD-treated plasma, these methods aredesigned for small-volume use at blood banks,33 and theavailability of such plasmas is limited to certain regions andcountries. Immunological reactions, including allergic reac-tions, and transfusion-related acute lung injury can also resultfrom FFP administration.32
FFP contains approximately 2.0 g/L34 of fibrinogen, butfibrinogen concentrations do vary between units; thuspredicting the increase in patient plasma fibrinogen con-centrations after transfusion is difficult.28 When the in vivofibrinogen concentration was measured in patients trans-fused with 30 mL/kg of FFP (approximating to 2.1 L of FFPfor a 70-kg patient), a median increase of 1.0 g/L (range, 0.9to 2.4 g/L) was observed.35 Thus, large volumes of FFP arerequired to increase plasma fibrinogen concentrations inbleeding patients, increasing the risk of hypervolemia andtransfusion-related circulatory overload.36 FFP is used in-creasingly in situations such as massive transfusion coagu-lopathy; however, a recent systematic review of massiveplasma transfusion found very-low-quality evidence thatsuch treatment reduces the risk of patient death.36
CryoprecipitateCryoprecipitate is a human plasma concentrate that wasfirst described in the 1960s.37 It is manufactured from FFP,and the processes involved have changed little since it was
Table 1. A Comparison of the Constituent Components of the Transfusion Options for Fibrinogen Supplementation
Coagulationfactor
FFP, relative content (%)in comparison withnormal plasma28,34
Cryoprecipitate, relativecontent (%) in comparison
with normal plasma: per singledonor unit (20–50 mL)38
Fibrinogen concentrates
Riastap™d/Haemocomplettan P/HS�e
(per 50-mL vial) (CSLBehring, Marburg, Germany)
Clottafact�f
(LFB-biomedicaments)(per 100-mL vial)
(LFB-biomedicaments,Paris, France)
Fibrinogen 2.0 mg/mL (0.9–3.2)34b 388 mgc (range: 120–796 mg) 18–26 mg/mL �15 mg/mLFII 90 (72–108)34b — — —FV 88 (72–108)34b — — —FVII 90 (59–120)34b — — —FVIII 53 (32–92)34b — — —FIX 68 (45–87)34b — — —FX 88 (72–108)34b — — —FXI 10028 — — —FXII 8328 — — —FXIII 10028 20%–30% — —Antithrombin III 10028 — — —VWF 8028c — — —FVIII and VWFa — 40%–70% — —Fibronectin — 20%–25% — —IgG — 5%–8% — —IgM — 1%–2% — —Albumin — 5%–8% 8–14 mg/mL —L-arginine — — 7.5–13.2 mg/mL —Sodium chloride — — 4–7 mg/mL —Sodium citrate — — 1–2 mg/mL —
F � factor; FFP � fresh frozen plasma; Ig � immunoglobulin; VWF � Von Willebrand factor.a Reported jointly. b Median (reported range). c With some loss of high molecular weight multimers, particularly if solvent/detergent treated. d Licensed inEuropean countries and the United States for congenital fibrinogen deficiency. e Licensed in Austria, Brazil, Bulgaria, Germany, the Czech Republic, Hungary,Kuwait, the Netherlands, Portugal, Romania, Switzerland, Taiwan, and Turkey for acquired bleeding. fLicensed in France for acquired bleeding.
Fibrinogen Management in Acquired Bleeding
February 2012 • Volume 114 • Number 2 www.anesthesia-analgesia.org 263

first discovered. In short, the thawing (between 1°C and 6°C)and subsequent centrifugation of FFP is followed by theremoval of the supernatant.38 The remaining 5 to 15 mL ofplasma is refrozen and can be stored in this way for up to 12months.38 According to recent testing, each unit of cryopre-cipitate contains a median fibrinogen concentration of 388 mg(range, 120 to 796 mg), whereas the minimum requirements ofthe American Association of Blood Banks (AABB) is 150 mgper unit.38 The typical concentrations of other constituentscontained in each unit are displayed in Table 1.
Because cryoprecipitate contains higher concentra-tions of fibrinogen than does FFP, it is the therapy optionoften used for fibrinogen supplementation in the UnitedStates (US) and United Kingdom. However, the existingrisk of immunological reactions and the transmission ofinfectious agents has led to its withdrawal in severalEuropean countries.39 Cryoprecipitate is unsuitable forviral inactivation processes in its native form,40 thoughplasma derivatives that have been pretreated with meth-ylene blue or SD can be used for its production.39
Unfortunately, such pretreatment processes can reducethe concentration of functional fibrinogen present.39,40
As with FFP, cryoprecipitate requires blood type match-ing and thawing before infusion, delaying administra-tion in time-critical situations.
Fibrinogen ConcentrateFibrinogen concentrate is derived from human plasma andis stored at room temperature as a pasteurized, lyophilizedpowder.41 It does not require blood type matching orthawing; thus it is available immediately when required. Itcan be reconstituted in low-volume concentrations of up to20 g/L.41 Doses as high as 6 g infused in as little as 1 to 2minutes have been reported in critical bleeding.42 A sum-mary of fibrinogen concentrates currently available isshown in Table 1. Commercially available fibrinogen con-centrates are primarily licensed for the treatment of con-genital fibrinogen deficiency across the US and Europe, anda license for the treatment of acquired bleeding has beengranted for only 1 of these products in some Europeancountries (Table 1).
The risk of viral infection with fibrinogen concentrates issignificantly reduced because of viral inactivation andremoval processes.43 This inherent viral reduction capacityalso minimizes the risk of transmitting new emergingviruses.43 Although fibrinogen concentrate is manufac-tured using human plasma from a large pool of donors, theproduction processes involved remove antibodies and an-tigens, largely mitigating the risk of immunological andallergic reactions resulting from its administration.39 Itshould be noted that although this risk is much reduced, aswith all blood products, fibrinogen concentrate administra-tion will always have the theoretical potential for transmis-sion of new emerging infectious agents.44
Historically, the occurrence of thromboembolic eventshas been a concern surrounding the administration ofclotting factor concentrates. With respect to fibrinogenconcentrate specifically, there are currently no results fromlarge prospective randomized controlled clinical trials onwhich any firm judgments can be based. Although anincrease in the amount of available prospective data would
provide valuable evidence for fully evaluating the throm-botic potential of fibrinogen concentrate, reviews of pub-lished clinical data and a recent pharmacovigilance reporthave demonstrated no significant thrombogenic concernswith fibrinogen concentrate.45,46 Furthermore, a study of151 separate infusions administered to 12 patients withcongenital fibrinogen deficiencies showed that the supple-mentation of fibrinogen using fibrinogen concentrate forprophylaxis, as well as during bleeding episodes andsurgery, was both efficient (with a median in vivo fibrino-gen recovery of 59.8% [n � 8; range: 32.5 to 93.9]) andgenerally well tolerated.47 In support of the clinical data,animal models of venous stasis have found that fibrinogenconcentrates demonstrated no thrombogenic activity.22,45 Itshould be noted, however, that the use of fibrinogenconcentrate in patients exhibiting disseminated intravascu-lar coagulation is potentially hazardous because of the riskof accelerated fibrin formation and should be avoided.41
Current opinion still remains divided regarding whatconstitutes the correct and appropriate administration offibrinogen concentrate in the critical care setting.44,48
Surveillance data may not provide reliable estimates ofthrombotic adverse events, which can occur up to 3months postsurgery at the doses used.44 It is also impor-tant to consider that there is no current prospectivecomparison of the safety profiles of FFP, cryoprecipitate,and fibrinogen concentrate, when administered for fi-brinogen supplementation.
CURRENT UNDERSTANDING OFFIBRINOGEN REPLACEMENTPreclinical DataIn a porcine model of thrombocytopenia, fibrinogen con-centrate was shown to better improve hemostatic functionand survival times than platelet transfusion alone afterblunt liver injury.22 A second porcine model of blunt livertrauma has compared bleeding and subject outcomesamong animals receiving varying concentrations of fibrino-gen concentrate. When compared with placebo, the admin-istration of fibrinogen concentrate (70 or 200 mg/kg) aftersevere dilutional coagulopathy both significantly improvedcoagulation and attenuated blood loss.49 Although theproper dosing cannot be determined from the studiesinvolving nonhuman species, in vitro clinical data usinghuman blood also demonstrate that increased fibrinogenconcentration improves clot strength independently ofplatelet count.1,50 Taken together, these results suggest thatrestoration of plasma fibrinogen concentrations using fi-brinogen concentrate could be an effective hemostatic treat-ment in cases of acquired bleeding.
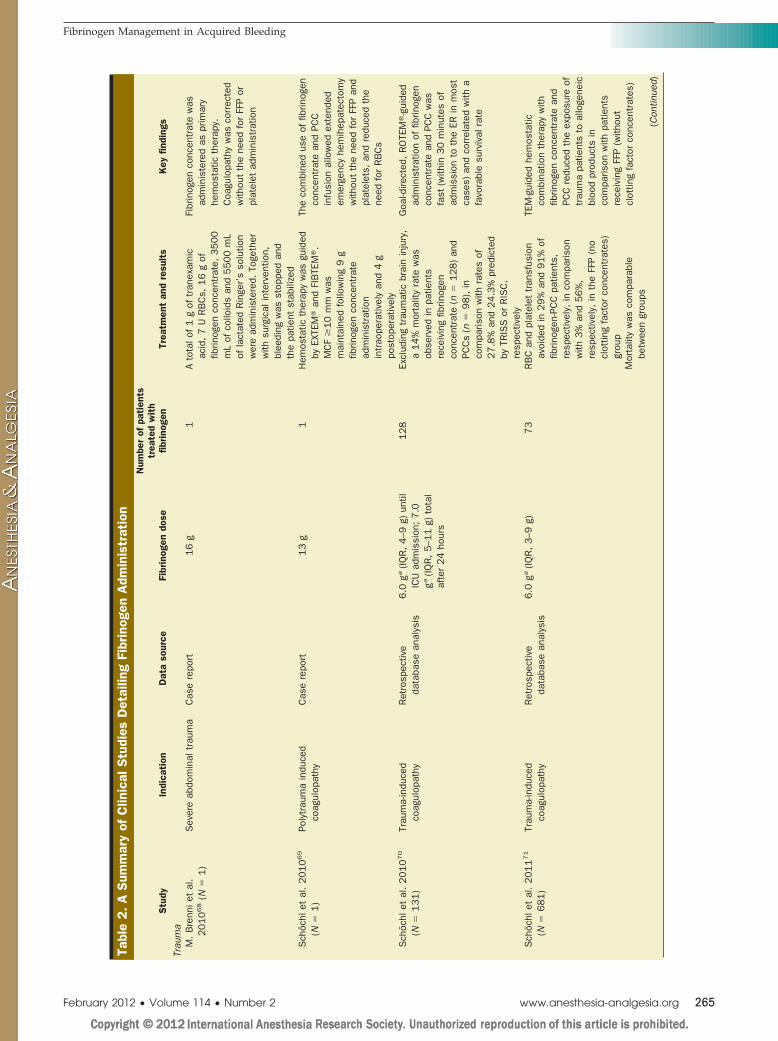
Clinical DataSince fibrinogen supplementation in cases of major bleed-ing was established as a potentially useful treatment ap-proach, the efficacy of fibrinogen concentrate has beenassessed by many retrospective and some prospectivestudies. Its administration for the treatment of acquiredbleeding has been studied in heterologous cohorts ofpatients across a range of critical care settings (summarizedin Table 2).
REVIEW ARTICLE
264 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Tabl
e2.A
Sum
mar
yof
Clin
ical
Stu
dies
Det
ailin
gFi
brin
ogen
Adm
inis
trat
ion
Stu
dyIn
dica
tion
Dat
aso
urce
Fibr
inog
endo
se
Num
ber
ofpa
tien
tstr
eate
dw
ith
fibrino
gen
Trea
tmen
tan
dre
sult
sK
eyfin
ding
sTr
aum
aM
.B
renn
iet
al.
2010
68
(N�
1)
Sev
ere
abdo
min
altr
aum
aC
ase
repo
rt16
g1
Ato
talo
f1
gof
tran
exam
icac
id,
7U
RB
Cs,
16
gof
fibrin
ogen
conc
entr
ate,
3500
mL
ofco
lloid
san
d5500
mL
ofla
ctat
edR
inge
r’s
solu
tion
wer
ead
min
iste
red.
Toge
ther
with
surg
ical
inte
rven
tion,
blee
ding
was
stop
ped
and
the
patie
ntst
abili
zed
Fibr
inog
enco
ncen
trat
ew
asad
min
iste
red
aspr
imar
yhe
mos
tatic
ther
apy.
Coa
gulo
path
yw
asco
rrec
ted
with
out
the
need
for
FFP
orpl
atel
etad
min
istr
atio
n
Sch
öchl
etal
.2010
69
(N�
1)
Poly
trau
ma
indu
ced
coag
ulop
athy
Cas
ere
port
13
g1
Hem
osta
ticth
erap
yw
asgu
ided
byEX
TEM
�an
dFI
BTE
M�.
MC
F�
10
mm
was
mai
ntai
ned
follo
win
g9
gfib
rinog
enco
ncen
trat
ead
min
istr
atio
nin
trao
pera
tivel
yan
d4
gpo
stop
erat
ivel
y
The
com
bine
dus
eof
fibrin
ogen
conc
entr
ate
and
PCC
infu
sion
allo
wed
exte
nded
emer
genc
yhe
mih
epat
ecto
my
with
out
the
need
for
FFP
and
plat
elet
s,an
dre
duce
dth
ene
edfo
rR
BC
s
Sch
öchl
etal
.2010
70
(N�
131)
Trau
ma-
indu
ced
coag
ulop
athy
Ret
rosp
ectiv
eda
taba
sean
alys
is6.0
ga(IQ
R,
4–9
g)un
tilIC
Uad
mis
sion
;7.0
ga(IQ
R,
5–1
1g)
tota
laf
ter
24
hour
s
128
Excl
udin
gtr
aum
atic
brai
nin
jury
,a
14%
mor
talit
yra
tew
asob
serv
edin
patie
nts
rece
ivin
gfib
rinog
enco
ncen
trat
e(n
�128)
and
PCC
s(n
�98),
inco
mpa
rison
with
rate
sof
27.8
%an
d24.3
%pr
edic
ted
byTR
ISS
orR
ISC
,re
spec
tivel
y
Goa
l-dire
cted
,R
OTE
M�-g
uide
dad
min
istr
atio
nof
fibrin
ogen
conc
entr
ate
and
PCC
was
fast
(with
in30
min
utes
ofad
mis
sion
toth
eER
inm
ost
case
s)an
dco
rrel
ated
with
afa
vora
ble
surv
ival
rate
Sch
öchl
etal
.2011
71
(N�
681)
Trau
ma-
indu
ced
coag
ulop
athy
Ret
rosp
ectiv
eda
taba
sean
alys
is6.0
ga(IQ
R,
3–9
g)73
RB
Can
dpl
atel
ettr
ansf
usio
nav
oide
din
29%
and
91%
offib
rinog
en-P
CC
patie
nts,
resp
ectiv
ely,
inco
mpa
rison
with
3%
and
56%
,re
spec
tivel
y,in
the
FFP
(no
clot
ting
fact
orco
ncen
trat
es)
grou
p
TEM
-gui
ded
hem
osta
ticco
mbi
natio
nth
erap
yw
ithfib
rinog
enco
ncen
trat
ean
dPC
Cre
duce
dth
eex
posu
reof
trau
ma
patie
nts
toal
loge
neic
bloo
dpr
oduc
tsin
com
paris
onw
ithpa
tient
sre
ceiv
ing
FFP
(with
out
clot
ting
fact
orco
ncen
trat
es)
Mor
talit
yw
asco
mpa
rabl
ebe
twee
ngr
oups
(Con
tinue
d)
Fibrinogen Management in Acquired Bleeding
February 2012 • Volume 114 • Number 2 www.anesthesia-analgesia.org 265

Tabl
e2.(C
onti
nued
)
Stu
dyIn
dica
tion
Dat
aso
urce
Fibr
inog
endo
se
Num
ber
ofpa
tien
tstr
eate
dw
ith
fibrino
gen
Trea
tmen
tan
dre
sult
sK
eyfin
ding
sC
ardi
ovas
cula
rsu
rger
yK
arls
son
etal
.2009
26
(N�
20)
Elec
tive
CAB
GPr
ospe
ctiv
era
ndom
ized
phas
eI/
IIst
udy
2.0
g10
Fibr
inog
enin
fusi
onre
duce
dpo
stop
erat
ive
blee
ding
(12
hour
s)by
32%
(565
�150
vs830
�268
mL;
P�
0.0
1).
No
clin
ical
lyde
tect
able
adve
rse
even
tsw
ere
reco
rded
inth
efib
rinog
engr
oup
Fibr
inog
enco
ncen
trat
ew
asad
min
iste
red
prio
rto
CAB
G(fi
brin
ogen
grou
p).
Red
uced
blee
ding
with
out
evid
ence
ofhy
perc
oagu
labi
lity
was
obse
rved
inth
efib
rinog
engr
oup
inco
mpa
rison
with
the
cont
rolg
roup
Rah
e-M
eyer
etal
.2009
74
(N�
15)
Aort
icva
lve
oper
atio
nan
das
cend
ing
aort
are
plac
emen
t
Pros
pect
ive,
nonr
ando
miz
edpi
lot
stud
y
5.7
(�0.7
)gb
10
Tota
ltra
nsfu
sion
requ
irem
ents
(fibr
inog
engr
oup
vsco
ntro
l)w
ere
0.7
U(�
1.5
)vs
8.2
U(�
2.3
),an
dpo
stop
erat
ive
drai
nage
volu
me
was
716
mL
(�219
mL)
vs366
mL
(�199
mL)
The
perio
pera
tive
adm
inis
trat
ion
offib
rinog
enco
ncen
trat
epr
ior
toth
ein
stig
atio
nof
the
esta
blis
hed
bloo
dpr
oduc
ttr
ansf
usio
nal
gorit
hmw
asin
vest
igat
edin
blee
ding
patie
nts.
Fibr
inog
enco
ncen
trat
ein
fusi
onre
duce
dtr
ansf
usio
nre
quire
men
tsan
d24-h
our
post
oper
ativ
ebl
eedi
ngR
ahe-
Mey
eret
al.
2009
80
(N�
18)
Thor
acoa
bdom
inal
aort
ican
eury
smsu
rger
yR
etro
spec
tive
cont
rol
grou
pvs
pros
pect
ive
fibrin
ogen
grou
p
7.8
gb(�
2.7
g)6
Tota
ltra
nsfu
sion
requ
irem
ents
(fibr
inog
engr
oup
vsco
ntro
l)w
ere
2.5
U(S
D,
�4.3
)vs
16.4
U(S
D,
�4.8
).4
of6
patie
nts
rece
ivin
gfib
rinog
enco
ncen
trat
ere
quire
dno
tran
sfus
ion
ofal
loge
neic
bloo
dpr
oduc
ts
Prop
hyla
ctic
adm
inis
trat
ion
offib
rinog
enco
ncen
trat
esi
gnifi
cant
lyre
duce
dtr
ansf
usio
nof
allo
gene
icbl
ood
prod
ucts
and
post
oper
ativ
ebl
eedi
ng
Sol
omon
etal
.2010
42
(N�
39)
Post
card
iopu
lmon
ary
bypa
sssu
rger
yO
pen-
labe
l,un
cont
rolle
d,re
tros
pect
ive
stud
y
6.5
gb(�
1.6
g)(7
8��
20
�m
g/kg
)39
Mea
nfib
rinog
enle
vel
incr
ease
dto
2.2
9(�
0.7
)m
g/dL
per
mg/
kgbo
dyw
eigh
tof
fibrin
ogen
conc
entr
ate
adm
inis
tere
d.M
axim
umcl
otfir
mne
ssin
crea
sed
from
10
to21
mm
Adm
inis
trat
ion
offib
rinog
enco
ncen
trat
era
ised
plas
ma
fibrin
ogen
conc
entr
atio
nan
dco
ntrib
uted
toth
eco
rrec
tion
ofpo
stop
erat
ive
blee
ding
(Con
tinue
d)
REVIEW ARTICLE
266 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA

Tabl
e2.
(Con
tinu
ed)
Stu
dyIn
dica
tion
Dat
aso
urce
Fibr
inog
endo
se
Num
ber
ofpa
tien
tstr
eate
dw
ith
fibrino
gen
Trea
tmen
tan
dre
sult
sK
eyfin
ding
sPe
riope
rativ
ebl
eedi
ngC
.Fe
nger
-Erik
sen
etal
.2009
98
(N�
20)
Rad
ical
cyst
ecto
my
Sin
gle-
cent
er,
pros
pect
ive,
doub
le-b
lind,
plac
ebo-
cont
rolle
d,ra
ndom
ized
clin
ical
tria
l
45
mg/
kg10
Sig
nific
ant
incr
ease
inm
axim
umcl
otfir
mne
ss.
Two
of10
patie
nts
who
rece
ived
fibrin
ogen
conc
entr
ate
requ
ired
pos
tope
rativ
eR
BC
svs
8of
10
inpl
aceb
ogr
oup
Ran
dom
ized
plac
ebo-
cont
rolle
dad
min
istr
atio
nof
fibrin
ogen
conc
entr
ate
sign
ifica
ntly
impr
oved
max
imum
clot
firm
ness
and
redu
ced
the
requ
irem
ent
for
post
oper
ativ
etr
ansf
usio
nM
itter
may
ret
al.
2007
82
(N�
66)
Ort
hope
dic
surg
ery
Pros
pect
ive
obse
rvat
iona
lst
udy
30
mg/
kg13
MC
Fan
dfib
rinog
enpo
lym
eriz
atio
nsi
gnifi
cant
lyde
crea
sed
inth
epa
tient
sre
ceiv
ing
HES
(are
aun
der
the
curv
em
inus
base
line
(�
5�
�9
to�
2�)
,fo
llow
edby
gela
tinso
lutio
n(
�3
��
8to
0�)
,w
ithth
esm
alle
stre
duct
ions
seen
for
Rin
ger’
sla
ctat
eso
lutio
n(
�2
��
4to
1�)
Dis
turb
ance
offib
rinog
en/fi
brin
poly
mer
izat
ion
isth
epr
imar
ypr
oble
mtr
igge
ring
dilu
tiona
lco
agul
opat
hy.
Fibr
inog
enco
ncen
trat
ead
min
istr
atio
nm
aint
aine
dcl
otfir
mne
ssin
thes
eca
ses,
even
inth
epr
esen
ceof
cont
inue
dbl
eedi
ng
Bel
let
al.
2010
87
(N�
6)
Obs
tetr
iche
mor
rhag
eC
olle
ctio
nof
6ca
sere
port
sN
/A6
Labo
rato
ryas
sess
edco
agul
atio
nw
asra
pidl
yno
rmal
ized
and
seve
rehe
mor
rhag
eim
prov
edfo
llow
ing
fibrin
ogen
conc
entr
ate
adm
inis
trat
ion
Fibr
inog
enco
ncen
trat
eco
uld
effe
ctiv
ely
redu
cepe
ripar
tum
bloo
dlo
ssas
soci
ated
with
hypo
fibrin
ogen
emia
Cro
ss-s
ettin
gad
min
istr
atio
nD
anes
etal
.2008
51
(N�
69)
Sur
gery
,tr
aum
aan
dga
stro
inte
stin
alhe
mor
rhag
e.H
epat
icdy
sfun
ctio
nan
dhe
mat
olog
ical
mal
igna
ncie
s
Ope
n-la
bel,
nonc
ontr
olle
dre
tros
pect
ive
stud
y
3.52
ga(ra
nge,
0.5–
8.0g
)69
Mea
nab
solu
tein
crea
sein
plas
ma
fibrin
ogen
was
1.0
9g/
L24
hour
saf
ter
trea
tmen
t;co
agul
atio
nva
riabl
essi
gnifi
cant
lyim
prov
ed;
mor
talit
yra
tes
of32.3
%an
d44.2
%af
ter
24
hour
san
d72
hour
s
Fibr
inog
enco
ncen
trat
ead
min
istr
atio
nim
prov
edla
bora
tory
coag
ulat
ion
mea
sure
san
dm
aybe
life
savi
ngin
patie
nts
with
life-
thre
aten
ing,
unre
spon
sive
coag
ulop
athy
(Con
tinue
d)
Fibrinogen Management in Acquired Bleeding
February 2012 • Volume 114 • Number 2 www.anesthesia-analgesia.org 267

Retrospective analyses (n � 30) of fibrinogen concen-trate administration to treat acquired hypofibrinogenemiaand life-threatening bleeding found it was effective in themanagement of such events,46 improving laboratory coagu-lation measures and survival rates in unresponsive coagu-lopathy.51 Laboratory monitoring of plasma fibrinogenconcentrations has shown significant increases after fi-brinogen concentrate administration (median dose, 3.52 g[range: 0.5 to 8.0]; mean increase [� sd] in plasma fibrino-gen, 1.09 [�0.68] g/L),51 with associated improvements inboth prothrombin time and activated partial thromboplas-tin time.51,52 Retrospective analysis of such laboratorycoagulation measurements, in bleeding patients (n � 43)treated with fibrinogen concentrate, demonstrated thatsuch improvements have led to reduced blood loss andlower requirements for RBCs (�12 U vs �2 U), FFP (�8 Uvs �2 U), and platelets (�2.5 U vs �0.5 U).53 Theseblood-sparing effects indicate that fibrinogen concentratecould potentially challenge traditional hemostatic ap-proaches using FFP and platelet concentrates.
TraumaThe significant loss of blood volume associated withtrauma-related bleeding often precipitates the “lethal triad”of acidosis, hypothermia, and coagulopathy. Coagulopathyin trauma patients results from the rapid depletion ofcirculating coagulation factors because of consumption andblood loss. Although acidemia, hypothermia, and subse-quent dilution all interact to contribute to trauma-relatedcoagulopathy, the interplay between these mechanisms isyet to be fully elucidated.54 Importantly, trauma-relatedcoagulopathy is a leading cause of mortality,55,56 and isresponsible for up to 40% of trauma-related deaths.19 Insuch cases, the need for effective and rapid hemostasismanagement is important, in addition to the rapid surgicalcontrol of bleeding. In cases of trauma-related massivebleeding, European transfusion guidelines recommend theprimary restoration of circulating volume and secondaryhemostatic measures via transfusion of blood products orpharmaceutical agents.19,27 Recent military experience oftrauma has strongly influenced transfusion practices in UStrauma centers.57,58 Several observational studies have sug-gested that transfusion of high ratios of FFP to RBCs (1:1) iskey to improving survival rates in patients with majortrauma.59–61 Consequently, many civilian trauma centersare now adopting massive transfusion protocols, whichinclude the transfusion of FFP in high volumes.62 Althoughthis approach is not universally accepted,63–65 and thecomplete restoration of circulating volume is not recom-mended in the US, it is becoming clear that the timelysupplementation of coagulation factors during majortrauma-related bleeding is important for the improvementof patient outcomes.66 A retrospective review of battlefieldtrauma reported 252 patients receiving massive transfu-sion, in which the total amount of fibrinogen infused withinall administered blood products (FFP, RBCs, and platelets)correlated with reductions in mortality.67
There are increasing reports of fibrinogen replacementusing concentrates administered as a first-line treatment oftrauma. Brenni et al. detailed a case study in whichfibrinogen concentrate was used in combination with RBCsTa
ble
2.(C
onti
nued
)
Stu
dyIn
dica
tion
Dat
aso
urce
Fibr
inog
endo
se
Num
ber
ofpa
tien
tstr
eate
dw
ith
fibrino
gen
Trea
tmen
tan
dre
sult
sK
eyfin
ding
sW
eink
ove
etal
.2008
46
(N�
30)
Plac
enta
labr
uptio
n,m
assi
vebl
ood
loss
and
tran
sfus
ion,
liver
failu
re,
card
iac
surg
ery
Ret
rosp
ectiv
eda
taba
sean
alys
is4.
0(ra
nge,
2.0–
14.0
g)a
30
Med
ian
abso
lute
incr
ease
inpl
asm
afib
rinog
enpe
r1
gof
fibrin
ogen
conc
entr
ate
was
0.2
5g/
L(0
.65–2
.01
g).
Ble
edin
gst
oppe
din
46%
ofpa
tient
str
eate
dw
ithfib
rinog
enan
dbl
ood
com
pone
nts
alon
e
Fibr
inog
enco
ncen
trat
eap
pear
sto
beef
fect
ive
inth
em
anag
emen
tof
acqu
ired
blee
ding
,be
ing
able
topr
ovid
ea
cons
iste
ntdo
sein
the
emer
genc
yse
ttin
g
Feng
er-E
rikse
net
al.5
2
2008
(N�
43)
Ser
ious
acqu
ired
blee
ding
:pr
imar
ilyob
stet
ricco
mpl
icat
ions
,ca
rdio
thor
acic
and
intr
a-ab
dom
inal
blee
ding
Ret
rosp
ectiv
eda
taba
sean
alys
isAd
ults
:2.0
ga(r
ange
,1–5
g);
child
ren:
0.3
5ga
(ran
ge,
0.2
–0.5
g)
43
Med
ian
incr
ease
inpl
asm
afib
rinog
enco
ncen
trat
ion
was
1.0
g/L
(fro
m1.4
�1.0
–1.8
�to
2.4
�2.1
–2.6
�).
Inad
ults
,m
edia
nto
talb
lood
loss
decr
ease
dsi
gnifi
cant
lyfr
om4000
ml(
1500–7
750
mL)
to50
mL
(0–4
25
mL)
Off-la
belfi
brin
ogen
conc
entr
ate
adm
inis
trat
ion
led
tosi
gnifi
cant
redu
ctio
nsin
both
blee
ding
and
the
requ
irem
ent
for
tran
sfus
ion
ofR
BC
s,pl
atel
ets,
and
FFP
CAB
G�
coro
nary
arte
ryby
pass
graf
t;ER
�em
erge
ncy
room
;FF
P�
fres
hfr
ozen
plas
ma;
ICU
�in
tens
ive
care
unit;
PCC
�pr
othr
ombi
nco
mpl
exco
ncen
trat
e;R
BC
s�
red
bloo
dce
lls;
RIS
C�
revi
sed
inju
ryse
verit
ycl
assi
ficat
ion;
RO
TEM
�ro
tatio
nalt
hrom
boel
asto
met
ry;
TRIS
S�
trau
ma
inju
ryse
verit
ysc
ore;
MC
F�
max
imum
clot
firm
ness
;H
ES�
hydr
oxye
thyl
star
ch;
N/A
�no
tap
plic
able
;IQ
R�
inte
rqua
rtile
rang
e.a
Med
ian.
bM
ean.
REVIEW ARTICLE
268 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA

as a primary hemostatic agent for the treatment of coagu-lopathy resulting from major abdominal trauma.68 Coagu-lopathy was corrected without the use of allogeneic bloodproducts, highlighting the potential efficacy and safetybenefits of such management protocols. The coadministra-tion of fibrinogen concentrate with other prohemostaticagents is an effective management protocol for traumapatients. A separate case study details the administration offibrinogen concentrate, in combination with prothrombincomplex concentrate (PCC), for the successful treatment ofpolytrauma.69 The combined use of these coagulation fac-tor concentrates, guided by point-of-care assessment (rota-tional thromboelastometry [ROTEM�; TEM InnovationsGmbH, Munich, Germany]), eliminated the need for allo-geneic factors (including FFP and platelet transfusion) andreduced the need for RBCs. A larger, retrospective analysisof a patient cohort with acquired bleeding (n � 131 total)receiving similar transfusion protocols adds weight to theconclusions drawn by these case studies.70 Patients infusedwith fibrinogen concentrates (n � 128) and PCCs (n � 98),using ROTEM-guided goal-directed coagulation manage-ment, displayed favorable survival rates in relation to thosepredicted by the trauma injury severity score (TRISS).70 Asimilar retrospective analysis compared a group of traumapatients (n � 80) receiving TEM-guided fibrinogen concen-trate (median 6 g [range: 0 to 15 g]) and PCC administration(median 1200 U [range: 0 to 6600]) with trauma patientsadministered FFP in the absence of coagulation factorconcentrates (n � 601, median 6 U [range: 2 to 51]).71 Theneed for RBC and platelet transfusion was avoided in 29%and 91% of fibrinogen-PCC patients, respectively, in com-parison with 3% and 56%, respectively, in the FFP group.The study authors concluded that the TEM-guided admin-istration of coagulation factor concentrates reduced theexposure level of trauma patients to allogeneic bloodproducts; however, it should be noted that mortality ratesbetween groups remained broadly comparable (7.5%vs.10.0% [fibrinogen-PCC versus FFP; P � 0.69]).
These studies highlight the potentially useful combina-tion of modern, real-time, coagulation monitoring with theadministration of clotting factor concentrates capable ofrapidly increasing the plasma concentrations of procoagu-lants in a goal-directed fashion. Currently, evidence, whichdemonstrates the efficacy of this approach, is restricted tocase studies and retrospective analyses. There are concernsthat highlight the limitations in study design that areinherent in such retrospective analyses, and care should betaken regarding the strength of conclusions that can bedrawn on the basis of their results.72 It is clear that thoughpromising, further prospective studies are required tobetter establish the dosing efficacy and safety of thisapproach.
Perioperative BleedingFibrinogen concentrate is now used across a range ofsurgical settings to maintain patient hemostasis and controlbleeding. There follows an overview of recent studies thatexamines the efficacy of fibrinogen concentrate adminis-tered perioperatively.
Cardiovascular and Vascular SurgeryCardiovascular and vascular surgical procedures are oftenaccompanied by excessive bleeding.73–75 Perioperativebleeding is a serious problem that can lead to increases inboth morbidity and mortality rates.76,77 The effective man-agement of such bleeding is the key to improved patientoutcomes, and a variety of approaches are now available tophysicians.78 Increasing numbers of both prospective andretrospective studies allow analysis of the impact of coagu-lation management in surgical procedures typically associ-ated with excessive hemorrhage.
A retrospective study investigating mortality rates inpatients (n � 128) undergoing ruptured abdominal aorticaneurysm repair found a significant reduction in mortalityrates (15% vs 39%; P � 0.03) in patients receiving RBC:FFPratio of �2:1 (high FFP cohort) in comparison with thosereceiving �2:1 ratios (low FFP cohort).79 These resultssuggest that high volumes of FFP can effectively aidhemostatic function and improve patient outcomes duringhigh-risk procedures. Fibrinogen concentrate may also beof benefit during such procedures. A study comparing bothretrospective and prospective data investigated the use offibrinogen concentrate during aortic valve and ascendingaorta surgery. Eight of 10 patients (prospective group)receiving fibrinogen concentrate before surgery requiredno transfusion of RBCs during cardiopulmonary bypass orwithin the subsequent 24 hours. In comparison, 41 of 42patients (retrospective group) receiving conventional he-mostatic therapy did require RBC transfusion within thesame period (P � 0.05).74 A follow-up study evaluatedprospective fibrinogen replacement using concentrates in 6patients as an initial treatment of postbypass bleedingduring thoracoabdominal aortic aneurysm repair in com-parison with a retrospective cohort of patients receiving noprophylaxis (n � 20).80 The need for transfusion of alloge-neic blood products was reduced in patients receivingfibrinogen concentrate in comparison with those who didnot (2.5 � 4.3 U vs 16.4 � 4.8 U), as was both the amountof bleeding during the following 24 hours, and the averagelength of treatment in the intensive care unit.80 Thesepreliminary data have led to the initiation of a prospectiverandomized clinical trial to further elucidate the potentialof fibrinogen concentrate in this setting (ClinicalTrials.govidentifier number NCT00701142).
A retrospective analysis (n � 39) of fibrinogen concen-trate infusion after cardiopulmonary bypass showed it tobe an effective method of increasing the plasma fibrinogenconcentration (mean dose [�sd]: 6.5 [�1.6]; absolute in-crease: 1.7 [�0.5] g/L).42 As was mentioned previously,serious intraoperative bleeding was treated successfullyusing rapid fibrinogen concentrate infusion in some cases(�6 g in 1 to 2 minutes). The study authors concluded thatthe use of fibrinogen concentrate contributed to the correc-tion of bleeding after surgery.42
Noncardiovascular SurgeryPatients undergoing orthopedic surgery are at risk of signifi-cant bleeding and developing dilutional coagulopathy, whichmay be influenced by the solution used for intravascularvolume replacement.21,81,82 A prospective study comparedpatients receiving colloids (either hydroxyethyl starch [HES]
Fibrinogen Management in Acquired Bleeding
February 2012 • Volume 114 • Number 2 www.anesthesia-analgesia.org 269

[n � 19] or a modified gelatin solution [n � 21]) with thosereceiving Ringer’s lactate solution (n � 21) for volume re-placement during major orthopedic surgery, and examinedcoagulation variables using ROTEM.82 Fibrinogen polymer-ization was significantly impaired in patients receiving colloidrather than crystalloid. Different HES solutions variably im-pede fibrinogen polymerization, resulting in reduced clotfirmness. The administration of fibrinogen concentrate led tothe restoration and maintenance of clot firmness, even duringcontinued blood loss and further colloid administration.82
A prospective, placebo-controlled, randomized study(n � 20) of patients undergoing elective radical cystectomyinvestigated the ability of fibrinogen concentrate to restorehemostasis in patients experiencing excessive blood loss.83
Patients received HES for volume replacement when re-quired as part of the established blood replacement regi-men; treatment with fibrinogen concentrate was triggeredonce 30% volume dilution had occurred. In comparisonwith placebo, fibrinogen supplementation significantly im-proved both whole blood clot firmness and the rate of clotformation. Additionally, the requirement for postoperativetransfusion of RBCs was significantly reduced.83
Obstetric HemorrhageObstetric hemorrhage remains a major cause of mortalityand morbidity associated with childbirth.84,85 The increasein uterine arterial bloodflow during labor means thatmassive obstetric hemorrhage (�1500 mL) can rapidlyresult in life-threatening blood loss, occurring in approxi-mately 0.67% of all deliveries.86 Such events require vol-ume resuscitation and allogeneic transfusion; however, thisapproach can contribute to coagulopathy because of furtherdilution of coagulation factors. A review of 6 cases of severeobstetric hemorrhage suggested that the addition of fi-brinogen concentrate to traditional therapies was effectivein the treatment of peripartum blood loss associated withhypofibrinogenemia.87 Fibrinogen administration in com-bination with other blood products can control bleedingeven during continuing consumption and hemodilution.
These initial studies detail potential mechanisms bywhich severe obstetric hemorrhage could be both predictedand attenuated. However, it should be noted that there iscurrently little published evidence conclusively showingfibrinogen concentrate to be effective in preventing obstet-ric bleeding. Further prospective studies are needed toelucidate the full potential of this treatment option.
RECOMMENDED TRIGGER CONCENTRATIONSFOR FIBRINOGENFibrinogen Detection AssaysQuantitative fibrinogen detection can be performed immu-nologically, measuring both functional and nonfunctionalfibrinogen molecules. Functional assays that measurefibrinogen-dependent clot formation are used most oftenand utilize spectroscopic or viscoelastic detection. TheClauss method is a frequently used functional fibrinogenassay, whereby diluted citrated plasma is activated withthrombin and the time-to-clot formation is recorded spec-troscopically.41 Viscoelastic detection is performed usingwhole blood. When tested this way, the blood is housed ina cup (maintained at 37°C) and a pin is suspended within
the sample. The cup and pin are oscillated in relation toeach other and any subsequent impedance to this oscilla-tion provides a measure of clot formation.88 Point-of-caretesting using viscoelastic measures of clot strength (TEG�;Hemonetics�, Braintree, MA, or ROTEM) allow patient-specific, rapid, and guided supplementation of depletedcoagulation elements.69,70,89,90 The extent of fibrin polym-erization in whole blood can be estimated by inhibitingplatelet-fibrin(ogen) interactions on the TEG-based Func-tional Fibrinogen Test or ROTEM-based FIBTEM. The latteris commonly used in European countries to titrate thedosing of fibrinogen concentrates.69,70,89
When deciding which functional test is most appropri-ate for fibrinogen detection, several considerations must bemade. One advantage of using viscoelastic testing forfibrinogen determination is the inherent variability ofClauss-based fibrinogen assays. Clauss-based fibrinogenmeasurements may be falsely decreased in the presence ofdirect thrombin inhibitors,91 and falsely increased in thepresence of HES solutions.92 In general, the turbidimetric(optical) detection method is affected more than mechanicaldetections by these agents.93 However, it should be notedthat the viscoelastic methodology described has not beenprospectively validated for the measurement of fibrinogen-dependent clot formation during acute bleeding. It is notuniversally available, and furthermore, recent evidencesuggests that the measurement of fibrinogen levels usingFIBTEM can vary after hemostatic therapy, dependingupon the type of coagulometer being used.93
Treatment Thresholds and Dosing of FibrinogenAlthough there are increasing data on the importance ofplasma fibrinogen levels to prevent profuse bleeding, thethreshold levels for transfusing either cryoprecipitate orfibrinogen concentrates have not been agreed on univer-sally because of a lack of prospective evidence or consistentobservations across different clinical settings. There hasbeen some concern over iatrogenic hyperfibrinogenemiabecause increased plasma fibrinogen concentrations havebeen linked to an increased risk of coronary heart diseaseand myocardial infarction.94 However, a study by Reinhartdemonstrated that fibrinogen is a marker rather than amediator of coronary heart disease.95
The revised European trauma guidelines published in 2010recommend a trigger fibrinogen concentration of 1.5 to 2.0g/L,27 which was increased from below 1.0 g/L in earlierguidelines.96 This change is in agreement with other in vitroevidence that concentrations larger than 2.0 g/L are requiredto produce effective clot formation.50 Importantly, fibrinogenconcentrations can vary among patients, as well as duringincidences of acquired bleeding. Although the target plasmafibrinogen concentration that should be reached in a bleedingpatient is not known, and the optimum dose of fibrinogen hasnot been established by dose-ranging trials, bleeding increasesfor each 1.0 g/L decrease in plasma fibrinogen in parturi-ents.25 In vitro viscoelastic analysis of whole blood shows clotstrength increases linearly up to a fibrinogen concentration of3.0 g/L, with a minimum threshold of 2.0 g/L required for theoptimal rate of clot formation.50,97
Because of the large variability in fibrinogen concentra-tions among bleeding patients, increasing fibrinogen levels
REVIEW ARTICLE
270 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA

should be individualized and based upon both the level ofbleeding and the plasma fibrinogen concentration.41 Aninitial dose of 10 U of cryoprecipitate, or 2.0 to 4.0 g offibrinogen concentrate is recommended for a 70-kg pa-tient,41 with subsequent administration dependent upon anindividual’s bleeding status. For fibrinogen concentrates,the required dose can be estimated as follows41,74:
Fibrinogen dose � desired increase (g/L) �
plasma volume (L).
Thus, administration of 3 g of fibrinogen concentrate in a70-kg patient approximates to an overall increase in plasmafibrinogen concentration of 1.0 g/L (assuming 0.04 L/kgplasma volume). Predicting the increase in plasma fibrino-gen concentrations that will result after cryoprecipitateadministration is troublesome, because of the wide varia-tion in fibrinogen concentration between units.39
SUMMARYFibrinogen is critical for effective clot formation, and itsmonitoring and guided supplementation in the treatmentof major bleeding is increasingly recognized. A growingnumber of reports note the importance of fibrinogen re-placement in the treatment of massive bleeding across abroad range of clinical settings.1,22,42,51,68–70,74,80,82,87,98
Available sources of fibrinogen for supplementation in-clude FFP, cryoprecipitate, and fibrinogen concentrates.Coagulation factor concentrates offer potential advantagesover allogeneic blood products, such as decreased immu-nogenic and infectious complications, as well as rapidavailability. Studies of the efficacy and safety of fibrinogensupplementation during acute bleeding has been mostoften retrospective or performed in prospective trials withlimited participant numbers owing to ethical and practicalconstraints. This must be considered when evaluating theevidence on the administration of fibrinogen in bleedingpatients. As such, further prospective, randomized con-trolled studies on the use of fibrinogen concentrate areessential to help define the breadth of clinical settings inwhich fibrinogen supplementation may be beneficial. Ad-ditional evidence would also help further define optimaltrigger concentrations and doses for fibrinogensupplementation.
RECUSE NOTEJerrold H. Levy is section Editor of Hemostasis and Transfu-sion Medicine for Anesthesia & Analgesia. This manuscript washandled by Steve Shafer, Editor-in-Chief, and Dr. Levy was notinvolved in any way with the editorial process or decision.
DISCLOSURESName: Jerrold H. Levy.Contribution: Performed literature search and manuscriptpreparation, oversaw ongoing revisions and corrections.Conflict of Interest: Dr. Levy receives research support from CSIBehring.Name: Fania Szlam.Contribution: Reviewed manuscript, added additional infor-mation and references.Conflict of Interest: This author has no conflict to declare.
Name: Kenichi A. Tanaka, MD.Contribution: Reviewed manuscript, added additional infor-mation and references.Conflict of Interest: Dr. Tanaka receives research support fromCSL Behring and Octapharma.Name: Roman M. Sniecienski, MD.Contribution: Reviewed manuscript, added additional infor-mation, references, and developed figures for manuscript.Conflict of Interest: This author has no conflict to declare.This manuscript was handled by: Steven L. Shafer, MD.
REFERENCES1. Lang T, Johanning K, Metzler H, Piepenbrock S, Solomon C,
Rahe-Meyer N, Tanaka KA. The effects of fibrinogen levels onthromboelastometric variables in the presence of thrombocy-topenia. Anesth Analg 2009;108:751–8
2. Simon L, Santi TM, Sacquin P, Hamza J. Pre-anaestheticassessment of coagulation abnormalities in obstetric patients:usefulness, timing and clinical implications. Br J Anaesth1997;78:678–83
3. Kollman JM, Pandi L, Sawaya MR, Riley M, Doolittle RF. Crystalstructure of human fibrinogen. Biochemistry 2009;48:3877–86
4. Mosesson MW. Fibrinogen and fibrin structure and functions.J Thromb Haemost 2005;3:1894–904
5. Nielsen VG, Cohen JB, Malayaman SN, Nowak M, Vosseller K.Fibrinogen is a heme-associated, carbon monoxide sensing molecule:a preliminary report. Blood Coagul Fibrinolysis 2011;22:443–7
6. He S, Blomback M, Jacobsson Ekman G, Hedner U. The role ofrecombinant factor VIIa (FVIIa) in fibrin structure in theabsence of FVIII/FIX. J Thromb Haemost 2003;1:1215–9
7. Johansson PI, Jacobsen N, Viuff D, Olsen EH, Rojkjaer R,Andersen S, Petersen LC, Kjalke M. Differential clot stabilisingeffects of rFVIIa and rFXIII-A2 in whole blood from thrombo-cytopenic patients and healthy volunteers. Br J Haematol2008;143:559–69
8. Kjalke M, Ezban M, Monroe DM, Hoffman M, Roberts HR,Hedner U. High-dose factor VIIa increases initial thrombingeneration and mediates faster platelet activation inthrombocytopenia-like conditions in a cell-based model sys-tem. Br J Haematol 2001;114:114–20
9. Roberts HR, Hoffman M, Monroe DM. A cell-based model ofthrombin generation. Semin Thromb Hemost 2006;32(suppl 1):32–8
10. Tanaka KA, Key NS, Levy JH. Blood coagulation: hemostasisand thrombin regulation. Anesth Analg 2009;108:1433–46
11. Bolliger D, Gorlinger K, Tanaka KA. Pathophysiology andtreatment of coagulopathy in massive hemorrhage and he-modilution. Anesthesiology 2010;113:1205–19
12. Weisel JW, Veklich Y, Gorkun O. The sequence of cleavage offibrinopeptides from fibrinogen is important for protofibrilformation and enhancement of lateral aggregation in fibrinclots. J Mol Biol 1993;232:285–97
13. Gorkun OV, Veklich YI, Weisel JW, Lord ST. The conversion offibrinogen to fibrin: recombinant fibrinogen typifies plasmafibrinogen. Blood 1997;89:4407–14
14. Weisel JW, Nagaswami C, Vilaire G, Bennett JS. Examinationof the platelet membrane glycoprotein IIb-IIIa complex and itsinteraction with fibrinogen and other ligands by electronmicroscopy. J Biol Chem 1992;267:16637–43
15. Brohi K, Singh J, Heron M, Coats T. Acute traumatic coagu-lopathy. J Trauma 2003;54:1127–30
16. Hiippala ST, Myllyla GJ, Vahtera EM. Hemostatic factors andreplacement of major blood loss with plasma-poor red cellconcentrates. Anesth Analg 1995;81:360–5
17. Hoffman M, Monroe DM 3rd. A cell-based model of hemosta-sis. Thromb Haemost 2001;85:958–65
18. Ruggeri ZM. The role of von Willebrand factor and fibrinogenin the initiation of platelet adhesion to thrombogenic surfaces.Thromb Haemost 1995;74:460–3
19. Stainsby D, MacLennan S, Thomas D, Isaac J, Hamilton PJ.Guidelines on the management of massive blood loss. Br JHaematol 2006;135:634–41
20. Donaldson MD, Seaman MJ, Park GR. Massive blood transfu-sion. Br J Anaesth 1992;69:621–30
Fibrinogen Management in Acquired Bleeding
February 2012 • Volume 114 • Number 2 www.anesthesia-analgesia.org 271

21. Fenger-Eriksen C, Anker-Moller E, Heslop J, Ingerslev J, So-rensen B. Thrombelastographic whole blood clot formationafter ex vivo addition of plasma substitutes: improvements ofthe induced coagulopathy with fibrinogen concentrate. Br JAnaesth 2005;94:324–9
22. Velik-Salchner C, Haas T, Innerhofer P, Streif W, NussbaumerW, Klingler A, Klima G, Martinowitz U, Fries D. The effect offibrinogen concentrate on thrombocytopenia. J ThrombHaemost 2007;5:1019–25
23. Kashuk JL, Moore EE, Sawyer M, Wohlauer M, Pezold M,Barnett C, Biffl WL, Burlew CC, Johnson JL, Sauaia A. Primaryfibrinolysis is integral in the pathogenesis of the acute coagu-lopathy of trauma. Ann Surg 2010;252:434–42
24. Karlsson M, Ternstrom L, Hyllner M, Baghaei F, Nilsson S,Jeppsson A. Plasma fibrinogen level, bleeding, and transfusionafter on-pump coronary artery bypass grafting surgery: aprospective observational study. Transfusion 2008;48:2152–8
25. Charbit B, Mandelbrot L, Samain E, Baron G, Haddaoui B,Keita H, Sibony O, Mahieu-Caputo D, Hurtaud-Roux MF,Huisse MG, Denninger MH, de Prost D. The decrease offibrinogen is an early predictor of the severity of postpartumhemorrhage. J Thromb Haemost 2007;5:266–73
26. Karlsson M, Ternstrom L, Hyllner M, Baghaei F, Flinck A,Skrtic S, Jeppsson A. Prophylactic fibrinogen infusion re-duces bleeding after coronary artery bypass surgery. Aprospective randomised pilot study. Thromb Haemost2009;102:137– 44
27. Rossaint R, Bouillon B, Cerny V, Coats TJ, Duranteau J,Fernandez-Mondejar E, Hunt BJ, Komadina R, Nardi G,Neugebauer E, Ozier Y, Riddez L, Schultz A, Stahel PF,Vincent JL, Spahn DR. Management of bleeding followingmajor trauma: an updated European guideline. Crit Care2010;14:R52
28. O’Shaughnessy DF, Atterbury C, Bolton Maggs P, Murphy M,Thomas D, Yates S, Williamson LM. Guidelines for the use offresh-frozen plasma, cryoprecipitate and cryosupernatant. Br JHaematol 2004;126:11–28
29. Stanworth SJ, Brunskill SJ, Hyde CJ, Murphy MF, McClellandDB. Appraisal of the evidence for the clinical use of FFP andplasma fractions. Best Pract Res Clin Haematol 2006;19:67–82
30. Shaz BH, Dente CJ, Harris RS, MacLeod JB, Hillyer CD.Transfusion management of trauma patients. Anesth Analg2009;108:1760–8
31. Sarani B, Dunkman WJ, Dean L, Sonnad S, Rohrbach JI, GraciasVH. Transfusion of fresh frozen plasma in critically ill surgicalpatients is associated with an increased risk of infection. CritCare Med 2008;36:1114–8
32. Holness L, Knippen MA, Simmons L, Lachenbruch PA. Fatali-ties caused by TRALI. Transfus Med Rev 2004;18:184–8
33. Rock G. A comparison of methods of pathogen inactivation ofFFP. Vox Sang 2011;100:169–78
34. Theusinger OM, Baulig W, Seifert B, Emmert MY, Spahn DR,Asmis LM. Relative concentrations of haemostatic factors andcytokines in solvent/detergent-treated and fresh-frozenplasma. Br J Anaesth 2011;106:505–11
35. Chowdhury P, Saayman AG, Paulus U, Findlay GP, CollinsPW. Efficacy of standard dose and 30 ml/kg fresh frozenplasma in correcting laboratory parameters of haemostasis incritically ill patients. Br J Haematol 2004;125:69–73
36. Murad MH, Stubbs JR, Gandhi MJ, Wang AT, Paul A, ErwinPJ, Montori VM, Roback JD. The effect of plasma transfusionon morbidity and mortality: a systematic review and meta-analysis. Transfusion 2010;50:1370–83
37. Pool JG, Gershgold EJ, Pappenhagen AR. High-potency antih-aemophilic factor concentrate prepared from cryoglobulin pre-cipitate. Nature 1964;203:312
38. Callum JL, Karkouti K, Lin Y. Cryoprecipitate: the current stateof knowledge. Transfus Med Rev 2009;23:177–88
39. Sorensen B, Bevan D. A critical evaluation of cryoprecipitatefor replacement of fibrinogen. Br J Haematol 2010;149:834 – 43
40. Seghatchian J, Krailadsiri P. What’s happening? The quality ofmethylene blue treated FFP and cryo. Transfus Apher Sci2001;25:227–31
41. Fenger-Eriksen C, Ingerslev J, Sorensen B. Fibrinogenconcentrate—a potential universal hemostatic agent. ExpertOpin Biol Ther 2009;9:1325–33
42. Solomon C, Pichlmaier U, Schoechl H, Hagl C, Raymondos K,Scheinichen D, Koppert W, Rahe-Meyer N. Recovery of fi-brinogen after administration of fibrinogen concentrate topatients with severe bleeding after cardiopulmonary bypasssurgery. Br J Anaesth 2010;104:555–62
43. Pereira A. Cryoprecipitate versus commercial fibrinogenconcentrate in patients who occasionally require a therapeu-tic supply of fibrinogen: risk comparison in the case of anemerging transfusion-transmitted infection. Haematologica2007;92:846 –9
44. Ozier Y, Hunt BJ. Against: Fibrinogen concentrate for manage-ment of bleeding: against indiscriminate use. J Thromb Hae-most 2011;9:6–8
45. Dickneite G, Pragst I, Joch C, Bergman GE. Animal model andclinical evidence indicating low thrombogenic potential offibrinogen concentrate (Haemocomplettan P). Blood CoagulFibrinolysis 2009;20:535–40
46. Weinkove R, Rangarajan S. Fibrinogen concentrate for acquiredhypofibrinogenaemic states. Transfus Med 2008;18:151–7
47. Kreuz W, Meili E, Peter-Salonen K, Haertel S, Devay J, KrzenskU, Egbring R. Efficacy and tolerability of a pasteurised humanfibrinogen concentrate in patients with congenital fibrinogendeficiency. Transfus Apher Sci 2005;32:247–53
48. Rahe-Meyer N, Sorensen B. For: Fibrinogen concentrate formanagement of bleeding. J Thromb Haemost 2011;9:1–5
49. Grottke O, Braunschweig T, Henzler D, Coburn M, Tolba R,Rossaint R. Effects of different fibrinogen concentrations onblood loss and coagulation parameters in a pig model ofcoagulopathy with blunt liver injury. Crit Care 2010;14:R62
50. Bolliger D, Szlam F, Molinaro RJ, Rahe-Meyer N, Levy JH,Tanaka KA. Finding the optimal concentration range forfibrinogen replacement after severe haemodilution: an in vitromodel. Br J Anaesth 2009;102:793–9
51. Danes AF, Cuenca LG, Bueno SR, Mendarte Barrenechea L,Ronsano JB. Efficacy and tolerability of human fibrinogenconcentrate administration to patients with acquired fibrino-gen deficiency and active or in high-risk severe bleeding. VoxSang 2008;94:221–6
52. Fenger-Eriksen C, Lindberg-Larsen M, Christensen AQ, IngerslevJ, Sørensen B. Fibrinogen concentrate substitution therapy inpatients with massive haemorrhage and low plasma fibrinogenconcentrations. Br J Anaesth 2008;101:769–73
53. Fenger-Eriksen C, Lindberg-Larsen M, Christensen AQ, Inger-slev J, Sorensen B. Fibrinogen concentrate substitution therapyin patients with massive haemorrhage and low plasma fibrino-gen concentrations. Br J Anaesth 2008;101:769–73
54. Hess JR, Brohi K, Dutton RP, Hauser CJ, Holcomb JB, Kluger Y,Mackway-Jones K, Parr MJ, Rizoli SB, Yukioka T, Hoyt DB,Bouillon B. The coagulopathy of trauma: a review of mecha-nisms. J Trauma 2008;65:748–54
55. Murray CJ, Lopez AD. Mortality by cause for eight regions ofthe world: Global Burden of Disease Study. Lancet1997;349:1269–76
56. Krug EG, Sharma GK, Lozano R. The global burden of injuries.Am J Public Health 2000;90:523–6
57. Geeraedts LM Jr, Demiral H, Schaap NP, Kamphuisen PW,Pompe JC, Frolke JP. ‘Blind’ transfusion of blood products inexsanguinating trauma patients. Resuscitation 2007;73:382–8
58. Gonzalez EA, Moore FA, Holcomb JB, Miller CC, Kozar RA,Todd SR, Cocanour CS, Balldin BC, McKinley BA. Fresh frozenplasma should be given earlier to patients requiring massivetransfusion. J Trauma 2007;62:112–9
59. Borgman MA, Spinella PC, Perkins JG, Grathwohl KW, RepineT, Beekley AC, Sebesta J, Jenkins D, Wade CE, Holcomb JB. Theratio of blood products transfused affects mortality in patientsreceiving massive transfusions at a combat support hospital.J Trauma 2007;63:805–13
60. Gunter OL Jr, Au BK, Isbell JM, Mowery NT, Young PP, CottonBA. Optimizing outcomes in damage control resuscitation:identifying blood product ratios associated with improvedsurvival. J Trauma 2008;65:527–34
REVIEW ARTICLE
272 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA

61. Zink KA, Sambasivan CN, Holcomb JB, Chisholm G, SchreiberMA. A high ratio of plasma and platelets to packed red bloodcells in the first 6 hours of massive transfusion improves out-comes in a large multicenter study. Am J Surg 2009;197:565–70
62. Schuster KM, Davis KA, Lui FY, Maerz LL, Kaplan LJ. Thestatus of massive transfusion protocols in United States traumacenters: massive transfusion or massive confusion? Transfu-sion 2010;50:1545–51
63. Dirks J, Jorgensen H, Jensen CH, Ostrowski SR, Johansson PI.Blood product ratio in acute traumatic coagulopathy—effecton mortality in a Scandinavian level 1 trauma centre. ScandJ Trauma Resusc Emerg Med 2010;18:65
64. Scalea TM, Bochicchio KM, Lumpkins K, Hess JR, Dutton R,Pyle A, Bochicchio GV. Early aggressive use of fresh frozenplasma does not improve outcome in critically injured traumapatients. Ann Surg 2008;248:578–84
65. Snyder CW, Weinberg JA, McGwin G Jr, Melton SM, GeorgeRL, Reiff DA, Cross JM, Hubbard-Brown J, Rue LW 3rd, KerbyJD. The relationship of blood product ratio to mortality:survival benefit or survival bias? J Trauma 2009;66:358–62
66. Riskin DJ, Tsai TC, Riskin L, Hernandez-Boussard T, Purtill M,Maggio PM, Spain DA, Brundage SI. Massive transfusionprotocols: the role of aggressive resuscitation versus productratio in mortality reduction. J Am Coll Surg 2009;209:198–205
67. Stinger HK, Spinella PC, Perkins JG, Grathwohl KW, Salinas J,Martini WZ, Hess JR, Dubick MA, Simon CD, Beekley AC,Wolf SE, Wade CE, Holcomb JB. The ratio of fibrinogen to redcells transfused affects survival in casualties receiving massivetransfusions at an army combat support hospital. J Trauma2008;64:S79–85
68. Brenni M, Worn M, Bruesch M, Spahn DR, Ganter MT.Successful rotational thromboelastometry-guided treatment oftraumatic haemorrhage, hyperfibrinolysis and coagulopathy.Acta Anaesthesiol Scand 2010;54:111–7
69. Schochl H, Forster L, Woidke R, Solomon C, Voelckel W. Useof rotation thromboelastometry (ROTEM) to achieve successfultreatment of polytrauma with fibrinogen concentrate andprothrombin complex concentrate. Anaesthesia 2010;65:199–203
70. Schochl H, Nienaber U, Hofer G, Voelckel W, Jambor C,Scharbert G, Kozek-Langenecker S, Solomon C. Goal-directedcoagulation management of major trauma patients usingthromboelastometry (ROTEM(R))-guided administration of fi-brinogen concentrate and prothrombin complex concentrate.Crit Care 2010;14:R55
71. Schochl H, Nienaber U, Maegele M, Hochleitner G, PrimavesiF, Steitz B, Arndt C, Hanke A, Voelckel W, Solomon C.Transfusion in trauma: thromboelastometry-guided coagula-tion factor concentrate-based therapy versus standard freshfrozen plasma-based therapy. Crit Care 2011;15:R83
72. David J-S, Marchal V, Levrat A, Inaba K. Which is the mosteffective strategy: early detection of coagulopathy with throm-boelastometry or use of hemostatic factors or both? Crit Care2011;15:433
73. Nuttall GA, Oliver WC, Santrach PJ, Bryant S, Dearani JA,Schaff HV, Ereth MH. Efficacy of a simple intraoperativetransfusion algorithm for nonerythrocyte component utiliza-tion after cardiopulmonary bypass. Anesthesiology 2001;94:773–81
74. Rahe-Meyer N, Pichlmaier M, Haverich A, Solomon C, Win-terhalter M, Piepenbrock S, Tanaka KA. Bleeding managementwith fibrinogen concentrate targeting a high-normal plasmafibrinogen level: a pilot study. Br J Anaesth 2009;102:785–92
75. Dacey LJ, Munoz JJ, Baribeau YR, Johnson ER, Lahey SJ,Leavitt BJ, Quinn RD, Nugent WC, Birkmeyer JD, O’ConnorGT. Reexploration for hemorrhage following coronary arterybypass grafting: incidence and risk factors. Northern New EnglCardiovascular Disease Study group. Arch Surg 1998;133:442–7
76. Levi M, Cromheecke ME, de Jonge E, Prins MH, de Mol BJ,Briet E, Buller HR. Pharmacological strategies to decreaseexcessive blood loss in cardiac surgery: a meta-analysis ofclinically relevant endpoints. Lancet 1999;354:1940–7
77. Unsworth-White MJ, Herriot A, Valencia O, Poloniecki J, SmithEE, Murday AJ, Parker DJ, Treasure T. Resternotomy forbleeding after cardiac operation: a marker for increased mor-bidity and mortality. Ann Thorac Surg 1995;59:664–7
78. Sniecinski RM, Levy JH. Bleeding and management of coagu-lopathy. J Thora Cardio Surg 2011;142:662–7
79. Mell MW, O’Neil AS, Callcut RA, Acher CW, Hoch JR, TeferaG, Turnipseed WD. Effect of early plasma transfusion onmortality in patients with ruptured abdominal aortic aneu-rysm. Surgery 2010;148:955–62
80. Rahe-Meyer N, Solomon C, Winterhalter M, Piepenbrock S,Tanaka K, Haverich A, Pichlmaier M. Thromboelastometry-guided administration of fibrinogen concentrate for the treat-ment of excessive intraoperative bleeding in thoracoabdominalaortic aneurysm surgery. J Thorac Cardiovasc Surg 2009;138:694–702
81. Innerhofer P, Fries D, Margreiter J, Klingler A, Kuhbacher G,Wachter B, Oswald E, Salner E, Frischhut B, Schobersberger W.The effects of perioperatively administered colloids and crys-talloids on primary platelet-mediated hemostasis and clotformation. Anesth Analg 2002;95:858–65
82. Mittermayr M, Streif W, Haas T, Fries D, Velik-Salchner C,Klingler A, Oswald E, Bach C, Schnapka-Koepf M, InnerhoferP. Hemostatic changes after crystalloid or colloid fluid admin-istration during major orthopedic surgery: the role of fibrino-gen administration. Anesth Analg 2007;105:905–17
83. Fenger-Eriksen C, Jensen TM, Kristensen BS, Jensen KM,Tonnesen E, Ingerslev J, Sørensen B. Fibrinogen substitutionimproves whole blood clot firmness after dilution with hy-droxyethyl starch in bleeding patients undergoing radicalcystectomy: a randomized, placebo-controlled clinical trial.J Thromb Haemost 2009;7:795–802
84. Hazra S, Chilaka VN, Rajendran S, Konje JC. Massive postpar-tum haemorrhage as a cause of maternal morbidity in a largetertiary hospital. J Obstet Gynaecol 2004;24:519–20
85. Zhang WH, Alexander S, Bouvier-Colle MH, Macfarlane A.Incidence of severe pre-eclampsia, postpartum haemorrhageand sepsis as a surrogate marker for severe maternal morbidityin a European population-based study: the MOMS-B survey.BJOG 2005;112:89–96
86. Waterstone M, Bewley S, Wolfe C. Incidence and predictors ofsevere obstetric morbidity: case-control study. BMJ 2001;322:1089–93
87. Bell SF, Rayment R, Collins PW, Collis RE. The use offibrinogen concentrate to correct hypofibrinogenaemia rap-idly during obstetric haemorrhage. Int J Obstet Anesth 2010;19:218 –23
88. Luddington RJ. Thrombelastography/thromboelastometry.Clin Lab Haematol 2005;27:81–90
89. Holcomb JB. Traditional transfusion practices are changing.Crit Care 2010;14:162
90. Kalina U, Stohr HA, Bickhard H, Knaub S, Siboni SM, Man-nucci PM, Peyvandi F. Rotational thromboelastography formonitoring of fibrinogen concentrate therapy in fibrinogendeficiency. Blood Coagul Fibrinolysis 2008;19:777–83
91. Molinaro RJ, Szlam F, Levy JH, Fantz CR, Tanaka KA. Lowplasma fibrinogen levels with the Clauss method during antico-agulation with bivalirudin. Anesthesiology 2008;109:160–1
92. Fenger-Eriksen C, Moore GW, Rangarajan S, Ingerslev J, So-rensen B. Fibrinogen estimates are influenced by methods ofmeasurement and hemodilution with colloid plasma expand-ers. Transfusion 2010;50:2571–6
93. Solomon C, Cadamuro J, Ziegler B, Schochl H, Varvenne M,Sorensen B, Hochleitner G, Rahe-Meyer N. A comparison offibrinogen measurement methods with fibrin clot elasticity as-sessed by thromboelastometry, before and after administration offibrinogen concentrate in cardiac surgery patients. Transfusion2011;51:1695–1706
94. Kannel WB, Wolf PA, Castelli WP, D’Agostino RB. Fibrinogenand risk of cardiovascular disease. The Framingham Study.JAMA 1987;258:1183–6
95. Reinhart WH. Fibrinogen—marker or mediator of vasculardisease? Vasc Med 2003;8:211–6
Fibrinogen Management in Acquired Bleeding
February 2012 • Volume 114 • Number 2 www.anesthesia-analgesia.org 273

96. Spahn DR, Cerny V, Coats TJ, Duranteau J, Fernandez-Mondejar E, Gordini G, Stahel PF, Hunt BJ, Komadina R,Neugebauer E, Ozier Y, Riddez L, Schultz A, Vincent JL,Rossaint R. Management of bleeding following major trauma:a European guideline. Crit Care 2007;11:R17
97. Nielsen VG, Cohen BM, Cohen E. Effects of coagulation factordeficiency on plasma coagulation kinetics determined viathrombelastography: critical roles of fibrinogen and factors II,VII, X and XII. Acta Anaesthesiol Scand 2005;49:222–31
98. Fenger-Eriksen C, Jensen TM, Kristensen BS, Jensen KM,Tonnesen E, Ingerslev J, Sorensen B. Fibrinogen substitutionimproves whole blood clot firmness after dilution with hy-droxyethyl starch in bleeding patients undergoing radicalcystectomy: a randomized, placebo-controlled clinical trial.J Thromb Haemost 2009;7:795–802
Nominations Sought for FAER Mentoring Excellence in Research Award
FAER is seeking nominations for the annual FAER Mentoring Excellence in Research Award. This award was created to ensure that the value of outstanding mentors is recognized and to encourage, develop, and retain these valuable individuals in our specialty. The FAER Mentoring Excellence in Research Award recognizes mentorship rather than scientific accomplishment. Nominees must have mentored anesthesiologists or scientists who have worked in the U.S. and contributed significantly to the practice. The award is focused on the successful development of mentees, not the professional accomplishments of the mentor. Nominees should be superior mentors, seen as supporting the future of the specialty. An overview of the award and the nomination process and a nomination form are posted on FAER’s website at faer.org/about/MentorResearchAward.html. The nomination form and supporting materials are due by March 31. Please submit all nomination materials by email to Mary Schrandt at [email protected].
REVIEW ARTICLE
274 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA





























